Embed Size (px)
Citation preview
ESTROGEN REPLACEMENT THERAPY AND ANTIESTROGENTRATMENT IN POSTMENOPAUSAL BREAST CANCER PATIENTS– EFFECTS ON RECURRENCE, GYNECOLOGICAL ORGANS,VASCULAR ENDOTHELIUM, AND BONE
Merja Metsä-Heikkilä(formerly Marttunen)
UNIVERSITY OF HELSINKIHelsinki 2001
Merja Metsä-Heikkilä(formerly Marttunen)
Department of Obstetrics and GynecologyHelsinki University Central Hospital
University of Helsinki, Finland
ACADEMIC DISSERTATION
To be presented for public examination by permission of the Medical Facultyof the University of Helsinki, in the Auditorium of the Department of Obstetricsand Gynecology, Helsinki University Central Hospital, Haartmaninkatu 2,Helsinki, on May 23rd 2001, at 12 noon.
ESTROGEN REPLACEMENT THERAPYAND ANTIESTROGEN TREATMENT
IN POSTMENOPAUSAL BREASTCANCER PATIENTS – EFFECTS ONRECURRENCE, GYNECOLOGICAL
ORGANS, VASCULARENDOTHELIUM, AND BONE
SUPERVISED BY
Professor Olavi Ylikorkala, M.D., Ph.D.Department of Obstetrics and GynecologyHelsinki University Central HospitalUniversity of Helsinki
REVIEWED BY
Emeritus Professor Antti Kauppila, M.D., Ph.D.Department of Obstetrics and GynecologyOulu University HospitalUniversity of Oulu
Docent Guillermo Blanco, M.D., Ph.D.Department of OncologyOulu University HospitalUniversity of Oulu
OFFICIAL OPPONENT
Docent Tuula Salmi, M.D., Ph.D.Department of Obstetrics and GynecologyTurku University Central HospitalUniversity of Turku
Graphic design Hanna Metsä-Heikkilä
Multiprint OyHelsinki 2001
ISBN 952-91-3428-2ISBN 951-45-9969-1 (pdf)http://ethesis.helsinki.fi/
To my family
5CONTENTS
CONTENTS
LIST OF ORIGINAL COMMUNICATIONS 7ABBREVIATIONS 8I INTRODUCTION 9II REVIEW OF THE LITERATURE 10
1 BREAST CANCER 101.1 Incidence 101.2 Risk factors 121.3 Treatment 141.4 Prognosis and prognostic factors 15
2 ESTROGEN REPLACEMENT THERAPYIN POSTMENOPAUSAL WOMEN 17
2.1 Postmenopausal health and estrogen 172.2 Benefits of estrogen replacement therapy 182.2.1 Quality of life 182.2.2 Cardiovascular diseases 202.2.2.1 Mechanisms of vascular protection by estrogens 222.2.3 Postmenopausal bone loss 242.3 Hazards of estrogen replacement therapy 262.3.1 Breast cancer 262.3.2 Endometrial cancer 272.3.3 Venous thromboembolism 282.4 Estrogen replacement therapy in
women with previous breast cancer 29
3 TAMOXIFEN AND TOREMIFENE 323.1 Pharmacological and biological characteristics 323.2 Clinical use 333.3 Gynecological consequences 343.4 Cardiovascular organs 363.5 Bone 37
III AIMS OF THE PRESENT STUDY 38IV PATIENTS AND METHODS 39
1 PATIENTS 392 STUDY TREATMENTS 42
6 CONTENTS
3 METHODS 433.1 Clinical examinations and follow-up 433.2 Transvaginal sonography and endometrial sampling 443.3 Laboratory measurements 453.4 Bone density measurement 473.5 Statistical analyses 47
V RESULTS 48
1 ESTROGEN REPLACEMENT THERAPYIN BREAST CANCER PATIENTS 482 TAMOXIFEN AND TOREMIFENE 50
2.1 Endometrial findings 512.2 Vascular effects 532.2.1 Uterine artery resistance 532.2.2 Prostacyclin and thromboxane 532.2.3 Endothelin-1 and nitric oxide 542.3 Bone 55
VI DISCUSSION 59VII SUMMARY AND CONCLUSIONS 65ACKNOWLEDGEMENTS 67REFERENCES 69
7LIST OF ORIGINAL COMMUNICATIONS
LIST OF ORIGINALCOMMUNICATIONS
I Merja B. Marttunen, Päivi Hietanen, Seppo Pyrhönen, AilaTiitinen, Olavi Ylikorkala. A prospective study on wom-en with a history of breast cancer and with or withoutoestrogen replacement therapy. Maturitas. In press.
II Merja B. Marttunen, Bruno Cacciatore, Päivi Hietanen,Seppo Pyrhönen, Aila Tiitinen, Torsten Wahlström, OlaviYlikorkala. Prospective study on gynecological effects oftwo antiestrogens tamoxifen and toremifene in postmen-opausal women. Br J Cancer 84:897-902, 2001.
III Merja B. Marttunen, Seppo Pyrhönen, Aila Tiitinen, LasseViinikka, Olavi Ylikorkala. Effect of antiestrogen regimenon prostacyclin and thromboxane A
2 in postmenopausal
patients with breast cancer: evidence of significance ofhypertension, smoking or previous use of estrogen ther-apy. Prostaglandins 52:317-326, 1996.
IV Merja B. Marttunen, Päivi Hietanen, Aila Tiitinen, OlaviYlikorkala. Antiestrogens reduce plasma levels of endothe-lin-1 without affecting nitrate levels in breast cancer pa-tients. Gynecol Endocrinol 14:55-59, 2000.
V Merja B. Marttunen, Päivi Hietanen, Aila Tiitinen, OlaviYlikorkala. Comparison of effects of tamoxifen andtoremifene on bone biochemistry and bone mineral den-sity in postmenopausal breast cancer patients. J Clin En-docrinol Metab 83:1158-1162, 1998.
VI Merja B. Marttunen, Päivi Hietanen, Aila Tiitinen, Hans-Jürgen Roth, Lasse Viinikka, Olavi Ylikorkala. Effects oftamoxifen and toremifene on urinary excretion of pyridi-noline and deoxypyridinoline and bone density in post-menopausal patients with breast cancer. Calcif Tissue Int65:365-368, 1999.
8
ABBREVIATIONS
ANOVA analysis of varianceBMD bone mineral densityBMI body mass indexBRCA 1 and 2 breast cancer gene mutationsCA 15-3 tumor marker of breast cancerDEXA dual-energy x-ray absorptiometryDNA deoxyribonucleic acidDpyr deoxypyridinolineER estrogen receptorERA The estrogen replacement and
atherosclerosis trialERT estrogen replacement therapyERT/HRT hormone replacement therapyET-1 endothelin-1FSH follicle stimulating hormoneHDL high-density lipoprotein cholesterolHERS The heart and estrogen/progestin
replacement studyHOP hydroxyprolineHRT estrogen+progestin replacement therapyICTP carboxyterminal cross-linked telopeptideKi-67 proliferation marker of breast cancer cellsLDL low-density lipoprotein cholesterolLH luteinizing hormoneNO nitric oxideNOx nitrate+nitriteNTx aminoterminal cross-linked telopeptideOCC oral combined contraceptivesPI pulsatility indexPICP carboxyterminal propeptide of type I
procollagenPINP aminoterminal propeptide of type I
procollagenPMS premenstrual syndromePyr pyridinolineRIA radioimmuno assayRP-HPLC ion-pair reversed-phase high performance
liquid chromatographyRR relative riskSD standard deviationSE standard errorSERM selective estrogen receptor modulatorTam tamoxifenTFA trifluoroacetetic acidTor toremifeneTxA
2thromboxane A
2
TxB2
thromboxane B2
ABBREVIATIONS

9I INTRODUCTION
I INTRODUCTION
Breast cancer is the most common cancer of women in west-ern countries, and its incidence is increasing (Garfinkel et al.1994; Broeders and Verbeek 1997). Overall, 10-15% of allwomen will develop breast cancer during their lifetime(Broeders and Verbeek 1997; López-Otín and Diamandis1998). In Finland, each year are diagnosed approximately3300 new cases of breast cancer (Finnish Cancer Registry1997). Yet, in spite of the increasing incidence, the mortalityfor breast cancer has not increased during the last years.This apparent discrepancy can perhaps be explained by theearlier diagnosis (Garfinkel et al. 1994; Garne et al. 1997; UKTrial of Early Detection of Breast Cancer Group 2000), bythe appearance of less malignant forms of the disease (SEERCancer Statistics 1997), and also by the progress in treatment(Early Breast Cancer Trialists´ Collaborative Group 1992;2000).
The ethiopathogenesis of breast cancer is still unknown,but estrogen plays a major role (Mettlin 1992; Broeders andVerbeek 1997; López-Otín and Diamandis 1998). This is sup-ported for example by the fact that breast cancer occursalmost exclusively in women. Observational epidemiologi-cal studies also show increased risk of breast cancer afterthe long-term use of estrogen (ERT) or estrogen plus pro-gestin (HRT) replacement therapy (Collaborative Group onHormonal Factors in Breast Cancer 1997). Therefore ERT/HRT has not been recommended for postmenopausal wom-en with a history of breast cancer (Marchant 1994; Colditz1997; Consensus Statement 1998).
Antiestrogens are an interesting group of drugs owing bothantiestrogenic and estrogenic activity (Buckley and Goa 1989;Wiseman and Goa 1997). They are used in the treatment(Early Breast Cancer Trialists´ Collaborative Group 1998;Pyrhönen et al. 1999) and also in the prevention of breastcancer (Fisher et al. 1998). At present two antiestrogens,tamoxifen and toremifene, which are structurally relatedcompete for favor in clinical routine (Pyrhönen et al.1999).These drugs have a number of beneficial estrogenic effects(Neven et al. 1993) but on the other hand, antiestrogens donot alleviate vasomotor symptoms but may even aggravatethem (Love et al. 1991).
The present study was designed firstly to explore the use-fulness and safety of ERT/HRT in women with a history ofbreast cancer and secondly, to compare the effects oftamoxifen and toremifene on female reproductive organs,vascular endothelium, and bone.
10 1 BREAST CANCER
II REVIEW OF THE LITERATURE
1 BREAST CANCER
1.1 Incidence
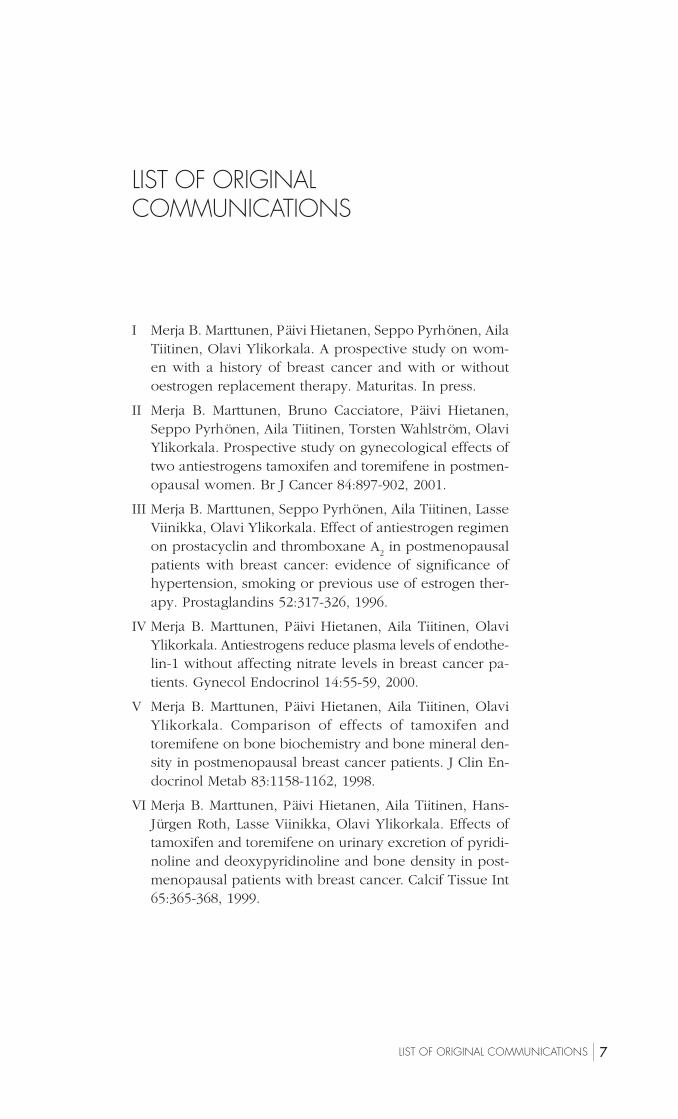
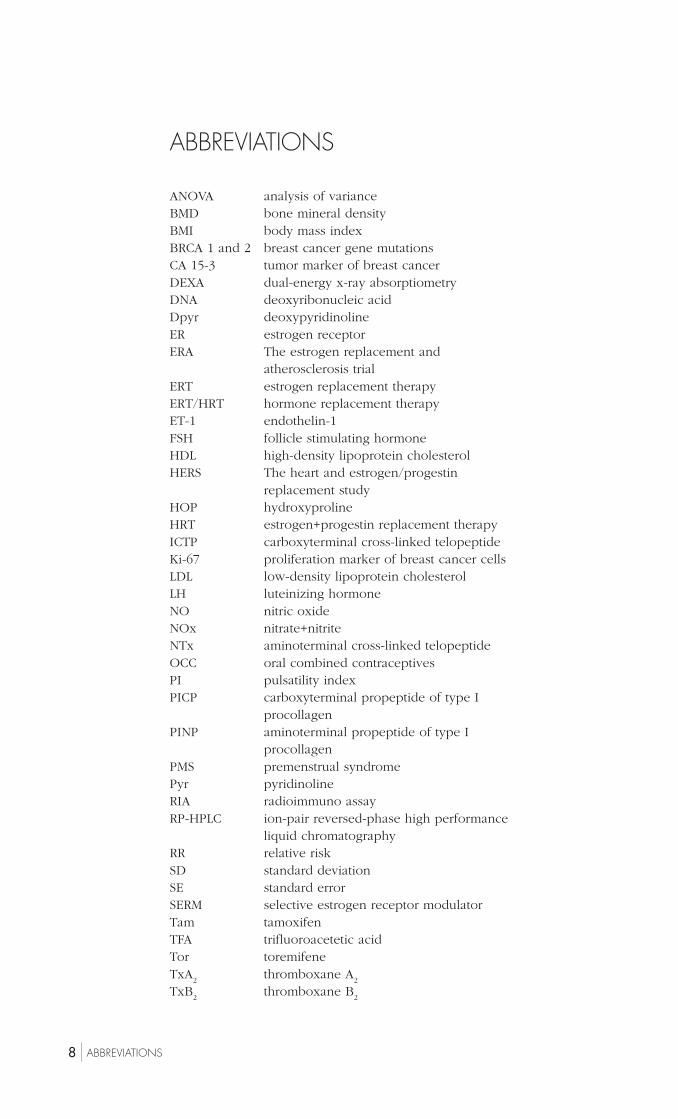
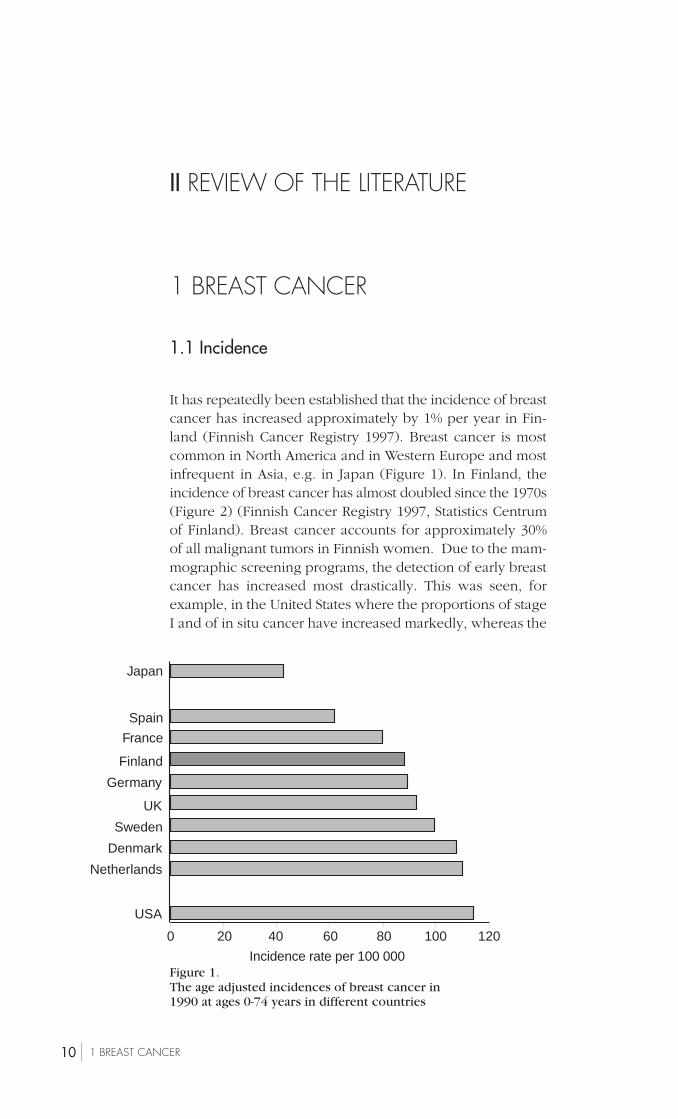
It has repeatedly been established that the incidence of breastcancer has increased approximately by 1% per year in Fin-land (Finnish Cancer Registry 1997). Breast cancer is mostcommon in North America and in Western Europe and mostinfrequent in Asia, e.g. in Japan (Figure 1). In Finland, theincidence of breast cancer has almost doubled since the 1970s(Figure 2) (Finnish Cancer Registry 1997, Statistics Centrumof Finland). Breast cancer accounts for approximately 30%of all malignant tumors in Finnish women. Due to the mam-mographic screening programs, the detection of early breastcancer has increased most drastically. This was seen, forexample, in the United States where the proportions of stageI and of in situ cancer have increased markedly, whereas the
Figure 1.The age adjusted incidences of breast cancer in1990 at ages 0-74 years in different countries
120100806040200
Incidence rate per 100 000
USA
Netherlands
Denmark
Sweden
UK
Germany
Finland
France
Spain
Japan
111 BREAST CANCER
Figure 2.The incidence of breast cancer (grey bars) and deaths (whitebars) for breast cancer in Finland (Finnish Cancer Registry,Statistics Centrum of Finland)
Figure 3.Percentual change in incidence of in situ and St I-IVbreast cancer from 1983 to 1995 in the United States
300
200
100
0
-100All In situ Stage I Stage II Stage III-IV Unknown
%
34.1%
252.2%
105.2%
-14.2% -11.2% -17.4%
80
70
60
50
40
30
20
10
0
1974 1994 1995 1996 1997
Inci
denc
e pe
r 10
0 00
0
proportions of stage II-IV breast cancer have decreased (Fig-ure 3) (SEER Cancer Statistics 1997). A similar phenomenonhas also taken place in Finland (Klemi et al.1992). This couldexplain, at least partly, why the increased incidence of thiscancer has not led to an increase in mortality, but in con-trast, the mortality rate due to breast cancer may even bedecreasing, at least in Finland (Figure 2) and also in Europe(Peto et al. 2000).

12 1 BREAST CANCER
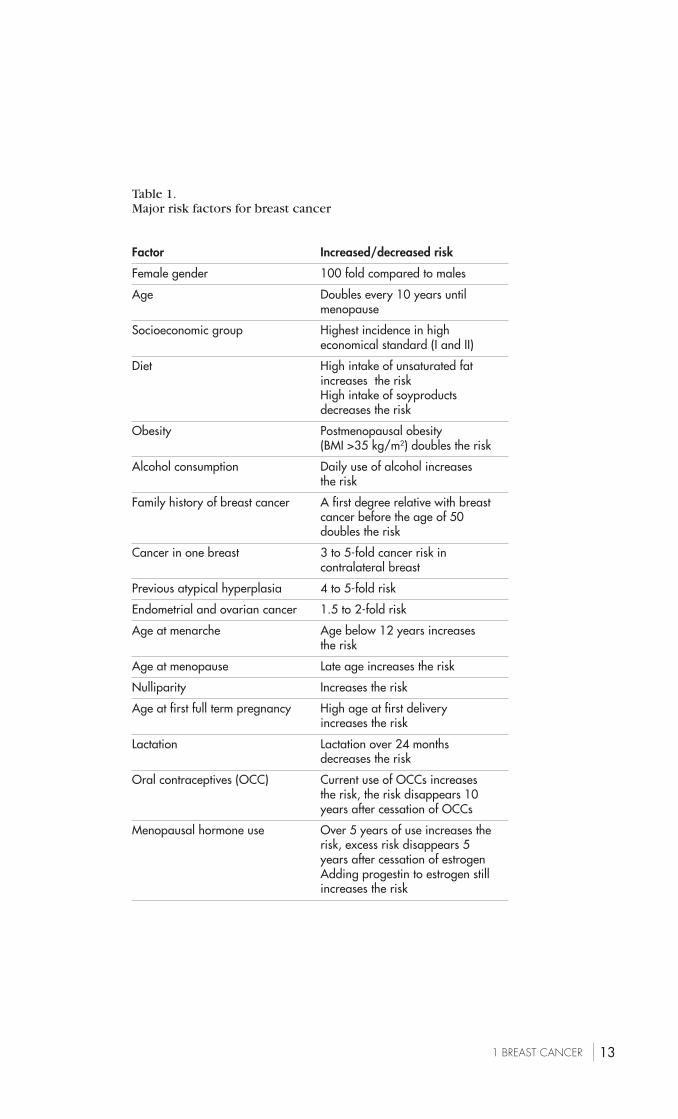
1.2 Risk factors
Although the pathogenesis of breast cancer is not under-stood, several inherent and/or clinical factors can indicatean increased risk (Table 1) (Mettlin 1992; Collaborative Groupon Hormonal Factors in Breast Cancer 1996, 1997; Broedersand Verbeek 1997; López-Otín and Diamandis 1998, Colditzand Rosner 2000). One of the well established risk factors isage because the incidence of breast cancer, as that of almostany cancer, increases with advancing age. Family history ofbreast cancer denotes a clearly increased risk, and geneticpredisposition is detectable in approximately 5-10% of allcases with breast cancer (Broeders and Verbeek 1997). Twomajor gene mutations related to breast cancer have beenidentified. BRCA1 gene is located on the long arm of chro-mosome 17 and BRCA2 on the long arm of chromosome 13(López-Otín and Diamandis 1998). Furthermore, the locusof the third candidate BRCA gene has been identified alsoon the long arm of chromosome 13 (Kainu et al. 2000).
Estrogen-related risk factors are for example female gen-der, young age at menarche, high age at menopause, andpostmenopausal obesity (Kelsey et al. 1993; Broeders andVerbeek 1997; López-Otín and Diamandis 1998). The effectof parity has been also widely studied. Women with a firstpregnancy after 35 years of age or nulliparous women havea higher risk for breast cancer, whereas an age below 21years at the first full-term pregnancy seems to protect againstbreast cancer (Kelsey et al. 1993; Pathak et al. 2000). Alsolong-term postmenopausal use of ERT/HRT has been linkedto the increased risk of breast cancer (Collaborative Groupon Hormonal Factors in Breast Cancer 1997; Colditz andRosner 2000). However, it is noteworthy that a quarter ofbreast cancer patients have none of these risk factors and allrisk factors combined could account for less than 30% of thebreast cancer incidence (Mettlin 1992).
131 BREAST CANCER
Table 1.Major risk factors for breast cancer
Factor Increased/decreased risk
Female gender 100 fold compared to males
Age Doubles every 10 years untilmenopause
Socioeconomic group Highest incidence in higheconomical standard (I and II)
Diet High intake of unsaturated fatincreases the riskHigh intake of soyproductsdecreases the risk
Obesity Postmenopausal obesity(BMI >35 kg/m2) doubles the risk
Alcohol consumption Daily use of alcohol increasesthe risk
Family history of breast cancer A first degree relative with breastcancer before the age of 50doubles the risk
Cancer in one breast 3 to 5-fold cancer risk incontralateral breast
Previous atypical hyperplasia 4 to 5-fold risk
Endometrial and ovarian cancer 1.5 to 2-fold risk
Age at menarche Age below 12 years increasesthe risk
Age at menopause Late age increases the risk
Nulliparity Increases the risk
Age at first full term pregnancy High age at first deliveryincreases the risk
Lactation Lactation over 24 monthsdecreases the risk
Oral contraceptives (OCC) Current use of OCCs increasesthe risk, the risk disappears 10years after cessation of OCCs
Menopausal hormone use Over 5 years of use increases therisk, excess risk disappears 5years after cessation of estrogenAdding progestin to estrogen stillincreases the risk

14 1 BREAST CANCER
1.3 Treatment
Surgery is the cornerstone in the treatment of breast cancer.It can be conservative (=local excision or segmental resec-tion) or radical (=mastectomy). The type of operation de-pends on the size and location of the tumor and also on thepatient´s opinion. Small (diameter below 4 cm), not central-ly located tumors are almost always suitable for breast sav-ing surgery, whereas multifocal and central lesions, as wellas large tumors usually require mastectomy. Dissection ofaxillary lymph nodes is commonly combined to surgery,because the nodal status is the most powerful prognosticfactor and guides the use of adjuvant therapy (Carter et al.1989; Hortobagyi 1998). Because the dissection of axillarylymph nodes is related to a number of postoperative seque-lae (lymphoedema, limited movements of shoulder, pain),recently has been introduced the removal of the sentinelnode to avoid the risk of later complications. The sentinelnode is most likely to drain the primary tumor, and the sta-tus of the sentinel node accurately predicts the nodal statusof the whole axilla (Krag et al. 1998).
Postoperative radiotherapy is given to reduce the risk oflocal recurrences which may occur after conservative sur-gery (Hortobagyi 1998; Early Breast Cancer Trialists´ Collab-orative group 2000). After mastectomy, radiotherapy is giv-en only to patients with T3 tumor (diameter >5 cm) or topatients with positive axillary nodes because they still havea risk of local recurrence (Early Breast Cancer Trialists´ Col-laborative Group 2000).
Postoperative adjuvant chemotherapy and/or hormonaltherapy is given if the cancer has spread to axillary nodes orif patients have other clinically relevant risk factors for can-cer recurrence (Early Breast Cancer Trialists´ CollaborativeGroup 1992; 1998). Adjuvant chemotherapy is given at threeweeks interval by using a combination of cyclophosphamideand doxorubicin (CA) or a combination of cyclophospha-mide, fluorouracil, and methotrexate or epirubicin (CMF orCEF). CMF regimen improved the 10-year survival by 7% innode-negative and by 11% in node-positive patients (EarlyBreast Cancer Trialists´ Collaborative Group 1992). Also therate of local recurrences decreased by 35% (Early BreastCancer Trialists´ Collaborative Group 1992).
Postoperative antiestrogen treatment, which has been avail-able from the seventies (Buckley and Goa 1989), is primarilygiven to postmenopausal women with estrogen and/or pro-

151 BREAST CANCER
gesterone receptor positive tumors (Early Breast Cancer Tri-alists´ Collaborative Group 1992; 1998). Tamoxifen (20-40mg/day) was the first drug to enter clinical use, and it re-duced the risk of recurrence by 21% after 1 year of use, by29% after 2 years of use, and by 47% after 5 years of use(Early Breast Cancer Trialists´ Collaborative Group 1998).Correspondingly, mortality decreased by 12%, 17%, and 26%,respectively (Early Breast Cancer Trialists´ CollaborativeGroup 1998). Tamoxifen treatment also prevented the de-velopment of cancer in the contralateral breast by 47% after5 years of use (Early Breast Cancer Trialists´ CollaborativeGroup 1998).
Toremifene, developed in the 1980´s, is an antiestrogenwhich has been clinically used since 1989. Until now it hasbeen used primarily in the treatment of advanced breast can-cer (Wiseman and Goa 1997). Toremifene at the dose of 40-60 mg has an antitumor activity comparable to that oftamoxifen at the dose of 20 mg (Homesley et al. 1993;Pyrhönen et al. 1999). The trial on toremifene as an adjuvanttreatment of breast cancer is still continuing (Holli 1998),and according to the preliminary results tamoxifen andtoremifene appear to have equal clinical efficacy (Holli et al.2000).
1.4 Prognosis and prognostic factors
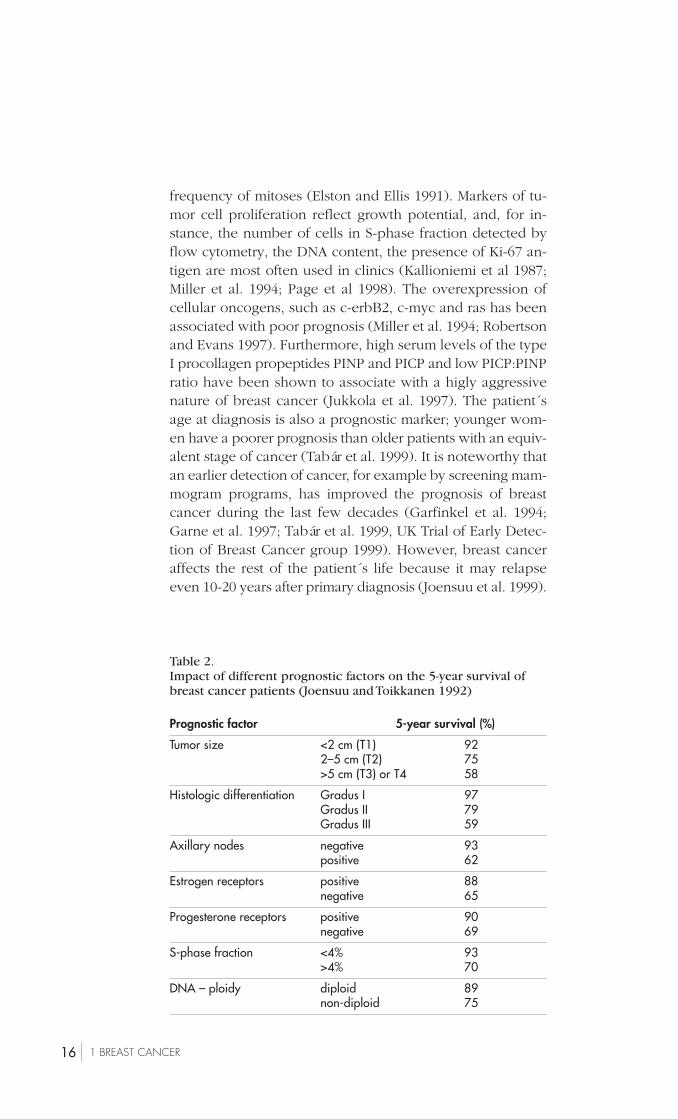
Prognosis of breast cancer depends on many different fac-tors (Table 2) (Joensuu and Toikkanen 1992). The size oftumor and its possible spread to axillary lymph nodes arethe major prognostic factors (Miller et al. 1994; Abner et al.1998; Page et al. 1998; Tabár et al. 1999). Patients in whomcancer has spread beyond the axillary nodes have a muchworse survival rate than patients whose tumor is limited tothe breast (Carter et al. 1989; Page et al 1998). Biologicalfactors, such as the estrogen and progesterone receptor sta-tus, histological grading, and proliferation markers, predictsthe behavior of the tumor and helps in choosing suitabletreatments for individual patients (Alanko et al. 1984; Blancoet al. 1984; Elston and Ellis 1991; Miller et al. 1994; Page etal. 1998). Histological grading on the scale from I to III isbased on glandular formation, nuclear pleomorphism, and
16 1 BREAST CANCER
frequency of mitoses (Elston and Ellis 1991). Markers of tu-mor cell proliferation reflect growth potential, and, for in-stance, the number of cells in S-phase fraction detected byflow cytometry, the DNA content, the presence of Ki-67 an-tigen are most often used in clinics (Kallioniemi et al 1987;Miller et al. 1994; Page et al 1998). The overexpression ofcellular oncogens, such as c-erbB2, c-myc and ras has beenassociated with poor prognosis (Miller et al. 1994; Robertsonand Evans 1997). Furthermore, high serum levels of the typeI procollagen propeptides PINP and PICP and low PICP:PINPratio have been shown to associate with a higly aggressivenature of breast cancer (Jukkola et al. 1997). The patient´sage at diagnosis is also a prognostic marker; younger wom-en have a poorer prognosis than older patients with an equiv-alent stage of cancer (Tabár et al. 1999). It is noteworthy thatan earlier detection of cancer, for example by screening mam-mogram programs, has improved the prognosis of breastcancer during the last few decades (Garfinkel et al. 1994;Garne et al. 1997; Tabár et al. 1999, UK Trial of Early Detec-tion of Breast Cancer group 1999). However, breast canceraffects the rest of the patient´s life because it may relapseeven 10-20 years after primary diagnosis (Joensuu et al. 1999).
Table 2.Impact of different prognostic factors on the 5-year survival ofbreast cancer patients (Joensuu and Toikkanen 1992)
Prognostic factor 5-year survival (%)
Tumor size <2 cm (T1) 922–5 cm (T2) 75>5 cm (T3) or T4 58
Histologic differentiation Gradus I 97Gradus II 79Gradus III 59
Axillary nodes negative 93positive 62
Estrogen receptors positive 88negative 65
Progesterone receptors positive 90negative 69
S-phase fraction <4% 93>4% 70
DNA – ploidy diploid 89non-diploid 75
172 ESTROGEN REPLACEMENT THERAPY IN POSTMENOPAUSAL WOMEN
2 ESTROGEN REPLACEMENTTHERAPY IN POSTMENOPAUSALWOMEN
2.1 Postmenopausal health and estrogen
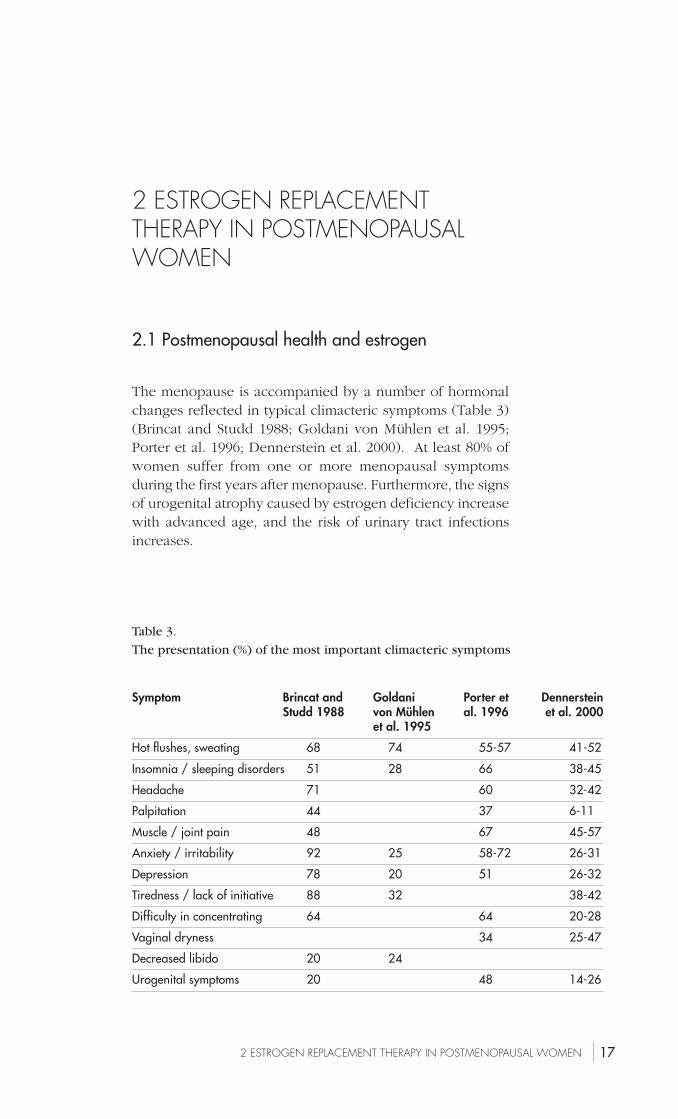
The menopause is accompanied by a number of hormonalchanges reflected in typical climacteric symptoms (Table 3)(Brincat and Studd 1988; Goldani von Mühlen et al. 1995;Porter et al. 1996; Dennerstein et al. 2000). At least 80% ofwomen suffer from one or more menopausal symptomsduring the first years after menopause. Furthermore, the signsof urogenital atrophy caused by estrogen deficiency increasewith advanced age, and the risk of urinary tract infectionsincreases.
Table 3.
The presentation (%) of the most important climacteric symptoms
Symptom Brincat and Goldani Porter et DennersteinStudd 1988 von Mühlen al. 1996 et al. 2000
et al. 1995
Hot flushes, sweating 68 74 55-57 41-52
Insomnia / sleeping disorders 51 28 66 38-45
Headache 71 60 32-42
Palpitation 44 37 6-11
Muscle / joint pain 48 67 45-57
Anxiety / irritability 92 25 58-72 26-31
Depression 78 20 51 26-32
Tiredness / lack of initiative 88 32 38-42
Difficulty in concentrating 64 64 20-28
Vaginal dryness 34 25-47
Decreased libido 20 24
Urogenital symptoms 20 48 14-26

18 2 ESTROGEN REPLACEMENT THERAPY IN POSTMENOPAUSAL WOMEN
Postmenopausal hypoestrogenism affects also the cardio-vascular system. The risk of cardiovascular diseases increas-es after menopause, and women tend to reach the incidencein that of men (Sullivan and Fowlkes 1996). Indeed, a half ofthe women in the western world will get coronary arterydisease and one-third will die from it (Grady et al. 1992).Therefore, it is understandable that the prevention of cardi-ovascular disease has been, and still is, one of the prioritiesin public health programs.
The peak bone mass, which is reached normally at 25-30years of age, is 30-50% lower in women than in men (Chris-tiansen 1995). Neverthless, bone is affected by estrogen. Thisis supported by the finding that estrogen receptors are presentin osteoblasts and osteoclasts, the cells responsible for boneformation and bone resorption, respectively (Oursler et al.1993). In menopause, estrogen deficiency leads to increasedosteoclast formation and activity, and thereby it enhancesbone resorption both in trabecular and cortical bone (Rood-man 1996). This may lead to osteoporosis if a woman liveslong enough (Marcus 1996). The World Health Organisationhas defined osteoporosis as a bone mineral density (BMD),measured by dual-energy x-ray absorptiometry, which is 2.5standard deviation (SD) or more below the mean peak valuein young adults. Immediately after menopause, bone massdecreases by 1-5% per year, and even after the age of 65, thedecrease is 0.5-1% per year (Riis 1996). It has been estimat-ed that 21% of postmenopausal women in the western coun-tries will eventually develop osteoporosis (Looker et al. 1995).Postmenopausal women have a 15% lifetime probability ofsuffering a hip fracture and a 1.5% probability of dying fromit (Grady et al. 1992). Also the risk of vertebral fracturesincreases, and although these fractures are not associatedwith increased mortality, they may cause significant morbid-ity (Lindsay et al. 1980; Grady et al. 1992). Thus, the preven-tion of osteoporosis is one of the major challenges in thehealth care system in western countries.
2.2 Benefits of estrogen replacement therapy
2.2.1 Quality of life
Menopausal symptoms, such as hot flushes, insomnia, de-pressive mood and tiredness, are the most common causesfor the initiation of ERT/HRT in clinical routine. Estrogen
192 ESTROGEN REPLACEMENT THERAPY IN POSTMENOPAUSAL WOMEN
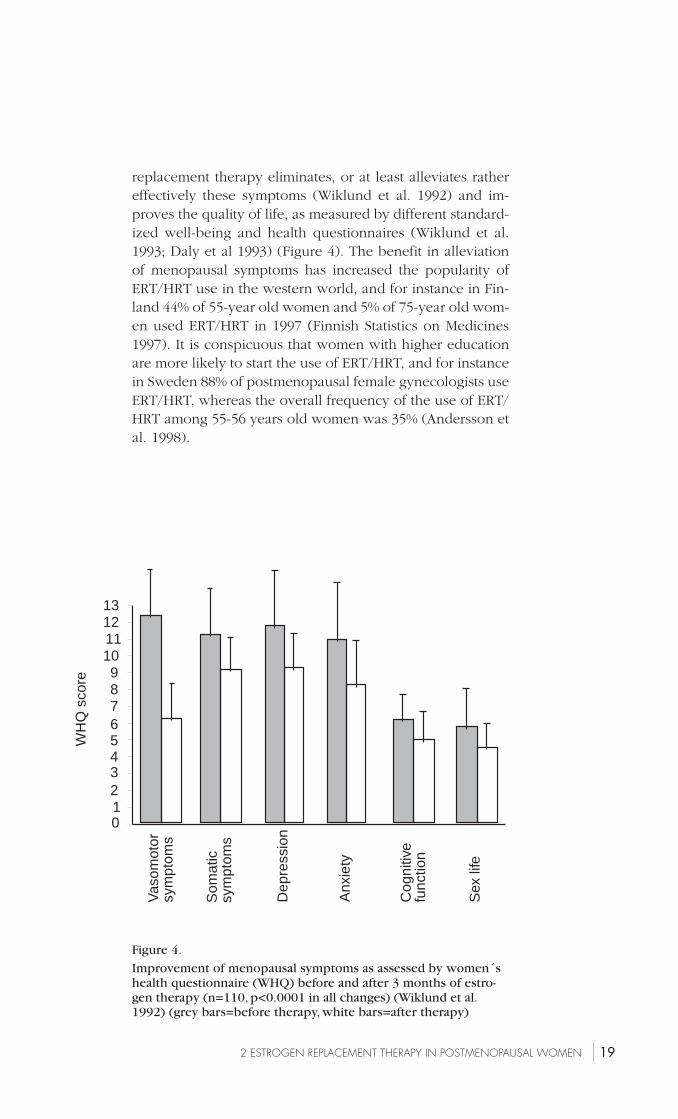
Figure 4.
Improvement of menopausal symptoms as assessed by women´shealth questionnaire (WHQ) before and after 3 months of estro-gen therapy (n=110, p<0.0001 in all changes) (Wiklund et al.1992) (grey bars=before therapy, white bars=after therapy)
131211109876543210
WH
Q s
core
Vas
omot
orsy
mpt
oms
Som
atic
sym
ptom
s
Dep
ress
ion
Anx
iety
Cog
nitiv
efu
nctio
n
Sex
life
replacement therapy eliminates, or at least alleviates rathereffectively these symptoms (Wiklund et al. 1992) and im-proves the quality of life, as measured by different standard-ized well-being and health questionnaires (Wiklund et al.1993; Daly et al 1993) (Figure 4). The benefit in alleviationof menopausal symptoms has increased the popularity ofERT/HRT use in the western world, and for instance in Fin-land 44% of 55-year old women and 5% of 75-year old wom-en used ERT/HRT in 1997 (Finnish Statistics on Medicines1997). It is conspicuous that women with higher educationare more likely to start the use of ERT/HRT, and for instancein Sweden 88% of postmenopausal female gynecologists useERT/HRT, whereas the overall frequency of the use of ERT/HRT among 55-56 years old women was 35% (Andersson etal. 1998).
20 2 ESTROGEN REPLACEMENT THERAPY IN POSTMENOPAUSAL WOMEN
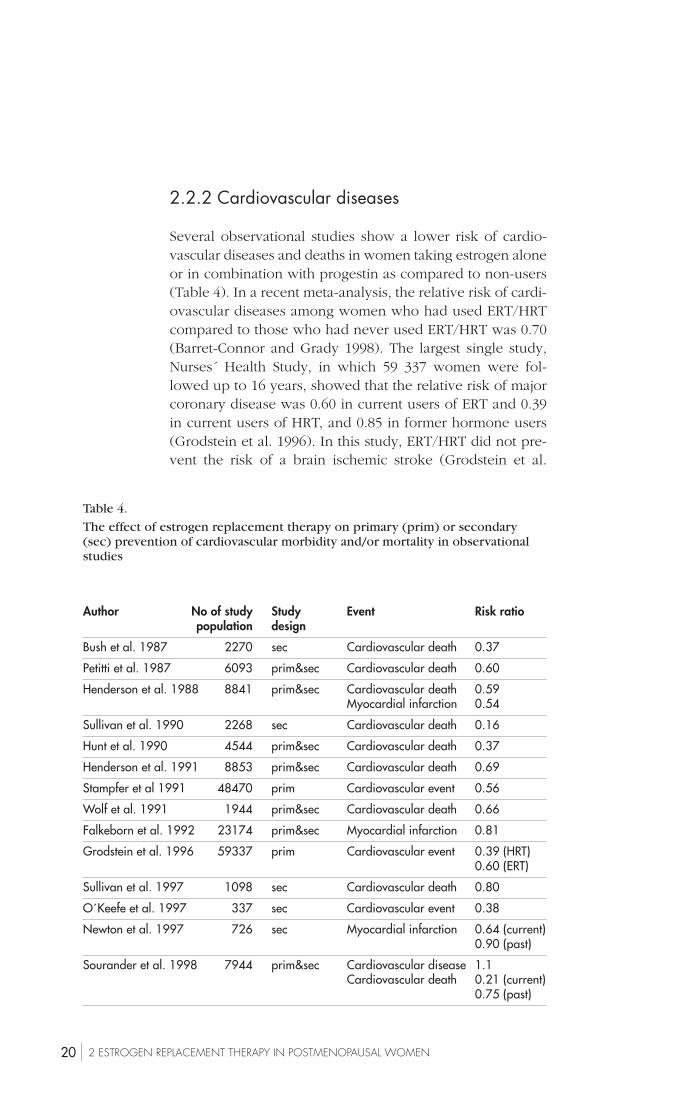
Table 4.
The effect of estrogen replacement therapy on primary (prim) or secondary(sec) prevention of cardiovascular morbidity and/or mortality in observationalstudies
Author No of study Study Event Risk ratiopopulation design
Bush et al. 1987 2270 sec Cardiovascular death 0.37
Petitti et al. 1987 6093 prim&sec Cardiovascular death 0.60
Henderson et al. 1988 8841 prim&sec Cardiovascular death 0.59Myocardial infarction 0.54
Sullivan et al. 1990 2268 sec Cardiovascular death 0.16
Hunt et al. 1990 4544 prim&sec Cardiovascular death 0.37
Henderson et al. 1991 8853 prim&sec Cardiovascular death 0.69
Stampfer et al 1991 48470 prim Cardiovascular event 0.56
Wolf et al. 1991 1944 prim&sec Cardiovascular death 0.66
Falkeborn et al. 1992 23174 prim&sec Myocardial infarction 0.81
Grodstein et al. 1996 59337 prim Cardiovascular event 0.39 (HRT)0.60 (ERT)
Sullivan et al. 1997 1098 sec Cardiovascular death 0.80
O´Keefe et al. 1997 337 sec Cardiovascular event 0.38
Newton et al. 1997 726 sec Myocardial infarction 0.64 (current)0.90 (past)
Sourander et al. 1998 7944 prim&sec Cardiovascular disease 1.1Cardiovascular death 0.21 (current)
0.75 (past)
2.2.2 Cardiovascular diseases
Several observational studies show a lower risk of cardio-vascular diseases and deaths in women taking estrogen aloneor in combination with progestin as compared to non-users(Table 4). In a recent meta-analysis, the relative risk of cardi-ovascular diseases among women who had used ERT/HRTcompared to those who had never used ERT/HRT was 0.70(Barret-Connor and Grady 1998). The largest single study,Nurses´ Health Study, in which 59 337 women were fol-lowed up to 16 years, showed that the relative risk of majorcoronary disease was 0.60 in current users of ERT and 0.39in current users of HRT, and 0.85 in former hormone users(Grodstein et al. 1996). In this study, ERT/HRT did not pre-vent the risk of a brain ischemic stroke (Grodstein et al.

212 ESTROGEN REPLACEMENT THERAPY IN POSTMENOPAUSAL WOMEN
1996). However, all these observational studies have beencriticized because healthier women may have been moreprone to start ERT/HRT (“selection bias”): the ERT users havehad fewer cardiovascular risk factors, such as hypertension,hypercholesterolemia, or obesity before the start of ERT/HRT (Matthews et al.1996; Rödström et al. 1999).
The clinical data on the cardiovascular benefits of ERT/HRT in women with ischemic heart disease (“secondary pre-vention”) are controversial. Previous observational studieshave shown decreased risk of recurrent cardiovascular eventsin estrogen users (Bush et al 1987; Sullivan et al. 1990; Hend-erson et al. 1991; Sullivan et al. 1997; O´Keefe et al. 1997;Newton et al. 1997) but the only randomized, placebo-con-trolled trial (HERS study) failed to show any benefit at leastin older (an average of 67 years) women (Hulley et al. 1998).In this study, placebo or 0.625 mg of conjugated equineestrogen in combination with 2.5 mg of medroxyprogester-one acetate were given continuously to 2763 women for anaverage of 4.1 years (Hulley et al. 1998). During the firstyear of use, the risk of cardiac recurrence was increased (RR1.52) in hormone users, whereas in 3-5 years, a clear trend(RR 0.87-0.67) for the favor of HRT was seen (Hulley et al.1998). In another study, the effect of ERT/HRT on the pro-gression of coronary atherosclerosis was studied in a rand-omized, placebo-controlled setting (ERA trial) (Herringtonet al. 2000). In 309 women with angiographically verifiedcoronary disease, conjugated estrogen with or without pro-gestin, did not prevent the progression of coronary occlu-sion during a mean of 3.2 years follow-up, even if ERT/HRThad favorable effects on LDL and HDL cholesterol levels(Herrington et al. 2000).
In future, the benefit of estrogen in the primary preven-tion of cardiovascular diseases should be ascertained by ran-domized, placebo-controlled studies, and some studies arepresently conducted (The Women´s Health Initiative StudyGroup 1998). Before these results are available there is nodefinite truth about the role of ERT/HRT in the primary pre-vention of coronary heart disease. Yet, it can be questionedwhether truly randomized and placebo-controlled trials inmenopausal research are possible (Ylikorkala 2000).

22 2 ESTROGEN REPLACEMENT THERAPY IN POSTMENOPAUSAL WOMEN
2.2.2.1 Mechanisms of vascular protection byestrogens
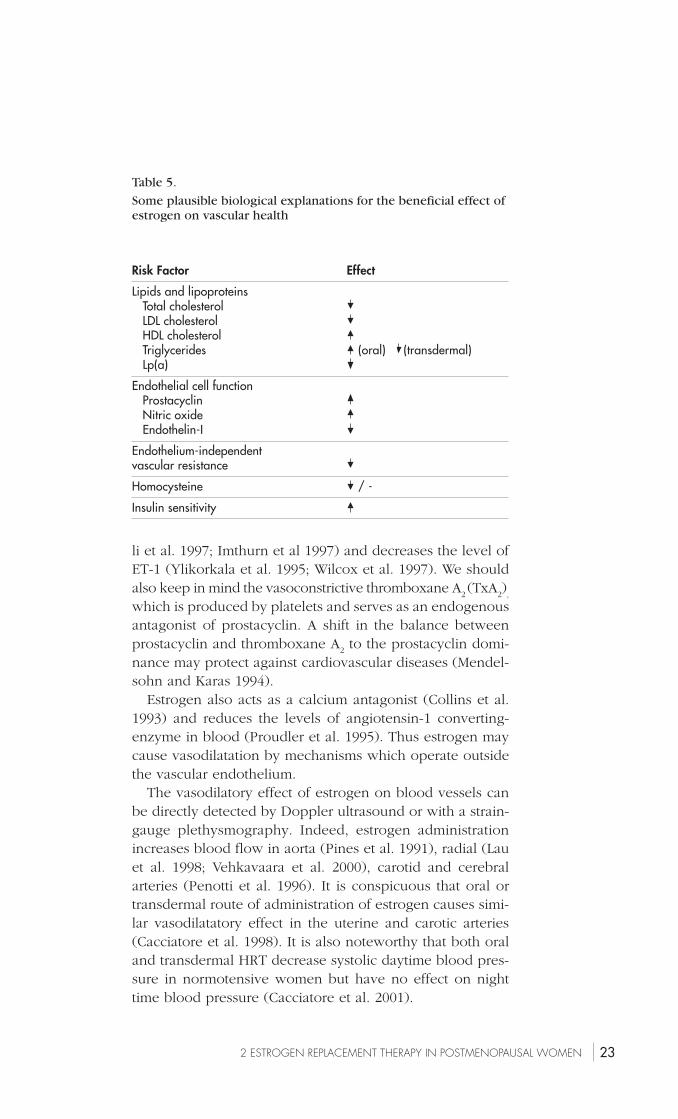
Estrogen has several favorable vascular effects, which mayexplain its cardiovascular protective efficacy (Table 5). It hasbeen estimated that the favorable effect of estrogen on plas-ma lipids can explain approximately 20-30% of cardiovascu-lar benefits of ERT/HRT (Wild 1996; Tikkanen 1999). Be-sides high lipid levels, also high plasma homocysteine levelsmay indicate a risk of atherosclerosis (Welch and Loscalzo1998). In a Dutch study, estrogen has been shown to de-crease these levels especially when the baseline levels werehigh (Mijatovic et al. 1998), whereas this was not seen inFinnish women with normal baseline homocysteine levels(Eviö et al. 2000). Estrogen has also a favorable effect onglucose metabolism by enhancing tissue insulin sensitivity(Barrett-Connor and Laakso 1990; Lindheim et al. 1994; Rau-daskoski et al. 1999). It is likely that these biochemical find-ings may require a more prolonged use of ERT before theybecome clinically apparent.
Estrogen has also the direct and immediate effects on thevascular wall. This was first supported by the data whichshowed that estrogen binds to the estrogen receptors of vas-cular endothelial and smooth muscle cells (Mendelsohn andKaras 1999). Endothelial cells produce a number of agentswith vasodilatory or vasoconstricive activity. One of the beststudied agents is vasodilatory prostacyclin, which is an im-portant mediator in several occlusive and hypertensive dis-orders (Ylikorkala et al. 1986; Cinotti and Pugliese 1989; Vaneet al. 1990). It is stimulated by estrogen, at least in culturedendothelial cells (Mikkola et al. 1995). Endothelial cells alsosecrete free radical gas, nitric oxide (NO), which causes va-sodilatation and inhibits platelet aggregation (Moncada et al.1991). Nitric oxide production is diminished in conditionscharacterized by endothelial damage, such as atherosclero-sis, hypertension, or diabetes (Moncada et al. 1991). Endothe-lin-1 (ET-1) is a peptide hormone which is also produced byendothelial and smooth muscle cells (Masaki 1993). Endothe-lin-1 is the most potent vasoconstrictor yet discovered (Ma-saki 1993), and indeed, elevated plasma ET-1 levels havebeen detected in several vasoconstrictive diseases, such asin myocardial infarction, pulmonary hypertension, and athero-sclerosis (Masaki 1993). Estrogen administration in postmen-opausal women increases the circulating levels of NO (Cicinel-
232 ESTROGEN REPLACEMENT THERAPY IN POSTMENOPAUSAL WOMEN
Table 5.
Some plausible biological explanations for the beneficial effect ofestrogen on vascular health
Risk Factor Effect
Lipids and lipoproteins Total cholesterol LDL cholesterol HDL cholesterol Triglycerides (oral) (transdermal) Lp(a)
Endothelial cell function Prostacyclin Nitric oxide Endothelin-I
Endothelium-independentvascular resistance
Homocysteine / -
Insulin sensitivity
li et al. 1997; Imthurn et al 1997) and decreases the level ofET-1 (Ylikorkala et al. 1995; Wilcox et al. 1997). We shouldalso keep in mind the vasoconstrictive thromboxane A
2 (TxA
2),
which is produced by platelets and serves as an endogenousantagonist of prostacyclin. A shift in the balance betweenprostacyclin and thromboxane A
2 to the prostacyclin domi-
nance may protect against cardiovascular diseases (Mendel-sohn and Karas 1994).
Estrogen also acts as a calcium antagonist (Collins et al.1993) and reduces the levels of angiotensin-1 converting-enzyme in blood (Proudler et al. 1995). Thus estrogen maycause vasodilatation by mechanisms which operate outsidethe vascular endothelium.
The vasodilatory effect of estrogen on blood vessels canbe directly detected by Doppler ultrasound or with a strain-gauge plethysmography. Indeed, estrogen administrationincreases blood flow in aorta (Pines et al. 1991), radial (Lauet al. 1998; Vehkavaara et al. 2000), carotid and cerebralarteries (Penotti et al. 1996). It is conspicuous that oral ortransdermal route of administration of estrogen causes simi-lar vasodilatatory effect in the uterine and carotic arteries(Cacciatore et al. 1998). It is also noteworthy that both oraland transdermal HRT decrease systolic daytime blood pres-sure in normotensive women but have no effect on nighttime blood pressure (Cacciatore et al. 2001).
24 2 ESTROGEN REPLACEMENT THERAPY IN POSTMENOPAUSAL WOMEN
The biology of vascular endothelium is a complex entityand presently a target for hectic research. In the above Ihave very briefly outlined a few aspects of endothelial re-search, which have been most clearly linked to the use ofERT/HRT. For those readers who wish to learn more aboutvascular endothelial physiology and cardiovascular diseas-es, I refer to two current reviews (Vogel 1997; Lind et al.2000).
2.2.3 Postmenopausal bone loss
Estrogen replacement therapy reduces the rate of bone lossmainly by decreasing bone resorption (Turner et al. 1994).In this regard, daily oral doses of 2 mg of estradiol or 0.626mg of conjugated estrogens daily seem to be equally effec-tive as daily 50 µg of estradiol from a patch or 1.5 mg estra-diol from a gel (Compston 1997). Recent studies indicatethat also smaller doses of estrogen may protect bone (Weisset al. 1999). Progestin added to ERT has been shown topotentiate the protective effect of estrogen on bone in some(The Writing Group for the PEPI Trial 1996), but not in allstudies (Adachi et al. 1997). Data from observational studiesshow that ERT decreases the risk of hip fracture by at least25% (Grady et al. 1992) and vertebral fractures by 50% to80% (Lindsay et al. 1980; Maxim et al. 1995). In a large pop-ulation-based case-controlled study the odds ratio for hipfracture was 0.35 in current users and 0.76 in past users(Michaëlsson et al. 1998). Furthermore, the bone protectiveeffect of ERT increases with the duration of use (Moore et al.1990; Grady et al. 1992), and the initiation of estrogen in latemenopause also reduces the risk of hip fracture (Lindsayand Tohme 1990).
The generally accepted method for bone mineral density(BMD) measurement is dual-energy x-ray absorptiometry(DEXA), and The World Health Organisation criteria for os-teoporosis are based on this method. However, in order todetect the rate of bone turnover and to identify patients withincreased bone loss, serial DEXA measurements are neededat one or two-year intervals. This calls for a need for mark-ers that show changes in the rate of bone turnover within afew months. It has also been shown that high bone turnoveris an independent predictor of increased fracture risk (Milleret al. 1999; Looker et al. 2000). Presently, there is a general
252 ESTROGEN REPLACEMENT THERAPY IN POSTMENOPAUSAL WOMEN
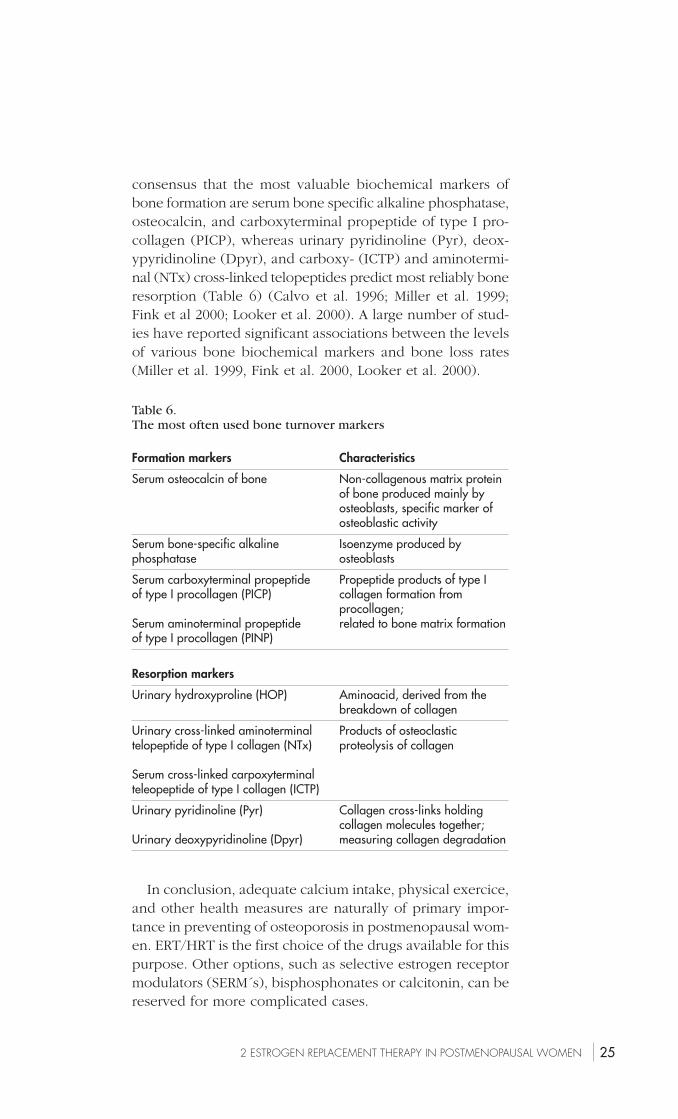
Table 6.The most often used bone turnover markers
Formation markers Characteristics
Serum osteocalcin of bone Non-collagenous matrix proteinof bone produced mainly byosteoblasts, specific marker ofosteoblastic activity
Serum bone-specific alkaline Isoenzyme produced byphosphatase osteoblasts
Serum carboxyterminal propeptide Propeptide products of type Iof type I procollagen (PICP) collagen formation from
procollagen;Serum aminoterminal propeptide related to bone matrix formationof type I procollagen (PINP)
Resorption markers
Urinary hydroxyproline (HOP) Aminoacid, derived from thebreakdown of collagen
Urinary cross-linked aminoterminal Products of osteoclastictelopeptide of type I collagen (NTx) proteolysis of collagen
Serum cross-linked carpoxyterminalteleopeptide of type I collagen (ICTP)
Urinary pyridinoline (Pyr) Collagen cross-links holdingcollagen molecules together;
Urinary deoxypyridinoline (Dpyr) measuring collagen degradation
consensus that the most valuable biochemical markers ofbone formation are serum bone specific alkaline phosphatase,osteocalcin, and carboxyterminal propeptide of type I pro-collagen (PICP), whereas urinary pyridinoline (Pyr), deox-ypyridinoline (Dpyr), and carboxy- (ICTP) and aminotermi-nal (NTx) cross-linked telopeptides predict most reliably boneresorption (Table 6) (Calvo et al. 1996; Miller et al. 1999;Fink et al 2000; Looker et al. 2000). A large number of stud-ies have reported significant associations between the levelsof various bone biochemical markers and bone loss rates(Miller et al. 1999, Fink et al. 2000, Looker et al. 2000).
In conclusion, adequate calcium intake, physical exercice,and other health measures are naturally of primary impor-tance in preventing of osteoporosis in postmenopausal wom-en. ERT/HRT is the first choice of the drugs available for thispurpose. Other options, such as selective estrogen receptormodulators (SERM´s), bisphosphonates or calcitonin, can bereserved for more complicated cases.
26 2 ESTROGEN REPLACEMENT THERAPY IN POSTMENOPAUSAL WOMEN
2.3 Hazards of estrogen replacement therapy
2.3.1 Breast cancer
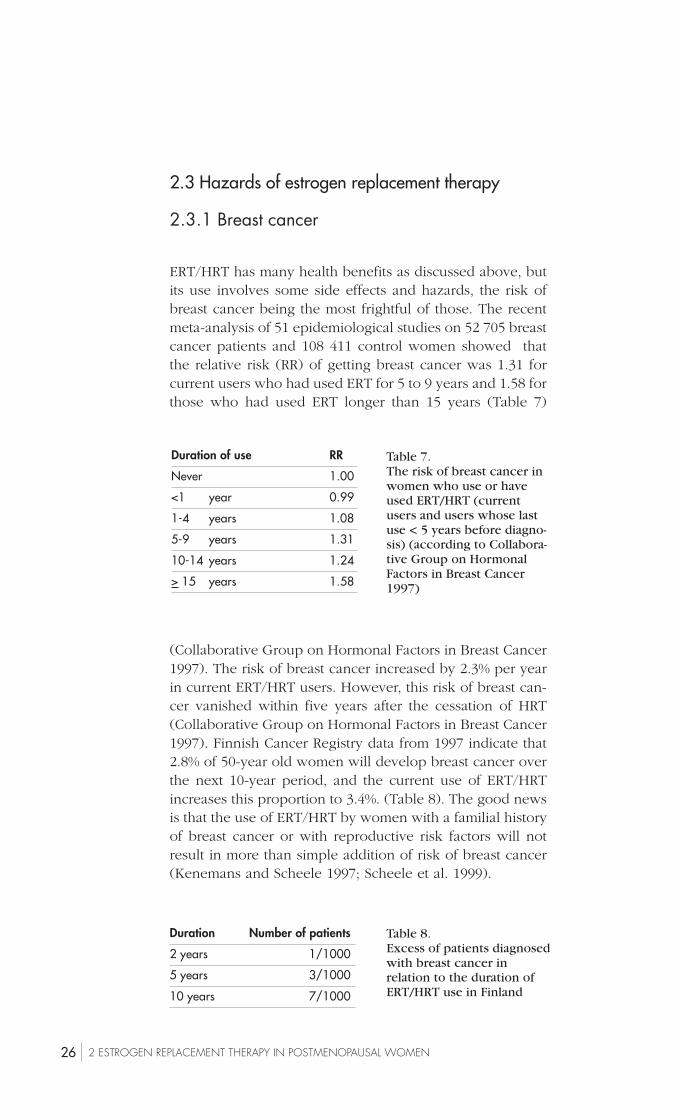
ERT/HRT has many health benefits as discussed above, butits use involves some side effects and hazards, the risk ofbreast cancer being the most frightful of those. The recentmeta-analysis of 51 epidemiological studies on 52 705 breastcancer patients and 108 411 control women showed thatthe relative risk (RR) of getting breast cancer was 1.31 forcurrent users who had used ERT for 5 to 9 years and 1.58 forthose who had used ERT longer than 15 years (Table 7)
(Collaborative Group on Hormonal Factors in Breast Cancer1997). The risk of breast cancer increased by 2.3% per yearin current ERT/HRT users. However, this risk of breast can-cer vanished within five years after the cessation of HRT(Collaborative Group on Hormonal Factors in Breast Cancer1997). Finnish Cancer Registry data from 1997 indicate that2.8% of 50-year old women will develop breast cancer overthe next 10-year period, and the current use of ERT/HRTincreases this proportion to 3.4%. (Table 8). The good newsis that the use of ERT/HRT by women with a familial historyof breast cancer or with reproductive risk factors will notresult in more than simple addition of risk of breast cancer(Kenemans and Scheele 1997; Scheele et al. 1999).
Duration of use RR
Never 1.00
<1 year 0.99
1-4 years 1.08
5-9 years 1.31
10-14 years 1.24
> 15 years 1.58
Table 7.The risk of breast cancer inwomen who use or haveused ERT/HRT (currentusers and users whose lastuse < 5 years before diagno-sis) (according to Collabora-tive Group on HormonalFactors in Breast Cancer1997)
Duration Number of patients
2 years 1/1000
5 years 3/1000
10 years 7/1000
Table 8.Excess of patients diagnosedwith breast cancer inrelation to the duration ofERT/HRT use in Finland

272 ESTROGEN REPLACEMENT THERAPY IN POSTMENOPAUSAL WOMEN
The mechanisms by which estrogen increases the risk ofbreast cancer are not known (Theriault 1996). Moreover, theimpact of the progestin component of HRT on the breastcancer risk is not clear. Previous data demonstrated that pro-gestin did not affect the risk of breast cancer caused by es-trogen only (Collaborative Group on Hormonal Factors inBreast Cancer 1997), but recent data from Sweden and theUnited States showed that progestin increased this risk by14-40% (Persson et al. 1999; Schairer et al. 2000; Ross et al.2000; Colditz and Rosner 2000).
In interpreting the data on the risk of breast cancer inhormone users, we must keep in mind that there are noplacebo controlled, randomized trials on this topic. Thus allthe epidemiological data discussed above are prone to anumber of confounding factors and biases. First, high socio-economic status is an independent risk factor of breast can-cer (McPherson et al. 1994), and women belonging to thisgroup more likely use ERT/HRT (Matthews et al. 1996; Röd-ström et al. 1999). Second, ERT/HRT users undergo breastexaminations and mammography more frequently than non-users. This can lead to detection bias; ERT/HRT users aremore likely to be diagnosed with breast cancer than non-users. The use of estrogen may also favor the developmentof cancers with less malignant potential (Gapstur et al. 1999),which might explain the better prognosis of breast cancer inpatients with ERT/HRT use than in those without ERT/HRTuse (Jernström et al. 1999).
2.3.2 Endometrial cancer
Endometrial cancer is the third commonest cancer in wom-en in Finland; its incidence was 14.3 in 100 000 women in1997 (Finnish Cancer Registry 1997). Endogen and exogenestrogen exposure is one of the risk factors of endometrialcancer (Franceschi 1989, Grady et al. 1995). Estrogen pro-motes the formation of estrogen receptors and proliferationof endometrium whereas progesterone down-regulates thesereceptors and causes secretory changes. This explains whyestrogen without the use of progestin leads to an increase inthe risk of endometrial hyperplasia (Kurman et al. 1985).This can progress to endometrial cancer, albeit only in aminor part of patients (Grady et al. 1995, Westhoff et al.2000).
28 2 ESTROGEN REPLACEMENT THERAPY IN POSTMENOPAUSAL WOMEN
The meta-analysis of 29 epidemiological studies showed a2.3-fold increase in the risk of endometrial cancer during theuse of unopposed estrogen (Grady et al. 1995). This riskwas higher with a prolonged duration of estrogen use. Lessthan one year of use caused a 1.4-fold risk, whereas morethan 10 years of use increased the risk to 9.5-fold. Therefore,progestin has to be added to ERT in non-hysterectomizedwomen. Progestin can be administered sequentially or con-tinuously. The sequential addition of progestin has to belong enough; an addition of 10 days or more per monthresulted in a RR of 0.9 of endometrial cancer (Voigt et al.1991) and the interval between progestin phases should beshort enough (Pukkala et al 2001). Thus, in regard to en-dometrial cancer, estrogen replacement therapy can be safe-ly used if progestin is added concomintantly.
2.3.3 Venous thromboembolism
The balance between coagulation and fibrinolysis systemdetermines the risk of thrombosis in a given individual. Theeffect of estrogen on this balance is complex. Although ERT/HRT causes a reduction in the concentration of fibrinogen inplasma and activates fibrinolysis (Gebara et al. 1995; Conradet al. 1997), it increases the risk of venous thromboembo-lism (Daly et al. 1996, Jick et al. 1996, Grodstein et al. 1996,Pérez Gutthnn et al. 1997, Hulley et al. 1998, Varas-Lorenzoet al. 1998). This risk appears to be most pronounced duringthe first months of use, and there is no clear dose-depend-ence of ERT/HRT in this regard (Oger and Scarabin 1999).Moreover, progestin addition does not modify this risk (Ogerand Scarabin 1999), finding which was confirmed also in theHERS study. The risk of venous thromboembolism was 2.3in 1000 woman-years in a placebo group and 6.2 in 1000woman-years in a hormone treated group (Grady et al. 2000).Fractures of the hip or other parts of the lower extremitycausing immobilisation, the presence of cancer, and hospi-talization increased this risk whereas intake of aspirin orlipid lowering statins decreased it (Grady et al. 2000). Anti-estrogens, such as tamoxifen and raloxifene, have also in-creased the risk of thromboembolism from 2 to 5-fold inrandomized trials (Fisher et al. 1998, Cummings et al. 1999),and in this regard antiestrogens behave similarly to ERT.

292 ESTROGEN REPLACEMENT THERAPY IN POSTMENOPAUSAL WOMEN
Furthermore, in the study comparing tamoxifen andtoremifene, the incidence of thromboembolic events wasslightly more common in the tamoxifen group (5.9%) thanin the toremifene group (3.5%), but the difference was notsignificant (Holli et al. 2000). However, the absolute numberof thromboembolic events in these studies remains low (inthe order of 5 in 1000 women per year), and they are onlyseldom fatal. Therefore the risk of thromboembolism is nota serious concern during the use of ERT/HRT.
2.4 Estrogen replacement therapy in womenwith previous breast cancer
Due to the increased incidence and better prognosis of breastcancer, the number of breast cancer survivors has substan-tially increased in all western countries during the last twodecades (Garfinkel et al. 1994). The general consensus hasbeen that these patients should not use ERT/HRT, becausetheoretically such use can increase the risk of recurrence(Marchant 1994; Colditz 1997; Consensus Statement 1998).However, also these women can suffer from invalidatingmenopausal symptoms and certainly become exposed to sim-ilar postmenopausal health consequences related to estro-gen deprivation as healthy postmenopausal women. There-fore, it there is justified reason to ask if a categoric refusal ofERT/HRT from these women will do more harm than good.
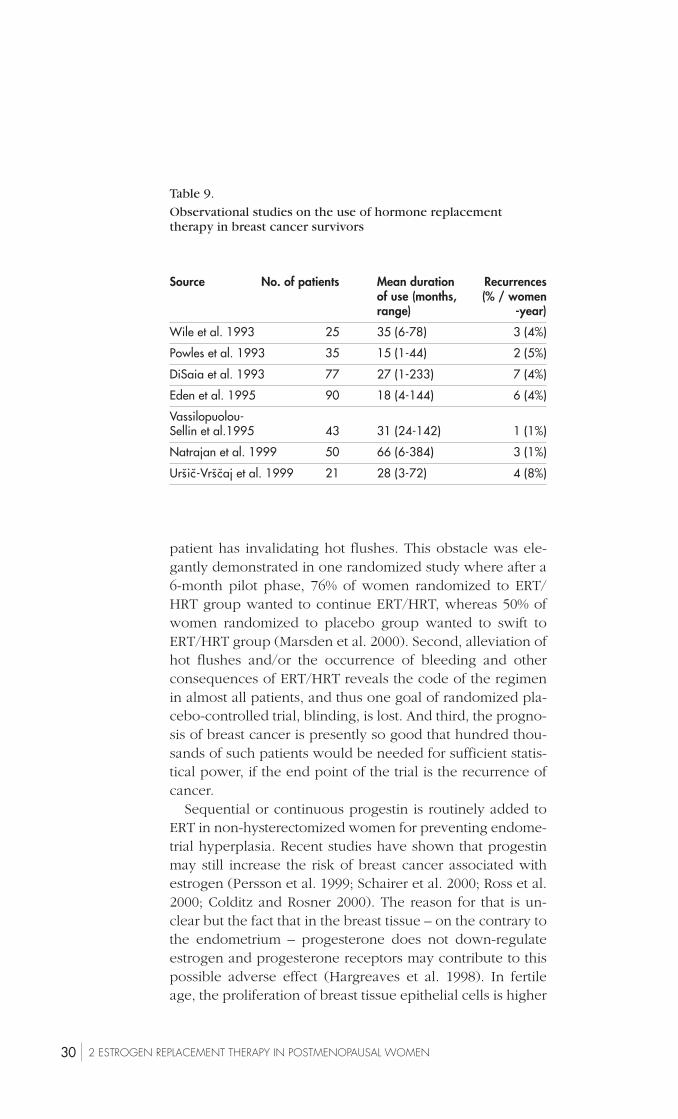
Some non-randomized and mainly retrospective studieshave been conducted on the use of ERT in patients with ahistory of breast cancer (Wile et al 1993; Powles et al.1993;DiSaia et al 1993; Eden et al. 1995; Vassilopoulou-Sellin et al.1995; Natrajan et al. 1999; Urs̆ic̆-Vrs̆c̆aj and Bebar 1999) (Ta-ble 9). No excess risk for the recurrence of breast cancer hasbeen found in these studies. The number of study subjectshas ranged from 25 to 90 and the mean duration of ERT/HRT from 15 to 66 months. Naturally, the data are far toolimited to show the final risk or safety of using ERT/HRT inthese patients.
It is obvious that we need randomized, preferably place-bo-controlled trials to assess the safety of ERT/HRT in breastcancer survivors. Conducting such trials is problematic. First,the randomization of breast cancer patients to hormone orplacebo treatment may be ethically questionable at least if a
30 2 ESTROGEN REPLACEMENT THERAPY IN POSTMENOPAUSAL WOMEN
Table 9.
Observational studies on the use of hormone replacementtherapy in breast cancer survivors
Source No. of patients Mean duration Recurrencesof use (months, (% / womenrange) -year)
Wile et al. 1993 25 35 (6-78) 3 (4%)
Powles et al. 1993 35 15 (1-44) 2 (5%)
DiSaia et al. 1993 77 27 (1-233) 7 (4%)
Eden et al. 1995 90 18 (4-144) 6 (4%)
Vassilopuolou-Sellin et al.1995 43 31 (24-142) 1 (1%)
Natrajan et al. 1999 50 66 (6-384) 3 (1%)
Urs̆ic̆-Vrs̆c̆aj et al. 1999 21 28 (3-72) 4 (8%)
patient has invalidating hot flushes. This obstacle was ele-gantly demonstrated in one randomized study where after a6-month pilot phase, 76% of women randomized to ERT/HRT group wanted to continue ERT/HRT, whereas 50% ofwomen randomized to placebo group wanted to swift toERT/HRT group (Marsden et al. 2000). Second, alleviation ofhot flushes and/or the occurrence of bleeding and otherconsequences of ERT/HRT reveals the code of the regimenin almost all patients, and thus one goal of randomized pla-cebo-controlled trial, blinding, is lost. And third, the progno-sis of breast cancer is presently so good that hundred thou-sands of such patients would be needed for sufficient statis-tical power, if the end point of the trial is the recurrence ofcancer.
Sequential or continuous progestin is routinely added toERT in non-hysterectomized women for preventing endome-trial hyperplasia. Recent studies have shown that progestinmay still increase the risk of breast cancer associated withestrogen (Persson et al. 1999; Schairer et al. 2000; Ross et al.2000; Colditz and Rosner 2000). The reason for that is un-clear but the fact that in the breast tissue – on the contrary tothe endometrium – progesterone does not down-regulateestrogen and progesterone receptors may contribute to thispossible adverse effect (Hargreaves et al. 1998). In fertileage, the proliferation of breast tissue epithelial cells is higher

312 ESTROGEN REPLACEMENT THERAPY IN POSTMENOPAUSAL WOMEN
during the luteal phase which is characterised by high se-rum progesterone levels (Södergvist 1998). It has also beenshown that in postmenopausal women estrogen combinedto continuous medroxyprogesterone acetate causes signifi-cantly higher proliferation rate in normal breast tissue thanestrogen alone does (Hofseth et al. 1999). However, we stillneed more clinical data to answer the questions whetherestrogen alone is more safe than estrogen + progestin, orwhether there is any difference between sequential and con-tinuous progestin in regard to the risk of breast cancer re-currence.

32 3 TAMOXIFEN AND TOREMIFENE
Tamoxifen
C = C
CH3CH3
OCH2 CH2N
CH2
CH3
C = C
CH2
CH2CI
Toremifene
CH3CH3
OCH2 CH2 N
Figure 5.
The chemical structures of tamoxifen and toremifene
3 TAMOXIFEN AND TOREMIFENE
3.1 Pharmacological and biological characteristics
Tamoxifen and toremifene are non-steroidal triphenylethyl-ene derivatives with antiestrogenic properties used in thetreatment of breast cancer (Figure 5). Tamoxifen is the cit-rate salt of the trans isomer of a triphenylethylene compound,and toremifene is a chlorinated derivative of tamoxifen (Kan-gas 1990). They are almost completely absorbed after oralintake, and bioavailability is nearly 100%. Maximal plasmaconcentrations of parent compound and metabolites arereached within 4-7 hours (Buckley and Goa 1989; Wisemanand Goa 1997). Tamoxifen and toremifene are almost com-pletly (99%) bound to plasma proteins, mainly to albumin.They are metabolized in the liver, and the majority of metab-olites are excreted in the feces (Buckley and Goa 1989; Wise-man and Goa 1997).

333 TAMOXIFEN AND TOREMIFENE
Tamoxifen and toremifene which are also called selectiveestrogen receptor modulators (SERM´s), possess both an es-trogenic and antiestrogenic activity, depending upon the doseor target organ (Robinson and Jordan 1989; Wiseman andGoa 1997). These drugs exert an antitumor activity which ismediated principally through a specific and competitive in-hibition of the binding of estrogen to estrogen receptor (Buck-ley and Goa 1989; Wiseman and Goa 1997). This activity isvery similar for tamoxifen and toremifene (Kangas 1990).They both prevent the growth of estrogen sensitive cells ofhuman breast cancer in vitro (Coezy et al 1982; Grenman etal 1991), but have no effect on the growth of estrogen re-ceptor negative cell lines (Robinson and Jordan 1989). How-ever, blocking of estrogen receptors is not the only mecha-nism of antitumor action, but antiestrogens may operate alsothrough different growth factors, such as alfa and beta trans-forming growth factor (Dickson and Lippman 1987; Knabbeet al. 1987; Colletta et al. 1994) and epidermal growth factor(Freiss et al.1990). Furthermore, antiestrogens inhibit theactivity of protein kinase C, which is a mediator of sometumor promoting factors (O´Brian et al. 1985).
3.2 Clinical use of tamoxifen and toremifene
Tamoxifen was introduced more than 20 years ago for thepalliative treatment of advanced breast cancer in postmeno-pausal women (Buckley and Goa 1989). Since then, tamoxifenhas become the treatment of choice for patients at all stagesof estrogen receptor (ER) positive breast cancer (Early BreastCancer Trialists´ Collaborative Group 1998). Fifty-five rand-omized clinical studies on 37 000 patients with local ER pos-itive breast cancer have shown that 5 years´ use of adjuvanttamoxifen reduces the recurrence rate by 47% and the mor-tality rate by 26% during the 10-year follow-up time (EarlyBreast Cancer Trialists´ Collaborative Group 1998).
Although toremifene has been developed later, it com-petes for favor in the treatment of advanced breast cancer.Five studies have compared the efficacy of tamoxifen (20,30, or 40 mg/day) and that of toremifene (40 or 60 mg/day)in postmenopausal patients with metastatic breast cancer(Pyrhönen et al. 1999). The overall response rates were 25.3%and 24.0% for tamoxifen and toremifene, respectively

34 3 TAMOXIFEN AND TOREMIFENE
(Pyrhönen et al 1999). A complete response was seen in5.5% of patients treated with tamoxifen and in 7.0% of thepatients treated with toremifene (Pyrhönen et al. 1999). Treat-ment failure occurred equally soon in the tamoxifen (5.5months) compared to the toremifene group (4.9 months),(Pyrhönen et al 1999). These data suggest that tamoxifen 20-40 mg/day and toremifene 60 mg are equally effective in thetreatment of metastatic breast cancer (Homesley et al. 1993;Pyrhönen et al. 1997; Pyrhönen et al. 1999). However, moredata on whether tamoxifen (20 mg/day) and toremifene (40mg/day) are equally effective in the adjuvant treatment ofbreast cancer are beginning to appear and the first data on899 patients with node-positive breast cancer have been re-cently published (Holli et al. 2000). According to this studybreast cancer recurrence rate was 26.1% in the tamoxifengroup and 23.1% in the toremifene group (p=0.31), and alsothe mean time to breast cancer recurrence and overall sur-vival time was similar in both groups (Holli et al. 2000).
Tamoxifen prevents also the occurrence of new cancersin the contralateral breast (Early Breast Cancer Trialists´ Col-laborative Group 1992, 1998). This finding, combined withthe proven efficacy of tamoxifen in the treatment of breastcancer (Hortobagyi 1998) has led to the rationale to use an-tiestrogens for breast cancer prevention (Chlebowski et al.1993). Indeed, tamoxifen decreased the incidence of inva-sive breast cancer by 49% in one large, randomized, place-bo-controlled study (Fisher et al. 1998) but not in two otherstudies with smaller number of participants (Powles et al.1998, Veronesi et al. 1998). The newer SERM´s, such as e.g.raloxifene, appear also effective in the prevention of breastcancer, because raloxifene decreased the risk of breast can-cer by 76% during the three years of use in older postmeno-pausal women with osteoporosis (Cummings et al. 1999).All this implies that antiestrogenic compounds may have aplace also in the prevention of breast cancer in future.
3.3 Gynecological consequenses of antiestrogens
Tamoxifen and toremifene have both antiestrogenic and es-trogenic activity, which are briefly summarized in table 10.Therefore, the whole impact of their intake on woman bodyand life is complex. They cause and aggravate vasomotor

353 TAMOXIFEN AND TOREMIFENE
Table 10.
Antiestrogenic and estrogenic effects of tamoxifen and toremifene inpostmenopausal women
Antiestrogenic Estrogenic
Gonadotropins FSHLH
Gynecologic organs Vasomotor symptoms Karyopycnotic indexEndometrial hyperplasiaEndometrial polypsEndometrial cancer
Breast tissue ER-positive breast cancertissue proliferation
Cardiovascular system Risk of myocardial infarctionTotal cholesterolLDL cholesterolHDL cholesterol /-Lipoprotein (a)VasodilatationRisk of venous thrombosis
Bone Rate of bone loss
symptoms in postmenopausal women, although they reduceblood levels of FSH and LH (Jordan et al. 1987; Ellmén et al.2000). Tamoxifen causes also maturation of the vaginal epi-thelial cells and increases their karyopyknotic index (Lahtiet al. 1994). Both tamoxifen and toremifene cause the prolif-eration of the endometrium and increase the risk of endome-trial polyps and hyperplasia (Tomas et al. 1995), and thesechanges are dependent on the duration of tamoxifen use(Cohen et al. 1999). The worst complication of tamoxifenuse can be endometrial cancer. Tamoxifen treatment has beenassociated with a 4.1 to 7.5-fold relative risk of developingendometrial carcinoma in two extensive studies (Fisher et al.1994; Rutqvist et al. 1995). These data were confirmed in ameta-analysis on 55 adjuvant tamoxifen trials with altogeth-er 37 000 breast cancer patients; the risk of endometrial can-cer was doubled by 1 or 2 years use of tamoxifen, and ap-proximately 4-fold after the use of 5 years of tamoxifen (Ear-ly Breast Cancer Trialists´ Collaborative Group 1998). Thereare also some data which link tamoxifen to the formation ofovarian cysts and endometriomas, but this evidence is notso strong that it could be regarded as well established so far(Neven et al. 1993; Cohen 1993).
36 3 TAMOXIFEN AND TOREMIFENE
In view of rather similar pharmacology and clinical profileof tamoxifen and toremifene, it is likely that toremifene causessimilar estrogenic effects in the female body as doestamoxifen, although some authors have questioned it (Wise-man and Goa 1997). In some animal studies toremifene hascaused fewer tumours in the liver than tamoxifen (Hirsimäkiet al 1993), reflecting perhaps a weaker estrogenic effect. Itis not known if the estrogenic activities of tamoxifen andtoremifene are similar in human, and therefore more clinicalcomparative data are needed.
3.4 Antiestrogens and cardiovascular organs
Cardiovascular system seems to be a target tissue for estro-gen and an important issue is to clear up the role of anties-trogen in the cardiovascular organs. In a Scottish adjuvanttrial tamoxifen reduced the occurrence of myocardial infarc-tion by 50% in 5 years (McDonald et al. 1995). This benefitmay be mediated in part through the falls in total cholesteroland low-density lipoprotein (LDL) cholesterol (Love et al.1994; Grey et al. 1995). Also toremifene reduces total cho-lesterol and LDL cholesterol levels (Gylling et al. 1995; Saar-to et al. 1996). As regards the cardioprotective high-densitylipoprotein (HDL) cholesterol, tamoxifen reduced it by 5%whereas toremifene increased it by 14% (Saarto et al. 1996).Both tamoxifen and toremifene decreased the level of lipo-protein (a) (Saarto et al.1996) which is a cholesterol-inde-pendent risk factor of ischemic heart disease. Tamoxifen alsoreduced the level of fibrinogen (Love et al. 1994) and that ofhomocysteine (Anker et al. 1995), which effects may alsocontribute to cardiovascular protection.
All these effects may be related to the estrogenic activityof tamoxifen and toremifene. In contrast no data exist so faron whether antiestrogens could trigger a direct dilatation inthe arteries or affect the endothelial factors, such as prostag-landins, NO, or ET-1.

373 TAMOXIFEN AND TOREMIFENE
3.5 Antiestrogens and bone
Because antiestrogens are given often for 5 or more years inpostmenopausal women as an adjuvant therapy of breastcancer, it is important to know also their effect on boneintegrity which, on the other hand, is already affected bypostmenopausal hypoestrogenism. Tamoxifen has beenshown to increase bone mineral density in postmenopausalwomen by 1-2% per year (Grey et al. 1995; Powles et al.1996; Chang et al. 1996). However, so far we do not haveany epidemiological data on the risk of hip and other frac-tures during tamoxifen use.
Tamoxifen has been shown to reduce bone resorption asmeasured by the output of hydroxyproline (Ward et al.1993),pyridinoline, and deoxypyridinoline (Kenny et al. 1995), andalso bone formation measured by bone-specific alkalinephosphatase and osteocalcin (Kenny et al. 1995).
The data on the effect of toremifene on bone are scanty.Yet in one comparison tamoxifen (20 mg/day) and toremifene(60 mg/day) used for two years did not decrease BMD, where-as the addition of bisphosphonate clodronate to antiestro-gens increased BMD by 2-4% (Saarto et al. 1997).
38
III AIMS OF THE STUDY
The objectives of the present study were to
1. evaluate the effects and safety of estrogen replacementin postmenopausal women with a history of breastcancer (publication I)
2. assess and compare the gynecological consequences oftamoxifen and toremifene (publication II)
3. explore some biological mechanisms dealing preferablywith endothelial cells during the use of tamoxifen andtoremifene (publications III and IV)
4. compare the effects of tamoxifen and toremifene on bonemetabolism and density (publications V and VI)
III AIMS OF THE STUDY
391 PATIENTS
IV PATIENTS AND METHODS
1 PATIENTS
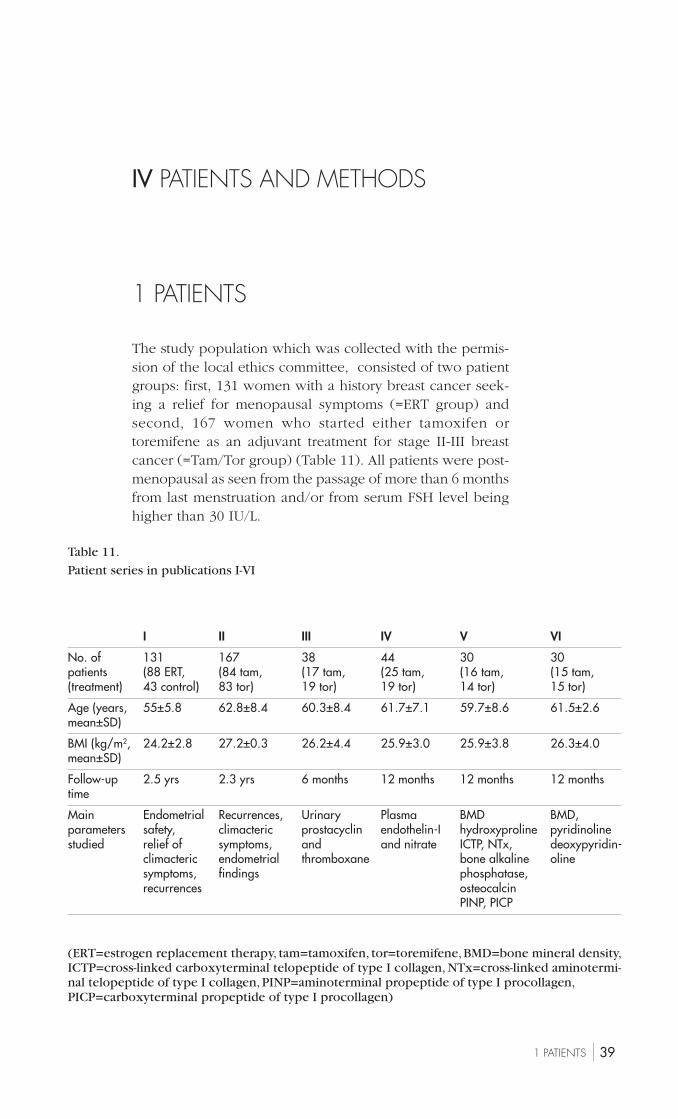
The study population which was collected with the permis-sion of the local ethics committee, consisted of two patientgroups: first, 131 women with a history breast cancer seek-ing a relief for menopausal symptoms (=ERT group) andsecond, 167 women who started either tamoxifen ortoremifene as an adjuvant treatment for stage II-III breastcancer (=Tam/Tor group) (Table 11). All patients were post-menopausal as seen from the passage of more than 6 monthsfrom last menstruation and/or from serum FSH level beinghigher than 30 IU/L.
Table 11.
Patient series in publications I-VI
I II III IV V VI
No. of 131 167 38 44 30 30patients (88 ERT, (84 tam, (17 tam, (25 tam, (16 tam, (15 tam,(treatment) 43 control) 83 tor) 19 tor) 19 tor) 14 tor) 15 tor)
Age (years, 55±5.8 62.8±8.4 60.3±8.4 61.7±7.1 59.7±8.6 61.5±2.6mean±SD)
BMI (kg/m2, 24.2±2.8 27.2±0.3 26.2±4.4 25.9±3.0 25.9±3.8 26.3±4.0mean±SD)
Follow-up 2.5 yrs 2.3 yrs 6 months 12 months 12 months 12 monthstime
Main Endometrial Recurrences, Urinary Plasma BMD BMD,parameters safety, climacteric prostacyclin endothelin-I hydroxyproline pyridinolinestudied relief of symptoms, and and nitrate ICTP, NTx, deoxypyridin-
climacteric endometrial thromboxane bone alkaline olinesymptoms, findings phosphatase,recurrences osteocalcin
PINP, PICP
(ERT=estrogen replacement therapy, tam=tamoxifen, tor=toremifene, BMD=bone mineral density,ICTP=cross-linked carboxyterminal telopeptide of type I collagen, NTx=cross-linked aminotermi-nal telopeptide of type I collagen, PINP=aminoterminal propeptide of type I procollagen,PICP=carboxyterminal propeptide of type I procollagen)
40
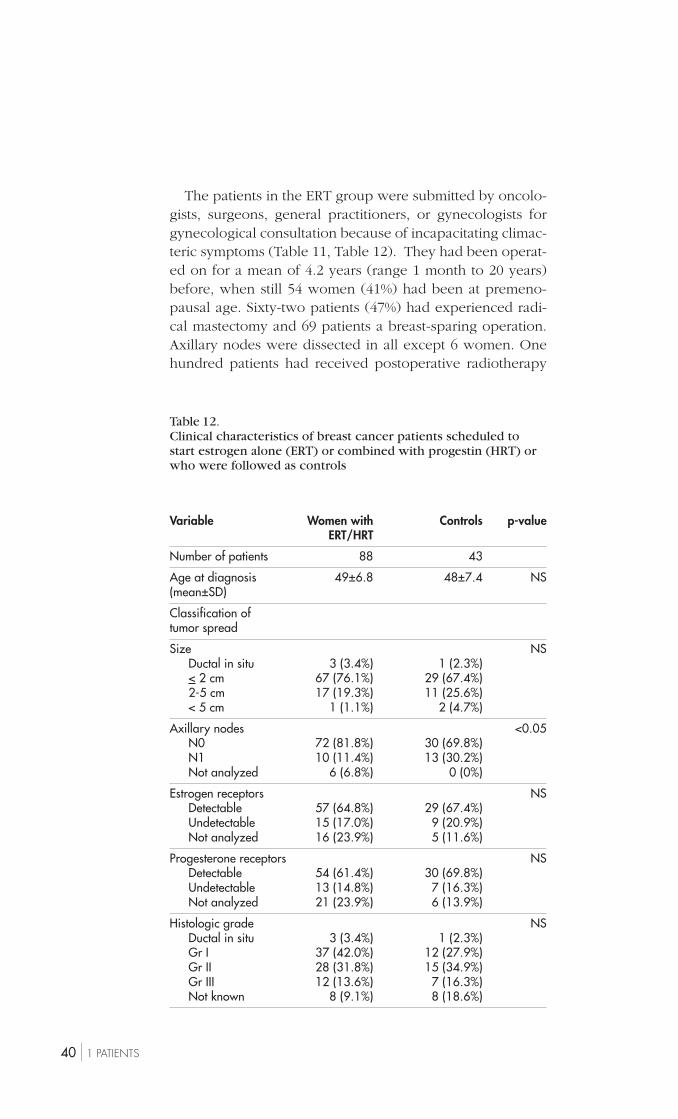
Table 12.Clinical characteristics of breast cancer patients scheduled tostart estrogen alone (ERT) or combined with progestin (HRT) orwho were followed as controls
Variable Women with Controls p-valueERT/HRT
Number of patients 88 43
Age at diagnosis 49±6.8 48±7.4 NS(mean±SD)
Classification oftumor spread
Size NSDuctal in situ 3 (3.4%) 1 (2.3%)< 2 cm 67 (76.1%) 29 (67.4%)2-5 cm 17 (19.3%) 11 (25.6%)< 5 cm 1 (1.1%) 2 (4.7%)
Axillary nodes <0.05N0 72 (81.8%) 30 (69.8%)N1 10 (11.4%) 13 (30.2%)Not analyzed 6 (6.8%) 0 (0%)
Estrogen receptors NSDetectable 57 (64.8%) 29 (67.4%)Undetectable 15 (17.0%) 9 (20.9%)Not analyzed 16 (23.9%) 5 (11.6%)
Progesterone receptors NSDetectable 54 (61.4%) 30 (69.8%)Undetectable 13 (14.8%) 7 (16.3%)Not analyzed 21 (23.9%) 6 (13.9%)
Histologic grade NSDuctal in situ 3 (3.4%) 1 (2.3%)Gr I 37 (42.0%) 12 (27.9%)Gr II 28 (31.8%) 15 (34.9%)Gr III 12 (13.6%) 7 (16.3%)Not known 8 (9.1%) 8 (18.6%)
1 PATIENTS
The patients in the ERT group were submitted by oncolo-gists, surgeons, general practitioners, or gynecologists forgynecological consultation because of incapacitating climac-teric symptoms (Table 11, Table 12). They had been operat-ed on for a mean of 4.2 years (range 1 month to 20 years)before, when still 54 women (41%) had been at premeno-pausal age. Sixty-two patients (47%) had experienced radi-cal mastectomy and 69 patients a breast-sparing operation.Axillary nodes were dissected in all except 6 women. Onehundred patients had received postoperative radiotherapy

411 PATIENTS
and 19 patients adjuvant chemotherapy. Five patients hadused antiestrogens but stopped it 3 to 5 years before theinitiation of the trial. Forty-three women were hysterect-omised. Before the start of ERT/HRT, all patients underwentgynecological examinations (e.g. mammography, pelvic ex-amination, Pap smear collection), and the benefits and risksof ERT/HRT were explained thoroughly orally and in writ-ten form, and all patients gave their written consent.
The patients of Tam/Tor group were referred to gyneco-logical follow-up after they had been randomized at thedepartment of oncology to receive either tamoxifen (20 mg/day) or toremifene (40 mg/day) for three years (Table 11).They were participants in the Finnish Breast Cancer GroupAdjuvant Toremifene versus Tamoxifen Trial, and randomi-zation was done by Finnish Cancer Register. Fifty-six pa-tients had experienced conservative surgery and 111 patientsmastectomy 6 to 8 weeks before the start of antiestrogens,and axillary nodes were dissected in all women. In addition,all women had received postoperative local radiotherapy.Thirty-eight patients were hysterectomized, 53 used antihy-pertensive drugs, and 27 smoked.
42 2 STUDY TREATMENTS
2 STUDY TREATMENTS
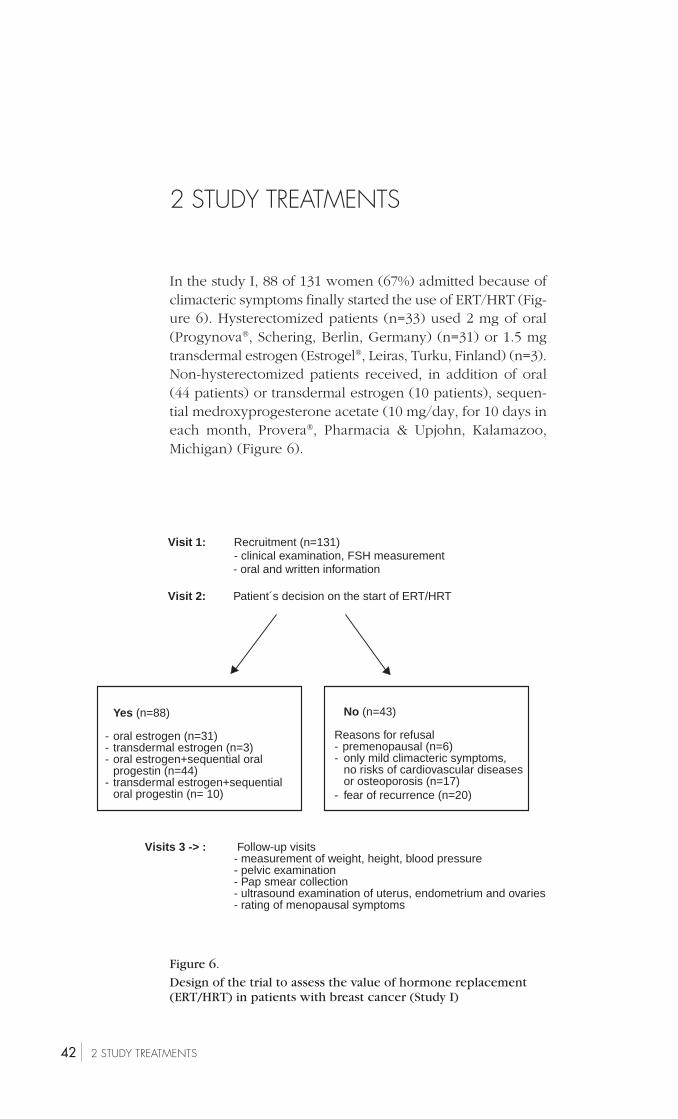
In the study I, 88 of 131 women (67%) admitted because ofclimacteric symptoms finally started the use of ERT/HRT (Fig-ure 6). Hysterectomized patients (n=33) used 2 mg of oral(Progynova®, Schering, Berlin, Germany) (n=31) or 1.5 mgtransdermal estrogen (Estrogel®, Leiras, Turku, Finland) (n=3).Non-hysterectomized patients received, in addition of oral(44 patients) or transdermal estrogen (10 patients), sequen-tial medroxyprogesterone acetate (10 mg/day, for 10 days ineach month, Provera®, Pharmacia & Upjohn, Kalamazoo,Michigan) (Figure 6).
No (n=43)
Reasons for refusal- premenopausal (n=6)- only mild climacteric symptoms,
no risks of cardiovascular diseasesor osteoporosis (n=17)
- fear of recurrence (n=20)
Visits 3 -> : Follow-up visits- measurement of weight, height, blood pressure- pelvic examination- Pap smear collection- ultrasound examination of uterus, endometrium and ovaries- rating of menopausal symptoms
Visit 1: Recruitment (n=131)- clinical examination, FSH measurement- oral and written information
Visit 2: Patient´s decision on the start of ERT/HRT
Yes (n=88)
- oral estrogen (n=31)- transdermal estrogen (n=3)- oral estrogen+sequential oral
progestin (n=44)- transdermal estrogen+sequential
oral progestin (n= 10)
Figure 6.
Design of the trial to assess the value of hormone replacement(ERT/HRT) in patients with breast cancer (Study I)
433 METHODS
In the study II, 84 patients used tamoxifen (20 mg/day,Tadex®, Orion, Turku, Finland) and 83 used toremifene (40mg/day, Fareston®, Orion, Turku, Finland). The follow-uptimes of both study group are presented in Table 13.
Table 13.
Follow-up times completed by patients using either estrogen orestrogen + sequential progestin (ERT/HRT), or tamoxifen (Tam)or toremifene (Tor)
Time ERT/HRT Tam Tor(n=88) (n=84) (n=83)
< 1 year 12
1-2 years 20 23 14
2-3 years 20 19 17
3 years or more 36 42 52
3 METHODS
3.1 Clinical examinations and follow-up
Clinical examinations including measurements of weight,height, and blood pressure, as well as pelvic examinationand Pap smear collection were performed in all patientsbefore the start of hormone treatment. The same examina-tions were repeated 6 and 12 months later and then annual-ly. Blood and urinary samples were collected after the over-night fast before the start of hormone regimens and at 6 and12 months of treatment. Serum, plasma, and urinary sampleswere stored at -22°C until assayed. Before the sampling, pa-tients were instructed to avoid nitrate-rich (meat, fish, greenvegetables, malt beverages and wine) and gelatin containing(meat, fish, poultry, yoghurt and pudding) food for 48 hours.
The patients recorded menopausal symptoms (hot flush-es, sweating, sleep disturbance, nervousness, depression,vertigo, fatigue, arthralgia, headache, tachycardia and vagi-nal dryness) on the modified Kupperman scale at each visit
44 3 METHODS
(Wiklund et al. 1992). The severity of each symptom wasgraded form 0 to 3, and the severity score for hot flusheswas multiplied by 4 and that for sweating, sleep disturbance,and nervousness by 2, and the scores were summed up.
The patients were followed at the oncological or surgicaldepartments in regard to the status of breast cancer. Thebreasts were carefully palpated at each visit, and mammog-raphy was performed annually. In addition, the serum levelof CA 15-3, reflecting a possible growth or recurrence ofbreast cancer, was assessed at each visit.
3.2 Transvaginal sonography and endometrialsampling
Transvaginal sonography (Aloka SSD 500) was performed ateach visit to assess gynecological organs including the en-dometrial thickness. Sonographic examination was comple-mented by saline sonohysterography (Widrich et al. 1996), ifendometrial polyp was suspected (study I and II) or en-dometrial thickness exceeded 8 mm (study II). In patientswith endometrial polyp diagnosed by saline sonohysterog-raphy, polyp was removed with electroresector through hys-teroscopy.
To assess the blood flow in the uterine artery, pulsatilityindex (PI) was measured by using doppler ultrasound (Hi-tachi 515A, Tokyo, Japan, 6.5 MHz endovaginal transducer)before the start of medication and at 6 and 12 months of trialin 30 patients using either tamoxifen (n=15) or toremifene(n=15) (Study II).
Endometrial biopsy was collected with Pipelle endometri-al aspirator (Unimar, Wilmington, CN) (Chambers and Cham-bers, 1992) from patients with intact uterus, in the study I ifendometrial thickness exceeded 5 mm at entry or 10 mm ona follow-up visit, or if there was abnormal uterine bleedingbefore recruitment or during the trial. Endometrial biopsywas collected at each visit in the trial II. The endometriumwas classified as atrophic (small simple tubular glands linedby cuboidal epithelium, the nuclei centrally located, no mi-toses) or mildly proliferative (small tubular glands lined bycuboidal to columnar epithelium, ovoid nuclei basally orcentrally located, some mitoses). The same experienced pa-thologist (Dr. T. Wahlstöm) studied all histological samples.

453 METHODS
3.3 Laboratory measurments
The serum concentration of FSH was measured by time-re-solved fluoroimmunoassay (DELFIA; Wallac, Turku, Finland)according to the instructions of the manufacturer. Tumormarker CA 15-3 was measured by immunoradiometric assay(O´Hanlon et al. 1995).
Prostacyclin and thromboxane output were assessed bytheir stable urinary metabolites 2,3-dinor-6-keto prostaglan-din F
1α and 2,3-dinor-thromboxane B2, respectively, by radi-
oimmunoassays after solid-phase extraction and purificationof the sample by high-performance liquid chromatography(Ylikorkala et al. 1986, Tulppala et al. 1991). To avoid theeffect of differences in the dilution of urine, excretions wereexpressed against creatinine, which was measured by a rou-tine laboratory method. The capacity of platelets to produceTxA
2 was assayed by measuring the serum concentration of
TxB2, a metabolite of TxA
2, by specific radioimmunoassay
(Viinikka and Ylikorkala 1980). Before measurement, bloodsamples were allowed to clot at +37°C for 30 minutes andserum was then separated. The intra-assay coefficient of var-iation in measurements of prostacyclin and thromboxanemetabolites was less than 8%, and the interassay coefficientof variation was between 10.4-14.1%.
Plasma endothelin-1 was analyzed by radioimmunoassay(Ylikorkala et al. 1995). Acidified 3 ml plasma samples wereextracted with Sep-Pak-Vac tC18 cartidges. After washes with0.1% trifluoroacetetic acid (TFA) and 45% methanol-0.1% TFA,ET-1 was eluted with 90% methanol-0.1% TFA. The evapo-rated samples were dissolved in 0.45 ml of assay buffer (50mmol/l phosphate buffer, pH 7.4, 150 mmol/l NaCl 1% bo-vine serum albumin). The radioimmunoassay was performedin tubes coated first with goat anti-rabbit immunoglobulinand then with diluted ET-1 antibody raised in rabbits. Thesamples were incubated for 24 hours and then with 10000dpm of 125I-ET-1 for 48 hours. The bound radioactivity re-maining in tubes after washing was counted, and the resultscalculated on the basis of a dilution series of authentic ET-1.The intra-assay coefficient of variation for measurement was5.7%.
Nitric oxide production was evaluated on the basis of theconcentration of nitrate+nitrite (NOx). Nitrate was reducedto nitrite by nitrate reductase, the sample deproteinized withZnSO
4, and the concentration of nitrite was measured by the
46 3 METHODS
spectrophotometrically based Griess reaction (Ylikorkala etal. 1998). The intra-assay coefficient of variation of NOx was1.7% and 2.2% in the lower and higher concentration range,respectively.
Bone resorption markers
Urinary hydroxyproline (HOP) was measured with high-per-formance liquid chromatography (Turpeinen and Pomoell1985). The intra-assay coefficient of variation of this methodwas 8.9%. Urinary cross-linked aminoterminal telopeptideof type I collagen (NTx) was measured with an enzyme-linked immunosorbent assay using monoclonal antibody di-rected against th N-telopeptide of type I collagen isolatedfrom human urine (Hanson et al. 1992). The intra-assay var-iation of this method was 6.2%. To avoid errors caused bydifferences in urine dilution, both HOP and NTx data wereexpressed against creatinine assessed by a routine laborato-ry method. Serum cross-linked carboxyterminal telopeptideof type I collagen (ICTP) was determined by radioimmu-noassay (Telopeptide ICTP, Orion Diagnostica, Espoo, Fin-land) (Risteli et al. 1993), and the intra-assay coefficient ofvariation for this measurement ranged from 3% to 9%. Uri-nary excretion of pyridinoline (Pyr) and deoxypyridinoline(Dpyr) was measured by ion-pair reversed-phase high per-formance liquid chromatoraphy (RP-HPLC) (Garnero et al.1994). To avoid any effect of different dilutions of urine, Pyrand Dpyr data are expressed against grams of creatinine.The intra-assay coefficient of variation is less than 10% forPyr and less than 15% for Dpyr.
Bone formation markers
Bone-specific alkaline phosphatase in serum was measuredby immunoradiometric assay (Tandem-R Ostase, HybritecEurope, Liege, Belgium) (Epstein 1988). The intra-assay var-iation in this method was below 7%. Serum osteocalcin wasmeasured by an immunoradiometric assay using antibodiesagainst human osteocalcin (Osteocalcin FEIA, Farmacia CAPSystem, Uppsala, Sweden) (Epstein 1988). The intra-assaycoefficient of variation was 7%. Serum aminoterminal (PINP)and carboxyterminal (PICP) propeptide of type I procolla-gen were determined by RIA (Procollagen Intact PINP RIAKit, Procollagen PICP RIA Kit, Orion Diagnostica) (Melkko

473 METHODS
et al. 1996). The intra-assay coefficient of variation of themeasurement of PINP was 5-8% and for measurement ofPICP 3%.
3.4 Bone density measurement
Bone mineral density (BMD) in the lumbar spine (LI-IV) andin different sites of the proximal femur was measured bydual-energy x-ray absorptiometry (DEXA) (Hologic QDR-1000, Waltham, MA) (De Boer et al. 1994). Data were givenas density against area (g/cm2). The intra-assay coefficient ofvariation in our department was 0.5% in lumbar spine and1% in femoral neck.
3.5 Statistical analyses
All data are expressed as a mean ± standard deviation (SD)(Studies I-III ) or standard error (SE) (Studies IV and VI). Thesignificance of differences between the groups with numer-ical variables was determined with paired and unpairedStudent´s t-test. When repeated measures were obtained, thetwo-way analysis of variance (ANOVA) was used. The com-parison of two proportions in case of paired samples wasperformed by McNemar´s test in study II. Chi-square testwas used to compare the distribution of categorical varia-bles of two independent samples (Studies I and II). Pearsoncoefficient (study IV) or Spearman nonparametric correla-tion analysis (study V, VI) were used for the determinationof correlation between the two variables.
48 1 ESTROGEN REPLACEMENT THERAPY IN BREAST CANCER PATIENTS
V RESULTS
1 ESTROGEN REPLACEMENTTHERAPY IN BREAST CANCERPATIENTS (Study I)
The mean follow-up time with estrogen regimen was2.5±1.5 years (range 1 month to 5.2 years), which corre-sponds to 216 woman-years. Forty-three women were fol-lowed as control population without estrogen regimen for amean of 2.5±1.3 years (range 1 month to 4.6 years) (= 111woman-years). Ten of the 88 patients discontinued estrogentreatment within the 12 to 39 months; four because of lackof climacteric symptoms and six because of recurrence ofdisease or new breast cancer. One woman with contralateralbreast cancer wanted to continue ERT/HRT. Five patientsneeded to increase the dose of oral estradiol to 3 mg be-tween 6 and 12 months for sufficient alleviation of symp-toms, and three women reduced the dose from 2 to 1 mgbetween 1 and 4 months because of breast tenderness.Three women with sequential regimen experienced PMS-like symptoms during progestin phase, and these womensubsequently took progestin courses at two-month intervals.
ERT/HRT abolished or alleviated vasomotor or other cli-macteric symptoms (Figure 7). Forty-seven patients with in-tact uterus had regular withdrawal bleeding, seven patientshad spotting, and seven patients did not bleed al all. Nonediscontinued the treatment because of adverse effects. Twowomen had transient simple endometrial hyperplasia afterone and two years of the regimen.
Five of 88 patients using ERT/HRT experienced the recur-rence of the cancer after a mean of 19 months (range from12 to 36 months) use of ERT/HRT, and two developed con-tralateral breast cancer after 14 and 24 months use of ERT/HRT, respectively. All the recurrences or contralateral breastcancers were detected as a consequence of clinical symp-toms, Ca 15-3 levels was of no help to predict these cases.
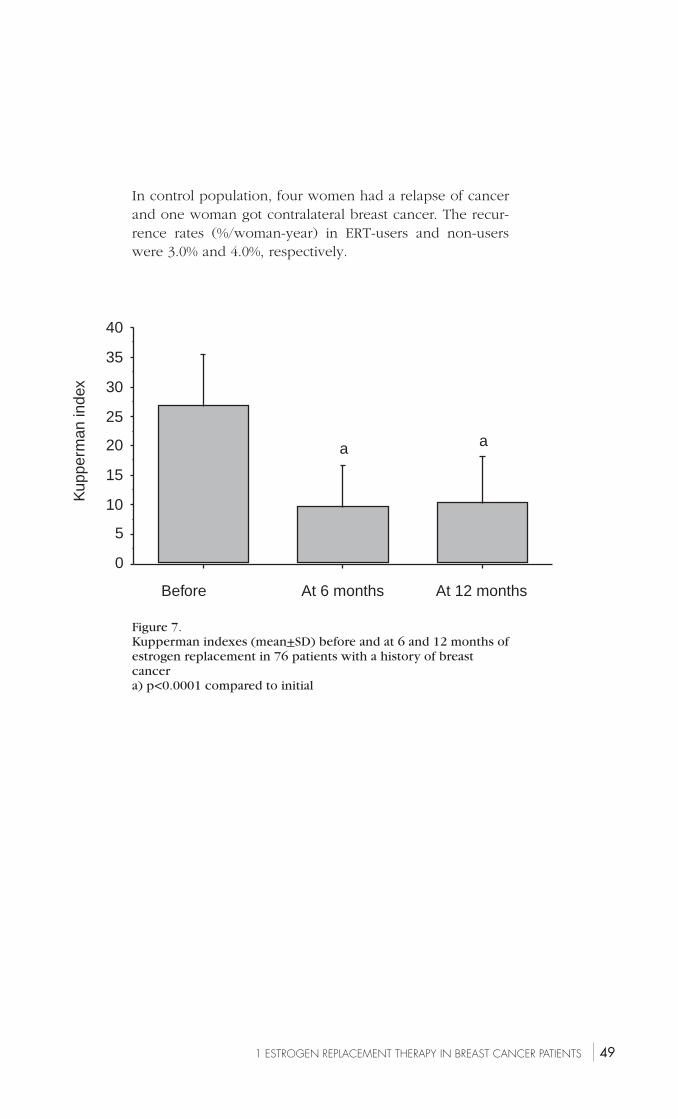
491 ESTROGEN REPLACEMENT THERAPY IN BREAST CANCER PATIENTS
Figure 7.Kupperman indexes (mean+SD) before and at 6 and 12 months ofestrogen replacement in 76 patients with a history of breastcancera) p<0.0001 compared to initial
0
5
10
15
20
25
30
35
40
Before At 6 months At 12 months
a a
Kup
perm
an in
dex
In control population, four women had a relapse of cancerand one woman got contralateral breast cancer. The recur-rence rates (%/woman-year) in ERT-users and non-userswere 3.0% and 4.0%, respectively.
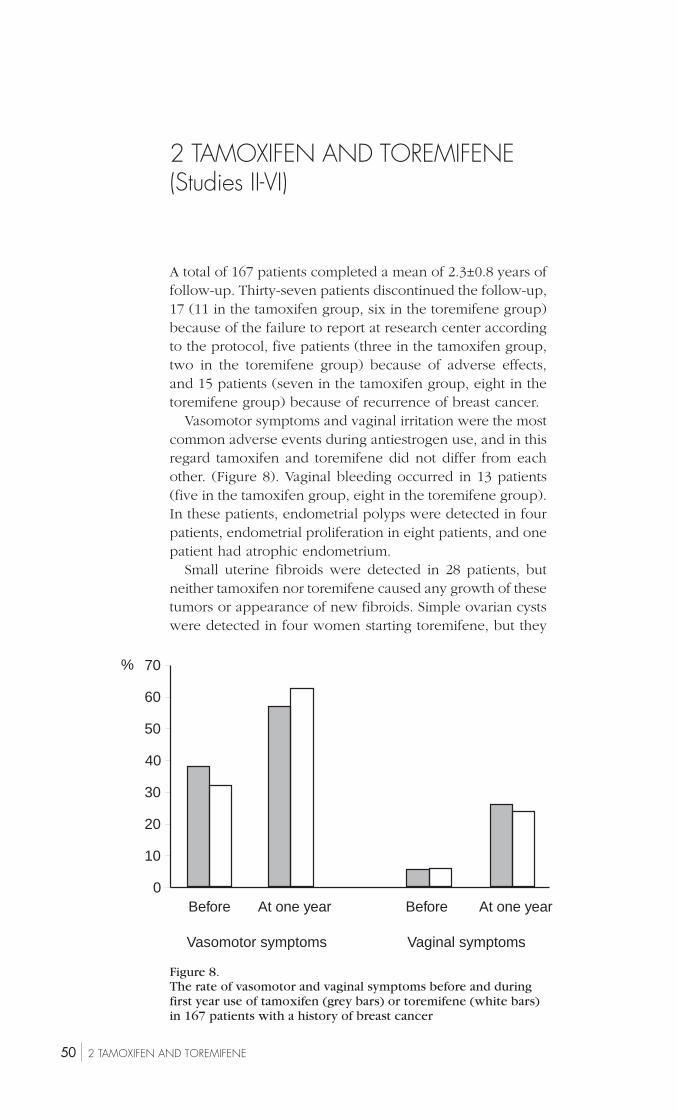
50 2 TAMOXIFEN AND TOREMIFENE
Figure 8.The rate of vasomotor and vaginal symptoms before and duringfirst year use of tamoxifen (grey bars) or toremifene (white bars)in 167 patients with a history of breast cancer
70
60
50
40
30
20
10
0
%
Before At one year Before At one year
Vasomotor symptoms Vaginal symptoms
2 TAMOXIFEN AND TOREMIFENE(Studies II-VI)
A total of 167 patients completed a mean of 2.3±0.8 years offollow-up. Thirty-seven patients discontinued the follow-up,17 (11 in the tamoxifen group, six in the toremifene group)because of the failure to report at research center accordingto the protocol, five patients (three in the tamoxifen group,two in the toremifene group) because of adverse effects,and 15 patients (seven in the tamoxifen group, eight in thetoremifene group) because of recurrence of breast cancer.
Vasomotor symptoms and vaginal irritation were the mostcommon adverse events during antiestrogen use, and in thisregard tamoxifen and toremifene did not differ from eachother. (Figure 8). Vaginal bleeding occurred in 13 patients(five in the tamoxifen group, eight in the toremifene group).In these patients, endometrial polyps were detected in fourpatients, endometrial proliferation in eight patients, and onepatient had atrophic endometrium.
Small uterine fibroids were detected in 28 patients, butneither tamoxifen nor toremifene caused any growth of thesetumors or appearance of new fibroids. Simple ovarian cystswere detected in four women starting toremifene, but they
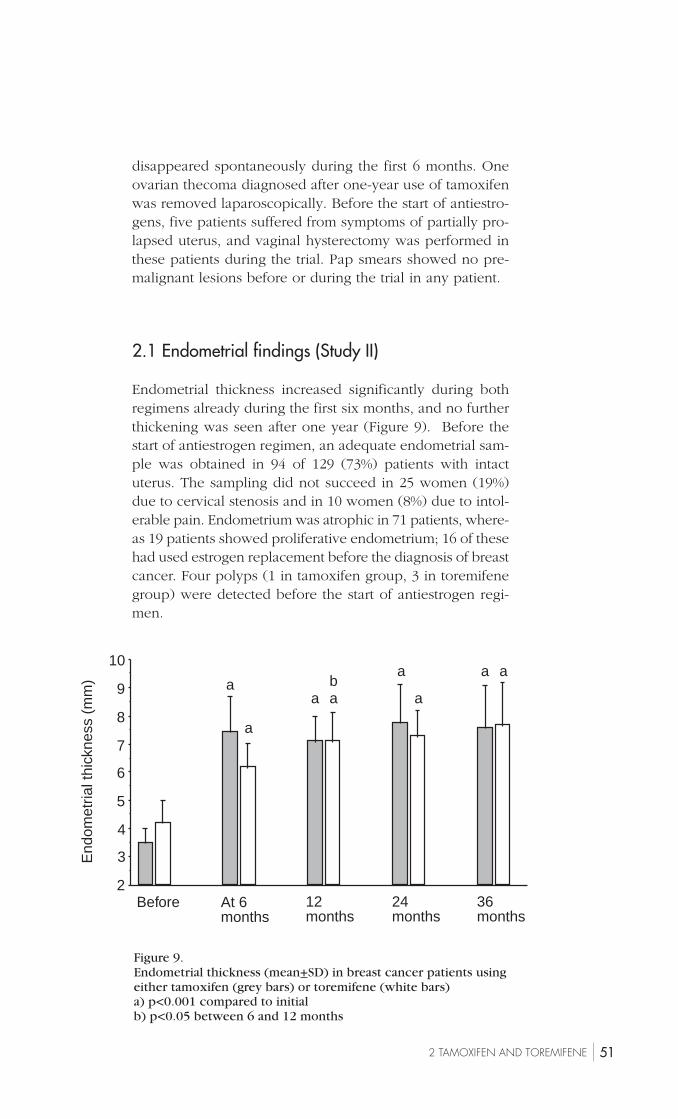
512 TAMOXIFEN AND TOREMIFENE
disappeared spontaneously during the first 6 months. Oneovarian thecoma diagnosed after one-year use of tamoxifenwas removed laparoscopically. Before the start of antiestro-gens, five patients suffered from symptoms of partially pro-lapsed uterus, and vaginal hysterectomy was performed inthese patients during the trial. Pap smears showed no pre-malignant lesions before or during the trial in any patient.
2.1 Endometrial findings (Study II)
Endometrial thickness increased significantly during bothregimens already during the first six months, and no furtherthickening was seen after one year (Figure 9). Before thestart of antiestrogen regimen, an adequate endometrial sam-ple was obtained in 94 of 129 (73%) patients with intactuterus. The sampling did not succeed in 25 women (19%)due to cervical stenosis and in 10 women (8%) due to intol-erable pain. Endometrium was atrophic in 71 patients, where-as 19 patients showed proliferative endometrium; 16 of thesehad used estrogen replacement before the diagnosis of breastcancer. Four polyps (1 in tamoxifen group, 3 in toremifenegroup) were detected before the start of antiestrogen regi-men.
Figure 9.Endometrial thickness (mean+SD) in breast cancer patients usingeither tamoxifen (grey bars) or toremifene (white bars)a) p<0.001 compared to initialb) p<0.05 between 6 and 12 months
2
3
4
5
6
7
8
9
10
Before
a
a
a ab
a
a
a a
At 6months
12months
24months
36months
End
omet
rial t
hick
ness
(m
m)
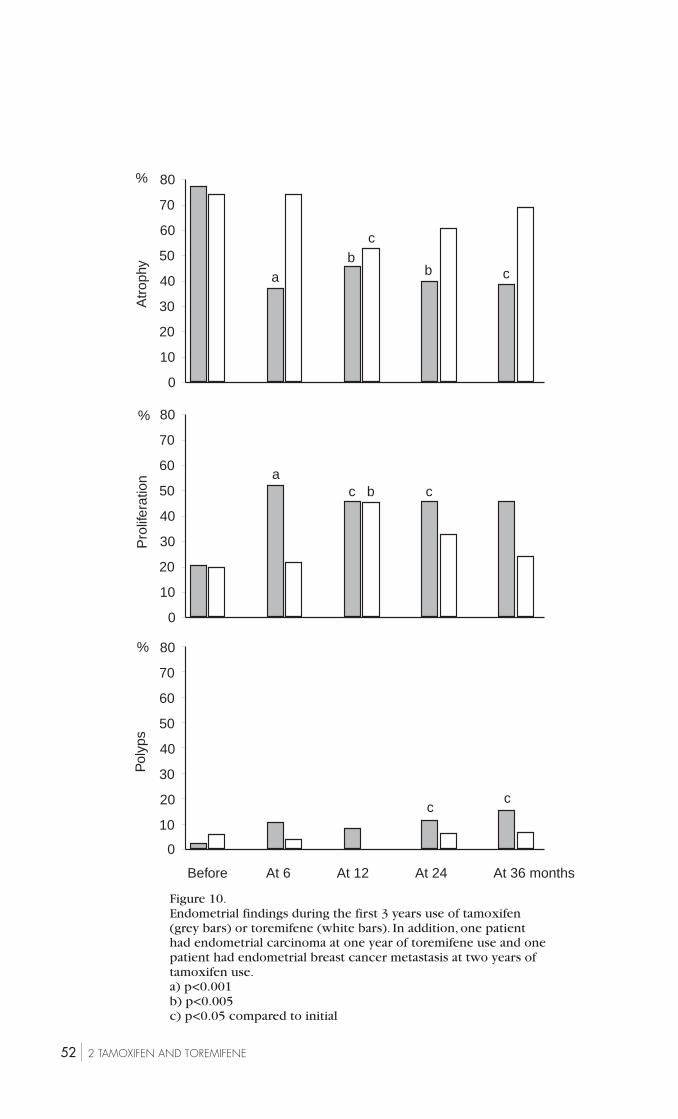
52 2 TAMOXIFEN AND TOREMIFENE
Figure 10.Endometrial findings during the first 3 years use of tamoxifen(grey bars) or toremifene (white bars). In addition, one patienthad endometrial carcinoma at one year of toremifene use and onepatient had endometrial breast cancer metastasis at two years oftamoxifen use.a) p<0.001b) p<0.005c) p<0.05 compared to initial
%
%
Pol
yps
%
Pro
lifer
atio
nA
trop
hy
80
70
60
50
40
30
20
10
0
ac cb
80
70
60
50
40
30
20
10
0
Before At 6 At 12 At 24 At 36 months
cc
80
70
60
50
40
30
20
10
0
ab
b c
c

532 TAMOXIFEN AND TOREMIFENE
During the control visits, endometrial sampling succeed-ed in 81% of patients. Proliferative endometrium was seen in46.8% of samples in tamoxifen users and in 32.2% of sam-ples in toremifene users (p<0.0001 between groups) (Figure10). From the 24 polyps diagnosed during the antiestrogenregimen, 17 existed in tamoxifen users and seven intoremifene users (p<0.05). All polyps detected before andduring the antiestrogen regimen were removed hysteroscop-ically. One patient on toremifene developed endometrialcarcinoma at 12 months and she also had a metastasis ofbreast cancer in her ovary. One patient got breast cancermetastasis on her endometrium after 24 months of tamoxifenuse.
2.2 Vascular effects
2.2.1 Uterine artery resistance (Study II)
Tamoxifen did not have any effect on uterine artery resist-ance, but toremifene reduced it significantly (p<0.05) by 12months. The changes in PI or endometrial thickness did notcorrelate with each other in the whole series or in eithersubgroup.
2.2.2 Prostacyclin and thromboxane
Neither tamoxifen (n=15) nor toremifene (n=19) caused anychange in the production of prostacyclin or thromboxane A
2
(Figure 11). Before the start of the antiestrogen regimen,patients using antihypertensive drugs had lower urinary pros-tacyclin metabolite (dinor-6-keto) level (18.5±6.1 vs 35.5±18.5ng/mmol, p<0.05) and also lower platelet capacity to pro-duce thromboxane A
2 (62.6±67.8 vs 134.6±75.6 ng/mL,
p<0.05) than did the normotensive patients.
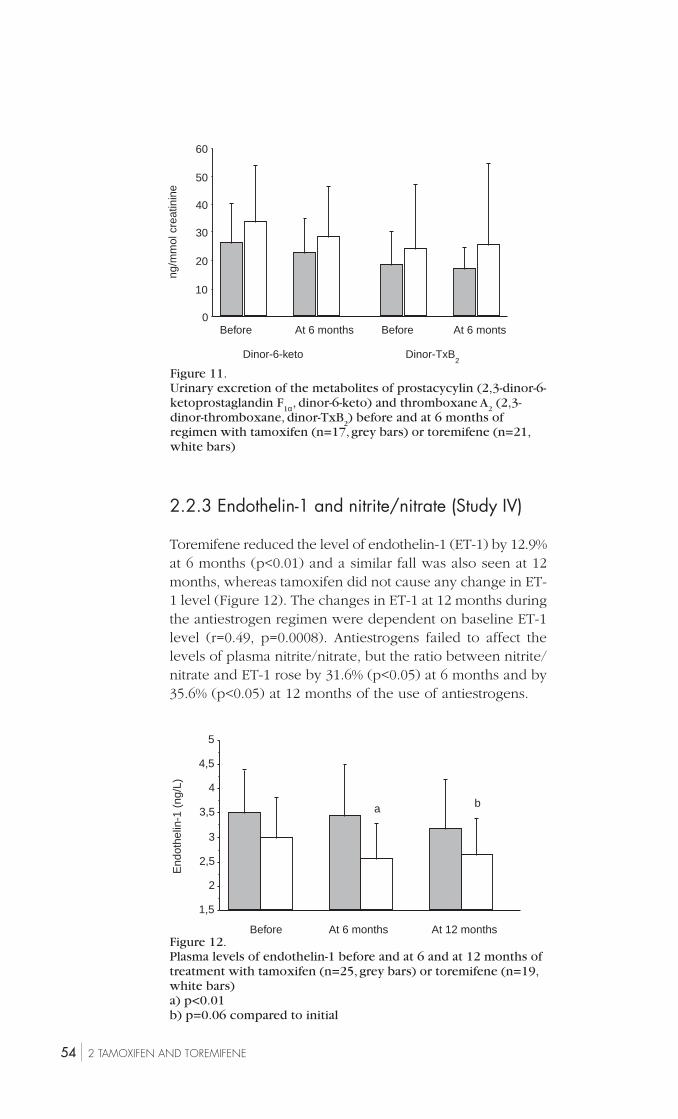
54 2 TAMOXIFEN AND TOREMIFENE
2.2.3 Endothelin-1 and nitrite/nitrate (Study IV)
Toremifene reduced the level of endothelin-1 (ET-1) by 12.9%at 6 months (p<0.01) and a similar fall was also seen at 12months, whereas tamoxifen did not cause any change in ET-1 level (Figure 12). The changes in ET-1 at 12 months duringthe antiestrogen regimen were dependent on baseline ET-1level (r=0.49, p=0.0008). Antiestrogens failed to affect thelevels of plasma nitrite/nitrate, but the ratio between nitrite/nitrate and ET-1 rose by 31.6% (p<0.05) at 6 months and by35.6% (p<0.05) at 12 months of the use of antiestrogens.
Figure 11.Urinary excretion of the metabolites of prostacycylin (2,3-dinor-6-ketoprostaglandin F
1α, dinor-6-keto) and thromboxane A2 (2,3-
dinor-thromboxane, dinor-TxB2) before and at 6 months of
regimen with tamoxifen (n=17, grey bars) or toremifene (n=21,white bars)
Figure 12.Plasma levels of endothelin-1 before and at 6 and at 12 months oftreatment with tamoxifen (n=25, grey bars) or toremifene (n=19,white bars)a) p<0.01b) p=0.06 compared to initial
1,5
2
2,5
3
3,5
4
4,5
5
a b
Before At 6 months At 12 months
End
othe
lin-1
(ng
/L)
0
10
20
30
40
50
60
Before At 6 months Before At 6 monts
Dinor-6-keto Dinor-TxB2
ng/m
mol
cre
atin
ine
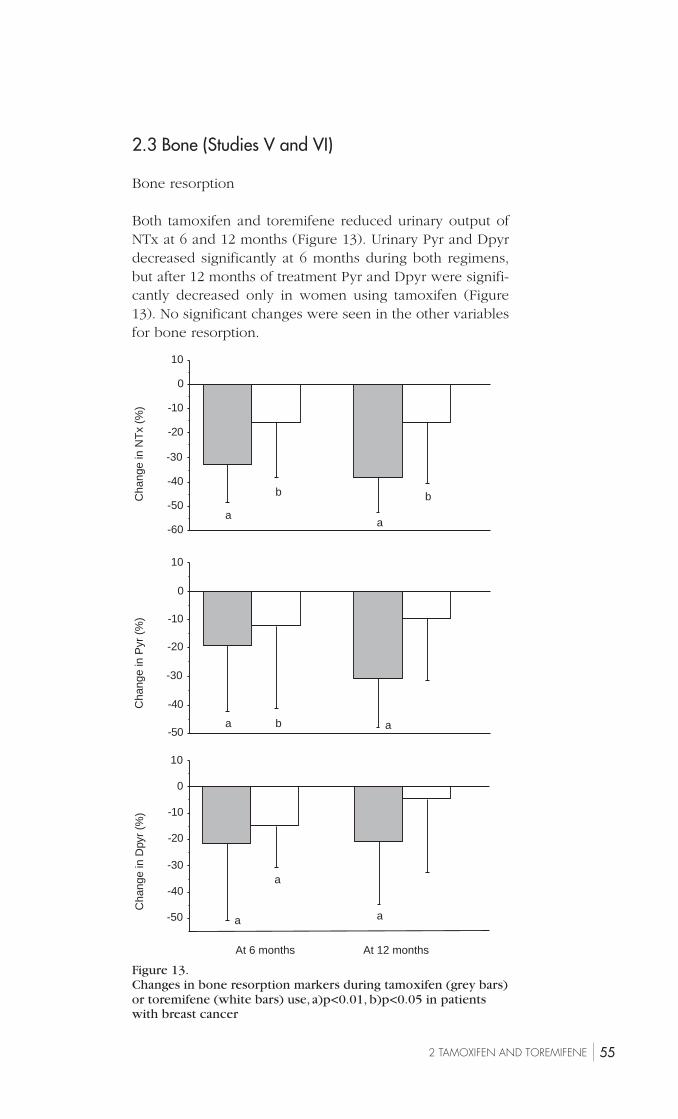
552 TAMOXIFEN AND TOREMIFENE
2.3 Bone (Studies V and VI)
Bone resorption
Both tamoxifen and toremifene reduced urinary output ofNTx at 6 and 12 months (Figure 13). Urinary Pyr and Dpyrdecreased significantly at 6 months during both regimens,but after 12 months of treatment Pyr and Dpyr were signifi-cantly decreased only in women using tamoxifen (Figure13). No significant changes were seen in the other variablesfor bone resorption.
-60
-50
-40
-30
-20
-10
0
10
10
-50
-40
-30
-20
-10
0
-50
-40
-30
-20
-10
0
10
At 6 months At 12 months
aa
b b
a ab
a
a
a
Cha
nge
in N
Tx
(%)
Cha
nge
in P
yr (
%)
Cha
nge
in D
pyr
(%)
Figure 13.Changes in bone resorption markers during tamoxifen (grey bars)or toremifene (white bars) use, a)p<0.01, b)p<0.05 in patientswith breast cancer
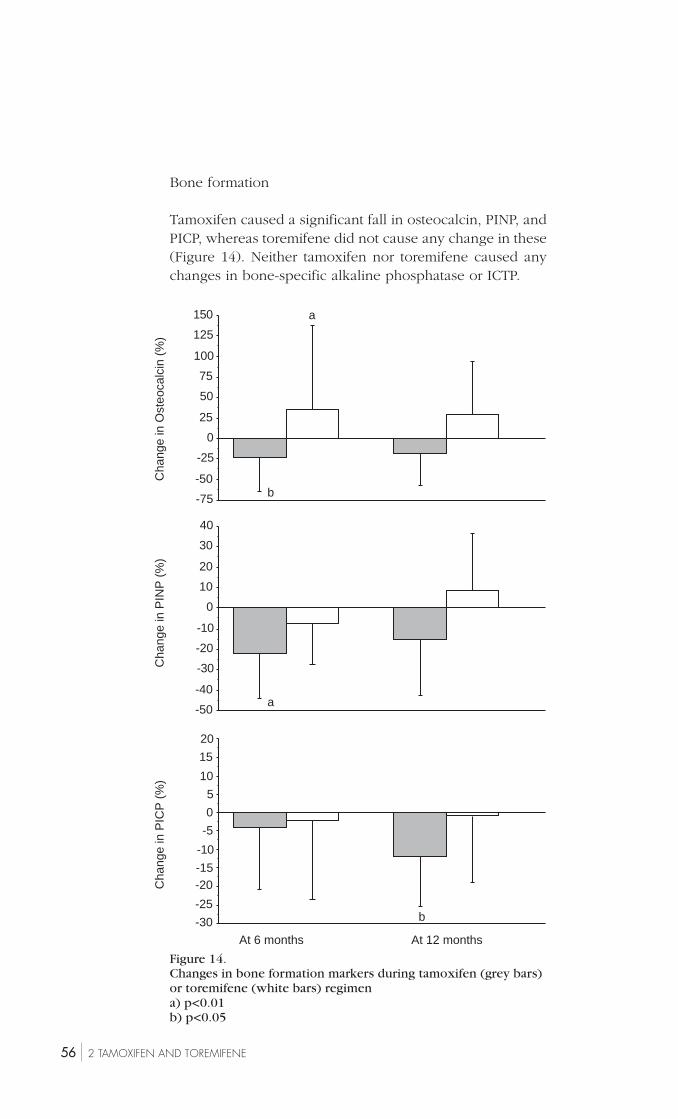
56 2 TAMOXIFEN AND TOREMIFENE
Figure 14.Changes in bone formation markers during tamoxifen (grey bars)or toremifene (white bars) regimena) p<0.01b) p<0.05
At 6 months At 12 months
-50
-40
-30
-20
-10
0
10
20
30
40
20
-30
-25
-20-15
-10
-5
0
5
10
15
-75
-50
-25
0
25
50
75
100
125
150 a
b
a
b
Cha
nge
in O
steo
calc
in (
%)
Cha
nge
in P
INP
(%
)C
hang
e in
PIC
P (
%)
Bone formation
Tamoxifen caused a significant fall in osteocalcin, PINP, andPICP, whereas toremifene did not cause any change in these(Figure 14). Neither tamoxifen nor toremifene caused anychanges in bone-specific alkaline phosphatase or ICTP.
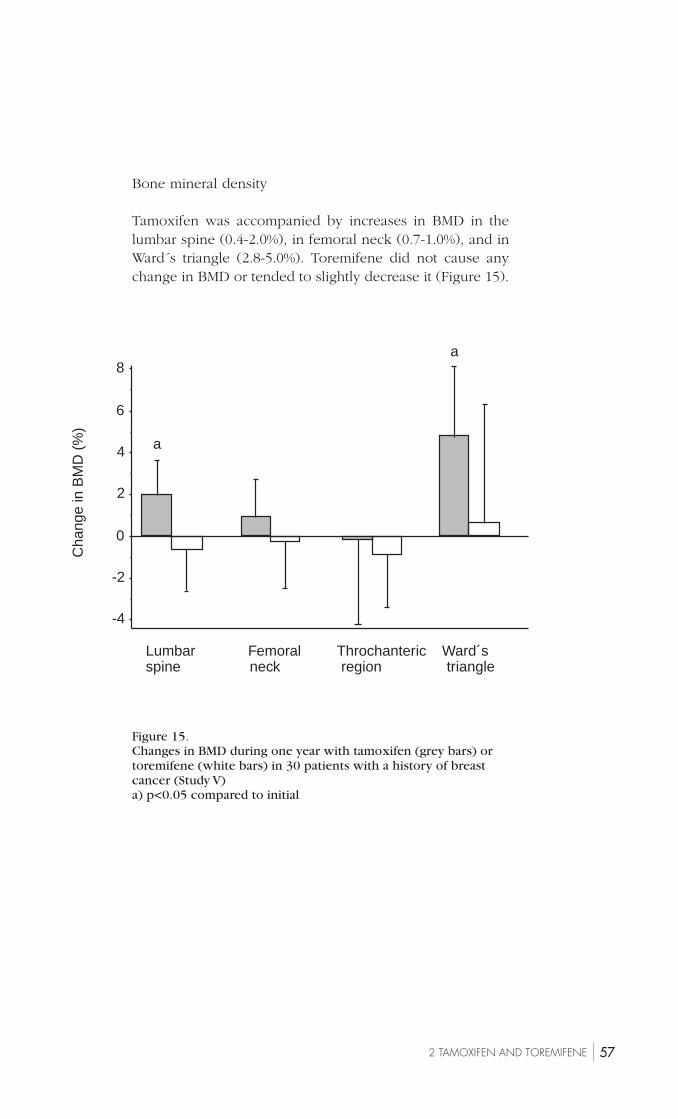
572 TAMOXIFEN AND TOREMIFENE
Figure 15.Changes in BMD during one year with tamoxifen (grey bars) ortoremifene (white bars) in 30 patients with a history of breastcancer (Study V)a) p<0.05 compared to initial
-4
-2
0
2
4
6
8
Lumbar Femoral Throchanteric Ward´sspine neck region triangle
a
a
Cha
nge
in B
MD
(%
)
Bone mineral density
Tamoxifen was accompanied by increases in BMD in thelumbar spine (0.4-2.0%), in femoral neck (0.7-1.0%), and inWard´s triangle (2.8-5.0%). Toremifene did not cause anychange in BMD or tended to slightly decrease it (Figure 15).
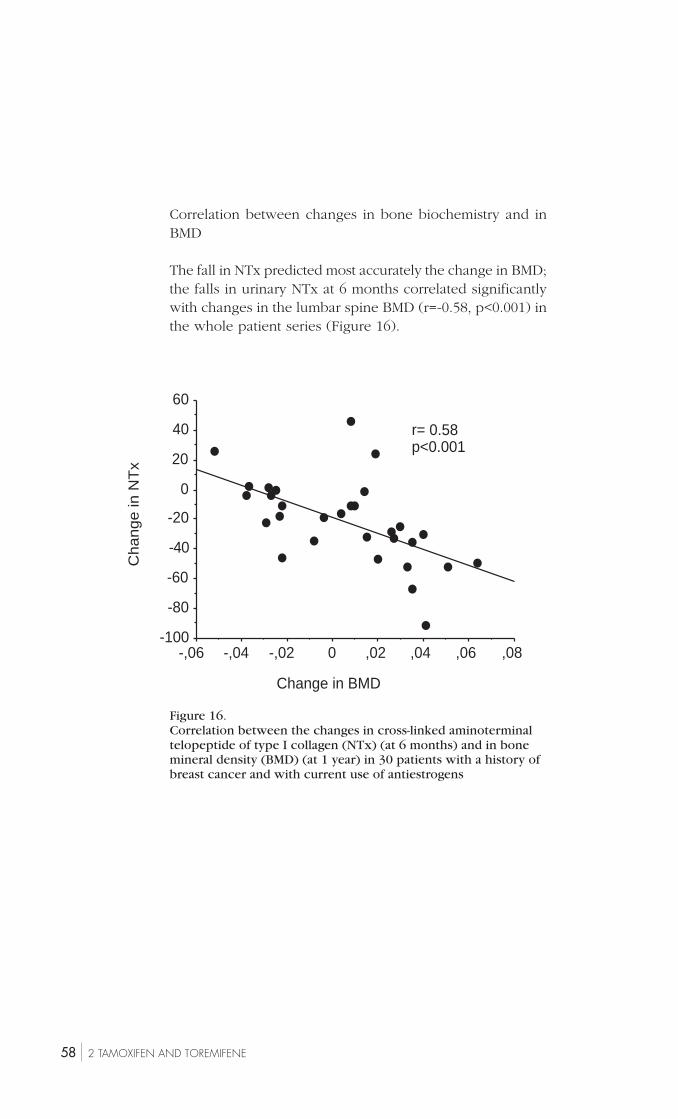
58 2 TAMOXIFEN AND TOREMIFENE
Figure 16.Correlation between the changes in cross-linked aminoterminaltelopeptide of type I collagen (NTx) (at 6 months) and in bonemineral density (BMD) (at 1 year) in 30 patients with a history ofbreast cancer and with current use of antiestrogens
-100
-80
-60
-40
-20
0
20
40
60
-,06 -,04 -,02 0 ,02 ,04 ,06 ,08
r= 0.58p<0.001
Change in BMD
Ch
an
ge
in N
Tx
Correlation between changes in bone biochemistry and inBMD
The fall in NTx predicted most accurately the change in BMD;the falls in urinary NTx at 6 months correlated significantlywith changes in the lumbar spine BMD (r=-0.58, p<0.001) inthe whole patient series (Figure 16).

59VI DISCUSSION
VI DISCUSSION
One in ten Finnish women will be diagnosed with breastcancer during her lifetime (Finnish Cancer Registry 1997).Nowadays breast cancer is diagnosed in an earlier phaseperhaps as a consequence of mammographic screening pro-grams (Garfinkel et al. 1994; Garne et al. 1997; UK Trial ofEarly Detection of Breast Cancer Group 2000), and also thetreatment of breast cancer has improved (Early Breast Can-cer Trialists´ Collaborative Group 1992, 2000). Therefore, inspite of the 100% rise in incidence from the beginning of1970ies, the absolute breast cancer mortality has not increased(Finnish Cancer Registry 1997, Statistics Centrum of Finland;Peto et al. 2000). Therefore clinicians see nowadays increas-ing numbers of women who have survived their breast can-cer. Because of the possible role of estrogen in the etiologyof breast cancer, it has been thought that ERT/HRT can trig-ger the recurrence of breast cancer, and therefore a historyof breast cancer has been regarded as a rather absolute con-traindication for ERT/HRT (Marchant 1994; Colditz 1997;Consensus Statement 1998). However, the rationale of thisdenial has been questioned (Cobleigh et al. 1994; Braendle1998) because the prognosis of breast cancer is presently sogood that most women with a history of breast cancer maydie from other diseases than breast cancer. One factor con-tributing to improved prognosis of breast cancer is the useof antiestrogens (Early Breast Cancer Trialists´ CollaborativeGroup 1992, 1998). This effect must be mediated throughantiestrogenic effect in the breast cancer tissue (Buckley andGoa 1989; Wiseman and Goa 1997), but in some other tis-sues and organs antiestrogens, for example tamoxifen, haveestrogenic effects (McDonald et al. 1995; Grey et al. 1995;Powles et al. 1996; Chang et al 1996). Furthermore, the riskof endometrial cancer has been reported to increase duringthe long-term use of tamoxifen (Early Breast Cancer Trial-ists´ Collaborative Group 1998) which can also be seen asone sign of estrogenic effect. On the other hand, tamoxifencauses or worsens typical menopausal vasomotor symptoms(Buckley and Goa 1989).Toremifene is a newer antiestro-genic compound which has similar antiestrogenic activityon breast cancer tissue to tamoxifen (Pyrhönen et al. 1999),

60 VI DISCUSSION
but so far little has been known about the estrogenic conse-quences of toremifene.
In this study, it has been evaluated the usefulness andsafety of ERT/HRT and compared the gynecologic and otherconsequences of tamoxifen and toremifene in postmeno-pausal breast cancer patients.
I studied 131 postmenopausal patients with breast cancerseeking help for menopausal symptoms. From those, 108women had a sound indication for using ERT/HRT, and 88patients finally started ERT/HRT. Forty-three women whodid not start ERT/HRT were followed as a control group. Allpatients were carefully examined at the oncological depart-ment before being included in the trial to ensure that nonehad any recurrence at recruitment. Similar oncological ex-aminations (mammography, tumor marker CA 15-3 meas-urement) were annually repeated during the trial to detectany possible recurrences as soon as possible. The history ofbreast cancer denotes a 1.5- to 2-fold risk of endometrialcancer in these women (Adami et al. 1997). Therefore en-dometrium was assessed by serial histological samples andultrasonography.
The use of estrogen effectively alleviated climacteric symp-toms in these patients. This was expected because no dataimply that this effect of ERT/HRT should be different in thesepatients. A high continuation rate (88.4%) of ERT/HRT pro-vides an additional proof of the good efficacy of ERT/HRTin the control of vasomotor symptoms, although the chanceto see always the same gynecologist, often after a very shortnotice, may have contributed to the high compliance.
The overall risk of recurrence or contralateral breast can-cer was similar in patients with (3%) or without ERT/HRT(4%). This result is in line with previous data showing noexcess risk of relapse during 2-3 years of use of ERT/HRT(Table 14). Furthermore, although breast cancer per se indi-cates an increased risk of endometrial cancer (Adami et al.1997), no primary endometrial cancer developed during thefollow-up. Even if our patient series was small and not ran-domized or placebo-controlled, and control patients had ahigher risk of cancer recurrece than ERT/HRT patients, ourdata on breast safety provides an important piece of infor-mation to clinicians.Yet I would like to emphasize that toprove the final safety of ERT/HRT in breast cancer patients,much larger prospective and preferably placebo-controlledtrials are needed, and the follow-up time must be at least in
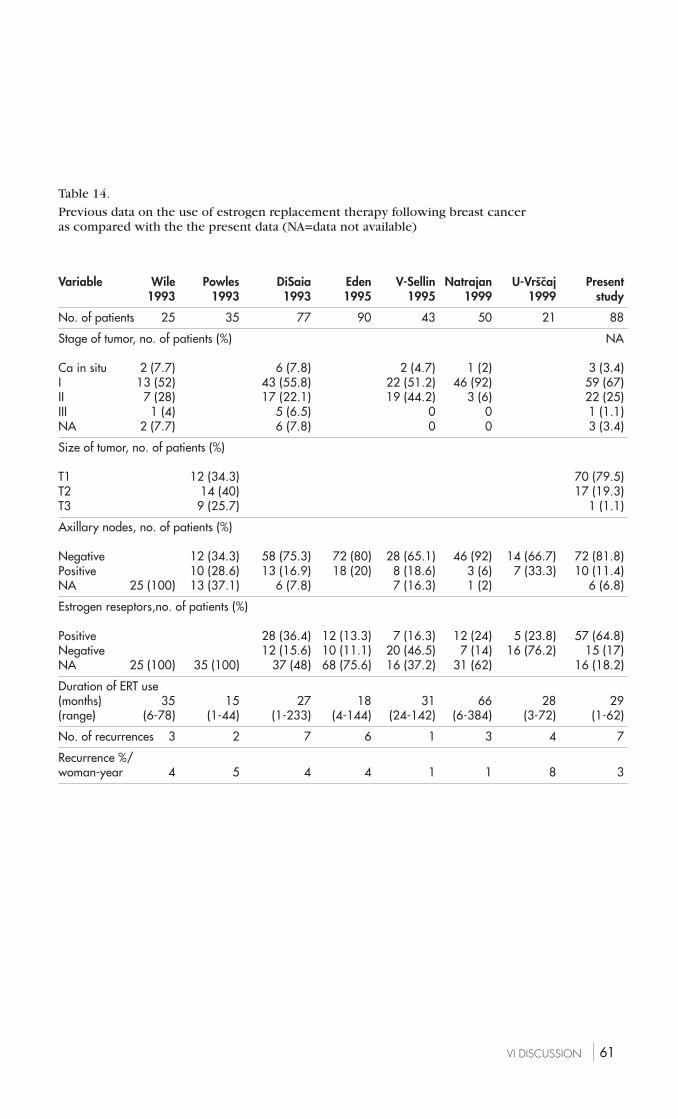
61VI DISCUSSION
Table 14.
Previous data on the use of estrogen replacement therapy following breast canceras compared with the the present data (NA=data not available)
Variable Wile Powles DiSaia Eden V-Sellin Natrajan U-Vrs̆c̆aj Present1993 1993 1993 1995 1995 1999 1999 study
No. of patients 25 35 77 90 43 50 21 88
Stage of tumor, no. of patients (%) NA
Ca in situ 2 (7.7) 6 (7.8) 2 (4.7) 1 (2) 3 (3.4)I 13 (52) 43 (55.8) 22 (51.2) 46 (92) 59 (67)II 7 (28) 17 (22.1) 19 (44.2) 3 (6) 22 (25)III 1 (4) 5 (6.5) 0 0 1 (1.1)NA 2 (7.7) 6 (7.8) 0 0 3 (3.4)
Size of tumor, no. of patients (%)
T1 12 (34.3) 70 (79.5)T2 14 (40) 17 (19.3)T3 9 (25.7) 1 (1.1)
Axillary nodes, no. of patients (%)
Negative 12 (34.3) 58 (75.3) 72 (80) 28 (65.1) 46 (92) 14 (66.7) 72 (81.8)Positive 10 (28.6) 13 (16.9) 18 (20) 8 (18.6) 3 (6) 7 (33.3) 10 (11.4)NA 25 (100) 13 (37.1) 6 (7.8) 7 (16.3) 1 (2) 6 (6.8)
Estrogen reseptors,no. of patients (%)
Positive 28 (36.4) 12 (13.3) 7 (16.3) 12 (24) 5 (23.8) 57 (64.8)Negative 12 (15.6) 10 (11.1) 20 (46.5) 7 (14) 16 (76.2) 15 (17)NA 25 (100) 35 (100) 37 (48) 68 (75.6) 16 (37.2) 31 (62) 16 (18.2)
Duration of ERT use(months) 35 15 27 18 31 66 28 29(range) (6-78) (1-44) (1-233) (4-144) (24-142) (6-384) (3-72) (1-62)
No. of recurrences 3 2 7 6 1 3 4 7
Recurrence %/woman-year 4 5 4 4 1 1 8 3

62 VI DISCUSSION
Table 15.Studies reporting on the incidences of tamoxifen–associatedendometrial pathologies
Author No of study Polyps Hyperplasia CarcinomaPopulation % % %
Lahti et al. 1993 51 33.3 3.9 2.0Kedar et al. 1994 61 8.2 16.4 0Gibson et al. 1996 75 13.3 1.3 8.0Cohen et al. 1997 175 8.0 15.4 0Marconi et al. 1997 101 43.6 8.9 2.0Ozsener et al. 1998 104 4.8 16.3 3.8Seoud et al. 1999 67 10.4 4.5 1.5Cohen et al. 1999 261 11.5 8.4 0.4Barakat et al. 2000 111 4.5 2.7 0Gerberet et al. 2000 247 5.7 3.2 1.2
the order of decades. In practice such studies are difficult toarrange and perhaps even unethical. Amelioration of climac-teric symptoms during ERT/HRT reveals the code of treat-ment, and then it is no longer genuinely “placebo-control-led”. Moreover, how can a physician offer a placebo to asymptomatic climacteric patient wishing to receive estrogen.We can hope that newer SERM´s will be useful and safe andthus replace the use of ERT/HRT in breast cancer survivors.
Tamoxifen and toremifene showed both antiestrogenic andestrogenic effects in our patients. They similarly worsenedvasomotor climacteric symptoms, but fortunately these symp-toms were tolerable and/or alleviated by time during thetrial, and caused the discontinuation of antiestrogens only infive patients (3%). Breast cancer patients have a 1.6-fold riskof endometrial cancer compared to healthy women (Adamiet al 1997), and previous data imply that tamoxifen use stillincreases this risk to 2-4-fold (Early Breast Cancer Trialists´Collaborative Group 1998). No similar epidemiological evi-dence exists for the carcinogenic effect of toremifene.Tamoxifen has been shown to increase the endometrial thick-ness and to cause the proliferation or hyperplasia of en-dometrium, as well as endometrial polyps (Table 15) (Lahtiet al. 1993; Kedar et al. 1994; Gibson et al. 1996; Cohen et al.1997; Marconi et al. 1997; Ozsener et al. 1998; Seoud et al.1999; Cohen et al. 1999; Barakat et al. 2000; Gerberet et al.2000). In our study tamoxifen and toremifene caused a sim-ilar thickening in the endometrium but this did not correlatewith the histology of the endometrium. The incidence ofproliferative endometrium, which was before the start of reg-imens 20.4% and 20.0% in tamoxifen and toremifene users,

63VI DISCUSSION
respectively, increased more markedly in women usingtamoxifen (47.8%) than in those using toremifene (32.2%).Furthermore, the incidence of endometrial polyps was high-er in patients using tamoxifen. These findings are in contra-diction to the results of the previous prospective compari-son between tamoxifen and toremifene showing the equalnumber of endometrial polyps and proliferative endometrialsamples in the both groups (Tomas et al. 1995). One possi-ble explanation to this contradiction might be the shorterfollow-up time and also the smaller number of study partic-ipants in the study of Tomas et al. In our study, yet only onepatient using toremifene developed endometrial carcinoma,which was detected at 12 months´ follow-up visit. Thusthe incidence of endometrial cancer in antiestrogen users(3/10 000 women-years) was lower than that in the Finnishgeneral population of the same age (6/10 000 women-years;Finnish Cancer Registry 1997). Despite the limited numberof patients and short follow-up time, data in this study showthe safety of antiestrogens towards endometrium at least ifthe duration of exposure does not exceed three years. Yet aword of caution is needed because a 2-4-fold risk of en-dometrial cancer in tamoxifen users has been seen in largeepidemiological studies (Fisher et al. 1994; Early Breast Can-cer Trialists´ Collaborative Group 1998). Therefore a closeendometrial surveillance has been recommended for the long-term users of antiestrogens (Barakat 1996). The results ofthis study suggest that such a surveillance is not neededduring the first 2-3 years of treatment. Based on animal stud-ies, toremifene may be less estrogenic than tamoxifen (Hir-simäki et al. 1993). This may be reflected in women as well,because toremifene had a weaker estrogenic effect in theendometrium than did tamoxifen. At the present it could bestated that large and long-term epidemiological data are need-ed for the assessment of endometrial safety in the long-termuse of toremifene.
Tamoxifen has been shown to protect against myocardialinfarction (McDonald et al. 1995). The mechanism of thisaction of antiestrogens is poorly understood, although ben-eficial changes in blood lipids are likely (Love et al. 1994;Grey et al. 1995; Gylling et al. 1995; Saarto et al. 1996). It isalso known that the vascular wall and endothelium are ofimportance for vascular health (Ylikorkala et al. 1986; Mik-kola et al. 1995), but no data existed on the effect of tamoxifenor toremifene on these tissues.

64 VI DISCUSSION
Therefore, an important finding of this study was that nei-ther tamoxifen nor toremifene affected the production ofprostacyclin, TxA
2, or NO. In contrast, toremifene, but not
tamoxifen, decreased the release of ET-1. The vascular func-tion was also assessed directly by Doppler equipment.Toremifene significantly reduced the pulsatility index (PI) inthe uterine artery, reflecting a vasodilatory effect of toremifenein this artery, whereas this effect was not seen with tamoxifen.In principle the vasodilatory effect of toremifene resemblesthat of estrogens (Cacciatore et al. 1998). The toremifene-induced vasodilatation at least in the uterine artery may havebeen caused, in part, by the fall in ET-1. If a similar vasodil-atation would appear to be systemic affecting the vascularbed, toremifene may prove to have in that way cardiovascu-lar protective properties; yet long-term detailed data on vas-cular physiology during antiestrogen use are still needed.
Bone is also one target organ for the action of estrogenand antiestrogens, and this is supported by the presence ofboth α- and β-estrogen receptors in bone (Gustafsson 1999).In our patients tamoxifen increased BMD, whereas toremifeneonly prevented the menopause-induced bone loss. This find-ing of the favorable effect of tamoxifen on bone is in linewith some previous data (Grey et al. 1995; Powles et al 1998;Chang et al. 1996), but the bone-preserving effect oftoremifene is new. This study shows that by measuring uri-nary NTx, it is possible to predict the subsequent change inBMD. This data does not allow to deduce the reasons for thedifference in the bone effects of tamoxifen and toremifenebut, naturally, one can ask if the dosages used were reallyequipotent and if equipotency is uniform. It can be possiblethat estrogen receptors in bone cells are stimulated more bytamoxifen than by toremifene. Furthermore, it can be possi-ble that tamoxifen and toremifene have similar effect on boneif used for longer periods, but the first year data of this studydo not allow further conclusion.
Summing up our comparative data I may conclude thattamoxifen appears slightly more estrogenic than toremifeneon the endometrium and bone, whereas toremifene hasstronger estrogenic vasodilatory effect. Our results collectedduring relatively short follow-up time do not allow us todeduce if these differences persist during more prolongeduse of antiestrogens and if they lead to clinically significantchanges in patients´ outcomes.

65VII SUMMARY AND CONCLUSION
VII SUMMARY AND CONCLUSION
One hundred and thirty-one postmenopausal women with ahistory of breast cancer were studied. Eighty-eight patientsstarted ERT/HRT and 43 patients served as controls; the ini-tiation of ERT/HRT was not randomized and the study groupswere not strictly comparable. The patients were followed amean of 2.5 years. In 88 women starting ERT/HRT, five re-currences and two contralateral breast cancers were detect-ed. In the control group (n=43), four patients developedrecurrence and one a contralateral breast cancer. The riskper year in ERT/HRT users was 7/216 woman-years (3%)and in control group 5/111 woman-years (4%). Thus ERT/HRT did not increase the risk of breast cancer recurrenceduring this rather short period of time.
I also followed 167 women who started either tamoxifen(20 mg/day, n=84) or toremifene (40 mg/day, n=83) as anadjuvant therapy for st II-III breast cancer. The mean follow-up time was 2.3 years. Tamoxifen and toremifene causedsimilar vasomotor symptoms in postmenopausal breast can-cer patients. During the follow-up, only one endometrialcancer developed in a woman using toremifene. As a sign ofestrogenic effect, the rate of proliferative endometrium in-creased from 20.4% to 47.8% in tamoxifen users, whereasthe rise from 20.0% to 32.2% in toremifene users was smaller(p<0.0001). Also the number of endometrial polyps duringthe antiestrogen use was greater in the tamoxifen group (17polyps) than in the toremifene group (7 polyps) (p<0.05).
Prostacyclin and TxA2 may be mediators responsible for
the favorable cardiovascular effect of estrogen. Neithertamoxifen nor toremifene caused any change in the produc-tion of these vasoactive agents. Toremifene decreased thelevel of vasoconstrictive ET-1 by 12.9% at 6 months (p=0.01),and by 9.2% at 12 months (p=0.06), whereas tamoxifen didnot have any effect on ET-1.
Both tamoxifen and toremifene prevented postmenopau-sal bone loss, as assessed by bone mineral density (BMD)measurement. Tamoxifen increased BMD by 0.4-5%, where-as toremifene did not increase it. Bone preserving effect could
66 VII SUMMARY AND CONCLUSION
also be verified by measuring various bone markers reflect-ing bone turn-over. Both tamoxifen and toremifene causeda fall in urinary aminoterminal cross-linked telopeptide (NTx),pyridinoline, and deoxypyridinoline, and tamoxifen causeda fall in serum osteocalcin, aminoterminal and carboxyter-minal propeptide of type I procollagen. Yet only NTx showedcorrelations to the subsequent changes in BMD.
Based on the findings it is possible to make the followingconclusions:
1. Short lasting hormone replacement therapy in womenwith a history of breast cancer is not related to a detri-mental effect on the number of recurrences due to thisdisease, but follow-up of this population was short andthe number of patients was small.
2. Tamoxifen and toremifene do not cause premalignant ormalignant endometrial lesions during the first 2-3 yearsof their use. Thus close endometrial surveillance, as hasoften been advocated recently, is not be warranted dur-ing the first three years of antiestrogen treatment provid-ing that patients are asymptomatic.
3. The probable cardiovascular protection provided by an-tiestrogens is unlikely to be associated with any changesin prostacyclin or TxA
2. However, toremifene reduces
ET-1 and arterial resistance at least in the uterine artery.4. Both tamoxifen and toremifene protects against bone loss
in postmenopausal breast cancer patients.
67ACKNOWLEDGEMENTS
ACKNOWLEDGEMENTS
This study was carried out at the Department of Obstetricsand Gynecology, Helsinki University Central Hospital, Uni-versity of Helsinki, Finland during the years 1993-1999. I amvery grateful to Professor Olavi Ylikorkala, M.D., Ph.D. andProfessor Markku Seppälä, M.D., Ph.D., Heads of the De-partment of Obstetrics and Gynecology, Helsinki UniversityCentral Hospital, for providing me the excellent facilities tocarry out this study. I would also like to thank the personnelof the department and my colleagues for their support.
I gratefully acknowledge:
Professor Olavi Ylikorkala, my supervisor, for guiding mewith enthusiasm and unending patience in this work throughthe years. He always found time for me and encouraged mein many arduous days. Without his help and guidance I wouldnever have completed this thesis.
Docent Aila Tiitinen, M.D., Ph.D., for introducing me to thepractice of clinical research. I appreciate very highly her ex-perience in clinical work which has been an irreplaceableexample for me. I also express my deepest gratitude forsupporting and helping me in many study problems as wellas in personal life.
Professor Antti Kauppila, M.D., Ph.D. and Docent GuillermoBlanco, M.D., Ph.D., the official reviewers, for their interestand careful review of the final manuscript. Their valuablecomments and constructive criticism greatly improved thetext.
Professor Seppo Pyrhönen, M.D., Ph.D. and Docent PäiviHietanen, M.D., Ph.D., for their collaboration during the dif-ferent phases of this study. Their viewpoints, comments, andkindly support have been necessary for this work.
Docent Bruno Cacciatore, M.D., Ph.D., Docent Torsten Wahl-ström, M.D., Ph.D., Docent Lasse Viinikka, M.D., Ph.D. andMr. Hans-Jürgen Roth, Head of Laboratory Group, for theirexcellent scientific work as collaborators and co-authors ofthe published articles.
68 ACKNOWLEDGEMENTS
Ms. Jaana Matero, Ms. Teija Karkkulainen, Ms. Marja-LeenaPekonen, Mrs. Eira Halenius, and Ms. Marjatta Vallas, fortheir excellent assistance.
Dr. Martti Törnwall, M.D., Ph.D., Medical Director of LeirasOy and Dr. Juhani Elo, M.D., Ph.D., Director of Medical Unitand Health Economics of Leiras Oy for positive and encour-aging attitude to this work, without which it would neverhave been possible to finalise this thesis.
Ms. Carol Norris and Mrs. Auni Aflatuni, for the languagerevision of the manuscripts and this doctoral thesis.
Ms. Raili Alanne, Mrs. Kirsi Siivonen, Mrs. Eila Niemi and Mr.Mika Järviö, for providing me library services.
Mrs. Laila Selkinen and Mrs. Pirjo Peippo-Lavikka, for theirkind help in many practical matters.
Ms. Hanna Metsä-Heikkilä, for the graphic design of thisthesis.
My mother Niina, and my father Aarne, for their supportduring my whole life. They have offered me resources for agood life and happiness.
My husband Tauno, for his love and patience during the lastyears of this study. He never questioned the rationale of thiswork, and his help in every day life has been irreplaceable.
My two sons, Mikko and Markus, for all the love and happi-ness they have brought. They are the best that has hap-pened to me during my life.
This study was financially supported by Helsinki UniversityCentral Hospital Research Funds.
Helsinki, May 2001
69REFERENCES
REFERENCES
Abner AL, Collins L, Peiro G et al. Correlation of tumor size and
axillary lymph node involvement with prognosis in patients
with T1 breast carcinoma. Cancer 83:2502-2508, 1998.
Adachi JD, Sargeant EJ, Sagle MA et al. A double-blind randomized
controlled trial of the effects of medroxyprogesterone acetate
on bone density of women taking oestrogen repalcement ther-
apy. Br J Obstet Gynaecol 104:64-70, 1997.
Adami H-O, Bergström R, Weiderpass, Persson I, Barlow L,
McLaughlin JK. Risk for endometrial cancer following breast
cancer: a prospective study in Sweden. Cancer Causes Control
8:821-827, 1997.
Alanko A, Mäkinen J, Scheinin TM, Topllanen E-M, Vihko R. Cor-
relation of estrogen and progesterone receptors and histologi-
cal grade in human primary breast cancer. Acta Path Micobiol
Immunol Scand 92:311-315, 1984.
Andersson K, Pedersen AT, Mattson L-Å, Milsom I. Swedish gyne-
cologists´ and general pactitioners´ views on the climacteric
period: Knowledge, attitudes and management strategies. Acta
Obstet Gynecol Scand 77:909-916, 1998.
Anker G, Lonning PE, Ueland PM, Refsum H, Lien EA. Plasma
levels of the atherogenic amino acid homocysteine in post-
menopausal women with breast cancer treated with tamoxifen.
Int J Cancer 60:365-368, 1995.
Barakat RR, Gilewski TA, Almadrones L et al. Effect of adjuvant
tamoxifen on the endometrium in women with breast cancer:
a prospective study using office endometrial biopsy. J Clin Oncol
18:3459-3463, 2000.
Barakat RR. Tamoxifen and endometrial neoplasia. Clin Obstet
Gynecol 39;629-640, 1996.
Barrett-Connor E, Grady D. Hormone replacement therapy, heart
disease, and other considerations. Annu Rev Public Health 19:55-
72, 1998.
Barrett-Connor E, Laakso M. Ischemic heart disease risk in post-
menopausal women. Effect of estrogen use on glucose and
insulin levels. Arteriosclerosis 10:531-534, 1990.
Blanco G, Alavaikko M, Ojala A et al. Estrogen and progesterone
receptors in breast cancer: Relationships to tumour histopa-
thology and survival of patients. Anticancer Res 4:383-390, 1984.

70 REFERENCES
Braendle W. Hormone replacement therapy in women with breast
cancer. Anticancer Res 18: 2253-2256, 1998.
Brincat M, Studd JWW. Menopause – a multisystem disease.
Baillière´s Clin Obstet Gynecol 2: 289-316, 1988.
Broeders MJM, Verbeek ALM. Breast cancer epidemiology and
risk factors. Q J Nucl Med 41:179-188, 1997.
Buckley MM-T, Goa KL. Tamoxifen. A reappraisal of its pharma-
codynamic and pharmacokinetic properties, and therapeutic
use. Drugs 37:451-490, 1989.
Bush TL, Barrett-Connor E, Cowan LD et al. Cardiovascular mor-
tality and noncontraceptive use of estrogen in women: results
from the Lipid Research Clinics Program Follow-up Study. Cir-
culation 75:1102-1109, 1987.
Cacciatore B, Paakkari I, Hasselblatt R et al. Randomized compar-
ison between long-term effects of oral and transdermal hor-
mone replacement on 24-hour ambulatory blood pressure in
postmenopausal women. Am J Obstet Gynecol, 184:904-909,
2001.
Cacciatore B, Paakkari I, Toivonen J, Tikkanen MJ, Ylikorkala O.
Randomized comparison of oral and transdermal hormone re-
placement on the carotid and uterine artery resistance to blood
flow. Obstet Gynecol 92:563-568, 1998.
Calvo MS, Eyre DR, Gundberg M. Molecular basis and clinical ap-
plication of biological markesr of bone turnover. Endocrine
Rev 17:333-368, 1996.
Carnero P, Shih WJ, Gineyts E, Karpf DB, Delmas P. Comparison
of new biochemical markers of bone turnover in late postmen-
opausal osteoporotic women in response to alendronate treat-
ment. J Clin Endocrinol Metab 79:1693-1700, 1994.
Carter CL, Allen C, Henson DE. Relation of tumor size, lymph
node status, and survival in 24 740 breast cancer cases. Cancer
63:181-187, 1989.
Chambers JT, Chambers SK. Endometrial sampling: When? Where?
Why? With what? Clin Obstet Gynecol 35:28-39, 1992.
Chang J, Powles TJ, Ashley SE et al. The effect of tamoxifen and
hormone replacement therapy on serum cholesterol, bone min-
eral density and coagulation factors in healthy postmenopau-
sal women participating in a randomized, controlled tamoxifen
prevention study. Ann Oncol 7:671-675, 1996.
Chlebowski RT, Butler J, Nelson A, Lillington L. Breast cancer che-
moprevention. Tamoxifen: current issues and future prospec-
tive. Cancer 72:1032-1037, 1993.
71REFERENCES
Christiansen C. Menopausal osteoporosis: impact of sex steroid
replacement. In: Adashi EY, Rock JA, Rosenwaks Z, eds. Re-
productive endocrinology, surgery, and technology. Philadel-
phia, Lippincott-Raven Publishers, pp 1826-1839, 1995.
Cicinelli E, Ignarro LJ, Lograno M, Matteo G, Falco N, Schonauer
LM. Acute effects of transdermal estradiol administration on
plasma levels of nitric oxide in postmenopausal women. Fertil
Steril 67:63-66, 1997.
Cinotti GA, Pugliese F. Prostaglandins and hypertension. Am J
Hypertens 2(S):10-15, 1989.
Cobleigh MA, Berris RF, Bush T et al. Estrogen replacement thera-
py in breast cancer survivors. A time for change. JAMA 272:540-
545, 1994.
Coezy E, Borgna J-L, Rochefort H. Tamoxifen and metabolites in
MCF7 cells: correlation between binding to estrogen receptor
and inhibition of cell growth. Cancer Res 42:317-323, 1982.
Cohen I, Altaras MM, Lew S, Tepper R, Beyth Y, Ben-Baruch G.
Ovarian endometrioid carcinoma and endometriosis develop-
ing in a postmenopausal breast cancer patient during tamoxifen
therapy: a case report and review of the literature. Gynecol
Oncol 55:443-447, 1994.
Cohen I, Altaras MM, Shapira J et al. Different coexisting endome-
trial histological features in asymptomatic postmenopausal breast
cancer patients treated with tamoxifen. Gynecol Obstet Invest
43:60-63, 1997.
Cohen I, Azaria R, Aviram R et al. Postmenopausal endometrial
pathologies with tamoxifen treatment: comparison between
hysteroscopic and hysterectomy findings. Gynecol Obstet In-
vest 48:187-192, 1999.
Cohen I, Perel E, Tepper R et al. Dose-dependent effect of tamoxifen
therapy on endometrial pathologies in postmenopausal breast
cancer patients. Breast Cancer Res treat 53:255-262, 1999.
Colditz GA. Estrogen replacement therapy for breast cancer pa-
tients. Oncology 11:1491-1497, 1997.
Colditz GA and Rosner B. Cumulative risk of breast cancer to age
70 years according to risk factor status: Data from the Nurses´
Health Study. Am J Epidemiol 152:950-964, 2000.
Collaborative Group on Hormonal Factors in Breast Cancer. Breast
cancer and hormone replacement therapy: collaborative rean-
alysis of data from 51 epidemiological studies of 52 705 wom-
en with breast cancer and 108 411 women without breast can-
cer. Lancet 350:1047-1059, 1997.
72 REFERENCES
Collaborative Group on Hormonal Factors in Breast Cancer. Breast
cancer and hormonal contraceptives: collaborative reanalysis
of individual data on 53 297 women with breast cancer and
100 239 women without breast cancer from 54 epidemiological
studies. Lancet 347:1713-1727, 1996.
Colletta AA, Benson JR, Baum M. Alternative mechanisms of ac-
tion of anti-oestrogens. Breast Cancer Res Treat 31:5-9, 1994.
Collins P, Rosano GMC, Jiang C, Lindsay D, Sarrel PM, Poole-Wil-
son PA. Cardiovascular protection by estrogen – a calcium an-
tagonist effect? Lancet 341:1264-1265, 1993.
Compston JE. Prevention and management of osteoporosis. Drugs
53:727-735, 1997.
Conrad J, Gompel A, Pelissier C, Mirabel C, Basdevant A. Fibrino-
gen and plasminogen modifications during oral estradiol re-
placement therapy. Fertil Steril 68:449-453, 1997.
Consensus Statement. Treatment of estrogen deficiency symptoms
in women surviving breast cancer. J Clin Endocrinol Metab
83:1993-2000, 1998.
Cummings SR, Eckert S, Krueger KA et al. The effect of raloxifene
on risk of breast cancer in post-menopausal women. Results
from the MORE randomized trial. JAMA 281:2189-2197, 1999.
Daly E, Gray A, Barlow D, McPherson K, Roche M, Vessey M.
Measuring the impact of menopausal symptoms on quality of
life. BMJ 307:836-840, 1993.
Daly E, Vessey MP, Hawkins MM, Carson JL, Gough P, Marsh S.
Risk of venous thromboembolism in users of hormone replace-
ment therapy. Lancet 348:977-980, 1996.
De Boer H, Blok GJ, Van Lingen A, Teule GJJ, Lips P, Van der Veen
EA. Consequences of childhood-onset growth hormone defi-
ciency for adult bone mass. J Bone Miner Res 9:1319-1326,
1994.
Dennerstein L, Dudley EC, Hopper JL, Guthrie JR, Burger HG. A
prospective population-based study of menopausal symptoms.
Obstet Gynecol 96:351-358, 2000.
Dickson RB, Lippman ME. Estrogenic regulation of growth and
polypeptide growth factor secretion in breast carcinoma. En-
docrine Rev 8:29-43, 1987.
DiSaia PJ, Odicino F, Grosen EA, Cowan B, Pecorelli S, Wile AG.
Hormone replacement therapy in breast cancer. Lancet 342:1232,
1993.
Early Breast Cancer Trialists´ Collaborative Group. Favourable and
unfavourable effects on long-term survival of radiotherapy for
early breast cancer: an overview of the randomized trials. Lan-
cet 355:1757-1770, 2000.
73REFERENCES
Early Breast Cancer Trialists´ Collaborative Group. Systemic treat-
ment of early breast cancer by hormonal, cytotoxic, or im-
mune therapy. Lancet 339:1-5, 71-85, 1992.
Early Breast Cancer Trialists´ Collaborative Group. Tamoxifen for
early breast cancer: an overview of the randomized trials. Lan-
cet 351:1451-1467, 1998.
Eden JA, Bush T, Nand S, Wren BG. A case-control study of com-
bined continuous estrogen-progestin replacement therapy
among women with a personal history of breast cancer. Meno-
pause 2:67-72, 1995.
Ellmén J, Werner D, Hakulinen P et al. Dose-dependent hormonal
effects of toremifene in postmenopausal breast cancer patients.
Cancer Chemother Pharmacol 45:402-408, 2000.
Elston CW and Ellis IO. Pathological prognostic factors in breast
cancer. I. The value of histological grade in breast cancer: ex-
perience from a large study with long-term follow-up. Histopa-
thology 19:403-410, 1991.
Epstein S. Serum and urinary markers of bone remodeling: assess-
ment of bone turnover. Endocrine Rev 9:437-449, 1988.
Eviö S, Tiitinen A, Turpeinen U, Ylikorkala O. Failure of the com-
bination of sequential oral and transdermal estradiol plus nore-
thisterone acetate to affect plasma homocysteine levels. Fertil-
ity and Sterility 74:1080-1083, 2000.
Falkeborn M, Persson I, Adami H-O et al. The risk of acute myo-
cardial infarction after oestrogen and oestrogen-progestogen
replacement. Br J Obstet Gynecol 99:821-828, 1992.
Fink E, Cormier C, Steinmetz P, Kindermans C, Le Bouc Y, Souber-
bielle J-C. Differences in the capacity of several biochemical
bone markers to assess high bone turnover in early meno-
pause and response to alendronate therapy. Osteoporosis Int
11:295-303, 2000.
Finnish Cancer Registry – Institute for Statistical and Epidemiolog-
ical Cancer Research. Cancer Incidence in Finland 1996 and
1997. Cancer Society of Finland, Publication No. 61, 2000.
Fisher B, Costantino JP, Redmond CK et al. Endometrial cancer in
tamoxifen-treated breast cancer Patients: findings from the
National Surgical Adjuvant Breast and Bowel Project (NSABP)
B-14. J Natl Cancer Inst 86:527-537, 1994.
Fisher B, Costantino JP, Wickerham DL, et al. Tamoxifen for pre-
vention of breast cancer: Report of the National Surgical Adju-
vant Breast and Bowel Project P-1 Study. J Natl Cancer Inst
90:1371-1388, 1998.
Franceschi S. Reproductive factors and cancers of the breast, ova-
ry and endometrium. Eur J Clin Oncol 25:1933-1943, 1989.
74 REFERENCES
Freiss G, Prebois C, Rochefort H, Vignon F. Anti-steroidal and anti-
growth factor activities of anti-estrogens. J Steroid Biochem
Molec Biol 37:777-781, 1990.
Gapstur SM, Morrow M, Sellers TA. Hormone replacement therapy
and risk of breast cancer with a favorable histology. Results of
the Iowa Women´s Health Study. JAMA 281:2091-2097, 1999.
Garfinkel L, Boring CC, Heath CW. Changing trends. An overview
of breast cancer incidence and mortality. Cancer 74:222-227,
1994
Garne JP, Aspegren K, Balldin G, Ranstam J. Increasing incidence
of and declining mortality from breast carcinoma. Cancer 79:69-
74, 1997.
Gebara OCE, Mittleman MA, Sutherland P et al. Association be-
tween increased estrogen status and increased fibrinolytic po-
tential in the Framingham Offspring Study. Circulation 91:1952-
1958, 1995.
Gerber B, Krause A, Muller H et al. Effects of adjuvant tamoxifen
on the endometrium in postmenopausal women with breast
cancer: a prospective long-term study using transvaginal ultra-
sound. J Clin Oncol 18:3464-3470, 2000.
Gibson LE, Barakat RR, Venkatraman ES et al. Endometrial pathol-
ogy at dilatation and curettage in breast cancer patients: com-
parison of tamoxifen users and nonusers. The Cancer Journal
2:35-38, 1996.
Goldani von Mühlen D, Kritz-Silverstein D, Barrett-Connor E. A
community –based study of menopause symptoms and estro-
gen replacement in older women. Maturitas 22:71-78, 1995.
Grady D, Gebretsadik T, Kerlikowske K, Ernster V, Petitti D. Hor-
mone replacement therapy and endometrial cancer risk: a meta-
analysis. Obstet Gynecol 85:304-313, 1995.
Grady D, Rubin SM, Petitti DB et al. Hormone therapy to prevent
disease and prolong life in postmenopausal women. Ann Int
Med 117:1016-1037, 1992.
Grady D, Wenger NK, Herrington D et al. Postmenopausal hor-
mone therapy increases risk for venous thromboembolic dis-
ease. Ann Intern Med 132:689-696, 2000.
Grenman R, Laine K-M, Klemi PJ et al. Effects of the antiestrogen
toremifene on growth of the Human mammary carcinoma cell
line MCF-7. J Cancer Res Clin Oncol 117:223-226, 1991.
Grey AB, Stapleton JP, Evans MC, Reid IR. The effect of the anti-
estrogen tamoxifen on cardio-vascular risk factors in normal
postmenopausal women. J Clin Endocrinol Metab 80:3191-3195,
1995.
75REFERENCES
Grey AB, Stapleton JP, Evans MC, Tatnell MA, Ames RW, Reid IR.
The effect of the antiestrogen tamoxifen on bone density in
normal late postmenopausal women. Am J Med 99:636-641,
1995.
Grodstein F, Stampfer MJ, Goldhaber SZ et al. Prospective study of
exogenous hormones and risk of pulmonary embolism in wom-
en. Lancet 348:983-987, 1996.
Grodstein F, Stampfer MJ, Manson JE et al. Postmenopausal estro-
gen and progestin use and the risk of cardiovascular disease. N
Engl J Med 335;453-461, 1996.
Gustafsson J-Å. Estrogen receptor ß - a new dimension in estro-
gen mechanism of action. J Endocrinol 163:379-383, 1999.
Gylling H, Pyrhönen S, Mäntylä E, Mäenpää H, Kangas L, Mietti-
nen TA. Tamoxifen and toremifene lower serum cholesterol by
inhibiting of ∆8 -cholestenol conversion to lathosterol in women
with breast cancer. J Clin Oncol 13:2900-2905, 1995.
Hanson DA, Weis MAE, Bollen A-M, Maslan SL, Singer FR, Eyre
DR. A specific immunoassay for monitoring human bone re-
sorption: quantitation of type I collagen cross-linked N-telo-
peptides in urine. J Bone Miner Res 7:1251-1258, 1992.
Hargreaves DF, Knox F, Swindell R, Potten CS, Bundred NJ. Epi-
thelial proliferation and hormone receptor status in the normal
post-menopausal breast and the effects of hormone replace-
ment therapy. Br J Cancer 78:945-949, 1998.
Henderson BE, Paganini-Hill A, Ross RK. Decreased mortality in
users of estrogen replacement therapy. Arch Intern Med 151:75-
78, 1991.
Henderson BE, Paganini-Hill A, Ross RK. Estrogen replacement
therapy and protection from acute myocardial infarction. Am J
Obstet Gynecol 159:312-317, 1988.
Herrington DM, Reboussin DM, Brosnihan KB et al. Effects of
estrogen repalcement on the progression of coronary-artery
atherosclerosis. N Engl J Med 343:522-529, 2000.
Hirsimäki P, Hirsimäki Y, Nimeinen Y, Payne BJ. Tamoxifen induc-
es hepatocellular carcinoma in rat liver: a 1-year study with
two antiestrogens. Arch Toxicol 67:49-54, 1993.
Hofseth LJ, Raafat AM, Osuch JR, Pathak DR, Slomski CA, Haslam
SZ. Hormone replacement therapy with estrogen plus medrox-
yprogesterone acetate is associated with increased epithelial
proliferation in the normal postmenopausal breast. J Clin En-
docrinol Metab 84:4559-4565, 1999.
76 REFERENCES
Holli K, Valavaara R, Blanco G et al. Safety and efficacy results of
a randomized trial comparing adjuvant toremifene and tamoxifen
in postmenopausal patients with node-positive breast cancer. J
Clin Oncol 18:3487-3494, 2000.
Holli K. Adjuvant trials of toremifene vs tamoxifen: the European
experience. Oncology 12:23S-27S, 1998.
Homesley HD, Shemano I, Gams R et al. Antiestrogenic potency
of toremifene and tamoxifen in postmenopausal women. Am J
Clin Oncol 16:117-122, 1993.
Hortobagyi GN. Treatment of breast cancer. N Engl J Med 339:974-
984, 1998.
Hulley S, Grady D, Bush T et al. Randomized trial of estrogen plus
progestin for secondary prevention of coronary heart disease
in postmenopausal women. JAMA 280:605-613, 1998.
Hunt K, Vessey M, McPherson K. Mortality in a cohort of long-
term users of hormone replacement therapy: an updated anal-
ysis. Br J Obstet Gynaecol 97:1080-1086, 1990.
Imthurn B, Rosselli M, Jaeger AW, Keller PJ, Dubey RK. Differen-
tial effects of hormone-replacement therapy on endogenous
nitric oxide (nitrite/nitrate) levels in postmenopausal women
substituted with 17beta-estradiol valerate and cyproterone ace-
tate or medroxy-progesterone acetate. J Clin Endocrinol Metab
82:388-394, 1997.
Jernström H, Frenander J, Fernö M, Olsson H. Hormone replace-
ment therapy before breast cancer diagnosis significantly re-
duces the overall death rate compared with never-use among
984 breast cancer patients. Br J Cancer 80:1453-1458, 1999.
Jick H, Derby LE, Wald Myers M, Vasilakis C, Newton KM. Risk of
hospital admission for idiopathic venous thromboembolism
among users of postmenopausal oestrogens. Lancet
348:981-.983, 1996.
Joensuu H, Pylkkänen L, Toikkanen S. Late mortality from pT1N0M0
breast carcinoma. Cancer 85:2183-2189, 1999.
Joensuu H, Toikkanen S. Identification of subgroups with favora-
ble prognosis in breast cancer, Acta Oncol 31:293-301, 1992.
Jordan VC, Fritz NF, Tormey DC, Endocrine effects of adjuvant
chemotherapy and long-term tamoxifen administration on node-
positive patients with breast cancer. Cancer Res 47:624-630,
1987.
Jukkola A, Tähtelä R, Thölix E et al. Aggressive breast cancer leads
to discrepant serum levels of the type I procollagen propep-
tides PINP and PICP. Cancer Res 57:5517-5520, 1997.
77REFERENCES
Kainu T, Juo S-H H, Desper R et al. Somatic deletions in hereditary
breast cancers implicate 13q21 as a putative novel breast can-
cer susceptibility locus. Proc Natl Acad Sci 97:9603-9608, 2000.
Kallioniemi O-P, Blanco G, Alavaikko M et al. TumouDNA ploidy
as an independent prognostic factor in breast cancer. Br J Can-
cer 56:637-642, 1987.
Kangas L. Introduction to toremifene. Breast Cancer Res Treat
16(S):3-7, 1990.
Kangas L. Review of the pharmacological properties of toremifene.
J Steroid Biochem 36:191-195,1990.
Kedar RP, Bourne TH, Powles TJ et al. Effects of tamoxifen on
uterus and ovaries of postmenopausal women in a randomised
breast cancer prevention trial. Lancet 343:1318-1321, 1994.
Kelsey JL, Gammon MD, John EM. Reproductive factors and breast
cancer. Epidemiol Rews 15:36-47, 1993.
Kenemans P, Scheele F. Hormone replacement therapy in patients
at high risk of developing breast cancer: the use of a combined
risk model. Gynecol Endocrinol 11(S1):17-22, 1997.
Kenny AM, Prestwood KM, Pilbeam CC, Raisz LG. The short term
effects of tamoxifen on bone turnover in older women. J Clin
Endocrinol Metab 80:3287-3291, 1995.
Klemi PJ, Joensuu H, Toikkanen J et al. Aggressiveness of breast
cancers found with and without screening. BMJ 304:467-469,
1992.
Knabbe C, Lippman ME, Wakefield LM et al. Evidence that trans-
forming growth factor-ß is a hormonally regulated negative
growth factor in human breast cancer cells. Cell 48:417-428,
1987.
Krag D, Weaver D, Ashikaga T et al. The sentinel node in breast
cancer: A multicenter validation study. N Engl J Med 339:941-
946, 1998.
Kurman RJ, Kaminsi P, Norris HJ. The behavior of endometrial
hyperplasia. A long-term study of “untreated” hyperplasia in
170 patients. Cancer 56:403-412, 1985.
Lahti E, Blanco G, Kauppila A, Apaja-Sarkkinen M, Taskinen PJ,
Laatikainen T. Endometrial changes in postmenopausal breast
cancer patients receiving tamoxifen. Obstet Gynecol 81:660-
664, 1993.
Lahti E, Vuopala S, Kauppila A, Blanco G, Ruokonen A, Laatikai-
nen T. Maturation of vaginal and endometrial epithelium in
postmenopausal breast cancer patients receiving long-term
tamoxifen. Gynecol Oncol 55:410-414, 1994.
78 REFERENCES
Lau TK, Wan D, Yim SF, Sanderson JE, Haines CJ. Prospective,
randomized, controlled study of the effect of hormone replace-
ment therapy on periferal blood flow velocity in postmeno-
pausal women. Fertil Steril 70:284-288, 1998.
Lind L, Granstam SO, Milligard J. Endothelium-dependent vasodil-
atation in hypertension: a review. Blood Press 9:4-15, 2000.
Lindheim SR, Duffy DM, Kojima T, Vijod MA, Stanczyk FZ, Lobo
RA. The route of administration influences the effect of estro-
gen on insulin sensitivity in postmenopausal women. Fertil Steril
62:1176-1180, 1994.
Lindsay R, Hart DM, Forrest C, Baird C. Prevention of spinal oste-
oporosis in oophorectomised women. Lancet 2:1151-1154, 1980.
Lindsay R, Tohme JF. Estrogen treatment of patients with estab-
lished postmenopausal osteoporosis. Obstet Gynecol 72:290-
295, 1990.
Looker AC, Bauer DC, Chesnut III CH et al. Clinical use of bio-
chemical markers of bone remodeling: Current status and fu-
ture directions. Osteoporos Int 11:467-480, 2000.
Looker AC, Johnston CC Jr, Wahner HW, et al. Prevalence of low
femoral bone density in older US women from NHANES III. J
Bone Miner Res 10:796-802, 1995.
López-Otín C, Diamandis EP. Breast and prostate cancer: An anal-
ysis of common epidemiological, genetic, and biochemical fea-
tures. Endocrine Rews 19:365-396, 1998.
Love RR, Cameron L, Connell BL, Leventhal H. Symptoms associ-
ated with tamoxifen treatment in postmenopausal women. Arch
Intern Med 151:1842-1847, 1991.
Love RR, Wiebe DA, Feyzi JM, Newcomb PA, Chappell RJ. Effects
of tamoxifen on cardiovascular risk factors in postmenopausal
women after 5 years of treatment. J Natl Cancer Inst 86: 1534-
1539, 1994.
Marchant DJ. Supplemental estrogen replacement. Cancer 74:512-
517, 1994.
Marconi D, Exacoustos C, Cangi B et al. Transvaginal sonographic
and hysteroscopic findings in postmenopausal women receiv-
ing tamoxifen. J Am Assoc Gynecol Laparosc 4:331-339, 1997.
Marcus R. The nature of osteoporosis. J Clin Endocrinol Metab
81:1-5, 1996.
Marsden J, Whitehead M, A´Hern R, Baum M, Sacks N. Are rand-
omized trials of hormone replacement therapy in symptomatic
women with breast cancer feasible? Fertil Steril 73:292-299, 2000.
Masaki T. Endothelins: homeostatic and compensatory actions in
the circulatory and endocrine system. Endocrine Rev 14:256-
268, 1993.
79REFERENCES
Matthews KA, Kuller LH, Wing RR, Meilahn EN, Plantinga P. Prior
to use estrogen replacement therapy, are users healthier than
nonusers? Am J Epidemiol 143:971-978, 1996.
Maxim P, Ettinger B, Spitalny GM. Fracture protection provided by
long-term estrogen treatment. Osteoporosis Int 5:23-29, 1995.
McDonald CC, Alexander FE, Whyte BW, Forrest PA, Stewart HJ.
Cardiac and vascular morbidity in women receiving adjuvant
tamoxifen for breast cancer in a randomised trial. BMJ 311:977-
980, 1995.
McPherson K, Steel CM, Dixon JM. Breast cancer – epidemiology,
risk factors, and genetics. BMJ 309:1003-1006, 1994.
Melkko J, Kauppila S, Niemi S et al. Immunoassay for intact ami-
no-terminal propeptide of human type I procollagen. Clin Chem
42:947-954, 1996.
Mendelsohn ME, Karas RH. Estrogen and the blood vessel wall.
Current Opinion in Cardiology 9:619-626, 1994.
Mettlin C. Breast cancer risk factors. Contributions to planning
breast cancer control. Cancer 69(S): 1904-1910, 1992.
Michaëlsson K, Baron JA, Farahmand BY et al. Hormone replace-
ment therapy and risk of hip fracture: population based case-
control study. BMJ 316:1858-1863, 1998.
Mijatovic V, Kenemans P, Jacobs C, Van Baal WM, Peters-Mullers
ER, van der Mooren MJ. A randomized controlled study of the
effects of 17beta-estradiol-dydrogesterone on plasma homo-
cysteine in postmenopausal women. Obstet Gynecol 91:432-
436, 1998.
Mikkola T, Turunen P, Avela K, Orpana A, Viinikka L, Ylikorkala
O. 17beta-estradiol stimulates prostacyclin, but not endothelin-
1, production in human vascular endothelial cells. J Clin Endo-
crinol Metab 80:1832-1836, 1995.
Miller PD, Baran DT, Bilezikian JP et al. Practical clinical applica-
tion of biochemical markers of bone turnover. J Clin Densitom
2:323-342, 1999.
Miller WR, Ellis IO, Sainsbury JRC, Dixon JM. Prognostic factors.
BMJ 309:1573-1576, 1994.
Moncada S, Palmer RMJ, Higgs EA. Nitric oxide: physiology, patho-
physiology, and pharmacology. Pharmacol Rev 43:109-142, 1991.
Moore M, Bracker M, Sartoris D, Saltman P, Strause L. Long-term
estrogen replacement therapy in postmenopausal women sus-
tains vertebral bone mineral density. J Bone Miner Res 5:659-
664, 1990.
National Agency for Medicines. Finnish Statistics on medicine 1997.
Helsinki 1998.
80 REFERENCES
Natrajan PK, Soumakis K, Gambrell Jr RD. Estrogen replacement
therapy in women with previous breast cancer. Am J Obstet
Gynecol 181:288-295, 1999.
Neven P, Shepherd JH, Lowe DG. Tamoxifen and gynecologist. Br
J Obstet Gynecol 100:893-897, 1993.
Newton KM, LaCroix AZ, McKnight B et al. Estrogen replacement
therapy and prognosis after first myocardial infarction. Am J
Epidemiol 145:269-277. 1997.
O´Brian CA, Liskamp R, Solomon DH, Weinstein IB. Inhibition of
protein kinase C by tamoxifen. Cancer Res 45:2462-2465, 1985.
O´Hanlon DM, Kerin MJ, Kent P, Maher D, Grimes H, Given HF.
An evaluation of preoperative CA 15-3 measurement in prima-
ry breast carcinoma. Br J Cancer 71:1288-1291, 1995.
O´Keefe JH, Kim SC, Hall RR, Cochran VC, Lawhorn SL, McCal-
lister BD. Estrogen replacement therapy after coronary angi-
oplasty in women. J Am Coll Cardiol 29:1-5, 1997.
Oger E, Scarabin P-Y. Assessment of the risk for venous throm-
boembolism among users of hormone replacement therapy.
Drugs & Aging 14:55-61, 1999.
Oursler MJ, Landers JP, Riggs BL, Spelsberg TC. Oestrogen effects
on osteoblasts and osteoclasts. Ann Med 25:361-371, 1993.
Ozsener S, Ozaran A, Itil I, Dikmen Y. Endometrial pathology of
104 postmenopausal breast cancer patients treated with
tamoxifen. Eur J Gynecol Oncol 19:580-583, 1998.
Page DL, Jensen RA, Simpson JF. Routinely available indicators of
prognosis in breast cancer. Breast Cancer Res Treat 51:195-208,
1998.
Pathak DP, Osuch JR, He J. Breast carcinoma etiology. Current
knowledge and new insights into the effects of reproductive
and hormonal risk factors in black and white populations. Can-
cer 88:1230-1238, 2000.
Penotti M, Farina M, Castiglioni E et al. Alteration in the pulsatility
index values of the internal carotid and middle cerebral arter-
ies after suspension of postmenopausal hormone replacement
therapy: a randomized crossover study. Am J Obstet Gynecol
175:606-611, 1996.
Pérez Gutthann S, García Rodríguez LA, Castellsague J, Duque
Oliart A. Hormone replacement therapy and risk of venous
thromboembolism: population based case-control study. BMJ
314:796-800, 1997.
Persson I, Weiderpass E, Bergström R, Schairer C. Risks of breast
and endometrial cancer after estrogen and estrogen-progestin
replacement therapy. Cancer Causes Control.10:253-260, 1999.
81REFERENCES
Petitti DB, Perlman JA, Sidney S. Noncontraceptive estrogens and
mortality: long-term follow-up of women in the Walnut Creek
Study. Obstet Gynecol 70:289-293, 1987.
Peto R, Boreham J, Clarke M, Davies C, Beral V. UK and USA
breast cancer deaths down 25% in year 2000 at ages 20-69
years. Lancet 355:1822, 2000.
Pines A, Fisman EZ, Levo Y et al. The effects of hormone replace-
ment therapy in normal postmenopausal women: Measurements
of Doppler-derived parameters of aortic flow. Am J Obstet
Gynecol 164:806-812, 1991.
Porter M, Penney GC, Russell D, Russell E, Templeton A. A popu-
lation based survey of women´s experience of the menopause.
Br J Obstet Gynaecol 103:1025-1028, 1996.
Powles T, Eeles R, Ashley S et al. Interim analysis of the incidence
of breast cancer in the Royal Marsden Hospital tamoxifen ran-
domised chemoprevention trial. Lancet 352:98-101, 1998.
Powles TJ, Hickish T, Casey S, O´Brien M. Hormone replacement
after breast cancer. Lancet 342:60-61, 1993.
Powles TJ, Hickish T, Kanis JA, Tidy A, Ashley S. Effect of tamoxifen
on bone mineral density measured by dual-energy x-ray ab-
sorptiometry in healthy premenopausal and postmenopausal
women. J Clin Oncol 14:78-84, 1996.
Proudler AJ, Ahmed AIH, Crook D, Fogelman I, Rymer JM, Steven-
son JC. Hormone replacement therapy and serum angiotensin-
converting-enzyme activity in postmenopausal women. Lancet
346:89-90, 1995.
Pukkala E, Tulenheimo-Silfast A, Leminen A. Incidence of cancer
among women using long versus monthly cycle hormonal re-
placement therapy, Finland 1994-1997. Cancer Causes Control
12:111-115, 2001.
Pyrhönen S, Ellmén J, Vuorinen J et al. Meta-analysis of trials com-
paring toremifene with tamoxifen and factors predicting out-
come of antiestrogen therapy in postmenopausal women with
breast cancer. Breast Cancer Res Treat 56:133-143, 1999.
Pyrhönen S, Valavaara R, Modig H et al. Comparison of toremifene
and tamoxifen in postmeno-pausal patients with advanced
breast cancer: a randomized double-blind, the ‘nordic´ phase
III study. Br J Cancer 76:270-277, 1997.
Raudaskoski T, Tomás C, Laatikainen T. Insulin sensitivity during
postmenopausal hormone replacement with transdermal oes-
trogen and levonorgestrel-releasing intra-uterine system. Acta
Obstet Gynecol Scand 78:540-545, 1999.
Riis BJ. The role of bone turnover in the pathophysiology of oste-
oporosis. Br J Obstet Gynecol 103(S):9-15, 1996.
82 REFERENCES
Risteli J, Elomaa I, Niemi S, Novamo A, Risteli L. Radioimmunoassay
for the pyridinoline cross-linked carboxy-terminal telopeptide
of type I collagen: a new serum marker of bone collagen deg-
radation. Clin Chem 39:635-640, 1993.
Robertson JFR and Evans AJ. Diagnosis and prognosis of primary
breast cancer. Q J Nucl Med 41:200-210, 1997.
Robinson SP, Jordan VJ. Antiestrogenic action of toremifene on
hormone-dependent, -independent, and heterogenous breast
tumor growth in the athymic mouse. Cancer Res 49:1758-1762,
1989.
Roodman GD. Advances in bone biology: the osteoclast. Endo-
crine Revs 17:308-332, 1996.
Ross RK, Paganini-Hill A, Wan PC, Pike MC. Effect of hormone
replacement therapy on breast cancer risk: estrogen versus es-
trogen plus progestin. J Natl Cancer Inst 92:328-332, 2000.
Rutqvist LE, Johansson H, Signomklao T, Johansson U, Fornander
T, Wilking N. Adjuvant tamoxifen therapy for early stage breast
cancer and second primary malignancies. J Natl Cancer Inst
87:645-651, 1995.
Rödström K, Bengtsson C, Lissner L, Björkelund C. Pre-existing
risk factor profiles in users and non-users of hormone replace-
ment therapy: prospective cohort study in Gothenburg, Swe-
den. BMJ 319:890-893, 1999.
Saarto T, Blomqvist C, Ehnholm C, Taskinen M-R, Elomaa I. Antia-
therogenic effects of adjuvant antiestrogens: a randomized trial
comparing the effects of tamoxifen and toremifene on plasma
lipid levels in postmenopausal women with node-positive breast
cancer. J Clin Oncol 14:429-433, 1996.
Saarto T, Blomqvist C, Välimäki M, Mäkelä P, Sarna S, Elomaa I.
Clodronate improves bone mineral density in postmenopausal
breast cancer patients treated with adjuvant antiestrogens.Br J
Cancer 75:602-605, 1997.
Schairer C, Lubin J, Troisi R, Sturgeon S, Brinton L, Hoover R.
Menopausal estrogen and estrogen-progestin replacement ther-
apy and breast cancer risk. JAMA 283:485-491, 2000.
Scheele F, Burger CW, Kenemans P. Postmenopausal hormone
replacement in the women with a reproductive risk factor for
breast cancer. Maturitas 33:191-196;1999.
Seoud M, Shamseddine A, Khalil A et al. Tamoxifen and endome-
trial pathologies: a prospective study. Gynecol Oncol 75:15-19,
1999.
Sourander L, Rajala T, Räihä I, Mäkinen J, Erkkola R, Helenius H.
Cardiovascular and cancer morbidity and mortality and sudden
cardiac death in postmenopausal women on estrogen replace-
ment therapy (ERT). Lancet 352:1965-1969, 1998.
83REFERENCES
Stampfer MJ, Colditz GA, Willett WC et al. Postmenopausal estro-
gen therapy and cardiovascular disease. Ten-year follow-up
from the Nurses Health Study. N Engl J Med 325:756-762, 1991.
Sullivan JM, El-Zeky F, Vander Zwaag R, Ramanathan KB. Effect
on survival of estrogen replacement therapy after coronary ar-
tery bypass grafting. Am J Cardiol 79:847-850, 1997.
Sullivan JM, Fowlkes LP. The clinical aspects of estrogen and the
cardiovascular system. Obstet Gynecol 87:36S-43S, 1996.
Sullivan JM, Vander Zwaag R, Hughes JP et al. Estrogen replace-
ment and coronary artery disease. Effect on survival in post-
menopausal women. Arch Intern med 150:2557-2562, 1990.
Söderqvist G. Effects of sex steroids on proliferation in normal
mammary tissue. Ann Med 30:511-524, 1998.
Tabár L, Duffy SW, Vitak B, Chen H-H, Prevost TC. The natural
history of breast carcinoma. What have we learned fron screen-
ing? Cancer 86:449-462, 1999.
The Women´s Health Initiative Study Group. Design of the women´s
health initiative clinical trial and observational study. Control
Clin Trials 19:61-109, 1998.
Theriault RL. Hormone replacement therapy and breast cancer: an
overview. Br J Obstet Gynecol 103(S):87-91, 1996.
Tikkanen MJ. Sex hormones. In Shepherd J, Betteridge J, Illing-
worth R, eds. Lipoproteins in Health and Disease. London: Ar-
nold 1999:967-984.
Tomás E, Kauppila A, Blanco G, Apaja-Sarkkinen M, Laatikainen
T. Comparison between the effects of tamoxifen and toremifene
on the uterus in postmenopausal breast cancer patients. Gyne-
col Oncol 59:261-266, 1995.
Tulppala M, Viinikka L, Ylikorkala O. Thromboxane dominance
and prostacyclin deficiency in habitual abortion. Lancet 337:879-
881, 1991.
Turner RT, Riggs BL, Spelsberg TC. Skeletal effects of estrogen.
Endocrine Rev 15:275-300, 1994.
Turpeinen U and Pomoell U-M. Liquid-chromatographic determi-
nation of total hydroxyproline in urine. Clin Chem 31:828-830,
1985.
UK Trial of Early Detection of Breast Cancer Group. 16-year mor-
tality from breast cancer in the UK Trial of Early Detection of
Breast Cancer. Lancet 353:1909-1914, 1999.
Urs̆ic̆-Vrs̆c̆aj M, Bebar S. A case-control study of hormone replace-
ment therapy after primary surgical breast cancer treatment.
Eur J Surg Oncol 25:146-151, 1999.
Vane JR, Änggård EE, Botting RM. Regulatory functions of the vas-
cular endothelium. N Engl J Med 323:27-36, 1990.
84 REFERENCES
Varas-Lorenzo C, García-Rodríguez LA, Cattaruzzi C, Grazia Tron-
con M, Agostinis L, Pérez-Gutthann S. Hormone replacement
therapy and the risk of hospitalization for venous thromboem-
bolism: a population-based study in Southern Europe. Am J
Epidemiol 147:387-390, 1998.
Ward RL, Morgan G, Dalley D, Kelly PJ. Tamoxifen reduces bone
turnover and prevents lumbar spine and proximal femoral bone
loss in early postmenopausal women. Bone and Mineral 22:
87-94, 1993.
Vassilopoulou-Sellin R, Theriault R, Klein MJ. Estrogen replace-
ment therapy in women with prior diagnosis and treatment for
breast cancer. Gynecol Oncol 65:89-93, 1997.
Vehkavaara S. Westerbacka J, Hakala-Ala-Pietilä T et al. Effect of
estrogen replacement therapy on insulin sensitivity of glucose
metabolism and preresistance and resistance vessel function in
healthy postmenopausal women. J Clin Endocrinol Metab
85:4663-4670, 2000.
Weiss SR, Ellman H, Dolker M. A randomized controlled trial of
four doses of transdermal estradiol for preventing postmeno-
pausal bone loss. Obstet Gynecol 94:330-336, 1999.
Welch GN, Loscalzo J. Homocysteine and atherothrombosis. N
Engl J Med 338:1042-1050, 1998.
Veronesi U, Maisonneuve P, Costa A et al. Prevention of breast
cancer with tamoxifen: preliminary findings from the Italian
randomised trial among hysterectomised women. Lancet 352:93-
97, 1998.
Westhoff C, Heller D, Drosinos S, Tancer L. Risk factors for hyper-
plasia-associated versus atrophy-associated endometrial carci-
noma. Am J Obstet Gynecol 182:506-508, 2000.
Widrich T, Bradley LD, Mitchinson AR, Collins RI. Comparison of
saline infusion sonography with office hysteroscopy for the
evaluation of the endometrium. Am J Obstet Gynecol 174:1327-
1334, 1996.
Viinikka L and Ylikorkala O. Measurement of thromboxane B2 in
human plasma or serum by radio-immunoassay. Prostagland-
ins 20:759-766, 1980.
Viinikka L. Nitric oxide as a challenge for the clinical chemistry
laboratory. Scand J Clin Lab Invest 56: 577-581, 1996.
Wiklund I, Berg G, Hammar M, Karlberg J, Lindgren R, Sandin K.
Long-term effect of transdermal hormonal therapy on aspects
of quality of life in postmenopausal women. Maturitas 14:225-
236, 1992.
85REFERENCES
Wiklund I, Karlberg J, Mattsson L-Å. Quality of life of postmeno-
pausal women on a regimen of transdermal estradiol therapy:
a double-blind palcebo-controlled study. Am J Obstet Gynecol
168:824-830, 1993.
Wilcox JG, Hatch IE, Gentzschein E, Stanczyk FZ, Lobo RA. En-
dothelin levels decrease after oral and nonoral estrogen in
postmenopausal women with increased cardiovascular risk fac-
tors. Fertil Steril 67:273-277, 1997.
Wild RA. Estrogen: effects on the cardiovascular tree. Obstet Gyne-
col 87(S):27-35, 1996.
Wile AG, Opfell RW, Margileth DA. Hormone replacement therapy
in previously treated breast cancer patients. Am J Surg 165:372-
375, 1993.
Wiseman LR, Goa KL. Toremifene. A review of its pharmacologi-
cal properties and clinical efficacy in the management of ad-
vanced breast cancer. Drugs 54:141-160, 1997.
Vogel RA. Coronary risk factors, endothelial function, and athero-
sclerosis: a review. Clin Cardiol 20:426-432, 1997.
Voigt LF, Weiss NS, Chi J, Daling JR, McKnight B, van Belle G.
Progestogen supplementation of exogenous estrogens and the
risk of endometrial cancer. Lancet 338:274-277, 1991.
Wolf PH, Madans JH, Finucane FF, Higgins M, Kleinman JC. Re-
duction of cardiovascular disease-related mortality among wom-
en who use hormones: Evidence from a national cohort. Am J
Obstet Gynecol 164:489-494, 1991.
Writing Group for the PEPI Trial. Effects of hormone therapy on
bone mineral density: Results from the Postmenopausal Estro-
gen/Progestin Interventions (PEPI) Trial. JAMA 276:1389-1396,
1996.
Ylikorkala O, Ortpana A, Puolakka J, Pyörälä T, Viinikka L. Post-
menopausal hormonal replacement decreases plasma levels of
endothelin-1. J Clin Endocrinol Metab 80:3384-3387, 1995.
Ylikorkala O, Pekonen F, Viinikka L. Renal prostacyclin and throm-
boxane in normotensive and preeclamptic pregnant women
and their infants. J Clin Endocrinol Metab 63:1307-1312, 1986.
Ylikorkala O. Balancing between observational studies and rand-
omized trials in prevention of coronary heart disease by estro-
gen replacement: HERS study was no revolution. Acta Obstet
Gynecol Scand 79;1029-1036, 2000.
ISBN 951-45-9969-1 (pdf)