Embed Size (px)
DESCRIPTION
Living on the Peninsula article on stroke
Citation preview

36
An emergency dispatcher trips a local ambulance squad: A 58-year-old male caller says his arm feels numb and he’s dizzy; the dispatcher also advises the medics his speech is beginning to slur. A woman in her mid-70s complains she has the worst headache of her life and wants to sleep it off but her husband sees one side of her face is drooping. He immediately
calls 9-1-1. They both may be having
a stroke and
time of treatment is of the essence because “Time is brain.” “So far this year (Aug. 13) our providers have listed the
primary impression of a patient as stroke/CVA 86 times,” said Capt. Bryan Swanberg, Clallam County Fire District 3 medical safety officer. “We have been dispatched 13 times to a chief complaint of stoke from our dispatch.”
A stroke or cardiovascular accident occurs when a blood clot forms in any vessel in the brain (ischemic), blocking blood from delivering oxygen and nutrients and causing cell and tissue death; or when a blood vessel bursts (hemorrhagic) such as in an aneurysm, the ballooning of a vessel to the point of rupture. Brain tissue past the tear will starve for oxygen and die. Of the 800,000 Americans annually who have a stroke, about 140,000 of them will die. Stroke is the third-leading cause of death in the U.S. after heart attacks and cancer. About 87 percent of strokes are ischemic.
A stroke is a sudden, rapidly evolving event and always is a medical emergency. It can occur in any part of brain and is described as being left-sided, right-sided or brain stem. The residual effects of each differ because each portion is the seat of separate physical and cognitive functions and one side of the brain controls the opposite side of the body. Someone whose stroke happened on the right side of the brain, accord-ing to the American Stroke Association, could have left-side paralysis, vision problems, a quick, inquisitive behavioral style and memory loss. In a left-side stroke, there will be paralysis on the right side, speech and language problems, a slow, cautious behavioral style and memory loss. It’s doubly damaging when the stroke occurs in the brain stem because generally paralysis is bilateral and the patient also loses the ability to speak.
What’s key to ameliorating the damage is to dissolve the clot or repair the rupture within a three-hour window. “Time is brain” is the man-tra of all emergency medical personnel and the odds of a better recovery have improved on the Olympic Peninsula since Olympic Medical Center in Port Angeles (2010) and Jefferson Healthcare in Port Townsend (2009) partnered with the Swedish Neuroscience Institute in Seattle in its TeleStroke program which links stroke team experts to local emer-gency room physicians 24/7 for real time diagnosis and treatment.
Azella’s storyMost strokes occur in people over age
65 but can happen at any age, so stroke symptoms shouldn’t be ignored in any-one. Azella, who prefers to go by a single name, knows that better than most. Now living in Sequim, she suffered sud-den cardiac arrest at a friend’s house in Olympia in 2005 at age 52. A right-sided stroke followed in the hospital.
“My friend began CPR and I remember nothing of that weekend. I do know that the Big Guy had everything all planned because had this happened at home alone, I wouldn’t be here today,” Azella said, from her rocking chair. “I threw a clot in the hospital and I’d not be able to do the things I do without having been in the hospital when it happened. The doctor said if 10 people had the stroke I had, nine would be dead. People believe old wives’ tales that’s stroke only in the elderly, but stroke doesn’t know age, sex or color. A baby carried in the womb can experience a stroke,” Azella said.
She speaks with delibera-tion and clarity, a battle hard-won over the past seven years. “While I was in the hospital, someone told me I’d never walk again, but she did me a favor. ‘Well, you just watch,’ I said. I may not be graceful but I do walk.”
Weeks of inpatient rehabilitation were followed by months in intensive outpatient physical therapy with Azella relearning how to walk, as the stroke had partially paralyzed her left leg.
“I remember the first time I took a step, I screamed with joy! I had to relearn how to dress, to eat slowly and carefully because when I first had the stroke, swallowing was an is-sue.” Two more stints of rehab followed, the last in Sequim “because I was just not progressing the way I wanted to progress.”
Since then Azella’s heeded the advice of one of her thera-pists — just to live her life. She lives on disability and manages her activities of daily living with two part-time caretakers. Although she says her leg is “cooperative” now with a walker, her left arm isn’t and she’s unable to undress and dress or bathe without assistance. Azella gets together with friends, moves around downtown in her scooter chair, cooks and bakes, is active in the local chapter of the Brain Injury Association of Washington, and her church, the Olympic Unitarian Univer-salist Fellowship, and vocally advocates for the disabled.
“I may not like having had a stroke but I understand why,” Azella said. “Now I fight and advocate for the disabled and educate people about stroke.” She would like to start a stroke support group and give presentations about stroke; call her at 681-3191.
Azella said she and others with brain injury too often feel minimized by the rest of society regarding their personhood. “Just because we’re not whole doesn’t mean we’re not human. A lot of people believe once you become disabled, you have no rights.”
To dispel that misguided assumption at an official level, Azella is on the steering committee of the Disability Rights of Washington as a voice for change. She is vigorous in support-ing and educating the public and elected officials on strokes
Stroke Lives changed … not endedStory and photos by Patricia Morrison Coate
If you or someone with you has one or more of these signs, call without delay:
• Sudden numbness or weakness of the face, arm or leg, especially on one side of the body
• Sudden confusion, trouble speaking or understanding• Sudden trouble seeing in one or both eyes• Sudden trouble walking, dizziness, loss of balance or
coordination• Sudden, severe headache with no known cause
THINK F*A*S*T:Face: Does one side of the face droop?
Arms: Is one arm weak or numb?
Speech: Is the speech slurred?
Time: Time is critical. Call 9-1-1 immediately!
AzellA
36 living on the PeninSulA | FAll | SePteMBeR 2012

in particular and the rights of the disabled.“I have strong beliefs about the disabled,” she said. “They
should be encouraged to be as independent as they possibly can, for example, you only help me when I ask you for help. I am a champion for them. I may not like having to be, (be-cause all people should be treated equally), but it is what I do. People who are disabled do not want more than others; we only wish to have the same.”
A game changerLiz Klawitter, an occupational therapist specialized in low
vision rehabilitation with Olympic Medical Physical Therapy & Rehabilitation in Port Angeles, is a career veteran with 22 years of experience in helping people regain as much of their pre-stroke function as possible.
“Stroke is a game changer in many people’s lives,” Klawit-ter began. “We are so defined by what our bodies can do for us. If suddenly our physical bodies don’t function the way they used to, as with a stroke, we have to go through a process of redefining who we are now. That becomes a key element in the occupational therapeutic process.”
As with Azella, most of Klawitter’s stroke patients have had inpatient therapy prior to outpatient.
“An occupational therapist addresses the functional limitations created by the stroke in activities of daily living and works to restore or remediate functionality,” Klawitter explained. “The types of things I work on include physical skills, visual perceptual and cognitive skills. For example, a person may have weakness and lack of coordination of their arm and hand in using it to get dressed, feed themselves or open containers. Another limitation can be a visual-percep-tual impairment where a person is having difficulty visually attending to the side of the weakness. A functional visual assessment is an important part of the occupational therapy evaluation for a stroke patient.”
Klawitter explained that part of a person’s field of vision may be diminished or absent so he doesn’t “see” completely to that side. “He’s going to have trouble moving around and will be bumping into things.”
Visual-perceptual problems also can impair a person’s ability to read or see things accurately at close range. A nor-mal visual search strategy is typically from left to right, top
to bottom and is organized. “When someone’s had a stroke,
often I see a random, unorganized search strategy. It’s very discom-bobulating, as visual attention is a critical prerequisite for cognitive functioning. For example with reading, if a person is not attend-ing to his left side, he'll be missing the beginning of the lines; with the right side, he might only read half way across the line, so reading can be a real issue.”
The brain is remarkably adapt-able and in many instances, with repetition, new pathways can be formed to take over for damaged areas. Klawitter said much of her work revolves around retraining patients in compensation, which can include strategic scanning of
their environment for obstacles. “If they can mentally picture and anticipate their space,
they have much more confidence in moving about it,” Klawit-ter said.
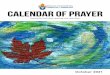
One of the aids she and patients use to improve their visual perception is the DynaVision, a large square wall-mounted board with lights that flash on in programmed patterns. Ac-cording to the company’s website, “For persons with visual and visuomotor impairment, the apparatus is used to train compensatory search strategies, improve oculomotor skills such as localization, fixation, gaze shift and tracking, increase peripheral visual awareness, visual attention and anticipa-tion, and improve eye-hand coordination and visuomotor reaction time.”
Klawitter has been using the DynaVision with 65-year-old Jim Kelly of Port Angeles for several sessions after his stroke and they’ve both seen his improvement.
“The response time is recorded for visual search speed and accuracy and the device can be programmed to challenge divided attention skills between your central and peripheral visual fields,” Klawitter said. “Visual and cognitive skills can improve because if you can increase visual attention to be able to see and respond to your environment, you have a chance of performing as independently as possible.”
Klawitter said she’s drawn to her patients for their deter-mination to overcome or adapt to their deficits.
“The people I work with are at a critical point in their lives. Although life has often changed for them, they come to see that it’s not over. Therapy can give them another shot at it.”
The gift of speechThe use of language to understand and be understood is at
the core of human communications. When a stroke damages a person’s language center, as in 25-40 percent of stroke survivors, he or she will have problems with any or all of these functions: speaking, comprehending, reading and writing, collectively known as aphasia. It’s a very lonely, bewildering and frustrating place to be.
“Speech therapy after a stroke treats aphasia, the loss of language skills in understanding others or expressing yourself.” said Jim Everrett, a speech-language pathologist, also with Olympic Medical Physical Therapy & Rehabilitation. “Someone may experience word-finding problems, have
difficulty following instructions. I do an evaluation to determine where the areas of need are.”
Speech-language disorders related to stroke and other brain injuries may include aphasia, apraxia, dysarthria and dysphagia.
“Apraxia is knowing what you want to say but the brain damage may not let the words out,” Everrett explained. “Dys-arthria or slurred speech may develop due to weakness in the mouth muscles. People often develop difficulty swallowing or dysphagia due to weakness in the mouth and throat. It’s rare that I would find a person without a mixture of conditions.”
Everrett designs an individualized treatment plan to work on all the speech-language deficits a stroke survivor has. Some of them include naming items in pictures, categorizing items by groups and giving synonyms and antonyms.
“I also evaluate and treat changes in cognitive communica-tion such as problem solving, numerical reasoning, organi-zational skills and multitasking,” Everrett said. “For example, there can be a change in orientation such as not knowing time, year and place for yourself. Sometimes people are aware of that and sometimes not. If it’s very disturbing to them, they may withdraw within. Therapy gives them confidence to practice and improvement can be made,” he said, noting the best window of opportunity for recovery is within three months post-stroke. However, good recovery can be made within a year after a stroke, he said.
Everrett related that one of his most memorable cases was a man in his mid-50s, a mechanic by trade, who’d lost his ability to speak after a stroke. He was his family’s sole breadwinner.
“Eventually, he was able to return to work and his family was so grateful that speech therapy allowed him to return to work. I find this a very rewarding job because I can help a person return to work, to the community to live a good quality life.”
Unfortunately, about 18 percent of Americans who have a stroke die from it. However, everyone understanding that “time is brain” and knowing the warning signs of stroke can have an important impact on the quality of life of the 82 percent who do survive a stroke by getting them to a hospital immediately. Remember F*A*S*T (see box) and act fast to save a life.
Did you know?• Some 800,000 people in the United States experi-
ence a new or recurrent stroke each year.• Stroke is the third-leading cause of death in the
U.S. and the leading cause of disability.• Stroke kills about 140,000 Americans each year.• 3 million Americans currently are disabled from
stroke.• In the U.S., stroke costs about $30 billion per
year in direct costs and loss of productivity.• Two-thirds of strokes occur in people over age 65
but they can occur at any age.• Strokes affect men more often than women,
although women are more likely to die from a stroke.
• Strokes affect black people more often and are more likely to be fatal.
occupational therapist liz Klawitter works with 65-year-old Jim Kelly of Port Angeles on the Dynavision to improve his visual perception.
living on the PeninSulA | FAll | SePteMBeR 2012 37