Embed Size (px)
Citation preview
1
Department of Obstetrics and Gynaecology,
Helsinki University Central Hospital,
University of Helsinki, Finland
UNEXPLAINED INFERTILITYStudies on aetiology, treatment options and obstetric outcome
RITA ISAKSSON
ACADEMIC DISSERTATION
To be presented by permission of the Medical Faculty of the University of Helsinki for
public criticism in the Auditorium of the Department of Obstetrics and Gynaecology,
Helsinki University Central Hospital, Haartmaninkatu 2, Helsinki,
on October 18th, 2002, at 12 noon.
Helsinki 2002
2
Supervised by
Docent Aila Tiitinen, M.D., Ph.D.
Department of Obstetrics and Gynaecology
Helsinki University Central Hospital
Docent Bruno Cacciatore, M.D., Ph.D.
Department of Obstetrics and Gynaecology
Helsinki University Central Hospital
Reviewed by
Docent Anne-Maria Suikkari, M.D., Ph.D.
The Family Federation of Finland,
Infertility Clinic, Helsinki
Docent Aydin Tekay, M.D., Ph.D.
Department of Obstetrics and Gynaecology
Oulu University Central Hospital
Offi cial opponent
Docent Hannu Martikainen, M.D., Ph.D.
Department of Obstetrics and Gynaecology
Oulu University Central Hospital
ISBN 952-91-5071-7 (print)
ISBN 952-10-0712-5 (PDF)
Yliopistopaino
Helsinki 2002
3
To my family

CONTENTS
LIST OF ORIGINAL PUBLICATIONS ....................................................................7
ABBREVIATIONS .................................................................................................. 8
ABSTRACT ............................................................................................................. 9
I INTRODUCTION .............................................................................................. 11
II REVIEW OF THE LITERATURE
1. Infertility ................................................................................................. 12
2. Unexplained infertility ............................................................................ 13
2.1. Defi nition and incidence ............................................................ 13
2.2. Speculations on possible underlying causes ...............................14
2.3. Treatment options ...................................................................... 17
3. Ultrasound examination .......................................................................... 20
3.1. Basic ........................................................................................... 20
3.2. Doppler ultrasound .................................................................... 21
3.3. Doppler ultrasound during natural and IVF cycles .................... 22
4. Assisted reproductive technology ........................................................... 28
4.1. Defi nition and rate of success .................................................... 28
4.2. Prognostic markers for successful outcome .............................. 31
4.3. Pregnancy outcome of ART-induced pregnancies ...................... 35
III AIMS OF THE STUDY ................................................................................... 41
IV PATIENTS AND METHODS ........................................................................... 42
1. Study populations and protocols ............................................................ 42
Study I ............................................................................................... 43
Study II ...............................................................................................43
Studies III and IV ............................................................................... 44
Study V .............................................................................................. 44
2. Hormonal assays ...................................................................................... 47
3. Ultrasound and Doppler assessment ....................................................... 47
4. Statistical analysis .................................................................................... 48
V RESULTS .......................................................................................................... 49
1. Uterine and spiral artery blood fl ow in unexplained infertility .............. 49
2. Prognostic signifi cance of uterine artery impedance ............................. 50
3. Comparison of ovulation induction combined with intra-uterine
......... 50 insemination, intraperitoneal insemination and timed intercourse
4. Course of ART-induced and spontaneous pregnancies ........................... 52
VI DISCUSSION .................................................................................................. 55
1. Uterine and spiral artery impedance among women with
55
unexplained infertility
2. Prediction of pregnancy outcome with uterine artery
57 impedance measurement
3. Treatment options of women with unexplained infertility ..................... 58
4. Long-term prognosis of couples with unexplained infertility ................. 59
5. Obstetric outcome of couples with unexplained infertility ................... 60
VII SUMMARY AND CONCLUSIONS ................................................................ 62
ACKNOWLEDGEMENTS .................................................................................... 63
REFERENCES ...................................................................................................... 65
......................................................................
............................................................................

7
LIST OF ORIGINAL PUBLICATIONS
I. Isaksson R, Tiitinen A, Reinikainen L and Cacciatore B. Comparison of the
uterine and spiral artery blood fl ow in women with unexplained and tubal
infertility.
II. Isaksson R, Tiitinen A and Cacciatore B. Uterine artery impedance to blood
fl ow on the day of embryo transfer does not predict obstetric outcome.
Ultrasound Obstet Gynecol 2000; 15: 527-530.
III. Isaksson R and Tiitinen A. Superovulation combined with insemination or
intercourse in the treatment of couples with unexplained infertility and
minimal endometriosis.
Acta Obstet Gynecol Scand 1997; 76: 550-554.
IV. Isaksson R and Tiitinen A. Obstetric outcome in patients with unexplained
infertility: Comparison of treatment-related and spontaneous pregnancies.
Acta Obstet Gynecol Scand 1998; 77: 849-853.
V. Isaksson R, Gissler M and Tiitinen A. Obstetric outcome among women with
unexplained infertility after IVF: a matched case-control study.
Hum Reprod 2002; 17: 1755-1761.
The orginal Publications are reproduced with permission of the copyright holders.
Ultrasound Obstet Gynecol, in press.
8
ABBREVIATIONS
ART assisted reproductive technology
CC clomiphene citrate
COH controlled ovarian hyperstimulation
CV coeffi cient of variation
DIPI direct intraperitoneal insemination
ET embryo transfer
FSH follicle-stimulating hormone
GIFT gamete intra-fallopian transfer
GnRHa gonadotrophin-releasing hormone agonist
hCG human chorionic gonadotrophin
hMG human menopausal gonadotrophin
HSG hysterosalpingography
HSSG hysterosalpingosonography
ICD international classifi cation of diseases
ICSI intracytoplasmic sperm injection
im intramuscular
IU international unit
IUI intra-uterine insemination
IUGR intra-uterine growth retardation
IVF in-vitro fertilization
LH luteinizing hormone
Mhz megahertz
MBR Medical Birth Register
OPU ovum pick-up
PIH pregnancy-induced hypertension
PI pulsatility index
PSV peak systolic velocity
RI resistance index
sc subcutaneous
SE standard error of mean
SD standard deviation
SGA small for gestational age
SPSS statistical package for social sciences
TI timed intercourse
US ultrasound
WHO World Health Organization
ZIFT zygote intra-fallopian transfer
9
ABSTRACT
Unexplained infertility, refering to the failure to conceive of a couple in whom
no defi nitive cause for infertility can be found, has an incidence of 10-20% in
all infertile couples. The purpose of this study was to examine the impedance
to uterine blood fl ow, different treatments and obstetric outcome in unexplained
infertility.
Main uterine and spiral artery impedance to blood fl ow was compared in 20
women with unexplained and 18 women with tubal infertility. Measurements were
taken both during the natural cycle (on days 11-12, 16-17 and 21-23) and during
the in-vitro fertilization (IVF) treatment cycle (on days 1, 5, 10, ovum pick-up
and embryo transfer). The mean uterine artery impedance was below three in
women with unexplained infertility during the natural and IVF cycles, and no
signifi cant differences were observed between the groups. The mean impedance
(± SD) in spiral arteareries was lower (pulsatility index 0.96 ± 0.25) in women
with unexplained infertility on day 5 of gonadotrophin stimulation compared with
women with tubal infertility (pulsatility index 1.24 ± 0.30; p<0.05).
The main uterine artery impedance to blood fl ow was studied among 102
women during 111 conceptional IVF cycles. The aetiology of infertility was
either unexplained, tubal, endometriosis or multifactorial. Predicting obstetric
complications with measurement of uterine artery impedance among these women
was not possible. The mean uterine artery pulsatility index (PI) was comparable in
pregnancies leading to spontaneous abortion (PI 2.71 ± 0.67), ectopic pregnancy
(PI 2.36 ± 0.54) and normal intra-uterine pregnancy (PI 2.69 ± 0.71).
Seventy women with unexplained infertility were treated with ovulation induction
combined with intra-uterine insemination, direct intraperitoneal insemination and
timed intercourse, and these treatments were equally effective.
The same seventy women were followed for six years after completed ovulation
induction treatment. In all, 64% of these couples conceived during the follow-up,
with the majority (60%) of pregnancies beginning spontaneously. In spontaneous
pregnancies, both the mean birthweight (3387 g vs. 3120 g) and the relative
birthweight were signifi cantly higher than in treatment pregnancies.
10
One hundred and seven women with unexplained infertility who conceived
with in-vitro fertilization treatment were studied. Two control groups (n=445
and n=2377) were chosen from the Finnish Medical Birth Register. The rate of
spontaneous abortion was 24% and the multiple pregnancy rate was 23%, including
one triplet pregnancy. No difference was found in mean birthweight, incidence
of low birthweight, gestational duration, umbilical artery pH and rate of major
congenital malformations in women with unexplained infertility as compared
with normally conceived or IVF pregnancies. The rate of pregnancy-induced
hypertension was signifi cantly lower among singletons in the study group compared
with other IVF singletons.
No difference was observed in uterine artery impedance when women with
unexplained infertility and women with tubal infertility were compared. Predicting
pregnancy outcome with measurement of uterine artery impedance during IVF
treatment was not possible. Ovulation induction was an effective treatment for
women with unexplained infertility. Obstetric outcome among women with
unexplained infertility was good, being similar to that of spontaneous pregnancies
and IVF pregnancies.
11
I INTRODUCTION
Infertility, defi ned as failure to conceive within one year despite normal cohabitation
(Zabrek 1996; Barbieri 1996) or within two years according to the European Society
for Human Reproduction and Embryology (Forti and Krausz 1998), presents in
10-15% of all couples. Typically, 80% of couples (aged 18-28 years) will conceive
over a one-year period and another 10% conceive during the following year. The
rate of infertility has slowly been increasing (Stephen and Chandra 1998; Silverberg
2000).
While many of these couples will conceive with assisted reproductive technology
(ART), about 20% will never conceive. The fi rst artifi cial insemination was reported
in 1799 in the United Kingdom. In-vitro fertilization (IVF) was developed more than
one century later, and the fi rst IVF baby was born in 1978 in the United Kingdom
(Steptoe and Edwards 1978). In Finland, the fi rst IVF baby was born in 1984 at the
Helsinki University Central Hospital (Koskimies et al. 1984). ART has subsequently
become an effective and widely used therapy for childless couples (Wikland et al.
1985). Approximately 7200 embryo transfers are performed in Finland each year,
and more than 10 000 IVF babies have been born since 1984 (Nygren and Nybo
Andersen 2001). Of all newborn babies, about 2.6% are born as the result of IVF
treatment compared with 1.3% in other European countries. More than half of all
IVF cycles world-wide are provided in Europe, mostly in France, United Kingdom
and Germany (Nygren and Nybo Andersen 2001). During IVF treatment trans-
vaginal ultrasound is an essential tool for monitoring follicular growth and
performing ovum pick-up. Since the mid-1980s, when transvaginal ultrasound
gained popularity among gynaecologists, its image quality and diagnostic accuracy
in infertility and many other gynaecological conditions have improved dramatically.
The Colour Doppler method has enabled non-invasive evaluation of pelvic and
foetal blood fl ow, which is useful in different pathological conditions.
IVF has revolutionalized the treatment of infertile couples, as well as profoundly
increasing the basic understanding of human reproduction. Treatment options and
results today are promising in most subgroups of infertility, including unexplained
infertility, where IVF is used both as a diagnostic and therapeutic tool.

12
II REVIEW OF THE LITERATURE
1. INFERTILITY
The incidence of infertility is approximately 10-15% (Lilford and Dalton 1987;
Templeton et al. 1991; Crosignani et al. 1996). Primary infertility refers to the
condition of an infertile woman who has never conceived, and secondary infertility
to one who has had a previous pregnancy. At present, almost 80% of infertile
couples can be helped to have a child. The incidence of voluntary infertility is very
low, approximately below 3% (Templeton et al. 1991).
Reasons for the increasing incidence of infertility include postponement of
childbearing, increased pelvic infections and, in some countries, deteriorating
sperm quality (Unkila-Kallio 2001). The reasons for infertility are related to female
factors, male factors, to a combination of the two or to unknown causes, each
comprising 25%. The most frequent causes for infertility are ovulatory disorder or
anovulation, tubal factor, abnormal semen parameters, endometriosis and uterine or
cervical factor (Table 1; Jaffe and Jewelewicz 1991; Collins et al. 1995). Less common
causes for infertility are immunological factors and genetic defects. Smoking also
decreases the ability to conceive (Stillman et al. 1986; Mueller and Daling 1989).
Infertility in many couples has multiple aetiologies; however, in approximately
15-17% of couples, no reason for infertility is found and the infertility is defi ned as
unexplained (Templeton and Penney 1982; Collins et al. 1995; Aboulghar et al. 2001).
Table 1. Most frequent causes of infertility (Jaffe and Jewelewicz 1991; Collins et al. 1995).
_______________________________________________
Cause of infertility %_______________________________________________
Ovulatory disorder or anovulation 27-30
Tubal factor 20-22
Abnormal semen parameter 25-40
Unexplained 15
Endometriosis 5
Uterine or cervical factor 4-5_______________________________________________

13
2. UNEXPLAINED INFERTILITY
2.1. Defi nition and incidence
Unexplained infertility, sometimes also called idiopathic infertility, refers to failure
to conceive in a couple for whom no defi nitive cause for infertility can be found.
Usually, the duration of infertility is more than two years (Jaffe and Jewelewicz
1991; Crosignani et al. 1993; Aboulghar et al. 2001). The incidence of unexplained
infertility varies in different studies but is usually 10-20% (Templeton and Penney
1982; Crosignani et al. 1993; Guzick et al. 1994, 1998; Lessey et al. 1995; Miller et al.
1999). Incidence depends on the selection and age of the study population and,
to some extent, on infertility evaluations. Unexplained infertility is not an absolute
condition but a relative inability to conceive, and while many of these couples may
conceive without treatment, treatment will often hasten conception (Fish et al.
1989).
The diagnosis is possible only after a complete infertility evaluation, including
a physical examination of both partners, has been performed (Templeton and
Penney 1982; Jaffe and Jewelewicz 1991). The basic infertility work-up includes
demonstration of 1) ovulation and normal luteal phase, 2) patent fallopian tubes and
3) normal fi ndings in semen analysis according to the World Health Organization
(WHO; Guzick et al. 1994; Forti and Krausz 1998). However, the recommended basic
infertility evaluation varies among different practitioners and no consensus exists
on which investigations are the most appropriate (Forti and Krausz 1998; Kelly et
al. 2001).
Ovulation is indicated by the existence of a regular menstrual cycle (26-32 days,
with the cycle length varying no more than 4 days from cycle to cycle), an ovulatory
progesterone rise at midcycle and a luteal phase of ≥12 days (Jaffe and Jewelewicz
1991). Different cut-off values indicative of ovulation are progesterone levels >16
nmol/l (Crosignani et al. 1993), >18 nmol/l at two assays (Forti and Krausz 1998) or
>25 nmol/l in midluteal phase (Miller et al. 1999).
Tubal patency is determined by ultrasound-assisted hysterosalpingosonography
(HSSG), hysterosalpingography (HSG) or, if necessary, laparoscopy and
chromopertubation (Heikkinen et al. 1995; Forti and Krausz 1998). The agreement
of HSSG with HSG is 84-94% (Spalding et al. 1998, 1999). When comparing HSSG
14
with laparoscopy in evaluation of tubal patency, results are consistent in 76-93%
of women (Allahbadia 1992, Stern et al. 1992; Spalding et al. 1997). There is also a
75% correlation with fi ndings in HSG and laparoscopy (Jaffe and Jewelewicz 1991).
Laparoscopy is indicated if the woman has suffered from pelvic infl ammatory
disease (PID), if endometriosis is suspected in cases of dysmenorrea or dyspareunia,
or if the woman has previously undergone many abdominal operations such as
complicated appendicectomy (Forti and Krausz 1998). Assessment of tubal patency
is unnecessary if IVF or intracytoplasmic sperm injection (ICSI) is indicated, as in
cases of severe male infertility (Forti and Krausz 1998).
Based on the WHO criteria for normality, a sperm concentration of ≥ 20 million/ml,
motility of ≥ 50% and normal morphology of ≥ 15% are required (World Health
Organization 1999).
The post-coital test (PCT) has been used to study the sperm-cervical mucus
interaction, but the predictive value of PCT is poor because of diffi culty in timing
the test. The test has mostly been abandoned due to poor standardization of the
technique and differences in interpretation of results (Glatstein et al. 1995; Forti and
Krausz 1998).
2.2. Speculations on possible underlying causes
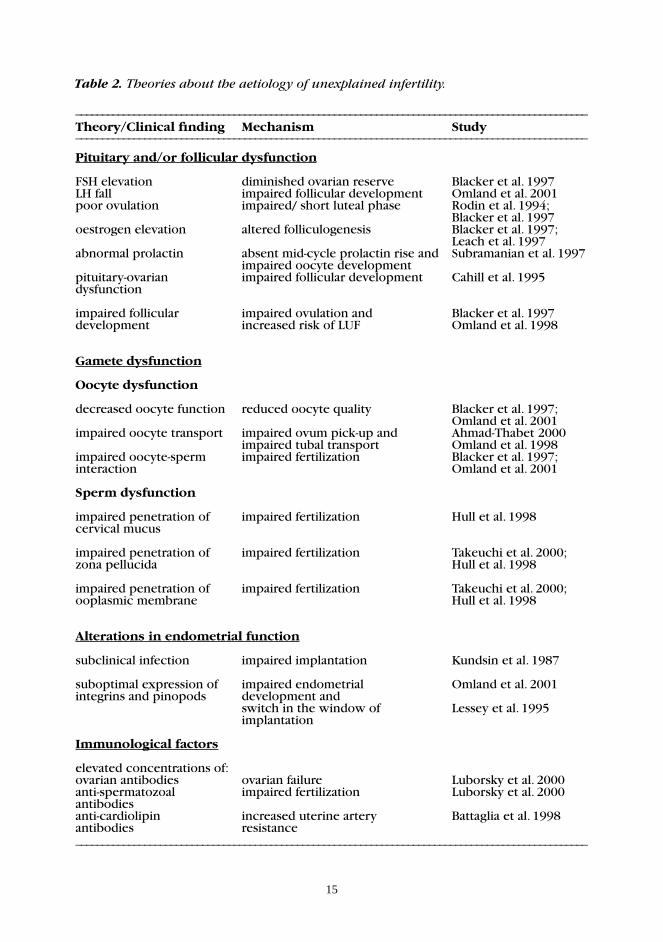
Several theories have been tendered on the aetiology of unexplained infertility
(Table 2). Diminished ovarian reserve, as shown by elevated serum follicle-stimulating
hormone (FSH) level, may be one cause (Cahill et al. 1995; Blacker et al. 1997;
Luborsky et al. 2000) and can result in alterations to other hormonal levels. One
study revealed that 5% of women with unexplained infertility had elevated FSH
levels in the early follicular phase (Rodin et al. 1994). Changes in LH levels,
a low FSH/LH ratio and reduced LH concentration in follicular fl uid have also been
speculated to play a role in unexplained infertility (Cahill et al. 1995; Omland et al.
2001). FSH and LH abnormalities may refl ect a dysfunction on the pituitary-ovarian
axis (Leach et al. 1997; Omland et al. 2001). Both the serum estradiol levels in
follicular phase and the E2/P ratio have been shown to be elevated in women with
unexplained infertility, suggesting altered folliculogenesis (Blacker et al. 1997; Leach
et al. 1997) and an absent midcycle elevation of the hormone prolactin, which is
present in fertile women (Subramanian et al. 1997).
15
Table 2. Theories about the aetiology of unexplained infertility.
_________________________________________________________________________________________________Theory/Clinical fi nding Mechanism Study_________________________________________________________________________________________________
Pituitary and/or follicular dysfunction
FSH elevation diminished ovarian reserve Blacker et al. 1997LH fall impaired follicular development Omland et al. 2001poor ovulation impaired/ short luteal phase Rodin et al. 1994; Blacker et al. 1997oestrogen elevation altered folliculogenesis Blacker et al. 1997; Leach et al. 1997abnormal prolactin absent mid-cycle prolactin rise and Subramanian et al. 1997 impaired oocyte developmentpituitary-ovarian impaired follicular development Cahill et al. 1995dysfunction
impaired follicular impaired ovulation and Blacker et al. 1997development increased risk of LUF Omland et al. 1998
Gamete dysfunction
Oocyte dysfunction
decreased oocyte function reduced oocyte quality Blacker et al. 1997; Omland et al. 2001impaired oocyte transport impaired ovum pick-up and Ahmad-Thabet 2000 impaired tubal transport Omland et al. 1998impaired oocyte-sperm impaired fertilization Blacker et al. 1997;interaction Omland et al. 2001 Sperm dysfunction
impaired penetration of impaired fertilization Hull et al. 1998cervical mucus
impaired penetration of impaired fertilization Takeuchi et al. 2000;zona pellucida Hull et al. 1998 impaired penetration of impaired fertilization Takeuchi et al. 2000;ooplasmic membrane Hull et al. 1998
Alterations in endometrial function
subclinical infection impaired implantation Kundsin et al. 1987 suboptimal expression of impaired endometrial Omland et al. 2001integrins and pinopods development and switch in the window of Lessey et al. 1995 implantation
Immunological factors
elevated concentrations of:ovarian antibodies ovarian failure Luborsky et al. 2000anti-spermatozoal impaired fertilization Luborsky et al. 2000antibodiesanti-cardiolipin increased uterine artery Battaglia et al. 1998antibodies resistance_________________________________________________________________________________________________

16
Another possible explanation is an impaired luteal phase, with a shorter luteal
phase or a decreased peak serum progesterone level (Li et al. 1990; Guzic et
al. 1994; Blacker et al. 1997; Leach et al. 1997). Impaired luteal phase has been
demonstrated in about 30% of women with unexplained infertility. Among women
aged 40-45 years, the rate of impaired luteal phase is higher than among women
aged 20-29, as is also the incidence of unexplained infertility (Rodin et al. 1994;
Miller et al. 1999). Both increased and decreased follicular LH-pulse frequency and a
lower FSH/LH ratio or decreased midfollicular FSH have been postulated to induce
impaired luteal phase, which may primarily be due to a functional imbalance in the
hypothalamus (Nakajima and Gibson 1991).
Besides hormonal factors, gamete dysfunction may contribute to unexplained
infertility. Altered folliculogenesis, impaired oocyte maturation, reduced oocyte
quality and defects in gamete interaction have all been suggested (Gabrielsen et al.
1996; Blacker et al. 1997; Omland et al. 2001). A sperm dysfunction would impair
the ability of spermatozoa to penetrate the cervical mucus, the zona pellucida and
the ooplasmic membrane (Hull et al. 1998; Takeuchi et al. 2000). An insuffi cient
acrosome reaction could cause a fertilization failure, which is sometimes seen in IVF
(Esterhuizen et al. 2001). In addition, genetic defects may affect success rates of IVF
among women with unexplained infertility. Total failure of fertilization is reported
in 5-30% of the cycles in conventional IVF among these women, which is more
frequent than among other subgroups (Gürgan et al. 1995; Ruiz et al. 1997;
Takeuchi et al. 2000). One theory suggests that a failure in the natural ovum pick-
up mechanism by the fallopian tube may occur in these women, although this is
diffi cult to verify (Ahmad-Thabet 2000).
Altered endometrial function may be another cause of unexplained infertility
(Kleintzeris 1997). A subacute infl ammation may be present as differences have
been observed between fertile and infertile women in endometrial leucocyte
populations (Kundsin et al. 1987; Viniker 1999). Low endometrial progesterone
receptor concentrations, inadequate estrogenic induction of progesterone receptors,
decreased inhibin levels (Nakajima and Gibson 1991) and suboptimal expression
of integrins or pinopode formation in the endometrium have also been reported
in women with unexplained infertility (Kleintzeris 1997; Garcia-Velasco and Arici
1999; Nikas et al. 1999; Omland et al. 2001).
17
Ovarian antibodies are frequent (33%) in some reports among women with
unexplained infertility (Geva et al. 1997; Luborsky et al. 1999, 2000), as are
elevated antispermatozoal (Luborsky et al. 2000; Szczepanska et al. 2001) and
anticardiolipin antibodies; the antibody levels have been shown to correlate
with uterine artery resistance (Battaglia et al. 1998). Moreover, an inadequate
maternal immunosuppression, which might cause embryo rejection in women with
unexplained infertility, has been suspected (Kleintzeris 1997). The prevalence of
coelic disease is also higher among women with unexplained infertility compared
with both the general population and other infertile women (Meloni et al. 1999),
which may be due to the elevated antibody levels found in their tissues.
Unexplained infertility may also be functionally linked to endometriosis since many
women with unexplained infertility later develop endometriosis (Cahill et al. 1995;
Guzick et al. 1998; Hull et al. 1998). Furthermore, occupational exposure to noise,
chemicals, radiation, mercury and cadmium may be linked to unexplained infertility
(Mueller and Daling 1989). Women’s anxiety and stress levels may also lower the
chances of conception (Sarell et al. 1985).
Abnormal uterine artery blood fl ow might be associated with unexplained infertility
(Goswamy et al. 1988; Kupesic and Kurjak 1993; Steer et al. 1994). Increased uterine
artery impedance in midluteal phase or an abnormal fl ow in spiral arteries would
impair the implantation process, and have been suggested as possible mechanisms
for infertility (Kupesic and Kurjak 1993; Steer et al. 1994).
2.3. Treatment options
Different treatment options in unexplained infertility include: a) expectant
management, b) clomiphene citrate (CC), or c) gonadotrophins used for ovulation
induction, d) intra-uterine insemination (IUI), e) ovulation induction with CC or
gonadotrophins combined with IUI or direct intraperitoneal insemination (DIPI)
and f) in-vitro fertilization and its modifi cations.
18
Expectant management
Couples with unexplained infertility have a chance of spontaneous conception.
With expectant management, the pregnancy rate per cycle is estimated to be
0.9-4.1% (Collins et al. 1995; Guzick et al. 1998; Donderwinkel et al. 2000; Goverde
et al. 2000). Observation can be offered if the woman is under 28-30 years and the
infertility duration is less than 2-3 years (Crosignani et al. 1993; Forti and Krausz
1998). About 14-20% of all couples with unexplained infertility will conceive
without treatment within one year and 25-30% within two years (Eimers et al. 1994;
Collins et al. 1995). The cumulative three-year pregnancy rate without treatment is
30-80% (Hull et al 1985; Guzick et al. 1998) and the fi ve-year cumulative pregnancy
rate is 80% (Randolph 2000). Moreover, a life table analysis showed that as many
as 64% of primary and 79% of secondary unexplained infertility patients conceived
within nine years (Jaffe and Jewelewicz 1991).
Ovulation induction with clomiphene citrate
Clomiphene citrate is usually used for ovulation induction. CC has been shown to
increase pregnancy rate from 1-2% to 5% per cycle in women with unexplained
infertility (Hughes et al. 2001).
Ovulation induction with gonadotrophins
When gonadotrophins are used, a low starting dose (50-75 IU) for ovulation
induction is usually recommended (Goverde et al. 2000), and the dose is adjusted
according to ovarian response (Salha and Balen 2000). The ovarian response
and follicular count and size are monitored with serial ultrasound and serum E2
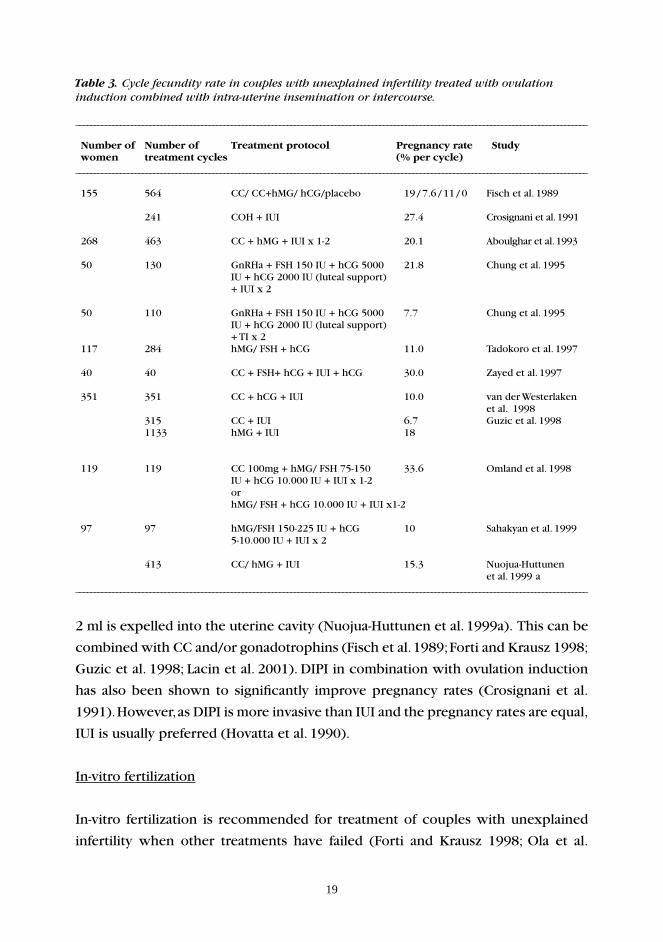
measurements (Nachtigall and Schwartz 1996; Sahakyan et al. 1999). Treatment
results of ovulation induction are shown in Table 3.
Intra-uterine insemination
Intra-uterine insemination in the spontaneous cycle is an alternative fi rst choice
of treatment of women with unexplained infertility (Goverde et al. 2000). After
standard swim-up or Percoll gradient preparation of the semen, a catheter is passed
through the cervical canal and the washed sperm suspension at volumes of 0.5-
19
2 ml is expelled into the uterine cavity (Nuojua-Huttunen et al. 1999a). This can be
combined with CC and/or gonadotrophins (Fisch et al. 1989; Forti and Krausz 1998;
Guzic et al. 1998; Lacin et al. 2001). DIPI in combination with ovulation induction
has also been shown to signifi cantly improve pregnancy rates (Crosignani et al.
1991). However, as DIPI is more invasive than IUI and the pregnancy rates are equal,
IUI is usually preferred (Hovatta et al. 1990).
In-vitro fertilization
In-vitro fertilization is recommended for treatment of couples with unexplained
infertility when other treatments have failed (Forti and Krausz 1998; Ola et al.
Table 3. Cycle fecundity rate in couples with unexplained infertility treated with ovulation induction combined with intra-uterine insemination or intercourse.
__________________________________________________________________________________________________________________________________________
Number of Number of Treatment protocol Pregnancy rate Study women treatment cycles (% per cycle)__________________________________________________________________________________________________________________________________________
155 564 CC/ CC+hMG/ hCG/placebo Fisch et al. 1989
241 COH + IUI 27.4 Crosignani et al. 1991 268 463 CC + hMG + IUI x 1-2 20.1 Aboulghar et al. 1993
50 130 GnRHa + FSH 150 IU + hCG 5000 21.8 Chung et al. 1995 IU + hCG 2000 IU (luteal support) + IUI x 2
50 110 GnRHa + FSH 150 IU + hCG 5000 7.7 Chung et al. 1995 IU + hCG 2000 IU (luteal support) + TI x 2 117 284 11.0 Tadokoro et al. 1997
40 40 30.0 Zayed et al. 1997
351 351 CC + hCG + IUI 10.0 van der Westerlaken et al. 1998 315 CC + IUI 6.7 Guzic et al. 1998 1133 hMG + IUI 18
119 119 CC 100mg + hMG/ FSH 75-150 33.6 Omland et al. 1998 or hMG/ FSH + hCG 10.000 IU + IUI x1-2
97 97 hMG/FSH 150-225 IU + hCG 10 Sahakyan et al. 1999 5-10.000 IU + IUI x 2
413 CC/ hMG + IUI 15.3 Nuojua-Huttunen __________________________________________________________________________________________________________________________________________
IU + hCG 10.000 IU + IUI x 1-2
hMG/ FSH + hCG
CC + FSH+ hCG + IUI + hCG
19 / 7.6 / 11 / 0
et al. 1999 a
20
2001). IVF is useful for detecting abnormalities in gametes and for evaluating the
fertilizing capacity of spermatozoa and oocytes. If no fertilization has occurred in
a previous IVF attempt, intracytoplasmic sperm injection (ICSI) is the treatment of
choice, as also in cases of low fertilization percentage with conventional IVF.
Gamete intrafallopian transfer (GIFT) and zygote intrafallopian transfer (ZIFT) are
variations of IVF. Their fi rst indication was unexplained infertility (Asch et al.
1986), and they were used in the 1980s and 1990s. These treatments required
similar stimulation as IVF, patent fallopian tubes and earlier also laparoscopic
approach (Crosignani et al. 1993). As both these treatments were more invasive and
expensive and offered no advantages compared with IVF, they have largely been
abandoned (Randolph 2000). The oviduct was thought to provide an optimized
environment for fertilization and fi rst cell divisions, and the embryo was thought
to enter the uterine cavity at a more physiological time in the luteal phase than
in IVF (Boatman 1997; Guzic et al. 1998). However, GIFT does not allow the
determination of fertilization and neither technique permits the assessment of
embryonic development (Randolph 2000).
Reported pregnancy rates with GIFT are 27-55%, and delivery rate per retrieval
29-34% per treatment cycle (Trounson and Wood 1993; Hull et al. 1994; Guzick
1998). With ZIFT, the pregnancy rates are 32-48% (Guzic et al. 1998; Randolph
2000). One reason for good pregnancy rates in GIFT as compared with IVF in some
studies may be the greater number of oocytes transferred, resulting in an increased
rate of multiple pregnancies (Cohen 1991). No prospective, large-scale, randomized
studies have proved GIFT and ZIFT to be superior to IVF.
3. Ultrasound examination
3.1. Basic
In vaginal ultrasound, the typical operating frequency is 5-7.5 MHz, which enables
good image quality within 8-12 cm from the transducer (Dickey 1997). In abdominal
probes, the operating frequency is generally 3.5 MHz, which gives deeper tissue
penetration at lower frequencies and enables examination of inner structures
(Dickey 1997). The pioneering investigators developed transvaginal ultrasound
21
to study follicular growth and enable easy oocyte retrieval (Dellenbach et al.
1984; Meldrum et al. 1984; Schwimer and Lebovic 1984; Wikland et al. 1985).
The use of transvaginal ultrasound later expanded to include other gynaecological
applications. Transvaginal ultrasound is an important tool for studying the anatomy
and pathology of the uterus and ovaries of infertile women. With ultrasound
examination of the uterus, uterine fi broids, endometrial polyps, Asherman’s syndrome
and different developmental uterine anomalies, such as bicornuate uterus and septate
uterine confi guration, can be detected (Allahbadia 1992; Zabrek 1996). When studying
the ovaries, polycystic ovaries, endometriomas, pyo- and hydrosalpinx and tubo-
ovarian abscesses can be recognized (Allahbadia 1992; Zabrek 1996). Ultrasound
has also increased our basic knowledge of follicular growth and endometrial
development, and is essential for monitoring both natural and induced cycles.
3.2. Doppler ultrasound
Because the evaluation of quantitative blood fl ow on the basis of blood fl ow
velocity waveform is diffi cult various qualitative indices have been introduced.
These are the systolic/diastolic (S/D) ratio, the pulsatility index (PI), the resistance
index (RI), also called Pourcelot’s ratio, and peak systolic velocity (PSV). Uterine
artery resistance is measured by S/D, PI and RI.
SD= systolic/diastolic ratio
PI= S/D
mean
RI= S/D
S
The measurement of PI requires computer-assisted calculation of mean velocity.
The RI approaches 1.00 when diastolic velocities are abnormally low. Both high PI
and RI refl ect impairment of fl ow and are independent of insonating angle and true
velocity. The PI and RI are highly correlated.
22
Colour Doppler sonography is useful in identifying blood vessels and enables study
of blood fl ow characteristics of small vessels within the endometrium and the ovary.
Colour Doppler sonography facilitates study of branching of the uterine vasculature
from main uterine arteries to radial and spiral arteries in the endometrium. Apart
from the location, each of the vessels can be recognized by a characteristic
waveform pattern. Colour Doppler sonography uses lower sound intensity than
grey-scale ultrasound. It is an indispensable tool for studying ectopic pregnancy,
molar pregnancy and gynaecological tumours. Power Doppler, also called Doppler
power spectrum analysis, uses echo amplitude (intensity) in the analysis and is
independent of angle (Harman 1995).
3.3. Doppler ultrasound during natural and IVF cycles
Doppler ultrasound during natural cycle
The highest uterine artery PI values occur on day 1 of the menstrual cycle, when
a mean PI of 4.6 has been shown (Steer et al. 1990; Sladkevicius et al. 1994). The
uterine artery PI is also high 2-3 days after the LH peak (Steer et al. 1990; Sladkevicius
et al. 1993). Many studies have shown that the lowest impedance-to-fl ow in the
uterine artery in the spontaneous menstrual cycle occurs in the luteal phase, 6-12
days after the LH peak, which coincides with the implantation window during
cycle days 19-25 (Steer et al. 1990; Sladkevicius et al. 1993; Tan et al. 1996;
Bloechle et al. 1997; Ziegler et al. 1999; Chek et al. 2000). Some studies have
reported a correlation between plasma estradiol and PI and an inverse correlation
between plasma progesterone and PI (Steer et al. 1990). Another study demonstrated
that a high PI in the follicular phase was associated with low estradiol and
progesterone, but no association was observed between serum estradiol and
progesterone levels and uterine artery PI in the luteal phase (Tinkanen et al. 1994).
Other studies have not found any correlation between serum estradiol and uterine
artery impedance (Steer et al. 1994; Zaidi et al. 1995; Ziegler et al. 1999).
In midluteal phase, uterine artery PI is typically below 3.0 and RI below 0.90
(Cacciatore 1996c). Fertility is usually affected when the uterine artery resistance
during midluteal phase is increased and when normal haemodynamic changes
in uterine artery impedance do not occur (Steer et al. 1994; Tinkanen et al.
23
1994; Coulam et al. 1999; Ziegler et al. 1999). Therefore, 20-40% of infertile
women have a high PI (>3.0) in luteal phase, which earlier was associated with
a poorer chance of conception (Steer et al. 1994; Cacciatore et al. 1996a;
Cacciatore 1996c). Uterine artery impedance refl ects the impedance of the whole
uterine vascular bed and may be affected by many factors such as fi broids,
adenomyosis and uterine contractility. The uterine artery resistance in the luteal
phase is also shown to be elevated in different infertile subgroups (Kurjak
et al. 1991; Tinkanen et al. 1994; Zaidi et al. 1998). The explanation for this fi nding
among women with anovulatory cycles is a subnormal hormonal concentration
(Kurjak et al. 1991, Tinkanen et al. 1994), among women with polycystic ovaries
(PCO) an elevated androgen concentration (Zaidi et al. 1998), and among women
with endometriosis or chronic PID peritoneal scarring (Tinkanen and Kujansuu
1992; Steer et al. 1994; Tinkanen et al. 1994). Besides these subgroups, it has
been suggested that abnormal uterine perfusion may also be a contributing factor
to unexplained infertility (Coulam et al. 1994; Steer et al. 1994). However, one
study showed that the mean uterine artery PI in the midluteal phase did not
differ signifi cantly when comparing women with unexplained infertility, women
with adhesions due to PID and women with moderate or severe endometriosis
(Tinkanen et al. 1994).
Besides infertility, some factors may also increase uterine artery impedance in fertile
women. Levonorgestrel intrauterine device (IUD) increases the uterine artery PI in
fertile women during the luteal phase, whereas the copper IUD has no effect on
uterine artery blood fl ow (Järvelä et al. 1998a, 1998b).
In addition, vascular perfusion of the uterus is known to decrease and uterine
artery impedance to increase during menopause, mainly as a result of declining
estradiol concentrations (Goswamy et al. 1988; Battaglia et al. 1995; Kurjak and
Kupesic 1995). About 50% of postmenopausal women have a decreasing PSV in
uterine arteries and 10% have an absent or reversed diastolic fl ow (Sladkevicius et
al. 1994). Furthermore, the uterine arteries become smaller, the shape of the blood
fl ow velocity waveform changes and the uterine artery becomes more diffi cult
to visualize (Sladkevicius et al. 1994). Many studies have shown that estradiol
treatment in postmenopausal women reduces uterine artery impedance (de Ziegler
et al. 1991; Pirhonen et al. 1993; Järvelä et al. 1997). However, synthetic progestins
may antagonize the vasodilatory effect in uterine arteries induced by estrogen
24
treatment (Pirhonen et al. 1993; Järvelä 1998c). Results of different studies have
been confl icting as to the effect of adding progesterone to HRT and its infl uence
on uterine artery impedance (de Ziegler et al. 1991; Bonilla-Musoles et al. 1995).
Interestingly, some studies report no decrease in uterine perfusion with age (Chek
et al. 2000).
Doppler ultrasound during IVF cycle
Transvaginal ultrasound is essential in monitoring ovulation induction cycles and
IVF cycles to determine the number and size of developing follicles during
gonadotrophin stimulation. The uterine artery impedance is usually lower in
gonadotrophin-stimulated cycles compared with natural cycles, and the PI of
uterine arteries on the day of ET is lower in stimulated than in spontaneous cycles
(Tekay et al. 1996a). Early studies showed promising results where uterine artery PI
on day of ET was lower in conception than in non-conception cycles (Steer et al.
1990, 1995; Cacciatore et al. 1996a). In a study by Steer et al. (1995), for example,
the median PI (range) was 2.85 (1.4-3.6) in conception and 4.15 (2.1-6.8) in non-
conception FET cycles (p<0.01). Similar fi ndings were found by Cacciatore et al.
(1996a), who reported a mean PI (± SD) of 2.45 (± 0.54) in conception and 2.66
(± 0.39) in non-conception cycles (p<0.05) during IVF treatment. Different cut-off
values have been suggested to predict non-conception in the IVF cycle. Coulam
et al. (1994) found a uterine artery PI>3.3, and Steer et al. (1994) and Cacciatore
(1996c) reported a uterine artery PI >3.0, whereas Favre et al. (1993) reported a
PI>3.55 to predict non-conception. Tekay and co-workers found a nonsignifi cant
increase in receptivity when the uterine artery PI was between 2.0 and 2.99 and
suggested that a cut-off value of PI>4.0 would predict a non-conception cycle
(Tekay et al. 1995, 1996b). Furthermore, the uterine receptivity is found to be poor
when no end diastolic fl ow in uterine artery is detected (Goswamy et al. 1988;
Kurjak et al. 1991; Steer et al. 1992; Coulam et al. 1994; Cacciatore et al. 1996a;
Tekay et al. 1996a; Tan 1999). Women with absent end diastolic fl ow or poor uterine
blood fl ow have been shown to also have an increased risk of spontaneous abortion
(Cacciatore 1996c). In natural cycles with FET, the implantation has been shown to
decrease when PI>3.5 or with absent end diastolic velocities (Cacciatore 1996c).
Estradiol levels are generally much higher during IVF cycle than natural cycles
25
(Tekay et al. 1996a). Gonadotrophin stimulation with elevated estradiol levels
has been shown to decrease uterine artery PI by approximately 20% (Cacciatore
1996c). During IVF an inverse correlation has been shown between uterine artery
PI values and estradiol levels (Weiner et al. 1993; Cacciatore and Tiitinen 1996b).
Nevertheless, according to current knowledge, it is not possible to distinguish
between conception and non-conception cycles with the sole measurement of
uterine artery PI and RI (Favre et al. 1993; Coulam et al. 1994; Bassil et al. 1995; Tekay
et al. 1995, 1996a). Many factors make comparison of the results diffi cult. Different
study populations, different stimulation protocols, small size of study populations,
an overlap of measured PI values when comparing conception and non-conception
cycles, diurnal variation in uterine artery blood fl ow in the periovulatory period,
showing a lower PI early in the morning, and different results when examining
uterine blood fl ow in women standing and in recumbent position (Coulam et
al. 1994; Dickey et al. 1994; Zaidi et al. 1995; Tekay et al. 1996b). In conclusion,
measurement of uterine artery impedance during IVF treatment to predict outcome
of treatment is not useful in routine clinical practice.
Uterine artery impedance during pregnancy
Efforts have been made to predict pregnancy complications by uterine artery
measurements. Blood fl ow velocity in the uteroplacental arteries increases and the
PI decreases linearly with advancing gestation, indicating an exponential increase
in uterine arteries and uterine perfusion during the fi rst trimester (Valentin et al.
1996). Some studies have shown that uterine and spiral artery resistance were
lower at the end of the fi fth week in blighted ovum pregnancies (Alfi revic and
Kurjak 1990) and the uterine artery RI was lower in missed abortion than in
women with normal pregnancies (Alfi revic and Kurjak 1990; Kurjak 1994). Another
study showed that uterine artery PI measurement at 12-13 weeks of gestation
could predict subsequent hypertensive disorders, small-for-gestational-age fetuses
and gestational diabetes during pregnancy (van den Elzen et al. 1995). In contrast
to these studies uterine artery RI measurements during the fi rst trimester of
pregnancy have not in other studies predicted miscarriage or normal delivery
(Frates et al. 1996).
26
The uterine artery mean fl ow velocity rises progressively from a non-pregnant
value nearly eightfold by week 36 (Palmer et al. 1992). By measuring uteroplacental
and umbilical artery Doppler S/D ratios during the 24th gestational week, it was
possible to predict intrauterine growth retardation and hypoxia (Newnham et al.
1990). Another study suggested that uterine artery measurement at 21-24 weeks
could predict PIH and IUGR in high-risk but not low-risk populations (Zimmermann
et al. 1997). Numerous other studies have also shown that measurement of uterine
artery blood fl ow is useful in predicting pre-eclampsia or fetal growth restriction
(Bewley et al. 1991; Strigini et al. 1995; Harrington et al. 1996; Kurdi et al. 1998).
With advancing gestation, the spiral artery RI decreases in normal pregnancies
(Murakoshi et al. 1996). An abnormal spiral artery RI has been proven to have
better diagnostic accuracy than the RI of uterine artery waveform for predicting
PIH and IUGR, and in one study with 43 pregnancies complicated with PIH and/ or
IUGR, 19 had abnormal spiral artery RI when examinations were performed during
gestational weeks 18-41 (Murakoshi et al. 1996).
Impedance in spiral artery
In healthy fertile women, a signifi cant decrease in spiral artery resistance occurs
from the proliferative to the luteal phase, and the changes are equivalent to those
seen in uterine arteries (Kurjak and Kupesic 1995). Because the sensitivity of colour
Doppler is limited, weak vascular signals in endometrial vasculature can be diffi cult
to observe (Yang et al. 1999). However, endometrial blood fl ow has been suggested
to be a more specifi c parameter for predicting uterine receptivity in IVF cycles
than uterine blood fl ow, and when endometrial blood fl ow is poor, implantation
is less likely to occur (Zaidi et al. 1995; Tan 1999). In 88.8% of infertile patients,
spiral arteries can be demonstrated during the natural cycle from day 10-12
onwards (Kupesic 1996b). However, not all studies have found predictive value
of measurements of subendometrial PI (Yuval et al. 1999). The absence of
subendometrial fl ow on day of HCG administration during the IVF cycle has
been shown to predict failure of implantation irrespective of the morphological
appearance of the endometrium (Zaidi et al. 1995). Spiral artery impedance
measurement has greater inter-observer variability compared with that of uterine
arteries (Dickey et al. 1994). Levonorgestrel IUD has been shown to suppress the

27
formation of spiral arteries (Järvelä 1998c). Age also affects spiral artery blood fl ow.
With advancing age, blood fl ow to the endometrium decreases and blood fl ow in
spiral arteries is detected in only 30% of postmenopausal women within 1-5 years
of cessation of the menstrual cycle (Kurjak and Kupesic 1995).
A surprising fi nding is that better perfusion of the uterus, measured as lower PI
values both in the radial and spiral arteries in the natural cycle compared with
corresponding values in ovulation induction cycles, suggests that receptivity of the
uterus would be better in natural cycles (Kupesic and Kurjak 1993).
Most authors agree that treatment cycles with absent spiral arteries have poor
implantation rates. Despite some initially promising results in predicting conception
and non-conception cycles with measurement of spiral artery impedance in women
with detectable spiral arteries, some studies show no difference in spiral artery
impedance measurement in conception and non-conception cycles; therefore,
further research is clearly needed.
Impedance in ovarian artery
In ovarian arteries, the cyclic variations are smaller than in uterine arteries (Tekay
et al. 1995). In natural cycles, the ovarian artery RI has been shown to decline on
the day before ovulation and to remain low in the luteal phase both in healthy
and infertile women (Kurjak et al. 1991; Tinkanen et al. 1994; Kupesic et al. 1995).
Intrafollicular PSV has also been demonstrated to increase on the day of ovulation
and remain high for at least 72 hours (Campbell et al. 1993). This increases blood
supply to the corpus luteum, which is important for steroidogenesis and favours
implantation and early embryo development (Kupesic 1996a). The ovarian PI on
the dominant side is signifi cantly lower and PSV signifi cantly higher in the luteal
phase in the ovarian stroma and hilus (Sladkevicius et al. 1993). An increased intra-
ovarian impedance has been found in patients with out-of-phase endometrium
biopsies thoughout the luteal phase, since among menopausal women and later in
menopause, no blood fl ow can be detected in the ovaries (Sladkevicius et al. 1994;
Kurjak and Kupesic 1995).
28
Cyclic alterations in ovarian artery blood fl ow seen in natural cycles do not occur
in gonadotrophin-stimulated cycles, where arteries seem maximally dilated (Tekay
et al. 1995). In IVF cycles, no difference has been found in ovarian artery impedance
when comparing conception and non-conception cycles (Sterzic et al. 1989; Tekay
et al. 1995). According to a recent study, a follicle with high PSV in a natural or IVF
cycle will most likely have a good oocyte with high implantation potential (Kelly et
al. 2001). However, the role of ovarian blood fl ow in successful IVF treatment has
yet to be studied in larger study populations.
4. Assisted reproductive technology
4.1. Defi nition and rate of success
Assisted reproductive technology (ART) includes controlled ovarian stimulation
alone or combined with intra-uterine insemination or direct intraperitoneal
insemination and in-vitro fertilization and its modifi cations. The success rates of
treatment vary considerably with patient selection, infertility duration, indication
for treatment and type of treatment.
Ovarian stimulation and/or artifi cial insemination (IUI/DIPI)
Ovarian stimulation with CC or gonadotrophins increases the levels of gonadal
steroids as a result of development of multiple pre-ovulatory follicles and may
overcome subtle ovulatory defects, such as luteinized unruptured follicle syndrome,
not detected in routine diagnostic studies; pregnancy rate may increase with the
larger number of oocytes available for fertilization (Fish et al. 1989; Guzic et al. 1998;
Aboulghar et al. 1999; Sahakyan et al. 1999). Swim-up of sperm before insemination
may enhance the fertilizing capacity of sperm, and increase the density of motile
sperm in the uterus and fallopian tubes available for fertilization and implantation
(Aboulghar et al. 1999). By IUI or DIPI, problems in cervical mucus, mild defects in
sperm motility and function are overcome (Crosignani and Rubin 1996; Wolf 2000).
By bringing together multiple mature oocytes and highly motile sperm in the fallopian
tube, the likelihood of pregnancy is increased (Fish et al. 1989).
29
Although couples with unexplained infertility usually have ovulatory cycles even
without treatment, ovulation induction may overcome subtle defects in ovulatory
function not detected in conventional tests, and increase the number of oocytes
available for fertilization and implantation (Guzic et al. 1998; Aboulghar et al.
1999; Sahakyan et al. 1999). CC has also been shown to reduce the incidence of
luteal-phase defi ciency from 31% to 3% among women with unexplained infertility
(Rodin et al. 1994).
IUI in the spontaneous cycle among women with unexplained infertility yields
pregnancy rates of 2.4-7.4% per cycle (Guzic et al. 1998; Goverde et al. 2000);
which is similar to pregnancy rates of expectant management (Goverde et al. 2000).
If CC is used without IUI, the pregnancy rate per cycle is 4-5.6% among women
with unexplained infertility (Guzic et al. 1998; Hughes et al. 2001). The use of
gonadotrophins (hMG) alone is associated with a pregnancy rate of 7.7% (Guzic
et al. 1998). If CC is used in combination with IUI, the pregnancy rate per cycle is
approximately 8.3% (Guzic et al. 1998). If CC or hMG is used in combination with
IUI, the pregnancy rate per cycle increases to approximately 10-17.1% and 29.8%,
respectively, per patient after three treatment cycles (Guzic et al. 1998; Aboulghar
et al. 1999; Sahakyan et al. 1999).
In-vitro fertilization
IVF is now recommended for essentially all infertility conditions that have not been
successfully treated by other modalities (Dor et al. 1996; Forti and Krausz 1998;
Unkila-Kallio 2001). IVF is useful for recognizing abnormalities in gametes and for
evaluating the fertilizing capacity of spermatozoa and oocytes, i.e. we know whether
the sperm penetrate and fertilize the oocytes. This is especially important among
couples with unexplained infertility or male infertility. Figure 1 shows the treatment
protocol for IVF.

30
Figure 1. A model for ovarian hyperstimulation for IVF with long pituitary downregulation with a GnRH agonist. The squares in the fi gure represent days of stimulation.
The reason for the favourable success rate in IVF is partly the same as in COH, i.e.
it increases the production of a superabundance of oocytes with superovulation
which are then available for fertilization, overcomes ovulatory defects and
enhances fertilizing ability (Guzic et al. 1998; Hull et al. 1998). Furthermore, IVF is
useful for documenting the occurrence of fertilization and for evaluating embryo
quality.
The pregnancy rates are almost equally good in all indications. Couples with
unexplained infertility treated with IVF usually have the same oocyte recovery as
other groups, but they have been shown to have reduced fertilization and cleavage
rates, and a complete failure of fertilization has been reported in 5-30% of the cycles
(Hull et al. 1998; Takeuchi et al. 2000). However, the complete fertilization failure is
usually not repetitive (Hull et al. 1998). New evidence points to the possibility of
oocyte metaphase I maturation block, which is responsible for at least part of the
repetitive fertilization failures (Harrison et al. 2000; Bergere et al. 2001).
Among women with unexplained infertility treated with IVF, clinical pregnancy
rates per oocyte pick-up (OPU) are 21-37% (Crosignani et al. 1991; Tanbo et al. 1995;
Guzic et al. 1998; Aboulghar et al. 1999). The overall reported cumulative pregnancy
rates among unselected patients undergoing IVF treatment are 22-32% after one,
36-57% after two, 47-71% after three and 53-81% after four IVF attempts (Rowlands
et al. 1994; Stolwijk et al. 2000). The reported corresponding cumulative birth rates
are 29%, 52%, 63% and 75%, respectively (Rowlands et al. 1994).

31
4.2. Prognostic markers for successful outcome
Many investigators have tried to fi nd predictive markers for successful outcome of
IVF treatment. Traditionally, the woman’s age and early follicular phase serum FSH
are the most useful parameters for prediction of ovarian reserve (Chek et al. 1994;
Kupesic and Kurjak 2002). The most important predictive factor for success in IVF
treatment in many studies is age of the woman. The highest livebirth rates after IVF
are equivalent in both age group 25-30 years (Templeton et al. 1996) and in age
group below 35 years (Abdelmassih et al. 1996; Engmann et al. 2001). Conception
rates begin to decline at 30-33 years due to oocyte and endometrial aging
(Battaglia et al. 1996; Dor et al. 1996; Lim and Tsakok 1997). Another study reported
declining pregnancy rates after IVF-ET with increasing female age as follows: in
women aged <30 years, clinical pregnancy rate 29.4%; in women 30-35 years,
19.8%; in women 36-39 years, 17.1%; in women >40 years, 12.8% (Szamatowicz and
Grochowski 1998). With increasing age, the number and quality of oocytes decline,
a larger proportion of the oocytes remain unfertilized in IVF and the pregnancy
rates tend to be lower (Lim and Tsakok 1997). After the mid-thirties, follicles also
have fewer granulosa cells, thus producing less steroids and glucoproteins, and
decreased mitosis and increased apoptosis appear (Nikolaou et al. 2002). Female
age is also of important prognostic value in gonadotrophin-induced COH-IUI cycles
(Buyalos et al. 1997; Sahakyan et al. 1999). Increased early follicular phase FSH and
E2 values have been shown to correlate with poor ovarian reserve and reduced
fertility potential in COH treatment cycles (Magarelli et al. 1996; Buyalos et al.
1997). Elevated FSH has been suggested to induce enhanced E2 production by
granulosa cells (Buyalos et al. 1997).
Besides female age, the cause of infertility may also infl uence the outcome of
ART treatment; couples with unexplained infertility are reported to have a better
prognosis than couples with tubal infertility or endometriosis (Templeton et al.
1996; Omland et al. 1998; Nuojua-Huttunen et al. 1999a; Sahakyan et al. 1999).
Women with tubal infertility have also been reported to have lower cumulative
delivery rates than other subgroups of infertility (Sundström et al. 1997). Among
women with tubal infertility, a relationship exists between grade of tubal damage
and pregnancy rate following IVF. Patients with milder tubal damage have higher
take-home baby rates per started IVF cycle (48%) than patients with severe tubal
damage (6%; Csemiczky et al. 1996). The pregnancy rates of infertile women with
32
hydrosalpinx are signifi cantly lower (19.7%) than those of women with tubal
infertility without hydrosalpinx (31.2%; Camus et al. 1999). One study showed that
women with endometriosis had a higher and couples with male factor infertility a
lower pregnancy rate after IVF than in other aetiologies of infertility (Minaretzis et
al. 1998). In addition, women with ovulatory disorders or endometriosis have also
been reported to have good pregnancy rates compared with male and tubal factor
infertility in COH-IUI treatment cycles (Sahakyan et al. 1999). However, some other
studies have not shown any difference in pregnancy rate after IVF when comparing
different subgroups of infertile patients (Tan et al. 1992; Dor et al. 1996).
The duration of infertility and parity of women infl uence pregnancy rates in ART.
An increase in duration of infertility decreases the chance of success after IVF
treatment (Templeton et al. 1996) and COH-IUI cycles (Nuojua-Huttunen et al.
1999a). In COH-IUI cycles, an infertility duration of over six years has been shown to
decrease the chance of success (Tomlinson et al. 1996; Nuojua-Huttunen et al. 1999a).
A previous pregnancy and delivery, especially if the earlier pregnancy was achieved
after IVF treatment, increases the chance of success in a subsequent IVF treatment
(Templeton et al. 1996; Engmann et al. 2001). Patients with secondary infertility
have been reported to have nearly double the pregnancy rate of women with
primary infertility (Lessing et al. 1988; Collins and Rowe 1989). On the other hand,
the highest livebirth pregnancy rate is reported in the fi rst three treatment cycles
(Engmann et al. 2001). Another study showed that the clinical pregnancy rate
remained similar during the fi rst six IVF cycles (Dor et al. 1996). A recent study
revealed that the following factors increased the chance of success in the IVF cycle:
age of woman (<35 years), previous IVF live birth, other than tubal infertility, large
number of embryos created and fewer than three previous unsuccessful IVF cycles
(Engmann et al. 2001). All of these factors increase the chance of both singleton
and multiple births (Engmann et al. 2001).
An ideal method to predict uterine receptivity has yet to be established (Friedler
et al. 1996). Furthermore, the overall success rate of the clinic is very important
when predicting success for a particular couple (Templeton et al. 1996). According
to recent studies, major determinants of successful in-vitro fertilization besides
woman’s age are embryo quality, number of embryos transferred and endometrial
thickness (Goverde et al. 2000; Bassil 2001).
33
Embryo quality is largely based on cleavage rate and the degree of fragmentation,
which are important factor in predicting implantation (Ziebe et al. 1997; Alikani
et al. 1999). Lundin et al. (2001) showed that embryos which cleave early, i.e.
complete the fi rst mitotic division within 25-27 hours post-insemination, provide
higher pregnancy per transfer rate (40.5% vs. 31.5%; p=0.0049) than slower-cleaving
embryos (van Royen et al. 1999). Furthermore, the rate of twin pregnancies has
been found to be higher (33.3% vs. 22.3%; p=0.036), and the rate of spontaneous
abortion to be lower in the early-cleaving group (Lundin et al. 2001). Unevenly
cleaved embryos with large differences in blastomere size have higher rate
of aneuploidy and lower implantation rates than embryos with equally sized
blastomeres (Hardarson et al. 2001).
The presence of large fragments is detrimental to the developing embryo and
these embryos have signifi cantly lower pregnancy rates, whereas small fragments
do not affect implantation (Alikani et al. 1999). It is possible to score embryos
in IVF cycles, and according to this scoring, decide how many embryos should
be transferred. A top-quality embryo is characterized by the presence of 4 or 5
blastomeres on day 2 and at least 7 blastomeres on day 3 after insemination, the
absence of multinucleated blastomeres and <20% cellular fragments on day 2 and
day 3 after fertilization (Gerris and van Royen 2000). By transferring only one top-
quality embryo in the fi rst IVF/ICSI cycle of women <34 years of age, a prospective
study showed that the implantation rate was 42.3%, and thus, the pregnancy rate
was similar or even better compared with normal fertile couples (Te Velde and
Cohlen 1999). Moreover, this procedure limited the twin pregnancy rate to <1%
of pregnancies (Gerris and van Royen 2000). The number of normally developed
embryos, i.e. the number of embryos available for transfer, is more important
in determining the probability of birth than the number of embryos actually
transferred (Engmann et al. 2001). In contrast, the risk of multiple gestation
increased both with the number of embryos available and the number of embryos
transferred (Engmann et al. 2001). Also, if several embryos are created, it increases
the likelihood of selecting good-quality embryos for transfer, thus, the number of
embryos available may be an indirect measure of embryo quality (Devreker et al.
1999; Engmann et al. 2001). The cell stage at transfer of the embryo is also important
in predicting success of treatment (Yang et al. 1999; Bassil 2001).

34
The type of embryo transfer catheter has also been shown to infl uence pregnancy
rates, which in a recent study were signifi cantly higher with a soft catheter
compared with a stiff catheter (27.1% vs. 20.5%; van Weering et al. 2002).
Studies have shown that a small ovarian volume, reduced stromal area and decreased
number of antral follicles predict poor response in controlled ovarian stimulation
(Chek et al. 1994; Syrop et al. 1995; Pellicer et al. 1998; Kupesic and Kurjak
2002). A strong association between ovarian volume and ovarian reserve has been
demonstrated, and measurement of ovarian volume was recommended as an
essential part of infertility evaluation (Lass et al. 1997). A cut-off value of less than
3 cm3 may refl ect failure to respond to gonadotrophin stimuli (Lass et al. 1997).
However, when measured with three dimensional ultrasound, it was shown that
some patients may have diminished ovarian reserve without changes in ovarian
volume (Kupesic and Kurjak 2002). Other authors suggested that predicting ovarian
response was possible by counting the number of antral follicles (Tomas et al.
1997). The best predictive factor for ovarian response to stimulation is in fact
assessment of the total number of antral follicles by ultrasound (Ng et al. 2000;
Kupesic and Kurjak 2002). The number of antral follicles is clearly related to
reproductive age and refl ects the remaining primordial follicle pool (Kupesic and
Kurjak 2002). Measurement of ovarian stromal PSV in early follicular phase may also
predict follicular response (Zaidi et al. 1995). Poor responders have been shown to
have a poor ovarian stromal PSV (Zaidi et al. 1995).
Measurements of the intra-endometrial power Doppler area (Yang et al. 1999) have
been postulated to predict implantation. According to another study, however,
the three-dimensional power Doppler measurement of the endometrial area is not
helpful in predicting implantation (Kupesic et al. 2001). Nevertheless, in a study
of 56 infertile women, statistically signifi cant differences were shown in the antral
follicle number, ovarian volume, ovarian stromal area and ovarian stromal fl ow
index in conception and non-conception cycles when ovaries were studied after
pituitary suppression during IVF treatment (Kupesic and Kurjak 2002).
Uterine artery impedance has previously been demonstrated to predict conception
in IVF cycles, but it is an inaccurate method and no consensus on a cut-off rate for
good pregnancy rates exists. However, most authors agree that an absent end diastolic
fl ow on day of ET predicts non-conception during the present IVF cycle (Goswamy
35
et al. 1988; Kurjak et al. 1991; Steer et al. 1992; Coulam et al. 1994; Cacciatore
et al. 1996a; Tekay et al. 1996b; Tan 1999).
The endometrium is thicker in ART cycles compared with natural cycles mainly
due to higher E2 levels in ART cycles (De Geyter et al. 2000). No differences were
found in endometrial thickness between conception and non-conception cycles
during ART treatment (Coulam et al. 1994; Bohrer et al. 1996; De Geyter et al.
2000), although cut-off values of 6-8 mm have been suggested as the minimum
for embryo implantation (Steer et al. 1992; Coulam et al. 1994; Zaidi et al. 1995).
A multilayer endometrial pattern has also been shown to predict conception in
ovulation induction cycles (Check et al. 1991; Coulam et al. 1994; Serafi ni et al. 1994;
Hock et al. 1997). In addition, a conversion of the endometrial pattern from the
homogeneous pattern seen in the early proliferative phase to the trilaminar pattern
must occur to produce optimal receptivity (Zaidi et al. 1995; Hock et al. 1997).
A pre-ovulatory triple-line endometrium combined with end diastolic velocity in
the fi rst branch of uterine artery was the most important predictor of conception in
one study (Serafi ni et al. 1994). However, endometrial thickness and morphological
appearance of the endometrium are rather inaccurate methods for predicting
conception, and evaluation of morphological appearance is quite subjective (Tan
1999; Kupesic et al. 2001). Furthermore, measurements of spiral artery impedance
to predict conception have given inconsistent results (Zaidi et al. 1995; Schild
et al. 2001). Most authors do, however, agree that absent spiral arteries predicts
non-conception during the present IVF cycle (Zaidi et al. 1995; Yang et al. 1999).
4.3. Pregnancy outcome of ART-induced pregnancies
The rate of spontaneous abortions is approximately 19-25% after IVF, and this rate
is similar to that of women with normal fertility (Wilcox et al. 1999; Pezeshki et
al. 2000; Gissler and Tiitinen 2001). No association has been shown between the
aetiology of infertility and the risk of spontaneous abortion after IVF (Pezeshki et
al. 2000). The risk of spontaneous abortion is similar in IVF and ICSI pregnancies
(Govaerts et al. 1996; Gissler and Tiitinen 2001), but results of other studies are
confl icting (Aytoz et al. 1999; Griffi ths et al. 2000; Ola 2000; Bonduelle et al. 2002).
Bleeding, particularly in the fi rst trimester, is more common in IVF pregnancies
than in spontaneous pregnancies (Olivennes et al. 1993; Verlanen et al. 1995;
36
Wennerholm et al. 1996; Koudstaal et al. 2000a).
The rate of ectopic pregnancies after IVF is reported to be 2-4%, and the
corresponding fi gure after natural conception is 2% (Marcus et al. 1995; Strandell
et al. 1999; Adamsson and Brzyski 2000). Tubal infertility, tubal surgery and PID
increase the risk to 7-10% after IVF treatment, while male factor infertility has
a protective effect against ectopic pregnancy (Verlust et al. 1993; Strandell et
al. 1999). Among IVF pregnancies, the rate of heterotopic pregnancies is <1.0%
(Ludwig et al. 2001).
A period of infertility of more than 12 months signifi cantly increases the woman’s
risk of preterm birth (1.6- to 1.8-fold) and a low birth weight baby (1.9-fold) even
in the absence of infertility treatment (Williams et al. 1991; Henriksen et al. 1997).
COH-IUI treatment has been reported to reduce the mean birthweight of newborns
compared with spontaneous pregnancies (Nuojua-Huttunen et al. 1999b). Another
study showed increased risk of non-insulin-dependent diabetes mellitus (12.7%
vs. 6.9%), pregnancy-induced hypertension (9.3% vs. 6.2%) and Caesarean section
(18.4% vs. 13.1%) after COH treatment compared with spontaneous pregnancies
(Maman et al. 1998). Moreover, a small increase in the rate of preterm birth after
COH-IUI or donor insemination has been reported (Wang et al. 2002).
The risk of pregnancy-induced hypertension, pre-eclampsia, placenta previa and
non-insulin-dependent gestational diabetes increase in IVF-pregnancies, also among
singletons (Wennerholm et al. 1991; Doyle et al. 1992; Tan et al. 1992; Wang et
al. 1994; Tallo et al. 1995; Tanbo et al. 1995; Maman et al. 1998; Minakami et al.
1998; Hansen et al. 2002), but some authors have suggested that these increased
risks are associated with patient characteristics, such as increased maternal age and
lower parity (Doyle et al. 1992; Lansac 1995; Wennerholm et al. 1996). Pregnancies
achieved after IVF also increase the risk of premature deliveries and low birthweight
also in singleton pregnancies (Bergh et al. 1999; Tarlatzis and Grimbizis 1999;
Westergaard et al. 1999; Hansen et al. 2002; Schieve et al. 2002; Wang et al.
2002). On average, IVF singletons were born 5.1 days earlier and weighed
214 grams less than spontaneously conceived infants (Koudstaal et al. 2000a).
A signifi cant increase in rate of low birthweight babies has been shown both among
preterm and full-term singletons (Schieve et al. 2002). The risk of low birthweight
37
infants is estimated to be 2.6-fold that of the general population (Schieve et al.
2002). In singleton pregnancies, the rate of preterm delivery is approximately 9-15%
in IVF vs. 3-6% in spontaneously conceived pregnancies (Maman et al. 1998; Tarlatzis
and Grimbizis 1999), the rate of low birthweight newborns (<2500 g) is 13.4% vs.
7.3% (Tarlatzis and Grimbizis 1999; Koudstaal et al. 2000a) and the rate of very low
birthweight newborns (<1500 g) is approximately 2.6% (Tan et al. 1992; Olivennes
et al. 1993; Schieve et al. 2002) vs. 1% (Hansen et al. 2002). Low birthweight is
less common in infants conceived with ICSI treatment due to male factor infertility
compared with other subgroups (Schieve et al. 2002). In comparing IVF and ICSI
pregnancies, statistically signifi cant differences have been seen in the rate of very
low birthweight infants (IVF 5.6% vs. ICSI 4.4%), whereas the rate of preterm birth
was signifi cantly higher in ICSI pregnancies (Bonduelle et al. 2002). Many reports
also show an elevated rate of Caesarean section among both singleton and multiple
pregnancies after IVF, as well as increased induction of labour in unselected IVF
patients (Verlanen et al. 1995; Maman et al. 1998; Westergaard et al. 1999).
Studies among women with unexplained infertility have shown an especially high
risk of IUGR after ART compared with other subgroups (Wang et al. 1994; Dawood
1996). Also signifi cantly higher incidences of pre-eclampsia, placental abruption,
preterm labour, induction of labour and emergency Caesarean section have been
demonstrated among women with unexplained infertility compared to the general
population (Pandian et al. 2001). In addition, spontaneous pregnancies among these
women had elevated rates of obstetric complications.
Pregnancies achieved after IVF bear an increased risk of multiple pregnancy, the
rate of multiple pregnancy being approximately 25-35% (Koudstaal et al. 2000b;
Nygren and Nyboe Andersen 2001; Tiitinen et al. 2001), compared with only 1%
in naturally conceived pregnancies (Addor et al. 1998). Multiple pregnancy is,
according to many authors, the most serious complication of ART (Vilska et al.
1999; Tiitinen et al. 2001; Koivurova et al. 2002). The risk of multiple pregnancy
is related to the number of embryos transferred and not to IVF per se. Multiple
pregnancies, either conceived spontaneously or after IVF, increase the risk of many
complications, the most important being low birthweight infants (Koudstaal et
al. 2000b). IVF twins have also higher rates of very low birthweight, discordant
birthweight, prematurity, neonatal morbidity and mortality and women with IVF
twins have an elevated risk of vaginal bleeding compared with women with
38
spontaneously conceived twins (Bernasko et al. 1997; Moise et al. 1998; Koudstaal
et al. 2000b). However, in some studies, twins conceived with ART did not have an
increased rate of low birthweight compared with spontaneously conceived twins
(Westergaard et al. 1999; Schieve et al. 2002).
In most earlier studies, the incidence of congenital and chromosomal anomalies
after IVF and ICSI has been comparable to that in the general population,
approximately 1.8-4.5% (Lancaster et al. 1995; Govaerts et al. 1996; Palermo et
al. 1996; Wennerholm et al. 1996; Johnson 1998; Tarlatzis and Grimbizis 1999;
Westergaard et al. 1999; Ludwig et al. 2001; Bonduelle et al. 1996, 1999, 2002).
No statistically signifi cant difference has been observed in major malformation
rates when ICSI and IVF children were compared (Bonduelle et al. 2002). In some
studies higher rates, such as 7.6% congenital malformations after ICSI, have been
reported (4.1% were classifi ed as major; Wennerholm et al. 2000). And a recent
report from Australia showed an increased rate of major congenital anomalies after
IVF (9.0%) and ICSI (8.6%), compared with 4.2% for naturally conceived infants
(Hansen et al. 2002). Signifi cantly increased rates of cardiovascular, urogenital,
musculoskeletal and chromosomal defects were demonstrated among infants
conceived with IVF, and musculoskeletal and chromosomal defects among infants
conceived with ICSI. The reason for these fi ndings may be the relatively small
number of patients included in the latter study as well as the follow-up of newborn
being extended to one year of age. Furthermore, infants conceived with ART had
more multiple major congenital anomalies compared with their naturally conceived
counterparts (Hansen et al. 2002). Other studies have also shown a slightly
increased rate of neural tube defect, alimentary atresia, omphalocele, hypospadia
and congenital heart anomalies (ASD, VSD or transposition of the great vessels)
among infants conceived with IVF or ICSI (Lancaster 1987; Bergh et al. 1999; Silver
et al. 1999; Ericson and Källén 2001; Koivurova et al. 2002).
Malformation rates in both IVF and ICSI multiples are signifi cantly higher than in
IVF and ICSI singletons (Wennerholm et al. 2000; Bonduelle et al. 2002). In addition,
a signifi cantly higher malformation rate has been shown in IVF twins compared
with ICSI twins (Bonduelle et al. 2002). It should be noted that follow-up of
children conceived with ART is often more detailed, and thus anomalies that would
likely have gone unnoticed in the general population might be detected in the
ART population, elevating congenital anomaly rates in some studies (Tarlatzis and

39
Grimbizis 1999; Hansen et al. 2002).
In a recent study, no difference was observed in the rate of abnormal foetal karyotype
among ICSI (2.9%) and IVF (3.0%) foetuses (Bonduelle et al. 2002). However,
a small increase in sex-chromosomal abnormalities (1%) has been reported in
many studies, which could be explained by ICSI bypassing the natural selection
of spermatozoa and sub-optimal male gametes being used in ICSI (Bonduelle et
al. 1996; Govaerts et al. 1996; Tarlatzis and Grimbizis 1999; Macas et al. 2001; Ola
et al. 2001). A follow-up of 1987 children born with ICSI reported 0.83% sex-
chromosomal abnormalities, which is four times greater than the expected rate
of 0.19% (Bonduelle et al. 1999); these results are in concordance with several
other studies (Wisanto et al. 1996; Johnson 1998; Bonduelle et al. 1999; Tarlatzis and
Grimbizis 1999; Macas et al. 2001; Ola et al. 2001). A small increase in autosomal
aberrations has also been reported (Bonduelle et al. 1999). ICSI does not increase
the risk of chromosomal anomalies or congenital malformations, unless parents
have an abnormal karyotype or family history of some disease (Johnson 1998),
but the possibility of transmitting fertility problems of genetic origin to the male
offspring cannot be excluded (Tarlazis and Grimbizis 1999), although the risk is
marginal (Bonduelle et al. 1999, 2002).
In conclusion, the absolute risk for a serious malformation to occur after IVF
is, according to several studies, small; however, the results of some studies are
confl icting. ICSI may marginally increase the risk of sex-chromosomal abnormalities,
which are diffi cult to detect in routine examination of newborns (Ericson and
Källén 2001). The slightly increased risk for a congenital malformation after IVF
may partly be explained by maternal characteristics. Increased risk of hypospadia
may be explained genetically as due to paternal subfertility, while increased risk
of alimentary atresia might be connected to the monozygotic twinning process
(Ericson and Källén 2001). Multiple births can increase malformation rate to some
extent, and some malformations, such as persistent ductus arteriosus, may be related
to premature birth (Bergh et al. 1999).
Children born after IVF in Sweden have in one large study been shown to have an
increased risk of neurological disability, such as cerebral palsy, and an increased risk
of developmental delay (Strömberg et al. 2002). These risks are elevated mainly due
to the high frequency of twin pregnancies, low birthweight infants and premature
40
births among IVF children. However, long follow-up of children aged 6-13 years
conceived with IVF revealed no difference in school performance; 92% of these
children presented an encouraging outcome (Olivennes et al. 1997), and no large
differences in IVF children’s psychosocial development were shown compared
with naturally conceived children (Colpin and Soenen 2002).
The need for treatment in the neonatal care unit among IVF children is higher
primarily due to the increased rate of preterm and multiple births (Ericson et
al. 2002; Koivurova et al. 2002), and an increased rate of hospital care was also
present among full-term and singleton IVF children up to an age of six years
(Ericson et al. 2002). IVF twins did not have an excessive hospitalization rate
compared with other twins (Ericson et al. 2002). The reported stillbirth rate is
1.7% in ICSI and 1.3% in IVF pregnancies (Bonduelle et al. 2002). The neonatal
death rate was, in another report, 1.0% after IVF treatment (Bustillo and Yee
1999), but the Finnish study showed a perinatal mortality rate which was twice
as high in IVF children compared with national fi gures for the general population
(Koivurova et al. 2002).
The postnatal growth of children born with IVF is usually normal if the neonatal
period is uncomplicated (Wennerholm et al. 1991; Tarlatzis and Grimbizis 1999;
Ludwig et al. 2001). No excessive risk of childhood cancer has been found after
IVF treatment (Ericson et al. 2002). In a follow-up study of pregnancy outcome
following cryopreserved ET, fresh IVF-ET and spontaneous pregnancies until the
age of 5.5 years of the child, no differences were found when length, weight,
head circumference and chronic illnesses (at 18 months of age) were compared
(Olivennes et al. 1997; Wennerholm et al. 1998).
41
1. To assess uterine and spiral artery impedance in natural and IVF cycles
among women with unexplained infertility compared with women with tubal
infertility and to evaluate the usefulness of uterine artery impedance in the
prediction of outcome of treatment and pregnancy.
2. To compare the effi cacy of ovulation induction combined with intra-uterine
insemination, direct intraperitoneal insemination and timed intercourse in
treatment of unexplained infertility.
3. To study the long-term prognosis of couples with unexplained infertility.
4. To compare the obstetric outcome of treatment and spontaneous pregnancies.
III AIMS OF THE STUDY
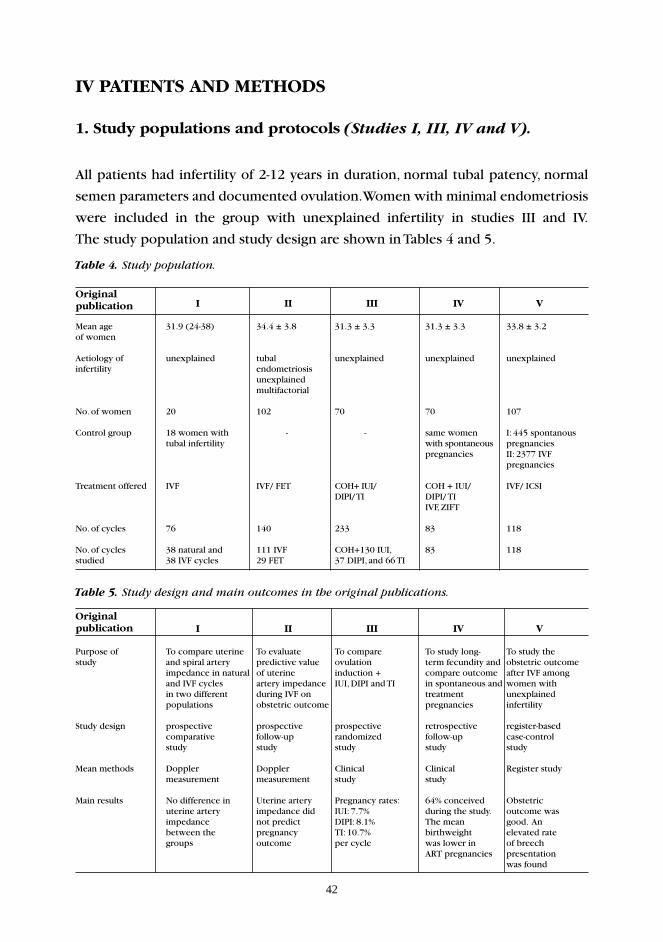
42
IV PATIENTS AND METHODS
1. Study populations and protocols (Studies I, III, IV and V).
All patients had infertility of 2-12 years in duration, normal tubal patency, normal
semen parameters and documented ovulation. Women with minimal endometriosis
were included in the group with unexplained infertility in studies III and IV.
The study population and study design are shown in Tables 4 and 5.
Table 4. Study population.
Original I II III IV Vpublication
Mean age 31.9 (24-38) 34.4 ± 3.8 31.3 ± 3.3 31.3 ± 3.3 33.8 ± 3.2of women
Aetiology of unexplained tubal unexplained unexplained unexplainedinfertility endometriosis unexplained multifactorial No. of women 20 102 70 70 107
Control group 18 women with - - same women I: 445 spontanous tubal infertility with spontaneous pregnancies pregnancies II: 2377 IVF pregnancies
Treatment offered IVF IVF/ FET COH+ IUI/ COH + IUI/ IVF/ ICSI DIPI/ TI DIPI/ TI IVF, ZIFT
No. of cycles 76 140 233 83 118
No. of cycles 38 natural and 111 IVF COH+130 IUI, 83 118studied 38 IVF cycles 29 FET 37 DIPI, and 66 TI
Table 5. Study design and main outcomes in the original publications.
Original I II III IV Vpublication
Purpose of To compare uterine To evaluate To compare To study long- To study the study and spiral artery predictive value ovulation term fecundity and obstetric outcome impedance in natural of uterine induction + compare outcome after IVF among and IVF cycles artery impedance IUI, DIPI and TI in spontaneous and women with in two different during IVF on treatment unexplained populations obstetric outcome pregnancies infertility
Study design prospective prospective prospective retrospective register-based comparative follow-up randomized follow-up case-control study study study study study
Mean methods Doppler Doppler Clinical Clinical Register study measurement measurement study study
Main results No difference in Uterine artery Pregnancy rates: 64% conceived Obstetric uterine artery impedance did IUI: 7.7% during the study. outcome was impedance not predict DIPI: 8.1% The mean good. An between the pregnancy TI: 10.7% birthweight elevated rate groups outcome per cycle was lower in of breech ART pregnancies presentation was found
43
Study I
Twenty women with unexplained infertility and 18 women with tubal infertility,
all scheduled for treatment with IVF (or ICSI) were recruited to participate. The mean
age of women in the group with unexplained infertility was 32.6 (range 26-39) years,
and in the control group 31.9 (range 24-38 years; NS). The mean (± SD) duration
of infertility was 69 (± 32.4) months among women with unexplained infertility
and 44 (± 16.5) months (p<0.01) among women with tubal infertility. Infertility
was primary in 13 (65%) of the women with unexplained and in 7 (38.9%) of
women with tubal infertility (NS). We prospectively longitudinally measured the
uterine and spiral artery pulsatility index (PI) and peak systolic velocity (PSV) on
cycle days 11-12, 16-17 and 21-23 in the natural cycle and on days 1, 5, 10, OPU
and ET during the subsequent IVF cycle. The reproducibility of uterine artery PI
measurement was assessed by calculation of the coeffi cient of variation (CV). CV
was calculated by dividing the within-subject variance by the population mean.
Variances required for the calculation of CV were estimated by ANOVA.
Study II
A total of 102 infertile women were studied on the day of ET during the IVF
cycle or replacement cycle for frozen-thawed embryo transfer. Of these women, 56
(55%) had tubal infertility, 13 (13%) endometriosis, 23 (22%) unexplained and 10
(10%) were multifactorial. The mean age (± SD) of women was 34.4 (± 3.8) years.
The uterine artery impedance (PI and RI) was prospectively evaluated one hour
before ET and the impedance was compared with obstetric outcome in the
conceptional cycles. Of the 111 cycles studied, 82 were fresh (IVF-ET) and 29
frozen-thawed embryo transfers. Of these frozen-thawed ET, 20 were performed in
natural cycles and nine in substitution cycles. In the substitution cycles, goserelin
acetate (Zoladex; Zeneca, Macclesfi eld, UK), estradiol valerate (Progynova; Schering
AG, Berlin, Germany) and natural micronized progesterone were administered.
The predictive value of uterine artery impedance measurement for spontaneous
abortion, ectopic pregnancy, multiple pregnancy, birthweight, relative birthweight
and obstetric complications (IUGR, pregnancy-induced hypertension, preterm
birth) was studied. Relative birthweight was calculated as the difference between
actual and expected birthweight (according to sex and pregnancy duration)/ SD of
expected birthweight.
44
The uterine artery blood fl ow was defi ned as good if the uterine artery PI was < 3.0
(Cacciatore et al. 1996a).
We studied 70 couples with unexplained infertility of over 2 years in duration
during 1988-1992, including 23 women with minimal endometriosis. The mean age
(± SD) of women was 31.3 (± 3.3 years, range 23-38). The average duration of
infertility was 4.8 (range 2-12) years. Couples were offered superovulation treatments
combined with IUI, DIPI or timed intercourse (totally 233 treatment cycles) and
most couples received 1-4 treatment cycles. The stimulation protocol, pregnancy
rate, pregnancy outcome and complications of treatment were analysed.
A follow-up study was carried out 6 (range 4-7) years later. Information regarding
all treatment and spontaneous pregnancies was collected. Obstetric outcome
(birthweight, rate of SGA (<-2 SD) infants and preterm births (<37 weeks), Apgar
scores, obstetric complications and congenital malformations) was compared in
spontaneous and treatment pregnancies. The long-term prognosis of fecundity was
determined.
Study V
Altogether 107 women with unexplained infertility and 118 clinical pregnancies
after treatment with IVF or ICSI during 1.1.1993-30.3.1999 were studied. These
pregnancies resulted in 90 deliveries, of which 69 were singleton, 20 twin and
one triplet. Twenty-eight pregnancies (23.7%) resulted in a spontaneous abortion.
The multiple pregnancy rate was 23.3%. Two different control groups for the
deliveries and infants were chosen from the Finnish Medical Birth Register (MBR).
One control group included spontaneous pregnancies leading to birth (comprising
445 women and 545 children), which was matched according to year of delivery,
woman’s age, parity, number of foetuses and area of residence (Southern Finland).
The other control group included all pregnancies after ART treatment leading to
birth in Southern Finland during the study period (2377 women and 545 children).
The following factors were studied: maternal background, use of antenatal care,
gestational age at birth, birthweight, pregnancy and delivery complications, mode of
delivery, major congenital anomalies, infant’s outcome and need for intensive care.
Studies III and IV

45
Ovarian stimulation and preparation of spermatozoa for IUI and DIPI
(Study III)
Clomiphene citrate 50-100 mg (on cycle days 3-7) and human menopausal
gonadotrophin 75-150 IU (on cycle days 8-10 or 5-8) was used for ovarian
stimulation. The number of follicles was examined on day 10-12 during stimulation
with transvaginal sonography. Typically hCG (Pregnyl) 5000-10000 IU was also
given when the diameter of the leading follicle was at least 17 mm. Semen was
prepared by swim-up using the husband’s semen. Sperm was gently centrifuged
in Ham’s F 10 medium (HF 10, Gibco, Grand Island, NY, USA) supplemented with
human serum albumin. The spermatozoa were injected in 0.5 ml of medium into
the uterine or peritoneal cavity. Insemination was usually performed on cycle day
13 or 14.
Ovarian stimulation for IVF and ICSI (Studies I, II, and V)
Most patients were treated with the long protocol for ovarian stimulation.
A standardized ovarian stimulation protocol for IVF was used in all cycles. After
pituitary down-regulation with a gonadotrophin-releasing hormone analogue,
buserelin (Suprecur, Hoechst) or nafarelin (Synarela, Syntex), administered
intranasally usually beginning on cycle day 21, suppression was confi rmed by
transvaginal sonography. Ovarian stimulation commenced with daily injections
of gonadotrophins/FSH (Puregon, Organon, Oss, The Netherlands, or Gonal-F,
Laboratories Serono, Aubonne, Switzerland). The cycle was monitored by repeated
serum oestradiol assays and vaginal ultrasounds. When two or more follicles were
≥17 mm in diameter, human chorionic gonadotrophin (hCG, Pregnyl, Organon or
Profasi, Laboratories Serono) was administered and OPU was performed 36-38 hours
later. Embryo transfer was performed two days after follicle aspiration and luteal
phase was supplemented with vaginally administered progesterone (Lugesteron,
Leiras, Tampere, Finland).
In Study V, the starting dose of FSH was 100 IU in 1.7%, 150 IU in 66.1%, 200 IU in
11.6%, 225 IU in 19.5% and 300 IU in 1.7% of cycles.
46
Follow-up of IVF and ICSI pregnancies (Studies I, II and V).
If the quantitative hCG in serum was found to be positive 12 days after ET, the fi rst
ultrasound examination was performed fi ve weeks after ET. A clinical pregnancy
was defi ned as a pregnancy showing a visible gestational sac upon the ultrasound
fi ve weeks after ET; no biochemical pregnancies were included in the studies. All
pregnancies were followed at antenatal care units. Women attended the screening
ultrasound for examination of foetal morphology in weeks 16-18. The pregnancies
were followed at the delivery hospital and included repeated clinical examinations,
measurement of maternal blood pressure, urinary analysis, cervical status, foetal
cardiotocography (usually after 30 weeks of pregnancy) and repeated ultrasound
examinations to assess foetal growth and bioprofi le.
Preterm delivery was defi ned as delivery before 37 completed weeks. Small for
gestational age was defi ned as a birthweight below -2 SD according to Finnish
birthweight standards adjusted for gestational age and sex (Pihkala et al. 1989).
Pregnancy-induced hypertension was defi ned as a blood pressure of ≥140/90
mmHg (after 20 weeks of gestation), an increase in systolic blood pressure of ≥30
mmHg or an increase in diastolic blood pressure of ≥15mmHg (Gifford et al. 1990).
A major congenital anomaly is defi ned as a signifi cant congenital structural
anomaly, chromosomal defect or congenital hypothyroidism involved in a birth
with congenital anomalies. This does not include hereditary diseases and other
diseases not associated with congenital anomalies, dysfunction of organs or
tissues, developmental disabilities, congenital infections, isolated minor dysmorphic
features, normal variations and common less signifi cant congenital anomalies, which
are included in the exclusion list utilized by the Finnish Malformation Register
(Stakes 2001).
The Finnish Medical Birth Register (MBR) is a statutory nation-wide register, which
includes information on maternal background, pregnancy, delivery and perinatal
outcome. The MBR was used to get information on pregnancies and deliveries
and to select the two control groups (Study V). Diagnoses of malformations were
verifi ed from the Finnish Malformation Register.

47
2. Hormonal assays
Estradiol was quantitated using the Immuno 1 analyser (Tarrytown, NY, USA).
The detection limit of the assay is 37 pmol/l. Total variation is <6% at
concentrations of 270-5300 pmol/l. For progesterone, Spectria Progesterone (125 I)
Radioimmunoassay (Farmos Diagnostica, Turku, Finland) was used. The inter-assay
CV is 7-9% at concentrations of 1.6-27 nmol/l.
In FET cycles, the luteinizing hormone (LH) surge was determined with home
urinary kits (Clearplan, Unipath Limited, Bedford, England) to detect ovulation,
and women began testing 3-4 days before expected ovulation.
HCG was analysed with an immunofl uorometric assay (DELFIA, Wallac, Turku,
Finland) 12 days after ET. Inter-assay CV is <10% in the concentration range of
1-5000 IU/l.
3. Ultrasound and Doppler assessment (Studies I and II).
The examination began with inspection of the uterus and measurement of
endometrial thickness in the antero-posterior dimension. The transducer was then
angled to the right and left of midline in the sagittal plane to examine the number
and size of follicles in the ovaries. The uterine vessels were located with colour
Doppler sonography and the ascending branch was identifi ed lateral to the cervix,
at the level of the internal os. A gate was placed over the vessel, the width of the
sample gate (2-3 mm) was adjusted according to the vessel diameter and a blood
velocity waveform was obtained. When the signals passing the gate returned, the
Doppler frequency shift echoes were converted electronically by a mathematical
technique and displayed as a Doppler shift versus time waveform. The PI was
calculated using three consecutive uniform heart beats and averaged. The mean
value of uterine artery PI and RI/PSV from both ascending uterine artery branches
was used in calculations.
Blood vessels in the subendometrial region were located using the Power Doppler
and colour Doppler techniques. Areas of maximum colour intensity were selected,
a Doppler range gate applied and the pulsed Doppler function activated to assess
48
blood fl ow velocity. Peak systolic blood fl ow velocity waveforms were detected. No
correction was made for insonation angle since the angle of insonation for small
vessels cannot be determined (Zaidi et al. 1995).
All measurements in Studies I and II were performed between 7 and 9 a.m.
using US equipment (model ATL HDI 5000, Seattle WA, USA, model 515A; Hitachi,
Tokyo, Japan, or model SS-2000; Aloka, Tokyo, Japan) with 5.0-6.5 MHz transvaginal
transducer. The high-pass Doppler fi lter was set at 100 Hz. The average duration of
the procedure was 30 minutes.
4. Statistical analysis
Statistical analysis of the data was performed using the Statistical Package for Social
Sciences (SPSS 8.0.1., Chicago, IL, USA) in Studies I-IV. The SAS statistical package
was used in Study V.
The shape of the frequency distribution of continuous variables was evaluated by
means of histograms to determine whether or not it had a normal (symmetrical)
or skewed distribution, and by using the Kolmogorov-Smirnov normality test. In
normal distributed data, differences between means of the variables were assessed
by Student’s t-test, and in data without normal distribution, differences between
medians were assessed by the Mann-Whitney U-test. In cases of categorical data,
statistical signifi cance of differences in frequency between groups or comparisons
between proportions were assessed using the Chi-square test. The Wilcoxon signed-
rank test and Pearson’s correlation coeffi cient were used to analyse associations
between variables measured from the same patient on different days. Group
comparisons were performed with Fisher’s exact test, test for relative proportions
and Chi-square test, which were also adjusted by the Bonferroni method.
The level of statistical signifi cance in all studies was defi ned as p<0.05.
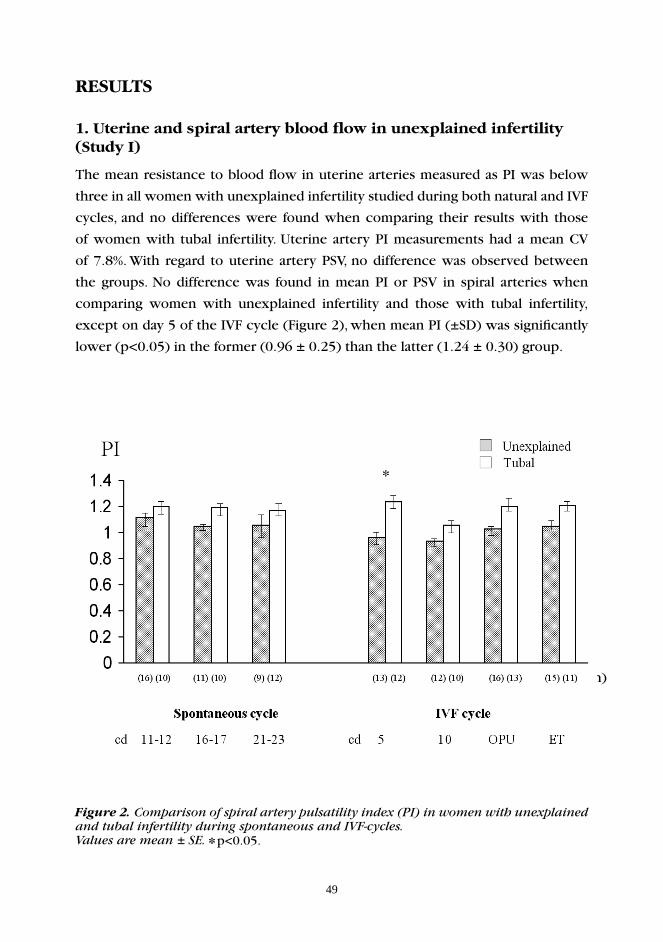
49
RESULTS
1. Uterine and spiral artery blood fl ow in unexplained infertility (Study I)
The mean resistance to blood fl ow in uterine arteries measured as PI was below
three in all women with unexplained infertility studied during both natural and IVF
cycles, and no differences were found when comparing their results with those
of women with tubal infertility. Uterine artery PI measurements had a mean CV
of 7.8%. With regard to uterine artery PSV, no difference was observed between
the groups. No difference was found in mean PI or PSV in spiral arteries when
comparing women with unexplained infertility and those with tubal infertility,
except on day 5 of the IVF cycle (Figure 2), when mean PI (±SD) was signifi cantly
lower (p<0.05) in the former (0.96 ± 0.25) than the latter (1.24 ± 0.30) group.
Figure 2. Comparison of spiral artery pulsatility index (PI) in women with unexplained and tubal infertility during spontaneous and IVF-cycles.
(n)
Values are mean ± SE. *p<0.05.
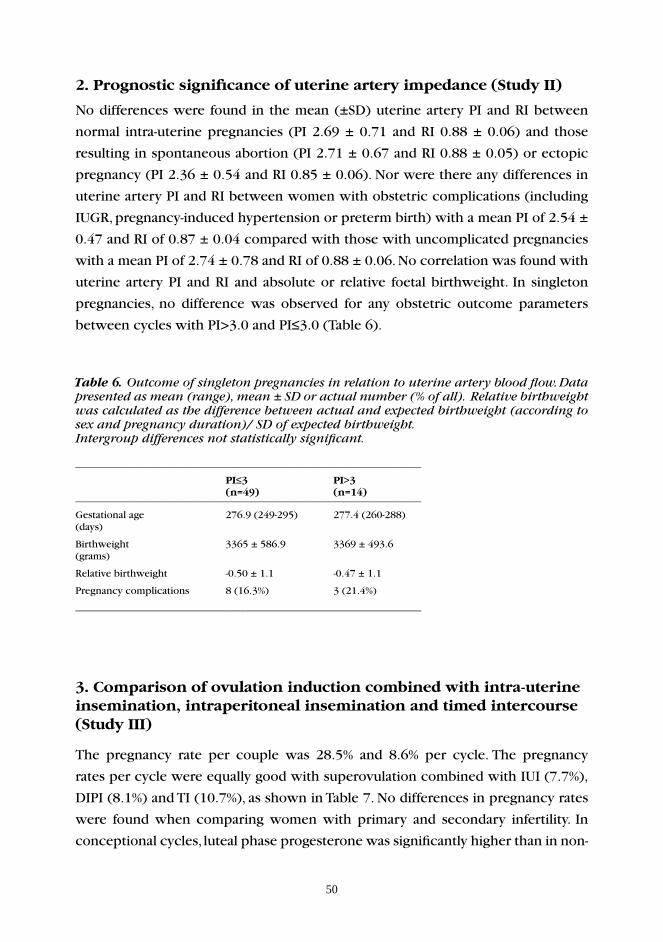
50
2. Prognostic signifi cance of uterine artery impedance (Study II)
No differences were found in the mean (±SD) uterine artery PI and RI between
normal intra-uterine pregnancies (PI 2.69 ± 0.71 and RI 0.88 ± 0.06) and those
resulting in spontaneous abortion (PI 2.71 ± 0.67 and RI 0.88 ± 0.05) or ectopic
pregnancy (PI 2.36 ± 0.54 and RI 0.85 ± 0.06). Nor were there any differences in
uterine artery PI and RI between women with obstetric complications (including
IUGR, pregnancy-induced hypertension or preterm birth) with a mean PI of 2.54 ±
0.47 and RI of 0.87 ± 0.04 compared with those with uncomplicated pregnancies
with a mean PI of 2.74 ± 0.78 and RI of 0.88 ± 0.06. No correlation was found with
uterine artery PI and RI and absolute or relative foetal birthweight. In singleton
pregnancies, no difference was observed for any obstetric outcome parameters
between cycles with PI>3.0 and PI≤3.0 (Table 6).
Table 6. Outcome of singleton pregnancies in relation to uterine artery blood fl ow. Data presented as mean (range), mean ± SD or actual number (% of all). Relative birthweight was calculated as the difference between actual and expected birthweight (according to sex and pregnancy duration)/ SD of expected birthweight.Intergroup differences not statistically signifi cant.
_________________________________________________________________
PI≤3 PI>3 (n=49) (n=14)_________________________________________________________________
Gestational age 276.9 (249-295) 277.4 (260-288)(days)
Birthweight 3365 ± 586.9 3369 ± 493.6(grams)
Relative birthweight -0.50 ± 1.1 -0.47 ± 1.1
Pregnancy complications 8 (16.3%) 3 (21.4%)
_________________________________________________________________
3. Comparison of ovulation induction combined with intra-uterine insemination, intraperitoneal insemination and timed intercourse (Study III)
The pregnancy rate per couple was 28.5% and 8.6% per cycle. The pregnancy
rates per cycle were equally good with superovulation combined with IUI (7.7%),
DIPI (8.1%) and TI (10.7%), as shown in Table 7. No differences in pregnancy rates
were found when comparing women with primary and secondary infertility. In
conceptional cycles, luteal phase progesterone was signifi cantly higher than in non-
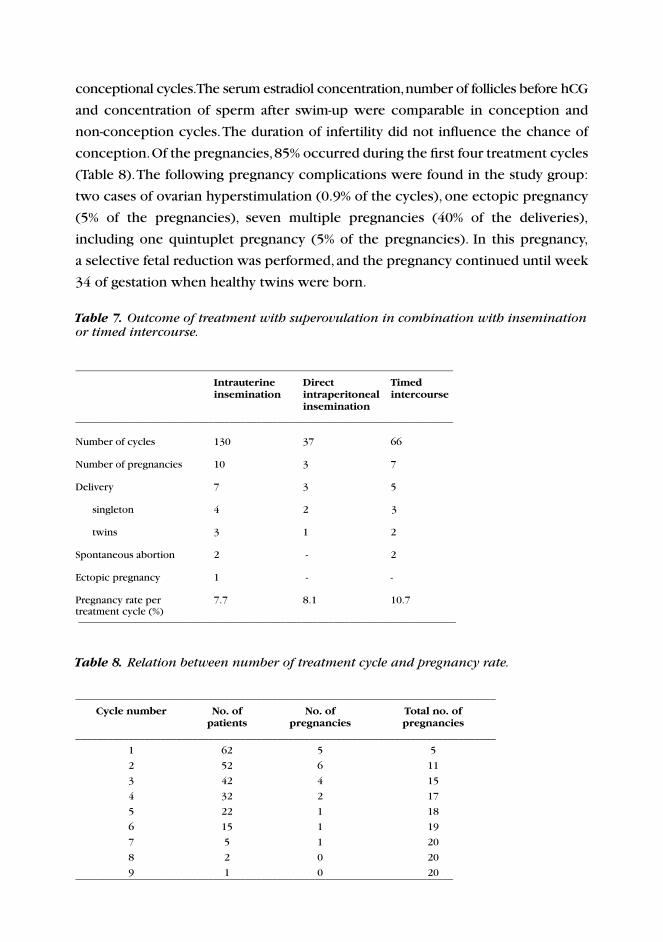
conceptional cycles. The serum estradiol concentration, number of follicles before hCG
and concentration of sperm after swim-up were comparable in conception and
non-conception cycles. The duration of infertility did not infl uence the chance of
conception. Of the pregnancies, 85% occurred during the fi rst four treatment cycles
(Table 8). The following pregnancy complications were found in the study group:
two cases of ovarian hyperstimulation (0.9% of the cycles), one ectopic pregnancy
(5% of the pregnancies), seven multiple pregnancies (40% of the deliveries),
including one quintuplet pregnancy (5% of the pregnancies). In this pregnancy,
a selective fetal reduction was performed, and the pregnancy continued until week
34 of gestation when healthy twins were born.
Table 7. Outcome of treatment with superovulation in combination with insemination or timed intercourse.
_______________________________________________________________________
Intrauterine Direct Timed insemination intraperitoneal intercourse insemination_______________________________________________________________________
Number of cycles 130 37 66
Number of pregnancies 10 3 7
Delivery 7 3 5
singleton 4 2 3
twins 3 1 2
Spontaneous abortion 2 - 2
Ectopic pregnancy 1 - -
Pregnancy rate per 7.7 8.1 10.7treatment cycle (%) _______________________________________________________________________
Table 8. Relation between number of treatment cycle and pregnancy rate.
_______________________________________________________________________________
Cycle number No. of No. of Total no. of patients pregnancies pregnancies_______________________________________________________________________________
1 62 5 5
2 52 6 11
3 42 4 15
4 32 2 17
5 22 1 18
6 15 1 19
7 5 1 20
8 2 0 20
9 1 0 20_______________________________________________________________________

52
4. Course of ART-induced and spontaneous pregnancies(Studies IV and V)
The treatment pregnancies in Study IV included pregnancies achieved with
ovulation induction alone or in combination with IUI/ DIPI or IVF. Table 9
shows the respective rates of spontaneous abortion, ectopic pregnancies and
multiple pregnancies. Among singletons, the mean gestational duration was 39.6
weeks in treatment-related pregnancies, which was similar to that of spontaneous
pregnancies. The mean birthweight (±SD) of singletons was 3120 g (± 488) in
treatment-related pregnancies and 3387 g (± 470) in spontaneous pregnancies
(p<0.05). Table 10 shows a comparison of perinatal outcome in spontaneous and
treatment-related singleton pregnancies. In singletons, no difference was observed
in the rate of preterm delivery or small-for-gestational-age babies. Among women
with treatment-related twins and those with spontaneous twins, 66.7% and 100%,
respectively, were delivered preterm (NS). The rates of congenital anomalies were
18.2% in treatment related and 10% in spontaneous pregnancies (NS).
After IVF/ ICSI treatment, the rate of spontaneous abortion was 23.7% (Study V).
The multiple pregnancy rate was 23.3%, and all but one were twin pregnancies.
One triplet pregnancy that resulted from a two-embryo transfer occurred, and the
children were born healthy in week 33 of gestation.
Among singleton pregnancies, no difference was found in the mean birthweight, rate
of low birthweight (<2500 g) or very low birthweight (<1500 g) when comparing
the study group and control groups, as shown in Table 11. Nor were differences
found in gestational duration, major congenital malformations or perinatal mortality
among the groups studied. However, among singletons in the study group, more
term breech presentations (10.1%) occurred as compared with both spontaneously
conceiving women and all IVF women (p<0.01). The rate of pregnancy-induced
hypertension was signifi cantly lower among singletons in the study group (p< 0.05)
compared with other IVF singletons. Among study group singletons, the rate of
Caesarean section was 24.6%, which was comparable with the rates of control
groups.
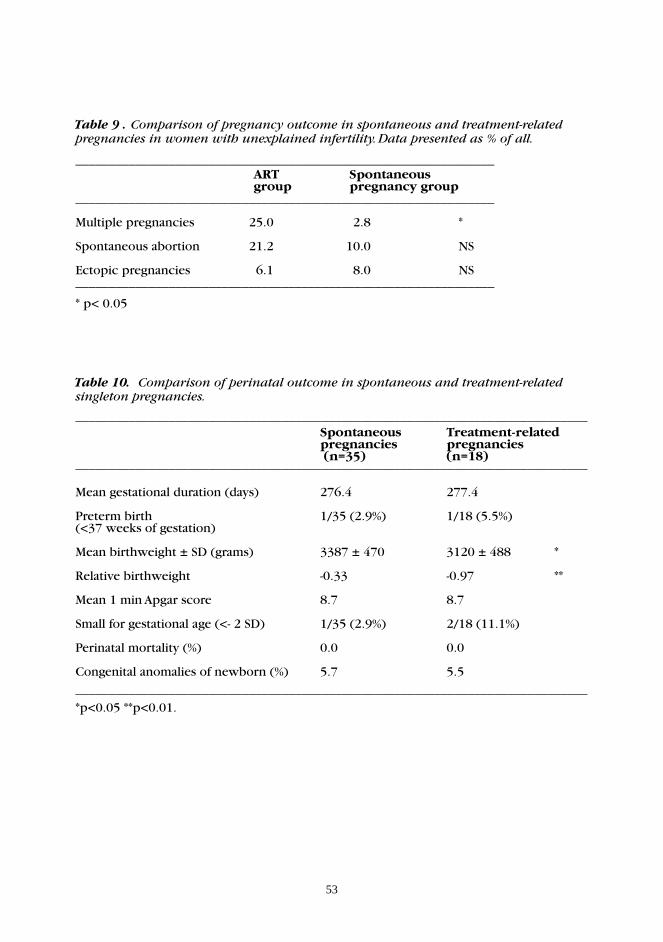
53
Table 9 . Comparison of pregnancy outcome in spontaneous and treatment-relatedpregnancies in women with unexplained infertility. Data presented as % of all.
_______________________________________________________________ ART Spontaneous group pregnancy group_______________________________________________________________
Multiple pregnancies 25.0 2.8 *
Spontaneous abortion 21.2 10.0 NS
Ectopic pregnancies 6.1 8.0 NS_______________________________________________________________
* p< 0.05
Table 10. Comparison of perinatal outcome in spontaneous and treatment-related singleton pregnancies.
_____________________________________________________________________________ Spontaneous Treatment-related pregnancies pregnancies (n=35) (n=18)_____________________________________________________________________________
Mean gestational duration (days) 276.4 277.4
Preterm birth 1/35 (2.9%) 1/18 (5.5%)(<37 weeks of gestation)
Mean birthweight ± SD (grams) 3387 ± 470 3120 ± 488 *
Relative birthweight -0.33 -0.97 **
Mean 1 min Apgar score 8.7 8.7
Small for gestational age (<- 2 SD) 1/35 (2.9%) 2/18 (11.1%)
Perinatal mortality (%) 0.0 0.0
Congenital anomalies of newborn (%) _____________________________________________________________________________
*p<0.05 **p<0.01.
5.7 5.5
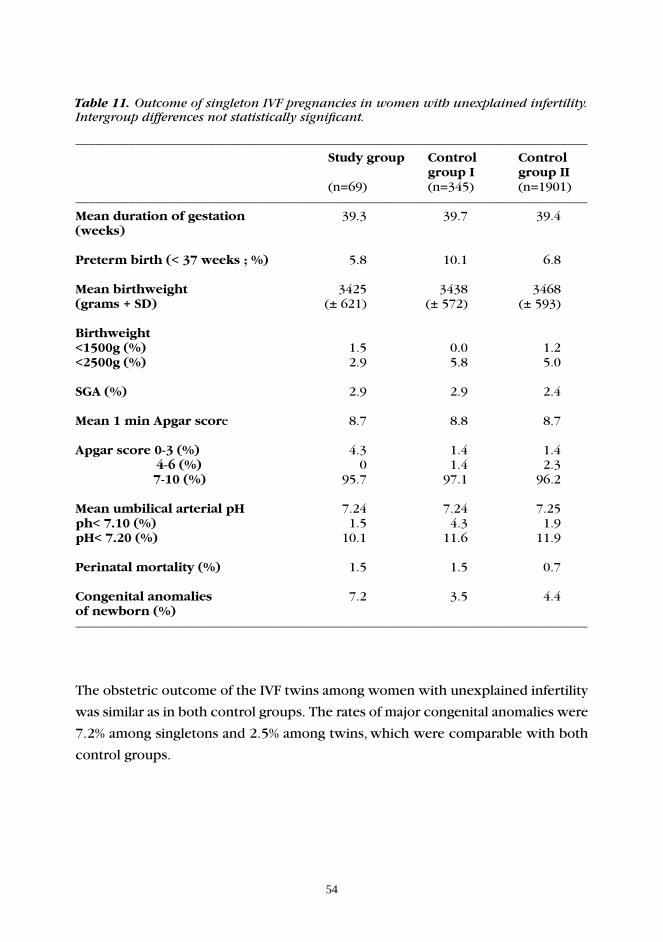
54
Table 11. Outcome of singleton IVF pregnancies in women with unexplained infertility. Intergroup differences not statistically signifi cant.
_____________________________________________________________________________
Study group Control Control group I group II (n=69) (n=345) (n=1901)_____________________________________________________________________________
Mean duration of gestation 39.3 39.7 39.4(weeks)
Preterm birth (< 37 weeks ; %) 5.8 10.1 6.8
Mean birthweight 3425 3438 3468(grams + SD) (± 621) (± 572) (± 593)
Birthweight<1500g (%) 1.5 0.0 1.2<2500g (%) 2.9 5.8 5.0
SGA (%) 2.9 2.9 2.4
Mean 1 min Apgar score 8.7 8.8 8.7
Apgar score 0-3 (%) 4.3 1.4 1.4 4-6 (%) 0 1.4 2.3 7-10 (%) 95.7 97.1 96.2
Mean umbilical arterial pH 7.24 7.24 7.25ph< 7.10 (%) 1.5 4.3 1.9pH< 7.20 (%) 10.1 11.6 11.9
Perinatal mortality (%) 1.5 1.5 0.7
Congenital anomalies 7.2 3.5 4.4of newborn (%)_____________________________________________________________________________
The obstetric outcome of the IVF twins among women with unexplained infertility
was similar as in both control groups. The rates of major congenital anomalies were
7.2% among singletons and 2.5% among twins, which were comparable with both
control groups.
55
VI DISCUSSION
1. Uterine and spiral artery impedance among women with unexplained infertility
Evidence suggests that uterine artery blood fl ow may be a factor affecting
successful implantation. Studies conducted among unselected infertile women both
in spontaneous and IVF cycles have shown poor implantation rates when the
uterine artery pulsatility index is over 3.0-3.3 or when there is an absence of end
diastolic velocities in the uterine artery Doppler velocity waveform (Coulam et al.
1994; Cacciatore et al. 1996a). All patients suffering from unexplained infertility
enrolled in our study had normal resistance to blood fl ow, i.e. PI below 3, at
all points during the spontaneous and IVF cycles. No differences in uterine
artery impedance were observed during the spontaneous or the IVF cycle when
women with unexplained and tubal infertility were compared. Therefore, under the
conditions of our study, uterine blood fl ow was not reduced among women with
unexplained infertility.
Some earlier studies have postulated that abnormal uterine perfusion might be
a contributing factor in unexplained infertility (Goswamy et al. 1988; Kupesic and
Kurjak 1993; Steer et al. 1994). Increased uterine artery impedance in midluteal
phase (Steer et al. 1994) and abnormal fl ow in spiral arteries have been suggested
as possible mechanisms for infertility in these women (Kupesic and Kurjak 1993).
But very few earlier studies have been conducted on uterine artery blood fl ow
among women with unexplained infertility. Steer and co-workers studied uterine
artery pulsatility index in 35 women with unexplained infertility as well as in
other subgroups of infertility. Limitations of their study were, however, that Dopper
assessments were only performed on day 21 of the unstimulated cycle and that
no evaluation of spiral artery impedance was conducted. The main results of their
study were in accord with our fi ndings; no signifi cant differences were observed in
the median PI for patients with different causes of infertility, although women in
all categories of infertility had signifi cantly higher PI than healthy women. Kupesic
and Kurjak (1993) investigated both natural and stimulated cycles, and also studied
spiral artery impedance, in contrast to the above-mentioned study. The spiral artery
PI was shown to be signifi cantly lower in unstimulated cycles than in hormonally
stimulated cycles. Limitations of this study were, however, that only patients with
male factor infertility were included as a study group and that ovarian stimulation
56
was performed with three different stimulation protocols: CC, CC combined with
hMG and hMG alone. Therefore, no direct comparison of results can be made
between their study and ours.
However, the results of Tinkanen and co-workers (1994) are in accord with our
results. In their study, the mean uterine artery PI was also normal among women
with unexplained infertility, both in the pre- and post-ovulatory period. In contrast
to our study, they showed that 15% of these women had a uterine artery PI over 2.8,
which was higher than among healthy women with no history of infertility. The use
of clomiphene citrate has also been shown to decrease the uterine blood fl ow in
the peri-implantation period among women with unexplained infertility (Hsu et al.
1995). In addition, another earlier study (Groutz et al. 1997) showed that the uterine
artery RI on day of hCG of the IVF cycle was signifi cantly higher in this patient
group as compared with women with tubal infertility. Our fi ndings differ slightly
from these studies. However, it is diffi cult to compare results because these studies
had different stimulation protocols and different days of Doppler measurement.
Furthermore, the information obtained from the study by Ziegler and co-workers
(1999) is limited because Doppler measurements were performed only among
healthy nulliparous women during natural cycles and they failed to measure spiral
artery impedance. Their study population also included both white and Asian
women. The study by Coulam and co-workers (1994), in addition to including IVF
cycles, also examined FET, COH, natural cycle-IUI and ovum donation cycles, and
therefore, their results are diffi cult to interpret. By contrast to the above studies,
our study protocol was new, with longitudinal evaluation of both uterine and spiral
artery impedance in women with unexplained infertility, with women with tubal
infertility serving as a control group.
Poor endometrial blood fl ow has in some studies predicted poor implantation
rate (Zaidi et al. 1995; Yang et al. 1999). Impedance to blood fl ow in the uterine
or spiral artery did not differ in women conceiving with IVF-ET compared with
the other women in our study. We did show that spiral artery PI on the 5th
day of gonadotrophin stimulation was signifi cantly lower among women with
unexplained infertility than among those with tubal infertility; however, on all
other days, the spiral artery impedance was comparable with the control group.
In addition, clinical pregnancy rates were comparable between these two groups:
57
40% for women with unexplained infertility and 33.3% for women with tubal
infertility, and therefore, it seems unlikely that the difference observed in spiral
artery impedance at the beginning of the IVF cycle would have clinical signifi cance.
We cannot exclude the possibility that this is a purely chance fi nding. As far as
we are aware, no earlier studies have focused on spiral artery impedance among
women with unexplained infertility. In conclusion, increased uterine or spiral
artery impedance is likely not an important factor in unexplained infertility since
no differences were found between the two study groups, neither during the
spontaneous nor during the IVF cycle, with the exception of day 5 of stimulation.
2. Prediction of pregnancy outcome with uterine artery impedance measurement
Comparing unexplained infertility and tubal infertility, we found no difference in
implantation rates during IVF treatment. Furthermore, no differences were present
in uterine or spiral artery impedance when comparing women who conceived with
IVF-ET with those who did not. Earlier studies are in concordance with this fi nding
(Tekay et al. 1995). However, this observation is in contrast to earlier fi ndings by
ourselves and other research groups, which show signifi cant differences in uterine
artery impedance between conception and non-conception cycles (Coulam et al.
1994; Tinkanen et al. 1994; Cacciatore et al. 1996a, 1996c). However, as all women
in our study had haemodynamic parameters within the normal range, this is not
a surprise. One reason for these fi ndings may be the limited size of the study
population.
This is the fi rst study in which preconceptional uterine blood fl ow and subsequent
pregnancy outcome have been related. Uterine artery PI and RI were unrelated to the
risk of spontaneous abortion or ectopic pregnancy. It seems that pre-implantation
uterine artery impedance does not infl uence trophoblast formation or placental
development. Uterine artery impedance was of no value in prediction of IUGR,
PIH or preterm birth among unselected infertile patients. Some studies have shown
that uterine and spiral artery resistance were lower at the end of the 5th week
in blighted ovum pregnancies (Alfi revic and Kurjak 1990), and the uterine artery
RI was lower in missed abortion compared with women with normal pregnancies
(Alfi revic and Kurjak 1990; Kurjak 1994). Uterine artery PI measurement at 12-13
weeks of gestation has been shown to predict subsequent hypertensive disorders,
58
SGA fetuses and gestational diabetes during pregnancy (van den Elzen et al. 1995).
However, uterine artery impedance measurements during the fi rst trimester in other
studies have not predicted pregnancy outcome (Frates et al. 1996). By contrast,
several studies show that the measurement of uterine artery blood fl ow in the
second and third trimesters may be valuable in predicting obstetric complications
(Strigini et al. 1995; Hofstaetter et al. 1996).
3. Treatment options of women with unexplained infertility
Ovulation induction in combination with insemination or timed intercourse was
an effective treatment for couples with unexplained infertility. The pregnancy rates
were equally good (7.7-10.7%) per cycle in all three treatment groups. Our results
are comparable with other studies reporting pregnancy rates of 8.7-15.3% per
cycle (Mascarenhas et al. 1994; Nuojua-Huttunen et al. 1999a; Sahakyan et al. 1999;
Goverde et al. 2000). Because the spontaneous pregnancy rate is 1-2% per cycle
among couples with unexplained infertility (Hughes et al. 2001), our ovulation
induction treatment must be considered satisfactory. No pregnancies began with
ovulation induction in the group of women aged over 36 years. The duration of
infertility did not infl uence the chance to conceive with this treatment. The majority
(85%) of the pregnancies began during the fi rst four treatment cycles, which is
in concordance with other studies (Nuojua-Huttunen et al. 1999a; Aboulghar et al
2001), reporting most pregnancies to occur within the fi rst three or four treatment
cycles. Several studies have demonstrated an improvement in pregnancy rates with
the addition of IUI to the ovulation induction protocol (Chaffkin et al. 1991; Guzick
et al. 1998), in contrast to our results. However, according to our fi ndings and other
studies no more than three to four ovulation induction cycles can be recommended
before proceeding to IVF (Aboulghar et al. 1999; Nuojua-Huttunen et al. 1999a;
Sahakyan et al. 1999; Goverde et al. 2000). The age of the woman is important
when deciding on the number of ovulation induction cycles and when selecting
the treatment schedule, consistent with other studies (Figure 3; Guzick et al. 1998;
Aboulghar et al. 1999; Sahakyan et al. 1999; Goverde et al. 2000). In the ovulation
induction cycles studied, the serum estradiol concentration, the number of follicles
and the concentration of sperm after swim-up were similar in conception and non-
conception cycles. The only predicting factor for conception appeared to be the
luteal phase progesterone concentration, which was signifi cantly higher in these
cycles.
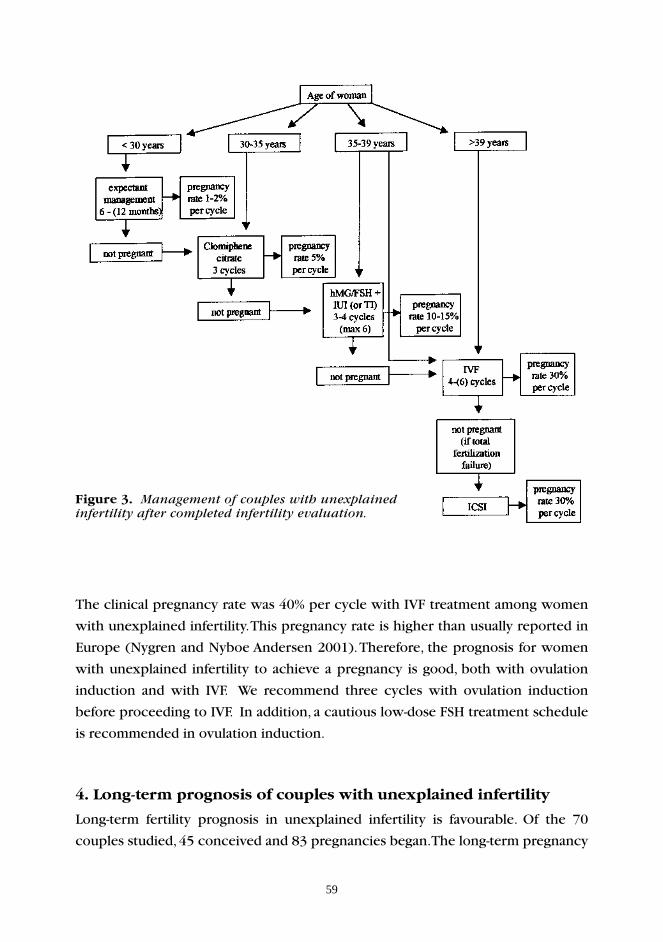
59
The clinical pregnancy rate was 40% per cycle with IVF treatment among women
with unexplained infertility. This pregnancy rate is higher than usually reported in
Europe (Nygren and Nyboe Andersen 2001). Therefore, the prognosis for women
with unexplained infertility to achieve a pregnancy is good, both with ovulation
induction and with IVF. We recommend three cycles with ovulation induction
before proceeding to IVF. In addition, a cautious low-dose FSH treatment schedule
is recommended in ovulation induction.
4. Long-term prognosis of couples with unexplained infertility
Long-term fertility prognosis in unexplained infertility is favourable. Of the 70
couples studied, 45 conceived and 83 pregnancies began. The long-term pregnancy
Figure 3. Management of couples with unexplained infertility after completed infertility evaluation.
60
rate was 64% per couple during the follow-up period and as many as 60% of the
pregnancies began spontaneously after completed ovulation induction treatment.
Of the women studied, 31% achieved two pregnancies or more during the follow-
up. Infertility treatment that resulted in pregnancy included IVF (n=10), CC (n=1),
ovulation induction combined with IUI (n=12), DIPI (n=3) and TI (n=7). These
fi ndings are in agreement with earlier life table analyses, which have shown that
many couples with unexplained infertility will ultimately conceive also without
treatment (Collins et al. 1983; Fish et al. 1989; Jaffe and Jewelewicz 1991). Duration
of infertility of more than three years has in several earlier studies been the
major negative prognostic factor (Levene et al. 1992; Crosignani et al. 1993), but
in our study, the duration of infertility did not infl uence the couple’s chances of
conception. The pregnancy rates were also equally good in women with primary
and secondary infertility. Therefore, many couples with unexplained infertility
do ultimately conceive but do so over a longer period of time than the fertile
population.
5. Obstetric outcome of couples with unexplained infertility
The rate of spontaneous abortion was similar with ovulation induction (20%) and
IVF (23.7%). The ectopic pregnancy rate was 5% after ovulation induction and 0%
after IVF, these fi gures being within the normal variation of rates reported earlier.
Multiple pregnancy rate was slightly higher after COH (30%) than after IVF (23.3%).
Our multiple pregnancy rate after COH was higher than in another report from
Finland, which claimed a multiple pregnancy rate of only 17% (Nuojua-Huttunen
et al. 1999b). However, the multiple pregnancy rate with IVF was similar to
other reports from Europe (Nygren and Nyboe Andersen 2001). The intensity
of stimulation used for COH is related to the multiple pregnancy rate. Our
treatment protocol for COH included CC combined with hMG, yielding mostly
5-6 preovulatory follicles. Today, low-dose FSH is preferred, which results in 1-2
preovulatory follicles. Milder stimulation protocols can achieve similar success rates
with a lower proportion of twins. Therefore, stimulation has become more cautious
in recent years, using lower doses of gonadotrophins. In our clinic, the multiple
pregnancy rate has also decreased since this study was conducted.
Only a few studies have been carried out to evaluate possible differences in
pregnancy complications in different infertility subgroups. Pregnancies achieved

61
with superovulation did not carry an increased risk of obstetric complications,
other than a slightly reduced birthweight and a relatively high rate of multiple
pregnancies. The malformation rate after COH seems higher than in another Finnish
report (Nuojua-Huttunen et al. 1999b). One reason for this difference might be
a different classifi cation of malformations. After IVF, no difference was observed
when comparing the malformation rates with the control groups. Moreover,
obstetric outcome of IVF pregnancies after unexplained infertility was good, with
no differences in mean birthweight, gestational duration, Caesarean section or
perinatal mortality when compared with the control groups. IVF twins had a
similar obstetric outcome as spontaneously conceived twins. This is in contrast
with a recent study showing that IVF twins had lower average birthweights than
spontaneously conceived twins (Koudstaal et al. 2000b). We found signifi cantly less
pregnancy-induced hypertension (0%) among singletons of the study group than
among other IVF pregnancies, and signifi cantly more term breech presentation
(10%) compared with both control groups; as far as we are aware, such fi ndings
have not been reported earlier. Another recent report showed an increased rate
of pre-eclampsia, placental abruption and preterm labour among women with
unexplained infertility, which is also in contrast to our results (Pandian et al. 2001).
Obstetric interventions, including Caesarean section and induction of labour, were
more common in their study. In addition, while an increased rate of IUGR has
been shown among women with unexplained infertility (Wang et al. 1994; Dawood
1996), our fi ndings do not support this. However, in pregnancies after ovulation
induction, the mean birthweight was lower than in spontaneous pregnancies. No
differences were observed after IVF treatment when mean birthweight, incidence
of low birthweight or very low birthweight babies among women with unexplained
infertility were compared with those of spontaneously conceived pregnancies.
Therefore, according to our results, the obstetric outcome of pregnancies among
women with unexplained infertility is promising and generally comparable with
spontaneous and ART pregnancies. The only factor affecting pregnancy outcome
adversely is the increased risk of multiple pregnancies after ART treatment, which
can be reduced by low-dose gonadotrophin stimulation and by the transfer of
a single embryo in IVF cycles.
62
VII SUMMARY AND CONCLUSIONS
1. Uterine artery and spiral artery impedance were low during both natural
and stimulated cycles in women with unexplained infertility and were
comparable with the results of women with tubal infertility. Therefore, under
the conditions of our study, uterine artery impedance does not appear to
be an important factor in the aetiology of unexplained infertility. Predicting
obstetric complications and outcome with measurement of uterine artery
impedance during IVF treatment was not possible. Pre-implantation uterine
artery impedance evidently has no infl uence on trophoblast formation or
placental development.
2. Treatment with superovulation combined with IUI, DIPI and TI were all good
treatment options for unexplained infertility, with similar pregnancy rates of
approximately 9% per treatment cycle and 28.5% per couple and limited
treatment complications.
3. The long-term pregnancy rate was good, with 64% of women conceiving;
the majority of pregnancies during follow-up began spontaneously. Expected
management can therefore be considered if the woman is young (<30 years)
and duration of infertility has been short (<2 years).
4. Obstetric outcome of IVF pregnancies, both singletons and twins, was good
among women with unexplained infertility. Birthweight, gestational duration
and major congenital malformation rates were comparable with those of
spontaneous pregnancies. Therefore, IVF treatment in this patient group seems
to be a good option when treatment with ovulation induction has failed.
The only factor affecting pregnancy outcome is an increased risk of multiple
pregnancies, which can be reduced by the transfer of a single embryo in
selected cases.
63
ACKNOWLEDGEMENTS
All studies of this thesis were carried out at the Department of Obstetrics and
Gynaecology, Helsinki University Central Hospital, during the years 1995-2002.
I wish to express my sincere gratitude to the Head of the Department of Obstetrics
and Gynaecology, Professor Olavi Ylikorkala, MD, PhD, to the Administrative Head
of the Department, Docent Maija Haukkamaa, MD, PhD, and to the former Head of
the Department, Professor Markku Seppälä, MD, PhD, for providing me with excellent
working facilities and for their support and interest in my research.
I am deeply grateful to Professor Olavi Ylikorkala for suggesting the topic of this
study and his generous advice. His support and encouragement have been essential
for fi nishing this study.
My sincere gratitude is due to my two supervisors:
Docent Aila Tiitinen, MD, PhD, for guiding me in scientifi c research and introducing
me to the fascinating fi elds of infertility and endocrinology, and for her insightful
comments and constructive criticism in preparing these manuscripts.
Docent Bruno Cacciatore, MD, PhD, for teaching me how to perform Doppler
measurements of uterine and spiral arteries, introducing me to ultrasound research
and providing valuable comments on my work.
Professors Jorma Paavonen, MD, PhD, and Carl Gustav Nilsson, MD, PhD, are warmly
acknowledged for continuous support and interest in my study.
I am very grateful to Professor Outi Hovatta, MD, PhD, Department of Obstetrics and
Gynaecology, Karolinska Institutet, Huddinge University Hospital, Stockholm, for
familiarizing me with the fi elds of infertility and IVF, for giving me the opportunity
to work at the IVF unit at Huddinge University Hospital in 1998, and for teaching
me about hormonal stimulations, oocyte pick-ups and embryo transfers in IVF.
I am most grateful to Docent Anne-Maria Suikkari, MD, PhD, and Docent Aydin Tekay,
MD, PhD, for carefully reviewing the fi nal manuscript.
64
My warmest thanks are due to Docent Mika Gissler, PhD, Leena Reinikainen, MD,
and Jarna Moilanen, MD, PhD, for helping me with the statistical analysis. Their
expertise and friendly co-operation are very much appreciated.
Docent Erja Halmesmäki, MD, PhD, is acknowledged for her valuable comments on
one of the manuscripts.
Laila Selkinen, Nina Hedkrok, Raili Alanne, Leena Vaara and Teija Karkkulainen are
thanked for their kind assistance in all manner of practical things.
All patients are gratefully acknowledged for volunteering for the time-consuming
ultrasound examinations that made this research possible.
I also wish to express a special thanks to all my friends and colleagues at the
Department of Obstetrics and Gynaecology, Helsinki University Central Hospital, for
companionship, friendly interest and support of my study. I thank all the midwives
and nurses at the Department for pleasant collaboration. I also thank my friends
outside the Clinic for their interest in my work.
Finally, my heartfelt thanks to my parents Mirjami and Erik Isaksson for standing
behind my decision to study medicine. I am very grateful to them and my sister
Kristina for ongoing support and love.
This study was supported by grants from the Helsinki University Central Hospital
Research Fund, Finska Läkaresällskapet, the Paulo Foundation for Medical Research,
the Clinical Research Institute of Helsinki University Central Hospital, the Perklen’s
Foundation for Medical Research, the Research Foundation of Orion Corporation
and the Finnish Foundation of Gynaecology and Obstetrics.
Helsinki, September 2002
Rita Isaksson
65
REFERENCES
Abdelmassih R, Sollia S, Moretto M, Acosta AA. Female age is an important parameter to predict treatment outcome in intracytoplasmic sperm injection. Fertil Steril 1996; 65: 573-577.
Aboulghar MA, Mansour RT, Serour GI, Amin Y, Abba AM, Salah IM. Ovarian superstimulation and intrauterine insemination for the treatment of unexplained infertility. Fertil Steril 1993; 60: 303-306.
Aboulghar MA, Mansour RT, Serour GI, Amin Y, Ramzy AM, Sattar MA, Kamal A. Management of long standing unexplained infertility. Am J Obstet Gynecol 1999; 181: 371-375.
Aboulghar M, Mansour R, Serour G, Abdrazek A, Amin Y, Rhodes C. Controlled ovarian hyperstimulation and intrauterine insemination for treatment of unexplained infertility should be limited to a maximum of three trials. Fertil Steril 2001; 75: 88-91.
Adamsson GD, Brzyski RG. Society for Assisted Reproductive Technology and American Society for Reproductive Medicine. Assisted reproductive techology in the United States: 1997 results generated from the American Society for Reproductive Medicine/ Society for Assisted Reproductive Technology Registry. Fertil Steril 2000; 74: 641-654.
Addor V, Santos-Eggimann B, Fawer C-L, Paccaud F, Calame A. Impact of infertility treatments on the health of newborns. Fertil Steril 1998; 69: 210-215.
Ahmad-Thabet SM. The fi mbrio-ovarian relation and its role on ovum picking in unexplained infertility: the fi mbrio-ovarian accessibility test. J Obstet Gynaecol Res 2000; 26: 65-70.
Alfi revic Z, Kurjak A. Transvaginal colour Doppler ultrasound in normal and abnormal early pregnancy. J Perinat Med 1990; 18: 173-180.
Alikani M, Cohen J, Tomkin G, Garrisi GJ, Mack C, Scott RT. Human embryo fragmentation in vitro and its implications for pregnancy and implantation. Fertil Steril 1999; 71: 836-842.
Allahbadia GN. Fallopian tubes and ultrasonogaphy: the Sion experience. Fertil Steril 1992; 58: 901-907.
Asch RH, Balmaceda JP, Ellsworth LR, Wong PC. Preliminary experience with gamete intrafallopian transfer (GIFT). Fertil Steril 1986; 45: 366-371.
Aytoz A, Van den Abbeel E, Bonduelle M, Camus M, Joris H, Van Steirteghem A, Devroey P. Obstetric outcome of pregnancies after the transfer of cryopreserved and fresh embryos obtained by conventional in-vitro fertilization and intracytoplasmic sperm injection. Hum Reprod 1999; 14: 2619-2624.
Barbieri RL. Infertility. In: Reproductive Endocrinology: physiology, pathophysiology, and clinical management. Yen, SSC, Jaffe RB, Barbieri RL, Eds. W.B. Saunders Company: Philadelphia, Pennysylvania, USA. 1999. PP 562-593.
Bassil S, Magritte JP, Roth J, Nisolle M, Donnez J, Gordts S. Uterine vascularity during stimulation and its correlation with implantation in in-vitro fertilization. Hum Reprod 1995; 10: 1497-1501.
Bassil S. Changes in endometrial thickness, width, length and pattern in predicting pregnancy outcome during ovarian stimulation in in vitro fertilization. Ultrasound Obstet Gynecol 2001; 18: 258-263.
Battaglia C, Artini PG, Bencini S, Bianchi R, D´Ambrogio G, Genazzani AR. Doppler analysis of uterine blood fl ow changes in spontaneous and medically menopause. Gynecol Endocrinol 1995; 9: 143-148.
Battaglia D, Goodwin P, Klein N, Soules M. Infl uence of maternal age on spindle assembly in oocytes from naturally cycling women. Hum Reprod 1996; 11:2217-2222.
66
Battaglia C, Sgarbi L, Salvatori M, Maxia N, Gallinelli A, Volpe A. Increased anticardiolipin antibodies are positively related to the uterine artery pulsatility index in unexplained infertility. Hum Reprod 1998; 13: 3487-3491.
Bergh T, Ericson A, Hillensjö T, Nygren K-G, Wennerholm U-B. Delivery and children born after in-vitro fertilisation in Sweden 1982-1995: a retrospective cohort study. Lancet 1999; 354: 1579-1585.
Bergere M, Lombroso R, Gombault M, Wainer R, Selva J. An idiopatic infertility with oocyte metaphase I maturation block. Hum Reprod 2001; 16: 2136-2138.
Bernasko J, Lynch L, Lapinski R, Berkowitz RL. Twin pregnancies conceived by assisted reproductive techniques: maternal and neonatal outcomes. Obstet Gynecol 1997; 89: 368-372.
Bewley S, Cooper D, Campbell S. Doppler investigation of uteroplacental blood fl ow resistance in the second trimester: a screening study for pre-eclampsia and uterine growth retardation. Br J Obstet Gynaecol 1991; 98: 871-879.
Blacker CM, Ginsburg KA, Leach RE, Randolph J, Moghissi KS. Unexplained infertility: evaluation of the luteal phase; results of the National Center for Infertility Research at Michigan. Fertil Steril 1997; 67: 437-442.
Bloechle M, Schreiner T, Lisse K. Recurrence of hydrosalpinges after transvaginal aspiration of tubal fl uid in an IVF cycle with development of a serometra. Hum Reprod 1997; 12: 703-705.
Boatman DE. Responses of gamete to oviductal environment. Hum Reprod 1997; 12: 133-149.
Bonduelle M, Wilikens A, Buysse A, Van Assche E, Wisanto A, Devroey P, Van Sterteghem AC. Prospective follow-up study of 877 children born after intracytoplasmic sperm injection (ICSI), with ejaculated epididymal and testicular spermatozoa and after replacement of cryopreserved embryos obtained after ICSI. Hum Reprod 1996; 11 (Suppl 4): 131-155.
Bonduelle M, Camus M, De Vos A, Staessen C, Tournaye H, Van Assche E, Verheyen G, Devroey P, Liebaers I, Van Steirteghem A. Seven years of intracytoplasmic sperm injection and follow-up of 1987 subsequent children. Hum Reprod 1999; 14 (Suppl 1), 243-264.
Bonduelle M, Liebaers I, Deketelaere V, Derde M-P, Camus M, Devroy P, Van Steirteghem A. Neonatal data on a cohort of 2889 infants born after ICSI (1991-1999) and of 2995 infants born after IVF (1983-1999). Hum Reprod 2002; 17: 671-694.
Bonilla-Musoles F, Marti MC, Ballester MJ, Raga F, Osborne NG. Normal uterine arterial blood fl ow in postmenopausal women assessed by transvaginal color Doppler sonography: the effect of hormone replacement therapy. J Ultrasound Med 1995; 14: 497-501.
Bustillo M, Yee B. Assisted reproductive technology in the United States: 1996 results generated from the American Society for Reproductive Medicine/ Society for Assisted Reproductive Technology Registry. Society for Assisted Reproductive Technology, The American Society for Reproductive Medicine. Fertil Steril 1999; 71: 798-807.
Buyalos RP, Daneshmand S, Brzechffa PR. Basal estradiol and follicle-stimulating hormone predict fecundity in women of advanced reproductive age undergoing ovulation induction therapy. Fertil Steril 1997; 68: 272-277.
Cacciatore B, Simberg N, Fusaro P, Tiitinen A. Transvaginal Doppler study of uterine artery blood fl ow in in vitro fertilization-embryo transfer cycles. Fertil Steril 1996a; 66: 130-134.
Cacciatore B, Tiitinen A. Does ovarian stimulation affect uterine artery impedance? J Assist Reprod Genet 1996b; 13: 15-18.
67
Cacciatore B. Transvaginal color Doppler assessment of uterine artery blood fl ow in in-vitro-fertilization cycles. In: Doppler in gynecology and infertility. Kurjak A, Kupesic S, Ed. Cic Edizioni Internali, Roma, Italy 1996c; PP 72-76.
Cahill DJ, Wardle PG, Maile LA, Harlow CR, Hull MG. Pituitary-ovarian dysfunction as a cause for endometriosis-associated and unexplained infertility. Hum Reprod 1995; 10, 3142-3146.
Campbell S, Bourne TH, Waterstone J, Reynolds KM, Crayford TJ, Jurkovic D, Okokon EV. Transvaginal color blood fl ow imaginig of the periovulatory follicle. Fertil Steril 1993; 60: 433-438.
Camus E, Poncelet C, Goffi net F, Wainer B, Merlet F, Nisand I, Philippe HJ. Pregnancy rates after in-vitro fertilization in cases of tubal infertility with and without hydrosalpinx: a meta-analysis of published comparative studies. Hum Reprod 1999; 14: 1243-1249.
Chaffkin LM, Nulsen JC, Luciano AA, Metzger DA. A comparative analysis of the cycle fecundity rates associated with combined human menopausal gonadotrophin (hMG) and intrauterine insemination (IUI) versus either hMG or IUI alone. Fertil Steril 1991; 55: 252-257.
Check JH, Nowroozi K, Choe J, Dietterich C. Infl uence of endometrial thickness and echogenic patterns on pregnancy rate during in vitro fertilization. Fertil Steril 1991; 56: 1173-1175.
Check JH, Lurie D, Callan C, Baker A, Benfer K. Comparison of the cumulative probability of pregnancy after in vitro fertilization-embryo transfer by infertility factor and age. Fertil Steril 1994; 61: 257-261.
Check JH, Chek ML, Katsoff D. Three pregnancies despite elevated serum FSH and advanced age. Hum Reprod 2000; 15: 1709-1712.
Chung CC, Fleming R, Jamieson ME, Yates RWS, Coutts JRT. Randomized comparison of ovulation induction with and without intrauterine insemination in the treatment of unexplained infertility. Hum Reprod 1995; 10: 3139-3141.
Cohen J. The effi ciency and effi cacy of IVF and GIFT. Hum Reprod 1991; 6: 613-618.
Collins JA, Wrixon W, Janes LB, Wilson EH. Treatment-independent pregnancy among infertile couples. N Engl J Med 1983; 309: 1201-1206.
Collins JA, Rowe TC. Age of the female partner is a prognostic factor in prolonged unexplained infertility: a multicenter study. Fertil Steril 1989; 52: 15-20.
Collins JA, Burrows EA, Willan AR. The prognosis for live birth among untreated infertile couples. Fertil Steril 1995; 64: 22-28.
Colpin H, Soenen S. Parenting and psychosocial development of IVF children: a follow-up study. Hum Reprod 2002; 17: 1116-1123.
Coulam CB, Bustillo M, Soenksen DM, Britten S. Ultrasonographic predictors of implantation after assisted reproduction. Fertil Steril 1994; 62: 1004-1010.
Coulam CB, Goodman C, Rinehart JS. Colour Doppler indices of follicular blood fl ow as predictors of pregnancy after in-vitro fertilization and embryo transfer. Hum Reprod 1999; 14: 1979-1982.
Crosignani PG, Walters DE, Soliani A. The ESHRE multicentre trial on the treatment of
Crosignani PG, Collins J, Cooke ID, Diczfalusy E, Rubin B. Unexplained infertility. Hum Reprod 1993; 8:
unexplained infertility: a preliminary report. Hum Reprod 1991; 6: 953-958.
977-980.
68
Crosignani PG, Rubin B. The ESHRE Capri Workshop. Guidlines to the prevalence, diagnosis, treatment and management of infertility. Hum Reprod 1996; 11: 1775-1807.
Csemiczky G, Landgren BM, Fried G, Wramsby H. High tubal damage grade is associated with low pregnancy rate in women undergoing in-vitro fertilization treatment. Hum Reprod 1996; 11: 2438-2440.
Dawood MY. In vitro fertilization, gamete intrafallopian transfer, and superovulation with intrauterine insemination: Effi cacy and potential health hazards on babies delivered. Am J Obstet Gynecol 1996; 174: 1208-1217.
De Geyter C, Schmitter M, De Geyter M, Nieschlag E, Holzgreve W, Schneider HP. Prospective evaluation of the ultrasound appearance of the endometrium in a cohort of 1186 infertile women. Fertil Steril 2000; 73: 106-113.
Dellenbach P, Nisand I, Moreau L, Feger B, Plumere C, Gerlinger P, Brun B, Rumpler Y. Transvaginal sonographically controlled ovarian follicle puncture for egg retrieval. Lancet 1984; i: 1467.
Devreker F, Pogonici E, De Maertelaer V, Revelard P, Van den Bergh M, Englert Y. Selection of good embryos for transfer depends on embryo cohort size: implications for the ’mild ovarian stimulation’ debate. Hum Reprod 1999; 14: 3002-3008.
de Ziegler D, Bessis R, Frydman R. Vascular resistance of the uterine arteries: physiological effects of estradiol and progesterone. Fertil Steril 1991; 55: 775-779.
Dickey RP, Hower JF, Matulich EM, Brown GT. Effect of standing on non-pregnant uterine blood fl ow. Ultrasound Obstet Gynecol 1994; 4: 480-487.
Dickey RP. Doppler ultrasound investigation of uterine and ovarian blood fl ow in infertility and early pregnancy. Hum Reprod 1997; 3: 467-503.
Donderwinkel PF, van der Vaart H, Wolters VM, Simons AH, Kroon G, Heineman M-J. Treatment of patients with longstanding unexplained infertility with in vitro fertilization. Fertil Steril 2000; 73: 334-337.
Dor J, Seidman DS, Ben-Shlomo I, Levran D, Ben-Rafael Z, Mashiach S. Cumulative pregnancy rate following in-vitro fertilization: the signifi cance of age and infertility aetiology. Hum Reprod 1996; 11: 425-428.
Doyle P, Beral V, Maconochie N. Preterm delivery, low birthweight and small-for-gestational-age in liveborn singleton babies resulting from in-vitro fertilization. Hum Reprod 1992; 7: 425-428.
Eimers JM, te Velde ER, Gerritse R, Vogelzang ET, Looman CW, Habbema JD. The prediction of the chance to conceive in subfertile couples. Fertil Steril 1994; 61: 44-52.
Engmann L, Maconochie N, Tan SL, Bekir J. Trends in the incidence of births and multiple births and the factors that determine the probability of multiple birth and IVF treatment. Hum Reprod 2001; 16: 2598-2605.
Ericson A, Källén B. Congenital malformations in infants born after IVF: a population-based study. Hum Reprod 2001; 16: 504-509.
Ericson A, Nygren KG, Otterblad Olausson P, Källén B. Hospital care utilization of infants born after IVF. Hum Reprod 2002; 17: 929-932.
Esterhuizen AD, Franken DR, Lourens JG, van Rooyen LH. Clinical importance of zona pellucida-induced acrosome reaction and its predictive value for IVF. Hum Reprod 2001; 16: 138-144.
69
Favre R, Bettahar K, Grange G, Ohl J, Arbogast E, Moreau L, Dellenbach P. Predictive value of transvaginal uterine doppler assessment in an in vitro fertilization program. Ultrasound Obstet Gynecol 1993; 4: 350-353.
Fisch P, Casper RF, Brown SE, Wrixon W, Collins JA, Reid RL, Simpson C. Unexplained infertility: evaluation of treatment with clomiphene citrate and human chorionic gonadotropin. Fertil Steril 1989; 51: 828-833.
Forti G, Krausz C. Clinical review 100: Evaluation and treatment of the infertile couple. J Clin Endocrinol Metab 1998; 83: 4177-4188.
Frates MC, Doubilet PM, Brown DL, Benson CB, DiSalvo DN, Laing FC, Berck DJ, Hill JA. Role of doppler
abortion. J Ultrasound Med 1996; 15: 557-562.
Friedler S, Schenker JG, Herman A, Lewin A. The role of ultrasonography in evaluation of endometrial receptivity following assisted reproductive treatment: a critical review. Hum Reprod Update 1996; 2: 323-335.
Gabrielsen A, Petersen K, Mikkelsen AL, Lindenberg S. Intracytoplasmic sperm injection does not overcome an oocyte defect in previous fertilization failure with conventional in-vitro fertilization and normal spermatozoa. Hum Reprod 1996; 11: 1963-1965.
Garcia-Velasco JA, Arici A. Is the endometrium or oocyte/embryo affected in endometriosis? Hum Reprod 1999; 14 (Suppl 2): 77-89.
Gerris J, De Neubourg D, Mangelschots K, Van Royen E, Van de Meerssche M, Valkenburg M. Prevention of twin pregnancy after in-vitro fertilization or intracytoplasmic sperm injection based on strict embryo criteria: a prospective randomized clinical trial. Hum Reprod 1999; 14: 2581-2587.
Gerris J, Van Royen E. Avoiding multiple pregnancies in ART. A plea for single embryo transfer. Hum Reprod 2000; 15: 1884-1888.
Geva E, Amit A, Lerner-Geva L, Lessing JB. Autoimmunity and reproduction. Fertil Steril 1997; 67: 599-611.
Gifford RW, August P, Chesley LC, Cunningham G, Ferris TF, Lindheimer MD, Redman CWG, Roberts JM, Zuspan FP, Horan MJ. National high blood pressure education program working group report on high blood pressure in pregnancy. Am J Obstet Gynecol 1990; 163: 1689-1712.
Gissler M, Tiitinen A. IVF treatments and their outcomes in Finland in the 1990s. Acta Obstet Gynecol Scand 2001; 80: 937-944.
Glatstein IZ, Best CL, Palumbo A, Sleeper LA, Friedman AJ, Hornstein MD. The reproducibility of the postcoital test. Obstet Gynecol 1995; 85: 396-400.
Goswamy RK, Williams G, Steptoe PC. Decreased uterine perfusion -a cause of infertility. 3: 955-959.
Govaerts I, Koenig I, Van den Bergh M, Bertrand E, Revelard P, Englert Y. Is intracytoplasmic sperm injection (ICSI) a safe procedure? What do we learn from early pregnancy data about ICSI? Hum Reprod 1996; 11: 440-443.
Goverde AJ, McDonnell J, Vermeiden JPW, Schats R, Rutten FFH, Schoemaker J. Intrauterine insemination or in-vitro fertilisation in idiopatic subfertility and male subfertility: a randomised trial and cost-effectiveness analysis. Lancet 2000; 355: 13- 18.
ultrasonography in the prediction of pregnancy outcome in women with recurrent spontaneous
Hum Reprod 1988;
70
Griffi ths TA, Murdoch AP, Herbert M. Embryonic development in vitro is compromised by the ICSI procedure. Hum Reprod 2000; 15: 1592-1596.
Groutz A, Wolman I, Jaffa AJ, Lessing JB, Yovel I, Amit A. Infl uence of ovulation induction with human menopausal gonadotropin on uterine blood fl ow. J Ultrasound Med 1997; 16: 455-58.
Gürgan T, Urman B, Yarali H, Kisnisci HA. The results of in vitro fertilization-embryo transfer in couples with unexplained infertility failing to conceive with superovulation and intrauterine insemination. Fertil Steril 1995; 64: 93-97.
Guzic DS, Grefenstette I, Baffone K, Berga SL, Krasnow JS, Stovall DW, Naus GJ. Infertility evaluation in fertile women: a model for assessing the effi cacy of infetility testing. Hum Reprod 1994; 9: 2306-2310.
Guzic DS, Sullivan MW, Adamson GD, Cedars MI, Falk RJ, Peterson EP, Steinkampf MP. Effi cacy of treatment for unexplained infertility. Fertil Steril 1998; 70: 207-213.
Hansen M, Kurinczuk JJ, Bower C, Webb S. The risk of major birth defects after intracytoplasmic sperm injection and in vitro fertilization. N Engl J Med 2002; 346: 725-730.
Hardarson T, Hanson C, Sjögren A, Lundin K. Human embryos with unevenly sized blastomeres have lower pregnancy and implantation rates: indications for aneuploidy and multinucleation. Hum Reprod 2001; 16: 313-318.
Harman C. Doppler Ultrasound: Maternal applications. In: Sonography in Obstetrics and Gynecology. Principles and Practice. Fleischer AC, Manning FA, Jeahty P, Romero R, Ed. Fifth Edition. Prentice-Hall International Inc; London, UK, 1995, pp 223-249.
Harrington K, Cooper D, Lees C, Hecher K, Campbell S. Doppler ultrasound of the uterine arteries: the importance of bilateral notching in the prediction of pre-eclampsia, placental abruption or delivery of a small-for-gestation-age baby. Ultrasound Obstet Gynecol 1996; 7: 182-188.
Harrison K, Sherring D, Keeping J. Repeated maturation block. J Assist Reprod Genet 2000; 17: 231-233.
Heikkinen H, Tekay A, Volpi E, Martikainen H, Jouppila P. Transvaginal salpingosonography for the assessment of tubal patency in infertile women: methodological and clinical experiences. Fertil Steril 1995; 64: 293-298.
Henriksen TB, Baird DD, Olsen J, Hedegaard M, Secher NJ, Wilcox AJ. Time to pregnancy and preterm delivery. Obstet Gynecol 1997; 89: 594-599.
Hock DL, Bohrer MK, Ananth CV, Kemmann E. Sonographic assessment of endometrial pattern and thickness in patients treated with clomiphene citrate, human menopausal gonadotropins, and intrauterine insemination. Fertil Steril 1997; 68: 242-245.
Hofstaetter C, Dubiel M, Gudmundsson S, Marsal K. Uterine artery color Doppler assisted velocimetry and perinatal outcome. Acta Obstet Gynecol Scand 1996; 75: 612-619.
Hovatta O, Kurunmäki H, Tiitinen A, Lähteenmäki P, Koskimies A. Direct intraperitoneal or intrauterine insemination and superovulation in infertility treatment: a randomized study. Fertil Steril 1990; 54: 339-341.
Hsu C-C, Kuo H-C, Wang S-T, Huang K-E. Interference with uterine blood fl ow by clomiphene citrate in women with unexplained infertility. Obstet Gynecol 1995; 86: 917-921.
Hughes E, Collins J, Vandekerckhove P. Clomiphene citrate for unexplained subfertility in women (Cochrane Review). In: The Cochrane Library, Issue 4, 2001. Oxford: Update Software.

71
Hull MGR, Glazener CMA, Kelly NJ, Conway DI, Foster PA, Hinton RA, Coulson C, Lambert PA, Watt EM,
Hull MG, Armitage RJ, McDermott A. Use of follicle-stimulating hormone alone (urofollitropin) to stimulate the ovaries for assisted conception after pituitary desensitization. Fertil Steril 1994; 62: 977-1003.
Hull MGR, Williams JAC, Ray B, McLaughlin EA, Akande VA, Ford WCL. The contribution of subtle oocyte or sperm dysfunction affecting fertilization in endometriosis-associated or unexplained infertility: a controlled comparison with tubal infertility and use of donor spermatozoa. Hum Reprod 1998; 13: 1825-1830.
Jaffe SB, Jewelewicz R. The basic infertility investigation. Fertil Steril 1991; 56: 599-613.
Johnson MD. Genetic risk of intracytoplasmic sperm injection in the treatment of male infertility: recommendations for genetic counseling and screening. Fertil Steril 1998; 70: 397-411.
Järvelä I, Raudaskoski T, Tekay A, Jouppila P. Effect of the levonorgestrel-relasing intrauterine system on the uterine artery pulsatility index in postmenopausal hormone replacement therapy. Ultrasound Obstet Gynecol 1997; 10: 350-355.
Järvelä I, Tekay A, Jouppila P. The effect of a copper-intrauterine device on the uterine artery blood fl ow in regularly menstruationg women. Hum Reprod 1998a; 13: 1841-1845.
Järvelä I, Tekay A, Jouppila P. The effect of a levonorgestrel-releasing intrauterine system on the uterine artery blood fl ow, hormone levels and ovarian cyst formation in fertile women. Hum Reprod 1998b; 13: 3379-3383.
Järvelä I. Intrauterine devices and blood fl ow impedance in the uterine arteries. A transvaginal colour Doppler ultrasonographic study. Thesis. University of Oulu, 1998c.
Kelly SM, Sladkevicius P, Campbell S, Nargund G. Investigation of the infertile couple: a one-stop ultrasound-based approach. Hum Reprod 2001; 16: 2481-2484.
Klentzeris LD. The role of endometrium in implantation. Hum Reprod 1997; 12 (suppl 11): 170-175.
Koivurova S, Hartikainen A-L, Gissler M, Hemminki E, Sovio U, Järvelin M-R. Neonatal outcome and congenital malformations in children born after in-vitro fertilization. Hum Reprod 2002; 17: 1391-1398.
Koskimies AI, Tenhunen A, Ylöstalo P, Liukkonen S, Widholm O, Seppälä M. The in vitro fertilization program in Helsinki. J In Vitro Fert Embryo Transf 1984; 1: 208-209.
Koudstaal J, Braat DDM, Bruinse HW, Naaktgeboren N, Vermeiden JPW, Visser GHA. Obstetric outcome of singleton pregnancies after IVF: a matched control study in four Dutch university hospitals. Hum Reprod 2000a; 15: 1819-1825.
Koudstaal J, Bruinse HW, Helmerhorst FM, Vermeiden JPW, Willemsen WNP, Visser GHA. Obstetric outcome of twin pregnancies after in-vitro fertilization: A matched control study in four Dutch University Hospitals. Hum Reprod 2000b; 15: 935-940.
Kundsin RB, Falk L, Hertig AT, Horne HW. Acyclovir treatment of twelve unexplained infertile couples. Int J Fertil 1987; 32: 200-204.
Kupesic S, Kurjak A. Uterine and ovarian perfusion during the preovulatory period assessed by transvaginal color Doppler. Fertil Steril 1993; 60: 439-443.
Kupesic S, Kurjak A, Pasalic L, Benic S, Ilijas M. The value of transvaginal color Doppler in the assessment of pelvic infl ammatory disease. Ultrasound Med Biol 1995; 21: 733-738.
Desai KM. Population study on causes, treatment, and outcome of infertility. BMJ 1985; 304: 1693-1697.
72
Kupesic S. The fi rst three weeks assessed by transvaginal color Doppler. J Perinat Med 1996a; 24: 301-317.
Kupesic S. Transvaginal color Doppler in the assessment of infertility. In:Doppler in gynecology and infertility. Kurjak A, Kupesic S, Ed. Cic Edizioni Internali, Roma, Italy 1996b, PP 13-21.
Kupesic S, Bekavac I, Bjelos D, Kurjak A. Assessment of endometrial receptivity by transvaginal
fertilization procedures. J Ultrasound Med 2001; 20: 125-134.
Kupesic S, Kurjak A. Predictors of IVF outcome by three-dimensional ultrasound. Hum Reprod 2002; 17: 950-955.
Kurdi W, Campbell S, Aquilina J, England P, Harrington K. The role of color Doppler imaging of the uterine arteries at 20 weeks’ gestation in stratifying antenatal care. Ultrasound Obstet Gynecol 1998; 12: 339-345.
Kurjak A, Kupesic-Urec S, Schulman H, Zalud I. Transvaginal color fl ow Doppler in assessment of ovarian and uterine blood fl ow in infertile women. Fertil Steril 1991; 56: 870-873.
Kurjak A, Kupesic S. Ovarian senescence and its signifi cance on uterine and ovarian perfusion. Fertil Steril 1995; 64: 532-537.
Lacin S, Vatansever S, Kuscu NK, Koyuncu F, Ozbilgin K, Ceylan E. Clomiphene citrate does not affect the secretion of 3, V and ß1 integrin molecules during the implantation window in patients with unexplained infertility. Hum Reprod 2001; 16: 2305-2309.
Lancaster PAL. Congenital malformations after in vitro fertilization. Lancet 1987; ii: 1392-1393.
Lancaster P, Shafi r E, Huang J. Assisted Conception Australia and New-Zealand 1992 and 1993. AIHW National Perinatal Statistics Unit Sydney 1995; 1: 1-71.
Lansac J. Delayed parenting. Is delayed childbearing a good thing? Hum Reprod 1995; 10: 1033-1035.
Lass A, Skull J, McVeigh E, Margara R, Winston RML. Measurement of ovarian volume by transvaginal sonography before ovulation induction with human menopausal gonadotropin for in-vitro fetilization can predict poor response. Hum Reprod 1997; 12: 294-297.
Leach RE, Moghissi KS, Randolph JF, Reame NE, Blacker CM, Ginsburg KA, Diamond MP. Intensive hormone monitoring in women with unexplained infertility: evidence for subtle abnormalities suggestive of diminished ovarian reserve. Fertil Steril 1997; 68: 413-420.
Lessey BA, Castelbaum AJ, Sawin SW, Sun J. Integrins as markers of uterine receptivity in women with primary unexplained infertility. Fertil Steril 1995; 63: 535-542.
Lessing JB, Amit A, Barak Y, Kugosowski A, Gruber A, Yovel I, David MP, Peyser MR. The performance of primary and secondary unexplained infertility in an in vitro fertilization-embryo transfer program. Fertil Steril 1988; 50: 903-905.
Levene MI, Wild J, Steer P. Higher multiple births and modern management of infertility in Britain. The British Association of Perinatal Medicine. Br J Obstet Gynaecol 1992; 99: 607-613.
Li TC, Lenton EA, Dockery P, Cook ID. A comparison of some clinical and endocrinological features between cycles with normal and defective luteal phases in women with unexplained infertility. Hum Reprod 1990; 5: 805-810.
Kurjak A. Transvaginal color Doppler in early pregnancy. J Perinat Med 1994; 22 (Suppl 1): 189-192.
colour Doppler and three-dimensional power Doppler ultrasonography in patients undergoing in vitro
73
Lilford RJ, Dalton M. Effectiveness of treatment for infertility. BMJ 1987; 295: 155-156.
Lim T, Tsakok FH. Age related decline in fertility: a link to degenerative oocytes? Fertil Steril 1997; 68: 265-271.
Liu DY, Baker HWG. Defective sperm-zona pellucida interaction: a major cause of failure of fertilization in clinical in-vitro fertilization. Hum Reprod 2000; 15: 702-708.
Luborsky J, Llanes B, Davies S, Binor Z, Radwanska E, Pong R. Ovarian autoimmunity: greater prevalence of auto-antibodies in premature menopause and unexplained infertility than in the general population. Clin Immunol 1999; 90: 368-374.
Luborsky J, Llanes B, Roussev R, Coulam C. Ovarian antibodies, FSH and inhibin B: independent markers associated with unexplained infertility. Hum Reprod 2000; 15: 1046-1051.
Ludwig M, Riethmuller-Winzen H, Felberbaum RE, Olivennes F, Albano C, Devroey P, Diedrich K. Health of 227 children born after controlled ovarian stimulation for in vitro fertilization using the luteinizing hormone-releasing hormone antagonist cetrorelix. Fertil Steril 2001; 75: 18-22.
Lundin K, Bergh C, Hardarson T. Early embryo cleavage is a strong indicator of embryo quality in human IVF. Hum Reprod 2001; 16: 2652-2657.
Macas E, Imthurn B, Keller PJ. Increased incidence of numerical chromosome abnormalities in spermatozoa injected into human oocytes by ICSI. Hum Reprod 2001; 16: 115-120.
Magarelli PC, Pealstone AC, Buyalos RP. Discrimination between chronological and ovarian age in infertile women aged 35 years and older: predicting pregnancy using basal follicle stimulating hormone, age and number of ovulation induction/ intra-uterine insemination cycles. Hum Reprod 1996; 11: 1214-1219.
Maman E, Lunenfeld E, Levy A, Vardi H, Potashnik G. Obstetric outcome of singleton pregnancies conceived by in vitro fertilization and ovulation induction compared with those conceived spontaneously. Fertil Steril 1998; 70: 240-245.
Marcus S, Brisden P. Analysis of the incidence and risk factors associated with ectopic pregnancy following in-vitro fertilization and embryo transfer. Hum Reprod 1995; 10: 199-203.
Mascarenhas L, Khastgir G, Davies WAR, Lee S. Superovulation and timed intercourse: can it provide a reasonable alternative for those unable to afford assisted conception? Hum Reprod 1994; 9: 67-70.
Meldrum DR, Chetkowski RJ, Steingold KA, Randle D. Transvaginal ultrasound scanning of ovarian follicles. Fertil Steril 1984; 42: 803-805.
Meloni GF, Dessole S, Tomasi PA, Musumeci S. The prevalence of coelic disease in infertility. Hum Reprod 1999; 14: 2759-2761.
Miller JH, Weinberg RK, Canino NL, Klein NA, Soules MR. The pattern of infertility diagnoses in women of advanced reproductive age. Am J Obstet Gynecol 1999; 181: 952-957.
Minakami H, Sayama M, Honma Y, Matsubara S, Koike T, Sato I, Uchida A, Eguchi Y, Momoi M, Araki S. Lower risks of adverse outcome in twins conceived by artifi cial reproductive techniques compared with sponataneous conceived twins. Hum Reprod 1998; 13: 2005-2008.
predictive of successful live births in in vitro fertilization (IVF) suggests strategies to improve IVF outcome. J Assist Reprod Genet 1998; 15: 365-371.
Moise J, Laor A, Armon Y, Gur I, Gale R. The outcome of twin pregnancies after IVF. Hum Reprod 1998; 13; 1702-1705.
Minaretzis D, Harris D, Alper MM, Mortola JF, Berger MJ, Power D. Multivariate analysis of factors
74
Mueller BA, Daling JR. Epidemiology of infertility. In: Controversies in Reproductive Endocrinology and Infertility. Soules MR, Ed. Elsevier, New York, USA, 1989.
Murakoshi T, Sekizuka N, Takakuwa K, Yoshizawa H, Tanaka K. Uterine and spiral artery fl ow velocity waveforms in pregnancy-induced hypertension and/or intrauterine growth retardation. Ultrasound Obstet Gynecol 1996; 7: 122-128.
Nachtigall MJ, Schwartz LB. The application of transvaginal ultrasound for ovulation induction and in vitro fertilization. Clin Obstet Gynecol 1996; 39: 231-247.
Nakajima ST, Gibson M. Pathophysiology of luteal-phase defi ciency in human reproduction. Clin Obstet Gynecol 1991; 34: 167-179.
Newnham JP, Patterson LL, James IR, Diepeveen DA, Reid SE. An evaluation of the effi cacy of Doppler fl ow velocity waveform analysis as a screening test in pregnancy. Am J Obstet Gynecol 1990; 162: 403-410.
Ng EH, Tang OS, Ho PC. The signifi cance of the number of antral follicles prior to stimulation in predicting ovarian responses in an IVF programme. Hum Reprod 2000; 15: 1937-1942.
Nikas G, Develioglu OH, Toner JP, Jones HW Jr. Endometrial pinopodes indicate a shift in the window of receptivity in IVF cycles. Hum Reprod 1999; 14: 787-792.
Nikolaou D, Lavery S, Turner C, Margara R, Trew G. Is there a link between an extremely poor response to ovarian hyperstimulation and early ovarian failure? Hum Reprod 2002; 17: 1106-1111.
Nuojua-Huttunen S, Tomas C, Bloigu R, Tuomivaara L, Martikainen H. Intrauterine insemination
Nuojua-Huttunen S, Gissler M, Martikainen H, Tuomivaara L. Obstetric and perinatal outcome of pregnancies after intrauterine insemination. Hum Reprod 1999b; 8: 2110-2115.
from European registers by ESHRE. The European IVF-monitoring programme (EIM) for the European Society of Human Reproduction and Embryology (ESHRE). Hum Reprod 2001; 16: 384-391.
Ola B, Afnan M, Hammendieh N. Recombinant versus urinary FSH for ovarian stimulation in assisted reproduction. Hum Reprod 2000; 15: 1208-1209.
Ola B, Afnan M, Sharif K, Papaioannou S, Hammadieh N, Barratt CLR. Should ICSI be the treatment of choise for all cases of in-vitro conception? Considerations of fertilization and embryo development, cost effectiveness and safety. Hum Reprod 2001; 16: 2485-2490.
Olivennes F, Rufat P, Andre´B, Pourade A, Quiros MC, Frydman R. The increased risk of complication observed in singleton pregnancies resulting from in-vitro fertilization (IVF) does not seem to be related to the IVF method itself. Hum Reprod 1993; 8: 1297-1300.
Olivennes F, Kerbat V, Rufat P, Blanchet V, Fanchin R, Frydman R. Follow-up of a cohort of 422 children aged 6 to 13 years conceived by in vitro fertilization. Fertil Steril 1997; 67: 284-289.
Omland AK, Tanbo T, Dale PO, Abyholm T. Artifi cial insemination by husband in unexplained infertility compared with infertility associated with peritoneal endometriosis. Hum Reprod 1998; 13: 2602-2605.
Omland AK, Fedorcsak P, Storeng R, Dale PO, Åbyholm T, Tanbo T. Natural cycle IVF in unexplained, endometriosis-associated and tubal factor infertility. Hum Reprod 2001; 16; 2587-2592.
Palermo GD, Cohen J, Rosenwaks Z. Intracytoplasmic sperm injection: a powerful tool to overcome fertilization failure. Fertil Steril 1996; 65: 899-908.
treatment in subfertility: an analysis of factors affecting outcome. Hum Reprod 1999a; 14: 698-703.
Nygren KG, Nyboe Andersen A. Assisted reproductive technology in Europe, 1997. Results generated
75
Palmer SK, Zamudio S, Coffi n C, Parker S, Stamm E, Moore LG. Quantitative estimation of human artery blood fl ow and pelvic blood fl ow redistribution in pregnancy. Obstet Gynecol 1992; 80: 1000-1006.
Pandian Z, Bhattacharya S, Templeton A. Review of unexplained infertility and obstetric outcome: a 10 year review. Hum Reprod 2001; 16: 2593-2597.
Pellicer A, Ardilles G, Neuspiller F, Remoni J, Simon C, Bonilla-Musoles F. Evaluation of the ovarian reserve in young low responders with normal basal levels of follicle stimulating hormone using three-dimensional ultrasonography. Fertil Steril 1998; 70: 671-675.
Pezeshki K, Feldman J, Sten DE, Lobel SM, Grazi RV. Bleeding and spontaneous abortion after therapy for infertility. Fertil Steril 2000; 74: 504-508.
Pihkala J, Hakala T, Voutilainen P, Raivio K. Characteristics of recent fetal growth curves in Finland. Duodecim 1989; 105: 1540-1546.
Pirhonen JP, Vuento MH, Mäkinen JI, Salmi TA. Long-term effects of hormone replacement therapy on the uterus and on the uterine circulation. Am J Obstet Gynecol 1993; 168: 620-630.
Randolph JF Jr. Unexplained infertility. Clin Obstet Gynecol 2000; 43: 897-901.
Rodin DA, Fisher AM, Clayton RN. Cycle abnormalities in infertile women with regular mantrual cycles: effects of clomiphene citrate treatment. Fertil Steril 1994; 62: 42-47.
Rowlands DJ, McDermott A, Hull MG. The prognosis for assisted conception treatment after unexpected failure of fertilization in vitro: a comparative study. Hum Reprod 1994; 9: 2287-2290.
Ruiz A, Remohi J, Minguez Y, Guanes PP, Simon C, Pellicer A. The role of in vitro fertilization and intracytoplasmic sperm injection in couples with unexplained infertility after failed intrauterine insemination. Fertil Steril 1997; 68: 171-173.
Sahakyan M, Harlow BL, Hornstein MD. Infl uence of age, diagnosis, and cycle number on pregnancy rates with gonadotropin-induced controlled ovarian hyperstimulation and intrauterine insemination. Fertil Steril 1999; 72: 500-504.
Salha O, Balen AH. New concepts in superovulation strategies for assisted conception treatments. Curr Opin Obstet Gynecol 2000; 12: 201-206.
Sarell PM, DeCherney AH. Psychotherapeutic intervention for treatment of couples with secondary infertility. Fertil Steril 1985; 43: 897-900.
Schild RL, Knobloch C, Dorn C, Fimmers R, van der Ven H, Hansmann M. Endometrial receptivity in an in vitro fertilization program as assessed by spiral artery artery blood fl ow, endometrial thickness, endometrial volume, and uterine artery blood fl ow. Fertil Steril 2001; 75: 361-366.
Schieve LA, Meikle SF, Ferre C, Peterson HB, Jeng G, Wilcox LS. Low and very low birth weight in infants conceived with use of assisted reproductive technology. N Engl J Med 2002; 346: 731-737.
Schwimer SR, Lebovic J. Transvaginal pelvic ultrasonography. J Ultrasound Med 1984; 3: 381-383.
Serafi ni P, Batzofi n J, Nelson J, Olive D. Sonographic uterine predictors of pregnancy undergoing ovulation induction for assisted reproductive treatments. Fertil Steril 1994; 62: 815-822.
Silver RI, Rodrigues R, Chang TSK, Gearhart JP. In vitro fertilization is associated with an increased risk of hypospadias. J Urol 1999; 161:1954-1957.
Silverberg KM. Evaluation of the couple with infertility in a managed care environment. Clin Obstet Gynecol 2000; 43: 844-853.
76
Sladkevicius P, Valentin L, Marsal K. Blood fl ow velocity in the uterine arteries during the normal menstrual cycle. Ultrasound Obstet Gynecol 1993; 3: 199-208.
Sladkevicius P, Valentin L, Marsal K. Endometrial thickness and Doppler velocimetry of the uterine arteries as discriminators of endometrial status in women with postmenopausal bleeding: a comparative study. Am J Obstet Gynecol 1994; 171: 722-728.
Spalding H, Tekay A, Martikainen H, Jouppila P. Assessment of tubal patency with transvaginal salpingosonography after treatment for tubal pregnancy. Hum Reprod 1997; 12: 306-309.
Spalding H, Perala J, Martikainen H, Tekay A, Jouppila P. Assessing tubal patency with transvaginal salpingosonography after the reversal of tubal ligation for female sterilization. Hum Reprod 1998; 13: 2819-2822.
Spalding H, Martikainen H, Tekay A, Jouppila P. Transvaginal salpingosonography for assessing tubal patency in women previously treated for pelvic infl ammatory disease and benign ovarian tumors.
Stakes. Statistical yearbook on social welfare and health care 2000. National Research and Development Center for Welfare and Health. Social Security, 2000; 1.
Steer CV, Campbell S, Pampiglione JS, Kingsland CR, Mason BA, Collins WP. Transvaginal colour fl ow imaging of the uterine arteries during ovarian and menstrual cycles. Hum Reprod 1990; 5: 391-395.
Steer CV, Campbell S, Tan SL, Crayford T, Mills C, Mason B, Campbell S. The use of transvaginal color fl ow imaging after in vitro fertilization to identify optimum uterine conditions before embryo transfer. Fertil Steril 1992; 57: 372-376.
Steer CV, Tan SL, Mason BA, Campbell S. Midluteal-phase vaginal color Doppler assessment of uterine artery impedance in a subfertile population. Fertil Steril 1994; 61: 53-58.
Steer CV, Tan SL, Dillon D, Mason BA, Campbell S. Vaginal color Doppler assessment of uterine artery impedance correlates with immunohistochemical markers of endometrial receptivity required for the implantation of an embro. Fertil Steril 1995; 63: 101-108.
Stephen EH, Chandra A. Updated projections of infertility in the United States: 1995-2025. Fertil Steril 1998; 70: 30-34.
Steptoe PC, Edwards RG. Birth after reimplantation of a human embryo. Lancet 1978; 2: 366.
Stern J, Peters AJ, Coulam CB. Color Doppler ultrasonography assessment of tubal patency: a comparison study with traditional techniques. Fertil Steril 1992; 58: 897-900.
Sterzic K, Grab D, Sasse V, Hutter W, Rosenbusch B, Terinde R. Doppler sonographic fi ndings and their
Stillman RJ, Rosenberg MJ, Sachs BP. Smoking and reproduction. Fertil Steril 1986; 46: 545-566.
Stolwijk AM, Wetzels AMM, Braat DDM. Cumulative probability of achieving an ongoing pregnancy after in-vitro fertilization and intracytoplasmic sperm injection according to a woman’s age, subfertility diagnosis and primary or secondary subfertility. Hum Reprod 2000; 15: 203-209.
Strandell A, Lindhard A, Waldenstöm U, Thorburn J, Janson PO, Hamberger L. Hydrosalpinx and IVF outcome: a prospective, randomized multicentre trial in Scandinavia in salpingectomy prior to IVF. Hum Reprod 1999; 14: 2762-2769.
Strigini FA, Lencioni G, De Luca G, Lombardo M, Bianchi F, Genazzani AR. Uterine artery velocimetry and spontanous preterm delivery. Obstet Gynecol 1995; 85: 374-377.
correlation with implantation in an in vitro fertilization program. Fertil Steril 1989; 52: 825-828.
Ultrasound Obstet Gynecol 1999; 14: 205-209.
77
Strömberg B, Dahlquist G, Ericson A, Finnström O, Köster M, Stjernqvist K. Neurological sequelae in children born after in-vitro fertilisation: a population-based study. Lancet 2002; 359: 461-465.
Subramanian MG, Kowalczyk CL, Leach RE, Lawson DM, Blacker CM, Ginsburg KA, Randolph Jr. JF, Diamond MP, Moghissi KS. Midcycle increase of prolactin seen in normal women is absent in subjects
Sundström I, Ildgruben A, Högberg U. Treatment-related and treatment-independent deliveries among infertile couples, a long-term follow-up. Acta Obstet Gynecol Scand 1997; 76: 238-243.
Syrop CH, Willhoite A, Voorhis BJ. Ovarian volume: a novel outcome predictor for assisted reproduction. Fertil Steril 1995; 64: 1167-1171.
Szamatowicz M, Grochowski D. Fertility and infertility in aging women. Gynecol Endocrinol 1998; 12: 407-413.
Szczepanska M, Skrzypczak J, Kamieniczna M, Kurpisz M. Antizona and antisperm antibodies endometriosis and/or infertility. Fertil Steril 2001; 75: 97-105.
Tadokoro N, Vollenhoven B, Clark S, Baker G, Kovacs G, Burger H, Healy D. Cumulative pregnancy rates in couples with anovulatory infertility compared with unexplained infertility
Reprod 1997; 12: 1939-1944.
Takeuchi S, Minoura H, Shibahara T, Shen X, Futamura N, Toyoda N. In vitro fertilization and intracytoplasmic sperm injection for couples with unexplained infertility after failed direct intraperitoneal insemination. J Assist Reprod Genet 2000; 17: 515-520.
Tallo CP, Vohr B, Oh W, Rubin LP, Seifer DB, Haning RV Jr. Maternal and neonatal morbidity associated with in vitro fertilization. J Pediatrics 1995; 127: 794-800.
Tan SL, Royston P, Campbell S, Jacobs HS, Betts J. Cumulative conception and livebirth rates after in-vitro fertilization. Lancet 1992; 339: 1390-1394.
Tan SL, Zaidi J, Campbell S, Doyle P, Collins W. Blood fl ow changes in the ovarian and uterine arteries
Tan SL. Clinical applications of Doppler and three-dimensional ultrasound in assisted reproductive technology. Ultrasound Obstet Gynecol 1999; 13: 153-156.
Tanbo T, Dale PO, Lunde O, Moe N, Åbyholm T. Obstetric outcome in singleton pregnancies after assisted reproduction. Obstet Gynecol 1995; 86: 188-192.
Tarlatzis BC, Grimbizis G. Pregnancy and child outcome after assisted reproduction techniques. Hum Reprod 1999; 14 (suppl 1): 231-242.
Tekay A, Martikainen H, Jouppila P. Blood fl ow changes in uterine and ovarian vasculature, and predictive value of transvaginal pulsed colour Doppler ultrasonography in an in-vitro fertilization programme. Hum Reprod 1995; 10: 688-693.
Tekay A, Martikainen H, Jouppila P. Comparison of uterine blood fl ow characteristics between spontaneous and stimulated cycles before embryo transfer. Hum Reprod 1996a; 11: 364-368.
Tekay A, Martikainen H, Jouppila P. The clinical value of transvaginal colour Doppler ultrasound in assisted reproductive technology procedures. Hum Reprod 1996b; 11: 1589-1591.
Templeton AA, Penney GC. The incidence, characteristics, and prognosis of patients whose infertility is unexplained. Fertil Steril 1982; 37: 175-182.
with unexplained infertility. Fertil Steril 1997; 67: 644-647.
in women with
ovulation induction programme. Hum
during the normal menstrual cycle. Am J Obstet Gynecol 1996; 175: 625-631.
in an
78
Templeton A, Fraser C, Thompson B. Infertility -epidemiology and referral practice. Hum Reprod 1991; 6: 1391-1394.
Templeton A, Morris JK, Parslow W. Factors that affect outcome of in-vitro fertilisation treatment. Lancet 1996; 348: 1402-1406.
Te Velde ER, Cohlen BJ. The management of infertility. N Engl J Med 1999; 340: 224-225.
Tiitinen A, Halttunen M, Härkki P, Vuoristo P, Hyden-Granskog C. Elective single embryo transfer: the value of cryopreservation. Hum Reprod 2001; 16: 1140-1144.
Tinkanen H, Kujansuu E. Doppler ultrasound studies in pelvic infl ammatory disease. Gynecol Obstet Invest 1992; 34: 240-243.
Tinkanen H, Kujansuu E, Laippala P. Vascular resistance in uterine and ovarian arteries: its association
Tomas C, Nuojua-Huttunen S, Martikainen H. Pretreatment transvaginal ultrasound examination predicts ovarian responsiveness to gonadotophins in in-vitro fertilization. Hum Reprod 1997; 12: 220-223.
Trounson AO, Wood C. IVF and related technology. The present and future. Med J Aust 1993; 158: 853-857.
Unkila-Kallio L. Infertility and its treatment: Association with ovarian granulosa cell tumour and impact on vascular endotelial growth factor, leptin and selected tumour markers in serum. Thesis. University of Helsinki, 2001.
Valentin L, Sladkevicius P, Laurini R, Söderberg H, Marsal K. Uteroplacental and luteal circulation in
Gynecol 1996; 174: 768-775.
van den Elzen HJ, Cohen-Overbeek TE, Grobbee DE, Quartero RW, Wladimiroff JW. Early uterine artery Doppler velocimetry and the outcome of pregnancy in women aged 35 years and older. Ultrasound Obstet Gynecol 1995; 5: 328-333.
Van der Westerlaken LA, Naaktgeboren N, Helmerhorst FM. Evaluation of pregnancy rates after intrauterine insemination according to indication, age, and sperm parameters. J Assist Reprod Genet 1998; 15: 359-364.
Van Royen E, Mangelschots K, De Neubourg D, Valkenburg M, Van de Meerssche M, Ryckaert G, Eestermans W, Gerris J. Characterization of a top quality embryo, a step towards single embryo transfer. Hum Reprod 1999; 14: 2345-2349.
van Weering HGI, Schats R, McDonnell J, Vink JM, Vermeiden JPW, Hompes PGA. The impact of the embryo transfer catheter on the pregnancy rate in IVF. Hum Reprod 2002; 17: 666-670.
Verlanen H, Cammu H, Derde MP, Amy JJ. Singleton pregnancy after in vitro fertilization: Expectations and outcome. Obstet Gynecol 1995; 86: 906-910.
Verlust G, Camus M, Bollen N, Van Steiterghem A, Devroey P. Analysis of risk factors with regard to the occurrence of ectopic pregnancy after medically assisted procreation. Hum Reprod 1993; 8: 1284-1287.
Vilska S, Tiitinen A, Hyden-Granskog C, Hovatta O. Elective transfer of one embryo results in an acceptable pregnancy rate and eliminates the risk of multiple birth. Hum Reprod 1999; 14: 2392-2395.
with infertility and the prognosis of infertility. Eur J Obstet Gynecol Reprod Biol 1994; 57: 111-115.
normal fi rst-trimester pregnancies: Doppler ultrasonographic and morphologic study. Am J Obstet
79
Viniker DA. Hypothesis on the role of sub-clinical bacteria of the endometrium (bacteria endometrialis) in gynaecological and obstetric enigmas. Hum Reprod Update 1999; 5: 373-385.
Wang JX, Clark AM, Kirby CA, Philipson G, Petrucco O, Anderson G, Matthews CD. The obstetric outcome of singleton pregnancies following in-vitro fertilization/ gamete intra-Fallopian transfer. Hum Reprod 1994; 9: 141-146.
Wang JX, Norman RJ, Kristiansson P. The effect of various infertility treatments on the risk of preterm birth. Hum Reprod 2002; 17: 945-949.
Weiner Z, Thaler I, Levron J, Lewit N, Itskovitz-Eldor J. Assessment of ovarian and uterine blood fl ow by transvaginal color Doppler in ovarian-stimulated women: Correlation with the number of follicles and steroid hormone levels. Fertil Steril 1993; 59: 743-749.
Wennerholm UB, Janson PO, Wennergren M, Kjellmer I. Pregnancy complications and short-term follow-up of infants born after in vitro fertilization and embryo transfer (IVF/ET). Acta Obstet Gynaecol Scand 1991; 70: 565-573.
Wennerholm UB, Berg C, Hamberger L, Nilsson L, Reismer E, Wennergren M, Wikland M. Obstetric and perinatal outcome of pregnancies following intracytoplasmic sperm injection. Hum Reprod 1996; 11: 1113-1119.
Wennerholm U-B, Albertsson-Wikland K, Berg C, Hamberger L, Niklasson A, Nilsson A, Nilsson L, Thiringer K, Wennergren M, Wikland M, Borres MP. Postnatal growth and health in children born after cryopreservation as embryos. Lancet 1998; 351: 1085-1090.
Wennerholm UB, Berg C, Hamberger L, Lundin K, Nilsson L, Wikland M, Källén B. Incidence of congenital malformations in children born after ICSI. Hum Reprod 2000; 15: 944-948.
Westergaard HB, Tranberg Johansen AM, Erb K, Nyboe Andersen A. Danish National In-vitro and 1995: a controlled study of births, malformations and cytogenetic
fi ndings. Hum Reprod 1999; 14: 1896-1902.
Wikland M, Enk L, Hamberger L. Transvesical and transvaginal approaches for aspiration of follicles by use of ultrasound. Ann N Y Acad Sci 1985; 442: 184-190.
Williams MA, Goldman MB, Mittendorf R, Monson RR. Subfertility and the risk of low birth weight. Fertil Steril 1991; 56: 668-671.
Wilcox AJ, Baird DD, Weinberg CR. Time of implantation of the conceptus and loss of pregnancy. N Engl J Med 1999; 340: 1796-1799.
Wisanto A, Bonduelle M, Camus M, Tournaye H, Magnus M, Liebaers I, Van Steirteghem A, Devroey P. Obstetric outcome of 904 pregnancies after intracytoplasmic sperm injection. Hum Reprod 1996; 11 (Suppl 4): 121-130.
Wolf LJ. Ovulation induction. Clin Obstet Gynecol 2000; 43: 902-915.
World Health Organization. Laboratory manual for the examination of human semen and sperm-cervical mucus interaction. Cambridge University Press, Cambridge, 1999; pp 60-61.
Yang JH, Wu MY, Chen CD, Jiang MC, Ho HN, Yang YS. Association of endometrial blood fl ow as determined by a modifi ed colour Doppler technique with subsequent outcome of in-vitro fertilization. Hum Reprod 1999; 14: 1606-1610.
Yuval Y, Lipitz S, Dor J, Achiron R. The relationships between endometrial thickness, and blood fl ow and pregnancy rates in in-vitro fertilization. Hum Reprod 1999; 14: 1067-1071.
Fertilization Registry 1994
80
Zabrek EM. Can I get pregnant? The basic infertility workup. Clin Obstet Gynecol 1996; 39: 223-230.
Zaidi J, Campbell S, Pittrof R, Tan SL. Endometrial thickness, morphology, vascular penetration and velocimetry in predicting implantation in an in vitro fertilization program. Ultrasound Obstet Gynecol 1995; 6: 191-198.
Zaidi J, Jacobs H, Campbell S, Tan SL. Blood fl ow changes in the ovarian and uterine arteries in women with polycystic ovary syndrome who respond to clomiphene citrate: correlation with serum hormone concentrations. Ultrasound Obstet Gynecol 1998; 12: 188-196.
Zayed F, Lenton EA, Cook ID. Comparison between stimulated in-vitro fertilization and stimulated intrauterine insemination for the treatment of unexplained infertility and mild male factor infertility. Hum Reprod 1997; 12: 2408-2413.
Ziebe S, Petersen K, Lindenberg S, Andersen AG, Gabrielsen A, Andersen AN. Embryo morphology or cleavage stage: how to select the best embryos for transfer after in vitro fertilization. Hum Reprod 1997; 12: 1545-1549.
Ziegler WF, Bernstein I, Badger G, Leavitt T, Cerrero ML. Regional hemodynamic adaptation during the menstrual cycle. Obstet Gynecol 1999; 94: 695-699.
Zimmermann P, Eiriö V, Koskinen J, Kujansuu E, Ranta T. Doppler assessment of the uterine and uteroplacental circulation in the second trimester in pregnancies at high risk for pre-eclampsia and/ or intrauterine growth retardation: comparison and correlation between different Doppler parameters. Utrasound Obstet Gynecol 1997; 9: 330-338.