Embed Size (px)
Citation preview
Hospital for Children and Adolescents Jorvi Hospital Skin and Allergy Hospital University of Helsinki, Finland
Children Born Very Prematurely at School Age:
Lung Function and Outcome after
Antenatal and Neonatal Dexamethasone Treatment
SUVI MIESKONEN
Academic dissertation
To be publicly discussed with the permission of the Medical Faculty of the University of Helsinki, in the Niilo Hallman Auditorium of the Hospital for Children and Adolescents, on January 21st, 2005, at 12 noon.
Helsinki 2005
2
Supervised by: Professor Mikko Hallman Department of Pediatrics University of Oulu Oulu, Finland Docent Markku Turpeinen Skin and Allergy Hospital University of Helsinki Helsinki, Finland Reviewed by: Docent Kirsti Heinonen Department of Pediatrics University of Kuopio Kuopio, Finland Kirsi Timonen, MD, PhD Department of Clinical Physiology and Nuclear Medicine University of Kuopio Kuopio, Finland Opponent: Docent Outi Tammela Department of Pediatrics University of Tampere Tampere, Finland Cover photo: Suvi Mieskonen Anniina held by her mother (warm thanks) ISBN 952-91-8184-1 (paperback) ISBN 952-10-2261-2 (pdf) Yliopistopaino Helsinki 2005

3
To Elsa, Alpo and Sara

4
5
ABSTRACT
Glucocorticoids enhance the maturation of premature lung. Antenatal glucocorticoids reduce
the risk of respiratory distress syndrome and neonatal death in preterm infants, and postnatal
dexamethasone (DEX) facilitates weaning from the ventilator. However, these drugs may
disturb the growth and development of lung and brain. To evaluate the long-term effects of
antenatal or postnatal DEX treatment, we studied 49 children aged 7.3-9.2 years, born very
prematurely at 24-30 gestational weeks and with 600-1575 g of birth weight in 1989-1991,
who had participated in randomized placebo-controlled trials of neonatal DEX therapy
administered to ventilated infants at high risk for bronchopulmonary dysplasia (BPD) (n=16)
or/and antenatal DEX therapy in conjunction with exogenous surfactant (n=35).
Cardiorespiratory morbidity, neurological outcome and the family history of smoking or
atopy were evaluated using hospital records and questionnaires. Physical examination, skin
prick tests, impulse oscillometry, flow-volume spirometry, pulmonary diffusing capacity test
and whole-body plethysmography were carried out, and the oscillometric method was
compared with the conventional lung function methods. Lung inflammation was studied by
exhaled nitric oxide (eNO) measurement and cardiac outcome by chest X-ray,
electrocardiogram and echocardiography. The control group consisted of 18 non-atopic
children born at term and tested for lung function.
Antenatal or neonatal DEX had no negative effect on cardiopulmonary outcome. On the
contrary, the children born after antenatal placebo showed greater bronchodilator
responsiveness (∆FEV1) than those born after antenatal DEX.
Severe or moderate disability was common in our prematurely born children (29%).
Neurosensory outcome did not differ between the neonatal DEX and placebo groups.
However, antenatal DEX treatment associated with a higher rate of normal school attendance
and less severe or moderate disability.
The children born prematurely, particularly boys, were shorter for age than the controls.
The BPD children weighed less adjusted for height than the non-BPD children. Antenatal or
postnatal DEX treatment had no significant effect on weight or height.
Half of the children born prematurely reported frequent respiratory symptoms during the
preceding year, with no association with BPD or either DEX treatment. Poorer exercise
tolerance and more common use of inhaled medication were reported in the BPD group.
6
Atopy was rare in the children with BPD. Atopy associated with significantly increased
eNO concentrations. In non-atopic children, eNO levels correlated neither with the values of
lung function measurements nor with BPD. Thus, eNO was not an inflammatory marker of
BPD at school age, but it may be valuable in studying atopic asthma even in children born
prematurely.
Airway obstruction, bronchial hyperreactivity and decreased gas exchange were evident in
the children born very prematurely, especially those with BPD. Smoking in the family
associated with decreased gas exchange, and these children should therefore be strongly
advised against smoking or passive smoking. Impulse oscillometry yielded lung function
information concordant with the conventional methods and served well in studying even
children with neurological handicap or small lung volumes.
To conclude, abnormal lung function, somatic growth and neurosensory development
were common at school age in children born very prematurely. However, we found no
negative effect associated with antenatal or neonatal DEX treatment. Less strenuous lung
function methods, such as impulse oscillometry, help to assess the pulmonary disease of
disabled or young children who cannot cooperate in conventional lung function studies.
Despite the few abnormal findings, cardiac follow-up is important, as the chronic lung disease
of prematurity may later in life lead to cardiac sequelae or mask the cardiac symptoms. If
possible, very prematurely born children should also be protected from additional risk factors
for impaired lung function, such as infections or smoking.
7
LIST OF ORIGINAL PUBLICATIONS
This thesis is based on the following publications, which are referred to in the text by their
Roman numerals (I to IV).
I Malmberg LP, Mieskonen S, Pelkonen A, Kari A, Sovijärvi AR, Turpeinen M.
Lung function measured by the oscillometric method in prematurely born children
with chronic lung disease. Eur Respir J 2000 Oct; 16(4): 598-603.
II Mieskonen ST, Malmberg LP, Kari MA, Pelkonen AS, Turpeinen MT,
Hallman NMK, Sovijärvi AR. Exhaled nitric oxide at school age in prematurely
born infants with neonatal chronic lung disease. Pediatr Pulmonol 2002 May;
33(5): 347-355.
III Mieskonen S, Eronen M, Malmberg LP, Turpeinen M, Kari MA, Hallman M.
Controlled trial of dexamethasone in neonatal chronic lung disease: an 8-year
follow-up of cardiopulmonary function and growth. Acta Paediatr 2003 Aug;
92(8): 896-904.
IV Mieskonen S, Kari MA, Eronen M, Malmberg LP, Turpeinen M, Hallman M.
Randomized trial of antenatal dexamethasone before preterm birth:
cardiopulmonary function, growth, and neurosensory outcome at 8 years.
Submitted for publication.
In addition, some unpublished data are presented.
All refers to data of all study children born very prematurely.
2
ABBREVIATIONS AT acceleration time ACTH adrenocorticotrophic hormone ASD atrial septal defect BPD bronchopulmonary dysplasia C compliance CLD chronic lung disease COPD chronic obstructive
pulmonary disease CP cerebral palsy CPAP continuous positive airway
pressure DEX dexamethasone ∆FEV1 percentage change in FEV1
from baseline DLCO pulmonary diffusing capacity ∆Rrs5 percentage change in Rrs5
from baseline ∆Xrs5 percentage change in Xrs5
from baseline ECG electrocardiogram ELBW extremely low birth weight,
<1000 g eNO exhaled nitric oxide FEF50 forced expiratory flow at 50%
of FVC FEF25-75 forced expiratory flow during
the middle half of FVC FEV1 forced expiratory volume in
one second FiO2 fraction of inspiratory oxygen FOT forced oscillation technique FRC functional residual capacity fres resonance frequency FVC forced vital capacity
IMV intermittent mandatory
ventilation IOS impulse oscillometry IVH intraventricular hemorrhage KCO diffusing coefficient for
carbon monoxide LBW low birth weight, <2500 g MEF maximal expiratory flow NEC necrotizing enterocolitis NO nitric oxide NOS nitric oxide synthase PAP pulmonary arterial pressure PDA patent ductus arteriosus PEF peak expiratory flow PVL periventricular leukomalacia Raw airway resistance RBBB right bundle branch block RDS respiratory distress syndrome ROP retinopathy of prematurity Rrs5 respiratory resistance at 5 Hz RV residual volume RVET right ventricular ejection time SGA small for gestational age, birth
weight <-2 SD from the mean birth weight for each gestational week
SGaw specific conductance in the airways
TGV thoracic gas volume TLC total lung capacity VC vital capacity VLBW very low birth weight,
<1500 g Xrs5 respiratory reactance at 5 Hz
Gaw airway conductance
3
CONTENTS ABSTRACT 1 LIST OF ORIGINAL PUBLICATIONS 3 ABBREVIATIONS 4 CONTENTS 5 INTRODUCTION 8 REVIEW OF LITERATURE 11 1. Human lung growth and development............................................................................................. 11 Factors affecting lung growth and development 2. Respiratory distress syndrome (RDS)............................................................................................. 12 Clinical presentation and pathology
Pulmonary surfactant Surfactant therapy Incidence and prevention of RDS
3. Bronchopulmonary dysplasia (BPD)............................................................................................... 14 �Old� BPD
�Changing� BPD �New� BPD
3.1. Pathogenesis of BPD.............................................................................................................. 16 Oxygen toxicity
Barotrauma - volutrama Inflammatory injury Vascular injury Surfactant dysfunction Genetic predisposition
3.2. Incidence of BPD.................................................................................................................... 20 3.3. Prevention and treatment of BPD........................................................................................... 21 Optimization of oxygen administration Antioxidant therapy Mode of ventilation Infection/inflammation Pulmonary vascular resistance Nutrition and growth Improving respiratory mechanics, prevention of oedema Glucocorticoids 4. Respiratory morbidity in children born prematurely....................................................................... 24 5. Tests of lung function in infancy and childhood............................................................................. 26
Measures of forced expiratory flow Measures of lung volume Measures of compliance and resistance Measures of gas exchange
6. Lung function in children born prematurely.................................................................................... 28 Infancy School age
7. Other indices associated with lung disease...................................................................................... 32 Immune response Exhaled nitric oxide (eNO)
8. Follow-up of growth, neurodevelopment and cardiac function in children born prematurely........ 34 Growth Neurosensory development Cardiac function
4
9. Pharmacologic effects of glucocorticoids........................................................................................ 37 Effects on the pulmonary defence system Effects on lung structure and growth
Effects on other tissues Brain development
10. Trials on glucocorticoids during the antenatal - neonatal period.................................................... 40 10.1. Glucocorticoid treatment of preterm infants......................................................................... 40 Early postnatal glucocorticoid treatment
Moderately early postnatal glucocorticoid treatment Delayed postnatal glucocorticoid treatment Neurodevelopmental outcome after postnatal dexamethasone treatment Growth after postnatal dexamethasone treatment Respiratory morbidity and lung function after postnatal dexamethasone treatment Cardiovascular findings after postnatal dexamethasone treatment Recommendations and practice of postnatal dexamethasone treatment
10.2. Antenatal glucocorticoid treatment...................................................................................... 47 Prevention of neonatal diseases Neurodevelopmental outcome after antenatal glucocorticoids Growth after antenatal glucocorticoids Respiratory morbidity and lung function after antenatal glucocorticoids Cardiovascular findings after antenatal glucocorticoids
AIMS OF THE STUDY 52 PATIENTS AND METHODS 53 1. Patients............................................................................................................................................. 53 2. Neonatal and follow-up data collection........................................................................................... 54 3. Study protocol.................................................................................................................................. 55 4. Lung function methods.................................................................................................................... 56
Flow-volume spirometry Impulse oscillometry Pulmonary diffusing capacity test Whole-body plethysmography
5. Exhaled nitric oxide......................................................................................................................... 58 6. Cardiological measurements............................................................................................................ 58 7. Statistics........................................................................................................................................... 59 RESULTS 61 1. Population characteristics................................................................................................................ 61
Children born very prematurely Children with BPD Atopic children Children in the postnatal dexamethasone study Children in the antenatal dexamethasone study
2. Growth............................................................................................................................................. 63 Children born very prematurely Children with BPD Children after postnatal dexamethasone treatment Children after antenatal dexamethasone treatment
3. Respiratory symptoms and medication............................................................................................ 64 Children born very prematurely Children with BPD Children after postnatal dexamethasone treatment
5
Children after antenatal dexamethasone treatment 4. Smoking in the family..................................................................................................................... 66
Influence on growth Influence on respiratory symptoms Influence on lung function
5. Atopy............................................................................................................................................... 67 Children born very prematurely Children with BPD Children after postnatal dexamethasone treatment Children after antenatal dexamethasone treatment
6. Lung function.................................................................................................................................. 69 Oscillometric method Children born very prematurely Children with BPD Children after postnatal dexamethasone treatment Children after antenatal dexamethasone treatment Effect of smoking
7. Exhaled nitric oxide........................................................................................................................ 75 Children born very prematurely Influence of atopy, familial smoking or glucocorticoid inhalation Non-atopic children with BPD
8. Cardiac function.............................................................................................................................. 76 Children after postnatal dexamethasone treatment Children after antenatal dexamethasone treatment
9. Neurological follow-up................................................................................................................... 78 Children after postnatal dexamethasone treatment Children after antenatal dexamethasone treatment
DISCUSSION 81 1. Methodological aspects................................................................................................................... 81 Definition of bronchopulmonary dysplasia 2. Oscillometric method...................................................................................................................... 83 3. Exhaled nitric oxide ........................................................................................................................ 84 4. Growth............................................................................................................................................. 86 5. Atopy............................................................................................................................................... 87 6. Respiratory symptoms and medication........................................................................................... 88 7. Smoking in the family..................................................................................................................... 89 8. Lung function.................................................................................................................................. 89
Prematurely born children with or without BPD Glucocorticoids versus lung function Lung function after postnatal dexamethasone treatment Lung function after antenatal glucocorticoids
9. Cardiovascular findings................................................................................................................... 93 Cardiovascular findings after postnatal dexamethasone treatment Cardiovascular findings after antenatal glucocorticoids
10. Neurosensory development............................................................................................................. 95 Neurosensory development after glucocorticoid treatment Neurosensory development after postnatal dexamethasone treatment Neurosensory development after antenatal glucocorticoids
CONCLUSIONS 100 ACKNOWLEDGEMENTS 102 REFERENCES 104 ORIGINAL PUBLICATIONS 119
6
INTRODUCTION
Prematurity is a major cause of mortality and chronic morbidity in childhood. The outcome of
preterm birth (<37 gestational weeks) depends on time and place. In developed countries, the
survival of very low birth weight (VLBW, <1500 g) infants has increased, and their initial
outcome has improved along with the advances in perinatal care (Lemons et al 2001,
Saugstad 2001, Koivisto et al 2004). However, their infant mortality rate, i.e. death until one
year of age per 1000 live births, is more than 100-fold compared to infants with normal birth
weight. Neonatal deaths during the first four weeks of life account for two thirds of overall
infant mortality, and half of the deaths take place during the first week of life. (Mathews et al
2003) Neonatal mortality of VLBW infants is highest during the first few days of life, mainly
due to respiratory distress syndrome (RDS), infections and immaturity (Stevenson et al 1998).
In a recent Finnish study of extremely low birth weight (ELBW, <1000 g) infants, neonatal
mortality was 38%. Perinatal mortality (death from the 20th week of gestation to seven days of
age) was 55%, accounting for 39% of all perinatal deaths. (Tommiska et al 2001) In a large
multicenter study of VLBW infants in 1989-1990, 78% survived until discharge (Hack et al
1995); in 1995-1996, 84% survived (Lemons et al 2001). In Finland, 834 VLBW infants were
born alive in 1987 and 611 in 2003, accounting for 1.4% and 1.0% of live births, respectively
(Stakes 2004).
The clinical course and definitions of bronchopulmonary dysplasia (BPD), also called the
chronic lung disease (CLD) of prematurity, have changed over time, but with no clear decline
in incidence (Parker et al 1992). Besides BPD, defined as a need for supplemental oxygen at
36 postconceptional weeks in the present study (Shennan et al 1988), periventricular brain
damage, including intraventricular-periventricular haemorrhage (IVH) and periventricular
leukomalacia (PVL), necrotizing enterocolitis (NEC) and retinopathy of prematurity (ROP)
cause severe morbidity in VLBW infants. Pulmonary problems persist well beyond the
neonatal period or infancy. They may be associated with disturbances in growth, cardiac
function and neurodevelopment that may continue until school age or adulthood.
The pathogenesis of BPD is multifactorial and incompletely understood. Immaturity, oxygen
toxicity, baro/volutrauma and other perinatal factors, such as infection, promote lung injury.
Inflammation plays an important role in the progress of initial changes into a chronic lung
7
disease. In the less mature survivors, BPD is characterized by an arrest in lung development,
including minimal alveolarization and impaired vascular growth. (Jobe 1999)
Dexamethasone (DEX) and betamethasone are synthetic glucocorticoids with multiple acute
beneficial effects on immature lung (Ballard & Ballard 1995). In 1972, Liggins and Howie
showed that maternal treatment with betamethasone before preterm birth reduced the rate of
RDS and neonatal death. This result was confirmed more extensively in multiple trials during
the following years (Crowley 1995), and antenatal glucocorticoid therapy is now
recommended for women at risk of delivery at 24-34 gestational weeks (National Institutes of
Health, NIH 1995).
An early trial with hydrocortisone as treatment of RDS revealed no significant benefits
(Baden et al 1972). In the 1980´s, DEX treatment for severe BPD was found to decrease the
time on mechanical ventilation and supplemental oxygen (Mammel et al 1983, Avery et al
1985). With growing evidence of the inflammatory basis of BPD, DEX was considered as an
early treatment of very high-risk infants (Yeh et al 1990). However, treatment after birth was
associated with severe side effects, and animal experiments provided evidence of abnormal
brain growth and development after corticosteroids (Whitelaw & Thoresen 2000). The
widespread use of glucocorticoids postnatally and even antenatal use, particularly as multiple
courses, evoked concern about long-term adverse effects. After the initiation of our study,
early treatment with postnatal DEX was shown to associate with an increased risk of cerebral
palsy (CP) and a delay in neurodevelopment (Yeh et al 1998, O´Shea et al 1999, Shinwell et
al 2000). New guidelines limited the use of DEX to exceptional circumstances, i.e. infants on
maximal ventilatory and oxygen support (American Academy of Pediatrics, AAP 2002), but
the final role of postnatal corticosteroid is still undefined (Halliday 2003). Although antenatal
DEX treatment was associated with serious adverse consequences, long-term data after
antenatal or neonatal glucocorticoid trials are sparse or completely missing.
The lung function of prematurely born children cannot usually be assessed until school age,
since the conventional tests require considerable cooperation. Even then, the examinations
may be hampered by neurological disabilities and small lung volumes. The forced oscillation
technique (FOT) and impulse oscillometry (IOS), a modification of FOT, enable the
measurement of lung function during normal quiet tidal breathing. They therefore require
8
only minimal cooperation and are suitable at preschool age. Scant FOT data are available on
prematurely born children (Duiverman et al 1988).
Inhaled glucocorticoid treatment of low birth weight (LBW) children had no effect on the
baseline lung function or the airway response to histamine at school age in one study, arguing
against an inflammatory basis of airway hyperresponsiveness (Chan & Silverman 1993).
However, changes in T lymphocyte subsets, with an association with bronchial lability,
suggested that the abnormal immunological alteration may be related to BPD (Pelkonen et al
1999). Measurement of the exhaled nitric oxide (eNO) concentration has been proposed as a
non-invasive method to assess airway inflammation in asthma (Alving et al 1993, Lundberg
et al 1996) and disease activity in chronic obstructive pulmonary disease (COPD) (Maziak et
al 1998). ENO has been associated with eosinophilic inflammation in the lungs (Piacentini et
al 1999, Mattes et al 1999), but the role in non-atopic asthma remains undefined. No reports
exist of eNO in school-aged children with BPD.
In the present follow-up study of two randomized placebo-controlled trials, we evaluated the
effect of antenatal or neonatal DEX on cardiopulmonary function, growth and neurosensory
development at school age in children born very prematurely. Elaborate non-invasive methods
were used to measure lung function, exhaled NO and cardiac function. The children born
very prematurely were born very preterm (<31 gestational weeks) as well as with a very low
birth weight (<1575 g) in 1989-1991.

9
REVIEW OF LITERATURE
1. Human lung growth and development
Normal lung development during organogenesis can be divided into five stages (Burri 1997,
Kotecha 2000). During the embryonic stage (3-7 weeks of gestation), the lung develops as an
outgrowth of the ventral wall of the primitive foregut endoderm. Epithelial cells from the
endoderm invade the surrounding mesoderm to form the proximal structures of the respiratory
tract: the trachea, main bronchi, five lobes and 18 major lobules. The pulmonary arteries
develop to accompany the branching airways. During the pseudo-glandular stage (7-16
weeks), the epithelial tubules are surrounded by thick mesenchymal tissue, and the conducting
airways, terminal bronchioles and primitive acinus are formed. The pseudo-stratified
columnar epithelium is progressively replaced by tall columnar cells in the proximal airways
and cuboidal cells in the distal acinar structures. During the canalicular stage (16-26 weeks),
primary acini develop, consisting of respiratory bronchioles, alveolar ducts and rudimentary
alveoli. The intra-acinar capillaries derive from the surrounding mesenchyme. Many cells in
the distal epithelium differentiate into lamellar body-containing cells resembling type II
pneumocytes. During the saccular stage (24-36 weeks), the peripheral airways enlarge as the
acinar tubules dilate and the walls become thinner, resulting in increased gas-exchanging
surface area. Lamellar bodies increase, and terminal differentiation of type II cells into type I
pneumocytes takes place. Capillaries closely associated with type I cells reduce the distance
between the future air-blood interface. During the alveolar stage (32 weeks - 10 years), the
secondary alveolar septa are formed. Mesenchymal cells proliferate to deposit the
extracellular matrix, epithelial cells (type I and type II pneumocytes) line the alveolar walls,
and endothelial cells grow into the secondary septa and, after remodelling, form a single
capillary loop. This maturation results in a marked increase in gas-exchanging surface area, as
the estimated 20 to 50 million alveoli present at birth increase to 300 million by adulthood.
Factors affecting lung growth and development
Data on lung growth are mainly derived from studies of animals with differences in timing of
lung maturation. Different mechanisms and a number of hormones, growth factors, cytokines
and transcription factors are involved in normal lung growth, differentiation and repair
processes after lung injury. (Kotecha 2000)
10
During the canalicular stage, pulmonary hypoplasia may be secondary to oligohydramnion
as a result of prolonged rupture of membranes, to the restriction of fetal breathing movements
or to space-occupying abdominal organs in diaphragmatic hernia. Severe pulmonary
hypoplasia leads to severe respiratory distress because of poorly developed peripheral airways
and small lung size. On the other hand, overdistention of the lung by fluid seems to improve
lung growth by releasing many growth factors. Severe malnutrition decreases lung volumes
without interfering with maturation, whereas postnatal food restriction may exacerbate severe
lung injury and resistance against toxic agents, such as hyperoxia. (Kotecha 2000)
Glucocorticoids are involved in both lung growth and differentiation. A genetic lack of
glucocorticoid receptor in fetal mice results in hypoplastic immature lungs and impaired gas
exchange at term birth (Cole et al 1995). Glucocorticoids bind with high affinity to
cytoplasmic receptors, and the activated steroid-receptor complex binds to several response
elements in the promoters of a number of genes profoundly influencing transcription.
Glucocorticoid activity partly controls the synthesis and secretion of alveolar surfactant.
Furthermore, the increase in compliance and maximal lung volume, the decrease in vascular
permeability, the maturation of the parenchymal structure and the clearance of lung water are
controlled by glucocorticoids, adrenergic agents and other agonists. (Ballard & Ballard 1995,
Mallampalli et al 1997, Jobe & Bancalari 2001)
2. Respiratory distress syndrome (RDS)
Clinical presentation and pathology
RDS in the premature infant presents with an acute, severe respiratory distress and
requirement for supplemental oxygen shortly after birth. The chest radiograph shows
increased density in the lung fields with fine granularity, air bronchograms and elevation of
the diaphragm, indicating generalized atelectasis and lung oedema. Traditionally, the severity
increases for three days, and normal lung function is restored within a week. Nearly all infants
die with supportive care only, and about 50% die with the administration of supplemental
oxygen alone. In infants <32 gestational weeks, who rarely survive without ventilation using
continuous distending pressures, the condition is usually prolonged and commonly involves
pulmonary complications, such as pneumothorax, pulmonary interstitial emphysema and
infection. Immaturity of the lung and the cardiovascular system (leaky pulmonary capillaries
shortly after birth, immature pulmonary connective tissue, compliant chest cage, patency of
ductus arteriosus, immature host defence against microbes and other external noxious agents)
11
further predispose these infants to lung injury. RDS is a major risk factor of BPD and IVH
and involves significant mortality. (Bancalari & Bidegain 1999)
Pulmonary surfactant
In 1959, Avery and Mead discovered evidence of deficient surface activity in lung lavage of
infants dying of hyaline membrane disease. These findings marked the beginning of
systematic research leading to the introduction of surfactant therapy for RDS and further
therapeutic applications. Lung surfactant is needed to decrease surface tension and to prevent
the collapse of the small airways. The composition of surfactant, as reviewed by Jobe (1993a)
and Hallman et al (2001), consists of specific phospholipids (85-95%), neutral lipids (3-8%)
and specific proteins (5-10%). Of the four identified surfactant-associated proteins, SP-A
improves surface properties and has roles in pulmonary host defence. The lipophilic proteins
SP-B and SP-C facilitate rapid adsorption and spreading of surfactant phospholipids to the
gas-liquid interface. The timetable of the maturation of the human lung and surfactant system
is highly variable. Generally, it takes place before term, increasing towards term.
RDS is caused by a deficiency in alveolar surfactant due to immaturity of alveolar type II
epithelial cells. Many premature infants have sufficient quantities of surfactant in the airways
and do not develop RDS, even when born after only 65-80% of the pregnancy has lapsed.
(Hallman et al 2001) The antenatal development of surfactant secretion corresponds closely to
the risk of RDS, and the suspectibility to RDS is influenced by variations in the SP-A and SP-
B genes, race, sex and perinatal complications. Besides providing alveolar stability, individual
components of surfactant have important roles in the innate immune response and in the
defence against microbes. (Marttila et al 2003b, Marttila 2003a, Hallman et al 2002)
Surfactant therapy
The first pilot study of exogenous surfactant given to severely ill preterm infants in 1980
(Fujiwara et al) was soon followed by randomized clinical trials on exogenous surfactant
from human amniotic fluid, from mammalian lungs or from broncho-alveolar lavage fluid and
on synthetic surfactant (Merritt & Hallman 1988). Surfactant therapy ameliorates or prevents
the expiratory failure dramatically when administered into the airways in RDS or at very
premature birth. Neonatal mortality decreased by 45-55% and serious pulmonary air leak by
50-80%. Since the early 1990´s, administration of animal-based or synthetic surfactant into
the airways has been an approved treatment of RDS, and it has since been accepted into
common use as effective and life-saving treatment. (Hallman et al 2001) As more and more
12
very immature infants survive, there has been no significant decrease in the incidence of BPD
or patent ductus arteriosus (PDA) or IVH (Jobe 1993a).
Incidence and prevention of RDS
Despite surfactant and antenatal glucocorticoid treatments (Chapter 10.2.), RDS remains a
major cause of mortality and morbidity, as the survival of more immature infants increases. In
Finland, the incidence of RDS increased during the 1960-1970´s, but remained stable from
1990-1995 to 1996-1999 (8.7-7.6 per 1000 livebirths). The gestational-age-specific incidence
of and mortality from RDS decreased, but still accounted for 15% of neonatal deaths.
(Koivisto et al 2004) In the USA, in an inborn cohort of 4438 infants in 14 centres (1995-
1996), RDS occurred in 50% of VLBW infants and in 78% of those with 501-750 g birth
weight (Lemons et al 2001). In a Finnish national study (1996-1997), the neonatal mortality
of ELBW infants was 38%, and in 39% of the cases the reported leading cause of death was
RDS. In that study, of the infants surviving >12 hours, 76% had RDS, and 74% of those <30
weeks of gestational age received surfactant. (Tommiska et al 2001)
Expectant management of high-risk pregnancies, analysis of fetal lung maturity,
avoidance of near-term caesarean sections without labour and glucocorticoid treatment in
imminent preterm birth (<34 gestational weeks) are practices that decrease the risk of RDS
(Hallman 1992a, Crowley 2000).
3. Bronchopulmonary dysplasia (BPD)
�Old� BPD
BPD was first described by Northway et al in 1967 as a severe lung injury in mechanically
ventilated large preterm infants, who required 80-100% oxygen and had a prolonged course of
severe respiratory distress. The clinical, radiological and pathological progression of the
primary lung disease had several stages. The initial RDS (stage I, days 1-3) was characterized
by severe diffuse lung disease. It was followed by increasing opacification of the lungs,
corresponding to pathological findings of exudation in the airways and patchy bronchiolar and
alveolar epithelial necrosis (stage II, days 4-10). Stage III (days 10-20) was a transition to
chronic lung disease with small, round areas of radiolucency alternating with areas of sponge-
like irregular density in chest radiographs, representing emphysematous alveoli adjacent to
atelectatic alveoli, and pulmonary fibrosis. At stage IV (after 30 days), chronic lung disease
with hyperexpansion and larger cysts became evident in the basal lung fields. This stage was

13
frequently accompanied by right ventricular hypertrophy and cardiomegaly with cor
pulmonale. Pathologically, emphysema with thickened lung interstitium, dysplastic airways
and lung vasculature were frequently evident. (Northway et al 1967, Northway 1990a)
�Changing� BPD
In the 1970´s, BPD was defined as a respiratory failure in the neonatal period requiring
assisted ventilation for at least three days, with persistent respiratory symptoms and
radiological findings and oxygen dependency at four weeks of age (Bancalari et al 1979,
Tooley 1979, Edwards 1979a). In the 1980´s, with improvements in the ventilation techniques,
the survival of infants <1000 g increased, and oxygen concentrations and peak inspiratory
pressures decreased, modifying the radiological changes into a fine reticular pattern, with or
without hyperexpansion (Northway 1990a). O´Brodovich & Mellins (1985) reviewed BPD
and suggested it to represent a non-specific reaction of the lung to slowly resolving acute
injury. Hyperinflation was seen as the predominant radiographic abnormality along with
chronic respiratory difficulties, prolonged and recurrent hospitalization, neurodevelopmental
disabilities and growth restriction associated with BPD. In VLBW infants, apart from
classical coarse reticulation, a milder type with homogenous or patchy opacification,
particularly perihilar, was present in radiographs (Hyde et al 1989), and the pathological
progression of lung injury differed from that originally seen: a largely parenchymal picture
with marked increases in interstitial elastic tissue, less severe squamous metaplasia and poor
development and simplification of the terminal respiratory unit (Chambers & van Velzen
1989).
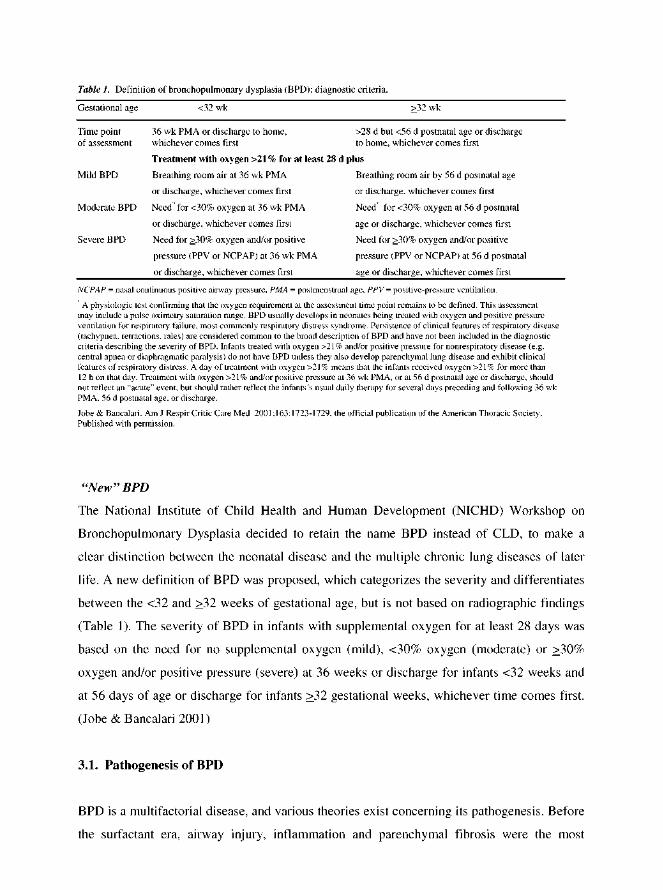
With the survival of increasingly immature infants, the criterion of supplemental oxygen
at 28 days became insufficient in anticipating long-term morbidity. In 1988, Shennan et al
proposed that the need for supplemental oxygen at 36 gestational weeks was a better predictor
of abnormal outcome during the first two years of life. This criterion was adopted into wide
use, and it is often also referred to as chronic lung disease (CLD).
Palta et al (1998) compared different criteria, such as supplemental oxygen and/or
radiograph or a severity score based on oxygen need, ventilatory variables, blood gases and
radiograph at 30 days of age, and supplemental oxygen at 36 gestational weeks. All criteria,
especially the radiographic ones, were predictive of long-term outcome at five years of age,
but the combination of radiograph and supplemental oxygen at 36 weeks was proposed.
15
prominent findings, accompanied by early vascular lesions, right ventricular hypertrophy and
cardiomegaly with cor pulmonale. Infants dying of BPD in the era of surfactant treatment had
fewer and larger alveoli with less fibrosis and inflammation than in the past (Husain et al
1998, Jobe & Bancalari 2001), and alveolar hypoplasia was accompanied by bronchial
smooth muscle hypertrophy and bronchial gland hyperplasia, contributing to airflow
limitation (Margraf et al 1991). Preterm baboons (75% of gestation) exposed to 100% oxygen
and mechanical ventilation, used to model the �old� BPD, had a lower alveolar number at the
age of 33 weeks compared to those ventilated with clinically appropriate oxygen (Coalson et
al 1995). Similar pathology was seen in baboons delivered extremely preterm (67% of
gestation) after prenatal glucocorticoid, surfactant treatment and mechanical ventilation with
even less than 50% oxygen (Coalson et al 1999). The �new� BPD is characterized by an
arrest of lung development with minimal alveolarization, less airway epithelial disease and
less interstitial fibrosis (Jobe 1999), with dysmorphic capillary configurations (Coalson 2003).
The predominant pathogenetic factor in BPD is a recurrent inflammatory reaction,
whether provoked by an intrauterine infection or inflammation that persists after birth or
caused by neonatal damage to the airways and airspaces due to hypoxia,
barotrauma/volutrauma or infection (Groneck & Speer 1995, Watterberg et al 1996, Speer
1999, Hallman et al 2001). Other antenatal or postnatal factors, such as intrauterine growth
retardation, preeclampsia, drugs or malnutrition may also affect the risk of BPD (Kotecha
2000).
Oxygen toxicity
Preterm infants are predisposed to changing levels of supplemental oxygen and mechanical
ventilation soon after birth, as reviewed by Barrington & Finer (1998), Kotecha & Silverman
(1999) and Jobe & Bancalari (2001). According to the traditional view, BPD is caused
primarily by oxidant- and ventilation-mediated injury. In animal studies, oxygen can arrest the
septation of lungs at the saccular stage (Coalson et al 1995), with more impairment at higher
oxygen levels (Coalson et al 1999).
High concentrations of oxygen induce lung inflammation and may lead to chronic fibrotic
and destructive changes, as the production of reactive oxygen species and the release of
chemotactic factors lead to the release of inflammatory mediators and proteolytic enzymes.
The low levels of antiproteases and antioxidant enzymes in the serum and lung of preterm
infants result in increased susceptibility to oxygen toxicity and to BPD. (Barrington & Finer
1998)

16
Barotrauma - volutrauma
Multiple factors act additively or synergistically to promote lung injury. The initiation of
mechanical ventilation causes a proinflammatory response. In preterm baboons, mechanical
ventilation even without high levels of oxygen may result in the pathologic lesion of BPD
(Coalson et al 1999). Although the exact mechanisms of lung injury are unknown, attempts to
reduce barotraumas are suggested to reduce the incidence of BPD (Kotecha & Silverman
1999). The avoidance of intubation and mechanical ventilation by administering continuous
positive airway pressure (CPAP) in the delivery room has been associated with a lower
incidence of BPD (Avery et al 1987, Van Marter et al 2000).
Inflammatory injury
Pulmonary inflammation is maximal at 7-10 days in infants who develop BPD (Vyas &
Kotecha 1997), as evidenced by the increase in neutrophils and multiple proinflammatory and
chemotactic factors present in the airspaces of ventilated preterm infants (Merritt et al 1983,
Groneck & Speer 1995, Vyas & Kotecha 1997). Infants exposed to chorioamnionitis had IL-
1β more frequently present in their tracheal fluid from the first day, which associated with the
development of BPD, despite the lower risk of RDS (Watterberg et al 1996). Colonization of
the airways of preterm infants with Ureaplasma urealyticum associated with acute respiratory
insufficiency (Ollikainen et al 1993); others found protection against RDS, but an increase in
BPD (Hannaford et al 1999). Chemotaxis of inflammatory cells and release of cytokines and
other mediators may cause lung injury and initiate the repair process. The same factors may
be released in nosocomial pneumonia. (Barrington & Finer 1998)
In very preterm born baboons, significant elevations of certain proinflammatory cytokines
(TNF-α, IL-6, IL-8, but not IL-1β and IL-10) in tracheal aspirate fluids were present at
various times during ventilatory treatment, supporting a role for mediator-induced
autoinflammation; IL-8 was elevated mostly in the presence of significant lung infection
(Coalson et al 1995). Preterm lung contains very few macrophages or granulocytes.
Granulocytes appear in the lung soon after the initiation of ventilation in animals (Carlton et
al 1997), which correlates with pulmonary oedema and the appearance of early indicators of
injury and occurs parallel to a decrease in circulating granulocytes. This decrease in
granulocytes at one hour of age associates with an increased risk of BPD (Ferreira et al 2000).
Proteases produced by activated white blood cells in the lung may contribute to the
progression of lung injury.
17
Vascular injury
Pulmonary vascular resistance is often increased in infants with BPD, and decreased vascular
development may be important in the pathopsysiology of BPD (Jobe & Bancalari 2001). The
vascular injury may result from direct toxicity of stimuli, such as oxygen and mechanical
ventilation, to the developing vasculature or from the release of toxic inflammatory mediators.
Damage to the developing alveolar epithelium is suggested to interrupt the signalling between
vascular endothelial growth factor (VEGF) and its receptors and to result in abnormal
pulmonary capillary growth and function. Converse theories suggest that the primary
disruption of pulmonary vascular development impairs alveolarization and may result in
histologic changes similar to BPD. (Parker & Abman 2003) Low VEGF levels in tracheal
aspirates have been found in preterm infants who later develop BPD (Lassus et al 1999),
while high levels have been seen in infants treated with DEX (D´Angio et al 1999).
Surfactant dysfunction
The recovery of surfactant phospholipids during the first week of life among infants who
develop BPD is not strikingly different from those who have an uncomplicated course of
RDS. The most clearly detectable difference, low surfactant phosphatidylinositol in infants
developing BPD, was eliminated by inositol supplementation at birth. (Hallman et al 1992b)
Infants developing BPD also had very low SP-A levels in airway specimens, but according to
recent evidence, surfactant dysfunction in infants developing BPD is not prevented by
surfactant therapy (Hallman et al 2001).
Genetic predisposition
Genetics may contribute to BPD at multiple levels (Marttila 2003a). According to an early
study, HLA-A2 is associated with susceptibility to BPD (Clark et al 1982). The
alleles/genotypes of SP-A, SP-C or SP-D associate with the risk of inflammatory lung and
airway diseases. Rare mutations in SP-B and SP-C cause serious, often fatal, lung diseases
(Hallman et al 2002, Marttila 2003a, Hallman 2004). Thus far, one allelic variant of the
surfactant protein B gene (intron 4 deletion variant) has been shown to associate with an
increased risk of BPD (Rova et al 2004).
18
3.2. Incidence of BPD
The original BPD occurred in 11-21% of mechanically ventilated infants and in 1-8% of all
infants with RDS (Northway 1979), showing a relationship with low birth weight: 38% of
survivors of RDS with birth weights of 750-1500 g had BPD compared with less than 10% of
those >1500 g (Tooley 1979). Even after controlling for birth weight, race and sex, the
incidence at 28-30 days varied among intensive care units, correlating with differences in
treatment (Avery et al 1987, Horbar et al 1988, Kraybill et al 1987, Kraybill et al 1989). In
ELBW infants after mechanical ventilation, the most powerful predictors of BPD were male
sex and lower PaCO2 at 48 hours, indicating that it might be possible to reduce the risk by
adjusting ventilation (Kraybill et al 1989). The incidence of BPD at 28 days in VLBW infants
increased from 11% in the late 1970´s to 33% in the late 1980´s, mostly but not exclusively
due to improved survival. The increase persisted even with the criterion of oxygen at 36
gestational weeks for infants <32 gestational weeks at birth. Gestational age was a significant
predictor of BPD after adjustment for birth weight. (Parker et al 1992) In a Finnish study of
VLBW infants born in one hospital in 1990-1994, 31% of the surviving infants had BPD, i.e.
supplemental oxygen with radiographic changes, at 28 days and 13% at 36 gestational weeks.
Besides low birth weight and gestational age, early weight gain, preeclampsia and possibly
intrauterine growth retardation were important risk factors for BPD at 36 weeks. (Korhonen et
al 1999b)
BPD is currently rare in infants with >1200 g or >30 gestational weeks at birth, as gentler
ventilation techniques, antenatal glucocorticoids and surfactant treatment have minimized
severe lung injury. However, BPD is the most common complication in ELBW infants (Jobe
1999, Jobe & Bancalari 2001), and it may also occur in infants with minimal or no lung
disease initially (Charafeddine et al 1999), some of them exposed to chorioamnionitis
(Watterberg et al 1996). In the NICHD multicentre study (1995-1996), the incidence of BPD
at 36 weeks was 23% in surviving infants with birth weights of 501-1500 g, with a slight
increase over five years (19-23%, survival 80-84%); the incidence increased markedly with
decreasing gestational age, and nearly all survivors with birth weight of 400-500 g had BPD
(Lemons et al 2001). In comparison, of the VLBW infants born in 1989-1990, 78% survived
and 8% of the survivors had BPD (Hack et al 1995). Thus, no evidence suggests a decline in
the incidence of BPD.
19
3.3. Prevention and treatment of BPD
The prevention of preterm births and various maternal conditions harmful for the fetus is a
continuing challenge, with major effects on the development of BPD. O´Brodovich & Mellins
(1985) presented that the means to treat BPD are identical to those initiating the injury.
Despite the advances in perinatal care, the means to prevent and treat BPD are still
unsatisfactory, as reviewed by Barrington & Finer (1998) and more recently by Korhonen
(2004a).
Optimization of oxygen administration
As far as possible, high oxygen concentrations should be avoided in the treatment of preterm
infants. However, the saturation target range is still controversial. (Kotecha & Allen 2002, Tin
2004) Exogenous surfactant should be administered to intubated VLBW infants with
significant lung disease prior to two hours of age, to reduce the need for oxygen and
ventilatory support, even though no clear effect is seen in the incidence of BPD (Jobe &
Bancalari 2001). In BPD infants, avoidance of hypoxia is important, to alleviate the
progressive muscularisation of small pulmonary arteries and enhanced vasoreactivity (Parker
& Abman 2003). According to the present proposal, O2 saturations of 94-96% should be
aimed at for infants with established BPD who are not at risk of further progression of ROP
(Kotecha & Allen 2002).
Antioxidant therapy
Hyperoxic lung injury may be ameliorated in animals by the administration of exogenous
antioxidants, such as recombinant superoxide dismutase. In humans, no difference in the
primary outcome of death and/or BPD was found, but IVH and PVL were less severe.
(Barrington & Finer 1998) Nor did N-acetylcysteine prevent BPD (Ahola et al 2003). Specific
nutrients, such as vitamins and cofactors, may also function in antioxidant defence (Kotecha
& Silverman 1999). Despite initial suggestions, vitamin E supplementation failed to show
benefits in reducing BPD (Jobe & Bancalari 2001).
Mode of ventilation
Different modes of ventilation have been used to minimize baro- and volutrauma, but none of
them have proven superior to the others (Henderson-Smart et al 2004). In 1963, the first
infant survived intubation and ventilation without air leak or cerebral abnormalities
20
(McGettigan et al 1998). Since 1971, CPAP has been used to treat infants with RDS (Mariani
& Carlo 1998), and it is considered to lower the risk of BPD by reducing barotrauma (Avery
et al 1987). Since that time, ventilation with continuous distending pressures has been the
basis of neonatal ventilatory support. During intermittent mandatory ventilation (IMV),
asynchronous breathing may result in irregular systemic and cerebral flow patterns, air leak
and neurological complications. In 1986, patient-triggered ventilation was first described:
synchronous IMV (SIMV), assist control and pressure support ventilation were further
developed. However, conventional mechanical ventilation still induced severe lung injury.
High-frequency oscillatory ventilation, using very low tidal volumes, is used to rescue
patients and to avoid lung injury in severe respiratory distress. (McGettigan et al 1998)
Assisted ventilation is recommended to be used with the lowest possible pressures required
for adequate gas exchange, in the most gentle ways available, followed by weaning and
extubation as soon as possible, allowing moderate hypercarbia. Nasal CPAP at birth or after a
brief period of ventilation is currently studied as a non-invasive method of ventilation. (Avery
et al 1987, Kraybill et al 1989, Barrington & Finer 1998)
Infection / inflammation
Infection may contribute to the development of inflammation with an adverse effect on lung
growth and pulmonary defence functions (Watterberg et al 1996). The prevention and
treatment of perinatal and nosocomial infections have been studied in relation to BPD.
Prevention of later infections by immune globulins, including those against respiratory
syncytial virus, and vaccinations are considered to reduce further risks for the lung in BPD.
Anti-inflammatory agents have been used in treatment (sodium cromoglycate,
glucocorticoids). (Barrington & Finer 1998)
Pulmonary vascular resistance
In infants with severe RDS, vasodilators, such as inhaled nitric oxide, can be used along with
oxygen therapy to decrease pulmonary vascular resistance. Inhalation of NO may improve
oxygenation and decrease the risk of BPD by minimising intra- and extrapulmonary shunting
and by decreasing inflammation. (Jobe & Bancalari 2001)
Nutrition and growth
Nutrition plays a supportive role in normal lung development and maturation. General
undernutrition, especially insufficient protein intake, may increase the vulnerability to
21
oxidant-induced lung injury. (Jobe & Bancalari 2001) Inositol (Hallman et al 1992b), vitamin
A (Tyson et al 1999) and retinoic acid have been studied in experimental models of lung
injury (Massaro & Massaro 2000). Supplementation of inositol (Hallman et al 1992b) or
vitamin A (Tyson et al 1999) to small preterm infants may reduce the risk of BPD, although
the evidence is not convincing. Nutrition should be optimized early after birth but probably
with some delay in intravenous lipid administration until pulmonary vascular resistance has
decreased (Barrington & Finer 1998).
Growth failure is common in infants with severe BPD (Northway 1979, Markestad &
Fitzhardinge 1981,Yu et al 1983), possibly because of their increased energy expenditure and
high metabolic rate. Hypoxemia, gastroesophageal reflux, poor feeding with inadequate
nutritional intake, heart failure, neurodevelopmental handicap and socioeconomic factors
further predispose BPD infants to unsatisfactory growth (Kotecha & Silverman 1999).
However, data on the ability of optimal growth and nutrition to improve long-term outcome
are sparse.
Improving respiratory mechanics, prevention of oedema
Bronchodilating agents improve lung mechanics in ventilator-dependent infants, but their
long-term effects are unknown. Methylxanthines (theophylline) are used to prevent apnoea in
preterm infants, but they also function as bronchodilators and diuretics. Increased fluid intake
may aggravate pulmonary oedema directly or by increasing the incidence of PDA (Kotecha &
Silverman 1999). Relative fluid restriction in very preterm infants at risk for BPD decreased
both mortality and BPD rates (Tammela & Koivisto 1992). Interstitial lung water can be
reduced by loop diuretics (furosemide), which decrease pulmonary resistance and increase
dynamic compliance. Non-loop diuretics (hydrochlorothiazide and spironolactone) improve
lung mechanics, but with no consistent long-term benefit. In BPD, furosemide and inhaled
bronchodilator agents are considered to allow weaning and extubation of ventilator-dependent
infants. (Barrington & Finer 1998)
Glucocorticoids
Glucocorticoids serve as anti-inflammatory and antioedematic agents. They accelerate the
differentiation of immature lung by increasing the synthesis and secretion of lung surfactant
and the activity of antioxidants. However, they also interfere with alveolarization and
angiogenesis (See Chapter 9 and 10). Antenatal glucocorticoids should be used in imminent
preterm delivery to attenuate initial respiratory distress (Crowley 1995, NIH 1995). Inhaled
22
glucocorticoids have been used to shorten the duration of mechanical ventilation (Cole et al
1999, Shah et al 2003). Postnatal glucocorticoid treatment may be considered in severely ill,
ventilator-dependent infants to facilitate weaning (AAP 2002). However, no clear decline has
been seen in the incidence of BPD after either modality of glucocorticoid treatment.
4. Respiratory morbidity in children born prematurely
The survivors of �old� BPD born in the 1960-1970´s frequently had persistent respiratory
symptoms at school age (Smyth et al 1981) and more wheezing, upper respiratory tract
infections, pneumonia, limitations of exercise capacity and long-term medication than full-
term controls at school age (Bader et al 1987) or preterm born adolescents with no BPD
(Northway et al 1990b).
In the late 1970´s, mechanically ventilated VLBW infants had tracheobronchial
hypersecretion and frequent lower respiratory infections during the first year of life. The need
for hospitalization was associated with male gender, CPAP, mechanical ventilation and
oxygen therapy. (Wong et al 1982a) Myers et al (1986) used regular physical examination,
respiratory illness score and viral cultures until the age of one year to show that LBW infants
(<2000 g) with or without RDS did not have an increased risk for respiratory illness compared
with full-term controls. However, the RDS survivors, particularly those with BPD,
experienced their lower respiratory tract infections earlier and with more severe symptoms
than the controls.
A prospective cohort study compared LBW children (<2000 g) with unselected
schoolchildren using questionnaires. Wheezing (16%) and troublesome cough (17%) were
common in healthy schoolchildren. There were no differences in maternal smoking (40%) or
the family history of asthma (12%) between the LBW and control children. However,
whooping cough, previous chest infection and previous admission into hospital for chest
illness were twice as common in the LBW cohort than in the controls. Oxygen
supplementation, mechanical ventilation and BPD increased the rate of chest infections during
the first two years (30% in the BPD group) and also increased admission into hospital for
respiratory infection (40% in the BPD group). In the subgroup of VLBW children after
neonatal respiratory treatment, frequent and troublesome cough was more common at seven
years than in unselected controls. No excess of wheezing, but a weak correlation between
wheezing and the oxygen score, or absence from school due to respiratory symptoms was
23
found in LBW children. Wheezing associated with maternal smoking. Of the VLBW
children, those with BPD had a high prevalence of symptoms, but they did not differ
significantly from the non-BPD group. (Chan et al 1989a)
Another study confirmed the previous findings of excess respiratory morbidity associated
with mechanical ventilation in children born very prematurely, particularly during the first
two years, but found dyspnea to be uncommon at school age. BPD children needed
adenoidectomy and tympanostomy tubes more commonly. (Hakulinen et al 1990) At
preschool age, BPD children had an increased risk for respiratory infections compared to
controls born at term, with no significant difference compared to non-BPD children
(Korhonen et al 1999a). In a prospective study, the persistence of respiratory symptoms into
the second year of life was associated with mechanical ventilation, supplemental oxygen, air
leak and increased resistance in body plethysmography at six months (Yuksel & Greenough
1992).
In ELBW survivors, clinical respiratory health at the age of 14 years, based on wheezing
requiring bronchodilators or readmissions into hospital for pneumonia or asthma, was found
to be similar to normal birth weight controls, despite differences in lung function (Doyle
2000a).
The studies of VLBW children born in the 1980´s have mainly used the criterion of oxygen at
36 weeks for BPD. In a Finnish study, half of the VLBW children had had dyspneic
symptoms, and two out of 29 had suffered from prolonged coughing (>3 weeks) during the
previous year. Atopy was diagnosed in 17% of the BPD and 29% of the non-BPD children; in
their families, atopy (41% vs 50%) and smoking (50%) were common. (Pelkonen et al 1997)
Others found atopy less often in VLBW children (15%) at ten years than in full-term controls
(31%) (Siltanen et al 2001), and the lifetime prevalence of wheezing was 43% vs 17%,
respectively (Siltanen et al 2004). After severe BPD requiring oxygen at home, the children
had a higher incidence of activity limitation because of their respiratory symptoms than non-
BPD controls at the age of 11 years (Jacob et al 1998). Children born very preterm (<32
gestational weeks), especially those with BPD, required more hospitalizations during the first
two years than their full-term controls. Wheezing and chronic cough were common at school
age, with no differences between the BPD and non-BPD groups, but the BPD children used
more bronchodilators. (Gross et al 1998)
24
5. Tests of lung function in infancy and childhood
Lung function can be assessed in infancy and childhood by measuring forced expiratory flow,
lung volume, compliance and resistance, respiratory pattern, chest wall motion and gas
mixing, as reviewed by the American Thoracic Society (ATS)/ European Respiratory Society
(ERS) (1993), Sovijärvi et al (1994), Kotecha & Silverman (1999) and Sly et al (1999).
Measures of forced expiratory flow
Maximal expiratory flow (MEF) on the descending portion of the MEF-volume curve is
independent of effort and reflects airway caliber peripheral to the segment subjected to flow
limitation. The measurement of MEF is a standardized and sensitive test of abnormalities in
the intrathoracic airways. Forced expiratory flow-volume relationship can be measured by the
forced deflation technique in intubated infants and by the rapid thoracoabdominal impression
method in non-intubated infants, and it can also be used with bronchodilating or
bronchoconstricting agents. Near school age, the measurements become more accurate.
Ventilatory capacity is influenced by lung volume, airway caliber, compliance and elasticity
of the lungs and chest and respiratory muscle function. In flow-volume spirometry, forced
expiratory volume in one second (FEV1) (or in 0.5 or 0.75 s) is the best indicator of
ventilation capacity and represents mainly the larger airways, as does peak expiratory flow
(PEF). Forced vital capacity (FVC) measures the dynamic volume of the lungs. Forced
expiratory flow at 50% (FEF50) and during the middle half of FVC (FEF25-75) represent the
airflow in medium-sized and small airways and the compliance of lung tissue as well.
Spirometry is used to differentiate between obstructive and restrictive dysfunction and,
combined with bronchodilators, bronchoconstrictors or exercise, to assess hyperreactivity.
Measures of lung volume
Functional residual capacity (FRC), i.e. the volume of air in the lungs and airways at end-
expiration, is a balance between the outward recoil of the chest wall and the inward recoil of
the lungs. FRC is the only lung volume that can be measured accurately and repeatedly in
infants, by the whole-body plethysmography or gas dilution techniques (helium dilution and
nitrogen washout). In whole-body plethysmography, a child, placed on a rigid container,
makes respiratory efforts against an occlusion at the airway opening. The changes in pressure
at the airway are related to the changes in volume, and thoracic gas volume (TGV) can be
calculated by applying Boyle´s law. Plethysmography measures all gas present in the thorax,
25
including that not in direct communication with the airway (gas trapping). In healthy infants,
TGV measurements tend to be reproducible. The helium dilution technique is based on the
principle of gas equilibration between an unknown lung volume and a known volume
containing helium as an indicator gas. Gas mixing is produced by ventilatory movements, and
assuming a mass balance, the unknown lung volume can be derived from the change in
helium concentration. The nitrogen washout technique measures the volume of nitrogen
washed out of the lungs when the infant rebreathes nitrogen-free gas. Gas dilution techniques
may underestimate FRC with gas trapping due to airway obstruction. At preschool age, lung
volumes, such as total lung capacity (TLC), residual volume (RV) and RV/TLC ratio, can be
measured by whole-body plethysmography with the patient sitting in a cabine. The static lung
volumes [vital capacity (VC), TLC, RV/TLC] can be estimated by the single-breath method
of the pulmonary diffusing capacity, even if the presence of air trapping can underestimate
TLC.
Measures of compliance and resistance
The intrinsic elastic properties of the lungs and the chest can be assessed by measuring
compliance and resistance during maturation. Dynamic techniques, such as body
plethysmography, forced oscillation and the interrupter technique, are applied during
spontaneous breathing or mechanically assisted ventilation. Passive techniques, such as
multiple occlusion, passive flow-volume and weighted spirometry, are done after silencing of
the respiratory muscles. All require measurements of airflow, volume and pressure;
transpulmonary pressure is approximated by measuring the difference between the airway and
esophageal pressures. Compliance (C) is calculated as the quotient of the change in volume
divided by the pressure applied. As it is proportional to changes in lung volume, specific
compliance (corrected for FRC) can be used instead. Respiratory system resistance, i.e. the
change in pressure divided by flow, is dominated by the upper airways, and the measured
values hence do not reflect modest changes in lower airway pressure. Therefore, only
relatively large changes in airway resistance (Raw) due to bronchodilators can be detected. At
preschool age, plethysmographic measurements of Raw and specific conductance (SGaw) can
be performed with the patient sitting in a cabin; Gaw is the reciprocal of Raw, and SGaw is
related to volume [SGaw = 1/(Raw xTGV)].
Forced oscillation technique (FOT) was introduced by DuBois et al in 1956 as a method to
characterize respiratory impedance and its two components, resistance (Rrs) and reactance
(Xrs), over a wide range of frequencies. Flow oscillations generated by a loudspeaker are
26
applied to the mouth and superimposed on normal breathing: FOT uses pseudorandom noise,
and its user-friendly commercial modification, impulse oscillometry (IOS), uses rectangular
pulse signals containing harmocis up to 35 Hz or higher (Vogel & Smidt 1994, Hellinckx et al
2001). The output pressure and flow signals are analyzed for their amplitude and phase
difference, to determine the Rrs and Xrs of the total respiratory system and even to study
airway mechanics during quiet tidal breathing. The oscillometric method has been used to
describe the mechanical properties of the lung in children with asthma, cystic fibrosis and
chronic respiratory symptoms (Solymar et al 1984, Lebecque et al 1987, Lebecque &
Stănescu 1997, Timonen et al 1997, Hellinckx et al 1998) as early as the age of 2-4 years
(König et al 1984, Duiverman et al 1985, Bisgaard & Klug 1995, Klug & Bisgaard 1996).
Scant data are available on preterm children (Duiverman et al 1988). Recently, the values of
IOS and FOT were shown to be similar, but not identical (Hellinckx et al 2001).
Measures of gas exchange
The function of the lung parenchyma can be assessed by measuring the pulmonary diffusing
capacity, i.e. the diffusion of the inspired gas from the lungs into the circulation. At preschool
or school age, a single-breath method, using an inhalation of a known mixture of an inert gas
(helium) and a diffusing gas, can be used for the analysis of the total pulmonary diffusing
capacity (DLCO) and the diffusing coefficient for carbon monoxide (KCO). (Salorinne 1994)
6. Lung function in children born prematurely
Infancy
During the neonatal intensive care, due to difficulties in performance and interpretation,
measurements of lung function have been mostly done as part of trials of medication or
ventilation techniques. More studies have been done on infants, but the interpretation of data
is influenced by sedation, considerable short-term variability and normalization procedures,
such as weight. Forced expiratory techniques have improved the accuracy of measurement
and made it possible to define the degree of dysfunction, the responses to specific therapy and
the onset of and recovery from respiratory problems. Both static and dynamic compliances are
low during neonatal intensive care and largely influenced by the ventilation technique and the
distending pressures applied. Compliance measurements have been used to investigate the
effect of surfactant in neonates and the effect of glucocorticoids in young children with
interstitial lung disease. Studies with bronchodilators have shown bronchoconstriction to
27
occur even in preterm infants during the first weeks of life. (ATS/ERS 1993, Kotecha &
Silverman 1999) In infants, chest wall compliance is 3-fold compared to lung compliance,
and it may be even higher in preterm infants (5-7-fold greater), making the respiratory pump
less efficient in moving the tidal volume (Gerhardt & Bancalari 1980, ATS/ERS 1993). Raw
values are high at birth but decrease rapidly during the first year of life. After birth,
conductance increases much more slowly than FRC, resulting in a rapid drop of SGaw
(Gerhardt et al 1987a). The age-specific changes in Raw can be only evaluated in relation to
changes in lung volume, as by using SGaw.
The survivors of �old� BPD in the 1960-1970´s had increased Raw, increased airway
reactivity, increased FRC, high arterial carbon dioxide tension, low arterial oxygen tension,
right or/and left ventricular hypertrophy and pulmonary and systemic hypertension in infancy
(Northway et al 1990b).
In VLBW children born before the surfactant era in the late 1970´s, TGV was higher, and
dynamic compliance and pulmonary and airway conductance were lower at the age of six
months and normalized by the end of the first year in those ventilated for RDS compared with
non-RDS infants, regardless of whether or not normalized for body weight or TGV. The
disturbances of lung function were particularly severe in infants with lower respiratory tract
infection. (Wong et al 1982a)
In VLBW infants born in the 1980´s, FRC was in the normal range, but compliance
decreased and Raw increased after both intermittent mandatory ventilation and high-frequency
oscillatory ventilation at two months of age (Gerhardt et al 1989). In larger preterm infants
with RDS, pulmonary mechanics were almost similar during early infancy after surfactant or
placebo treatment but, at the age of one year, total pulmonary resistance and the resistive
work of breathing were lower and expiratory airflow higher in surfactant-treated individuals,
suggesting decreased residual bronchopulmonary damage (Abbasi et al 1993).
In BPD, the flow-volume curves of tidal breathing generated by the compression
technique were clearly abnormal, exhibiting severe flow restrictions (Tepper et al 1986).
Respiratory system compliance was low during the first months, returning to normal by 1-3
years. Specific compliance was also low, indicating that other factors apart from lung volume
were making the lung stiff. Resistance values were mostly high, indicating the severity of the
disease. SGaw was low (60% of predicted) in infancy and increased only slightly (to 70%)
during the first three years of life. FRC was reported to be low during the first six months of
life, exceeding the normal by 12 months, measured as nitrogen washout. (Gerhardt et al
28
1987b) Plethysmographic lung volumes, which represent all gas present in the chest, tended to
be higher, while FRC and the FRC/TGV ratio were lower in symptomatic than in
asymptomatic infants, suggesting true hyperinflation, as shown in LBW infants at 12 months
of age (Yuksel & Greenough 1991).
School age
The survivors of �old� BPD continued to have airway obstruction, bronchial hyperreactivity
and hyperinflation in lung function studies at school age (Smyth et al 1981, Bader et al 1987)
and even in adolescence (Northway et al 1990b). Catch-up improvement in abnormal lung
function during the early school years was also reported (Blayney et al 1991). Of the original
BPD group, 24% had fixed airway obstruction, and 52% had reactive airway disease in
adolescence; the BPD children had a higher Raw and a lower SGaw than those with no BPD
(Northway et al 1990b). Limited exercise tolerance, defined as reported symptoms or
measured abnormal oxygen saturation, was seen (Bader et al 1987, Northway et al 1990b).
DLCO was found to be normal (Smyth et al 1981) or slightly decreased (Northway et al
1990b). The duration of both endotracheal intubation and mechanical ventilation associated
significantly with values of lung function (RV/TLC, FRC). Lung injury in BPD was
suggested to have a role in the pathogenesis of later pulmonary dysfunction, as the reduction
of airway growth during the rapid postnatal phase of lung growth could contribute to
disproportionate undergrowth of the airway lumen, resulting in increased airway resistance.
(Northway et al 1990b)
A cohort of LBW children born in the late 1970´s, irrespective of neonatal respiratory illness,
were shown to have lower expiratory flow indices with well preserved VC than controls
representing local school children. Airway function correlated strongly with birth weight and,
to a lesser extent, with gestational age, maternal smoking, male sex and cough. The BPD
subgroup also had reduced FVC. (Chan et al 1989b) Four-week inhalation of beclomethasone
had no effect on symptoms or lung function in the 44% of the children who showed increased
airway responsiveness in histamine challenge (Chan & Silverman 1993). A Finnish cohort
study of children born very prematurely in the same period compared BPD, ventilated non-
BPD, non-ventilated and full-term control children. Despite few clinical problems at school
age, the BPD children had markedly lower SGaw and larger RV than the term controls,
explained by increased Raw, air trapping and reduced elasticity of the lungs. The non-
ventilated children did not differ from the controls. Contrary to the study of Chan et al,
29
neonatal oxygen treatment associated with more severely impaired SGaw, RV and FEV1.
(Hakulinen et al 1990) VLBW children showed increased airway reactivity, irrespective of
RDS, at 10-13 years of age, and DLCO was decreased in the non-RDS group (Galdès-Sebaldt
et al 1989). Later studies showed that VLBW children had a significant change towards
normal in FEV1 and RV in follow-up at 8-14 years. More improvement was seen in ELBW
children, who still had significantly more impaired values reflecting airflow, but not lung
volume and air trapping at age 14 years compared with term controls. Mechanical ventilation,
oxygen supplementation and BPD at 28 days had no effect on changes over time, but asthma
and exposure to smoking decreased the improvement. (Doyle et al 1999, Doyle 2000a)
Nikolajev et al (2002) assessed the lung function of discordant twins with LBW. They
showed that bronchial hyperreactivity was common in challenge tests at school age, but
small-for-gestational-age (SGA) was not associated with major impairment in lung function.
The increasing survival of more immature infants in the 1980´s focused the lung function
studies on VLBW, and oxygen supplementation at 36 weeks was mainly used as a definition
of BPD. These children had reduced values of airway flow, lower SGaw and lower DLCO than
controls, with associations with birth weight, suggesting structural changes in lung tissue due
to prematurity itself (Hakulinen et al 1996). BPD children had even more severely impaired
expiratory flow values and were more responsive to histamine than non-BPD children, which
was of clinical significance, as the latter finding associated significantly with respiratory
symptoms (Pelkonen et al 1997). In another study, impaired lung function was confirmed in
BPD, but not in non-BPD children born very prematurely, but their mean birth weight was
higher than in the former studies (Gross et al 1998). After severe BPD with a need for home
oxygen therapy, those with the most severely impaired expiratory flow had seriously
decreased diffusing capacity at the age of 11 years. Pulmonary dysfunction correlated with the
time of oxygen supplementation. Symptoms correlated with the reversible component of
airway obstruction rather than the fixed component. (Jacob et al 1998) In children born with
<800g of birth weight, low oxygen consumption in a treadmill test suggested a lower level of
fitness. Even with such a low birth weight and without apparent pulmonary abnormalities, the
children with BPD differed from the non-BPD group in the frequency of obstructive
abnormalities in lung function. (Kilbride et al 2003) After an exogenous surfactant trial,
spirometric parameters were better in children treated with surfactant compared to placebo,
suggesting that even in small preterm infants, advances in initial intensive care can improve
the pulmonary outcome (Pelkonen et al 1998).
30
7. Other indices associated with lung disease
Immune response
In asthma, the degree of inflammation is associated with the severity of basic lung function
impairment or the reactivity to bronchoconstrictors or exercise (Bousquet et al 1990, Venge
1994). The soluble markers of allergic inflammation have been reviewed by Venge (1994)
and the biopsy markers by Jeffery et al (2000b). Eosinophil-mediated damage of the
respiratory epithelium emerged as a major pathogenetic mechanism in asthma (Bousquet et al
1990), whereas COPD in adults involved a prominence of neutrophils (Lacoste et al 1993).
Merritt et al (1981) found a prominence of neutrophils and evidence of inflammatory injury in
the airways of newborn infants developing BPD. A secretion product of activated eosinophils,
eosinophil cationic protein, was elevated in the serum of asthma patients (Venge 1994).
Myeloperoxidase, secreted by activated neutrophils, was increased in bronchoalveolar lavage
fluid in COPD (Lacoste et al 1993). Lymphocytes were shown to be important in the
pathogenesis of both asthma (Robinson et al 1993, Azzawi et al 1990) and COPD
(O´Shaughnessy et al 1997, De Jong et al 1997), CD4 T-lymphocytes predominating in
asthma with eosinophils and CD8 T-lymphocytes in COPD with neutrophils and
macrophages, as reviewed by Jeffery (2000a).
Data on the inflammatory basis of lung function abnormalities at school age in children born
very prematurely are sparse. Treatment of low birth weight children with inhaled
glucocorticoids had no significant effect on baseline lung function or the airway response to
histamine, arguing against an inflammatory basis of the airway hyperresponsiveness in these
children (Chan & Silverman 1993). However, schoolchildren born very preterm were shown
to have a low CD4:CD8 lymphocyte ratio in peripheral blood in contrast to a normal
CD4:CD8 ratio found in asthma, bronchial lability associated with specific T-cell subsets and
elevated serum eosinophil cationic protein. The changes in lymphocyte subsets suggested the
immunological abnormalities to be related to BPD. (Pelkonen et al 1999)
Examination of induced sputum differential cell counts were a non-invasive method to
evaluate airway inflammation (Pavord et al 1997), but it is not an ideal routine test for
children, as it requires much work of skilled personnel and good cooperation of the patients.
31
Exhaled nitric oxide (eNO)
Nitric oxide (NO) gas is produced by various cells within the respiratory tract from L-arginine
in synthesis catalyzed by NO synthase (NOS) enzymes, as reviewed by Barnes & Belvisi
(1993) and Morris & Billiar (1994). There are at least three NOS isoenzymes: NOS1 (nNOS
or neuronal NOS), NOS2 (iNOS or inducible NOS) and NOS3 (eNOS or endothelial NOS)
(Yates et al 1995). All of the three isoenzymes have been detected in fetal lung and are
individually regulated (Sherman et al 1999, Aikio et al 2002). NO derived from constitutive
NOS (NOS1 and NOS3) is involved in the physiological regulation of airway function,
whereas NO derived from inducible NOS (in macrophages, endothelial, smooth muscle and
epithelial cells, fibroblasts and neutrophils) has an important role in respiratory inflammatory
reactions and host defence. NO is a potent vasodilator of bronchial circulation, a regulator of
pulmonary circulation and an important neurotransmitter in the neural bronchodilator system.
In 1991, Gustafsson et al first described NO in the exhaled air (eNO) of guinea pigs, rabbits
and human. Soon thereafter, elevated levels of eNO were reported in asthma patients (Alving
et al 1993, Kharitonov et al 1994, Persson et al 1994). The cellular origin of eNO was still
unclear. High concentrations were detected in the nasal air of normal subjects (Alving et al
1993), but when nasal contamination was prevented by expiration against resistance, eNO
was shown to originate from the lower respiratory tract (Kharitonov et al 1997). Oral
glucocorticoids reduced eNO in asthmatic patients, but not in healthy subjects (Yates et al
1995, Baraldi et al 1997). In patients with atopic asthma, inhaled glucocorticoids decreased
eNO (Kharitonov et at 1996), but did not prevent the increase in acute exacerbations in
children (Baraldi et al 1997). Viral respiratory infections raised (Kharitonov et al 1997) and
smoking reduced eNO (Persson et al 1994). In chronic obstructive disease (COPD), normal or
low eNO values were measured during the stable phase, but elevated levels might serve in
monitoring disease activity (Maziak et al 1998). In cystic fibrosis, low nasal and normal
exhaled NO values were reported (Lundberg et al 1996, Balfour-Lynn et al 1996). In a recent
study, eNO was superior to baseline lung function and bronchial responsiveness in identifying
preschool children with asthma (Malmberg et al 2003).
Infants with acute wheezy bronchitis had low eNO levels, while premature infants without
respiratory disease did not differ from term infants (Ratjen et al 2000). In ventilated preterm
infants, bronchoalveolar lavage fluid nitrate was similar in BPD, RDS and control children
during the first week of life, but remained high in those who later developed BPD (Vyas et al
1999). ENO levels were high during the second day in ventilated preterm infants. Despite the

32
absence of any significant association with the respiratory variables, the infants with the
highest levels manifested most severe BPD (Aikio et al 2002). Recently, high eNO
concentrations were related to BPD in face mask measurements at term (Leipälä et al 2004).
In evaluating the degree of airway inflammation in asthmatic children, eNO concentration and
sputum eosinophil counts were concordant. Thus, eNO was proposed as an easy-to-measure
marker of eosinophilic airway inflammation. (Piacentini et al 1999, Mattes et al 1999)
8. Follow-up of growth, neurodevelopment and cardiac function in children born
prematurely
Growth
In BPD children born in 1970-1980´s, growth retardation was common in early observations
at three years (Northway 1979) and in a follow-up at two years of age (Markestad &
Fitzhardinge 1981); in the latter study, it associated with severe and prolonged respiratory
dysfunction. In adolescence or early adulthood, those with BPD were significantly shorter and
weighed less than non-BPD individuals or term controls (Northway et al 1990b). Others found
no impairment of growth in severe BPD at the age of 10 (Bader et al 1987).
At school age, heights in relation to age among 20 children with BPD at 28 days were
significantly lower than those of term controls, and weights adjusted for height were also
lower. The non-BPD children did not differ from term controls. (Hakulinen et al 1996) The
children with BPD at 36 gestational weeks were shorter for age than those with no BPD or
controls (Pelkonen et al 1997). In a cohort study, VLBW children were shorter and lighter
and had smaller head circumferences at 14 years than those with normal birth weight, with
catch-up growth at 8-14 years. There were no differences in the stage of puberty. (Ford et al
2000) In that study, the ELBW girls were 4.5 cm and the ELBW boys 5.8 cm shorter at 14
years than the controls (Doyle 2000a), but no similar difference was detected at age 11 by
others (Kilbride et al 2003). In a 20-year follow up of VLBW children, boys were shorter and
lighter than controls at eight years, whereas girls were only lighter. Catch-up growth in
weight, height and body mass index occurred during 8-20 years of age among females; the
males remained smaller at 20 years, especially those who were SGA. (Hack et al 2003)
In the 1990´s, Barker presented a hypothesis of the fetal origin of coronary heart disease
(1995), and further studies consistently supported this finding of an association between low
33
birth weight, especially thinness at birth, catch-up growth in childhood and coronary disease
in adulthood (Forsén et al 1999). In a follow-up of growth, most VLBW infants born in the
surfactant era had not achieved the median birth weight of a fetus at the same gestational age
on hospital discharge. Appropriate-for-gestational-age infants, who did not develop BPD,
IVH, NEC or late sepsis, gained weight faster. (Ehrenkranz et al 1999) In a prospective study
of longitudinal growth, infants born at <29 gestational weeks had an initial period of poor
growth and a catch-up period at 4-5 years and mainly achieved normal weight and height by
seven years (Niklasson et al 2003).
Neurosensory development
Among the survivors of the original BPD group, grade repetition at school and abnormalities
in coordination, gait and muscle tone were reported; five out of 26 had CP, three had hearing
loss and one ROP compared with none of the controls (Northway 1990a). In a follow-up of 26
infants with BPD, 25% had low Bayley scores (<85) at 18 months, related to perinatal and
neonatal events rather than BPD (Markestad & Fitzhardinge 1981). In a population-based
Swedish follow-up cohort, the live birth prevalence of CP, especially spastic diplegia,
increased during the 1970-1980´s, reflecting the improved survival of VLBW infants
(Hagberg et al 1989). Later, no further increase was seen, but a slight decrease in preterm CP.
In 1991-1994, the prevalence was 81 per 1000 for infants of 1000-1499 g birth weight.
(Hagberg et al 2001) IVH and PVL were powerful predictors of CP (Hagberg et al 1996,
Salokorpi et al 1999). Despite the improved survival of more immature infants, the overall
incidences of CP and IVH have not increased. However, the risk of abnormal neurological
outcome increases sharply with decreasing birth weight. In a multicenter study (1995-1996),
30% of VLBW infants with brain ultrasound examinations (89%) had IVH, 11% had grade 3-
4 and 26% of the infants with 501-750 g birth weight had severe IVH. Cystic PVL was noted
in 5%. (Lemons et al 2001)
Besides IVH and CP, VLBW infants have an increased risk for other neurosensory
impairments, as reviewed recently by Tommiska [2003 (ELBW) and 2004a]. The families of
BPD children reported more need for physiotherapy and occupational therapy and more
concern for the child and impact of the child´s health on family life compared to non-BPD
children (Korhonen et al 1999a). At age 11, ELBW children were judged as occasionally
active or inactive by their parents, which differed from controls (Kilbride et al 2003).
34
Cardiac function
The severe �old� BPD was frequently accompanied by right ventricular hypertrophy and
cardiomegaly with cor pulmonale in electrocardiogram (Northway et al 1967, Markestad &
Fitzhardinge 1981, Northway 1990a) and by elevated right ventricular end-diastolic volume
and increased right ventricular wall thickness in echocardiography as late as school age
(Smyth et al 1981). After severe BPD with a need for home oxygen therapy, recurrent
episodes of heart failure were found in the children with most severely impaired lung function
(Jacob et al 1998). Pulmonary hypertension with increased pulmonary vascular resistance and
intrapulmonary shunting was demonstrated at cardiac catheterisation in children with severe
BPD at 3 months - 5 years of age associated with poor prognosis (Abman et al 1985, Berman
et al 1986, Bush et al 1990).
Pulmonary arterial pressure (PAP) can be assessed non-invasively by Doppler
echocardiography by measuring tricuspid valve regurgitation or pulmonary flow indices. PAP
is inversely related to the ratio between acceleration time (AT) and right ventricular ejection
time (RVET) (Kosturakis et al 1984). The VLBW children with BPD at 28 days born in the
late 1980´s had a slower drop in PAP than those without BPD, followed by an increase during
14-28 days of age (Gill & Weindling 1993). Furthermore, the children with BPD had lower
Doppler-mode-derived variables of pulmonary flow (AT, AT/RVET, pulmonary flow
velocity) at two years of age than those without BPD. The children with clinically severe BPD
and the most severe peripheral airway obstruction had the shortest acceleration time. (Farstad
et al 1995) In infants with RDS born in the 1990´s, the initially raised PAP remained
persistently elevated in a one-year follow-up in those who developed BPD. PAP was
inversely related to gestational age and corrected age at examination in preterm born infants
and to the duration of supplemental oxygen administration in infants with BPD. (Subhedar &
Shaw 2000) Previously, early findings of pulmonary hypertension were independently
associated with BPD at 36 weeks and suggested to be a sensitive marker of pulmonary injury
(Subhedar et al 1998). The cardiac findings in BPD have been recently reviewed by
Korhonen (2004a).
In children born in the late 1980´s or early 1990´s, no cardiac hypertrophy (Farstad et al 1995,
Korhonen et al 2004b) or significant pulmonary hypertension was seen at 2-7 years of age
(Korhonen et al 2004b).

35
9. Pharmacologic effects of glucocorticoids
Synthetic glucocorticoids, DEX and betamethasone, have a greater affinity for glucocorticoid
receptor than cortisol (7.1- and 5.4-fold higher, respectively), which additionally possesses
mineralocorticoid activity (Ballard & Ballard 1995, Jobe & Bancalari 2001).
Effects on the pulmonary defence systems
The initial studies in lambs suggested a response of the surfactant system to antenatal
glucocorticoids (Liggins 1969). Thereafter, all known components of surfactant have been
induced by treatment with glucocorticoids, presumably resulting in an increased content of
surfactant of normal composition and function, the effects depending on dosage and the stage
of lung development (Ballard & Ballard 1995, Vyas & Kotecha 1997). In the original
perinatal trial of our study population, after antenatal DEX, the requirements for surfactant
treatment were lower (Kari et al 1994), but no significant differences were seen in tracheal
fluid phosphatidylcholine despite the lesser need for ventilatory support (Kari et al 1995).
Another study showed an increase in surfactant proteins after postnatal glucocorticoid,
associated with improved initial lung function (Wang et al 1996).
In animals, glucocorticoids cause precocious increases in the activity of the antioxidant
enzymes superoxide dismutase, glutathione peroxidase and catalase. They regulate a
relatively small subset of proteins in lung cells, which act as important mediators of hormonal
effects. They induce both sodium-potassium-APTase and a subunit of the sodium channel
involved in the clearance of lung fluid from airspaces. (Ballard & Ballard 1995) Recently, in
preterm infants, the expression of epithelial sodium channel subunits was low but it was
increased by therapeutic doses of glucocorticoids (Helve et al 2004).
Glucocorticoids are among the most potent anti-inflammatory agents, but their role in lung
inflammation is poorly understood. DEX treatment has been shown to decrease nearly all
studied inflammatory indicators (Groneck & Speer 1995). In ventilated infants with BPD
(Yoder et al 1991) or RDS (Wang et al 1997), neutrophils and other anti-inflammatory
mediators were reduced in tracheal fluid, associated with improved pulmonary function, and
recently, early in RDS, downregulation of polymorphonuclear leukocytes and monocyte
activation was seen (Nupponen et al 2002). In rats, antenatal DEX has been shown to enhance
the abundance of endothelial NOS protein expression in lungs at birth (Lin et al 2001).
Recently, in ventilator-dependent infants, high eNO levels were shown to decrease after DEX
treatment (Williams et al 2004).
36
Effects on lung structure and growth
In animal studies, glucocorticoid treatment decreased the number of alveoli, which appeared
larger and more mature with reduced septal mesenchyme (Vyas & Kotecha 1997). In rats,
changes in the capillaries within the septa impaired the future formation of further alveoli
(Tschanz et al 1995, Tschanz et al 2003). Low-dose long-lasting postnatal DEX therapy
resulted in larger and fewer alveoli with reduced septal mesenchyme, leading to an
emphysematous condition, but a high-dose short-term treatment accelerated lung maturation,
followed by a step-back after discontinuation, with almost complete recovery, indicating that
both dosage and duration might be critical in terms of lung response (Tschanz et al 2003).
After antenatal glucocorticoids, the small but mature rat lungs at birth showed a growth
rebound and normal later development (Adamson & King 1988); others reported impaired
postnatal lung growth (Okajima et al 2001).
Retinoids are essential developmental mediators, and particularly all-trans retinoic acid
plays a key role in promoting septation. In neonatal rats, it also reversed the glucocorticoid-
induced inhibition of septation. (Massaro & Massaro 2000)
In sheep, single or repetitive maternal, but not fetal, betamethasone treatment caused
growth retardation persisting to term. Fetal treatment also improved lung function less,
suggesting that maternal glucocorticoids induce factors participating in lung maturation.
Repetitive treatment improved lung function more effectively than single treatment, but
concerns arose about decreased growth and neurodevelopment. (Jobe et al 1998) A review of
animal studies suggested that multiple courses of antenatal glucocorticoids improve lung
function, but decrease birth and lung weight and restrict brain growth (Aghajafari et al 2002a).
Scant data exist on human lung growth, mainly derived from lung function tests: no adverse
effect of antenatal DEX was seen in VLBW infants with little or no neonatal lung disease
during the first year of life (Wong et al 1982b).
Effects on other tissues
Glucocorticoids stimulate cytodifferentiation and cause precocious changes in different
tissues, accelerating the rate of differentiation without altering the sequence of developmental
events. They take part in glycogen metabolism, bile canaliculus formation, hematopoesis,
enzyme induction, intestinal maturation and ion exchange in kidneys and enhance the insulin
response to glucose and the adrenocorticotrophic hormone (ACTH) responsiveness of the
adrenal cortex, resulting in maturation of the catecholamine responses to birth in preterm
animals. The increased activity of myocardial adenylyl cyclase accounts for the improved

37
respiratory, cardiovascular and metabolic responses seen after treatment. (Ballard & Ballard
1995) The modulating effects on tissue differentiation involve interactions with other fetal
hormones, i.e. prolactin, thyroid hormones and catecholamines, insulin, EGF, interferon-γ and
testosterone. In humans, antenatal therapy with glucocorticoid and thyrotropin-releasing
hormone did not affect the incidence of RDS or BPD more than corticosteroid alone (Ballard
et al 1998), despite previous results (Ballard & Ballard 1995). Antenatal DEX decreased
plasma catecholamines, attenuating the birth-related increase (Kallio et al 1998, Banks et al
1999); others reported normal responses in tests stimulating human corticotrophin release at
one and two weeks after >8 courses and mild suppression in only some (Ng et al 1999). In
sheep, antenatal low-dose DEX suppressed the pituitary-adrenal function but augmented the
glycemic response to hypoxia (Fletcher et al 2000).
In human, concentrations of amniotic fluid cortisol and corticoid conjugates, primarily
derived from fetal cortisol, increase several-fold during the third trimester. Many infants with
RDS begin their recovery 48-72 hours after birth, which timing is consistent with the
accelerated production of surfactant in response to the elevation of cortisol that occurs in this
disease. Postnatal administration of hydrocortisone to infants with RDS did not improve their
clinical course, suggesting the postnatal elevation in endogenous levels to be sufficient to
induce lung maturity (Baden et al 1972). Thus, antenatal steroid is believed to mimic the
intrauterine and postnatal exposure to endogenous glucocorticoid (Ballard & Ballard 1995).
Very preterm infants may lack the capacity to produce enough cortisol to respond to
extrauterine stress, and infants who develop BPD were seen to have low cortisol levels and a
decreased response to ACTH after birth (Watterberg & Scott 1995). Low-dose hydrocortisone
increased survival without BPD in ELBW infants, when instituted shortly after birth,
particularly in those with chorioamnionitis (Watterberg et al 1999).
Brain development
Despite differences in the timing of the peak brain growth, the general sequence is similar in
animals and humans. Animal experiments have provided ample evidence of corticosteroid-
induced decrease in brain growth and abnormal development of the immature brain, but
depending on dosage and timing, glucocorticoids may either enhance or reduce brain injury
after a hypoxic insult (Huang et al 1999, Whitelaw & Thoresen 2000, Aghajafari et al 2002a).
In general, neurones in the human brain have stopped dividing by the third trimester, but
those in the dentate gyrus continue to divide long after full term and are thus vulnerable to
adverse influences. Despite the small molecular difference between betamethasone and
38
dexamethasone, their biological effects may differ. Among mice followed up into adulthood,
the antenatally betamethasone-treated group showed enhancement of memory compared with
the placebo group, whereas DEX treatment resulted in a decrement. (Rayburn et al 1997)
10. Trials on glucocorticoids during the antenatal - neonatal period
10.1. Glucocorticoid treatment of preterm infants
After initial discouraging attempts to prevent BPD in children with RDS by using
hydrocortisone (Baden et al 1972), DEX was adopted into use to facilitate the weaning of
VLBW infants from the ventilator (Mammel et al 1983, Avery et al 1985, Harkavy et al
1989, Kazzi et al 1990, Ohlsson et al 1992). The usual initial dose of DEX was 0.5 mg/kg/d
administered for 2-42 days with a different tapering schedule. In most studies, �open� steroids
were allowed afterwards. In a small study, a 42-day course at two weeks of age in infants
dependent on supplemental oxygen and mechanical ventilation was superior to an 18-day
course or placebo with respect to the pulmonary and neurodevelopmental outcome
(Cummings et al 1989). One study on oxygen-dependent infants at four weeks of age showed
more rapid improvement of ventilation in the DEX group, but no difference in the duration of
oxygen supplementation; new periventricular abnormalities on brain ultrasound scans were
reported (Noble-Jamieson et al 1989). A multicentre international trial, organized by
Collaborative Dexamethasone Trial Group (CDTG) (1991), studied the effect of 7-day
treatment on chronic oxygen dependency at three weeks of age in 287 VLBW infants born in
1986-1989. In the DEX group, the duration of further assisted ventilation was reduced, and
the infants with no mechanical ventilation at entry tended to need oxygen supplementation for
a shorter time. Hypertension and hyperglycemia were encountered. The Finnish study, in
which our study children participated, aimed to prevent BPD in infants dependent on
mechanical ventilation by earlier treatment at ten days of age. A shorter duration of
supplemental oxygen in DEX-treated girls, but not in all infants, and short-lived suppression
of basal cortisol were reported. Infants requiring ventilator at the age of ten days were at high
risk of developing BPD, as evaluated at the age of four weeks, and were thus not treated early
enough for the treatment to be truly prophylactic. (Kari et al 1993)
Apart from chronic oxygen dependency, with growing evidence of the inflammatory basis
of BPD (Yoder et al 1991, Groneck & Speer 1995), DEX was increasingly given soon after
birth to infants on mechanical ventilation for severe RDS. Pulmonary mechanics had already
39
been shown to improve and extubation by two weeks of age to increase among infants treated
within 12 hours after birth in an early study before the surfactant era (Yeh et al 1990). In an
Israeli multicentre trial of 248 preterm infants on mechanical ventilation with more than 40%
oxygen for RDS, treated with rescue surfactant, early postnatal DEX did not reduce the
incidence of BPD at either 28 days or 36 gestational weeks of age. The lesser need for
mechanical ventilation at the age of three days was not sustained at seven days of age.
Gastrointestinal hemorrhage associated with DEX. (Shinwell et al 1996) However, 43 VLBW
infants on mechanical ventilation showed significant improvement in respiratory compliance
and tidal volume, with further increase until seven days of age: the fraction of inspiratory
oxygen (FiO2) was reduced, weaning was facilitated, and there was less BPD at 36 weeks
(DEX 10%, placebo 47%). As the decreasing beneficial effect of surfactant increases the
susceptibility to barotrauma in the second week of life, the initiation of glucocorticoids during
this time could have minimized the lung injury and thus explained these results. (Durand et al
1995)
The initial goal was to rescue severely ill VLBW infants from prolonged mechanical
ventilation and to prevent BPD. With the increasing use in less severe disease or as
prophylaxis, there was growing concern of the long-term sequelae. Ng (1993) reviewed ten
postnatal DEX trials: hyperglycemia, hypertension, adrenal suppression and growth
impairment were common but usually reversible. Gastrointestinal bleeding, pulmonary air
leak, osteopenia, bone fracture, immunosuppressive effects and hypertrophic cardiomyopathy
were seen. Although no major neurodevelopmental risk was found in studies of antenatal
DEX, attention was raised to identify all treatable causes preventing successful weaning
before starting steroid treatment, such as anemia, PDA and sepsis.
Bhuta & Ohlsson (1998) reviewed ten studies of postnatal DEX treatment before 14 days of
life. The risk of BPD at 28 days or 36 gestational weeks was significantly reduced, especially
in infants treated at 7-14 days of age, in whom mortality was reduced as well. In this group,
only three children would need to be treated to prevent one infant from developing BPD.
More recent meta-analyses reviewed separately trials in which glucocorticoid, usually DEX,
was started either early (<96 hours), moderately early (7-14 days) or delayed (>3 weeks) after
birth (Halliday & Ehrenkranz 2000a, 2000b, 2000c).
40
Early postnatal glucocorticoid treatment
A meta-analysis of early postnatal corticosteroids for preventing BPD covered the following
studies: Baden et al 1972 (hydrocortisone), Yeh et al 1990, Sanders et al 1994, Shinwell et al
1996, Rastogi et al 1996, Suske et al 1996, Subhedar et al 1998, Wang et al 1997, Yeh et al
1997, Mukhopadhyay et al 1998, Tapia et al 1998, Garland et al 1999, Kopelman et al 1999,
Lin et al 1999, Romagnoli et al 1999, Soll et al 1999, Stark et al 1999, Watterberg et al 1999
(hydrocortisone) and Sinkin et al 2000 (Halliday & Ehrenkranz 2000a). Surfactant use was
common in most studies. DEX treatment did not reduce mortality, but facilitated weaning and
reduced the risk of PDA and pulmonary air leaks. Death or BPD and BPD at 28 days or 36
weeks were decreased, and the recipients of DEX required less steroids during the later
respiratory course. The risks of hyperglycemia, hypertension and growth failure,
gastrointestinal bleeding, intestinal perforation and hypertrophic cardiomyopathy were
increased, but no increase of NEC, infection or pulmonary hemorrhage was detectable. The
risk of severe IVH, PVL or severe or any ROP was not affected, either. The infants who
underwent cranial ultrasound scans showed a borderline increase in the risk of PVL (Soll et al
1999). In one study of a 3-day course in surfactant-treated RDS infants with a high risk for
BPD, IVH of any grade was more common in the placebo group (Garland et al 1999). Two
studies presented neurological follow-up data with increased risks of abnormal neurological
examination, developmental delay, CP and death or CP (Yeh et al 1998, Shinwell et al 2000).
A pilot study of low-dose hydrocortisone for 12 days in 40 ELBW infants revealed increased
survival without BPD at 36 weeks and reductions in the duration of oxygen supplementation
and mechanical ventilation with no detectable difference in side effects (Watterberg et al
1999).
In a recent study, early postnatal DEX was given as a 3-day course at a lower dose of 0.15
mg/kg/d, followed by 7-day tapering, to 220 ELBW infants on mechanical ventilation. The
risks of death and BPD at 36 weeks did not differ, but the DEX-treated infants were less
likely to receive supplemental oxygen at 28 days and open DEX later. Spontaneous
gastrointestinal perforation, especially with indomethacin use, was more common in the DEX
group, as were lower weight and smaller head circumference at 36 gestational weeks. (Stark
et al 2001)
Moderately early postnatal glucocorticoid treatment
A meta-analysis of moderately early postnatal corticosteroids for preventing BPD included
the following studies: Cummings et al 1989, Kari et al 1993, Brozanski et al 1995, Durand et

41
al 1995, Kovacs et al 1998, Papile et al 1998 and Romagnoli et al 1998 (Halliday &
Ehrenkranz 2000b). DEX treatment reduced mortality at 28 days, death or BPD and BPD at
28 days or 36 weeks and the need for later steroids and facilitated extubation, but had no
effect on the risk of pneumothorax or NEC. Adverse effects included hyperglycemia,
hypertension, gastrointestinal bleeding, hypertrophic cardiomyopathy, adrenal suppression
(Kari et al 1993) and infection. One study showed significant differences in pulmonary
mechanics and oxygen need at two days after DEX treatment with less BPD at 36 weeks
(Durand et al 1995). In a study of 3-day treatment followed by 18 days of nebulized
budesonide, the steroid group required less ventilatory support and supplemental oxygen at
the second week of age and had better pulmonary compliance at ten days, but the
improvements were not maintained, and the incidence of BPD at 36 weeks was not decreased
(Kovács et al 1998). There was no effect on the incidence of severe IVH or severe ROP, but
one study presented, apart from diminished weight gain, slowing down of head growth during
DEX treatment in both 2-week and 4-week groups (Papile et al 1998). Only one long-term
follow-up was available, with no increase in adverse neurological outcome (Cummings et al
1989).
Delayed postnatal glucocorticoid treatment
A meta-analysis of delayed postnatal corticosteroids for chronic lung disease included the
following studies: Ariagno et al 1987, Avery et al 1985, Harkavy et al 1989, Noble-Jamieson
et al 1989, Kazzi et al 1990, CDTG 1991, Ohlsson et al 1992, Vincer et al 1998 and Kothadia
et al 1999 (Halliday & Ehrenkranz 2000c). Surfactant was not used in most of the studies.
DEX treatment improved respiratory compliance, facilitated extubation and reduced the need
for oxygen supplementation and later steroids, but had no effect on survival or the duration of
hospitalization. Only one study reported the incidence of BPD at 36 weeks to be decreased
with borderline significance and death or BPD at 36 weeks to be decreased (Kothadia et al
1999). Poor weight gain was seen in the DEX group, but no increase in the risk of infection,
NEC or gastrointestinal bleeding. Abnormal neurological findings were increased in the
DEX-treated children, but moderate to severe neurological impairment was not, either overall
or in survivors. The increased risk of CP in survivors was of borderline significance, but in
keeping with the findings of early postnatal treatment. No increase in blindness was detected.
42
Neurodevelopmental outcome after postnatal dexamethasone treatment
A non-significant increase in cranial ultrasound abnormalities was reported after DEX
treatment (Noble-Jamieson et al 1989, O´Shea et al 1999, Shinwell et al 2000), and an �early�
trial of ELBW infants was discontinued because of adverse outcome, particularly PVL (Soll
et al 1999, the Vermont Oxford Network Steroid Study Group 2001). On the contrary, one
study reported more IVH in the placebo group (Garland et al 1999). In a study of ELBW
infants, postnatal but not antenatal DEX exposure was associated with abnormal brain
ultrasound findings and worse neurodevelopmental outcome at 18 months (LeFlore et al
2002). Poorer head growth was detected at the age of 30 days in infants treated moderately
early with 14-day DEX, compared to a 7-day early course (Romagnoli et al 1999). Later, even
an early 3-day course at a lower dose of 0.15 mg/kg/d associated with a smaller head
circumference at 36 weeks of gestational age in ELBW infants (Stark et al 2001).
Follow-up studies of randomized trials have been few in number. In the trial of Cummings et
al (1989), less abnormal neurodevelopmental outcomes (abnormal examination or Bayley
developmental index) were seen at 15 months of age after a 42-day course at two weeks (2
infants out of 9) compared to a 18-day course (7 out of 9) or placebo (3 out of 5), but another
small study of a 12-day course failed to reveal any difference in Bayley scores at two years of
age (Bhuta & Ohlsson 1998).
In the follow-up of 209 children oxygen-dependent at three weeks in the CDTG trial
(1991), no clear difference was evident at the age of three years in CP (20% vs 17%) or any
other neurological disability after a 7-day course, but less hearing loss was suggested in the
DEX group. Their disability score was described in our methods. Altogether 19% of the
infants had CP, 8% had visual loss, and 16% suffered from hearing loss; 19% were classified
as severely disabled and 35% as severely or moderately disabled; 18% were expected to need
special school education and 13% extra help at school. The need for physiotherapy (42%),
speech therapy (32%), occupational therapy (16%) and special schooling was common, but
similar in both groups. Underestimation of disability was suggested to be due to the methods
used. Neurological impairment was more common in the subgroup dependent on a ventilator
at recruitment than those on oxygen only. (Jones et al 1995)
In another trial of 118 infants, a 42-day course at 15-25 days of age increased the risk of
CP (DEX 25% vs placebo 7%) and abnormal neurological examinations, such as hypotonia or
possible or definite CP (45% vs 16%) at one year of age. Of the DEX-treated infants with CP,
44% had normal neonatal brain ultrasound scans. (Kothadia et al 1999, O´Shea et al 1999)

43
Similarly, in two trials of early DEX, a 3-day course increased the incidence of CP (49%
vs 15%), particularly spastic diplegia (28% vs 6%), and developmental delay (55% vs 29%) at
2-6 years of age (Shinwell et al 1996, Shinwell et al 2000), and a 4-week course increased
neurological abnormality, especially diplegia and hypotonia, at two years (40% vs 17%) (Yeh
et al 1997, Yeh et al 1998). In the study of Shinwell et al, all infants with PVL, 38% of IVH
grade 1-2 and 53% of IVH grade 3-4 developed CP; 22% of the children with CP had normal
neonatal ultrasound scans, all treated with DEX. In the study of Yeh et al, more fast activity
in electroencephalograms (EEG) was seen in the DEX group, with no correlation with the
outcome, but the overall abnormalities in EEG, brain stem auditory evoked potential and
visual evoked potential did not differ between the groups. The incidence of CP was twofold in
children treated with DEX compared to those with placebo. No difference was seen in either
visual (Yeh et al 1998, Shinwell et al 2000) or hearing problems (Shinwell et al 2000).
The differences in neurological outcome were not confirmed in a recent small follow-up
study at three years (Romagnoli et al 2002).
Barrington (2001) reviewed eight randomized controlled trials with neurodevelopmental
follow-up data of 679 survivors out of 1052 participants. According to the meta-analysis,
postnatal glucocorticoid was associated with an increase in CP and neurodevelopmental
impairment. The studies with less than 30% contamination with open steroid later showed a
greater steroid effect, and the relative risk of CP was 2.86 (95% confidence interval: 1.95-
4.19). The conclusion was to abandon the use of steroids for this indication in the absence of
evidence of any long-term benefits.
Growth after postnatal dexamethasone treatment
Poor growth and weight gain are common findings associated with DEX, but usually
reversible (Ng 1993, Halliday & Ehrenkranz 2000ac). Diminished weight gain was shown
during 2-week and 4-week courses (Papile et al 1998) and after a 2-week moderately early
and a one-week early course, but catch-up occurred soon (Romagnoli et al 1999). A recent
study of ELBW infants reported a significantly lower weight even after a low dose (Stark et al
2001).
In the follow-up of the CDTG trial (1991), no statistical differences emerged in growth at
the age of three years after 7-day postnatal treatment with DEX or placebo. Height, weight
and head circumference were below the average in both groups. (Jones et al 1995) After early
treatment, in a study of a 4-week course, which initially decreased the high need for oxygen,
44
somatic growth did not differ at two years of age in girls, but the DEX-treated boys were
shorter and weighed less than the controls (Yeh et al 1998), while a 7-day course had no
effect on growth at three years of age (Romagnoli et al 2002).
Respiratory morbidity and lung function after postnatal dexamethasone treatment
The short-term benefits of DEX to respiratory morbidity are evident and have been described
previously. The initial improvement of pulmonary mechanics (Yeh et al 1990, Durand et al
1995) was concomitant with the acute suppression of pulmonary inflammation (Yoder et al
1991), but resulted in only a modest decrease in the incidence of BPD at 36 gestational weeks.
In the follow-up of the CDTG trial (1991), despite improved weaning from the ventilator,
no beneficial or adverse effects of a 7-day course on respiratory morbidity were evident at the
age of three years. In all, based on questionnaires, 38% had frequent episodes of coughing or
wheezing on exercise, at night or with common cold, and 48% had had at least one admission
to hospital. In the DEX group, consultations for respiratory problems were more common and
an excess of cot deaths were reported, even though late mortality was similar in both groups.
(Jones et al 1995) However, a 4-week course of early DEX, which decreased the initially high
need for oxygen and the incidence of PDA, associated with a lower incidence of upper
respiratory infections and rehospitalization for respiratory reasons at the age of two years
(Yeh et al 1998); frequent rehospitalizations until the age of one year were also less common
after a delayed 42-day course (O´Shea et al 1999). The follow-up studies of randomized trials
did not assess lung function after treatment.
Cardiovascular findings after postnatal dexamethasone treatment
Hypertension, as a common finding, and cardiomyopathy or myocardial hypertrophy were
encountered after DEX treatment, but were usually reversible (Werner et al 1992, Ng 1993,
Evans 1994, Yeh et al 1997). However, DEX-induced fatal cardiomyopathy has been reported
(Riede et al 2001).
In the cardiac follow-ups during randomized trials of a 42-day (Kothadia et al 1999) and a
7-day course (Romagnoli et al 1999), DEX-associated ventricular septal hypertrophy and left
ventricular ourflow obstruction were usually reversible within one month, but had clinical
significance in some infants (Bensky et al 1996, Zecca et al 2001). Long-term follow-up has
not been reported.
45
Recommendations and practice of postnatal dexamethasone treatment
Despite the short-term benefits seen in infants treated moderately early, due to the initial
findings on neurological outcome, early postnatal treatment is not indicated as a treatment of
respiratory failure. Corticosteroids have been suggested to be reserved for infants not weaning
from mechanical ventilation and studies made on lower doses, other steroids, alternative
routes and late outcomes among survivors of randomized trials. (Halliday & Ehrenkranz
2000abc) Others proposed to abandon the use of steroids for this indication, as no evidence of
long-term benefits exists. In 2002, The American Academy of Pediatrics published guidelines
for the use of postnatal steroid treatment and stated that it should not be routine and should be
limited to �exceptional clinical circumstances�, such as infants on maximal ventilatory and
oxygen support. The publication of concerns reduced the use of postnatal DEX: in Israel, 22%
of infants were treated with open DEX after the age of seven days in 1994, compared with 6%
of similarly high-risk infants in 2001 (Shinwell et al 2003). Still, the Vermont-Oxford
Network data showed that 40% of ELBW infants in the participating institutions received
postnatal DEX by the age of 28 days in 1999 (Barrington 2001), and 48% of European units
also used DEX for non-intubated infants (Truffert et al 2003). The possible indications,
quality, dosage, duration and time of administration of corticosteroid for the prevention or
treatment of BPD remain one of the most controversial issues in neonatal medicine (Halliday
2003).
10.2. Antenatal glucocorticoid treatment
Prevention of neonatal diseases
After their introduction for fetal maturation 30 years ago, antenatal glucocorticoids were
slowly incorporated into clinical practice, due to the variable interpretations of the evidence
leading to conflicting advise, fear of long-term adverse effects and advances in the care of
VLBW infants. A meta-analysis of 15 randomized controlled trials showed them to reduce
mortality, RDS, IVH and NEC (overall reduction in the odds about 40%, 50%, 60% and 70%,
respectively) in infants born before 34 gestational weeks: Liggins & Howie 1972, Block et al
1977, Morrison et al 1978, Papageorgiou et al 1979, Schutte et al 1979, Taeusch et al 1979,
Doran et al 1980, Teramo et al 1980, Collaborative Group on Antenatal Steroid Therapy
(CGAST) 1981, Schmidt et al 1984, Morales et al 1986, Carlan et al 1991, Garite et al 1992,
Kari et al 1994 (Crowley 1995). The benefits were greater when the glucocorticoids were
administered 24 hours - 7 days before birth or even earlier, additively to those derived from
46
surfactant, and in case of premature rupture of membranes. Even treatment <24 hours before
birth decreased IVH (Kari et al 1994). Their effect on infection was equivocal, and no effect
was found on PDA (Eronen et al 1993, Kari et al 1994) or BPD. The few available follow-up
studies did not reveal adverse neurological outcomes (MacArthur et al 1982, CGAST 1984,
Smolders-de Haas et al 1990); on the contrary, protective effects were suggested (Crowley
1995). A study of an observational database of 35 000 VLBW infants supported the reduction
in IVH but not in NEC and reported a decrease in PDA and an increase in infection (Wright et
al 1995). In 1994, based on the meta-analysis, the NIH Consensus Development Conference
recommended antenatal glucocorticoids for women at risk of premature delivery (24-34
gestational weeks), as cost-saving therapies to reduce mortality and morbidity: either two 12-
mg doses of betamethasone given intramuscularly 24 hours apart or four 6-mg doses of DEX
12 hours apart, preferably 24 hours - 7 days before birth, but even later. The role in high-risk
conditions, such as hypertension and diabetes, was not established. Treatment was
recommended even with the available surfactant, as the latter alone had little or no impact on
the incidence of IVH or PDA. (NIH 1995)
Thereafter, maternal administration increased, even as repeated courses after seven days
for those who remained undelivered. Multiple courses were not recommended, as no
additional short-term benefits were seen in non-randomized studies, but instead, there was
increased mortality with lower gestational age (Banks et al 1999) and a trend towards more
BPD (French et al 1999). Randomized or quasi-randomized trials of 3700 infants showed a
consistently significant reduction in mortality, RDS and IVH with no adverse consequences
of a single course of betamethasone, DEX or hydrocortisone, but treatment >7 days before
delivery was not proved effective (Crowley 2000), as initially suggested by Liggins & Howie
(1972). In a further analysis of three randomized controlled trials of 551 infants (Guinn et al
2001, Aghajafari et al 2002b, McEvoy et al 2002), repeated doses decreased the risk of any
severe lung disease (Guinn et al 2001) and the need for surfactant (Guinn et al 2001, McEvoy
et al 2002). No difference was found in perinatal death, IVH or PVL. (Crowther & Harding
2003)
Neurodevelopmental outcome after antenatal glucocorticoids
Antenatal glucocorticoids prevent IVH (Crowley 1995, Wright et al 1995, Crowley 2000),
and the first follow-up studies also suggested protection against adverse neurological outcome
(MacArthur et al 1982, CGAST 1984, Smolders-de Haas et al 1990, Crowley 1995, Salokorpi
et al 1997). Data on animal studies (Jobe et al 1998, Huang et al 1999, Whitelaw & Thoresen
47
2000, Aghajafari et al 2002a) and postnatal glucocorticoids (Yeh et al 1998, Shinwell et al
2000) aroused concern about possible long-term effects on neurodevelopmental outcome. In a
prospective cohort study, repeated courses were associated with a 4% reduction in head
circumference at birth, representing a nearly 11% reduction in cranial volume (French et al
1999) and presenting an increased risk for abnormal neurodevelopment (Hack et al 1991). In
a retrospective study of 883 infants, DEX (11%) but not betamethasone (4.4%) was
associated with an increased risk of cystic PVL, a major cause of CP, compared with no
glucocorticoid treatment (8.4%) (Baud et al 1999). In the original trial of our study, abnormal
brain ultrasound findings, including PVL, were decreased (Kari et al 1994), and in a
prospective study of ELBW infants, they were not increased after antenatal DEX on hospital
discharge (LeFlore et al 2002). No association was found between brain weight and antenatal
glucocorticoids in preterm infants who died (Murphy 2001).
Few long-term follow-up results of randomized antenatal glucocorticoid trials continued until
school age or adulthood are available. In a Dutch follow-up trial of 81 adults born at 27-40
gestational weeks in the 1970´s, those treated with a single course of betamethasone did not
differ from placebo-treated controls in CP or cognitive function at the age of 20 years
(Schutte et al 1980, Dessens et al 2000). Previous follow-up studies of 250 out of 304
survivors after antenatal betamethasone (Liggins & Howie 1972, MacArthur et al 1982) and
406 out of 739 infants after DEX trial (CGAST 1981, 1984), revealed no negative
neurological outcome at six years or three years of age, respectively. In the previous
Auckland trial, betamethasone-treated girls scored better than control girls in school
behaviour. In the Collaborative study, mental and psychomotor development was assessed at
nine and 18 months and cognitive abilities at 36 months of age.
In an Australian cohort study, teenagers who had been exposed to antenatal betamethasone
in the early 1980´s showed better cognitive functioning at 14 years of age compared to
VLBW controls and tended to have less CP (Doyle et al 2000b). The cohort study of French et
al (1999) assessed 327 infants at three years of age: CP was found in 7.8% of the non-
corticosteroid group, 5.1% of the single-course group, and none in the group given repeated
courses. The disability rate did not differ, despite initial differences in head growth, but was
small in all groups.
48
Growth after antenatal glucocorticoids
Decreased birth weight has been associated with antenatal DEX (Bloom et al 2001) and with
multiple courses of glucocorticoids (Banks et al 1999). In the study of French et al (1999),
repetitive courses impaired fetal growth, but no difference persisted at the age of three years.
In the follow-up studies of randomized trials, no harmful effects on growth, i.e. height,
weight or head circumference, were reported at 3-20 years of age (MacArthur et al 1982,
CGAST 1984, Smolders-de Haas et al 1990, Dessens et al 2000). After antenatal DEX, body
weight and height were slightly greater at three years of age (CGAST 1984), and girls given
betamethasone were taller and heavier at six years (MacArthur et al 1982) than the controls in
the placebo group. The Dutch study reported a delay in puberty in boys (Smolders-de Haas et
al 1990).
In a non-random cohort study, the children exposed to antenatal betamethasone were
significantly taller than those not exposed, with no difference in sexual development (Doyle et
al 2000b).
Respiratory morbidity and lung function after antenatal glucocorticoids
Antenatal glucocorticoids halved the risk of RDS, but had no consistent effect on BPD at 28
days (Crowley 1995, Wright et al 1995, Crowley 2000). Nor did a case-referent study of 1454
VLBW infants born in the surfactant era show any change in BPD at 36 gestational weeks
(Van Marter et al 2001). Repeated doses have been shown to decrease the risk of severe lung
disease and the need for surfactant, but there are no data on long-term safety (Crowther &
Harding 2003).
In studies of lung function, infants treated with a single course of betamethasone were
shown to have higher FRC and better respiratory system compliance than matched untreated
infants within 36 hours, prior to surfactant treatment. No significant difference was found in
specific compliance or Raw, suggesting that there was recruitment of alveoli without
significant overdistension (McEvoy et al 2001). Compliance was higher after multiple courses
(McEvoy et al 2000).
Respiratory morbidity is infrequently assessed in follow-up studies of randomized trials.
More hospital admissions because of infections or respiratory diseases during the first year
were reported after betamethasone (Smolders-de Haas et al 1990) and more respiratory
complications at 18 months of age after DEX (CGAST 1984).
Data on the long-term effects of DEX treatment on lung function are sparse. Follow-up
studies of 75 children 10-12 years after a betamethasone trial (Smolders-de Haas et al 1990)
49
and of 20 children six years after a DEX trial (Wiebicke et al 1988) revealed no negative
effects of glucocorticoid on lung function. In a cohort study of betamethasone, no significant
differences were seen in lung function, assessed by spirometry and body plethysmography, at
the age of 14 years between those with and without exposure to glucocorticoids (Doyle et al
2000b).
Cardiovascular findings after antenatal glucocorticoids
In randomized trials comparing the fetal effects of antenatal glucocorticoids, betamethasone
reduced and DEX increased fetal heart rate variation (Mulder et al 1997), both induced
profound suppression of heart rate acceleration and variability at 48 hours, with a more
marked decrease after betamethasone (Rotmensch et al 1999), and the reversible fall in
variability was preceded by an initial increase with no differences between the groups (Subtil
et al 2003). All changes were reversible. In the meta-analyses of randomized studies, no effect
was found on PDA (Crowley 1995), but the observational database showed a decrease in
incidence (Wright et al 1995). No overall effect, but a beneficial effect on ductal closure in
infants born at <30 gestational weeks was reported (Eronen et al 1993).
Antenatal DEX did not appear to affect cardiac dimensions and blood flow velocity in
preterm infants during the first month of age (Skelton et al 1998). No studies exist on the
long-term effects of antenatal glucocorticoid on heart function or growth.
50
AIMS OF THE STUDY
In this follow-up study of two randomized trials, we investigated the effects of antenatal or
neonatal dexamethasone treatment on cardiopulmonary function, somatic growth and
neurosensory development at school age in children born very prematurely, by using different
lung function methods, cardiac evaluation, hospital data and questionnaires. Furthermore, we
wanted to assess the possible role of inflammation in bronchopulmonary dysplasia.
The specific aims of the present study:
I To assess the oscillometric method in detecting abnormalities of lung function
in children with or without bronchopulmonary dysplasia, compared with
conventional lung function tests.
II To study the possible inflammatory basis of abnormal lung function in
bronchopulmonary dysplasia by measuring exhaled nitric oxide concentrations.
III To evaluate cardiopulmonary function, growth and neurosensory development
after neonatal dexamethasone treatment for persistent respiratory failure.
IV To investigate cardiopulmonary function, growth and neurosensory
development after antenatal dexamethasone treatment for imminent preterm birth.
51
PATIENTS AND METHODS
1. Patients
The 49 children in the present study were born very prematurely in 1989-1991, at gestational
ages of <31 weeks or birth weights of <1500 g, and they were treated in the Neonatal
Intensive Care Unit of the Hospital for Children and Adolescents, Helsinki University Central
Hospital. They were included in one of two randomized double-blind placebo-controlled
trials: postnatal DEX therapy in VLBW infants at risk for BPD (Trial 1) (Kari et al 1993) or
prenatal DEX therapy in conjunction with exogenous surfactant therapy (Trial 2) (Kari et al
1994). They represent the major arms of multicentre trials, where the patients in Helsinki
were randomized as separate groups. Three children participated in both trials. Additionally,
one twin sister of a Trial 1 participant was included in the present study (I and II).
The entry criteria for Trial 1 were: 1) birth weight <1500 g; 2) gestational age >24 weeks; 3)
dependence on mechanical ventilation at ten days of age; and 4) no signs of ductus arteriosus,
sepsis, gastrointestinal bleeding or major malformation. A total of 23 infants received either
DEX (Oradexon®, Organon, Oss., The Netherlands) 0.5 mg/kg per day, divided into two
doses, for one week (DEX group) or an equivalent volume of saline (placebo group). Open-
label DEX therapy was allowed after 28 days of age at the discretion of the attending
neonatologist. During the initial hospitalization, three infants died: one boy in the DEX group
and one boy and one girl in the placebo group. The 20 surviving children (DEX 10, placebo
10) were invited to participate in this follow-up study: one child was excluded because of
neurological handicap, one family refused to participate and two could not be traced. Thus, 16
(80%) children participated in the present study (I, II and III). In addition, data on the
neurological outcome of all non-participants were collected from hospital records up to the
age of 5-7 years (III).
In Trial 2, 112 pregnant women with imminent preterm delivery before 32 weeks of gestation
were recruited and received either four doses of DEX (Oradexon®, Organon, Oss., The
Netherlands), 6 mg at 12-hour intervals intramuscularly (DEX group) or an equivalent volume
of saline (placebo group). 138 live-born babies were delivered (DEX 74, placebo 64).
Fiftynine infants were born at <31 weeks of gestation (DEX 37, placebo 22), of whom 14 died
52
during the initial hospitalization and one at five months of age (DEX 6, placebo 9). The 44
surviving children (DEX 31, placebo 13) were invited to participate in this follow-up study:
nine of them could not be evaluated, but data on their outcome were collected from hospital
records. A total of 35 (80%) children participated in the present study (DEX 87%, placebo
62%) (I, II and IV). Besides, the limited data available on the neurological outcome of 43
children at school age were analyzed (DEX 100%, placebo 92%) (IV).
Eighteen healthy non-atopic children born at term were recruited as controls for the lung
function tests. The study was approved by the institutional ethics committees. Written
informed consent was obtained from the parents.
2. Neonatal and follow-up data collection
Data on the initial hospitalization and supplemental oxygen requirements were collected in
order to characterize the severity of the infants´ primary respiratory and neurosensory disease.
The fraction of inspiratory oxygen (FiO2) was recorded at the postnatal ages of 2, 6, 12, 18,
24, 48, 72, 96 and 120 hours. The mean FiO2 requirements during 120 hours were calculated
on the basis of the areas under the curve. The duration of supplemental oxygen, FiO2 >0.4
requirements and dependence on supplemental oxygen at the ages of 28 days and 36 and 40
gestational weeks were recorded, as were the duration of ventilator treatment and initial
hospitalization. BPD was defined as a requirement for supplemental oxygen at a postnatal
gestational age of 36 weeks (Shennan et al 1988). The length of open-label DEX therapy after
28 days was recorded. The diagnoses of IVH (Papile et al 1978), PVL (Bejar et al 1986) and
ROP (International classification 1984) were established using standard methods. Abnormal
brain ultrasound findings were defined as IVH or PVL. PDA was regarded as significant if it
required indomethacin treatment or surgical closure. Small-for-gestational-age (SGA) infants
weighed <-2 SD from the mean birth weight for each gestational week (Pihkala et al 1989).
All hospital records were reviewed. Secondary hospitalization during infections, history of
wheezing and use of glucocorticoids or bronchodilators were regarded as signs of respiratory
morbidity. Major neurological problems and neuropsychological status at the age of five
years, major visual and hearing deficits and the conclusions drawn from school maturity
assessments were recorded. The diagnosis of CP was based on findings of abnormal muscle
tone, exaggerated tendon reflexes and a positive Babinsky sign and on persistent or
exaggerated primitive reflexes, dyskinesia or ataxia. The degree of disability was classified
53
according to Jones et al (1995): severe disability was defined as CP, severe global delay or
sensory or other impairment necessitating special school attendance. Moderate disability was
defined as mild CP, severe deafness, moderate global delay (extra help needed at school,
assessment of global retardation or language problems) or home oxygen use beyond three
years of age, but not severe enough to require education at a special school. Possible
cardiovascular medication or intervention was recorded.
3. Study protocol
All of the 49 children enrolled in the study were serially evaluated during 1998-1999 in the
Outpatient Department of Allergic Diseases, Helsinki University Central Hospital. At the first
visit, the principal investigator carried out the physical examination. The transformation of
body height into standard deviations (SDs) was based on the Finnish growth standards, with
standard curves constructed using group mean values and SDs for height at certain ages and
according to gender (Sorva et al 1990). Relative weight was calculated as the percentage
deviation from the median weight of Finnish children of the same height and gender.
Moderate or severe neurological impairment was recorded. The questionnaires focused on
respiratory symptoms and medication used during the preceding year and the history of
smoking or atopy in the family. Frequent respiratory symptoms were defined as dyspnea,
prolonged coughing for >2 months or recurrent coughing during exercise or at night. Impulse
oscillometry, flow-volume spirometry and pulmonary diffusing capacity test were done in the
Lung Function Laboratory of the Division of Allergy, Helsinki University Central Hospital.
The principal investigator, unaware of the neonatal history of each child at the time of testing,
supervised the lung function tests, supported the children to succeed in the test performance
and evaluated their co-operation for further lung tests. The children were examined clinically
when free of respiratory infections or allergic symptoms. Skin tests were performed by skin
prick with ten common environmental allergen extracts (birch, timothy grass, meadow fescue
and mugwort pollens, cat, dog, horse and cow epithelial danders, house dust mite Dermato-
phagoides pteronyssimus and spores of Cladosporium herbarum), negative vehicle and
positive histamine hydrochloride (10 mg/ml). Atopy was defined as at least one wheal
reaction >3 mm in diameter in the absence of a response to the negative control solution.
During the second visit, exhaled nitric oxide measurement and whole-body plethysmography
were performed in the Division of Clinical Physiology, Helsinki University Central Hospital.
54
The children were to have been clinically free of respiratory infections or allergic symptoms
for at least three weeks. Children on glucocorticoid inhalation therapy during infections were
examined more than three weeks after the discontinuation of their glucocorticoid, and those
on regular glucocorticoid inhalation therapy had a 24-hour glucocorticoid-free interval before
the measurement. β2-sympathomimetic agents were not allowed for 12 hours before the
measurement. Exposure to tobacco smoke and physical exercise were avoided on the same
morning.
During the third visit, a chest X-ray was taken, echocardiography was performed, and
electrocardiogram (ECG) readings were analysed by a pediatric cardiologist at the Division of
Pediatric Cardiology, Helsinki University Central Hospital.
.
4. Lung function methods
Flow-volume spirometry (I to IV)
Flow-volume spirometry was performed with a pneumotachometer-based spirometer
(Spirotrac III, Vitalograph Ltd, Buckingham, UK). A nose clip was used, and a visual
computer program helped to optimize the forced exhalations. At least three acceptable forced
expiratory curves were recorded according to the reproducibility criteria of the American
Thoracic Society (ATS) (1995). The curve with the highest sum of forced expiratory volume
in one second (FEV1) and forced vital capacity (FVC) was selected for the analysis. FVC,
FEV1 and forced expiratory flow at 50% of FVC (FEF50) were recorded, and the results were
expressed as percentages of predicted value (Polgar & Promadhat 1971). Spirometric
parameters were measured before and 15 min after the inhalation of 0.3 mg of salbutamol
(Ventoline®, Glaxo, Greenford, UK) via a large-volume plastic spacer (Volumatic®). The
bronchodilator response was expressed as the percentage change in FEV1 from baseline
(∆FEV1). Abnormal basic spirometric finding was defined as FVC<80%, FEV1<80% or
FEF50<62% of predicted values, and ∆FEV1>15% was considered as an increased
bronchodilator response.
Impulse oscillometry (I, III and IV)
Impulse oscillometry (Jaeger GmbH, Würzburg, Germany) (Vogel & Smidt 1994) was
performed, when the child was sitting and breathing quietly through a mouthpiece. A nose
clip was used, and the cheeks were supported by the investigator, to minimize pressure loss
55
through the upper airway shunt. The impulse interval was set to 0.3 seconds, and by using
Fast Fourier transformation, the resistance (Rrs) and reactance (Xrs) of the total respiratory
system were calculated as functions of an oscillation frequency of 5�35 Hz. The
measurements were repeated at least three times, and three acceptable, visually uniform
recordings were used to calculate a mean value for Rrs at 5, 10 and 20 Hz (Rrs5, Rrs10,
Rrs20) and for Xrs at 5 and 10 Hz (Xrs5, Xrs10) and the resonance frequency (fres; the
frequency where reactance has the value of zero). The results were expressed as SDs of
reference values (Duiverman et al 1985). IOS measurements were repeated 15 min after the
inhalation of 0.3 mg of salbutamol. The bronchodilator response was expressed as the
percentage change in Rrs5 from baseline (∆Rrs5). Abnormal IOS findings were defined as
Rrs5>1.65 SD or Xrs5<-1.65 SD, and ∆Rrs5>30% was considered as an increased
bronchodilator response.
Pulmonary diffusing capacity test (I to IV)
Pulmonary diffusing capacity and static lung volumes were measured using the single-breath
method (Cotes et al 1993) (PFT, Jaeger GmbH, Würzburg, Germany). A volume of 90% of
inspired vital capacity was used for breath holding; the washout volume was preset at 500 ml
and the sample for expiratory gas fraction was 750 ml. Mean values of three acceptable
measurements were used for the analysis of pulmonary diffusing capacity (DLCO) and the
diffusing coefficient (KCO) for carbon monoxide. The results were expressed as percentages of
the predicted values of Polgar & Promadhat (1971) for static lung volumes (I) and for
diffusing capacity (II), and as percentages of the predicted values of Cotes et al (1979) for
diffusing capacity (I, III and IV).
Whole-body plethysmography (I)
Whole-body plethysmography (Body-Screen II, Jaeger) was performed for those who showed
sufficient cooperation in previous lung function studies. The mean values of three acceptable
measurements of total lung capacity (TLC), residual volume (RV), airway resistance (Raw)
and specific conductance (SGaw) were recorded, and the RV/TLC ratio was recorded to assess
hyperinflation. The reference values of Polgar & Promadhat (1971) were used for the
analysis.
56
5. Exhaled nitric oxide (II)
Exhaled nitric oxide was measured using a chemiluminescence analyzer (Sievers 270B,
Boulder, CO) (Kharitonov et al 1997) with a rapid-response time (<200 ms) and an accuracy
of +1 ppb (parts per billion). In addition, the analyzer also measured expiratory flow and
exhaled volume in real time. The sampling rate through the reaction chamber of the analyzer
was 250 mL/min for all measurements. The analyzer was calibrated daily, using NO-free
oxygen to set the absolute zero and certified NO gas of 184 ppb NO in nitrogen (AGA
Edelgas, Germany).
For eNO measurements, after inhaling NO-free oxygen, the children exhaled slowly from
TLC for 15 seconds through a flow resistor (Hans Rudolp, Model 7100R, 50cmH20/L/s, flow
range 0-0.5 L/s), which created a positive pressure necessary to close the soft palate. Due to
the small lung volumes of the children, the target flows recommended by the European
Respiratory Society (ERS) (Kharitonov et al 1997) (0.16-0.25 L/s) appeared to be unsuitable,
as they presumed a volume of at least 2.4-3.7 L for 15-second exhalation. Therefore, lower
target flows were used in this study (0.10-0.20 L/s). A visual computer program was used to
help to maintain the flow as fairly constant. A nose clip was used, and the cheeks and lips
were supported to prevent any air leak. During a steady exhalation, eNO reaches a plateau
after 5-10 seconds, while the exhaled volume continues to increase. The mean value of the
last three seconds of the end-expiratory plateau of NO concentration was taken for analysis.
The results of the analyses were computed and graphically displayed on a plot showing eNO
levels, flow and volume against time and expressed as eNO concentration (ppb) and NO
output (pmol/s). At least three successive recordings were made, with a coefficient of
variation of <10%. The mean value of the measurements was recorded on the case record
form.
6. Cardiological measurements (III and IV)
ECG criteria for right ventricular hypertrophy were defined as R wave >20 mm or >S wave at
lead V1. Incomplete right bundle branch block (RBBB) was registered. Cardiac volume was
derived from the size of the heart on plain chest x-ray. The anatomy and function of the heart
and the large vessels were studied using two-dimensionally guided, pulsed, continuous-wave
and colour Doppler equipment (Acuson 128 XP machine, Mountain View, CA, USA) with
2.5, 3.5 and 5.0 MHz probes and recorded on videotape. Pulmonary arterial pressure was non-

57
invasively assessed by measuring tricuspid valve regurgitation flow (Farstad et al 1995,
Subhedar et al 2000). In the main pulmonary artery, peak systolic velocities (cm/s) and
acceleration time (ms) were registered.
7. Statistics
The results of lung function tests were expressed as percentages or SDs of predicted values. In
Study I, ANOVA with Bonferroni/Dunn´s application for multiple comparisons was used to
compare the lung function test results of the thre groups. Pearson´s correlation coefficient was
calculated for the relationship between the different lung function tests. Kappa (κ) statistics
were used to describe the agreement between spirometry and the IOS method, and
McNemar´s test to compare the agreement of oscillometric variables with spirometry. A p-
value <0.05/3=0.017 was considered significant in group comparisons, otherwise p<0.05. In
the Studies II to IV and in supplemental analyses of the whole population, the Kruskall-Wallis
non-parametric test was used to determine the significances of the differences between the
three groups. The Mann-Whitney test and the χ2 test with continuity correction were used for
the comparisons between two groups. P<0.05 was considered significant. Spearman´s rank
correlation was used to evaluate the association between individual values of neonatal data,
lung function and cardiological measurements.

59
RESULTS
1. Population characteristics
Children born very prematurely (All, I to IV)
The basic perinatal and neonatal data of the study children and the different subgroups are
presented in Table 2. The children were born at 24.1 to 30.9 gestational weeks with birth
weights of 600-1575 g (I to IV). 45% of them were male and 12% SGA. 55% had received
antenatal DEX. All except one child required mechanical ventilation after birth, which was
provided by a pressure-limited Baby Bird ventilator (Bird Corporation, Palm Springs, CA,
USA). 84% had RDS, and 43% received surfactant for treatment. 6% had air leak syndrome.
73% required indomethacin and 6% surgical ligation for PDA. At the age of 28 days, 29%
were on ventilator support and 63% on supplemental oxygen. 33% were on supplemental
oxygen at 36 gestational weeks and 22% at 40 gestational weeks. 33% received postnatal
DEX before two months of age for weaning from the ventilator. 22% had IVH grade 1-4, 8%
IVH grade 3-4 and 28% abnormal brain ultrasound findings. 6% had NEC, 12% had ROP,
and 8% needed cryocoagulation (not shown in the original studies).
Children with BPD (All, I and II)
Apart from the more long-term need for supplemental oxygen, the BPD children had
significantly lower gestational age (I) and birth weight and a longer need for ventilator
treatment and initial hospital care than those with no BPD (I and II). Subsequent hospital data
on oxygen need caused one child to be re-classified into the BPD group after the completion
of Study I, and therefore, in the subsequent studies, 16 children had BPD and 33 did not.
Atopic children (II)
The difference in gestational age was not significant, but the atopic children had higher birth
weight and a shorter need for initial respiratory support and hospital care (p<0.01) than the
non-atopic children.
Children in the postnatal dexamethasone study (III)
The DEX and placebo groups did not differ in basic neonatal data. One child in each group
had received antenatal DEX, and 3 out of 16 received surfactant therapy for RDS. Half of the
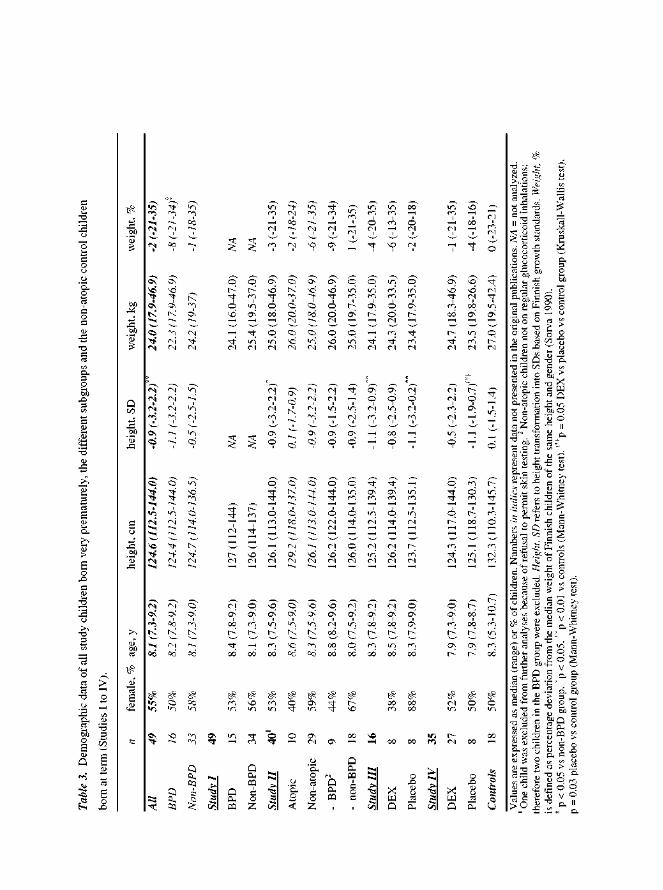

61
children in the placebo group and 25% in the DEX group received open-label DEX treatment
after the trial. Half of the children in each group had BPD.
Children in the antenatal dexamethasone study (IV)
Abnormal brain ultrasound findings were more common in the placebo group than in the
DEX group (p=0.02), which was the only significant difference in the neonatal data. 33% of
the infants in the DEX group and all in the placebo group received indomethacin for PDA
(p=0.06); nor was the difference in surfactant therapy (DEX 52%, placebo 88%) or ROP
(DEX 7%, placebo 25%) significant. All of the 6 SGA infants were in the DEX group. 11% in
the DEX group and 38% in the placebo group received postnatal DEX treatment. One fourth
in each group had BPD.
2. Growth
Children born very prematurely (All, I to IV)
The demographic data of all study children and the non-atopic control children born at term
are presented in Table 3. The study children did not differ significantly from the controls in
age, height, weight (I and II) or relative weight. However, standardized height was lower in
the prematurely born children than in the controls (p=0.03 in II; p=0.008 in All); this
difference was significant in boys (p=0.007 in All, not shown in the studies), but not in girls.
Children with BPD (All, I)
Despite their lower gestational age and birth weight, the BPD children did not differ
significantly at school age in height, weight (I) or standardized height, but they weighed less
after adjustment for height and gender than the non-BPD children (p=0.03, not shown in the
studies).
Children after postnatal dexamethasone treatment (III)
The children treated with DEX did not differ significantly from the placebo-treated children
or the controls in height, standardized height, weight or relative weight. Standardized height
was lower in the placebo group than in the controls (p=0.006). No significant correlation was
found between the duration of DEX therapy before one year of age and the variables of
growth (not in Tables).
62
Children after antenatal dexamethasone treatment (IV)
Height, standardized height, weight and relative weight did not differ significantly between
the children given antenatal DEX or placebo and the controls. Standardized height showed a
tendency towards a difference (p=0.05) between the three groups; further comparisons proved
it to be lower in the placebo group than in the control group (p=0.03). Adjusted for gender,
this difference was significant in boys (p=0.01) (not shown in the studies).
3. Respiratory symptoms and medication
Children born very prematurely (All, I, III and IV)
Table 4 shows the respiratory symptoms and medication of the study children in the different
subgroups. 33% received glucocorticoid inhalations at 12 months and 37% at 24 months of
age. One child was on oral systemic glucocorticoid until the age of 7.5 years. Adenoidectomy
was performed on 57% of the children, and 39% needed tympanostomy tubes. Regarding the
symptoms during the preceding year, 22% were reported to have asthma, 29% dyspnoea, 35%
prolonged cough for >2 months, 12% cough during the pollen season, 14% on exercise and
18% at night. A total of 49% reported either dyspnoea or prolonged cough. Glucocorticoid
inhalations were used regularly by 5 (10%) and occasionally by 8 (16%) children. Combined
with glucocorticoids, 4% used bronchodilators and 4% chromone inhalations regularly. 41%
used β2-sympathomimetic agents. None had required hospitalization because of respiratory
symptoms during the preceding year. Previous diagnosis of asthma, i.e. a history of asthma
symptoms and regular therapy, correlated significantly with the use of glucocorticoids and
bronchodilators and cough during the pollen season, but not with cough on exercise or at
night, nor was the correlation with frequent symptoms during the preceding year significant.
Dyspnoea or prolonged cough associated with lower age (p=0.02) and shortness for age
(p=0.02) at the time of the study, but not with gestational age or birth weight. The use of
glucocorticoid inhalations associated with lower age (p=0.007), low birth weight (p=0.02) and
need for ventilator treatment (p=0.007), oxygen supplementation (p=0.02) and initial hospital
care (p=0.02) (not shown in the studies). Worse exercise tolerance compared to others and at
school, subjectively assessed by parents, was reported for 14 children: a correlation was found
with shortness for age (p=0.046), low birth weight (p=0.03), ventilator treatment (p=0.03),
oxygen supplementation (p=0.009) and initial hospital care (p=0.01). Only 3 of these 14
children were free from severe or moderate disability (p=0.001) (not shown in the studies).
Two children received medication for epilepsy (I).
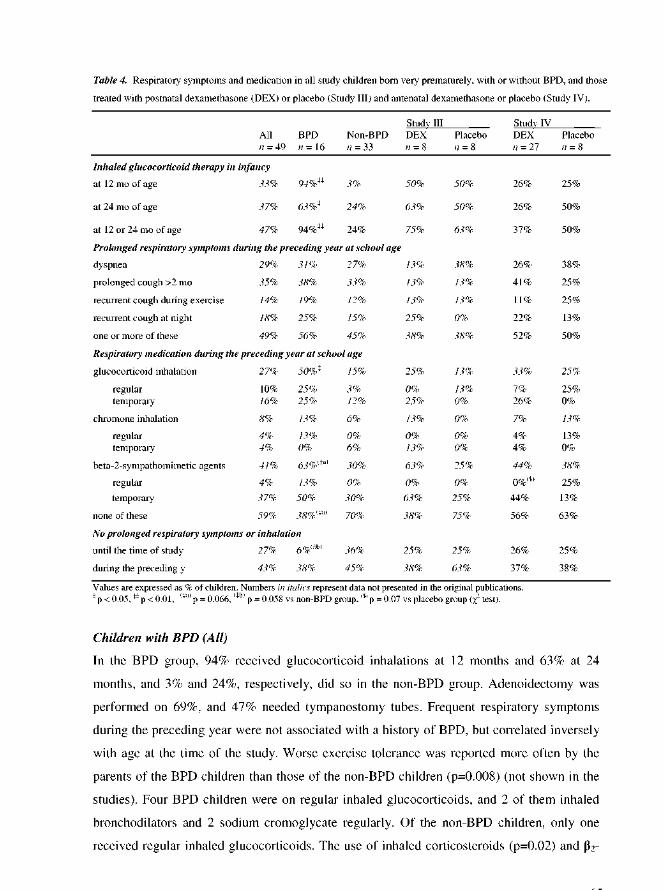
64
sympathomimetic agents tended to be (p=0.07) more common in the children with BPD
during the preceding year. 38% of the BPD and 45% of the non-BPD children had had neither
prolonged respiratory symptoms nor inhalation therapy during the preceding year (not shown
in the studies).
Children after postnatal dexamethasone treatment (III)
In the DEX group, 50% received glucocorticoid inhalations at 12 months and 63% at 24
months, and in the placebo group, 50% and 50% did so, respectively; in addition, one child in
the latter group received oral systemic glucocorticoid by the age of 7.5 years. Frequent
respiratory symptoms during the preceding year were reported by 38% in each group. In the
DEX group, none received regular glucocorticoids, although occasional use of inhalations
was common. In the placebo group, one child out of 8 was on regular glucocorticoid
inhalation, and 2 used β2-sympathomimetic agents occasionally. One fourth in each group had
had neither prolonged respiratory symptoms nor a need for inhalations during childhood. No
significant differences were seen in respiratory symptoms or medication associated with
postnatal DEX treatment.
Children after antenatal dexamethasone treatment (IV)
In the DEX group, 26% received glucocorticoid inhalations at 12 months and 26% at 24
months, compared with 25% and 50% in the placebo group. Half of the children in each group
reported frequent respiratory symptoms during the preceding year. In each group, 2 children
were on regular glucocorticoid inhalation (DEX 7%, placebo 25%), and β2-sympathomimetic
agents were used commonly (DEX 44%, placebo 38%). The 2 children on regular inhaled
bronchodilators were in the placebo group (p=0.07). One fourth in each group were free from
frequent respiratory symptoms and inhalations until school age. Antenatal DEX treatment did
not associate with respiratory symptoms or medication.
4. Smoking in the family (I to IV)
Exposure to tobacco smoke was common in this series of children born very prematurely,
defined as smoking during pregnancy (33% from hospital records, 25% reported), maternal
smoking (39%), smoking within the family (45%) or smoking at home (6%) (not shown in the
studies), with no difference between the subgroups in individual studies (III and IV) (I and II,
not shown in the studies).
65
Influence on growth
No significant correlation emerged between maternal smoking or smoking during pregnancy
and growth (III) (in All, not shown in the studies).
Influence on respiratory symptoms
No associations were found between maternal smoking or smoking during pregnancy and
dyspnea or prolonged cough (III and IV). Of the 15 study children with no prolonged
respiratory morbidity and no need for inhalation during childhood, 60% had smoking
mothers, and 47% had mothers who had smoked during pregnancy (not shown in the studies).
Influence on lung function
Maternal smoking or smoking during pregnancy was not associated with basic lung function
as assessed by spirometry or oscillometry. However, maternal smoking or smoking in the
family associated with poorer diffusion capacity at school age (see results in page 73).
5. Atopy
Children born very prematurely (All, II)
30% of the families reported having medically diagnosed atopy and 32% probably atopic
symptoms; 39% had animals. 12 out of 48 (25%) study children were skin prick-positive (not
shown in the studies); one child refused to be tested. The atopic children did not differ
significantly from the non-atopic children in gestational age (p=0.06), but they had higher
birth weight (p=0.001) and a shorter duration of ventilator treatment (p=0.001), oxygen
therapy (p=0.007) and initial hospital care (p=0.001) (II; p<0.01 in All, not shown in the
studies). None of the skin prick-positive children had received postnatal DEX, differing
significantly from the skin prick-negative ones (p=0.01). Prick positivity correlated neither
with respiratory symptoms nor with medication (not shown in the studies).
Children with BPD (All, II)
In Study II, only one out of 12 (8%) BPD children had positive skin prick tests compared with
9 out of 27 (33%) non-BPD children. In the whole group of study children, this finding of less
atopy in the BPD group (1 out of 16) compared with the non-BPD group (11 out of 32) was
statistically significant (p=0.04) (not shown in the studies).
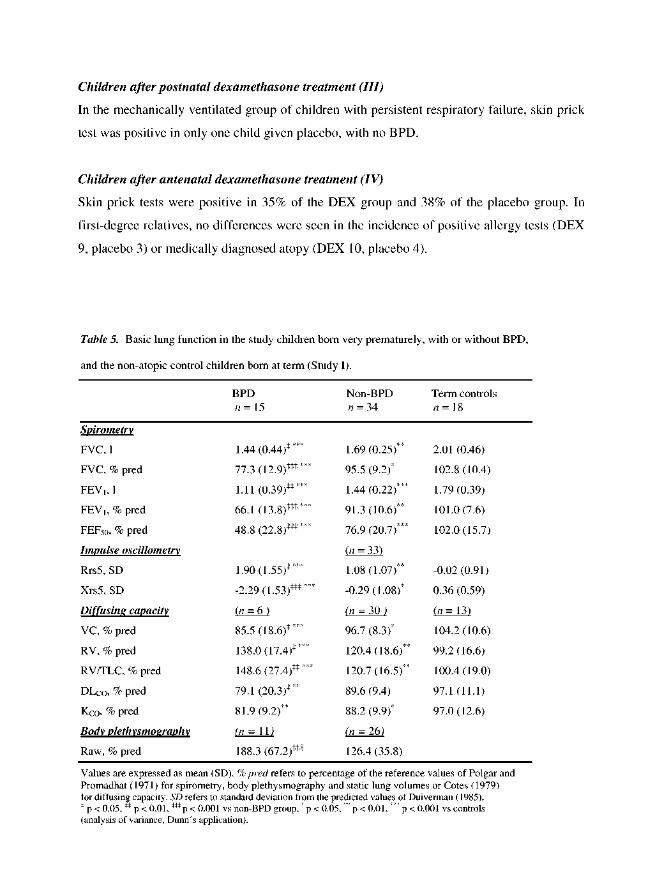
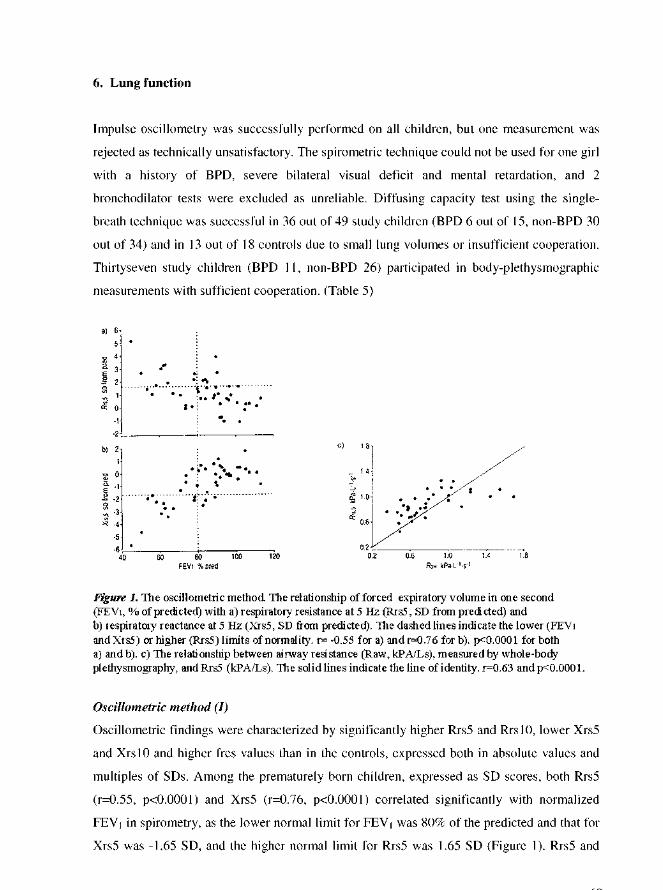
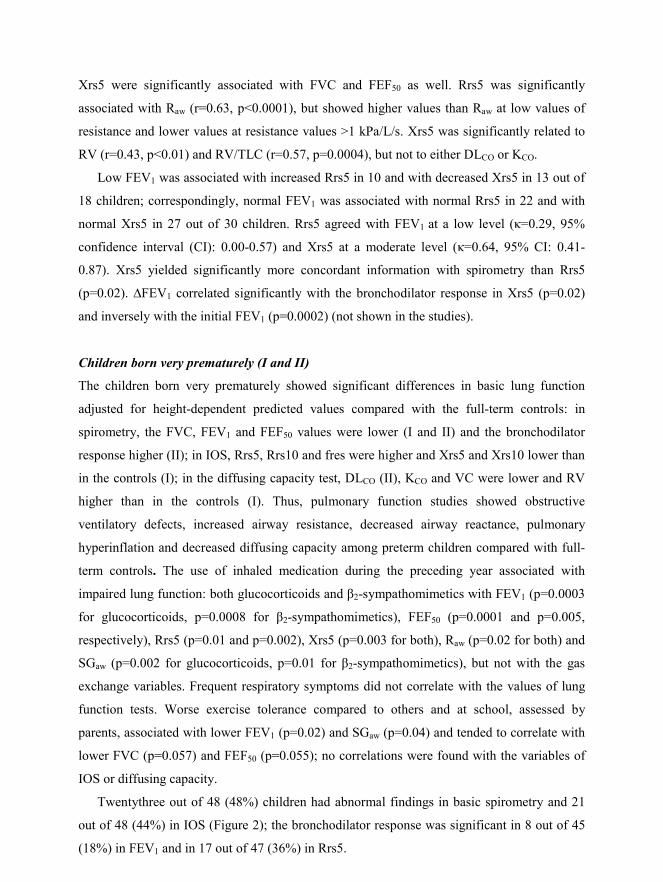
68
Xrs5 were significantly associated with FVC and FEF50 as well. Rrs5 was significantly
associated with Raw (r=0.63, p<0.0001), but showed higher values than Raw at low values of
resistance and lower values at resistance values >1 kPa/L/s. Xrs5 was significantly related to
RV (r=0.43, p<0.01) and RV/TLC (r=0.57, p=0.0004), but not to either DLCO or KCO.
Low FEV1 was associated with increased Rrs5 in 10 and with decreased Xrs5 in 13 out of
18 children; correspondingly, normal FEV1 was associated with normal Rrs5 in 22 and with
normal Xrs5 in 27 out of 30 children. Rrs5 agreed with FEV1 at a low level (κ=0.29, 95%
confidence interval (CI): 0.00-0.57) and Xrs5 at a moderate level (κ=0.64, 95% CI: 0.41-
0.87). Xrs5 yielded significantly more concordant information with spirometry than Rrs5
(p=0.02). ∆FEV1 correlated significantly with the bronchodilator response in Xrs5 (p=0.02)
and inversely with the initial FEV1 (p=0.0002) (not shown in the studies).
Children born very prematurely (I and II)
The children born very prematurely showed significant differences in basic lung function
adjusted for height-dependent predicted values compared with the full-term controls: in
spirometry, the FVC, FEV1 and FEF50 values were lower (I and II) and the bronchodilator
response higher (II); in IOS, Rrs5, Rrs10 and fres were higher and Xrs5 and Xrs10 lower than
in the controls (I); in the diffusing capacity test, DLCO (II), KCO and VC were lower and RV
higher than in the controls (I). Thus, pulmonary function studies showed obstructive
ventilatory defects, increased airway resistance, decreased airway reactance, pulmonary
hyperinflation and decreased diffusing capacity among preterm children compared with full-
term controls. The use of inhaled medication during the preceding year associated with
impaired lung function: both glucocorticoids and β2-sympathomimetics with FEV1 (p=0.0003
for glucocorticoids, p=0.0008 for β2-sympathomimetics), FEF50 (p=0.0001 and p=0.005,
respectively), Rrs5 (p=0.01 and p=0.002), Xrs5 (p=0.003 for both), Raw (p=0.02 for both) and
SGaw (p=0.002 for glucocorticoids, p=0.01 for β2-sympathomimetics), but not with the gas
exchange variables. Frequent respiratory symptoms did not correlate with the values of lung
function tests. Worse exercise tolerance compared to others and at school, assessed by
parents, associated with lower FEV1 (p=0.02) and SGaw (p=0.04) and tended to correlate with
lower FVC (p=0.057) and FEF50 (p=0.055); no correlations were found with the variables of
IOS or diffusing capacity.
Twentythree out of 48 (48%) children had abnormal findings in basic spirometry and 21
out of 48 (44%) in IOS (Figure 2); the bronchodilator response was significant in 8 out of 45
(18%) in FEV1 and in 17 out of 47 (36%) in Rrs5.
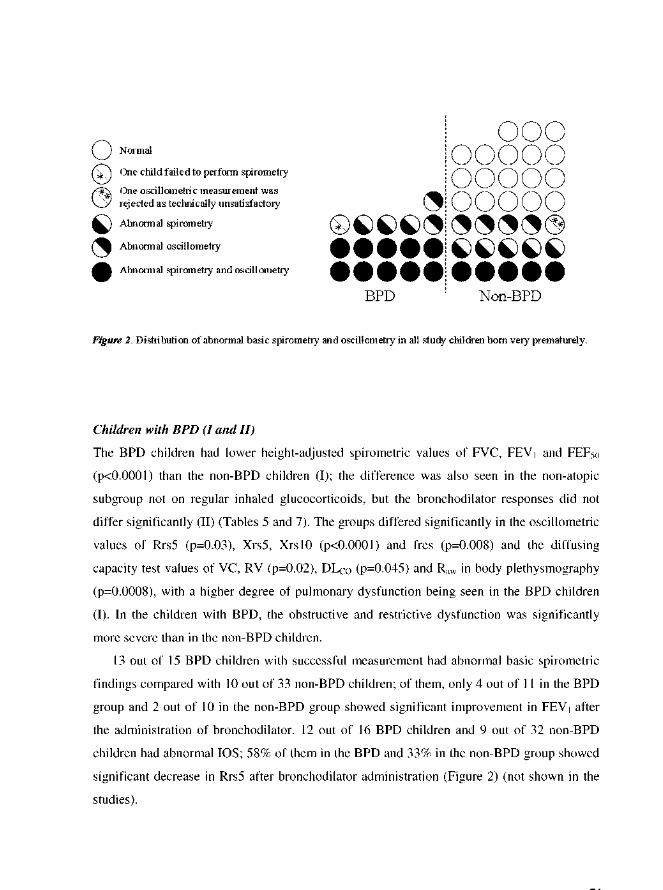
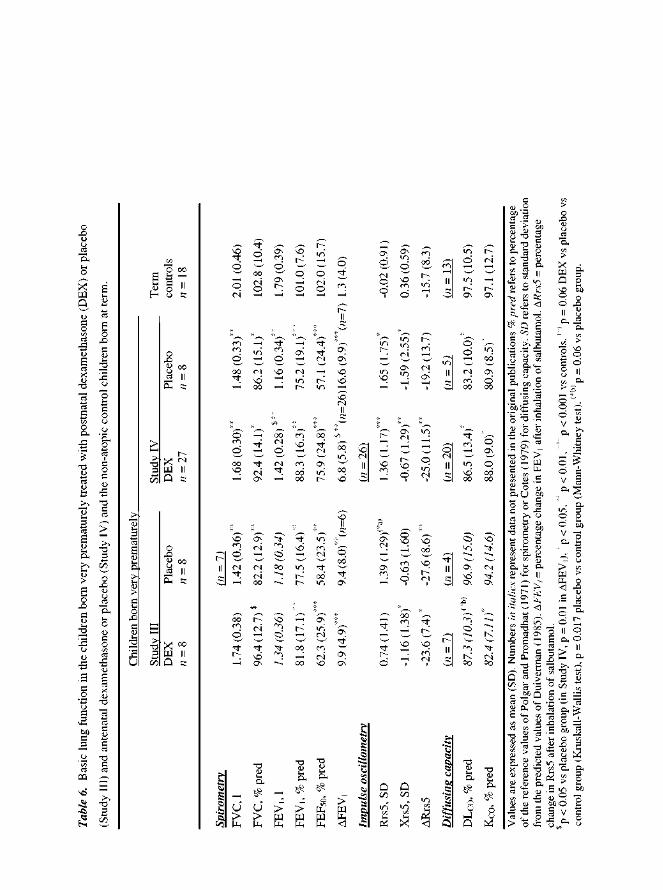
71
Children after postnatal dexamethasone treatment (III)
Spirometry and IOS showed significant impairment in pulmonary function in both study
groups compared with the controls´ values (Table 6). FVC was higher in the DEX group
(p=0.04), this being the only significant difference between the DEX and placebo groups. In
IOS, Rrs5 was higher in the placebo group and Xrs5 was lower in the DEX group as signs of
airway obstruction, and the bronchodilator response was increased in both groups compared
with the full-term controls. DEX treatment was not shown to have any negative effect on
pulmonary outcome.
Children after antenatal dexamethasone treatment (IV)
The study children had significantly impaired basic spirometric values and increased ∆FEV1,
suggesting bronchial lability (Table 6). The more pronounced bronchodilator response in the
placebo group was the only significant difference between the study groups in height-adjusted
spirometric values (p=0.01). IOS revealed no significant differences between the DEX and
placebo groups. Compared with the control group, Rrs5 was significantly higher and Xrs5
lower in both study groups. Diffusing capacity test failed in 7 DEX and 3 placebo children
and in 5 controls, thus rendering the comparisons between the preterm groups invalid.
However, the mean DLCO and KCO values were significantly lower in all study children than
in the controls. Antenatal DEX treatment was not shown to have any negative effect on
pulmonary outcome.
Effect of smoking
Basic spirometric, oscillometric and body-plethysmographic values did not correlate with
maternal smoking or smoking during pregnancy (III and IV). Nor did the values of the
diffusing capacity test correlate with smoking during pregnancy. However, in Study IV, the
prematurely born children with smoking mothers had significantly lower DLCO values
(p=0.009) and a slight tendency towards lower KCO values (p=0.08) compared with the
children of non-smoking mothers. Smoking in the family also tended to correlate with lower
DLCO (p=0.08) and KCO (p=0.08) (IV); the difference in KCO was significant in all study
children (p=0.02, not shown in the studies).
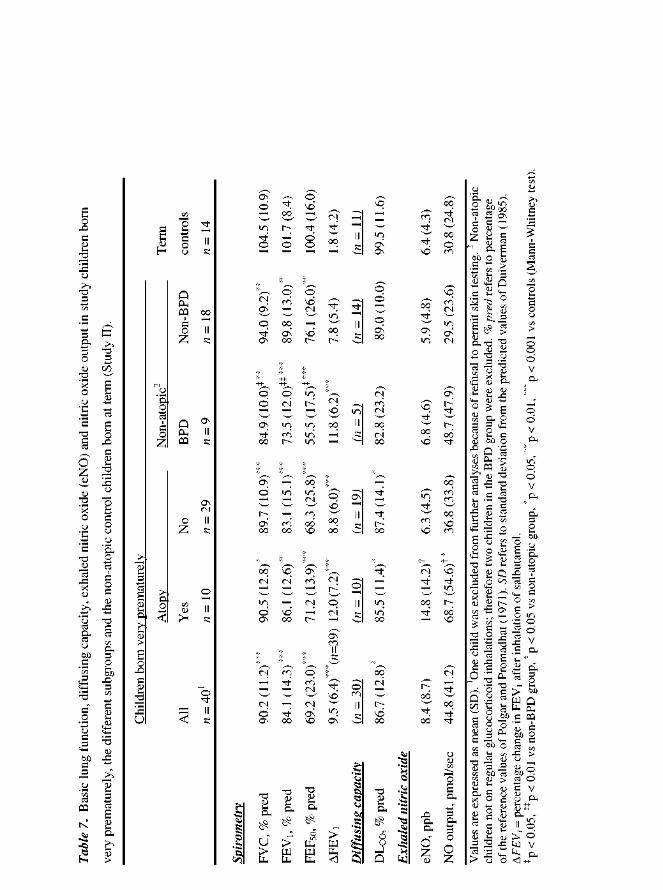
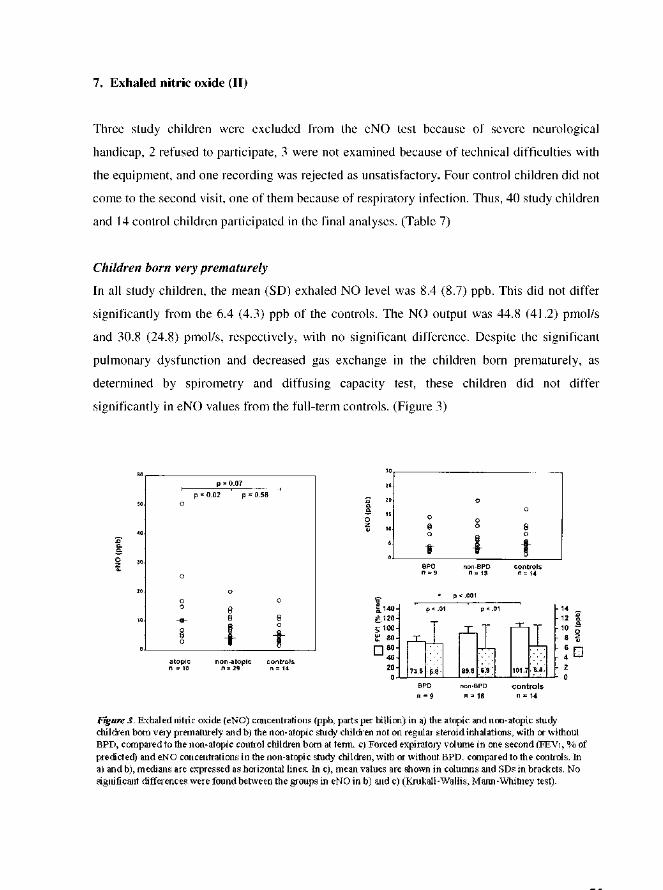
74
Influence of atopy, familial smoking or glucocorticoid inhalation
In the prematurely born group, the atopic children had higher mean (SD) eNO values than the
non-atopic ones [14.8 (14.2) vs 6.3 (4.5) ppb, p=0.02] and higher mean (SD) NO outputs of
68.7 (54.6) and 36.8 (33.8) pmol/s, respectively (p=0.04) (Figure 3). The eNO concentrations
and NO output values of the non-atopic study children did not differ significantly from those
of the controls. Gender and exposure to smoking in the family were not significant predictors
of eNO concentrations or output in the study children, nor was the use of inhaled
glucocorticoids during the first two years of life or during the preceding year.
Non-atopic children with BPD
Due to the significant association of atopy with increased eNO in our study and of
glucocorticoids with decreased eNO in previous studies, we excluded the 10 atopic children
and the 3 children on regular glucocorticoid inhalation therapy from the further analyses. Of
the remaining 27 non-atopic study children, 9 had a history of BPD and 18 had no BPD.
These two groups did not differ in gestational age or demographic data at the time of the
study, but the BPD children had lower birth weights and needed more oxygen
supplementation, as by definition, and ventilator treatment (Tables 2 and 3). Despite
significant differences in spirometry, the eNO concentrations did not differ between the BPD,
non-BPD and control children [6.8 (4.6), 5.9 (4.8) and 6.4 (4.3) ppb, respectively], nor did the
eNO output values [48.7 (47.9), 29.5 (23.6) and 30.8 (24.8) pmol/s] (Figure 3). In the non-
atopic children born very prematurely with a history of BPD, we found no evidence of airway
inflammation associated with increased eNO concentration. No association was found
between eNO levels and the severity of chronic lung disease, determined by conventional
lung function tests, either.
8. Cardiac function
Children after postnatal dexamethasone treatment (III)
No significant difference between the study groups was seen in cardiac volumes, Doppler-
mode-derived variables of pulmonary flow (peak velocity or acceleration time) or left
ventricular function (Table 8). Tricuspid valve regurgitation of >30 mmHg was detected in 3
children in the DEX group and one child in the placebo group. The placebo group child had
elevated pulmonary arterial pressure of 42 mmHg in cardiac catheterization at three years of
age and was treated with digoxin and nifedipine. In the follow-up at eight years of age,

76
cardiomyopathy was seen. One girl in the DEX group had a tiny PDA 1.5 mm in diameter. No
murmur was heard, and no closure was needed. None required cardiovascular medication.
51% of the children born prematurely presented with RBBB in ECG. These children had
more severely impaired values of FEV1 (p=0.03), Rrs5 (p=0.02) and Xrs5 (p=0.02) than those
without RBBB. However, RBBB did not associate with BPD or PDA.
9. Neurological follow-up
Children after postnatal dexamethasone treatment (III)
At the age of five years, 50% of the children in each study group needed physiotherapy,
occupational therapy or evaluation for the most appropriate type of school because of
neurological impairment or difficulties in speech, learning or comprehension. All were able to
walk without aid or support. All of the children in the DEX group attended normal school,
and 3 of them had CP: one girl with mild, spastic diplegia and mild cognitive difficulties
needed a personally adjusted course in mathematics as well as physiotherapy; one girl with a
shunted hydrocephalus, epilepsy, mild, spastic diplegia and strabismus needed a personal
assistant at school (IVH grade 3-4); one boy with mild, spastic hemiplegia needed
physiotherapy, and one boy with no previous problems needed speech therapy because of
reading difficulties (Table 9). In the placebo group, 7 (88%) children attended normal school,
and 2 of them had CP: one girl who had received oxygen therapy for 4.5 years had a personal
assistant because of moderate spastic diplegia, and she also needed physiotherapy, and one
boy with mild, hypotonic diplegia had a personal assistant and had problems in mathematics
(IVH grade 2-3), but spoke three languages. One girl attended a preparatory class before
entering normal school. Another mentally retarded girl attended a special school for blind
children because of a severe bilateral visual deficit caused by ROP.
Thus, 38% of the children in the DEX group and 25% in the placebo group had CP. In the
DEX group, 38% were moderately disabled, while in the placebo group, 25% were severely
and 25% moderately disabled. The neurodevelopmental outcome at school age did not differ
significantly between the DEX and placebo groups.
The data from the hospital records of the 4 children lost to this follow-up did not add to
any differences between the groups, as no CP was found, all could walk without support and
attended or planned to attend normal school, and one child in each group was moderately
disabled.


78
Thus, 11% of the children in the DEX group and 50% in the placebo group had CP. 22%
of the children in the DEX group and 75% in the placebo group were either severely or
moderately disabled. In the DEX group, the rate of normal school attendance was higher
(p=0.01), and there were fewer instances of severe to moderate disability (p=0.02) and a
tendency towards a lower incidence of CP (p=0.06) than in the placebo group.
The limited data on the neurological outcome of 8 out of the 9 children lost to this follow-
up study (Table 1 in IV) confirmed these results. Furthermore, out of the 59 infants in the
original antenatal DEX study, 26 of the 37 (70%) children in the DEX group survived without
CP compared with 6 of the 21 (29%) in the placebo group (p=0.003).
79
DISCUSSION
1. Methodological aspects
Our study population consisted of VLBW children born very preterm, who participated in one
of the following two randomized placebo-controlled perinatal trials: study of neonatal DEX
given to severely ill ventilator-dependent infants at a high risk of BPD (Trial 1) (Kari et al
1993) or very preterm infants born to mothers who participated in the study of antenatal DEX
in imminent preterm birth (Trial 2) (Kari et al 1994). All infants were treated in the same
hospital during a 3-year period, with no major changes in ventilator treatment. Thus, the
infants in Trial 1 were a relatively homogenous group, with minimal variations in neonatal
treatment. The infants in Trial 2 were born after the anticipation of preterm birth, with the best
possible perinatal care available. The latter setting may underestimate the morbidities and the
long-term sequelae of very preterm birth.
Altogether 49 (79%) of the 62 recruited children participated in this follow-up. About one
third of the non-participants refused, one third were excluded because of severe neurological
problems, and the rest were not traced. The perinatal data of the non-participants did not differ
significantly from those of the study children. The neurological outcome data were extracted
from hospital records in the case of 61 (98%) children. Inclusion of the non-participants in the
neurologic assessment did not change the results (III and IV). Therefore, our study children
can be considered good representatives of the original trials.
Despite occasional severe neurological impairments, all could perform the IOS procedure
and all but one the spirometric measurements. The children with most severe lung disease or
small lung volumes could not perform the diffusing capacity test or the body
plethysmography. This may underestimate the impairment of lung function or conceal the
differences between the subgroups. However, occasional children with severe neurological
handicap, with or without lung disease, also either failed in performance or were
prospectively excluded. Even though the study population was small, the lung function tests
were carefully standardized with low variability (<5% in FVC and FEV1 and <10% in eNO).
All cardiac measurements were performed by the same pediatric cardiologist.
Only non-atopic full-term children were selected as a control group in the lung function
studies. The larger age range in the control group compared to the study groups made the
range of body heights, to which the lung function results were adjusted, very similar in all groups.
80
Compared to IOS, spirometry showed significant concordance, as did also body
plethysmography. Still, the different methods could not be compared in the children with the
most severe lung disease or the smallest lung volumes. One BPD child was misclassified into
the non-BPD group in Study I, but this had no significant effect on the results. (I)
The impairment of lung function was compared with one marker of inflammation, eNO.
To avoid the bronchodilator effect, eNO measurements were performed at another visit than
spirometry, which could influence the associations. (II)
The sample size in Study III was too small to warrant definite conclusions. The power of
this study alone is low, but it will be of value in future meta-analyses. The homogeneity of the
group (Trial 1), the successful lung function tests and the abundant neurological data are a
strength, but the frequent use of DEX after the study could be considered a weakness of the
study.
In Study IV, the size of the placebo group was small, due to the small number of infants
born very preterm and the high mortality (Trial 2). This emphasizes the better outcome in the
original DEX group, if perinatal death is included. This group was heterogenous in perinatal
respiratory morbidity; differences in treatment may individually affect the long-term outcome,
causing bias, or represent the effects of antenatal DEX. This follow-up is important in meta-
analyses of the long-term outcome, especially as new placebo-controlled randomized studies
will hardly follow, because of the well-established short-term benefits of antenatal DEX.
Definition of bronchopulmonary dysplasia
We used a simple criterion for BPD, i.e. supplemental oxygen at 36 gestational weeks.
Despite the variations in treatment strategies, discontinuation of oxygen is one clinical
descriptor of infant stability. In our study, the diagnosis of BPD is used more as a tool to
divide the preterm born children into those at a �high risk� and those at a �risk� of long-term
sequelae of prematurity than as a strictly defined disease. The infants in Trial 1 were born
before the introduction of antenatal glucocorticoid and surfactant therapy into common use,
and due to the entry criteria, represent VLBW children with severe lung disease and hence
with a high incidence of BPD (50%). The infants in Trial 2 were born at the beginning of the
era of antenatal glucocorticoid and surfactant therapy, and the incidence of BPD was 23%.
The differences in the definitions of BPD make comparisons of the incidences and long-term
sequelae in studies between different centres and periods extremely rough.
81
2. Oscillometric method
In our study, IOS yielded lung function information concordant with conventional methods,
such as spirometry and whole-body plethysmography, and served well in studying
prematurely born children. The findings probably reflect the peripheral or more widespread
airway obstruction and are most valuable in combination with other lung function tests.
Using the oscillometric method, the mechanical properties of the lung have been described
previously in children with asthma (Solymar et al 1984, König et al 1984, Lebecque et al
1987, Bisgaard & Klug 1995, Klug & Bisgaard 1996), cystic fibrosis (Lebecque & Stănescu
1997, Hellinckx et al 1998) and chronic respiratory symptoms (Timonen et al 1997). In
asthma, airway obstruction is associated with increased Rrs, the values measured at the lowest
oscillatory frequencies (2-5 Hz) showing the best sensitivity (Clément et al 1983, Solymar et
al 1984, Bisgaard & Klug 1995). This pattern of abnormality has been similar regardless of
whether the FOT (Clément et al 1983, Solymar et al 1984) or the IOS method has been
applied (Bisgaard & Klug 1995, Klug & Bisgaard 1996). Despite the concordant results in
asthma, the concordance between FEV1 and Raw in cystic fibrosis has been reported to be poor
(Lebecque & Stănescu 1997). This may be due to the effect of dynamic compression of the
airways during forced expiratory manoeuvres, which is lacking when Raw is measured at tidal
breathing. In the present study, a significant but low concordance between Rrs5 and FEV1
was found. However, the concordance was better in Xrs, which delineated the severely
affected children (BPD) more accurately than Rrs. (I) This is in agreement with the previous
findings on asthmatic children, where Xrs has been shown to correlate well with FEV1 and
Raw during challenge tests (Solymar et al 1984, Bisgaard & Klug 1995, Klug & Bisgaard
1996, Bouaziz et al 1996). Compared to an increase in Rrs, a decrease in Xrs has been
reported to be a more sensitive (Buhr et al 1990, Bisgaard & Klug 1995, Klug & Bisgaard
1996) and specific (Bouaziz et al 1996) indicator of thoracic obstruction.
Theoretically, Xrs is mainly determined by the elastic and mass-inertial properties of the
respiratory system; at low frequencies the former predominate and Xrs varies in relation to
dynamic compliance (Solymar et al 1989). The dynamic compliance of the lung is impaired
in both peripheral airway obstruction and disorders causing stiffness of the lungs, such as
interstitial fibrosis, both changes likely to be present in BPD. As in our study, no significant
relationship was found between Xrs and DLCO, the decreased Xrs values are more likely to be
due to airway obstruction than interstitial fibrosis. Rrs5 was closely associated in Raw in body
82
plethysmography. At the lower rate of resistance, IOS showed higher values than Raw, since
the method measures total respiratory resistance. At high values, Rrs5 underestimates
resistance (Cauberghs & Van de Woestijne 1989), as in our study.
The data on the range of normality in the bronchodilator response elicited with oscillatory
methods are still sparse (Delacourt et al 2000). In our study, the bronchodilator response in
Xrs5 correlated significantly with ∆FEV1, which was in line with the concordance found
between Xrs5 and FEV1.
To conclude, being easy to perform, IOS measurement alone may produce important
information on the lung function of preschool or school-aged children with neurological
handicap or other disabilities impairing cooperation. The bronchodilator test might be
valuable in examining children unable to produce forced expiration, and it should be further
evaluated. In combination with conventional lung function tests, IOS yields both concordant
and also additive information, as it assesses the quiet tidal breathing instead of forced
expiration. We chose to use the IOS method in our studies of long-term sequelae after the
administration of perinatal DEX (III and IV).
3. Exhaled nitric oxide
In eNO measurement, to avoid nasal NO contamination (Alving et al 1993), we used a
technique of single exhalation through a mouthpiece against a resistance, creating a back
pressure to close the soft palate (Kharitonov et al 1997). The present guidelines do not
recommend the use of a nose clip, but allow it in cases when the subject cannot avoid nasal
inspiration or nasal exhalation (ATS 1999). We used it systematically, as this technique of
breathing was familiar to the children from previous tests. Because neurological disabilities
and small lung volumes affect cooperation, the children were individually supported in the
performance. This technique was considered reliable in all study children, including the
youngest control child, who was 5.3 years old. The eNO concentration is highly flow-
dependent (Silkoff et al 1997). The expiratory target flows recommended at that time by the
ERS appeared unsuitable for us, as they require large lung volumes. Therefore, we used lower
target flows, which were still higher than those subsequently recommended by the ATS
(1999). Some variation of flows had to be accepted because of limited cooperation. Despite
this variation, we achieved recordings with acceptable individual variation in eNO, and the
flows in the different groups did not differ significantly. Even though relatively high flows

83
may mask some differences, they did not mask the differences between the atopic and non-
atopic groups.
In our prematurely born children, the atopic children presented with higher eNO values than
the non-atopic ones, in line with the previous findings (Frank et al 1998, Franklin et al 1999,
Mattes et al 1999, Piacentini et al 1999). Therefore, we excluded the atopic children and those
on regular glucocorticoid inhalations, known to suppress eNO, from the main study of eNO in
BPD. Living with a smoker (45%) had no detectable impact on eNO values either, in
agreement with previous findings (Franklin et al 1999). Despite the evident presence of
significant obstructive and restrictive lung function abnormalities in the study children,
especially those with BPD, we found no significant differences in eNO concentrations and
output between the non-atopic BPD, non-BPD and full-term control children. (II)
While prior studies on the inflammatory characteristics of BPD focused on the early neonatal
period (Merritt et al 1981, Speer 1999), postnatal follow-up data are scanty. Airway
inflammation has been assessed by eNO measurements in adult asthmatics (Alving et al 1993,
Kharitonov et al 1994, Persson et al 1994), in exacerbations of COPD (Maziak et al 1998)
and in asthmatic children (Lundberg et al 1996, Baraldi et al 1997, Nelson et al 1997),
particularly ones with atopy (Frank et al 1998). In asthmatic children, eNO concentration and
sputum eosinophil counts were found to be concordant, and eNO was proposed as an easy-to-
perform marker of eosinophilic airway inflammation (Mattes et al 1999, Piacentini et al
1999). In a recent study, eNO was superior to baseline lung function and bronchial
responsiveness in identifying preschool children with asthma (Malmberg et al 2003).
However, the role in non-atopic asthma was still unclear. In ventilated preterm infants, the
persistence of high bronchoalveolar lavage fluid nitrate associated with the development of
BPD (Vyas et al 1999), and high eNO levels shortly after birth were found in some infants
developing BPD (Aikio et al 2002). Exhaled NO concentrations decreased after DEX
treatment (Williams et al 2004). In face mask measurements at term, high eNO levels were
related to the presence of BPD (Leipälä et al 2004). No previous reports of eNO values in
children born very preterm with BPD exist.
As high eNO in atopic asthma is likely to represent airway inflammation, the lack of eNO
elevation in the school children with BPD in our study is evidence against airway
inflammation. However, high inducible NOS activity in the airway inflammatory cells or high
eNO is not a constant finding in neonatal inflammatory lung disease (Aikio et al 2000, Aikio

84
et al 2003). Non-atopic children born very prematurely showed no evidence of increased
concentrations of eNO. Nor did the eNO levels correlate with the severity of lung disease, as
determined by conventional lung function studies. As our study children with most severe
lung disease were all non-atopic, the eNO measurement did not serve in assessing the degree
of lung disease in a stable phase in these children.
To conclude, in non-atopic children born very prematurely, exhaled NO values did not
correlate with impaired lung function, indicating that eNO was not an inflammatory marker in
established BPD. However, because asthma is a common disease, eNO measurements may be
beneficial in the differential diagnosis of symptomatic children with chronic lung disease of
prematurity and atopic asthma.
4. Growth
In our study, the prematurely born children had significantly lower standardized height than
the controls, but the difference was seen only in boys. This confirms the findings of Hack et
al (2003), who showed that boys were shorter and lighter at the age of eight years, followed
by poorer catch-up growth until 20 years, and that this trend was especially obvious in those
who were SGA. Weight adjusted for height in our study did not differ between the groups.
Our BPD children weighed less adjusted for height than the non-BPD children, but in contrast
to earlier findings (Northway et al 1990b, Hakulinen et al 1996, Pelkonen et al 1997), they
were not shorter for age.
In previous studies, BPD children born during 1970-1980´s commonly showed growth
retardation in infancy (Northway 1979, Markestad & Fitzhardinge 1981), at school age
(Hakulinen et al 1996, Pelkonen et al 1997) or in adolescence (Northway et al 1990b), while
some others found no impairment (Bader et al 1987). Growth impairment was also seen in
VLBW children at preschool or school age or in adolescence, with or without catch-up
growth (Niklasson et al 2003, Hack et al 2003, Korhonen et al 2004c), and in ELBW children
(Doyle 2000a), but this findind has not been confirmed by others (Kilbride et al 2003).
Postnatal DEX may impair growth during treatment, but this effect is usually reversible
(Jones et al 1995, O´Shea et al 1999). Our study did not reveal any significant differences in
growth between the postnatal DEX and placebo groups, but the latter were shorter for age
than the controls. Among boys, the difference persisted. The cumulative dose of postnatal

85
DEX during the first year of life did not correlate with the growth parameters, either (III and
IV). Thus, postnatal DEX was not shown to have a negative effect on somatic growth at
school age, in line with the previous findings at 2-3 years (Jones et al 1995, Romagnoli et al
2002). (III)
A single dose of antenatal DEX had no harmful effect on the growth parameters in our
study, as reported in the follow-ups of randomized glucocorticoid trials at 3-20 years of age
(MacArthur et al 1982, CGAST 1984, Smolders-de Haas et al 1990, Dessens et al 2000).
After antenatal DEX, body height and weight were slightly greater at three years (CGAST
1984), and after betamethasone, girls were taller and heavier at six years (MacArthur et al
1982) than after placebo treatment. In our study, the placebo group was shorter for age than
the controls. (IV)
Our DEX studies suggest that the diseases associated with prematurity itself rather than
glucocorticoid caused the growth retardation.
5. Atopy
One fourth of the study children were atopic, i.e. had positive skin prick tests. In Study II,
atopy was less common in the children with BPD (8%) than in those without BPD (33%). The
atopic children had a higher birth weight and needed less initial respiratory care than the non-
atopic study children. Of the children with severe initial respiratory disease in Study III, only
one was atopic, in contrast to 35% of the Study IV participants, even though the rates reported
for familial atopy did not differ. None of the skin prick-positive children had received
postnatal DEX, which differed significantly from the skin prick-negative children.
In a Finnish population-based study, positive skin prick tests were found in 77% of
schoolchildren with asthma or other symptoms from lower airways and in 40% of controls
with no chronic or recurrent respiratory symptoms (Remes & Korppi 1996).
Our results support the proposal that severe neonatal lung disease is not associated with an
increased incidence of atopy (Pelkonen et al 1997). Thus, we propose that the initial
inflammation and inflammatory response, the medications used or the strategies to support
preterm infants may modify the direction of the inflammatory sequence towards skin prick
negativity.
86
6. Respiratory symptoms and medication
Half of our study children had glucocorticoid inhalations at 12 or 24 months of age, half
reported prolonged respiratory symptoms, and 10% reported regular use of inhalations. In the
Finnish study of schoolchildren, 7% had asthma and 8% other symptoms from lower airways
at the age of 7-12 years (Remes & Korppi 1996). The excess of morbidity and medication in
our study is in line with the previous studies of preschool or school-aged children born
preterm during the same period (Pelkonen et al 1997, Gross et al 1998, Korhonen et al
1999a). The abundant use of glucocorticoid inhalation by the BPD children at 12 months
might partly reflect, besides their high respiratory morbidity, the strategies to treat and follow
up BPD at that time; the use at 24 months probably reflects more accurately the prevailing
respiratory morbidity. The frequency of reported symptoms did not associate with BPD, as in
other studies (Gross et al 1998, Korhonen et al 1999a), but had a negative association with age
at the time of the study. The use of inhaled glucocorticoid was (Korhonen et al 1999a) and β2-
sympathomimetic agents (Gross et al 1998, Korhonen et al 1999a) tended to be more common
in BPD children. The use of inhaled medication during the preceding year associated with
impaired lung function, and no extra use due to the diagnosis of BPD was suspected at school
age. 27% of our study children had neither had prolonged respiratory symptoms nor used
inhalations until the time of study.
Reports of respiratory symptoms during follow-up after postnatal DEX trials are few: Jones et
al (1995) found no difference at three years, Yeh et al (1998) reported less upper respiratory
infections and rehospitalization at two years, and O´Shea et al (1999) found less frequent
rehospitalizations by the age of one year in the DEX than in the placebo group. Our finding of
no association between a �moderately early� course of postnatal DEX or the length of DEX
therapy during the first year of life and respiratory morbidity and medication are in line with
these previous findings in younger children. One fourth in each group had neither had
prolonged symptoms nor used inhalations by their enrolment in the study. (III)
The follow-up studies of randomized trials infrequently assess respiratory morbidity after
antenatal glucocorticoids: Smolders-de Haas et al (1990) reported more hospital admissions
because of infections or respiratory diseases during the first year after betamethasone
treatment. In our study, the use of antenatal DEX did not associate with respiratory morbidity
or medication at school age. (IV)
87
In all, half of our study children with and also without BPD reported prolonged respiratory
symptoms during the preceding year, suggesting that preterm infants even without a �high
risk� for respiratory morbidity may need a careful follow-up.
7. Smoking in the family
Exposure to tobacco smoke was common in our study children, as shown in the children born
very prematurely, but did not differ between the BPD and non-BPD groups or between the
subgroups in the DEX studies.
In contrast to previous findings (Chan et al 1989a), maternal smoking or smoking during
pregnancy had no detectable association with respiratory symptoms. Maternal smoking or
smoking during pregnancy was not associated with impairment of basic lung function, as
assessed by spirometry and IOS. Nor did smoking during pregnancy correlate with the values
of diffusing capacity tests. In the antenatal DEX study, however, the preterm children with
smoking mothers had significantly lower DLCO values and a tendency towards lower KCO
values compared with the children of non-smoking mothers. Smoking in the family also
tended to associate with decreased diffusion capacity. (IV)
Our study suggests that daily exposure to tobacco smoke might present a major threat to the
already impaired lung function of children born very preterm. Therefore, it is of utmost
importance to prevent children born very prematurely from starting smoking themselves, as
already emphasized by Northway et al (1990b) and more recently by Doyle et al (2003).
8. Lung function
Prematurely born children with or without BPD
Our study children had significantly impaired basic lung function in spirometry, comparable
to the previous studies of children born nearly ten years earlier (Hakulinen et al 1996,
Pelkonen et al 1997). The response to bronchodilator was increased, in line with the previous
findings of increased bronchial responsiveness and lability in home monitoring of PEF
(Pelkonen et al 1997). The values of basic spirometry were strikingly more seriously impaired
in BPD than in non-BPD children, similarly to the other studies using the criterion of oxygen
at 36 weeks (Pelkonen et al 1997, Gross et al 1998, Jacob et al 1998, Kilbride et al 2003), but
see Hakulinen et al (1996). (I)
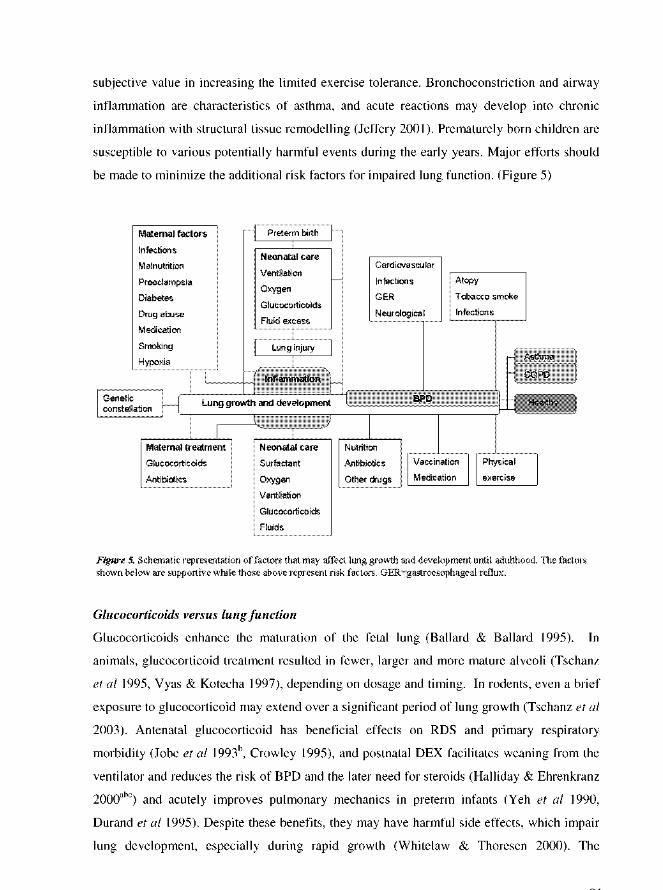

90
combination of antenatal and postnatal glucocorticoids or their repetitive use may further
increase the hazards. On the other hand, low dosage may decrease side effects. The possible
beneficial and adverse long-term effects on lung growth remain to be studied further.
Lung function after postnatal dexamethasone treatment
Few follow-up studies of postnatal DEX trials are available (Jones et al 1995, Yeh et al 1998,
O´Shea et al 1999, Shinwell et al 2000), with no results of long-term lung function. In both
groups of the present study, mechanically ventilated infants showed signs of airway
obstruction and increased bronchodilator responsiveness at school age in spirometry and,
correspondingly, in IOS. The only significant difference between the randomized groups was
the lower FVC in the placebo group. Half of the children in the placebo group failed to
perform the diffusing capacity test, rendering their results invalid.
Thus, we did not find any negative effects of our �moderately early� postnatal DEX
treatment on pulmonary outcome. The common use of later DEX treatment in the placebo
group (50%) may bias the results. (III)
Lung function after antenatal glucocorticoids
Follow-up studies of lung function after randomized antenatal trials continued until school
age are scarce: no negative effects of glucocorticoid on lung function were found at 10-12
years after betamethasone (Smolders-de Haas et al 1990) or at six years after DEX treatment
(Wiebicke et al 1988). In the latter case, however, only 12% of the original participants were
studied. In a cohort study, no significant differences were seen in lung function between the
betamethasone and control groups at the age of 14 years (Doyle et al 2000b).
In the present study, both groups of children born very prematurely showed signs of
airway obstruction and increased bronchodilator responsiveness in flow-volume spirometry
compared with the controls. Increased resistance and lower reactance in IOS in VLBW
children indicated airway obstruction. The study groups had lower diffusing capacity than the
controls. The only significant difference in lung function tests between our DEX and placebo
groups was the higher bronchodilator responsiveness (∆FEV1) in the placebo group. Although
the lower mean reactance, which mainly reflects respiratory dynamic compliance, and KCO
would seem to suggest more pronounced parenchymal involvement in the placebo group than
in the DEX group, the size of the placebo group was too small to warrant definite conclusions.
In line with previous studies, our data imply that antenatal DEX treatment has no negative
effects on pulmonary outcome. (IV)
91
9. Cardiovascular findings
In our study, only one girl with severe BPD had cardiac hypertrophy and increased pulmonary
arterial pressure still at school age (III and IV). This confirms the previous findings of no
cardiac hypertrophy (Farstad et al 1995, Korhonen et al 2004b) or significant pulmonary
hypertension at 2-7 years of age (Korhonen et al 2004b) in children born in the late 1980´s or
early 1990´s, contrary to the frequent finding of right ventricular hypertrophy and
cardiomegaly with cor pulmonale that accompanied the severe �old� BPD (Northway et al
1967, Markestad & Fitzhardinge 1981, Smyth et al 1981, Northway 1990a).
Abnormal lung vascular growth may be important in disturbing alveolar septation and the
formation of lung alveoli (Burri & Hislop 1998, Jobe & Bancalari 2001, Abman 2001, Parker
& Abman 2003). Glucocorticoids regulate lung and vascular growth and maturation at
different levels. Pharmacological doses may impair alveolarization by suppressing the
proliferation of capillaries within the septa (Tschanz et al 1995, Burri & Hislop 1998,
Tschanz et al 2003). However, this process may be reversible and depend on the length and
dosage of glucocorticoid therapy. As there are large interspecies differences in the duration of
vascular growth and the structural maturation of the lung, the interpretation of the
experimental results remains uncertain. (Burri & Hislop 1998, Tschanz et al 2003)
Pulmonary hypertension with raised pulmonary vascular resistance has been demonstrated
by cardiac catheterization in children with severe BPD until five years of age, associated with
poor prognosis, especially in those not responding to oxygen (Abman et al 1985, Berman et al
1986, Bush et al 1990). The neonatal decrease in pulmonary arterial pressure, assessed non-
invasively by echocardiography, is delayed in infants with RDS and may remain persistently
elevated in infants who subsequently develop BPD and serve as a sensitive marker of lung
injury (Gill & Weindling 1993, Subhedar et al 1998); it was still elevated at the age of one
year in BPD children (Subhedar & Shaw 2000). Pulmonary vasodilators, particularly inhaled
NO, may decrease the risk of BPD by decreasing intrapulmonary and extrapulmonary
shunting (Jobe & Bancalari 2001) and promoting lung growth and alveolarization by serving
as a downstream agonist of VEGF (Tang et al 2004).
Thus, the cardiac findings following BPD are modified in accordance with the changing
disease and treatments.
92
Cardiological findings after postnatal dexamethasone treatment
In our study of survivors, no hypertrophic cardiomyopathy was found (III).
After postnatal DEX treatment, hypertension was frequent (CDTG 1991, Ng 1993)
contributing to the development of myocardial hypertrophy or cardiomyopathy (Werner et al
1992, Ng 1993, Evans 1994, Yeh et al 1997), and fatal cardiomyopathy was reported (Riede
et al 2001). However, in randomized trials (Kothadia et al 1999, Romagnoli et al 1999),
DEX-associated ventricular septal hypertrophy and left ventricular outflow obstruction were
usually reversible, although some infants presented with clinical symptoms (Bensky et al
1996, Zecca et al 2001).
The fall in PAP seen after DEX treatment did not correlate with the respiratory
improvement. This did not support the theory of a DEX effect mediated through a reduction
in pulmonary vascular resistance. (Evans 1994) We found no differences in the Doppler-
mode-derived variables between the DEX and placebo groups. Two patients in the DEX
group tended to have a short pulmonary artery acceleration time, but with no evidence of
elevated PAP, in contrast to a previous study showing short acceleration times (<100 ms) to
be associated with increased pulmonary vascular resistance (Farstad et al 1995). In the DEX
group, three patients had a tricuspid regurgitation gradient of 30-40 mmHg, with no clinical or
X-ray findings of pulmonary hypertension. Clinical and echocardiographic manifestations of
cor pulmonale were evident in one placebo group girl with BPD. Our DEX and placebo
groups did not differ in PAP measured non-invasively. Mild tricuspid regurgitation was found
in three asymptomatic patients. One girl in the placebo group had ASD secundum with a
remarkable left-to-right shunt of 2.0. She had no BPD, but chest X-ray revealed an enlarged
heart and minor congestion in the lungs without evidence of chronic pulmonary changes. The
ASD was successfully closed with a device at the age of nine years. (III) However, in early
infancy, ASD may be a risk factor for BPD (Motz et al 2000).
Cardiological findings after antenatal glucocorticoids
In the present study, a trend towards less PDA after DEX treatment (33%) than after placebo
(100%) was seen, as suggested previously (Eronen et al 1993), with no significance in
difference (IV).
In randomized trials comparing fetal effects, both betamethasone and DEX induced
significant but reversible changes in heart rate acceleration and variability (Mulder et al 1997,
Rotmensch et al 1999, Subtil et al 2003). No constant effect has been confirmed on PDA
(Crowley 1995, Wright et al 1995). Antenatal DEX did not appear to affect cardiac
93
dimensions and blood flow velocity in neonatal preterm infants (Skelton et al 1998).
In a follow-up of randomized trials, more abnormalities, mostly heart murmur, were
reported at three years in the placebo group (CGAST 1984). Systolic blood pressure was
significantly lower in the betamethasone group, but no difference was seen at 20 years
(Dessens et al 2000). No echocardiographic studies exist on the long-term effects of antenatal
glucocorticoid on heart function or growth. In the present study, the cardiac outcome did not
differ significantly at school age, regardless of whether antenatal DEX or placebo was
administered. None of the infants required cardiovascular treatment. (IV)
To conclude, antenatal or postnatal DEX treatment was not associated with abnormal cardiac
function or growth. Nor was BPD frequently accompanied by cardiac findings. However,
cardiac evaluation is important in symptomatic children after DEX treatment, as some
individuals may be liable to serious side-effects, and in preterm born children with severe
lung disease, as the lung disease may lead to cardiac sequelae or mask the cardiac symptoms.
10. Neurosensory development
Before the era of antenatal glucocorticoid and surfactant in the 1970-1980´s, the live birth
prevalence of CP, especially spastic diplegia, increased in a population-based Swedish
follow-up, reflecting the improved survival of VLBW infants (Hagberg et al 1989). Later, no
further increase was seen, but there was a slight decrease in preterm CP. In 1991-1994, the
prevalence was 82 per 1000 for infants of 1000-1499 g birth weight (Hagberg et al 2001).
IVH and PVL were powerful predictors of CP (Hagberg et al 1996, Salokorpi et al 1999). The
neurosensory development of ELBW infants was recently reviewed by Tommiska (2003).
Previously, VLBW infants born in the 1970´s, especially those with BPD, were shown to
have more neurological abnormality than term controls at the age of 10-12 years (Vohr et al
1991).
Neurosensory development after glucocorticoid treatment
Glucocorticoids impair the growth and development of the immature brain, but they may
either enhance or reduce brain injury after hypoxia, depending on dosage or timing.
(Whitelaw & Thoresen 2000) After widespread use of postnatal DEX and initial reports of
adverse neurodevelopment in follow-up, concern also arose about the possible long-term
adverse effects of antenatal glucocorticoid, especially when used repetitively (Ng 1993).
94
Antenatal glucocorticoid treatment has been considered a �physiological� glucocorticoid
stress for the fetus, comparable to other maternal environmental stress factors. During a
sensitive time �window�, it may program the cardiopulmonary system, brain and other organs
for postnatal life. The effect may be modified by the immediate postnatal environment.
Apparently, similar events early in life may produce different responses, depending on their
intensity and timing. (Matthews 2000, Seckl 2001) Thus, by improving neonatal adaptation,
antenatal glucocorticoid treatment may improve the outcome.
Neurosensory development after postnatal dexamethasone treatment
After �delayed� DEX treatment, new periventricular abnormalities on brain ultrasound scans
were reported (Noble-Jamieson et al 1989). The following studies of �moderately early� and
�early� treatment did not reveal any significant effects on the incidence of severe IVH or
severe ROP (Halliday & Ehrenkranz 2000ab), but did reveal slower head growth during DEX
treatment in 2-week and 4-week groups (Papile et al 1998). One �early� trial was terminated
owing to the adverse outcome, particularly PVL, in the DEX group (Soll et al 1999, Vermont
Oxford Study 2001), but one study found more IVH of any grade in the placebo group
(Garland et al 1999). Head circumference was smaller at 36 gestational weeks in the DEX
group in a recent study of �early� low-dose treatment (Stark et al 2001).
In our study of �moderately early� DEX treatment, no differences emerged between the
groups in abnormal ultrasound findings; one girl in the DEX had IVH grade 3-4 and one boy
in the placebo group IVH grade 2-3, both diagnosed before study entry. In each group, one
child received cryotherapy for ROP. (III)
Few follow-up results of DEX trials are available. At first, the small trial of a 42-day
�moderately early� course showed improved neurodevelopmental outcome at 15 months of
age (Cummings et al 1989). Thereafter, in the 209 VLBW children of the CDTG trial (1991)
born before the era of antenatal glucocorticoid and surfactant, no difference was evident at
three years after �delayed� treatment in CP (DEX vs placebo, 20% vs 17%), severe disability,
severe or moderate disability, visual or hearing loss or expected need for special school or
extra help at school (Jones et al 1995). Later, a 42-day �delayed� course in surfactant-treated
infants (Kothadia et al 1999) increased the risk of CP (25% vs 7%) (O´Shea et al 1999).
Similarly, in two �early� trials, a 4-week course (Yeh et al 1997) increased neurological
abnormality at two years (40% vs 17%) (Yeh et al 1998), and a 3-day course in surfactant-
treated infants (Shinwell et al 1996) increased the incidence of CP (49% vs 15%) and
95
developmental delay at 2-6 years of age (55% vs 29%) (Shinwell et al 2000). In the latter
trial, the DEX-treated infants tended to have more PVL and less IVH than the placebo-treated
ones, with no significant difference; all infants with PVL, 38% of those with IVH grade 1-2
and 53% of those with IVH grade 3-4 developed CP. In these �early� studies, the children
were more mature at birth than ours. In a recent follow-up of an early trial, the 4-week course
associated with smaller head circumference, poorer motor skills, lower IQ and more
significant disabilities at eight years of age (Yeh et al 2004).
Five (31%) of our preterm study children had CP (DEX 38%, placebo 25%) and 13%
were severely and 44% severely or moderately disabled (DEX 38%, placebo 50%), one with
visual loss. All the children were able to walk without support, and 88% attended normal
school. All could perform at least some lung function tests. The hospital record data of the
four children lost from this follow-up did not change the results: no CP was found, all could
walk without support, all attended normal school, and one in each group had learning
difficulties. Our findings of CP and disability are in line with those of Jones et al (1995).
Thus, severe or moderate disability was common, as were minor neurological impairment and
learning disabilities. We found no significant association between postnatal DEX treatment
and neurological outcome at school age.
In the recent trials, DEX was used less often in the placebo group than earlier (Yeh et al
11%, O´Shea et al 0%, Shinwell et al 33%, our study 50%, Jones et al 40%), and the use of
antenatal glucocorticoid was more common (Yeh et al 32%, O´Shea et al 32%, Shinwell et al
26%, our study 25%, Jones et al 0%). In a review by Barrington (2001), the studies with less
than 30% contamination with open-label DEX showed a greater steroid effect and a high risk
of CP associated with postnatal DEX. As half of our placebo children received open-label
DEX, the long-term safety of DEX cannot be suggested based on the similar outcomes
between the DEX and placebo groups.
After the documented effects of DEX on developing brain, based on �early� and some
�delayed� trials, the American Academy of Pediatrics and the Canadian Paediatric Society
(2002) published guidelines for postnatal glucocorticoid treatment: the use was to be limited
to exceptional clinical circumstances. However, glucocorticoids continue to be used
frequently in the USA and Europe (Soll 2003, Truffert et al 2003), especially in ELBW
infants (Barrington 2001). The excess of adverse neurological outcomes after �early� DEX
treatment may be explained by the instability of the infant in the first few days after birth,
when its tolerance of adverse events may be low, and the risk of cerebral ischemia may be
96
increased. According to currently available evidence, neurodevelopmental risks supervene the
benefits to lung function. The cost-benefit ratio of DEX treatment may possibly shift from
negative to positive when treatment is started after the age of 7-10 days. (Halliday 2003) This
assumption is supported by the present results. This is constant dilemma in neonatological
practise. Antenatal glucocorticoids, especially repeated courses, may influence the effect of
DEX and complicate the conclusions of long-term sequelae. Further research is needed to
assess the dosage and duration of DEX or other glucocorticoid in the treatment of VLBW
infants predisposed to various antenatal insults, infections, mechanical ventilation and
postnatal interventions.
Neurosensory development after antenatal glucocorticoids
Antenatal glucocorticoids prevent IVH (Crowley 1995, NIH 1995, Wright et al 1995).
However, in a retrospective study of 883 preterm infants, antenatal DEX, but not
betamethasone, predisposed infants to cystic PVL (Baud et al 1999), while others found no
increase in abnormal brain ultrasound findings, including PVL, after DEX in ELBW infants
(LeFlore et al 2002). Contrary to this, our study showed abnormal brain ultrasound findings to
be less common in the DEX group than in the placebo group. In a prospective cohort study,
repeated doses of glucocorticoids associated with a decrease in head circumference at birth,
representing a reduction in cranial volume of nearly 11% (French et al 1999). Recently,
betamethasone was preferred to DEX, and no more than two courses were recommended
(Baud 2004).
Few long-term follow-up results of randomized antenatal trials continued until school age or
adulthood are available. In a Dutch study of 81 adults at 20 years of age, no significant
differences were found in CP or cognitive function between the betamethasone and placebo
groups (Dessens et al 2000); these adults had been more mature at birth than our children,
ranging from 27 to 40 gestational weeks. Previous follow-up studies after antenatal
betamethasone (MacArthur et al 1982) and DEX trials (CGAST 1984) revealed no negative
neurological outcomes at six years (MacArthur et al 1982) or three years (CGAST 1984) of
age: 82% and 55% of the survivors were studied, respectively. A cohort study showed
teenagers exposed to antenatal betamethasone to have better cognitive functioning at 14 years
compared with VLBW controls (Doyle et al 2000b).
In our study, seven (20%) children had CP (DEX 11%, placebo 50%), 6% needed a
wheelchair or a walking aid, 9% had visual loss, and 6% needed a hearing aid. 17% were
97
severely and 34% severely or moderately disabled (DEX 22%, placebo 75%). Minor
neurological impairment and learning problems were common in both groups. 89% of the
children in the DEX group and 38% in the placebo group attended normal school; speech
therapy, physiotherapy or extra help at school was frequently needed. In the DEX group, the
normal school attendance rate was higher, and there were less severe to moderate disability
and a tendency to less CP than in the placebo group, in line with the previous findings of no
negative outcome at school age after antenatal betamethasone (MacArthur et al 1982, Dessens
et al 2000). In contrast to previous studies, we presented the data of non-participants, i.e. 98%
of the survivors of the original trial, with no change in the results. (IV)
Thus, in our study, antenatal DEX associated with better neurological outcome at school age.
98
CONCLUSIONS
1. Obstructive and restrictive pulmonary dysfunction, bronchial hyperreactivity
and decreased gas exchange were evident in children born very prematurely,
especially in those with BPD. The impulse oscillometric method yielded lung
function information concordant with conventional methods. Being easier to
perform than spirometry, IOS served well in studying school-aged children, even
ones with neurological handicap or severe lung disease, and it may be useful in
preschool children as well.
2. Children with BPD rarely suffered from atopy. In non-atopic children born
very prematurely, exhaled nitric oxide values did not correlate with impaired lung
function, indicating that eNO was not an inflammatory marker in established BPD.
However, since atopy associated with increased eNO levels, we suggest that eNO
measurements may be valuable when studying atopic asthma even in preterm
children.
3. Neonatal dexamethasone therapy beginning ten days after birth in severely ill
ventilator-dependent infants associated with no detectable adverse effect on
cardiopulmonary function, somatic growth or neurosensory development at school
age. Severe or moderate disability was common. As half of the placebo children
received DEX after the trial, long-term safety cannot be suggested. More research is
needed for future conclusions.
4. Antenatal DEX treatment was not associated with any detectable adverse effect
on cardiopulmonary function or somatic growth. Besides initially helping more
infants to survive, it also caused a tendency for the children to have an improved
neurological outcome, as they had a higher rate of normal school attendance and
less severe or moderate disability. Survival without CP increased. In future studies
of different treatment strategies, the golden standard will be antenatal
betamethasone rather than placebo.
99
5. Children born very prematurely have an increased risk of abnormal lung
function and frequent respiratory symptoms at school age. Even though those with
the most severe initial lung disease were non-atopic, some children may
additionally develop atopic asthma. With immature survivors and differences in the
etiology of preterm birth, the clinical course of chronic lung disease may be
modified. We propose that lung function studies are important in the follow-up of
children born very preterm or with VLBW, with or without BPD. Asthma
medication should be tried if the clinical picture is reminiscent of asthma. Early
exposure to tobacco smoke associated with impaired gas exchange. These and other
very high-risk children should be strongly advised against smoking.
6. Antenatal or postnatal DEX treatment was not associated with abnormal
cardiac function or growth. We propose that cardiac evaluation should be included
in the follow-up of preterm children with severe lung disease, as the lung disease
may lead to cardiac sequelae or mask the symptoms of a cardiac defect.
100
ACKNOWLEDGEMENTS
This follow-up study was carried out at the Hospital for Children and Adolescents and the Skin and Allergy Hospital, in collaboration with the Division of Clinical Physiology and the Division of Pediatric Cardiology, during the years 1998-1999. I express my sincere gratitude to Professor Jaakko Perheentupa, former Head of the Hospital for Children and Adolescents, and his successors Professor Christer Holmberg, Professor Mikael Knip, Professor Martti Siimes and Docent Veli Ylitalo, Administrative Head of the Hospital for Children and Adolescents, and Docent Sture Andersson, Head of the Neonatal Unit, for creating and maintaining the excellent research facilities of the hospital. I am indebted to Docent Kaisu Juntunen-Backman, former Head of the Pediatric Department, and to Professor Tari Haahtela, Head of the Division of Allergy, for promoting my work and providing me with excellent research facilities.
I warmly thank my first teachers in neonatology: Professor Kari Raivio, Professor of Perinatology, aroused in me an interest in poorly breathing infants during my medical studies already with his unforgettable enthusiasm, curiosity and optimism. Docent Anna-Liisa Järvenpää taught me systematically the basic facts of neonatology in the Neonatal Intensive Care Unit and later in the Helsinki Maternity Hospital. I owe my deepest thanks to her and Docent Leena Lope, in memoriam, former Chief of the Neonatal Ward at Jorvi Hospital, for teaching and sharing the challenging work of neonatal care and follow-up after intensive care, as well as to all the skilful colleagues and staff in the neonatal units.
I am most grateful to my supervisors, Docent Markku Turpeinen at the Skin and Allergy Hospital and Professor Mikko Hallman, Head of the Department of Pediatrics, University of Oulu, for their encouragement and guidance throughout this process. I warmly thank Docent Turpeinen for the wide range of conversations on asthma and premature lung during these years. I admire his enthusiasm, open mind and creativeness in scientific thinking as well as his wide experience in pediatric pulmonology. I am very grateful to Professor Hallman whose constructive advice, thorough answers and never-failing support and interest were of essential importance, especially at the state of finishing the final manuscript. I had the honour to benefit from his profound knowledge in perinatal pulmonology already when adjusting ventilators during night shifts at the time when our study children were treated in the Neonatal Intensive Care Unit.
Docent Kirsti Heinonen and Kirsi Timonen, M.D., Ph.D., are gratefully acknowledged for their thorough interest and careful review of the final manuscript as well as for the enjoyable conversations and valuable comments.
I warmly thank Anneli Kari, M.D., for her consistent collaboration and support during these years. Her initial studies during 1989-1991 were the basis of this follow-up study. Her help in reaching the families and her interest in this study and valuable advise in writing the neonatological parts of the original manuscripts were essential.
I deeply thank Docent Pekka Malmberg, Chief of the Lung Function Laboratory of the Division of Allergy, for placing his expert knowledge at my disposal and guiding me into the world of pediatric lung function measurements. He supervised all the lung function tests at the Skin and Allergy Hospital and patiently helped in writing the original papers. His encouragement at the time of my first oral presentation in Florence is to be underlined.
I owe my thanks to Anna Pelkonen, M.D., for arousing my interest in this study. Her previous studies of premature infants have shown the importance of pulmonary follow-up of these children and facilitated further research. She also collaborated in studying the control children.
102
REFERENCES
AAP, see American Academy of Pediatrics. Abbasi S, Bhutani VK, Gerdes JS. Long-term pulmonary consequences of respiratory distress syndrome in preterm infants treated with exogenous surfactant. J Pediatr 1993;122:446-452. Abman SH. Bronchopulmonary dysplasia. �A vascular hypothesis�. Am J Respir Crit Care Med 2001;164:1755-1756. Abman SH, Wolfe RR, Accurso FJ, Koops BL, Bowman CM, Wiggins JW Jr. Pulmonary vascular response to oxygen in infants with severe bronchopulmonary dysplasia. Pediatrics 1985;75:80-84. Adamson IYR, King GM. Postnatal development of rat lung following retarded fetal lung growth. Pediatr Pulmonol 1988;4:230-236. Aghajafari F, Murphy K, Matthews S, Ohlsson A, Amankwah K, Hannah M. Repeated doses of antenatal corticosteroids in animals: a systematic review. Am J Obstet Gynecol 2002a;186:843-849. Aghajafari F, Murphy K, Ohlsson A, Amankwah K, Matthews S, Hannah M. Multiple versus single courses of antenatal corticosteroids for preterm birth: a pilot study. J Obstet Gynaecol Can 2002b;24:321-329. Ahola T, Lapatto R, Raivio KO, Selander B, Stigson L, Jonsson B, Jonsbo F, Esberg G, Stövring S, Kjartansson S, Stiris T, Lossius K, Virkola K, Fellman V. N-acetylcysteine does not prevent bronchopulmonary dysplasia in immature infants: a randomized controlled trial. J Pediatr 2003;143:713-719. Aikio O, Pokela ML, Hallman M. Exhaled and nasal nitric oxide in mechanically ventilated preterm and term newborns. Acta Paediatr 2002;91:1078-1086. Aikio O, Saarela T, Pokela ML, Hallman M. Nitric oxide treatment and acute pulmonary inflammatory response in very premature infants with intractable respiratory failure shortly after birth. Acta Paediatr 2003;92:65-69. Aikio O, Vuopala K, Pokela ML, Hallman M. Diminished inducible nitric oxide synthase expression in fulminant early-onset neonatal pneumonia. Pediatrics 2000;105:1013-1019. Alving K, Weitzberg E, Lundberg JM. Increased amount of nitric oxide in exhaled air of asthmatics. Eur Respir J 1993;6:1368-1370. American Academy of Pediatrics, Committee on Fetus and Newborn, and Canadian Paediatric Society, Fetus and Newborn Committee. Postnatal corticosteroids to treat or prevent chronic lung disease in preterm infants. Pediatrics 2002;109:330-338. American Thoracic Society. Recommendations for standardized procedures for the online and offline measurement of exhaled lower respiratory nitric oxide and nasal nitric oxide in adults and children�1999. Am J Respir Crit Care Med 1999;160:2104-2117. American Thoracic Society. Standardization of spirometry. 1994 update. Am J Respir Crit Care Med 1995;152:1107-1136. American Thoracic Society/European Respiratory Society. Respiratory mechanics in infants: physiologic evaluation in health and disease. Am Rev Respir Dis 1993;147:474-496. ATS, see American Thoracic Society. Avery GB, Fletcher AB, Kaplan M, Brudno DS. Controlled trial of dexamethasone in respirator-dependent infants with bronchopulmonary dysplasia. Pediatrics 1985;75:106-111. Avery ME, Mead J. Surface properties in relation to atelectasis and hyaline membrane disease. Am J Dis Child 1959;97:517-523. Avery ME, Tooley WH, Keller JB, Hurd SS, Bryan MH, Cotton RB, Epstein MF, Fitzhardinge PM, Hansen CB, Hansen TN, Hodson WA, James LS, Kitterman JA, Nielsen HC, Poirier TA, Truog WE, Wung JT. Is chronic lung disease in low birth weight infants preventable? A survey of eight centers. Pediatrics 1987;79:26-30. Azzawi M, Bradley B, Jeffery PK, Frew AJ, Wardlaw AJ, Knowles G, Assoufi B, Collins JV, Durham S, Kay AB. Identification of activated T lymphocytes and eosinophils in bronchial biopsies in stable atopic asthma. Am Rev Respir Dis 1990;142:1407-1413. Baden M, Bauer CR, Colle E, Klein G, Taeusch HW Jr, Stern L. A controlled trial of hydrocortisone therapy in infants with respiratory distress syndrome. Pediatrics 1972;50:526-534.
103
Bader D, Ramos AD, Cheryl DL, Platzker ACG, Stabile MW, Keens TG. Childhood sequelae of infant lung disease: exercise and pulmonary function abnormalities after bronchopulmonary dysplasia. J Pediatr 1987;110:693-699. Balfour-Lynn IM, Laverty A, Dinwiddie R. Reduced upper airway nitric oxide in cystic fibrosis. Arch Dis Child 1996;75:319-322. Ballard PL, Ballard RA. Scientific basis and therapeutic regimens for use of antenatal glucocorticoids.Am J Obstet Gynecol 1995;173:254-262. Ballard RA, Ballard PL, Cnaan A, Pinto-Martin J, Davis DJ, Padbury JF, Phibbs RH, Parer JT, Hart MC, Mannino FL, Sawai SK. Antenatal thyrotropin-releasing hormone to prevent lung disease in preterm infants. N Engl J Med 1998;338:493-498. Bancalari E, Abdenour GE, Feller R, Gannon J. Bronchopulmonary dysplasia: clinical presentation. J Pediatr 1979;95:819-823. Bancalari E, Bidegain M. Respiratory disorders of the newborn. In: Taussig LM, Landau LI, ed. Pediatric Respiratory Medicine. Mosby, Inc., St. Louis, 1999, pp. 464-488. Banks BA, Cnaan A, Morgan MA, Parer JT, Merrill JD, Ballard PL, Ballard RA, The North American Thyrotropin-Releasing Hormone Study Group. Multiple courses of antenatal corticosteroids and outcome of premature neonates. Am J Obstet Gynecol 1999;181:709-717. Baraldi E, Azzolin NM, Zanconato S, Dario C, Zacchello F. Corticosteroids decrease exhaled nitric oxide in children with acute asthma. J Pediatr 1997;131:381-385. Barker DJP. Fetal origins of coronary heart disease. BMJ 1995;311:171-174. Barnes PJ, Belvisi M. Nitric oxide and lung disease. Thorax 1993;48:1034-1043. Barrington KJ. The adverse neuro-developmental effects of postnatal steroids in the preterm infant: a systematic review of RCTs. BMC Pediatr 2001;1:1. Barrington KJ, Finer NN. Treatment of bronchopulmonary dysplasia. In: Goldsmith JP, Spitzer AR, ed. Clinics in Perinatology. Controversies in neonatal pulmonary care. W.B. Saunders Company, Philadelphia, 1998;25:177-202. Baud O. Antenatal corticosteroid therapy: benefits and risks. Acta Paediatr 2004;Suppl 444:6-10. Baud O, Foix-L´Helias L, Kaminski M, Audibert F, Jarreau PH, Papiernik E, Huon C, Lepercq J, Dehan M, Lacaze-Masmonteil T. Antenatal glucocorticoid treatment and cystic periventricular leukomalacia in very premature infants. N Engl J Med 1999;341:1190-1196. Bejar R, Coen RW, Merritt TA, Vaucher Y, Trice J, Centeno R, Gilles F. Focal necrosis of the white matter (periventricular leukomalacia): sonographic, pathologic, and electroencephalographic features. AJNR Am J Neuroradiol 1986;7:1073-1080. Bensky AS, Kothadia JM, Covitz W. Cardiac effects of dexamethasone in very low birth weight infants. Pediatrics 1996;97:818-821. Berman W Jr, Katz R, Yabek SM, Dillon T, Fripp RR, Papile LA. Long-term follow-up of bronchopulmonary dysplasia. J Pediatr 1986;109:45-50. Bhuta T, Ohlsson A. Systematic review and meta-analysis of early postnatal dexamethasone for prevention of chronic lung disease. Arch Dis Child Fetal Neonatal Ed 1998;79:F26-F33. Bisgaard H, Klug B. Lung function measurement in awake young children. Eur Respir J 1995;8:2067-2075. Blayney M, Kerern E, Whyte H, O´Brodovich H. Bronchopulmonary dysplasia: improvement in lung function between 7 and 10 years of age. J Pediatr 1991;118:201-206. Bloom SL, Sheffield JS, McIntire DD, Leveno KJ. Antenatal dexamethasone and decreased birth weight. Obstet Gynecol 2001;97:485-490. Bouaziz N, Beyaert C, Gauthier R, Monin P, Peslin R, Marchal F. Respiratory system reactance as an indicator of the intrathoracic airway response to methacholine in children. Pediatr Pulmonol 1996;22:7-13. Bousquet J, Chanez P, Lacoste JY, Barnéon G, Ghavanian N, Enander I, Venge P, Ahlstedt S, Simony-Lafontaine J, Godard P, Michel FB. Eosinophilic inflammation in asthma. N Engl J Med 1990;323:1033-1039. Buhr W, Jörres R, Berdel D, Làndsér FJ. Correspondence between forced oscillation and body plethysmography during bronchoprovocation with carbachol in children. Pediatr Pulmonol 1990;8:280-288.

104
Burri PH. Structural aspects of prenatal and postnatal development and growth of the lung. In: McDonald JA, ed. Lung Growth and Development. Marcel Dekker, Inc, New York, 1997, pp. 1-35. Burri PH, Hislop AA. Structural considerations. Eur Respir J 1998;12 Suppl 27:59S-65S. Bush A, Busst CM, Knight WB, Hislop AA, Haworth SG, Shinebourne EA. Changes in pulmonary circulation in severe bronchopulmonary dysplasia. Arch Dis Child 1990;65:739-745. Carlton DP, Albertine KH, Cho SC, Lont M, Bland RD. Role of neutrophils in lung vascular injury and edema after premature birth in lambs. J Appl Physiol 1997;83:1307-1317. Cauberghs M, Van de Woestijne KP. Effect of upper airway shunt and series properties on respiratory impedance measurements. J Appl Physiol 1989;66:2274-2279. CDTG, see Collaborative Dexamethasone Trial Group. CGAST, see Collaborative Group on Antenatal Steroid Therapy. Chambers HM, van Velzen D. Ventilator-related pathology in the extremely immature lung. Pathology 1989;21:79-83. Chan KN, Elliman A, Bryan EM, Silverman M. Respiratory symptoms in children of low birth weight. Arch Dis Child 1989a;64:1294-1304. Chan KN, Noble-Jamieson CM, Elliman A, Bryan EM, Silverman M. Lung function in children of low birth weight. Arch Dis Child 1989b;64:1284-1293. Chan KN, Silverman M. Increased airway responsiveness in children of low birth weight at school age: effect of topical corticosteroids. Arch Dis Child 1993;69:120-124. Charafeddine L, D´Angio CT, Phelps DL. Atypical chronic lung disease patterns in neonates. Pediatrics 1999;103:759-765. Clark DA, Pincus LG, Oliphant M, Hubbell C, Oates RP, Davey FR. HLA-A2 and chronic lung disease in neonates. JAMA 1982;248:1868-1869. Clément J, Lándsèr FJ, Van de Woestijne KP. Total resistance and reactance in patients with respiratory complaints with and without airway obstruction. Chest 1983;83:215-220. Coalson JJ. Pathology of new bronchopulmonary dysplasia. Semin Neonatol 2003;8:73-81. Coalson JJ, Winter V, deLemos RA. Decreased alveolarization in baboon survivors with bronchopulmonary dysplasia. Am J Respir Crit Care Med 1995;152:640-646. Coalson JJ, Winter VT, Siler-Khodr T, Yoder BA. Neonatal chronic lung disease in extremely immature baboons. Am J Respir Crit Care Med 1999;160:1333-1346. Cole CH, Colton T, Shah BL, Abbasi S, MacKinnon BL, Demissie S, Frantz ID. Early inhaled glucocorticoid therapy to prevent bronchopulmonary dysplasia. N Engl J Med 1999;340:1005-1010. Cole TJ, Blendy JA, Monaghan AP, Krieglstein K, Schmid W, Aguzzi A, Fantuzzi G, Hummler E, Unsicker K, Schütz G. Targeted disruption of the glucocorticoid receptor gene blocks adrenergic chromaffin cell development and severely retards lung maturation. Genes Dev 1995;9:1608-1621. Collaborative Dexamethasone Trial Group (CDTG). Dexamethasone therapy in neonatal chronic lung disease: an international placebo-controlled trial. Pediatrics 1991;88:421-427. Collaborative Group on Antenatal Steroid Therapy (CGAST). Effect of antenatal dexamethasone administration on the prevention of respiratory distress syndrome. Am J Obstet Gynecol 1981;141:276-287. Collaborative Group on Antenatal Steroid Therapy (CGAST). Effects of antenatal dexamethasone administration in the infant: long-term follow-up. J Pediatr 1984;104:259-267. Cotes JE, Chinn DJ, Quanjer PH, Roca J, Yernault JC. Standardization of the measurement of transfer factor (diffusing capacity). Eur Respir J 1993;6 Suppl 16:41-52. Cotes JE, Dabbs JM, Hall AM, Heywood C, Laurence KM. Sitting height, fat-free mass and body fat as reference variables for lung function in healthy British children: comparison with stature. Ann Hum Biol 1979;6:307-314. Crowley P. Prophylactic corticosteroids for preterm birth (Cochrane Review). In: The Cochrane Library, Issue 2, 2004. Chichester, UK: John Wiley & Sons, Ltd. Cochrane Database Syst Rev 2000;(2):CD000065. Crowley PA. Antenatal corticosteroid therapy: a meta-analysis of the randomized trials, 1972 to 1994. Am J Obstet Gynecol 1995;173:322-335. Crowther CA, Harding J. Repeat doses of prenatal corticosteroids for women at risk of preterm birth for preventing neonatal respiratory disease (Cochrane Review). In: The Cochrane Library, Issue 2, 2004. Chichester, UK: John Wiley & Sons, Ltd. Cochrane Database Syst Rev 2003;(3):CD003935.
105
Cummings JJ, D´Eugenio DB, Gross SJ. A controlled trial of dexamethasone in preterm infants at high risk for bronchopulmonary dysplasia. N Engl J Med 1989;320:1505-1510. D´Angio CT, Maniscalco WM, Ryan RM, Avissar NE, Basevegowda K, Sinkin RA. Vascular endothelial growth factor in pulmonary lavage fluid from premature infants: effects of age and postnatal dexamethasone. Biol Neonate 1999;76:266-273. De Jong JW, van der Belt-Gritter B, Koëter GH, Postma DS. Peripheral blood lymphocyte cell subsets in subjects with chronic obstructive pulmonary disease: association with smoking, IgE and lung function. Respir Med 1997;91:67-76. Delacourt C, Lorino H, Herve-Guillot M, Reinert P, Harf A, Housset B. Use of the forced oscillation technique to assess airway obstruction and reversibility in children. Am J Respir Crit Care Med 2000;161:730-736. Dessens AB, Smolders-de Haas H, Koppe JG. Twenty-year follow-up of antenatal corticosteroid treatment. Pediatrics 2000;105(6):e77. Doyle LW. Growth and respiratory health in adolescence of the extremely low-birth weight survivor. In: Vohr BR, ed. Clinics in Perinatology. Outcome of the very low-birth weight infant. W.B. Saunders Company, Philadelphia, 2000a;27:421-432. Doyle LW, Chavasse R, Ford GW, Olinsky A, Davis NM, Callanan C. Changes in lung function between age 8 and 14 years in children with birth weight of less than 1,501 g. Pediatr Pulmonol 1999;27:185-190. Doyle LW, Ford GW, Rickards AL, Kelly EA, Davis NM, Callanan C, Olinsky A. Antenatal corticosteroids and outcome at 14 years of age in children with birth weight less than 1501 grams. Pediatrics 2000b;106(1):e2. Doyle LW, Olinsky A, Faber B, Callanan C. Adverse effects of smoking on respiratory function in young adults born weighing less than 1000 grams. Pediatrics 2003;112:565-569. DuBois AB, Brody AW, Lewis DH, Burgess BF. Oscillation mechanics of lungs and chest in man. J Appl Physiol 1956;8:587-594. Duiverman EJ, Clément J, van de Woestijne KP, Neijens HJ, van den Bergh ACM, Kerrebijn KF. Forced oscillation technique. Reference values for resistance and reactance over a frequency spectrum of 2-26 Hz in healthy children aged 2.3-12.5 years. Bull Eur Physiopathol Respir 1985;21:171-178. Duiverman EJ, den Boer JA, Roorda RJ, Rooyackers CMHM, Valsstar M, Kerrebijn KF. Lung function and bronchial responsiveness measured by forced oscillometry after bronchopulmonary dysplasia. Arch Dis Child 1988;63:727-732. Durand M, Sardesai S, McEvoy C. Effects of early dexamethasone therapy on pulmonary mechanics and chronic lung disease in very low birth weight infants: a randomized, controlled trial. Pediatrics 1995;95:584-590. Edwards DK. Radiographic aspects of bronchopulmonary dysplasia. J Pediatr 1979a;95:823-829. Edwards DK, Colby TV, Northway WN Jr. Radiographic-pathologic correlation in bronchopulmonary dysplasia. J Pediatr 1979b;95:834-836. Ehrenkranz RA, Younes N, Lemons JA, Fanaroff AA, Donovan EF, Wright LL, Katsikiotis V, Tyson JE, Oh W, Shankaran S, Bauer CR, Korones SB, Stoll BJ, Stevenson DK, Papile LA. Longitudinal growth of hospitalized very low birth weight infants. Pediatrics 1999;104:280-289. Eronen M, Kari A, Pesonen E, Hallman M. The effect of antenatal dexamethasone administration on the fetal and neonatal ductus arteriosus. A randomized double-blind study. Am J Dis Child 1993;147:187-192. Evans N. Cardiovascular effects of dexamethasone in the preterm infant. Arch Dis Child Fetal Neonatal Ed 1994;70:F25-F30. Farstad T, Brockmeier F, Bratlid D. Cardiopulmonary function in premature infants with bronchopulmonary dysplasia � a 2-year follow up. Eur J Pediatr 1995;154:853-858. Ferreira PJ, Bunch TJ, Albertine KH, Carlton DP. Circulating neutrophil concentration and respiratory distress in premature infants. J Pediatr 2000;136:466-472. Fletcher AJW, Goodfellow MR, Forhead AJ, Gardner DS, McGarrigle HHG, Fowden AL, Giussani DA. Low doses of dexamethasone suppress pituitary-adrenal function but augment the glycemic response to acute hypoxemia in fetal sheep during late gestation. Pediatr Res 2000;47:684-691. Ford GW, Doyle LW, Davis NM, Callanan C. Very low birth weight and growth into adolescence. Arch Pediatr Adolesc Med 2000;154:778-784.
106
Forsén T, Eriksson JG, Tuomilehto J, Osmond C, Barker DJP. Growth in utero and during childhood among women who develop coronary heart disease: longitudinal study. BMJ 1999;7222:1403-1407. Frank TL, Adisesh A, Pickering AC, Morrison JFJ, Wright T, Francis H, Fletcher A, Frank PI, Hannaford P. Relationship between exhaled nitric oxide and childhood asthma. Am J Respir Crit Care Med 1998;158:1032-1036. Franklin PJ, Taplin R, Stick SM. A community study of exhaled nitric oxide in healthy children. Am J Respir Crit Care Med 1999;159:69-73. French NP, Hagan R, Evans SF, Godfrey M, Newnham JP. Repeated antenatal corticosteroids: size at birth and subsequent development. Am J Obstet Gynecol 1999;180:114-121. Fujiwara T, Maeta H, Chida S, Morita T, Watabe Y, Abe T. Artificial surfactant therapy in hyaline-membrane disease. Lancet 1980;8159:55-59. Galdès-Sebaldt M, Sheller JR, Grogaard J, Stahlman M. Prematurity is associated with abnormal airway function in childhood. Pediatr Pulmonol 1989;7:259-264. Garland JS, Alex CP, Pauly TH, Whitehead VL, Brand J, Winston JF, Samuels DP, McAuliffe TL. A three-day course of dexamethasone therapy to prevent chronic lung disease in ventilated neonates: a randomized trial. Pediatrics 1999;104:91-99. Gerhardt T, Bancalari E. Chestwall compliance in full-term and premature infants. Acta Paediatr Scand 1980;69:359-364. Gerhardt T, Hehre D, Feller R, Reifenberg L, Bancalari E. Pulmonary mechanics in normal infants and young children during first 5 years of life. Pediatr Pulmonol 1987a;3:309-316. Gerhardt T, Hehre D, Feller R, Reifenberg L, Bancalari E. Serial determination of pulmonary function in infants with chronic lung disease. J Pediatr 1987b;110:448-456. Gerhardt T, Reifenberg L, Goldberg RN, Bancalari E. Pulmonary function in preterm infants whose lungs were ventilated conventionally or by high-frequency oscillation J Pediatr 1989;115:121-126. Gill AB, Weindling AM. Pulmonary artery pressure changes in the very low birthweight infant developing chronic lung disease. Arch Dis Child 1993;68:303-307. Groneck P, Speer CP. Inflammatory mediators and bronchopulmonary dysplasia. Arch Dis Child Fetal Neonatal Ed 1995;73:F1-F3. Gross SJ, Iannuzzi DM, Kveselis DA, Anbar RD. Effect of preterm birth on pulmonary function at school age: a prospective controlled study. J Pediatr 1998;133:188-192. Guinn DA, Atkinson MW, Sullivan L, Lee MJ, MacGregor S, Parilla BV, Davies J, Hanlon-Lundberg K, Simpson L, Stone J, Wing D, Ogasawara K, Muraskas J. Single vs weekly courses of antenatal corticosteroids for womene at risk of preterm delivery: a randomized controlled trial. JAMA 2001;286:1581-1587. Gustafsson LE, Leone AM, Persson MG, Wiklund NP, Moncada S. Endogenous nitric oxide is present in the exhaled air of rabbits, guinea pigs and humans. Biochem and Biophys Res Commun 1991;181:852-857. Hack M, Breslau N, Weissman B, Aram D, Klein N, Borawski E. Effect of very low birth weight and subnormal head size on cognitive abilities at school age. N Engl J Med 1991;325:231-237. Hack M, Schluchter M, Cartar L, Rahman M, Cuttler L, Borawski E. Growth of very low birth weight infants to age 20 years. Pediatrics 2003;112(1):e30-e38. Hack M, Wright LL, Shankaran S, Tyson JE, Horbar JD, Bauer CR, Younes N. Very-low-birth-weight outcomes of the National Institute of Child Health and Human Development Neonatal Network, November 1989 to October 1990. Am J Obstet Gynecol 1995;172:457-464. Hagberg B, Hagberg G, Beckung E, Uvebrant. Changing panorama of cerebral palsy in Sweden. VIII. Prevalence and origin in the birth year period 1991-94. Acta Paediatr 2001;90:271-277. Hagberg B, Hagberg G, Olow I, v Wendt L. The changing panorama of cerebral palsy in Sweden. VII. Prevalence and origin in the birth year period 1987-90. Acta Paediatr 1996;85:954-960. Hagberg B, Hagberg G, Zetterström R. Decreasing perinatal mortality � increase in cerebral palsy morbidity? Acta Paediatr Scand 1989;78:664-670. Hakulinen AL, Heinonen K, Länsimies E, Kiekara O. Pulmonary function and respiratory morbidity in school-age children born prematurely and ventilated for neonatal respiratory insufficiency. Pediatr Pulmonol 1990;8:226-232.
107
Hakulinen AL, Järvenpää AL, Turpeinen M, Sovijärvi A. Diffusing capacity of the lung in school-aged children born very preterm, with and without bronchopulmonary dysplasia. Pediatr Pulmonol 1996;21:353-360. Halliday HL. Postnatal dexamethasone: what is the real cost-benefit ratio? Acta Paediatr 2003;92:888-889. Halliday HL, Ehrenkranz RA. Early postnatal (<96 hours) corticosteroids for preventing chronic lung disease in preterm infants. In: The Cochrane Library, Issue 2, 2000. Oxford: Update software. Cochrane Database Syst Rev 2000a;(2):CD001146. Halliday HL, Ehrenkranz RA. Moderately early (7-14 days) corticosteroids for preventing chronic lung disease in preterm infants. In: The Cochrane Library, Issue 2, 2000. Oxford: Update software. Cochrane Database Syst Rev 2000b;(2):CD001144. Halliday HL, Ehrenkranz RA. Delayed (>3 weeks) postnatal corticosteroids for chronic lung disease in preterm infants. In: The Cochrane Library, Issue 2, 2000. Oxford: Update software. Cochrane Database Syst Rev 2000c;(2):CD001145. Hallman M. Antenatal diagnosis of lung maturity. In: Robertson B, Van Golde LMG, Batenburg JJ, ed. Pulmonary Surfactant. From molecular biology to clinical practice. Elsevier, Amsterdam, 1992a, pp. 425-458. Hallman M. Lung surfactant, respiratory failure, and genes. N Engl J Med 2004;350:1278-1280. Hallman M, Bry K, Hoppu K, Lappi M, Pohjavuori M. Inositol supplementation in premature infants with respiratory distress syndrome. N Engl J Med 1992b;326:1233-1239. Hallman M, Glumoff V, Rämet M. Surfactant in respiratory distress syndrome and lung injury. Comp Biochem Physiol A Mol Integr Physiol 2001;129:287-294. Hallman M, Haataja R, Marttila R. Surfactant proteins and genetic predisposition to respiratory distress syndrome. Semin Perinatol 2002;26:450-460. Hannaford K, Todd DA, Jeffery H, John E, Byth K, Gilbert GL. Role of ureaplasma urealyticum in lung disease of prematurity. Arch Dis Child Fetal Neonatal Ed 1999;81:F162-F167. Harkavy KL, Scanlon JW, Chowdhry PK, Grylack LJ. Dexamethasone therapy for chronic lung disease in ventilator- and oxygen-dependent infants: a controlled trial. J Pediatr 1989;115:979-983. Hellinckx J, Cauberghs M, De Boeck K, Demedts M. Evaluation of impulse oscillation system: comparison with forced oscillation technique and body plethysmography. Eur Respir J 2001;18:564-570. Hellinckx J, De Boeck K, Demedts M. No paradoxical bronchodilator response with forced oscillation techniques in children with cystic fibrosis. Chest 1998;113:55-59. Helve O, Pitkänen OM, Andersson S, O´Brodovich H, Kirjavainen T, Otulakowski G. Low expression of human epithelial sodium channel in airway epithelium of preterm infants with respiratory distress. Pediatrics 2004;113:1267-72. Henderson-Smart DJ, Bhuta T, Cools F, Offringa M. Elective high frequency oscillatory ventilation versus conventional ventilation for acute pulmonary dysfunction in preterm infants (Cochrane Review). In: The Cochrane Library, Issue 3, 2004. Chichester, UK: John Wiley & Sons, Ltd. Cochrane Database Syst Rev 2003;(4):CD000104. Horbar JD, McAuliffe TL, Adler SM, Albersheim S, Cassady G, Edwards W, Jones R, Kattwinkel J, Kraybill EN, Krishnan V, Raschko P, Wilkinson AR. Variability in 28-day outcomes for very low birth weight infants: an analysis of 11 neonatal intensive care units. Pediatrics 1988;82:554-559. Huang WL, Beazley LD, Quinlivan JA, Evans SF, Newnham JP, Dunlop SA. Effect of corticosteroids on brain growth in fetal sheep. Obstet Gynecol 1999;94:213-218. Husain AN, Siddiqui NH, Stocker JT. Pathology of arrested acinar development in postsurfactant bronchopulmonary dysplasia. Hum Pathol 1998;29:710-717. Hyde I, English RE, Williams JD. The changing pattern of chronic lung disease of prematurity. Arch Dis Child 1989;64:448-451. An International classification of retinopathy of prematurity. Pediatrics 1984;74:127-133. Jacob SV, Coates AL, Lands LC, MacNeish CF, Riley SP, Hornby L, Outerbridge EW, Davis GM, Williams RL. Long-term pulmonary sequelae of severe bronchopulmonary dysplasia. J Pediatr 1998;133:193-200. Jeffery P. Inflammation and remodeling in the adult and child with asthma. Pediatr Pulmonol 2001;Suppl 21:3-16.
108
Jeffery PK. Comparison of the structural and inflammatory features of COPD and asthma: Giles F. Filley lecture. Chest 2000a;117 Suppl 1:251S-260S. Jeffery PK, Laitinen A, Venge P. Biopsy markers of airway inflammation and remodelling. Respir Med 2000b;94 Suppl F:S9-S15. Jobe AH. Pulmonary surfactant therapy. N Engl J Med 1993a;328:861-868. Jobe AH, Bancalari E. Bronchopulmonary dysplasia. NICHD/NHLBI/ORD Workshop summary. Am J Respir Crit Care Med 2001;163:1723-1729. Jobe AH, Mitchell BR, Gunkel JH. Beneficial effects of the combined use of prenatal corticosteroids and postnatal surfactant on preterm infants. Am J Obstet Gynecol 1993b;168:508-513. Jobe AH, Newnham J, Willet K, Sly P, Ikegami M. Fetal versus maternal and gestational age effects of repetitive antenatal glucocorticoids. Pediatrics 1998;102:1116-1125. Jobe AJ. The new BPD: an arrest of lung development. Pediatr Res 1999;46:641-643. Jones R, Wincott E, Elbourne D, Grant A. Controlled trial of dexamethasone in neonatal chronic lung disease: a 3 year follow-up. Pediatrics 1995;96:897-906. Kallio J, Karlsson R, Toppari J, Helminen T, Scheinin M, Kero P. Antenatal dexamethasone treatment decreases plasma catecholamine levels in preterm infants. Pediatr Res 1998;43:801-807. Kari MA, Akino T, Hallman M. Prenatal dexamethasone and exogenous surfactant therapy: surface activity and surfactant components in airway specimens. Pediatr Res 1995;38:676-684. Kari MA, Hallman M, Eronen M, Teramo K, Virtanen M, Koivisto M, Ikonen RS. Prenatal dexamethasone treatment in conjunction with rescue therapy of human surfactant: a randomized placebo-controlled multicenter study. Pediatrics 1994;93:730-736. Kari MA, Heinonen K, Ikonen RS, Koivisto M, Raivio KO. Dexamethasone treatment in preterm infants at risk for bronchopulmonary dysplasia. Arch Dis Child 1993;68:566-569. Kazzi NJ, Brans YW, Poland RL. Dexamethasone effects on the hospital course of infants with bronchopulmonary dysplasia who are dependent on artificial ventilation. Pediatrics 1990;86:722-727. Kharitonov S, Alving K. Barnes PJ. Exhaled and nasal nitric oxide measurements: recommendations. European Respiratory Society Task Force report. Eur Respir J 1997;10:1683-1693. Kharitonov SA, Yates DH, Barnes PJ. Inhaled glucocorticoids decrease nitric oxide in exhaled air of asthmatic patients. Am J Respir Crit Care Med 1996;153:454-457. Kharitonov SA, Yates D, Robbins RA, Logan-Sinclair R, Shinebourne EA, Barnes PJ. Increased nitric oxide in exhaled air of asthmatic patients. Lancet 1994;343:133-135. Kilbride HW, Gelatt MC, Sabath RJ. Pulmonary function and exercise capacity for ELBW survivors in preadolescence: effect of neonatal chronic lung disease. J Pediatr 2003;143:488-493. Klug B, Bisgaard H. Measurement of lung function in awake 2-4-year-old asthmatic children during methacholine challenge and acute asthma: a comparison of the impulse oscillation technique, the interrupter technique, and transcutaneous measurement of oxygen versus whole-body plethysmography. Pediatr Pulmonol 1996;21:290-300. Koivisto M, Marttila R, Kurkinen-Räty M, Saarela T, Pokela ML, Jouppila P, Hallman M. Changing incidence and outcome of infants with respiratory distress syndrome in the 1990s: a population-based survey. Acta Paediatr 2004;93:177-184. Korhonen P. Bronchopulmonary dysplasia in very low birth weight infants. Frequency, risk factors and 7-year outcome. Academic dissertation, University of Tampere. Tampereen yliopistopaino Oy Juvenes Print, Tampere, 2004a. Korhonen P, Hyödynmaa E, Lautamatti V, Iivanainen T, Tammela O. Cardiovascular findings in very low birth weight schoolchildren with and without bronchopulmonary dysplasia. 2004b. In: Korhonen 2004a. Korhonen P, Hyödynmaa E, Lenko HL, Tammela O. Growth and adrenal androgen status at 7 years in very low birth weight survivors with and without bronchopulmonary dysplasia. Arch Dis Child 2004c;89:320-324. Korhonen P, Koivisto AM, Ikonen S, Laippala P, Tammela O. Very low birthweight, bronchopulmonary dysplasia and health in early childhood. Acta Paediatr 1999a;88:1385-1391. Korhonen P, Tammela O, Koivisto AM, Laippala P, Ikonen S. Frequency and risk factors in bronchopulmonary dysplasia in a cohort of very low birth weight infants. Early Hum Dev 1999b;54:245-258.
109
Kosturakis D, Goldberg SJ, Allen HD, Loeber C. Doppler echocardiographic prediction of pulmonary arterial hypertension in congenital heart disease. Am J Cardiol 1984;53:1110-1115. Kotecha S. Lung growth: implications for the newborn infant. Arch Dis Child Fetal Neonatal Ed 2000;82:F69-F74. Kotecha S, Allen J. Oxygen therapy for infants with chronic lung disease. Arch Dis Child Fetal Neonatal Ed 2002;87:F11-F14. Kotecha S, Silverman M. Chronic respiratory complications of prematurity. In: Taussig LM, Landau LI, ed. Pediatric Respiratory Medicine. Mosby, Inc., St. Louis, 1999, pp. 488-528. Kothadia JM, O´Shea TM, Roberts D, Auringer ST, Weaver RG, Dillard RG. Randomized placebo-controlled trial of a 42-day tapering course of dexamethasone to reduce the duration of ventilator dependency in very low birth weight infants. Pediatrics 1999;104:22-27. Kovács L, Davis GM, Faucher D, Papageorgiou A. Efficacy of sequential early systemic and inhaled corticosteroid therapy in the prevention of chronic lung disease of prematurity. Acta Paediatr 1998;87:792-798. Kraybill EN, Bose CL, D'Ercole AJ. Chronic lung disease in infants with very low birth weight. A population-based study. Am J Dis Child 1987;141:784-788. Kraybill EN, Runyan DK, Bose CL, Khan JH. Risk factors for chronic lung disease in infants with birth weights of 751 to 1000 grams. J Pediatr 1989;115:115-120. König P, Hordvik NL, Pimmel RL. Forced random noise resistance determination in childhood asthma. Chest 1984;86:884-890. Lacoste JY, Bousquet J, Chanez P, Van Vyve T, Simony-Lafontaine J, Lequeu N, Vic P, Enander I, Godard P, Michel FB. Eosinophilic and neutrophilic inflammation in asthma, chronic bronchitis, and chronic obstructive pulmonary disease. J Allergy Clin Immunol 1993;92:537-548. Lassus P, Ristimäki A, Ylikorkala O, Viinikka L, Andersson S. Vascular endothelial growth factor in human preterm lung. Am J Respir Crit Care Med 1999;159:1429-1433. Lebecque P, Spier S, Lapierre JG, Lamarre A, Zinman R, Coates AL. Histamine challenge test in children using forced oscillation to measure total respiratory resistance. Chest 1987;92:313-318. Lebecque P, Stănescu D. Respiratory resistance by the forced oscillation technique in asthmatic children and cystic fibrosis patients. Eur Respir J 1997;10:891-895. LeFlore JL, Salhab WA, Broyles RS, Engle WD. Association of antenatal and postnatal dexamethasone exposure with outcomes in extremely low birth weight neonates. Pediatrics 2002;110:275-279. Leipälä JA, Williams O, Sreekumar S, Cheeseman P, Rafferty GF, Hannam S, Milner A, Greenough A. Exhaled nitric oxide levels in infants with chronic lung disease. Eur J Pediatr 2004;163:555-558. Lemons JA, Bauer CR, Oh W, Korones SB, Papile LA, Stoll BJ, Verter J, Temprosa M, Wright LL, Ehrenkranz RA, Fanaroff AA, Stark A, Carlo W, Tyson JE, Donovan EF, Shankaran S, Stevenson DK. Very low birth weight outcomes of the National Institute of Child Health and Human Development Neonatal Research Network, January 1995 through December 1996. Pediatrics 2001;107:e1. Liggins GC. Premature delivery of foetal lambs infused with glucocorticoids. J Endocr 1969;45:515-523. Liggins GC, Howie RN. A controlled trial of antepartum glucocorticoid treatment for prevention of the respiratory distress syndrome in premature infants. Pediatrics 1972;50:515-525. Lin YJ, Yeh TF, Hsieh WS, Chi YC, Lin HC, Lin CH. Prevention of chronic lung disease in preterm infants by early postnatal dexamethasone therapy. Pediatr Pulmonol 1999;27:21-26. Lin CH, Tsai ML, Chou SJ, Yeh TF. Effect of antenatal dexamethasone on the expression of endothelial nitric oxide synthase in the lungs of postnatal pups. Semin Perinatol 2001;25:94-99. Lundberg JON, Nordvall SL, Weitzberg E, Kollberg H, Alving K. Exhaled nitric oxide in paediatric asthma and cystic fibrosis. Arch Dis Child 1996;75:323-326. MacArthur BA, Howie RN, Dezoete JA, Elkins J. School progress and cognitive development of 6-year-old children whose mothers were treated antenatally with betamethasone. Pediatrics 1982;70:99-105. Mallampalli RK, Acarregui MJ, Snyder JM. Differentiation of the alveolar epithelium in the fetal lung. In: McDonald JA, ed. Lung Growth and Development. Marcel Dekker, Inc, New York, 1997, pp. 119-162.
110
Malmberg LP, Pelkonen AS, Haahtela T, Turpeinen M. Exhaled nitric oxide rather than lung function distinguishes preschool children with probable asthma. Thorax 2003;58:494-499. Mammel MC, Green TP, Johnson DE, Thompson TR. Controlled trial of dexamethasone therapy in infants with bronchopulmonary dysplasia. Lancet 1983;8338:1356-1358. Margraf LR, Tomashefski JF Jr, Bruce MC, Dahms BB. Morphometric analysis of the lung in bronchopulmonary dysplasia. Am Rev Respir Dis 1991;143:391-400. Mariani GL, Carlo WA. Ventilatory management in neonates. Science or art? In: Goldsmith JP, Spitzer AR, ed. Clinics in Perinatology. Controversies in neonatal care. W.B. Saunders Company, Philadelphia, 1998;25:33-48. Markestad T, Fitzhardinge PM. Growth and development in children recovering from bronchopulmonary dysplasia. J Pediatr 1981;98:597-602. Marttila R. Epidemiological and genetic study of respiratory distress syndrome in preterm infants. Specific aspects of twin and multiple births. Acta Univ Oul 2003a, D 766. Oulu University Press, Oulu. Marttila R, Haataja R, Rämet M, Löfgren J, Hallman M. Surfactant protein B polymorphism and respiratory distress syndrome in premature twins. Hum Genet 2003b;112:18-23. Massaro GD, Massaro D. Retinoic acid treatment partially rescues failed septation in rats and in mice. Am J Physiol Lung Cell Mol Physiol 2000;278:L955-L960. Mathews TJ, Menacker F, MacDorman MF. Infant mortality statistics from the 2001 period linked birth/infant death data set. Natl Vital Stat Rep 2003;52:1-28. Mattes J, Storm van´s Gravesande K, Reining U, Alving K, Ihorst G, Henschen M, Kuehr J. NO in exhaled air is correlated with markers of eosinophilic airway inflammation in corticosteroid-dependent childhood asthma. Eur Respir J 1999;13:1391-1395. Matthews SG. Antenatal glucocorticoids and programming of the developing CNS. Pediatr Res 2000;47:291-300. Maziak W, Loukides S, Culpitt S, Sullivan P, Kharitonov SA, Barnes PJ. Exhaled nitric oxide in chronic obstructive pulmonary disease. Am J Respir Crit Care Med 1998;157:998-1002. McEvoy C, Bowling S, Williamson K, Collins J, Tolaymat L, Maher J. Timing of antenatal corticosteroids and neonatal pulmonary mechanics. Am J Obstet Gynecol 2000;183:895-899. McEvoy C, Bowling S, Williamson K, Lozano D, Tolaymat L, Izquierdo L, Maher J, Helfgott A. The effect of a single remote course versus weekly courses of antenatal corticosteroids on functional residual capacity in preterm infants: a randomized trial. Pediatrics 2002;110:280-284. McEvoy C, Bowling S, Williamson K, Stewart M, Durand M. Functional residual capacity and passive compliance measurements after antenatal steroid therapy in preterm infants. Pediatr Pulmonol 2001;31:425-430. McGettigan MC, Adolph VR, Ginsberg HG, Goldsmith JP. New ways to ventilate newborns in acute respiratory failure. In: Hageman JR, ed. The Pediatric Clinics of North America. Neonatology Update. W.B. Saunders Company, Philadelphia, 1998;45:475-509. Merritt TA, Cochrane CG, Holcomb K, Bohl B, Hallman M, Strayer D, Edwards DK, Gluck L. Elastase and α1-proteinase inhibitor activity in tracheal aspirates during respiratory distress syndrome. Role of inflammation in the pathogenesis of bronchopulmonary dysplasia. J Clin Invest 1983;72:656-666. Merritt TA, Hallman M. Surfactant replacement. A new era with many challenges for neonatal medicine. Am J Dis Child 1988;142:1333-1339. Merritt TA, Stuard ID, Puccia J, Wood B, Edwards DK, Finkelstein J, Shapiro DL. Newborn tracheal aspirate cytology: classification during respiratory distress syndrome and bronchopulmonary dysplasia. J Pediatr 1981;98:949-956. Morris SM, Billiar TR. New insights into the regulation of inducible nitric oxide synthesis. Am J Physiol (Endocrinol Metab) 1994;266:E829-E839. Motz R, Grassl G, Trawoger R. Dependence on a respiratory ventilator due to an atrial septal defect. Cardiol in the Young 2000;10:150-152. Mulder EJH, Derks JB, Visser GHA. Antenatal corticosteroid therapy and fetal behaviour: a randomised study of the effects of betamethasone and dexamethasone. Br J Obstet Gynaecol 1997;104:1239-1247. Murphy DJ. Effect of antenatal corticosteroids on postmortem brain weight of preterm babies. Early Hum Dev 2001;63:113-122.
111
Myers MG, McGuinness GA, Lachenbruch PA, Koontz FP, Hollingshead R, Olson DB. Respiratory illnesses in survivors of infant respiratory distress syndrome. Am Rev Respir Dis 1986;133:1011-1018. National Institutes of Health Consensus Development Statement. Effect of corticosteroids for fetal maturation on perinatal outcomes, February 28-March 2, 1994. Am J Obstet Gynecol 1995;173:246-252. Nelson BV, Sears S, Woods J, Ling CY, Hunt J, Clapper LM, Gaston B. Expired nitric oxide as a marker for childhood asthma. J Pediatr 1997;130:423-427. Ng PC. The effectiveness and side effects of dexamethasone in preterm infants with bronchopulmonary dysplasia. Arch Dis Child 1993;68:330-336. Ng PC, Wong GWK, Lam CWK, Lee CH, Fok TF, Wong MY, Ma KC. Effect of multiple courses of antenatal corticosteroids on pituitary-adrenal function in preterm infants. Arch Dis Child Fetal Neonatal Ed 1999;80:F213-F216. NIH, see National Institutes of Health. Niklasson A, Engström E, Hård AL, Albertsson Wikland K, Hellström A. Growth in very preterm children: a longitudinal study. Pediatr Res 2003;54:899-905. Nikolajev K, Korppi M, Koskela H, Remes K, Jokela V, Länsimies E, Heinonen K. Methacholine, cold air and exercise challenge tests in the diagnosis of bronchial responsiveness at school age: a follow-up study from birth to school age. Allergol Internat 2002;51:131-138. Noble-Jamieson CM, Regev R, Silverman M. Dexamethasone in neonatal chronic lung disease: pulmonary effects and intracranial complications. Eur J Pediatr 1989;148:365-367. Northway WH Jr. Observations on bronchopulmonary dysplasia. J Pediatr 1979;95:815-817. Northway WH Jr. Bronchopulmonary dysplasia: then and now. Arch Dis Child 1990a;65:1076-1081. Northway WH Jr, Moss RB, Carlisle KB, Parker BR, Popp RL, Pitlick PT, Eichler I, Lamm RL, Brown BW Jr. Late pulmonary sequelae of bronchopulmonary dysplasia. N Engl J Med 1990b;323:1793-1799. Northway WH Jr, Rosan RC, Porter DY. Pulmonary disease following respirator therapy of hyaline-membrane disease. Bronchopulmonary dysplasia. N Engl J Med 1967;276:357-368. Nupponen I, Repo H, Kari A, Pohjavuori M, Andersson S. Early dexamethasone decreases expression of activation markers on neutrophils and monocytes in preterm infants. Acta Paediatr 2002;91:1200-1207. O´Brodovich HM, Mellins RB. Bronchopulmonary dysplasia. Unresolved neonatal acute lung injury. Am Rev Respir Dis 1985;132:694-709. Ohlsson A, Calvert SA, Hosking M, Shennan AT. Randomized controlled trial of dexamethasone treatment in very-low-birth-weight infants with ventilator-dependent chronic lung disease. Acta Paediatr 1992;81:751-756. Okajima S, Matsuda T, Cho K, Matsumoto Y, Kobayashi Y, Fujimoto S. Antenatal dexamethasone administration impairs normal postnatal lung growth in rats. Pediatr Res 2001;49:777-781. Ollikainen J, Hiekkaniemi H, Korppi M, Sarkkinen H, Heinonen K. Ureaplasma urealyticum infection associated with acute respiratory insufficiency and death in premature infants. J Pediatr 1993;122:756-760. O´Shaughnessy TC, Ansari TW, Barnes NC, Jeffery PK. Inflammation in bronchial biopsies of subjects with chronic bronchitis: inverse relationship of CD8+ T lymphocytes with FEV1. Am J Respir Crit Care Med 1997;155:852-857. O´Shea TM, Kothadia JM, Klinepeter KL, Goldstein DJ, Jackson BG, Weaver RG, Dillard RG. Randomized placebo-controlled trial of a 42-day tapering course of dexamethasone to reduce the duration of ventilator dependency in very low birth weight infants: outcome of study participants at 1-year adjusted age. Pediatrics 1999;104:15-21. Palta M, Sadek M, Barnet JH, Evans M, Weinstein MR, McGuinness G, Peters ME, Gabbert D, Fryback D, Farrell P. Evaluation of criteria for chronic lung disease in surviving very low birth weight infants. J Pediatr 1998;132:57-63. Papile LA, Burstein J, Burstein R, Koffler H. Incidence and evolution of subependymal and intraventricular hemorrhage: a study of infants with birthweights less than 1,500 gm. J Pediatr 1978;92:529-534.
112
Papile LA, Tyson JE, Stoll BJ, Wright LL, Donovan EF, Bauer CR, Krause-Steinrauf H, Verter J, Korones SB, Lemons JA, Fanaroff AA, Stevenson DK, Oh W, Ehrenkranz RA, Shankaran S. A multicenter trial of two dexamethasone regimens in ventilator-dependent premature infants. N Engl J Med 1998;338:1112-1119. Parker RA, Lindstrom DP, Cotton RB. Improved survival accounts for most, but not all, of the increase in bronchopulmonary dysplasia. Pediatrics 1992;90:663-668. Parker TA, Abman SH. The pulmonary circulation in bronchopulmonary dysplasia. Semin Neonatol 2003;8:51-62. Pavord ID, Pizzichini MMM, Pizzichini E, Hargreave FE. The use of induced sputum to investigate airway inflammation. Thorax 1997;52:498-501. Pelkonen AS, Hakulinen AL, Turpeinen M. Bronchial lability and responsiveness in school children born very preterm. Am J Respir Crit Care Med 1997;156:1178-1184 Pelkonen AS, Hakulinen AL, Turpeinen M, Hallman M. Effect of neonatal surfactant therapy on lung function at school age in children born very preterm. Pediatr Pulmonol 1998;25:182-190. Pelkonen AS, Suomalainen H, Hallman M, Turpeinen M. Peripheral blood lymphocyte subpopulations in schoolchildren born very preterm. Arch Dis Child Fetal Neonatal Ed 1999;81:F0-F5. Persson MG, Zetterström O, Agrenius V, Ihre E, Gustafsson LE. Single-breath nitric oxide measurements in asthmatic patients and smokers. Lancet 1994;343:146-147. Piacentini GL, Bodini A, Costella S, Vicentini L, Mazzi P, Sperandio S, Boner AL. Exhaled nitric oxide and sputum eosinophil markers of inflammation in asthmatic children. Eur Respir J 1999;13:1386-1390. Pihkala J, Hakala T, Voutilainen P, Raivio K. Uudet suomalaiset sikiön kasvukäyrät (Characteristic of recent fetal growth curves in Finland). Duodecim 1989;105:1540-1546. Polgar G, Promadhat V. Pulmonary function testing in children: Technics and standards. WB Saunders, Philadelphia, 1971, pp. 42-212. Ratjen F, Kavuk I, Gärtig S, Wiesemann HG, Grasemann H. Airway nitric oxide in infants with acute wheezy bronchitis. Pediatr Allergy Immunol 2000;11:230-235. Rayburn WF, Christensen HD, Gonzalez CL. A placebo-controlled comparison between betamethasone and dexamethasone for fetal maturation: differences in neurobehavioral development of mice offspring. Am J Obstet Gynecol 1997;176:842-851. Remes ST, Korppi M. Asthma and atopy in schoolchildren in a defined population. Acta Paediatr 1996;85:965-970. Riede FT, Schulze E, Vogt L, Scramm D. Irreversible cardiac changes after dexamethasone treatment for bronchopulmonary dysplasia. Letter. Pediatr Cardiol 2001;22:363-364. Robinson DS, Bentley AM, Hartnell A, Kay AB, Durham SR. Activated memory T helper cells in bronchoalveolar lavage fluid from patients with atopic asthma: relation to asthma symptoms, lung function, and bronchial responsiveness. Thorax 1993;48:26-32. Romagnoli C, Zecca E, Vento G, Maggio L, Papacci P, Tortorolo G. Effect on growth of two different dexamethasone courses for preterm infants at risk of chronic lung disease. A randomized trial. Pharmacology 1999;59:266-274. Romagnoli C, Zecca E, Luciano R, Torrioli G, Tortorolo G. Controlled trial of early dexamethasone treatment for the prevention of chronic lung disease in preterm infants: a 3-year follow-up. Pediatrics 2002;109(6):e85. Rotmensch S, Liberati M, Vishne TH, Celentano C, Ben-Rafael Z, Bellati U. The effect of betamethasone and dexamethasone on fetal heart rate patterns and biophysical activities. A prospective randomized trial. Acta Obstet et Gynecol Scand 1999;78:493-500. Rova M, Haataja R, Marttila R, Ollikainen V, Tammela O, Hallman M. Data mining and multiparameter analysis of lung surfactant protein genes in bronchopulmonary dysplasia. Hum Mol Genet 2004;13:1095-1104. Salokorpi T, Sajaniemi N, Hällback H, Kari A, Rita H, von Wendt L. Randomized study of the effect of antenatal dexamethasone on growth and development of premature children at the corrected age of 2 years. Acta Paediatr 1997;86:294-298. Salokorpi T, Rajantie I, Viitala J, Rita H, von Wendt L. Does perinatal hypocarbia play a role in the pathogenesis of cerebral palsy? Acta Paediatr 1999;88:571-575.
113
Salorinne Y. Keuhkojen diffuusiokapasiteetin mittaaminen. In: Kliininen fysiologia. Sovijärvi A, Uusitalo A, Länsimies E, Vuori I, ed. Kustannus Oy Duodecim, Jyväskylä, 1994, pp. 51-56. Saugstad OD. Promoting neonatal health in the world. Prenat Neonat Med 2001;6:329-330. Schutte MF, Treffers PE, Koppe JG, Breuer W. The influence of betamethasone and orciprenaline on the incidence of respiratory distress syndrome in the newborn after preterm labour. Br J Obstet Gynaecol 1980;87:127-131. Seckl JR. Glucocorticoid programming of the fetus; adult phenotypes and molecular mechanisms. Mol Cell Endocrinol 2001;185:61-71. Shah SS, Ohlsson A, Halliday H, Shah VS. Inhaled versus systemic corticosteroids for the treatment of chronic lung disease in ventilated very low birth weight preterm infants (Cochrane Review). In: The Cochrane Library, Issue 2, 2004. Chichester, UK: John Wiley & Sons, Ltd. Cochrane Database Syst Rev 2003;(2):CD002057. Shennan AT, Dunn MS, Ohlsson A, Lennox K, Hoskins EM. Abnormal pulmonary outcomes in premature infants: prediction from oxygen requirement in the neonatal period. Pediatrics 1988;82:527-532. Sherman TS, Chen Z, Yuhanna IS, Lau KS, Margraf LR, Shaul PW. Nitric oxide synthase isoform expression in the developing lung epithelium. Am J Physiol Lung Cell Mol Physiol 1999;276:L383-L390. Shinwell ES, Karplus M, Bader D, Dollberg S, Gur I, Weintraub Z, Arnon S, Gottfreid E, Zaritsky A, Makhoul IR, Reich D, Sirota L, Berger I, Kogan A, Yurman S, Goldberg M, Kohelet D. Neonatologists are using much less dexamethasone. Arch Dis Child Fetal Neonatal Ed 2003;88:F432-F433. Shinwell ES, Karplus M, Reich D, Weintraub Z, Blazer S, Bader D, Yurman S, Dolfin T, Kogan A, Dollberg S, Arbel E, Goldberg M, Gur I, Naor N, Sirota L, Mogilner S, Zaritsky A, Barak M, Gottfried E. Early postnatal dexamethasone treatment and increased incidence of cerebral palsy. Arch Dis Child Fetal Neonatal Ed 2000;83:F177-F181. Shinwell ES, Karplus M, Zmora E, Reich D, Rothschild A, Blazer S, Bader D, Yurman S, Dolfin T, Kuint J, Milbauer B, Kohelet D, Goldberg M, Armon Y, Davidson S, Sirota L, Amitai M, Zaretsky A, Barak M, Gottfried S. Failure of early postnatal dexamethasone to prevent chronic lung disease in infants with respiratory distress syndrome. Arch Dis Child Fetal Neonatal Ed 1996;74:F33-F37. Silkoff PE, McClean PA, Slutsky AS, Furlott HG, Hoffstein E, Wakita S, Chapman KR, Szalai JP, Zamel N. Marked flow-dependence of exhaled nitric oxide using a new technique to exclude nasal nitric oxide. Am J Respir Crit Care Med 1997;155:260-267. Siltanen M, Kajosaari M, Pohjavuori, M, Savilahti E. Prematurity at birth reduces the long-term risk of atopy. J Allergy Clin Immunol 2001;107:229-234. Siltanen M, Savilahti E, Pohjavuori M, Kajosaari M. Respiratory symptoms and lung function in relation to atopy in children born very preterm. Pediatr Pulmonol 2004;37:43-49. Skelton R, Gill AB, Parsons JM. Reference ranges for cardiac dimensions and blood flow velocity in preterm infants. Heart 1998;80:281-285. Sly PD, Hayden MJ, Morgan WJ. Lung function in cooperative subjects. In: Taussig LM, Landau LI, ed. Pediatric Respiratory Medicine. Mosby, Inc., St. Louis, 1999, pp. 205-212. Smolders-de Haas H, Neuvel J, Schmand B, Treffers PE, Koppe JG, Hoeks J. Physical development and medical history of children who were treated antenatally with corticosteroids to prevent respiratory distress syndrome: a 10- to 12-year follow-up. Pediatrics 1990;86:65-70. Smyth JA, Tabachnik E, Duncan WJ, Reilly BJ, Levison H. Pulmonary function and bronchial hyperreactivity in long-term survivors of bronchopulmonary dysplasia. Pediatrics 1981;68:336-340. Soll RF. Corticosteroids for the treatment and prevention of chronic lung disease. Acta Paediatr 2003;92:886-889. Soll RF, the Vermont Oxford Network Steroid Study Group. Early postnatal dexamethasone therapy for the prevention of chronic lung disease. Abstract. Pediatr Res 1999;45:226A. Solymar L, Aronsson PH, Engström I, Bake B, Bjure J. Forced oscillation technique and maximum expiratory flows in bronchial provocation tests in children. Eur J Respir Dis 1984;65:486-495. Solymar L, Làndsér FJ, Duiverman E. Measurement of resistance with forced oscillation technique. Eur Respir J 1989;2 Suppl 4:150S-153S.

114
Sorva R, Lankinen S, Tolppanen EM, Perheentupa J. Variation of growth in height and weight of children. Acta Paediatr Scand 1990;79:498-506. Speer CP. Inflammatory mechanisms of neonatal chronic lung disease. Eur J Pediatr 1999;158 Suppl 1:S18-S22. STAKES. The National Research and Development Centre for Welfare and Health. Statistical Summary 26/2004. http://www.stakes.info/files/pdf/Tilastotiedotteet/Tt26_04.pdf Stark AR, Carlo WA, Tyson JE, Papile LA, Wright LL, Shankaran S, Donovan EF, Oh W, Bauer CR, Saha S, Poole WK, Stoll BJ. Adverse effects of early dexamethasone treatment in extremely-low-birth-weight infants. N Engl J Med 2001;344:95-101. Stevenson DK, Wright LL, Lemons JA, Oh W, Korones SB, Papile LA, Bauer CR, Stoll BJ, Tyson JE, Shankaran S, Faranoff AA, Donovan EF, Ehrenkranz RA, Verter J. Very low birth weight outcomes of the National Institute of Child Health and Human Development Neonatal Research Network, January 1993 through December 1994. Am J Obstet Gynecol 1998;179:1632-1639. Subhedar NV, Hamdan AH, Ryan SW, Shaw NJ. Pulmonary artery pressure: early predictor of chronic lung disease in preterm infants. Arch Dis Child Fetal Neonatal Ed 1998;78:F20-F24. Subhedar NV, Shaw NJ. Changes in pulmonary arterial pressure in preterm infants with chronic lung disease. Arch Dis Child Fetal Neonatal Ed 2000;82:F243-F247. Subtil D, Tiberghien P, Devos P, Therby D, Leclerc G, Vaast P, Puech F. Immediate and delayed effects of antenatal corticosteroids on fetal heart rate: a randomized trial that compares betamethasone acetate and phosphate, betamethasone phosphate, and dexamethasone. Am J Obstet Gynecol 2003;188:524-531. Tammela OKT, Koivisto ME. Fluid restriction for preventing bronchopulmonary dysplasia? Reduced fluid intake during the first weeks of life improves the outcome of low-birth-weight infants. Acta Paediatr 1992;81:207-212. Tang JR, Markham NE, Lin YJ, McMurtry IF, Maxey A, Kinsella JP, Abman SH. Inhaled nitric oxide attenuates pulmonary hypertension and improves lung growth in infant rats after neonatal treatment with a VEGF receptor inhibitor. Am J Physiol Lung Cell Mol Physiol 2004;287:L344-L351. Tepper RS, Morgan WJ, Cota K, Taussig LM. Expiratory flow limitation in infants with bronchopulmonary dysplasia. J Pediatr 1986;109:1040-1046. Timonen KL, Randell JT, Salonen RO, Pekkanen J. Short-term variations in oscillatory and spirometric lung function indices among school children. Eur Respir J 1997;10:82-87. Tin W. Optimal oxygen saturation for preterm babies. Biol Neonate 2004;85:319-325. Tommiska V. Extremely low birthweight infants in Finland. Early outcome, costs of care, and parenteral distress with infants of birth weight below 1000 grams. Academic dissertation, University of Helsinki. Yliopistopaino, Helsinki, 2003. Tommiska V, Heinonen K, Ikonen S, Kero P, Pokela ML, Renlund M, Virtanen M, Fellman V. A national short-term follow-up of extremely low birth weight infants born in Finland in 1996-1997. Pediatrics 2001;107(1):e2. Tooley WH. Epidemiology of bronchopulmonary dysplasia. J Pediatr 1979;95:851-855. Truffert P, Empana JP, Bréart G, Saugstad OD, Goelz R, Halliday HL, Anceschi M. Treatment strategies for bronchopulmonary dysplasia with postnatal corticosteroids in Europe: the EURAIL survey. Acta Paediatr 2003;92:948-951. Tschanz SA, Damke BM, Burri PH. Influence of postnatally administered glucocorticoids on rat lung growth. Biol Neonate 1995;68:229-245. Tschanz SA, Makanya AN, Haenni B, Burri PH. Effects of neonatal high-dose short-term glucocorticoid treatment on the lung: a morphologic and morphometric study in the rat. Pediatr Res 2003;53:72-80. Tyson JE, Wright LL, Oh W, Kennedy KA, Mele L, Ehrenkranz RA, Stoll BJ, Lemons JA, Stevenson DK, Bauer CR, Korones SB, Fanaroff AA. Vitamin A supplementation for extremely-low-birth-weight infants. N Engl J Med 1999;340:1962-1968. Van Marter LJ, Allred EN, Leviton A, Pagano M, Parad R, Moore M, The Neonatology Committee for the Developmental Epidemiology Network. Antenatal glucocorticoid treatment does not reduce chronic lung disease among surviving preterm infants. J Pediatr 2001;138:198-204.
115
Van Marter LJ, Allred EN, Pagano M, Sanocka U, Parad R, Moore M, Susser M, Paneth N, Leviton A, The Neonatology Committee for the Developmental Epidemiology Network. Do clinical markers of barotrauma and oxygen toxicity explain interhospital variation in rates of chronic lung disease? Pediatrics 2000;105:1194-1201. Venge P. Soluble markers of allergic inflammation. Allergy 1994;49:1-8. The Vermont Oxford Network Steroid Study Group. Early postnatal dexamethasone therapy for the prevention of chronic lung disease. Pediatrics 2001;108:741-748. Vogel J, Smidt U. Impulse oscillometry. Pmi Verlagsgruppe GmbH, Frankfurt am Main, 1994, pp. 1-176. Vohr BR, Coll CG, Lobato D, Yunis KA, O´Dea C, Oh W. Neurodevelopmental and medical status of low-birthweight survivors of bronchopulmonary dysplasia at 10 to 12 years of age. Dev Med Child Neurol 1991;33:690-697. Vyas JR, Currie AE, Shuker DEG, Field DJ, Kotecha S. Concentration of nitric oxide products in bronchoalveolar fluid obtained from infants who develop chronic lung disease of prematurity. Arch Dis Child Fetal Neonatal Ed 1999;81:F217-F220. Vyas J, Kotecha S. Effects of antenatal and postnatal corticosteroids on the preterm lung. Arch Dis Child Fetal Neonatal Ed 1997;77:F147-F150. Wang JY, Yeh TF, Lin YJ, Chen WY, Lin CH. Early postnatal dexamethasone therapy may lessen lung inflammation in premature infants with respiratory distress syndrome on mechanical ventilation. Pediatr Pulmonol 1997;23:193-197. Wang JY, Yeh TF, Lin YC, Miyamura K, Holmskov U, Reid KBM. Measurement of pulmonary status and surfactant protein levels during dexamethasone treatment of neonatal respiratory distress syndrome. Thorax 1996;51:907-913. Watterberg KL, Demers LM, Scott SM, Murphy S. Chorioamnionitis and early lung inflammation in infants in whom bronchopulmonary dysplasia develops. Pediatrics 1996;97:210-215. Watterberg KL, Gerdes JS, Gifford KL, Lin HM. Prophylaxis against early adrenal insufficiency to prevent chronic lung disease in premature infants. Pediatrics 1999;104:1258-1263. Watterberg KL, Scott SM. Evidence of early adrenal insufficiency in babies who develop bronchopulmonary dysplasia. Pediatrics 1995;95:120-125. Werner JC, Sicard RE, Hansen TWR, Solomon E, Cowett RM, Oh W. Hypertrophic cardiomyopathy associated with dexamethasone therapy for bronchopulmonary dysplasia. J Pediatr 1992;120:286-291. Whitelaw A, Thoresen M. Antenatal steroids and the developing brain. Arch Dis Child Fetal Neonatal Ed 2000;83:F154-157. Wiebicke W, Poynter A, Chernick V. Normal lung growth following antenatal dexamethasone treatment for respiratory distress syndrome. Pediatr Pulmonol 1988;5:27-30. Williams O, Bhat RY, Cheeseman P, Rafferty GF, Hannam S, Greenough A. Exhaled nitric oxide in chronically ventilated preterm infants. Arch Dis Child Fetal Neonatal Ed 2004;89:F88-F89. Wright LL, Horbar JD, Gunkel H, Verter J, Younes N, Andrews EB, Long W. Evidence from multicenter networks on the current use and effectiveness of antenatal corticosteroids in low birth weight infants. Am J Obstet Gynecol 1995;173:263-268. Wong YC, Beardsmore CS, Silverman M. Pulmonary sequelae of neonatal respiratory distress in very low birthweight infants: a clinical and physiological study. Arch Dis Child 1982a;57:418-424. Wong YC, Beardsmore CS, Silverman M. Antenatal dexamethasone and subsequent lung growth. Arch Dis Child 1982b;57:536-538. Yates DH, Kharitonov SA, Robbins RA, Thomas PS, Barnes PJ. Effect of a nitric oxide synthase inhibitor and a glucocorticosteroid on exhaled nitric oxide. Am J Respir Crit Care Med 1995;152:892-896. Yeh TF, Lin YJ, Hsieh WS, Lin HC, Lin CH, Chen JY, Kao HA, Chien CH. Early postnatal dexamethasone therapy for the prevention of chronic lung disease in preterm infants with respiratory distress syndrome: a multicenter clinical trial. Pediatrics 1997;100(4):e3. Yeh TF, Lin YJ, Huang CC, Chen YJ, Lin CH, Lin HC, Hsieh WS, Lien YJ. Early dexamethasone therapy in preterm infants: a follow-up study. Pediatrics 1998;101(5):e7. Yeh TF, Lin YJ, Lin HC, Huang CC, Hsieh WS, Lin CH, Tsai CH. Outcomes at school age after postnatal dexamethasone therapy for lung disease of prematurity. N Engl J Med 2004;350:1304-1313.

116
Yeh TF, Torre JA, Rastogi A, Aneybuno MA, Pildes RS. Early postnatal dexamethasone therapy in premature infants with severe respiratory distress syndrome: a double-blind, controlled study. J Pediatr 1990:117:273-282. Yoder MC Jr, Chua R, Tepper R. Effect of dexamethasone on pulmonary inflammation and pulmonary function of ventilator-dependent infants with bronchopulmonary dysplasia. Am Rev Respir Dis 1991;143:1044-1048. Yu VYH, Orgil AA, Lim SB, Bajuk B, Astbury J. Growth and development of very low birthweight infants recovering from bronchopulmonary dysplasia. Arch Dis Child 1983;58:791-794. Yuksel B, Greenough A. Relationship of symptoms to lung function abnormalities in preterm infants at follow up. Pediatr Pulmonol 1991;11:202-206. Yuksel B, Greenough A. Persistence of respiratory symptoms into the second year of life: predictive factors in infants born preterm. Acta Paediatr 1992;81:832-835. Zecca E, Papacci P, Maggio L, Gallini F, Elia S, De Rosa G, Romagnoli C. Cardiac adverse effects of early dexamethasone treatment in preterm infants: a randomized clinical trial. J Clin Pharmacol 2001;41:1075-1081.





























