Embed Size (px)
Citation preview

Presenter: Dr Khaleel Moderator :Dr Arpitha
Date :3/6/14




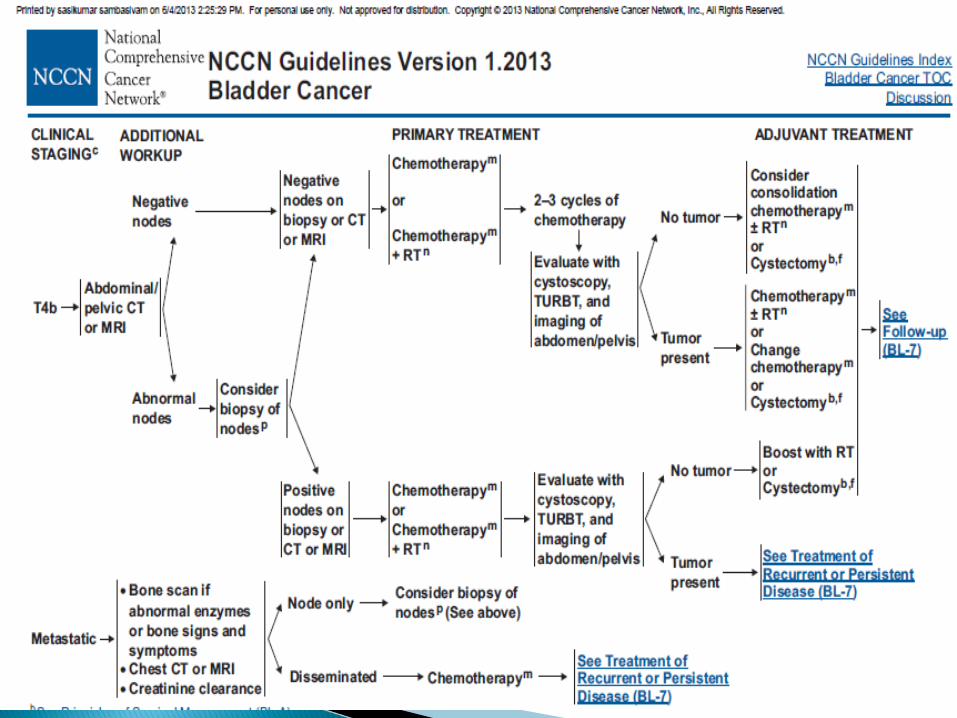

Non–muscle-invading tumors are managed by TURBT alone in the case of low-grade lesions and together with intravesicular bacille Calmette-Guérin (BCG) therapy for high-grade lamina propria invasion or CIS.
Over a span of 10 years, as many as 50% of the latter group will progress to muscle invasion.

• Intravesical therapy involves the instillation of high local concentrations of a therapeutic agent into the bladder, potentially destroying viable tumors cells and preventing implantation.
• A live attenuated form of Mycobacterium bovis, is currently the most effective and most commonly used intravesical agent for the treatment of non– muscle-invasive TCC of the bladder.
• BCG is typically instilled into the bladder weekly for 6 weeks.
• The role of maintenance BCG for longer than 6 weeks remains controversial.
• Triggers a variety of local immune responses and has been shown to be effective in reducing rates of disease progression, decreasing rates of recurrence and the need for subsequent cystectomy, and improving rates of survival.

Toxicities of intravesical therapy include symptoms of bladder irritation (dysuria and frequency).
To minimize the risk of systemic infection, intravesical therapy should not be given to patients with traumatic catheterization, active cystitis, or persistent gross hematuria.
Those treated with BCG had significantly fewer recurrences at 12 months
Nonetheless, 50% of patients with T1/CIS will experience muscle invading cancer at 10 years. Progression rates to muscle invasion among patients who respond to BCG are 1% at 1 year, 5% at 3 years, and 15% at 5 years
In the six published RCTs in which TURBT plus BCG was compared with TURBT alone, recurrence rates ranged from 20% to 42% with intravesical therapy versus 42% to 100% without it.
Other Agents--mitomycin, doxorubicin, epirubicin, valrubicin, thiotepa, gemcitabine, interferon, and docetaxel. None has proved consistently superior to BCG.

Role of Irradiation in High-Risk Superficial Bladder Cancer:
• Dutch South Eastern Bladder Cancer Group :– 121 patients with T1G3 cancers.– 119 EBRT with 50 Gy/25 fractions was one treatment
option, and 17 patients received this. Though the numbers are limited, the treatment appeared to be as effective as intravesical BCG or mitomycin.
• University of Rotterdam with interstitial implants– In this selective but prospective series, patients with
single T1 tumors of less than 5 cm in diameter underwent TURBT and subsequent local irradiation of the tumor area in the bladder wall by an interstitial radium implant.
– The definitive local control rate was 82% and the 10-year OS was 76%.

• 20% to 25%• The most appropriate treatment algorithm for
muscle-invading disease remains controversial.• Although radical cystectomy and urinary
diversion has been• the mainstay for treatment for decades, organ-
preserving regimens using predominantly multiple-modality therapy, consisting of TURBT followed by irradiation with concurrent chemotherapy, are emerging as viable proven alternatives in a subset of patients

Radical Cystectomy• Surgical removal of the bladder, adjacent organs,
and regional lymph nodes• In men, the bladder, prostate, seminal vesicles,
proximal vas deferens, and proximal urethra, with a margin of adipose tissue and peritoneum, are resected en bloc.
• In women, the procedure involves an anterior pelvic exenteration to remove the bladder, urethra, uterus, fallopian tubes, ovaries, anterior vaginal wall, and surrounding fascia en bloc.
• The extent of pelvic lymph node dissection is an important predictor of outcome, – extended template dissection --to include presacral and
common iliac lymph nodes to the aortic bifurcation and often more proximal to the origin of the inferior mesenteric artery, in addition to pelvic lymph nodes distal to the common iliac bifurcation.

Incontinent Urinary Tract Reconstruction: Ileal conduit-Urine drains directly from the
ureters through a segment of ileum to the skin surface, where it is collected by an external collection appliance.
Continent Urinary Tract Reconstruction.• Continent urinary reservoir made of bowel,
which drains to a stoma that can be catheterized– The Kock pouch(Cutaneous Urinary Reservoir)
• Creation of an orthotopic neobladder, in which a newly formed urinary reservoir made out of bowel is anastomosed to the urethra– The Mainz pouch(ileocecal)– The Hautmann pouch(W-shaped ileoneobladder)– Risk of urethral recurrence later on.

• University of South California experience N=633 [pT2-T4a]
• Actuarial 5 year OS at
5 years :48% and at 10years : 32%
Stein JP et al. J ClinOncol 2001;
19:666-675.
• MSKCC experience• N=184 [pT2-T4]• 5 year OS:36%Dalbagni G et al.JUrol 2001;
165:1111-1116.

• Preoperative Radiation Therapy– Danish National Bladder Cancer Group, DAVECA
protocol 8201, 1991– 183 pts, T2–T4a,RCT, Preop RT-Cystectomy Vs
Radical RT (Salvage cystectomy if residual)• A trend for a higher survival rate following
combined treatment with preoperative irradiation and cystectomy compared to radical irradiation followed by salvage cystectomy was observed
• There was no difference in surgical complications between planned and salvage
• T-stage, response to radiotherapy and frequency of LN metastases were found to be of prognostic importance

• Postoperative Radiation Therapy• Postoperative radiation therapy has been
evaluated in only one randomized study. • The National Cancer Institute of Egypt :– 236 patients with T3 to T4 tumors (68% were SCCs)
who received postoperative irradiation (using three daily fractions of 1.25 Gy each, with 3 hours between fractions, up to a total dose of 37.5 Gy in 12 days [75 patients]; or conventional fractionation for a total dose of 50 Gy over 5 weeks [78 patients]).
– The 5-year rates of disease-free survival (DFS) (44% to 49% vs. 25%) and
– local control (87% to 93% vs. 50%) were improved and the incidence of pelvic recurrence was significantly reduced in the groups receiving postoperative radiation.


Ideal candidate for bladder preservation– Criteria:◦ Primary T2 to T3a tumors that are unifocal◦ Tumor size less than 5 cm in maximum diameter◦ Tumor not associated with extensive CIS◦ No presence of ureteral obstruction or tumor-
associated hydronephrosis◦ Good capacity of the bladder◦ Visibly complete TURBT◦ Adequate renal function to allow cisplatin to be given
concurrently with irradiation

• Conservative Surgery• Partial Cystectomy:• Careful patient selection– the lesion is solitary and is located in a region of the
bladder that allows for complete excision with a 2-cm tumor-free margin, such as the bladder dome.
– Contradictions:• association with CIS in other sites of the bladder,• prostatic urethral involvement, • prior recurrent bladder or upper tract tumors, and • bladder neck or trigone tumors in which ureteral
reimplantation would be required to achieve an adequate margin
• Only 6 to 19% of pts qualify• Recurrence rates range 38% to 78%; half of the
recurrences appear in the first year and two thirds by 2 years

TURBT for invasive ca◦ Clinical complete response rates assessed
cystoscopically with repeat biopsy 3 weeks after initial TURBT for T2 and T3 cancers overall are in the 10% to 20% range
◦ Although potentially effective in a small proportion of favorable T2 tumors, TURBT is usually not sufficient as monotherapy in muscle-invading bladder cancer

• Radical EBRT:• Dose varied from 50 to 65 Gy, with 1.8 Gy to
2 Gy per fraction• Response was evaluated by cystoscopic
examination and biopsy 3 to 6 months after completion of RT
• Pts-Residual tumor and no known metastatic disease underwent salvage surgery
• The 5-year local control rate ranged from 31% to 50% for the entire patient population and from 49% to 79% for the subgroup of patients with a complete response.

Factors reported as having a significant favorable effect on local control with RT included:
• Early clinical stage (T2 and T3a)• Absence of ureteral obstruction• Complete response• Visibly complete TURBT• Absence of coexisting CIS• Small tumor size (<5 cm maximum diameter)• Solitary tumors
Tumor configuration (papillary vs. sessile) Hemoglobin level (>10 mg/dL)

• EBRT + Interstitial Brachytherapy:– Appropriate candidates --are those with a solitary TCC
with a diameter of less than 5 cm or stage T1 disease (with high grade) to T3a disease (muscle invasion but no extension through the wall).
– 5 yr- local control rates for selected patients treated with brachytherapy in combination with EBRT do appear to be excellent, varying between 70% and 90% with correspondingly high rates of bladder preservation.
– In selected patients, survival rates appear to be similar to those of cystectomy
– The most serious acute morbidity is fistula with wound leakage. This is most strongly predicted by tumor size, active length of radioactive sources, and use of a partial cystectomy.
(Table)

• Combined-Modality Therapy:• Chemotherapy and Conservative Surgery• CT /TURBT // Partial cystectomy– Criteria• Complete or major response to chemotherapy• Solitary lesion in the dome or the anterior wall of the
bladder• No history of prior invasive bladder cancer• No CIS• Good bladder capacity
• Although 5-year survival rate is high at close to 50%, bladder preservation is possible in less than half of these patients.

• Neoadjuvant Chemotherapy before Definitive Local Therapy:
• Most of the RCTs used single drug– No survival advantage compared to other arm
• Some studies which used cisplatin based multidrug regime – no consistency in results.
• A meta-analysis that included data from 3005 patients enrolled in 11 randomized trials demonstrated a 5% absolute 5-year OS advantage (50% vs. 45%; p = .003) for neoadjuvant cisplatin-based combination chemotherapy compared with local therapy alone.
(Table)

Adjuvant Chemotherapy after Definitive Local Therapy◦ Adjuvant chemotherapy allows for pathologic staging
and avoids delay in potentially curative local therapy. ◦ No randomized trials have compared neoadjuvant to
adjuvant CT in patients undergoing definitive local therapy
◦ A meta-analysis including 491 patients from six trials suggested a 25% relative reduction in the risk of death (p = .019) for patients receiving cisplatin-based combination adjuvant CT; however, the power of this meta-analysis was limited.
◦ A RCT phase III trial from the Spanish Oncology Genitourinary Group (99/01) comparing four cycles of adjuvant paclitaxel/gemcitabine/cisplatin to observation in patients with resected high-risk (pT3 to T4 or pN+) bladder cancer was prematurely closed due to poor accrual; however, preliminary results suggest improved 5-year OS (60% vs. 31%; p = .0009)

• Trimodality Therapy Using Limited Resection, Chemotherapy, and Radiation in Bladder Preservation:
• The rationale– Certain cytotoxic agents, in particular, cisplatin and 5-
fluorouracil (5-FU), are capable of sensitizing tumor tissue to irradiation, therefore increasing cell kill in a synergistic fashion
– Patients with muscle-invading TCC harbor occult metastases in approximately 50% of cases, which makes a case for the addition of systemic chemotherapy in an attempt to control occult distant disease.
• Many phase II trials have combined chemotherapy and RT in different sequences in patients with invasive bladder cancer.
• Although a variety of different drugs and radiation doses have been used, it is apparent that the highest clinical complete response rate (T0) was achieved in patients who received concurrent chemotherapy and RT compared with sequential regimens


• The MGH Experience:– T2 to T4aNXM0, 348 pts– Concurrent cisplatin-based CT and RT after maximal TURBT
with or without neoadjuvant/adjuvant CT– Visibly complete TURBT was achieved in approximately two
thirds of patients and a complete response rate to induction chemoradiation in 72%(≈40 Gy in 1.8- to 2-Gy fractions).
– Complete responders and those medically unfit for cystectomy received boost chemoradiation to 64 to 65 Gy.
– Five- and 10-year OS: 52% and 35%, respectively.
• 102 patients (29%) ultimately underwent radical cystectomy, 17% for a response that was less than a complete response and 12% for recurrent invasive tumors.
• Combined-modality therapy achieved a complete response and preserved the native bladder in approximately 70% of patients, while offering longterm survival rates comparable to those in contemporary radical cystectomy series

• RTOG 95-06, 2000• 34 patients with clinical stage T2–T4a, Nx M0 without
hydronephrosis.
–After performing as complete a transurethral resection as possible, induction chemoradiotherapy was administered. (cisplatin and 5-fluorouracil, radiation was given twice a day, 3 Gy per fraction to the pelvis for a total of 24 Gy).
–Patients with a complete response received the same drugs combined with twice-daily radiation therapy to the bladder and a bladder tumor volume of 2.5 Gy per fraction for a total consolidation dose of 20 Gy. Median follow-up was 29 months.
• After induction treatment, 22 (67%) of the 33 patients had no tumor detectable on urine cytology or rebiopsy.
• Of the 11 patients who still had detectable tumors, six underwent radical cystectomy.
• No patient required a cystectomy for radiation toxicity.• Three-year overall survival was 83%.• Three-year survival with intact bladder was 66%.• Both the complete response rate to induction therapy and
the 3-year survival with an intact bladder were encouraging.

• RTOG 97-06, 2003• 47 eligible patients with stage T2–T4aN0M0.– Median follow-up was 26 months. TURBT within 6 weeks of
the initiation of induction therapy [13 days of concomitant boost RT, 1.8 Gy to the pelvis in the morning followed by 1.6 Gy to the tumor 4–6 h later and cisplatin (20 mg/m2)].
– Three to four weeks after induction, the patients were evaluated for residual disease.
• In the consolidation phase, 1.5-Gy fractions were given to both, twice daily for 8 days (total dose, 45.6 Gy to the pelvis and bladder and 64.8 Gy to the bladder tumor).
• After consolidation chemoradiation or cystectomy (depending on the response), patients received three cycles of adjuvant MCV chemotherapy.– CR rate was 74%.– Three-year rates of locoregional failure, distant metastasis,
overall survival, and bladder- intact survival were 27, 29, 61, and 48%, respectively.
• Adjuvant MCV chemotherapy appears to be poorly tolerated.

RTOG 99-06(2009)◦ 80 patients with T2–T4a; twice-daily radiotherapy
with paclitaxel and cisplatin chemotherapy induction (TCI) was administered. Adjuvant gemcitabine and cisplatin were given to all patients.
◦ TCI resulted in 26% developing grade 3–4 acute toxicity, mainly gastrointestinal (25%).
◦ The post induction complete response rate was 81% (65/80).
◦ Thirty-six patients died (22 of bladder cancer).◦ Five-year overall and disease-specific survival rates
were 56 and 71%, respectively.

The primary goal of bladder-preserving therapy, as with any therapy for muscle-invading TCC of the bladder, is optimizing patient survival.
Bladder preservation in the interest of quality of life can only be considered a secondary objective.
The long-term outcome data presented above from single institution and cooperative group experience suggest that modern combined-modality therapy results in complete response rates of 60% to 80%, 5-year OS of 45% to 60%, and
5-year survival with an intact bladder of 40% to 45%.
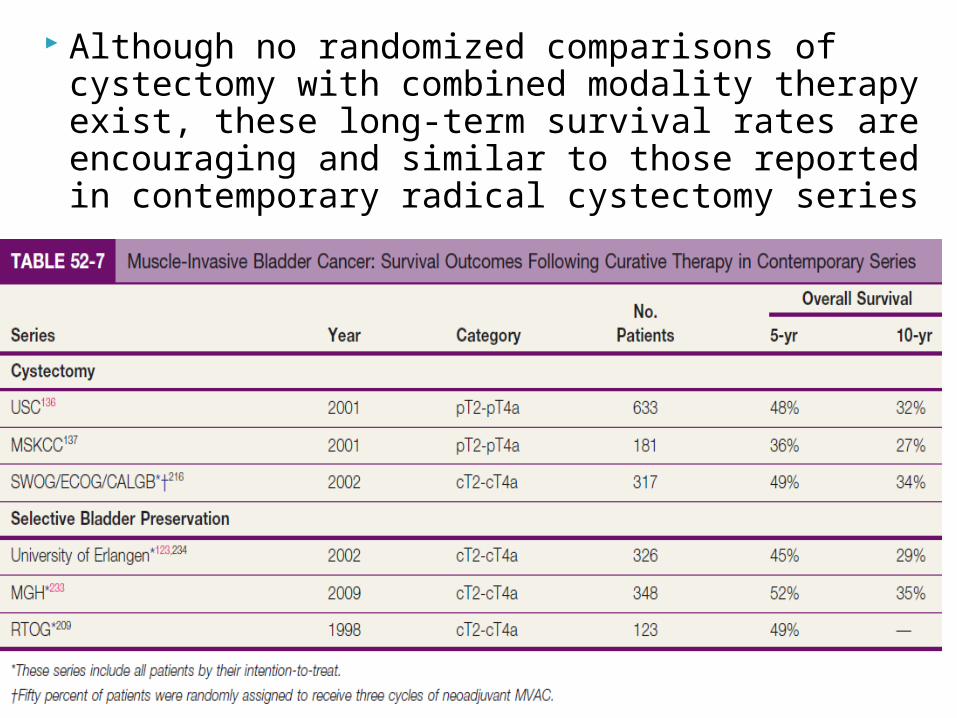
Although no randomized comparisons of cystectomy with combined modality therapy exist, these long-term survival rates are encouraging and similar to those reported in contemporary radical cystectomy series


NCI-Canada, 1996 (1st Trial)◦ 99 patients with T2–T4b.
Treated with either RT or CTRT (with concurrent cisplatin 100mg/m2)
Median follow up:6.5 years Loco-regional relapse rate better with CTRT
(50% vs. 33%) No difference in OS or distant metastasis
• Radiotherapy with or without chemotherapy in muscle invasive cancer bladder (Nicholas et al) NEJM 2012;366:1477-88–Multicenter Phase III randomized trial– N=360–Muscle invasive bladder cancers randomized to :• Whole bladder radiotherapy• Modified volume radiotherapy to bladder withconcurrent
fluorouracil and mitomycin C• Primary end points: Survival free of loco-
regional recurrence• Secondary end points: Overall survival and
toxic effects• At 2 years, DFS was 67% (CTRT) vs. 54%
(RT);P=0.03• Grade ¾ adverse events were 36% (CTRT) vs.
27.5% (RT);P=0.07
Prognostic factors in CT-RT◦ T Satge◦ Visibly complete TURBT◦ Presence of hydronephrosis◦ Presence of TCIS disease along with invasive◦ Managing recurrent disease
Managing recurrent disease◦ Superficial– TURBT and Intravesical BCG◦ Invasive– Salvage cystectomy
In selected series, salvage cystectomy results in a 40% to 50% survival rate at 5 years and a locoregional control rate of 60%.

• Voiding symptoms are not severe and if renal function allows, it is common to give combination chemotherapy () if not non platinum based)
• If patients have had a good response, they may receive consolidation chemoradiation delivered with “curative” intent.
• PCN if hydronephrosis.• ? Resection and IORT• Unfit for cystectomy : ? Role of RT• Metastatic: MVAC /MACregimen• Palliative RT --for bone and brain mets; IVCO
in case of para aortic nodes
• Simulation:– Bladder filling variability to be minimized– Supine position with bladder empty [most
commonly recommended approach]• Target Volumes:– Initial Phase: Bladder with a margin of 2 cm
(Include prostate in males and proximal 2 cm of urethra in females). External and internal iliac group of lymph nodes covered. Care taken to exclude vulva and excess part of bowel (upper border usually not above mid SI Joint)
– Boost Phase: Controversial [Entire bladder vs. bladder tumor with a 2 cm margin]
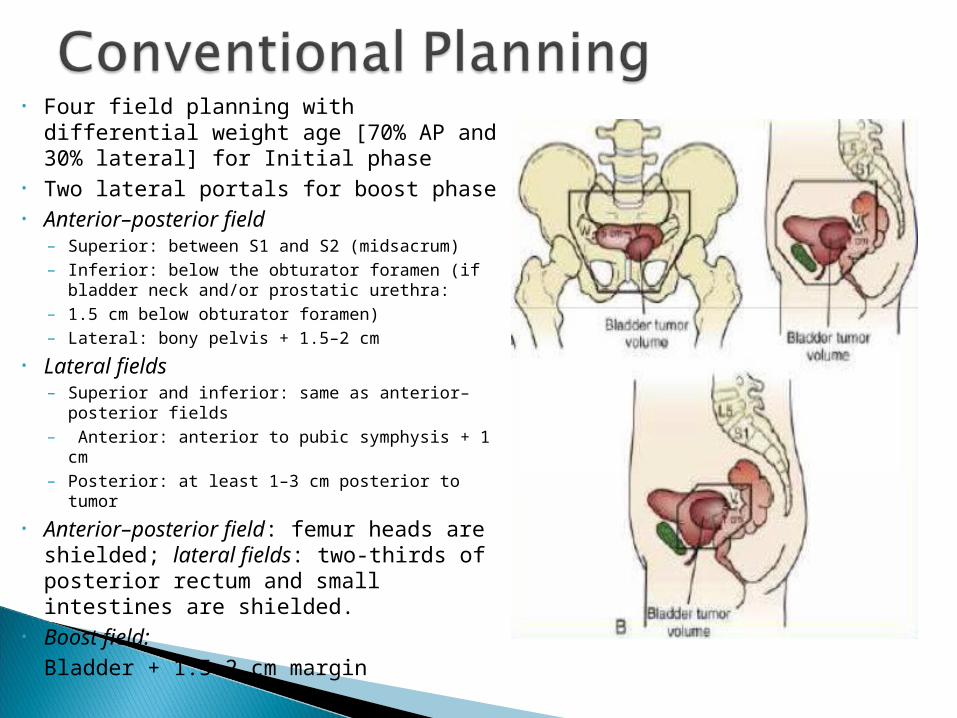
• Four field planning with differential weight age [70% AP and 30% lateral] for Initial phase
• Two lateral portals for boost phase• Anterior–posterior field
– Superior: between S1 and S2 (midsacrum)– Inferior: below the obturator foramen (if
bladder neck and/or prostatic urethra:– 1.5 cm below obturator foramen)– Lateral: bony pelvis + 1.5–2 cm
• Lateral fields– Superior and inferior: same as anterior–
posterior fields– Anterior: anterior to pubic symphysis + 1 cm– Posterior: at least 1–3 cm posterior to tumor
• Anterior–posterior field: femur heads are shielded; lateral fields: two-thirds of posterior rectum and small intestines are shielded.
• Boost field:Bladder + 1.5–2 cm margin
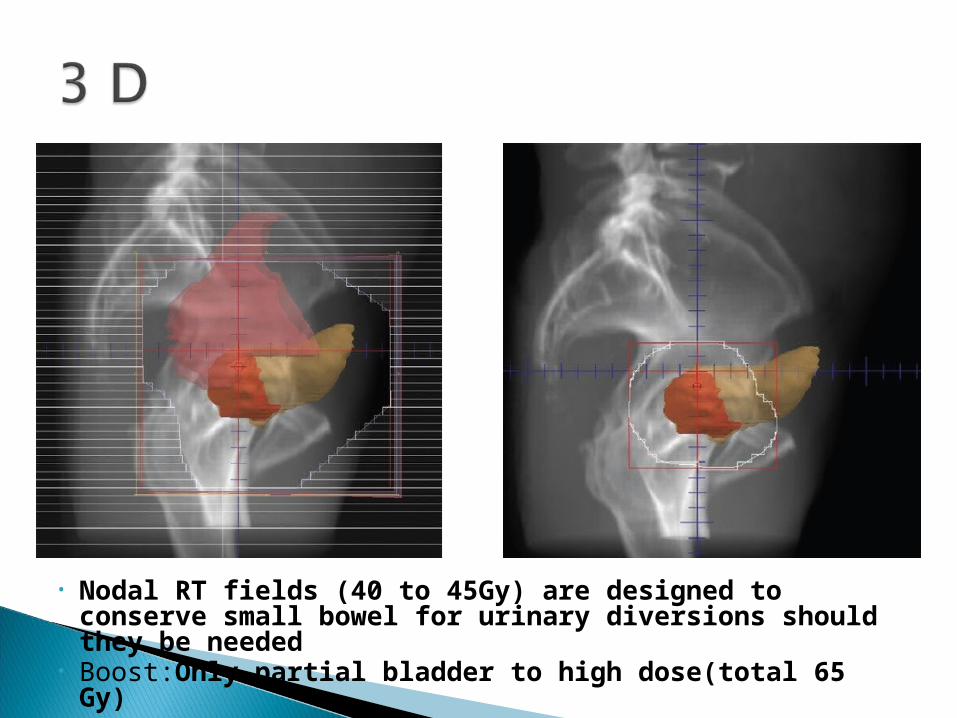
• Nodal RT fields (40 to 45Gy) are designed to conserve small bowel for urinary diversions should they be needed
• Boost:Only partial bladder to high dose(total 65 Gy)

Radiation dose: 40-45 Gy for the initial phase and 10-20 Gy for the boost phase [Dose response > 62 Gy]
Dose Fractionation: 1.8- 2 Gy/fraction [Hyperfractionation has also been tried]
Different practiced fractionation regimens: 64 Gy/32#, 55 Gy/20#,36 Gy/6#

• Partial Bladder Treatment:– Careful selection is, however, necessary, with such
approaches being limited to patients with smaller tumors (<5 cm) or unifocal tumors or those without extensive Tis disease elsewhere in the bladder
– Estimates of bladder tolerance have been made that suggest that up to 80 Gy could be given if one-third of the bladder is spared, whereas 65 Gy is the limit for whole-bladder treatment
– RCT from UK --has shown that partial bladder irradiation does allow for the delivery of a higher dose to the tumor than the whole
– But didn’t show improvement in either local control or survival rates

• Treatment Margins• PTV margin -- isotropic 2-cm margins around
either the bladder(first phase of treatment) or tumor (boost) in all three dimensions
• This is to account for setup errors and organ motion
• The greatest degree of bladder wall positional change occurred in the cranial direction, with the least variation in the anteroinferior direction, limited by the pubic symphysis.
• It is clear that organ motion is the dominant source of error
• Graham and associates have recommended anisotropic margin widths of 1.6 cm anteriorly and posteriorly, 1.4 cm laterally, 3 cm superiorly, and 1.4 cm inferiorly. The problem is that these margin incorporate much normal tissue.Hence daily image guidance is preferred.
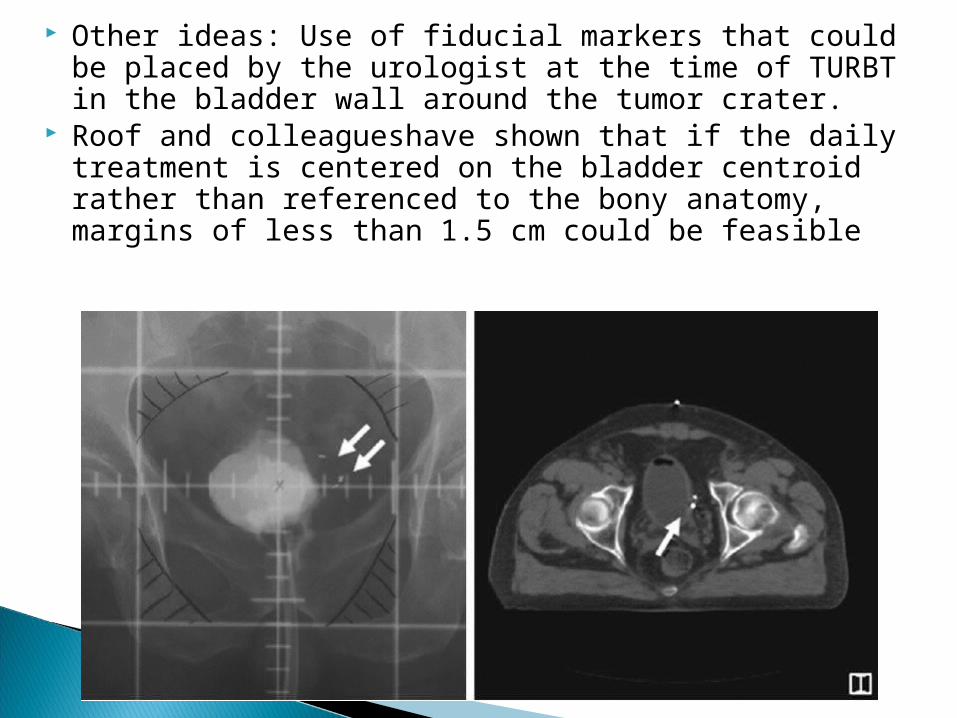
Other ideas: Use of fiducial markers that could be placed by the urologist at the time of TURBT in the bladder wall around the tumor crater.
Roof and colleagueshave shown that if the daily treatment is centered on the bladder centroid rather than referenced to the bony anatomy, margins of less than 1.5 cm could be feasible

• HyperFractionation:– Acceleration with fraction sizes of 2 Gy seems to increase
the acute toxicity.– The RTOG has therefore explored acceleration with
hyperfractionation, and recent protocols have employed fraction sizes of 1.2 to 1.8 Gy with a concomitant boost technique.
– A randomized trial of 168 patients with T2 to T4 tumors, unsuited for cystectomy, compared hyperfractionated EBRT (1 Gy three times a day to a total dose of 84 Gy) with conventional fractionation (2 Gy every day to 64 Gy)• Hyperfractionation achieved superior results with respect to
survival at 5 years (27% vs. 18%), local control (12% vs. 7%), and clinical complete response rates (59% vs. 36%), with an increase in late toxicity.
• It should be noted, however, that patients in the conventional fractionation arm did poorly compared with those receiving similar treatment in other studies, largely because patients unfit for cystectomy were taken in this study.
• Brachytherapy:– Shortly after completion of the preoperative irradiation
regimen (<2 weeks), a suprapubic cystotomy is performed to ascertain the true dimensions of the tumor and to confirm that it is indeed unifocal.
– The target area is determined by the surgery and is either the bladder scar after partial cystectomy or the macroscopic tumor plus a 1.5- to 2-cm margin.
– Narrow afterloading tubes are then inserted into the target area parallel and halfway through the bladder wall.
– If less than 10 to 15 Gy is given preoperatively, then 30 to 60 Gy is given using low-dose-rate therapy. The lower doses are given to those who have had partial cystectomies or complete resections.
– In the Netherlands, 30-Gy EBRT is either supplemented with 40-Gy low-dose-rate treatment or 10 fractions of 3.2-Gy, high-dose-rate treatment (two fractions per day with a 6-hour interval between fractions).

• Radical Cystectomy:– Urinary– Sexual–Overcome with continent diversions
• Bladder conservation protocol:– Reduced bladder compliance– Hypersensitivity– Involuntary detrusor contractions– Incontinence– Rectal urgency