Embed Size (px)
Citation preview
Sindrome Metabolica ed Iperparatiroidismo
Dr. Francesco Tassone
S.C. di Endocrinologia e Malattie del RicambioA.S.O. S. Croce e Carle - Cuneo
PremessaDerangement of glucose metabolism in hyperparathyroidism.Procopio M, Borretta G. J Endocrinol Invest. 2003;26:1136-42.
The derangement of glucose metabolism is found frequently in all forms of hyperparathyroidism. Both in primary (PHPT) and secondary hyperparathyroidism (SHPT) PTH excess is thought tobe involved in deteriorating insulin sensitivity and secretion though their different clinical and pathophysiological conditions. In PHPT these abnormalities are related to a high frequency of Type 2 diabetes mellitus and also impaired glucose tolerance according to recent clinicalstudies, without differences between symptomatic and asymptomatic clinical presentation. In chronic renal failure (CRF), the disorders of glucose metabolism due to SHPT do not bear an increased risk for diabetes whereas they seem to be involved in the progression of atherosclerotic vascular damage which connotes CRF. Moreover, clinical and experimental studies have shown that vitamin D deficiency associated with glucosemetabolism abnormalities favors the development of the metabolic syndrome. The potential for metabolic and cardiovascular harm related to hyperparathyroidism, especiallyPHPT, is the most interesting issue for clinical endocrinologists. This short review of the clinical and pathophysiological data of literature on glucose homeostasis disorders in hyperparathyroidism focuses on its potential clinical and therapeutic impact, particularly in the management of PHPT.
Perche’ affrontare questo tema?
• Cadiovascular Endocrinology: “Link” tra MS e pHPT
Come affrontero’ questo tema?
• Dati presenti in letteratura• Dati casistica cuneese
Perche’ affrontare questo tema?
- SINDROME METABOLICA“...This group of people is at high risk of macrovascular disease. “World Health Organisation. Definition, Diagnosis
and classification of Diabetes Mellitus and itsComplications (WHO, Geneva, 1999)
- IPERPARATIROIDISMO Primitivo ?
IPERPARATIROIDISMO PRIMITIVO
- Frequenza: 3° patologia endocrina dopo Diabete Mellito e Tireopatie(Pesenti et al. 2003);
- Incidenza= 1/1000 M; 2-3/1000 F (Kearns et al. MayoClinProc 2002);
- Eziologia: Adenoma singolo --> 85 % ;
Mal. multighiandolare (adenomi multipli/ iperplasia) -->15 %;
- Forma sporadica --> 97%,
- Forma familiare (MEN 1, MEN 2A, FIHP; associato a Jaw Tumor Syndrome) --> 3 %
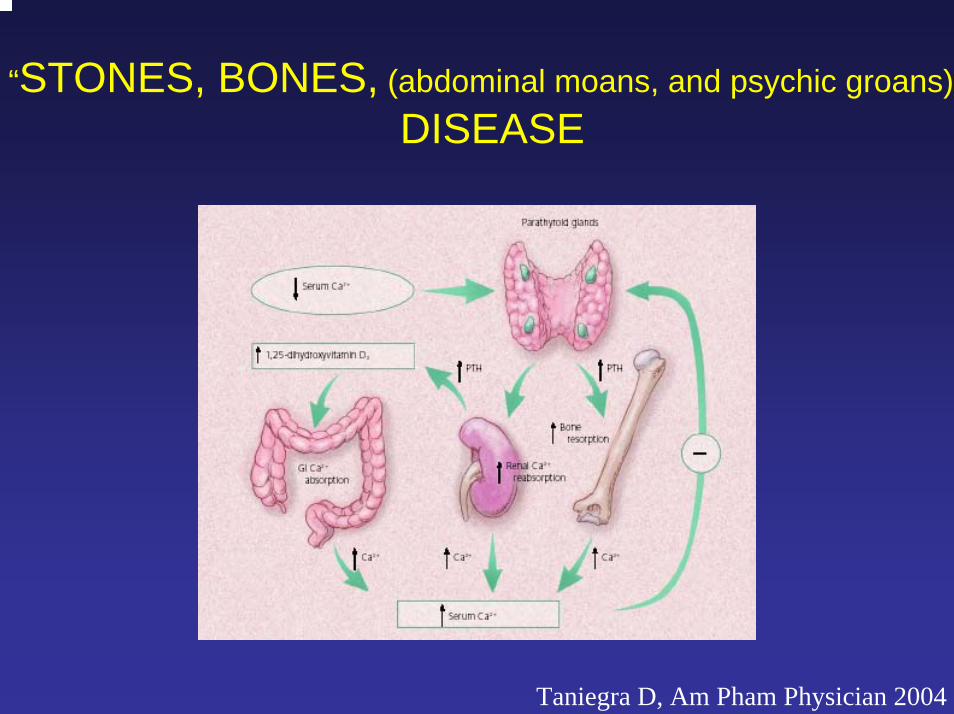
“STONES, BONES, (abdominal moans, and psychic groans)”DISEASE
Taniegra D, Am Pham Physician 2004
“..the clinical profile had shifted from a symptomatic disorder, withhypercalcemic symptoms, kidney stones, overt bone disease, or a specific neuromuscular dysfunction, toward a more asymptomatic state.
The modern clinical profile of asymptomatic primary hyperparathyroidismis best characterized as a disorder in which there are neither signs nor symptoms typically associated with hypercalcemia or parathyroid hormone excess..”.
“…nontraditional aspects of asymptomatic pHPT lead to a need for more controlled studies. The nontraditional elements of pHPT extend in particular to cardiovascular and neurobehavioural functioning ..”
Pro
babi
lity
of s
urvi
val (
%)
0
20
40
60
80
100
0 5 10 15 20
I
II
III
IV
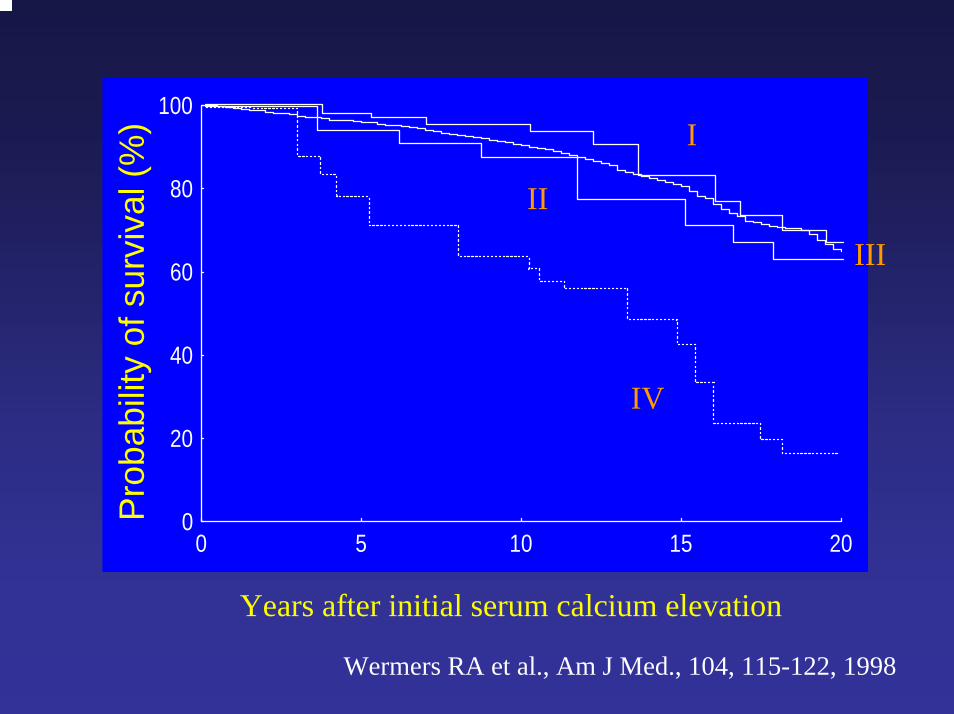
Years after initial serum calcium elevation
Wermers RA et al., Am J Med., 104, 115-122, 1998
Clinical presentation of primary hyperparathyroidism in Europe--nationwide cohort analysis on mortality from nonmalignant causes.Nilsson IL, Yin L, Lundgren E, Rastad J, Ekbom A. - J Bone Miner Res. 2002; 17 S 2:N68-74.
...By use of the nationwide Cancer Registry and Causes-of-Death Registry, mortality was analyzed in 10,995 Swedish patients (> 20 years of age) subjected to extirpation of single parathyroid adenomaof PHPT during 1958-1997. The Swedish population standardized for age, sex, and calendar year was used as control. - 102,515 observed person-years in the patients.
Results verify an increased risk of dying after operation for PHPT (standard mortality ratio, 1.2; 95% CI, 1.19-1.27). The increased risk persisted far beyond 15 years postoperatively and occurred in both sexes and in all investigated age groups. Principal causes of excess mortality were cardiovascular diseases, diabetes mellitus, and urogenital diseases in all age groups. However, in patients operated on between 1985 and 1997 (n = 6386), overall mortality did not differfrom that of the normal population, although there was maintained excess death in stroke,diabetes mellitus, and urogenital diseases. These findings infer that modern paradigms of surgical treatment normalize the risk of dying fromPHPT. This improvement may be a late consequence of liberalized calcium screenings that were introduced about 30 years ago and indicate that operation at early disease stages may offer a survival advantage. An association between diabetes mellitus and PHPT is substantiated.
STUDI IN SOGGETTI NORMALI
1- Serum calcium: a new, independent, prospective risk factor for myocardial infarction inmiddle-aged men followed for 18 years.Lind L, Skarfors E, Berglund L, Lithell H, Ljunghall S. J Clin Epidemiol. 1997;50:967-73
2183 Males; follow-up 18 years. RESULTS: 180 subjects experienced a myocardial infarction (MI). -The serum calcium levels were significantly elevated at the baseline (2.37 +/- 0.09 SD versus 2.35 +/- 0.09 mmol/l, p < 0.03) in the subjects who developed a MI when compared with the rest of the cohort. - Cox's proportional hazard analysis showed that only serum calcium (p < 0.01), BMI (p < 0.0003),diastolic blood pressure (p < 0.0009), and the atherogenic index (p < 0.002) were significantly independent risk factors for MI.
2-Serum parathyroid hormone levels predict coronary heart disease: the Tromso Study.Kamycheva E, Sundsfjord J, Jorde R. Eur J Cardiovasc Prev Rehabil. 2004 11(1):69-74.
Population-based cross-sectional study. 1459 men and 1753 women. questionari. RESULTS: When stratified for age the rate of CHD was higher in the subjects with serum PTH > 6.8pmol/l than in those with normal or low serum PTH levels [relative risk 1.67, 95% confidence interval(CI) 1.26-2.23 in men and 1.78, 95% CI 1.22-2.57 in women]. The highest PTH quartile (> 3.50pmol/l in men and > 3.30 pmol/l in women) predicted CHD, with odds ratios of 1.70 (95% CI 1.08-2.70) for men and 1.73 (95% CI 1.04-2.88) for women, versus the lowest PTH quartile (< 1.90 pmol/lfor men and <1.80 pmol/l for women).
Dati in letteratura
pHPT e vari componenti del ‘cluster’ di anormalità della MS
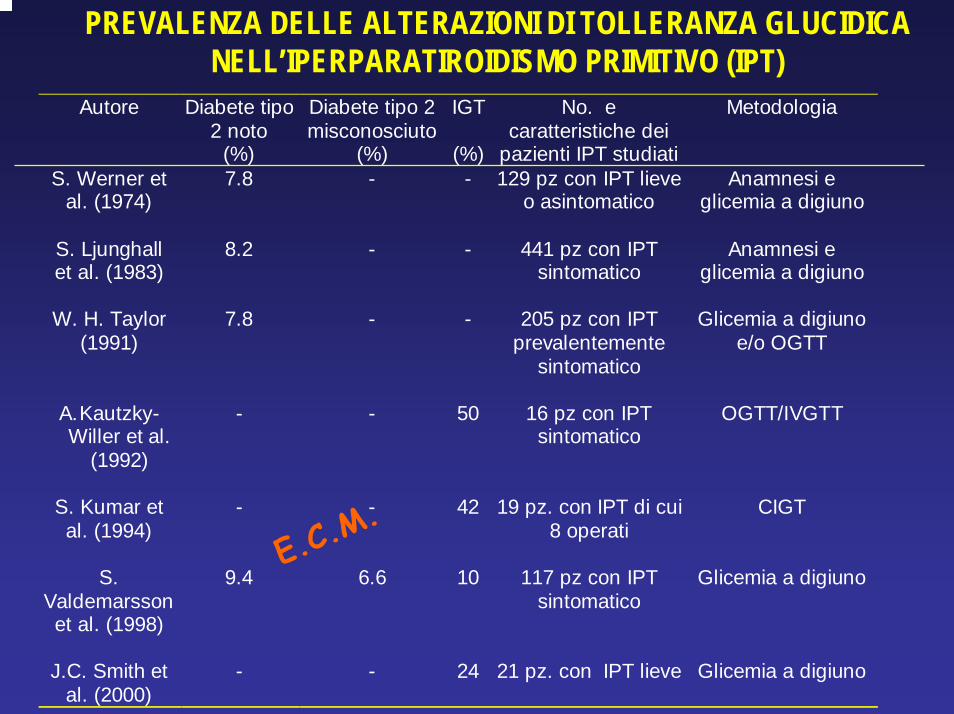
PREVALENZA DELLE ALTERAZIONI DI TOLLERANZA GLUCIDICA NELL’IPERPARATIROIDISMO PRIMITIVO (IPT)
Autore Diabete tipo2 noto
(%)
Diabete tipo 2misconosciuto
(%)
IGT
(%)
No. ecaratteristiche dei
pazienti IPT studiati
Metodologia
S. Werner etal. (1974)
7.8 - - 129 pz con IPT lieveo asintomatico
Anamnesi eglicemia a digiuno
S. Ljunghallet al. (1983)
8.2 - - 441 pz con IPTsintomatico
Anamnesi eglicemia a digiuno
W. H. Taylor(1991)
7.8 - - 205 pz con IPTprevalentemente
sintomatico
Glicemia a digiunoe/o OGTT
A. Kautzky-Willer et al.
(1992)
- - 50 16 pz con IPTsintomatico
OGTT/IVGTT
S. Kumar etal. (1994)
- - 42 19 pz. con IPT di cui8 operati
CIGT
S.Valdemarssonet al. (1998)
9.4 6.6 10 117 pz con IPTsintomatico
Glicemia a digiuno
J.C. Smith etal. (2000)
- - 24 21 pz. con IPT lieve Glicemia a digiuno
E.C.M.
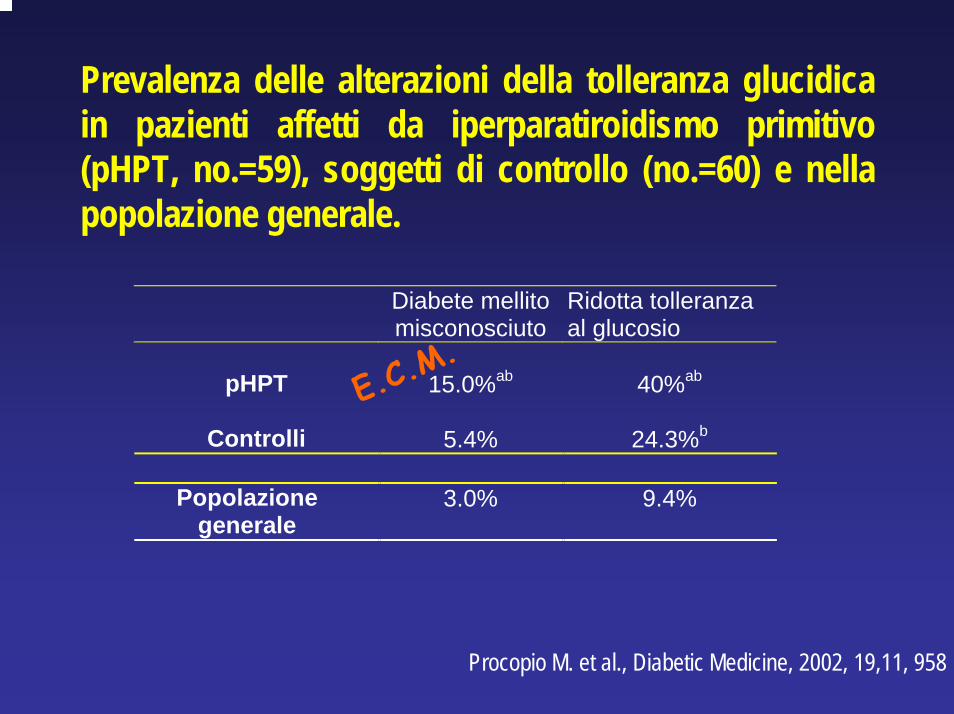
Prevalenza delle alterazioni della tolleranza glucidica in pazienti affetti da iperparatiroidismo primitivo (pHPT, no.=59), soggetti di controllo (no.=60) e nella popolazione generale.
Diabete mellitomisconosciuto
Ridotta tolleranzaal glucosio
pHPT 15.0%ab 40%ab
Controlli 5.4% 24.3%b
Popolazionegenerale
3.0% 9.4%
E.C.M.
Procopio M. et al., Diabetic Medicine, 2002, 19,11, 958
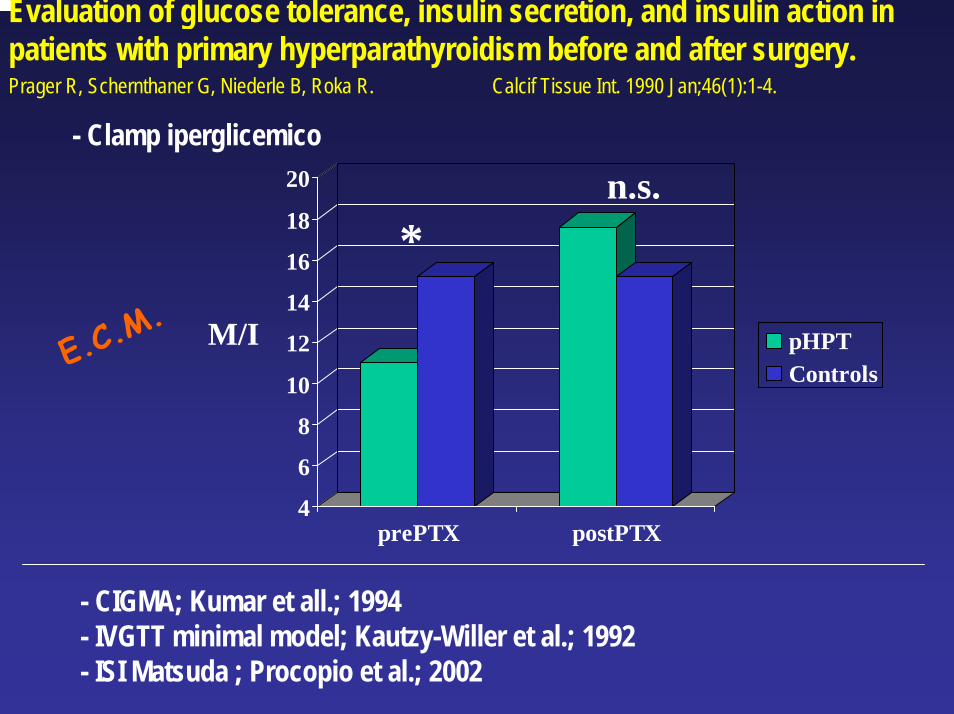
Evaluation of glucose tolerance, insulin secretion, and insulin action in patients with primary hyperparathyroidism before and after surgery.Prager R, Schernthaner G, Niederle B, Roka R. Calcif Tissue Int. 1990 Jan;46(1):1-4.
4
6
8
10
12
14
16
18
20
prePTX postPTX
pHPTControls
M/I
*
- Clamp iperglicemico
n.s.
E.C.M.
- CIGMA; Kumar et all.; 1994- IVGTT minimal model; Kautzy-Willer et al.; 1992- ISI Matsuda ; Procopio et al.; 2002
•Non correlazioni tra Insulino-sensibilità e calcio/fosforo/PTH in pazienti affetti da pHPT
•in soggetti normali:
•DeFronzo et al.(NEJM 1980)--> ipofosfatemia èassociata a diminuità insulino-sensibilità (clamp)
• Chiu KC et al. (Metabolism 2000)-->52 SN , clamp, - ISI negativamente correlato a iPTH (r2 = .104, P = .020);
- 1st PHpositively correlated with plasma iPTH level (r2 = .098, P = .023), - After adjusting (age/gender/ethnicity/WHR) iPTH level was an independentdeterminant of insulin sensitivity index (P = .019).- In normotensive, glucose-tolerant, and healthy subjects, plasma iPTH levelaccounts for 10.4% of the variation in insulin sensitivity index.
IPOTESI PATOGENETICHE DELL’ALTERATO METABOLISMO GLUCIDICO NELL’IPERPARATIROIDISMO PRIMITIVO
• Ipercalcemia:
1) stimolo diretto glucosio-indotto della secrezione insulinica (in acuto);
2) inibizione dell’utilizzazione periferica di glucosio (inibizione defosforilazione di GLUT4 in tess. adiposo e muscolare)
• Aumentati livelli di PTH:
1) aumento della gluconeogenesi epatica (in vivo ed in vitro) e stimolo indiretto della secrezione insulinica.
• Ipofosforemia:
1) riduzione della sensibilità insulinica (in vivo) nell’animale e nell’uomo.
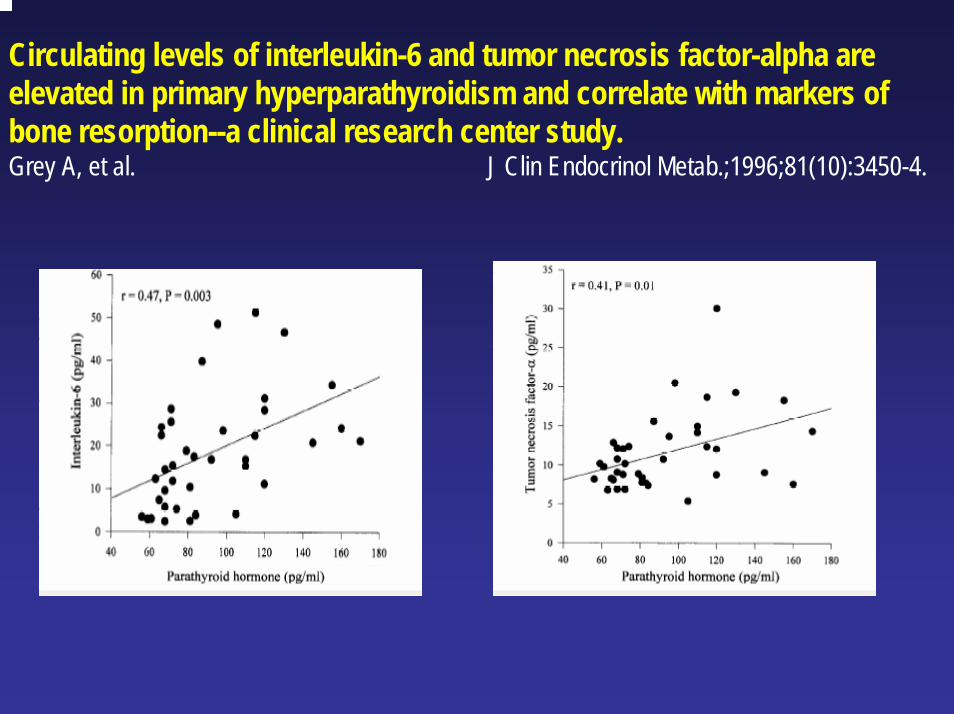
Circulating levels of interleukin-6 and tumor necrosis factor-alpha areelevated in primary hyperparathyroidism and correlate with markers ofbone resorption--a clinical research center study.Grey A, et al. J Clin Endocrinol Metab.;1996;81(10):3450-4.
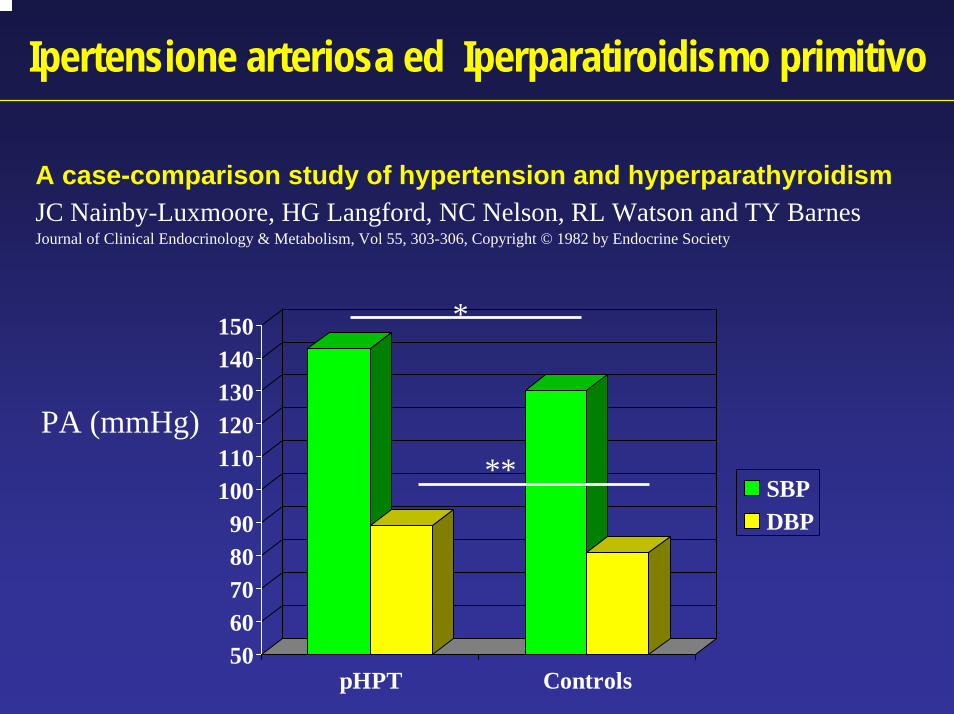
Ipertensione arteriosa ed Iperparatiroidismo primitivo
A case-comparison study of hypertension and hyperparathyroidismJC Nainby-Luxmoore, HG Langford, NC Nelson, RL Watson and TY BarnesJournal of Clinical Endocrinology & Metabolism, Vol 55, 303-306, Copyright © 1982 by Endocrine Society
5060708090
100110120130140150
pHPT Controls
SBPDBP
PA (mmHg)
*
**
IPOTESI PATOGENETICHE DELL’IPERTENSIONE ARTERIOSA NELL’IPERPARATIROIDISMO PRIMITIVO
• ipomagnesiemiaSangal AK ET AL., DS, Rival J. South Med J.; 1989;
•effetto diretto del paratormone
•incremento dell'attività dell'asse renina-aldosteroneGanguly A et al., Metabolism. 1982;31(6):595-600.
•alterato ritmo pressorio circadiano con riduzione del dipping notturno. (dati controversi….)
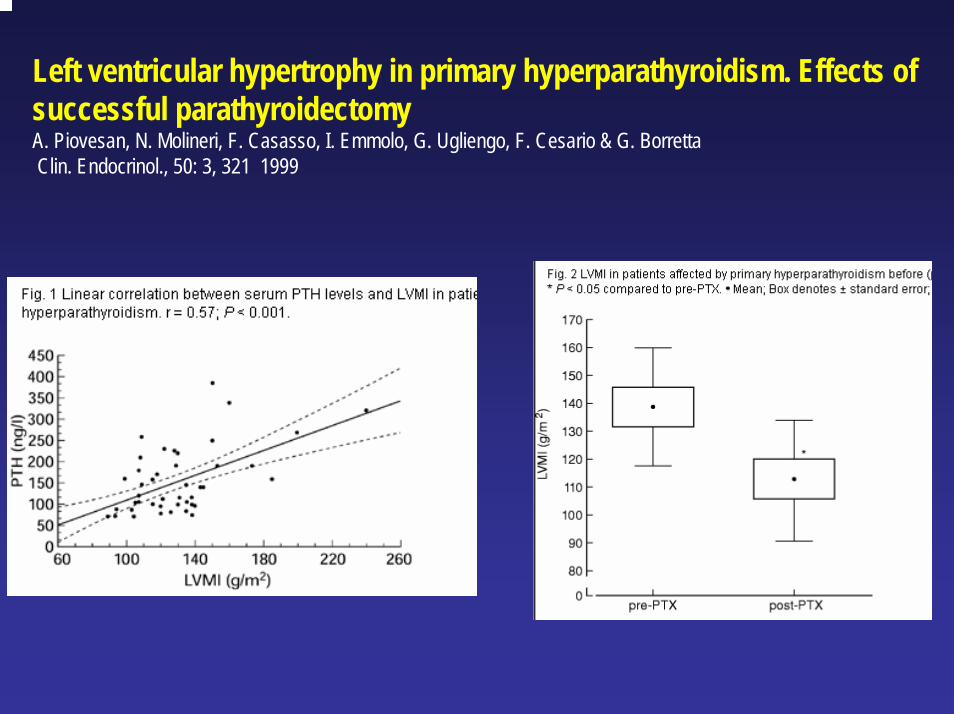
Left ventricular hypertrophy in primary hyperparathyroidism. Effects of successful parathyroidectomyA. Piovesan, N. Molineri, F. Casasso, I. Emmolo, G. Ugliengo, F. Cesario & G. Borretta Clin. Endocrinol., 50: 3, 321 1999
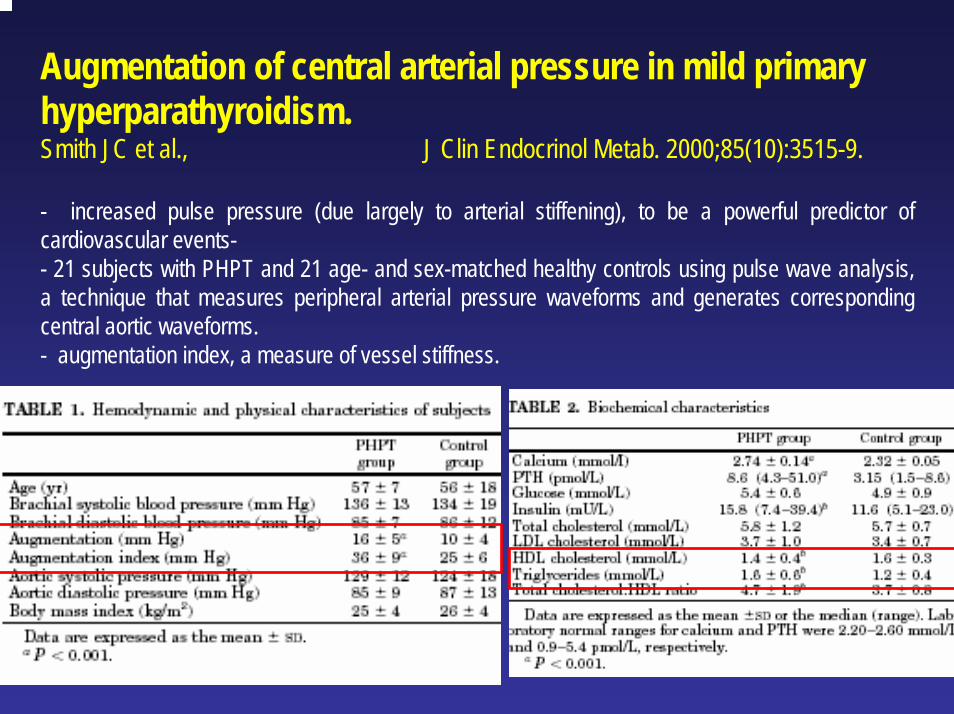
Augmentation of central arterial pressure in mild primary hyperparathyroidism.Smith JC et al., J Clin Endocrinol Metab. 2000;85(10):3515-9.
- increased pulse pressure (due largely to arterial stiffening), to be a powerful predictor of cardiovascular events-- 21 subjects with PHPT and 21 age- and sex-matched healthy controls using pulse wave analysis, a technique that measures peripheral arterial pressure waveforms and generates corresponding central aortic waveforms. - augmentation index, a measure of vessel stiffness.
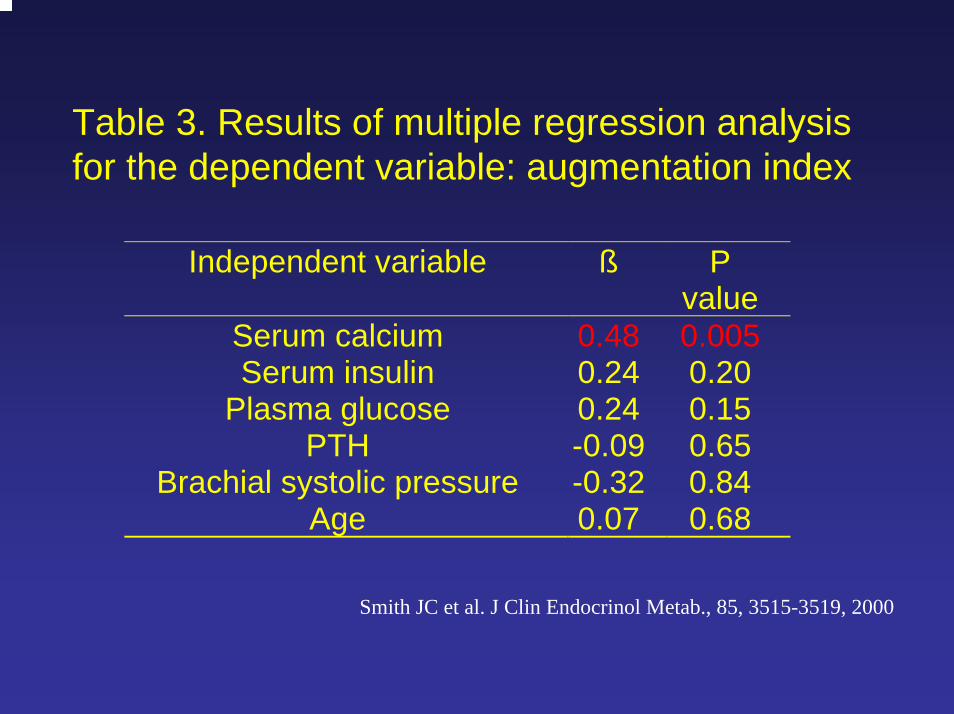
Table 3. Results of multiple regression analysis for the dependent variable: augmentation index
Independent variable ß Pvalue
Serum calcium 0.48 0.005Serum insulin 0.24 0.20
Plasma glucose 0.24 0.15PTH -0.09 0.65
Brachial systolic pressure -0.32 0.84Age 0.07 0.68
Smith JC et al. J Clin Endocrinol Metab., 85, 3515-3519, 2000
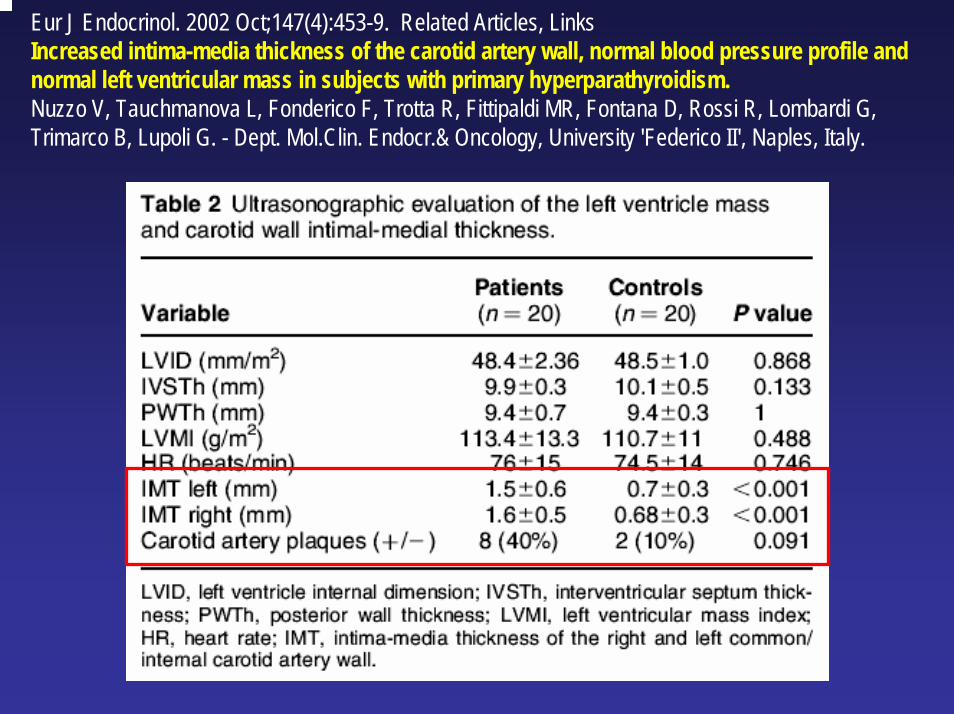
Eur J Endocrinol. 2002 Oct;147(4):453-9. Related Articles, Links Increased intima-media thickness of the carotid artery wall, normal blood pressure profile and normal left ventricular mass in subjects with primary hyperparathyroidism.Nuzzo V, Tauchmanova L, Fonderico F, Trotta R, Fittipaldi MR, Fontana D, Rossi R, Lombardi G,Trimarco B, Lupoli G. - Dept. Mol.Clin. Endocr.& Oncology, University 'Federico II', Naples, Italy.
Obesità ed Iperparatiroidismo primitivo
Body weight and bone mineral density in postmenopausal women with primary hyperparathyroidism.Grey AB et al. Ann Intern Med. 1994 Nov 15;121(10):745-9.
PATIENTS: 41 postmenopausal women with mild primary hyperparathyroidism and 43 eucalcemic, age-matchedcontrols. MEASUREMENTS: dual-energy x-ray absorptiometry. RESULTS: Women with primary hyperparathyroidism were heavier (75.5 kg compared with 66.3 kg; difference, 9.2 kg [95% CI, 3.7 to 14.7 kg]; P = 0.002), had a higher fat mass (33.3 kg compared with 26.1 kg; difference, 7.2 kg [CI, 3.0 to 11.4 kg]; P = 0.001), and had a more android pattern of fat distribution (android-to-gynoid fat ratio, 1.05 compared with 0.84; difference, 0.21 [CI, 0.1 to 0.32]; P = 0.0004) than the controls.
Serum parathyroid hormone level is associated with body mass index. The 5th Tromsø study.Kamycheva E et al. Eur J Endocrinol. 2004 Aug;151(2):167-72.
Serum calcium and PTH were measured in a subset of 3447 men and 4507 women. RESULTS: For serum calcium and PTH there was a significant positive relation to BMI in both genders(P<0.001).. . The highest quartile of serum PTH (>4.20 pmol/l) was a significant predictor for obesity(P<0.001) in both genders, adjusted for age, physical activity and serum calcium.
Profilo lipidico ed Iperparatiroidismo primitivo
Metabolic abnormalities related to cardiovascular risk in primary hyperparathyroidism: effects of surgical treatment.Valdemarsson S et al. J Intern Med. 1998; 244(3):241-9. - Longitudinal study of patients with pHPT before and 1 year after surgical treatment. - SUBJECTS: 117 consecutive patients with pHPT; INTERVENTION: PTX- RESULTS: Total cholesterol and trigylceride concentrations were not changed. However, malepatients had significantly lower triglyceride levels at follow-up, 1.16+/-0.09 mmol/L compared to1.57+/-0.14 mmol/L before surgery (P < 0.05). - The serum level of urate decreased in both male and female patients after surgery.
Normalized dyslipidaemia after parathyroidectomy in mild primary hyperparathyroidism: population-based study over five years.Hagstrom E et al. Clin Endocrinol. 2002;56(2):253-60. - 87 postmenopausal women with mild, asymptomatic pHPT and matched controls (69 of whom completed a 5-year follow-up period). - RESULTS: pHPT showed decreased HDL-cholesterol, increased total triglycerides, VLDL-triglycerides and an elevated atherogenic index. - The differences were ..inversely correlated to the serum parathyroid hormone level. - PTX, with or without additive hormone replacement therapy, normalized the dyslipidaemia. - Five-year surveillance of pHPT without treatment was associated with a maintained increase in total triglycerides and the atherogenic index and a decrease in HDL-cholesterol levels.
Disfunzione endoteliale ed Iperparatiroidismo primitivoEndothelial vasodilatory dysfunction in primary hyperparathyroidism is reversed after parathyroidectomy.Nilsson IL et al. Surgery. 1999; 126(6):1049-55 25 HPT patients and 25 normocalcemic control subjects, matched for age and gender- forearm venous occlusion plethysmography. EDV and EIDV were evaluated during local infusion of metacholine (2 and 4 micrograms/min) and nitroprusside (5 and 10 micrograms/min), respectively. RESULTS: EDV lower in the HPT patients compared with control subjects. Reinvestigation 10 months after parathyroidectomy showed increase in EDV and decrease in EIDV.
Studies on flow-mediated vasodilation and intima-media thickness of the brachial artery in patients with primary hyperparathyroidism.Kosch M et al. Am J Hypertens. 2000 Jul;13(7):759-64Endothelium-dependent vasodilation is impaired in patients with primary hyperparathyroidism despite normal IMT. Endothelial dysfunction may contribute to increased cardiovascular morbidity and mortality in pHPT.
Impaired flow-mediated vasodilation of the brachial artery in patients with primary hyperparathyroidism improves after parathyroidectomy.Kosch M et al. Cardiovasc Res. 2000; 47(4):813-8. - brachial flow-mediated vasodilation (FMD) and brachial and carotid intima-media thickness (IMT) inpatients with primary hyperparathyroidism (pHPT) before and after Ptx and in healthy controls.Endothelium dependent FMD at baseline was impaired in patients compared to controls (4.7+/-1.2 vs. 18.2+/-3.7%, P<0.01), however, FMD improved significantly after Ptx (16.7+/-3.0%, P<0.01).
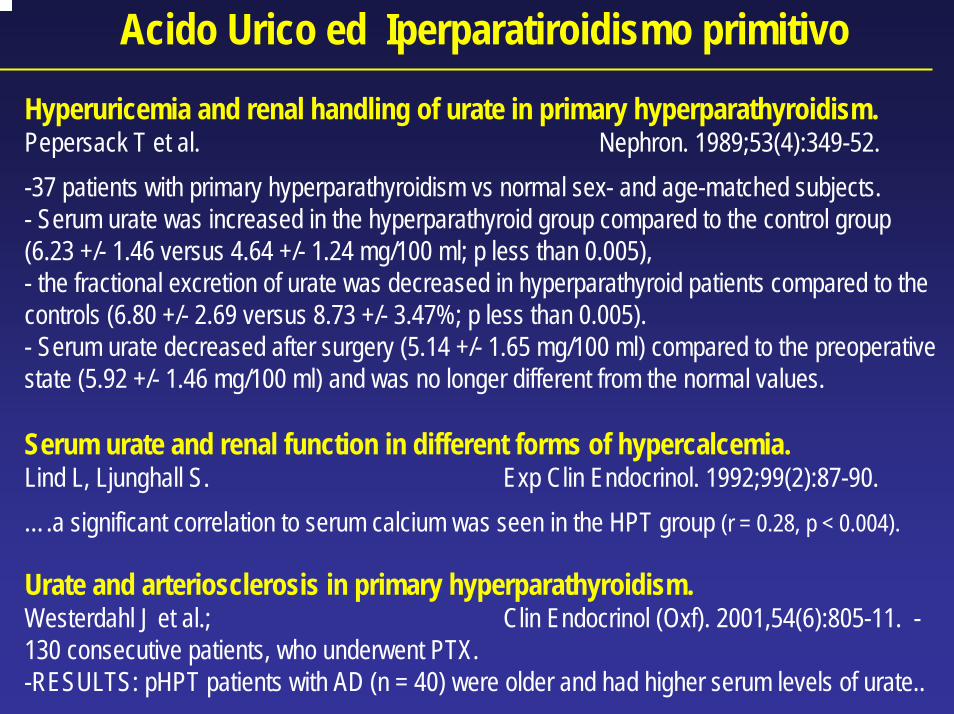
Acido Urico ed Iperparatiroidismo primitivoHyperuricemia and renal handling of urate in primary hyperparathyroidism.Pepersack T et al. Nephron. 1989;53(4):349-52. -37 patients with primary hyperparathyroidism vs normal sex- and age-matched subjects. - Serum urate was increased in the hyperparathyroid group compared to the control group(6.23 +/- 1.46 versus 4.64 +/- 1.24 mg/100 ml; p less than 0.005), - the fractional excretion of urate was decreased in hyperparathyroid patients compared to the controls (6.80 +/- 2.69 versus 8.73 +/- 3.47%; p less than 0.005). - Serum urate decreased after surgery (5.14 +/- 1.65 mg/100 ml) compared to the preoperativestate (5.92 +/- 1.46 mg/100 ml) and was no longer different from the normal values.
Serum urate and renal function in different forms of hypercalcemia.Lind L, Ljunghall S. Exp Clin Endocrinol. 1992;99(2):87-90. ….a significant correlation to serum calcium was seen in the HPT group (r = 0.28, p < 0.004).
Urate and arteriosclerosis in primary hyperparathyroidism.Westerdahl J et al.; Clin Endocrinol (Oxf). 2001,54(6):805-11. -130 consecutive patients, who underwent PTX.-RESULTS: pHPT patients with AD (n = 40) were older and had higher serum levels of urate..
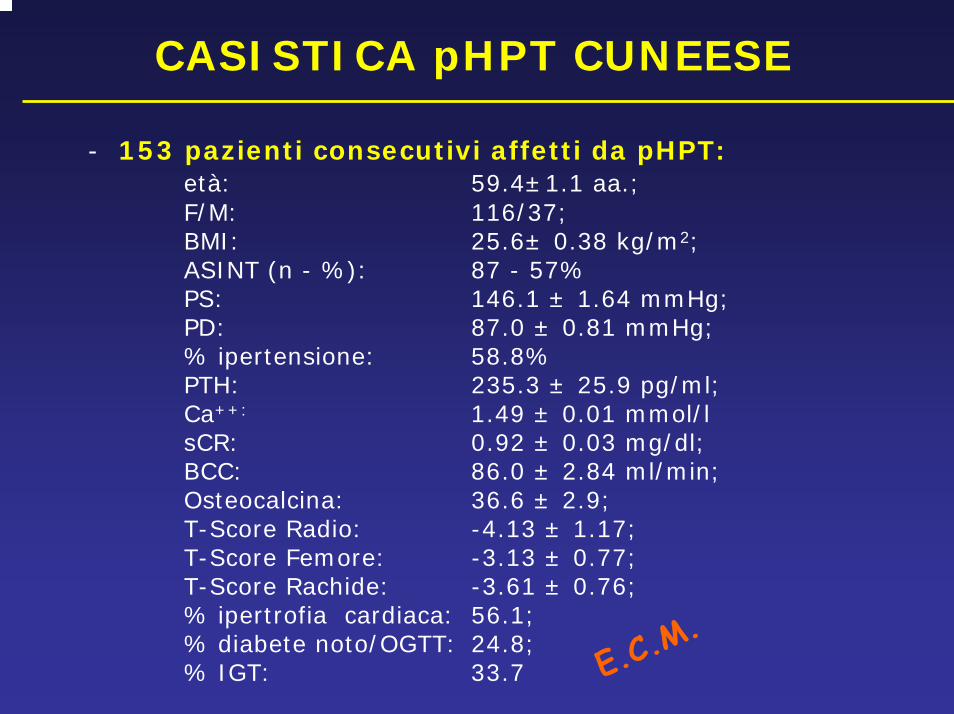
CASISTICA pHPT CUNEESE
- 153 pazienti consecutivi affetti da pHPT:età: 59.4±1.1 aa.; F/M: 116/37; BMI: 25.6± 0.38 kg/m2; ASINT (n - %): 87 - 57%PS: 146.1 ± 1.64 mmHg;PD: 87.0 ± 0.81 mmHg;% ipertensione: 58.8%PTH: 235.3 ± 25.9 pg/ml; Ca++: 1.49 ± 0.01 mmol/lsCR: 0.92 ± 0.03 mg/dl;BCC: 86.0 ± 2.84 ml/min;Osteocalcina: 36.6 ± 2.9;T-Score Radio: -4.13 ± 1.17;T-Score Femore: -3.13 ± 0.77;T-Score Rachide: -3.61 ± 0.76;% ipertrofia cardiaca: 56.1;% diabete noto/OGTT: 24.8; % IGT: 33.7 E.C.
M.
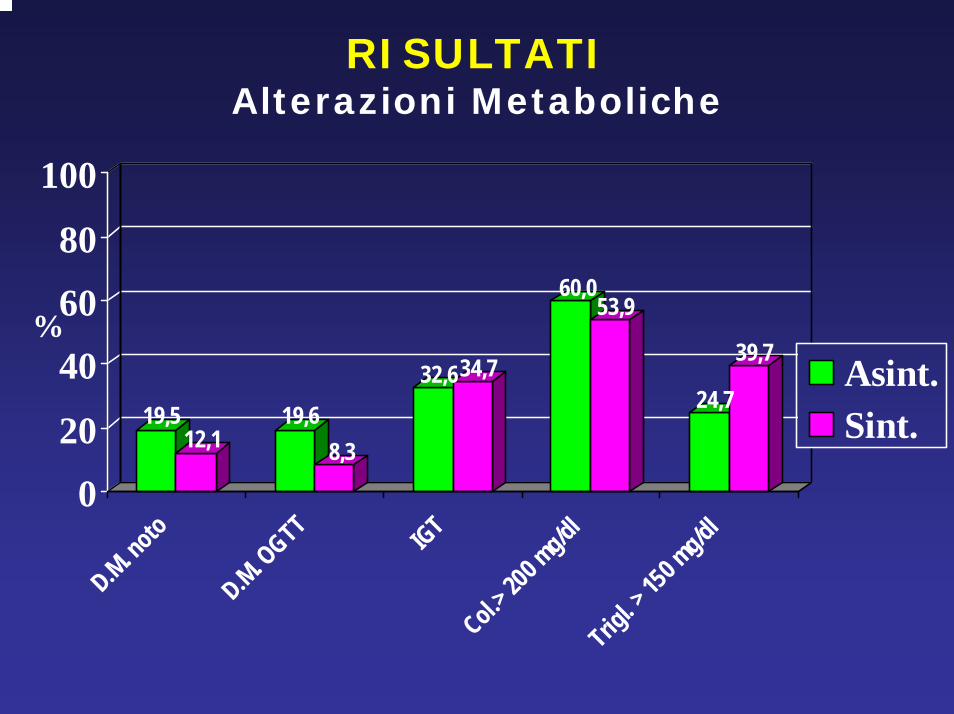
RISULTATIAlterazioni Metaboliche
19,512,1
19,68,3
32,634,7
60,053,9
24,7
39,7
0
20
40
60
80
100
D.M. noto
D.M. OGTT IGT
Col.> 200 m
g/dlTrig
l. > 15
0 mg/dl
Asint.Sint.
%
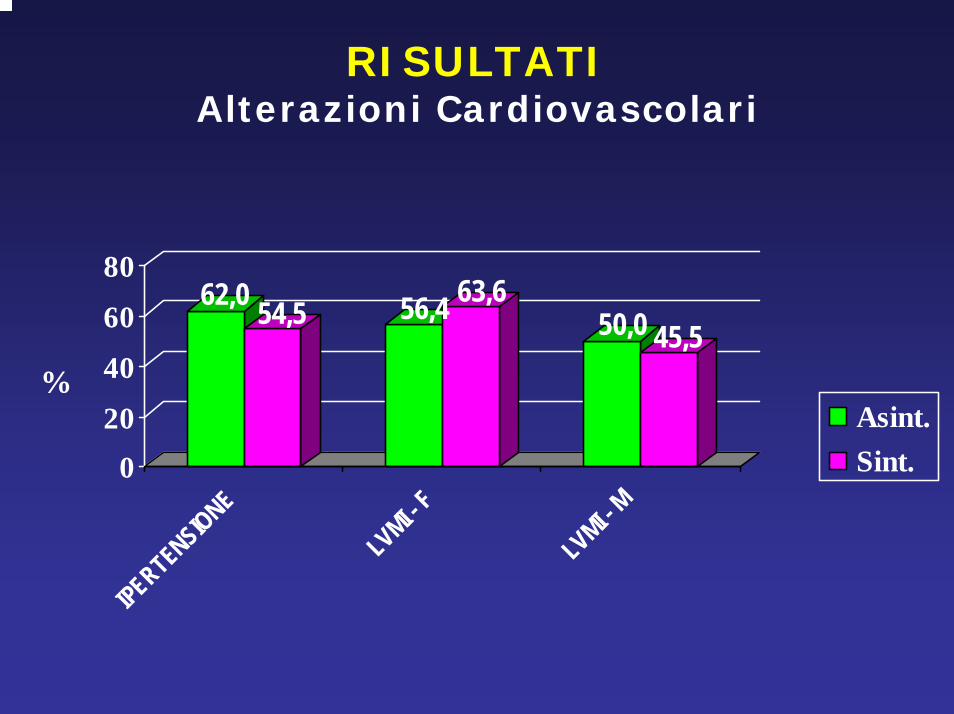
RISULTATIAlterazioni Cardiovascolari
62,0 54,5 56,4 63,650,0 45,5
020
40
60
80
IPERTENSIONE
LVMI - F
LVMI - M
Asint.Sint.
%
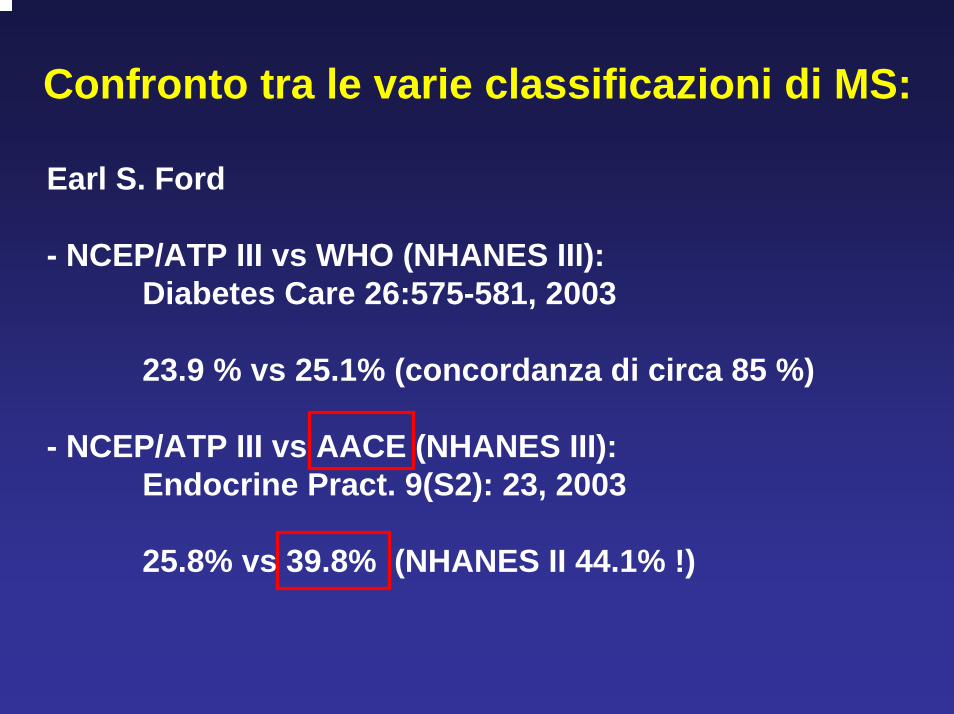
Confronto tra le varie classificazioni di MS:
Earl S. Ford
- NCEP/ATP III vs WHO (NHANES III):Diabetes Care 26:575-581, 2003
23.9 % vs 25.1% (concordanza di circa 85 %)
- NCEP/ATP III vs AACE (NHANES III):Endocrine Pract. 9(S2): 23, 2003
25.8% vs 39.8% (NHANES II 44.1% !)
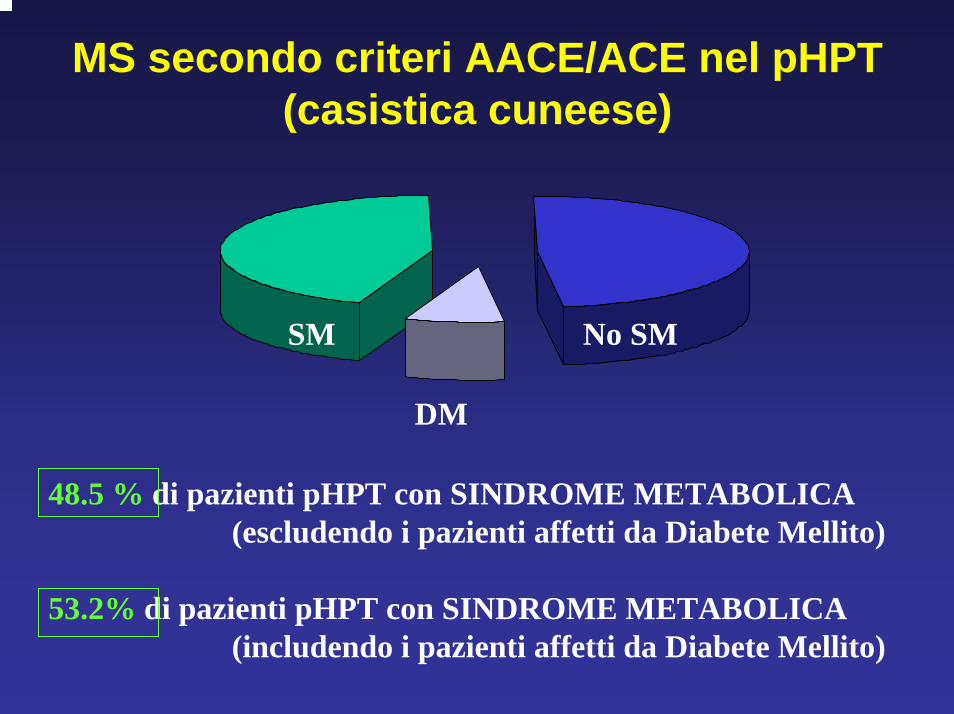
MS secondo criteri AACE/ACE nel pHPT(casistica cuneese)
48.5 % di pazienti pHPT con SINDROME METABOLICA (escludendo i pazienti affetti da Diabete Mellito)
53.2% di pazienti pHPT con SINDROME METABOLICA (includendo i pazienti affetti da Diabete Mellito)
DM
SM No SM
Appendice
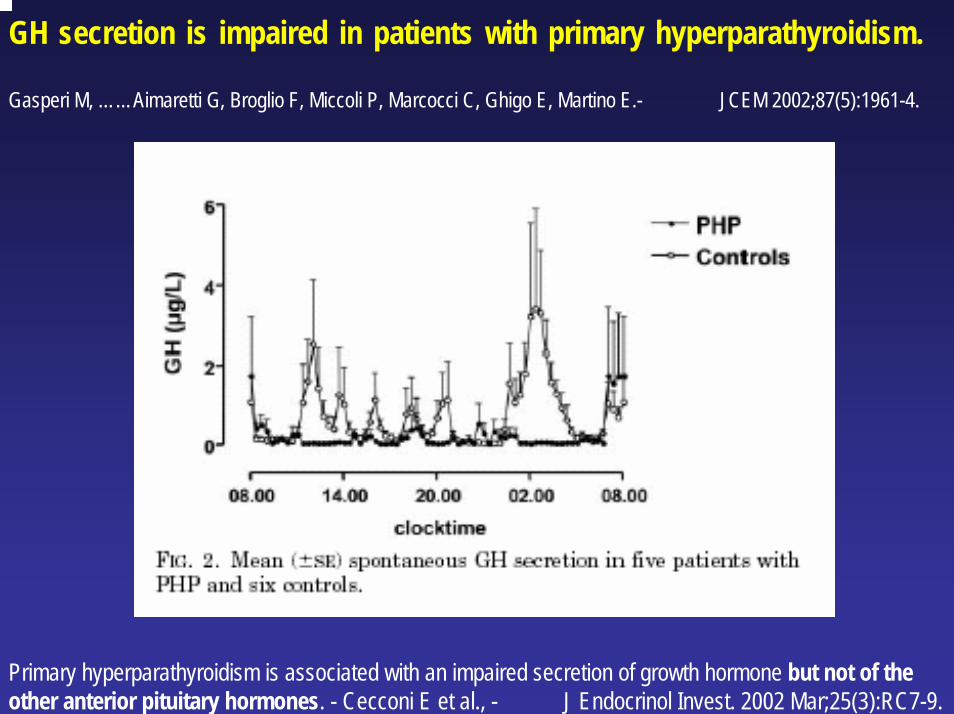
GH secretion is impaired in patients with primary hyperparathyroidism.
Gasperi M, ……Aimaretti G, Broglio F, Miccoli P, Marcocci C, Ghigo E, Martino E.- JCEM 2002;87(5):1961-4.
Primary hyperparathyroidism is associated with an impaired secretion of growth hormone but not of the other anterior pituitary hormones. - Cecconi E et al., - J Endocrinol Invest. 2002 Mar;25(3):RC7-9.
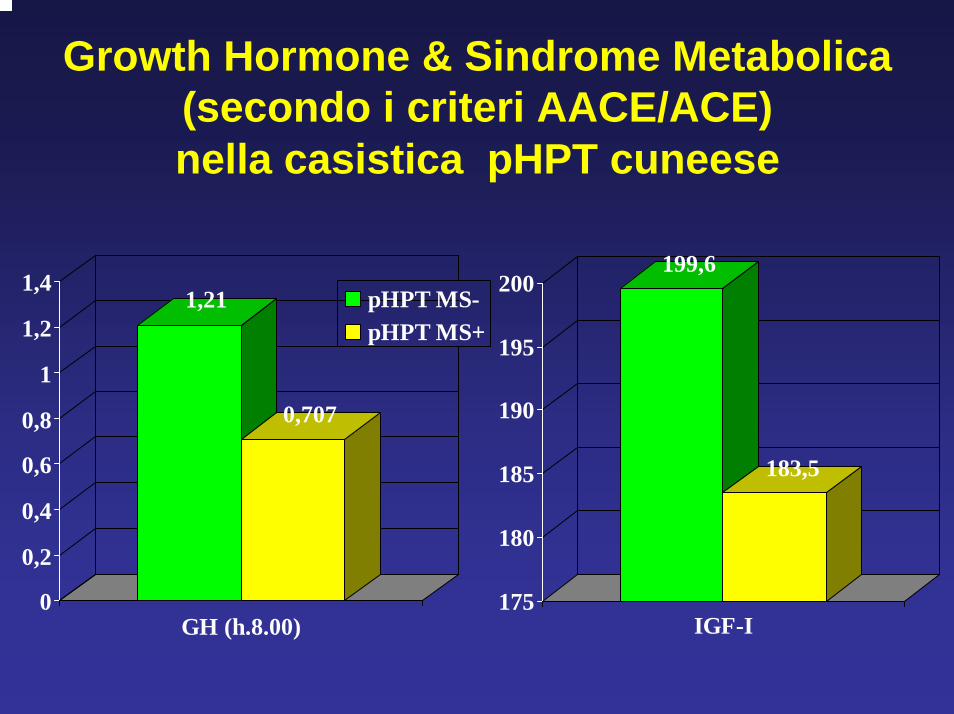
Growth Hormone & Sindrome Metabolica (secondo i criteri AACE/ACE)nella casistica pHPT cuneese
199,6
183,5
1,21
0,707
0
0,2
0,4
0,6
0,8
1
1,2
1,4
GH (h.8.00)
pHPT MS-pHPT MS+
175
180
185
190
195
200
IGF-I
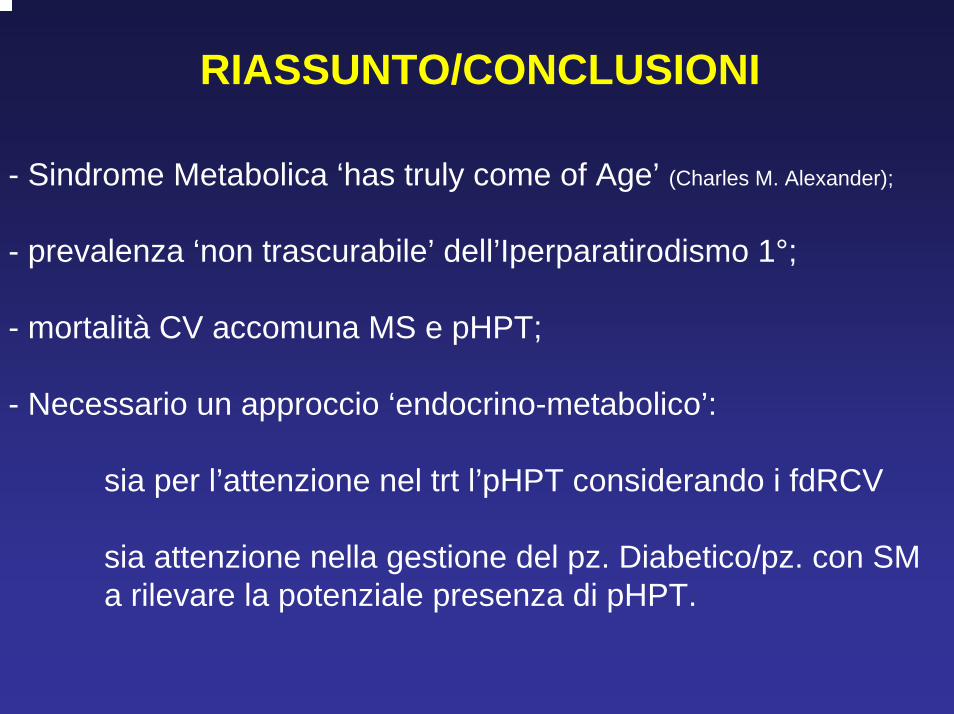
RIASSUNTO/CONCLUSIONI
- Sindrome Metabolica ‘has truly come of Age’ (Charles M. Alexander);
- prevalenza ‘non trascurabile’ dell’Iperparatirodismo 1°;
- mortalità CV accomuna MS e pHPT;
- Necessario un approccio ‘endocrino-metabolico’:
sia per l’attenzione nel trt l’pHPT considerando i fdRCV
sia attenzione nella gestione del pz. Diabetico/pz. con SM a rilevare la potenziale presenza di pHPT.
Ringraziamenti
Giorgio Borretta
Massimo ProcopioAlessandro Piovesan