Embed Size (px)
Citation preview
Paediatric blood transfusion
Dr. Chitra Rajeswari TDr. Lokesh Kashyap
www.anaesthesia.co.in [email protected]
Why to transfuse blood Basic physiological function is to ensure
adequate oxygenation of the tissues Physiology of oxygen transport
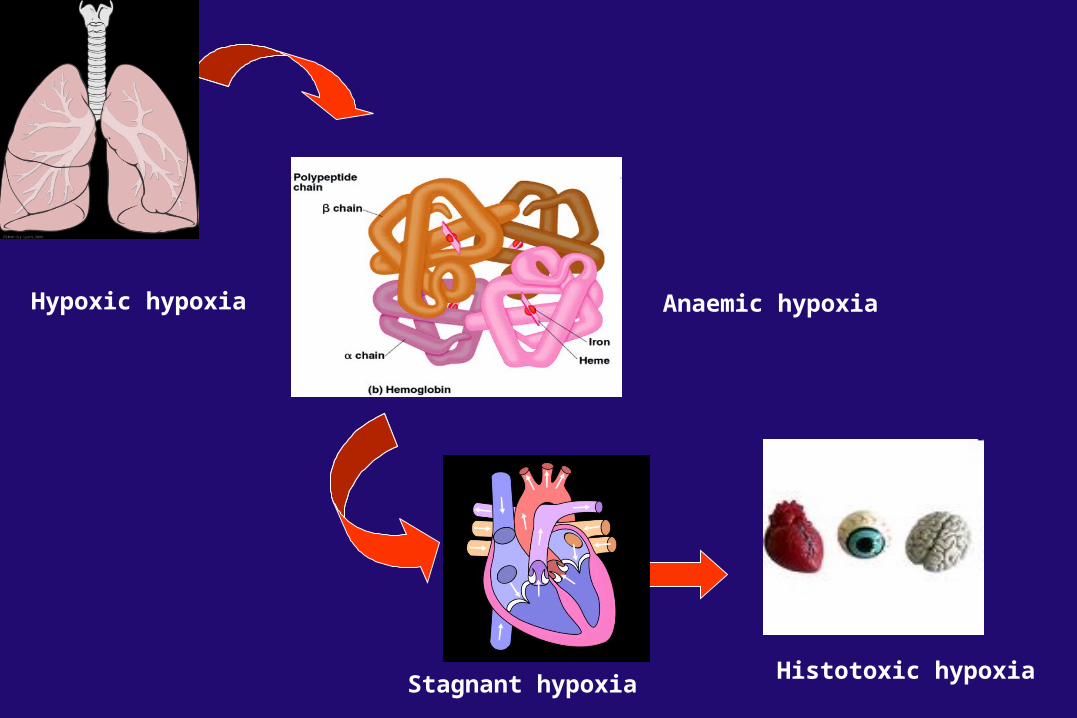
Hypoxic hypoxia Anaemic hypoxia
Histotoxic hypoxiaStagnant hypoxia
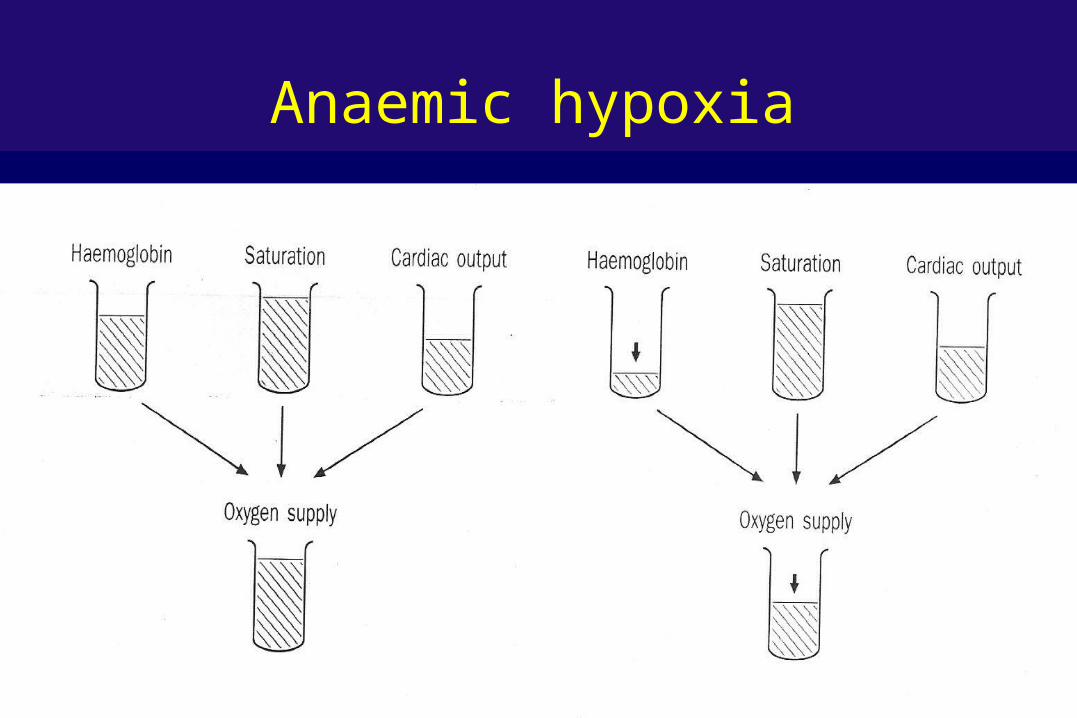
Anaemic hypoxia
Oxygen delivery DaO2
=Cardiac output X CaO2 [oxygen content]
Oxygen content[Hb saturation X 1.34 X Hb conc] + 0.003 X PO2Amount of oxygen carried by 100 ml of blood
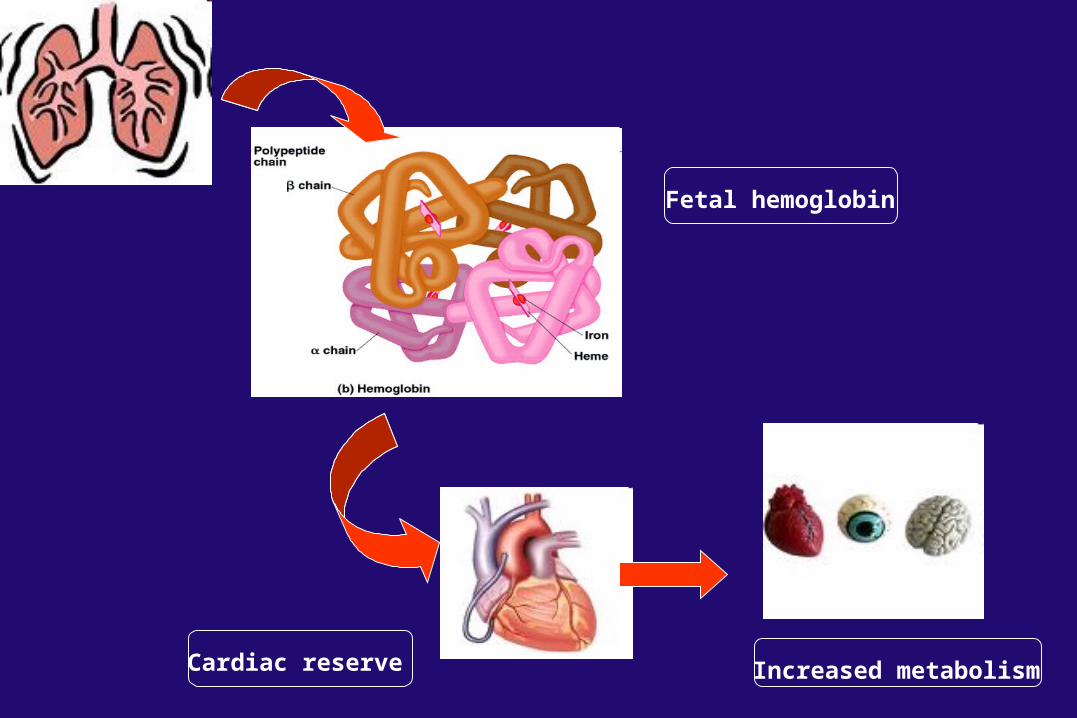
Fetal hemoglobin
Cardiac reserve Increased metabolism
Fetal hemoglobin
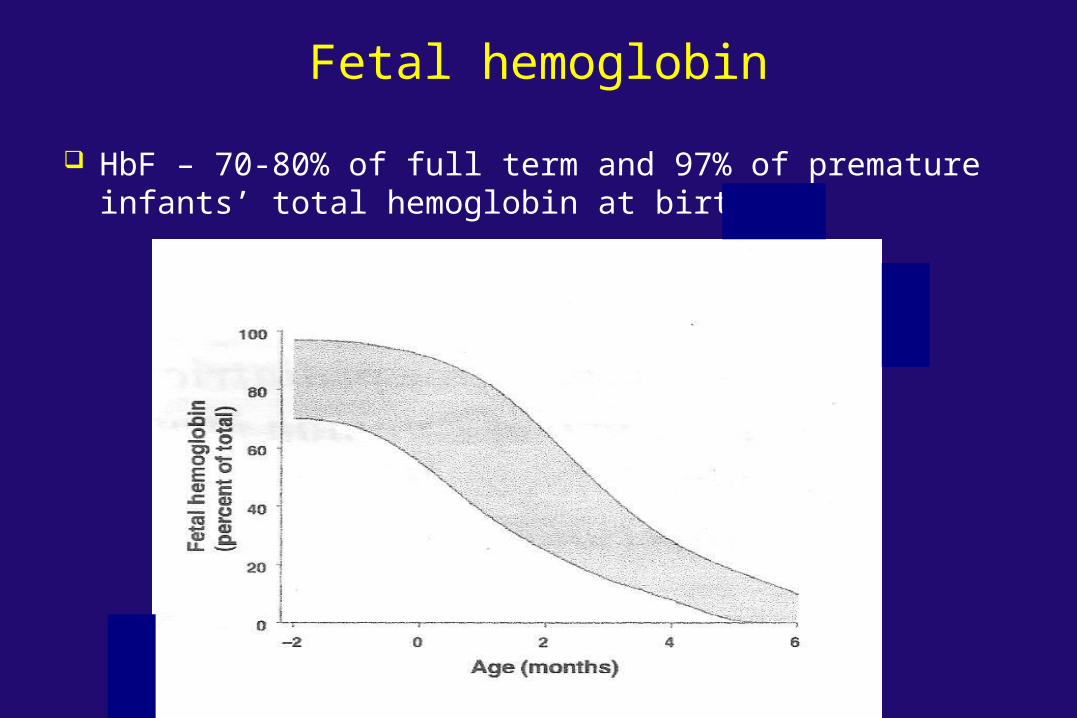
HbF – 70-80% of full term and 97% of premature infants’ total hemoglobin at birth
Fetal hemoglobin
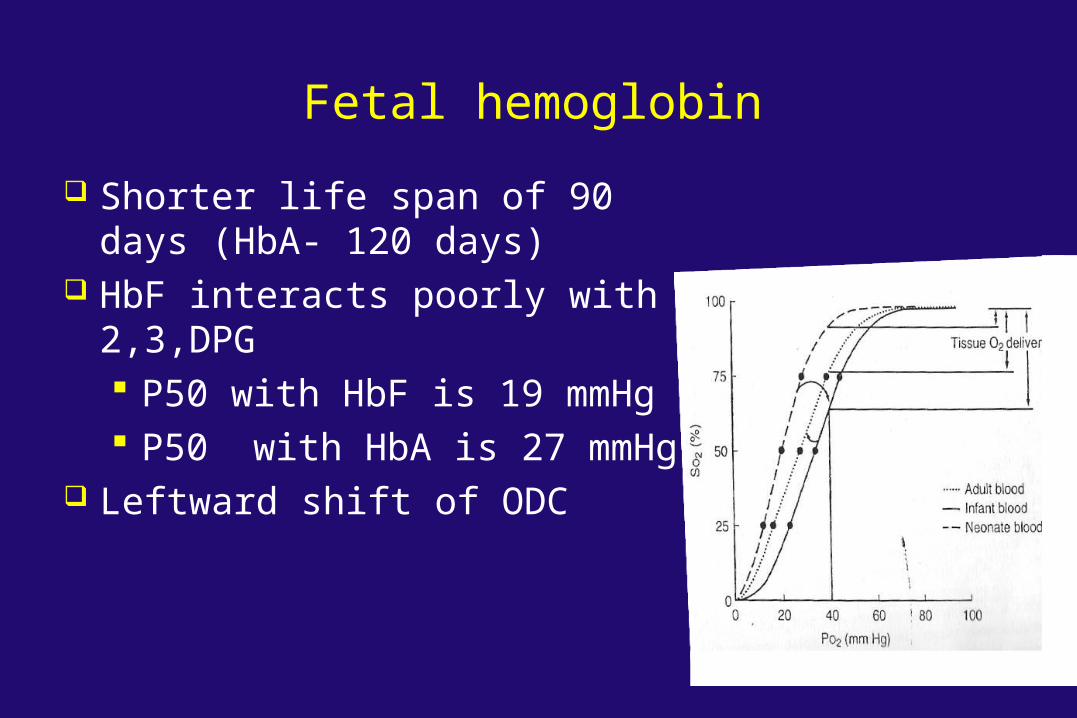
Shorter life span of 90 days (HbA- 120 days)
HbF interacts poorly with 2,3,DPG P50 with HbF is 19 mmHg P50 with HbA is 27 mmHg
Leftward shift of ODC
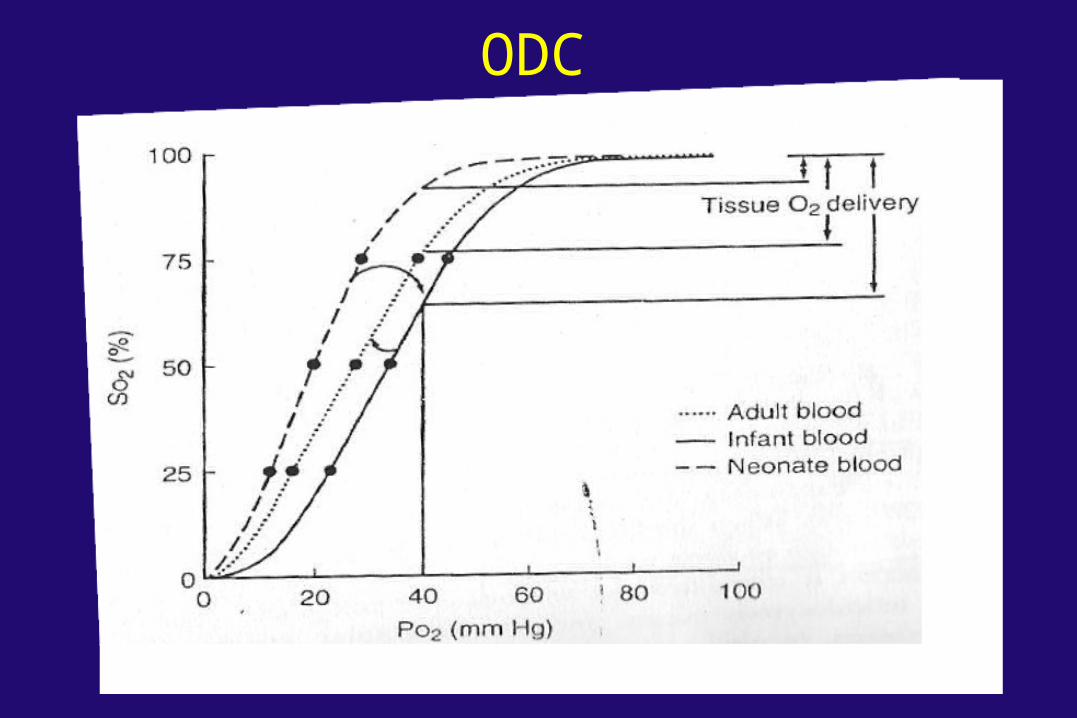
ODC
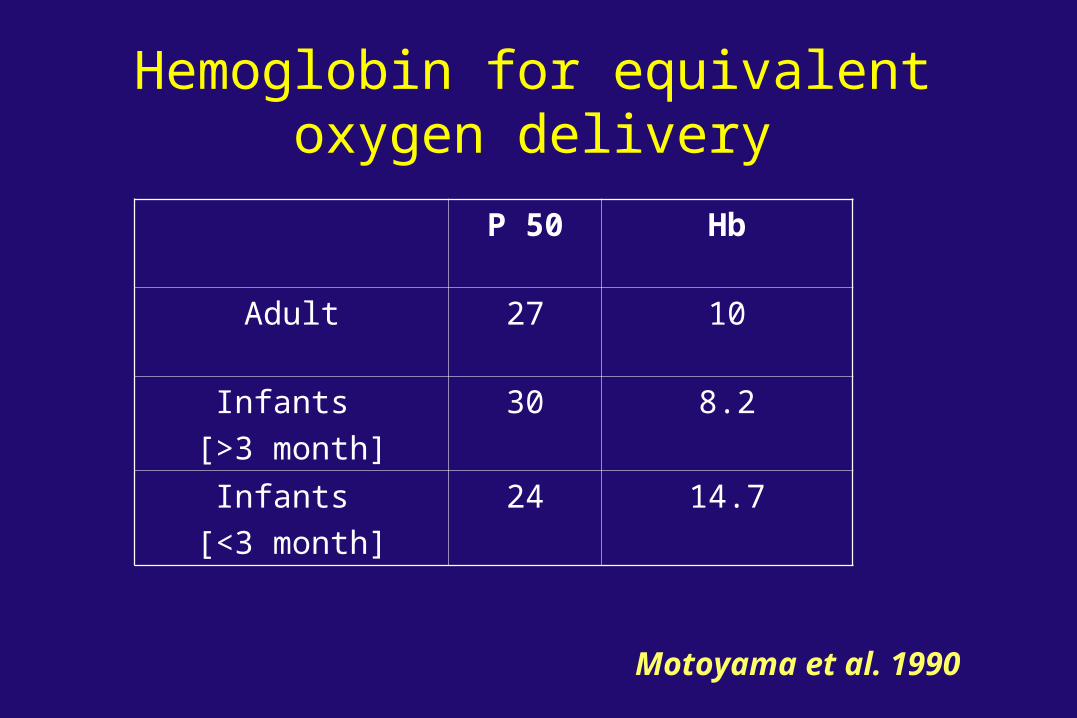
Hemoglobin for equivalent oxygen delivery
P 50 Hb
Adult 27 10
Infants [>3 month]
30 8.2
Infants [<3 month]
24 14.7
Motoyama et al. 1990
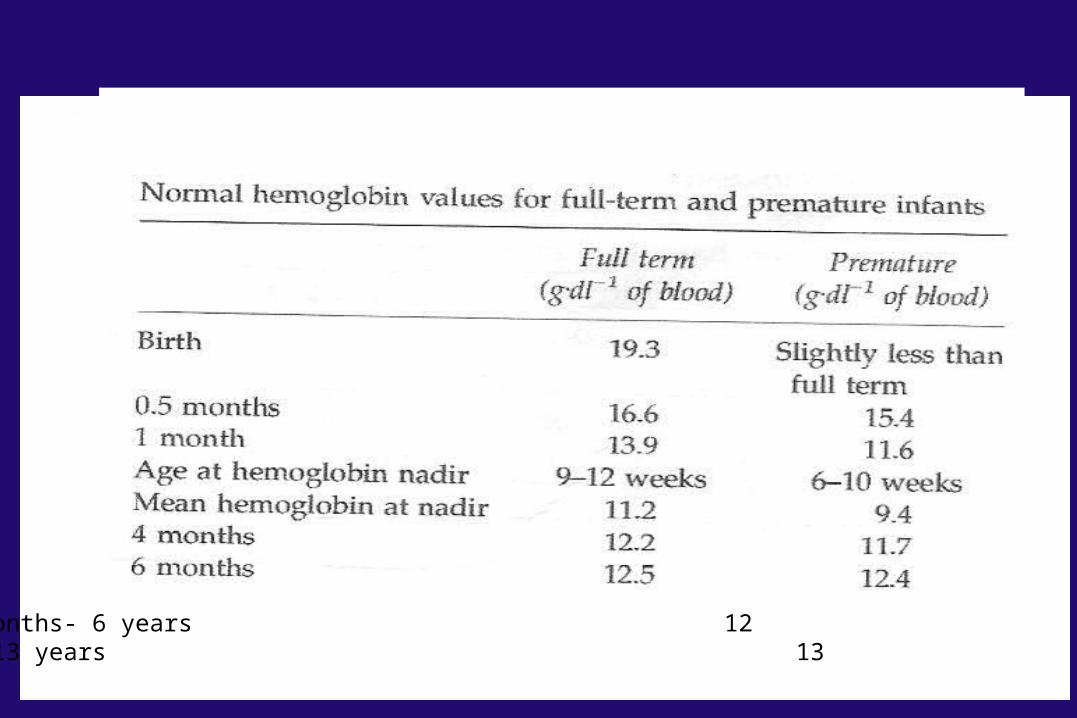
6 months- 6 years12
7-13 years 136 months- 6 years 127- 13 years 13
Preoperative hemoglobin At the time of nadir
Term infant with Hb < 9 g/dl Preterm infant <7 g/dl
Haemoglobin levels that are adequate for the older patients may be suboptimal in the younger infant
Fetal hemoglobin
Cardiac reserve Increased metabolism
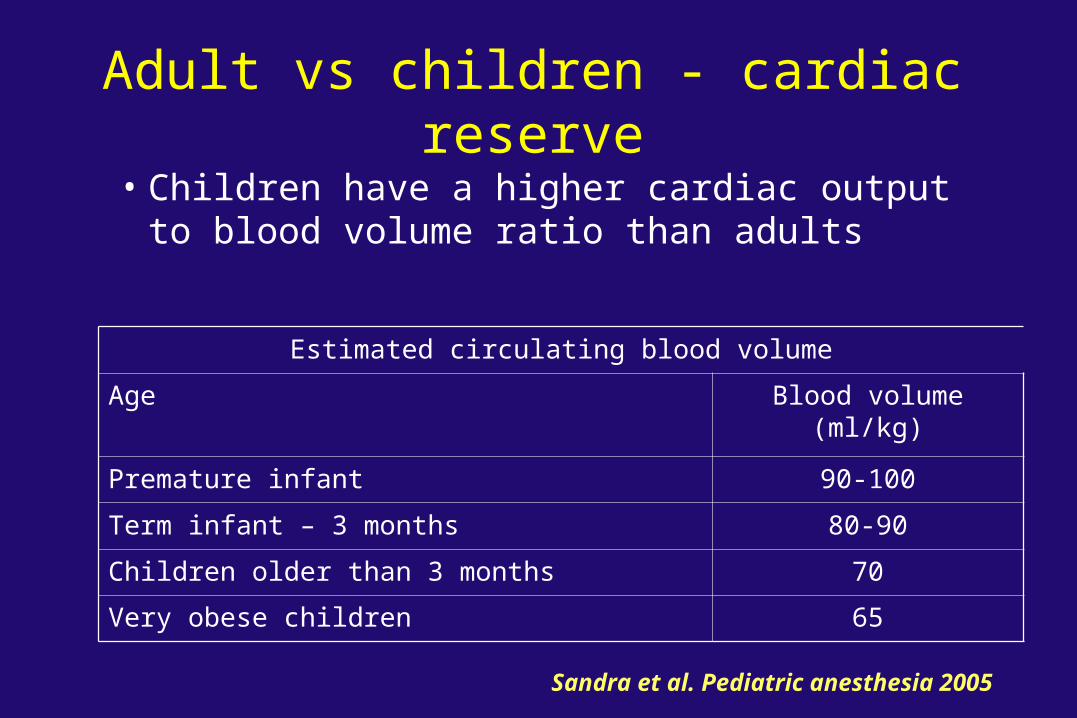
Adult vs children - cardiac reserve
• Children have a higher cardiac output to blood volume ratio than adults
Estimated circulating blood volume
Age Blood volume (ml/kg)
Premature infant 90-100
Term infant – 3 months 80-90
Children older than 3 months 70
Very obese children 65
Sandra et al. Pediatric anesthesia 2005
• The neonatal myocardium operates at near maximum level of performance as a baseline
• The newborn’s heart may be unable to compensate for a decreased oxygen carrying capacity by increasing cardiac output
• The neonatal myocardium will also suffer a greater degree of decompensation when exposed to decreased oxygen delivery
Adult vs children - cardiac reserve
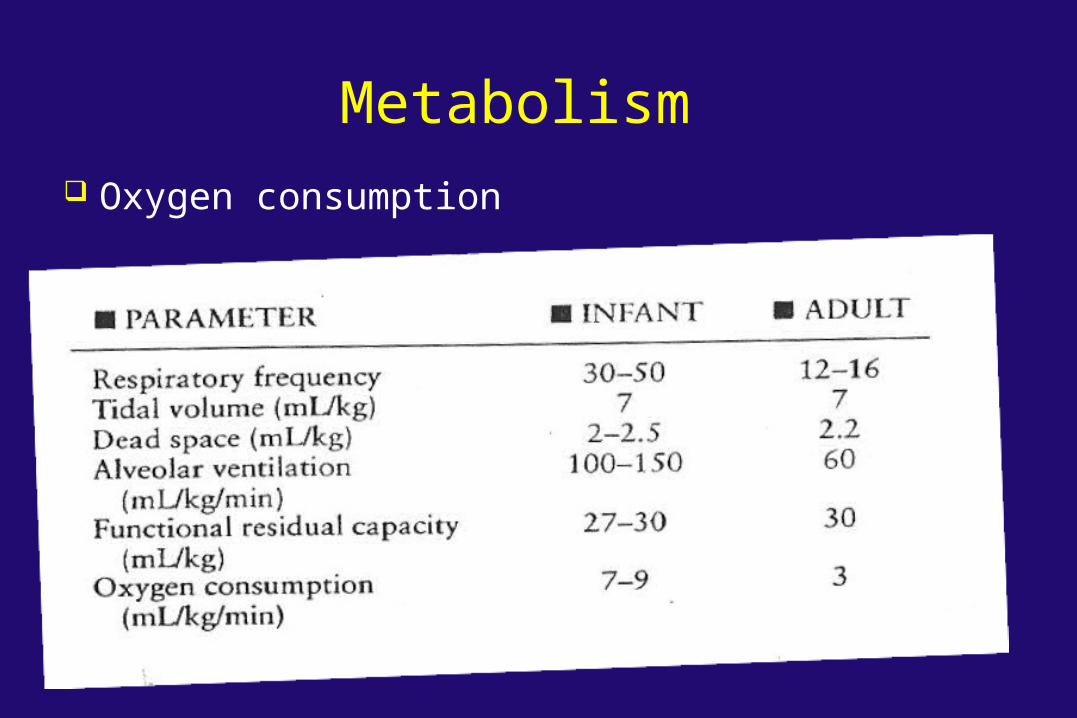
Metabolism Oxygen consumption
When to transfuse blood?
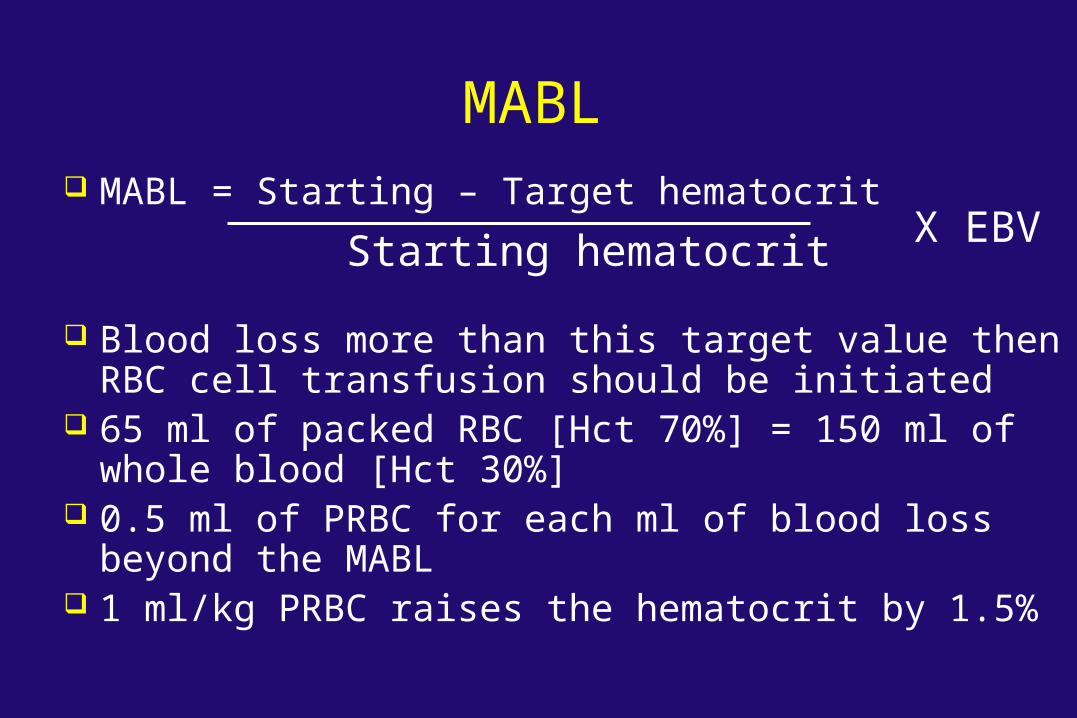
MABL MABL = Starting – Target hematocrit
Blood loss more than this target value then RBC cell transfusion should be initiated
65 ml of packed RBC [Hct 70%] = 150 ml of whole blood [Hct 30%]
0.5 ml of PRBC for each ml of blood loss beyond the MABL
1 ml/kg PRBC raises the hematocrit by 1.5%
Starting hematocritX EBV
May benefit from higher hematocrit Preterm and term infants Cyanotic congenital heart disease Large ventilation/ perfusion mismatch High metabolic demand Respiratory failure
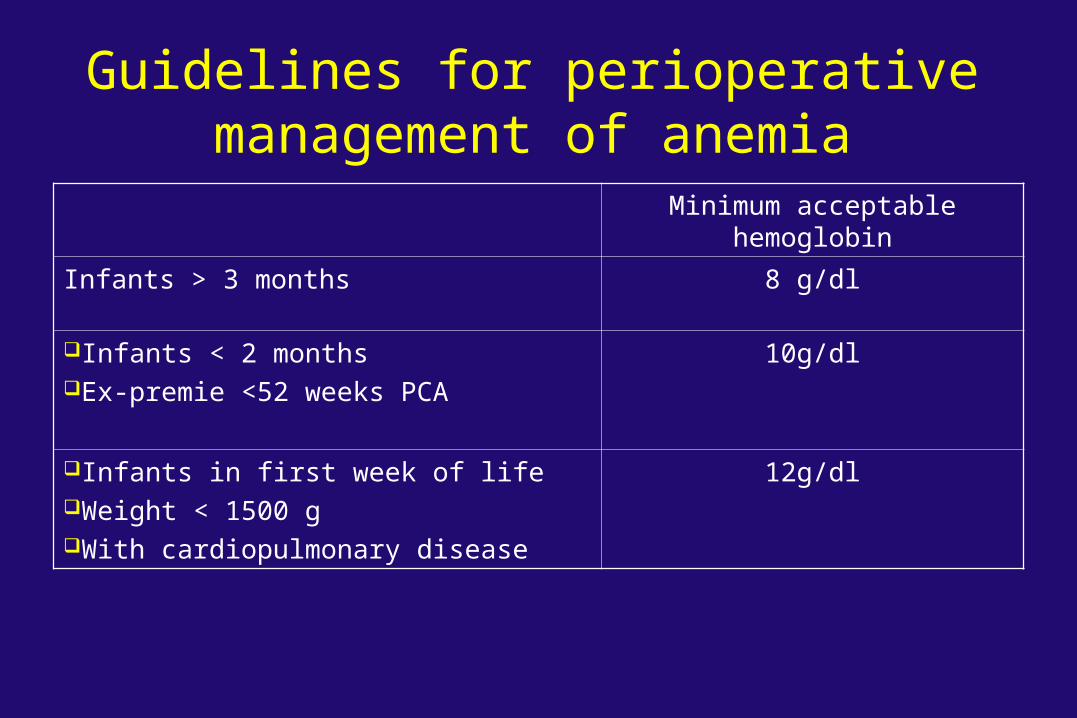
Guidelines for perioperative management of anemia
Minimum acceptable hemoglobin
Infants > 3 months 8 g/dl
Infants < 2 months Ex-premie <52 weeks PCA
10g/dl
Infants in first week of lifeWeight < 1500 gWith cardiopulmonary disease
12g/dl
Guidelines contd… In an elective setting, anemia should be
evaluated and treated,surgery may be postponed for a month or longer
Cumulative record of blood loss should be kept for critically ill infants and loss replaced when it exceeds 10% of blood volume
In an emergency setting, anesthesia administered with extreme caution Maintain high PaO2 Adequate cardiac output Adequate intravascular volume Avoid factors increasing oxygen consumption Avoid leftward shift of ODC
Guidelines contd…
Oxygen extraction ratioas hematocrit drops to 15%, OER increases
from 38 to 60% Central venous Po2
- Decline of pVo2 is the most sensitive indicator of anemia
- Normal => 38 mm Hg
Holland et al. 1987
Guidelines contd…
Pediatric transfusions – guidelines
Platelet transfusions platelet count less than 50000 in acute bleeding Less than 1 lakh for intracranial and Subarachnoid or
extra corporeal circulation procedures 5 mL/kg - 10 mL/kg causes a rise of platelets of 50 to
100 * 109/L Fresh frozen plasma
aPTT or PT > 1.5 times normal 10-15 ml/kg
Cryoprecipitate Fibrinogen 100 mg/dl 1 unit /10 kg BW raises plasma fibrinogen by 50 mg/dl
Acute transfusion reactions ( < 24 hours) Febrile nonhemolytic reaction Urticarial/allergic reaction Acute hemolytic reaction Bacterial contamination and sepsis Fluid overload Anaphylaxis TRALI
Delayed transfusion reaction Infection Delayed hemolytic reaction Post transfusion purpura Graft Vs host disease Iron overload
Transfusion reactions
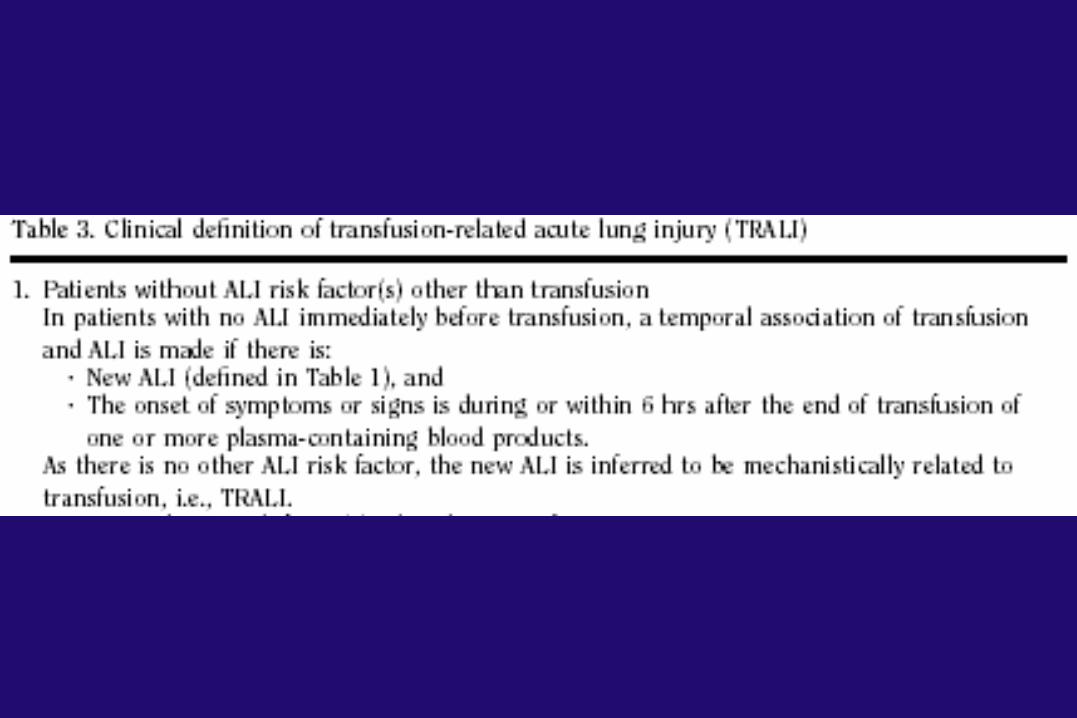
TRALI TRALI
Acute hypoxemia Non-cardiogenic pulmonary edema During or after transfusion
Leading cause of transfusion-related mortality in 2003 – FDA, TRALI conference
Underdiagnosis & underreporting
Incidence All plasma-containing blood & blood
components 1/5,000 blood & blood component 1/2,000 plasma-containing component 1/7,900 units of FFP 1/432 units of whole blood derived platelets
Pathophysiology
Leukocyte antibodies Biologically active substance
Lipids & cytokinesNeutrophil priming activity
Leukocyte Antibodies Neutrophil in pulmonary capillary → pulmonary damage
& capillary leak Antibody to donor leukocyte Ab to HLA I, II, granulocyte, monocyte, IgA
Management Supportive Stop transfusion if timely recognition Oxygen and ventilatory support as employed in
ARDS Avoid blood from multiparous female donors
Immunologic Transfusion related graft vs host disease Lymphocytes in transfused blood component proliferate
and cause host tissue destruction Immunocompromised patient Premature infants Children with cancer or severe systemic illness Acute blood loss Cardiopulmonary bypass
Prevented by irradiated blood
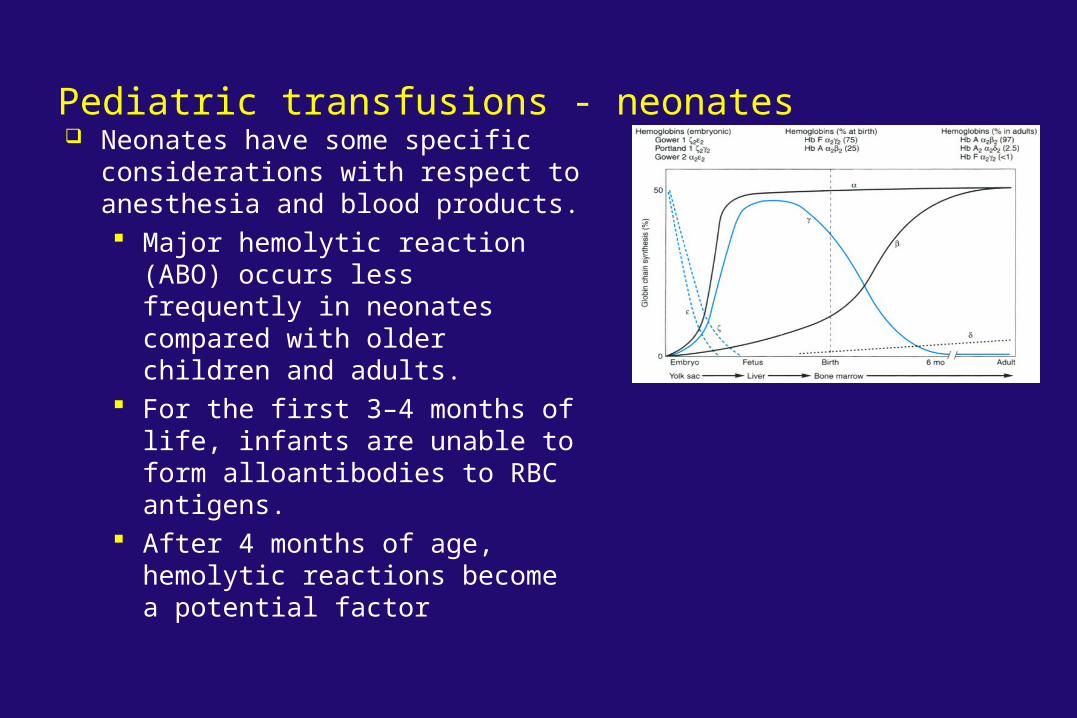
Pediatric transfusions - neonates Neonates have some specific
considerations with respect to anesthesia and blood products. Major hemolytic reaction (ABO)
occurs less frequently in neonates compared with older children and adults.
For the first 3–4 months of life, infants are unable to form alloantibodies to RBC antigens.
After 4 months of age, hemolytic reactions become a potential factor
Massive blood transfusion
Definition Loss of one or more circulating blood volume in
24 hour 50% blood volume in 3 hours Loss occurring at the rate of 2-3 ml/kg/min
Problems of massive transfusion Hypocalcemia Hyperkalemia Hypomagnesemia Hypothermia Volume overload Dilutional coagulopathy Acid base changes Shift of ODC curve Microaggregate delivery TRALI
Hypocalcemia Degree of ionized hypocalcemia depends upon
Blood product transfused Rate Hepatic blood flow Hepatic function
Hypocalcemia
Degree of ionized hypocalcemia depends upon Blood product transfused Rate Hepatic blood flow Hepatic function
FFP
Decreased ability to metabolise by neonate
> 1 ml / kg / min
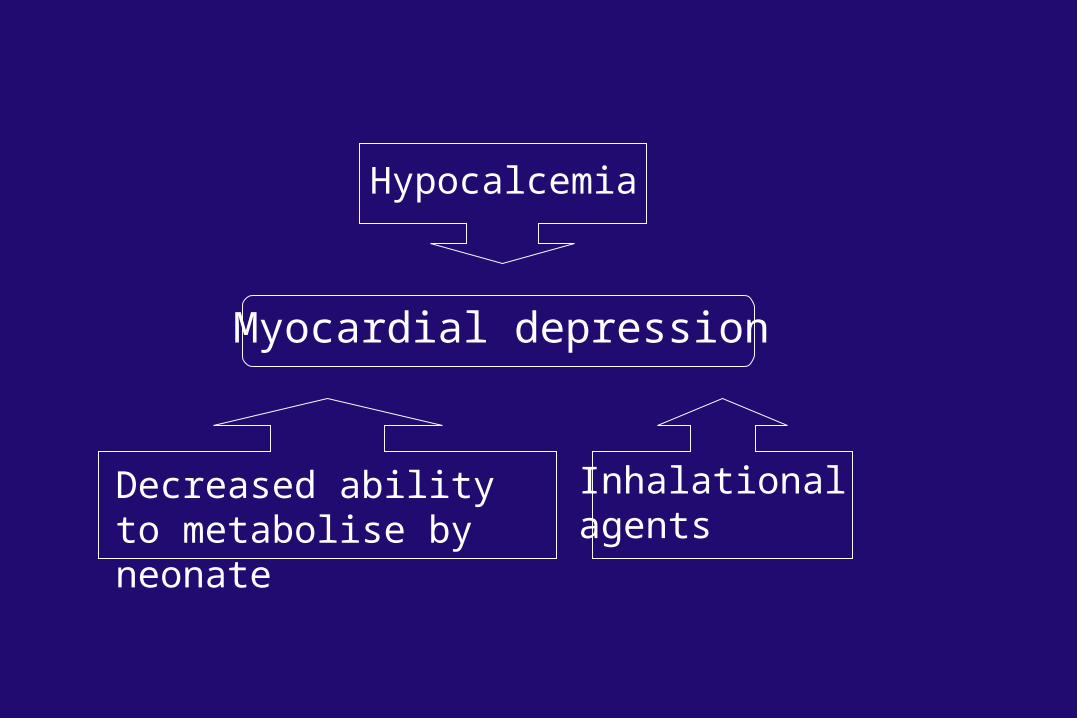
Myocardial depression
Hypocalcemia
Decreased ability to metabolise by neonate
Inhalational agents
Prevention of hypocalcemia Rate should be < 1 ml / kg / min If more than > 1 ml / kg / min calcium should
also be transfused Calcium infusion
Calcium chloride 5-10 mg/kg Calcium gluconate 15-30 mg/kg
Frequent measurement of ionised calcium
Hyperkalemia Blood components with high potassium
Whole blood Irradiated blood Near the expiry date
Prevention of hyperkalemia Washing of erythrocytes Newer blood (< 7 days) Avoiding whole blood and prefer packed RBC
Treatment CaCl2 15-20 mg/kg Calcium gluconate 45-60 mg/kg 1-2 min intervals until the arrhythmia is resolved Glucose and insulin Hyperventilation Albuterol kayexalate
Hypomagnesemia Result of citrate toxicity Stabilizes the resting membrane potential Life threatening arrhythmia that dose not
respond to exogenous calcium therapy needs magnesium sulphate
25-50 mg/kg followed by 30-60 mg/kg/24 hours
Acid-base changes RBC metabloism can elevate the dissolved CO2
to 180-210 mmHg Anaerobic metabolism increases the lactic acid
content Initial transient combined respiratory and
metabolic acidosis Citrate metabolism leads to metabolic alkalosis
Hypothermia Shift to left of ODC curve – decreased oxygen
delivery Apnea Hypoglycemia Decreased drug metabolism Increased oxygen consumption Coagulopathy

Coagulopathy Massive blood transfusion leads to
thrombocytopenia 40%, 20% and 10% of starting platelet count is
seen after 1st, 2nd and 3rd blood volume loss Dilution and loss of clotting factors Clotting factor deficiency should be anticipated
after one blood volume loss
Recombinant factor VIIa Retrospective review of use of factor 7a in
children undergoing major neurosurgical procedures experiencing massive uncontrollable hemorrhage
Useful adjunct to control life threatening bleeding,but more extensive research is needed
Uhring et al Ped crit care med, 2007
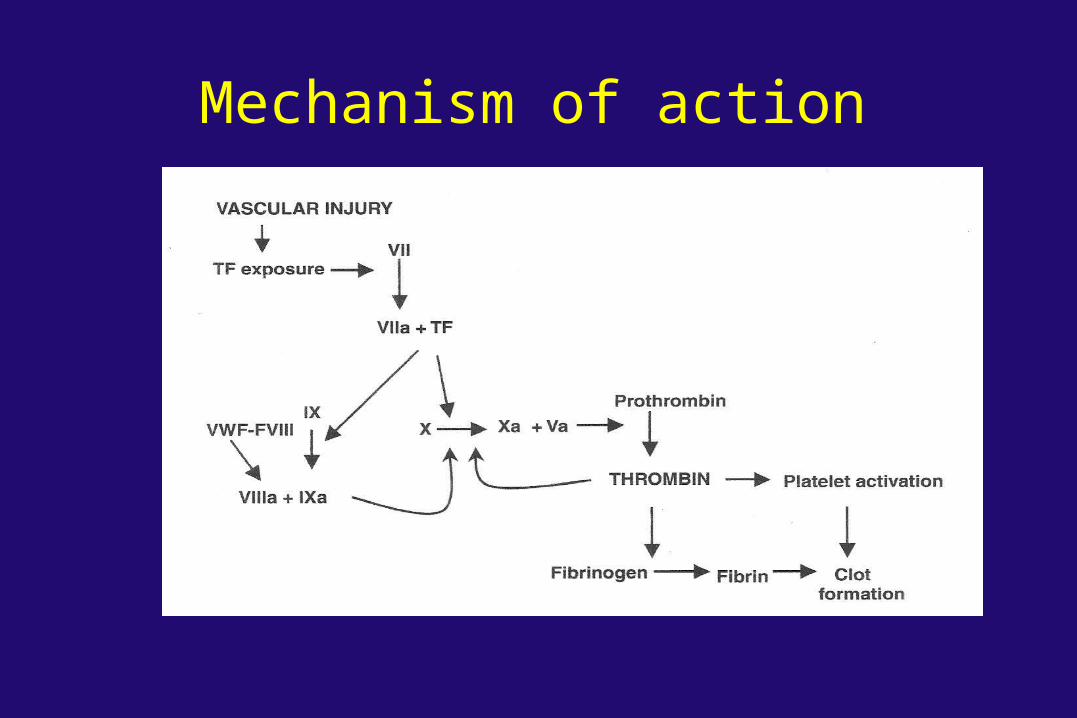
Mechanism of action
Blood Conservation Preoperative Autologous Donation Acute Normovolemic Hemodilution Intraoperative Blood Salvage Preoperative Erythropoietin Positioning Hypotensive anaesthesia Pharmacological enhancement of hemostasis Artificial blood
www.anaesthesia.co.in [email protected]