Embed Size (px)
Citation preview

Ravinder Kumar Batra
Professor
Department of Anaesthesiology, AIIMS
Obstructive Jaundice
www.anaesthesia.co.in [email protected]

Chief Complaints
4O yr male presented with :
• Yellow coloration of Eye -8 months• Yellow coloration of urine – 8 months

History of present illness
• Gradually progressive yellowish coloration eye• Recurrent episode of itching• White stools 4 months back, persisted for 2
months• Abdominal pain- Right upper quadrant- 6
months
• Generalized weakness & fatigability- 6 months• Weight loss 75-50 kg in 7 months• Reduced appetite• No fever

H/o past illness• Typhoid fever – 9 months back• No h/o DM, HT, TB, Chest pain• No previous surgery
Personal History• Normal Bowel & bladder habits• Smoker – 25 yrs• Non-alcoholic• Effort tolerance good

Important points in History
• Duration of Jaundice• Progress & previous attacks of jaundice• Prodrome• Fever• Abdominal pain: Biliary/pancreatic/Dull• Pruritis, Colour of urine and stool• Drug ingestion• Manifestations of fat soluble Vit deficiency• Weight loss

History suggestive of• Normal colored urine/cola color in hemolysis• Recurrent episodes• Recurrent anaemia• No prodrome
• Pain• Chills, fever, systemic illness• Biliary surgery
Unconjugated hyperbilirubinemia/hemolysis
Bile duct stones/cholangitis/obstructive jaundice

History suggestive of
• Contact with other jaundiced patient• History of injections or blood transfusions• Exposure to drugs• Prodrome of anorexia, nausea, vomiting
• Pruritis• Clay coloured stools
VH/Drug induced Hepatitis
Cholestasis

Examinations
General Physical Examination:– Pulse 88/min,BP 110/70
Pallor +, Jaundice +– No Lymphadenopathy
Per abdomen– Soft non-tender– Gall bladder palpable– Liver: 3cm below costal margin– No free fluid

Airway Examination
• MMP grade II• Mouth opening: Adequate• Teeth intact, no loose tooth





General Examination
• Body mass index• Vital signs: Pulse• Pallor: GI bleeding, Hemolysis• Icterus• Pedal oedema: hypoproteinemia/cirrihosis• Shiny nail & scratch marks (pruritis)• Xanthoma• Ecchymosis, Bitot spots (Vitamin deficiency)

Abdomial Examination
• Abdominal distension, distended veins, scar• Hepatomegaly• Splenomegaly• Gall bladder or any mass, • Free fluid

Define Jaundice and where all you will look for this?

• Yellowish pigmentation of the sclera, skin, mucous membrane & other tissues: Jaune
• Excess plasma bilirubin
• Normal range < 1 mg/dl
• (I: 0.2-0.7mg/dl;D:0.1—0.4mg/ dl, <5% in Conjugated form)
• Clinically obvious 2-3 mg/dl
• Sites – Sclera, undersurface of the tongue, palms, nails, skin, hard-palate
• High Affinity for Collagenous tissue

Describe Bilirubin Formation & Excretion?

Bilirubin Metabolism
Ret En System Plasma Liver BileHeme oxygenase Biliverdin reductase
Haem BVD UCB UCB UCB
Albumin
70% 30% BMG BMG
BMG & BDG
Hb other BDG BDG
haemoproteins
Glomerulus Urine
Bilirubin production: 250-350mg/day

Portal vein

How will you Differentiate the three types of Jaundice Biochemically?

Features Prehepatic (hemolytic)
Intrahepatic Heptocellular
Post-hepatic (Obstructive)
UCB ↑ Normal Normal
CB Normal ↑ ↑
AST or ALT Normal ↑↑ Normal
SAP Normal Normal ↑↑
Urine Bilirubin
Absent Present Increased
Urobilinogen Increased Present Absent

Features Prehepatic (hemolytic)
Intrahepatic Heptocellular
Post-hepatic (Obstructive)
Plasma Albumin
Normal Decreased Normal or decreased
PT Normal Increased Increased but correccted by Vitamin K

How will you Evaluate a Case of Jaundice?

HISTORY clinical evaluation
Hemolysis Vs Cong Hyperbilirubinemia Normal
Abnormal
AST, ALT, ALP
USG if biliary obstruction is suspectedNon-dilated
ducts Dilated ducts
Hepatocellular jaundice
Biliary ObstructionEvaluation for:
•Acute vs Chronic•Etiology
Evaluation for: •Cause•ExtentGGT, Viral Markers,
Autoimmune Markers Liver Biopsy
ERCP, MRCP, PTC, CT

Investigations
• Bilirubin, Serum enzymes (SGOT, SGPT)• SAP, GGT, 5-nucleotidase• Proteins: Albumin, Globulins, INR or PT, markers• Ultrasound, CT scan• ERCP• Percutaneous Transhepatic Cholangiography• Magnetic resonance cholangiopancreaticography• Liver Biopsy

What are the Pathophysiological consequences of Obstructive / Cholestatic Jaundice?

Consequences of Cholestasis
Retention of bile salt in liver•Decreased hepatocyte function •Dysfunction of Cyto -450•Albumin & clotting factors synthesis decreased•Decreased Kuffer cell activityBile constituents in serum•Jaundice, Pruritis•CVS depression•Nephrotoxicity•Hypercholesterolemia, atheroma, Xanthoma

Consequences of Cholestasis
Absence of bile in Intestine•Escape of endotoxins into portal blood•Malabsorption of fats, Vit A, D, E & K•Clay colored stools
Pruritis: Exact pathology is not known:Central mechanism: ↑ central opioidoergic tonePeripheral: accumulation of bile acids, histamine, serotonin & endogenous opioids

Anaesthetic Problems associated with Obstructive
Jaundice

– Impaired myocardial contractility– Bradycardia– Vasodilatation ↓ ability to mobilise blood from
splanchnic vasculature during haemorrhage– ↓ sensitivity to vasopressors
Hypotension & circulatory collapse Small blood losses poorly tolerated Replace volume losses immediately in
perioperative period
Anaesthetic Problems: CVS

Anaesthetic Problems: Renal system
Etiology Multifactorial
• Arterial hypotension-myocardial depression
• Reduction in intravascular volume
• Nephrotoxicity - bile salt, endotoxins & Inflammatory mediators
– Incidence 5 -10%, mortality: 32 – 100%
– Level of hyperbilirubinemia correlates with postoperative decrease in creatinine clearance

Anaesthetic Problems: Sepsis
• Associated cholangitis and bactibilia• Escape of endotoxins from intestine portal
blood • ↓ kuffer cell activity
Prevention Perioperative antibiotics Preoperative oral bile salts

Anaesthetic Problems: Coagulopathy
• Vit. K malabsorption
(Activation II,VII,IX,X ) ↑ PT
Pre-op. Vit. K 10 mg OD × 3 days
• long lasting biliary obstruction Sec.
biliary cirrhosis ↓ syn. of coag factors
(poor prognosis) transfusion of FFP

Anaesthetic Problems
• Multiple Vitamin Deficiency - A, D, E, K ( A - night blindness ,D – osteoporosis
and ms weakness, E- leg cramps ,K- easy bruising )
• Haemorrhagic gastritis and stress ulcer • Impaired wound healing• Altered drug handling due to cholestasis• Long standing extrahepatic biliary
obstruction > 1yr → biliary cirrhosis → problems of liver dysfunction

Investigations for Assessing Liver Functions?

Assessment for liver cell injury
• S. Bilirubin • Transaminase SGOT/SGPT - 0 – 35 IU/L
SGOT -extrahepatic- heart/sk ms/kidney/brain:less specific
SGPT - primarily found in liver, more specificAlcoholic hepatitis SGOT/SGPT > 2 (deficiency
of pyridoxine-5-PO4 )
• Alkaline phosphatase – 35 – 100 IU/L Extrahepatic- bone, intestine, liver, placenta• 5- Nucleotidase - confirms hepatic origin of ALP• Gamma Glutamyl Transpeptidase – most
sensitive indicator of biliary tract disease

Aminotransferases Alk PO4 Diag. Likelihood
Viral hep. Obstr.
> X 6 < X 2.5 90% 10%< X 6 > x 2..5 10% 80%
Parenchymal diseases ultimately produce an obstructive component & Long standing Obstructive diseases cause cellular dysfunction

Assessment of Synthetic Ability of Liver
• Prothrombin time – factors II, VII, IX & X short t ½ 2 - 6hr Good Indicator of liver fn. in both Acute &
Chronic Liver disease. D/D - Obst. jaundice parentral vit. K → PT normalises in 24 – 48 hrs• Serum albumin – t ½ life - 14-20days
Liver – substantial reserve for alb. syn.
Not a good indicator for acute or mild liver damage
Indicator of severity of chronic liver disease
< 2·5 gm% - severe damage

What are the other Preoperative Investigations
required ?

Preoperative Investigations
• Hb - ↓ in concealed blood loss, haemolysis,
• TLC, DLC - ↑ infection
• Platelet Count , clotting studies - PT, PTTK
• Urea, S. Creatinine, Electrolyte
• HBV, HCV
• Chest X-ray, ECG, blood gases
•

Investigations• Hb-9.7, TLC-16200, PC-4.56 Lac• LFT-S.Bil T-14.0/D11.3/2.7• SGOT/SGPT-183/81, SAP-1493• Urea/Creatinine: 15/1• PT : normal• CxR: Normal• CA-19-9: 10.6U/ml (1.9 -24 u/ml –male)• Side View Endoscopy: Ampulla bulky friable,
ulcerated• Ampullary Biopsy: Few displasia & atypical cells

Investigations
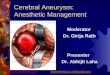
• USG-Abd: solid mass in distal CBD, dilated CBD, Intrahepatic Biliary distension with distended GB with hepatomegaly
• Dual Phase CT: Mass at lower end of CBD with dilated upper stream Biliary system
• Endoscopy US: Mass in uncinate process likely malignant

CT imaging

CT imaging

CT imaging

CT imaging

CT imaging

CT imaging

Case : Diagnosis
Periampullary Carcinoma

What are Troisier’s sign and Courvoisier’s law?

Troisier’s sign
Enlargement of
Left Supraclavicular Lymph Node due to
Secondary involvement seen in
malignancies of
G.I.T., Breast and Testis.

Courvoisier’s law
If the CBD is obst. due to calculus , the GB is usually not distended owing to previous inflammatory fibrosis.
In obstr. of the CBD due
to growth, the GB becomes distended in order to reduce the press. in the biliary system.

What are the Surgical Procedures done for Obstructive Jaundice?

Ca GB: Radical Cholecystectomy with wedge ressection and CBD excision
Choledocholithiasis: ERCP removal or CBD exploration/ bilio-enteric anastmosis
Cholangio Ca: Liver resection and or local excision of the lesion or Whipple
Biliary Stricture: Hepatico-jejunostomy/ liver resection

Periampullary Ca:
Whipple’s Procedure
Chronic Pancreatits with head Mass: Whipple/ bilio-enteric anastmosis

Whipple’s Procedure
Pancreaticojejunostomy- end to end
Hepatico-jejunostomy – end to side
Gastrojejunostomy – end to side
Feeding Jejunostomy

What are the Risk factors for Operative Mortality in these
patients?

Dixon etal – GUT 1983
• Hematocrit < 30 %, S. bilirubin > 12mg%
• Malignant cause of biliary obstruction
Mortality 60% if above present, 5 % otherwise
Blamey et al 1983 : Brit J of Surg 8 factors
Age >60 , Malignant D, S Bil> 6mg/dl, Hct <30%, TLC>10000,
S. alb <3, S creatinine>1.5, SALP >600
Preoperative Risk factors

Bose et al Ind J Surg 1990
Age >60, Associated DM, Previous Biliary tract
surgery & prolonged surgery
Friedman –Hepatology June1999
• Azotemia, Hypoalbuminemia & Cholangitis
Preoperative Risk factors

What are the anaestheic goals in surgery for an Obstructive Jaundice patient ?

Maintain
• Hepatic oxygen supply –
demand relationship
• Renal function
Anaesthetics Goals

MANTAINING HEPATIC BLOOD FLOW
AVOID :• Sympathetic stimulation•Hypotension (decreased venous return / cardiac output) caused by :
• Haemorrhage• Cardiac depressant drugs • Regional anaesthesia e.g.; thoracic epidural
analgesia •Hypocapnia•Pressure effects caused by
• Surgical retraction• Tumors• Ascites / Laparoscopy
•Hepatic venous congestion caused by • Head down position, IPPV, Rt. side heart failure

Maintaining Renal functionPreoperatively• Avoid NSAIDs & nephrotoxic
antibiotics e.g.; (aminoglycosides)• Oral bile salts to normalize gut flora • Prophylactic antibiotics to prevent sepsis • Drainage stent -↓ Hyperbilirubinaemia PTC, ERCP or papillotomy Intraoperatively • Avoid hypotension & hypoxaemia • Avoid dehydration• Renal dose dopamine?
mannitol/furosemide

Preoperative preparation
• Anxiolytic – oral short acting BDZ
• Oral H2 antagonist
• Vit. K (Obst. J) – 10 mg OD X 3 day,
FFP
• Perioperative broad spectrum
antibiotics
• Oral bile salts

Preoperative preparation for Anaesthesia
• Rehydration and adequate diuresis
1ml/kg/hr
• If Bilirubin > 8 mg% –
• I/V fluid – 1-2 ml/kg/hr.
• Furosemide/ Mannitol
• Catheterization & CVP monitoring

Choice of Anaesthesia?

Choosing appropriate anaesthetic agent
No drug is contraindicated in Cholestatic liver disease per se
Other considerations Coexisting hepatocellular disorderRenal dysfunction Drugs ↑ cholestasis e.g.; chlorpromazine
Anaesthetic agent of choice Not dependent on hepatic metabolism Maintains hepatic O2 supply – demand
relationship

General anesthesia
Induction agent - Thiopentone/Propofol
slow titrated dose → avoid hypotension
→ avoid symp. Stimulation during intubation
• Muscle relaxant
Suxamethonium - RSI
Atracurium (DOC) - Hoffman’s elimination
Vecuronium

Anaesthetic technique Opioids • fentanyl (DOC)- maintains hepatic oxygen
supply – demand • spasm of sphincter of Oddi – incidence < 3%• Bil. colic , false + cholangiogram • T/T naloxone, glucagon, atropine,
nitroglycerine
Volatile Anesthetics• Isoflurane - maintains HBF & oxygen supply IPPV –- Maintain eucapnia Avoid high airway pressures

Drug Duration Metab. Eli. Kid. %
Eli. Liv. %
Sch Ultrashort Butyrylcholinestras 99%
<2 None
Atra Intermediate Hoff & ester 60-90 % Urine & Bile
10-40 None
Cis Intermediate Hoff 77% 16%
Vec Intermediate Liver 30-40% Urine & Bile
40-50 50-60
Roc Long 10-20 85 15
dTc Long None 80%? 20%
Metabolism & Elimination of Ms Relaxants

Regional anaesthesiaas supplement to G.A.
Epidural anaesthesia : Concerns
–Coagulopathy
–Hypotension

Intraoperative Monitoring

Intra Operative Monitoring
Routine
• ECG, NIBP
• SaO2, EtCO2
• Urine output
• Temperature
• NMJ monitoring
Longer & extensive surgeries
• Intra arterial and CVP
• Biochemical: B.Sugar, ABG,
Electrolytes
• Hematology: Hb, PT, PTTK,
TEG

Post-operative Management?

Postoperative management
• Conscious, adequate NM recovery, vitals stable→ extubate → oxygen - enriched air
• Else - Continue IPPV - Correct Fluid & Electrolyte imbalance - Correct hypothermia - Achieve CVS stability• Adequate analgesia & chest physiotherapy• Antibiotics + H2 receptor antagonist• Maintain urine output• Replace blood and blood products

What are the Causes of Cholestasis:
Intrahepatic & Extrahepatic

Extrahepatic: Benign causes
• Choledocholithiasis
• Primary sclerosing cholangitis
• AIDS Cholangiopathy
• Post-surgical stricture
• Pancreatitis

Extrahepatic: Malignant Causes
• Carcinoma gall bladder
• Periampullary Carcinoma
• Cholangiocarcinoma
• Carcinoma of the head of pancreas
• Obstruction of the drug due to metastatic LN

Intrahepatic cholestasis
• Cholestasis phase of AVH• Alcoholic H• Drug induced liver D• Primary biliary cirrhosis• Primary sclerosing cholangitis• TPN

Intrahepatic cholestasis
• Graft-versus-host D• Cholestasis of pregnancy• Sepsis• Benign postoperative Cholestasis• Fibrosing cholestatic hepatitis.

Name the Drugs that lead to Cholestasis Jaundice?

• Estrogen
• Tamoxifen
• Anabolic steroid
• Azathioprine
• Chlorpromazine
• Carbamazepine
• Antibiotics- Erythromycin, Rifampicin
Drugs that lead to Cholestasis Jaundice?

Name the Conditions where Family H/o of jaundice is present?

Family H/o Jaundice
• Progressive Familial Intrahepatic
Cholestasis syndrome
( Dublin Johnson’s and Rotor’s syndrome)
• α- antitrypsin deficiency
• Wilson’s Disease ( Hepatolenticular
degenertion- copper accumulation)

Describe the structural/ architectural and the
functional units of liver.

Hepatic lobule: Str. Unit

Hepatic Acinus : Func. Unit - divided into zones that correspond to distance from the blood supply
Zone 1-Richer in O2 and nutrients
Zone 3-poorer in O2 and nutrients

• Zone I – Periportal –
• ↑ mitochondria
• Oxidative and phase 2 metabolism,
glycogen synthetase
Zone 3 - Centrilobular
• ↑ SER, cyt-P-450, NADH
• Anaerobic & phase 1 metabolism
• Most sensitive to injury from circulatory
disturbances and toxic byproducts


Isolated elevation of S.Bilirubin
Unconjugated hyperbilirubinemia• Increased Bil Production (Hemolysis)• Ineffective erythropoiesis, resorption of hematoma• Decreased hepatocellular uptake (Rifampicin)• Decreased conjugation (Gilbert & Crigler-Najjar)
Conjugated hyperbilirubinemia• Dubin Johnson Syndrome and Rotar syndrom

Hepatocellular Jaundice
Acute or subacute hepatocellular injury• VH, alcohol, drugs, ischemic hepatitis, Wilson’s
disease, acute fatty liver of pregnancy
Chronic hepatocellular disease• VH, Alc liver D, autoimmune H, Wilson’s disease• Non-alcoholic steatohepatitis, α-antitrypsin
deficiency

Hepatocellular Jaundice
Hepatic disorders with prominent cholestasis• Diffuse infiltrative disorders: granulomatous D –
myobacterial infestions, sarcoidosis, lymphoma, drugs, amyloidosis, malignancy
• Inflammation of the intrahepatic bile ductules &/or portal ducts (primary biliary cirrhosis), graft-vs host D, chlorpromazine

Hepatocellular Jaundice: Miscellaneous
• Benign recurrent intrahepatic cholestasis• Use of oestrogens and steroids• TPN, bacterial infections• Paraneoplastic, syndromes• Intrahepatic cholestasis of pregnancy• postoperative cholestasis

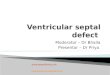
DESCRIBE THE LIVER BLOOD SUPPLY ?
and different factors affecting it?

1
2

30 % BLOOD 70 % BLOOD 40 – 50 % OXYGEN 50- 60% OXYGEN
25% of C.O.- 1500 ml/min, Dual Bld Supply

FACTORS AFFECTING LIVER BLD. SUPPLY
Increased by:
• Supine position
• Food
• Hypercapnia
• Acute hepatitis
• Drugs: barbiturates,
P450 enzyme
inducers, b agonists
Decreased by:
• Upright position
• IPPV/PEEP, Surgery
• Hypocapnia, hypoxia
• Cirrhosis
• Anaesthetics agents
volatile, inhalational,
b blockers, a
agonists
• Surgical
Manipulations

What are the Functions of Liver ?

• Protein metabolism – synthesis of plasma pr( albumin & α-acid glcoprotein, C-reactive protein, haptaglobin, pseudocholinestrase, deamination of A.A , formation of urea,
• Glucose Homeostasis - gluconeogenesis, glycogenolysis( glucagon), glycogenesis (Insulin)
• Fat Metabolism - Synthesis of lipoproteins, cholesterol, triglycerides, oxidation of FA to ketone bodies
• Reservoir of Blood• Endocrine Function: IGF1, Thrombopoitin,
Angiotensinogen, Thyroid homeostasis, steroid hormone inactivation( Testesterone, estradiol, glucocorticoid, ald.)


Functions of the Liver• Bilirubin formation & excretion
• Drug & Hormone Metabolism Phase I & II reactions
• Hematological function – haematopoiesis in fetus, heme synthesis,
• Immunological function – largest RE organ, Kupffer cells - phagocytosis of Antigen from GIT.
• Synthesis of Coagulation factors:I,II,V,VII,IX, X,XI, XII,XIII, prekallikrein,kininogen- Anticoagulants: Antithrombin III, α1antitrypsin, α2 antiplasmin,protein C & S, plasminogen, plasminogen activator inhibitor