Embed Size (px)
Citation preview
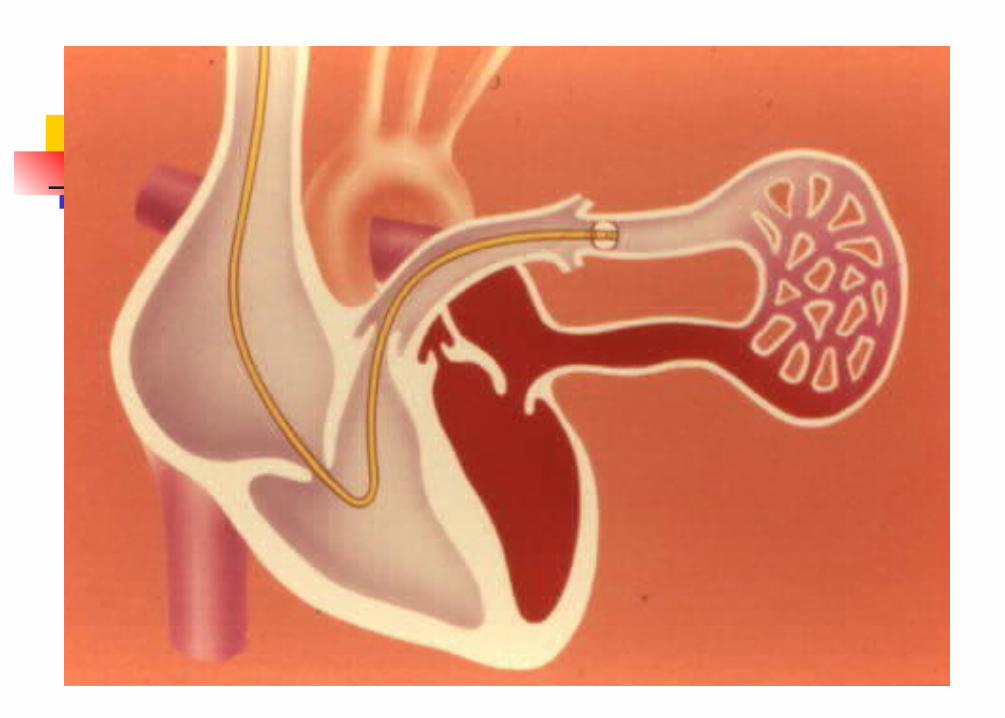
CAD Vs VHD Unlike CAD the symptoms are not
related to poor myocardial performance in VHD
The ventricular function may be normal or even supranormal in VHD
Symptoms are related to the alterations in the loading conditions in VHD: Volume overload Pressure overload
Anaesthetic management
Patient is asleep Maintain haemodynamics
Pathophysiology Haemodynamic effects of anaesthetic agents
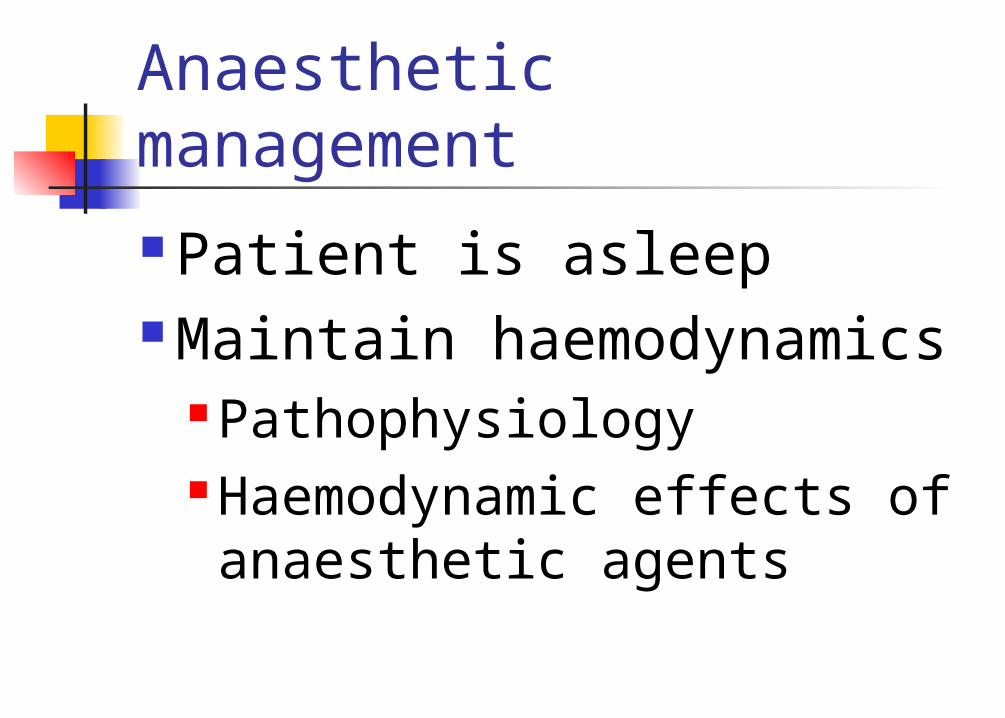
NormalEverything goes in the right direction without impediment
7
25 / 7
12
120 / 12RV
RA LA
LV
PA25 / 12
Ao120 / 80
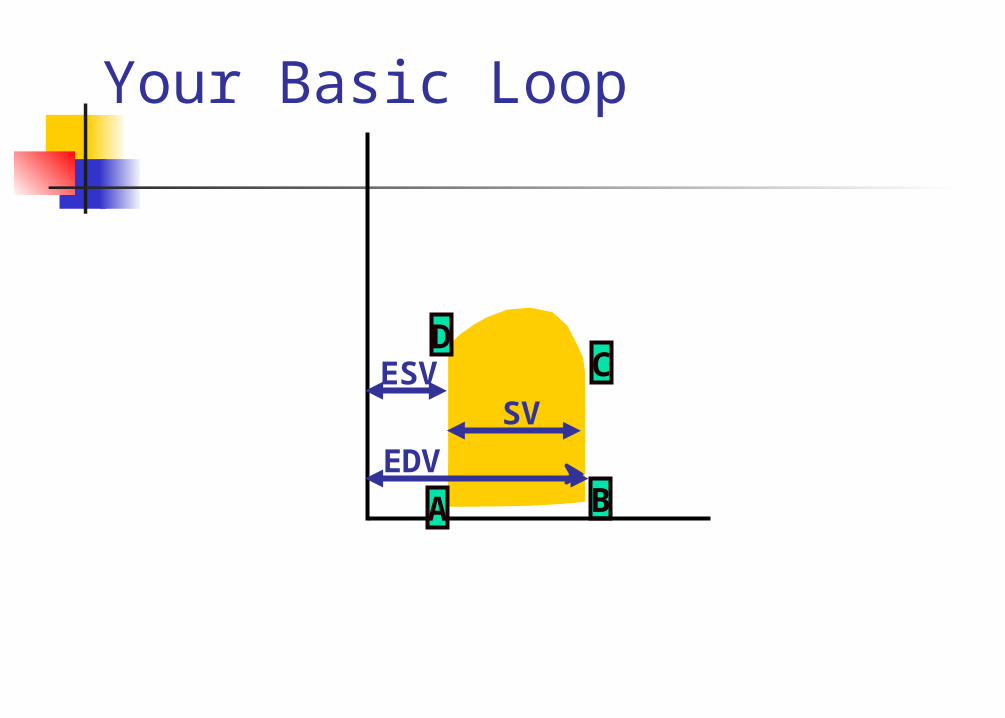
Your Basic Loop
B
C
A
D
EDV
ESVSV
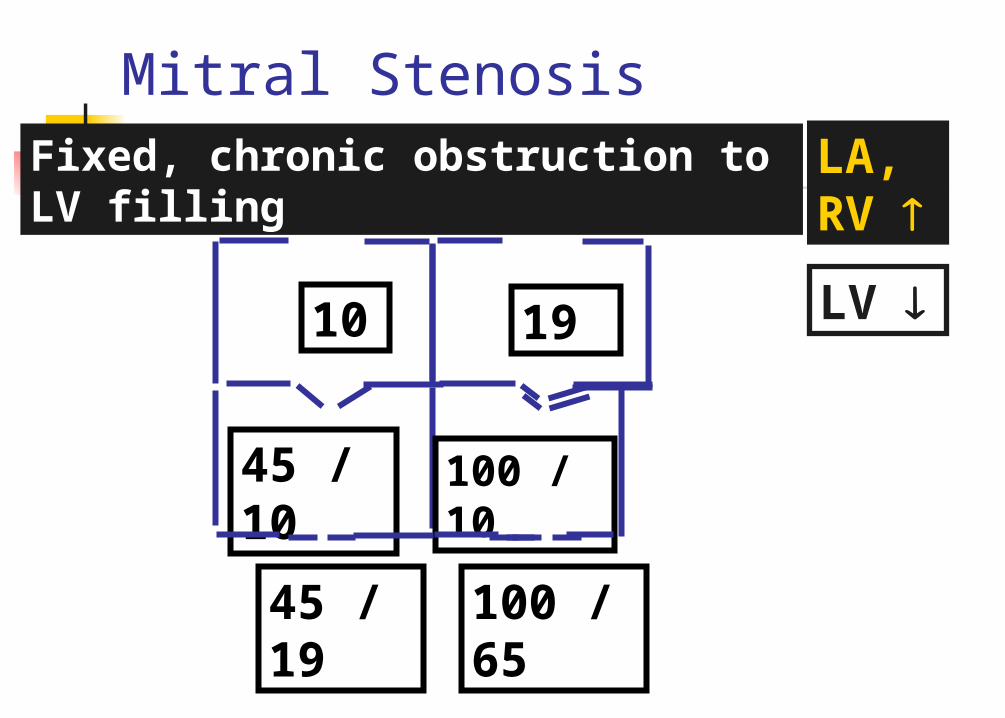
Mitral StenosisFixed, chronic obstruction to LV filling
10
45 / 10
19
100 / 10
45 / 19 100 / 65
LA, RV
LV
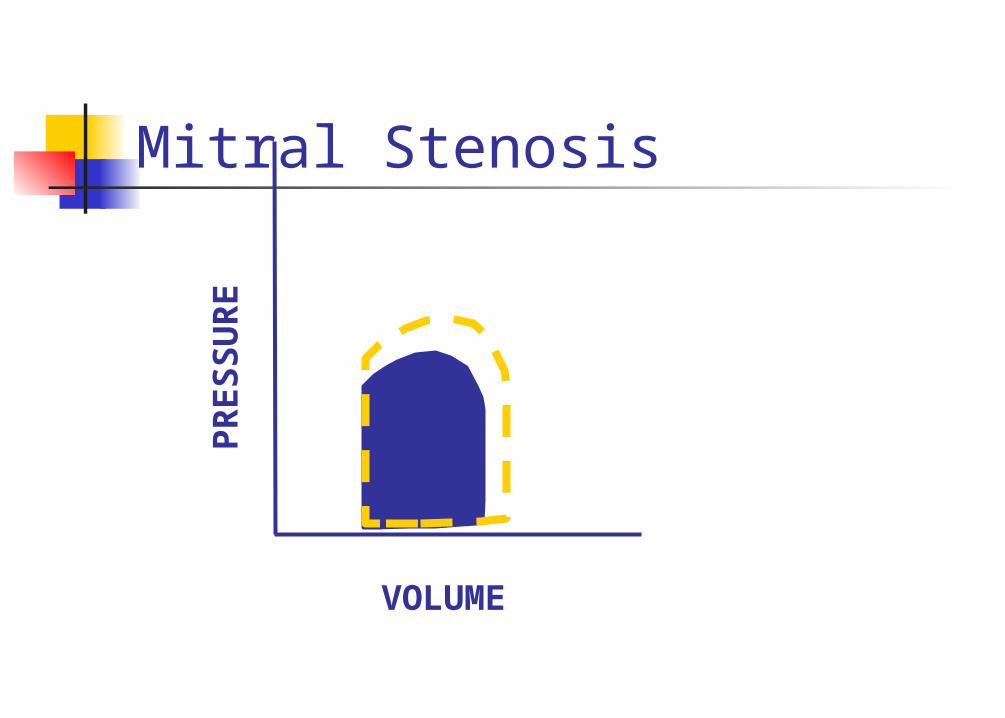
Mitral Stenosis
VOLUME
PR
ES
SU
RE
Left atrial pressure overload Diastolic inflow to LV: maintained by
development of elevated pressure gradient across mitral valve
Dilatation of LA Pressure Increase in PVR: pulmonary hypertension RV dilatation TR Biventricular failure with pulmonary
congestion, peripheral edema and ascites
Changes in left ventricle Restriction of diastolic inflow:
preload reserve is limited Intrinsic myocardial depression:
rheumatic etiology Excess afterload: inadequate wall
thickness, accounts for higher afterload at relatively normal end-systolic pressure
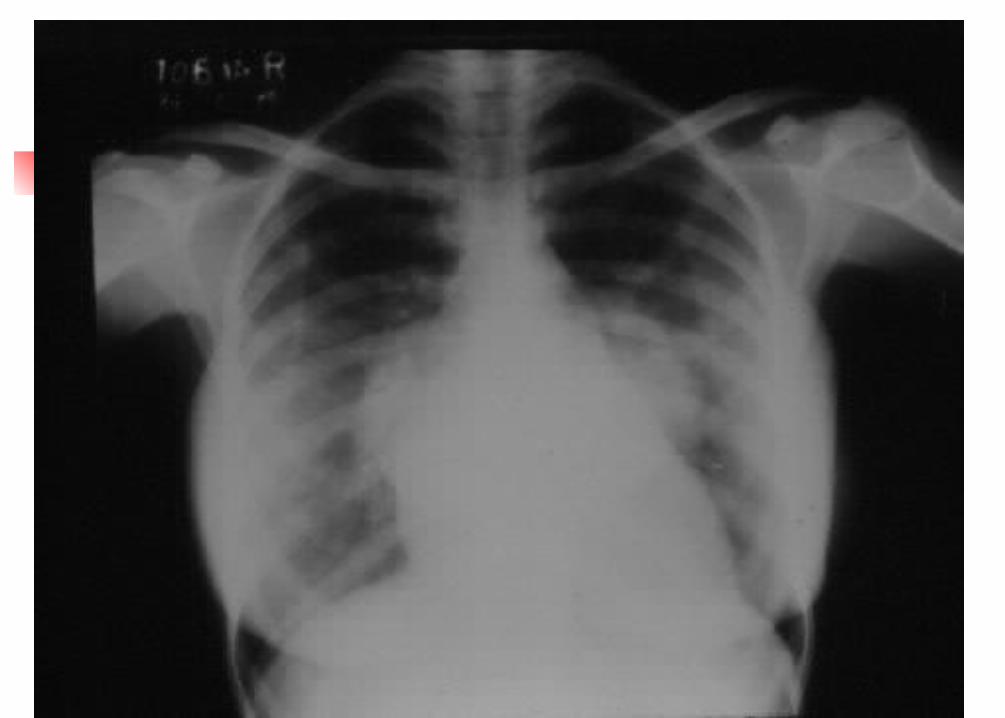
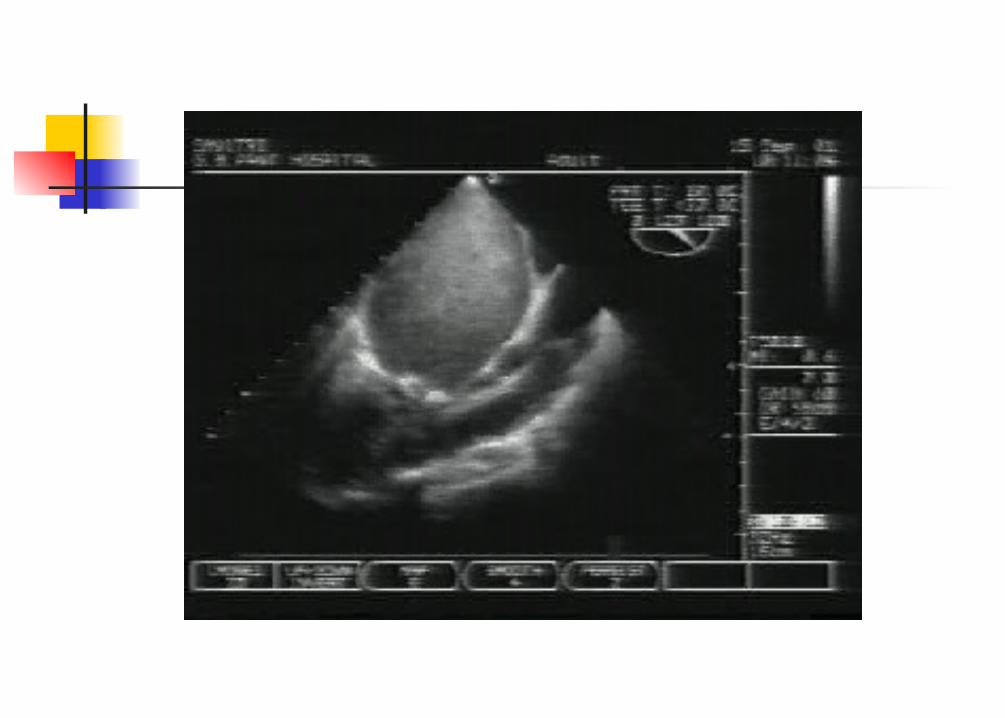
Assessment of severity Symptoms and Clinical examination X-ray chest Echo:
Valve area: Normal: 4.5 cm2
Mild: 1.5 to 2.5 cm2
Moderate: 1 to 1.5 cm2
Severe: < 1 cm2
RVSP
Anaesthetic goals Mild disease: not to worry? Control the heart rate Restore and preserve sinus rhythm if
possible Avoid hypovolemia
Avoid systemic vasodilators Maintain normocarbia Nitroglycerin/nitroprusside
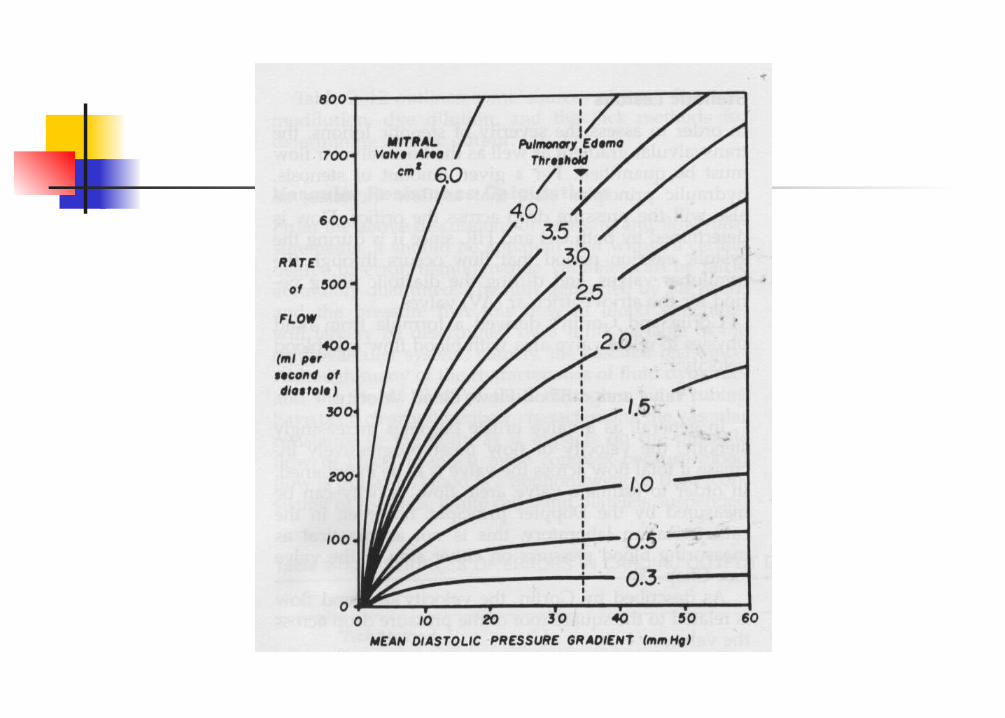
Effect of tachycardia Tachycardia shortens diastole
proportionately more than systole Decreases the overall time available
for transmitral flow In order to maintain CO, the flow
rate per unit time must increase Pressure gradient increases by the
square of the increase in flow rate
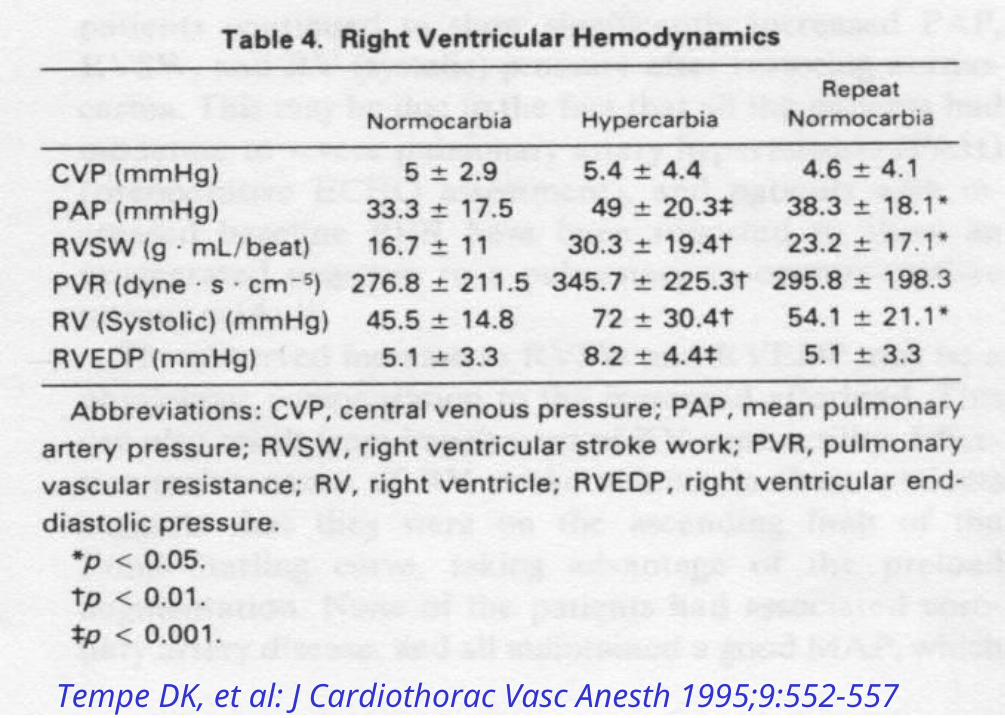
Tempe DK, et al: J Cardiothorac Vasc Anesth 1995;9:552-557
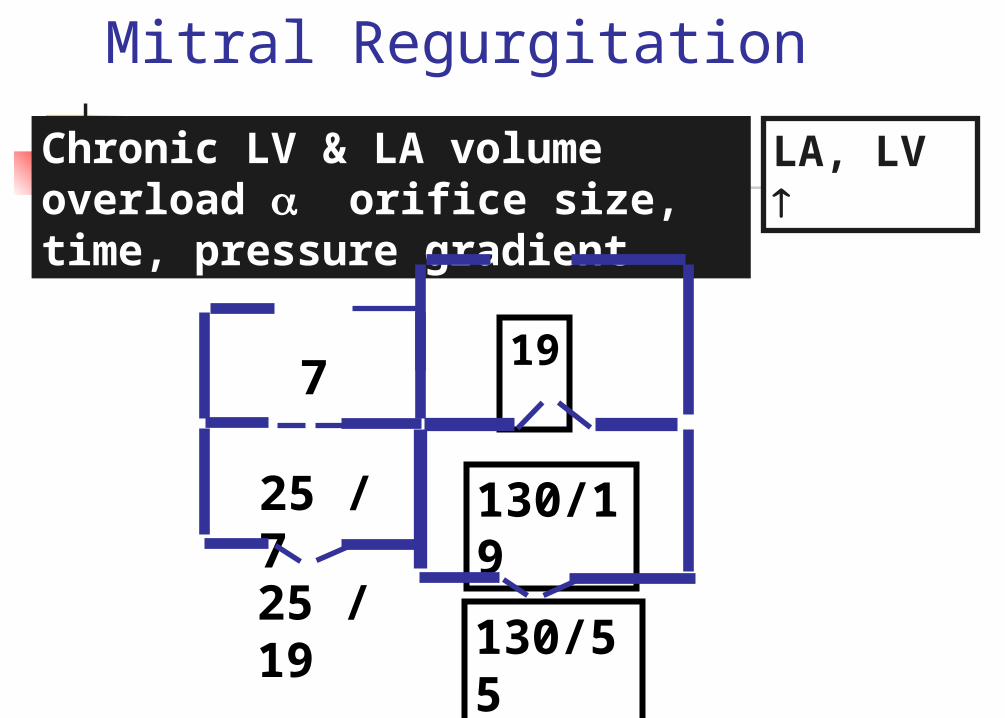
Mitral Regurgitation
Chronic LV & LA volume overload orifice size, time, pressure gradient
7
25 / 7
19
130/19
25 / 19130/55
LA, LV
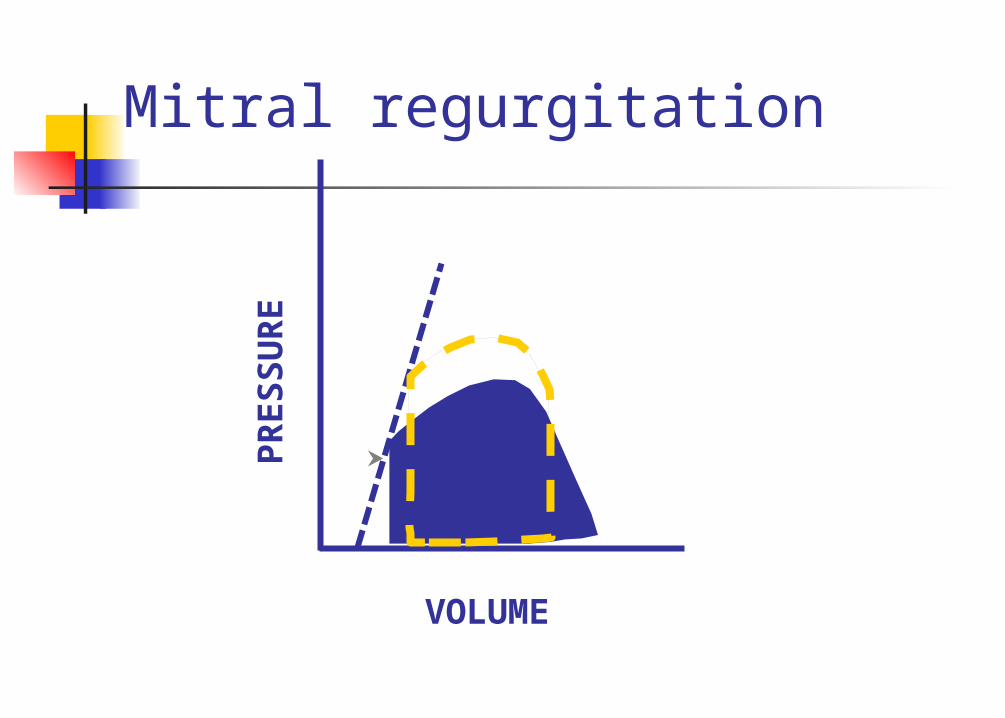
Mitral regurgitation
VOLUME
PR
ES
SU
RE
Pulmonary hypertension in mitral regurgitation Passive congestion of the
pulmonary circulation Reactive pulmonary
vasoconstriction Intrinsic LV dysfunction Combination of above
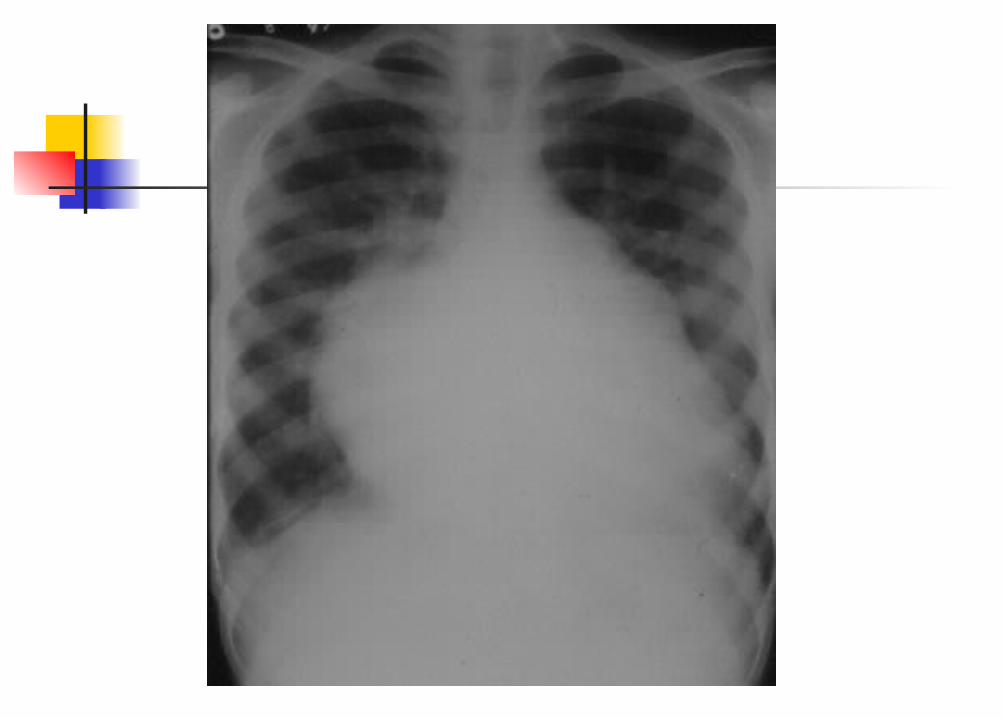
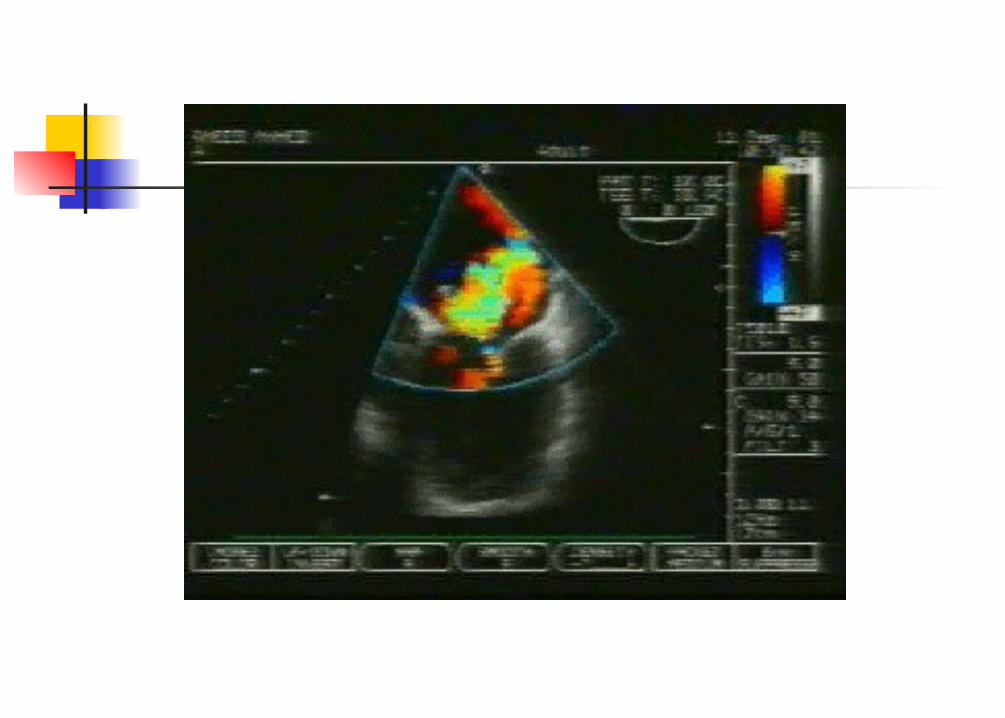
MR: assessment of the severity Symptoms and clinical examination X-ray chest Echo:
Jet area RVSP LV dimensions: end-systolic > 4.5 cm LV ejection fraction
Anaesthetic goals
In general, patients suffering from MR (except those with severe MR and severe PAH) tolerate anaesthesia well
Faster, fuller, vasodilated
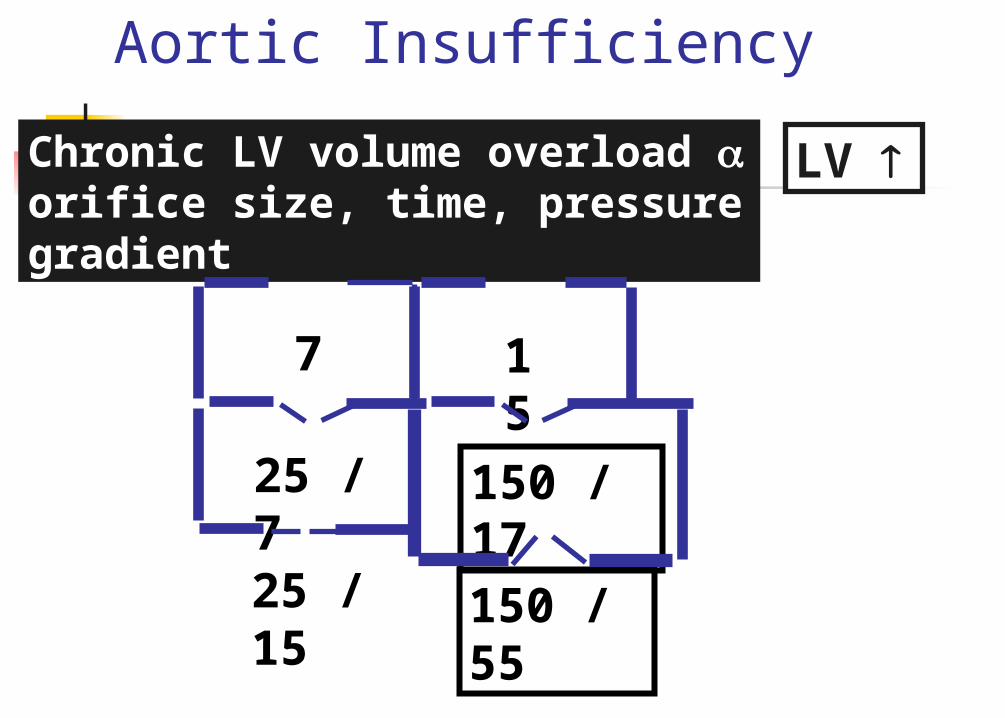
Aortic Insufficiency
Chronic LV volume overload orifice size, time, pressure gradient
7
25 / 7
15
150 / 17
25 / 15 150 / 55
LV
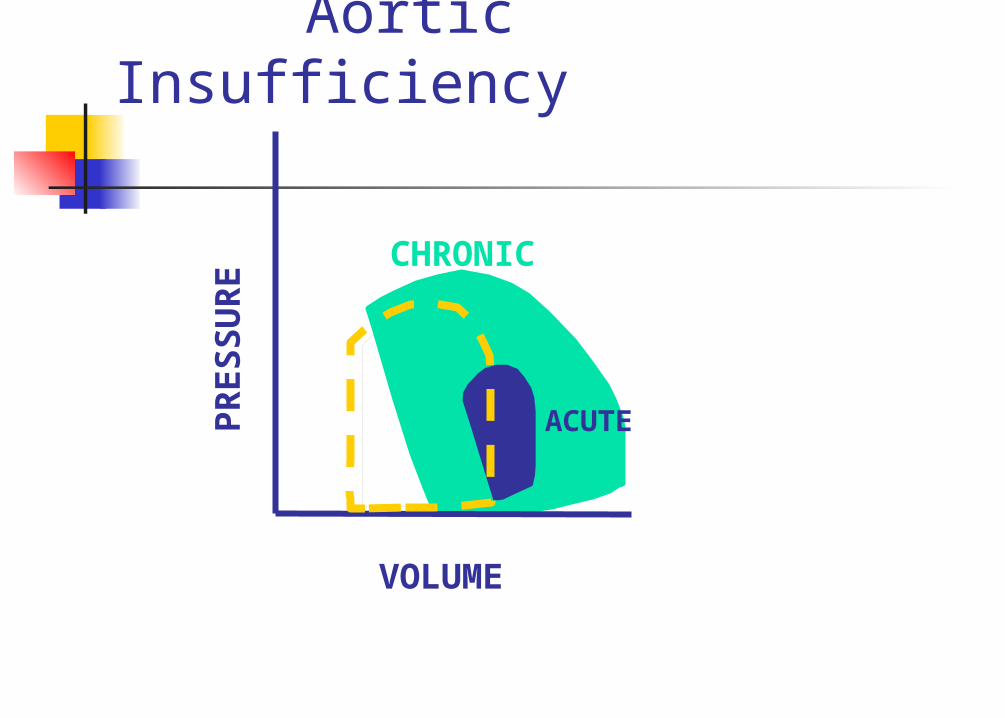
Aortic Insufficiency
VOLUME
PR
ES
SU
RE
ACUTE
CHRONIC
AR: assessment of severity History and clinical examination X-ray chest Echo:
Mild, moderate, severe LV dimensions: End-systolic >5.5 cm
AR: anaesthetic goals In general, patients tolerate
surgery and anaesthesia well, unless CHF or LV dysfunction is present
Aim: to decrease the regurgitant fraction
Faster, fuller and vasodilated Monitor MAP
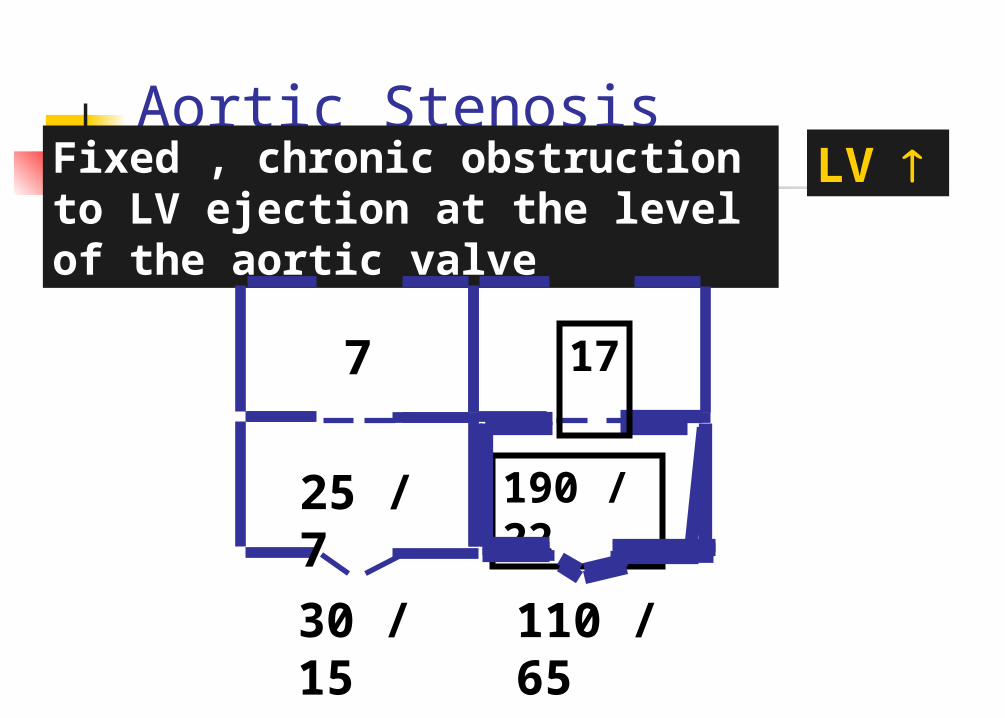
Aortic Stenosis Fixed , chronic obstruction to LV ejection at the level of the aortic valve
LV
7
25 / 7 190 / 22
30 / 15 110 / 65
17
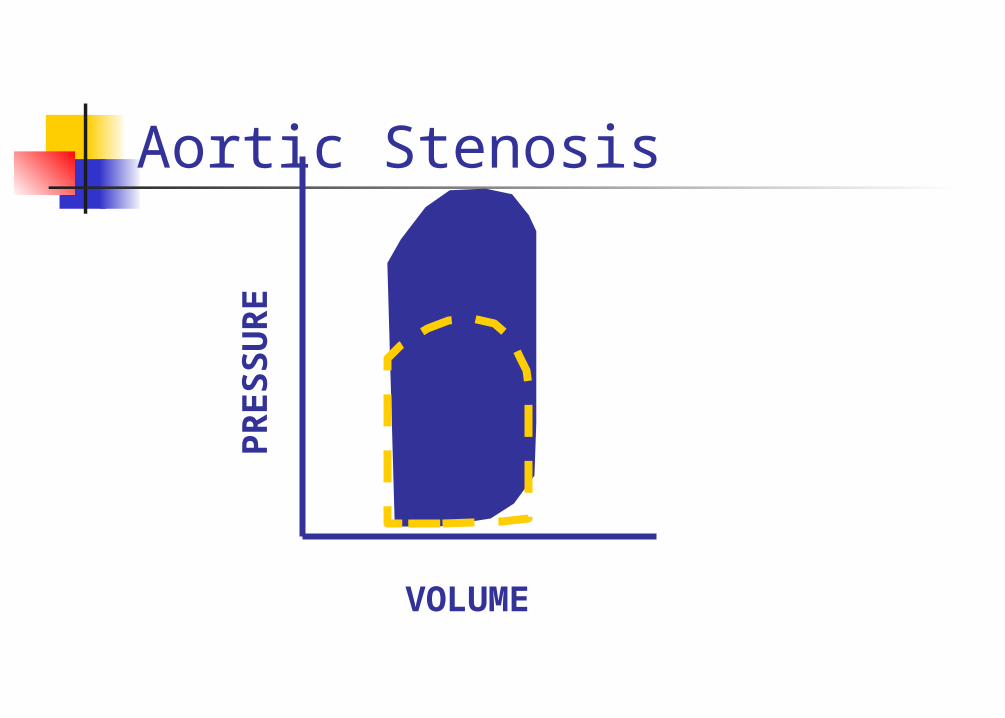
Aortic Stenosis
VOLUME
PR
ES
SU
RE
Pre
ssur
e
Volume
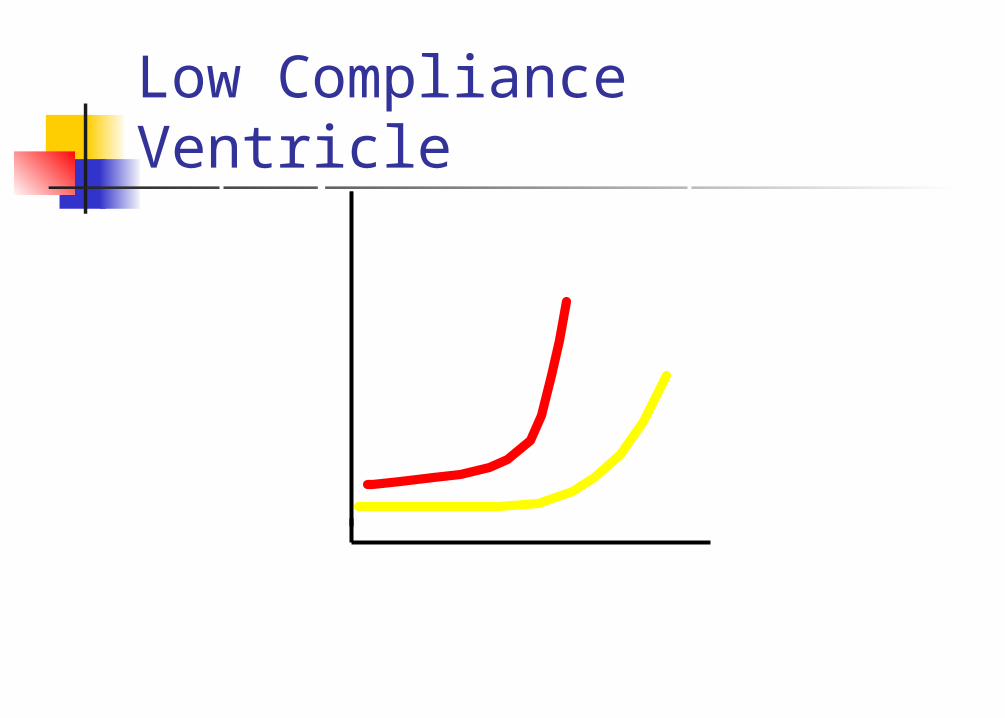
Low Compliance Ventricle
Aortic stenosis: pathophysiology Normal aortic valve area: 2.5 to
3.5 cm2
Haemodynamically significant obstruction occurs at valve area of < 1 cm2
Pressure overload causes concentric hypertrophy of LV
Thickened LV wall
compliance of LV
Ventricular filling depends upon adequate intravascular volume and atrial contraction
NSR is very important: atrial contraction can contribute up to 40% of LV filling
Decreased compliance
Increased LVEDP
Pulmonary congestion CPP
CHF Ischaemia
Myocardial contractility is usually well preserved with normal ejection fraction until very late in the course of the disease
Aortic stenosis: anaesthetic goals Mild disease: not to worry Sinus rhythm is important Bradycardia is dangerous Maintain adequate preload Avoid ischaemia
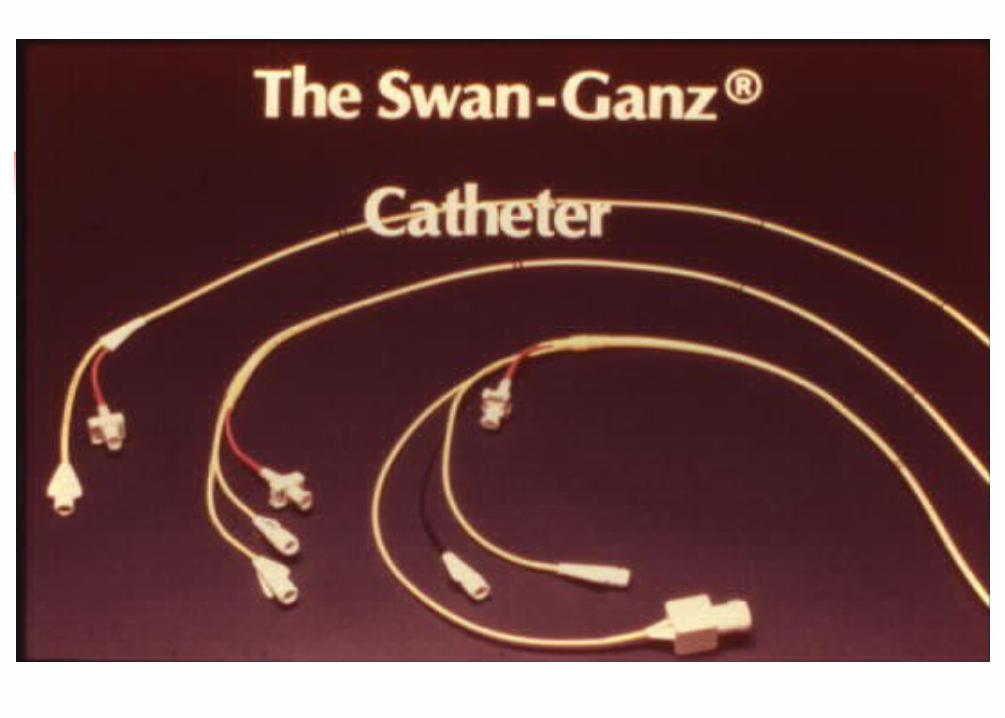
(Hypertension/Hypotension) PA catheter?
OPEN HEART SURGERY
Open heart surgery Induction of anaesthesia Monitoring Heparinisation Establishing the bypass Termination of bypass Protamine administration Transfer to ICU
Postoperative management Ventilation Management of pain and sedation
Anaesthetic management
Opioids should form a “base” Hypnotics and / or
benzodiazepines in small doses used as supplemental agents during induction of anaesthesia
Muscle relaxants
Succinylcholine : 1 to 1.5 mg/ Kg Pancuronium : 0.08 to 0.15 mg/Kg Vecuronium : 0.08 to 0.2 mg/Kg Atracurium : 0.5 to 1 mg/Kg rocuronium : 0.6 mg/Kg
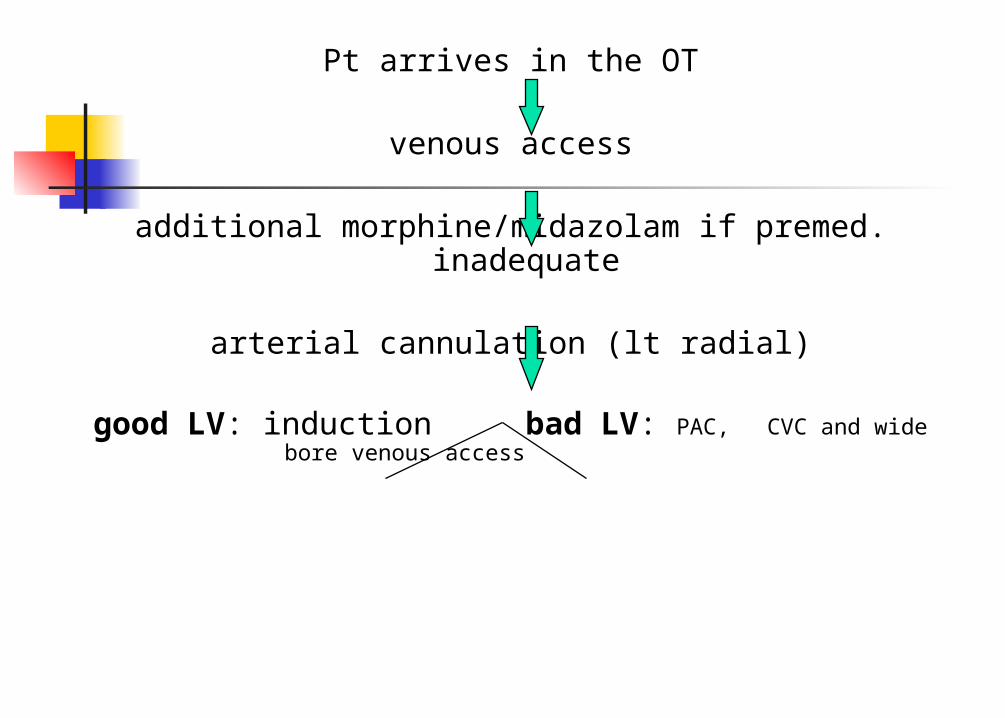
Pt arrives in the OT
venous access
additional morphine/midazolam if premed. inadequate
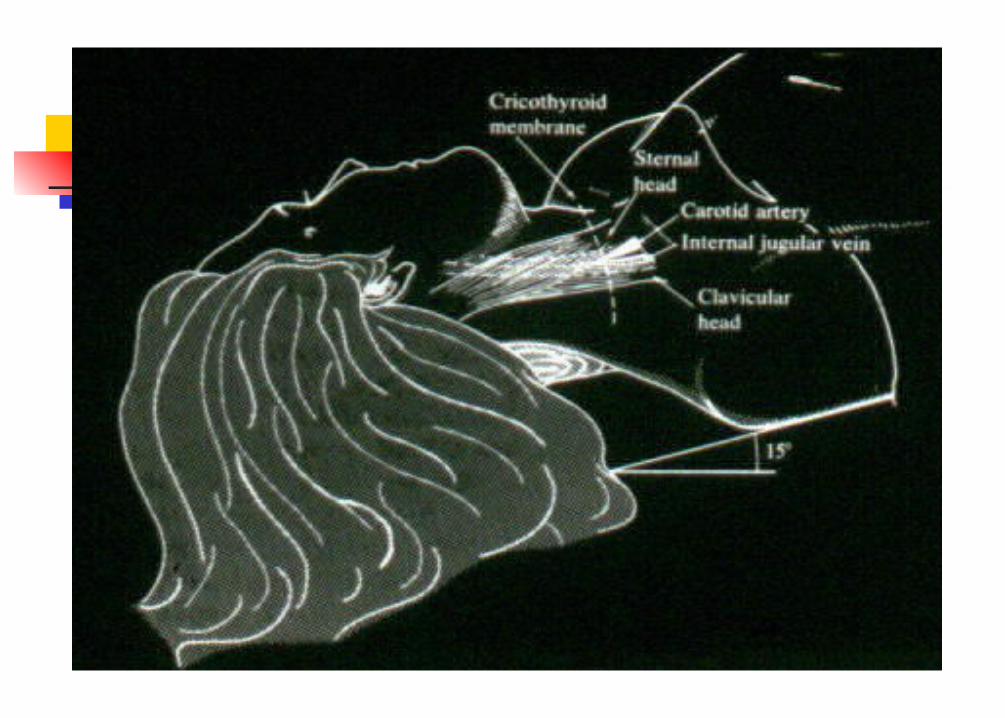
arterial cannulation (lt radial)
good LV: induction bad LV: PAC, CVC and wide bore venous access
Induction
Morphine : 0.5 to 0.75 mg/Kg
OR Fentanyl : 5 to 10 µg/Kg Hypnosis with: diazepam or midazolam
(2-5 mg)
:thiopental (50-100 mg)
Maintenance of anaesthesia
Opioid Nitrous oxide Volatile agents
Halothane Isoflurane
Isoflurane: The clinical evidence suggests that isoflurane is safe in patients with CAD and if hypotention is avoided, it is safe even in patients with steal prone anatomy
Maintenance of anaesthesia (contd.)
On bypass Opioid + relaxant + benzodiazepine
in the prime Repeat half dose every hour
Propofol Inhalational agent
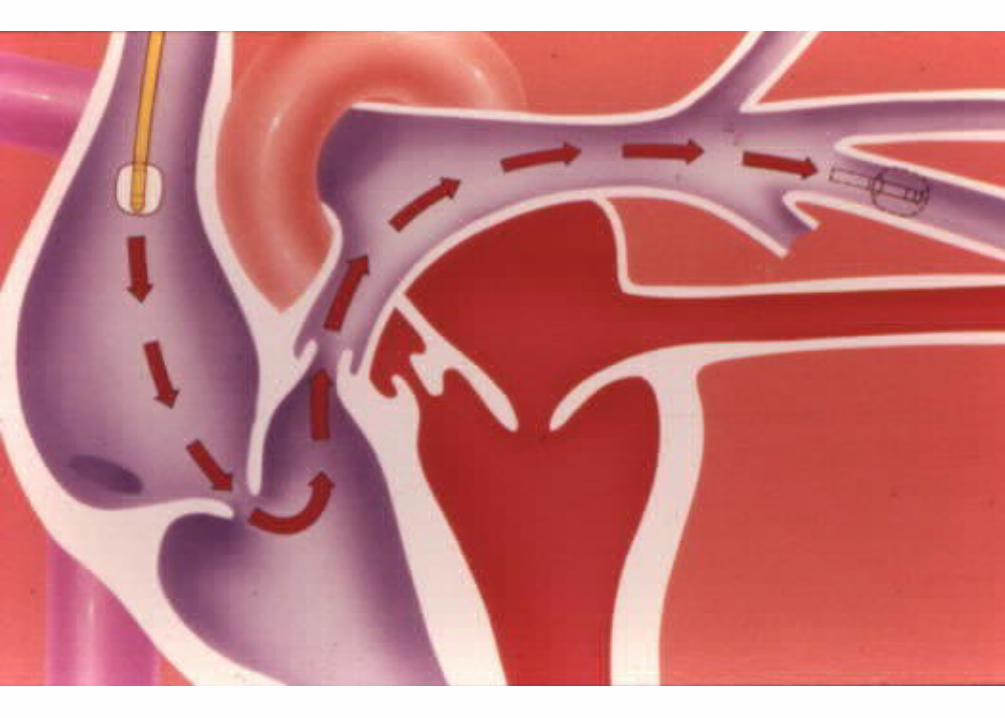
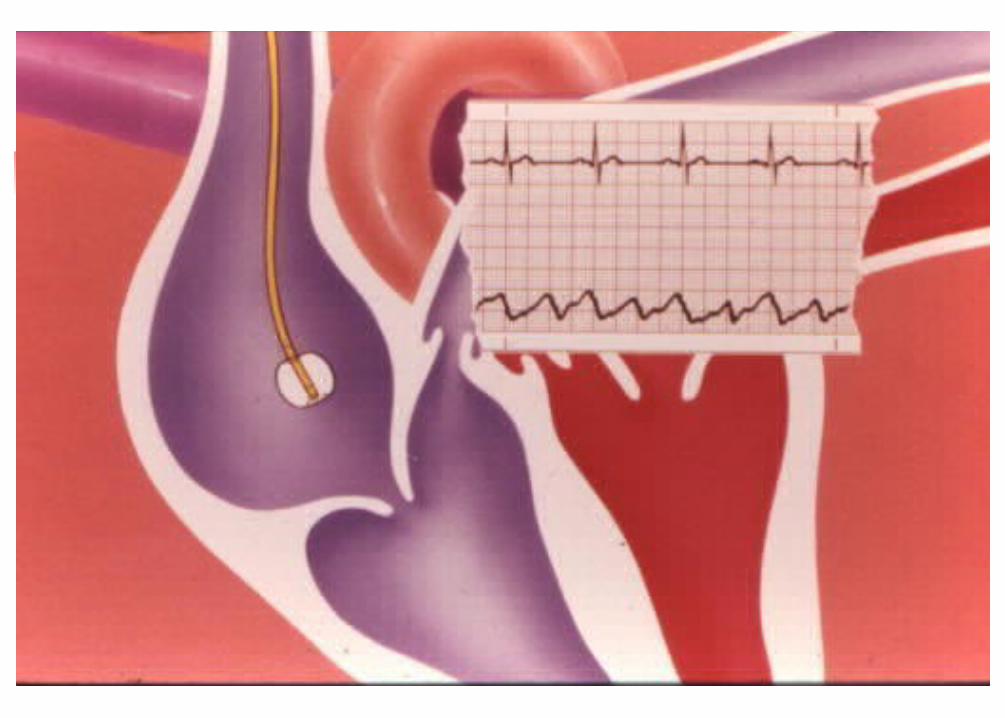
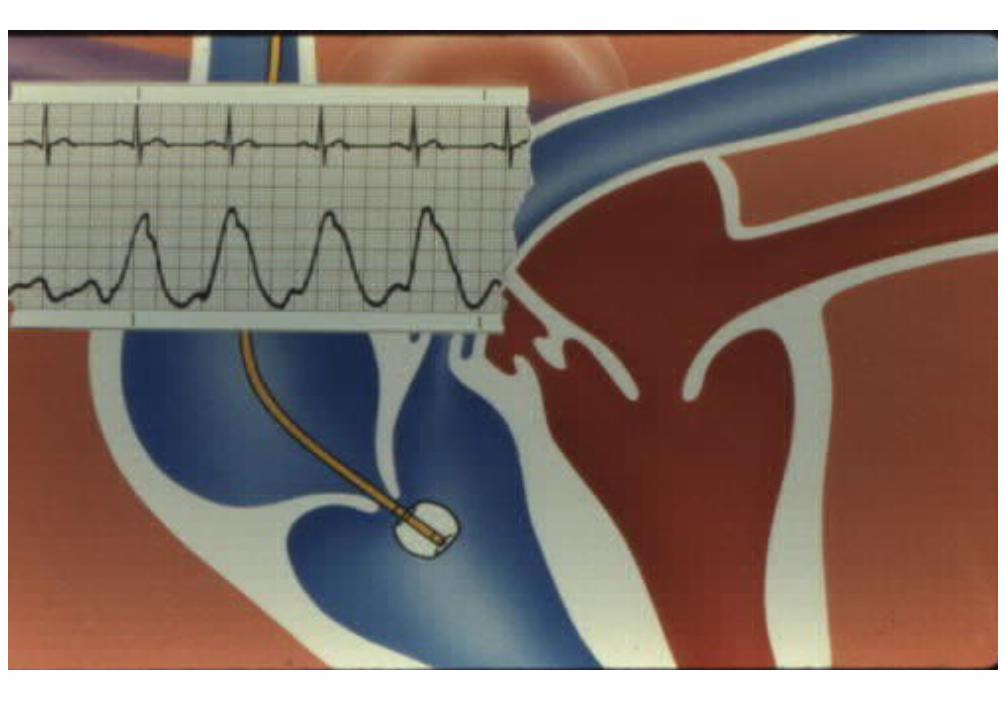
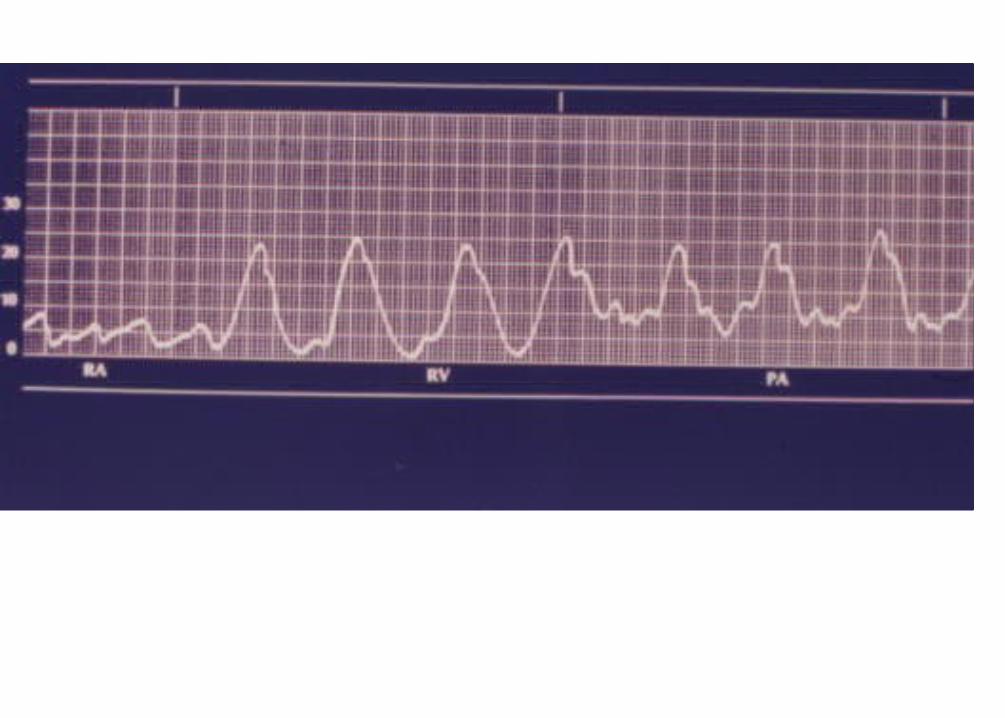
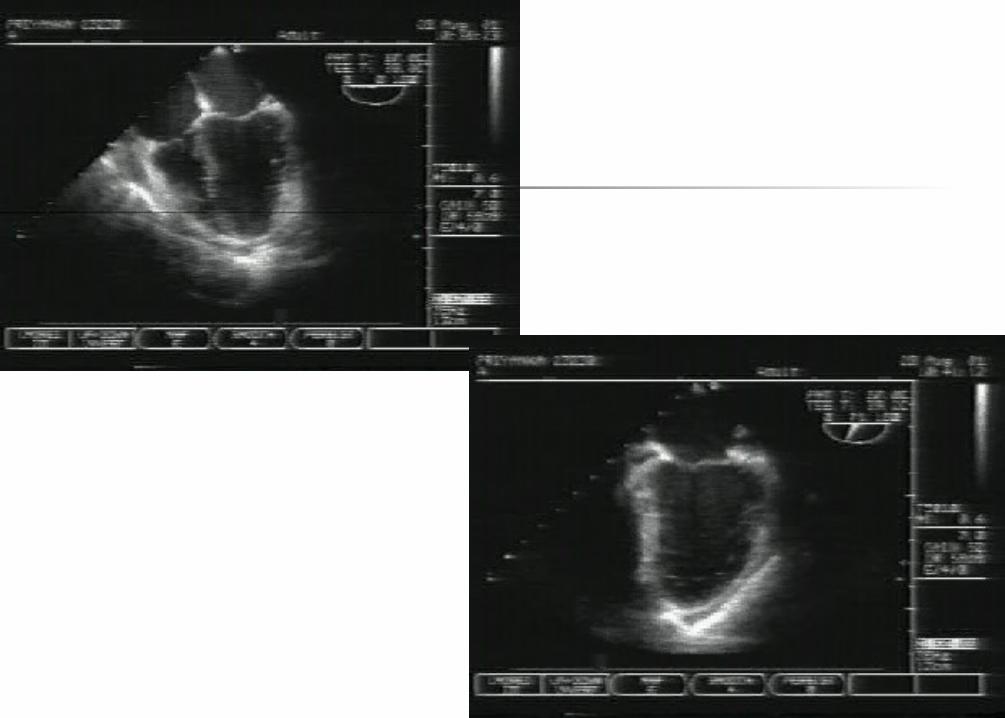
Haemodynamic monitoring
ECG Arterial pressure CVP PA catheter LA pressure Trans-oesophageal echo (TOE)

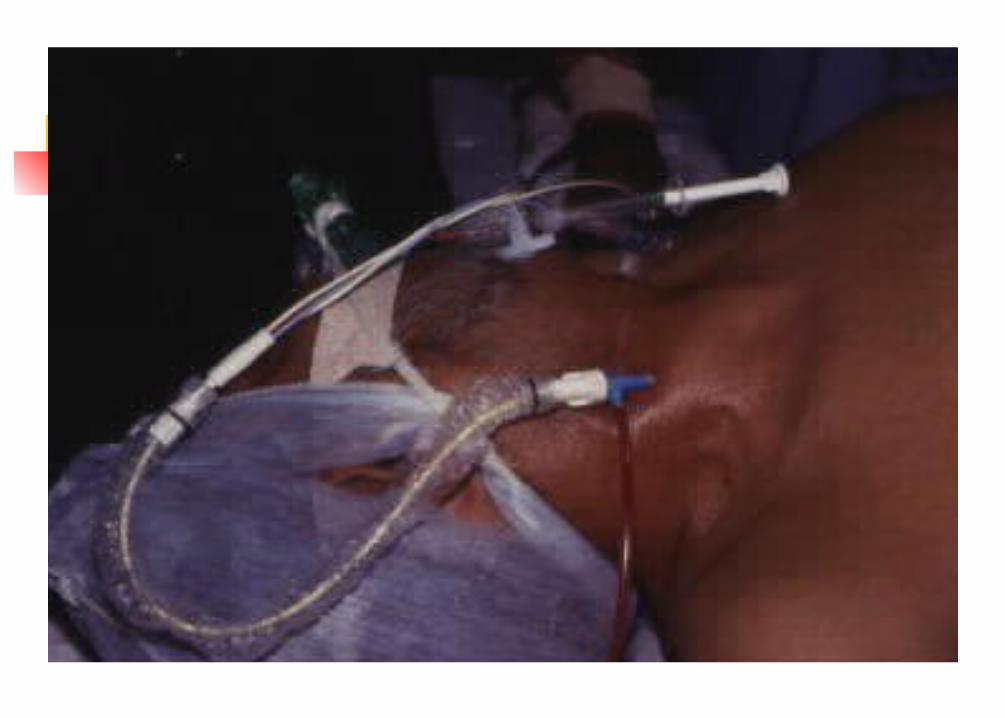
Mehta N, Lochab S, Tempe DK, Cath Cardiovasc Diag1998;43:87




Heparinisation 3-4 mg/Kg of heparin is administered
3-5 min before aortic cannulation ACT monitoring
>300 sec is safe as no clot formation has been reported below this limit
Generally acceptable figure is >400 sec Dose response curve
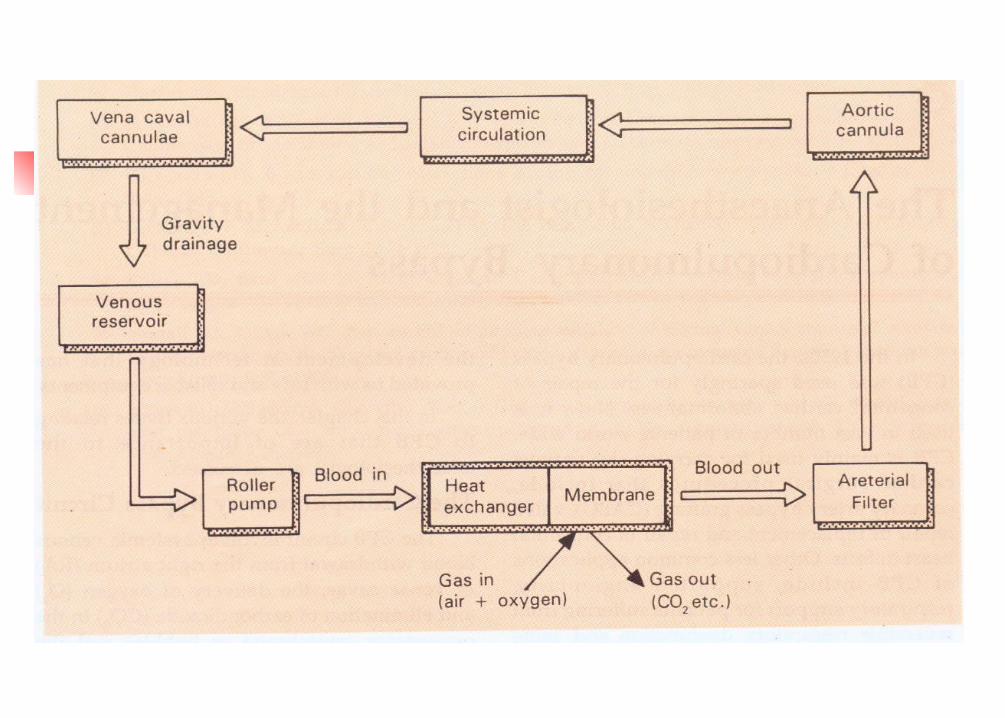
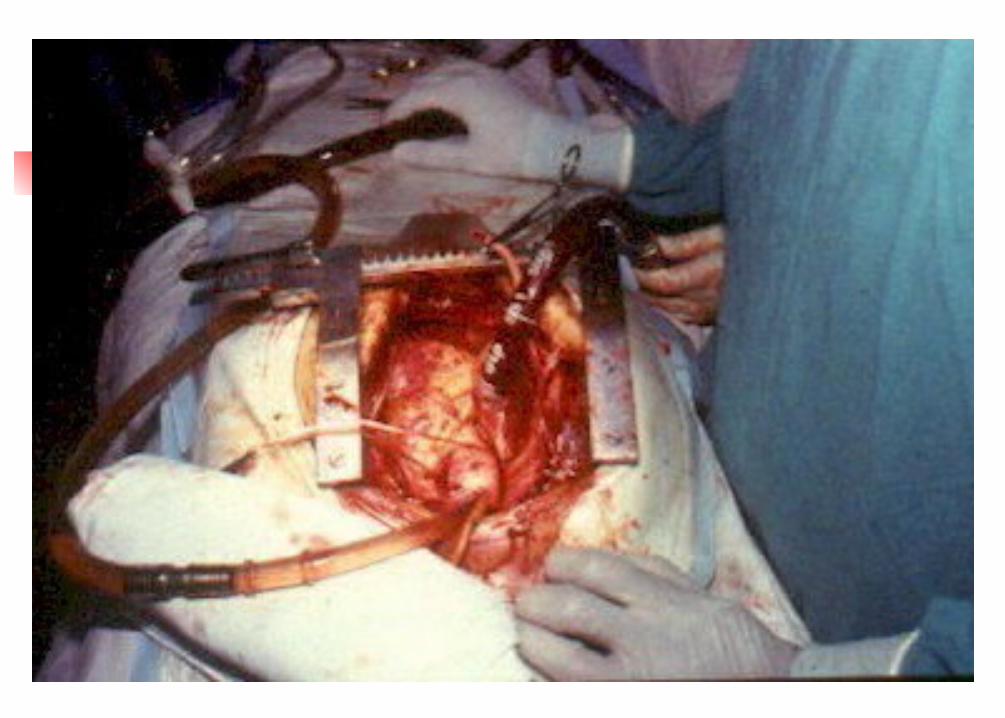

Cardiopulmonary bypass Partial bypass Total bypass Aortic cross clamping Infusion of cardioplegia
Into the root of aorta Directly in to the coronaries Retrograde: coronary sinus
Release the aortic clamp Come off CPB
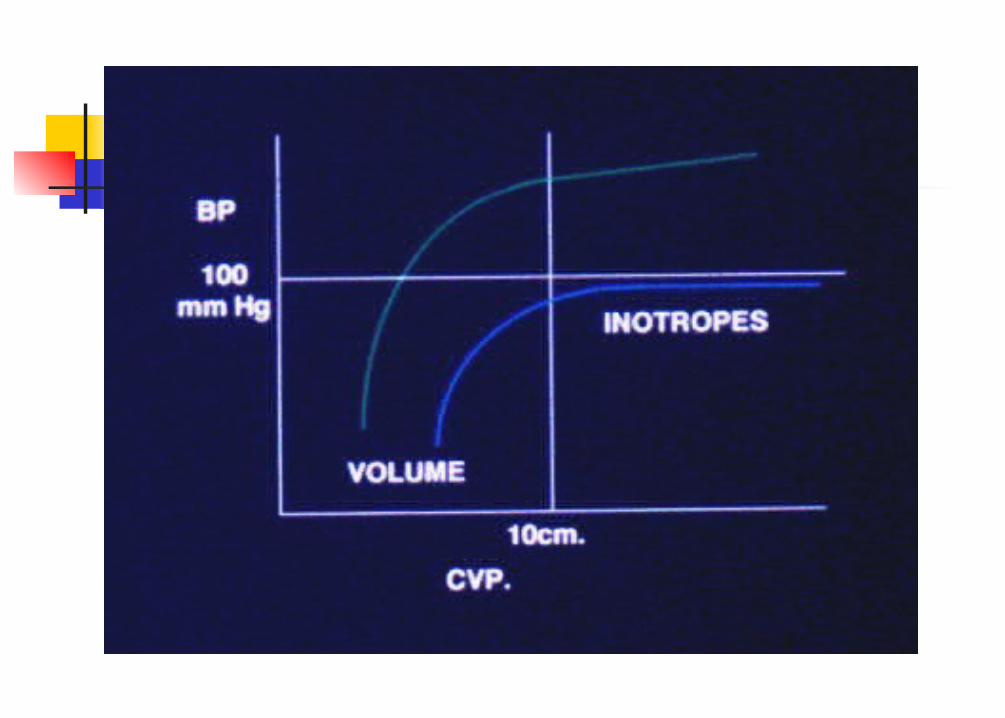
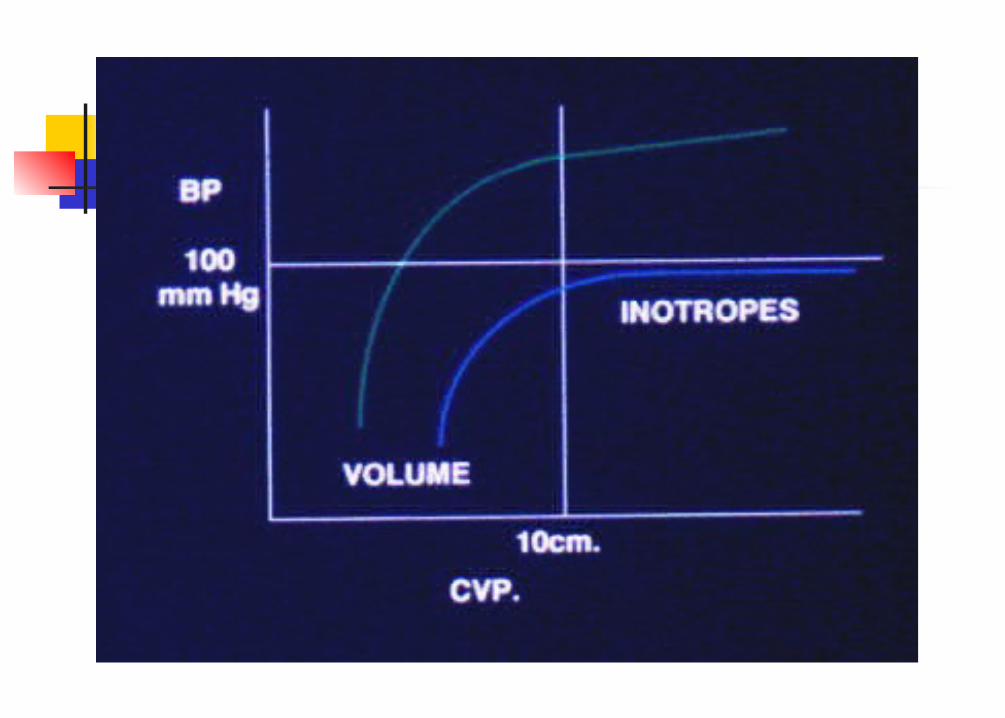
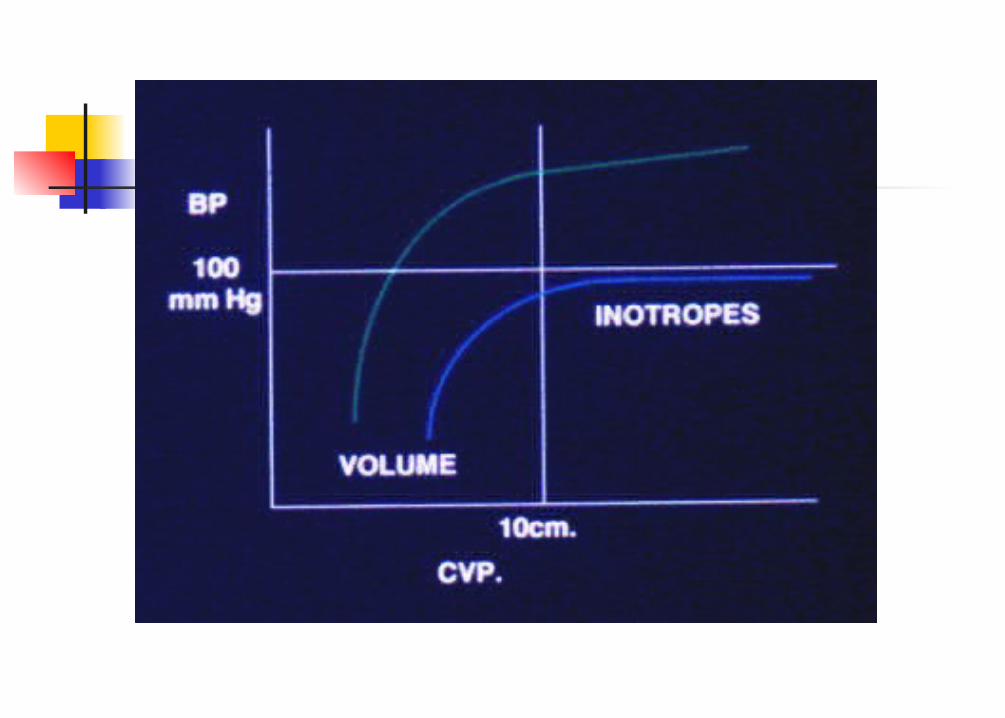
Cardiovascular support
Inotropes Epinephrine Milrinone Dobutamine Amrinone Dopamine Enoximone Dopexamine Norepinephrine IsoprenalineDilators NTG SNPCa blockers, Beta blockers
Changing trends in anaesthetic management
Based on the objective of facilitating early extubation
General anaesthesia Lower or no doses of opioids Propofol Isoflurane, sevoflurane vecuronium
Problems of such anaesthetic technique
Awareness Postoperative pain relief Haemodynamic instability?
Patients can be reversed with neostigmine at the end of the surgery
Extubation can be managed in the ICU
Postoperative pain relief Thoracic epidural (bupivacaine
0.5%, 0.05-0.1 mL/Kg) with general anaesthesia
Intrathecal morphine (5-10 µg/Kg) by lumbar approach with general anaesthesia
Intrapleural analgesia Intercostal block

Conclusions Opioids in variable doses still form the
basis of cardiac anaesthesia With the availability of newer
anaesthetic agents, the safety has improved
Early extubation in valvular heart surgery is being practiced at few centres, but care should be exercised in sicker patients.
www.anaesthesia.co.in [email protected]