Embed Size (px)
Citation preview

Anemia in PregnancyAnemia in Pregnancy
Presenter: Dr. Imran KhanPresenter: Dr. Imran Khan
Moderator: Prof. ChandralekhaModerator: Prof. Chandralekha
www.anaesthesia.co.in [email protected]

Definition Definition
ClassificationClassification
Hematological changes in pregnancyHematological changes in pregnancy
Problems related to AnemiaProblems related to Anemia
Anaesthetic considerationsAnaesthetic considerations

DefinitionDefinition
Anemia - insufficient Hb to carry out O2
requirement by tissues.
WHO definition : Hb conc. 11 gm %
CDC definition : Hb conc. < 11gm % in 1st and 3rd trimesters and < 10.5 gm% in 2nd trimester
For developing countries : cut off level suggested is 10 gm %
- WHO technical report Series no. 405, Geneva 1968
Centre for disease control, MMWR 1989;38:400-4
Anemia - insufficient Hb to carry out O2
requirement by tissues.
WHO definition : Hb conc. 11 gm %
CDC definition : Hb conc. < 11gm % in 1st and 3rd trimesters and < 10.5 gm% in 2nd trimester
For developing countries : cut off level suggested is 10 gm %
- WHO technical report Series no. 405, Geneva 1968
Centre for disease control, MMWR 1989;38:400-4

Increased mortality figuresIncreased mortality figures
ConditionCondition Increased Increased mortality/morbidity mortality/morbidity below hemoglobinbelow hemoglobin
ReferenceReference
Old ageOld age <11 g/100 ml<11 g/100 ml Culleton 2006
Heart valve Heart valve operationoperation
<12 g/100 ml<12 g/100 ml Cladellas 2006
Heart failureHeart failure <11 g/100 ml<11 g/100 ml Ezekowitz 2003
PTCAPTCA <10 g/100 ml<10 g/100 ml Lee 2004
COPDCOPD <13 g/100 ml<13 g/100 ml Cote 2007
Figures are consequences of the reduced oxygen transport due to anemia

Degree Hb% Haematocrit (%)
Moderate 7-10.9 24-37%
Severe 4-6.9 13-23%
Very Severe <4 <13%
Degree Hb% Haematocrit (%)
Moderate 7-10.9 24-37%
Severe 4-6.9 13-23%
Very Severe <4 <13%
WHO Classification of Anaemia WHO Classification of Anaemia

Magnitude of ProblemMagnitude of ProblemMagnitude of ProblemMagnitude of Problem
Globally, is about 30 %Globally, is about 30 %
In developing countries & In developing countries & India, incidence is around India, incidence is around 40 – 90%. 40 – 90%.
Responsible for 40% of Responsible for 40% of maternal deaths in third maternal deaths in third world countries.world countries.
Important cause of direct Important cause of direct and and indirect maternal deathsindirect maternal deaths
- Vitere FE Adv Exp Med Biol 1994;352:127- Vitere FE Adv Exp Med Biol 1994;352:127
Globally, is about 30 %Globally, is about 30 %
In developing countries & In developing countries & India, incidence is around India, incidence is around 40 – 90%. 40 – 90%.
Responsible for 40% of Responsible for 40% of maternal deaths in third maternal deaths in third world countries.world countries.
Important cause of direct Important cause of direct and and indirect maternal deathsindirect maternal deaths
- Vitere FE Adv Exp Med Biol 1994;352:127- Vitere FE Adv Exp Med Biol 1994;352:127

Relation b/w symptoms of anemia to the Relation b/w symptoms of anemia to the hemoglobin level hemoglobin level
Hemoglobin (g/100 Hemoglobin (g/100 ml) ml)
SymptomsSymptoms
9-119-11 Slight pallor and tachycardiaSlight pallor and tachycardia
7-87-8 More pronounced pallor, plus dyspnea More pronounced pallor, plus dyspnea on exertionon exertion
66 All the above, plus many complain of All the above, plus many complain of weaknessweakness
33 All the above, plus people complain of All the above, plus people complain of dyspnea at restdyspnea at rest
2-2.52-2.5 All the above, plus congestive heart All the above, plus congestive heart failure may occurfailure may occur
Varat 1972 and Linman 1968

Brannon 1944, Duke 1969, Roy 1963

100
80
60
40
20
020 40 60 80 100
%S
atu
rati
on
PO2 (mmHg)
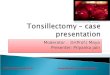
P50
Temp, CO2 , 2-3 DPG; pH(favors unloading)
OxygenTransport
P50
Temp, CO2 , 2-3 DPG; pH(favors loading) Bohr Effect

Physiological Changes
Blood volume increases +1500 ml
RBC 450 ml
Plasma 1000 ml
– Increase starts in the first trimester and gradually rises
Increased erythropoiesis but since more plasma is produced, a relative decrease in Hb and PCV
Iron stores +/- 500 mg
Iron requirements +/- 800 mg [500 mg for mother; 300 mg for fetus]. Hence need for supplementation
Hypercoagulable state increased risk of thrombosis

PROBLEMS RELATED TO PROBLEMS RELATED TO ANAEMIA..ANAEMIA..
OXYGEN AVAILABLE TO TISSUESOXYGEN AVAILABLE TO TISSUES
MANNER IN WHICH BODY COMPENSATESMANNER IN WHICH BODY COMPENSATES

COMPENSATORY COMPENSATORY MECHANISMSMECHANISMS
Increase in CORightward shift of ODCDecrease in blood viscosityIncrease in 2,3-DPG concentration
in RBCRelease of renal erythropoietin leading to stimulation of erythroid precursors in bone marrow

SymptomsSymptoms
Irritability
Fatigue
Weakness
Dizziness
Palpitation
Infection

Clinical FeaturesClinical FeaturesClinical FeaturesClinical Features
Pallor of skin And m/m
Edema
PlatynychiaKoilonychia PlatynychiaKoilonychia
Glossitis
Stomatitis
Tachycardia
Soft ejectionsystolic murmur
SignsSigns

Physiological anaemia of pregnancy
Acquired
Causes of Anaemia Causes of Anaemia Causes of Anaemia Causes of Anaemia
Nutritional-• Iron deficiency Anaemia
Folic Acid deficiency anaemia
Vitamin B12 deficiency anaemia
Infections- Malaria, hookworm infestation, etc
Haemorrhagic- Acute or chronic blood loss
Bone marrow suppression- Aplastic anaemia, drugs,
Renal disease
Genetic - haemoglobinopathies – sickle cell disease, thalassaemia
Nutritional-• Iron deficiency Anaemia
Folic Acid deficiency anaemia
Vitamin B12 deficiency anaemia
Infections- Malaria, hookworm infestation, etc
Haemorrhagic- Acute or chronic blood loss
Bone marrow suppression- Aplastic anaemia, drugs,
Renal disease
Genetic - haemoglobinopathies – sickle cell disease, thalassaemia

Physiological Anaemia
Caused by pregnancy changes
Hb can vary from 10.0-14.5 g/dl
“Pathological” anaemia usually defined as Hb level <10.5 g/dl

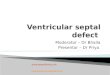
Iron RequirementIron Requirement
Iron Absorption Iron Absorption
11
Amount of iron in the body
Amount of iron in the body
Iron Loss
Skin
Urine
Feces
Menstruation
1-2mg/d
1-2mg/d
20-30mg/c20-30mg/c

Early Pregnanc
y2.5 mg / day
32 to 40 weeks
6.8 mg / day
TOTAL800 – 1000
mg
20 to 32 weeks
5.5 mg / day
RBC =500mgFetus+Placenta =450mgThird stage blood loss=200mgTotal = 1150mg
Iron Requirement During PregnancyIron Requirement During Pregnancy

Laboratory Diagnosis of AnaemiaLaboratory Diagnosis of Anaemia
IDAIDA ThalassemiaThalassemia Chronic DiseasesChronic Diseases
Serum IronSerum Iron Decreased Decreased Normal / Normal / Increased Increased
DecreasedDecreased
TIBCTIBC IncreasedIncreased NormalNormal Decreased or NDecreased or N
TransferrinTransferrin
SaturationSaturation
DecreasedDecreased N or IncreasedN or Increased N or DecreasedN or Decreased
Serum FerritinSerum Ferritin DecreasedDecreased N or IncreasedN or Increased NN
Marrow IronMarrow Iron Decreased / Decreased / absentabsent
N or IncreasedN or Increased NN
Therapeutic test Therapeutic test with oral ironwith oral iron
Rise in HbRise in Hb No rise in HbNo rise in Hb No riseNo rise

Reason For Increased Reason For Increased Incidence Of AnemiaIncidence Of Anemia
Reason For Increased Reason For Increased Incidence Of AnemiaIncidence Of Anemia
Poor pre-pregnancy iron balance Poor pre-pregnancy iron balance
Improper supplementation Improper supplementation
Repeated childbearingRepeated childbearing
Lack of awareness and illiteracyLack of awareness and illiteracy
GI infections and infestationsGI infections and infestations
Poor pre-pregnancy iron balance Poor pre-pregnancy iron balance
Improper supplementation Improper supplementation
Repeated childbearingRepeated childbearing
Lack of awareness and illiteracyLack of awareness and illiteracy
GI infections and infestationsGI infections and infestations

ANAESTHETIC CONSIDERATIONSANAESTHETIC CONSIDERATIONS
Elective LSCS - Elective LSCS - Emergency LSCS - Blood TransfusionEmergency LSCS - Blood Transfusion
Not a Day before SurgeryNot a Day before Surgery
Fresh ( 2, 3 DPG Fresh ( 2, 3 DPG 24 HRS. ) 24 HRS. ) Chronic, Well compensated- Hb upto 8 gm% Chronic, Well compensated- Hb upto 8 gm% Safe Safe
Avoid Hypoxia ( ↑ Fi OAvoid Hypoxia ( ↑ Fi O22 ) , Maintain C V S Stability ) , Maintain C V S Stability Avoid Hypovolemia and Aortocaval CompressionAvoid Hypovolemia and Aortocaval Compression Minimize -Minimize -
• Lt. O D CLt. O D C
• HyperventilationHyperventilation
• AlkalosisAlkalosis
• HypothermiaHypothermia
• ↓ ↓ 2, 3 DPG2, 3 DPG Monitor- Complications like CCF & ShockMonitor- Complications like CCF & Shock

CHOICE OF ANAESTHETIC TECHNIQUECHOICE OF ANAESTHETIC TECHNIQUE
Regional Anaesthesia - Regional Anaesthesia -
Safe - Safe - Hb > 9 gm% OR 8 gm% Hb > 9 gm% OR 8 gm% No Cardiac Decomp. No Cardiac Decomp.
Avoid - Avoid -
•Hb < 8 gm % , Hb < 8 gm % ,
•Hemostatic Abnormalities, Hemostatic Abnormalities,
•Megaloblastic AnemiaMegaloblastic Anemia Precautions - Precautions - Fi OFi O2 2 , Low Dose L. A. + Opioid, Low Dose L. A. + Opioid
Disadvantages - Disadvantages - PreloadingPreloading
-- Sympath. Block Sympath. Block Ppt. Hypotension Ppt. Hypotension

ADVANTAGES OF REGIONAL ADVANTAGES OF REGIONAL ANAESTHESIAANAESTHESIA
Mother is aware of Child Birth Mother is aware of Child Birth
Less blood lossLess blood loss
Analgesia can be extended Analgesia can be extended post op period post op period
No risk of AspirationNo risk of Aspiration
No risk of Complications d/t intubation and drug induced S/ENo risk of Complications d/t intubation and drug induced S/E

EPIDURAL V/ S S.A.B.EPIDURAL V/ S S.A.B.
Adv. Of Epidural - Adv. Of Epidural - Less precipitous fall in B>PLess precipitous fall in B>P
- - Post Op AnalgesiaPost Op Analgesia
Disadv. Of Epidural - Disadv. Of Epidural - Time ConsumingTime Consuming
- - L.A Toxicity. L.A Toxicity.
-- Patchy, Inadeq. Blocks Patchy, Inadeq. Blocks
Adv of SAB. - Adv of SAB. - Easy Rapid onset with High Success Rate Easy Rapid onset with High Success Rate
-- Small Vol. of drug Small Vol. of drug Less Toxicity Less Toxicity
- - low dose L.A + Opioidlow dose L.A + Opioid
» Less Hypotension» Less Hypotension
» Intense surgical Anaesthesia.» Intense surgical Anaesthesia.
» Post op analgesia» Post op analgesia
-- Fine bore needle Fine bore needle No P.D.P.H. No P.D.P.H.

C. S. E.C. S. E.
S.A.B. - S.A.B. - Speed of Onset Speed of Onset
-- Reliability Reliability
-- Low Toxicity Low Toxicity
++
Epidural Catheter - Epidural Catheter - Control of Height of Block Control of Height of Block
- - Supplement Inadeq. BlockSupplement Inadeq. Block
-- Post Op Analgesia Post Op Analgesia

GENERAL ANAESTHESIAGENERAL ANAESTHESIA
choice - choice - If Hb = 8 gm % with cardiac decomp..If Hb = 8 gm % with cardiac decomp..
-- Hb < 8 gm % Hb < 8 gm %
Adv. - Adv. - Rapid InductionRapid Induction
-- less hypotension and better CVS. stability less hypotension and better CVS. stability
-- Control of Airway and Ventilation Control of Airway and Ventilation
-- Severe Anemia Severe Anemia Post op Ventilatory Support Post op Ventilatory Support
- - No Anxiety of being AwakeNo Anxiety of being Awake
Disadv. Disadv. --Failed IntubationFailed Intubation
-- Gastric Aspiration Gastric Aspiration

G. A. TECHNIQUEG. A. TECHNIQUE
Supine with wedge under right hipSupine with wedge under right hip
Pre oxygenationPre oxygenation
Thio+ Sux/Roc.Thio+ Sux/Roc.
Problems - Problems - Safe cricoid pressure Safe cricoid pressure
-- Failed Intubation Failed Intubation
-- Awareness Awareness
-- Neonatal Effects Neonatal Effects
» I. D. I. > 8 MIN.» I. D. I. > 8 MIN.
» U. D. I. > 3 MIN.» U. D. I. > 3 MIN.
Severity of anemia- Post Op VentilationSeverity of anemia- Post Op Ventilation

THANK YOUTHANK YOUwww.anaesthesia.co.in [email protected]

ODCODC