-
8/17/2019 mc_m6_Cancer+ovario+precoz
1/9
Prognostic Factors for High-Risk Early-Stage
Epithelial Ovarian CancerA Gynecologic Oncology Group
Study
John K. Chan, MD1
Chunqiao Tian, MS2
Bradley J. Monk, MD3
Thomas Herzog, MD4
Daniel S. Kapp, MD, PhD5
Jeffrey Bell, MD6
Robert C. Young, MD7
1Department of Obstetrics, Gynecology, and
Reproductive Sciences, University of California,
San Francisco School of Medicine, UCSF Helen
Diller Family Comprehensive Cancer Center, San
Francisco, California.
2GOG Statistical & Data Center, Roswell Park
Cancer Institute, Buffalo, New York.
3Department of Obstetrics and Gynecology, Chao
Family Comprehensive Cancer Center, University
of California, Irvine – Medical Center, Orange,
California.
4Department of Obstetrics and Gynecology, Co-
lumbia University, New York, New York.
5Department of Radiation Oncology, Stanford
University School of Medicine, Stanford Cancer
Center, Stanford, California.
BACKGROUND. The purpose was to identify the factors
predictive of recurrence
and survival in patients with high-risk (stage I, grade 3; stage
IC, stage II, or clear
cell) epithelial ovarian cancer after adjuvant therapy.
METHODS. Data was extracted from patients who underwent
primary surgery fol-
lowed by adjuvant therapy in 2 randomized trials by the
Gynecologic Oncology
Group (Protocols 95 and 157). Kaplan-Meier survival estimates
and Cox propor-
tional hazards model adjusted for covariates were used for
analyses.
RESULTS. Of 506 patients (median age 5 56.2 years),
347 (68.6%) had stage I and
159 (31.4%) had stage II cancers. The 5-year recurrence-free
(RFS) and overall sur-
vivals (OS) were 75.5% and 81.7%, respectively. On multivariate
analysis, older age,
higher stage, higher grade, and malignant cytology were
independent prognostic
factors predictive for recurrence and poorer survival. The risk
of recurrence was
higher for those 60 versus < 60 years (hazards
ratio [HR] 5 1.57, 95% confidence
interval [CI], 1.12–2.19), stage II (stage II: HR 5 2.70, 95%
CI, 1.41–5.16) versus
stage IA or IB, grade 2 (HR 5 1.84, 95% CI, 1.04–3.27) and
grade 3 (HR 5 2.47, 95%
CI, 1.39–4.37) versus grade 1, and positive versus negative
cytology (HR 5 1.72,
95% CI, 1.21–2.45). By using these factors in a prognostic
index, those with low-
risk (no or 1 risk factor), intermediate-risk (2 factors), and
high-risk (3–4 risk fac-
tors) disease had survivals of 88%, 82%, and 75%, respectively
(P < .05).
CONCLUSIONS. Age, stage, grade, and cytology are
important prognostic factors in high-risk early-stage epithelial
ovarian cancer. This information may be used in the design
of future clinical
trials.Cancer 2008;112:2202–10. 2008 American
Cancer Society.
KEYWORDS: ovarian cancer, early-stage, prognosis, survival.
6Department of Obstetrics and Gynecology, Ohio
State University, Riverside Methodist Hospital,
Columbus, Ohio.
7Department of Medical Oncology, Fox Chase
Cancer Center, Philadelphia, Pennsylvania.
This study was supported by National Cancer
Institute grants to the Gynecologic Oncology
Group Administrative Office (CA27469), the
Gynecologic Oncology Group Statistical and Data
Center (CA37517), and Gynecologic OncologyGroup new investigator
award to JKC.
The following Gynecologic Oncology Group
member institutions participated in this study:
University of Alabama at Birmingham, Oregon
Health Sciences University, Duke University
Medical Center, Abington Memorial Hospital,
University of Rochester Medical Center, Walter
Reed Army Medical Center, Wayne State
University, University of Minnesota Medical
School, University of Southern California at Los
Angeles, University of Mississippi Medical Center,
Colorado Gynecologic Oncology Group P.C.,
University of California at Los Angeles, University
of Pennsylvania Cancer Center, University of
Miami School of Medicine, Milton S. Hershey
Medical Center, Georgetown University Hospital,
University of Cincinnati, University of North
Carolina School of Medicine, University of Iowa
Hospitals and Clinics, University of Texas
Southwestern Medical Center at Dallas, Indiana
University School of Medicine, Wake Forest
University School of Medicine, Albany Medical
College, University of California Medical Center at
Irvine, Tufts-New England Medical Center, Rush-
Presbyterian-St. Luke’s Medical Center, SUNY
Downstate Medical Center, University of
Kentucky, Eastern Virginia Medical School, The
Cleveland Clinic Foundation, Johns Hopkins
Oncology Center, State University of New York at
Stony Brook, Eastern Pennsylvania GYN/ONC
Center, P.C., Southwestern Oncology Group,
Washington University School of Medicine,
Cooper Hospital/University Medical Center,
Columbus Cancer Council, North Central
Cancer Treatment Group, University of Massa-
chusetts Medical School, Fox Chase Cancer
Center, Medical University of South Carolina,
Women’s Cancer Center, University of Oklahoma,
University of Chicago, and Tacoma General
Hospital.
Address for reprints: John K. Chan, MD, Department
of Obstetrics, Gynecology, and Reproductive Sciences,
University of California, San Francisco School of
Medicine, UCSF Helen Diller Family Comprehensive
Cancer Center, 1600 Divisadero St., Box 1702, San
Francisco, CA 94143-1702; Fax: 415-885-3586;
E-mail: chanjohn@ obgyn.ucsf.edu
Received September 25, 2007; revision received
November 9, 2007; accepted November 19, 2007.
ª 2008 American Cancer SocietyDOI 10.1002/cncr.23390Published
online 17 March 2008 in Wiley InterScience
(www.interscience.wiley.com).
2202
-
8/17/2019 mc_m6_Cancer+ovario+precoz
2/9
I n 2006 there will be an estimated 20,180 new epithelial
ovarian cancers diagnosed in the US, with approximately
one-third having FIGO (Interna-
tional Federation of Obstetrics and Gynecology) stage
I and II disease.1 Although the survival of
early-stage
disease is significantly higher than those with ad-vanced
cancers, approximately 20% to 30% of these
patients will die of their disease.2–7
The clinical and pathologic prognostic factors
that have been previously described for patients with
early-stage epithelial ovarian cancers include: age,
stage, tumor rupture, cell type, tumor grade, large
volume ascites, and dense adhesions.8–16 The limita-
tions of many of these prior studies include the small
sample size, inadequacy of surgical staging, inclusion
of borderline tumors, stage III cancers with minimal
residual disease, lack of central pathology review,
and variation in adjuvant therapies.
Young et al.10
suggested that women with low-risk cancers, defined as stage IA,
IB, grade 1 or 2,
nonclear-cell histologies, do not need further adju-
vant therapy. Patients with high-risk early-stage
epithelial ovarian cancer, defined as stage I, grade 3;
stage IC, stage II, and clear-cell cancers, were felt to
require postsurgical adjuvant treatment. Over the
past 20 years, the Gynecologic Oncology Group
(GOG) has conducted 2 large prospective clinical
trials on this population. Because both clinical trials
had the same eligibility criteria for patient entry,
these studies provide a unique opportunity to inves-
tigate the prognostic factors for high-risk early-stage
ovarian cancer. The results of this analysis can
potentially allow us to assess factors that are predic-
tive for recurrence and survival in these women.
More important, it can help identify subgroups at
significant risk for recurrence after chemotherapy
treatments who may warrant novel therapies and
more aggressive treatment.
MATERIALS AND METHODSIn all, 506 women diagnosed with high-risk
early-stage
epithelial ovarian cancer patients enrolled in 2 pro-
spective randomized clinical trials conducted by
the GOG, protocol 95 (n 5 205) and protocol 157
(n 5 301). High-risk early-stage epithelial ovarian
can-
cer was defined as stage IA or IB (grade 3), stage IC orII (any
grade), and stage I or II clear-cell epithelial
ovarian cancer. Of these, 150 patients with incomplete
staging information were excluded from this analysis.
Patients provided written informed consent consistent
with all federal, state, and local requirements before
enrolling in the protocols. Details regarding
eligibility
criteria, treatment, and outcome for each particular
study have been previously published.17,19 On the
basis of the study entry criteria, a complete surgical
staging procedure was required. In summary, all peri-
toneal surfaces, including the undersurfaces of both
diaphragms, serosa, and mesentery, were to be visually
inspected and palpated for evidence of implants. If
there was no evidence of disease beyond the ovary orpelvis,
biopsies of the cul-de-sac, vesico uterine perito-
neum, bilateral pelvic side walls, paracolic gutters, and
undersurface of the diaphragm, and sampling of the
pelvic and para-aortic nodes, were to be performed.
All patients who underwent surgical staging were oper-
ated on by gynecologic oncologists mostly from aca-
demic institutions. In addition, all tumors underwent
central pathology review by expert gynecologic oncol-
ogy pathologists.
Baseline performance status before initiating
chemotherapy was defined according to GOG criteria
as: 0 5 normal activity; 1 5 symptomatic, fully
am-
bulatory; 2 5
symptomatic, in bed less than 50% of the time. The primary
endpoints for both studies
were disease recurrence-free survival (RFS) and over-
all survival (OS). RFS was calculated from the date of
study enrollment to the date of disease recurrence
(confirmed on physical, serologic, or radiologic exam),
or most recent follow-up visit. OS was calculated
from the date of study enrollment to the date of
death regardless of cause or last follow-up.
Kaplan-Meier survival analyses were performed
initially to estimate RFS and OS by each variable,
using
a log-rank test to compare the differences in survival
functions. Multivariate analysis was then conducted to
identify the independent prognostic factors as well as
to estimate their effects on RFS and OS adjusted forcovariates.
In survival analysis, patients with a GOG
performance status of 1 or 2 were combined because
of comparable associations with prognosis. In addition,
those with suspicious positive washings were consid-
ered positive for cytology. Furthermore, stage I patients
were further divided into 2 subgroups (stage IA/IB and
stage IC). We elected to use a categorical variable for
age, defined as < 60 years versus 60 years
old based
on preassessment. Multivariate analysis was conducted
using a stepwise Cox proportional hazards model, stra-
tified by type of treatment to control for potential con-
founding effects of the 2 study protocols and type of
treatment. All statistical tests were 2-tailed with a
sig-nificance level set at 5%. Statistical analyses were per-
formed using Statistical Analysis Software (SAS) v. 9.1
(SAS Institute, Cary, NC).
RESULTSOf the 506 patients included in this analysis, the
me-
dian age at diagnosis was 56 years (range, 22–88
Stage I-II Prognostic Factors/Chan et al. 2203
-
8/17/2019 mc_m6_Cancer+ovario+precoz
3/9
years) (Table 1). The majority (89.1%) of these
patients were white and the remainder were charac-
terized as Black (4%), Hispanic (4.2%), and Others
(2.8%). The baseline GOG performance status of
these women was 0, 1, and 2 in 52.2%, 43.9%, and
4.0%, respectively. All women underwent primary surgery
based on GOG standards. In all, 347 (68.6%)
patients had stage I disease, with stage IA in 13.6%,
IB in 2.0%, and 1C in 53.0%; 159 (31.4%) had stage II
cancers with stage IIA in 8.5%, IIB in 5.5%, and IIC
in 17.4%. Histologic cell types were distributed as
follows: clear cell (27.1%), endometrioid (26.5%),
serous (21.3%), mucinous (9.9%), and other cell types
(15.2%). Tumor grades were distributed as: grade 1
(18.8%), grade 2 (25.1%), grade 3 (29.1%), and not
graded (for clear cell) (27.1%). Of all patients, 153
(30.2%) were found to have ascites, and 219 (43.3%)
had tumor rupture found on surgery. On final pathol-
ogy review of all washings and ascites, 148 (29.6%) were
cytologically positive (n 5 125) or suspicious
positive (n 5 23). The presence of ascites during sur-
gery was greater in stage IC (33.6%) and stage II
(32.7%) compared with stage IA/IB (13.9%). The pre-
sence of ascites was also associated with positive
cytology: 46.4% of patients with malignant cells cyto-
logically had ascites and 21.8% of patients without
ascites had positive cytology. Furthermore, most
patients with stage IC (61.9%) or mucinous (62.0%)
tumors had tumor rupture at the time of surgery.
Stage of disease was associated with tumor histology
and grade. Patients with mucinous or clear-cell
histologies were more likely to have stage I rather
than stage II disease compared with other histologies(81.0% for
clear cell, 94.0% for mucinous vs 67.7%
for other histologies). Univariate analysis of prog-
nostic factors for RFS and OS are demonstrated in
Table 2.
All of the patients on these 2 trials (GOG 157 and
95) were treated with adjuvant platinum-based
chemotherapy or intraperitoneal radioactive chromic
phosphate. Nineteen percent of patients were treated
with intraperitoneal phosphate (32P), 21% with cyclo-
phosphamide/cisplatin (CP), 31% with carboplatin/
paclitaxel (PC) for 3 courses, and 29% with carbopla-
tin/paclitaxel for 6 courses.
With a median follow-up of 98 months (136months for
protocol 95 and 92 months for protocol
157), 140 recurrences (28%) and 151 (30%) deaths
were observed. The estimates of RFS and OS by
patient characteristics are shown in Table 2. Overall,
5-year RFS and OS were predicted to be 76% and
82%, respectively. Patients with age 60 years, stage
II, tumor grade 2 or 3, with the presence of ascites or
positive cytology had significantly worse RFS. There
TABLE 1Patient and Clinicopathologic Characteristics (N
5 506)
No. of patients %
Age, y
-
8/17/2019 mc_m6_Cancer+ovario+precoz
4/9
is also a suggestion that patients treated by PC and
CP had comparable RFS, but both of them had
improved RFS compared with patients treated by
32P.
Multivariate analysis identified 4 factors (age,
stage, tumor grade, and cytology) independently pre-
dictive of disease recurrence (Table 3). The relative
risk of disease recurrence for patients at age 60
years versus age
-
8/17/2019 mc_m6_Cancer+ovario+precoz
5/9
ease, tumor grade, and cytology. Among the prognos-
tic parameters, these independent prognostic factors were
used to develop a prognostic index for potential
clinical application. The prognostic model for RFS is
based on the 4 risk factors: age 60 years (vs
age < 60 years), stage II disease (vs stage I
disease),
positive cytology (vs negative cytology), and grade 2–
3 tumors or clear cell (vs grade 1 disease). Low-risk
patients were defined as those with no or 1 risk fac-
tor; intermediate-risk patients as those with any 2
risk factors; and high-risk patients as women with
any 3 or 4 risk factors. The 5-year RFS of the low-,
intermediate-, and high-risk groups was estimated to
be 88%, 71%, and 62%, respectively. On the basis of
the number of risk factors, patients in the low-, inter-
mediate-, and high-risk groups had corresponding
OSs of 88%, 82%, and 75% (P < .05) (Fig.
5A,B).
DISCUSSIONEarly-stage ovarian cancer patients constitute a
het-
erogeneous group with respect to risk of recurrence
and survival. Prior reports have shown that patients
with early-stage disease have overall survivals ran-
ging from 60% to 100%.1,2,4–6,20 Thus, stratifying this
heterogeneous group of patients can potentially
identify subgroups of high-risk patients for indivi-
dualized novel therapies in an attempt to improve
outcome. Likewise, it is important to identify a low-
risk group that may not require further cytotoxic
treatment. In this current analysis of 506 women
diagnosed with high-risk stage I and II epithelial
ovarian cancer treated on 2 GOG prospective rando-
mized trials, we found that older age, higher stage,
higher grade, and positive cytology are important
prognostic factors for recurrence and survival.
Earlier studies on the prognostic significance of
age in ovarian cancer have been inconclusive.
Although most reports have shown that younger
women are diagnosed with lower-stage and
more well-differentiated tumors, and have an improved
outcome compared with older women,21–25 others
have found that age is not an independent prognos-
tic factor after adjusting for stage and grade of dis-
ease.26–28 In addition, because of the low prevalence
of young patients diagnosed with invasive ovarian
cancer, these studies have also been limited by small
numbers of patients, inclusion of low malignant
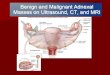
FIGURE 1. (A) Kaplan-Meier recurrence-free survival by
age group
(P 5 .004). (B) Kaplan-Meier overall survival by age group
(P < .001).
FIGURE 2. (A) Kaplan-Meier recurrence-free survival by
stage (P 5 .001).
(B) Kaplan-Meier overall survival by stage (P 5 .009).
2206 CANCER May 15, 2008 / Volume 112 / Number 10
-
8/17/2019 mc_m6_Cancer+ovario+precoz
6/9
potential tumors, germ cell or sex cord stromal
tumors, and unstaged cancers. In a recent analysis of
28,165 patients, Chan et al.28 identified 400 women
who were 60
(older) (57.4%) years of age. Across all stages, very
young women had a significant survival advantage
over the young and older groups, with 5-year dis-
ease-specific survival estimates at 78.7% versus
58.8% and 35.3%, respectively (P < .001). In this
cur-
rent analysis of a well-characterized group of early-
stage ovarian cancer patients with long follow-up,
younger age was an independent prognostic factor
for improved survival after controlling for surgery,
stage, grade, adjuvant therapy, and other clinicopath-
ologic factors.Previous studies have also demonstrated that
stage of disease is a prognostic factor in early-stage
ovarian cancers.13,16,29–33 Patients in this current
study with stage I cancers have a 5-year disease-spe-
cific survival of 84% compared with 76% in those
with stage II disease. An analysis on the subgroups
of stage I cancers found that those with stage IA or
IB disease have a survival of 85.9%. Given the excel-
lent outcome of these patients and the potential
toxicities associated with adjuvant chemotherapy,17,18
future studies must be carefully structured to deter-
mine the risk and benefit of cytotoxic chemotherapy
in low-risk disease. However, the outcome for
patients with stage II is significantly poorer, with RFS
and OS of 65.9 and 76.2%, respectively. Prior studies
have included these patients in clinical trials along
with more advanced (stage III and IV) cancers.31,34
Although the survival of stage II patients is poorer
compared with stage I disease, these women still
have a distinct survival advantage over those with
more advanced cancers.
Tumor grade was also found to be an independ-
ent prognostic factor for progression-free and dis-
ease-specific survival in our study. Similarly, Vergoteet al.35
studied a group of 1545 patients with stage I
disease and found that grade of disease was an inde-
pendent prognostic factor associated with disease-
free survival. These findings have also been con-
firmed by other, smaller studies.11,14,16,30,36–44
In this current analysis, malignant cytology was
an independent prognostic factor for increased risk
of recurrence and poorer survival. Early studies have
FIGURE 3. (A) Kaplan-Meier recurrence-free survival by
grade of disease
(P 5 .004). (B) Kaplan-Meier overall survival by grade of
disease (P 5 .01).
FIGURE 4. (A) Kaplan-Meier recurrence-free survival by
cytology
(P < .001). (B) Kaplan-Meier overall survival by
cytology (P 5 .01).
Stage I-II Prognostic Factors/Chan et al. 2207
-
8/17/2019 mc_m6_Cancer+ovario+precoz
7/9
demonstrated that patients with positive washing have
a poorer prognosis.45,46 Creasman and Rutledge47
reported that 60% of 98 patients with ovarian cancer
who underwent surgery had abnormal peritoneal
cytologic specimens. Likewise, a more recent report
also found positive peritoneal washing cytology at
initial surgery in 90 (80.4%) of 112 patients with
ovarian carcinomas.48 Those authors also showed
that positive cytology portends a poorer prognosis.
The prognostic significance of clear-cell histology
compared with other subtypes of epithelial ovarian
cancers remains controversial. In a recent review of 54
studies on ovarian clear-cell carcinoma, Pecta-
sides et al.49 showed that clear-cell cancers have a
significantly poorer survival compared with other
histologic subtypes of epithelial ovarian cancer. In
patients with more advanced stage cancer, the
response rate to platinum-based chemotherapy and
survival were significantly lower than those with se-
rous tumors. However, others have not been able to
find an association between cell type and prognosis
in early-stage disease. Contributing factors for these
conflicting results may include the lack of central
pathology review and intraobserver variabilities on
determining cell type50,51 and various treatment regi-
mens.49 In this current study of early-stage ovariancancer where
the majority of patients were uniformly
staged and treated on 2 standardized protocols, we
were unable find a statistically significant survival
difference between clear-cell and other histologies.
Consistent with prior reports, our data did not
reveal that tumor rupture was associated with a
poorer outcome.15,30,39 However, Vergote et al.35
found a deleterious effect of rupture either during or
before surgery on disease-free survival. The interac-
tion between tumor rupture and more early-stage
cancers in our study may have influenced our ability
to determine the true significance of tumor rupture.
One of the shortcomings of our study is that there isa lack of
information regarding the time of rupture,
eg, preoperatively or intraoperatively. Some prior stu-
dies have found that preoperative rupture may carry
a worse prognosis compared with intraoperative rup-
ture.14,52 In addition, this current analysis did not
find ascites to be a significant prognostic factor. This
may be explained by the interaction between ascites,
cytology, and stage of disease. For, after adjusting for
these factors, ascites was no longer prognostically
important.
Our study was limited by the potential selection
bias inherent in randomized trials. This study cohort
may comprise a subset of high-risk patients treated
at research centers that may not represent the expe-
rience in the general population. Furthermore, given
that these patients were enrolled in these 2 large
trials ranging from 1986 to 1998, there may exist sig-
nificant differences related to cancer supportive care
and treatment of recurrences over this time period.
Moreover, there was a lack of complete information
regarding the extent of the comprehensive staging
procedures on all patients. In fact, 29.5% of patients
in the GOG 157 trial had incomplete or inadequately
documented surgical staging information.17 It is im-
portant to note that the descriptive statistics and
results of this study were based on a selected group
of patients with high-risk early-stage cancers definedby the
eligibility criteria from 2 randomized clinical
trials of the GOG. Thus, in this specific subset of
patients there is a significantly higher proportion
(27.1%) of clear-cell histologies compared with other
cell types. Therefore, these results may not apply to
the overall group of stage I and II patients, particu-
larly those with stage I, grade 1 or 2 disease, and
nonclear-cell type. Although it is important to iden-
FIGURE 5. (A) Kaplan-Meier recurrence-free survival by
number of risk
factors (age 60 years, stage II disease, positive
cytology, and grade 23
tumors or clear cell). Low-risk: 01 risk factors; mid-risk: 2
risk factors;
high-risk: 34 risk factors (P < .001). (B)
Kaplan-Meier overall survival by
number of risk factors (P < .001).
2208 CANCER May 15, 2008 / Volume 112 / Number 10
-
8/17/2019 mc_m6_Cancer+ovario+precoz
8/9
tify a low-risk group that may not require further
cytotoxic treatment, we are unable to define such a
low-risk group of patients from this report because
all of the women in these clinical trials received ad-
juvant therapy. Thus, a prospective trial designed to
analyze the benefits of adjuvant therapy versus ob-servation is
warranted in this low-risk group defined
by this current study.
The strengths of our study include the high
number of patients reported from 2 randomized pro-
spective trials with defined selection criteria and over
80 months of follow-up. Furthermore, these patients
underwent staging by gynecologic oncologists mostly
from academic institutions. In addition, these tumors
underwent central pathology review by expert gyne-
cologic oncology pathologists.
In summary, our findings suggest that age, stage,
grade, and malignant cytology are important prog-
nostic factors in early-stage epithelial ovarian cancer.This
information may be considered in the design of
future clinical trials.
REFERENCES1. Jemal A, Siegel R, Ward E, et al. Cancer
statistics, 2006. CA
Cancer J Clin. 2006;56:106–130.
2. Partridge EE, Phillips JL, Menck HR. The National Cancer
Data Base report on ovarian cancer treatment in United
States hospitals. Cancer . 1996;78:2236–2246.
3. Hoskins PJ, Swenerton KD, Manji M, et al. ‘Moderate-risk’
ovarian cancer (stage I, grade 2; stage II, grade 1 or 2)
trea-
ted with cisplatin chemotherapy (single agent or combina-
tion) and pelvi-abdominal irradiation. Int J Gynecol
Cancer .1994;4:272–278.
4. Heintz AP, Odicino F, Maisonneuve P, et al. Carcinoma
of
the ovary. Int J Gynaecol Obstet . 2003;83(Suppl
1):135–166.
5. Averette HE, Janicek MF, Menck HR. The National Cancer
Data Base report on ovarian cancer. American College
of
Surgeons Commission on Cancer and the American Cancer
Society. Cancer . 1995;76:1096–1103.
6. Kosary CL. FIGO stage, histology, histologic grade, age
and
race as prognostic factors in determining survival for can-
cers of the female gynecological system: an analysis
of
1973–87 SEER cases of cancers of the endometrium, cervix,
ovary, vulva, and vagina. Semin Surg Oncol .
1994;10:31–46.
7. Nguyen HN, Averette HE, Hoskins W, et al. National
survey
of ovarian carcinoma. VI. Critical assessment of current
International Federation of Gynecology and Obstetrics sta-
ging system. Cancer . 1993;72:3007–3011.8. Dembo AJ,
Davy M, Stenwig AE, et al. Prognostic factors in
patients with stage I epithelial ovarian cancer. Obstet
Gyne-
col . 1990;75:263–273.
9. Sevelda P, Vavra N, Schemper M, et al. Prognostic factors
for survival in stage I epithelial ovarian carcinoma.
Cancer .
1990;65:2349–2352.
10. Young RC, Walton LA, Ellenberg SS, et al. Adjuvant
therapy
in stage I and stage II epithelial ovarian cancer. Results
of
2 prospective randomized trials. N Engl J Med .
1990;322:
1021–107.
11. Finn CB, Luesley DM, Buxton EJ, et al. Is stage I
epithelial
ovarian cancer overtreated both surgically and systemi-
cally? Results of a 5-year cancer registry review. Br J
Obstet
Gynaecol . 1992;99:54–58.
12. Vergote IB, Kaern J, Abeler VM, et al. Analysis of
prognostic
factors in stage I epithelial ovarian carcinoma: importance
of degree of differentiation and deoxyribonucleic acid
ploidy in predicting relapse. Am J Obstet Gynecol .
1993;169:40–52.
13. Bertelsen K, Holund B, Andersen JE, et al. Prognostic
fac-
tors and adjuvant treatment in early epithelial ovarian can-
cer. Int J Gynecol Cancer . 1993;3:211–218.
14. Sjovall K, Nilsson B, Einhorn N. Different types of
rupture
of the tumor capsule and the impact on survival in
early
ovarian carcinoma. Int J Gynecol Cancer .
1994;4:333–336.
15. Ahmed FY, Wiltshaw E, A’Hern RP, et al. Natural
history
and prognosis of untreated stage I epithelial ovarian carci-
noma. J Clin Oncol . 1996;14:2968–2975.
16. Trope C, Kaern J, Hogberg T, et al. Randomized study on
adjuvant chemotherapy in stage I high-risk ovarian cancer
with evaluation of DNA-ploidy as prognostic
instrument.
Ann Oncol . 2000;11:281–288.
17. Bell J, Brady MF, Young RC, et al. Randomized phase III
trial of 3 versus 6 cycles of adjuvant carboplatin and
pacli-taxel in early stage epithelial ovarian carcinoma: a
Gyneco-
logic Oncology Group study. Gynecol Oncol .
2006;102:432–439.
18. Travis LB, Holowaty EJ, Bergfeldt K, et al. Risk of
leukemia after platinum-based chemotherapy for ovarian
cancer.
N Engl J Med . 1999;340:351–357.
19. Young RC, Brady MF, Nieberg RK, et al. Adjuvant
treatment
for early ovarian cancer: a randomized phase III trial
of intraperitoneal 32P or intravenous cyclophosphamide and
cisplatin—a gynecologic oncology group study. J Clin
Oncol . 2003;21:4350–4355.20. Nguyen HN, Averette HE,
Hoskins W, et al. National survey
of ovarian carcinoma. Part V. The impact of physician’s
specialty on patients’ survival. Cancer .
1993;72:3663–3670.
21. Chan JK, Loizzi V, Lin YG, et al. Stages III and IV
invasive
epithelial ovarian carcinoma in younger versus older
women: what prognostic factors are important?
Obstet Gynecol . 2003;102:156–161.
22. Plaxe SC, Braly PS, Freddo JL, et al. Profiles of women
age
30–39 and age less than 30 with epithelial ovarian cancer.
Obstet Gynecol . 1993;81:651–654.
23. Rodriguez M, Nguyen HN, Averette HE, et al. National
sur-
vey of ovarian carcinoma XII. Epithelial ovarian malignan-
cies in women less than or equal to 25 years of age.
Cancer . 1994;73:1245–1250.
24. Smedley H, Sikora K. Age as a prognostic factor in
epithelial
ovarian carcinoma. Br J Obstet Gynaecol .
1985;92:839–842.
25. Thigpen T, Brady MF, Omura GA, et al. Age as a
prognostic
factor in ovarian carcinoma. The Gynecologic Oncology
Group experience. Cancer . 1993;71:606–614.
26. Duska LR, Chang YC, Flynn CE, et al. Epithelial ovarian
carcinoma in the reproductive age group. Cancer .
1999;
85:2623–269.
27. Massi D, Susini T, Savino L, et al. Epithelial ovarian
tumors
in the reproductive age group: age is not an independent
prognostic factor. Cancer . 1996;77:1131–116.
28. Chan JK, Urban R, Cheung MK, et al. Ovarian cancer in
younger vs older women: a population-based
analysis. Br J
Cancer . 2006;95:1314–1320.
29. Nagele F, Petru E, Medl M, et al. Preoperative CA 125:
an
independent prognostic factor in patients with stage I
epithelial ovarian cancer. Obstet Gynecol .
1995;86:259–264.
Stage I-II Prognostic Factors/Chan et al. 2209
-
8/17/2019 mc_m6_Cancer+ovario+precoz
9/9
30. Brugghe J, Baak JP, Wiltshaw E, et al. Quantitative
prognos-
tic features in FIGO I ovarian cancer patients without post-
operative treatment. Gynecol Oncol .
1998;68:47–53.
31. Du Bois A, Rochon J, Lamparter C, et al. Pattern of care
and
impact of participation in clinical studies on the outcome
in
ovarian cancer. Int J Gynecol Cancer .
2005;15:183–191.
32. Mizuno M, Kikkawa F, Shibata K, et al. Long-term progno-sis
of stage I ovarian carcinoma. Prognostic importance of
intraoperative rupture. Oncology . 2003;65:29–36.
33. Valverde JJ, Martin M, Garcia-Asenjo JA, et al.
Prognostic
value of DNA quantification in early epithelial ovarian car-
cinoma. Obstet Gynecol . 2001;97:409–416.
34. International Collaborative Ovarian Neoplasm Group. Pa-
clitaxel plus carboplatin versus standard chemotherapy
with either single-agent carboplatin or
cyclophosphamide,
doxorubicin, and cisplatin in women with ovarian cancer:
the ICON3 randomised trial. Lancet .
2002;360:505–515.
35. Vergote I, De Brabanter J, Fyles A, et al. Prognostic
impor-
tance of degree of differentiation and cyst rupture in stage
I invasive epithelial ovarian carcinoma. Lancet .
2001;357:
176–182.
36. Skirnisdottir I, Seidal T, Sorbe B. A new prognostic model
com-
prising p53, EGFR, and tumor grade in early stage
epithelialovarian carcinoma and avoiding the problem of
inaccurate
surgical staging. Int J Gynecol Cancer .
2004;14:259–270.
37. Trimbos JB, Vergote I, Bolis G, et al. Impact of
adjuvant
chemotherapy and surgical staging in early-stage ovarian
carcinoma: European Organisation for Research and Treat-
ment of Cancer-Adjuvant ChemoTherapy in Ovarian Neo-
plasm trial. J Natl Cancer Inst .
2003;95:113–125.
38. Le T, Adolph A, Krepart GV, et al. The benefits of
compre-
hensive surgical staging in the management of early-stage
epithelial ovarian carcinoma. Gynecol Oncol .
2002;85:351–
355.
39. Zanetta G, Rota S, Chiari S, et al. The accuracy of
staging:
an important prognostic determinator in stage I ovarian
carcinoma. A multivariate analysis. Ann Oncol .
1998;9:
1097–1101.
40. Rubin SC, Wong GY, Curtin JP, et al. Platinum-based
chemo-therapy of high-risk stage I epithelial ovarian cancer after
com-
prehensive surgical staging. Obstet Gynecol . 1993;82:
143–147.
41. Villa A, Parazzini F, Acerboni S, et al. Survival and
prognos-
tic factors of early ovarian cancer. Br J Cancer .
1998;77:
123–124.
42. Bolis G, Colombo N, Pecorelli S, et al. Adjuvant
treatment
for early epithelial ovarian cancer: results of 2 randomised
clinical trials comparing cisplatin to no further treatment
or chromic phosphate (32P). G.I.C.O.G.: Gruppo Interregio-nale
Collaborativo in Ginecologia Oncologica. Ann Oncol .
1995;6:887–893.
43. Sainz de la Cuesta R, Goff BA, Fuller AF Jr, et al.
Prognostic
importance of intraoperative rupture of malignant ovarian
epithelial neoplasms. Obstet Gynecol .
1994;84:1–7.
44. Paramasivam S, Tripcony L, Crandon A, et al. Prognostic
importance of preoperative CA-125 in International Fed-
eration of Gynecology and Obstetrics stage I epithelial
ovarian cancer: an Australian multicenter study. J
Clin
Oncol . 2005;23:5938–5942.
45. Keettel WC, Pixley E. Diagnostic value of peritoneal
wash-
ings. Clin Obstet Gynecol . 1958;1:592–606.
46. Morton DG, Moore JG, Chang N. The clinical value of
peri-
toneal lavage for cytologic examination. Am J Obstet
Gyne-
col . 1961;81:1115–1125.
47. Creasman WT, Rutledge F. The prognostic value of perito-neal
cytology in gynecologic malignant disease. Am J
Obstet Gynecol . 1971;110:773–781.
48. Zuna RE, Behrens A. Peritoneal washing cytology in gyne-
cologic cancers: long-term follow-up of 355 patients. J
Natl
Cancer Inst . 1996;88:980–987.
49. Pectasides D, Pectasides E, Psyrri A, et al. Treatment
issues
in clear cell carcinoma of the ovary: a different entity?
Oncologist . 2006;11:1089–1094.
50. Baak JP, Langley FA, Talerman A, et al. Interpathologist
and intrapathologist disagreement in ovarian tumor
grading and typing. Anal Quant Cytol Histol .
1986;8:354–
357.
51. Hernandez E, Bhagavan BS, Parmley TH, et al. Interobser-
ver variability in the interpretation of epithelial ovarian
cancer. Gynecol Oncol . 1984;17:117–123.
52. Kodama S, Tanaka K, Tokunaga A, et al. Multivariate
analy-sis of prognostic factors in patients with ovarian cancer
stage I and II. Int J Gynaecol Obstet .
1997;56:147–153.
2210 CANCER May 15, 2008 / Volume 112 / Number 10