Embed Size (px)
Citation preview
Maternal, neonatal &
reproductive health
www.hrhhub.unsw.edu.au
Angela Dawson, Tara Howes, Natalie Gray and Elissa Kennedy
HUMAN RESOURCES FORHEALTH KNOWLEDGE HUB
Indonesia
HUMAN RESOURCES
FOR HEALTHin maternal, neonatal and reproductive
health at community level
A profile of Indonesia

© Human Resources for Health Knowledge Hub and Burnet Institute
on behalf of the Women’s and Children’s Health Knowledge Hub 2011
Suggested citation:
Dawson et al. 2011, Human resources for health in maternal, neonatal and reproductive health at community level: A profile of Indonesia, Human
Resources for Health Knowledge Hub and Burnet Institute, Sydney, Australia.
National Library of Australia Cataloguing-in-Publication entry
Dawson, Angela
Human resources for health in maternal, neonatal and reproductive health
at community level: A profile of Indonesia / Angela Dawson ... [et al.]
9780733429767 (pbk.)
Maternal health services--Indonesia--Personnel management.
Community health services--Indonesia--Personnel management.
Howes, Tara.
University of New South Wales. Human Resources for Health.
Gray, Natalie.
Kennedy, Elissa.
Burnet Institute. Women and Children’s Health Knowledge Hub.
362.198209598
Published by the Human Resources for Health Knowledge Hub of the
School of Public Health and Community Medicine at the University of
New South Wales.
Level 2, Samuels Building, School of Public Health and Community
Medicine, Faculty of Medicine, The University of New South Wales,
Sydney, NSW, 2052, Australia
Telephone: +61 2 9385 8464
Facsimile: +61 2 9385 1104
www.hrhhub.unsw.edu.au
Please contact us for additional copies of this publication, or send us your
email address and be the first to receive copies of our latest publications
in Adobe Acrobat PDF.
Design by Gigglemedia, Sydney, Australia.
The Human Resources for Health Knowledge HubThis technical report series has been produced by the Human Resources for Health Knowledge Hub of the School of Public Health and Community Medicine at the University of New South Wales.
Hub publications report on a number of significant issues in human resources for health (HRH), currently under the following themes:
� leadership and management issues, especially at district level
� maternal, neonatal and reproductive health workforce at the community level
� intranational and international mobility of health workers
� HRH issues in public health emergencies.
The HRH Hub welcomes your feedback and any questions you may have for its research staff. For further information on these topics as well as a list of the latest reports, summaries and contact details of our researchers, please visit www.hrhhub.unsw.edu.au or email [email protected]
1MNRH at community level: A profile of Indonesia Dawson et al.
CoNTENTS
2 Acronyms
3 Executive summary
4 Indonesia: selected HRH and MNRH indicators
5 Key background information
6 Overview of maternal, neonatal and reproductive health
7 Services and cadres at community level
8 Coverage and distribution
9 Competency
9 Supervision and scope of practice
12 Education and training
12 Teamwork
12 Country registration
12 HRH policy and plans
13 MNRH policy and plans
13 Remuneration and incentives
13 Key issues or barriers
14 Key initiatives
15 Critique
16 References
18 Appendix 1: Pre- and in-service education and training in Indonesia
19 Appendix 2: Country registration in Indonesia
20 Appendix 3: Country HRH and MNRH policies in Indonesia
LIST of TAbLES
5 Table 1. Key statistics
7 Table 2. Cadres involved in MNRH at community level in Indonesia
9 Table 3. Health worker distribution in Indonesia
10 Table 4. Distribution of the health workforce, village maternal huts and community clinics over the districts of Indonesia
2MNRH at community level: A profile of Indonesia Dawson et al.
ACRoNyMS
A note about the use of acronyms in this publication
Acronyms are used in both the singular and the plural, e.g. MDG (singular) and MDGs (plural). Acronyms are also used throughout the references and citations to shorten some organisations with long names.
AAAH Asia-Pacific Action Alliance on Human Resources for Health
ANMC Australian Nursing and Midwifery Council
AusAID Australian Agency for International Development
bDD bidan di desa (village-based midwife)
bPK Badan Pusat Statistik (Statistics Indonesia)
GDP gross domestic product
HRH human resources for health
JNPK Jaringan Nasional Pelatihan Klinis (Indonesia’s national training network for health providers)
MDG Millennium Development Goal
MNRH maternal, neonatal and reproductive health
MoH Ministry of Health
PNS pegawai negeri sibil (permanent employee)
PoDES Potensi Desa (Village Potential Statistics)
PTT pegawai tidak tetap (contractual employee)
USAID United States Agency for International Development
UNDESA United Nations Department of Economic and Social Affairs
USD$ United States dollar
WHo World Health Organization

3MNRH at community level: A profile of Indonesia Dawson et al.
Accurate and accessible information about the providers of maternal, neonatal and reproductive health (MNRH) services at the community level (how they are performing, managed, trained and supported) is central to workforce planning, personnel administration, performance management and policy making. Data on human resources for health (HRH) is also essential to ensure and monitor quality service delivery. Yet, despite the importance of such information, there is a paucity of available knowledge for decision making.
This highlights a particular challenge to determining the workforce required to deliver evidence-based interventions at community level to achieve Millennium Development Goal (MDG) 5 targets. This profile summarises the available information on the cadres working at community level in Indonesia; their diversity, distribution, supervisory structures, education and training, as well as the policy and regulations that govern their practice.
The profile provides baseline information that can inform policy and program planning by donors, multilateral agencies, non-government organisations and international health practitioners. Ministry of Health staff may also find the information from other countries useful in planning their own HRH initiatives.
The information was collected through a desk review and strengthened by input from key experts and practitioners in the country. Selected findings are summarised in the table below. There are key gaps in the collated information which may point to the need for consensus regarding what HRH indicators should be routinely collected and how such collection should take place at community level.
EXECUTIVE SUMMARy
This profile provides baseline information that can inform policy and program planning by donors, multilateral agencies, non-government organisations and international health practitioners.
4MNRH at community level: A profile of Indonesia Dawson et al.
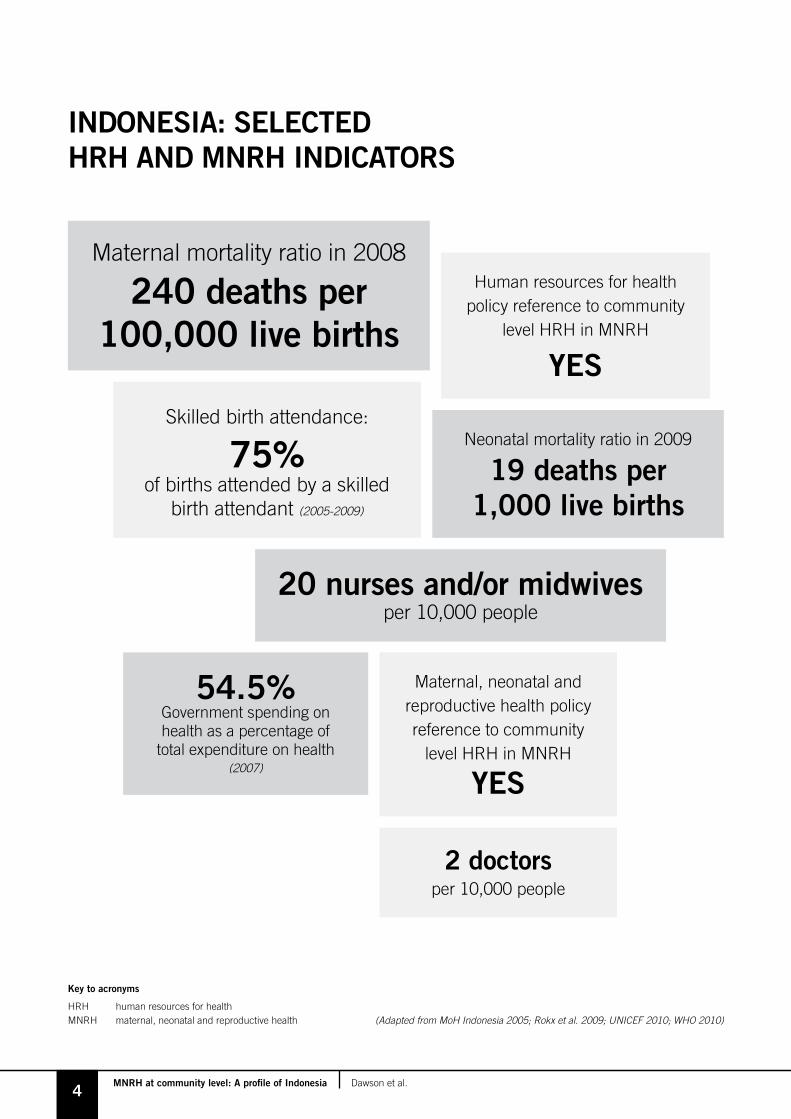
INDoNESIA: SELECTED HRH AND MNRH INDICAToRS
Maternal, neonatal and reproductive health policy reference to community
level HRH in MNRH
yES
Maternal mortality ratio in 2008
240 deaths per 100,000 live births
20 nurses and/or midwivesper 10,000 people
2 doctorsper 10,000 people
54.5% Government spending on health as a percentage of
total expenditure on health (2007)
Skilled birth attendance:
75% of births attended by a skilled
birth attendant (2005-2009)
Key to acronyms
HRH human resources for healthMNRH maternal, neonatal and reproductive health (Adapted from MoH Indonesia 2005; Rokx et al. 2009; UNICEF 2010; WHO 2010)
Neonatal mortality ratio in 2009
19 deaths per 1,000 live births
Human resources for health policy reference to community
level HRH in MNRH
yES
5MNRH at community level: A profile of Indonesia Dawson et al.
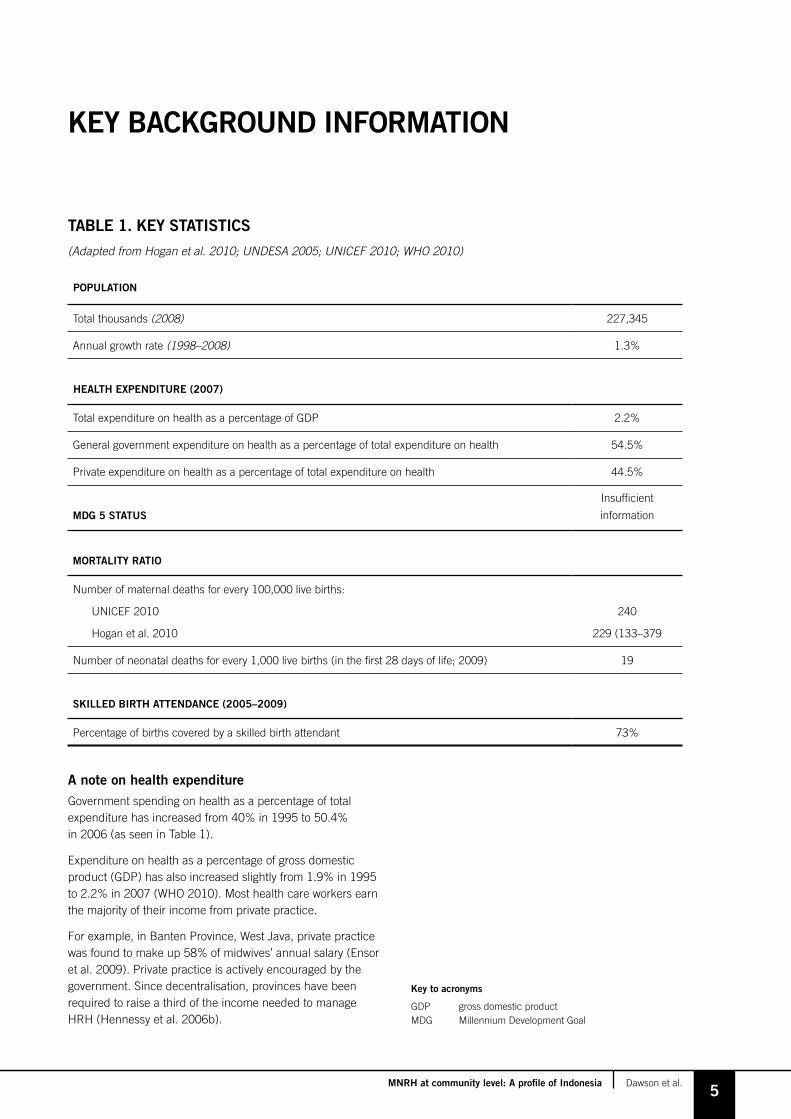
A note on health expenditure Government spending on health as a percentage of total expenditure has increased from 40% in 1995 to 50.4% in 2006 (as seen in Table 1).
Expenditure on health as a percentage of gross domestic product (GDP) has also increased slightly from 1.9% in 1995 to 2.2% in 2007 (WHO 2010). Most health care workers earn the majority of their income from private practice.
For example, in Banten Province, West Java, private practice was found to make up 58% of midwives’ annual salary (Ensor et al. 2009). Private practice is actively encouraged by the government. Since decentralisation, provinces have been required to raise a third of the income needed to manage HRH (Hennessy et al. 2006b).
KEy bACKGRoUND INfoRMATIoN
TAbLE 1. KEy STATISTICS
(Adapted from Hogan et al. 2010; UNDESA 2005; UNICEF 2010; WHO 2010)
PoPULATIoN
Total thousands (2008) 227,345
Annual growth rate (1998–2008) 1.3%
HEALTH EXPENDITURE (2007)
Total expenditure on health as a percentage of GDP 2.2%
General government expenditure on health as a percentage of total expenditure on health 54.5%
Private expenditure on health as a percentage of total expenditure on health 44.5%
MDG 5 STATUS
Insufficient
information
MoRTALITy RATIo
Number of maternal deaths for every 100,000 live births:
UNICEF 2010
Hogan et al. 2010
240
229 (133–379
Number of neonatal deaths for every 1,000 live births (in the first 28 days of life; 2009) 19
SKILLED bIRTH ATTENDANCE (2005–2009)
Percentage of births covered by a skilled birth attendant 73%
Key to acronyms
GDP gross domestic productMDG Millennium Development Goal

6MNRH at community level: A profile of Indonesia Dawson et al.
In 2007, 73% of births were attended by trained personnel in Indonesia (Rokx et al. 2009). The majority of births take place in either the woman’s home (64%) or a midwife’s home (28%)1, with home births more common in rural areas (Thind and Bannerjee 2004; Makowiecka et al. 2008).
There has been a general increase in facility-based births, with these increasing from 20% in 1997 to 46% in 2007. Amongst the poor, only 11% of women give birth in a facility, with two-thirds of these women choosing private clinics.
There is currently an aim to reduce the maternal mortality ratio to 125 for every 100,000 live births by 2010 (Thind and Bannerjee 2004). Midwife densities in Indonesia are 2.2 for every 1,000 people. This is comparable with countries such as Malaysia (3.4) and Sri Lanka (1.6), who have achieved high rates of coverage by a skilled birth attendant (Ronsmans et al. 2009). However, referral facilities have lagged behind these other countries (Shankar et al. 2008).
There is a high coverage of antenatal care, with 82% of women attending at least four antenatal visits. The majority of women (79.3%) receive antenatal care from a nurse, midwife or village midwife. Although 70% of Indonesian women receive a postnatal check-up within two days of birth, 16% of women receive no postnatal care (BPK and Macro International 2008).
The majority of public service providers are also employed in the private sector (between 60% and 70%). Dual practice was introduced in the 1970s to allow health care staff to supplement their low incomes.
Currently, there is a health information system in place to record public workforce data, but not information about private providers (Rokx et al. 2009). In 2001, the government started the process of decentralisation. This created some issues concerning health workforce planning and distribution – how it is carried out and who is responsible for different aspects of this planning. Decentralisation has led to a greater focus on district-based training and the opening of new training institutes.
Following decentralisation in 2001 the management of puskesmas (community health centres) and public hospitals was transferred to the provincial governments. Training institutes are currently producing more nurses and midwives than can be absorbed by the system, with places only being available for about 10% of midwifery graduates. The Healthy Indonesia Plan calls for a tripling of the total health workforce; this is not a major concern for nurse training, as large numbers are already in training (Rokx et al. 2009).
oVERVIEW of MATERNAL, NEoNATAL AND REPRoDUCTIVE HEALTH
Although 70% of Indonesian women receive a postnatal check-up within two days of birth, 16% of women receive no postnatal care.
1 In the 2007 Demographic Health Survey, the rate of home births was recorded as lower, with 53% of births taking place at home.
7MNRH at community level: A profile of Indonesia Dawson et al.
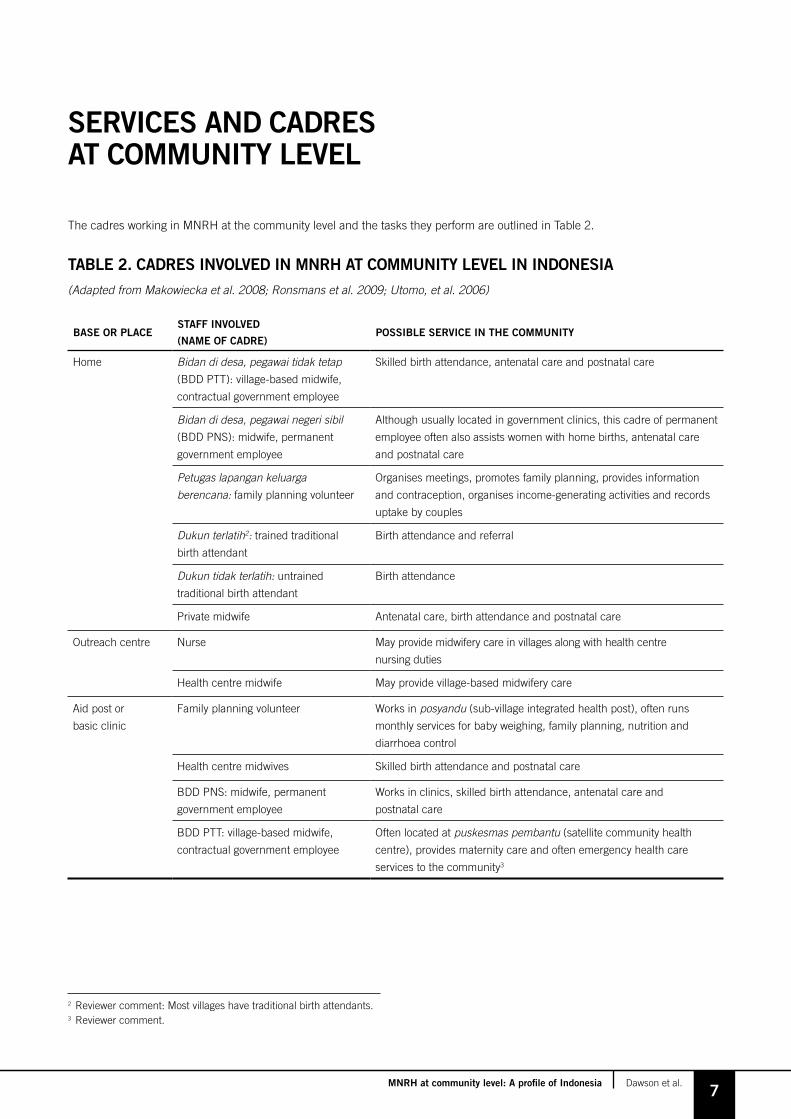
The cadres working in MNRH at the community level and the tasks they perform are outlined in Table 2.
SERVICES AND CADRES AT CoMMUNITy LEVEL
2 Reviewer comment: Most villages have traditional birth attendants.3 Reviewer comment.
TAbLE 2. CADRES INVoLVED IN MNRH AT CoMMUNITy LEVEL IN INDoNESIA
(Adapted from Makowiecka et al. 2008; Ronsmans et al. 2009; Utomo, et al. 2006)
bASE oR PLACESTAff INVoLVED
(NAME of CADRE)PoSSIbLE SERVICE IN THE CoMMUNITy
Home Bidan di desa, pegawai tidak tetap (BDD PTT): village-based midwife,
contractual government employee
Skilled birth attendance, antenatal care and postnatal care
Bidan di desa, pegawai negeri sibil (BDD PNS): midwife, permanent
government employee
Although usually located in government clinics, this cadre of permanent
employee often also assists women with home births, antenatal care
and postnatal care
Petugas lapangan keluarga berencana: family planning volunteer
Organises meetings, promotes family planning, provides information
and contraception, organises income-generating activities and records
uptake by couples
Dukun terlatih2: trained traditional
birth attendant
Birth attendance and referral
Dukun tidak terlatih: untrained
traditional birth attendant
Birth attendance
Private midwife Antenatal care, birth attendance and postnatal care
Outreach centre Nurse May provide midwifery care in villages along with health centre
nursing duties
Health centre midwife May provide village-based midwifery care
Aid post or
basic clinic
Family planning volunteer Works in posyandu (sub-village integrated health post), often runs
monthly services for baby weighing, family planning, nutrition and
diarrhoea control
Health centre midwives Skilled birth attendance and postnatal care
BDD PNS: midwife, permanent
government employee
Works in clinics, skilled birth attendance, antenatal care and
postnatal care
BDD PTT: village-based midwife,
contractual government employee
Often located at puskesmas pembantu (satellite community health
centre), provides maternity care and often emergency health care
services to the community3

8MNRH at community level: A profile of Indonesia Dawson et al.
CoVERAGE AND DISTRIbUTIoN
There are two main cadres of midwives. The first midwife is the pegawai negeri sibil (PNS; permanent) midwife. They are employed by the government on a permanent contract, are usually more experienced and work in clinics and villages. Due to their greater level of experience they often run their own private practice.
The cadre of pegawai tidak tetap (PTT; contract) midwife emerged from the government Village Midwife Program. PTT midwives are employed by the government on a temporary (but renewable) three-year contract. They are often recent graduates with little experience (Hull and Mosley 2009; Makowiecka et al. 2008)4.
There are no job descriptions attached to either cadre of midwives (Hennessy et al. 2006c). Of all village-based midwives, 46% are PTT and 54% are PNS. On the other hand, of those working in health centres, only 3% are PTT and 97% are PNS (Makowiecka et al. 2008). One study based in Serang and Pandeglang found that the largest group of midwifery service providers was village midwives (49% of the midwife workforce), followed by health centre midwives (26%), nurses (9%), public hospital midwives (7%) and other hospital midwives (4%).
Irrespective of numbers in each cadre, most women prefer to use midwives operating from their own private practice as they are considered to be more experienced (Makowiecka et al. 2008).
There is a maldistribution of staff between rural and urban areas. For example, in urban Java there is 1 doctor to 3,000 people, compared with 1 doctor for every 22,000 people in rural Java.5
This trend is changing with an increase in the ratios of doctors to population in rural and remote areas and decreasing ratios in urban areas. This could be the result of rural-urban migration (Rokx et al. 2009).
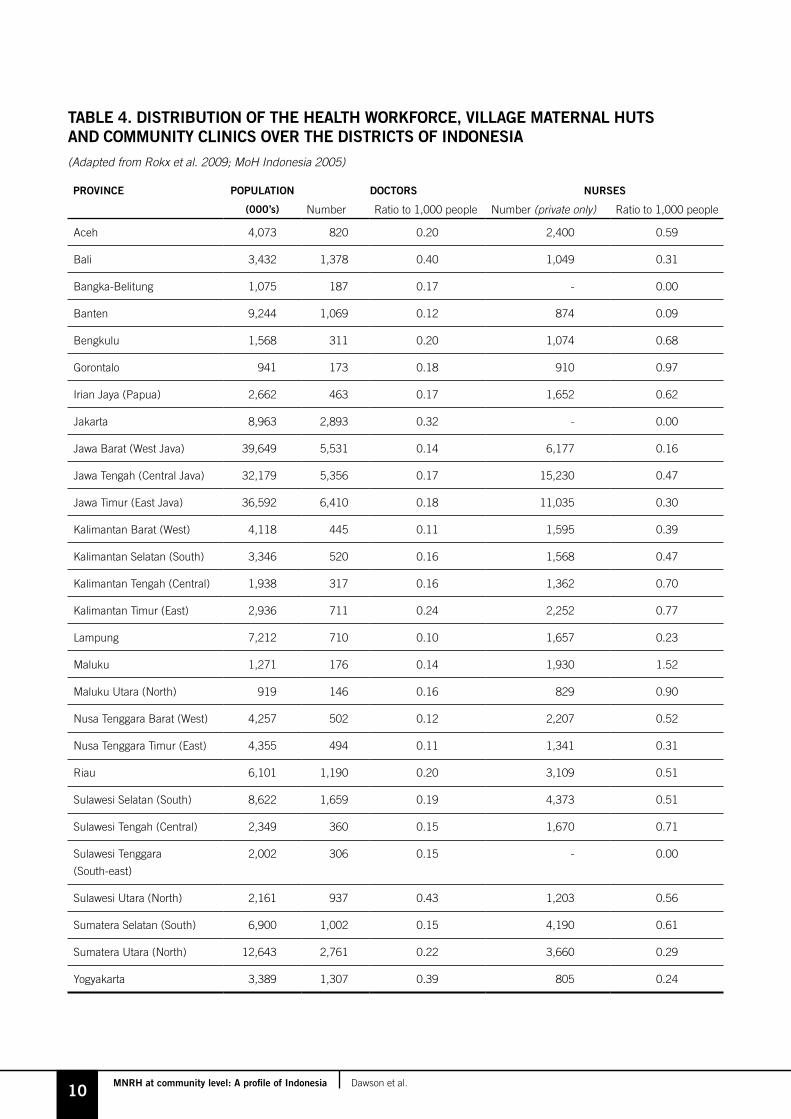
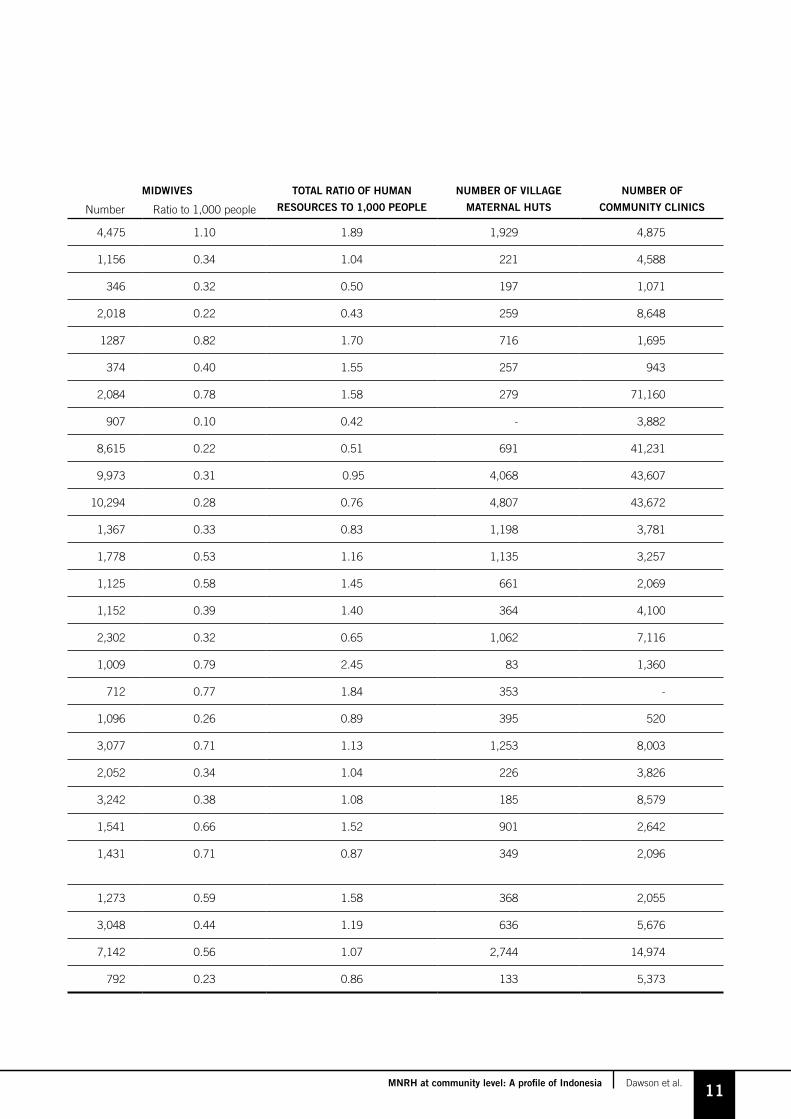
Table 4 (pp.10–11) outlines the provinces of Indonesia and the numbers of doctors, nurses, midwives, village maternal huts and community clinics in each province.
There is uncertainty about the number of health workers due to different methods of reporting. The PODES Survey (Potensi Desa; Village Potential Statistics) asks village leaders about the number of health professionals serving in their area and the Governance and Decentralisation Survey relies on information from district health offices. However, this was restricted to 139 out of 400 districts (Rokx et al. 2009). There is no central register of nurses which makes determining their number difficult (Hennessy et al. 2006b).
Midwives typically serve one or more villages, catering for 3,500 people, and attend 36 deliveries a year (Ensor et al. 2009). Midwives working in rural areas often have a large workload, with one midwife being responsible for up to five villages. Only 29% of villages have their own resident midwife (Immpact 2007). While this means that there is a higher ratio of midwife to population, it also means that midwives working in rural areas have the potential to bring in a higher income as they have a greater patient load (Ensor et al. 2009).
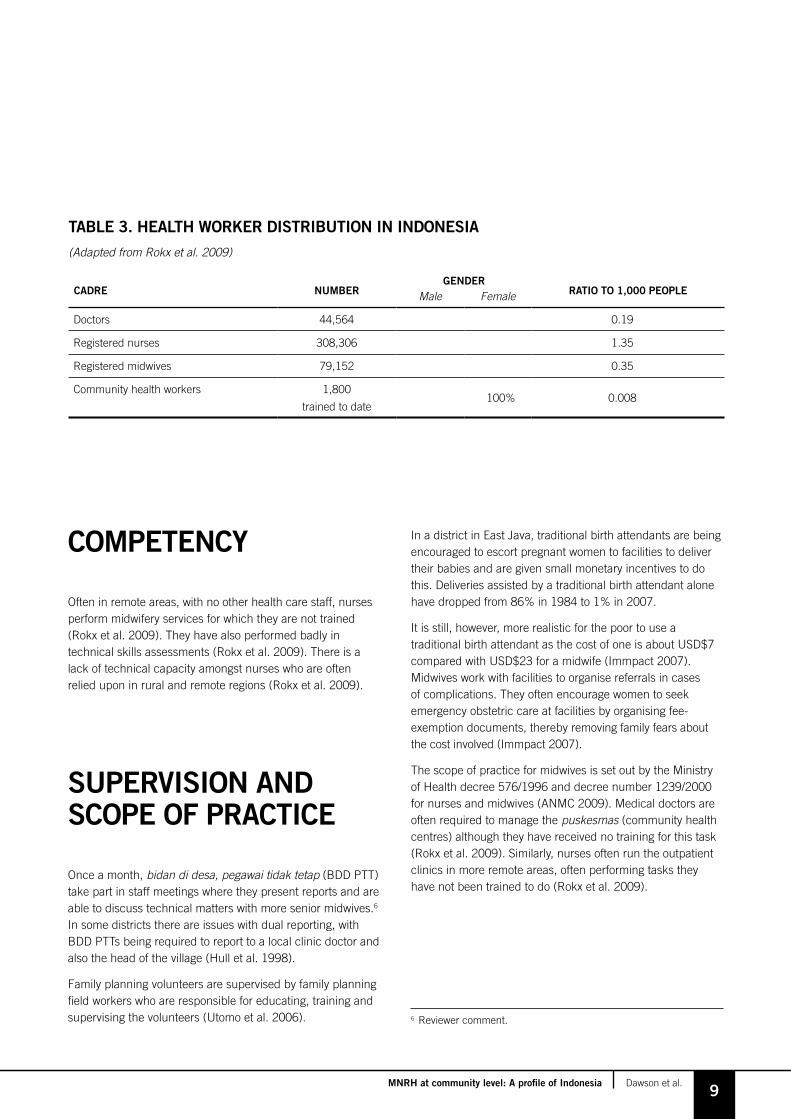
This section provides an overview of the numbers of health workers who may be engaged in MNRH at community level. Table 3 describes the distribution of this workforce according to gender and employment in the public and private sectors where available.
4 Reviewer comment: Village midwives may sometimes work in areas where there is a low population density and will therefore only care for a very small number of women each year, making it difficult to maintain professional skills.
5 Reviewer comment: There is also a great difference in health outcomes between different provinces, with eastern Indonesia having the highest burden of maternal and child mortality. For example, in Papua Province the maternal mortality ratio is 1,025 for every 100,000 live births.
9MNRH at community level: A profile of Indonesia Dawson et al.
TAbLE 3. HEALTH WoRKER DISTRIbUTIoN IN INDoNESIA
(Adapted from Rokx et al. 2009)
CADRE NUMbERGENDER
RATIo To 1,000 PEoPLEMale Female
Doctors 44,564 0.19
Registered nurses 308,306 1.35
Registered midwives 79,152 0.35
Community health workers 1,800
trained to date100% 0.008
CoMPETENCy
Often in remote areas, with no other health care staff, nurses perform midwifery services for which they are not trained (Rokx et al. 2009). They have also performed badly in technical skills assessments (Rokx et al. 2009). There is a lack of technical capacity amongst nurses who are often relied upon in rural and remote regions (Rokx et al. 2009).
SUPERVISIoN AND SCoPE of PRACTICE
Once a month, bidan di desa, pegawai tidak tetap (BDD PTT) take part in staff meetings where they present reports and are able to discuss technical matters with more senior midwives.6 In some districts there are issues with dual reporting, with BDD PTTs being required to report to a local clinic doctor and also the head of the village (Hull et al. 1998).
Family planning volunteers are supervised by family planning field workers who are responsible for educating, training and supervising the volunteers (Utomo et al. 2006).
In a district in East Java, traditional birth attendants are being encouraged to escort pregnant women to facilities to deliver their babies and are given small monetary incentives to do this. Deliveries assisted by a traditional birth attendant alone have dropped from 86% in 1984 to 1% in 2007.
It is still, however, more realistic for the poor to use a traditional birth attendant as the cost of one is about USD$7 compared with USD$23 for a midwife (Immpact 2007). Midwives work with facilities to organise referrals in cases of complications. They often encourage women to seek emergency obstetric care at facilities by organising fee-exemption documents, thereby removing family fears about the cost involved (Immpact 2007).
The scope of practice for midwives is set out by the Ministry of Health decree 576/1996 and decree number 1239/2000 for nurses and midwives (ANMC 2009). Medical doctors are often required to manage the puskesmas (community health centres) although they have received no training for this task (Rokx et al. 2009). Similarly, nurses often run the outpatient clinics in more remote areas, often performing tasks they have not been trained to do (Rokx et al. 2009).
6 Reviewer comment.
10MNRH at community level: A profile of Indonesia Dawson et al.
TAbLE 4. DISTRIbUTIoN of THE HEALTH WoRKfoRCE, VILLAGE MATERNAL HUTS AND CoMMUNITy CLINICS oVER THE DISTRICTS of INDoNESIA
(Adapted from Rokx et al. 2009; MoH Indonesia 2005)
PRoVINCE PoPULATIoN DoCToRS NURSES MIDWIVES ToTAL RATIo of HUMAN
RESoURCES To 1,000 PEoPLE
NUMbER of VILLAGE
MATERNAL HUTS
NUMbER of
CoMMUNITy CLINICS(000’s) Number Ratio to 1,000 people Number (private only) Ratio to 1,000 people Number Ratio to 1,000 people
Aceh 4,073 820 0.20 2,400 0.59 4,475 1.10 1.89 1,929 4,875
Bali 3,432 1,378 0.40 1,049 0.31 1,156 0.34 1.04 221 4,588
Bangka-Belitung 1,075 187 0.17 - 0.00 346 0.32 0.50 197 1,071
Banten 9,244 1,069 0.12 874 0.09 2,018 0.22 0.43 259 8,648
Bengkulu 1,568 311 0.20 1,074 0.68 1287 0.82 1.70 716 1,695
Gorontalo 941 173 0.18 910 0.97 374 0.40 1.55 257 943
Irian Jaya (Papua) 2,662 463 0.17 1,652 0.62 2,084 0.78 1.58 279 71,160
Jakarta 8,963 2,893 0.32 - 0.00 907 0.10 0.42 - 3,882
Jawa Barat (West Java) 39,649 5,531 0.14 6,177 0.16 8,615 0.22 0.51 691 41,231
Jawa Tengah (Central Java) 32,179 5,356 0.17 15,230 0.47 9,973 0.31 0.95 4,068 43,607
Jawa Timur (East Java) 36,592 6,410 0.18 11,035 0.30 10,294 0.28 0.76 4,807 43,672
Kalimantan Barat (West) 4,118 445 0.11 1,595 0.39 1,367 0.33 0.83 1,198 3,781
Kalimantan Selatan (South) 3,346 520 0.16 1,568 0.47 1,778 0.53 1.16 1,135 3,257
Kalimantan Tengah (Central) 1,938 317 0.16 1,362 0.70 1,125 0.58 1.45 661 2,069
Kalimantan Timur (East) 2,936 711 0.24 2,252 0.77 1,152 0.39 1.40 364 4,100
Lampung 7,212 710 0.10 1,657 0.23 2,302 0.32 0.65 1,062 7,116
Maluku 1,271 176 0.14 1,930 1.52 1,009 0.79 2.45 83 1,360
Maluku Utara (North) 919 146 0.16 829 0.90 712 0.77 1.84 353 -
Nusa Tenggara Barat (West) 4,257 502 0.12 2,207 0.52 1,096 0.26 0.89 395 520
Nusa Tenggara Timur (East) 4,355 494 0.11 1,341 0.31 3,077 0.71 1.13 1,253 8,003
Riau 6,101 1,190 0.20 3,109 0.51 2,052 0.34 1.04 226 3,826
Sulawesi Selatan (South) 8,622 1,659 0.19 4,373 0.51 3,242 0.38 1.08 185 8,579
Sulawesi Tengah (Central) 2,349 360 0.15 1,670 0.71 1,541 0.66 1.52 901 2,642
Sulawesi Tenggara
(South-east)
2,002 306 0.15 - 0.00 1,431 0.71 0.87 349 2,096
Sulawesi Utara (North) 2,161 937 0.43 1,203 0.56 1,273 0.59 1.58 368 2,055
Sumatera Selatan (South) 6,900 1,002 0.15 4,190 0.61 3,048 0.44 1.19 636 5,676
Sumatera Utara (North) 12,643 2,761 0.22 3,660 0.29 7,142 0.56 1.07 2,744 14,974
Yogyakarta 3,389 1,307 0.39 805 0.24 792 0.23 0.86 133 5,373
11MNRH at community level: A profile of Indonesia Dawson et al.
TAbLE 4. DISTRIbUTIoN of THE HEALTH WoRKfoRCE, VILLAGE MATERNAL HUTS AND CoMMUNITy CLINICS oVER THE DISTRICTS of INDoNESIA
(Adapted from Rokx et al. 2009; MoH Indonesia 2005)
PRoVINCE PoPULATIoN DoCToRS NURSES MIDWIVES ToTAL RATIo of HUMAN
RESoURCES To 1,000 PEoPLE
NUMbER of VILLAGE
MATERNAL HUTS
NUMbER of
CoMMUNITy CLINICS(000’s) Number Ratio to 1,000 people Number (private only) Ratio to 1,000 people Number Ratio to 1,000 people
Aceh 4,073 820 0.20 2,400 0.59 4,475 1.10 1.89 1,929 4,875
Bali 3,432 1,378 0.40 1,049 0.31 1,156 0.34 1.04 221 4,588
Bangka-Belitung 1,075 187 0.17 - 0.00 346 0.32 0.50 197 1,071
Banten 9,244 1,069 0.12 874 0.09 2,018 0.22 0.43 259 8,648
Bengkulu 1,568 311 0.20 1,074 0.68 1287 0.82 1.70 716 1,695
Gorontalo 941 173 0.18 910 0.97 374 0.40 1.55 257 943
Irian Jaya (Papua) 2,662 463 0.17 1,652 0.62 2,084 0.78 1.58 279 71,160
Jakarta 8,963 2,893 0.32 - 0.00 907 0.10 0.42 - 3,882
Jawa Barat (West Java) 39,649 5,531 0.14 6,177 0.16 8,615 0.22 0.51 691 41,231
Jawa Tengah (Central Java) 32,179 5,356 0.17 15,230 0.47 9,973 0.31 0.95 4,068 43,607
Jawa Timur (East Java) 36,592 6,410 0.18 11,035 0.30 10,294 0.28 0.76 4,807 43,672
Kalimantan Barat (West) 4,118 445 0.11 1,595 0.39 1,367 0.33 0.83 1,198 3,781
Kalimantan Selatan (South) 3,346 520 0.16 1,568 0.47 1,778 0.53 1.16 1,135 3,257
Kalimantan Tengah (Central) 1,938 317 0.16 1,362 0.70 1,125 0.58 1.45 661 2,069
Kalimantan Timur (East) 2,936 711 0.24 2,252 0.77 1,152 0.39 1.40 364 4,100
Lampung 7,212 710 0.10 1,657 0.23 2,302 0.32 0.65 1,062 7,116
Maluku 1,271 176 0.14 1,930 1.52 1,009 0.79 2.45 83 1,360
Maluku Utara (North) 919 146 0.16 829 0.90 712 0.77 1.84 353 -
Nusa Tenggara Barat (West) 4,257 502 0.12 2,207 0.52 1,096 0.26 0.89 395 520
Nusa Tenggara Timur (East) 4,355 494 0.11 1,341 0.31 3,077 0.71 1.13 1,253 8,003
Riau 6,101 1,190 0.20 3,109 0.51 2,052 0.34 1.04 226 3,826
Sulawesi Selatan (South) 8,622 1,659 0.19 4,373 0.51 3,242 0.38 1.08 185 8,579
Sulawesi Tengah (Central) 2,349 360 0.15 1,670 0.71 1,541 0.66 1.52 901 2,642
Sulawesi Tenggara
(South-east)
2,002 306 0.15 - 0.00 1,431 0.71 0.87 349 2,096
Sulawesi Utara (North) 2,161 937 0.43 1,203 0.56 1,273 0.59 1.58 368 2,055
Sumatera Selatan (South) 6,900 1,002 0.15 4,190 0.61 3,048 0.44 1.19 636 5,676
Sumatera Utara (North) 12,643 2,761 0.22 3,660 0.29 7,142 0.56 1.07 2,744 14,974
Yogyakarta 3,389 1,307 0.39 805 0.24 792 0.23 0.86 133 5,373
12MNRH at community level: A profile of Indonesia Dawson et al.
TEAMWoRK
There has been an increase in the number of medical training schools, especially since the process of decentralisation began. The regulation of education is still unclear. Current legislation is covered by Law 20/2003 (Law on the National Education System) and Law 29/2004 (Law on Medical Practice; Rokx et al. 2009). Law 20/2003 gives The Indonesian Medical Council responsibility for curriculum development, registration and certification of graduates.
The Ministry of Health Centre Workforce Education oversees all publicly owned nursing education above high school level which is often carried out through the poltekkes (polytechnic schools). Privately owned and other nursing and midwifery educational institutes are overseen by the National Accreditation Board for Higher Education. These two different agencies have different accreditation processes which are not in line with international standards (Rokx et al. 2009).
A new curriculum was introduced for medical students in 2005. The aim is to train doctors for work in primary health care clinics. The new curriculum outlines seven semesters of general teaching, followed by three semesters of clinical teaching. There is currently a plan to include a one-year internship at a primary health care clinic at the completion of training (Rokx et al. 2009).
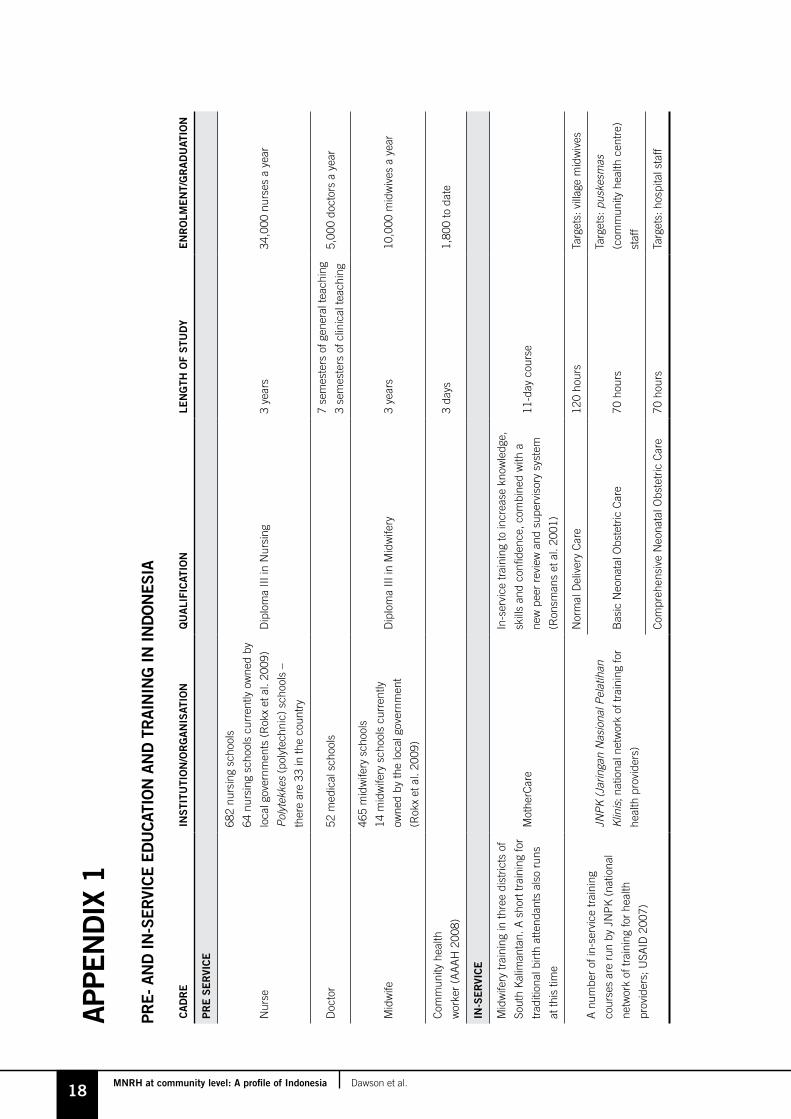
There are 682 nursing schools throughout the country offering a Diploma III in Nursing, with approximately 34,000 graduates each year (Rokx et al. 2009). Currently 39% of nurses have obtained a Diploma of Nursing, 1% have a degree and 60% have only secondary school education with on-the-job training (Hennessy et al. 2006b).
Between 1989 and 1996, under the BDD Program, one-year midwifery training was provided for graduates of the junior high school nursing program. Seventy-nine percent of public midwives currently working were trained under the one-year diploma program (Makowiecka et al. 2008). This was replaced in 1996 with a three-year diploma for high school graduates.
There are currently 465 midwifery schools throughout the country offering a Diploma III in Midwifery with approximately 10,000 graduates a year (Rokx et al. 2009). In 1997, an in-service training in the core competencies of maternal health was run. It covered topics such as care of normal birth, basic emergency obstetric procedures and post-abortion care (Hennessy et al. 2006c).
For more information on education and training, please refer to Appendix 1.
Posyandu (family planning volunteers at the village health-post level) are often invited to participate in monthly village coordination meetings and advise leaders when issues about family planning arise in villages (Utomo et al. 2006).
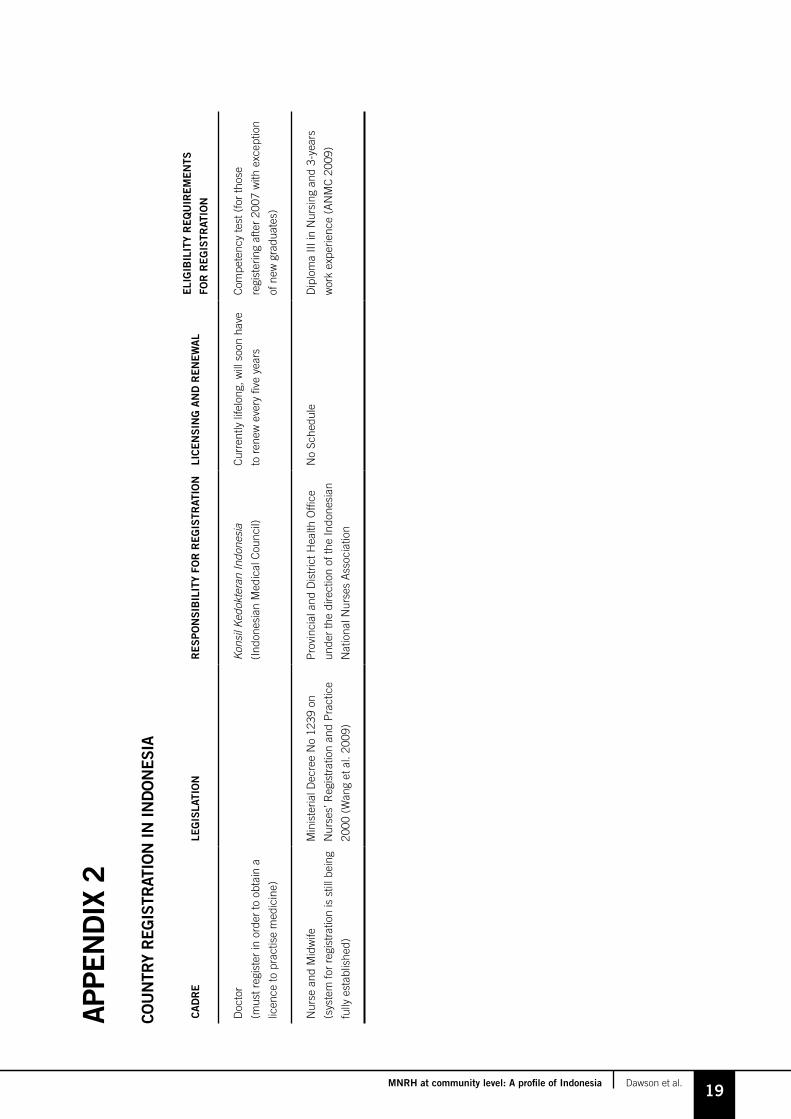
CoUNTRy REGISTRATIoN
There is no registration system for nurses and midwives which makes establishing numbers difficult (Rokx et al. 2009).
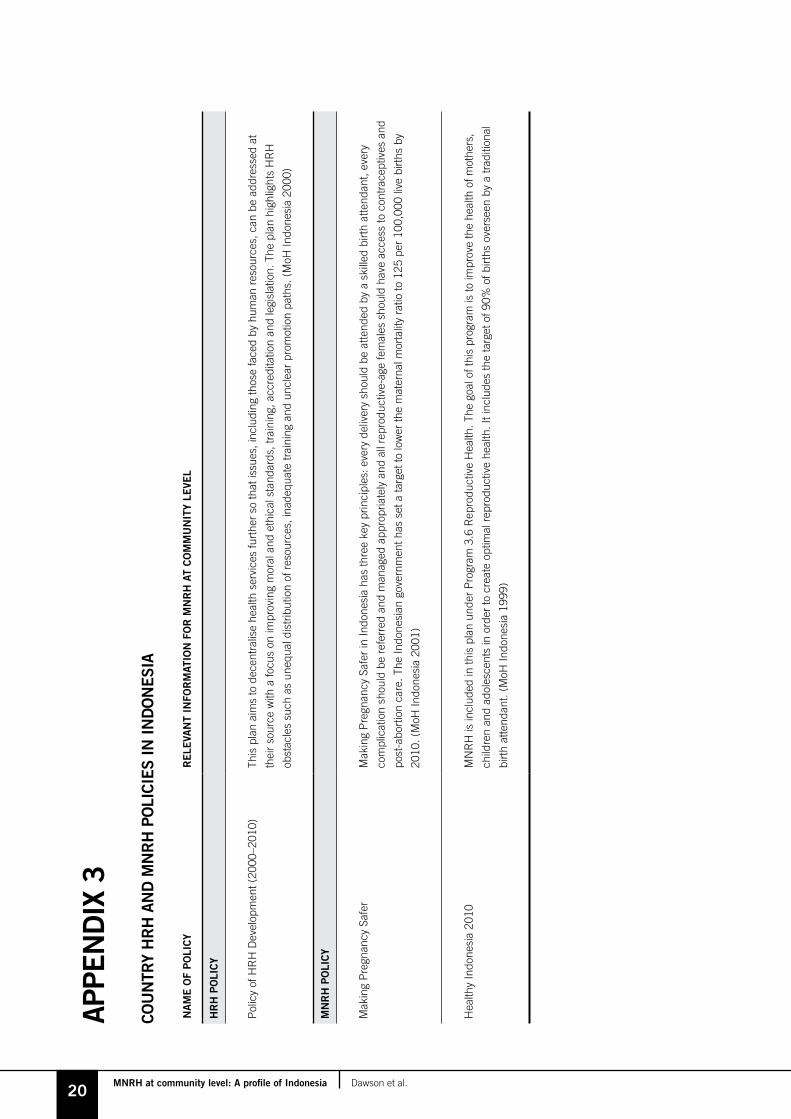
HRH PoLICy AND PLANS
Human resources for health in Indonesia are set out in the Policy for HRH Development 2000–2010 (MoH Indonesia 2000). Challenges of HRH and HRH plans are also set out in the country’s health strategy, Healthy Indonesia 2010 (Moh Indonesia 1999).
This plan aims to decentralise health services so that issues, including those faced by human resources, can be addressed at their source and to create a health workforce with ethical training standards and an improved structure of accreditation and legislation.
EDUCATIoN AND TRAINING
13MNRH at community level: A profile of Indonesia Dawson et al.
MNRH PoLICy AND PLANS
KEy ISSUES oR bARRIERS
MNRH priorities and plans have been outlined in the Making Pregnancy Safer Plan (MoH Indonesia 2001). This has three key principles: every delivery should be attended by a skilled birth attendant, every complication should be referred and managed appropriately, and all reproductive-age females should have access to contraceptives and post-abortion care. The Indonesian government has set a target to lower the maternal mortality ratio to 125 per 100,000 live births by 2010. Maternal child health and reproductive health is also included in the Healthy Indonesia 2010 strategy with a goal of one midwife to every 1,000 people (MoH Indonesia 1999).
REMUNERATIoN AND INCENTIVES
The incentives structure of the workforce is overseen by the national civil service agency, Badan Kepegawaian Negara (BKN). They oversee guidelines on hiring, firing and promotions, as well as policies on salary, retirement, transfer and management (Rokx et al. 2009). In May 2006, the Ministry of Health implemented a plan to provide incentives for serving in remote and very remote posts, such as increasing financial incentives and shortening service periods to six months in very remote areas and one year in remote areas (AAAH 2008). Incentives to keep doctors in puskesmas were deemed to be insufficient, and doctor numbers in these areas dropped by 30% between 1994 and 1998 (Rokx et al. 2009). The BDD Program (for village midwives) was more effective at keeping midwives in remote areas, and now midwives and nurses provide the majority of health services.
Midwives earn approximately USD$364 a month, while midwives in Banten province, Java, can earn USD$4,368 a year (including income from private practice). The top 10% of midwives earn USD$11,000 from private practice. Midwives with more than 15-years experience can earn twice as much as midwives who have less than five-years experience (Ensor et al. 2009). In Banten province, a survey found that, although the reason for becoming a midwife was almost evenly distributed between career/income (21%), community (27%) and family (25%), the main reasons for remaining a midwife were for career and/or incentives. Of the respondents, 71% listed career and incentives as the primary reason to remain in the profession (Ensor et al. 2009).
� Skill level of midwives trained under the Village Midwife Program (Shankar et al. 2008).
� Lack of emergency obstetric care system to back up referrals from the community level.
� Absenteeism of doctors during work hours (Rokx et al. 2009).
� Lack of midwives in very remote areas. Studies have found that the greatest hindrance to midwives moving to more remote areas is not income, as in many instances they are able to increase their income levels in remote areas due to lack of competition.
Reluctance to move has been found to be related to the relationships that midwives have established through marriage and building a family. They are reluctant to separate their ties with the community and move their family away from schools and work.
The solution may therefore be to attract midwives to work in these areas early in their careers before they have married and established ties in communities (Ensor et al. 2009).
� Lack of community confidence in young, recently trained BDD PTTs, who may be viewed as outsiders, combined with lack of training for midwives in building good relations with the community.7
� Doctors have inadequate skills in basic emergency and obstetric care.8
� Poor supportive supervision provided by district health officers to maintain health worker skills in remote areas.9
7 Reviewer comment: Some community midwives who have had excellent interpersonal skills have managed to engage with communities in areas where there had been low levels of community participation and interest in health care projects. This highlights the importance of including community engagement and interpersonal communication skills as a part of pre-service training.
8 Reviewer comment.9 Reviewer comment.

14MNRH at community level: A profile of Indonesia Dawson et al.
Bidan Di Desa Program (for village midwives)Launched in 1989, this program was a push by the government to increase the number of midwives in rural areas to assist with home births (Shankar et al. 2008). At the time, there were approximately 13,000 midwives in the country (Shiffman 2003). The aim was to send 54,000 midwives to rural areas, with each village having at least one midwife. Fifty thousand midwives were dispatched to rural areas as part of the program. Under this program, the births supervised by a skilled birth attendant rose from 22.5% in 1990 to 55% in 2003 (Makowiecka et al. 2008), women who received antenatal care rose from 57% in 1987 to 88% in 1998 (Shiffman 2003). By the end of the program the government reported that 96% of villages had a midwife (Thind and Bannerjee 2004).
The government created a new cadre – BDD PTT. Those who had completed the three-year nursing course were recruited into the one-year midwife training program and then deployed to rural posts on three-year contracts (with the possibility of renewal) where they would be provided with a polindes (public clinic) which would double as housing for the midwife and a birthing house. As a result, this cadre of workers were young and had little or no practical experience. The training course also included little practical clinical experience, and there were few clinics providing emergency obstetric care to which to refer women (Shankar et al. 2008).
There were conflicts in some areas between this new cadre and the existing midwives who, in general, were older, more experienced, receiving lower remuneration from the government, working in clinics and often running their own private practices (Hull et al. 1998). There have also been issues with retention of these midwives (Makowiecka et al. 2008). The MotherCare/Indonesia Project, along with the Ministry of Health and Indonesian Midwifery Association, went on to conduct in-service training for this new cadre between 1995 and 1999 in the district of South Kalimantan. This involved 11 days of training, follow-up workshops, clinical delivery experience and participation in a new peer support and supervision structure. A study found that those who were chosen to be part of the training achieved an average 71% skill score when tested, compared with an average score of 51% for those who did not participate (McDermott et al. 2001). In 1996, the one-year midwifery course was replaced by a three-year specialised midwifery course open to school leavers (Makowiecka et al. 2008). There was strong political support for this movement. President Suharto played an important role in the campaign, opening a number of conferences and seminars on the topic and stating
that a seven-year time frame was too long – progress would need to be made in shorter time (Shiffman 2003). This was also helped by a very active Minister for Women’s Roles who encouraged President Suharto’s involvement.
Health Insurance for the Poor Program (ASKESKIN)This scheme exempts the poorest families from paying for routine and emergency care. Under this scheme, midwives are paid to manage deliveries either in their own home or in the mother’s home. This increases the number of women able to access the service of the midwives and increases the practice and income of the midwives (Ronsmans et al. 2009).
family Planning ProgramThis program started in 1970 with the establishment of the Indonesian National Family Planning Coordination Board. Originally family planning field workers who were employed by the Board and later family planning volunteers would visit villages, educating communities about family planning through meetings and counselling. They would also distribute contraception and record family planning progress in villages. Through this program the attitude towards family planning changed from being a taboo topic to something that was essential (Utomo et al. 2006). Decentralisation in 2004 weakened the program and it no longer receives the political commitment it had before (Hull and Mosley 2009).
Partnership between midwives and traditional birth attendantsAn agreement was reached between midwives and traditional birth attendants in 2007 to work together to improve maternal health outcomes. Traditional birth attendants are now able to carry out their traditional cultural duties during the birth, while midwives are able to oversee the medical processes (UNICEF 2008).10
Establishment of community health centresDuring the 1980s, in a push by the government to implement the principles of primary health, Community Health Centres were established throughout the country with the aim of establishing one centre per 30,000 people.
They were staffed significantly by medical graduates on bonded placements for up to five years (Rokx et al. 2009; bonded placements were abolished as a result of increasing pressure from the Indonesian Medical Association in 2007 under law 512/2007).
KEy INITIATIVES
10 Information given by one reviewer.

15MNRH at community level: A profile of Indonesia Dawson et al.
DocumentationThere was a wide range of articles published on HRH for MNRH in Indonesia. This made this map less reliant on grey literature. Government reports and policies were less easily accessible, with key documents such as the Human Resources for Health Development Policy 2000–2010 (MoH Indonesia 2000) and the Making Pregnancy Safer Plan (MoH Indonesia 2001) not being located in the public domain. Peer-reviewed journal articles explored the issues of remuneration and incentives, private practice, education and training, cadres, government programs, barriers, supervision and team work (Ensor et al. 2009; Hennessy et al. 2006c; Hull and Mosley 2009; Makowiecka et al. 2008; Ronsmans et al. 2009; Shankar et al. 2008; Utomo, et al. 2006). This provided a much wider scope, compared with the other countries reviewed. There was an even representation of the public and private sector.
The main report used for this map was the World Bank report, Indonesia’s Doctors, Midwives and Nurses by Rokx et al. (2009). This gave detailed information about the rate of skilled birth attendance, workforce numbers, education and training and key barriers and issues. Information for this report was gathered using a number of methods, including the records of district health systems and interviews with community members and village and city block leaders (Rokx et al. 2009).
ReviewersThere were three reviewers for this map. The first reviewer is a representative from the United Nations Population Fund country office and provided updated information about what is currently occurring with programs in the country, provided corrections and highlighted the discrepancy in the maternal mortality ratio reported by different sources. The second reviewer is from the Burnet Institute’s country office.
They provided some in-depth comments and corrections on the implementation of the BDD Program. Information was also given by a midwifery expert from Indonesia currently undertaking a PhD in Australia who provided feedback on a number of different issues, in particular, the uneven distribution of health workers and the burden of maternal mortality and morbidity between different areas of the country. This reviewer also provided input on other HRH issues faced by the country.
CRITIQUE
A study found that those who were chosen to be part of the training achieved an average 71% skill score when tested, compared with an average score of 51% for those who did not participate.

16MNRH at community level: A profile of Indonesia Dawson et al.
AAAH 2008, Annual Review of HRH Situation in Asia-Pacific Region 2006–2007, Asia-Pacific Action Alliance for Human Resources for Health.
ANMC 2009, Country Profile – Indonesia, Australian Nursing and Midwifery Council, accessed 5 November 2009, <http://www.anmc.org.au/indonesia>.
Ensor, T Quayyum, Z, Nadjib, M and Sucahya, P 2009, ‘Level and determinants of incentives for village midwives in Indonesia’, Health Policy and Planning, vol. 24, no. 1, pp. 26–35.
Hennessy, D Hicks, C, Hilan, A and Kawonal, Y 2006a, ‘A methodology for assessing the professional development needs of nurses and midwives in Indonesia: paper 1 of 3’, Human Resources for Health, vol. 4, no. 1, p. 8.
Hennessy, D Hicks, C, Hilan, A and Kawonal, Y 2006b, ‘The Training and Development Needs of Nurses in Indonesia: paper 3 of 3’, Human Resources for Health, vol. 4, no. 10.
Hennessy, D Hicks, C and Koesno, H 2006c, ‘The training and development needs of midwives in Indonesia: paper 2 of 3’, Human Resources for Health, vol. 4, no. 1, p. 9.
Hogan, MC, Foreman, KJ, Naghavi, M, Ahn, SY, Wang, M, Makela, SM, Lopez, AD, Lozano, R and Murray, CJL 2010, ‘Maternal mortality for 181 countries, 1980–2008: a systematic analysis of progress towards Millennium Development Goal 5’, Lancet, vol. 375, no. 9726, pp. 1609–1623.
Hull, T and Mosley, H 2009, Revitalization of Family Planning in Indonesia, Government of Indonesia and the United Nations Population Fund.
Hull, T, Widayatun, Raharto, A and Setiawan, B 1998, ‘Village Midwives in Maluku’, policy paper, Center for Population and Manpower Studies, Jakarta, Indonesia.
Immpact 2007, Indonesia: Resident Midwives Help Avert Maternal Deaths When Financial Barriers are Removed, Immpact International, Population Reference Bureau.
Makowiecka, K, Achadi, E, Izati, Y and Ronsmans, C 2008, ‘Midwifery provision in two districts in Indonesia: how well are rural areas served?’, Health Policy and Planning, vol. 23, no. 1, pp. 67–75.
McDermott, J, Beck, D, Buffington, S, Annas, J, Supratikto, G, Prenggono, D, Ekonomi, D and Achadi, E 2001, ‘Two models of in-service training to improve midwifery skills:
how well do they work?’, Journal of Midwifery and Women’s Health, vol. 46, no. 4, pp. 217–25.
MoH Indonesia 1999, Health Development Plan Towards Healthy Indonesia 2010, Ministry of Health Indonesia, Jakarta.
MoH Indonesia 2000, Policy of HRH Development 2000-2010, policy paper in Indonesian language, Ministry of Health Indonesia, Jakarta.
MoH Indonesia 2001, National Strategic Plan on Making Pregnancy Safer (MPS) Indonesia 2001-2010, Ministry of Health Indonesia, Jakarta.
MoH Indonesia 2005, Indonesia Health Profile 2005, Ministry of Health Indonesia, Jakarta.
Rokx, C, Marzoeki, P, Harimurti, P and Satriawan, E 2009, Indonesia’s Doctors, Midwives and Nurses: Current Stock, Increasing Needs, Future Challenges and Options, World Bank, Jakarta.
Ronsmans, C, Endang, A, Gunawan, S, Zazri, A, McDermott, J, Koblinsky, M and Marshall, T 2001, ‘Evaluation of a Comprehensive Home-Based Midwifery Programme in South Kalimantan, Indonesia’, Tropical Medicine and International Health, vol. 6, no. 10, pp. 799–810.
Ronsmans, C, Scott, S, Qomariyah, SN, Achadi, E, Braunholtz, D, Marshall, T, Pambudi, E, Witten, KH and Graham, WJ 2009, ‘Professional assistance during birth and maternal mortality in two Indonesian districts’, Bulletin of the World Health Organization, vol. 87, no. 6, pp. 405–84.
Shankar, A, Sebayang, S, Guarenti, L, Utomo, B, Islam, M, Fauveau, V and Jalal, F 2008, ‘The village-based midwife programme in Indonesia’, The Lancet, vol. 371, no. 9620, pp. 1226–9.
Shiffman, J 2003, ‘Generating political will for safe motherhood in Indonesia’, Social Science and Medicine, vol. 56, no. 6, pp. 1197–207.
BPK and Macro International 2008, Demographic Health Survey 2007, Marylands, USA.
Thind, A and Banerjee K 2004, ‘Home deliveries in Indonesia: who provides assistance?’, Journal of Community Health, vol. 29, no. 4, pp. 285–303.
UNDESA 2005, The Millennium Development Goals Report, United Nations Department of Economic and Social Affairs, New York.
REfERENCES

17MNRH at community level: A profile of Indonesia Dawson et al.
UNICEF 2008, Traditional Birth Attendants and Midwives Partner for Women’s Health in Indonesia, <http://www.unicef.org/infobycountry/indonesia_43515.html>.
UNICEF 2010, Indonesia: Statistics, accessed 5 May 2011, <http://www.unicef.org/infobycountry/indonesia_statistics.html>.
USAID 2007, Health Services Program: 2007 Annual Report, report by JSI Research and Training Institute, Inc. for the United States Agency for International Development (USAID).
Utomo, ID, Arsyad, SS and Hasmi, EN 2006, ‘Village family planning volunteers in Indonesia: Their role in the family planning programme’, Reproductive Health Matters, vol. 14, no. 27, pp. 73–82.
Wang, H, McEuen, M, Mize, L, Cisek, C and Barraclough, A 2009, Private Sector Health Indonesia: A Desk Review, Health Systems 20/20 Project, Abt Associates Inc., Bethesda, MD.
WHO 2010, World Health Statistics 2010, World Health Organization, Geneva.
18MNRH at community level: A profile of Indonesia Dawson et al.
APPE
ND
IX 1
PRE-
AN
D IN
-SER
VICE
ED
UCA
TIo
N A
ND
TR
AIN
ING
IN IN
Do
NES
IA
CA
DR
EIN
STI
TUTI
oN
/oR
GA
NIS
ATIo
NQ
UA
LIfI
CAT
IoN
LEN
GTH
of
STU
Dy
EN
Ro
LME
NT/
GR
AD
UAT
IoN
PR
E S
ER
VIC
E
Nur
se
682
nurs
ing
scho
ols
64 n
ursi
ng s
choo
ls c
urre
ntly
ow
ned
by
loca
l gov
ernm
ents
(R
okx
et a
l. 20
09)
Poly
tekk
es (
poly
tech
nic)
sch
ools
–
ther
e ar
e 33
in th
e co
untr
y
Dip
lom
a III
in N
ursi
ng3
year
s34
,000
nur
ses
a ye
ar
Doc
tor
52 m
edic
al s
choo
ls7
sem
este
rs o
f gen
eral
teac
hing
3 se
mes
ters
of c
linic
al te
achi
ng5,
000
doct
ors
a ye
ar
Mid
wife
465
mid
wife
ry s
choo
ls
14 m
idw
ifery
sch
ools
cur
rent
ly
owne
d by
the
loca
l gov
ernm
ent
(Rok
x et
al.
2009
)
Dip
lom
a III
in M
idw
ifery
3 ye
ars
10,0
00 m
idw
ives
a y
ear
Com
mun
ity h
ealth
wor
ker
(AA
AH
200
8)3
days
1,80
0 to
dat
e
IN-S
ER
VIC
E
Mid
wife
ry tr
aini
ng in
thre
e di
stric
ts o
f
Sout
h K
alim
anta
n. A
sho
rt tr
aini
ng fo
r
trad
ition
al b
irth
atte
ndan
ts a
lso
runs
at th
is ti
me
Mot
herC
are
In-s
ervi
ce tr
aini
ng to
incr
ease
kno
wle
dge,
skill
s an
d co
nfide
nce,
com
bine
d w
ith a
new
pee
r re
view
and
sup
ervi
sory
sys
tem
(Ron
sman
s et
al.
2001
)
11-d
ay c
ours
e
A n
umbe
r of
in-s
ervi
ce tr
aini
ng
cour
ses
are
run
by J
NP
K (
natio
nal
netw
ork
of tr
aini
ng fo
r he
alth
prov
ider
s; U
SAID
200
7)
JNPK
(Jar
inga
n N
asio
nal P
elat
ihan
Kl
inis
; nat
iona
l net
wor
k of
trai
ning
for
heal
th p
rovi
ders
)
Nor
mal
Del
iver
y C
are
120
hour
sTa
rget
s: v
illag
e m
idw
ives
Bas
ic N
eona
tal O
bste
tric
Car
e70
hou
rs
Targ
ets:
pus
kesm
as
(com
mun
ity h
ealth
cen
tre)
staf
f
Com
preh
ensi
ve N
eona
tal O
bste
tric
Car
e70
hou
rsTa
rget
s: h
ospi
tal s
taff
19MNRH at community level: A profile of Indonesia Dawson et al.
APPE
ND
IX 2
CoU
NTR
y R
EGIS
TRAT
IoN
IN IN
Do
NES
IA
CA
DR
ELE
GIS
LATI
oN
RE
SP
oN
SIb
ILIT
y fo
R R
EG
ISTR
ATIo
NLI
CE
NS
ING
AN
D R
EN
EW
AL
ELI
GIb
ILIT
y R
EQ
UIR
EM
EN
TS
foR
RE
GIS
TRAT
IoN
Doc
tor
(mus
t reg
iste
r in
ord
er to
obt
ain
a
licen
ce to
pra
ctis
e m
edic
ine)
Kons
il Ke
dokt
eran
Indo
nesi
a (I
ndon
esia
n M
edic
al C
ounc
il)
Cur
rent
ly li
felo
ng, w
ill s
oon
have
to r
enew
eve
ry fi
ve y
ears
Com
pete
ncy
test
(fo
r th
ose
regi
ster
ing
afte
r 20
07 w
ith e
xcep
tion
of n
ew g
radu
ates
)
Nur
se a
nd M
idw
ife
(sys
tem
for
regi
stra
tion
is s
till b
eing
fully
est
ablis
hed)
Min
iste
rial D
ecre
e N
o 12
39 o
n
Nur
ses’
Reg
istr
atio
n an
d P
ract
ice
2000
(W
ang
et a
l. 20
09)
Pro
vinc
ial a
nd D
istr
ict H
ealth
Offi
ce
unde
r th
e di
rect
ion
of th
e In
done
sian
Nat
iona
l Nur
ses
Ass
ocia
tion
No
Sche
dule
Dip
lom
a III
in N
ursi
ng a
nd 3
-yea
rs
wor
k ex
perie
nce
(AN
MC
200
9)
20MNRH at community level: A profile of Indonesia Dawson et al.
APPE
ND
IX 3
CoU
NTR
y H
RH
AN
D M
NR
H P
oLI
CIES
IN IN
Do
NES
IA
NA
ME
of
Po
LIC
yR
ELE
VAN
T IN
foR
MAT
IoN
fo
R M
NR
H A
T C
oM
MU
NIT
y LE
VEL
HR
H P
oLI
Cy
Pol
icy
of H
RH
Dev
elop
men
t (20
00–2
010)
This
pla
n ai
ms
to d
ecen
tral
ise
heal
th s
ervi
ces
furt
her
so th
at is
sues
, inc
ludi
ng th
ose
face
d by
hum
an r
esou
rces
, can
be
addr
esse
d at
thei
r so
urce
with
a fo
cus
on im
prov
ing
mor
al a
nd e
thic
al s
tand
ards
, tra
inin
g, a
ccre
dita
tion
and
legi
slat
ion.
The
pla
n hi
ghlig
hts
HR
H
obst
acle
s su
ch a
s un
equa
l dis
trib
utio
n of
res
ourc
es, i
nade
quat
e tr
aini
ng a
nd u
ncle
ar p
rom
otio
n pa
ths.
(M
oH In
done
sia
2000
)
MN
RH
Po
LIC
y
Mak
ing
Pre
gnan
cy S
afer
Mak
ing
Pre
gnan
cy S
afer
in In
done
sia
has
thre
e ke
y pr
inci
ples
: eve
ry d
eliv
ery
shou
ld b
e at
tend
ed b
y a
skill
ed b
irth
atte
ndan
t, ev
ery
com
plic
atio
n sh
ould
be
refe
rred
and
man
aged
app
ropr
iate
ly a
nd a
ll re
prod
uctiv
e-ag
e fe
mal
es s
houl
d ha
ve a
cces
s to
con
trac
eptiv
es a
nd
post
-abo
rtio
n ca
re. T
he In
done
sian
gov
ernm
ent h
as s
et a
targ
et to
low
er th
e m
ater
nal m
orta
lity
ratio
to 1
25 p
er 1
00,0
00 li
ve b
irths
by
2010
. (M
oH In
done
sia
2001
)
Hea
lthy
Indo
nesi
a 20
10M
NR
H is
incl
uded
in th
is p
lan
unde
r P
rogr
am 3
.6 R
epro
duct
ive
Hea
lth. T
he g
oal o
f thi
s pr
ogra
m is
to im
prov
e th
e he
alth
of m
othe
rs,
child
ren
and
adol
esce
nts
in o
rder
to c
reat
e op
timal
rep
rodu
ctiv
e he
alth
. It i
nclu
des
the
targ
et o
f 90%
of b
irths
ove
rsee
n by
a tr
aditi
onal
birt
h at
tend
ant.
(MoH
Indo
nesi
a 19
99)

THE KNoWLEDGE HUbS foR HEALTH INITIATIVE
The Human Resources for Health Knowledge
Hub is one of four hubs established by
AusAID in 2008 as part of the Australian
Government’s commitment to meeting the
Millennium Development Goals and improving
health in the Asia and Pacific regions.
All four Hubs share the common goal of
expanding the expertise and knowledge
base in order to help inform and guide
health policy.
Human Resource for Health Knowledge Hub, University of New South Wales
Some of the key thematic areas for this Hub include governance, leadership and management; maternal, neonatal and reproductive health workforce; public health emergencies; and migration. www.hrhhub.unsw.edu.au
Health Information Systems Knowledge Hub, University of Queensland
Aims to facilitate the development and integration of health information systems in the broader health system strengthening agenda as well as increase local capacity to ensure that cost-effective, timely, reliable and relevant information is available, and used, to better inform health development policies. www.uq.edu.au/hishub
Health finance and Health Policy Knowledge Hub, The Nossal Institute for Global Health (University of Melbourne)
Aims to support regional, national and international partners to develop effective evidence-informed national policy-making, particularly in the field of health finance and health systems. Key thematic areas for this Hub include comparative analysis of health finance interventions and health system outcomes; the role of non-state providers of health care; and health policy development in the Pacific. www.ni.unimelb.edu.au
Compass: Women’s and Children’s Health Knowledge Hub, Compass is a partnership between the Centre for International Child Health, University of Melbourne, Menzies School of Health Research and Burnet Institute’s Centre for International Health.
Aims to enhance the quality and effectiveness of WCH interventions and focuses on supporting the Millennium Development Goals 4 and 5 – improved maternal and child health and universal access to reproductive health. Key thematic areas for this Hub include regional strategies for child survival; strengthening health systems for maternal and newborn health; adolescent reproductive health; and nutrition. www.wchknowledgehub.com.au
HRH Hub @ UNSW School of Public Health and Community Medicine Samuels Building, Level 2, Room 209The University of New South WalesSydney, NSW, 2052Australia
T +61 2 9385 8464F +61 2 9385 1104 [email protected]
www.hrhhub.unsw.edu.au
HUMAN RESOURCES FORHEALTH KNOWLEDGE HUB
Human Resources for Health HubSend us your email and be the first to receive copies of future publications. We also welcome your questions and feedback.