-
7/29/2019 ALTERACIONES DEL POTASIO 2006.pdf
1/16
Resuscitation (2006) 70, 1025
REVIEW PAPER
Potassium disordersclinical spectrum and
emergency management
Annette V.M. Alfonzo a,, Chris Isles b, Colin Geddes c, Chris
Deighan a
a Renal Unit, Glasgow Royal Infirmary, Castle Street, Glasgow G4
0SF, UKb Renal Unit, Dumfries & Galloway Royal Infirmary,
Bankend Road, Dumfries DG1 4AP, UKc Renal Unit, Western Infirmary,
Dumbarton Road, Glasgow G11 6NT, UK
Received 12 August 2005 ; received in revised form 28 October
2005; accepted 3 November 2005
KEYWORDS
Hyperkalaemia;
Hypokalaemia;
Renal failure;
Dialysis;
Arrhythmias;
Cardiac arrest
Summary Potassium disorders are common and may precipitate
cardiac arrhyth-mias or cardiopulmonary arrest. They are an
anticipated complication in patientswith renal failure, but may
also occur in patients with no previous history of renaldisease.
They have a broad clinical spectrum of presentation and this paper
willhighlight the life-threatening arrhythmias associated with both
hyperkalaemia andhypokalaemia. Although the medical literature to
date has provided a foundationfor the therapeutic options
available, this has not translated into consistent medicalpractice.
Treatment algorithms have undoubtedly been useful in the
managementof other medical emergencies such as cardiac arrest and
acute asthma. Hence, we
have applied this strategy to the treatment of hyperkalaemia and
hypokalaemiawhich may prove valuable in clinical practice. 2005
Elsevier Ireland Ltd. All rights reserved.
Contents
Introduction..................................................................................................
11Hyperkalaemia...............................................................................................
11
Clinical spectrum of presentation of hyperkalaemia ... ... ....
... ... .... ... ... .... ... ... ... .... ... ... ....
12Symptoms.........................................................................................
12ECG abnormalities........ ....... ...... ....... ....... ......
....... ....... ...... ....... ...... ....... 12Arrhythmias
associated with hyperkalaemia .... ... ... .... ... ... .... ...
... .... ... ... .... ... ... ... .. 14
Pseudohyperkalaemia ....... ....... ...... ....... ......
....... ....... ...... ....... ....... ...... ....... ...
15Emergency treatment of hyperkalaemia ...... ....... ......
....... ....... ...... ....... ....... ...... ...... 15
Abbreviations: K, potassium; ARF, acute renal failure; CRF,
chronic renal failure; ESRF, end-stage renal failure A Spanish
translated version of the summary of this article appears as
Appendix in the online version at
10.1016/j.resuscitation.2005.11.002. Corresponding author. Tel.:
+44 141 211 4842; fax: +44 141 211 4843.
E-mail address: [email protected] (A.V.M.
Alfonzo).
0300-9572/$ see front matter 2005 Elsevier Ireland Ltd. All
rights reserved.doi:10.1016/j.resuscitation.2005.11.002
http://dx.doi.org/10.1016/j.resuscitation.2005.11.002mailto:[email protected]://localhost/var/www/apps/conversion/tmp/scratch_2/dx.doi.org/10.1016/j.resuscitation.2005.11.002http://localhost/var/www/apps/conversion/tmp/scratch_2/dx.doi.org/10.1016/j.resuscitation.2005.11.002mailto:[email protected]://dx.doi.org/10.1016/j.resuscitation.2005.11.002
-
7/29/2019 ALTERACIONES DEL POTASIO 2006.pdf
2/16
Potassium disordersclinical spectrum and emergency management
11
Protecting the heart....... ....... ...... ....... .......
...... ....... ...... ....... ....... ...... ...... 16Shifting of
potassium into cells....... ....... ....... ...... ....... .......
...... ....... ...... ....... . 16Removing potassium from the
body......... ...... ....... ...... ....... ....... ...... .......
....... .. 17
Influence of degree of renal impairment on management.. ... ....
... ... .... ... ... ... .... ... ... .... ... ... 17Interventions
in cardiopulmonary arrest... ....... ...... ....... ....... ......
....... ...... ....... ....... .. 18
Haemodialysis during resuscitation..... ....... ...... .......
....... ...... ....... ...... ....... ...... 18Post-resuscitation
care..... ....... ....... ...... ....... ....... ...... .......
....... ...... ....... .... 18
Development of an emergency treatment algorithm .... ... ...
.... ... ... .... ... ... .... ... ... .... ... ... ... 19
Acute severe hyperkalaemia ...... ....... ....... ...... .......
...... ....... ....... ...... ....... .... 20Life-threatening
hyperkalaemia ...... ....... ....... ...... ....... ....... ......
....... ...... ....... . 20Cardiac
arrest.....................................................................................
20Principles of treatment algorithm ....... ....... ...... .......
....... ...... ....... ....... ...... ..... 20
Prevention of hyperkalaemia ...... ....... ....... ......
....... ....... ...... ....... ...... ....... ....... ...
20Hypokalaemia................................................................................................
20
Clinical spectrum of hypokalaemia ...... ....... ....... ......
....... ...... ....... ....... ...... ....... ....
21Symptoms.........................................................................................
21ECG abnormalities........ ....... ....... ...... ....... ......
....... ....... ...... ....... ....... ...... 21Arrhythmias
associated with hypokalaemia... .... ... ... .... ... ... .... ...
... .... ... ... ... .... ... ... 21
Treatment of hypokalaemia........... ....... ...... .......
....... ...... ....... ....... ...... ....... ....... 22Developing
a treatment algorithm for hypokalaemia.... .... ... ... ... ....
... ... .... ... ... .... ... ... .... .. 22
Patients with no symptoms....... ....... ...... ....... ......
....... ....... ...... ....... ....... ..... 22Life-threatening
arrhythmias... ...... ....... ....... ...... ....... ....... ......
....... ....... ...... . 22
Cardiac
arrest.....................................................................................
22Prevention of hypokalaemia ....... ...... ....... ....... ......
....... ....... ...... ....... ....... ...... .... 22
Summary.....................................................................................................
24Conflict of interest........ ....... ...... ....... ......
....... ....... ...... ....... ....... ...... ....... ....... ...
24Acknowledgement........ ....... ...... ....... ....... ......
....... ...... ....... ....... ...... ....... ....... ....
24References...................................................................................................
24
Introduction
Potassium (K) is the most abundant cation in thebody. Under
normal circumstances, only 2% of totalbody potassium stores are
found in the extracellularspace and serum potassium concentration
is tightlyregulated between 3.5 and 5.0 mmol/l.1 Therefore,there is
normally a large potassium concentrationgradient between
intracellular and extracellularfluid compartments and it is the
magnitude of thepotassium gradient across cell membranes that
con-tributes to the excitability of nerve and musclecells,
including the myocardium.2
Potassium homeostasis is largely regulated bythe kidney
accounting for excretion of 90% of daily
potassium loss.1 Therefore patients with renal fail-ure, acute
or chronic, who have impaired regulatorymechanisms are prone to
hyperkalaemia. Patientswith normal renal function eliminate only
510%of their daily potassium load through the gut.However, in
patients with end-stage renal failure(ESRF), gut elimination is
increased and accountsfor up to 25% of daily potassium
elimination.3
Potassium disorders are common in clinical prac-tice and may be
life-threatening. Before approach-ing the treatment of these
conditions, it is impor-
tant to understand the basis of potassium home-ostasis and to
recognise that these disorders maypresent with a diverse clinical
spectrum includingsymptoms, ECG abnormalities and/or
arrhythmias.There remains little consistency in treatment
ofhyperkalaemia and hypokalaemia, therefore treat-ment algorithms
have been developed to assistemergency management.
Hyperkalaemia
Hyperkalaemia is the most common electrolyte dis-order
associated with potentially life-threateningarrhythmias and
cardiopulmonary arrest. It is
defined as a serum potassium concentration above5.0 mmol/l2 and
may be classified as mild (K5.05.9 mmol/l), moderate (K 6.06.4
mmol/l) orsevere (K6.5 mmol/l). A potassium concentra-tion above
10.0mmol/l is usually fatal unlessemergency treatment is readily
instituted, how-ever survival with extreme hyperkalaemia (K14
mmol/l) has been reported.4 There are a num-ber of potential causes
of hyperkalaemia whichare listed in Table 1, but most commonly itis
the result of impaired excretion by the kid-
-
7/29/2019 ALTERACIONES DEL POTASIO 2006.pdf
3/16
12 A.V.M. Alfonzo et al.
Table 1 Causes of Hyperkalaemia
Drugs ACE-inhibitors e.g. ramipril, captoprilAngiotensin
Receptor Blockers e.g. losartanNSAIDs e.g. ibuprofen,
diclofenacBeta-blockers e.g. atenololK+ supplements e.g. oral or IV
replacementK+ sparing diuretics e.g. spironolactone
Antibiotics e.g. trimethoprimAnaesthetic agents e.g.
suxamethonium
Renal and metabolic diseases Acute renal failureChronic renal
failureType 4 renal tubular acidosisMetabolic acidosis
Diet Foods with high potassium contentFasting relative lack of
insulinSalt substitute Lo salt
Endocrine disorders Addisons DiseaseHyporeninaemiaInsulin
deficiency/Hyperglycaemia
Haematological disorder/Massive Cell Death Tumour lysis
syndromeRhabdomyolysisMassive blood transfusionMassive haemolysis
mechanical cell damage
Others Hyperkalaemic periodic paralysisPseudo-hyperkalaemia
Abnormal erythrocytesThrombocytosisLeucocytosis
ACE: angiotensin converting enzyme; K+: potassium; NSAIDs:
non-steroidal anti-inflammatory drugs; IV: intravenous.
neys or increased release of potassium fromcells.2
Clinical spectrum of presentation ofhyperkalaemia
Symptoms
Patients may present with weakness progressing toflaccid
paralysis, paraesthesia, depressed deep ten-don reflexes or
respiratory difficulties.13 However,these symptoms usually only
occur in severe cases,are not specific to hyperkalaemia and are
oftenover-shadowed by the primary illness precipitating
hyperkalaemia. On the other hand, the absence ofthese symptoms
should not lead to a false sense ofsecurity if the clinical history
suggests a high riskof an electrolyte disturbance. In any event,
moreinformation is required to guide medical manage-ment and the
most useful tests are serum biochem-istry and ECG.
ECG abnormalities
The first indicator of hyperkalaemia may bethe presence of ECG
abnormalities, arrhythmias,
or cardiac arrest. The effect of hyperkalaemiaon the ECG depends
on the absolute serumpotassium as well as the rate of
increase.3,5,6
There is great variability in the level of serumpotassium which
results in ECG changes, butmost patients appear to show ECG
abnormalitiesat a serum potassium level above 6.7 mmol/l.3
In rare instances, the ECG may be normaleven in extreme
hyperkalaemia and this shouldraise the possibility of
pseudo-hyperkalaemia.7,8
In the context of diabetic ketoacidosis, hyper-kalaemia may also
present with ECG changessuggestive of myocardial ischaemia or
pseudo-
infarction.9 The presence of other metabolic dis-turbances, such
as hypocalcaemia, hyponatraemia,and acidaemia, may exacerbate the
effects ofhyperkalaemia.3
Cardiac sensitivity to hyperkalaemia is maxi-mal in the atrium,
and later in decreasing order,the ventricular cells, His cells,
sinoatrial node andinter-atrial tracts.10 This may help to explain
theprogressive changes seen in the ECG with increas-ing severity of
hyperkalaemia (Table 2). As serumpotassium rises above 5.56.5
mmol/l, tall peaked
-
7/29/2019 ALTERACIONES DEL POTASIO 2006.pdf
4/16
Potassium disordersclinical spectrum and emergency management
13
Table 2 ECG changes associated with the severity of
hyperkalaemia
There is some degree of overlap of ECG features in
hyperkalaemia. As serum potassium rises above 7 mmol/l, more than
oneabnormality may be present. The risk of cardiac arrest increases
with rising serum potassium and the presence of ominous ECGsigns
indicated above.
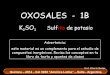
Figure 1 Life-threatening ECG changes in hyperkalaemia. (a)
Illustrates tented T waves, loss of P waves and a wideQRS complex
in a patient presenting with paralysis and acute renal failure
(serum K 9.3 mmol/l). (b) Illustrates a sine-wave pattern in a
patient with acute renal failure and digoxin toxicity (serum K 9.3
mmol/l). (c) Illustrates a severebradycardia at a rate of 28
beats/min in a haemodialysis patient presenting with syncope (serum
K 8.1mmol/l). (d) Illus-trates ventricular tachycardia in a
haemodialysis patient presenting with generalised weakness (serum K
9.1 mmol/l).The paper speed is 25 mm/s.
-
7/29/2019 ALTERACIONES DEL POTASIO 2006.pdf
5/16
14 A.V.M. Alfonzo et al.
T waves may appear. However, only 20% of hyper-kalaemic patients
show the classical symmetricallynarrow peaked T waves, while the
others showlarge amplitude T waves.11 As serum potassiumrises to
6.57.5 mmol/l, the PR interval becomesprolonged and the P wave
becomes flattened andeventually lost. This is followed by
prolongation of
the QRS complex when serum potassium rises to7.08.0 mmol/l. In
severe hyperkalaemia, many ofthese features may occur
simultaneously as shownin Figure 1a. Untreated, the QRS complex
mergeswith the T wave to form a sine-wave pattern withimpending
cardiac arrest (Figure 1b).
The effect of hyperkalaemia on the ECG inpatients with end-stage
renal failure is less wellunderstood. Early investigators suggested
thatpatients with ESRF have a tolerance to hyper-kalaemia and
thereby do not manifest the usualneuromuscular and cardiac
features.7,12 Morerecently, it has been postulated that the
absence
of typical ECG changes may be partly explainedby changes in
serum calcium.6 Nevertheless, theECG remains central to the
management of hyper-kalaemia in all patients, including those with
renalfailure.
Arrhythmias associated with hyperkalaemia
In addition to the ECG changes, virtually anyarrhythmia or
conduction disturbance can occur inthe presence of hyperkalaemia.
In some instances,treatment may be delayed as the rhythm
distur-bance may not be immediately related to the elec-
trolyte disorder. The following is a review of thespectrum of
arrhythmias associated with severehyperkalaemia.Bradycardia.
Bradycardia is an ominous complica-tion of hyperkalaemia, but there
are few reportsin the literature.1315 Patients presenting witha
severe bradycardia in the context of hyper-kalaemia, as shown in
Figure 1c, pose several dilem-mas. Firstly, there is no widely
available guidancefor the use of calcium salts for bradycardia
inducedby hyperkalaemia. As bradycardia is listed as apotential
adverse effect of calcium salts, there maybe further reluctance to
use calcium salts even in
the context of severe hyperkalaemia. However, theadministration
of calcium to patients with AV blockmay avert progression to
asystole while potassiumlowering drugs take effect and definitive
treatmentis being planned.16
Secondly, the response to atropine is usually poorand a
cardiology opinion is often sought. In this sit-uation, it may seem
compelling to pace the heartprior to haemodialysis. Indeed there is
one report oftemporary pacing for complete heart block inducedby
hyperkalaemia (K 7.99 mmol/l), in which pacing
improved the haemodynamic status and appearedto facilitate an
uneventful haemodialysis.15 In thiscase report, the ECG returned to
normal sinusrhythm after haemodialysis. However, temporarypacing is
not without risk, may not be effective anddelays definitive
treatment of the underlying dis-order. Furthermore, proceeding with
haemodialysis
without pacing may have led to the same outcome,which is often
the case in our own clinical experi-ence.
Thirdly, there is some evidence to suggest areduced efficacy of
temporary pacing. In severehyperkalaemia, there is elevation of the
stimu-lation threshold at the electrode tissue interfaceduring
cardiac pacing which can lead to failureof ventricular
depolarisation.17 This was evidentin a case report of a
post-operative patient whoprogressed to asystole due to
hyperkalaemia (K10.2 mmol/l) despite the presence of a function-ing
temporary pacemaker inserted at the time of
cardiac surgery.18 Similarly, transvenous pacing wasunsuccessful
in a 16-year-old patient with severehyperkalaemia (K 9.8 mmol/l)
despite good wireposition on screening.19 In terms of safety, in
addi-tion to the usual risks of central venous cannu-lation,
temporary pacing may be complicated byarrhythmias as hyperkalaemia
increases myocardialexcitability.
Lastly, patients with permanent pacemakersare not protected from
the cardiac consequencesof hyperkalaemia. Loss of atrial capture
hasbeen reported in patients with dual-chamber pac-
ing devices who become hyperkalaemic.17,20
Itis postulated that the high atrial myocardialsensitivity to
hyperkalaemia may be responsi-ble for the atrial unresponsiveness
observed dur-ing dual-chamber pacing.17 In another
report,hyperkalaemia-induced 2:1 AV block in a patientwith a
dual-chamber pacemaker.21 Other mech-anisms by which hyperkalaemia
may affect thepaced heart include prolongation of intraventric-ular
conduction manifesting as a very wide QRScomplex17,22 and pacemaker
latency which is anincrease in the interval between the
pacemakerstimulus artefact and the onset of the paced beat.23
Treatment of hyperkalaemia leads to resolution ofconduction
abnormalities and narrowing of the QRScomplex.
A universal recommendation is difficult in theface of little
evidence, but haemodialysis per-formed without initial
ultrafiltration and withappropriate cardiac monitoring, usually
resolvesthe bradycardia without the need for cardiac inter-vention.
A defibrillator with external pacing facil-ities should be
available although this is rarelyneeded. Persistent bradycardia
when the serum
-
7/29/2019 ALTERACIONES DEL POTASIO 2006.pdf
6/16
Potassium disordersclinical spectrum and emergency management
15
potassium becomes normal requires further inves-tigation and
management.Asytole. The outcome of asystolic cardiac arrestdue to
hyperkalaemia is usually fatal unless theserum potassium can be
returned to normal.One explanation is that severe
hyperkalaemiacauses myocardial conductivity and excitability
to decrease eventually, thereby blocking car-diac conduction
globally and maintaining cardiacstandstill.10 Despite this, there
are several reportsof successful resuscitation in patients
present-ing with or developing asystole as a result ofsevere
hyperkalaemia.13,18,19,24 Dialysis was neces-sary during the course
of cardiopulmonary resusci-tation (CPR) in most of these cases to
lower theserum potassium. All of the resuscitation attemptswere
prolonged and notably, the only patient man-aged medically without
dialysis was reported tomake a spontaneous recovery 8 min after
termi-nation of resuscitation.24 This suggests that the
effects of medical therapy may be delayed in thecontext of a
cardiac arrest. Hyperkalaemia-inducedasystole is thought to be more
common in chronicthan in acute hyperkalaemia,11 however, one ofthe
above cases illustrated acute hyperkalaemia (K9.8 mmol/l) induced
by suxamethonium in the pres-ence of otherwise normal renal
function.19
Ventricular tachycardia. Ventricular tachy-cardia (VT) is a
recognised manifestation ofhyperkalaemia,25,26 but it is more
commonlyreported in association with hypokalaemia.11 Ithas also
been suggested that the presence of a
broad complex tachycardia induced by hyper-kalaemia may be
misinterpreted as VT instead ofa sine-wave pattern.24 However,
pulseless VT hasbeen documented as the presenting cardiac
arrestrhythm4,2729 or may occur during the resuscitationattempt of
another primary rhythm19,24,30 in thepresence of hyperkalaemia. VT
in the presenceof a cardiac output may also be a manifestationof
severe hyperkalaemia in children31 as wellas adults,32 and this is
confirmed by our ownobservations as shown in Figure 1d.Ventricular
fibrillation. Ventricular fibrillation(VF) is often presented as
the natural transi-
tion from a sine-wave pattern in the presenceof extreme
hyperkalaemia (K > 8.0 mmol/l).1,3,11,32
However, in another report, ventricular arrhyth-mias or cardiac
arrest was said to occur at any timepoint along the transition from
peaked T waves tothe sine-wave pattern.6 In reality, a sine-wave
pat-tern is a rare phenomenon probably because it givesrise to VF
fairly rapidly, although it can also progressto VT or asystole.24
Additionally, the threshold forVF in hyperkalaemic patients is
likely to be vari-able and may be influenced by the presence of
other electrolyte disorders. Therefore to pre-emptcardiac
arrest, it is important to recognise all warn-ing signs (Table 2),
institute treatment early andto be vigilant at all times. Analogous
to resuscita-tion for hypothermia, it is important to recognisethat
defibrillation is frequently unsuccessful untilthe serum potassium
is controlled and CPR should
be prolonged.Pulseless electrical activity (PEA). Any
elec-trolyte disorder may present as PEA, includinghyperkalaemia.
There are few reports in the liter-ature of successful
resuscitation with PEA as thepresenting rhythm of cardiac arrest.
In each case,prolonged resuscitation was required.24,33,34
Pseudohyperkalaemia
Pseudohyperkalaemia, also known as spuri-ous hyperkalaemia, is
defined as a differencebetween serum and plasma potassium
greater
than 0.4mmol/l.35 It should be suspected inpatients with
hyperviscosity syndromes such aspolycythemia rubra vera,35 in the
absence ofECG changes despite severe hyperkalaemia,7,8
and when sample storage has been prolonged orinadequate.36
Arterial blood sampling is commonpractice in intensive care
settings, but rarely pseu-dohyperkalaemia may occur due to
malpositionof the arterial cannula resulting in a high shearrate
and haemolysis.37 Recognition of pseudo-hyperkalaemia may avoid
potentially hazardousmedical intervention, but the rapid
detection
and treatment of true hyperkalaemia remains ofparamount
importance.
Emergency treatment of hyperkalaemia
There is currently no standardised treatment strat-egy for the
emergency management of hyper-kalaemia in clinical practice largely
because thereis no agreement on a treatment threshold. This
hasresulted in much confusion, over or under treat-ment, late
specialist referral and patient deaths.Despite its clinical
importance, the first systematicreview of the treatment of
hyperkalaemia was pub-
lished only this year.26 To date, management hasbeen recommended
on the basis of the severity ofhyperkalaemia and the effect on the
ECG, but clearguidelines on the basis of the clinical
circumstanceshas been lacking, particularly in the event of
car-diac arrest. Before developing a treatment algo-rithm, several
factors have been considered includ-ing the evidence for the
therapeutic strategies cur-rently available, the influence of the
degree ofrenal impairment on management and the approachto
resuscitation in the event of cardiac arrest.
-
7/29/2019 ALTERACIONES DEL POTASIO 2006.pdf
7/16
16 A.V.M. Alfonzo et al.
Table 3 Summary of therapeutic agents for the management of
hyperkalaemia
Therapy Dose Mechanism Onset (min) Duration (h)
Calcium chloride 10 ml of 10% IV Antagonise 13 0.51Insulin/50%
glucose 10 units in 25 g IV Shift 1530 46Salbutamol 0.5 mg IV 20 mg
Neb Shift 1530 46Sodium bicarbonate 1 mmol/kg IV Shift 1530
SeveralCalcium resonium 1530 g PO/PR Removes Variable 46
IV: intravenous; Neb: nebulised; PO: oral; PR: per rectum; min:
minute.
The drugs available to treat hyperkalaemia havenot changed for
several decades and despite exten-sive investigation of their
individual and combinedefficacy, their remains much variability in
howthese agents are used in clinical practice. In gen-eral, the
choice of agents is influenced by theseverity of hyperkalaemia and
the presence ofECG changes or concurrent metabolic disturbances.In
most instances, more than one agent is oftenrequired for adequate
control and some agents(salbutamol and sodium bicarbonate) are not
suit-able as monotherapy. A brief summary of the impor-tant drugs
used to treat hyperkalaemia is givenbelow and the mechanism of
action, rate of onsetand duration of action of these agents are
shown inTable 3.
Protecting the heart
Calcium chloride. Although there are no clinicalstudies
assessing the efficacy of calcium salts in theemergency management
of hyperkalaemia, there
remains little doubt of their importance in emer-gency
management even in patients with normalserum calcium. Both calcium
salts, calcium chlo-ride and calcium gluconate, antagonise the
car-diac membrane excitability and have been widelyrecommended for
the treatment and prophylaxisof arrhythmias due to hyperkalaemia
when life-threatening ECG changes (absent P waves, wideQRS,
sine-wave pattern) are present2426 or whencardiac arrest occurs.
Some reports also suggestthe use of calcium salts for isolated
peaked Twaves which is an early ECG manifestation
ofhyperkalaemia.16,25,38 This approach seems appro-
priate since the transition period from peaked Twaves to broad
QRS complex is unknown and islikely to be highly variable from
patient to patient.As peaked T waves are a frequently recollected
signof hyperkalaemia, it may also prompt earlier recog-nition and
treatment.
The decision of which calcium salt should beused, chloride or
gluconate, is largely guided bypracticalities such as availability
and local practice.Calcium chloride contains more calcium (6.8
mmolin 10ml) than calcium gluconate (2.2 mmol in 10 ml)
and has greater bioavailability, but is more likelyto cause
tissue injury if extravasation occurs. Insome institutions, calcium
gluconate is the pre-ferred option in a non-arrested patient, but
it isimportant to bear in mind that a higher dose maybe necessary
to block the toxic effects of hyper-kalaemia on the heart.
Efficacy: calcium chloride and calcium gluconatedo not lower
serum potassium.
Cautions: known or suspected digoxin toxicity.Rate of
administration should be slower (over30 min) in patients taking
digoxin as calcium saltsmay contribute to toxicity.38,39
Adverse effects: bradycardia, arrhythmias, tis-sue necrosis if
extravasation occurs.
Shifting of potassium into cells
Insulinglucose therapy. Several studies haveevaluated the
efficacy of insulin with glucosefor the treatment of
hyperkalaemia.4042 Insulinenhances cellular uptake of potassium by
stim-
ulating the sodiumpotassium (NaK) adenosinetriphosphatase (ATP)
pump.38 This effect is inde-pendent of its effect on cellular
glucose uptake.3
Administration of glucose without insulin is not rec-ommended in
non-diabetics as endogenous insulinrelease may be insufficient and
paradoxically couldincrease serum potassium further.43 It is
importantto note that the potassium lowering effect of insulinis
preserved in renal failure, but uraemia attenu-ates the
hypoglycaemic response.38
Efficacy: insulin reduces potassium by 0.651mmol/l within 60 min
of administration.3,16,38,40
Cautions: regular (soluble) insulin should beused. Adverse
effects: hypoglycaemia. This may be
delayed (3060min post-infusion) if less than30 g glucose is
given.38
Sodium bicarbonate. Sodium bicarbonatedecreases the
concentration of H+ in the extra-cellular fluid compartment which
increasesintracellular Na+ via the Na+/H+ exchanger andfacilitates
K+ shift into cells via the NaKATPasepump. However, bicarbonate
does not lower serum
-
7/29/2019 ALTERACIONES DEL POTASIO 2006.pdf
8/16
Potassium disordersclinical spectrum and emergency management
17
potassium in the absence of metabolic acidosis.43
Disappointingly, there is limited evidence for theuse of sodium
bicarbonate in the treatment ofhyperkalaemia.3,41,42,44,45
Efficacy: no study has shown an independentpotassium lowering
effect within 60 min,26 butwhen used in combination with
insulinglucose
or salbutamol, it lowered potassium by0.47 0.31 mmol/l at 30
min.42
Cautions: calcium salts and sodium bicarbonateshould not be
administered simultaneously viathe same route to avoid
precipitation of calciumcarbonate.
Adverse effects: hypernatraemia; pulmonaryoedema due to large
sodium load; tetany inpatients with coexistent hypocalcaemia.
Salbutamol. Beta agonists have been widely stud-ied for the
treatment of hyperkalaemia.4051 Salbu-tamol binds to beta-2
receptors stimulating adeny-
lase cyclase which converts ATP to 35 cyclic adeno-sine
monophospate. This results in stimulation ofthe NaK ATP pump and
intracellular potassiumuptake.38
Efficacy: salbutamol lowers serum potas-sium by 0.871.4 mmol/l
after intravenousadministration46,50 and by 0.530.98 mmol/lafter
administration in the nebulised form.40
The response is dependent on the dose admin-istered as greater
efficacy was reported inpatients receiving 20 mg versus 10 mg of
neb-ulised salbutamol.26 It is important to notethat beta-blockers
may affect the response totreatment and up to 40% of patients with
ESRFdo not respond to salbutamol.3
Cautions: beta-agonists may exacerbate tachy-cardia in patients
with tachyarrhythmias.
Adverse effects: tachycardia, tremor, anxietyand flushing.
Removing potassium from the body
Exchange resins. Cation exchange resins arecross-linked polymers
with negatively chargedstructural units which exchange calcium
(cal-
cium resonium) or sodium (sodium polystyrenesulphonate;
Kayexalate) for potassium across theintestinal wall.
Efficacy: resins do not appear to increase faecalpotassium
excretion above the effect of induc-tion of diarrhoea with
laxatives.52,53 These stud-ies have reported no reduction in serum
potas-sium at 4 h.26,53
Cautions: slow acting, therefore unsuitablefor urgent management
of hyperkalaemia. Co-administration of laxative is recommended.
Adverse effects: constipation, intestinal necro-sis.
Diuretics. The theoretical basis for the use ofdiuretics in the
treatment of hyperkalaemia isto enhance urinary potassium
excretion. However,there are no clinical trials to support their
use inthe treatment of hyperkalaemia.26
Intravenous fluids. Although there is no clinicaltrial to
support fluid replacement,26 it is advisableto administer 0.9%
saline intravenously if there isclinical evidence of volume
depletion with the aimof improving renal perfusion and enhancing
urinarypotassium excretion.Dialysis. Dialysis is the most immediate
and reli-able way of removing potassium from the body.The principle
mechanism of action is the diffu-sion of potassium across the
transmembrane gra-dient. Haemodialysis can remove 2540 mmol/h
ofpotassium54 and is more effective than peritoneal
dialysis. The typical decline in serum potassium is1 mmol/l in
the first 60 min, followed by 1 mmol/lover next 2h.3 The efficacy
of haemodialysis inlowering serum potassium can be improved by
per-forming dialysis with a low potassium concentrationin the
dialysate,55 a high blood flow rate56 or a highdialysate
bicarbonate concentration.57
Influence of degree of renal impairment onmanagement
Hyperkalaemia may occur in the context of acute
(ARF), chronic (CRF) or end-stage renal failure(ESRF). The
aetiology may vary depending on thedegree of renal impairment.
Drugs are the mostcommon cause of hyperkalaemia in ARF and CRF.In
patients with severe CRF (GFR < 30 ml/min) orESRF, additional
factors including dietary potassiumintake become important.
Non-compliance with thehaemodialysis schedule can also result in
lethalhyperkalaemia. Hyperkalaemia has been reportedto be the
indication for emergency dialysis 24% ofthe time in patients on
maintenance haemodialysisin one centre.58
The clinical sequelae of hyperkalaemia may
be influenced by the rate of onset of hyper-kalaemia and the
frequency of its occurrence. InARF, hyperkalaemia often develops
rapidly and isusually poorly tolerated, therefore prompt
aggres-sive treatment is warranted. It has been suggestedthat the
slower onset of hyperkalaemia in CRFis better tolerated and ECG
signs may be absentdespite a serum potassium of 7.07.5
mmol/l.24
A relative tolerance to hyperkalaemia has alsobeen postulated in
patients with ESRF who expe-rience frequent mild hyperkalaemia,12
however
-
7/29/2019 ALTERACIONES DEL POTASIO 2006.pdf
9/16
18 A.V.M. Alfonzo et al.
there remains little evidence to support this the-ory as 35% of
deaths in dialysis patients maybe attributable to hyperkalaemia.59
Therefore, theeffects of hyperkalaemia should not be
underesti-mated in patients with advanced renal impairment.
Most studies investigating the therapeuticeffects of
pharmacological agents for the treat-
ment of hyperkalaemia have been performedin patients with ESRF
as this model provides asignificant cohort of patients with mild
hyper-kalaemia who pass little urine, thereby makinginterpretation
of treatment efficacy much easier.26
The therapeutic options are the same irrespectiveof the nature
and severity of the underlying renaldisease. However in ESRF,
sodium bicarbonate hasbeen found to be less effective,3,26 and
medicalmeasures only provide temporary relief until dial-ysis can
be initiated. Overall, the main differencein approach to treatment
may be the urgency forcorrection of serum potassium of
mild-moderate
severity, but prompt treatment is warranted forsevere
hyperkalaemia irrespective of the degreeof renal impairment.
Interventions in cardiopulmonary arrest
The focus so far has been averting cardiac arrestwith prompt
treatment of hyperkalaemia. However,cardiac arrest may occur if
treatment of knownhyperkalaemia has been sub-optimal or
ineffective.In other cases, hyperkalaemia is discovered onlyafter
the resuscitation is underway. When hyper-
kalaemia is suspected to be the primary precipitantof cardiac
arrest, resuscitation should not be termi-nated until serum
potassium is controlled, by anymeans necessary, unless there are
extenuating cir-cumstances. Hyperkalaemia may also arise duringthe
resuscitation attempt as a result of metabolicchanges and hypoxia
but does not usually requirespecific intervention.39
During CPR, adrenaline (epinephrine) should bethe first drug to
be administered irrespective of thecause of cardiac arrest.
Adrenaline is a powerfulsympathomimetic amine with both alpha- and
beta-adrenergic activity which helps to drive potassium
into cells, thereby lowering serum potassium.24Next, calcium
chloride should be administered toantagonise the toxic effects of
hyperkalaemia.Sodium bicarbonate should be considered in thecontext
of a metabolic acidosis. Insulinglucose isthought to be ineffective
during CPR,39 however itis unlikely to cause harm and should begin
to haveeffect with minutes of return of spontaneous circu-lation.
There is no literature available on the use ofintravenous
salbutamol in this scenario. Optimisingventilation during CPR can
avoid compounding aci-
dosis and further extracellular shift of potassium.This approach
is summarised in Figure 2.
Haemodialysis during resuscitation
In cardiac arrest, dialysis modalities have beenused effectively
for the rewarming of hypother-mic patients, but there is relatively
little experi-
ence in its use for hyperkalaemia. It seems ironicthat the
indication for which dialysis is intendedis rarely implemented
during resuscitation, partic-ularly when medical therapy may be
less effec-tive. The hesitancy to initiate dialysis during CPRis
largely because technique failure is anticipated.The general
perception is that haemodialysis can-not be achieved during CPR as
the extracorporealcircuit will clot due to inadequate blood
pres-sure. However, there is evidence to suggest thatdialysis can
be effective despite reduced circula-tion. With the aid of the
blood pump, a bloodflow rate of up to 150 ml/min can be
achieved
with external chest compressions at a rate of60/min27 and up to
200 ml/min at a rate of80100/min.28
There are several reports of patients treated suc-cessfully with
dialysis during CPR for cardiac arrestsecondary to
hyperkalaemia.13,18,19,29,30,60,61,62 Inmany of these reports,
resuscitation combinedwith dialysis has been successful even after
pro-longed CPR (in excess of 90 min) with no neu-rological
sequelae. The dialysis mode used wasdependent on local availability
and practice,but success has been reported with haemodial-
ysis, veno-venous haemofiltration or
veno-venoushaemodiafiltration,62 and also with
peritonealdialysis.19 This growing series of reports over thelast
two decades suggests that external cardiaccompression can support
adequate blood flow forhaemodialysis. Ultimately, if the blood
clots in thecircuit, it would be reasonable to try again asthere is
little to lose. Haemodialysis is undoubt-edly the most effective
treatment for managinglife-threatening hyperkalaemia.
Post-resuscitation care
If the resuscitation attempt is successful, atten-
tion should turn to maintaining the circulation,performing
further investigations, deciding on thetiming for haemodialysis and
planning after-care.Insulinglucose may be more effective for
persis-tent hyperkalaemia.39 If vascular access for dialysishas not
been achieved during resuscitation, thismay now be possible with
the return of sponta-neous circulation. Femoral access is usually
fast anduncomplicated. Early specialist input will ensurethe
preparation of a dialysis machine to avoid fur-ther delay.
-
7/29/2019 ALTERACIONES DEL POTASIO 2006.pdf
10/16
Potassium disordersclinical spectrum and emergency management
19
Figure 2 Emergency treatment algorithm for hyperkalaemia in
adults.
Development of an emergency treatmentalgorithm
It has been previously noted that there is great vari-ability in
treatment of hyperkalaemia from patientto patient even within the
same centre, withouta clear rationale.63 This is not an isolated
phe-
nomenon and suggests a need for a consistent pro-tocol. The main
objectives in designing such a pro-tocol are to provide a level of
serum potassium atwhich action should be initiated, to prompt
earlyrecording of an ECG to guide management and tooutline a
structured approach depending on theclinical setting. Emergency
treatment is likely to
-
7/29/2019 ALTERACIONES DEL POTASIO 2006.pdf
11/16
20 A.V.M. Alfonzo et al.
be required for patients with moderate to severehyperkalaemia,
therefore the recommended treat-ment threshold of serum potassium
has been set at6.0 mmol/l (Figure 2). The ECG features and
clinicalcondition of the patient then guide immediate clin-ical
decisions. Analogous to acute asthma, we havedefined similar
treatment categories which incor-
porate the severity of hyperkalaemia, as reflectedby level of
serum potassium, ECG features and theclinical setting.
Acute severe hyperkalaemia
Acute severe hyperkalaemia is defined as a raisedserum potassium
in the presence of a normal ECG.As these patients do not show
evidence of cardiactoxicity, calcium chloride is not indicated. In
thesepatients, the intensity of treatment is guided by thelevel and
rate of rise of serum potassium and thelikelihood or
re-establishing good urine output.
Life-threatening hyperkalaemiaLife-threatening hyperkalaemia is
defined as hyper-kalaemia which is sufficiently severe to cause
ECGabnormalities ranging from tented T waves toarrhythmias. The
level of serum potassium causingthese abnormalities is highly
variable, but is likelyto exceed 6.5 mmol/l. Life-saving treatment
shouldbe initiated immediately, even before laboratoryresults are
available, in the presence of the ECGchanges outlined in Figure
2.
Cardiac arrest
Patients may suffer cardiac arrest as the initialpresentation or
following life-threatening hyper-kalaemia. Standard ALS should be
initiated, fol-lowed by the administration of calcium chloride
andshifting agents (Figure 2). Haemodialysis should beconsidered if
hyperkalaemia is resistant to initialmedical therapy.
Principles of treatment algorithm
The treatment of hyperkalaemia in all of the abovesettings is
based on five key principles:
1. Cardiac protection by antagonising the effects
of hyperkalaemia.2. Shifting K+ into cells.3. Removing K+ from
the body.4. Monitoring serum K+ for rebound hyperkalaemia.5.
Prevention of recurrence of hyperkalaemia.
These steps follow a logical sequence and suc-cessful treatment
is also dependent on seekingexpert advice as early as possible. It
is important tore-assess the effects of initial treatment by
mon-itoring the serum potassium. Rebound is a well-recognised
phenomenon, even after haemodialysis,
with 70% of potassium reduction being abolished at6 h after
dialysis.3
Prevention of hyperkalaemia
A treatment strategy is incomplete unless pre-ventative measures
are taken to avoid develop-
ment or recurrence of hyperkalaemia. Patientswith advanced renal
failure are most susceptibleto hyperkalaemia and care should be
taken withdrug prescribing and diet in this patient group.Patients
with other chronic illnesses including pro-teinuric kidney
diseases, cardiac failure, diabetesmellitus and portal hypertension
are also suscep-tible to hyperkalaemia. This risk may be
com-pounded by the presence of even mild renal fail-ure in
association with other co-morbidity. How-ever, medicines which may
increase serum potas-sium levels such as ACE inhibitors,
angiotensin II
antagonists, NSAIDs, and potassium sparing diuret-ics,
especially if combined, are the most commonpreventable cause of
hyperkalaemia. Severe hyper-kalaemia was reported in 2% of patients
in theRALES study despite multiple exclusion criteria.64
Hyperkalaemia may also occur in the setting ofacute illness in
patients taking these agents, espe-cially if there is a degree of
volume depletion.
For primary prevention, patients at risk of hyper-kalaemia
should have close monitoring of serumbiochemistry and should
discontinue drugs knownto potentiate serum potassium during acute
illness.Patients with severe renal failure, acute or chronic,
should receive specialist attention as early as pos-sible. For
secondary prevention after initial treat-ment of hyperkalaemia, it
is important to monitorelectrolyte levels and to prevent recurrence
of theabnormality by removing any precipitating factors(e.g.
drugs).
Hypokalaemia
Low serum potassium is reported to be the mostcommon electrolyte
abnormality in hospitalised
patients.1 There are many causes of hypokalaemiaas shown in
Table 4, but drugs and gastrointestinaldisease account for a
significant proportion. Potas-sium concentration in the blood is
also affectedby the metabolic status of the patient. In thepresence
of a metabolic alkalosis, potassium shiftsinto cells. Hypokalaemia
can also contribute to themaintenance of a metabolic alkalosis by
enhanc-ing bicarbonate absorption and increasing chlorideexcretion
in the kidney.1 Hypokalaemia is definedas a serum potassium 3.5
mmol/l.1,2,65,66 It may
-
7/29/2019 ALTERACIONES DEL POTASIO 2006.pdf
12/16
Potassium disordersclinical spectrum and emergency management
21
Table 4 Causes of hypokalaemia
Increase potassium lossDrugsdiuretics, laxative abuse,
liquorice, steroidsGI lossesdiarrhoea, vomiting, ileostomy,
intestinal fistula, villous adenomaRenalrenal tubular disorders,
Bartters syndrome, Liddles syndrome, Gitelmans syndrome,
nephrogenic
diabetes insipidousEndocrinehyperaldosteronism, Cushings
syndrome, Conns syndrome
Dialysishaemodialysis on low potassium dialysate, peritoneal
dialysisTranscellular shift
Insulin/glucose therapyBeta-adrenergic stimulatione.g.
salbutamolAlkalosisHypokalaemic periodic paralysis
Decreased potassium intakePoor dietary intake (less than 1
g/day)
Magnesium depletion (increases renal potassium loss)Poor dietary
intakeIncreased magnesium loss
be classified as mild (K 3.03.5 mmol/l), moderate(K 2.53.0
mmol/l) or severe (K < 2.5 mmol/l) andsymptoms are more likely
with increasing severity.
Clinical spectrum of hypokalaemia
Symptoms
Patients with mild hypokalaemia usually have nosymptoms. As
serum potassium level falls fur-ther, the nerves and muscles are
predominantly
affected causing fatigue, weakness, leg cramps,and constipation.
In severe cases, rhabdomyoly-sis, ascending paralysis and
respiratory difficultiesmay occur. The probability of symptoms
appears tocorrelate with the presence of pre-existing heartdisease
(ischaemia, heart failure, left ventricu-lar hypertrophy), and the
rapidity of the onset ofhypokalaemia.6567
ECG abnormalities
There are usually no ECG changes in patients withmild
hypokalaemia, but these may become evidentin moderate to severe
hypokalaemia including the
presence of U waves, T wave flattening, or ST seg-ment
changes.2
Arrhythmias associated with hypokalaemia
Severe hypokalaemia predisposes to arrhythmiasand cardiac
arrest. In patients treated with digoxin,hypokalaemia of any
severity can increase theincidence of arrhythmias.65 Patients with
estab-lished digoxin toxicity are particularly at risk.
Thefollowing is a review of the common arrhyth-mias associated with
hypokalaemia and the effect
of hypokalaemia in patients maintained on anti-arrhythmic
agents.Ventricular tachycardia/fibrillation. Hypokalae-mia can
predispose to ventricular tachycardia orventricular fibrillation.11
This risk is particularlyhigh following acute myocardial infarction
andmaintaining the serum potassium above 3.9 mmol/lmay reduce the
risk of early VF.66 The arrhyth-mia may not respond to electrical
or chemical car-dioversion until the serum potassium is
corrected.
Long QT syndrome and torsade de pointes. Thelong QT syndrome,
which may be inherited oracquired, is caused by malfunction of the
ion chan-nels responsible for ventricular repolarisation.68
Potassium and/or magnesium depletion are themain metabolic
disorders associated with channelmalfunction and hence predispose
to arrhythmias.The characteristic arrhythmia seen is torsade
depointes which may present as syncope or cardiacarrest. This is
recognised as a variant of ventricu-lar tachycardia in which the
QRS complexes changeamplitude around the isoelectric line and is
fre-quently preceded by pauses.68 The mainstay of
treatment is the correction of hypokalaemia andadministration of
magnesium sulphate.Patients taking anti-arrhythmic drugs.
Hypokalaemia may also interfere with the benefi-cial effects of
anti-arrhythmic drugs rendering thepatients susceptible to a
recurrence of the under-lying arrhythmia.66 In addition,
hypokalaemiacan compound the effects of Class III anti-arrhythmic
agents such as sotalol predisposing toarrhythmias.66,68 Indeed,
torsade de pointes hasbeen reported in 24% of patients treated
with
-
7/29/2019 ALTERACIONES DEL POTASIO 2006.pdf
13/16
22 A.V.M. Alfonzo et al.
sotalol and this risk is increased in older patientsand in the
presence of renal impairment.68
Although this risk is also dose-dependent, thereare reported
cases of torsade de pointes inducedby low doses of sotalol.69
Treatment of hypokalaemia
The treatment approach depends on the severityof hypokalaemia
and the presence of symptomsand ECG abnormalities. As a guide to
the deficit intotal body potassium, serum potassium decreasesby 0.3
mmol/l on average for every 100 mmol reduc-tion in total body
potassium stores, but this isvariable depending on body mass.1,65
Hence, thedeficit can be considerable in moderateseverehypokalaemia
and care should be taken duringreplacement. The administration of
potassium, par-ticularly by the intravenous route is not
without
risk. Gradual replacement of potassium is safer andavoids
excessive replacement.Many patients who are potassium deficient
are
also deficient in magnesium. Magnesium is impor-tant for
potassium uptake and for the maintenanceof intracellular potassium
levels, particularly in themyocardium. Combined deficiency may
potentiatethe risk of cardiac arrhythmias. Repletion of magne-sium
stores will facilitate more rapid correction ofhypokalaemia and is
recommended in severe casesof hypokalaemia.66,70
Developing a treatment algorithm forhypokalaemia
A recent report has highlighted the inadequacyof treating this
common medical problem.71 Thisreport assessing treatment adequacy
showed thathypokalaemia was found in 2.6% of hospitalisationsover a
one year period with inadequate manage-ment of hypokalaemia in 24%
of these cases. Theseinadequacies included failure to measure
serumpotassium subsequently in 6.4% of patients and fail-ure to
correct hypokalaemia in 30% of patients priorto discharge. The
mortality of the hypokalaemic
population was 10-fold higher than the generalhospitalised
population. Hence, it is important todetect, monitor and treat
hypokalaemia appropri-ately.
The main considerations in designing an emer-gency treatment
algorithm for hypokalaemia areto establish the level of serum
potassium whereintravenous replacement is indicated, the rate
ofpotassium replacement according to the clinicalsetting and the
need for co-administration of mag-nesium. Stable patients with mild
hypokalaemia (K
3.03.5 mmol/l) are not included in the treatmentalgorithm as
oral potassium replacement is usu-ally sufficient. Expert help
should be considered forpatients with hypokalaemia of any severity
whichis associated with arrhythmias or cardiac arrest.Continuous
ECG monitoring is essential during IVadministration and the dose
should be titrated after
repeated sampling of serum potassium levels. Theemergency
management of hypokalaemia is sum-marised in Figure 3. Treatment is
guided by thedegree of hypokalaemia and the clinical setting.
Patients with no symptoms
In the absence of digoxin toxicity or severe heartdisease,
potassium should be gradually replaced ata rate of 10 mmol/h in
asymptomatic patients. Mag-nesium replacement is required only if
found to bemagnesium deficient.
Life-threatening arrhythmias
In an emergency such as an arrhythmia, intra-venous potassium is
required, but the rate of cor-rection of serum potassium causes
uncertainty.The maximum recommended intravenous dose ofpotassium is
20 mmol/h, but more rapid adminis-tration (initial infusion of 2
mmol/min for 10 min,followed by 10 mmol over 510 min) is
indicatedfor unstable arrhythmias when cardiac arrest isimminent.2
Rapid bolus injection of potassiumshould be avoided in all
circumstances as thismay precipitate cardiac arrest. Magnesium
shouldbe administrated early after initiating potassium
replacement, even before the serum magnesiumlevel is known.
Cardiac arrest
Cardiac arrest may occur in patients known tobe hypokalaemic.
Alternatively, hypokalaemia mayonly be discovered after
resuscitation is underway.Although the metabolic status after
cardiac arrestusually favours an increase in serum potassium,total
body potassium remains low. Prompt correc-tion of hypokalaemia may
not only render defibrilla-tion more successful, but may reduce the
incidenceof further arrhythmias in the post-arrest period as
the metabolic status of the patient improves andpotassium shifts
back into cells.
Prevention of hypokalaemia
Hypokalaemia is frequently iatrogenic and hencepotentially
avoidable. For primary prevention,electrolytes should be monitored
in patients at risk.In the general population, this includes
patientstreated with diuretics and those with high
gastro-intestinal losses. For secondary prevention, it
-
7/29/2019 ALTERACIONES DEL POTASIO 2006.pdf
14/16
Potassium disordersclinical spectrum and emergency management
23
Figure 3 Emergency treatment algorithm for hypokalaemia in
adults.
is important to monitor serum potassium afterinitial treatment
and to prevent recurrence ofhypokalaemia by removing any
precipitating fac-tors.
Hypokalaemia may also occur in patients withrenal failure
requiring renal replacement ther-apy. Non-renal specialists may be
unaware of thedegree of potassium flux which occurs with
differ-
ent dialysis modalities. Hypokalaemia is a frequentoccurrence in
patients receiving peritoneal dialy-sis and potassium supplements
are often required.In those receiving haemodialysis, hypokalaemia
ismost likely toward the end or immediately after asession.
Patients most at risk are those with a lowserum potassium before
beginning a dialysis ses-sion, particularly if dialysed against an
inappropri-
-
7/29/2019 ALTERACIONES DEL POTASIO 2006.pdf
15/16
24 A.V.M. Alfonzo et al.
ately low potassium dialysate. Therefore, patientswith advanced
renal failure are also potentially sus-ceptible to hypokalaemia and
it is important to con-sider measures to prevent hypokalaemia in
patientsat all levels of renal function.
SummaryPotassium disorders may have life-threatening
con-sequences. It is important to recognise that bothhyperkalaemia
and hypokalaemia are potentiallyavoidable complications of commonly
prescribeddrugs. The clinician should be aware that both maypresent
with a range of ECG changes, virtually anyarrhythmia or cardiac
arrest. Treatment algorithmsprovide a stratified approach based on
biochemical,clinical and pharmacokinetic criteria and may
assistclinicians in the immediate care of these commonmedical
emergencies.
Conflict of interest
The authors have no conflict of interest in relationto this
paper.
Acknowledgement
The authors wish to thank Dr Keith Simpson, direc-tor of the
Scottish Renal Registry Group, for his
valuable contributions to the treatment algorithms.
References
1. Rastergar A, Soleimani M. Hypokalaemia and
hyperkalaemia.Postgrad Med J 2001;77:75964.
2. Guidelines 2000 for cardiopulmonary resuscitation and
emer-gency cardiovascular care: International Consensus on
Sci-ence. Part 8: Advanced Challenges in resuscitation: Section1:
Life-threatening electrolyte abnormalities.
Circulation2000;102:21722.
3. Ahmed J, Weisberg LS. Hyperkalaemia in dialysis
patients.Semin Dial 2001;14:34856.
4. Tran HA. Extreme hyperkalaemia. South Med J2005;98:72932.
5. Fisch C. Relation of electrolyte disturbances to
cardiacarrhythmia. Circulation 1973;47:40819.
6. Aslam S, Freidman EA, Ifudu O. Electrocardiography
isunreliable in detecting potentially lethal hyperkalaemiain
haemodialysis patients. Nephrol Dial Transplant2002;17:163942.
7. Szerlip HM, Weiss J, Singer I. Profound hyperkalaemia
with-out electrocardiographic manifestations. Am J Kidney
Dis1986;7:4615.
8. Bandyopadhyay S, Banerjee S. Severe hyperkalaemia withnormal
electrocardiogram. Int J Clin Pract 2001;55:4867.
9. Moulik PK, Nethaji C, Khaleeli AA. Misleading
electrocardio-graphic results in patient with hyperkalaemia and
diabeticketoacidosis. Br Med J 2002;325:13467.
10. Ettinger PO, Regan TS, Olderwurtel HA. Hyperkalaemia,
car-diac conduction, and the electrocardiogram: overview. AmHeart J
1974;88:36071.
11. Slovis C, Jenkins R. Conditions not primarily affecting
theheart. Br Med J 2002;324:13204.
12. Frohnert PP, Giuliani ER, Friedberg M, Johnson WJ,
Tauxe WN. Statistical investigation of correlations betweenserum
potassium levels and electrocardiographic findings inpatients on
intermittent haemodialysis therapy. Circulation1970;41:66776.
13. Costa P, Visetti E, Canavese C. Double
simultaneoushaemodialysis during prolonged cardiopulmonary
resuscita-tion for hyperkalaemic cardiopulmonary arrest. Case
report.Minerva Anaestesiol 1994;60:1434.
14. Walter RB, Bachli EB. Near fatal arrhythmia caused by
hyper-kalaemia. Heart 2002;88:578.
15. Kim NH, Oh SK, Jeong JW. Hyperkalaemia induced
completeatrioventricular block with a narrow QRS complex.
Heart2005;91:e5.
16. Emmett M. Non-dialytic treatment of acute hyperkalaemiain
the dialysis patient. Semin Dial 2000;13:27980.
17. Ortega-Carniecer J, Benezet J, Benezet-Mazuecos J.
Hyper-kalaemia causing loss of atrial capture and extremelywide QRS
complex during DDD pacing. Resuscitation2004;62:11920.
18. Torrecilla C, de la Serna JL. Hyperkalaemic cardiac
arrest,prolonged heart massage and simultaneous haemodialysis.Inten
Care Med 1989;15:3256.
19. Jackson MA, Lodwick R, Hutchison SG. Lesson of theweek:
hyperkalaemic cardiopulmonary arrest successfullytreated with
peritoneal dialysis. Br Med J 1996;312:128990.
20. Barold SS. Loss of atrial capture during DDD pacing: whatis
the mechanism? Pacing Clin Electrophysiol 1998;21:19889.
21. Luzza F, Carerj S, Oreto G. An unusual hyperkalaemia
induced block. Heart 2001;86:686.22. Tomcsanyi J. J. Extremely
wide QRS complex with VVI pac-
ing. Pacing Clin Electrophysiol 2002;25:11289.23. Kistler PM,
Mond HG, Vohra JK. Pacemaker ventricular block.
Pacing Clin Electrophysiol 2003;26:19979.24. Quick G, Bastani B.
Prolonged asystolic hyperkalaemic car-
diac arrest with no neurological sequelae. Ann Emerg
Med1994;24:30511.
25. An advisory statement on conditions which may require
mod-ifications in resuscitation procedures or techniques. Pre-pared
by Members of the International Liaison Committeeon Resuscitation.
Special resuscitation situations. Resuscita-tion 1997;34:12949.
26. Mahoney BA, Smith WAD, Lo DS. Emergency interven-tion for
hyperkalaemia. Cochrane Database SystemRev 2005;2(Issue). Art. No.:
CD003235.pub2. DOI:10.1002/14651858. CD003235. pub2.
27. Lin JL, Huang CC. Successful initiation of
haemodialysisduring cardiopulmonary resuscitation due to lethal
hyper-kalaemia. Crit Care Med 1990;18:423.
28. Strivens E, Siddiqi A, Fluck R, Hutton A, Bell D.
Hyper-kalaemic cardiac arrest: may occur secondary to mis-use of
diuretics and potassium supplements. Br Med J1996;313:693.
29. Kao KC, Huang CC, Tsai YH, et al. Hyperkalaemic
cardiopul-monary arrest successfully reversed by haemodialysis
dur-ing cardiopulmonary resuscitation: case report. ChanggengYiXue
Za Zhi 2000;23:5559.
http://dx.doi.org/10.1002/14651858http://dx.doi.org/10.1002/14651858
-
7/29/2019 ALTERACIONES DEL POTASIO 2006.pdf
16/16
Potassium disordersclinical spectrum and emergency management
25
30. Lin JL, Lim PS, Leu ML, et al. Outcomes of severe
hyper-kalaemia in cardiopulmonary resuscitation with
concomitanthaemodialysis. Intensive Care Med 1994;20:28790.
31. Virdi VS, Bharti B, Poddar B, Saus S, Parmar VR.
Ventricu-lar tachycardia in congenital adrenal hyperplasia.
AnaesthIntensive Care 2002;30:3802.
32. Grimm W, Alter P, Maisch B. Cardiac arrest due to
severehyperkalaemia. Herz 2004;29:353.
33. Lawton JM. Hyperkalaemic electromechanical dissociation.
Wis Med J 1990;89:45961.34. Pang P, Look RB, Brown DFM. Wide
complex rhythm and car-
diac arrest. J Emerg Med 2004;26:197200.35. The MM, Zaman MJS,
Brooks AP, Li Voon Chong JSW. When
is a high potassium not a high potassium? J Roy Soc
Med2003;96:3545.
36. Trull AK, Jackson C, Walsh S, et al. The perennial
problemwith potassium. Ann Clin Biochem 2004;41:4752.
37. Mehta V, Ahmed Z. Apparent hyperkalaemia from blood sam-pled
from an arterial cannula. Br J Anaesth 2004;93:4568.
38. Ahee PP, Crowe AV. The management of hyperkalaemiain the
emergency department. J Accid Emerg Med2000;17:18891.
39. Kloeck W, Cummins RO, Chamberlain D, et al.
Specialresuscitation situations: an advisory statement from the
international liaison committee on resuscitation.
Circulation1997;95:2196210.
40. Allon M, Copkney C. Albuterol and insulin for treatmentof
hyperkalaemia in haemodialysis patients. Kidney
Int1990;38:86972.
41. Allon M, Shanklin N. Effect of bicarbonate administrationon
plasma potassium in dialysis patients: interactions withinsulin and
albuterol. Am J Kidney Dis 1996;28:50814.
42. Ngugi NN, McLigeiyo SO, Kayima JK. Treatment of
hyper-kalaemia by altering the transcellular gradient in
patientswith renal failure: effect of various therapeutic
approaches.East Afr Med J 1997;74:5039.
43. Kamel SK, Wei C. Controversial issues in the treatment
ofhyperkalaemia. Nephrol Dial Transplant 2003;18:22158.
44. Blumberg A, Weidman P, Shaw S, Gnadinger M. Effect of
various therapeutic approaches on plasma potassium andmajor
regulating factors in terminal renal failure. Am J
Med1988;85:50712.
45. Kim HJ. Combined effect of bicarbonate and insulin
withglucose in acute therapy of hyperkalaemia in end-stage
renaldisease patients. Nephron 1996;72:47682.
46. Lens XM, Montoliu J, Cases A, et al. Treatment of
hyper-kalaemia in renal failure: salbutamol v insulin. Nephrol
DialTransplant 1989;4:22832.
47. Montoliu J, Almirall J, Ponz E, et al. Treatment of
hyper-kalaemia in renal failure with salbutamol inhalation. J
InternMed 1990;228:357.
48. Liou HH, Chiang SS, Wu SC, et al. Hypokalaemic effects
ofintravenous infusion or nebulisation of salbutamol in
patientswith chronic renal failure: comparative study. Am J
KidneyDis 1994;23:26671.
49. MandelbergA, Krupnik Z, Houri S, et al. Salbutamol
metered-dose inhaler with spacer for hyperkalaemia: how fast?
Howsafe? Chest 1999;115:61722.
50. McClure RJ, Prasad VK, Brocklebank JT. Treatment of
hyper-kalaemia using intravenous and nebulised salbutamol. ArchDis
Child 1994;70:1268.
51. Pancu D, LaFlamme M, Evans E, Reed J. Levalbuterol is
aseffective as racemic albuterol in lowering serum potassium.J
Emerg Med 2003;25:136.
52. Emmett M, Hootkins RE, Fine KD. Effect of three laxativesand
a cation exchange resin on faecal sodium and potassiumexcretion.
Gastroenterology 1995;108:75260.
53. Gruy-Kapral C, Emmett M, Santa Ana CA, Porter JL, Ford-tran
JS, Fine K. Effect of single dose resin-cathartic ther-apy on serum
potassium concentration in patients withend-stage renal failure. J
Am Soc Nephrol 1998;10:192430.
54. Defronzo PA, Bia M. Clinical disorders of hyperkalaemia.
Ann
Rev Med 1982;33:5212.55. Zehnder C, Gutzwiller JP, Huber A,
Schindler C, Schneditz
D. Low-potassium and glucose-free dialysis maintains ureabut
enhances potassium removal. Nephrol Dial
Transplant2001;16:7884.
56. Gutzwiller JP, Schneditz D, Huber AR, Schindler C, Garbani
E,Zehnder CE. Increasing blood flow increases kt/V (urea)
andpotassium removal but fails to improve phosphate removal.Clin
Nephrol 2003;59:1306.
57. Heguilen RM, Sciurano C, Bellusci AD, et al. The
fasterpotassium-lowering effect of high dialysate bicarbonate
con-centrations in chronic haemodialysis patients. Nephrol
DialTransplant 2005;20:5917.
58. Sacchetti A, Stuccio N, Panebianco P, Torres M.
Haemodialy-sis for treatment of renal failure emergencies. Am J
Emerg
Med 1999;17:3057.59. Morduchowicz G, Winkler J, Drazne E, et al.
Causes of death
in patients with end-stage renal disease treated by dialysisin a
centre in Israel. Isr J Med Sci 1992;28:7769.
60. Gomez-Arnau J, Criado A, Martinez MV, et al.
Hyperkalaemiccardiopulmonary arrest: prolonged heart massage and
simul-taneous haemodialysis. Crit Care Med 1981;9:5567.
61. Josephs W, Lenga P, Odenthal HJ, et al. Rate of successand
prognosis of cardiopulmonary resuscitation in patientson
maintenance haemodialysis. Intensiv und
Notfallmedizin1990;27:2159.
62. Schummer WJ, Schummer C. Hyperkalaemic cardiopul-monary
arrest: the method chosen depends on the localcircumstances. Crit
Care Med 2002;30:16745.
63. Acker C, Johnson JP, Palevsky PM, Greenberg A. Hyper-
kalaemia in hospitalised patients: causes, adequacy of
treat-ment, and results of an attempt to improve physician
com-pliance with published therapy guidelines. Arch Intern
Med1998;158:91724.
64. The RALES investigators, Effectiveness of
spironolactoneadded to an angiotensin-converting enzyme inhibitor
and aloop diuretic for severe chronic congestive heart failure. AmJ
Cardiol 1996;78:9027.
65. Gennari FJ. Hypokalaemia. New Eng J Med 1998;339:4518.66.
Cohn JN, Kowey PR, Whelton PK, et al. New guidelines for
potassium replacement in clinical practice. Arch Intern
Med2000;160:242936.
67. Schulman M, Nairns RG. Hypokalaemia and
cardiovasculardisease. Am J Cardiol 1990;65:4E9E.
68. Viskin S. Long QT syndromes and torsade de pointes.
Lancet1999;354:162533.
69. Tan HH, Hsu LF, Kam RM, Chua T, Teo WS. A case series
ofsotalol-induced torsade de pointes in patients with
atrialfibrillationa tale with a twist. Ann Acad Med
Singapore2003;32:4037.
70. Loughrey CM. Serum magnesium must also be known in pro-found
hypokalaemia. Br Med J 2002;324:103940.
71. Paltiel O, Salakhov E, Ronen I. Management of
severehypokalaemia in hospitalised patients. Arch Intern
Med2001;161:108995.