Embed Size (px)
Citation preview
From the Department of Surgery, University of Helsinki;Department of Surgery, Division of Plastic Surgery, Oulu University Hospital;
Department of Clinical Veterinary Sciences, University of Helsinki; andInstitute of Biomaterials, Tampere University of Technology, Finland
Biocompatibility and fixationproperties of absorbable miniplates and screws
in growing calvarium
An experimental study in sheep
Hilkka Peltoniemi
Academic dissertation
To be presented, with the assent of the Medical Faculty of the University of Helsinki,for public discussion in the auditorium of the Fourth Department of Surgery, Helsinki
University Central Hospital, Helsinki, Kasarmikatu 11-13, onMarch 3rd, 2000, at 12 noon.
Helsinki 2000
Supervised by:
Docent Timo Waris, M.D. Ph.D.Department of Surgery, Division of Plastic SurgeryOulu University Hospital,Oulu, Finland
Reviewed by:
Docent Claes Lauritzen, M.D., Ph.D.Department of Plastic Surgery, Division of Craniofacial SurgerySahlgrenska University HospitalGöteborg, SwedenandProfessor K. Elizabeth TannerDean of Engineering and Professor of Biomedical MaterialsIRC in Biomedical Materials and Department of MaterialsQueen Mary and Westfield CollegeLondon, UKand extra reviewerDocent Riitta Suuronen, M.D., Ph.D.Department of Oral and Maxillofacial SurgeryHelsinki University HospitalHelsinki, Finland
Opponent
Docent Willy Serlo, M.D., Ph.D.Chief Division of Paediatric Surgery, Department of Children and AdolescentsOulu University HospitalOulu, Finland
Published also in http://ethesis.helsinki.fi/julkaisut/laa/kliin/vk/peltoniemi/
ISBN 951-45-9143-7 (PDF version)Helsingin yliopiston verkkojulkaisutHelsinki 2000
to Matti
CONTENTS
LIST OF ORIGINAL PUBLICATIONS......................................................... 7
ABBREVIATIONS .......................................................................................... 8
INTRODUCTION ........................................................................................ 10
REVIEW OF THE LITERATURE ................................................................ 12
Development and growth of the human calvarium ................................. 12
Regeneration and consolidation of calvarial (membranous) bone ........... 13
The effects of surgical manipulation on regeneration of cranial bone ..................... 13
Role of the dura in regeneration of cranial bone ................................................ 13
Role of the periosteum in regeneration of cranial bone ......................................... 13
Guided bone regeneration .............................................................................. 14
Role of type of fixation on regeneration of cranial bone ....................................... 15
Rigid (metallic) fixation in craniofacial surgery ........................................ 15
Problems associated with rigid (metallic) fixation in
the growing skull ........................................................................................ 16
Restriction of growth .................................................................................... 16
Passive translocation of metallic implants ........................................................ 16
Other problems associated with metallic osteosynthesis materials .......................... 17
Biocompatibility of titanium ......................................................................... 17
Polyglycolic and polylactic acid ................................................................. 18
Chemical background ................................................................................... 18
Polyglycolic acid .......................................................................................... 18
Polylactic acid ............................................................................................ 18
Basic principles in manufacture of
implants ................................................................................................ 19
Biodegradation and bioabsorption of PGA and PLA implants .......................... 20
Biocompatibility of PGA ............................................................................. 21
Biocompatibility of PLA .............................................................................. 22
Biocompatibility and biodegradation of PLA-PGA copolymers and
P(L/DL) LA stereocopolymers ................................................................... 23
Biodegradable materials in fixation of craniofacial bones ....................... 24
Biomechanical demands on bioabsorbable plates in fixation of craniofacial bones
in children .................................................................................................. 24
Experimental studies .................................................................................... 25
Change-over from experimental to clinical applications in craniofacial surgery ...... 25
Properties of an ideal implant for craniofacial surgery ....................................... 29
THE PRESENT STUDY ............................................................................... 31
Aims of the study ........................................................................................ 31
MATERIALS AND METHODS.................................................................... 32
Experimental animals ................................................................................. 32
Implants ...................................................................................................... 32
Preoperative procedure, anaesthesia and postoperative care .................. 33
Operative techniques .................................................................................. 33
Follow-up .................................................................................................... 36
Examination methods ................................................................................. 36
Statistical methods ...................................................................................... 40
RESULTS........................................................................................................ 41
Consolidation of craniotomy lines plated with SR-PLLA and titanium
miniplates (I,II) ........................................................................................... 41
Intraosseal implantation of SR-PLLA plates with SR-PLLA miniscrew
fixation (III)................................................................................................. 46
Healing of cranial osteotomies fixed with flexible PLA96 plates
and SR-PLLAor SR-PGA miniscrews versus rigid titanium
miniplate fixation (IV,V) ............................................................................ 48
GENERAL DISCUSSION ............................................................................. 59
SUMMARY AND CONCLUSIONS ............................................................. 67
ACKNOWLEDGEMENTS ............................................................................ 69
REFERENCES ................................................................................................ 71
ORIGINAL PIBLICATIONS ........................................................................ 71
7
LIST OF ORIGINAL PUBLICATIONS
The present study is based on the following articles, referred to in the text by theirRoman numerals:
I Peltoniemi HH, Tulamo RM, Pihlajamäki HK, Kallioinen M, Pohjonen T,Törmälä P, Rokkanen PU, Waris T. Consolidation of craniotomy lines afterresorbable polylactide and titanium plating: a comparative experimentalstudy in sheep. Plast Reconstr Surg 101:123-33, 1998
II Peltoniemi HH, Ahovuo J, Tulamo RM, Törmälä P, Waris T. Biodegradableand titanium plating in experimental craniotomies: a radiographic follow-up study. J Craniofac Surg 8 (No 6):446-51; discussion 452-3, 1997
III Peltoniemi HH, Tulamo RM, Toivonen T, Pihlajamäki HK, Pohjonen T,Törmälä P, Waris T. Intraosseous plating: a new method for biodegradableosteofixation in craniofacial surgery. J Craniofac Surg 9 (No 2):171-176;discussion 9 (No 3):247, 1998
IV Peltoniemi HH, Hallikainen D, Toivonen T, Helevirta P, Waris T.SR-PLLA and SR-PGA miniscrews: biodegradation and tissue reactions in thecalvarium and dura mater. J Craniomaxillofac Surg 27(1):42-50, 1999
V Peltoniemi HH, Tulamo RM, Toivonen T, Hallikainen D, Törmälä P, Waris T.Biodegradable semirigid plate and miniscrew fixation in experimentalcalvarial osteotomies: A comparative study with rigid titanium fixation.J Neurosurg 90:910-917, 1999
8
ABBREVIATIONS
A surface area (in mechanical studies)
AO Arbeitsgemeinschaft für Osteosynthesefragen
AP anteroposterior
bwt body weight
CRP C-reactive protein
CT computerized tomography
DSC differential scanning calorimetry
EM electron microscopy
F force
FBR foreign-body reaction
FOV field of view
GBR guided bone regeneration
GPa giga Pascal (109 N/m2)
Gy Gray
HMM histomorphometry
hmw high molecular weight
HU Hounsfield Unit
im intramuscular
IU international unit
iv intravenous
MMF /mmf maxillo-mandibular fixation
MPa mega Pascal (106 N/m2)
MRI magnetic resonance imaging
Mv viscosity average molecular weight (g/mol)
Mw weight-average molecular weight (g/mol)
9
N newton
n number
OSF osteoid surface fraction
OTC oxytetracycline
Pa Pascal (N/m2)
PDLA poly-D-lactide
PDLLA poly-DL-lactide (50:50)
PDS polydioxanon
PGA polyglycolic acid or polyglycolide
PLA polylactic acid or polylactide
PLA96 poly-L,D-lactide (96% L-lactide, 4% D-lactide)
PLA 85/15 poly-L,D-lactide (85% L-lactide, 15% D-lactide)
(=70% L-lactide, 30% DL-lactide)
P(L/DL)LA poly-L,DL-lactide
P(L/DL)LA 70/30 poly-L,DL-lactide (70% L-lactide, 30% DL-lactide)
PLGA copolymer of polylactide and polyglycolide
PLGA70/30 copolymer of polylactide and polyglycolide (70%
polylactide, 30% polyglycolide)
PLLA poly-L-lactide
sc subcutaneous
SEM scanning electron microscopy
SR self-reinforced
Tg glass transition temperature (°C)
Tm melting temperature (°C)
Ti titanium
10
Since Paul Tessier´s revolutionary innova-tion, congenital craniofacial skeletal malfor-mations have generally been treated in in-fancy by extensive operative procedures,where skull bones are taken to pieces andreconstructed. The desired shape and spaceare secured by internal fixation (Jackson et al.1982). The development of rigid metallicmini- and microfixation techniques in the1980´s radically improved many surgicaltechniques, and the materials were readilytransferred from adult craniofacial surgeryto paediatric use (Mühlbauer et al. 1987;Sadove and Eppley 1991). However, a grow-ing dynamic human neurocranium sets spe-cial requirements for osteosynthesis materi-als. In 1995, the first report on passive in-tracranial translocation of metallic platesand screws was published (Fearon et al.1995), followed by several others (Goldberget al. 1995a; Honig et al. 1995; Yu et al.1996). Passive intracranial translocation car-ries a potential risk of brain damage andimpedes further operations. Metallic inter-nal fixation devices have also proved to re-strict the growth of the neurocranium(Yaremchuk 1994) and cause scatter in CTand MRI investigations (Sullivan et al.1994), which is of particular concern in in-tracranial areas immediately adjacent to theosteosynthesis devices.
The risks associated with metallic mini-and microfixation devices used in paediat-ric craniofacial surgery and the need of asubsequent removal operation have given a
INTRODUCTION
rise to the development of biodegradablemini-osteosynthesis devices. Devices madeof polylactic acid (PLA) and polyglycolicacid (PGA) and their copolymers havebeen used in the internal fixation of frac-tures and osteotomies in orthopaedic sur-gery since 1980´s after extensive experi-mental studies (Rokkanen et al. 1996). Cu-tright et al. started the development of bi-odegradable fracture fixation devices in thefield of maxillofacial surgery in 1971 (Cu-tright et al. 1971), followed by various ex-periments in the maxillofacial area (Suuro-nen 1993). Illi et al. were the first to useresorbable polydioxanone bands for fixa-tion of calvarial osteotomies (Illi et al.1989). The obvious biocompatibility ofcertain resorbable materials and the urgentneed of alternative methods to metallic fix-ation led to a rapid change-over to biode-gradable fixation in non-loaded osteosyn-theses in the infant neurocranium after1995.
Weakness of the materials was the majorlimiting factor in the manufacture of miniimplants in the 1980´s. Bulky, highlycrystalline PLLA implants caused foreign-body reactions (Bergsma et al. 1993), whichcast a shadow on all biodegradable im-plants. The self-reinforcing technique, in-vented by the Finnish professors Rokkanenand Törmälä, enables the manufacture oflarge, extremely strong orthopaedic im-plants and thin, delicate, but strong miniimplants (Törmälä 1992; Rokkanen et al.

11
1996). The new generation of SR-implantshas been used clinically in correction ofcraniofacial malformations in children(Waris et al. 1995) and in adult maxillofa-cial surgery (Haers et al. 1998; Suuronen etal. 1998a).
Because of the rapid formation and heal-ing of bone in infants, as a result of the os-teogenicity of infant dura, only a short pe-riod of biomechanical stability is required.Polymer type and plate size must be care-fully tailored to the dynamics of the skele-tal site (Eppley and Sadove 1992; Antikainen1993). The effects of applied strain fromextensive three-dimensional bone growthas in rapidly growing infants may hastenthe degradation process of the implants(Eppley and Sadove 1995a). In addition,craniofacial remodelling operations com-monly result in small or even large bonedefects, which may not consolidate as com-
pletely as has been assumed previously(Prevot et al. 1993), and which set specialrequirements as regards implants. The his-tological demonstration of complete deviceresorption without adverse local tissue ef-fects in thin calvarial bone is importantbefore clinical use because incomplete pol-ymer elimination may eventually be associ-ated with chronic inflammatory tissuechanges (Bergsma et al. 1995).
Thus, experiments in large mammals areneeded to study the effects of these materi-als on the osseous healing process of mem-branous calvarial bone osteotomies and thebiocompatibility and bioabsorption proc-esses of the materials. In these less loadedareas, a bioabsorbable method of fixationcould be an alternative to rigid metallicfixation methods in correction of congeni-tal malformations and in tumour and trau-ma surgery.

12
REVIEW OF THE LITERATURE
Development and growth of the human calvarium
The human skull consists of the bony neu-rocranium enveloping and protecting thebrain and the viscerocranium constitutingthe facial bones. The neurocranium con-sists of the concave calvarium and the cra-nial base. The bones of the calvarium andmost of the facial bones are membranousbones which are derived directly from mes-enchymal tissues (Enlow 1990). They differfrom endochondral bones in their way ofgrowing and healing. During early intra-uterine phases of development, the brain issurrounded by a mesenchymal capsule.This precursor of the dura mater becomesfolded in areas where different parts of thebrain arch against each other (Smith andTondury 1978). These folds later serve asthe basal origins of the cranial sutures.Most of the osseous calvarium is formeddirectly from the mesenchymal capsule byintramembranous ossification (Smith andTondury 1978). At the time of birth all thecalvarial bones (frontal, temporal, parietaland occipital) are present as fibrous plateswith centres of maturing bone. Membra-nous bones grow by membranous ossifica-tion in conjunction with the periosteal andendosteal (dura) membranes (Enlow 1990).Ossification proceeds rapidly during thefirst postnatal year, and finally the bonecenters become bone plates, now calvarial
bones, which come into intimate contactthrough fibrous sutures (Friede 1981). Su-tures are complexes of cellular and fibroustissue which unite bones, absorb forces, actas joints by permitting some movement ofadjacent bones and act as growth sites inthe growing skull (Wagemans et al. 1988).
During perinatal and early postnatallife, the rapid volume increase of the brainstimulates growth, development andmolding of the skull (Enlow 1990). Thebrain and cranial vault reach approximate-ly 75 percent of their eventual adult sizeby 3 years and 90 percent by 5 years of age(Waitzman et al. 1992). As the brain growsit pushes the cranial bone plates apart.This leads to tension in membranous layers(periosteum and dura) and sutures, andbone reacts by depositing bone in the bonemargins next to sutures. A very importantmechanism in the growth and remodella-tion of calvarium is deposition of new boneon the outer surface and resorption on theinner surface. When growing cranial boneencounters a rigid structure, it movesaround it through deposition and resorp-tion, which results in a relative change inthe position of for example a rigid plate(“passive translocation”) (Jackson et al.1982; Enlow 1990).

13
Regeneration andconsolidation of calvarial(membranous) bone
The effects of surgical manipulationon regeneration of cranial bone
Thermal damage during bone preparationleads to cell death and bone necrosis. Theextent of surgical trauma (Albrektsson1980a) and ischaemia (Albrektsson 1982)also have an effect on bone healing. Nei-ther osteogenesis nor resorption of bonewill occur before vascularization of thebone (Albrektsson 1980b). A membranousbone graft undergoes a process similar tothat seen with aseptic necrosis, i.e., resorp-tion of necrotic bone (Manson 1994), thebone graft becoming a combination of liv-ing cells and dead bone, with the graft fi-nally being replaced by new bone within10 weeks (Thaller et al. 1996). Surgicalprocedures themseves have been shown tohave a deleterious effect on frontal bonedevelopment: removing the frontal bonesof rabbits by craniotomy and replacingthem as free grafts (with wire osteosynthe-sis) reduced their anteroposterior growthpotential by 10% (Polley et al. 1995).
Role of the dura in regeneration ofcranial bone
Dural continuity has been considered ofmajor importance for bone regenerationexperimentally (Sirola 1960). An experi-mental study on 2 to 3-week-old rabbitsshowed that regeneration of parietal bonedefects was much greater than in adultrabbits, especially when the overlying pe-riosteum and dura were preserved, and
bony regeneration was greater in the ab-sence of periosteum provided that the durawas present (Reid et al. 1981). Anotherstudy with isogeneic guinea pigs demon-strated that only infant dura was capable ofsupporting complete or near completebone regeneration of surgically created cal-varial defects. Adult dura and periosteumlacked such osteogenic properties (Hobar etal. 1993; Hobar et al. 1996). In 6-week oldrabbits, bone deposition leading to calvari-al redevelopment was directly dependentupon the presence of the dura mater, andthe rate of deposition was apparently af-fected by dural continuity, animal age, andlocalized differences in the thickness of thedural layers (Mossaz and Kokich 1981).
In the literature, lack of ossification aftercranial remodelling in children has seldombeen considered with few exceptions. Poorosseous wound healing has been reportedin 6.3% of children aged 2-11 months atthe time of surgery (Prevot et al. 1993).Main explanations have included localpostoperative infection (75% of all affectedcases), forehead advancement especially inassociation with resorbable suture osteo-synthesis, and brachycephaly. Repairedtears of the dura mater do not appear topose a risk. Tears of the dura mater, if leftunrepaired, may contribute to incompleteossification (Powiertowski and Matlosz 1970;Prevot et al. 1993), and expanding cranialbone defects and brain herniation (Winstonet al. 1983; Muhonen et al. 1995; Umanskyand Schendel 1995).
Role of the periosteum in regenerationof cranial bone
Cutting et al. demonstrated that the outersurface of the calvaria receives blood dif-

14
fusely from the periosteum (Cutting et al.1984). They also reported an increased sur-viving volume of calvarial bone followingvascularized transfer versus a traditionalnonvascularized bone graft, which was pe-riosteally covered. The role of the perios-teum thus seems to be important when itsblood supply is preserved, but its role isminor or nonexistent if it is not preserved(Cutting and McCarthy 1983). The role ofperiosteum has been considered to be ofgreater importance than dura in adult age(Gosain and Persing 1999). In cases of fore-head advancement, although periostealflaps are preserved and replaced on the re-shaped skull, they are often not largeenough at the end of the operation to coverthe whole vault, which may also contrib-ute to incomplete ossification (Prevot et al.1993). In vascularized bone grafts, perios-teum provides a surviving population ofosteogenic cells and route for early revascu-larization, whereas free grafts are character-ized by significant resorption and a delayin subperiosteal bone formation (Antony-shyn et al. 1987).
Guided bone regeneration
In numerous studies, guided bone regener-ation (GBR) has been demonstrated to beeffective in osteoconduction and preven-tion of fibrous nonunions in craniofacialbone defects (Gottlow 1984; Dahlin et al.1988; Dahlin et al. 1991; Gottlow et al.1993; Karring et al. 1993; Linde et al.1993; Lundgren et al. 1995; Hutmacher et al.1996; Lemperle et al. 1998). In GBR, amembrane is positioned to “exclude” rap-idly colonizing fibroblastic cells from awound site during healing, and “guide”more slowly migrating osseous cells into
the wound site, resulting in direct bony re-generation and deposition (Linde et al.1993).
If a bone defect exists between the bonemargins, rigid fixation with membranecovering the bone defect shows most rapidand organized osseous wound healingwhen compared with non-rigid or non-cov-ering fixation. Mooney et al. studied heal-ing of 5 mm-wide zygomatic arch osteoto-mies in rabbits, when fixed rigidly (micro-plates and screws) or non-rigidly (wire fixa-tion) and the gap covered with collagenmembrane or left uncovered (Mooney et al.1996). Rigidly fixed and membrane-cov-ered defects consolidated most rapidly, fol-lowed by defects that were non-rigidlyfixed but membrane-covered, the differ-ence being statistically non-significant.The defects without membrane coverageresulted in non-union.
Periosteum alone (without any othermembrane) has also been considered tofunction as a biologically active membrane,excluding nonosteogenic, extraskeletal tis-sues from the organizing clot (Engdahl1971; Linde et al. 1993).
If a resorbable membrane or plate is usedfor GBR, it is essential that the implant re-tains integrity for a sufficient time periodfor bone regeneration. If degradation is toorapid or the implant too weak, osteoblastswill be deprived of a surface on which tomigrate and secrete bone matrix, the resultbeing fibrous repair rather than osseous re-generation (Levy et al. 1994; Meikle et al.1994). In addition, too rapid resorption ofthe polymer may interfere with the consoli-dation process: during resorption of PLGA,osteoneogenesis is slowed at the implant site(Winet and Bao 1997).
15
Role of type of fixation onregeneration of cranial bone
Typically, membranous bones heal by di-rect bony union without callus formation,which has been shown in sagittal ramusosteotomies in monkeys (Ellis et al. 1992)and in calvarial bone fractures in rats (Al-berius and Johnell 1991). Rigid fixation cre-ates a favourable environment for directbony deposition from stable, approximatedbony osteotomy margins (Ellis et al. 1992).Because the membranous bone is dense innature, new vessel ingrowth is sensitive toshearing forces, a situation which favoursrigid fixation (Phillips and Rahn 1990).
Instability and mobility, especially asso-ciated with functional loading of non-rig-idly -fixed osteotomy segments, may alsoretard the formation of osteogenic macro-molecules, cytokines, extracellular matrixand growth factors, thus resulting in theformation of fibrous or cartilaginous con-nective tissue, fibrous non-unions, andsubsequent osseous instability (Ellis et al.1992). In areas of motion, the applicationof rigid fixation also improves bone graftsurvival, whereas in a low-motion region,no differences in graft volume retention asa function of fixation have been observed(Lin et al. 1990).
In long bones, rigid metallic plate fixa-tion causes stress-shielding in the underly-ing cortical bone (Uhthoff and Dubuc 1971;Paavolainen et al. 1978). Protection fromstress will occur in a mechanical reparativesystem if the plate has a higher modulus ofelasticity than the bone to which it is at-tached. The reduction of bone mass is sig-nificant under stainless steel plates, andcan be compensated for by early removal(eight weeks) of the plates (Uhthoff andFinnegan 1983). In loaded membranous
bones, stress-shielding has also been re-ported (Kennady et al. 1989b; Iizuka et al.1991a). Less rigid plating systems haveshown superior healing in long bones(Foux et al. 1997) and in Le Fort I osteoto-mies in monkeys (Calhoun et al. 1989).
In the literature, there is only one pub-lished experimental study on fixation ofunstable craniotomies with bioadegradableimplants (Illi et al. 1990). In fixation ofbone grafts, biodegradable, initially rigidfixation has been shown to permit ade-quate stabilization for a finite period, al-lowing bone graft revascularization andeliminating osteolysis (Thaller et al. 1996).
Rigid (metallic) fixation incraniofacial surgery
Since the 1940´s, metallic wires have beenused to attach bone fragments non-rigidly,but rigid fixation with metallic miniplatesand miniscrews was a major breakthroughin the development of craniofacial surgeryin the 1980´s. The principle of the newoperative techniques in synostosis surgery,originally developed by Paul Tessier, con-sisted of complete release of all the stenosesof the neuro- and viscerocranium, anatomi-cal and physiological positioning of theskeleton, and temporary fixation withminiplates and sutures (Mühlbauer et al.1987). The approach was intracranial, ex-tranasal, and extraoral through a singlecoronal incision. The idea of temporaryrigid fixation was to maintain the desiredshape and space with bone gaps againstthe tractional forces of the soft tissues for 3to 6 months, and then remove the platesthrough stab incisions to create a “floating

16
cranio-orbitofacial complex”, to take opti-mal advantage of the formative power ofthe growing brain during the first 2 yearsof life (Mühlbauer and Anderl 1983; Mühl-bauer et al. 1987). In infants, disjunction ismore important than advancement, mak-ing this approach a dynamic one in con-trast to the static procedures used foradults (Mühlbauer et al. 1987), and the useof rigid fixation in growing children wasrecommended to be limited to unstablebone sites (Sadove and Eppley 1991) andloaded conditions with bone defects, e.g.,in orthognatic surgery. The advantages ofrigid fixation include greater bony stabili-ty of osteotomized bone flaps and grafts,greater accuracy in bone reshaping, simpli-fication of osteotomy design, and enhance-ment of primary bone healing with de-creased resorption and infection rates (Jack-son et al. 1986; Mühlbauer et al. 1987;Sadove and Eppley 1991). Hence the newmethods, especially microfixation tech-niques, were rapidly adopted in paediatricuse.
Problems associated withrigid (metallic) fixation inthe growing skull
Restriction of growth
Rigid metallic plating over craniofacial su-tures causes consistent asymmetry betweenthe plated and nonplated sides, with devi-ation of the midline towards the platedside (Resnick et al. 1990; Marschall et al.1991; Wong et al. 1991; Wong et al. 1993).Local restriction of growth has been docu-mented experimentally with both metallic
rigid and non-rigid wire fixation (Lin et al.1991; Yaremchuk et al. 1994; Polley et al.1995; Polley et al. 1998). The degree ofgrowth restriction increases with theamount of fixation hardware used, butwhen the fixation devices are appropriatelysized and located in non-growth centre re-gions, growth restriction can be limited(Lin et al. 1991; Wong et al. 1991; Mooney etal. 1992; Wong et al. 1993; Yaremchuk et al.1994; Polley et al. 1995; Polley et al. 1998).Also single-point fixation within oneplane, removal of rigid fixation hardware,and the use of semirigid fixation approach-es can significantly reduce the long-termgrowth effects (Polley et al. 1998).
Passive translocation of metallicimplants
The first reports on passive intracranialtranslocation of metallic hardware werepublished in 1995 (Fearon et al. 1995;Goldberg et al. 1995a; Papay et al. 1995),causing great concern and discussion (Pos-nick and Yaremchuk 1995; Yaremchuk andPosnick 1995; Persing et al. 1996). Devicetransposition is more likely to occur in in-fants (Goldberg et al. 1995), especially withsyndromic forms of craniosynostoses, andwhen (long) plates are placed in temporaland lateral areas (Goldberg et al.1995;Yaremchuk and Posnick 1995). How-ever, any implants, even wires, may trans-locate (Yaremchuk and Posnick 1995). CTimaging demonstrated translocation of mi-crofixation in 14 of 27 patients, who wereunder three years of age at the time of op-eration (Goldberg et al. 1995). Experimentalstudies on passive translocation haveshown transposition of microplates in pig-lets (Yu et al. 1996; Stelnicki and Hoffman

17
1998) and even in adolescent minipigs (Ho-nig et al. 1995). Unilateral fronto-orbital ad-vancement and rigid fixation using micro-plates and screws were performed in 3-week-old pigs (Yu et al. 1996). At 6 monthsof age, 28% of microplates showed com-plete intracranial translocation, 27% re-mained on the ectocranial surface, and 44%were located between the outer and innercortices of the calvaria. In the underlyingbrain and meninges, demonstrable histolog-ical alterations were demonstrated, but nei-ther signs of cerebritis, gliosis or hypoxicchange nor clinical sequelae were noticed.Implantation of titanium, Vitallium andstainless steel in the rabbit brain did notcause any behavioral changes or neurologi-cal defects as long as 26 weeks postimplan-tation (Mofid et al. 1997). Titanium and Vi-tallium incited a similar inflammatory re-sponse, which was less than that found withstainless steel wire.
There are no documented cases of earlyor late brain injury (i.e., seizures, stroke,haematoma, memory loss or infection) re-sulting from previously implanted internalfixation devices (Yaremchuk and Posnick1995; Goldberg et al. 1995; Persing et al.1996). Metallic materials can be incorpo-rated into the dura and pose a difficulty insurgical reoperations (Fearon et al. 1995)and possibly a risk in MRI.
Other problems associated withmetallic osteosynthesis materials
Metallic fixation devices may cause a dis-tinct cosmetic deformity, palpability orwound dehiscence especially if placed un-der a scarred, tight scalp (Fearon et al.1995). Plate exposure has been reported tobe associated especially with preoperative
radiotherapy (McCann et al. 1994). Com-mon reasons for hardware removal havebeen reported to include palpable or prom-inent hardware (34.5% of the patientsneeding implant removal), loosening ofplates and screws (25.5%), pain (25.5%),infection (23.6%), wound dehiscence/ex-posure of hardware (20%), and removal atthe time of secondary procedures (9.1%)(Orringer et al. 1998).
Metallic devices also interfere with radi-ological investigations. Titanium deviceshave superior imaging characteristics, cre-ating fewer computed tomographic andMR imaging artifacts and permitting bet-ter resolution of anatomical structures thanother metallic devices (Fiala et al. 1993;Fiala et al. 1994; Anastakis et al. 1996).
Biocompatibility of titanium
Compared with other metals, titanium hasbeen considered to be highly biocompati-ble and to have high corrosion resistancecharacteristics (Linder et al. 1983; Carlssonet al. 1986). The mechanical integrity ofthe oxide film that covers titanium alloys isessential for the long-term stability andsurvival of the implant. Combined stresses,motion and electrochemical processes occurat metal oxide film-tissue interfaces, whichmay lead to corrosion and release of titani-um ions or particles. Experiments withlaboratory animals (Schliephake et al.1993b), and limited analyses of human tis-sues (Rosenberg et al. 1993; Schliephake et al.1993a; Katou et al. 1996; Jorgenson et al.1997; Kim et al. 1997) have indicated evi-dence of titanium release into local tissues.Although titanium ions may stay bound tolocal tissue, there is increasing recognitionthat they may also bind to protein moieties
18
that are transported in the bloodstreamand lymphatics to remote organs (Woodmanet al. 1984). In the literature, hypersensi-tivity reactions to titanium have been re-ported (Lalor et al. 1990). Corrosion andwear have also been suspected to inducechemical carcinogenesis (Sunderman 1989).
Polyglycolic andpolylactic acid
Chemical background
Polylactic acid (PLA) and polyglycolic acid(PGA) are derivatives of cyclic diesters ofglycolic and lactic acid from which theyhave been produced by ring opening po-lymerization, resulting in poly-alpha-hy-droxy derivatives of the original acids (Gild-ing and Reed 1979). The polymers are com-posed of macromolecules with molecularweights typically from tens of thousands ofdaltons to more than 1 million daltons. Ahomopolymer (-AAAAAA-) is formed ifonly a single monomer is used, and a copol-ymer consists of two monomers (-ABABA-BA-). The properties of a copolymer are sig-nificantly different than those of homopoly-mers of any of its constituent monomers.The strength of a polymer depends on itsmicrostructure. If the polymeric chains arerandomly oriented in disorder and thusloosely packed, the polymer is called amor-phous and it is weak. If the chains lie paral-lel and thus are packed tightly, the polymeris called crystalline and it is strong. Copoly-mers are typically formed by random po-lymerization (-ABAAABABBBBBABBB-),and the polymeric structure is commonlyamorphous. Even crystalline homopolymersare not entirely crystalline and always con-
tain both crystalline and amorphous regionsand are best termed semicrystalline. Crystal-linity results in higher tensile strength, atranslucent to opaque optical quality, andbirefringence when exposed to polarizedlight. Conversely, amorphous polymers areless rigid, potentially transparent, and ex-hibit no response to polarized light. Poly-mers exhibit a glass transition temperature(Tg), below which the polymer is solid andstiff and above which it is soft (Pietrzak et al.1997).
Polyglycolic acid
Polyglycolic acid is a brownish, hard crys-talline polymer melting at about 224-228°C, with a glass transition temperature of36° C (Törmälä et al. 1998). It lacks a me-thyl group, which makes it hydrophilicand thus more susceptible to hydrolysisand faster degradation than polylactide.The oldest and best known commercialproduct made of PGA is Dexon® (Frazzaand Schmitt 1971).
Polylactic acid
Polylactic acid is a pale-coloured semicrys-talline polymer with a glass transitiontemperature of 57° C and a melting pointof 174-184° C (Vert et al. 1981; Hollingerand Battistone 1986; Törmälä et al. 1998).The asymmetric lactic acid molecule hastwo stereoisomeric forms, L and D lactide(Cutright et al. 1974). In the human body,the L-isomer exists in carbohydrate metab-olism, and the D-isomer is found in acidicmilk. If the polymer consists only of the Lisomer, it is called poly-L-lactic acid,PLLA, which has most commonly been
19
used in orthopaedic implants. If it containsboth isomers, it is called stereocopolymer,poly-D,L-lactic acid, often referred to asP(L/DL)LA or PDLLA. Because of the ster-eoregularity of the molecules, PLLA ishighly crystalline. The methyl groupmakes PLA hydrophobic and thus resistantto hydrolysis.
Basic principles in manufacture ofimplants
The two main methods of manufacturingpolymeric implants in this study weremelt moulding and solid state drawing.Melt moulding is the oldest method, andthe implants are mechanically weak, whichhas been compensated for by enlarging thesize of the implants. The melt mouldingprocess can be subdivided into three meth-ods to process implants from the melted
raw material: compression moulding, in-jection moulding and extrusion. In thepast, attempts to reinforce the weak im-plants led to use of carbon fibres as rein-forcing elements.
The first PGA product, Dexon® thread,was manufactured by drawing the poly-meric raw material into long fibres. This“drawing” technique was later used to pro-duce fibres processed in a parallel fashionto strengthen the implants. These im-plants are called “oriented”.
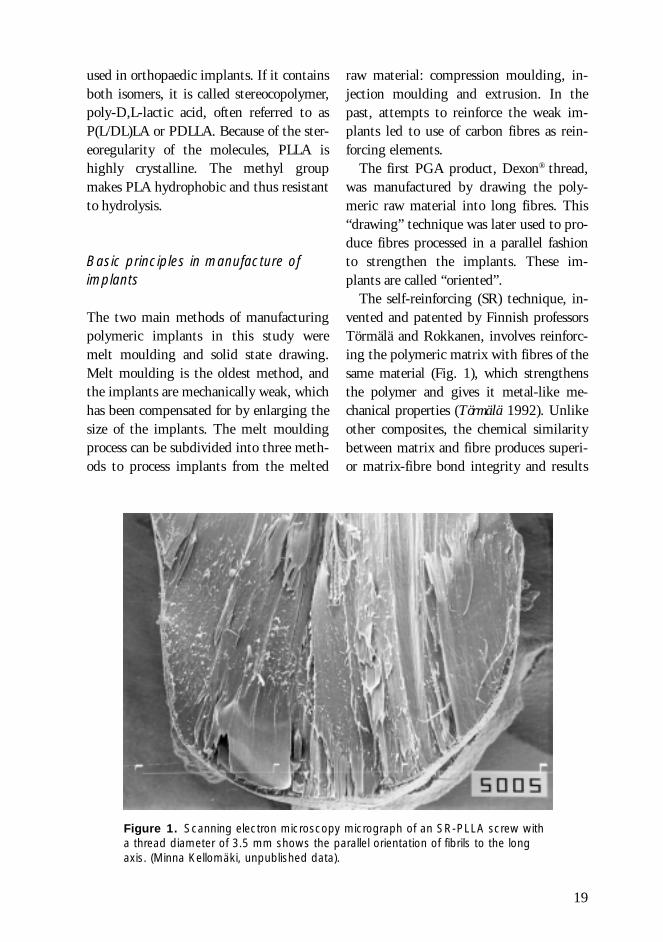
The self-reinforcing (SR) technique, in-vented and patented by Finnish professorsTörmälä and Rokkanen, involves reinforc-ing the polymeric matrix with fibres of thesame material (Fig. 1), which strengthensthe polymer and gives it metal-like me-chanical properties (Törmälä 1992). Unlikeother composites, the chemical similaritybetween matrix and fibre produces superi-or matrix-fibre bond integrity and results
Figure 1. Scanning electron microscopy micrograph of an SR-PLLA screw witha thread diameter of 3.5 mm shows the parallel orientation of fibrils to the longaxis. (Minna Kellomäki, unpublished data).

20
in a polymeric composite with goodstrength and stiffness. To manufacturescrews, the self-reinforced polymer can becompression-moulded or machine-cut. Thelatter, new technique has improved signifi-cantly the torque and bending strengths ofthe screws (Pohjonen et al. 1997).
Biodegradation and bioabsorption ofPGA and PLA implants
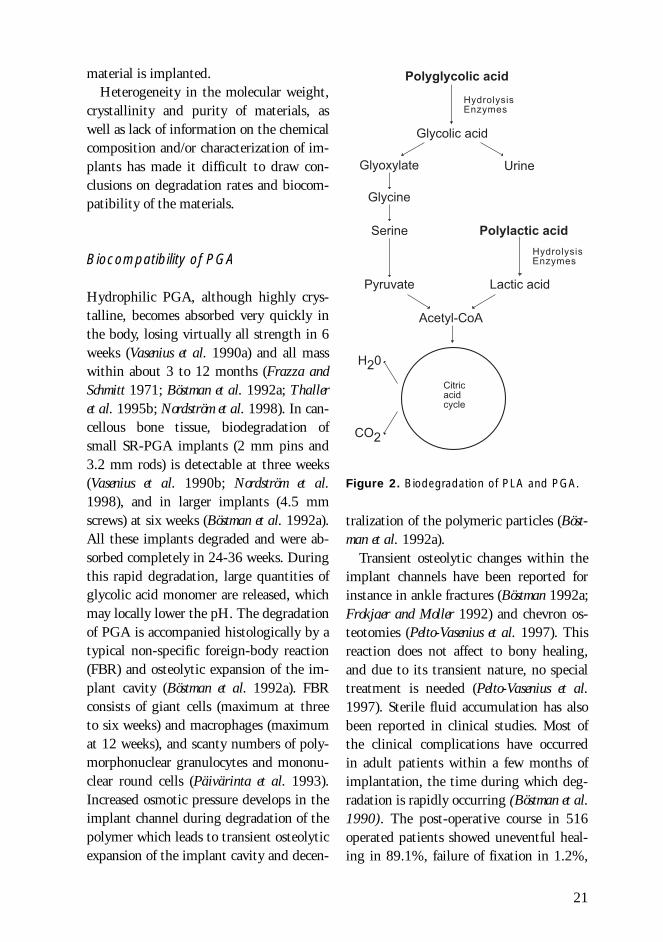
Bioabsorbable materials generally undergo atwo-phase degradation process in the body.In the first, mainly physical phase, watermolecules hydrolyse the chemical bonds ofthe polymer and cut long polymer chains toshort chains. During this depolymerizationprocess, the overall molecular weight andstrength of the polymer become reducedand the polymer fragments. The secondphase involves phagocytosis of the frag-ments by macrophages, and the polymermass rapidly disappears (Pietrzak et al.1997). PGA is converted hydrolytically intoglycolic acid and PLA into lactic acid (Fig.2.), which are further metabolized in thecitric acid cycle to carbon dioxide and wa-ter, and the final products are excreted viarespiration or urine (Kulkarni et al. 1966;Brady et al. 1973; Williams 1982; Hollingerand Battistone 1986). The degradation ofPGA and PLA is accelerated in vivo by cel-lular enzymes (Williams 1982;Vasenius et al.1990a) and free radicals (Williams 1992; Aliet al. 1993).
Hydrophilic polyglycolide degrades rap-idly, whereas hydrophobic polylevolactidehas a slow rate of degradation. Hydrolysisoccurs initially in the amorphous regionsand only later in the crystalline regions ofthe device. Higher amounts of crystallinestructure compared with amorphous com-
position slow the degradation process (Pis-tner et al. 1993; Bergsma et al. 1995)
Any implanted device stimulates for-eign-body tissue changes. After implanta-tion of a polymeric device, the normal ini-tial inflammatory response leads to granu-lation tissue enveloping the implant with-in one to three weeks. In early stages, poly-morphonuclear leucocytes and later, mac-rophages, giant cells and large mononu-clear cells are seen around the implant(Kulkarni et al. 1966; Cutright and Hunsuck1971; Getter et al. 1972). A latent periodcommences and continues until the degra-dation and following bioabsorption bymacrophages and giant cells begin. Thefaster the degradation process, the strongerthe tissue response (Nakamura et al. 1989).During the most intense stage of biodegra-dation some patients may show clinicallylocal fluid accumulation, which, if nottreated properly by aspiration, may lead totransient sinus formation (Törmälä et al.1998)
The rate of biodegradation depends onchemical composition (hydrophilic, hydro-phobic), molecular weight, the degree ofcrystallinity, impurities (presence of resid-ual low Mw compounds or monomers),enantiomeric purity (presence of D-iso-mers), sterilization (gamma irradiation vs.ethylene oxide), shape and size of the im-plant, site of implantation (hard or soft tis-sue; subcutaneously placed implants de-grade faster than intraosseously implantedones) (Törmälä et al. 1998), and biome-chanical stresses (Miller and Williams 1984)to which the implant is exposed. The in-tensity of the tissue reaction depends onthe quantity, degradation characteristics,and associated changes in the morphologyof the implanted material as well as thecharacteristics of the tissue in which the
21
����������
�����
�� ��
�� �����
���������������
��� ������������
��������
���������
� ��
��� ������������
������������
������
���
���
�� �����
material is implanted.Heterogeneity in the molecular weight,
crystallinity and purity of materials, aswell as lack of information on the chemicalcomposition and/or characterization of im-plants has made it difficult to draw con-clusions on degradation rates and biocom-patibility of the materials.
Biocompatibility of PGA
Hydrophilic PGA, although highly crys-talline, becomes absorbed very quickly inthe body, losing virtually all strength in 6weeks (Vasenius et al. 1990a) and all masswithin about 3 to 12 months (Frazza andSchmitt 1971; Böstman et al. 1992a; Thalleret al. 1995b; Nordström et al. 1998). In can-cellous bone tissue, biodegradation ofsmall SR-PGA implants (2 mm pins and3.2 mm rods) is detectable at three weeks(Vasenius et al. 1990b; Nordström et al.1998), and in larger implants (4.5 mmscrews) at six weeks (Böstman et al. 1992a).All these implants degraded and were ab-sorbed completely in 24-36 weeks. Duringthis rapid degradation, large quantities ofglycolic acid monomer are released, whichmay locally lower the pH. The degradationof PGA is accompanied histologically by atypical non-specific foreign-body reaction(FBR) and osteolytic expansion of the im-plant cavity (Böstman et al. 1992a). FBRconsists of giant cells (maximum at threeto six weeks) and macrophages (maximumat 12 weeks), and scanty numbers of poly-morphonuclear granulocytes and mononu-clear round cells (Päivärinta et al. 1993).Increased osmotic pressure develops in theimplant channel during degradation of thepolymer which leads to transient osteolyticexpansion of the implant cavity and decen-
tralization of the polymeric particles (Böst-man et al. 1992a).
Transient osteolytic changes within theimplant channels have been reported forinstance in ankle fractures (Böstman 1992a;Frokjaer and Moller 1992) and chevron os-teotomies (Pelto-Vasenius et al. 1997). Thisreaction does not affect to bony healing,and due to its transient nature, no specialtreatment is needed (Pelto-Vasenius et al.1997). Sterile fluid accumulation has alsobeen reported in clinical studies. Most ofthe clinical complications have occurredin adult patients within a few months ofimplantation, the time during which deg-radation is rapidly occurring (Böstman et al.1990). The post-operative course in 516operated patients showed uneventful heal-ing in 89.1%, failure of fixation in 1.2%,
Figure 2. Biodegradation of PLA and PGA.
22
bacterial wound infections in 1.7% and lo-cal fluid accumulation in 7.9%, which wastreated with aspiration or incision (Böstmanet al. 1990). The reaction is characterizedby local pain, redness, swelling and oede-ma, but bacterial cultures are negative,and the serum concentration of CRP islow. Cytological studies on the seroma flu-id have shown predominance of inflamma-tory monocytes and lymphocytes, therebyconfirming the non-infectious nature ofthis infiltrate (Santavirta et al. 1990).Granulomatous formation of monocyte-macrophages and foreign-body giant cellshas also been reported (Böstman 1992a).The fast degradation process of PGA, therapid release of acidic degradation prod-ucts, and the site of implantation (e.g.head of a screw located in a thin subcuta-neous layer) affect the tissue responses. Indistal radial fractures an incidence of clini-cal foreign-body reactions as high as 7/15has been reported, when PGA rods insert-ed in the bone protruded far into the sub-cutaneous space (Casteleyn et al. 1992).
Biocompatibility of PLA
Excellent biocompatibility and slow bio-degradation of PLA have been documentedin hundreds of publications, since the firstexperiments: no inflammatory cell infiltra-tions have been reported, and foreign-bodyreactions have been limited to around theimplanted material (Kulkarni et al. 1966;Cutright et al. 1971; Cutright and Hunsuck1972).
Intraosseally implanted SR-PLLA screwsand pins have been shown to cause similar,mild foreign-body reactions as correspond-ing metallic devices, without signs of in-flammatory reactions during follow-up of
48 weeks (Majola et al. 1991; Viljanen et al.1997). However, the resorption time ofPLLA is very long, and the relatively shortlife expectancy of most rodents and otherexperimental mammals has been a prob-lem in studying biodegradation and bioab-sorption of PLLA. During degradationPLLA forms crystals, which may take 5-7years to resorb. Matsusue et al. implantedultra-high-strength PLLA rods in the fem-oral medullary cavity of rabbits. At 18months histiocytes were observed; theirphagocytic activity was maximal from 24to 36 months, and at 62 months the mate-rial had been almost completely absorbed,with only a slight residual tissue reaction(Matsusue et al. 1995). Suuronen et al. fixedmandibular osteotomies in sheep with SR-PLLA multilayer plates (four 0.5-mmthick plates). After 5 years in vivo, the ma-terial was almost completely resorbed, butsmall particles of polymer could still bedetected at the implantation site. Howev-er, the FBR was mainly mild (Suuronen etal. 1998b). Bergsma et al. reported a latetissue response to as-polymerized, highmolecular weight (hmw) PLLA bone platesand screws used in the fixation of ten zygo-matic fractures in humans (Bergsma et al.1995). Their non-reinforced plates were 2mm thick. Initial stability and fracturehealing was good (Bos et al. 1987). Threeyears after implantation four patients re-turned because of a swelling in the opera-tion area, and the other patients showed anidentical type of swelling on recall. The 10mm-thick swollen areas were revised 3.3 to5.7 years postoperatively. The authors dis-covered remnants of degraded PLLA mate-rial digested by various cells and surround-ed by a dense fibrous capsule. Histologyshowed FBRs without signs of inflamma-tion. The remnants of PLLA were lying

23
within the macrophages, foreign-body gi-ant cells and fibrocytes. Electron microsco-py showed abundant amounts of crystal-like PLLA material, with a minimal thick-ness of 22 nm, internalized in the cyto-plasm of various cells. They concluded thatPLLA slowly degrades into particles withhigh crystallinity and a very slow degrada-tion rate, but they do not cause severe cellinjury or cell death. The origin of theswelling was supposed to be the increasedosmotic pressure caused by these fragmentsand subcutaneous implantation.
Eitenmüller et al. used injection-mould-ed, non-reinforced 3-mm-thick hmw PLLAplates for fixation of ankle fractures. Fifty-two per cent of the patients demonstratedan aseptic soft tissue problem caused bydelayed clearance of the degrading polylac-tide particles. In a second protocol, volume-reduced plates and screws did not causeany soft tissue reactions (Eitenmüller et al.1996). Foreign-body reactions caused byhmw, as-polymerized PLLA material usedby Bergsma and co-workers should not begeneralized to cover all PLLA materials.PLLA materials may differ considerably inpurity of the raw material and method ofprocessing. Crystals were also found by Su-uronen et al., but, in contrast, they foundno soft tissue reactions (Suuronen et al.1998b).
Subcutaneously implanted PLLA plates(20 x 10 x 1 mm) were associated withmesenchymal tumours in 22 out of 50 rats.Similar non-resorbable polyethylene plateswere associated with the same kind of tu-mours in 23 out of 50 rats (Nakamura et al.1994). This is typical of the so-called Op-penheimer effect, i.e., long-term implanta-tion of any material brings the problem offoreign-body tumourigenesis in rodents(Oppenheimer et al. 1955). In vitro, poly-L-
lactide has been shown to inhibit carcino-ma cell growth (Campbell et al. 1994).
Biocompatibility and biodegradationof PLA-PGA copolymers andP(L/DL) LA stereocopolymers
Copolymers of PLA and PGA (PLGA) havebeen used in numerous experimental andclinical applications (Tables 1 and 2).These copolymers offer the capability of al-tering the degradation rate and mechanicalproperties of implants by changing thePLA-PGA ratio, which offers the potentialto develop site-specific bone fixation andsoft tissue-anchoring devices (Cutright et al.1974; Miller et al. 1977; Eppley and Sadove1995a; Eppley and Reilly 1997). Completeabsorption of PLGA 75/25 has been re-ported in 220 days, PLGA 50/50 in 180days (Cutright et al. 1974), and PLGA 82/18 in 180-450 days (Eppley and Sadove1995a; Eppley and Reilly 1997).
With PLGA implants, no implant-relat-ed clinical foreign body reactions havebeen reported. Even biocompatibility inbrain tissue has been reported: followingimplantation of poly (DL-lactide-co-gly-colide) (PLG) into the brains of rats, nodifferences in GFAP reactivity were seenbetween the polymer-implanted and con-trol sides (injection of the suspension me-dium into the contralateral hemisphere) atany time point (Emerich et al. 1999), andthe brain tissue reaction has been shown tobe non-specific astrocytic proliferation anda macrophagous-microglial cell reaction,typically found following damage to thecentral nervous system (Menei et al. 1993).The latter group also found that the in-flammatory and macrophagous reactiondecreased along with biodegradation of the
24
material and considered the copolymerbiocompatible to the brain tissue. PLA-PGA copolymeric Polyglactin 910 (Vicr-yl®) sutures have been considered better forclosure of dural tears than polyglycolide(Dexon®) sutures (Vallfors et al. 1981).
P(L/DL)LA (also called PDLLA) is moreamorphous and less crystalline and thusdegrades faster than pure PLLA (Kulkarniet al. 1971). The plates have been shown todegrade more rapidly in subcutaneous tis-sue than on bone (Tschakaloff et al. 1994).SR-P(L/DL)LA plates and screws havebeen used clinically in orthognatic surgerywith a skeletal stability pattern which iscomparable to the ‘gold standard’ of titani-um plates and screws (Haers and Sailer1998) (Table 2). No clinical foreign-bodyreactions caused by P(L/DL)LA deviceshave been reported.
Biodegradable materialsin fixation of craniofacialbones
Biomechanical demands onbioabsorbable plates in fixation ofcraniofacial bones in children
To be biomechanically safe, bioabsorbableimplants should have 1) high initialstrength to carry physiological loads dur-ing healing, 2) appropriate initial modu-lus; not too stiff or too flexible for the spe-cial purpose where it is used, and 3) con-trolled strength and modulus retention invivo, in harmony with the increase ofstrength and modulus of the healing tissue(Törmälä and Pohjonen 1995). Of all cranio-facial bones, the mandible is prone to thehighest biomechanical stresses. Average
adult molar bite forces have been recordedto be 726 N, with a maximal force of 4346N (Gosain et al. 1998). Most of these mas-ticatory loads are transmitted to thecraniofacial complex through the temporo-mandibular articulation and maxillaryteeth. The occlusal, mainly compressiveforces disperse into the midface and neuro-cranium via trajectories in the zygomaticarch, canine eminence, orbital rims, nasalbones and pterygoid plates (Shetty andCaputo 1995). However, most of the neuro-cranium, especially in infants, is virtuallyfree of masticatory compressive or distrac-tive forces. In growing cranium, the mainbiomechanical stresses loading areas of os-teosynthesis consist of pulsating intracra-nial pressure, expansive forces caused bythe growing brain and cranium, distractiveforces caused by scalp closing tensions andwound contraction, and compressive ex-tracranial forces, e.g., the pressure of thechild´s head against the contact area. Inthe literature, biomechanical analyses ofneurocranial osteosyntheses are very rare,and they are generally considered “non-loaded”. Gosain et al. studied the distrac-tive and compressive forces (parallel to theplate) to failure in plate osteosyntheses insheep cadaveric cranial bones (Gosain et al.1998). The distractive force of 270 N andcompressive force of 200 N broke the non-reinforced, stiff PLGA plate-screw fixation.
In clinical practice, acute forces of re-lapse are not always negligible, and thefixation system should be initially strong.As a result of the plasticity of infant neuro-cranium, semi-rigid fixation could possi-bly be more physiological than rigid fixa-tion, but it should not lead to collapse af-ter remodeling. The fixation system shoulddegrade fast enough to avoid restriction ofgrowth, which may be caused by plates
27
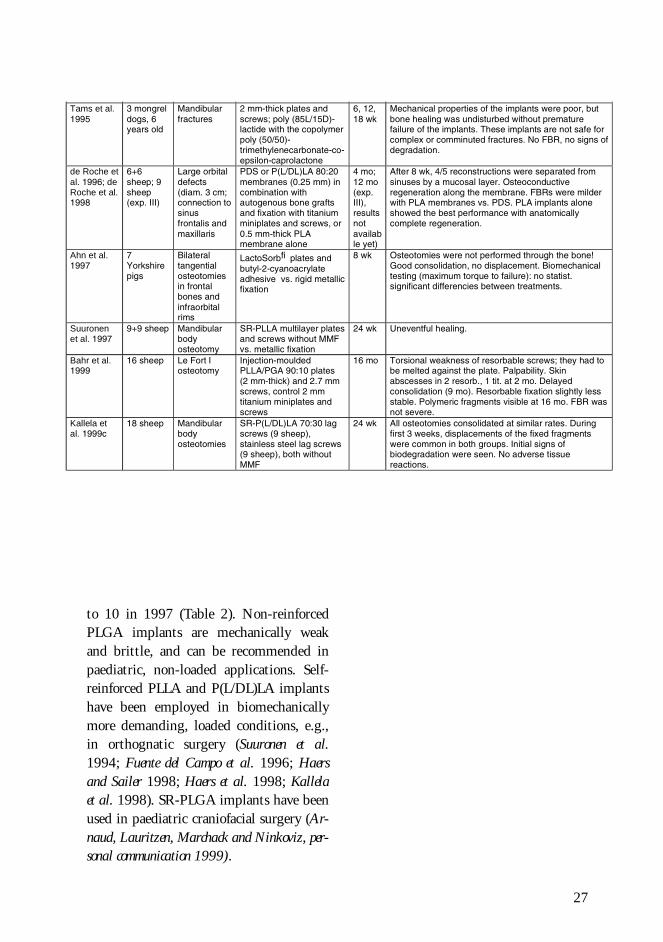
Tams et al.1995
3 mongreldogs, 6years old
Mandibularfractures
2 mm-thick plates andscrews; poly (85L/15D)-lactide with the copolymerpoly (50/50)-trimethylenecarbonate-co-epsilon-caprolactone
6, 12,18 wk
Mechanical properties of the implants were poor, butbone healing was undisturbed without prematurefailure of the implants. These implants are not safe forcomplex or comminuted fractures. No FBR, no signs ofdegradation.
de Roche etal. 1996; deRoche et al.1998
6+6sheep; 9sheep(exp. III)
Large orbitaldefects(diam. 3 cm;connection tosinusfrontalis andmaxillaris
PDS or P(L/DL)LA 80:20membranes (0.25 mm) incombination withautogenous bone graftsand fixation with titaniumminiplates and screws, or0.5 mm-thick PLAmembrane alone
4 mo;12 mo(exp.III),resultsnotavailable yet)
After 8 wk, 4/5 reconstructions were separated fromsinuses by a mucosal layer. Osteoconductiveregeneration along the membrane. FBRs were milderwith PLA membranes vs. PDS. PLA implants aloneshowed the best performance with anatomicallycomplete regeneration.
Ahn et al.1997
7Yorkshirepigs
Bilateraltangentialosteotomiesin frontalbones andinfraorbitalrims
LactoSorbfi plates andbutyl-2-cyanoacrylateadhesive vs. rigid metallicfixation
8 wk Osteotomies were not performed through the bone!Good consolidation, no displacement. Biomechanicaltesting (maximum torque to failure): no statist.significant differencies between treatments.
Suuronenet al. 1997
9+9 sheep Mandibularbodyosteotomy
SR-PLLA multilayer platesand screws without MMFvs. metallic fixation
24 wk Uneventful healing.
Bahr et al.1999
16 sheep Le Fort Iosteotomy
Injection-mouldedPLLA/PGA 90:10 plates(2 mm-thick) and 2.7 mmscrews, control 2 mmtitanium miniplates andscrews
16 mo Torsional weakness of resorbable screws; they had tobe melted against the plate. Palpability. Skinabscesses in 2 resorb., 1 tit. at 2 mo. Delayedconsolidation (9 mo). Resorbable fixation slightly lessstable. Polymeric fragments visible at 16 mo. FBR wasnot severe.
Kallela etal. 1999c
18 sheep Mandibularbodyosteotomies
SR-P(L/DL)LA 70:30 lagscrews (9 sheep),stainless steel lag screws(9 sheep), both withoutMMF
24 wk All osteotomies consolidated at similar rates. Duringfirst 3 weeks, displacements of the fixed fragmentswere common in both groups. Initial signs ofbiodegradation were seen. No adverse tissuereactions.
to 10 in 1997 (Table 2). Non-reinforcedPLGA implants are mechanically weakand brittle, and can be recommended inpaediatric, non-loaded applications. Self-reinforced PLLA and P(L/DL)LA implantshave been employed in biomechanicallymore demanding, loaded conditions, e.g.,in orthognatic surgery (Suuronen et al.1994; Fuente del Campo et al. 1996; Haersand Sailer 1998; Haers et al. 1998; Kallelaet al. 1998). SR-PLGA implants have beenused in paediatric craniofacial surgery (Ar-naud, Lauritzen, Marchack and Ninkoviz, per-sonal communication 1999).
28
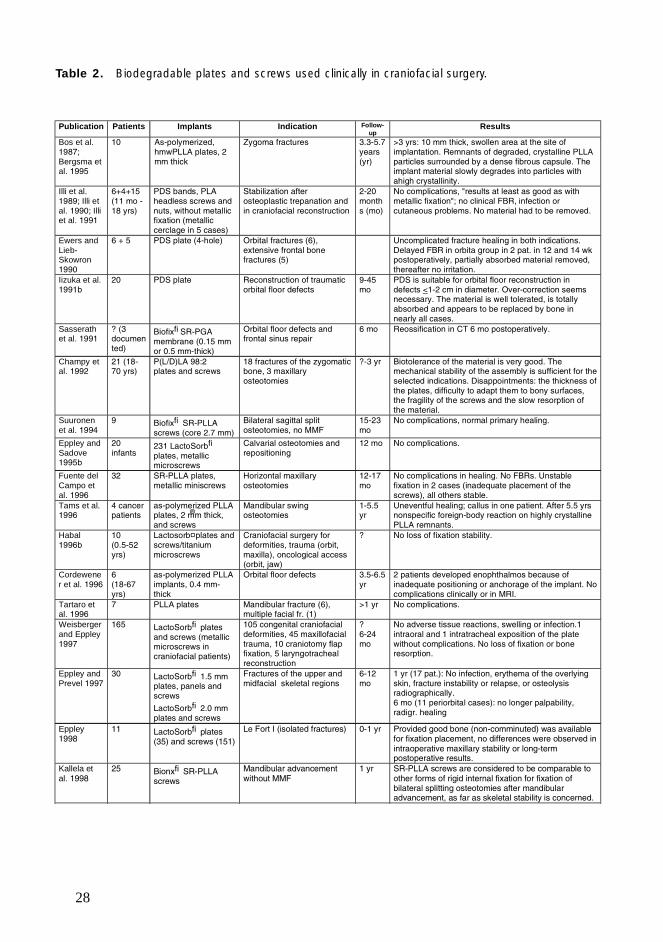
Publication Patients Implants Indication Follow-up
Results
Bos et al.1987;Bergsma etal. 1995
10 As-polymerized,hmwPLLA plates, 2mm thick
Zygoma fractures 3.3-5.7years(yr)
>3 yrs: 10 mm thick, swollen area at the site ofimplantation. Remnants of degraded, crystalline PLLAparticles surrounded by a dense fibrous capsule. Theimplant material slowly degrades into particles withahigh crystallinity.
Illi et al.1989; Illi etal. 1990; Illiet al. 1991
6+4+15(11 mo -18 yrs)
PDS bands, PLAheadless screws andnuts, without metallicfixation (metalliccerclage in 5 cases)
Stabilization afterosteoplastic trepanation andin craniofacial reconstruction
2-20months (mo)
No complications, "results at least as good as withmetallic fixation"; no clinical FBR, infection orcutaneous problems. No material had to be removed.
Ewers andLieb-Skowron1990
6 + 5 PDS plate (4-hole) Orbital fractures (6),extensive frontal bonefractures (5)
Uncomplicated fracture healing in both indications.Delayed FBR in orbita group in 2 pat. in 12 and 14 wkpostoperatively, partially absorbed material removed,thereafter no irritation.
Iizuka et al.1991b
20 PDS plate Reconstruction of traumaticorbital floor defects
9-45mo
PDS is suitable for orbital floor reconstruction indefects <1-2 cm in diameter. Over-correction seemsnecessary. The material is well tolerated, is totallyabsorbed and appears to be replaced by bone innearly all cases.
Sasserathet al. 1991
? (3documented)
Biofixfi SR-PGAmembrane (0.15 mmor 0.5 mm-thick)
Orbital floor defects andfrontal sinus repair
6 mo Reossification in CT 6 mo postoperatively.
Champy etal. 1992
21 (18-70 yrs)
P(L/D)LA 98:2plates and screws
18 fractures of the zygomaticbone, 3 maxillaryosteotomies
?-3 yr Biotolerance of the material is very good. Themechanical stability of the assembly is sufficient for theselected indications. Disappointments: the thickness ofthe plates, difficulty to adapt them to bony surfaces,the fragility of the screws and the slow resorption ofthe material.
Suuronenet al. 1994
9 Biofixfi SR-PLLAscrews (core 2.7 mm)
Bilateral sagittal splitosteotomies, no MMF
15-23mo
No complications, normal primary healing.
Eppley andSadove1995b
20infants
231 LactoSorbfi
plates, metallicmicroscrews
Calvarial osteotomies andrepositioning
12 mo No complications.
Fuente delCampo etal. 1996
32 SR-PLLA plates,metallic miniscrews
Horizontal maxillaryosteotomies
12-17mo
No complications in healing. No FBRs. Unstablefixation in 2 cases (inadequate placement of thescrews), all others stable.
Tams et al.1996
4 cancerpatients
as-polymerized PLLAplates, 2 mm thick,and screws
Mandibular swingosteotomies
1-5.5yr
Uneventful healing; callus in one patient. After 5.5 yrsnonspecific foreign-body reaction on highly crystallinePLLA remnants.
Habal1996b
10(0.5-52yrs)
Lactosorb¤ plates andscrews/titaniummicroscrews
Craniofacial surgery fordeformities, trauma (orbit,maxilla), oncological access(orbit, jaw)
? No loss of fixation stability.
Cordewener et al. 1996
6(18-67yrs)
as-polymerized PLLAimplants, 0.4 mm-thick
Orbital floor defects 3.5-6.5yr
2 patients developed enophthalmos because ofinadequate positioning or anchorage of the implant. Nocomplications clinically or in MRI.
Tartaro etal. 1996
7 PLLA plates Mandibular fracture (6),multiple facial fr. (1)
>1 yr No complications.
Weisbergerand Eppley1997
165 LactoSorbfi platesand screws (metallicmicroscrews incraniofacial patients)
105 congenital craniofacialdeformities, 45 maxillofacialtrauma, 10 craniotomy flapfixation, 5 laryngotrachealreconstruction
?6-24mo
No adverse tissue reactions, swelling or infection.1intraoral and 1 intratracheal exposition of the platewithout complications. No loss of fixation or boneresorption.
Eppley andPrevel 1997
30 LactoSorbfi 1.5 mmplates, panels andscrews
LactoSorbfi 2.0 mmplates and screws
Fractures of the upper andmidfacial skeletal regions
6-12mo
1 yr (17 pat.): No infection, erythema of the overlyingskin, fracture instability or relapse, or osteolysisradiographically.6 mo (11 periorbital cases): no longer palpability,radigr. healing
Eppley1998
11 LactoSorbfi plates(35) and screws (151)
Le Fort I (isolated fractures) 0-1 yr Provided good bone (non-comminuted) was availablefor fixation placement, no differences were observed inintraoperative maxillary stability or long-termpostoperative results.
Kallela etal. 1998
25 Bionxfi SR-PLLAscrews
Mandibular advancementwithout MMF
1 yr SR-PLLA screws are considered to be comparable toother forms of rigid internal fixation for fixation ofbilateral splitting osteotomies after mandibularadvancement, as far as skeletal stability is concerned.
Table 2. Biodegradable plates and screws used clinically in craniofacial surgery.
®
29
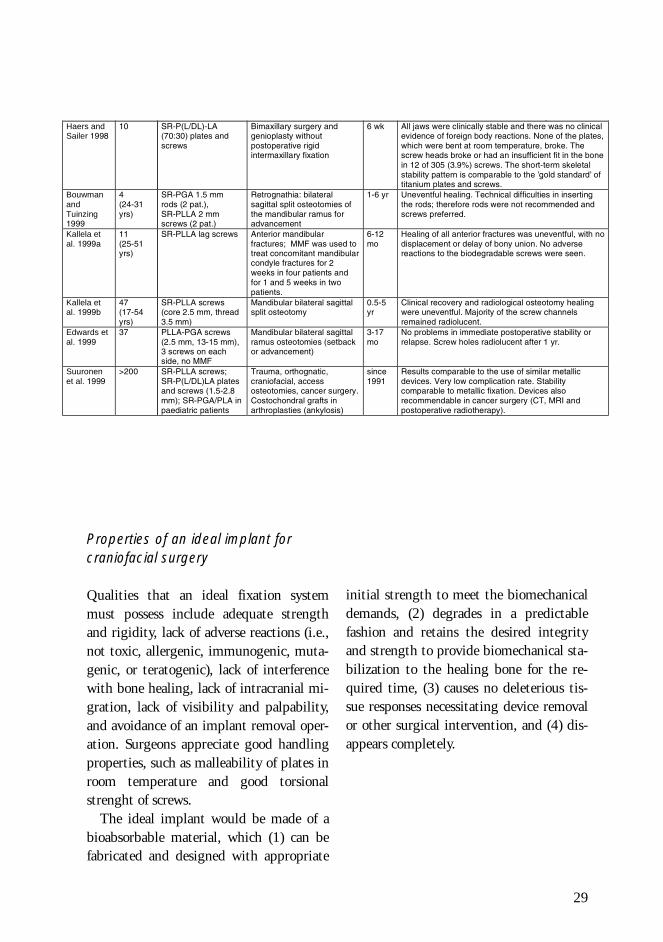
yHaers andSailer 1998
10 SR-P(L/DL)-LA(70:30) plates andscrews
Bimaxillary surgery andgenioplasty withoutpostoperative rigidintermaxillary fixation
6 wk All jaws were clinically stable and there was no clinicalevidence of foreign body reactions. None of the plates,which were bent at room temperature, broke. Thescrew heads broke or had an insufficient fit in the bonein 12 of 305 (3.9%) screws. The short-term skeletalstability pattern is comparable to the ’gold standard’ oftitanium plates and screws.
BouwmanandTuinzing1999
4(24-31yrs)
SR-PGA 1.5 mmrods (2 pat.),SR-PLLA 2 mmscrews (2 pat.)
Retrognathia: bilateralsagittal split osteotomies ofthe mandibular ramus foradvancement
1-6 yr Uneventful healing. Technical difficulties in insertingthe rods; therefore rods were not recommended andscrews preferred.
Kallela etal. 1999a
11(25-51yrs)
SR-PLLA lag screws Anterior mandibularfractures; MMF was used totreat concomitant mandibularcondyle fractures for 2weeks in four patients andfor 1 and 5 weeks in twopatients.
6-12mo
Healing of all anterior fractures was uneventful, with nodisplacement or delay of bony union. No adversereactions to the biodegradable screws were seen.
Kallela etal. 1999b
47(17-54yrs)
SR-PLLA screws(core 2.5 mm, thread3.5 mm)
Mandibular bilateral sagittalsplit osteotomy
0.5-5yr
Clinical recovery and radiological osteotomy healingwere uneventful. Majority of the screw channelsremained radiolucent.
Edwards etal. 1999
37 PLLA-PGA screws(2.5 mm, 13-15 mm),3 screws on eachside, no MMF
Mandibular bilateral sagittalramus osteotomies (setbackor advancement)
3-17mo
No problems in immediate postoperative stability orrelapse. Screw holes radiolucent after 1 yr.
Suuronenet al. 1999
>200 SR-PLLA screws;SR-P(L/DL)LA platesand screws (1.5-2.8mm); SR-PGA/PLA inpaediatric patients
Trauma, orthognatic,craniofacial, accessosteotomies, cancer surgery.Costochondral grafts inarthroplasties (ankylosis)
since1991
Results comparable to the use of similar metallicdevices. Very low complication rate. Stabilitycomparable to metallic fixation. Devices alsorecommendable in cancer surgery (CT, MRI andpostoperative radiotherapy).
Properties of an ideal implant forcraniofacial surgery
Qualities that an ideal fixation systemmust possess include adequate strengthand rigidity, lack of adverse reactions (i.e.,not toxic, allergenic, immunogenic, muta-genic, or teratogenic), lack of interferencewith bone healing, lack of intracranial mi-gration, lack of visibility and palpability,and avoidance of an implant removal oper-ation. Surgeons appreciate good handlingproperties, such as malleability of plates inroom temperature and good torsionalstrenght of screws.
The ideal implant would be made of abioabsorbable material, which (1) can befabricated and designed with appropriate
initial strength to meet the biomechanicaldemands, (2) degrades in a predictablefashion and retains the desired integrityand strength to provide biomechanical sta-bilization to the healing bone for the re-quired time, (3) causes no deleterious tis-sue responses necessitating device removalor other surgical intervention, and (4) dis-appears completely.
31
THE PRESENT STUDY
Aims of the study
The study was aimed at answering the following questions:
What is the nature of the basic consolidation process of a craniotomy line, whenplated with a titanium plate and an SR-PLLA plate?What is the biocompatibility of these implants, and what is the biodegradationrate of an SR-PLLA plate?(Paper I)
Radiographic assessment of these two kinds of plated craniotomy lines: is thereany difference in assessing the consolidation process of the lines?(Paper II)
What is the biocompatibility of and tissue reactions to an SR-PLLA plate in anintraosseous environment in sheep cranial membranous bone?(Paper III)
Can a non-reinforced, flexible, membrane-like PLA96 plate be used for fixation ofunstable craniotomies in lambs?What is its biocompatibility, effect on the consolidation process, and rate of bio-absorption?(Papers IV and V)
Can SR-PLLA and SR-PGA miniscrews be used for plate fixation of lamb cranialbones?What is their biocompatibility and rate of bioabsorption in lamb neurocranium?(Papers IV and V)
32
MATERIALS AND METHODS
Study n Follow-up time (weeks)
4 6 12 20 26 52 104
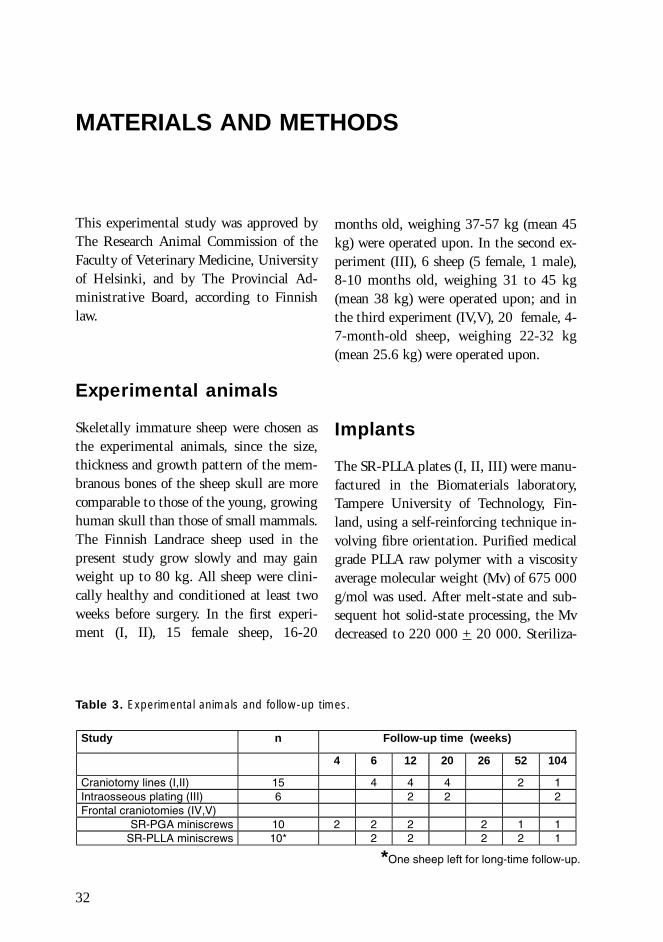
Craniotomy lines (I,II) 15 4 4 4 2 1Intraosseous plating (III) 6 2 2 2Frontal craniotomies (IV,V)
SR-PGA miniscrews 10 2 2 2 2 1 1SR-PLLA miniscrews 10* 2 2 2 2 1
*One sheep left for long-time follow-up.
Table 3. Experimental animals and follow-up times.
This experimental study was approved byThe Research Animal Commission of theFaculty of Veterinary Medicine, Universityof Helsinki, and by The Provincial Ad-ministrative Board, according to Finnishlaw.
Experimental animals
Skeletally immature sheep were chosen asthe experimental animals, since the size,thickness and growth pattern of the mem-branous bones of the sheep skull are morecomparable to those of the young, growinghuman skull than those of small mammals.The Finnish Landrace sheep used in thepresent study grow slowly and may gainweight up to 80 kg. All sheep were clini-cally healthy and conditioned at least twoweeks before surgery. In the first experi-ment (I, II), 15 female sheep, 16-20
months old, weighing 37-57 kg (mean 45kg) were operated upon. In the second ex-periment (III), 6 sheep (5 female, 1 male),8-10 months old, weighing 31 to 45 kg(mean 38 kg) were operated upon; and inthe third experiment (IV,V), 20 female, 4-7-month-old sheep, weighing 22-32 kg(mean 25.6 kg) were operated upon.
Implants
The SR-PLLA plates (I, II, III) were manu-factured in the Biomaterials laboratory,Tampere University of Technology, Fin-land, using a self-reinforcing technique in-volving fibre orientation. Purified medicalgrade PLLA raw polymer with a viscosityaverage molecular weight (Mv) of 675 000g/mol was used. After melt-state and sub-sequent hot solid-state processing, the Mvdecreased to 220 000 + 20 000. Steriliza-

33
tion by gamma irradiation with a mini-mum dose of 25 kGy further decreased theMv to 50 000 + 5 000. The percentagecrystallinity of the implants was 50 + 5 %as determined by DSC measurements. Theplates were punched, the 1.5 mm holes be-ing at the apices of an equilateral triangle,the side of which was 3 mm. The plex-iglass-like plates were 0.5 mm thick, 12mm wide, and originally 30 mm long butwere shortened with scissors to the desiredlength at operation. Titanium miniscrewswere used for fixation of the SR-PLLAplates (I, II).
The P(L/D)LA (96/4) plates (PLA96)and SR-PLLA and SR-PGA miniscrews(IV,V) were manufactured at Tampere Uni-versity of Technology, Tampere, Finland.The stereocopolymeric plates (researchsamples) were non-reinforced and non-ori-ented, and composed of 96% L- and 4%D-lactide, processed by compressionmoulding and gamma-sterilized (2.5Mrad). The 0.4 mm-thick, transparent,flexible, punched sheets were cut withscissors to 20 x 30 mm at operation. TheSR-PLLA and SR-PGA miniscrews wereprocessed by compression molding (diame-ter 2 mm, core 1.5 mm, length 5-8 mm,Biofix®, Tampere, Finland) and equippedwith cross heads. A special tapping instru-ment for these screws was used. When nec-essary, long screws were shortened with athin oscillating saw or a hot wire loop.
The 4-hole titanium miniplates (0,6x4x25mm, OsteoFix Inc., Oulu, Finland) werefixed with 3 mm- and 5 mm-long self-tap-ping titanium miniscrews (diameter 2 mm,core 1.5 mm, OsteoFix Inc., Oulu, Finland),four screws in one plate (I, II, IV, V).
Preoperative procedure,anaesthesia andpostoperative care
Food was withheld for two days preopera-tively. Water was supplied ad libitum. Me-detomidine at 20 microg per kg bwt wasgiven intravenously (iv). Anaesthesia wasinduced iv by using propofol at 3 mg perkg bwt and maintained with 2-2.5 % ha-lothane. The sheep were intubated and po-sitioned in sternal recumbency with thehead extended and fixed on a cushion.During the operation, 1000 ml of iv fluid(Ringersteril®, Medipolar, Oulu, Finland),metronidazole at 11 mg/kg iv, and ben-zylpenicillin sodium at 35 000 IU/kg ivwere administered. Methylcellulose eye-drops (Oftan-MC®, Leiras, Finland) wereused to avoid ocular drying and irritation.The entire head was shaved, washed, andsterilized with chlorhexidine gluconate.10-20 ml lidocain cum adrenalin (Lidocain10 mg/ml c. adrenalin®, Medipolar, Oulu,Finland) was injected subcutaneously inthe operative area. Before the animals re-covered (in the third experiment), Flunixin(Finadyne® 50 mg/ml, Orion, Espoo, Fin-land), 2.2 mg/kg, was administered.
Postoperatively, the sheep were returnedto their pens and fed ad libitum. Ben-zylpenicillinprocaine (Ethacilin vet injekt®
300 000 IU/ml, Intervet, Boxmeer, Hol-land), 35 000 IU/kg sc as infection proph-ylaxis, and phenylbutazone (Reumuzol®
vet injekt 200 mg/ml, Lääkefarmos,Turku, Finland), 8 mg/kg iv as an analge-sic were administered once a day for threedays. Before euthanasia the sheep werestunned with electricity.
34
� � !��!����
����������
������ ����
�"����� ����
���#�
$�"�
�
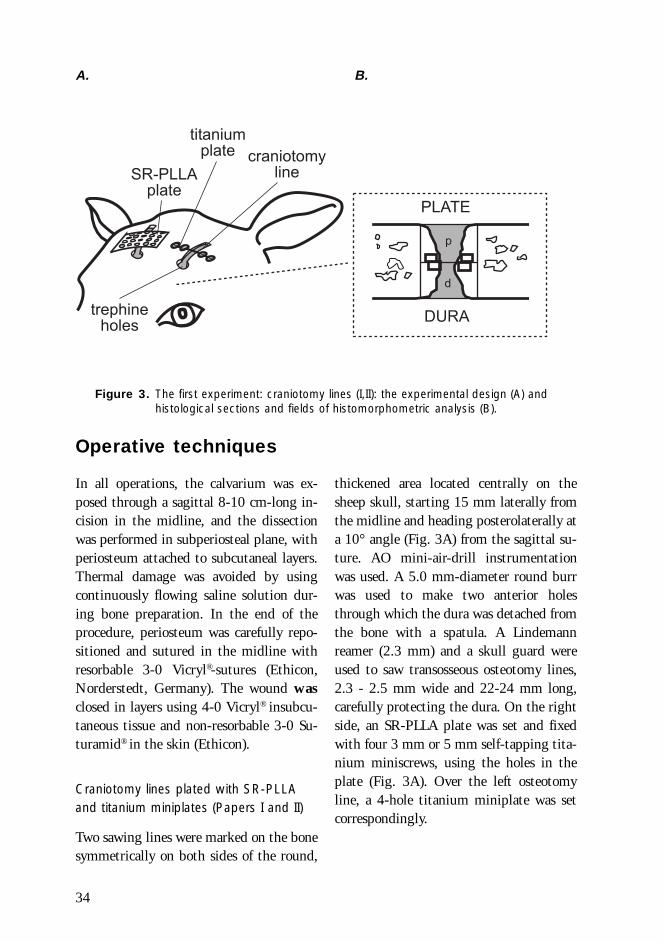
Figure 3. The first experiment: craniotomy lines (I,II): the experimental design (A) andhistological sections and fields of histomorphometric analysis (B).
Operative techniques
In all operations, the calvarium was ex-posed through a sagittal 8-10 cm-long in-cision in the midline, and the dissectionwas performed in subperiosteal plane, withperiosteum attached to subcutaneal layers.Thermal damage was avoided by usingcontinuously flowing saline solution dur-ing bone preparation. In the end of theprocedure, periosteum was carefully repo-sitioned and sutured in the midline withresorbable 3-0 Vicryl®-sutures (Ethicon,Norderstedt, Germany). The wound wasclosed in layers using 4-0 Vicryl® insubcu-taneous tissue and non-resorbable 3-0 Su-turamid® in the skin (Ethicon).
Craniotomy lines plated with SR-PLLAand titanium miniplates (Papers I and II)
Two sawing lines were marked on the bonesymmetrically on both sides of the round,
thickened area located centrally on thesheep skull, starting 15 mm laterally fromthe midline and heading posterolaterally ata 10° angle (Fig. 3A) from the sagittal su-ture. AO mini-air-drill instrumentationwas used. A 5.0 mm-diameter round burrwas used to make two anterior holesthrough which the dura was detached fromthe bone with a spatula. A Lindemannreamer (2.3 mm) and a skull guard wereused to saw transosseous osteotomy lines,2.3 - 2.5 mm wide and 22-24 mm long,carefully protecting the dura. On the rightside, an SR-PLLA plate was set and fixedwith four 3 mm or 5 mm self-tapping tita-nium miniscrews, using the holes in theplate (Fig. 3A). Over the left osteotomyline, a 4-hole titanium miniplate was setcorrespondingly.
A. B.
35
���#�
��"%��#��&
$�"�
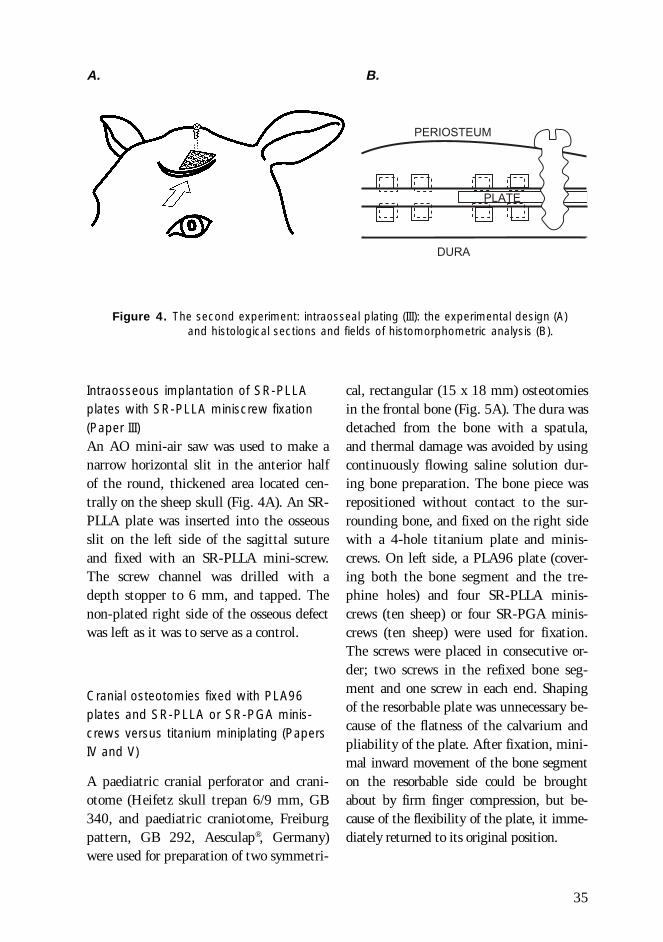
Intraosseous implantation of SR-PLLAplates with SR-PLLA miniscrew fixation(Paper III)An AO mini-air saw was used to make anarrow horizontal slit in the anterior halfof the round, thickened area located cen-trally on the sheep skull (Fig. 4A). An SR-PLLA plate was inserted into the osseousslit on the left side of the sagittal sutureand fixed with an SR-PLLA mini-screw.The screw channel was drilled with adepth stopper to 6 mm, and tapped. Thenon-plated right side of the osseous defectwas left as it was to serve as a control.
Cranial osteotomies fixed with PLA96plates and SR-PLLA or SR-PGA minis-crews versus titanium miniplating (PapersIV and V)
A paediatric cranial perforator and crani-otome (Heifetz skull trepan 6/9 mm, GB340, and paediatric craniotome, Freiburgpattern, GB 292, Aesculap®, Germany)were used for preparation of two symmetri-
Figure 4. The second experiment: intraosseal plating (III): the experimental design (A)and histological sections and fields of histomorphometric analysis (B).
A. B.
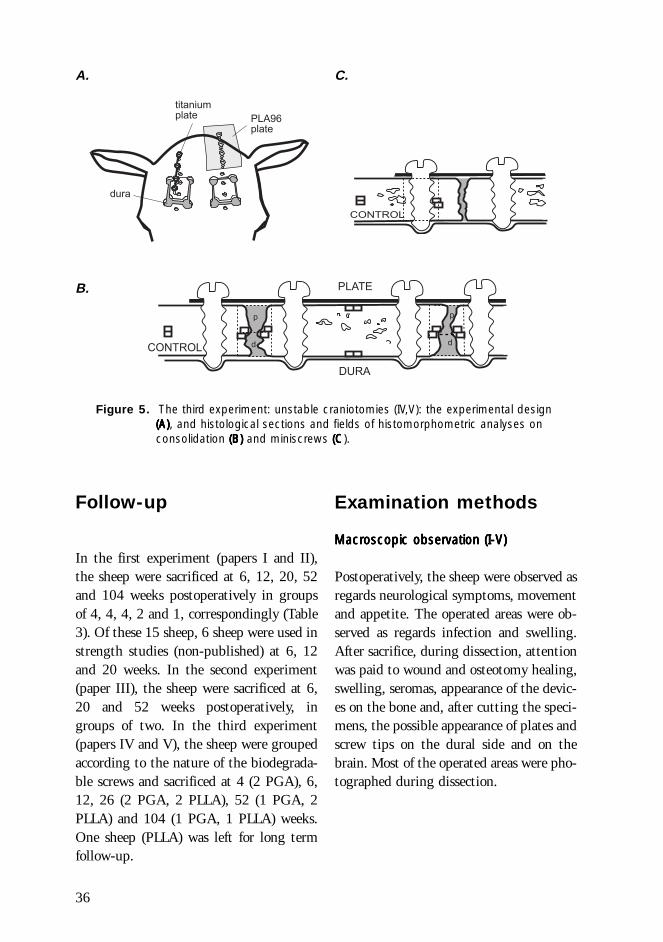
cal, rectangular (15 x 18 mm) osteotomiesin the frontal bone (Fig. 5A). The dura wasdetached from the bone with a spatula,and thermal damage was avoided by usingcontinuously flowing saline solution dur-ing bone preparation. The bone piece wasrepositioned without contact to the sur-rounding bone, and fixed on the right sidewith a 4-hole titanium plate and minis-crews. On left side, a PLA96 plate (cover-ing both the bone segment and the tre-phine holes) and four SR-PLLA minis-crews (ten sheep) or four SR-PGA minis-crews (ten sheep) were used for fixation.The screws were placed in consecutive or-der; two screws in the refixed bone seg-ment and one screw in each end. Shapingof the resorbable plate was unnecessary be-cause of the flatness of the calvarium andpliability of the plate. After fixation, mini-mal inward movement of the bone segmenton the resorbable side could be broughtabout by firm finger compression, but be-cause of the flexibility of the plate, it imme-diately returned to its original position.
36
�
�
�'
��(#"��
Follow-up
In the first experiment (papers I and II),the sheep were sacrificed at 6, 12, 20, 52and 104 weeks postoperatively in groupsof 4, 4, 4, 2 and 1, correspondingly (Table3). Of these 15 sheep, 6 sheep were used instrength studies (non-published) at 6, 12and 20 weeks. In the second experiment(paper III), the sheep were sacrificed at 6,20 and 52 weeks postoperatively, ingroups of two. In the third experiment(papers IV and V), the sheep were groupedaccording to the nature of the biodegrada-ble screws and sacrificed at 4 (2 PGA), 6,12, 26 (2 PGA, 2 PLLA), 52 (1 PGA, 2PLLA) and 104 (1 PGA, 1 PLLA) weeks.One sheep (PLLA) was left for long termfollow-up.
Figure 5. The third experiment: unstable craniotomies (IV,V): the experimental design(A)(A)(A)(A)(A), and histological sections and fields of histomorphometric analyses onconsolidation (B) (B) (B) (B) (B) and miniscrews (C(C(C(C(C).
Examination methods
MacrMacrMacrMacrMacroscopic observation (I-V)oscopic observation (I-V)oscopic observation (I-V)oscopic observation (I-V)oscopic observation (I-V)
Postoperatively, the sheep were observed asregards neurological symptoms, movementand appetite. The operated areas were ob-served as regards infection and swelling.After sacrifice, during dissection, attentionwas paid to wound and osteotomy healing,swelling, seromas, appearance of the devic-es on the bone and, after cutting the speci-mens, the possible appearance of plates andscrew tips on the dural side and on thebrain. Most of the operated areas were pho-tographed during dissection.
A.
B.
C.
���)* ����
������ ����
�� �
���#�
��(#"��
$�"�
�
�- - -

37
Histology (I-V)
The operated areas were dissected free ofskin and cut away from the skull with anoscillating saw. The titanium material wasremoved. The specimens were fixed in a se-ries of ethanol solutions of rising concen-tration (70-99%) and embedded in methyl-methacrylate. Five-micrometer-thick sectionswere cut in the middle of the plated area,perpendicular to the osteotomy line (I-III)(Figs. 3B and 4B), or through the screw line(IV,V) (Fig. 5B), with a Reichert-Jung mi-crotome (Nussloch, Germany) and stainedby using modified Masson-Goldner tri-chrome (Goldner 1938) and haematoxylin-eosin methods. Polarizing microscopy wasused to identify birefringent polymericmaterial in the specimens. The presence ofinflammatory cells within the samplefields was assessed qualitatively, using amagnification of 400 x for cell identifica-tion. The findings were checked by an ex-perienced pathologist.
Microradiography and OTC-fluorescence(I, II)In the first experiment (I, II), oxytetracy-cline hydrocloride (5 mg/kg iv), was in-jected 13 and 9 days before the end of thefollow-up time to mark newly-formedbone in tetracycline-labelling studies(Milch et al. 1958). For tetracycline fluores-cence and contact microradiography stud-ies, 80-micrometer-thick sections were cutwith a Leitz Saw Microtome 1600 (Wet-zlar, Germany). For contact microradiogra-phy (Faxitron X-ray system, Model 43855A, Hewlett Packard), IMTEC film wasused (High Resolution Plates, Ultra flat,Type 1A, Sunnyvale, California, USA), andthe technical values were 21 kV, 3 mA,with a 15 min exposure time and 0 cmfilm-focus distance. Fluorescence microsco-py was performed using an HBO 220 ul-traviolet lamp (Osram, Berlin, Germany)and a Leitz BG 812/6 primary filter (Wet-zlar, Germany). As the quality of the histo-logical sections was excellent, these meth-ods did not add a great deal of further in-formation and were used only in the firstexperiment.
Experiment n(sheep)
Histology
OTC-fluorescence
Histomorphom.
Micro-radiography
Radio-graphy
CT MRI Tensilestrength
Craniotomy lines (I) 9 9 9 9Craniotomy lines (non-publ.) 6 6Craniotomy lines (II) 9 9 9 9Intraosseous plating (III) 6 6 6Unstable craniotomies (IV,V)
SR-PGA miniscrews 10 10 10 10 10SR-PLLA miniscrews 10* 9 9 1** 1**
*One sheep left for long-term follow-up.**104-week follow-up
Table 4. Experiments and the examination methods.

38
Histomorphometry (I, III- V)
In each study (I,III-V), all histologicalspecimens were quantitatively analyzed fordifferent parameters histomorphometrical-ly (Revell 1983). A Leitz Diaplan micro-scope (Leitz, Wetzlar, Germany) waslinked via a television video camera to asemiautomatic imaging analysis system(Kontron MOP Videoplan, Munich, Ger-many). The microscopic field was shownon a visual display unit. Measurements ofsurface areas on the screen were carried outmanually by using a digitizer and a cursor.The technique was practised by repeatingseries of measurements until the resultswere reproducible.
In the first experiment (I), two standard-ized sample fields of 4.01 x 2.39 mm weredelineated above and below the midline ofthe osteotomy to the overall pericranialand endocranial levels, thus reflecting theplated (p) and dural (d) sides of the osteot-omy, correspondingly (Fig. 3B). The size ofthe non-ossified area (remaining bone de-fect) and the trabecular bone fraction ofthe whole tissue area on each side weremeasured. Within the sample fields, themarginal zone of the proliferating bone inthe middle of the osteotomy (Fig. 3B) wassystematically examined (using a magnifi-cation x 100) as regards the total trabecu-lar bone volume fraction (including calci-fied trabeculae and osteoid), the total oste-oid surface fraction (of the trabecular bonesurface), and the active osteoid formationsurface fraction (osteoid surface covered byactive osteoblasts). Four sample fields wereanalyzed in each specimen. Ongoing calci-fication of osteoid was confirmed by fluo-rescence microscopy.
In the second experiment (III), connectivetissue initially filled the created bone de-
fect. Replacement of the connective tissueby bone tissue and formation of osteoidwere measured on both the plated and thecontrol sides. Four sample fields of 0.37 x0.61 mm (magnification x 100) were de-lineated in the host tissue - implant inter-face to measure the percentage of connec-tive tissue in the total tissue volume (Fig.4B). Another four fields were delineated inthe bone adjacent to the connective tissuecapsule, and a corresponding number offields on the contralateral side to measurethe total trabecular bone volume fraction,including calcified trabeculae and osteoid,the total osteoid surface fraction, and theactive osteoid formation surface fraction.
In the third experiment (IV,V), principallythe same protocol was used as in the firstexperiment. The non-consolidated bonedefect areas (IV) were measured in win-dows corresponding to the original bonedefect (original width 2.35 mm, windowwidth 2.39 mm), using a magnification ofx 16 (Fig. 5B). The percentage of remain-ing defect was taken to be the mean valueof the plate (p) sides and dural (d) sides.New bone formation was analyzed in de-tail using a magnification of x 100 in tenstandardized windows (0.37 x 0.61 mm)(Fig. 5B). The areas of interest were theconsolidating bone defect (four fields; themore poorly consolidated line was select-ed), the plate/periosteal and dural sides ofthe fixed bone segment (two fields each,measurements in the intact dural area) andthe control area (two fields). The controlarea was selected in the same specimen inintact bone in the same sagittal planewhere the periosteum had been elevated.
Resorption of the polymeric material inthe screw channels and the effect of the pol-ymer on formation of new bone around thechannel were also analyzed (V) (Fig. 5C).
39
The screw channels were analyzed at amagnification of x 16, and 2.39 mm-widesample fields were delineated inside thebone tissue with the screw channel in themiddle. Because cutting the specimens ex-actly in the middle of all the screws orscrew channels was technically impossible,only the screws cut in the middle or chan-nels of maximum width were included inthe analysis. The percentage of tissue otherthan bone (including connective tissue andpolymeric material in the screw channel)and the percentage of polymeric materialin the total tissue volume were measured.Two smaller fields (0.37 x 0.61 mm) be-side the screw in the middle of the boneand outside the osteotomized segment inintact bone in the same section (control),were analyzed for total trabecular bone vol-ume fraction and osteoid surface fraction,using a magnification of x 100.
Radiography (II, IV, V)
In the first experiment (II), after sacrifice,the osteotomies in each skull were exam-ined by using tangential plain films (set-tings of 57 kV and 32 mAs and 120 cmfocus-object). The radiographs were evalu-ated as regards visibility of the osteotomyand osteosynthesis devices, new bone for-mation, osteolysis, and union of the osteot-omy.
In the third experiment (IV, V), thespecimens containing SR-PGA screws andthe two-year follow-up sheep with SR-PLLA screws, with their contralateral tita-nium-fixed counterparts, were investigatedby plain film radiography. Osteotomizedcalvarial areas were dissected free of softtissue and removed with an oscillatingsaw. The bone specimens were examined inanteroposterior (AP) and tangential direc-
tions (settings of 48 kV, 25-32 mAs and42-44 kV, 25 mAs, and 100 cm focus-ob-ject). The AP images were analyzed as fol-lows: The four trepanation holes weremeasured in two perpendicular directions.The result was expressed as the mean di-ameter of the four holes (IV). The minis-crew holes were measured for their greatestdiameter (V). The length of the visible os-teotomy line was measured and expressedas a percentage of the length of the origi-nal osteotomy line (IV). All measurementswere performed by a radiologist using amagnifying lens (x7, with a precision scaleof 0.1 mm).
Computerized tomography (II)
In the first experiment (II), after sacrifice,the skulls were examined by CT. Contigu-ous 3 mm-thick coronal slices were takenfrom the skulls of the first 6 sheep with ascanner (Philips, Tomoscan 60/TX, Tokyo,Japan). A field of view (FOV) of 25 cm, awindow of 2200-2500 Houndsfield Units(HU) and a level of 250-300 HU wereused. The 2 last sheep, at the time of 52weeks« follow-up, were examined by spiralCT (GE HiSpeed Advantage, Milwaukee,Wisconsin, U.S.A.). The 3 mm-thick sliceswere imaged in the coronal plane. An FOVof 12.5 cm, a window of 2200 HU and alevel of 600 HU were used. Blurring of theedges of the osteotomy line, new bone for-mation and bone bridges were regarded asradiographic signs of healing of the osteot-omy. The integrity of the screws and plateswas analyzed, and any migration or break-age of the material was noted.

40
Magnetic resonance imaging (IV)
In the third experiment (IV,V), the skullscontaining SR-PGA screws and the two-year follow-up sheep with SR-PLLA screwswere investigated by magnetic resonanceimaging (MRI) and plain film radiography,because PGA implants in particular andPLLA implants in the long term may beassociated with osteolytic reactions and for-eign-body reactions. MRI was performedusing a 0.1 T resistive unit (Merit, PickerNordstar Co., Helsinki) and a head coil. Ascout image in a coronal direction wasused to locate the craniotomy areas. Re-gions of the craniotomies were imaged incontiguous oblique slices. The examina-tion included a T1-weighted pulse se-quence (PS3D 125/20) with a flip angle of80 degrees and a T2-weighted pulse se-quence (PS 100-40) with a flip angle of 90degrees. The image acquisition time was 5min 24 s for the T1 images and 7 min 12 sfor the T2 images. The slice thicknesseswere 3 mm and 5 mm respectively, and thematrix ,144 x 256.
Mechanical testing procedure(unpublished)
The operated areas were carefully dissectedand removed with an oscillating saw alongthe border of the SR-PLLA plate, and a cor-
responding area on the titanium plated side.In 6-week specimens the SR-PLLA plate wasremoved; in other specimens the SR-PLLAplate could not be removed. All titaniummaterial was removed before testing. Thespecimens were kept in saline solution untilmechanical testing was carried out (within24 hours). Testing was performed at 20°Cwith a J.J. Lloyd testing machine (J.J. LloydInstruments, Southampton, England) at atesting speed 10 mm/min.
Tensile strength was measured along thelong axis (Fig. 6). The specimens were at-tached at both ends, and the free testinglength was 10 mm. Tensile strength wascalculated by using a formula:strength = F / A [MPa]
Statistical methods
The numerical data obtained in histomor-phometry allowed the results to be evalu-ated by statistical methods (I, IV,V). In thefirst experiment (I), paired t-tests with onetailed interpretation and two-way analysisof variance were used. In the third experi-ment (IV,V), repeated analyses of varianceand two-way analysis of variance wereused. P values less than 0.05 were consid-ered statistically significant. The statisticalanalysis was performed by a statistical ex-pert.
Figure 6.Tensile strength testingarrangements. The piece ofbone with craniotomy in themiddle was fixed by metallicthreads going through thescrew holes (screws re-moved).
�"����� ����
� �+�!�������������
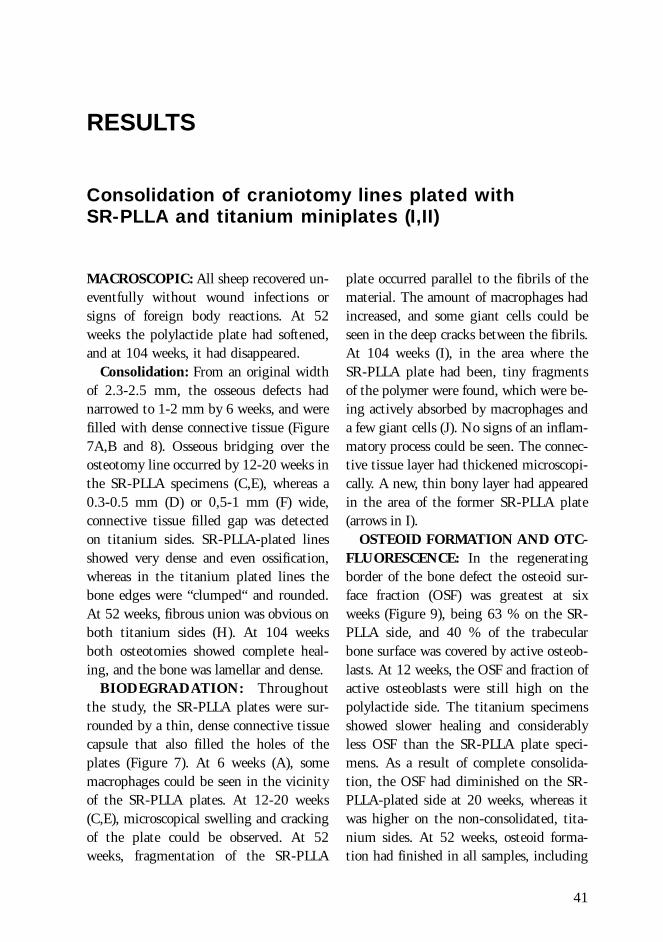
41
RESULTS
Consolidation of craniotomy lines plated withSR-PLLA and titanium miniplates (I,II)
MACROSCOPIC: All sheep recovered un-eventfully without wound infections orsigns of foreign body reactions. At 52weeks the polylactide plate had softened,and at 104 weeks, it had disappeared.
Consolidation: From an original widthof 2.3-2.5 mm, the osseous defects hadnarrowed to 1-2 mm by 6 weeks, and werefilled with dense connective tissue (Figure7A,B and 8). Osseous bridging over theosteotomy line occurred by 12-20 weeks inthe SR-PLLA specimens (C,E), whereas a0.3-0.5 mm (D) or 0,5-1 mm (F) wide,connective tissue filled gap was detectedon titanium sides. SR-PLLA-plated linesshowed very dense and even ossification,whereas in the titanium plated lines thebone edges were “clumped“ and rounded.At 52 weeks, fibrous union was obvious onboth titanium sides (H). At 104 weeksboth osteotomies showed complete heal-ing, and the bone was lamellar and dense.
BIODEGRADATION: Throughoutthe study, the SR-PLLA plates were sur-rounded by a thin, dense connective tissuecapsule that also filled the holes of theplates (Figure 7). At 6 weeks (A), somemacrophages could be seen in the vicinityof the SR-PLLA plates. At 12-20 weeks(C,E), microscopical swelling and crackingof the plate could be observed. At 52weeks, fragmentation of the SR-PLLA
plate occurred parallel to the fibrils of thematerial. The amount of macrophages hadincreased, and some giant cells could beseen in the deep cracks between the fibrils.At 104 weeks (I), in the area where theSR-PLLA plate had been, tiny fragmentsof the polymer were found, which were be-ing actively absorbed by macrophages anda few giant cells (J). No signs of an inflam-matory process could be seen. The connec-tive tissue layer had thickened microscopi-cally. A new, thin bony layer had appearedin the area of the former SR-PLLA plate(arrows in I).
OSTEOID FORMATION AND OTC-FLUORESCENCE: In the regeneratingborder of the bone defect the osteoid sur-face fraction (OSF) was greatest at sixweeks (Figure 9), being 63 % on the SR-PLLA side, and 40 % of the trabecularbone surface was covered by active osteob-lasts. At 12 weeks, the OSF and fraction ofactive osteoblasts were still high on thepolylactide side. The titanium specimensshowed slower healing and considerablyless OSF than the SR-PLLA plate speci-mens. As a result of complete consolida-tion, the OSF had diminished on the SR-PLLA-plated side at 20 weeks, whereas itwas higher on the non-consolidated, tita-nium sides. At 52 weeks, osteoid forma-tion had finished in all samples, including
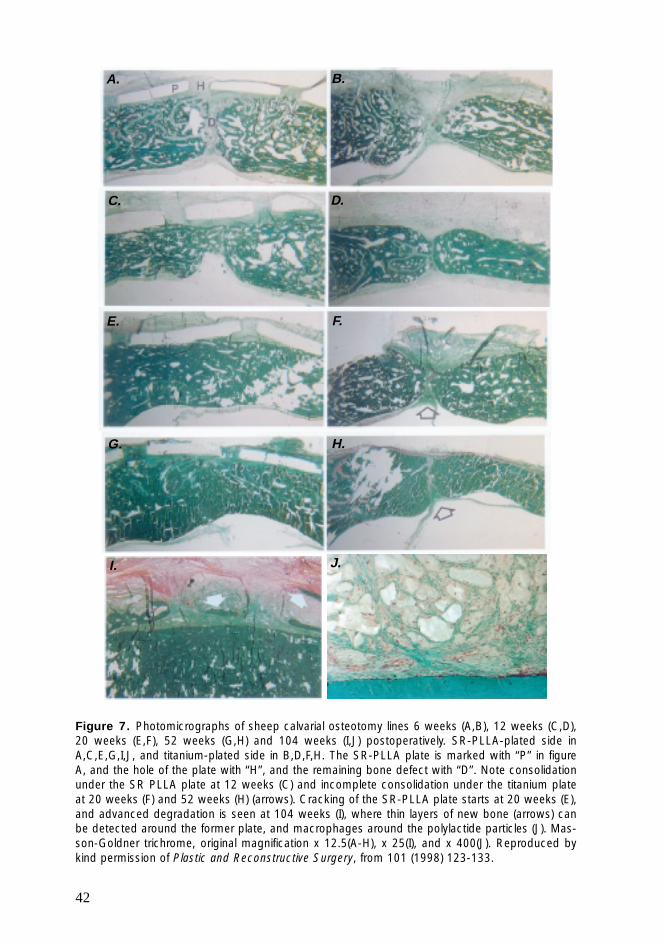
42
Figure 7. Photomicrographs of sheep calvarial osteotomy lines 6 weeks (A,B), 12 weeks (C,D),20 weeks (E,F), 52 weeks (G,H) and 104 weeks (I,J) postoperatively. SR-PLLA-plated side inA,C,E,G,I,J, and titanium-plated side in B,D,F,H. The SR-PLLA plate is marked with “P” in figureA, and the hole of the plate with “H”, and the remaining bone defect with “D”. Note consolidationunder the SR PLLA plate at 12 weeks (C) and incomplete consolidation under the titanium plateat 20 weeks (F) and 52 weeks (H) (arrows). Cracking of the SR-PLLA plate starts at 20 weeks (E),and advanced degradation is seen at 104 weeks (I), where thin layers of new bone (arrows) canbe detected around the former plate, and macrophages around the polylactide particles (J). Mas-son-Goldner trichrome, original magnification x 12.5(A-H), x 25(I), and x 400(J). Reproduced bykind permission of Plastic and Reconstructive Surgery, from 101 (1998) 123-133.
A. B.
C. D.
E. F.
G. H.
I. J.
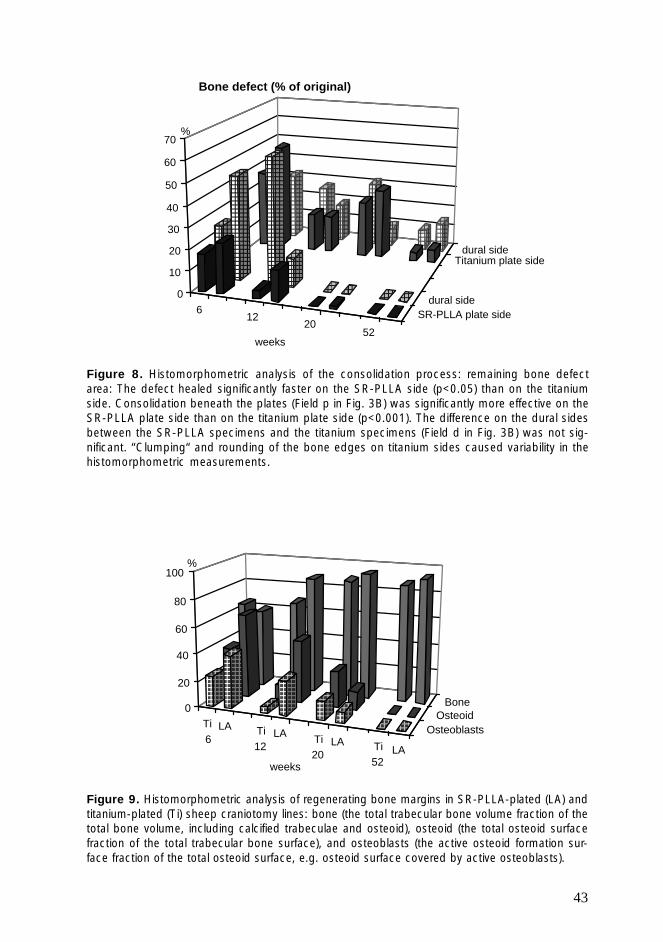
43
Ti6
LA Ti12
LA Ti20
LA Ti52
LA
OsteoblastsOsteoid
Bone
������������������
������������
��������
������������������������������
��������������������
����������������
�����������������
��������������������
����������������
��������������������
����������
���������������� ����
�������������������
��������������� ����������
������������
0
20
40
60
80
100
weeks
%
612
2052
SR-PLLA plate sidedural side
Titanium plate sidedural side
������������������������������
������������������������
�������������� ����
����������������
����������������
������������ ����
����������������
������������
������������ ����
������������
���������
������������
��������������������
��������������������
�����
������
�������������� ����
������������������
������������
������������
���������������
���������������
����������������
����������������
������������������������������������������������
�����������������������������������
����������������
������������������������������������������������������������
���������������������������������������������
����������������
����������������
������������
��������������
������������
�������������� ��������������� ����
��������������������������
�����������
��������������0
10
20
30
40
50
60
70
weeks
%
Bone defect (% of original)
Figure 8. Histomorphometric analysis of the consolidation process: remaining bone defectarea: The defect healed significantly faster on the SR-PLLA side (p<0.05) than on the titaniumside. Consolidation beneath the plates (Field p in Fig. 3B) was significantly more effective on theSR-PLLA plate side than on the titanium plate side (p<0.001). The difference on the dural sidesbetween the SR-PLLA specimens and the titanium specimens (Field d in Fig. 3B) was not sig-nificant. “Clumping“ and rounding of the bone edges on titanium sides caused variability in thehistomorphometric measurements.
Figure 9. Histomorphometric analysis of regenerating bone margins in SR-PLLA-plated (LA) andtitanium-plated (Ti) sheep craniotomy lines: bone (the total trabecular bone volume fraction of thetotal bone volume, including calcified trabeculae and osteoid), osteoid (the total osteoid surfacefraction of the total trabecular bone surface), and osteoblasts (the active osteoid formation sur-face fraction of the total osteoid surface, e.g. osteoid surface covered by active osteoblasts).

44
Figure 10. Microradiography: SR-PLLA-plated specimens on the left, titanium-plated speci-mens on the right, 6 weeks (A), 12 weeks (B), 20 weeks (C) and 52 weeks (D) postoperatively.An osseous defect is visible in all titanium-plated specimens (arrows). The SR-PLLA-platedcraniotomies appeared to consolidate by primary union, whereas clumpy bony masses wereevident on the bone margins on the titanium sides. Reproduced by kind permission of Journalof Craniofacial Surgery from 8 (1997) 446-451.
the titanium sides that had not consolidat-ed completely. OTC-fluorescence con-firmed these findings, as abundant two-layer fluorescence was observed in the oste-oid formation areas, and OTC-fluores-cence was not apparent at 52 weeks.
PLAIN FILM RADIOGRAPHY showedfalse positive union of the titanium-platedosteotomy in three cases and was thus notreliable in imaging ossification. This wasdue to the fact that the direction of thecentral X-ray of the beam was not parallelto the osteotomy line. This subsequentlyresulted in overlapping of the edges of thenarrow false union of the osteotomy. TheSR-PLLA plate was radiolucent, and nosigns of a foreign body reaction or osteoly-
sis around the biodegradable plate werenoted. Loosening of the titanium plate andscrews was noted in one sheep at 52 weeks.
COMPUTERIZED TOMOGRAPHY:The findings obtained from CT correlatedwell with findings in histology and micro-radiography. Signs of osseous bridging onthe SR-PLLA-plated side were visible 12weeks postoperatively, and complete con-solidaosteotomy line and was interpretedas tion was seen at 20 weeks. On the tita-nium side, CT revealed osseous defects androunding of the bone edges in consecutivecases. However, adjacent to the titaniumplate, scatter impeded evaluation of a verynarrow non-union, whereas the presence ofthe SR-PLLA plate did not result in any
A.
B.
C.
D.
D.
➤➤
➤➤
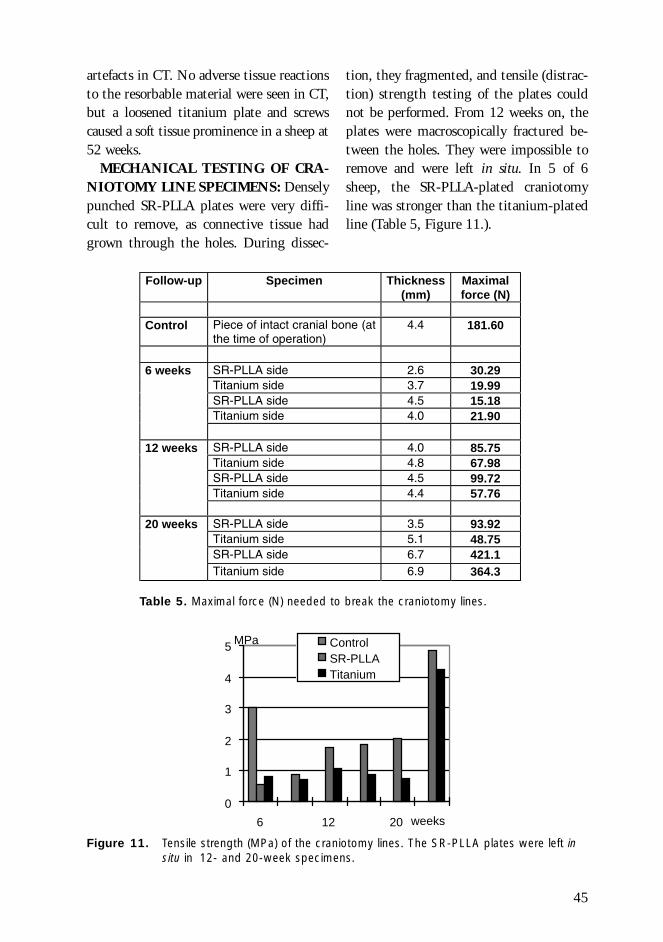
45
0
1
2
3
4
5
6 12 20 weeks
MPa ControlSR-PLLATitanium
artefacts in CT. No adverse tissue reactionsto the resorbable material were seen in CT,but a loosened titanium plate and screwscaused a soft tissue prominence in a sheep at52 weeks.
MECHANICAL TESTING OF CRA-NIOTOMY LINE SPECIMENS: Denselypunched SR-PLLA plates were very diffi-cult to remove, as connective tissue hadgrown through the holes. During dissec-
Follow-up Specimen Thickness(mm)
Maximalforce (N)
Control Piece of intact cranial bone (atthe time of operation)
4.4 181.60
6 weeks SR-PLLA side 2.6 30.29Titanium side 3.7 19.99SR-PLLA side 4.5 15.18Titanium side 4.0 21.90
12 weeks SR-PLLA side 4.0 85.75Titanium side 4.8 67.98SR-PLLA side 4.5 99.72Titanium side 4.4 57.76
20 weeks SR-PLLA side 3.5 93.92Titanium side 5.1 48.75SR-PLLA side 6.7 421.1Titanium side 6.9 364.3
Table 5. Maximal force (N) needed to break the craniotomy lines.
Figure 11. Tensile strength (MPa) of the craniotomy lines. The SR-PLLA plates were left insitu in 12- and 20-week specimens.
tion, they fragmented, and tensile (distrac-tion) strength testing of the plates couldnot be performed. From 12 weeks on, theplates were macroscopically fractured be-tween the holes. They were impossible toremove and were left in situ. In 5 of 6sheep, the SR-PLLA-plated craniotomyline was stronger than the titanium-platedline (Table 5, Figure 11.).
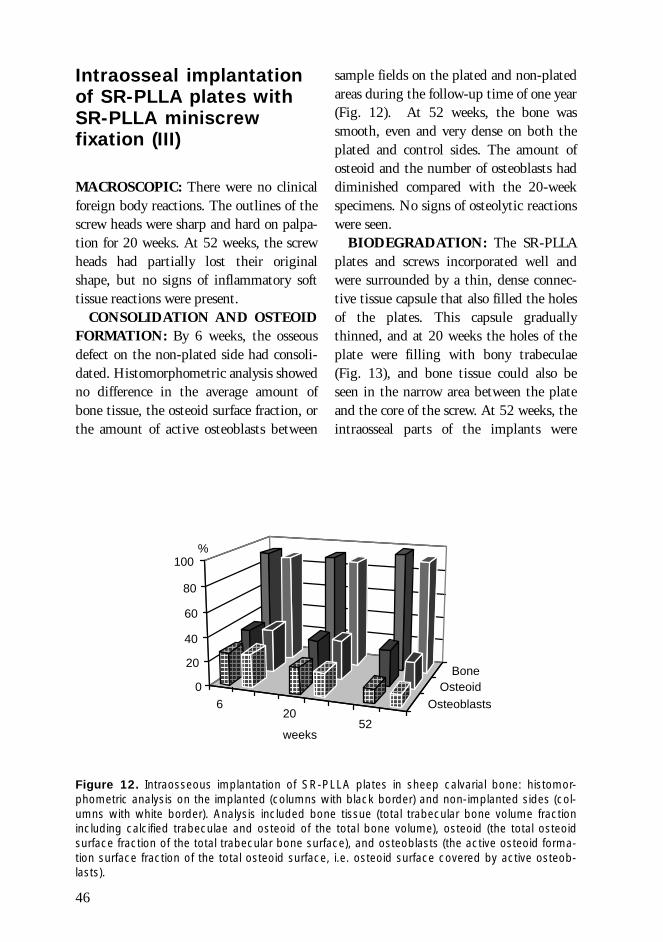
46
620
52
OsteoblastsOsteoid
Bone
����������������������������
���������������
��������������������
����������������������������
���������������
�������������������� ������
������������
����������
��������������������
������������������
����������
�������������������� �����
����������
����������
������������������ �����
���������������
������������������
0
20
40
60
80
100%
weeks
Figure 12. Intraosseous implantation of SR-PLLA plates in sheep calvarial bone: histomor-phometric analysis on the implanted (columns with black border) and non-implanted sides (col-umns with white border). Analysis included bone tissue (total trabecular bone volume fractionincluding calcified trabeculae and osteoid of the total bone volume), osteoid (the total osteoidsurface fraction of the total trabecular bone surface), and osteoblasts (the active osteoid forma-tion surface fraction of the total osteoid surface, i.e. osteoid surface covered by active osteob-lasts).
Intraosseal implantationof SR-PLLA plates withSR-PLLA miniscrewfixation (III)
MACROSCOPIC: There were no clinicalforeign body reactions. The outlines of thescrew heads were sharp and hard on palpa-tion for 20 weeks. At 52 weeks, the screwheads had partially lost their originalshape, but no signs of inflammatory softtissue reactions were present.
CONSOLIDATION AND OSTEOIDFORMATION: By 6 weeks, the osseousdefect on the non-plated side had consoli-dated. Histomorphometric analysis showedno difference in the average amount ofbone tissue, the osteoid surface fraction, orthe amount of active osteoblasts between
sample fields on the plated and non-platedareas during the follow-up time of one year(Fig. 12). At 52 weeks, the bone wassmooth, even and very dense on both theplated and control sides. The amount ofosteoid and the number of osteoblasts haddiminished compared with the 20-weekspecimens. No signs of osteolytic reactionswere seen.
BIODEGRADATION: The SR-PLLAplates and screws incorporated well andwere surrounded by a thin, dense connec-tive tissue capsule that also filled the holesof the plates. This capsule graduallythinned, and at 20 weeks the holes of theplate were filling with bony trabeculae(Fig. 13), and bone tissue could also beseen in the narrow area between the plateand the core of the screw. At 52 weeks, theintraosseal parts of the implants were
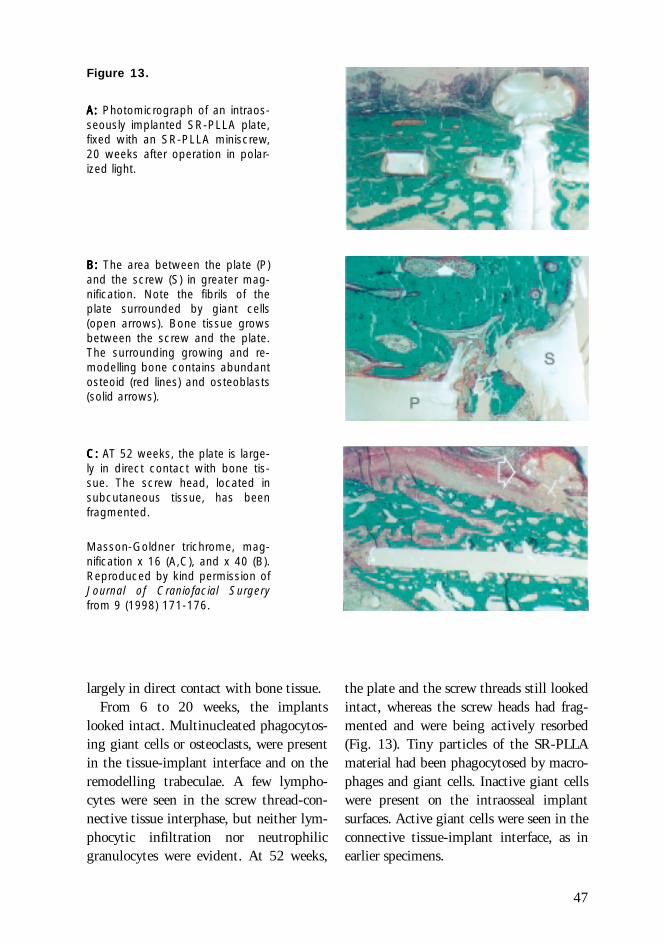
47
Figure 13.
A:A:A:A:A: Photomicrograph of an intraos-seously implanted SR-PLLA plate,fixed with an SR-PLLA miniscrew,20 weeks after operation in polar-ized light.
B:B:B:B:B: The area between the plate (P)and the screw (S) in greater mag-nification. Note the fibrils of theplate surrounded by giant cells(open arrows). Bone tissue growsbetween the screw and the plate.The surrounding growing and re-modelling bone contains abundantosteoid (red lines) and osteoblasts(solid arrows).
C: C: C: C: C: AT 52 weeks, the plate is large-ly in direct contact with bone tis-sue. The screw head, located insubcutaneous tissue, has beenfragmented.
Masson-Goldner trichrome, mag-nification x 16 (A,C), and x 40 (B).Reproduced by kind permission ofJournal of Craniofacial Surgeryfrom 9 (1998) 171-176.
largely in direct contact with bone tissue.From 6 to 20 weeks, the implants
looked intact. Multinucleated phagocytos-ing giant cells or osteoclasts, were presentin the tissue-implant interface and on theremodelling trabeculae. A few lympho-cytes were seen in the screw thread-con-nective tissue interphase, but neither lym-phocytic infiltration nor neutrophilicgranulocytes were evident. At 52 weeks,
the plate and the screw threads still lookedintact, whereas the screw heads had frag-mented and were being actively resorbed(Fig. 13). Tiny particles of the SR-PLLAmaterial had been phagocytosed by macro-phages and giant cells. Inactive giant cellswere present on the intraosseal implantsurfaces. Active giant cells were seen in theconnective tissue-implant interface, as inearlier specimens.

48
Healing of cranialosteotomies fixed withflexible PLA96 plates andSR-PLLA or SR-PGAminiscrews versus rigidtitanium miniplatefixation (IV,V)
No neurological symptoms, infections orclinical foreign-body reactions were seen.
MACROSCOPIC: The osteotomieswere stable on palpation, and investigationshowed no loss of fixation or even minimaldislocation of the bone segment in any ani-mal. The SR-PGA screws degraded rapid-ly: at four weeks, all the screw heads hadbeen replaced with vesicles 3 mm in diam-eter, 0.5-1.0 mm in height, filled withclear fluid, but the screw tips on the duralside were still palpable. All the vesiclesand screw tips had disappeared by sixweeks. The SR-PLLA screws retained theirintegrity until 52 weeks, when minimalaccumulation of fluid was noted aroundthe screw heads. The screw heads and tipswere easily identifiable and hard on palpa-tion (Fig. 14) until they became softenedat 52 weeks, and they had disappeared at104 weeks. The PLA96 plates integratedwith the surrounding contours and werehardly identifiable at 26-52 weeks. Theyfragmented to a yellowish powder-likethin layer in a year (Fig. 14C) and had dis-appeared by two years. Titanium platesand screws had translocated passively intothe bone tissue and frontal sinus at 52-104weeks.
MRI: Magnetic resonance imaging con-firmed that no signs of complications suchas displacement of the osteotomized bone,osteitis, gross inflammation at the osteoto-my area or signs of liquor leakage were vis-
ible. The resolution of the MR images wasinsufficient to allow detailed evaluation ofthe biodegradable fixation system or thedural and cortex areas. We recommend asurface coil in assessing superficial areas ofbiodegradable minifixation with MR im-aging.
Consolidation
RADIOGRAPHY: In AP radiography, nodisplacement of the osteotomized boneswas observed. Consolidation of the craniot-omy lines was slow and incomplete (Fig.15). At four weeks, only 7.3% of the crani-otomy lines appeared to be consolidated onthe SR-PGA side and 9.3% on the titani-um side, and at 26 weeks the figures were31.8% (SR-PGA) and 33.7% (titanium).Complete consolidation was not seen inany specimen. Most trephine holes hadconsolidated on both sides by 26 weekswithout significant differences betweencovered (PLA96 plate) and uncovered (ti-tanium plate) sides.
At 6 weeks, 7 out of 8 SR-PGA screwholes had enlarged from an original 1.5 mmto 1.6-2.0 mm, which was considered as asign of osteolysis and was histologically ver-ified. The borders were sharp, and no newbone formation was observed. From 12weeks onwards the SR-PGA screw holes de-creased in size (p<0.05), new bone forma-tion was observed, and at 52 weeks theholes were filled with bone. The SR-PLLAscrew holes at 104 weeks were sharp-edged,and 1.1 mm in diameter (original 1.5 mm).No reactions around the titanium screwswere observed.
HISTOLOGY AND HISTOMOR-PHOMETY: Histological cross sections re-vealed irregular bone growth from the
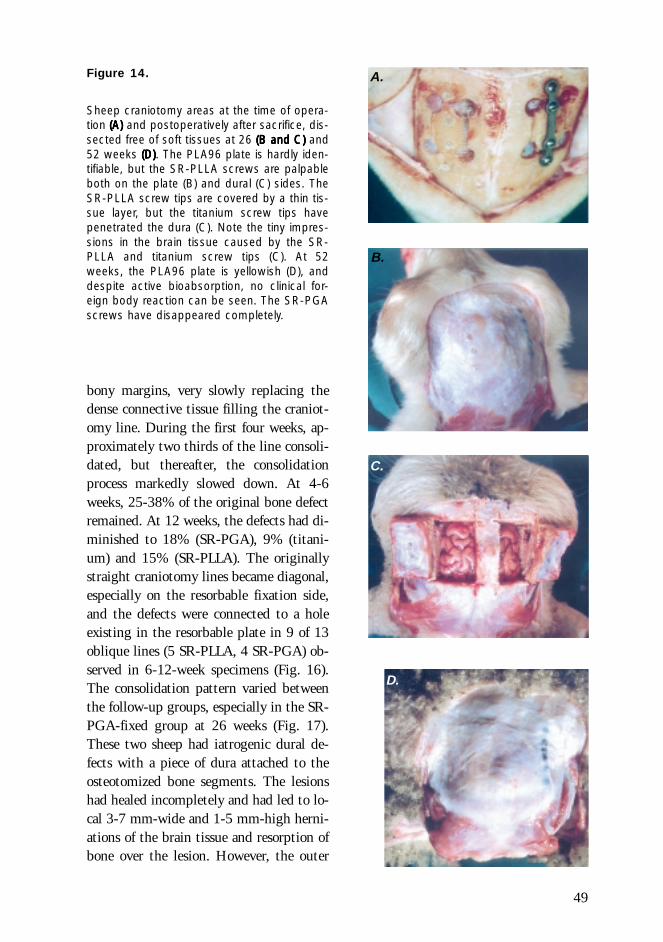
49
Figure 14.
Sheep craniotomy areas at the time of opera-tion (A)(A)(A)(A)(A) and postoperatively after sacrifice, dis-sected free of soft tissues at 26 (B and C)(B and C)(B and C)(B and C)(B and C) and52 weeks (D)(D)(D)(D)(D). The PLA96 plate is hardly iden-tifiable, but the SR-PLLA screws are palpableboth on the plate (B) and dural (C) sides. TheSR-PLLA screw tips are covered by a thin tis-sue layer, but the titanium screw tips havepenetrated the dura (C). Note the tiny impres-sions in the brain tissue caused by the SR-PLLA and titanium screw tips (C). At 52weeks, the PLA96 plate is yellowish (D), anddespite active bioabsorption, no clinical for-eign body reaction can be seen. The SR-PGAscrews have disappeared completely.
bony margins, very slowly replacing thedense connective tissue filling the craniot-omy line. During the first four weeks, ap-proximately two thirds of the line consoli-dated, but thereafter, the consolidationprocess markedly slowed down. At 4-6weeks, 25-38% of the original bone defectremained. At 12 weeks, the defects had di-minished to 18% (SR-PGA), 9% (titani-um) and 15% (SR-PLLA). The originallystraight craniotomy lines became diagonal,especially on the resorbable fixation side,and the defects were connected to a holeexisting in the resorbable plate in 9 of 13oblique lines (5 SR-PLLA, 4 SR-PGA) ob-served in 6-12-week specimens (Fig. 16).The consolidation pattern varied betweenthe follow-up groups, especially in the SR-PGA-fixed group at 26 weeks (Fig. 17).These two sheep had iatrogenic dural de-fects with a piece of dura attached to theosteotomized bone segments. The lesionshad healed incompletely and had led to lo-cal 3-7 mm-wide and 1-5 mm-high herni-ations of the brain tissue and resorption ofbone over the lesion. However, the outer
A.
B.
D.
C.
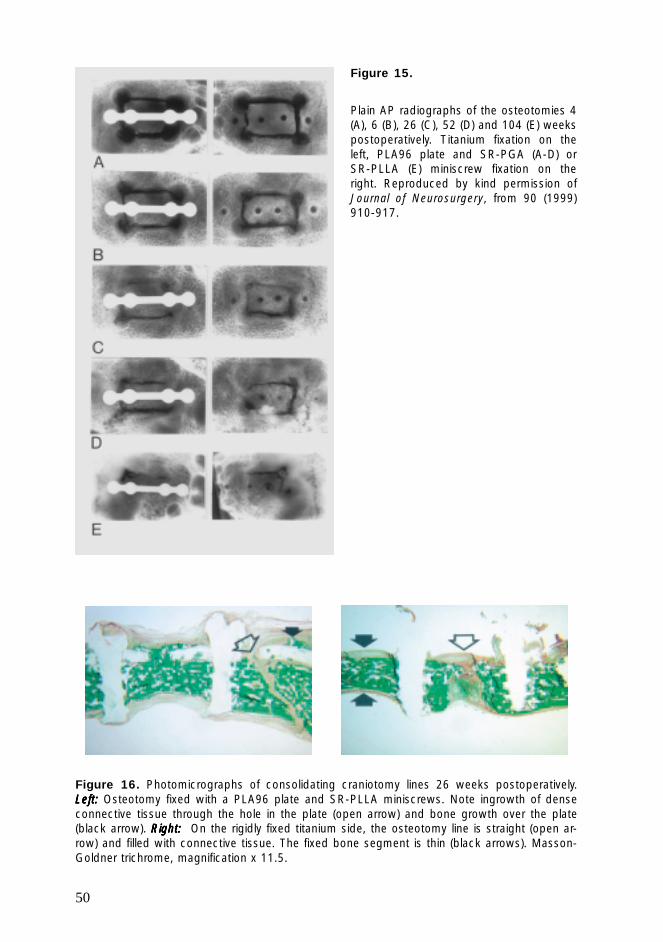
50
Figure 15.
Plain AP radiographs of the osteotomies 4(A), 6 (B), 26 (C), 52 (D) and 104 (E) weekspostoperatively. Titanium fixation on theleft, PLA96 plate and SR-PGA (A-D) orSR-PLLA (E) miniscrew fixation on theright. Reproduced by kind permission ofJournal of Neurosurgery, from 90 (1999)910-917.
Figure 16. Photomicrographs of consolidating craniotomy lines 26 weeks postoperatively.Left:Left:Left:Left:Left: Osteotomy fixed with a PLA96 plate and SR-PLLA miniscrews. Note ingrowth of denseconnective tissue through the hole in the plate (open arrow) and bone growth over the plate(black arrow). Right:Right:Right:Right:Right: On the rigidly fixed titanium side, the osteotomy line is straight (open ar-row) and filled with connective tissue. The fixed bone segment is thin (black arrows). Masson-Goldner trichrome, magnification x 11.5.
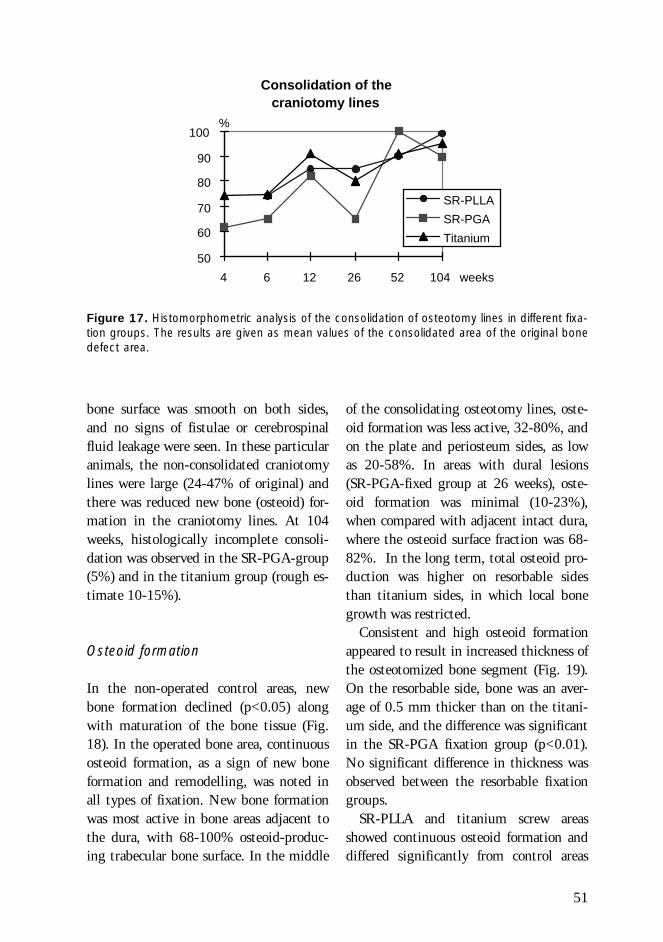
51
bone surface was smooth on both sides,and no signs of fistulae or cerebrospinalfluid leakage were seen. In these particularanimals, the non-consolidated craniotomylines were large (24-47% of original) andthere was reduced new bone (osteoid) for-mation in the craniotomy lines. At 104weeks, histologically incomplete consoli-dation was observed in the SR-PGA-group(5%) and in the titanium group (rough es-timate 10-15%).
Osteoid formation
In the non-operated control areas, newbone formation declined (p<0.05) alongwith maturation of the bone tissue (Fig.18). In the operated bone area, continuousosteoid formation, as a sign of new boneformation and remodelling, was noted inall types of fixation. New bone formationwas most active in bone areas adjacent tothe dura, with 68-100% osteoid-produc-ing trabecular bone surface. In the middle
of the consolidating osteotomy lines, oste-oid formation was less active, 32-80%, andon the plate and periosteum sides, as lowas 20-58%. In areas with dural lesions(SR-PGA-fixed group at 26 weeks), oste-oid formation was minimal (10-23%),when compared with adjacent intact dura,where the osteoid surface fraction was 68-82%. In the long term, total osteoid pro-duction was higher on resorbable sidesthan titanium sides, in which local bonegrowth was restricted.
Consistent and high osteoid formationappeared to result in increased thickness ofthe osteotomized bone segment (Fig. 19).On the resorbable side, bone was an aver-age of 0.5 mm thicker than on the titani-um side, and the difference was significantin the SR-PGA fixation group (p<0.01).No significant difference in thickness wasobserved between the resorbable fixationgroups.
SR-PLLA and titanium screw areasshowed continuous osteoid formation anddiffered significantly from control areas
Consolidation of the craniotomy lines
50
60
70
80
90
100
4 6 12 26 52 104 weeks
%
SR-PLLA
SR-PGA
Titanium
Figure 17. Histomorphometric analysis of the consolidation of osteotomy lines in different fixa-tion groups. The results are given as mean values of the consolidated area of the original bonedefect area.
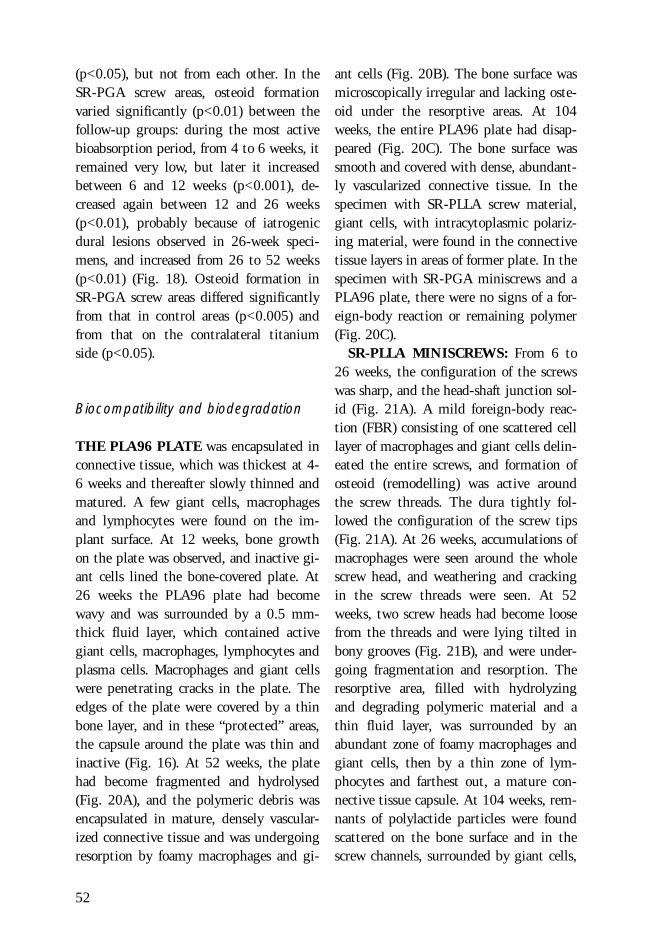
52
ant cells (Fig. 20B). The bone surface wasmicroscopically irregular and lacking oste-oid under the resorptive areas. At 104weeks, the entire PLA96 plate had disap-peared (Fig. 20C). The bone surface wassmooth and covered with dense, abundant-ly vascularized connective tissue. In thespecimen with SR-PLLA screw material,giant cells, with intracytoplasmic polariz-ing material, were found in the connectivetissue layers in areas of former plate. In thespecimen with SR-PGA miniscrews and aPLA96 plate, there were no signs of a for-eign-body reaction or remaining polymer(Fig. 20C).
SR-PLLA MINISCREWS: From 6 to26 weeks, the configuration of the screwswas sharp, and the head-shaft junction sol-id (Fig. 21A). A mild foreign-body reac-tion (FBR) consisting of one scattered celllayer of macrophages and giant cells delin-eated the entire screws, and formation ofosteoid (remodelling) was active aroundthe screw threads. The dura tightly fol-lowed the configuration of the screw tips(Fig. 21A). At 26 weeks, accumulations ofmacrophages were seen around the wholescrew head, and weathering and crackingin the screw threads were seen. At 52weeks, two screw heads had become loosefrom the threads and were lying tilted inbony grooves (Fig. 21B), and were under-going fragmentation and resorption. Theresorptive area, filled with hydrolyzingand degrading polymeric material and athin fluid layer, was surrounded by anabundant zone of foamy macrophages andgiant cells, then by a thin zone of lym-phocytes and farthest out, a mature con-nective tissue capsule. At 104 weeks, rem-nants of polylactide particles were foundscattered on the bone surface and in thescrew channels, surrounded by giant cells,
(p<0.05), but not from each other. In theSR-PGA screw areas, osteoid formationvaried significantly (p<0.01) between thefollow-up groups: during the most activebioabsorption period, from 4 to 6 weeks, itremained very low, but later it increasedbetween 6 and 12 weeks (p<0.001), de-creased again between 12 and 26 weeks(p<0.01), probably because of iatrogenicdural lesions observed in 26-week speci-mens, and increased from 26 to 52 weeks(p<0.01) (Fig. 18). Osteoid formation inSR-PGA screw areas differed significantlyfrom that in control areas (p<0.005) andfrom that on the contralateral titaniumside (p<0.05).
Biocompatibility and biodegradation
THE PLA96 PLATE was encapsulated inconnective tissue, which was thickest at 4-6 weeks and thereafter slowly thinned andmatured. A few giant cells, macrophagesand lymphocytes were found on the im-plant surface. At 12 weeks, bone growthon the plate was observed, and inactive gi-ant cells lined the bone-covered plate. At26 weeks the PLA96 plate had becomewavy and was surrounded by a 0.5 mm-thick fluid layer, which contained activegiant cells, macrophages, lymphocytes andplasma cells. Macrophages and giant cellswere penetrating cracks in the plate. Theedges of the plate were covered by a thinbone layer, and in these “protected” areas,the capsule around the plate was thin andinactive (Fig. 16). At 52 weeks, the platehad become fragmented and hydrolysed(Fig. 20A), and the polymeric debris wasencapsulated in mature, densely vascular-ized connective tissue and was undergoingresorption by foamy macrophages and gi-
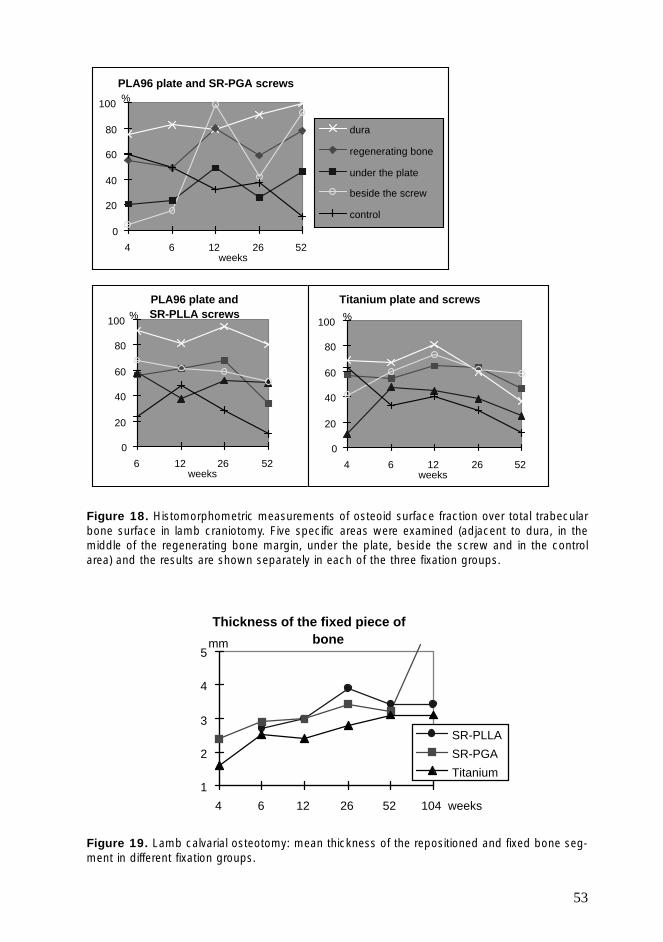
53
Thickness of the fixed piece of bone
1
2
3
4
5
4 6 12 26 52 104 weeks
mm
SR-PLLA
SR-PGA
Titanium
Figure 19. Lamb calvarial osteotomy: mean thickness of the repositioned and fixed bone seg-ment in different fixation groups.
Figure 18. Histomorphometric measurements of osteoid surface fraction over total trabecularbone surface in lamb craniotomy. Five specific areas were examined (adjacent to dura, in themiddle of the regenerating bone margin, under the plate, beside the screw and in the controlarea) and the results are shown separately in each of the three fixation groups.
PLA96 plate and SR-PGA screws
0
20
40
60
80
100
4 6 12 26 52weeks
%
dura
regenerating bone
under the plate
beside the screw
control
PLA96 plate and SR-PLLA screws
0
20
40
60
80
100
6 12 26 52weeks
%
Titanium plate and screws
0
20
40
60
80
100
4 6 12 26 52weeks
%
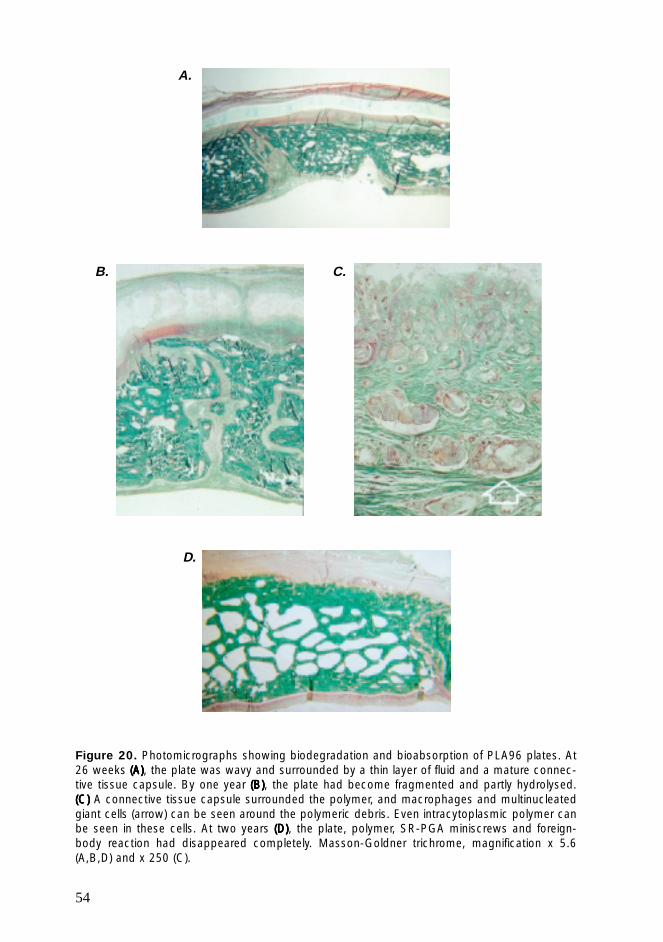
54
Figure 20. Photomicrographs showing biodegradation and bioabsorption of PLA96 plates. At26 weeks (A)(A)(A)(A)(A), the plate was wavy and surrounded by a thin layer of fluid and a mature connec-tive tissue capsule. By one year (B)(B)(B)(B)(B), the plate had become fragmented and partly hydrolysed.(C)(C)(C)(C)(C) A connective tissue capsule surrounded the polymer, and macrophages and multinucleatedgiant cells (arrow) can be seen around the polymeric debris. Even intracytoplasmic polymer canbe seen in these cells. At two years (D)(D)(D)(D)(D), the plate, polymer, SR-PGA miniscrews and foreign-body reaction had disappeared completely. Masson-Goldner trichrome, magnification x 5.6(A,B,D) and x 250 (C).
A.
B. C.
D.
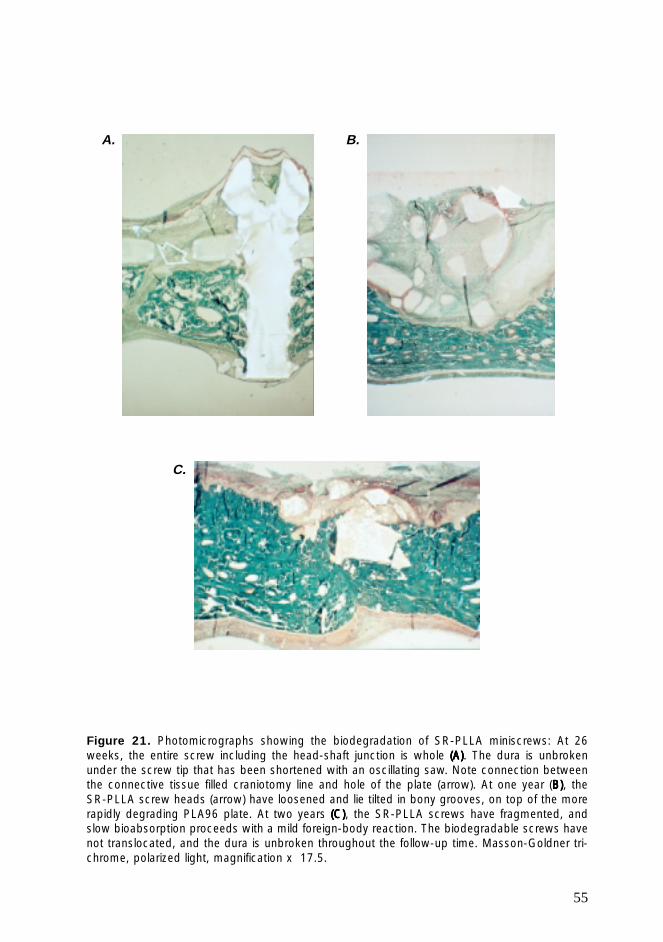
55
Figure 21. Photomicrographs showing the biodegradation of SR-PLLA miniscrews: At 26weeks, the entire screw including the head-shaft junction is whole (A)(A)(A)(A)(A). The dura is unbrokenunder the screw tip that has been shortened with an oscillating saw. Note connection betweenthe connective tissue filled craniotomy line and hole of the plate (arrow). At one year (B)B)B)B)B), theSR-PLLA screw heads (arrow) have loosened and lie tilted in bony grooves, on top of the morerapidly degrading PLA96 plate. At two years (C)(C)(C)(C)(C), the SR-PLLA screws have fragmented, andslow bioabsorption proceeds with a mild foreign-body reaction. The biodegradable screws havenot translocated, and the dura is unbroken throughout the follow-up time. Masson-Goldner tri-chrome, polarized light, magnification x 17.5.
A.
C.
B.
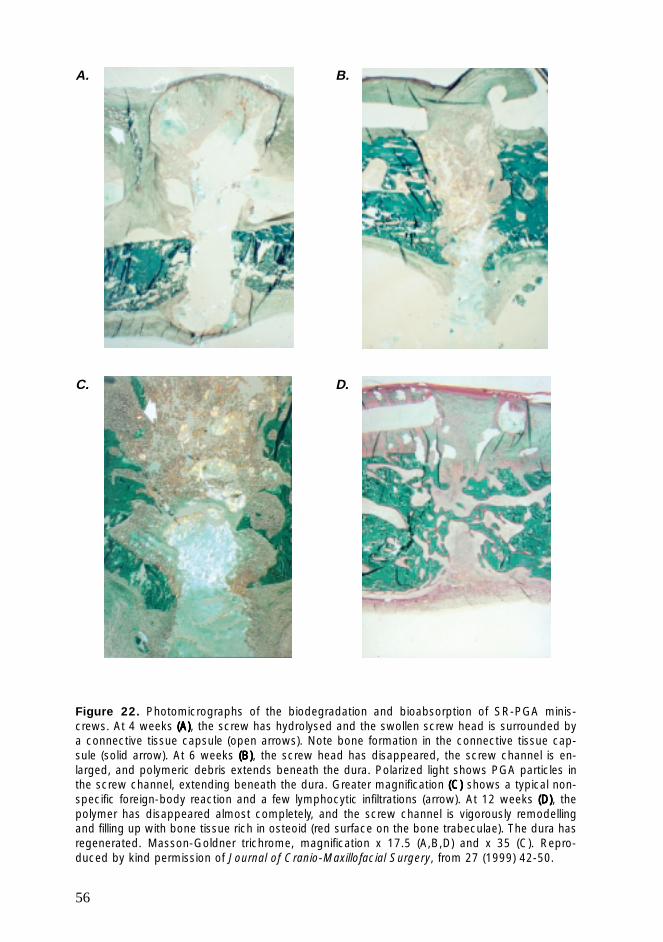
56
Figure 22. Photomicrographs of the biodegradation and bioabsorption of SR-PGA minis-crews. At 4 weeks (A)(A)(A)(A)(A), the screw has hydrolysed and the swollen screw head is surrounded bya connective tissue capsule (open arrows). Note bone formation in the connective tissue cap-sule (solid arrow). At 6 weeks (B)(B)(B)(B)(B), the screw head has disappeared, the screw channel is en-larged, and polymeric debris extends beneath the dura. Polarized light shows PGA particles inthe screw channel, extending beneath the dura. Greater magnification (C)(C)(C)(C)(C) shows a typical non-specific foreign-body reaction and a few lymphocytic infiltrations (arrow). At 12 weeks (D)(D)(D)(D)(D), thepolymer has disappeared almost completely, and the screw channel is vigorously remodellingand filling up with bone tissue rich in osteoid (red surface on the bone trabeculae). The dura hasregenerated. Masson-Goldner trichrome, magnification x 17.5 (A,B,D) and x 35 (C). Repro-duced by kind permission of Journal of Cranio-Maxillofacial Surgery, from 27 (1999) 42-50.
A.
C.
B.
D.
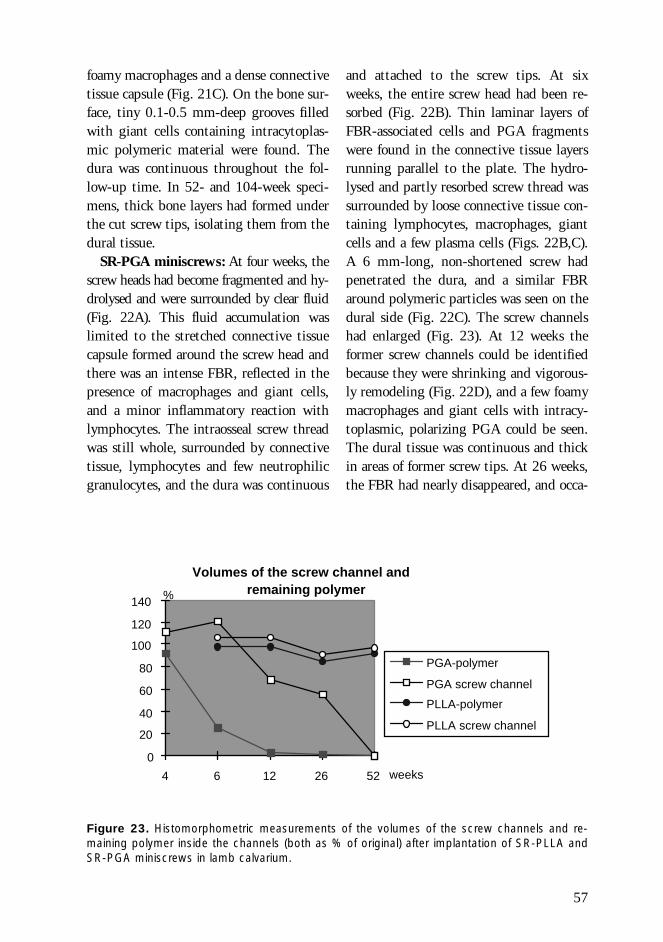
57
foamy macrophages and a dense connectivetissue capsule (Fig. 21C). On the bone sur-face, tiny 0.1-0.5 mm-deep grooves filledwith giant cells containing intracytoplas-mic polymeric material were found. Thedura was continuous throughout the fol-low-up time. In 52- and 104-week speci-mens, thick bone layers had formed underthe cut screw tips, isolating them from thedural tissue.
SR-PGA miniscrews: At four weeks, thescrew heads had become fragmented and hy-drolysed and were surrounded by clear fluid(Fig. 22A). This fluid accumulation waslimited to the stretched connective tissuecapsule formed around the screw head andthere was an intense FBR, reflected in thepresence of macrophages and giant cells,and a minor inflammatory reaction withlymphocytes. The intraosseal screw threadwas still whole, surrounded by connectivetissue, lymphocytes and few neutrophilicgranulocytes, and the dura was continuous
Figure 23. Histomorphometric measurements of the volumes of the screw channels and re-maining polymer inside the channels (both as % of original) after implantation of SR-PLLA andSR-PGA miniscrews in lamb calvarium.
and attached to the screw tips. At sixweeks, the entire screw head had been re-sorbed (Fig. 22B). Thin laminar layers ofFBR-associated cells and PGA fragmentswere found in the connective tissue layersrunning parallel to the plate. The hydro-lysed and partly resorbed screw thread wassurrounded by loose connective tissue con-taining lymphocytes, macrophages, giantcells and a few plasma cells (Figs. 22B,C).A 6 mm-long, non-shortened screw hadpenetrated the dura, and a similar FBRaround polymeric particles was seen on thedural side (Fig. 22C). The screw channelshad enlarged (Fig. 23). At 12 weeks theformer screw channels could be identifiedbecause they were shrinking and vigorous-ly remodeling (Fig. 22D), and a few foamymacrophages and giant cells with intracy-toplasmic, polarizing PGA could be seen.The dural tissue was continuous and thickin areas of former screw tips. At 26 weeks,the FBR had nearly disappeared, and occa-
Volumes of the screw channel and remaining polymer
0
20
40
60
80
100
120
140
4 6 12 26 52 weeks
%
PGA-polymer
PGA screw channel
PLLA-polymer
PLLA screw channel
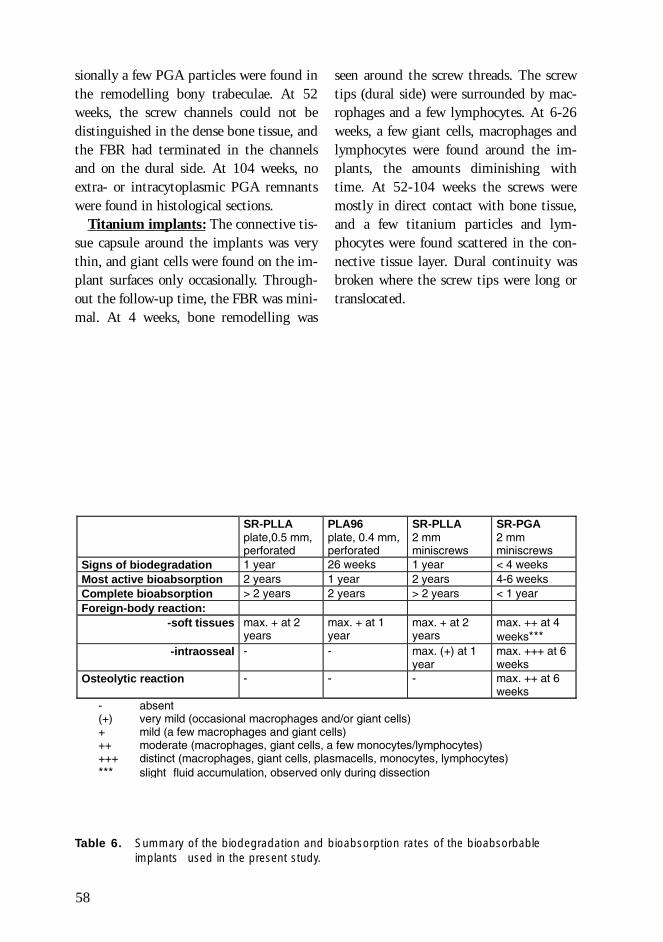
58
Table 6. Summary of the biodegradation and bioabsorption rates of the bioabsorbableimplants used in the present study.
- absent(+) very mild (occasional macrophages and/or giant cells)+ mild (a few macrophages and giant cells)++ moderate (macrophages, giant cells, a few monocytes/lymphocytes)+++ distinct (macrophages, giant cells, plasmacells, monocytes, lymphocytes)*** slight fluid accumulation, observed only during dissection
SR-PLLAplate,0.5 mm,perforated
PLA96plate, 0.4 mm,perforated
SR-PLLA2 mmminiscrews
SR-PGA2 mmminiscrews
Signs of biodegradation 1 year 26 weeks 1 year < 4 weeksMost active bioabsorption 2 years 1 year 2 years 4-6 weeksComplete bioabsorption > 2 years 2 years > 2 years < 1 yearForeign-body reaction:
-soft tissues max. + at 2years
max. + at 1year
max. + at 2years
max. ++ at 4weeks***
-intraosseal - - max. (+) at 1year
max. +++ at 6weeks
Osteolytic reaction - - - max. ++ at 6weeks
sionally a few PGA particles were found inthe remodelling bony trabeculae. At 52weeks, the screw channels could not bedistinguished in the dense bone tissue, andthe FBR had terminated in the channelsand on the dural side. At 104 weeks, noextra- or intracytoplasmic PGA remnantswere found in histological sections.
Titanium implants: The connective tis-sue capsule around the implants was verythin, and giant cells were found on the im-plant surfaces only occasionally. Through-out the follow-up time, the FBR was mini-mal. At 4 weeks, bone remodelling was
seen around the screw threads. The screwtips (dural side) were surrounded by mac-rophages and a few lymphocytes. At 6-26weeks, a few giant cells, macrophages andlymphocytes were found around the im-plants, the amounts diminishing withtime. At 52-104 weeks the screws weremostly in direct contact with bone tissue,and a few titanium particles and lym-phocytes were found scattered in the con-nective tissue layer. Dural continuity wasbroken where the screw tips were long ortranslocated.
59
In paediatric craniofacial surgery, bioab-sorbable osteosynthesis materials have be-come not only a choice among other fixa-tion techniques, but even a recommenda-tion (Habal 1996). The materials used inthe present studies reflect the developmentof bioabsorbable miniosteosynthesis devic-es. First generation materials, pure PLLAand PGA, have been replaced by their co-polymers and stereocopolymer P(L/DL)LA,which have more ideal bioabsorption char-acteristics. The mechanical qualities can besignificantly improved even in mini-im-plants by the self-reinforcing technique(Törmälä 1998).
In the literature, bioabsorbable materialshave been particularly recommended forfixation of osteotomies in the growingneurocranium, but there is only one pub-lished experimental study on fixation ofunstable craniotomies with bioabsorbableplates (Illi et al. 1990). Most earlier experi-ments have been performed on the viscero-cranium or endochondral bones. Operatingon the neurocranium is more time con-suming, requires special instrumentationand is subject to fatal complications. Theresults of earlier studies on viscerocranialosteosyntheses may not be directly applica-ble to osteosyntheses in the neurocranium.In addition, wide variability and insuffi-cient information on the fixation materialsadds to the difficulty of interpretation andcomparison with the results of earlier ex-perimental studies.
GENERAL DISCUSSION
Material and methods
Despite being young and growing, thesheep were not of the same age in the threeexperiments, which may have caused varia-bility in the results. Histological sectionsof the dense cranial bone were of goodquality, and the staining method was suc-cesful which enabled very exact histologi-cal and histomorphometric analyses of thespecimens. Because of the high quality ofthe histological sections, OTC-fluorescencestudies and microradiography did not addgreatly to the information, and were notperformed in later experiments. Plain filmradiographs, CT and MR images corre-sponded to clinical situations.
The experimental designs were simple,in order to avoid surgical complications, tolimit variability of the results and to allowdetailed, comparative analysis of the con-solidation process and biocompatibilityand biodegradation of the bioabsorbableimplants. In orthopaedic and most maxil-lofacial experiments, fractures or osteoto-mies have usually been exactly reposi-tioned before fixation, because contact be-tween bone edges is essential for bonehealing and prevention of non-union. Inreconstructive paediatric craniofacial sur-gery, bone defects in the form of narrowcraniotomy lines, trephine holes or larger,are an unavoidable consequence of surgery.Consolidation of craniotomy lines has notpreviously been studied experimentally,

60
possibly because it has been considered tobe uneventful.
In the first experiment, the only stresson the plate was slow completion of skele-tal growth. In the third experiment, theosteotomized bone segments were com-pletely detached from surrounding tissuesand reinserted and fixed without bonycontact with the surrounding bone tissue,and the stresses were a combination of in-tracranial pulsative pressure, skeletalgrowth, and occasional external forces.Specific findings in these animal modelsmay not be directly equivalent to that ob-served in paediatric craniofacial surgery, asin clinical craniofacial operations, pieces ofbone are preferably set together with asmuch bony contact as possible to ensurestability and consolidation. On the otherhand, the bone defects created in craniofa-cial surgery may be considerably largerthan 2.3 mm-wide craniotomy lines or 6mm-wide trephine holes. The experimentwith intraosseal plating was the first of itskind published in craniofacial surgery, andreflects the development of new surgicaltechniques based on new bioabsorbable os-teosynthesis devices.
Bone healing
Loss of fixation, or instability, did not oc-cur. No complications caused by the re-sorbable osteosynthesis devices were ob-served during the 4-104-week follow-upperiods. Passive translocation of the resorb-able devices did not occur.
In the first study in older sheep, the sta-ble osteotomy lines plated with narrow ti-tanium implants showed a consolidationpattern with bulky, uneven masses of bone,and complete osseous healing was seen
only in the 104-week sample, whereas theSR-PLLA-plated osteotomies had consoli-dated by 20 weeks. In the third experi-ment, in younger sheep, no such strikingdifferences in healing of the resorbable andtitanium-fixed osteotomies was noted. Thenarrow craniotomy lines surrounding thedevascularized bone segment consolidatedslowly and incompletely, independent ofthe type of fixation. During the first 4weeks, 60-70% of the original bone defecthad consolidated, but thereafter, consolida-tion remarkably slowed down. The crani-otomies were stable on palpation, and thesigns of incomplete and delayed consolida-tion were histological.
According to experienced clinicians,most osteotomies in infants heal rapidly(Lauritzen, personal communication 1999).Thus, slow consolidation in the present ex-perimental models was unexpected. As re-gards incomplete consolidation, dural le-sions could be an explanation, but the durawas intact in all but two cases. The osteo-genic importance of young dura was em-phasized in those two cases, which is inline with earlier experimental and clinicalreports (Mossaz and Kokich 1981; Winston etal. 1983; Hobar et al. 1993). New bone for-mation was most active in bone areas closeto undamaged dura.
Stability of fixation did not appear to beof crucial importance for consolidation, asthe first experimental osteotomies were ab-solutely stable but consolidation was in-complete, and in the third experiment,rigid and semi-rigid fixation had no sig-nificantly different effects on consolida-tion. Local restriction of growth can causegrowth disturbances, which has been doc-umented experimentally with rigid metal-lic fixation (Lin et al. 1991; Yaremchuk1994; Polley et al. 1995). There is no evi-

61
dence in the literature indicating that con-solidation of a rigidly restricted bone de-fect in growing animals may be impairedbecause of the rigidity. Local bone growthwas certainly restricted on the titaniumside in lamb craniotomies, which has beenproven earlier in several studies (Lin et al.1991; Yaremchuk 1994; Polley et al. 1995;Polley et al. 1998). In addition, titanium-fixed bone segments remained thinnerthan non-rigidly and transiently fixedbone segments, which has also been shownearlier (Thaller et al. 1996). However, thetrabecular bone volume in the fixed pieceof bone remained high independent on thetype of fixation, which is in contrast to aprevious report (Kennady et al. 1989a). Asin previous reports, passive translocation ofthe metallic implants into the bone andthe frontal sinus was observed (Fearon et al.1995; Goldberg et al. 1995; Honig et al.1995; Papay et al. 1995; Yaremchuk andPosnick 1995; Persing et al. 1996).
Guided bone regeneration (GBR) hasbeen demonstrated to be effective in osteo-promotion and prevention of fibrous non-union in craniofacial bone defects (Gottlowet al. 1984; Dahlin et al. 1988; Dahlin et al.1991; Gottlow 1993; Karring et al. 1993;Linde et al. 1993; Lundgren et al. 1995;Mooney et al. 1996;Lemperle et al. 1998),and seemed to be of greater importance inolder animals in the first experiment. Peri-osteum alone (without any other mem-brane) has been considered to function as abiologically active membrane (Engdahl1971; Linde et al. 1993), but in the presentexperiment, the role of periosteum was in-ferior to that of the SR-PLLA plate. Con-nective tissue invasion might be the expla-nation for the lack of ossification in clini-cal cases as well. In the third experiment, alarge, thin PLA96 plate covered the whole
osteotomy and bone defect area in younglambs. Nevertheless, connective tissue in-vasion was rapid and occurred freelythrough the holes in the PLA96 plate.Consolidation of the trephine holes cov-ered with a PLA96 plate was slightly bet-ter than in the titanium-fixed cranioto-mies, but the difference was not statistical-ly significant. Dural and periosteal sides ofthe osteotomy lines did not show signifi-cant differences either. Thus, the role ofGBR might be more important in olderanimals with diminished dural osteogeniccapacity.
Biocompatibility and biodegradation
In the present study, clinically significantforeign-body reactions, such as swelling orseroma, or infection, did not occur in the1-2 year follow-up periods. The biocom-patibility of SR-PLLA implants was good:Intraosseously implanted SR-PLLA platesbecame integrated with the bone tissue,and the connective tissue capsule sur-rounding the implant slowly thinned andpartly disappeared, resulting in direct con-tact between the implant and bone. Ko-skikare et al. used two identically manufac-tured, equally thick but non-perforatedSR-PLLA plates for intraosseal fixation ofrabbit distal femoral osteotomies (Koskikareet al. 1996). The amount of bone wasgreatest near the plates and especiallystrong between them (Koskikare et al.1997). Growth of bone tissue into theholes of a plate probably strengthens theosteosynthesis by uniting the bone layersseparated by the plate. Thus in an intraos-seal environment, perforated plates mightbe more advantageous than non-perforatedones.

62
Earlier experiments have shown that thedegradation kinetics of biodegradable im-plants depend on the site of implantation,probably because of differences in tissueperfusion (Tschakaloff et al. 1994). In thepresent study, subperiosteally implantedSR-PLLA plates and screw heads started tofragment in one year and resorb in twoyears. Intraosseal plates and screw parts,embedded in extremely dense calvarialbone, degraded more slowly. The subperio-steal implants, especially screw heads, werealso prone to mechanical stress because ofthe butting habit of the animals. The for-eign-body reaction was also milder aroundintraosseal than subcutaneously locatedparts of SR-PLLA implants, which is in ac-cordance with the results of earlier studies(Päivärinta et al. 1993; Suuronen et al.1994; Böstman et al. 1995).
Plates manufactured of high molecularweight, as-polymerized PLLA have causedstriking foreign-body reactions (Bergsma etal. 1993; Bergsma et al. 1995). As-polymer-ized material is not very well purified,which may have contributed to the disap-pointing results, in addition to the thick-ness of the relatively weak, non-reinforcedplates (2 mm) and subcutaneous implanta-tion under thin facial skin. Bioabsorptionof the PLA96 plate in the present studywas complete by two years, without theslightest clinical foreign-body reaction.Degradation of this stereocopolymer isconsiderably faster than that of pure poly-L-lactide.
In the present study, no adverse reac-tions to SR-PGA miniscrews were notedclinically, but transient, subcutaneous,tiny vesicles had developed in hydrolyzingminiscrew head areas at four weeks. Theyhad disappeared by the sixth postoperativeweek, probably because the implants used
were considerably smaller than those usedby Böstman et al. (1990), and were locatedin abundantly vascularized tissue in agrowing animal. As in earlier studies (Böst-man et al. 1992a; Böstman et al. 1992b), aminimal transient osteolytic reaction wasalso observed in the present study, butcompensatory, extremely active new boneformation and remodelling followed. Bio-absorption of a polymer activates themonocyte-macrophage-giant cell line. Gi-ant cells and osteoclasts are very difficultto distinguish from each other and mayeven be the same cells (Wang et al. 1997),and activation of giant cells in bone tissuemight lead in practice to activation of oste-oclasts, which may result in decreasing os-teoid formation or even transient osteolyticreactions during absorption of the poly-mer. Osteolytic reactions have been associ-ated with the use of PGA implants inadults (Pelto-Vasenius et al. 1997), whereasin children, no adverse effects have beenreported (Mäkelä et al. 1992). In thepresent study, PGA debris was extrudedfrom the enlarged channel to the subduralspace. The fluid here reflected a typicalnon-specific foreign-body reaction withoutsigns of infection, supporting the results ofearlier studies in other than calvarial tis-sues (Herrmann et al. 1970; Böstman et al.1992a; Böstman et al. 1992b; Thaller et al.1995b). In addition, the dural lesionscaused by screw tips completely regenerat-ed after resorption of the polymer.
The rate of bioabsorption of PLLA wastoo slow, and that of PGA too fast in sheepcranium, whereas that of PLA96 was ac-ceptable. The SR-technique enables manu-facture of mechanically strong implantswith relatively reduced polymer volumeand small implant size, which further addto the biocompatibility and clinical appli-
63
cations. Because of the high initialstrength, SR-implants can be sterilizedwith gamma irradiation, which has beenshown to decrease molecular weight andthus fasten the degradation process (Claeset al. 1996). Gamma irradiation has beenconsidered safer than sterilization withethylene oxide (Nair 1995), which hasbeen used for sterilization of non-SR-im-plants.
Fixation properties and strength retention
Until the development of self-reinforcedimplants, biodegradable plates were toobulky and thick to be inserted into the cal-varium or other thin bones. When the bio-compatibility and mechanical strength ofimplants are sufficient, the surgeon maychoose the method of fixation according tothe circumstances, free of concern as re-gards a removal operation. To be biome-chanically safe, bioabsorbable implantsshould have 1) high initial strength to car-ry physiological loads during healing, 2) anappropriate initial modulus; not too stiff ortoo flexible for the special purpose required,and 3) controlled strength and modulus re-tention in vivo, in harmony with the in-crease of strength and modulus of the heal-ing tissue (Törmälä et al. 1998). Very littleis known about the biomechanical and de-formational forces acting on the craniofacialskeleton under applied load conditions invivo. The biomechanical demands that aninfant neurocranium sets for fixation sys-tems have been based on assumptions morethan on biomechanical data.
Suuronen et al. have shown that 0.5mm-thick but non-perforated SR-PLLAplates in four layers are strong enough forfixation of experimental mandibular frac-
tures in sheep (Suuronen et al. 1992a). Sixweeks postoperatively, the bendingstrength of the SR-PLLA-fixed mandibleswas 88% of the intact control side, where-as that of titanium-fixed specimens wasonly 37%. After 12 weeks, the values were90% vs. 75%, and at 24 weeks, 105% vs.114%, respectively (Suuronen et al. 1992b).In our first experiment, consolidation ofthe stable bone slit was slower and theplate considerably weaker, although it wasnot prone to mechanical stress. Dense per-foration weakened the plate markedly andenlarged the resorptive area. In this SR-PLLA plate prototype, the polylactide fi-bres run parallel, and the very thin platemay fracture between the uniaxially ori-ented fibres, especially between the perfo-rations. This may have caused fracturing ofthe plate as early as at 6 weeks. In the newgeneration of SR-plates, this problem hasbeen solved by biaxial orientation in a net-like fashion. They are also malleable inroom temperature, which is especially app-reciated by surgeons.
The initial strength of PLA screws (Wit-tenberg et al. 1991) and SR-PLLA screws(Pohjonen et al. 1997) has been consideredcomparable to that of metallic screws, andin the present study, both self-reinforcedminiscrews could be properly tightenedagainst the plate without torsional loosen-ing of the screw head. The SR-system doesnot affect the hydrolytic timetable, whichdepends on the chemical composition ofthe polymer. Even minimal hydrolysis anddegradation of an initially strong screwwill result in loss of screw holding power(Kellman et al. 1994). The SR-PGA minis-crews had lost their holding power by fourweeks, whereas the SR-PLLA miniscrewsremained unchanged for 26 weeks. Earlyhydrolysis of the SR-PGA miniscrews al-
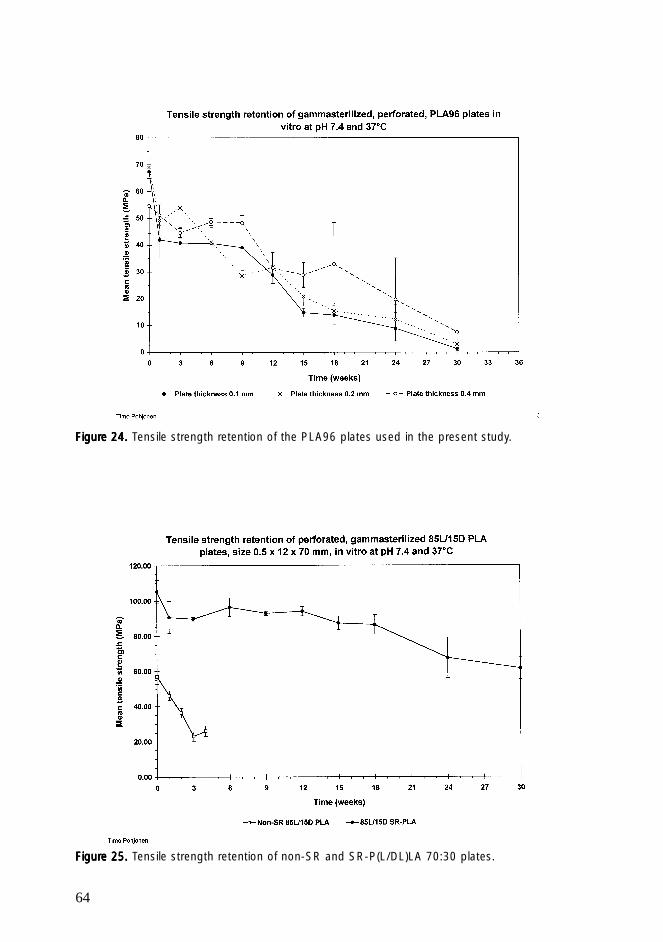
64
FigurFigurFigurFigurFigure 24. e 24. e 24. e 24. e 24. Tensile strength retention of the PLA96 plates used in the present study.
FigurFigurFigurFigurFigure 25. e 25. e 25. e 25. e 25. Tensile strength retention of non-SR and SR-P(L/DL)LA 70:30 plates.

65
lowed unrestricted local bone growth andskull expansion.
The initial strength of the experimentalPLA96 plate and SR-PLLA miniscrews(design with third experiment) has beenmeasured in cadaveric sheep skull by com-pressing the fixed bone segment from theoutside (Peltoniemi et al. unpublished data).The non-reinforced, flexible 0.4 mm-thickplate reversibly yielded 4-5 mm beforebreaking at 74 N (mean), whereas fixationwith four short metallic microplates and 8microscrews irreversibly yielded 7-8 mmbefore breaking at 305 N. The resorbableplate tended to break along the osteotomylines and through the screw holes, whereasnone of the bicortically inserted SR-PLLAscrews broke. The initial tensile strengthof these plates was 54 MPa (Fig. 24). Anidentical osteotomy, fixed with 0.4 mm-thick SR-PLA thread, broke at 143 N(mean). Non-reinforced PLGA plate-screwfixation in sheep cadaveric calvarial boneshas been reported to break at a distractionforce of 270 N and a compression of 200N, when measured on the long axis of theplate (Gosain et al. 1998). Even though thestrength values between these two studiesare not comparable, it would appear thatthe PLA96 plate should be reinforced, pos-sibly biaxially, to be sufficiently strong andreliable for fixation of larger cranial osteoto-mies. Tensile strength of P(L/DL)LA platescan be significantly increased by the SR-method (Figure 25).
The fixation system should be initiallystrong enough to tolerate acute forces, pos-sibly greater forces than 74 or even 200 N.Because of plasticity of infant neurocrani-um, a semi-rigid plate that maintainsspace and does not allow collapse, but al-lows minimal movement with return to itsoriginal position, might be preferable to a
rigid plate. As the rigidity of fixation doesnot appear to be crucial, flexibility of theplate to some extent, with an ability to re-turn to its original position could be anadvantage in infant cranium. The bonyframe of the cranium has to be reliably andrigidly fixed, but limited areas could beyielding.
Future research
Bioabsorbable plates and membranes maybe useful tools in both guided bone regen-eration and tissue engineering. Whether ornot bioabsorbable membranes could beused for patching dural lesions, also re-mains to be studied. Materials that are in-tended for intraosseal or intracranial im-plantation should be studied as regardstheir biocompatibility in leptomeningealand brain tissues.
A promising field of future research isthe incorporation of osteogenic proteins(Illi and Feldmann 1998) into resorbablefixation materials, i.e. using the fixationmaterial as a delivery system that wouldprevent soft tissue prolapse and maximizethe interaction between the osteoinductionagent and osteoprogenitor cells, whichwould probably lead to enhanced bone re-generative capacity.
Clinical significance
The results of the present experiments can-not be adapted to clinical practice as such,but they emphasize the importance of test-ing new materials and methods of fixationin specific sites and conditions before clin-ical use.
In paediatric craniofacial surgery, rigid

66
metallic fixation can be replaced by bioab-sorbable osteosynthesis devices. By usingbioabsorbable mini-implants, we can avoidseveral disadvantages associated with me-tallic devices, such as the removal opera-tion, growth restriction, irreversible pas-sive intracranial translocation, extrusion,cold sensitivity, stress shielding and corro-sion. New surgical techniques can be de-vised, as the placement of bioabsorbablefixation material is not a limiting factor.
Radiolucency of these devices facilitatesboth postoperative follow-up (Tschakaloff etal. 1993; Viljanen et al. 1998) and radio-therapy after tumour surgery (Rozema et al.1990b). Bioabsorbable implants with agreat range of applications can be manu-factured, and technological and medicalco-operation is important for developingsafe implants with ideal biomechanichal,mechanical and bioabsorption qualities.
67
odegradation of the SR-PLLA material waseven slower in an intraosseous environ-ment than in subcutaneous tissue.
In the third experiment, bilateral unstablecraniotomies were carried out in 20 lambs.For fixation, a non-reinforced, P(L/D)LA 96/4 stereocopolymer plate was used on oneside, and a rigid titanium miniplate on theother side. The PLA96 plate was 0.4 mm-thick and flexible, and fixed in 10 lambswith rapidly resorbing SR-PGA minis-crews, and in another 10, with slowly de-grading SR-PLLA miniscrews. During thefollow-up time of two years, no complica-tions were observed clinically or in mag-netic resonance imaging, and the cranioto-mies were stable on palpation. Plain filmradiography, histology and histomorphom-etry revealed incomplete consolidation ofthe 2.3 mm-wide craniotomy margins inall fixation groups. Bioabsorption of theSR-PGA miniscrews was rapid and tran-sient osteolytic reactions were seen in thescrew channels. The SR-PLLA miniscrewsdegraded in two years, but bioabsorptionwas incomplete. The PLA96 plate wascompletely absorbed in two years. Titani-um plates tended to become translocatedinto the frontal sinus in the long term, andthe fixed bone segments were thinner thanon the PLA96-plated side.
The craniotomy lines in the first experi-ment were tested for tensile strength in 6sheep at 6, 12 and 20 weeks. The SR-PLLA-plated specimens showed highertensile strength than the titanium-platedspecimens in 5 of 6 sheep, possibly as a re-sult of more effective consolidation.
The purpose of the present investigationwas to study the biocompatibility of SR-PLLA and PLA96 miniplates and SR-PLLA and SR-PGA miniscrews in grow-ing neurocranium and their suitability forfixation of calvarial osteotomies in sheep.The implants used in the present studywere prototypes manufactured during thesearch for ideal bioabsorbable mini-im-plants. A total of 41, skeletally immaturesheep were operated upon in three series ofexperiments. In the first, simple bilateralcraniotomy lines served as an experimentalmodel to study the basic consolidationprocess of a common bone defect in cranio-facial surgery. The craniotomy lines wereplated with an SR-PLLA plate on one sideand a narrow titanium plate on the con-tralateral side, and both were fixed with ti-tanium miniscrews. During the follow-uptime of two years, the results of computer-ized tomography, plain film radiography,microradiography, histology, histomor-phometry and fluorescence studies con-firmed that bony consolidation was signif-icantly more effective under the SR-PLLAplate, and the titanium-plated lines result-ed in non-union. The SR-PLLA plate bio-degraded in two years, but bioabsorptionwas incomplete.
In the second experiment, an SR-PLLAplate was inserted intraosseously in a bonyslit sawn tangentially in the calvarium ofsix sheep, and fixed with a prototype SR-PLLA miniscrew. The plate showed excel-lent biocompatibility during the follow-up time of one year and it became inte-grated as part of the bone tissue in histo-logical and histomorphometric studies. Bi-
SUMMARY AND CONCLUSIONS
68
On the basis of the present results, the following conclusions can be drawn:
A craniotomy line in the calvarial membranous bone of young sheep consolidatesvery slowly by primary ossification and is vulnerable to the invasion of connectivetissue. The consolidation process can be enhanced by a protective SR-PLLA plate,when compared with a narrow titanium plate, which results in non-union. An SR-PLLA plate is biocompatible when applied subperiosteally on sheep cranial bone,but it does not become absorbed in two years. The biodegradation process doesnot interfere negatively with bone regeneration. (I)
Consolidation of originally 2.3-2.5-mm wide craniotomy lines can be more relia-bly assessed by CT than by plain film radiography. Titanium plates and screwscreate artifacts and disturb detection of narrow non-union in CT, whereas SR-PLLA plates are completely radiolucent. (II)
SR-PLLA plates are very biocompatible in an intraosseous environment in calvari-al membranous bone of growing sheep. Biodegradation process of SR-PLLA mate-rial is even slower in intraosseous than in subcutaneous tissue, and it does not in-terfere negatively with bone regeneration. (III)
A non-reinforced, flexible, wide PLA96 plate can be used for fixation of unstable,small craniotomies. Consolidation of a semirigidly fixed calvarial bone segment(PLA96 plate and SR-PLLA miniscrews) does not differ significantly from that ofa rigidly fixed (titanium miniplate and screws) osteotomy. The biocompatibility of0.4 mm-thick PLA96 plates is excellent, and they are absorbed completely in twoyears without negative effects on bone regeneration. (IV,V)
Both SR-PLLA and SR-PGA miniscrews can be used for plate fixation of pieces ofcranial bone in growing sheep. As a result of a transient inflammatory and osteo-lytic reaction caused by rapid hydrolysis of PGA, a pure PGA implant is not asbiocompatible as a pure PLLA implant, which causes a very mild foreign-body re-action. SR-PGA miniscrews lose their mechanical strength in less than four weeks,whereas SR-PLLA miniscrews appear to retain screw-holding power for up to sixmonths. SR-PGA miniscrews are absorbed completely by 26-52 weeks, whereasSR-PLLA miniscrews are still undergoing biodegradation and bioabsorption attwo years. (IV,V)

69
The present study was carried out at theDepartments of Surgery and Clinical Vet-erinary Sciences, University of Helsinki; atOulu University Hospital, Department ofSurgery, Division of Plastic Surgery; atHelsinki University Central Hospital, De-partment of Radiology, and at the Insti-tute of Biomaterials, Tampere Universityof Technology, in the last century, duringthe years 1994-1999. I want to thank eve-ryone who helped and supported me dur-ing these years, and I express my warmestgratitude to:
Professor Juhani Ahonen, MD, PhD, Headof the Department of Surgery, Universityof Helsinki, for his confidence, supportand encouragement during this work.
Docent Timo Waris, MD, PhD, the super-visor of this thesis, for his enthusiastic,broad-minded and inspiring attitude toresearch, for giving me the topic of thestudy, for his endless patience and under-standing which helped me through thehard times, and the excellent research fa-cilities he provided for his research group.
Professor Riitta-Mari Tulamo, DVM, PhD,Dipl ECVS, my true friend, for her expertguidance, advice and great help in the ex-perimental work.
Professor Pertti Törmälä, PhD, BMS,Head of the Institute of Biomaterials,Timo Pohjonen, Lic. Tech., Pertti Helevir-ta, Lic. Tech., and Harri Happonen, Lic.Tech., for their inspiring cooperation, fordeveloping and testing the implants used
in the study, for introducing me to materi-als science, and for their time and advice.
Professor Elizabeth Tanner, Docent ClaesLauritzen and Docent Riitta Suuronen forreviewing this thesis and for their con-structive criticism and valuable advice.
Co-authors Terttu Toivonen, MD, andMatti Kallioinen, MD, PhD, specialists inpathology, for showing enthusiastic inter-est in my numerous specimens, ProfessorDorrit Hopfner-Hallikainen for preciseand effective evaluation of radiographic re-sults, Docent Juhani Ahovuo and the staffin the radiological departments of TöölöHospital and Tilkka Hospital for perform-ing radiographic examinations, DocentHarri Pihlajamäki for instructing me withpatience how to perform histomorphomet-rical measurements, and Emeritus Profes-sor Pentti Rokkanen, for his valuable ad-vice and constructive criticism.
Mr Antero Enqvist, Manager of StratecMedical, and his staff, for his patient helpwith instrumentation, Taina Hutko, labo-ratory technician, for preparing and cut-ting the specimens with incredible skill,Mr Arto Ketola for carrying out the statis-tical analysis, Mr Mauri Laakso and MrGeorges Faddi for assistance in photogra-phy, Ms Hanna Kurppa for drawing thegraphic works, Mr Nick Bolton for revis-ing the English language, and Mrs MirjaTörmälä, Ms Aini Hämäläinen and Ms SariSaarela for secretarial assistance.
Mr Seppo Koskensalo, Agr., his staff, vet-
ACKNOWLEDGEMENTS
70
erinary colleagues and butchers, especiallyMr Tapio Antila and Mr Seppo Salonen fortheir help and for taking such good care ofthe experimental animals.
Our research group, Nuri, Eero, Katja, andAnna-Liisa for shared interest and friend-ship.
My superiors, Docent Vesa Perhoniemi,Docent Mauri Lepäntalo, Docent Karl vonSmitten and Professor Sirpa Asko-Seljavaara,for supporting me and giving me time offduty to accomplish this work, and for giv-ing me too interesting work to take timeoff; and all colleagues and staff working intheir units for the enjoyable atmospherethey created.
My friends Monika Carpelan-Holmström,Anu Wartiovaara, Johanna Arola, SusanSchmidt, Kai Sahiluoma and Anne Kotola
for helping me to forget the bioresorba-bles.
My parents Sylvi and Allan, my sistersMarjo, Päivi, Eila and Riitta and mybrothers Antti, Heikki, Aaro, Juha, Paavo,Onni and Arvi and their families for theirlove and for enriching my life so much.
Matti Paatero, my beloved musician, forpatience with hundreds of tons of paperspread all over the house, for happy every-day life and for dreams come true.
The Emil Aaltonen Foundation, The Os-kar Öflund Foundation, The Instrumentar-ium Foundation, The Finnish MedicalFoundation, The Technology DevelopmentCentre of Finland (TEKES) and the BI-OMED 2 Programme of the EuropeanCommission for financial support.
Helsinki, February 2000
Hilkka Peltoniemi
71
Ahn, D. K., Sims, C. D., Randolph, M. A.,O’Connor, D., Butler, P. E., Amarante, M. T.,and Yaremchuk, M. J.: Craniofacial skeletalfixation using biodegradable plates and cy-anoacrylate glue. Plast Reconstr Surg 99(1997) 1508-15; discussion 1516-7.
Alberius, P., and Johnell, O.: Repair of in-tra-membranous bone fractures and defectsin rats. Immunolocalization of bone andcartilage proteins and proteoglycans. JCranio-Maxillo-Fac Surg 19 (1991) 15-20.
Albrektsson, T.: The healing of autolo-gous bone grafts after varying degrees ofsurgical trauma. A microscopic and histo-chemical study in the rabbit. J Bone JointSurg Br Vol 62 (1980a) 403-10.
Albrektsson, T.: Repair of bone grafts. Avital microscopic and histological investi-gation in the rabbit. Scand J Plast Recon-str Surg 14 (1980b) 1-12.
Albrektsson, T.: Ischaemia and bonegrafts. Scand J Plast Reconstr Surg - Suppl1982;19:21-4 (1982)
Ali, S. A., Doherty, P. J., and Williams, D.F.: Mechanisms of polymer degradation inimplantable devices. 2. Poly(DL-lacticacid). J Biomed Mater Res 27 (1993)1409-18.
Anastakis, D. J., Antonyshyn, O. M., Coop-er, P. W., Yaffe, M. J., Bush, K., and Mawds-ley, G. E.: Computed tomography artifactsassociated with craniofacial fixation devic-es: an experimental study. Ann Plast Surg37 (1996) 349-55.
Antikainen, T. Biocompatible materialsin the management of deformities of thegrowing skull. Thesis, University of Oulu,Oulu, Finland (1993).
Antikainen, T., Pernu, H., Törmälä, P.,Kallioinen, M., Waris, T., and Serlo, W.: De-velopment of the neurocranium after trans-sutural fixing by new, resorbable poly-L-lactide miniplates. A comparison to fixing
REFERENCES
with the common titanium miniplates.Acta Neurochir 128 (1994) 26-31.
Antonyshyn, O., Colcleugh, R. G., and An-derson, C.: Growth potential in onlay bonegrafts: a comparison of vascularized andfree calvarial bone and suture bone grafts.Plast Reconstr Surg79 (1987) 12-23.
Bahr, W., Stricker, A., Gutwald, R., andWellens, E.: Biodegradable osteosynthesismaterial for stabilization of midface frac-tures: experimental investigation in sheep.J Cranio Maxillofac Surg 27 (1999) 51-7.
Bergsma, E. J., Rozema, F. R., Bos, R. R.,and de Bruijn, W. C.: Foreign body reac-tions to resorbable poly(L-lactide) boneplates and screws used for the fixation ofunstable zygomatic fractures. J Oral Max-illofac Surg 51 (1993) 666-70.
Bergsma, J. E., de Bruijn, W. C., Rozema,F. R., Bos, R. R., and Boering, G.: Late deg-radation tissue response to poly(L-lactide)bone plates and screws. Biomaterials 16(1995) 25-31.
Bessho, K., Iizuka, T., and Murakami, K.:A bioabsorbable poly-L-lactide miniplateand screw system for osteosynthesis in oraland maxillofacial surgery. J Oral Maxillo-fac Surg 55 (1997) 941-5;discussion 945-6.
Bos, R. R., Boering, G., Rozema, F. R., andLeenslag, J. W.: Resorbable poly(L-lactide)plates and screws for the fixation of zygo-matic fractures. J Oral Maxillofac Surg 45(1987) 751-3.
Bos, R. R., Rozema, F. R., Boering, G., Ni-jenhuis, A. J., Pennings, A. J., and Jansen, H.W.: Bone-plates and screws of bioabsorba-ble poly (L-lactide)—an animal pilotstudy. Br J Oral Maxillofac Surg 27(1989a) 467-76.
Bos, R. R., Rozema, F. R., Boering, G., Ni-jenhuis, A. J., Pennings, A. J., and Verwey, A.B.: Bio-absorbable plates and screws for
72
internal fixation of mandibular fractures. Astudy in six dogs. Int J Oral MaxillofacialSurg 18 (1989b) 365-9.
Bouwman, J. P., and Tuinzing, D. B.: Bio-degradable osteosynthesis in mandibularadvancement: a pilot study. Br J Oral Max-illofac Surg 37 (1999) 6-10.
Brady, J. M., Cutright, D. E., Miller, R.A., and Barristone, G. C.: Resorption rate,route, route of elimination, and ultrastruc-ture of the implant site of polylactic acidin the abdominal wall of the rat. J BiomedMater Res 7 (1973) 155-66.
Böstman, O., Hirvensalo, E., Mäkinen, J.,and Rokkanen, P.: Foreign-body reactionsto fracture fixation implants of biodegrad-able synthetic polymers. J Bone Joint SurgBr Vol 72 (1990) 592-6.
Böstman, O., Päivärinta, U., Partio, E.,Vasenius, J., Manninen, M., and Rokkanen,P.: Degradation and tissue replacement ofan absorbable polyglycolide screw in thefixation of rabbit femoral osteotomies. JBone Joint Surg Am Vol 74 (1992a) 1021-31.
Böstman, O. M.: Intense granulomatousinflammatory lesions associated with ab-sorbable internal fixation devices made ofpolyglycolide in ankle fractures. Clin Or-thop Rel Res (1992a) 193-9.
Böstman, O. M., Päivärinta, U., Partio, E.,Manninen, M., Vasenius, J., Majola, A., andRokkanen, P.: The tissue-implant interfaceduring degradation of absorbable polygly-colide fracture fixation screws in the rabbitfemur. Clin Orthop Rel Res (1992b) 263-72.
Böstman, O. M., Pihlajamäki, H. K., Par-tio, E. K., and Rokkanen, P. U.: Clinicalbiocompatibility and degradation ofpolylevolactide screws in the ankle. ClinOrthop Rel Res No 320 (1995) 101-9.
Calhoun, N. R., Tsaknis, P. J., Hughes, D.,and Ajagbe, O.: Osseous repair with LeFort I osteotomy. Oral Surg Oral Med OralPathol67 (1989) 365-73.
Campbell, J. H., Edsberg, L., and Meyer, A.E.: Polylactide inhibition of carcinomacell growth in vitro. J Oral MaxillofacSurg 52 (1994) 49-51.
Carlsson, L., Rostlund, T., Albrektsson, B.,Albrektsson, T., and Branemark, P. I.: Os-seointegration of titanium implants. ActaOrthop Scand 57 (1986) 285-9.
Casteleyn, P. P., Handelberg, F., andHaentjens, P.: Biodegradable rods versusKirschner wire fixation of wrist fractures.A randomised trial. J Bone Joint Surg BrVol 74 (1992) 858-61.
Champy, M., Blez, P., and Kahn, J. L.:[Osteosynthesis using resorbable plates inmaxillofacial surgery: hopes and disap-pointments]. Chirurgie 118 (1992) 596-600.
Claes, L.E., Ignatius, A.A., Rehm, K.E.,and Scholz, C.: New bioresorbable pin forthe reduction of small bony fragments: de-sign, mechanical properties and in vitrodegradation. Biomaterials 17 (1996)1621-1626.
Cordewener, F. W., Bos, R. R., Rozema, F.R., and Houtman, W. A.: Poly(L-lactide)implants for repair of human orbital floordefects: clinical and magnetic resonanceimaging evaluation of long-term results. JOral Maxillofac Surg 54 (1996) 9-13; dis-cussion 13-4.
Cutright, D. E., and Hunsuck, E. E.: Tis-sue reaction to the biodegradable polylac-tic acid suture. Oral Surg Oral Med OralPathol 31 (1971) 134-9.
Cutright, D. E., and Hunsuck, E. E.: Therepair of fractures of the orbital floor usingbiodegradable polylactic acid. Oral SurgOral Med Oral Pathol 33 (1972) 28-34.
Cutright, D. E., Hunsuck, E. E., and Beas-ley, J. D.: Fracture reduction using a bio-degradable material, polylactic acid. J OralSurg29 (1971) 393-7.
Cutright, D. E., Perez, B., Beasley, J. D.d., Larson, W. J., and Posey, W. R.: Degra-dation rates of polymers and copolymers of
73
polylactic and polyglycolic acids. OralSurg Oral Med Oral Pathol 37 (1974)142-52.
Cutting, C. B., and McCarthy, J. G.:Comparison of residual osseous mass be-tween vascularized and nonvascularizedonlay bone transfers. Plast Reconstr Surg72 (1983) 672-5.
Cutting, C. B., McCarthy, J. G., and Ber-enstein, A.: Blood supply of the uppercraniofacial skeleton: the search for com-posite calvarial bone flaps. Plast ReconstrSurg 74 (1984) 603-10.
Dahlin, C., Alberius, P., and Linde, A.:Osteopromotion for cranioplasty. An ex-perimental study in rats using a membranetechnique. J Neurosurg 74 (1991) 487-91.
Dahlin, C., Linde, A., Gottlow, J., andNyman, S.: Healing of bone defects byguided tissue regeneration. Plast ReconstrSurg 81 (1988) 672-6.
de Roche, R., Kuhn, A., de Roche-Weber, P.,Gogolewski, S., Printzen, G., Geissmann, A.,De Jager, M., Hammer, B., Prein, J., andRahn, B.: [Experimental reconstruction ofthe sheep orbit with biodegradable im-plants]. Mund Kiefer Gesichtschir 2(1998) S117-20.
de Roche, V. R., Kuhn, A., de Roche-Weber,P., Printzen, G., Prein, J., Rahn, B., andHammer, B.: [Development of a resorbableimplant: experimental reconstruction ofthe orbits with polylactate membranes.Animal model and preliminary results].Handchir Mikrochir Plast Chir 28 (1996)28-33.
Edwards, R. C., Kiely, K., and Eppley, B.:Resorbable PLLA-PGA screw fixation ofmandibular sagittal split osteotomies. JCraniofac Surg 10 (1999) 230-236.
Edwards, R. C., and Kiely, K. D.: Resorb-able fixation of Le Fort I osteotomies. JCraniofac Surg 9 (1998) 210-4.
Eitenmüller, J., David, A., Pommer, A., andMuhr, G.: [Surgical treatment of anklejoint fractures with biodegradable screws
and plates of poly-l-lactide]. Chirurg 67(1996) 413-8.
Ellis, E. d., Carlson, D. S., and Billups, J.:Osseous healing of the sagittal ramus oste-otomy: a histologic comparison of rigidand nonrigid fixation in Macaca mulatta. JOral Maxillofac Surg 50 (1992) 718-23.
Emerich, D. F., Tracy, M. A., Ward, K. L.,Figueiredo, M., Qian, R., Henschel, C., andBartus, R. T.: Biocompatibility of poly(DL-lactide-co-glycolide) microspheres im-planted into the brain. Cell Transplant8(1) (1999) 47-58.
Engdahl, E.: [The significance of perios-teum in bone regeneration in the maxilla-premaxilla after bone resection (surgicalexperimental and histological study ingrowing rabbits). 2]. Nordisk Medicin 86(1971) 1221-2.
Enislidis, G., Pichorner, S., Kainberger, F.,and Ewers, R.: Lactosorb panel and screwsfor repair of large orbital floor defects. JCranio Maxillofac Surg 25 (1997) 316-21.
Enislidis, G., Pichorner, S., Lambert, F.,Wagner, A., Kainberger, F., Kautzky, M., andEwers, R.: Fixation of zygomatic fractureswith a new biodegradable copolymer oste-osynthesis system. Preliminary results. IntJ Oral Maxillofac Surg 27 (1998) 352-5.
Enlow, D. H. :Facial growth. 3rd edition(1990). W.B. Saunders, Philadelphia.
Eppley, B., and Reilly, M.: Degradationcharasteristics of PLLA-PGA bone fixationdevices. J Craniofac Surg 8 (1997) 116-120.
Eppley, B. L.: Potential for guided boneregeneration and bone graft fixation withresorbable membranes in pediatric cranio-facial surgery. J Craniofac Surg 8 (1997)127-128.Eppley, B. L.: Use of a resorbable fixationtechnique for maxillary fractures. J Cranio-fac Surg 9 (1998) 317-21.
Eppley, B. L., and Prevel, C. D.: Nonme-tallic fixation in traumatic midfacial frac-tures. J Craniofac Surg 8 (1997) 103-109.
74
Eppley, B. L., and Sadove, A. M.: Effectsof resorbable fixation on craniofacial skele-tal growth: a pilot experimental study. JCraniofac Surg 3 (1992) 190-6.
Eppley, B. L., and Sadove, A. M.: A com-parison of resorbable and metallic fixationin healing of calvarial bone grafts. PlastReconstr Surg 96 (1995a) 316-22.
Eppley, B. L., and Sadove, A. M.: Resorb-able coupling fixation in craniosynostosissurgery: experimental and clinical applica-tions. J Craniofac Surg 6 (1995b) 477-82.
Eppley, B. L., Sadove, A. M., and Havlik,R. J.: Resorbable plate fixation in pediat-ric craniofacial surgery. Plast ReconstrSurg 100 (1997) 1-7; discussion 8-13.
Ewers, R., and Lieb-Skowron, J.: Bioab-sorbable osteosynthesis materials. FacialPlast Surg 7 (1990) 206-14.
Fearon, J. A., Munro, I. R., and Bruce, D.A.: Observations on the use of rigid fixa-tion for craniofacial deformities in infantsand young children. Plast Reconstr Surg95 (1995) 634-7; discussion 638.
Fiala, T. G., Novelline, R. A., and Yarem-chuk, M. J.: Comparison of CT imaging ar-tifacts from craniomaxillofacial internalfixation devices. Plast Reconstr Surg 92(1993) 1227-32.
Fiala, T. G., Paige, K. T., Davis, T. L.,Campbell, T. A., Rosen, B. R., and Yarem-chuk, M. J.: Comparison of artifact fromcraniomaxillofacial internal fixation devic-es: magnetic resonance imaging. P Recon-str Surg 93 (1994) 725-31.
Foux, A., Yeadon, A. J., and Uhthoff, H.K.: Improved fracture healing with lessrigid plates. A biomechanical study indogs. Clin Orthop Rel Res (1997) 232-45.
Frazza, E. J., and Schmitt, E. E.: A newabsorbable suture. J Biomed Mater Res 5(1971) 43-58.
Friede, H.: Normal development andgrowth of the human neurocranium andcranial base. Scand J Plast Reconstr Surg15 (1981) 163-9.
Frokjaer, J., and Moller, B. N.: Biode-gradable fixation of ankle fractures. Com-plications in a prospective study of 25 cas-es. Acta Orthop Scand 63 (1992) 434-6.
Fuente del Campo, A., Pohjonen, T.,Törmälä, P., and Waris, T.: Fixation of hori-zontal maxillary osteotomies with biode-gradable self-reinforced absorbable poly-lactide plates: preliminary results. Eur JPlast Surg 19 (1996) 7-9.
Gerlach, K. L., Krause, H. R., and Eiten-müller, J.s:. Use of absorbable osteosynthe-sis material for mandibular fracture treat-ment of dogs, In: Biomaterials and ClinicalApplications. A. Pizzoferrato, P. G. Mar-chetti, A. Ravagliori, and A. C. J. Lees,Amsterdam Elsevier Science PublisherB.V. (1987) 459-464.
Getter, L., Cutright, D. E., Bhaskar, S. N.,and Augsburg, J. K.: A biodegradable in-traosseous appliance in the treatment ofmandibular fractures. J Oral Surg 30(1972) 344-8.
Gilding, D. K., and Reed, A. M.: Biode-gradable polymers for use in surgery -poly(glycolic)/poly(lactic acid) homo andcopolymers:1. Polymer 20 (1979) 1459-1464.
Goldberg, D. S., Bartlett, S., Yu, J. C.,Hunter, J. V., and Whitaker, L. A.: Criticalreview of microfixation in pediatric cranio-facial surgery. J Craniofac Surg 6 (1995)301-7; discussion 308.
Goldner, J.: A modification of the Mas-son trichrome technique for routine labo-ratory purposes. Am J Pathol14 (1938)237.
Goldstein, J. A., Quereshy, F. A., and Co-hen, A. R.: Early experience with biode-gradable fixation for congenital pediatriccraniofacial surgery. J Craniofac Surg 8(1997) 110-115.
Gosain, A.K., and Persing, J.A.: Biomate-rials in the face: benefits and risks. JCraniofac Surg 10 (1999) 404-414.
Gosain, A. K., Song, L., Corrao, M. A.,
75
and Pintar, F. A.: Biomechanical evalua-tion of titanium, biodegradable plate andscrew, and cyanoacrylate glue fixation sys-tems in craniofacial surgery. Plast ReconstrSurg 101 (1998) 582-91.
Gottlow, J.: Guided tissue regenerationusing bioresorbable and non-resorbable de-vices: initial healing and long-term results.J Periodontol 64 (1993) 1157-65.
Gottlow, J., Nyman, S., Karring, T., andLindhe, J.: New attachment formation asthe result of controlled tissue regeneration.J Clin Periodontol 11 (1984) 494-503.
Habal, M. B.: Fixation, imaging, andresorption [editorial]. J Craniofac Surg 7(1996a) 325.
Habal, M. B.: Triad of system applica-tions for absorbable rigid fixation of thecraniofacial skeleton. J Craniofac Surg 7(1996b) 394-8.
Habal, M. B.: Absorbable, invisible,and flexible plating system for the cranio-facial skeleton. J Craniofac Surg 8 (1997)121-126.
Haers, P. E., and Sailer, H. F.: Biodegrad-able self-reinforced poly-L/DL-lactideplates and screws in bimaxillary orthog-nathic surgery: short term skeletal stabilityand material related failures. J CranioMaxillofac Surg 26 (1998) 363-72.
Haers, P. E., Suuronen, R., Lindqvist, C.,and Sailer, H.: Biodegradable polylactideplates and screws in orthognathic surgery:technical note. J Cranio Maxillofac Surg26 (1998) 87-91.
Herrmann, J. B., Kelly, R. J., and Higgins,G. A.: Polyglycolic acid sutures. Laborato-ry and clinical evaluation of a new absorba-ble suture material. Arch Surg 100 (1970)486-90.
Hobar, P. C., Masson, J. A., Wilson, R.,and Zerwekh, J.: The importance of thedura in craniofacial surgery. Plast ReconstrSurg 98 (1996) 217-25.
Hobar, P. C., Schreiber, J. S., McCarthy, J.G., and Thomas, P. A.: The role of the dura
in cranial bone regeneration in the imma-ture animal. Plast Reconstr Surg 92 (1993)405-10.
Hollinger, J. O., and Battistone, G. C.: Bi-odegradable bone repair materials. Syn-thetic polymers and ceramics. Clin OrthopRel Res (1986) 290-305.
Honig, J. F., Merten, H. A., and Luhr, H.G.: Passive and active intracranial translo-cation of osteosynthesis plates in adoles-cent minipigs. J Craniofac Surg 6 (1995)292-8; discussion 299-300.
Hutmacher, D., Hurzeler, M. B., andSchliephake, H.: A review of material prop-erties of biodegradable and bioresorbablepolymers and devices for GTR and GBRapplications. Int J Oral Maxillofac Impl 11(1996) 667-78.
Iizuka, T., Lindqvist, C., Hallikainen, D.,Mikkonen, P., and Paukku, P.: Severe boneresorption and osteoarthrosis after mini-plate fixation of high condylar fractures. Aclinical and radiologic study of thirteenpatients. Oral Surg Oral Med Oral Pathol72 (1991a) 400-7.
Iizuka, T., Mikkonen, P., Paukku, P., andLindqvist, C.: Reconstruction of orbitalfloor with polydioxanone plate. Int J OralMaxillofac Surg 20 (1991b) 83-7.
Illi, O. E., and Feldmann, C. P.: Stimula-tion of fracture healing by local applica-tion of humoral factors integrated in bio-degradable implants. Eur J Ped Surg 8(1998) 251-5.
Illi, O. E., Sailer, H., and Stauffer, U. G.:[Preliminary results of biodegradable oste-osynthesis in craniofacial surgery in thechild]. Chir Pediatr 30 (1989) 284-7.
Illi, O. E., Stauffer, U. G., Sailer, H., andBeck, P.: [Biodegradable osteosynthesis ap-plied to craniofacial surgery]. Chir Pediatr31 (1990) 240-4.
Illi, O. E., Stauffer, U. G., Sailer, H. F.,and Weigum, H.: [Resorbable implants incraniofacial surgery in childhood. A contri-bution to the development of poly(lactide)

76
implants]. Helv Chir Acta 58 (1991) 123-7.
Jackson, I. T., Munro, I. R., Salyer, K. E.,and Whitaker, L. A. Atlas of Craniomaxil-lofacial Surgery, Mosby, St Louis (1982).
Jackson, I. T., Somers, P. C., and Kjar, J.G.: The use of Champy miniplates for os-teosynthesis in craniofacial deformities andtrauma. Plast Reconstr Surg 77 (1986)729-36.
Jorgenson, D. S., Mayer, M. H., Ellenbogen,R. G., Centeno, J. A., Johnson, F. B., Mullick,F. G., and Manson, P. N.: Detection of tita-nium in human tissues after craniofacialsurgery [see comments]. Plast ReconstrSurg 99 (1997) 976-9; discussion 980-1.
Kallela, I., Iizuka, T., Salo, A., andLindqvist, C.: Lag-screw fixation of anteri-or mandibular fractures using biodegrada-ble polylactide screws: a preliminary re-port. J Oral Maxillofac Surg 57 (1999a)113-8.
Kallela, I., Laine, P., Suuronen, R., Iizuka,T., Pirinen, S., and Lindqvist, C.: Skeletalstability following mandibular advance-ment and rigid fixation with polylactidebiodegradable screws. Int J Oral Maxillo-fac Surg 27 (1998) 3-8.
Kallela, I., Laine, P., Suuronen, R., Ranta,P., Iizuka, T., and Lindqvist, C.: Osteotomysite healing following mandibular sagittalsplit osteotomy and rigid fixation withpolylactide biodegradable screws. AesthReconstr Surg 28 (1999b) 166-170.
Kallela, I., Tulamo, R.-M., Hietanen, J.,Pohjonen, T., Suuronen, R., and Lindqvist, C.:Fixation of mandibular body osteotomiesusing biodegradable amorphous self-rein-forced (70L:30DL) polylactide or metal lagscrews: an experimental study in sheep. JCranio Maxillofac Surg 27 (1999c) 124-133.
Karring, T., Nyman, S., Gottlow, J., andLaurell, L.: Development of the biologicalconcept of guided tissue regeneration—an-imal and human studies. Periodontol 2000
1 (1993) 26-35.Katou, F., Andoh, N., Motegi, K., and
Nagura, H.: Immuno-inflammatory re-sponses in the tissue adjacent to titaniumminiplates used in the treatment of man-dibular fractures. J Cranio Maxillofac Surg24 (1996) 155-62.
Kellman, R. M., Huckins, S. C., King, J.,Humphrey, D., Marentette, L., and Osborn, D.C.: Bioresorbable screws for facial bone re-construction: a pilot study in rabbits.Laryngoscope 104 (1994) 556-61.
Kennady, M. C., Tucker, M. R., Lester, G.E., and Buckley, M. J.: Histomorphometricevaluation of stress shielding in mandibu-lar continuity defects treated with rigidfixation plates and bone grafts. Int J OralMaxillofac Surg18 (1989a) 170-4.
Kennady, M. C., Tucker, M. R., Lester, G.E., and Buckley, M. J.: Stress shielding ef-fect of rigid internal fixation plates onmandibular bone grafts. A photon absorp-tion densitometry and quantitative com-puterized tomographic evaluation. Int JOral Maxillofac Surg 18 (1989b) 307-10.
Kim, Y. K., Yeo, H. H., and Lim, S. C.:Tissue response to titanium plates: a trans-mitted electron microscopic study [seecomments]. J Oral Maxillofac Surg 55(1997) 322-6.
Koskikare, K., Hirvensalo, E., Pätiälä, H.,Rokkanen, P., Pohjonen, T., Törmälä, P., andLob, G.: Intraosseous plating with absorb-able self-reinforced poly-L-lactide plates inthe fixation of distal femoral osteotomieson rabbits. J Biomed Mater Res 30 (1996)417-21.
Koskikare, K., Pihlajamäki, H., Pätiälä,H., and Rokkanen, P. Comparison of intra-and extraosseally placed self-reinforcedpoly-L-lactide plates in the fixation of dis-tal femoral osteotomies in rabbits. AnnChir Gynaecol 86 (1997) 261-268.
Kulkarni, R. K., Moore, E. G., Hegyeli, A.F., and Leonard, F.: Biodegradablepoly(lactic acid) polymers. J Biomed Mater

77
Res 5 (1971) 169-81.Kulkarni, R. K., Pani, K. C., Neuman, C.,
and Leonard, F.: Polylactic acid for surgicalimplants. Arch Surg93 (1966) 839-43.
Kumar, A. V., Staffenberg, D. A., Petronio,J. A., and Wood, R. J.: Bioabsorbableplates and screws in pediatric craniofacialsurgery: a review of 22 cases. J CraniofacSurg8 (1997) 97-99.
Lalor, P. A., Gray, A. B., Wright, S., Rail-ton, G. T., Freeman, M. A., and Revell, P. A.:Contact sensitivity to titanium in a hipprosthesis? Contact Dermatitis 23 (1990)193-4.
Leenslag, J. W., Pennings, A. J., Bos, R. R.,Rozema, F. R., and Boering, G.: Resorbablematerials of poly(L-lactide). VI. Plates andscrews for internal fracture fixation. Bio-materials 8 (1987) 70-3.
Lemperle, S. M., Calhoun, C. J., Curran, R.W., and Holmes, R. E.: Bony healing oflarge cranial and mandibular defects pro-tected from soft-tissue interposition: Acomparative study of spontaneous bone re-generation, osteoconduction, and cancel-lous autografting in dogs. Plast ReconstrSurg 101 (1998) 660-72.
Levy, F. E., Hollinger, J. O., and Szachow-icz, E. H.: Effect of a bioresorbable film onregeneration of cranial bone. Plast Recon-str Surg 93 (1994) 307-11; discussion312.
Lin, K. Y., Bartlett, S. P., Yaremchuk, M.J., Fallon, M., Grossman, R. F., and Whitak-er, L. A.: The effect of rigid fixation on thesurvival of onlay bone grafts: an experi-mental study [see comments]. Plast Recon-str Surg 86 (1990) 449-56.
Lin, K. Y., Bartlett, S. P., Yaremchuk, M.J., Grossman, R. F., Udupa, J. K., andWhitaker, L. A.: An experimental study onthe effect of rigid fixation on the develop-ing craniofacial skeleton. Plast ReconstrSurg 87 (1991) 229-35.
Linde, A., Alberius, P., Dahlin, C., Bjur-stam, K., and Sundin, Y.: Osteopromotion:
a soft-tissue exclusion principle using amembrane for bone healing and bone neo-genesis. J Periodontol 64 (1993) 1116-28.
Linder, L., Albrektsson, T., Branemark, P.I., Hansson, H. A., Ivarsson, B., Jonsson, U.,and Lundstrom, I.: Electron microscopicanalysis of the bone-titanium interface.Acta Orthop Scand 54 (1983) 45-52.
Losken, H. W., Tschakaloff, A., von Oepen,R., Mooney, M. P., Moritz, O., Michaeli, W.,Lalikos, J., and Losken, A.: Memory of DL-polylactic acid biodegradable plates. AnnPlast Surg 32 (1994) 606-11.
Lundgren, D., Laurell, L., Gottlow, J., Ry-lander, H., Mathisen, T., Nyman, S., andRask, M.: The influence of the design oftwo different bioresorbable barriers on theresults of guided tissue regeneration thera-py. An intra-individual comparative studyin the monkey. J Periodontol 66 (1995)605-12.
Majola, A., Vainionpää, S., Vihtonen, K.,Mero, M., Vasenius, J., Törmälä, P., andRokkanen, P.: Absorption, biocompatibili-ty, and fixation properties of polylactic acidin bone tissue: an experimental study inrats. Clin Orthop Rel Res (1991) 260-9.
Manson, P. N.: Facial bone healing andbone grafts. A review of clinical physiolo-gy. Clin Plast Surg 21 (1994) 331-48.
Marschall, M. A., Chidyllo, S. A., Figuer-oa, A. A., and Cohen, M.: Long-term effectsof rigid fixation on the growing crani-omaxillofacial skeleton. J Craniofac Surg 2(1991) 63-8; discussion 69-70.
Matsusue, Y., Hanafusa, S., Yamamuro, T.,Shikinami, Y., and Ikada, Y.: Tissue reactionof bioabsorbable ultra high strength poly(L-lactide) rod. A long-term study in rab-bits. Clin Orthop Rel Res (1995) 246-53.
McCann, K. J., Irish, J. C., Gullane, P. J.,Holmes, H., Brown, D. H., and Rotstein, L.:Complications associated with rigid fixa-tion of mandibulotomies. J Otolaryngol 23(1994) 210-5.

78
Meikle, M. C., Papaioannou, S., Ratledge,T. J., Speight, P. M., Watt-Smith, S. R., Hill,P. A., and Reynolds, J. J.: Effect of polyDL-lactide—co-glycolide implants and xe-nogeneic bone matrix-derived growth fac-tors on calvarial bone repair in the rabbit.Biomaterials 15 (1994) 513-21.
Menei, P., Daniel, V., Montero-Menei, C.,Brouillard, M., Pouplard-Barthelaix, A., andBenoit, J. P.: Biodegradation and brain tis-sue reaction to poly(D,L-lactide-co-glycol-ide) microspheres. Biomaterials 14 (1993)470-8.
Milch, R.A., Rall, D.P., Tobie, J.E. et al.:Fluorescence of tetracycline antibiotics inbone. J Bone Joint Surg Am 40 (1958)897-910.
Miller, N. D., and Williams, D. F.: Thein vivo and in vitro degradation ofpoly(glycolic acid) suture material as afunction of applied strain. Biomaterials 5(1984) 365-8.
Miller, R. A., Brady, J. M., and Cutright,D. E.: Degradation rates of oral resorbableimplants (polylactates and polyglycolates):rate modification with changes in PLA/PGA copolymer ratios. J Biomed MaterRes 11 (1977) 711-9.
Mofid, M.M., Thompson, R.C., Pardo,C.A., Manson, P.N., and Vander Kolk, C.A.:Biocompatibility of fixation materials inthe brain. Plast Reconstr Surg 100 (1997)14-20; discussion 21-2.
Montag, M. E., Morales, J., L., and Daane,S.: Bioabsorbables: their use in pediatriccraniofacial surgery. J Craniofac Surg 8(1997) 100-102.
Mooney, M. P., Losken, H. W., Siegel, M. I.,Tsachakaloff, A., Losken, A., and Janosky, J.:Plate fixation of premaxillomaxillary su-ture and compensatory midfacial growthchanges in the rabbit. J Craniofac Surg 3(1992) 197-202.
Mooney, M. P., Mundell, R. D., Stetzer, K.,Ochs, M. W., Milch, E. A., Buckley, M. J.,and Siegel, M. I.: The effects of guided tis-
sue regeneration and fixation technique onosseous wound healing in rabbit zygomat-ic arch osteotomies. J Craniofac Surg 7(1996) 46-53.
Mossaz, C. F., and Kokich, V. G.: Rede-velopment of the calvaria after partialcraniectomy in growing rabbits: the effectof altering dural continuity. Acta Anat109 (1981) 321-31.
Mühlbauer, W., and Anderl, H.: [Mini-plate osteosynthesis in craniofacial sur-gery]. Handchir Mikrochir Plast Chir 15(1983) 77-82.
Mühlbauer, W., Anderl, H., Ramatschi, P.,Heeckt, P., Zenker, J., Deubzer, M., Hopner, F.,and Vertesy, E.: Radical treatment ofcraniofacial anomalies in infancy and theuse of miniplates in craniofacial surgery.Clin Plast Surg 14 (1987) 101-11.
Muhonen, M. G., Piper, J. G., and Menezes,A. H.: Pathogenesis and treatment ofgrowing skull fractures. Surg Neurol 43(1995) 367-72; discussion 372-3.
Mäkelä, E.A., Böstman, O., Kekomäki, M.,Södergård, J., Vainio, J., Törmälä, P., andRokkanen, P.: Biodegradable fixation of dis-tal humeral physeal fractures. Clin OrthopRel Res 283 (1992) 237-43.
Nair, P.D.: Currently practised steriliza-tion methods - some inadvertent conse-quences. J Biomater Appl 10 (1995) 121-135.
Nakamura, T., Hitomi, S., Watanabe, S.,Shimizu, Y., Jamshidi, K., Hyon, S. H., andIkada, Y.: Bioabsorption of polylactideswith different molecular properties. J Bi-omed Mater Res 23 (1989) 1115-30.
Nakamura, T., Shimizu, Y., Okumura, N.,Matsui, T., Hyon, S. H., and Shimamoto, T.:Tumorigenicity of poly-L-lactide (PLLA)plates compared with medical-grade poly-ethylene. J Biomed Mater Res 28 (1994)17-25.
Nordström, P., Pihlajamäki, H., Toivonen,T., Törmälä, P., and Rokkanen, P.: Tissue re-sponse to polyglycolide and polylactide
79
pins in cancellous bone. Arch OrthopTrauma Surg117 (1998) 197-204.
Oppenheimer, B. S., Oppenheimer, E. T.,Danishefsky, I., Stout, A. P., and Eirich, F. R.:Further studies of polymers as carcinogenicagents in animals. Cancer Res 15 (1955)333-345.
Orringer, J. S., Barcelona, V., and Buchman,S. R.: Reasons for removal of rigid internalfixation devices in craniofacial surgery. JCraniofac Surg 9 (1998) 40-4.
Paavolainen, P., Karaharju, E., Slätis, P.,Ahonen, J., and Holmström, T.: Effect of rig-id plate fixation on structure and mineralcontent of cortical bone. Clin Orthop RelRes (1978) 287-93.
Päivärinta, U., Böstman, O., Majola, A.,Toivonen, T., Törmälä, P., and Rokkanen, P.:Intraosseous cellular response to biode-gradable fracture fixation screws made ofpolyglycolide or polylactide. Arch OrthopTrauma Surg 112 (1993) 71-4.
Papay, F. A., Hardy, S., Morales, L., Jr.,Walker, M., and Enlow, D.: “False” migra-tion of rigid fixation appliances in pediat-ric craniofacial surgery. J Craniofac Surg 6(1995) 309-13.
Pelto-Vasenius, K., Hirvensalo, E., Vasenius,J., and Rokkanen, P.: Osteolytic changes af-ter polyglycolide pin fixation in chevronosteotomy. Foot Ankle Internat18 (1997)21-5.
Pensler, J. M.: Role of resorbable platesand screws in craniofacial surgery. JCraniofac Surg 8 (1997) 129-134.
Persing, J. A., Posnick, J., Magge, S.,Spinelli, H. M., Wolfe, S. A., Munro, I., andMulliken, J. B.: Cranial plate and screwfixation in infancy: an assessment of risk. JCraniofac Surg 7 (1996) 267-70.
Phillips, J. H., and Rahn, B. A.: Fixationeffects on membranous and endochondralonlay bone graft revascularization andbone deposition. Plast Reconstr Surg 85(1990) 891-7.
Pietrzak, W. S., Sarver, D. R., and Ver-
stynen, M. L.: Bioabsorbable polymer sci-ence for the practicing surgeon. J Cranio-fac Surg 8 (1997) 87-91.
Pistner, H., Gutwald, R., Ordung, R., Reu-ther, J., and Muhling, J.: Poly(L-lactide): along-term degradation study in vivo. I. Bi-ological results. Biomaterials 14 (1993)671-7.
Pohjonen, T., Helevirta, P., Törmälä, P., Ko-skikare, K., Pätiälä, H., and Rokkanen, P.:Strength retention of self-reinforced poly-L-lactide screws. A comparison of com-pression moulded and machine cut screws.J Mater Sci Mater Med 8 (1997) 311-320.
Polley, J. W., Figueroa, A., Hung, K. F.,Cohen, M., and Lakars, T.: Effect of rigidmicrofixation on the craniomaxillofacialskeleton. J Craniofac Surg 6 (1995) 132-8.
Polley, J. W., Hung, K. F., Figueroa, A.,Lakars, T., and Heiberger, H.: Alternativetechniques in rigid fixation of the crani-omaxillofacial skeleton. J Craniofac Surg 9(1998) 249-53.
Posnick, J. C., and Yaremchuk, M. J.: Theeffects of nonresorbable internal fixationdevices placed on and within a child’s cra-nial vault: brain function, morbidity, andgrowth restriction [editorial]. Plast Recon-str Surg 96 (1995) 966-8.
Powiertowski, H., and Matlosz, Z.: [Ef-fects of the treatment of craniostenosiswith upper skull resection]. Ann de Chir24 (1970) 1175-80.
Prevot, M., Renier, D., and Marchac, D.:Lack of ossification after cranioplasty forcraniosynostosis: a review of relevant factorsin 592 consecutive patients. J CraniofacSurg 4 (1993) 247-54; discussion 255-6.
Reid, C. A., McCarthy, J. G., and Kolber,A. B.: A study of regeneration in parietalbone defects in rabbits. Plast ReconstrSurg 67 (1981) 591-6.
Resnick, J. I., Kinney, B. M., and Kawamo-to, H. K., Jr.: The effect of rigid internalfixation on cranial growth. Ann PlastSurg25 (1990) 372-4.

80
Revell, P.A.: Histomorphometry of bone.J Clin Pathol 36 (1983) 1323-31.
Rokkanen, P., Böstman, O., Vainionpää, S.,Mäkelä, E. A., Hirvensalo, E., Partio, E. K.,Vihtonen, K., Pätiälä, H., and Törmälä, P.:Absorbable devices in the fixation of frac-tures. J Trauma 40 (1996) S123-7.
Rosenberg, A., Gratz, K. W., and Sailer, H.F.: Should titanium miniplates be re-moved after bone healing is complete? IntJ Oral Maxillofac Surg 22 (1993) 185-8.
Rozema, F. R., Bos, R. R., Boering, G.,Leenslag, J. W., and Pennings, A. J.: Experi-mental fractures of the mandibular body ofsheep and dogs. A new technique. Br JOral Maxillofac Surg 27 (1989) 163-8.
Rozema, F. R., Bos, R. R., Pennings, A. J.,and Jansen, H. W.: Poly(L-lactide) im-plants in repair of defects of the orbitalfloor: an animal study. J Oral MaxillofacSurg 48 (1990a) 1305-9; discussion 1310.
Rozema, F. R., Levendag, P. C., Bos, R. R.,Boering, G., and Pennings, A. J.: Influenceof resorbable poly(L-lactide) bone platesand screws on the dose distributions of ra-diotherapy beams. Int J Oral MaxillofacSurg 19 (1990b) 374-6.
Sadove, A. M., and Eppley, B. L.: Micro-fixation techniques in pediatric craniomax-illofacial surgery. Ann Plast Surg 27(1991) 36-43.
Salyer, K. E., Bardach, J., Squier, C. A.,and Kelly, K. M.: A comparative study ofthe effects of biodegradable and titaniumplating systems on cranial growth andstructure: experimental study in beagles.Plast Reconstr Surg 93 (1994) 705-13.
Santavirta, S., Konttinen, Y. T., Saito, T.,Grönblad, M., Partio, E., Kemppinen, P., andRokkanen, P.: Immune response to polygly-colic acid implants. J Bone Joint Surg BrVol 72 (1990) 597-600.
Sasserath, C., Van Reck, J., and Gitani, J.:[The use of a polyglycolic acid membranein the reconstruction of the orbital floorand in loss of bone substance in the maxil-
lofacial region]. Acta Stomatol Belg 88(1991) 5-11.
Schliephake, H., Lehmann, H., Kunz, U.,and Schmelzeisen, R.: Ultrastructural find-ings in soft tissues adjacent to titaniumplates used in jaw fracture treatment. Int JOral Maxillofac Surg 22 (1993a) 20-5.
Schliephake, H., Reiss, G., Urban, R., Neu-kam, F. W., and Guckel, S.: Metal releasefrom titanium fixtures during placementin the mandible: an experimental study.Int J Oral Maxillofac Impl 8 (1993b) 502-11.
Shetty, V., and Caputo, A.s:. Maxillofacialapplications of self-reinforced poly-l-lac-tide (SR-PLLA) devices: biomechanicalconciderations, In: Self-reinforced Bioab-sorbable Polymeric Composites in Surgery.P. Rokkanen and P. Törmälä (Eds.), Offset-paino, Tampere (1995) 84-101.
Sirola, K.: Regeneration of defects in thecalvaria. An experimental study. Ann MedExp Biol Fenn 38 (1960) 1-87.
Smith, D. W., and Tondury, G.: Origin ofthe calvaria and its sutures. Am J Dis Chil-dr 132 (1978) 662-6.
Stelnicki, E. J., and Hoffman, W.: Intracra-nial migration of microplates versus wiresin neonatal pigs after frontal advancement.J Craniofac Surg 9 (1998) 60-4.
Sullivan, P. K., Smith, J. F., and Rozzelle,A. A.: Cranio-orbital reconstruction: safe-ty and image quality of metallic implantson CT and MRI scanning. Plast ReconstrSurg 94 (1994) 589-96.
Sunderman, F. W., Jr.: Carcinogenicity ofmetal alloys in orthopedic prostheses: clin-ical and experimental studies. FundamAppl Toxicol13 (1989) 205-16.
Suuronen, R., Pohjonen, T., Wessman, L.,Törmälä, P., Vainionpää, S.: New genera-tion biodegradable plate for fracture fixa-tion. Comparison of bending strengths ofmandibular osteotomies fixed with absorb-able self-reinforced multi-layer poly-l-lac-tide plates and metallic plates. An experi-

81
mental study in sheep. Clin Mater 9(1992a) 77-84.
Suuronen, R.: Comparison of absorbableself-reinforced poly-L-lactide screws andmetallic screws in the fixation of mandibu-lar condyle osteotomies: an experimentalstudy in sheep. J Oral Maxillofac Surg 49(1991) 989-95.
Suuronen, R.: Biodegradable fracture-fix-ation devices in maxillofacial surgery. Int JOral Maxillofac Surg 22 (1993) 50-7.
Suuronen, R., Haers, P. E., Lindqvist, C.,and Sailer, H. F.: Update on bioresorbableplates in maxillofacial surgery. Facial PlastSurg 15 (1999) 61-72.
Suuronen, R., Iizuka, T., Pirinen, S., andLindqvist, C.: Skeletal stability followingmandibular advancement and rigid fixa-tion with polylactide biodegradablescrews. Int J Oral Maxillofac Surg 27(1998a) 3-8.
Suuronen, R., Laine, P., Pohjonen, T., andLindqvist, C.: Sagittal ramus osteotomiesfixed with biodegradable screws: a prelim-inary report. J Oral Maxillofac Surg 52(1994) 715-20; discussion 720-1.
Suuronen, R., Manninen, M. J., Pohjonen,T., Laitinen, O., and Lindqvist, C.: Mandib-ular osteotomy fixed with biodegradableplates and screws: an animal study. Br JOral Maxillofac Surg 35 (1997) 341-8.
Suuronen, R., Pohjonen, T., Hietanen, J.,and Lindqvist, C.: A 5-year in vitro and invivo study of the biodegradation of poly-lactide plates. J Oral Maxillofac Surg 56(1998b) 604-14; discussion 614-5.
Suuronen, R., Pohjonen, T., Vasenius, J., andVainionpää, S.: Comparison of absorbableself-reinforced multilayer poly-l-lactideand metallic plates for the fixation of man-dibular body osteotomies: an experimentalstudy in sheep. J Oral Maxillofac Surg 50(1992b) 255-62.
Tams, J., Joziasse, C. A., Bos, R. R., Roze-ma, F. R., Grijpma, D. W., and Pennings, A.J.: High-impact poly(L/D-lactide) for frac-
ture fixation: in vitro degradation and ani-mal pilot study. Biomaterials 16 (1995)1409-15.
Tams, J., Rozema, F. R., Bos, R. R., Rood-enburg, J. L., Nikkels, P. G., and Vermey, A.:Poly(L-lactide) bone plates and screws forinternal fixation of mandibular swing oste-otomies. Int J Oral Maxillofac Surg 25(1996) 20-4.
Tartaro, G. P., Adamo, C., Rubino, C., andColella, G.: [Clinical use of resorbable pol-ymer mini-plates in mandibular fractures:a one-year experience]. Minerva Stomatol45 (1996) 305-9.
Tatum, S. A., Kellman, R. M., and Freije,J. E.: Maxillofacial fixation with absorbableminiplates: computed tomographic follow-up. J Craniofac Surg 8 (1997) 135-40.
Thaller, S. R., Hoyt, J., Borjeson, K., Dart,A., and Tesluk, H.: Polyglyconate platesand screws to stabilize zygomatic osteoto-mies in a rabbit model. J Craniofac Surg 4(1993) 228-33.
Thaller, S. R., Huang, V., and Tesluk, H.:Use of biodegradable plates and screws in arabbit model. J Craniofac Surg 2 (1992)168-73.
Thaller, S. R., Lee, T., and Tesluk, H.:Polyglyconate fixation successfully stabi-lizes zygomatic osteotomies in a nonhu-man primate. J Craniofac Surg 6 (1995a)459-64; discussion 465.
Thaller, S. R., Moore, C., and Tesluk, H.:Biodegradable polyglyconate plates andscrews: a histological evaluation in a rabbitmodel. J Craniofac Surg 6 (1995b) 282-7.
Thaller, S. R., Moore, C., Tesluk, H., andHolmes, R.: Cranial bone grafting: biode-gradable versus titanium fixation in a rab-bit model. J Craniofac Surg 7 (1996) 54-9.
Tharanon, W., Sinn, D. P., Hobar, P. C.,Sklar, F. H., and Salomon, J.: Surgical out-comes using bioabsorbable plating systemsin pediatric craniofacial surgery. J Cranio-fac Surg 9 (1998) 441-4; discussion 445-7.
Törmälä, P.: Biodegradable self-rein-
82
forced composite materials; manufacturingstructure and mechanical properties. ClinMater 10 (1992) 29-34.
Törmälä, P., and Pohjonen, T.s:. Ultra-high strength bioabsorbable polymericcomposites for surgical applications, In:Self-reinforced Bioabsorbable PolymericComposites in Surgery. P. Rokkanen and P.Törmälä (Eds) Offsetpaino, Tampere(1995) 1-23.
Törmälä, P., Pohjonen, T., and Rokkanen,P.: Bioabsorbable polymers: materialstechnology and surgical applications. Pro-ceedings of the Institution of MechanicalEngineers. Part H - J Eng Med212 (1998)101-11.
Tschakaloff, A., Losken, H. W., Lalikos, J.,Link, J., Mooney, M. P., von Oepen, R.,Michaeli, W., and Losken, A.: Experimentalstudies of DL-polylactic acid biodegrada-ble plates and screws in rabbits: computedtomography and molecular weight loss. JCraniofac Surg 4 (1993) 223-7.
Tschakaloff, A., Losken, H. W., von Oepen,R., Michaeli, W., Moritz, O., Mooney, M. P.,and Losken, A.: Degradation kinetics of bi-odegradable DL-polylactic acid biodegrad-able implants depending on the site of im-plantation. Int J Oral Maxillofac Surg 23(1994) 443-5.
Uhthoff, H. K., and Dubuc, F. L.: Bonestructure changes in the dog under rigidinternal fixation. Clin Orthop Rel Res 81(1971) 165-70.
Uhthoff, H. K., and Finnegan, M.: Theeffects of metal plates on post-traumaticremodelling and bone mass. J Bone JointSurg Br Vol 65 (1983) 66-71.
Umansky, W., and Schendel, S. A.: Ex-panding cranial defects following craniofa-cial surgery. Plast Reconstr Surg 96 (1995)969-71.
Vallfors, B., Hansson, H. A., and Svensson,J.: Absorbable or nonabsorbable suturematerials for closure of the dura mater?Neurosurg 9 (1981) 407-13.
Vasenius, J., Vainionpää, S., Vihtonen, K.,Mäkelä, A., Rokkanen, P., Mero, M., andTörmälä, P.: Comparison of in vitro hy-drolysis, subcutaneous and intramedullaryimplantation to evaluate the strength re-tention of absorbable osteosynthesis im-plants. Biomaterials 11 (1990a) 501-4.
Vasenius, J., Vainionpää, S., Vihtonen, K.,Mero, M., Mäkelä, A., Törmälä, P., andRokkanen, P.: A histomorphological studyon self-reinforced polyglycolide (SR-PGA)osteosynthesis implants coated with slowlyabsorbable polymers. J Biomed Mater Res24 (1990b) 1615-35.
Vert, M., Chabot, F., Leray, J., and Chris-tel, P.: Stereoregular bioresorbable polyes-ters for orthopaedic surgery. MacromolecChem Physics Suppl 5 (1981) 221-231.
Viljanen, J., Kinnunen, J., Bondestam, S.,and Rokkanen, P.: Intramedullary fixationof distal femoral diaphyseal osteotomieswith absorbable self-reinforced poly-L-lac-tide and metallic intramedullary rods as-sessed by plain radiographs, quantitativecomputed tomography, and magnetic reso-nance imaging: an experimental study inrabbits. J Biomed Mater Res 39 (1998)222-8.
Viljanen, J., Pihlajamäki, H., Majola, A.,Törmälä, P., and Rokkanen, P.: Absorbablepolylactide pins versus metallic Kirschnerwires in the fixation of cancellous bone os-teotomies in rats. Ann Chir Gynaecol 86(1997) 66-73.
Wagemans, P. A., van de Velde, J. P., andKuijpers-Jagtman, A. M.: Sutures and forc-es: a review. Am J Orthodont Dentofac Or-thop 94 (1988) 129-41.
Waitzman, A. A., Posnick, J. C., Arm-strong, D. C., and Pron, G. E.: Craniofacialskeletal measurements based on computedtomography: Part II. Normal values andgrowth trends [see comments]. Cleft PalateCraniofac J 29 (1992) 118-28.
Wang, W., Ferguson, D. J., Quinn, J. M.,Simpson, A. H., and Athanasou, N. A.: Bio-
83
material particle phagocytosis by bone-re-sorbing osteoclasts. J Bone Joint Surg BrVol 79 (1997) 849-56.
Waris, T., Serlo, W., Öhman, J., Merikanto,J., Pohjonen, T., Lauritzen, C., Fuente delCampo, A., Peltoniemi, H., and Törmälä, P.:Craniofacial surgery with self-reinforcedpolylactide plates. Osteosynthese Internation-al, abstract 168, June 15-17, 1995, Oulu,Finland.
Weisberger, E. C., and Eppley, B. L.: Re-sorbable fixation plates in head and necksurgery. Laryngoscope 107 (1997) 716-9.
Williams, D. F.: Review. Biodegradationof surgical polymers. J Mater Sci 17 (1982)1233-1246.
Williams, D. F.: Mechanisms of biodeg-radation of implantable polymers. ClinMater 10 (1992) 9-12.
Winet, H., and Bao, J. Y.: Comparativebone healing near eroding polylactide-pol-yglycolide implants of differing crystallini-ty in rabbit tibial bone chambers. J Bio-mater Sci Polymer Edit 8 (1997) 517-32.
Winston, K., Beatty, R. M., and Fischer, E.G.: Consequences of dural defects ac-quired in infancy. J Neurosurg 59 (1983)839-46.
Wittenberg, J.M., Wittenberg, R.H., andHipp, J.A.: Biomechanical properties of re-sorbable poly-L-lactide plates and screws: acomparison with traditional systems. JOral Maxillofac Surg 49 (1991) 512-516.
Wong, L., Dufresne, C. R., Richtsmeier, J.T., and Manson, P. N.: The effect of rigid
fixation on growth of the neurocranium.Plast Reconstr Surg 88 (1991) 395-403.
Wong, L., Richtsmeier, J. T., and Manson, P.N.: Craniofacial growth following rigidfixation: suture excision, miniplating, andmicroplating. J Craniofac Surg 4 (1993)234-44; discussion 245-6.
Woodman, J. L., Jacobs, J. J., Galante, J.O., and Urban, R. M.: Metal ion releasefrom titanium-based prosthetic segmentalreplacements of long bones in baboons: along-term study. J Orthop Res 1 (1984)421-30.
Yaremchuk, M. J.: Experimental studiesaddressing rigid fixation in craniofacialsurgery. Clin Plast Surg 21 (1994) 517-24.
Yaremchuk, M. J., Fiala, T. G., Barker, F.,and Ragland, R.: The effects of rigid fixa-tion on craniofacial growth of rhesus mon-keys. Plast Reconstr Surg 93 (1994) 1-10;discussion 11-5.
Yaremchuk, M. J., and Posnick, J. C.: Re-solving controversies related to plate andscrew fixation in the growing craniofacialskeleton. J Craniofac Surg 6 (1995) 525-38.
Yu, J. C., Bartlett, S. P., Goldberg, D. S.,Gannon, F., Hunter, J., Habecker, P., andWhitaker, L. A.: An experimental study ofthe effects of craniofacial growth on thelong-term positional stability of microfixa-tion. J Craniofac Surg 7 (1996) 64-8.