Embed Size (px)
Citation preview

ACYANOTIC HEART DISEASE
PRESENTER :- BIKASH RAY
MODERATOR :- DR.VIMI REWARI
www.anaesthesia.co.in

Shubu
7 yr, male
D.O.A – 2.3. 2008
Res. - Karnal, Haryana
History by - mother

C/O
Swelling noted by the parents in Lt groin since last 1 yr

H/o present illness
Swelling in lt groin ,observed by parents -1yr
not associated with pain ,or tenderness
H/o recurrent respiratory infection since 1st yr of life, last episode x 4 months –
cough Respiratory distress. Rapid respiration. Rise in temperature (mild). Duration of symptom – few days to a week. Relieved by medication. No h/o bluish discoloration during crying.

No h/o Swelling of body & face. ↓ urine output. Yellowish discolouration. Abd. distension.
No h/o decreased /absent movement of extremities.

H/o past illness
Patient had h/o recurrent RTI in past
frequency gradually decreasing
No history of any other significant medical or surgical illness
No h/o failure to thrive

Family history not significant
Birth & developmental history Antenatal – no maternal illness no drug/alcohol intake
Natal – Full Term, vaginal delivery neonatal period uneventful
Development – normal motor and personal social development

Immunization history
Adequately immunised for age
Feeding & dietary history
Vegetarian
Normal solid and liquid intake
Treatment history
Patient not taking any medication

General examination Wt = 20 kg Ht = 96 cm A febrile Conscious, active, cooperative
No pallor ,cyanosis,jaundice,edema, clubbing
No lymphadenopathy
Neck veins- not engorged

Pulse – 98/min, regular ,good volume, no
radio-radial or radio-femoral delay
All peripheral pulse palpable
BP = 100/58 mmHg
( lt arm, supine position )
Peripheral venous access = adequate

Systemic examination
Cardiovascular system :-
Inspection –
Precordium normal on inspection
No visible apical impulse
No visible pulsation
No scar mark visible

Cont. Palpation :-
Apex Palpable at (L) 5th ICS, at mid-clavicular line No thrill palpable Parasternal heave not palpable
Auscultation :- S1 & S2 audible
Pan-systolic murmur at apex & LLSB

Cont.Respiratory system : - No chest wall deformity on inspection
Respiratory rate 20/min, regular, accessory muscles not working
Auscultation:B/L air entry equalNo added sounds

Cont.Central nervous system Higher functions – normal Cranial nerves, cerebellum, motor and sensory
examination – within normal limits
Abdomen :- no distension or venous engorgement swelling in Lt groin, soft, non-tender,
cough impulse positive no organomegaly

Cont.Airway assessment Mouth opening > 4 cm Neck movement adequate MMP class I No facial deformity noted Teeth –intact
Spine examination No abnormality detected

Provisional diagnosis
Acyanotic congenital heart disease with
L-R shunt, probably ventricular septal defect, not in failure, with Lt inguinal hernia

Differential diagnosis
ASD – age (older)
PAH ( absent)
murmur (ejection systolic)
PDA – murmur (cont. machinary)

Investigations Hb – 10.3
Tlc- 7300
Plt – 3.56
Bu -24
Na / k = 133 / 4.3
CXR-
normal heart size ECG –
WNL ECHO –
- small 3 mm VSD
- L-R shunt
- no ASD,PDA,COA
- normal ventricular
function

Diagnosis
Small asymptomatic VSD for herniotomy (Lt ) not in failure

PAC orders
Adequate NPO
Inform written consent of parents
Ampicilin 50 mg / kg ,iv ,30 minutes
before surgery

Anesthetic plan General anesthesia with neuraxial block Induction :-
pre o2 -- propofol + fentanyl
laryngeal mask airway Maintenance :
O2+ N2O+ ISOFLURANE
Controlled ventilation Post induction :- Lt lateral position
caudal epidural with PAP

INTRA-OPERATIVE CONCERNS
Air embolism
Shunt reversal
Pulmonary hypertension
Volume overload - LVF

BUBBLE AVOIDANCE
Remove all bubbles from IV tubing. Connect IV tubing to venous cannula while there is
free flow of IVF and blood. Eject small amount of solution from syringe to clear air
from hub to needle before injection. Aspirate injection port of 3-way before injection
Hold syringe upright - bubbles at plunger end.
Do not inject last ml from the syringe.
Do not leave central line open to air.

To prevent worsening of shunt SVR to be kept below normal PVR to be kept normal or above
- Minimal FiO2
- Adequate tidal volume
- Low RR, PEEP
- PaCO2 40-50 mmHg
- Temperature
- Epidural

FACTORS AFFECTING PVR ↑ PVR
Sympathetic stimulation– pain , light anesthesia
↓pH, ↑PaCO2 , ↓ PaO2
Hypothermia
↑ intrathoracic pressure--
Controlled vent, PEEP ,atelectasis
↓PVR
Anesthesia
↑ pH , ↓PaCO2, ↑ PaO2
↓intrathoracic
pressure--- SV, normal lung volumes
Drugs PDE inhibitors Isoproterenol PGE1,PGI2,NO

Indications of IE prophylaxis

Post-op
Sedation
Analgesia
Decongestive treatment
Pulmonary vasodilators
monitoring


Prevalence
CongenitalIncidence of CHD :8 / 1000 live birth
Cyanotic: 22%
Acyanotic: 68% VSD 25% ASD 6% PDA 6% PS 5% AS 5%

VSD

VSD Most common CHD 2.6 to 5.7 /1000 live birth 10 % of adult CHD TYPES :-
1. Subpulmonary (5-7 % )- with AV insufficiency
2. Perimembranous (80 %)-with tricuspid valve abnormality
3. A-V canal (5-8%)
4. Muscular (5 -20 % )- multiple defect
Restrictive , non- restrictive Small, medium, large (in relation to aortic root )

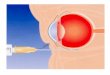
ANATOMY


Severity of VSD :–
- loud P2, parasternal lift/heave
- duration of murmur
- diastolic murmur at mitral area
- features of CCF

Syndrome associated with VSD
Extra cardiac malformation in 20-45 %
- Trisomy 21,18,13
- CHARGE syndrome
- Fetal hydantion syndrome
- Fetal alcohol syndrome
- Fetal valproate syndrome
- Apert syndrome

Features of VSD based on size
Shunt Gradient ↑ PVR RVP RVH LVH Murmur
Small L – R High -- N No Yes PSM
Medium L-R 20mm Hg ± Mild ↑ Mild Yes PSM
Large L-RR-L
None + ↑ Yes Yes Decreased
Large with PVR
R-L None + Yes No None

Severity of VSD :–
- loud P2, parasternal lift/heave
- duration of murmur
- diastolic murmur at mitral area
- features of CCF

NATURAL HISTORY Spontaneous closure of defects less than 5mm
before 5 yrs of age (40-50%). Natural course depends on – size, change in PVR,
age Large defects – CHF in infancy (2-6 wks), when
PVR falls Tachypnea, Distress, Sweating while feeding,
Failure to thrive CHF- apathetic, no movement, weak cry,
diaphoretic, hepatomegaly Indications for surgical closure- >6.5 mm, Qp:Qs
ratio >2

Severity of VSD :–
- loud P2, parasternal lift/heave
- duration of murmur
- diastolic murmur at mitral area
- features of CCF

LARGE L- R SHUNT
↑ PVR
↑ LA SIZE↑LA PRESSURE
INTERSTITIAL AND ALVEOLAR EDEMA
↑ PA FLOW↑PA PRESSURE
ENLARGEMENT OF VESSELS
BRONCHIAL HYPERTROPHY
AIRWAY OBSTRUCTION
↑ AIRWAY RESISTANCE↓ PULMONARY COMPLIANCE
INCREASED WORK OF BREATHINGGAS TRAPPING, ATELECTASIS, INFECTION

Severity of VSD :–
- loud P2, parasternal lift/heave
- duration of murmur
- diastolic murmur at mitral area
- features of CCF

Cardiac Grid
Preload
HR Contractility
PVR SVR
VSD (L→R) unrepaire
d
↑ N N ↑ ↓
VSD (L→R) repaired
↑ N N N N
VSD (R→L) ↑ N N ↓ ↑

Severity of VSD :–
- loud P2, parasternal lift/heave
- duration of murmur
- diastolic murmur at mitral area
- features of CCF

VSD IN PREGNANCY

Sobha
23 yr , female, primigravida
D.o.A - 25.2.08
Haryna

Presented with
36 week of pregnancy with h/o cardiac
disease for elective LSCS

Past history h/o "heart disease " diagnosed at birth but not on
any follow- up
H/o recurrent LRTI during childhood
h/0 progressive exertional dyspnea since the first trimester of her pregnancy.
Evaluated in 2nd trimester for dyspnea- diagnosed as a case of VSD
No h/O any other significant medical or surgical illness

Treatment history
Patient not on any medication
General examination
wt = 68 kg ,ht = 154 cm
Afebrile
Consious, oriented
No pallor ,cyanosis,jaundice,edema, clubbing
No lymphadenopathy
Neck veins- not engorged

Pulse – 9o/min, regular ,good volume, no radio-radial or radio-femoral delay
All peripheral pulse palpable
BP = 130/88 mmHg ( lt arm, supine position )
Peripheral venous access = adequate

Systemic examination Cardiovascular system :- Inspection –
Precordium normal on inspection
No visible apical impulse
No visible pulsation
No scar mark visible Palpation :-
Apex Palpable at (L) 5th ICS, at mid-clavicular line No thrill palpable Parasternal heave not palpable
Auscultation
:- S1 & S2 audible
Pan-systolic murmur at apex & LLSB

Respiratory system : - RR = 14/min Auscultation:
B/L air entry equalNo added sounds
Central nervous system Higher functions – normal Cranial nerves, motor and sensory examination –
within normal limits
Abdomen :- WNL for 34 week pregnancy

Investigations
Hb :- 14.4 g/dl Plt - 1.54 lakh Tlc – 6400 Bu -28 Sr. creatinine – 1 Na / K = 148/ 4.5 T. bil = 0.7 CXR – ECG – LVH ECHO - small VSD (5mm )

Anesthetic concern
1. Avoid accidental iv infusion of air bubble
2. Use loss of resistance to saline that air to identify epidural space
3. Early administration of epidural anesthesia is desirable.
4. Slow onset of epidural anesthesia is preferred
5. Patient should receive supplemental o2 & oxygen saturation should be monitored

EISENMENGER SYNDROME
Pathophysiology of the Eisenmenger syndrome.


Natural History: Course and Prognosis
8% of patients with CHD & 11% of those with L-R intracardiac shunting develop the Eisenmenger
syndrome [CHD that may result in the Eisenmenger syndrome include VSD,AV defect, PDA, ASD, D-TGA, and surgically created aortopulmonary connections
VSD :- 3% of patients who have a small or moderate-sized defect ( 1.5 cm) and about 50% who have a large defect (>1.5 cm ) develop the Eisenmenger
80% survival rate at 10 yr, 77% at 15 yr, and 42% at 25 yr

Wood's Units unit of measure for PVR. One Wood's Unit = PVR of an average healthy person. That is:MPAP = 13 mmHgLAP = 8 mmHgCO = 5 liters per minuteso average healthy PVR = (13 minus 8) divided by 5, which equals one Wood's Unit