Embed Size (px)
Citation preview
Anesthesia for Patients with Spinal Cord Injury
Dr. AshishModerator : Dr.R.Tope
www.anaesthesia.co.in [email protected]
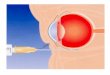
Blood supply
Two posterior spinal arteries Anterior spinal artery – formed by the confluence of
two vertebral arteries
The lower cervical cord is a region of relative ischemia and is vulnerable for ischemic injury should the anterior spinal artery be compromised between the foramen magnum and C8, the cervical watershed.
Spinal Cord Paralysis Levels
C1-C3 All daily functions must be totally assisted Breathing is dependant on a ventilator Motorised wheelchair controlled by sip and puff or
chin movements is requiredC4 Same as C1-C3 except breathing can be done
without a ventilatorC5 Good head, neck, shoulder movements, as well as
elbow flexion Electric wheelchair, or manual for short distances
C6 Wrist extension movements are good Assistance needed for dressing, and transitions from
bed to chair and car may also need assistanceC7-C8 All hand movements Ability to dress, eat, drive, do transfers, and do upper
body washes T1-T4 (paraplegia) Normal communication skills Help may only be needed for heavy household work
or loading wheelchair into car
T5-T9 Manual wheelchair for everyday living Independent for personal careT10-L1 Partial paralysis of lower bodyL2-S5 Some knee, hip and foot movements with possible
slow difficult walking with assistance or aids Only heavy home maintenance and hard cleaning will
need assistance
Treatment of Spinal Injuries
No Current Effective Treatment
Prevention is Key– all current medical and surgical treatments aimed
to prevent further injury to the spinal cord.
Spinal Cord Injuries
May occur with neck or back trauma Associated with blunt head trauma,
especially when casualty is unconscious Can occur with penetrating trauma of
vertebral column Improper handling may cause further injury
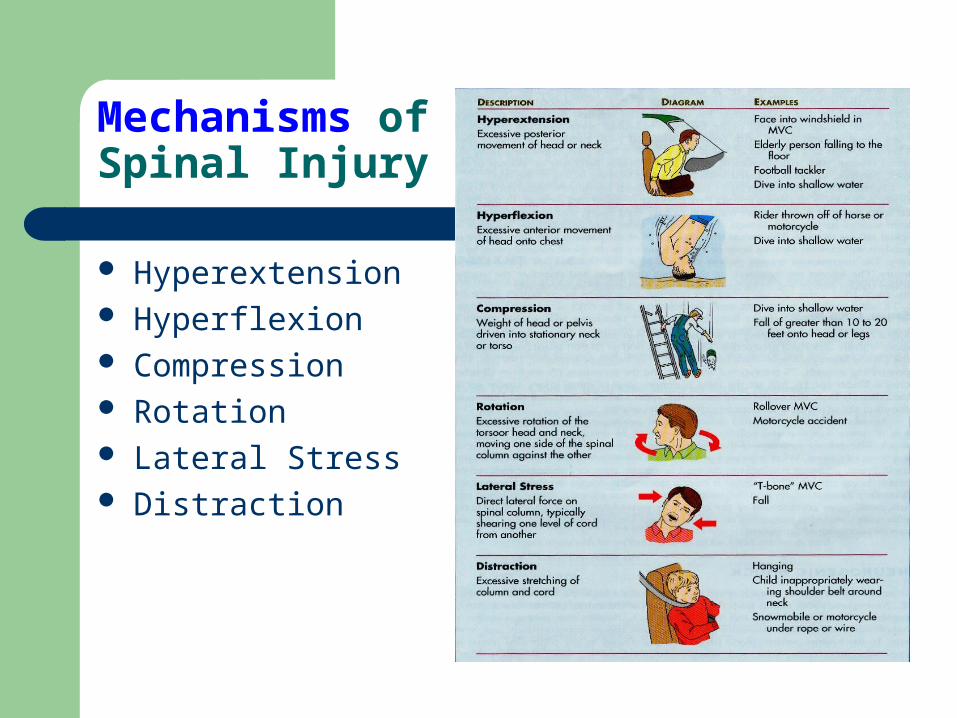
Mechanisms of Spinal Injury
Hyperextension Hyperflexion Compression Rotation Lateral Stress Distraction
Pathophysiology
Damage – Begins centrally in grey matter and spreads centrifugally.
Primary insult –B/W Time of injury and initial careSecondary insult – Delayed swelling Continued mechanical trauma Low perfusion Endogenous factors Initial segmental loss can be withstood because
only small portion of grey matter neuronal pool is involved.
– ASIA A: Complete: no motor or sensory function is preserved in the sacral segments S4-S5
– ASIA B: Incomplete: sensory but NOT motor function is preserved below the neurological level and includes the sacral segments
– ASIA C: Incomplete: motor function is preserved below the neurological level and more than half of key muscles below the neurological level have a muscle grade <3
– ASIA D: Incomplete: motor function is preserved w/ muscle grade > 3
– ASIA E: Normal
Diagnosis and management of acute spinal cord injury
Initial assessment and immobilization Resuscitation and medical management Radiological diagnostics Anaesthesia management Surgical therapy Post op critical care management
Initial assessment and immobilization
*HistoryPain/paresthesiasTransient or persistent motor or sensory symptoms
*Physical ExaminationAbrasions/hematomaTendernessInterspinous process widening
Immobilize the casualty’s head and neck manually
Apply a cervical collar, if available, or improvise one
Secure patient to short spine board if extracting from a vehicle
Secure head and neck to spine board for extraction
Transfer patient to long spine board as soon as feasible
Logroll in unison Stabilize head and neck
with sandbags or rolled blankets
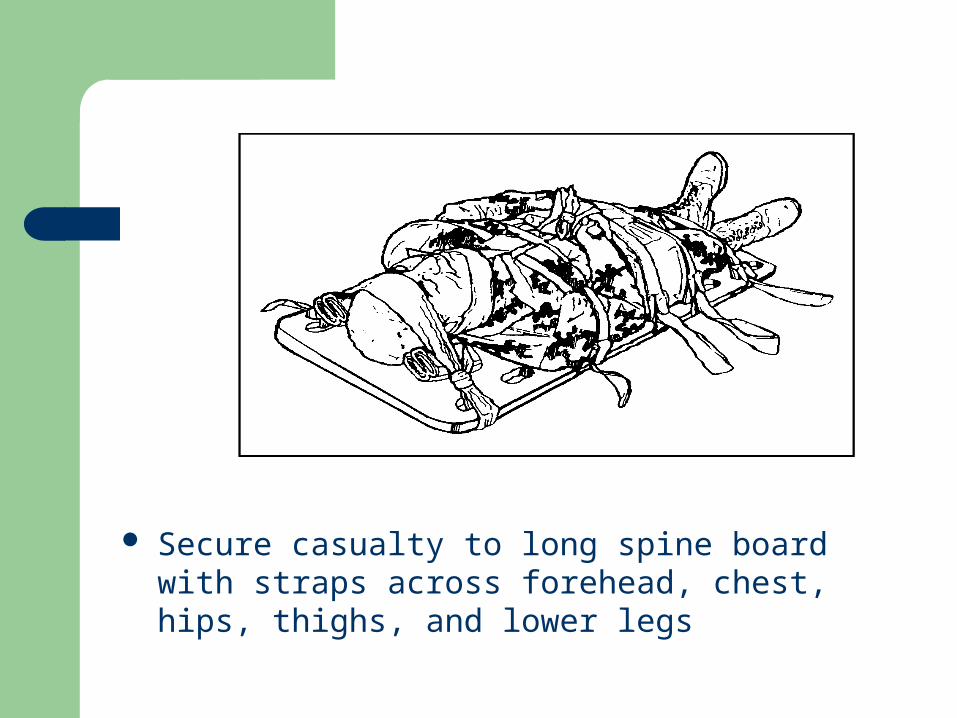
Secure casualty to long spine board with straps across forehead, chest, hips, thighs, and lower legs
Resuscitation and medical management ATLS principles
Airway Breathing Circulatory Neurologic Classification Spinal Imaging GastroIntestinal System Genitourinary System Skin
Airway
Risk Associated with Level of InjuryDecision to IntubateAirway Intervention
Risk Associated with Level of Injury cont’d
Ventilatory Function– C1 - C7 = accessory muscles– C3 - C5 = diaphragm
“C3-4-5 keeps the diaphragm alive!– T1 - T11 = intercostals– T6 - L1 = abdominals
Decision to Intubate:
Need for Artificial Airway is Usually Related to Resp Compromise e.g.
– Loss of innervation of the diaphragm (C 3-4-5 keep the diaphragm alive)– Fatigue of innervated resp muscles – Hypoventilation – SaO2 <60, PaCO2 >45– V/Q mismatch – PaO2/FiO2 <250– Secretion retention– Atelectasis
Decision to Intubate Related to Neurological Level
Occiput - C3 Injuries (ASIA A & B)– Require immediate intubation
and ventilation due to loss of innervation of diaphragm
Decision to Intubate Related to Neurological Levelcont’d
C4-C6 Injuries (ASIA A & B)– Serious consideration for prophylactic
intubation and ventilation if: Ascending injury (requires serial M/S
assessment by a trained clinician)Fatigue of unassisted diaphragmInability to clear secretions
Airway Intervention
Maintaining Spinal Precautions– Supine position
Maintain neutral C-spine– Remove rigid collar and sandbags– Manually stabilize C-spine2 person technique:
– 1st person to provide manual in-line stabilization (not traction) of C-spine
– 2nd person intubates

Complications of cervical spine immobilization
Airway:delayed tracheostomy-poor oral hygeine Breathing: prolonged mechanical ventillation-VAP Circulation:difficult central line insertion and access,
increased thromboembolism Neurological: increased ICP Gut: gastrostasis,reflux and aspiration;delayed
enteral nutrition Skin: pressure sores around collar Staffing: minimum 4 for log rolling; cross infection
Breathing
Cough Function C1-C3 = absent C4 = non-functional C5-T1 = non-functional T2-T4 = weak T5-T10 = poor T11 & below = normal
Breathing cont’d
Vital Capacity (acute phase) C1-C3 = 0 - 5% of normal C4 = 10-15% of normal C5-T1 = 30-40% of normal T2-T4 = 40-50% of normal T5-T10 = 75-100% of normal T11 and below = normal
Breathing cont’d
SCI Respiratory Sequale– Atelectasis– Ventilatory failure
(PaCO2 > 50mmHg and pH < 7.30)
– Increased secretions– Pneumonia– Pulmonary emboli– Pulmonary edema (Autonomic)
Breathing cont’d
Intervention
– O2 therapy
– Assisted ventilation – Medications (bronchodilators)
Circulatory
Spinal Shock
Temporary suppression of all reflex activity below the level of injury
Occurs immediately after injury
Intensity & duration vary with the level & degree of injury
Neurogenic Shock
The body’s response to the sudden loss of sympathetic control
Distributive shock
Occurs in people who have SCI above T6 (> 50% loss of sympathetic innervation)
Hemodynamic Instability: Intervention
First Line: Volume |Resuscitation (1-2 L)
Second line: Vasopressors- (dopamine/norepinephrine) to counter loss of sympathetic tone and provide chronotropic support to the heart
Hemodynamics and Cord Perfusion
Options:– Avoid hypotension – Maintain MAP 85-90mmHg for first 7 days
if possible
Bradycardia: Intervention
Prevention:– Avoid vagal stimulation– Hyperventilate and hyperoxygenate prior to
suctioning– Pre-medicate patients with known hypersensitivity
to vagal stimuli Treatment of Symptomatic Bradycardia:
– Atropine 0.5 - 1.0 mg IV
Neurological Classification
– Motor and sensory assessment – ASIA Impairment Scale (A-E)– Clinical Syndromes (patterns of incomplete injury)
Spinal Shock
An immediate loss of reflex function, called areflexia, below the level of injury
Signs: – Slow heart rate– Low blood pressure– Flaccid paralysis of skeletal muscles– Loss of somatic sensations– Urinary bladder dysfunction
Spinal shock may begin within an hour after injury and last from several minutes to several months, after which reflex activity gradually returns
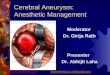
Central Cord Syndrome
Usually involves a cervical lesion May result from cervical hyperextension causing
ischemic injury to the central part of the cord Motor weakness is more present in the upper limbs
then the lower limbs Patient is more likely to lose pain and temperature
sensation than proprioception Patient may complain of a burning feeling in the
upper limbs More commonly seen in older patients with cervical
arthritis or narrowing of the spinal cord
Brown-Sequard Syndrome
Results from an injury to only half of the spinal cord and is most noticed in the cervical region
Often caused by spinal cord tumours, trauma, or inflammation
Motor loss is evident on the same side as the injury to the spinal cord
Sensory loss is evident on the opposite side of the injury location (pain and temperature loss)
Bowel and bladder functions are usually normal
Person is normally able to walk although some bracing or stability devices may be required
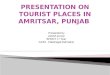
Anterior Spinal Cord Syndrome
Usually results from compression of the artery that runs along the front of the spinal cord
Compression of SC may be from bone fragments or a large disc herniation
Patients with anterior spinal cord syndrome have a variable amount of motor function below the level of injury
Sensation to pain and temperature are lost while sensitivity to vibration and proprioception are preserved
Cauda Equina Syndrome:
Injury to the lumbosacral nerve roots w/ in the neurocanal resulting in areflexive bladder, bowel and lower limbs
Spine Imaging
the Asymptomatic Patient – Option - Xray not needed in alert, sober, compliant
patient without neck pain and tenderness or major distracting injuries
Symptomatic Patient – Standard – Ap lat and odontoid view– Option – discontinue protection after….
normal and adequate dynamic radiography, or normal MRI within 48hrs of injury, or at the discretion of treating MD
CT myelogram – Bony detail of fracture site, and anatomic relation of segment to spinal cord.
MRI – anterior discs, ligamentum flava & cord contusion.
GI System
Risk of aspiration is high d/t:
– cervical immobilization– local cervical soft tissue swelling– delayed gastric emptying
Parasympathetic reflex activity is altered, resulting in:
– decreased gut motility and
– often prolonged paralytic ileus
GI Intervention- Nasogastric tubeIV H2 blockers
GU Intervention – Catheterisation
Skin Intervention – *Remove spine board *Turn or reposition individuals with SCI initially
every 2 hours in the acute phase if the medical condition allows.
Pharmacologic Therapy
Methylprednisolone-controversial – 30mg/kg IV loading dose + 5.4 mg/kg/hr (over
23hrs) effective if administered within 8 hours of injury
– If initiated < 3hrs continue for 24 hrs, if 3-8 hrs after injury, continue for 48hrs (morbidity higher - increased sepsis and pneumonia)
Thromboprophylaxis - LMWH, discontinued at 3months
Secondary Interventions
Without mechanical compression on CT myelogram – External stabilisation
Mean arterial pressures are kept b/w 80-90 mmHg and CO kept ( N/ high N )
Dopamine infusion may be necessary
Anaesthesia Management
Pre op assessmentMedical historyPremedication and pt. EducationAirway managementPositioningFluid requirementsSpecial intraop requirements(wake up test)Post op pain and pulmonary toilet
Airway evaluationMP classification and range of neck mobility and elicitation of
pain/ neurological symptom Pulmonary evaluationDuring spinal shock (3 days – 6 wks) ABG- assess adequacy of ventilation, intubation if
hypoxemia or hypercapnia (on O2 mask)Chronic stage PFT and Chest X ray – Restrictive pattern (FEV1&FVC)
Severity of functional impairment related to – Angle of scoliosis, No of vertebrae, cephalad location of curve and loss of normal kyphosis.
Respiratory function should be optimised – Treating infectionBronchodilation Chest physiotherapy
Cardiac evaluationECG – myocardial ischemia Cardiovascular instability evidenced by hypotension,
hypertension, brady & arry. – assessment of cardiac reserve and to optimise circulatory volume according to cardiac function and peri. Vas. Tone.
Pacemaker – persistently bardycardic.High spinal cord injury – initially spinal shock,autonomic
dys,impaired LVF and later autonomic dysreflexia.
Neurological evaluationDocument preexisting deficitsNeurological dys may dictate intubation
tech,monitoring and choice of agents.
PharmacologyAltered P/K because of muscle wasting,inc volume
of distribution,dec serum albumin
Preop preparation
Hb, Hct, WBC and urinalysis
Other tests indicated by history
SE, BUN, Creatinine, PT,aPTT, Platelet count, ECG, Chest radiograph, ABG and PFT.
Echo – to assess LV function pulmonary artery pressures and stress echo in sedentary patients
Premedication If anxious IV midazolam Under supervision Atropine if HR < 70 – Dose 0.04mg/kg H2 receptor blocker/ PPIInduction Unnecessary/ contraindicated for unconscious,
recently injured patients with spinal cord trauma / those with severe shock.
Technique of intubationElective - fiberoptic intubation
Emergency – MILS with rapid sequence
Maintenance
Nitrous oxide, inhalation agent
Positioning
Goals
Adequate surgical exposure
Anatomic position of extremities & head
Avoid abdominal pressure
Adequate padding
Various positions
a) Prone
b) Supine
c) Sitting (obsolete
PRONE POSITION MOST COMMONLY USED
EYES:
Corneal abrasionOptic neuropathyRetinal artery occlusion
HEAD & NECK
Venous and lymphatic obstuction
ABDOMENImpaired ventilationDecreased CO
Monitoring
Neurological
Wake up test SSEP Transcutaneus MEP
PhysiologicalPulse oximetryContinuous ECG monitoring EtCo2CVPTemperatureUrine outputInvasive BPSwan Ganz catheter?
Post operative pain relief
• NSAIDS (IM,IV,P/R)• IV opiods (Intermitent / continuous infusion )• PCA
Post op critical care management
Indications for post op ventilation – Preexisting NM disorder Severe restrictive – VC <35% Obesity / RVF Prolonged surgery Surgical invasion of thoracic cavity Blood loss > 30ml/kg
post op contd Prepare for weaning
Adequate nutrition and metabolic state
Infection – May be masked(Poikilothermia)
Optimal fluid management
Treat mechanical impairment to breathing like abd distention, tight halo cast, position
Psychological preperation
Post op contd
Chest Physiotherapy – Postural drainage, chest wall percussion and vibration, tracheal suctioning and breathing exercises.
Cough – Glossopharyngeal breathing and huffing.
Breathing exercises
Perioperative complications of spine surgery
a) Airway obstruction : edema, hematoma,recurrent laryngeal nerve palsy.
b) Respiratory: motor paralysis and infection (pneumonia).c) Cardiovascular: hypotension, bradycardia, arrhythmias,
hypertension ( spinal cord injury, carotid sinus stimulation).
d) Neurological: Injury to nerve roots – as a result of direct surgicalmanipulationInjury to lower cranial nerves – VII, IX, X, XIIInjury to peripheral nerves - as a result of positioningInjury to spinal cord .
e) Vessel injury – vertebral and carotid artery during dissection
f) Tracheal and oesophageal injury
g) CSF leaks - due to tear of dural and arachnoid membranes can lead to meningitis,
pseudomeningocoele, permanent CSF fistula
h) DVT – seen in 30% of neurosurgical patients, especially those who had been paraplegic. Pulmonary embolism may occur
Outcome
Acute spinal injury who survive >24hrs,85%alive at 10years
Most common causes of death-pneumonia, non-ischemic heart disease (occult autonomic dysfn), suicide (lifelong impact of injury)
www.anaesthesia.co.in [email protected]