-
7. Approaches to GlycemicTreatmentDiabetes Care 2015;38(Suppl.
1):S41S48 | DOI: 10.2337/dc15-S010
PHARMACOLOGICAL THERAPY FOR TYPE 1 DIABETES
Recommendations
c Most people with type 1 diabetes should be treated with
multiple-dose insulin(MDI) injections (three to four injections per
day of basal and prandial insulin)or continuous subcutaneous
insulin infusion (CSII). A
c Most people with type 1 diabetes should be educated in how to
match pran-dial insulin dose to carbohydrate intake, premeal blood
glucose, and antici-pated activity. E
c Most people with type 1 diabetes should use insulin analogs to
reduce hypo-glycemia risk. A
Insulin TherapyThere are excellent reviews to guide the
initiation and management of insulintherapy to achieve desired
glycemic goals (1,2,3). Although most studies of MDIversus pump
therapy have been small and of short duration, a systematic review
andmeta-analysis concluded that there were no systematic
differences in A1C or severehypoglycemia rates in children and
adults between the two forms of intensive in-sulin therapy (4). A
large randomized trial in type 1 diabetic patients with
nocturnalhypoglycemia reported that sensor-augmented insulin pump
therapy with thethreshold suspend feature reduced nocturnal
hypoglycemia, without increasingglycated hemoglobin values (5).
Overall, intensive management through pumptherapy/continuous
glucose monitoring and active patient/family participationshould be
strongly encouraged (68). For selected individuals who have
masteredcarbohydrate counting, education on the impact of protein
and fat on glycemicexcursions can be incorporated into diabetes
management (9).
The Diabetes Control and Complications Trial (DCCT) clearly
showed that intensiveinsulin therapy (three ormore injections per
day of insulin) or CSII (insulin pump therapy)was a key part of
improved glycemia and better outcomes (10,11). The studywas
carriedout with short- and intermediate-acting human insulins.
Despite better microvascularoutcomes, intensive insulin therapy was
associated with a high rate of severe hypogly-cemia (62 episodes
per 100 patient-years of therapy). Since the DCCT, a number of
rapid-acting and long-acting insulin analogs havebeendeveloped.
These analogs are associatedwith less hypoglycemia in type 1
diabetes, while matching the A1C lowering of humaninsulins
(1,12).
Recommended therapy for type 1 diabetes consists of the
following:1. Use MDI injections (three to four injections per day
of basal and prandial insulin)
or CSII therapy.2. Match prandial insulin to carbohydrate
intake, premeal blood glucose, and an-
ticipated physical activity.3. For most patients (especially
those at an elevated risk of hypoglycemia), use
insulin analogs.4. For patients with frequent nocturnal
hypoglycemia and/or hypoglycemia unawareness,
a sensor-augmented low glucose threshold suspend pump may be
considered.
PramlintidePramlintide, an amylin analog, is an agent that
delays gastric emptying, bluntspancreatic secretion of glucagon,
and enhances satiety. It is a U.S. Food and Drug
Suggested citation: American Diabetes Associa-tion. Approaches
to glycemic treatment. Sec. 7.In Standards ofMedical Care in
Diabetesd2015.Diabetes Care 2015;38(Suppl. 1):S41S48
2015 by the American Diabetes Association.Readers may use this
article as long as the workis properly cited, the use is
educational and notfor prot, and the work is not altered.
American Diabetes Association
Diabetes Care Volume 38, Supplement 1, January 2015 S41
POSITIO
NSTA
TEMEN
T
-
Administration (FDA)-approved therapyfor use in type 1 diabetes.
It has beenshown to induce weight loss and lowerinsulin dose;
however, it is only indi-cated in adults. Concurrent reductionof
prandial insulin dosing is required toreduce the risk of severe
hypoglycemia.
Investigational AgentsMetformin
Adding metformin to insulin therapy mayreduce insulin
requirements and improvemetabolic control in
overweight/obesepatients with poorly controlled type 1diabetes. In
a meta-analysis, metforminin type 1 diabetes was found to
reduceinsulin requirements (6.6 U/day, P ,0.001) and led to small
reductions inweight and total and LDL cholesterol butnot to
improved glycemic control (abso-lute A1C reduction 0.11%, P5 0.42)
(13).
Incretin-Based Therapies
Therapies approved for the treatment oftype 2 diabetes are
currently being eval-uated in type 1 diabetes. Glucagon-likepeptide
1 (GLP-1) agonists and dipep-tidyl peptidase 4 (DPP-4) inhibitors
arenot currently FDA approved for thosewith type 1 diabetes, but
are being stud-ied in this population.
SodiumGlucose Cotransporter 2 Inhibitors
Sodiumglucose cotransporter 2 (SGLT2)inhibitors provide
insulin-independentglucose lowering by blocking glucosereabsorption
in the proximal renal tubuleby inhibiting SGLT2. These agents
providemodest weight loss and blood pressurereduction. Although
there are two FDA-approved agents for use in patients withtype 2
diabetes, there are insufcientdata to recommend clinical use in
type 1diabetes at this time (14).
PHARMACOLOGICAL THERAPY FORTYPE 2 DIABETES
Recommendations
c Metformin, if not contraindicatedand if tolerated, is the
preferredinitial pharmacological agent fortype 2 diabetes. A
c In patients with newly diagnosedtype2 diabetes andmarkedly
symp-tomatic and/or elevated blood glu-cose levels or A1C, consider
initiatinginsulin therapy (with or withoutadditional agents). E
c If noninsulin monotherapy at max-imum tolerated dose does
not
achieve or maintain the A1C targetover 3 months, add a second
oralagent, a GLP-1 receptor agonist, orbasal insulin. A
c A patient-centered approachshould be used to guide choiceof
pharmacological agents. Con-siderations inc lude efcacy,cost,
potential side effects, weight,comorbidities, hypoglycemia risk,and
patient preferences. E
c Due to the progressive nature oftype 2 diabetes, insulin
therapy iseventually indicated for many pa-tients with type 2
diabetes. B
An updated American Diabetes Asso-ciation/European Association
for theStudy of Diabetes position statement(15) evaluated the data
and developedrecommendations, including advan-tages and
disadvantages, for antihyper-glycemic agents for type 2
diabeticpatients. A patient-centered approachis stressed, including
patient prefer-ences, cost and potential side effectsof each class,
effects on body weight,and hypoglycemia risk. Lifestyle
modi-cations that improve health (see Section4. Foundations of
Care) should be em-phasized along with any pharmacologi-cal
therapy.
Initial TherapyMost patients should begin with life-style
changes (lifestyle counseling,weight-loss education, exercise,
etc.).When lifestyle efforts alone have notachieved or maintained
glycemic goals,metformin monotherapy should beadded at, or soon
after, diagnosis, un-less there are contraindications or
intol-erance. Metformin has a long-standingevidence base for efcacy
and safety, isinexpensive, and may reduce risk of car-diovascular
events (16). In patients withmetformin intolerance or
contraindica-tions, consider an initial drug from otherclasses
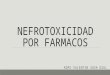
depicted in Fig. 7.1 under Dualtherapy and proceed accordingly.
Combination TherapyAlthough there are numerous trialscomparing
dual therapy with metforminalone, few directly compare drugs
asadd-on therapy. A comparative effec-tiveness meta-analysis (17)
suggeststhat overall each new class of noninsulinagents added to
initial therapy lowers
A1C around 0.91.1%. A comprehensivelisting, including the cost,
is available inTable 7.1.
If the A1C target is not achieved afterapproximately 3 months,
consider acombination of metformin and one ofthese six treatment
options: sulfonyl-urea, thiazolidinedione, DPP-4 inhibi-tors, SGLT2
inhibitors, GLP-1 receptoragonists, or basal insulin (Fig.
7.1).Drug choice is based on patient prefer-ences as well as
various patient, disease,and drug characteristics, with the goal
ofreducing blood glucose levels whileminimizing side effects,
especially hypo-glycemia. Figure 7.1 emphasizes drugscommonly used
in theU.S. and/or Europe.
Rapid-acting secretagogues (megliti-nides) may be used instead
of sulfonyl-ureas in patients with irregular mealschedules or who
develop late post-prandial hypoglycemia on a sulfonyl-urea. Other
drugs not shown in thegure (e.g., a-glucosidase inhibitors,
co-lesevelam, bromocriptine, pramlintide)may be tried in specic
situations, butare generally not favored due to modestefcacy, the
frequency of administra-tion, and/or side effects.
For all patients, consider initiatingtherapy with a dual
combination whenA1C is $9% to more expeditiouslyachieve the target
A1C level. Insulinhas the advantage of being effectivewhere other
agents may not be andshould be considered as part of anycombination
regimen when hyperglyce-mia is severe, especially if symptoms
arepresent or any catabolic features(weight loss, ketosis) are in
evidence.Consider initiating combination insulininjectable therapy
when blood glucoseis$300350 mg/dL (16.719.4 mmol/L)and/or A1C is
$1012%. As the pa-tients glucose toxicity resolves, theregimen can,
potentially, be subse-quently simplied.
Insulin TherapyMany patients with type 2 diabetes even-tually
require and benet from insulintherapy. Providers may wish to
considerregimen exibility when devising a planfor the initiation
and adjustment of insu-lin therapy in people with type 2
diabetes(Fig. 7.2). The progressive nature of type2 diabetes and
its therapies should beregularly and objectively explained to
pa-tients. Providers should avoid using insu-lin as a threat or
describing it as a failure
S42 Position Statement Diabetes Care Volume 38, Supplement 1,
January 2015
-
or punishment. Equipping patients withan algorithm for
self-titration of insulindoses based on self-monitoring of
bloodglucose (SMBG) improves glycemic con-trol in type 2 diabetic
patients initiatinginsulin (18).
Basal insulin alone is the most conve-nient initial insulin
regimen, beginningat 10 U or 0.10.2 U/kg, depending onthe degree of
hyperglycemia. Basal in-sulin is usually prescribed in
conjunctionwith metformin and possibly one addi-tional noninsulin
agent. If basal insulinhas been titrated to an acceptable fast-ing
blood glucose level, but A1C remainsabove target, consider
advancing to
combination injectable therapy (Fig. 7.2)to cover postprandial
glucose excur-sions. Options include adding a GLP-1receptor agonist
or mealtime insulin,consisting of one to three injections
ofrapid-acting insulin analog (lispro, as-part, or glulisine)
administered just be-fore eating. A less studied
alternative,transitioning from basal insulin totwice-daily premixed
(or biphasic) insu-lin analog (70/30 aspart mix, 75/25or 50/50
lispro mix), could also be con-sidered. Regular human insulin
andhuman NPH-Regular premixed formula-tions (70/30) are less costly
alternativesto rapid-acting insulin analogs and
premixed insulin analogs, respectively,but their pharmacodynamic
prolesmake them suboptimal for the coverageof postprandial glucose
excursions. Aless commonly used and more costlyalternative to
basalbolus therapywith multiple daily injections is CSII(insulin
pump). In addition to the sug-gestions provided for determiningthe
starting dose of mealtime insulinunder a basalbolus regimen,
anothermethod consists of adding up the totalcurrent insulin dose
and then providingone-half of this amount as basal andone-half as
mealtime insulin, the lattersplit evenly between three meals.
Figure 7.1Antihyperglycemic therapy in type 2 diabetes: general
recommendations (15). The order in the chart was determined by
historicalavailability and the route of administration, with
injectables to the right; it is not meant to denote any specic
preference. Potential sequences ofantihyperglycemic therapy for
patients with type 2 diabetes are displayed, with the usual
transition moving vertically from top to bottom (althoughhorizontal
movement within therapy stages is also possible, depending on the
circumstances). DPP-4-i, DPP-4 inhibitor; fxs, fractures; GI,
gastro-intestinal; GLP-1-RA, GLP-1 receptor agonist; GU,
genitourinary; HF, heart failure; Hypo, hypoglycemia; SGLT2-i,
SGLT2 inhibitor; SU, sulfonylurea;TZD, thiazolidinedione. *See ref.
15 for description of efcacy categorization. Consider starting at
this stage when A1C is$9%. Consider starting atthis stage when
blood glucose is$300350 mg/dL (16.719.4 mmol/L) and/or A1C
is$1012%, especially if symptomatic or catabolic features
arepresent, in which case basal insulin 1 mealtime insulin is the
preferred initial regimen. Usually a basal insulin (NPH, glargine,
detemir, degludec).Adapted with permission from Inzucchi et al.
(15).
care.diabetesjournals.org Position Statement S43
-
Table
7.1
Propertiesofavailable
glucose-loweringagen
tsin
theU.S.andEuropethat
mayguideindividualizedtreatm
entch
oicesin
patients
withtype2diabetes(15)
Class
Compound(s)
Cellularmechan
ism(s)
Prim
aryph
ysiologicalaction(s)
Advantage
sDisad
vantage
sCost*
Biguan
ides
cMetform
inActivates
AMP-kinase
(?other)
cHep
aticgluco
seproduction
cExtensive
experience
cGastrointestinalsideeffects(diarrhea
,ab
dominal
cram
ping)
Low
cNohyp
oglycem
iacLacticacidosisrisk
(rare)
cCVDeven
ts(U
KPDS)
cVitam
inB12de
cien
cycMultiple
contraindications:CKD
,acidosis,hyp
oxia,
deh
ydration,etc.
Sulfonylureas
2ndGen
eration
ClosesKATPchan
nelson
b-cellp
lasm
amem
branes
cInsulin
secretion
cExtensive
experience
cHyp
oglycem
iaLow
cGlyburide/gliben
clam
ide
cMicrovascularrisk
(UKP
DS)
cWeigh
tcGlip
izide
c?Blunts
myo
cardialischem
icpreco
nditioning
cGliclazide
cLow
durability
cGlim
epiride
Meg
litinides
(glin
ides)
cRep
aglin
ide
ClosesKATPchan
nelson
b-cellp
lasm
amem
branes
cInsulin
secretion
cP
ostprandialg
luco
seexcu
rsions
cHyp
oglycem
iaModerate
cNateg
linide
cDosingexibility
cWeigh
tc?Blunts
myo
cardialischem
icpreco
nditioning
cFreq
uen
tdosingsched
ule
TZDs
cPioglitazone
Activates
thenuclea
rtranscriptionfactor
PPAR-g
cInsulin
sensitivity
cNohyp
oglycem
iacWeigh
tLow
cRosiglitazone
cDurability
cEd
ema/hea
rtfailu
recHDL-C
cBonefractures
cTriglycerides
(pioglitazone)
cLD
L-C(rosiglitazone)
c?CVDeven
ts(PROactive,
pioglitazone)
c?MI(m
eta-an
alyses,rosiglitazone)
a-Glucosidase
inhibitors
cAcarbose
Inhibitsintestinal
a-glucosidase
cSlow
sintestinalcarboh
ydrate
digestion/absorption
cNohyp
oglycem
iacGen
erallymodestA1C
efcacy
Moderate
cMiglitol
cP
ostprandialg
luco
seexcu
rsions
c?CVDeven
ts(STO
P-NIDDM)
cGastrointestinal
sideeffects
(atulence,d
iarrhea
)
cNonsystem
ic
cFreq
uen
tdosingsched
ule
DPP
-4inhibitors
cSitagliptin
InhibitsDPP
-4activity,
increa
singpostprandial
active
incretin
(GLP-1,GIP)
concentrations
cInsulin
secretion
(glucose-dep
enden
t)cNohyp
oglycem
iacAngioed
ema/urticariaandothe
rim
mun
e-med
iatedde
rmatological
effects
High
cVild
aglip
tin
cGlucago
nsecretion
(glucose-dep
enden
t)
cWelltolerated
c?Acute
pan
crea
titis
cSaxagliptin
cLinag
liptin
c?Hea
rtfailu
rehospitalizations
cAlogliptin
Bile
acid
sequestran
tscColeseve
lam
Bindsbile
acidsin
intestinal
tract,increa
sing
hep
aticbile
acid
production
c?Hep
aticglucose
production
cNohyp
oglycem
iacGen
erallymodestA1C
efcacy
High
c?Incretin
leve
lscLD
L-C
cConstipation
cTriglycerides
cMay
ab
sorptionofo
ther
med
ications
Con
tinu
edon
p.S4
5
S44 Position Statement Diabetes Care Volume 38, Supplement 1,
January 2015
-
Table
7.1
Continued
Class
Compound(s)
Cellularmechan
ism(s)
Prim
aryph
ysiologicalaction(s)
Advantage
sDisad
vantage
sCost*
Dopam
ine-2
agonists
cBromocriptine(quickrelease)
Activates
dopam
inergic
receptors
cModulateshyp
othalam
icregu
lationofmetab
olism
cNohyp
oglycem
iacGen
erallymodestA1C
efcacy
High
cDizziness/synco
pe
cInsulin
sensitivity
c?CVDeven
ts(CyclosetSafety
Trial)
cNau
sea
cFatigu
ecRhinitis
SGLT2inhibitors
cCan
agli
ozin
InhibitsSG
LT2in
the
proximal
nep
hron
cBlocksgluco
sereab
sorption
bythekidney,increa
sing
gluco
suria
cNohyp
oglycem
iacGen
itourinaryinfections
High
cDap
agli
ozin
cWeigh
tcPo
lyuria
cEm
pagli
ozin
cVolumedep
letion/hyp
otension/
dizziness
cBloodpressure
cLD
L-C
cEffectiveat
allstage
sofT2
DM
cCreatinine(transien
t)
GLP-1
receptor
agonists
cExen
atide
Activates
GLP-1
receptors
cInsulin
secretion(glucose-
dep
enden
t)cNohyp
oglycem
iacGastrointestinal
sideeffects(nau
sea/
vomiting/diarrhea
)High
cExen
atideextended
release
cGlucago
nsecretion
(glucose-dep
enden
t)cHea
rtrate
cLiraglutide
cWeigh
t
c?Acu
tepan
crea
titis
cAlbiglutide
cSlowsgastricem
ptying
cPo
stprandialg
luco
seexcu
rsions
cC-cellh
yperplasia/med
ullary
thyroid
tumors
inan
imals
cLixisenatide
cSatiety
cSo
mecardiovascular
risk
factors
cInjectab
lecDulaglutide
cTrainingrequirem
ents
Amylin
mim
etics
cPram
lintide
Activates
amylin
receptors
cGlucago
nsecretion
cPo
stprandialglucose
excursions
cGen
erallymodestA1C
efcacy
High
cSatiety
cWeigh
tcGastrointestinal
sideeffects(nau
sea/
vomiting)
cHyp
oglycem
iaunless
insulin
dose
issimultan
eouslyreduced
cSlowsgastricem
ptying
cInjectab
lecFreq
uen
tdosingsched
ule
cTrainingrequirem
ents
Insulin
scRap
id-actingan
alogs
Activates
insulin
receptors
cGluco
sedisposal
cNea
rlyuniversal
response
cHyp
oglycem
iaVariable#
-Lispro
-Aspart
-Glulisine
cSh
ort-acting
-Human
Reg
ular
cInterm
ediate-acting
cWeigh
tgain
-Human
NPH
cBasal
insulin
analogs
cHep
aticglucose
production
cMicrovascularrisk
(UKPD
S)
c?Mitoge
niceffects
-Glargine
cInjectab
le
-Detem
ir
cTrainingrequirem
ents
-Deg
ludec
cOther
cTh
eoretically
unlim
ited
efcacy
cPa
tien
treluctan
ce
cPrem
ixed
(severaltypes)
CKD
,chronickidney
disea
se;CVD,cardiovasculardisea
se;GIP,g
lucose-dep
enden
tinsulin
otropicpep
tide;
HDL-C,H
DLcholesterol;LD
L-C,LDLcholesterol;MI,myo
cardialinfarction;PP
AR-g,p
eroxisome
proliferatoractivatedreceptorg;PR
Oactive
,Prospective
PioglitazoneClin
ical
TrialinMacrovascularEven
ts(30);STOP-NIDDM,S
tudyto
Prev
entNon-Insulin
-Dep
enden
tDiabetes
Mellitus(31);TZD,
thiazolid
ined
ione;
T2DM,typ
e2diabetes
mellitus;UKP
DS,UKProspective
Diabetes
Study(32,33
).Cyclosettrialofq
uick-releasebromocriptine(34).*Costisbased
onlowest-pricedmem
ber
oftheclass(see
ref.
15).Notlicen
sedintheU.S.Initialconcernsrega
rdingbladder
cancerrisk
aredecreasingaftersubsequen
tstudy.N
otlicen
sedinEu
ropefortype2diabetes.#Costishighlydep
enden
tontype/brand(analogs.
human
insulin
s)an
ddosage
.Adap
tedwithpermissionfrom
Inzucchie
tal.(15).
care.diabetesjournals.org Position Statement S45
-
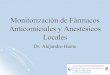
Figure 7.2 focuses solely on sequen-tial insulin strategies,
describing thenumber of injections and the relativecomplexity and
exibility of each stage.Once an insulin regimen is initiated,dose
titration is important, with adjust-ments made in both mealtime and
basalinsulins based on the prevailing bloodglucose levels and an
understanding ofthe pharmacodynamic prole of eachformulation
(pattern control).
Noninsulin agents may be continued,although sulfonylureas, DPP-4
inhibitors,and GLP-1 receptor agonists are typicallystopped once
more complex insulin regi-mens beyond basal are used. In
patientswith suboptimal blood glucose control,especially those
requiring increasing insu-lin doses, adjunctive use of
thiazolidine-diones (usually pioglitazone) or SGLT2
inhibitors may be helpful in improvingcontrol and reducing the
amount of in-sulin needed. Comprehensive educa-tion regarding SMBG,
diet, exercise,and the avoidance of and response tohypoglycemia are
critically important inany patient using insulin.
BARIATRIC SURGERY
Recommendations
c Bariatric surgery may be con-sidered for adults with BMI
.35kg/m2 and type 2 diabetes, espe-cially if diabetes or associated
co-morbidities are difcult to controlwith lifestyle and
pharmacologicaltherapy. B
c Patients with type 2 diabetes whohave undergone bariatric
surgery
need lifelong lifestyle supportand medical monitoring. B
c Although small trials have shownglycemic benet of bariatric
surgeryin patients with type 2 diabetes andBMI 3035 kg/m2, there is
currentlyinsufcient evidence to generallyrecommend surgery in
patientswith BMI,35 kg/m2. E
Bariatric and metabolic surgeries,either gastric banding or
proceduresthat involve resecting, bypassing, ortransposing sections
of the stomachand small intestine, can be effectiveweight-loss
treatments for severeobesity when performed as part of
acomprehensive weight-managementprogram with lifelong lifestyle
support
Figure 7.2Approach to starting and adjusting insulin in type 2
diabetes (15). FBG, fasting blood glucose; GLP-1-RA, GLP-1 receptor
agonist; hypo,hypoglycemia; mod., moderate; PPG, postprandial
glucose; #, number. Adapted with permission from Inzucchi et al.
(15).
S46 Position Statement Diabetes Care Volume 38, Supplement 1,
January 2015
-
andmedical monitoring. National guide-lines support
consideration for bariatricsurgery for people with type 2
diabeteswith BMI .35 kg/m2.
AdvantagesTreatment with bariatric surgery hasbeen shown to
achieve near- or com-plete normalization of glycemia 2
yearsfollowing surgery in 72% of patients(compared with 16% in a
matched con-trol group treated with lifestyle andpharmacological
interventions) (19). Astudy evaluated the long-term
(3-year)outcomes of surgical intervention(Roux-en-Y gastric bypass
or sleeve gas-trectomy) and intensive medical ther-apy (quarterly
visits, pharmacologicaltherapy, SMBG, diabetes education,
life-style counseling, and encouragement toparticipate in Weight
Watchers) com-pared with just intensive medical ther-apy on
achieving a target A1C #6%among obese patients with uncon-trolled
type 2 diabetes (mean A1C9.3%). This A1C target was achieved by38%
(P , 0.001) in the gastric bypassgroup, 24% (P5 0.01) in the sleeve
gas-trectomy group, and 5% in those receiv-ing medical therapy
(20). Diabetesremission rates tend to be higher withprocedures that
bypass portions of thesmall intestine and lower with proce-dures
that only restrict the stomach.
Younger age, shorter duration of type2 diabetes, lower A1C,
higher serum in-sulin levels, and nonuse of insulin haveall been
associated with higher remis-sion rates after bariatric surgery
(21).
Although bariatric surgery has beenshown to improve themetabolic
prolesof morbidly obese patients with type 1diabetes, the role of
bariatric surgery insuch patients will require larger and lon-ger
studies (22).
DisadvantagesBariatric surgery is costly and has asso-ciated
risks. Morbidity and mortalityrates directly related to the
surgeryhave decreased considerably in recentyears, with 30-day
mortality rates now0.28%, similar to those for
laparoscopiccholecystectomy (23). Outcomes varydepending on the
procedure and theexperience of the surgeon and center.Longer-term
concerns include vitaminand mineral deciencies, osteoporosis,and
rare but often severe hypoglycemiafrom insulin hypersecretion.
Cohort
studies attempting to match surgicaland nonsurgical subjects
suggest thatthe procedure may reduce longer-termmortality rates
(19). In contrast, a pro-pensity score-adjusted analysis of
older,severely obese patients in Veterans Af-fairs Medical Centers
found that bariatricsurgery was not associated with de-creased
mortality compared with usualcare (mean follow-up 6.7 years) (24).
Ret-rospective analyses and modeling studiessuggest that bariatric
surgery may becost-effective for patients with type 2diabetes, but
the results are largely de-pendent on assumptions about
thelong-term effectiveness and safety ofthe procedures (2527).
Understandingthe long-term benets and risks of bariat-ric surgery
in individuals with type 2 diabe-tes, especially those who are not
severelyobese, will require well-designed clinicaltrials, with
optimal medical therapy asthe comparator (28). Unfortunately,
suchstudies may not be feasible (29).
References1. DeWitt DE, Hirsch IB. Outpatient insulin ther-apy
in type 1 and type 2 diabetes mellitus: sci-entic review. JAMA
2003;289:225422642. American Diabetes Association.
IntensiveDiabetes Management. 4th ed. Wolfsdorf JI, Ed.Alexandria,
VA, American Diabetes Association,20093. Mooradian AD, Bernbaum M,
Albert SG. Nar-rative review: a rational approach to starting
in-sulin therapy. Ann Intern Med 2006;145:1251344. Yeh H-C, Brown
TT, Maruthur N, et al. Com-parative effectiveness and safety of
methods ofinsulin delivery and glucose monitoring for di-abetes
mellitus: a systematic review and meta-analysis. Ann Intern Med
2012;157:3363475. Bergenstal RM, Klonoff DC, Garg SK, et al.;ASPIRE
In-Home Study Group. Threshold-basedinsulin-pump interruption for
reduction of hy-poglycemia. N Engl J Med 2013;369:2242326. Wood JR,
Miller KM, Maahs DM, et al.; T1DExchange Clinic Network. Most youth
with type 1diabetes in the T1D Exchange clinic registry donot meet
American Diabetes Association or In-ternational Society for
Pediatric and AdolescentDiabetes clinical guidelines. Diabetes Care
2013;36:203520377. Kmietowicz Z. Insulin pumps improve controland
reduce complications in children with type1 diabetes. BMJ
2013;347:f51548. PhillipM, Battelino T, Atlas E, et al.
Nocturnalglucose control with an articial pancreas at adiabetes
camp. N Engl J Med 2013;368:8248339. Wolpert HA, Atakov-Castillo A,
Smith SA,Steil GM. Dietary fat acutely increases
glucoseconcentrations and insulin requirements inpatients with type
1 diabetes: implications forcarbohydrate-based bolus dose
calculation andintensive diabetes management. Diabetes
Care2013;36:810816
10. The Diabetes Control and ComplicationsTrial Research Group.
The effect of intensivetreatment of diabetes on the developmentand
progression of long-term complications ininsulin-dependent diabetes
mellitus. N Engl JMed 1993;329:97798611. Nathan DM, Cleary PA,
Backlund J-YC, et al.;Diabetes Control and Complications
Trial/Epi-demiology of Diabetes Interventions and Com-plications
(DCCT/EDIC) Study Research Group.Intensive diabetes treatment and
cardiovascu-lar disease in patients with type 1 diabetes.N Engl J
Med 2005;353:2643265312. Rosenstock J, Dailey G, Massi-Benedetti
M,Fritsche A, Lin Z, Salzman A. Reduced hypoglyce-mia risk with
insulin glargine: a meta-analysiscomparing insulin glargine with
human NPHinsulin in type 2 diabetes. Diabetes Care
2005;28:95095513. Vella S, Buetow L, Royle P, Livingstone S,Colhoun
HM, Petrie JR. The use of metforminin type 1 diabetes: a systematic
review of ef-cacy. Diabetologia 2010;53:80982014. Chiang JL,
KirkmanMS, Laffel LM, Peters AL;Type 1 Diabetes Sourcebook Authors.
Type 1diabetes through the life span: a position state-ment of the
American Diabetes Association. Di-abetes Care 2014;37:2034205415.
Inzucchi SE, Bergenstal RM, Buse JB, et al.Management of
hyperglycemia in type 2 diabe-tes, 2015: a patient-centered
approach. Updateto a position statement of the American Diabe-tes
Association and the European Associationfor the Study of Diabetes.
Diabetes Care 2015;38:14014916. Holman RR, Paul SK, Bethel MA,
MatthewsDR, Neil HA. 10-year follow-up of intensive glu-cose
control in type 2 diabetes. N Engl J Med2008;359:1577158917.
Bennett WL, Maruthur NM, Singh S, et al.Comparative effectiveness
and safety of medi-cations for type 2 diabetes: an update
includingnew drugs and 2-drug combinations. Ann InternMed
2011;154:60261318. Blonde L, Merilainen M, Karwe V, Raskin
P;TITRATE Study Group. Patient-directed titrationfor achieving
glycaemic goals using a once-dailybasal insulin analogue: an
assessment of two dif-ferent fasting plasma glucose targets - the
TITRATEstudy. Diabetes Obes Metab 2009;11:62363119. Sjostrom L,
Peltonen M, Jacobson P, et al.Association of bariatric surgery with
long-termremission of type 2 diabetes and with microvas-cular and
macrovascular complications. JAMA2014;311:2297230420. Schauer PR,
Bhatt DL, Kirwan JP, et al.;STAMPEDE Investigators. Bariatric
surgeryversus intensive medical therapy for diabetesd3-year
outcomes. N Engl J Med 2014;370:2002201321. Still CD, Wood GC,
Benotti P, et al. Preop-erative prediction of type 2 diabetes
remissionafter Roux-en-Y gastric bypass surgery: a retro-spective
cohort study. Lancet Diabetes Endocri-nol 2014;2:384522. Brethauer
SA, Aminian A, Rosenthal RJ,Kirwan JP, Kashyap SR, Schauer PR.
Bariatricsurgery improves the metabolic prole of mor-bidly obese
patients with type 1 diabetes. Di-abetes Care 2014;37:e51e5223.
Buchwald H, Estok R, Fahrbach K, Banel D,Sledge I. Trends in
mortality in bariatric surgery:
care.diabetesjournals.org Position Statement S47
-
a systematic review and meta-analysis. Surgery2007;142:62163224.
Maciejewski ML, Livingston EH, Smith VA,et al. Survival among
high-risk patients afterbariatric surgery. JAMA
2011;305:2419242625. Hoerger TJ, Zhang P, Segel JE, Kahn HS,Barker
LE, Couper S. Cost-effectiveness of bari-atric surgery for severely
obese adults with di-abetes. Diabetes Care 2010;33:1933193926.
Makary MA, Clark JM, Shore AD, et al. Med-ication utilization and
annual health care costsin patients with type 2 diabetes mellitus
beforeand after bariatric surgery. Arch Surg 2010;145:72673127.
Keating CL, Dixon JB,MoodieML, Peeters A,Playfair J, OBrien PE.
Cost-efcacy of surgicallyinduced weight loss for the management
oftype 2 diabetes: a randomized controlled trial.Diabetes Care
2009;32:580584
28. Wolfe BM, Belle SH. Long-term risks andbenets of bariatric
surgery: a research chal-lenge. JAMA 2014;312:1792179329.
Courcoulas AP, Goodpaster BH, Eagleton JK,et al. Surgical vs
medical treatments for type 2diabetes mellitus: a randomized
clinical trial.JAMA Surg 2014;149:70771530. Dormandy JA, Charbonnel
B, Eckland DJ,et al.; PROactive Investigators. Secondary
pre-vention of macrovascular events in patientswith type 2 diabetes
in the PROactive Study(PROspective pioglitAzone Clinical Trial In
mac-rovascular Events): a randomised controlled tri-al. Lancet
2005;366:1279128931. Chiasson JL, Gomis R, HanefeldM, Josse
RG,Karasik A, Laakso M; STOP-NIDDM TrialResearch Group. The
STOP-NIDDM Trial: an in-ternational study on the efcacy of an
alpha-glucosidase inhibitor to prevent type 2 diabetes
in a populationwith impaired glucose tolerance:rationale,
design, and preliminary screeningdata. Diabetes Care
1998;21:1720172532. UK Prospective Diabetes Study (UKPDS)Group.
Intensive blood-glucose control with sul-phonylureas or insulin
compared with conven-tional treatment and risk of complications
inpatients with type 2 diabetes (UKPDS 33). Lan-cet
1998;352:83785333. UK Prospective Diabetes Study (UKPDS)Group.
Effect of intensive blood-glucose controlwith metformin on
complications in overweightpatients with type 2 diabetes (UKPDS
34). Lan-cet 1998;352:85486534. Gaziano JM, Cincotta AH, OConnor
CM,et al. Randomized clinical trial of quick-releasebromocriptine
among patients with type 2 di-abetes on overall safety and
cardiovascular out-comes. Diabetes Care 2010;33:15031508
S48 Position Statement Diabetes Care Volume 38, Supplement 1,
January 2015