Embed Size (px)
Citation preview

MITRAL REGURGITATIONMITRAL REGURGITATION
DR SIVAKUMARAN & DR DR SIVAKUMARAN & DR CHITRACHITRA
MODERATORMODERATOR
DR DILIP SHENDEDR DILIP SHENDEwww.anaesthesia.co.in

An 80 year old woman with An 80 year old woman with increasing dyspneaincreasing dyspnea• Longstanding heart Longstanding heart
murmurmurmur
• Increasing dyspnea Increasing dyspnea & fatigue& fatigue
• Recent ER visit Dx Recent ER visit Dx CHFCHF

Mitral Regurgitation:Mitral Regurgitation:EtiologyEtiology
• Valvular-leafletsValvular-leaflets– Myxomatous MV Myxomatous MV
DiseaseDisease– RheumaticRheumatic– EndocarditisEndocarditis– Congenital-cleftsCongenital-clefts
• ChordaeChordae– Fused/inflammatoryFused/inflammatory– Torn/tTorn/traumarauma– DegenerativeDegenerative– IEIE
• AnnulusAnnulus– Calcification, Calcification, IE (abcess)IE (abcess)
• Papillary MusclesPapillary Muscles– CAD (Ischemia, CAD (Ischemia,
Infarction, Rupture)Infarction, Rupture)– HCMHCM– Infiltrative disordersInfiltrative disorders
• LV dilatation & LV dilatation & functional functional regurgitationregurgitation
• TraumaTrauma

MR Etiology:Surgical series MR Etiology:Surgical series
• MVP(20-70%)MVP(20-70%)
• Ischemia (13-40%)Ischemia (13-40%)
• RHD (3-40%)RHD (3-40%)
• Infectious endocarditis(10-12%)Infectious endocarditis(10-12%)

MR PathophysiologyMR Pathophysiology
• Chronic LV volume overload -» Chronic LV volume overload -» compensatory LVE initially maintaining compensatory LVE initially maintaining cardiac outputcardiac output
• Decompensation (increased LV wall Decompensation (increased LV wall tension) -»CHFtension) -»CHF
• LVE – » annulus dilation – » increased LVE – » annulus dilation – » increased MRMR
• Backflow – » LAE, Afib, Pulmonary HTNBackflow – » LAE, Afib, Pulmonary HTN

MRMR SymptomsSymptoms
• Similar to MSSimilar to MS
• Dyspnea, Orthopnea, PNDDyspnea, Orthopnea, PND
• FatigueFatigue
• Pulmonary HTN, right sided failurePulmonary HTN, right sided failure
• HemoptysisHemoptysis
• Systemic embolization in A FibSystemic embolization in A Fib

Recognizing ChronicRecognizing ChronicMitral RegurgitationMitral Regurgitation
• Pulse:Pulse:– brisk, low volumebrisk, low volume
• Apex:Apex:– hyperdynamichyperdynamic– laterally displacedlaterally displaced– palpable S3 +/- thrillpalpable S3 +/- thrill– late parasternal lift 2late parasternal lift 2 to to
LA fillingLA filling
• S 1 soft or normalS 1 soft or normal• S 2 wide split (early S 2 wide split (early
A2) unless LBBBA2) unless LBBB
• Murmer-Fixed MR:Murmer-Fixed MR:– pansystolicpansystolic– loudest apex to axillaloudest apex to axilla– no post extra-systolic no post extra-systolic
accentuationaccentuation• Murmer-Dynamic Murmer-Dynamic
MR(MVP)MR(MVP)– mid systolicmid systolic– +/- click+/- click– uprightupright
• S 3 / flow rumble if S 3 / flow rumble if severesevere
Wave Sound

Recognizing Acute SevereRecognizing Acute SevereMitral RegurgitationMitral Regurgitation• Acute severe dyspnea, Acute severe dyspnea,
CHF & hypotensionCHF & hypotension• LV size normalLV size normal• LV may/may not be LV may/may not be
hyperdynamichyperdynamic• Loud S1Loud S1• Systolic murmur Systolic murmur
may/may not be pan-may/may not be pan-systolicsystolic
• Inflow/rumbleInflow/rumble• S3 present-may be S3 present-may be
only abnormalityonly abnormality
• RV liftRV lift
• TTE/TEE for diagnosisTTE/TEE for diagnosis– Chordal or papilllary Chordal or papilllary
muscle rupture/tearmuscle rupture/tear– Infarction with papillary Infarction with papillary
muscle ischaemia or muscle ischaemia or teartear
– Infectious endocarditis Infectious endocarditis with leaflet perforation with leaflet perforation or disruption or chordal or disruption or chordal teartear
– Flail MV segmentFlail MV segment

Assessing Severity of Assessing Severity of Chronic Chronic Mitral RegurgitationMitral Regurgitation
Measure the Impact on the LV:Measure the Impact on the LV:
• Apical displacement and sizeApical displacement and size
• Palpable S3Palpable S3
• Longer/louder MR murmer (chronic MR)Longer/louder MR murmer (chronic MR)
• S3 intensity/ length of diastolic flow S3 intensity/ length of diastolic flow rumblerumble
• Wider split S2 (earlier A2)Wider split S2 (earlier A2)

Recognizing Mitral Recognizing Mitral Regurgitation Regurgitation investigationsinvestigations
• ECG:ECG:– LA enlargementLA enlargement– AfibAfib– LVH (50% pts. LVH (50% pts.
With severe MR)With severe MR)– RVH (15%)RVH (15%)– Combined Combined
hypertrophy (5%)hypertrophy (5%)
• CXR:CXR:– LVLV– LALA– pulmonary pulmonary
vascularityvascularity– CHFCHF

MR EchocardiographyMR Echocardiography
• Baseline evaluation to identify etiology, Baseline evaluation to identify etiology, quantify severity of MRquantify severity of MR
• Assess and quantify LV function and Assess and quantify LV function and dimensionsdimensions
• Annual or semi-annual surveillance of LV Annual or semi-annual surveillance of LV function, estimated EF and LVESD in function, estimated EF and LVESD in asymptomatic severe MRasymptomatic severe MR
• To establish cardiac status after change in To establish cardiac status after change in symptomssymptoms
• Baseline study post MVR or repair Baseline study post MVR or repair

MR EchocardiographyMR Echocardiography
• Etiology: Etiology: – flail leaflets (chord/pap rupture)flail leaflets (chord/pap rupture)– thick (RHD)thick (RHD)– post mvt of leaflets (MVP)post mvt of leaflets (MVP)– vegetations(IE)vegetations(IE)
• Severity: Severity: – regurgitant volume/fraction/orifice arearegurgitant volume/fraction/orifice area– LV systolic functionLV systolic function– increased LV/LA size, EFincreased LV/LA size, EF

MR StagesMR StagesMR StagesMR Stages
LV size and function defined by echoLV size and function defined by echo• Stage 1-compensated: Stage 1-compensated:
– End-diastolic dimension less 63mm, ESD less End-diastolic dimension less 63mm, ESD less 42mm42mm
– EF more than 60EF more than 60
• Stage 2-transitionalStage 2-transitional– EDD 65-68mm, ESD 44-45mm, EF 53-57EDD 65-68mm, ESD 44-45mm, EF 53-57
• Stage 3-decompensatedStage 3-decompensated– EDD more than 70mm, ESD more than 45mm, EDD more than 70mm, ESD more than 45mm,
EF less than 50EF less than 50

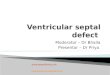
RECOMMENDED FREQUENCY OF ECHOCARDIOGRAPHYRECOMMENDED FREQUENCY OF ECHOCARDIOGRAPHYIN PATIENTS WITH CHRONIC MITRAL REGURGITATIONIN PATIENTS WITH CHRONIC MITRAL REGURGITATIONAND PRIMARY MITRAL-VALVE DISEASE. AND PRIMARY MITRAL-VALVE DISEASE.
SEVERITY OFSEVERITY OF
MITRALMITRAL
REGURGITATIONREGURGITATION
LEFT LEFT VENTRICULAR VENTRICULAR
FUNCTION*FUNCTION*
FREQUENCY OFFREQUENCY OF
ECHOCARDIOGRECHOCARDIOGRA-PHIC FOLLOW-A-PHIC FOLLOW-
UPUP
MildMild Normal ESD and EFNormal ESD and EF Every 5 yrEvery 5 yr
ModerateModerate Normal ESD and EFNormal ESD and EF Every 1 Every 1 ––2 yr2 yr
ModerateModerate ESD >40 mm or EF ESD >40 mm or EF <0.65<0.65
AnnuallyAnnually
SevereSevere Normal ESD and EFNormal ESD and EF AnnuallyAnnually
SevereSevere ESD >40 mm or EF ESD >40 mm or EF <0.65<0.65
Every 6 moEvery 6 mo*ESD denotes end-systolic dimension and EF ejection fraction. Otto C.M. NEJM 345:10.


Medical managementMedical management
• Goals : MR, CO, PUL Cong.Goals : MR, CO, PUL Cong.– VasodilatorsVasodilators– IonotropesIonotropes– Aortic baloon counter pulsationAortic baloon counter pulsation
• AntibioticsAntibiotics
• Treatment of AFTreatment of AF
• Anticoagulation Anticoagulation

Mitral Valve SurgeryMitral Valve Surgery
• Only effective treatment is valve Only effective treatment is valve repair/replacementrepair/replacement
• Optimal timing Optimal timing – Presence/absence of symptomsPresence/absence of symptoms– Functional state of ventricleFunctional state of ventricle– Feasability of valve repairFeasability of valve repair– Presence of Afib/PHTNPresence of Afib/PHTN– Preference/expectations of patientPreference/expectations of patient

SymptomsSymptoms
• Class III or IV symptoms (even if Class III or IV symptoms (even if transient) always indicate need for transient) always indicate need for surgerysurgery
• Class II symptoms indicate need for Class II symptoms indicate need for surgery in patients with repairable surgery in patients with repairable valvesvalves
• ETT may reveal concealed symptomsETT may reveal concealed symptoms

Ejection Fraction (LVEF)Ejection Fraction (LVEF)
• Strongest predictor of outcome following Strongest predictor of outcome following surgerysurgery
• Should be assessed quantitativelyShould be assessed quantitatively– MUGA or EchoMUGA or Echo
• Surgery indicated if LVEF is below normal Surgery indicated if LVEF is below normal (60%)(60%)
• If EF normal, follow every 6 to 12 monthsIf EF normal, follow every 6 to 12 months
• If EF <30%, medical management (valve If EF <30%, medical management (valve repair experimental in this setting)repair experimental in this setting)

Other IndicationsOther Indications
• Flail mitral leafletFlail mitral leaflet
• Left atrial dimension >45mmLeft atrial dimension >45mm
• Paroxysmal atrial fibrillationParoxysmal atrial fibrillation
• Pulmonary hypertensionPulmonary hypertension

Mitral RegurgitationMitral RegurgitationACC/AHA ACC/AHA recommendationsrecommendations
Surgery Recommended in patients who Surgery Recommended in patients who areare
• SymptomaticSymptomatic• Asymptomatic withAsymptomatic with
– Any LV dysfunctionAny LV dysfunction– Atrial fibrillationAtrial fibrillation– Pulmonary hypertensionPulmonary hypertension– Reparable valvesReparable valves– Recurrent VTRecurrent VT

Indications for Surgery Indications for Surgery Isolated,Severe Chronic Isolated,Severe Chronic MRMR
– NYHA Class III or IV heart failure (any NYHA Class III or IV heart failure (any duration)duration)
– EF <60%EF <60%– EF >60% but decreasing on serial EF >60% but decreasing on serial
measurementsmeasurements– LVED Diameter >45mmLVED Diameter >45mm

MV Repair vs. ReplacementMV Repair vs. Replacement
• Lower operative mortalityLower operative mortality
• Better late outcomeBetter late outcome
• LV function preservedLV function preserved
• Avoids anticoagulation unless atrial fibrillationAvoids anticoagulation unless atrial fibrillation
• incidence of thromboembolismincidence of thromboembolism
• durability of repairdurability of repair
• incidence of IEincidence of IE
• Open Afib ablationOpen Afib ablation

ANESTHESIA ANESTHESIA MANAGEMENTMANAGEMENT

Anesthetic consideration Anesthetic consideration • Patients with mild and moderate MR Patients with mild and moderate MR
tolerate non cardiac surgery bettertolerate non cardiac surgery better
• Factors influencing anesthesia areFactors influencing anesthesia are– Eccentric Hypertropy Eccentric Hypertropy – LV chamber dil.LV chamber dil.– LA enlargement & PHTLA enlargement & PHT
• Hemodynamic goals areHemodynamic goals are– Maintenance of forward cardiac output Maintenance of forward cardiac output – Reduction in regurgitant fraction Reduction in regurgitant fraction – Preventing deleterious increase in PAPPreventing deleterious increase in PAP

PREOP EVALUATIONPREOP EVALUATION
• History & physical examination History & physical examination – Focus on RVFFocus on RVF
• CXR, EKGCXR, EKG
• EchocardiographyEchocardiography
• Assess severity of MRAssess severity of MR
• Role of cardiac catheterizationRole of cardiac catheterization

Premedication Premedication
• Antibiotic prophylaxis Antibiotic prophylaxis • Preoperative sedationPreoperative sedation
– Titration Titration – Oral benzodiazepines are recommendedOral benzodiazepines are recommended
• Supplemental O2 Supplemental O2 • Continue AF medicationsContinue AF medications• Preferable to avoid diuretics on Preferable to avoid diuretics on
morning of surgery.morning of surgery.

Intraoperative Intraoperative ManagementManagement

MonitoringMonitoring
• To be tailored toTo be tailored to– Nature of surgery, severity of MR, Nature of surgery, severity of MR,
baseline LV function, rhythm.baseline LV function, rhythm.
• Standard monitoringStandard monitoring
• Invasive monitoringInvasive monitoring– IABPIABP– Role of PAC, TEE, Role of PAC, TEE,

FULL, FAST, FULL, FAST, AND AND VASODILATEDVASODILATED
also match the o2 demandalso match the o2 demand

Pre loadPre load
Adequate volume loadingAdequate volume loading
Consequences of overloadingConsequences of overloading•Worsening of MR, PHTWorsening of MR, PHT
•RVFRVF
Can be guided by PAC, TEECan be guided by PAC, TEE

AfterloadAfterload
• Decreased after load decreases Decreased after load decreases regurgitation fractionregurgitation fraction
• Vasodilators by lowering afterload, Vasodilators by lowering afterload, increase forward flow, decrease left increase forward flow, decrease left ventricular size and enhance ejection ventricular size and enhance ejection fraction fraction
• Sodium nirtoprussideSodium nirtoprusside
• DobutamineDobutamine
• INODILATORSINODILATORS

Rate Rate • Mild tachycardiaMild tachycardia
• > 90 beats per minute reduce the > 90 beats per minute reduce the diastolic regurgitation time and diastolic regurgitation time and degree of regurgitation degree of regurgitation
• filling time LV distension filling time LV distension mitral annular dilation mitral annular dilation regurgitationregurgitation
• Sinus rhythm and atrial contractility Sinus rhythm and atrial contractility relatively less important when relatively less important when compared to stenotic lesioncompared to stenotic lesion
• Hence AF better tolerated in MRHence AF better tolerated in MR

ContractilityContractility
• Avoid myocardial depressionAvoid myocardial depression
• Opioid based anesthesia was hence Opioid based anesthesia was hence more popularmore popular
• Lower dose opioid + potent Lower dose opioid + potent inhalational anesthetic is better inhalational anesthetic is better suitable in NHYA I,II.suitable in NHYA I,II.
• Consider inodilator, dobutamine, NTG, Consider inodilator, dobutamine, NTG, SNP.SNP.

Pulmonary circulationPulmonary circulation
• Goal – low PVRGoal – low PVR
• Avoid hypercapnia, hypoxia, acidosisAvoid hypercapnia, hypoxia, acidosis
• Mild hyperventilation Mild hyperventilation
• Use of N2O ?Use of N2O ?
• Role of PGE1Role of PGE1– PVR, PVR, – First pass metabolism in pulmonary circ.First pass metabolism in pulmonary circ.
• NONO

Anesthetic agentsAnesthetic agents
• GA requires the selection of an GA requires the selection of an induction agent with minimal induction agent with minimal myocardial depression.myocardial depression.
• Opioids: high and low dose opioidsOpioids: high and low dose opioids• Volatile anestheticsVolatile anesthetics
– ISOFLURANE has few advantagesISOFLURANE has few advantages
• Pancuronium – a better choice for Pancuronium – a better choice for muscle relaxation muscle relaxation
• N2O avoid preferablyN2O avoid preferably– Myocardial depressionMyocardial depression– Pulmonary hypertensionPulmonary hypertension

REGIONAL ANESTHESIAREGIONAL ANESTHESIA
• TEMPTING OPTION SVRTEMPTING OPTION SVR
• Caveat is both preload & afterload Caveat is both preload & afterload are decreased abruptlyare decreased abruptly
• Better choice is epidural Better choice is epidural
• Continuous spinal anesthesia does Continuous spinal anesthesia does have a rolehave a role

Postoperative managementPostoperative management
• Equally important for maintainingEqually important for maintaining– OxygenationOxygenation– Avoiding acidosis, hypercarbia, Avoiding acidosis, hypercarbia,
hypothermiahypothermia– Appropriate pain controlAppropriate pain control
•Prevents worsening of PHT or ppt of CHFPrevents worsening of PHT or ppt of CHF
•hypercarbia hypercarbia
www.anaesthesia.co.in