Embed Size (px)
Citation preview
Michele O. CarrubaDepartment of Pharmacology, Chemotherapy and Medical
Toxicology
Center for Study and Research on Obesity
SINDROME METABOLICA:PREVENIRE O CURARE?
School of Medicine
Department of Pharmacology, Chemotherapy and Medical Toxicology
CENTER FOR STUDY AND RESEARCH ON OBESITY
University of Milan, Italy
SINDROME METABOLICA:PREVENIRE O CURARE?
Michele O. CarrubaMichele O. CarrubaDepartment of Pharmacology, Chemotherapy and Medical ToxicologySchool of MedicineVia Vanvitelli, 3220129 – Milan (Italy)
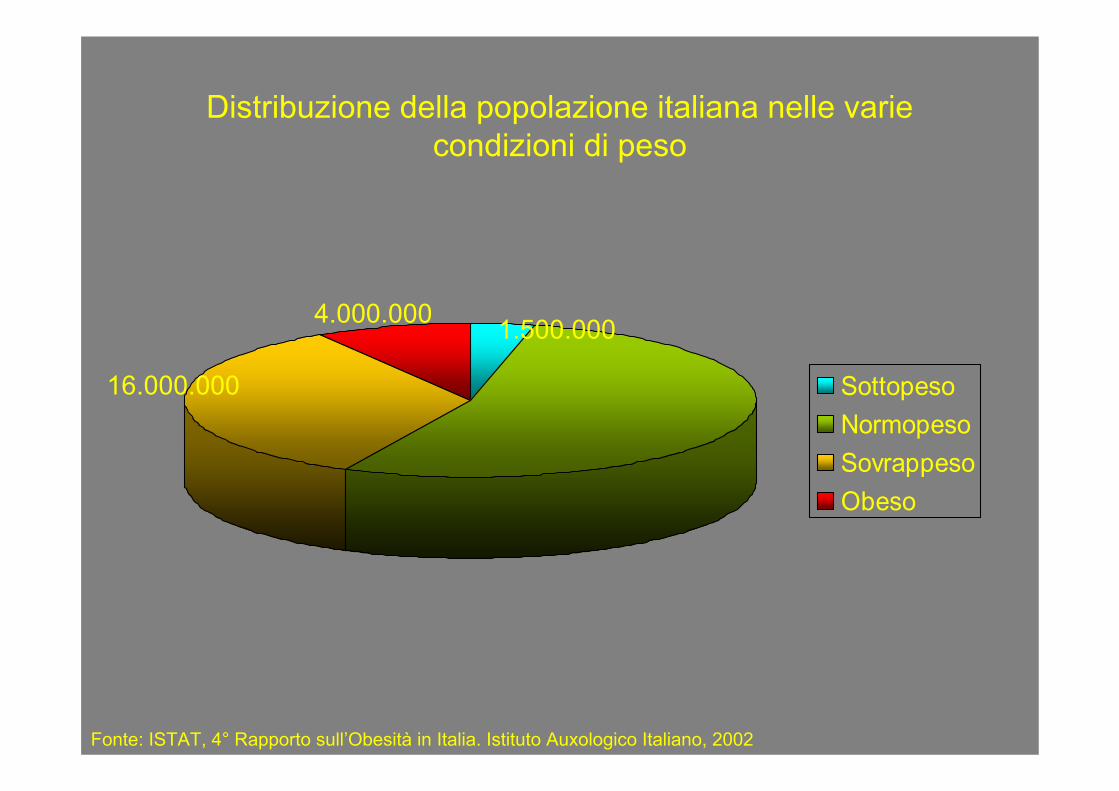
Distribuzione della popolazione italiana nelle varie condizioni di peso
SottopesoNormopesoSovrappesoObeso
4.000.000
16.000.000
1.500.000
Fonte: ISTAT, 4° Rapporto sull’Obesità in Italia. Istituto Auxologico Italiano, 2002
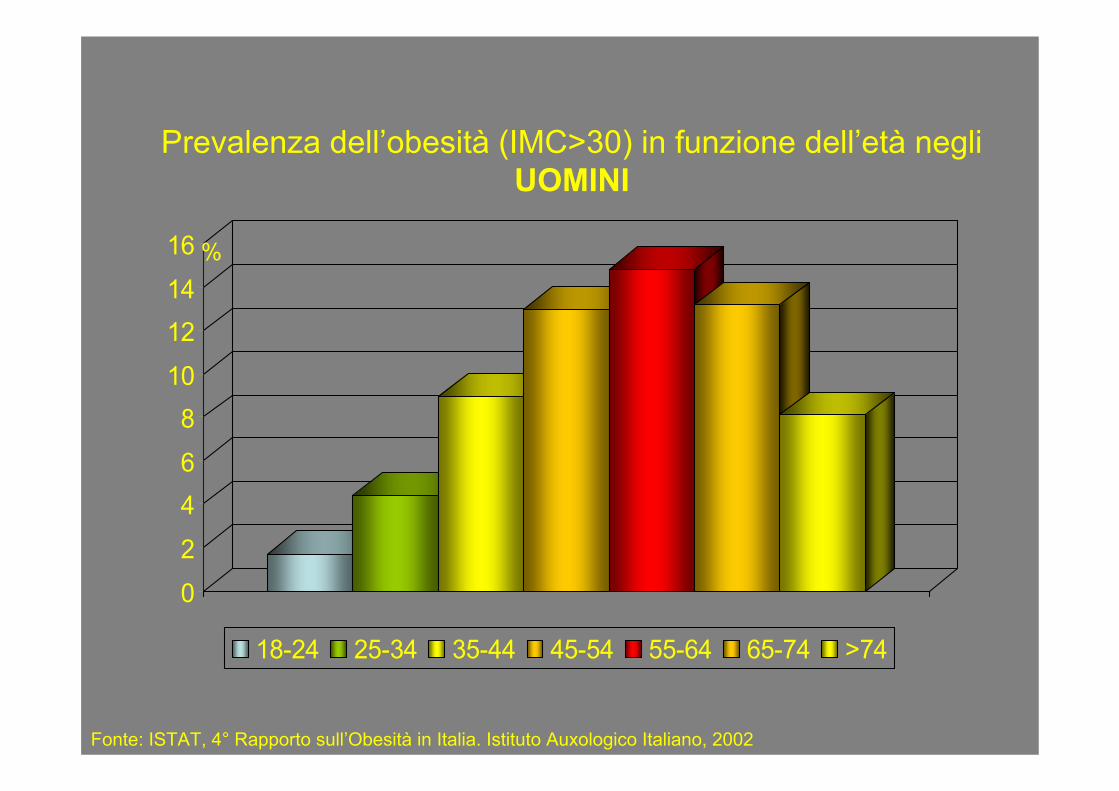
Prevalenza dell’obesità (IMC>30) in funzione dell’età negli UOMINI
0
2
46
810
1214
16
18-24 25-34 35-44 45-54 55-64 65-74 >74
%
Fonte: ISTAT, 4° Rapporto sull’Obesità in Italia. Istituto Auxologico Italiano, 2002
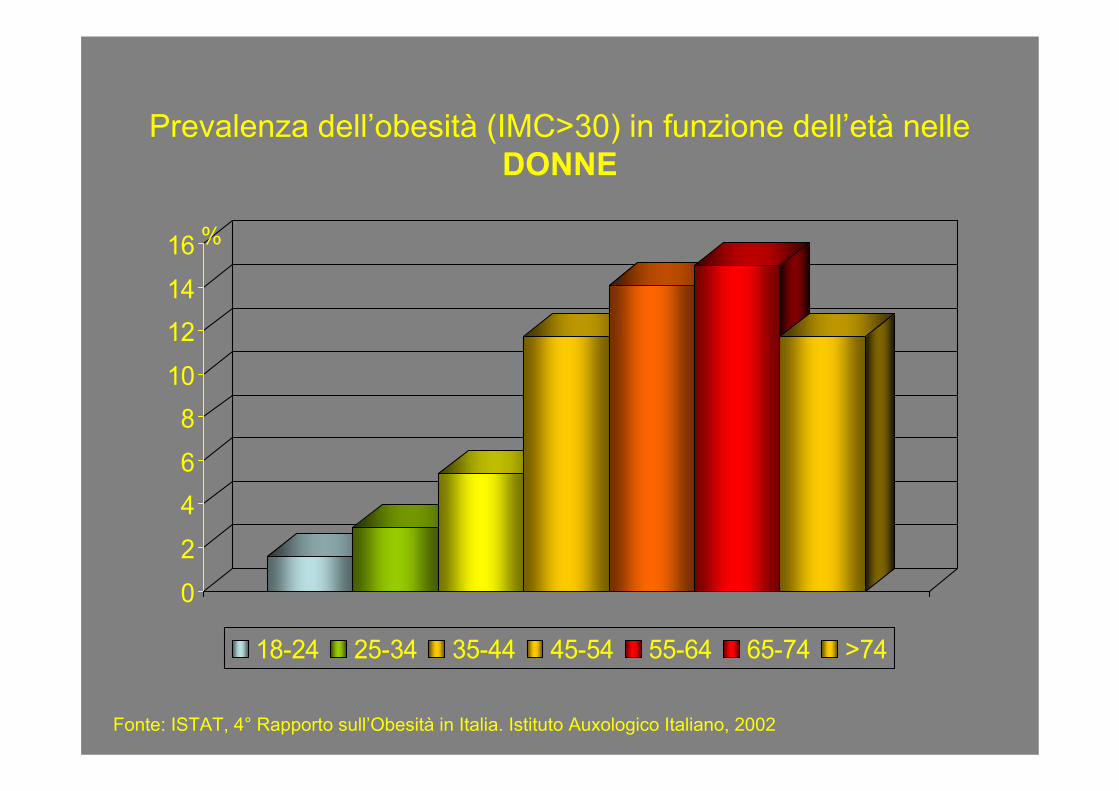
Prevalenza dell’obesità (IMC>30) in funzione dell’età nelle DONNE
0
2
46
810
1214
16
18-24 25-34 35-44 45-54 55-64 65-74 >74
%
Fonte: ISTAT, 4° Rapporto sull’Obesità in Italia. Istituto Auxologico Italiano, 2002
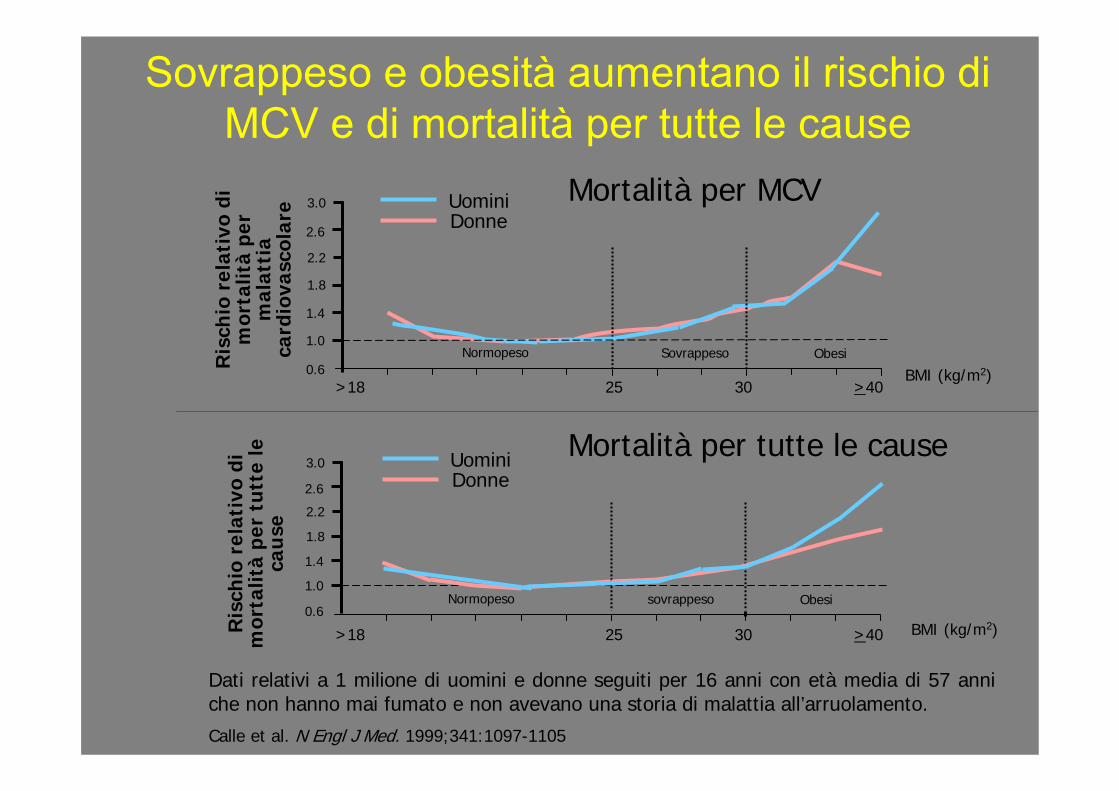
Sovrappeso e obesità aumentano il rischio di MCV e di mortalità per tutte le cause
Dati relativi a 1 milione di uomini e donne seguiti per 16 anni con età media di 57 anni che non hanno mai fumato e non avevano una storia di malattia all’arruolamento.
Calle et al. N Engl J Med. 1999;341:1097-1105
Ris
chio
rel
ativ
o di
mor
talit
àpe
r tu
tte
le
cau
se
Mortalità per tutte le cause
Ris
chio
rel
ativ
o di
m
orta
lità
per
mal
atti
a ca
rdio
vasc
olar
e Mortalità per MCV
0.6
3.0
2.6
2.2
1.8
1.4
1.0
>18 25 30 >40 BMI (kg/m2)
DonneUomini
Normopeso ObesiSovrappeso
BMI (kg/m2)0.6
3.0
2.6
2.2
1.8
1.4
1.0Normopeso Obesi
DonneUomini
sovrappeso
>18 25 30 >40
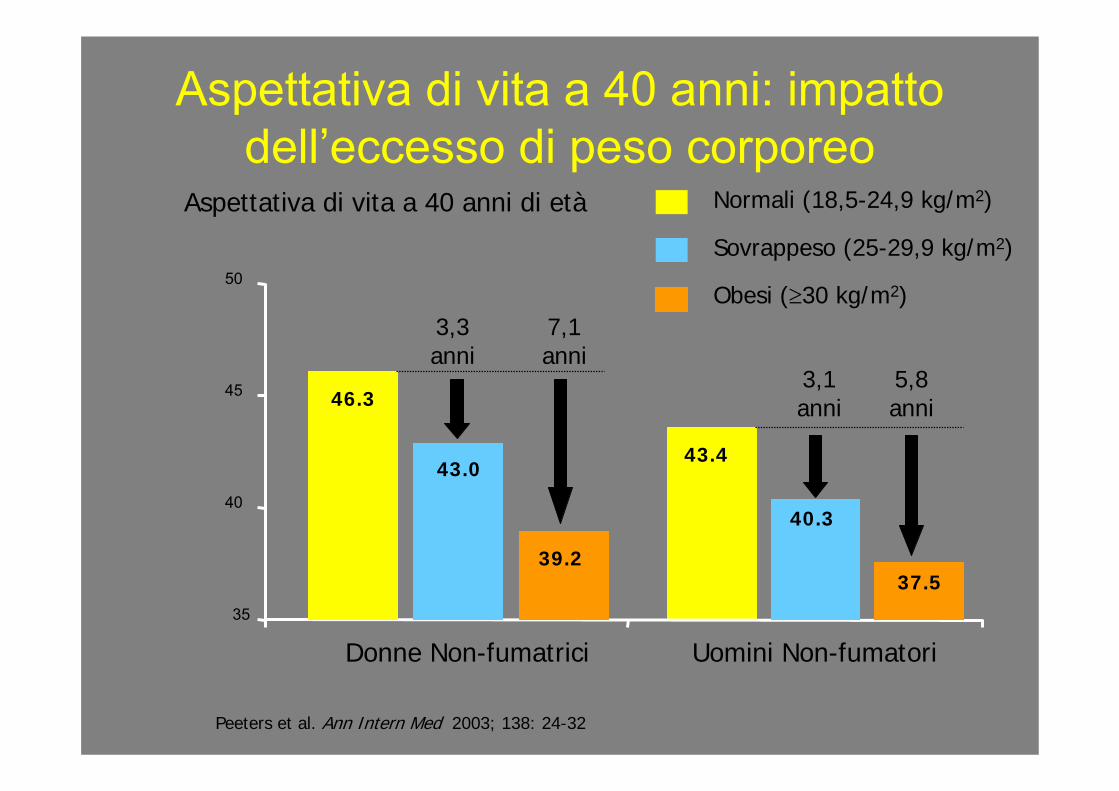
Peeters et al. Ann Intern Med 2003; 138: 24-32
35
40
45
50
Donne Non-fumatrici Uomini Non-fumatori
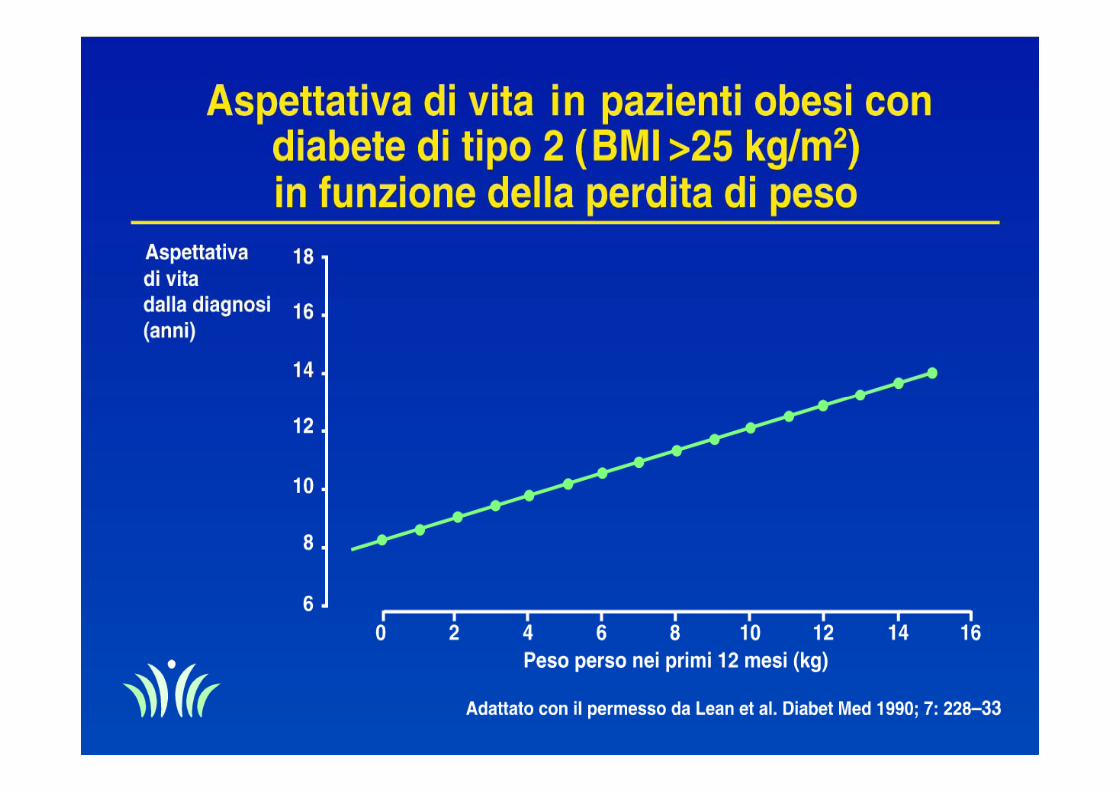
Aspettativa di vita a 40 anni di età Normali (18,5-24,9 kg/m2)
Sovrappeso (25-29,9 kg/m2)
Obesi (≥30 kg/m2)
46.3
43.0
39.2
43.4
40.3
37.5
7,1anni
5,8 anni
3,1 anni
3,3anni
Aspettativa di vita a 40 anni: impatto dell’eccesso di peso corporeo

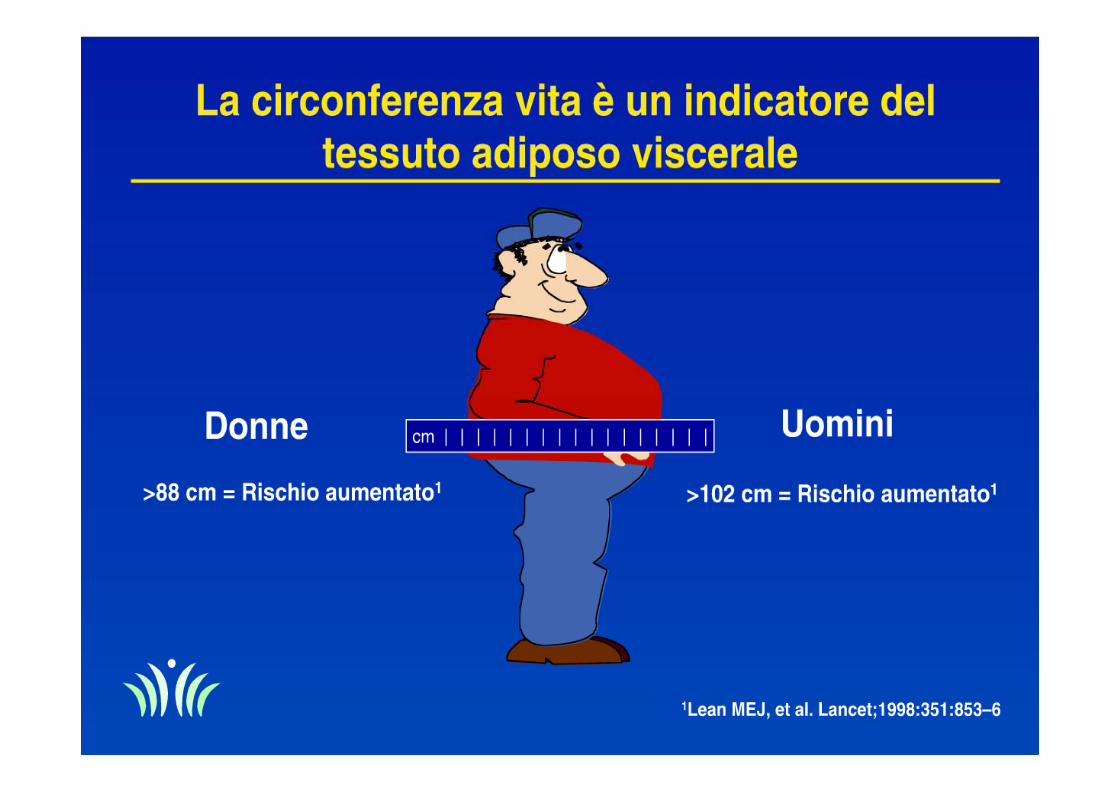
Un parametro fondamentale: la circonferenza addominale
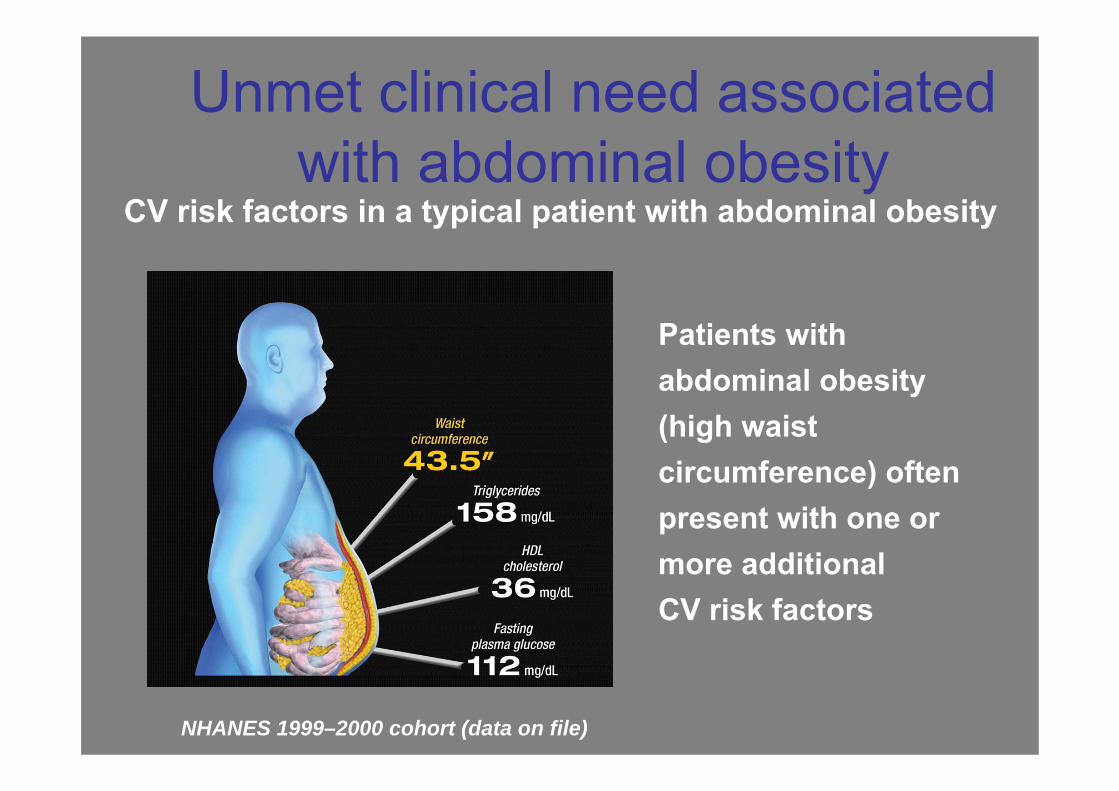
Unmet clinical need associated with abdominal obesity
Patients with abdominal obesity (high waist circumference) often present with one or more additional CV risk factors
NHANES 1999–2000 cohort (data on file)
CV risk factors in a typical patient with abdominal obesity
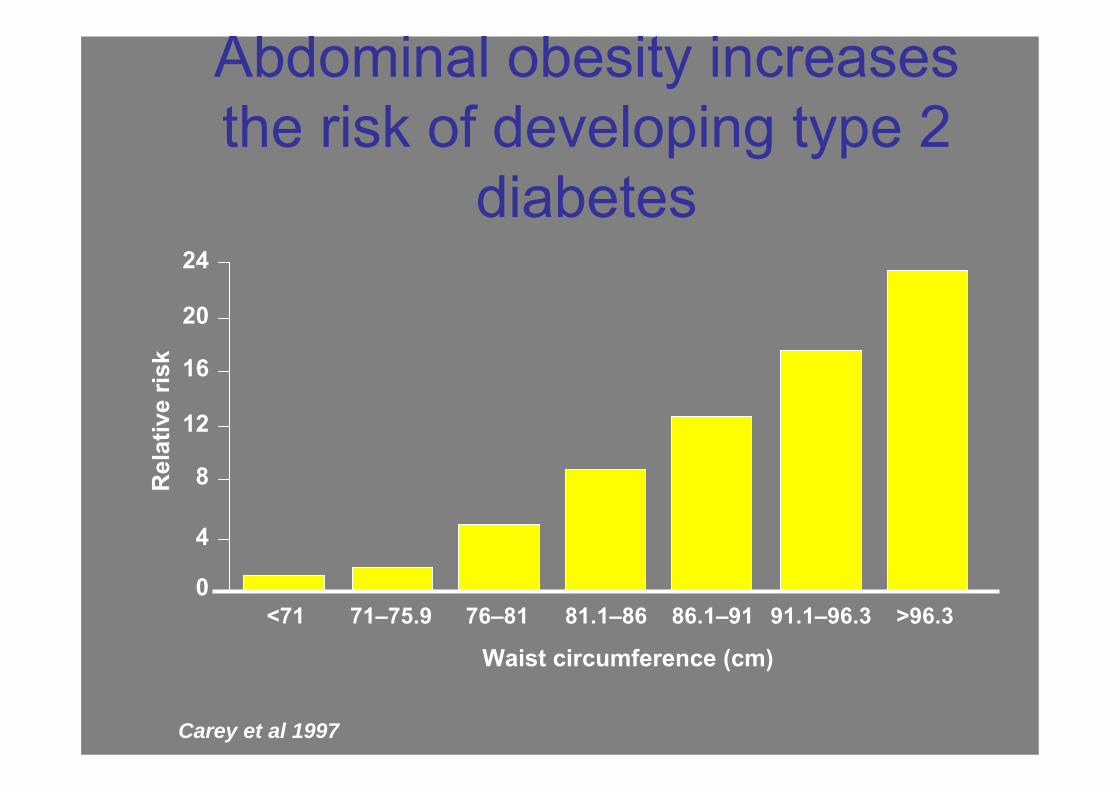
Abdominal obesity increases the risk of developing type 2
diabetes
<71 71–75.9 76–81 81.1–86 86.1–91 91.1–96.3 >96.3
24
20
16
12
8
4
0
Rel
ativ
e ris
k
Waist circumference (cm)
Carey et al 1997
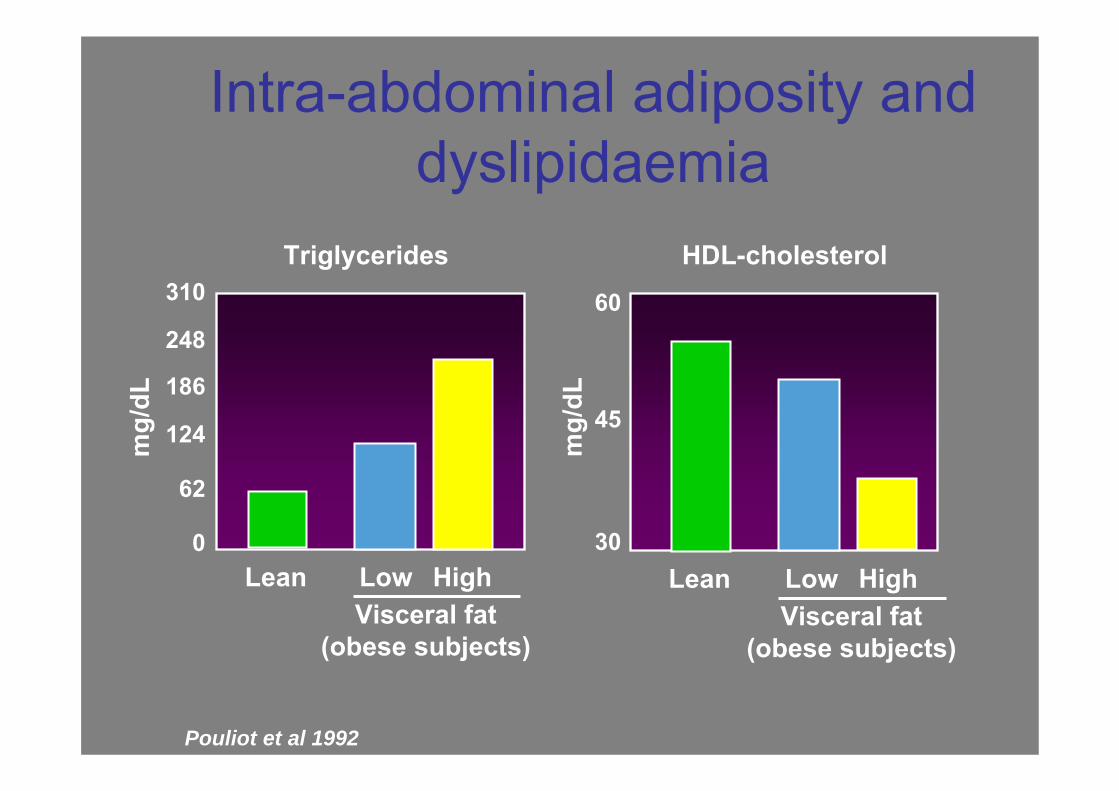
Intra-abdominal adiposity and dyslipidaemia
Pouliot et al 1992
310
248
186
124
62
0
60
45
30m
g/dL
mg/
dL
Triglycerides
Lean
HDL-cholesterol
Visceral fat(obese subjects)
Low High LeanVisceral fat
(obese subjects)
Low High
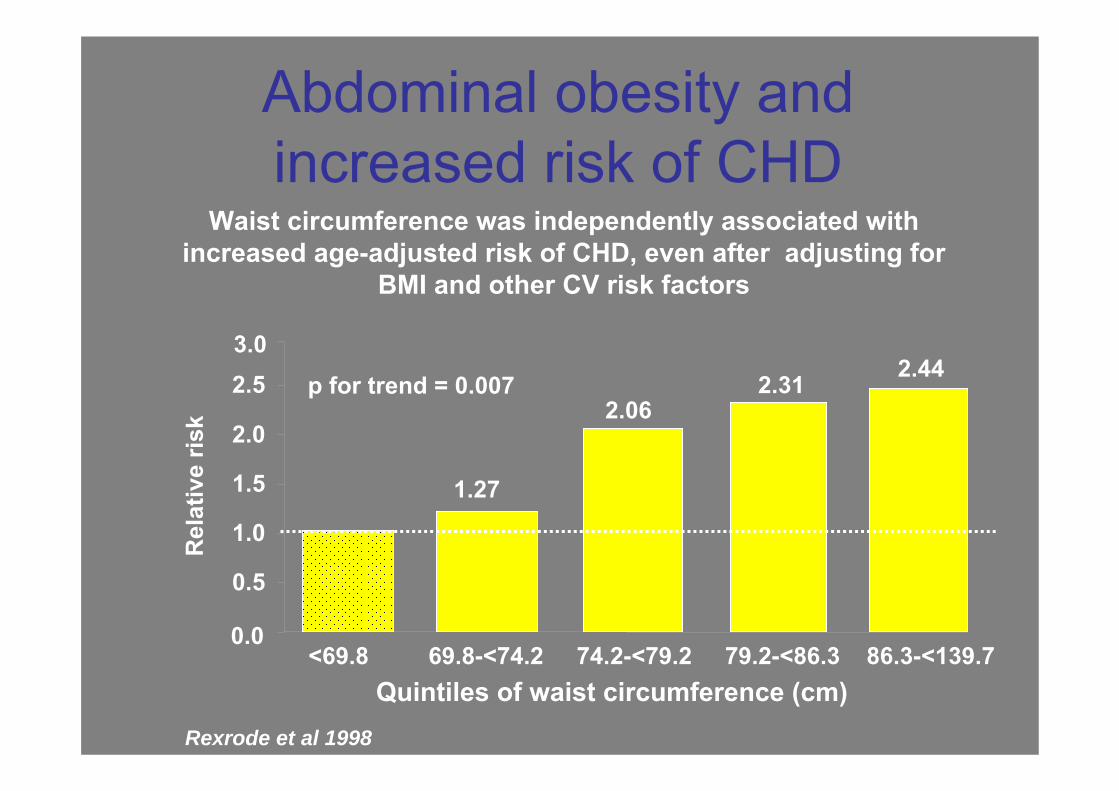
Abdominal obesity andincreased risk of CHD
Waist circumference was independently associated with increased age-adjusted risk of CHD, even after adjusting for
BMI and other CV risk factors
0.0
0.5
1.0
1.5
2.0
2.53.0
<69.8 69.8-<74.2 74.2-<79.2 79.2-<86.3 86.3-<139.7
1.27
2.06 2.31 2.44
p for trend = 0.007
Rel
ativ
e ris
k
Rexrode et al 1998
Quintiles of waist circumference (cm)
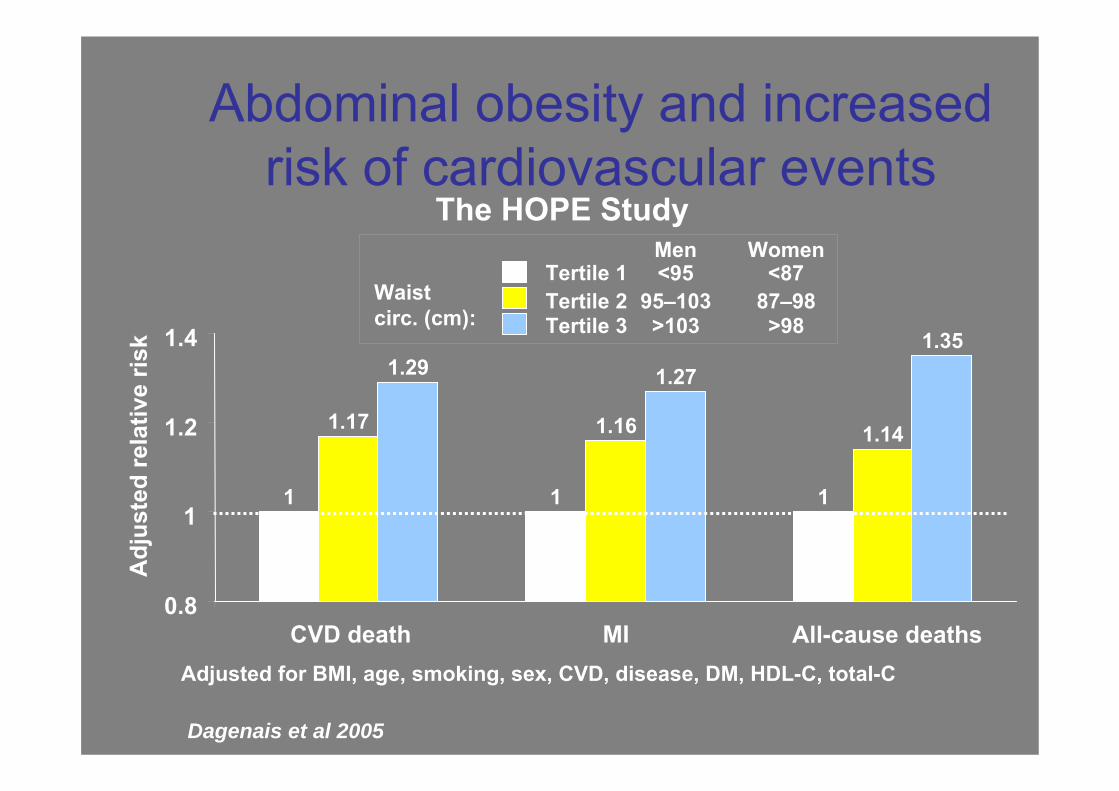
Abdominal obesity and increased risk of cardiovascular events
Dagenais et al 2005
Adj
uste
d re
lativ
e ris
k
1 1 1
1.17 1.16 1.14
1.29 1.271.35
0.8
1
1.2
1.4
CVD death MI All-cause deaths
Tertile 1Tertile 2Tertile 3
Men Women<95
95–103>103
<8787–98>98
Waistcirc. (cm):
Adjusted for BMI, age, smoking, sex, CVD, disease, DM, HDL-C, total-C
The HOPE Study
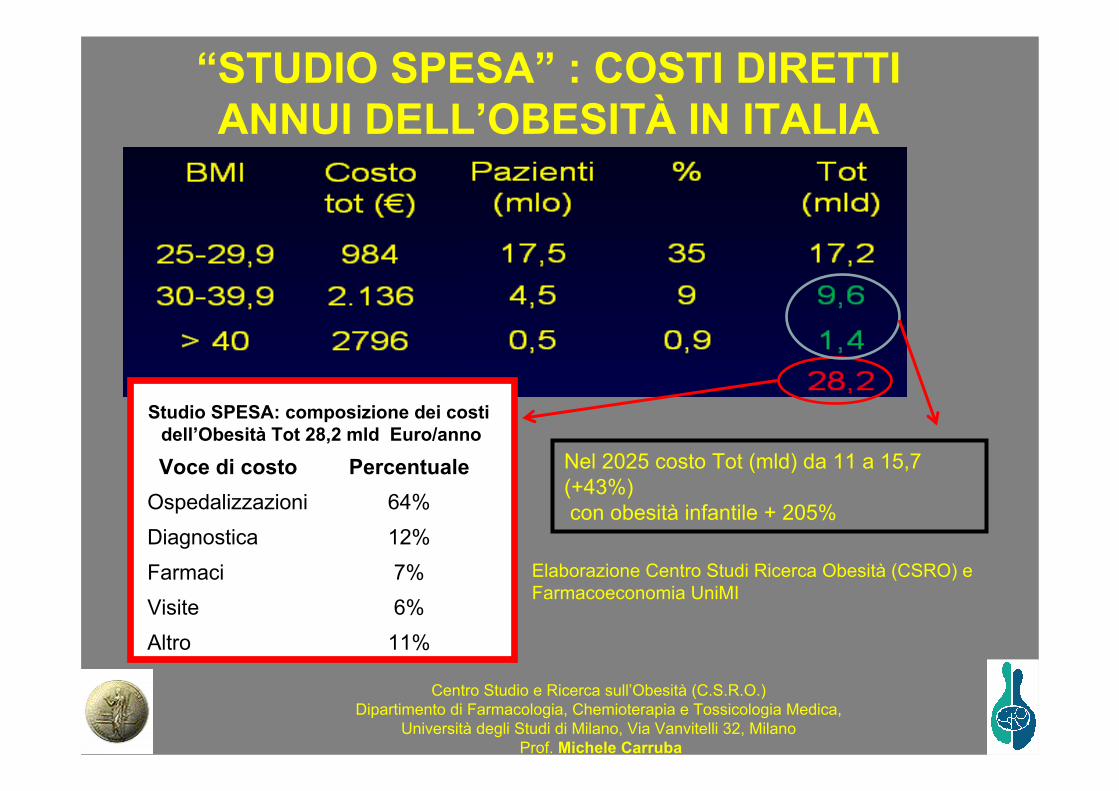
Elaborazione Centro Studi Ricerca Obesità (CSRO) e Farmacoeconomia UniMI
“STUDIO SPESA” : COSTI DIRETTI ANNUI DELL’OBESITÀ IN ITALIA
Nel 2025 costo Tot (mld) da 11 a 15,7 (+43%)con obesità infantile + 205%
Studio SPESA: composizione dei costidell’Obesità Tot 28,2 mld Euro/anno
Voce di costo PercentualeOspedalizzazioni 64%Diagnostica 12%Farmaci 7%Visite 6%Altro 11%
Centro Studio e Ricerca sull’Obesità (C.S.R.O.)Dipartimento di Farmacologia, Chemioterapia e Tossicologia Medica,
Università degli Studi di Milano, Via Vanvitelli 32, MilanoProf. Michele Carruba
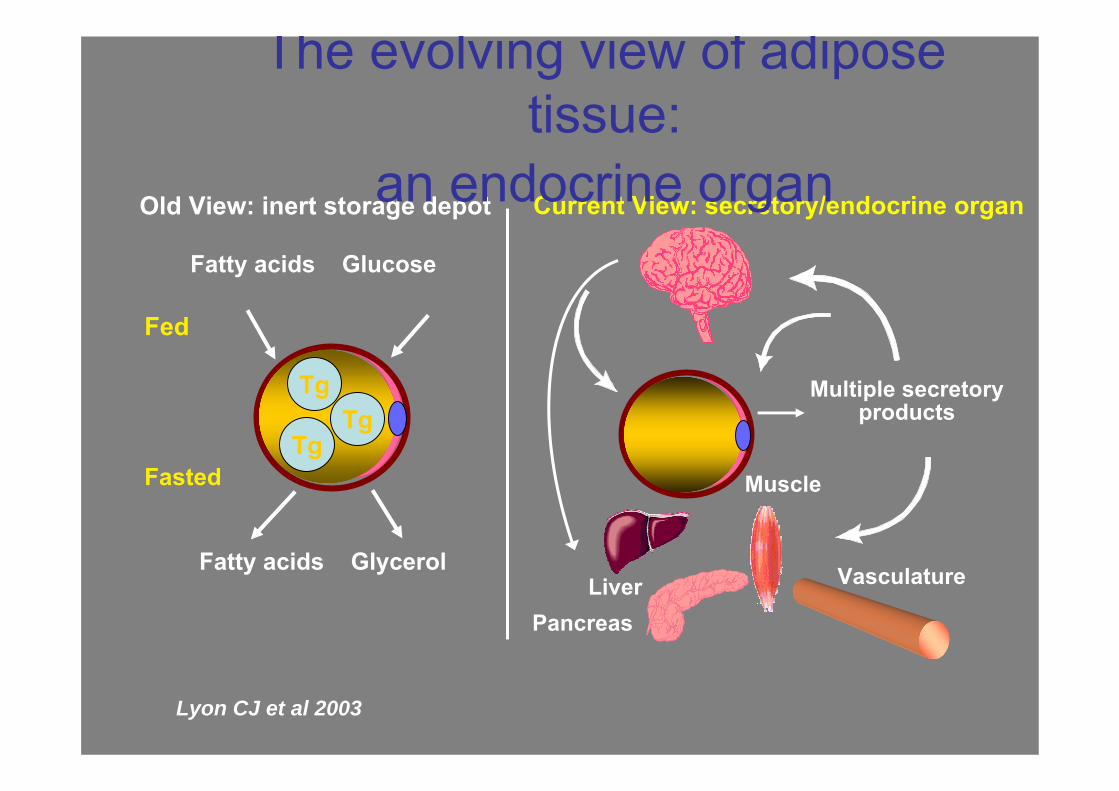
Multiple secretoryproducts
LiverPancreas
Muscle
Vasculature
Current View: secretory/endocrine organOld View: inert storage depot
Fatty acids Glucose
Fatty acids Glycerol
Fed
Fasted
TgTg
Tg
The evolving view of adipose tissue:
an endocrine organ
Lyon CJ et al 2003
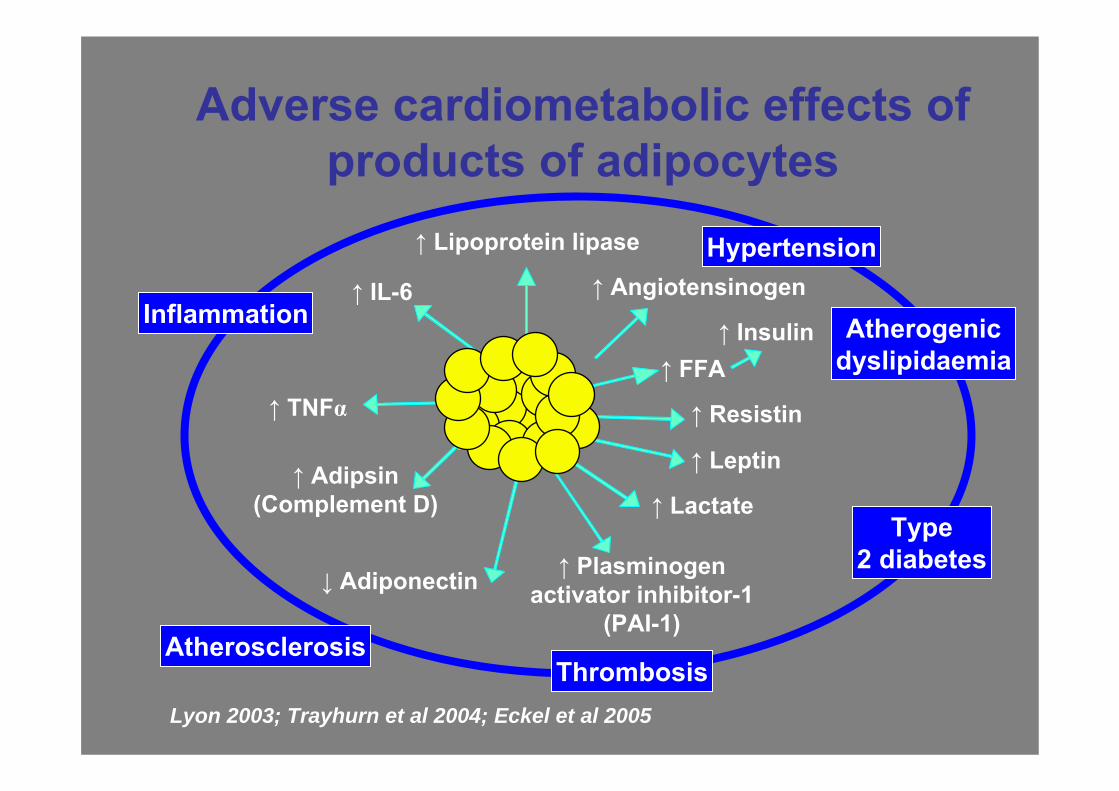
Adverse cardiometabolic effects of products of adipocytes
Adiposetissue
↑ IL-6
↓ Adiponectin
↑ Leptin
↑ TNFα
↑ Adipsin(Complement D)
↑ Plasminogenactivator inhibitor-1
(PAI-1)
↑ Resistin
↑ FFA↑ Insulin
↑ Angiotensinogen
↑ Lipoprotein lipase
↑ Lactate
Inflammation
Type2 diabetes
Hypertension
Atherogenicdyslipidaemia
ThrombosisAtherosclerosis
Lyon 2003; Trayhurn et al 2004; Eckel et al 2005
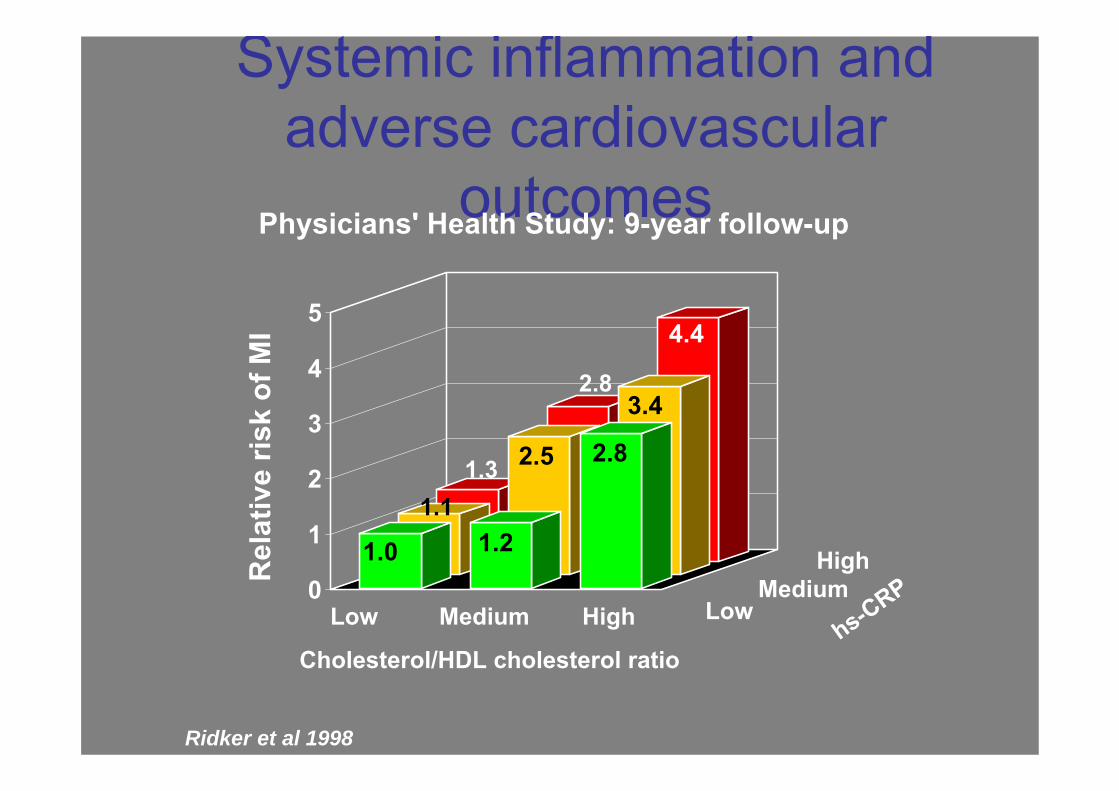
Systemic inflammation and adverse cardiovascular
outcomes
0
1
2
3
4
5
Rel
ativ
e ris
k of
MI
Cholesterol/HDL cholesterol ratiohs-CRP
1.0 1.2
2.8
1.11.3 2.5
3.4
4.4
Low LowMedium
High
Medium High
Physicians' Health Study: 9-year follow-up
Ridker et al 1998
2.8
Science 299: 896-899, 2003
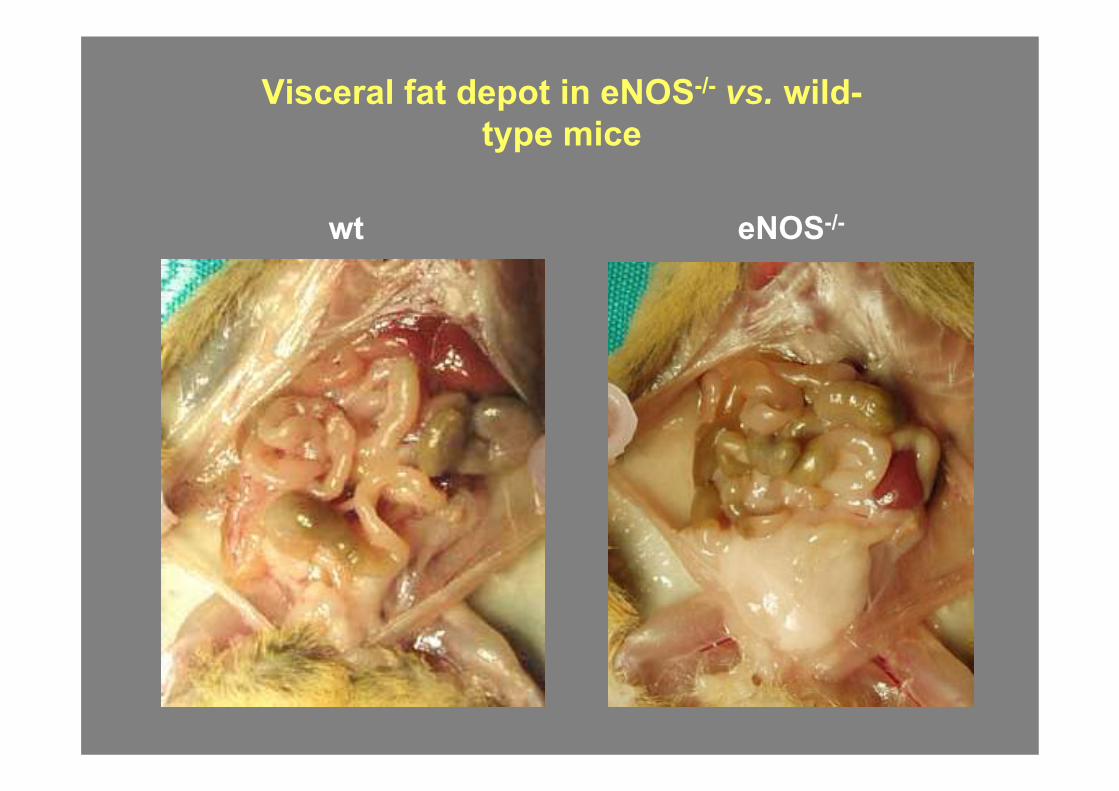
Visceral fat depot in eNOS-/- vs. wild-type mice
wt eNOS-/-
4545
55
40403535
3030252520201515
1010
00
4545
55
40403535
3030252520201515
1010
0044 88 1212 1616 2020 2424 2828 3232 3636 4040 4444 4848 5252 44 88 1212 1616 2020 2424 2828 3232 3636 4040 4444 4848 5252
Bod
y w
eigh
t (g)
Bod
y w
eigh
t (g)
Bod
y w
eigh
t (g)
Bod
y w
eigh
t (g)
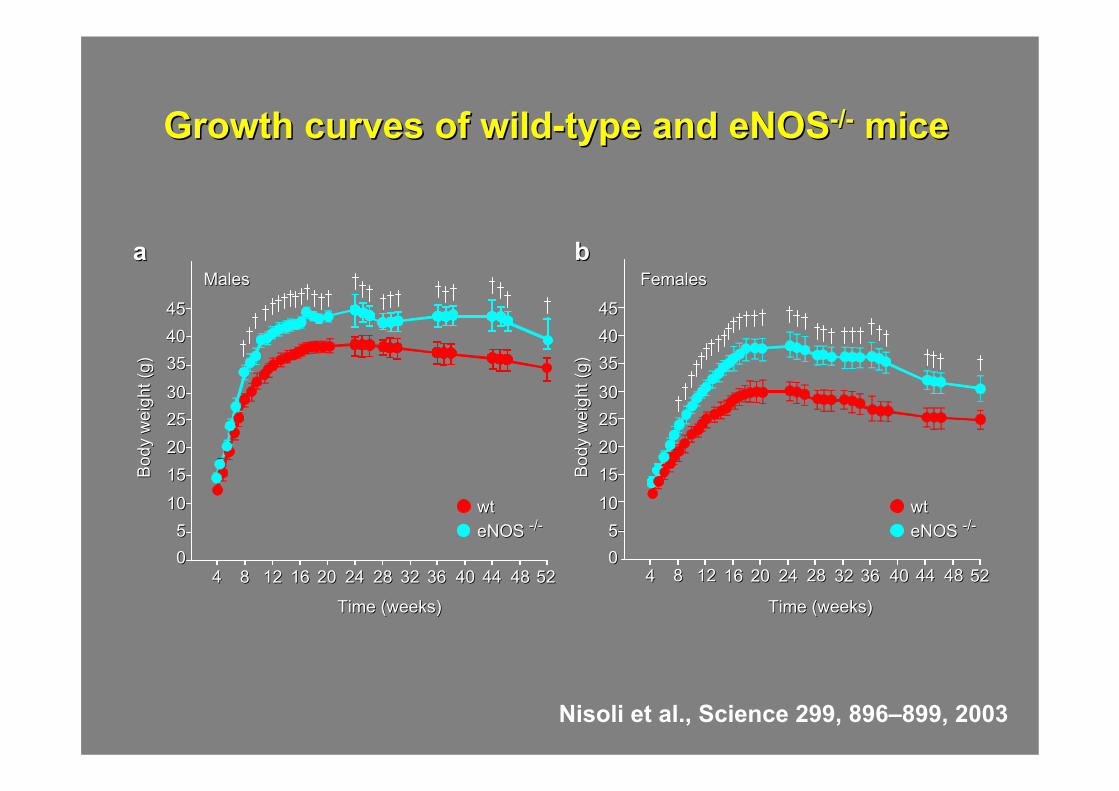
MalesMales FemalesFemales
Time (weeks)Time (weeks) Time (weeks)Time (weeks)
aa bb
Growth curves of wildGrowth curves of wild--type and eNOStype and eNOS--//-- micemice
wtwteNOS eNOS --//--
wtwteNOS eNOS --//--
Nisoli et al., Science 299, 896–899, 2003
SWISS MED WKLY 133: 360–363, 2003
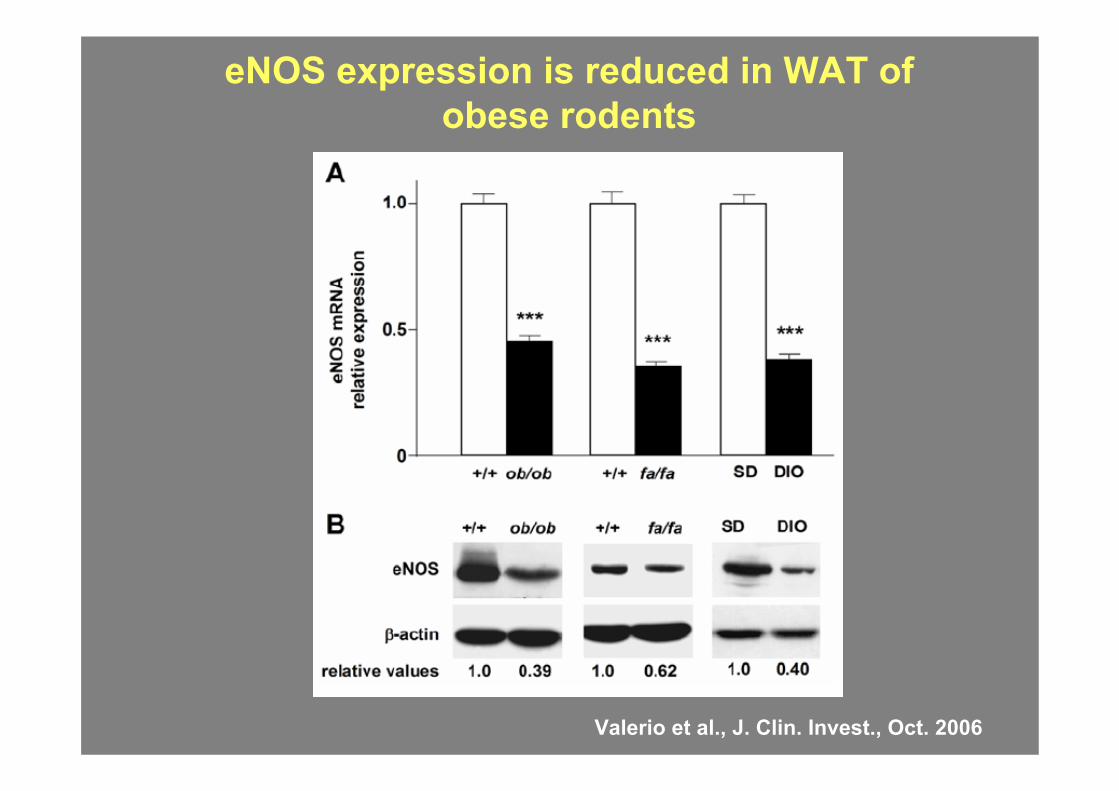
eNOS expression is reduced in WAT of obese rodents
Valerio et al., J. Clin. Invest., Oct. 2006
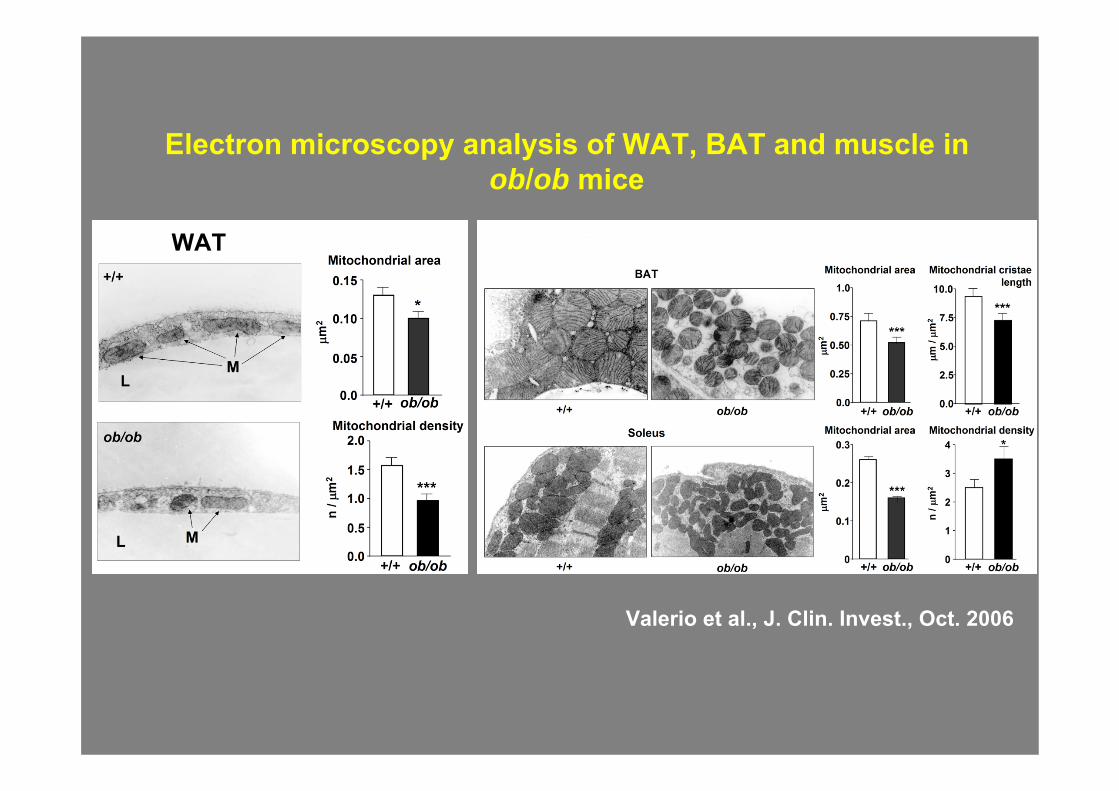
Electron microscopy analysis of WAT, BAT and muscle in ob/ob mice
WAT
Valerio et al., J. Clin. Invest., Oct. 2006
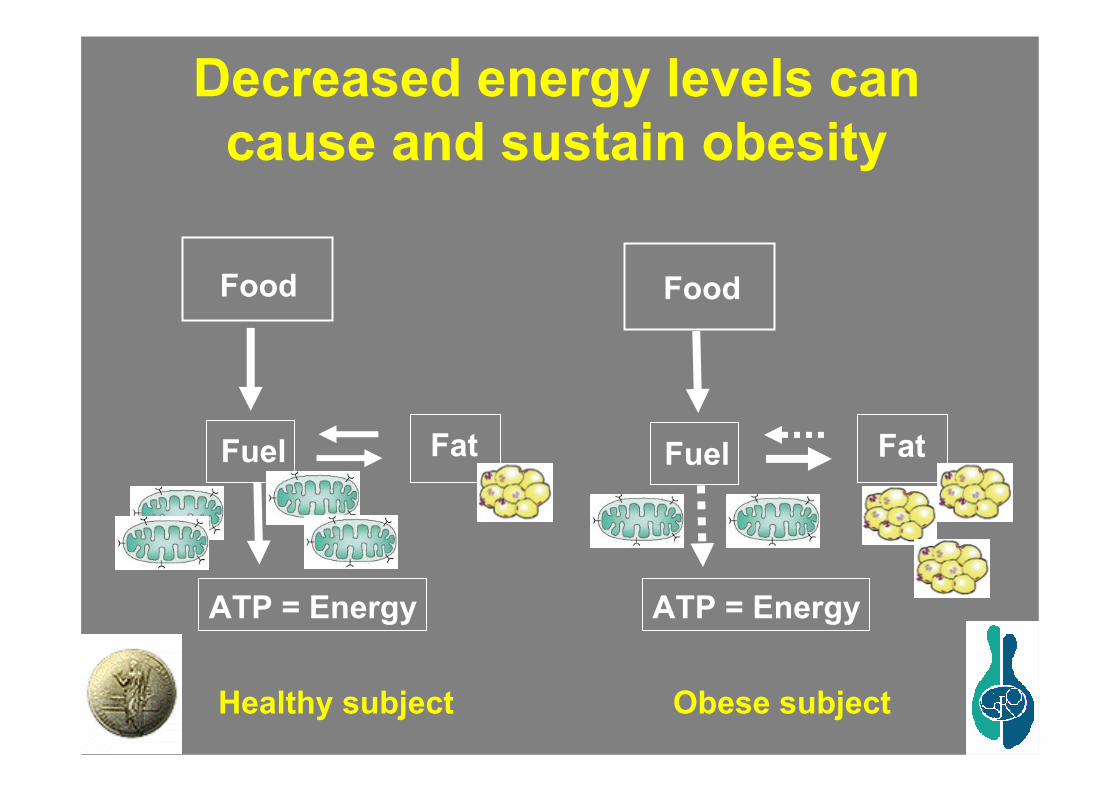
Decreased energy levels can cause and sustain obesity
Food
Fuel
ATP = Energy
Fat
Food
Fuel
ATP = Energy
Fat
Healthy subject Obese subject
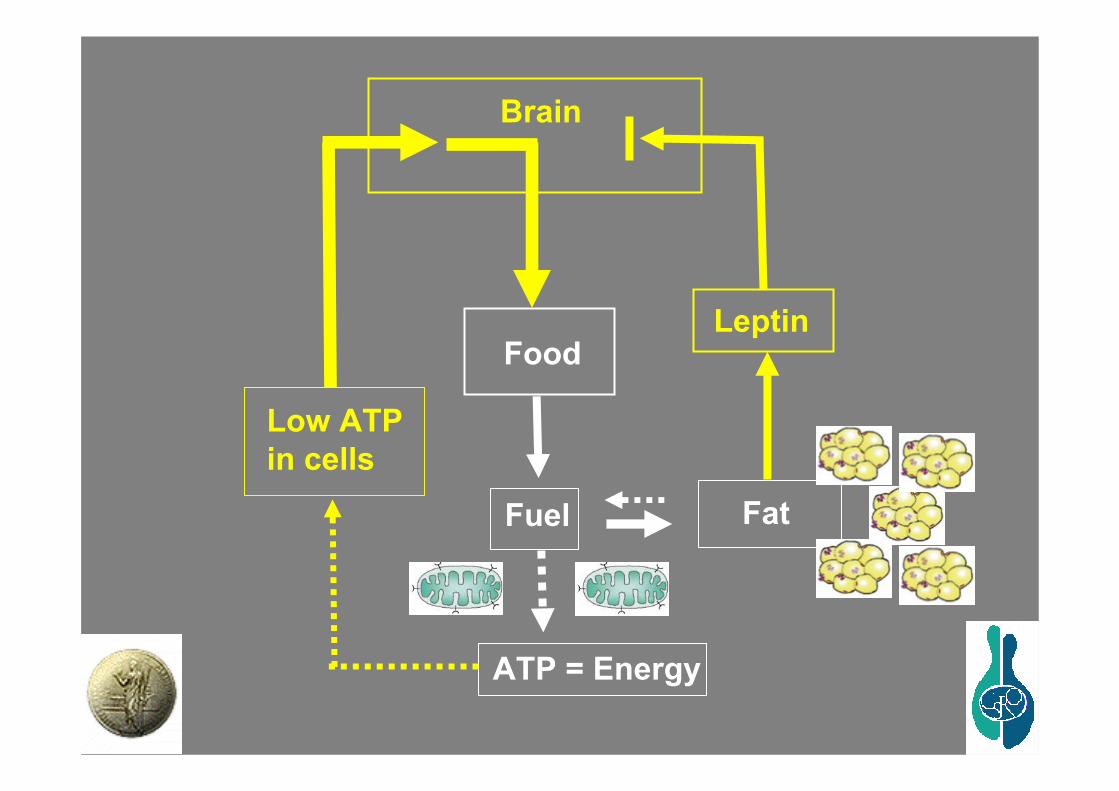
Food
Fuel
ATP = Energy
Fat
Low ATPin cells
Brain
Leptin
Sience October 14, 2005
Quindi? Stile di vita!
Abitudini alimentari
eAttività fisica
We conducted a population-based, prospective investigation involving 22,043 adults in Greece who completed an extensive, validated, food-frequency questionnaire at base line.
During a median of 44 months of follow-up, there were 275 deaths. A higher degree of adherence to the Mediterranean diet was associated with a reduction in total mortality.
An inverse association with greater adherence to this diet was evident for both death due to coronary heart disease and death due to cancer.
Conclusions. Greater adherence to the traditional Mediterranean diet is associated with a significant reduction in total mortality.
Adherence to a Mediterranean Diet and Survival in a Greek Population
Antonia Trichopoulou, M.D., Tina Costacou, Ph.D., Christina Bamia, Ph.D., and Dimitrios Trichopoulos, M.D.
The New England Journal of Medicine, 348: 2599-2608, 2003
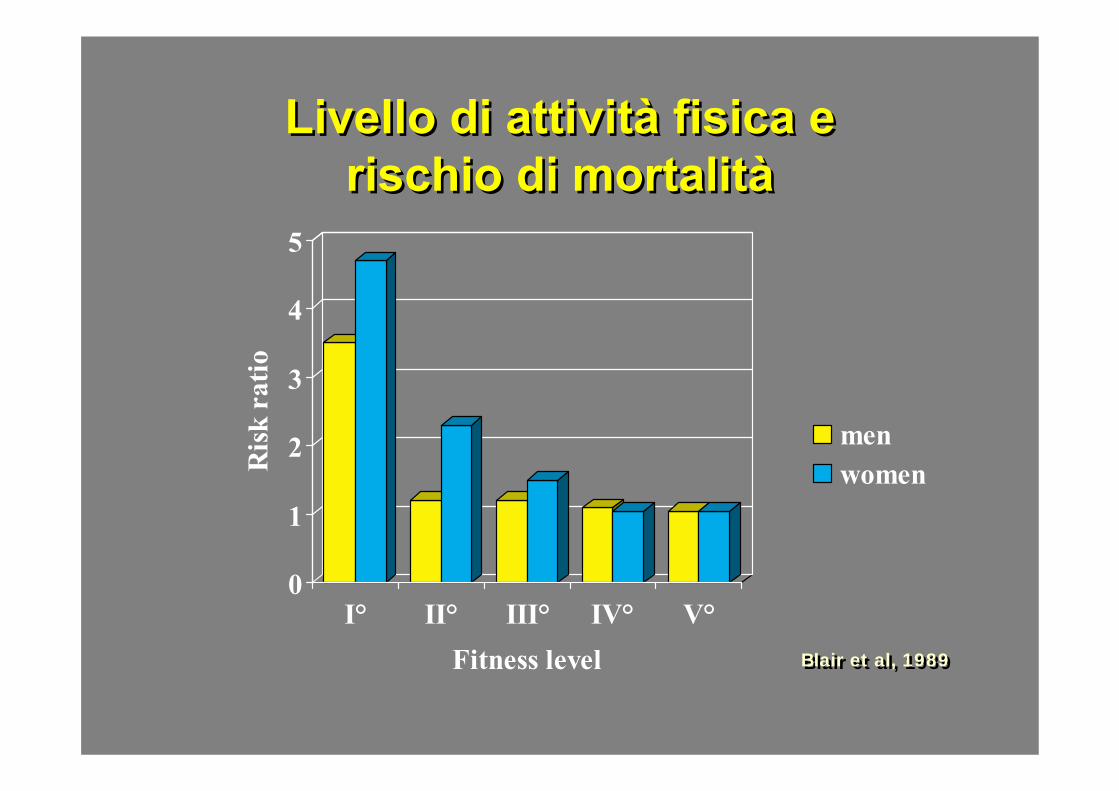
Livello di attività fisica e rischio di mortalità
Livello di attività fisica e rischio di mortalità
0
1
2
3
4
5R
isk
ratio
I° II° III° IV° V°Fitness level
menwomen
Blair et al, 1989Blair et al, 1989
Integrated Laboratories Network (InLaNe)
Center for Study and Research on Obesity, University of Milan
Michele Carruba, M.D. Ph.D.Enzo Nisoli, M.D. Ph.D. Cristina Tonello, Ph.D.Valeria Cozzi, Ph.D.Laura Tedesco, Ph.D. Annalisa Cardile, Ph.D. studentRenata Bracale, Ph.D. Student
DIBIT, S. Raffaele HMilan (Italy) and University of Milan
Emilio Clementi, M.D.Ph.D.Sestina Falcone, Ph.D.Addolorata Pisconti, Ph.D.
Istituto di Farmacologia e Farmacognosia, University of Urbino “Carlo Bo”, Urbino (Italy)
Orazio Cantoni, M.D. Ph.D.Letizia Palomba, Ph.D.
Department of Biomedical Sciences and Biotechnologies, University of Brescia (Italy)
Alessandra Valerio, M.D. Ph.D.Marta Dossena, Ph.D. student

Diabetes Care 28: 2289-2304, 2005
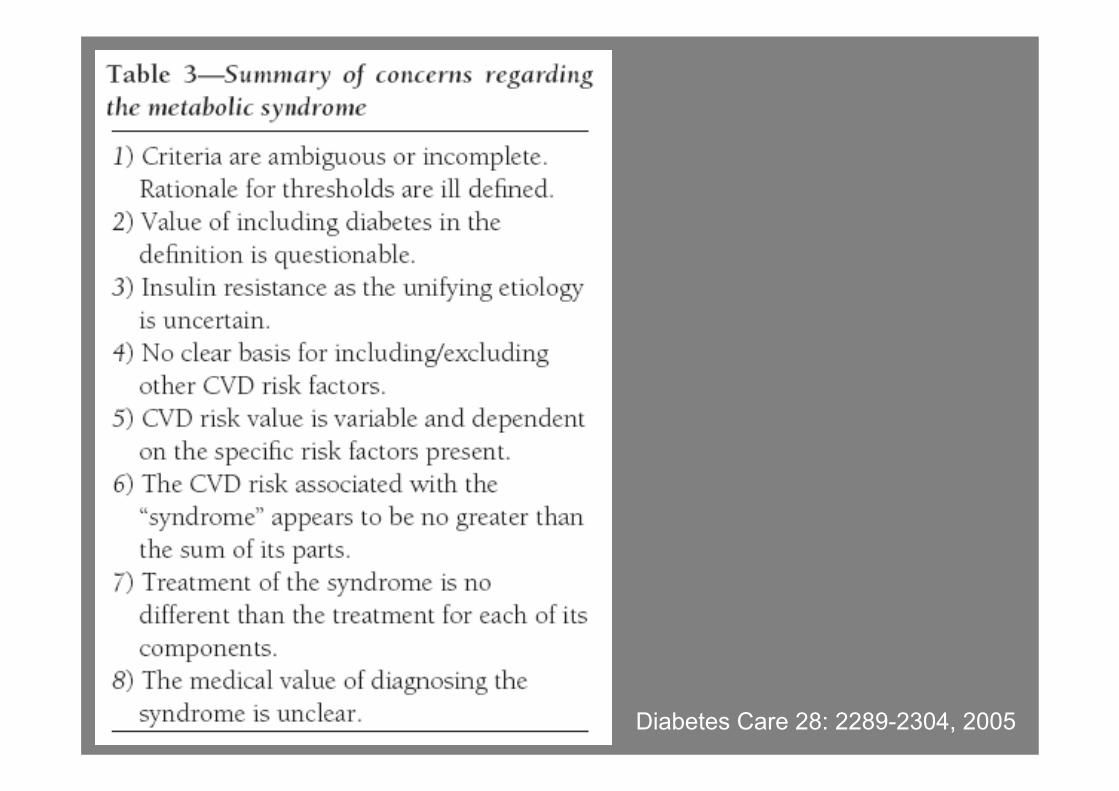
Diabetes Care 28: 2289-2304, 2005
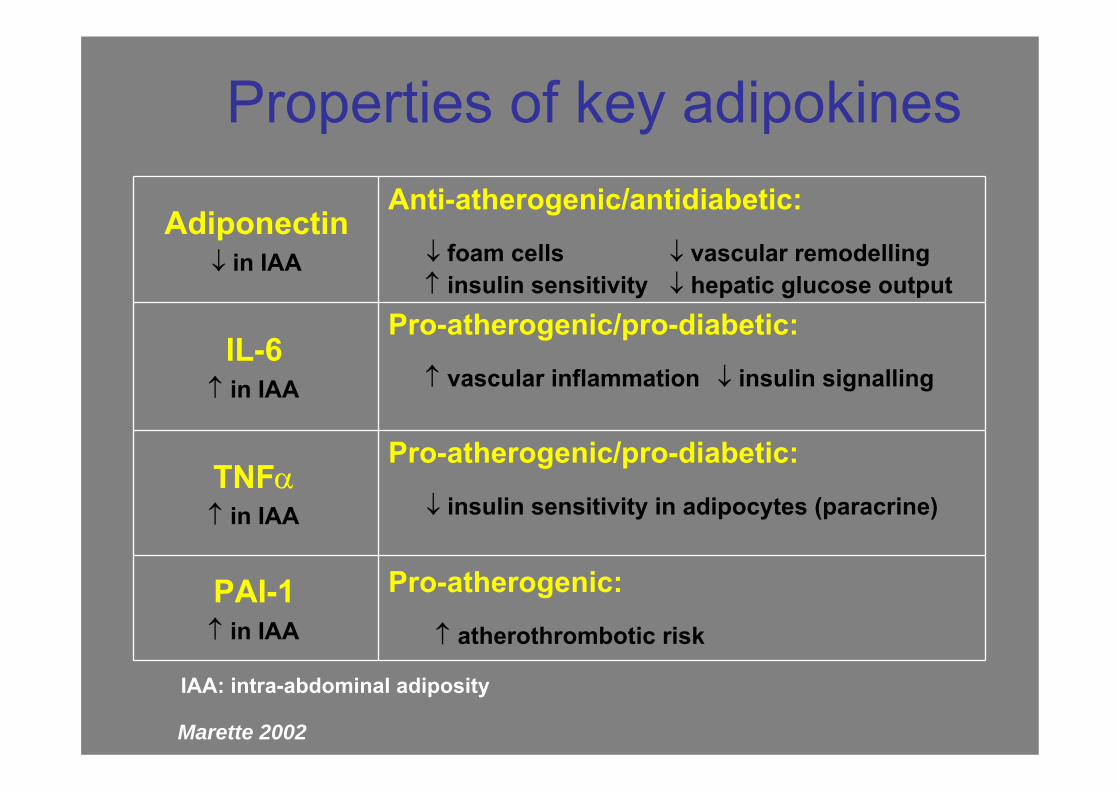
Adiponectin↓ in IAA
Anti-atherogenic/antidiabetic:
↓ foam cells ↓ vascular remodelling↑ insulin sensitivity ↓ hepatic glucose output
IL-6↑ in IAA
Pro-atherogenic/pro-diabetic:
↑ vascular inflammation ↓ insulin signalling
TNFα↑ in IAA
Pro-atherogenic/pro-diabetic:
↓ insulin sensitivity in adipocytes (paracrine)
PAI-1↑ in IAA
Pro-atherogenic:
↑ atherothrombotic risk
Properties of key adipokines
IAA: intra-abdominal adiposity
Marette 2002
Overweight, Obesity, and Mortality from Cancer in a Prospectively Studied Cohort of U.S. Adults
Eugenia E. Calle, Ph.D., Carmen Rodriguez, M.D., M.P.H., Kimberly Walker-Thurmond, B.A., and Michael J. Thun, M.D.
The New England Journal of Medicine, 348: 1625-1638, 2003
The heaviest members of this cohort (body-mass index of at least 40) had death rates from all cancers combined that were 52 percent higher (for men) and 62 percent higher (for women) than the rates in men and women of normal weight.
In both men and women, body-mass index was also significantly associated with higher rates of death due to cancer of the esophagus, colon and rectum, liver, gallbladder, pancreas, and kidney; the same was true for death due to non-Hodgkin's lymphoma and multiple myeloma. Significant trends of increasing risk with higher body-mass-index values were observed for death from cancers of the stomach and prostate in men and for death from cancers of the breast, uterus, cervix, and ovary in women.
Conclusions. Increased body weight was associated with increased death rates for all cancers combined and for cancers at multiple specific sites.
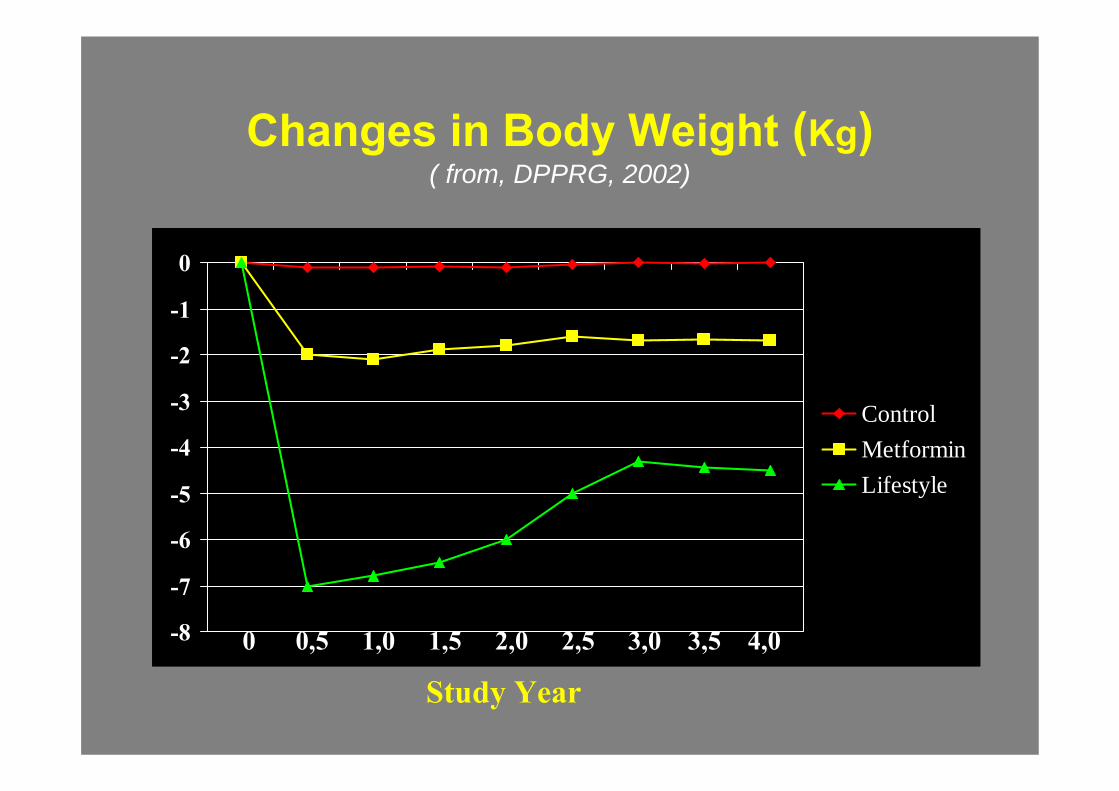
Changes in Body Weight (Kg)( from, DPPRG, 2002)
Study Year
-8
-7
-6
-5
-4
-3
-2
-1
0
ControlMetforminLifestyle
0 0,5 1,0 1,5 2,0 2,5 3,0 3,5 4,0
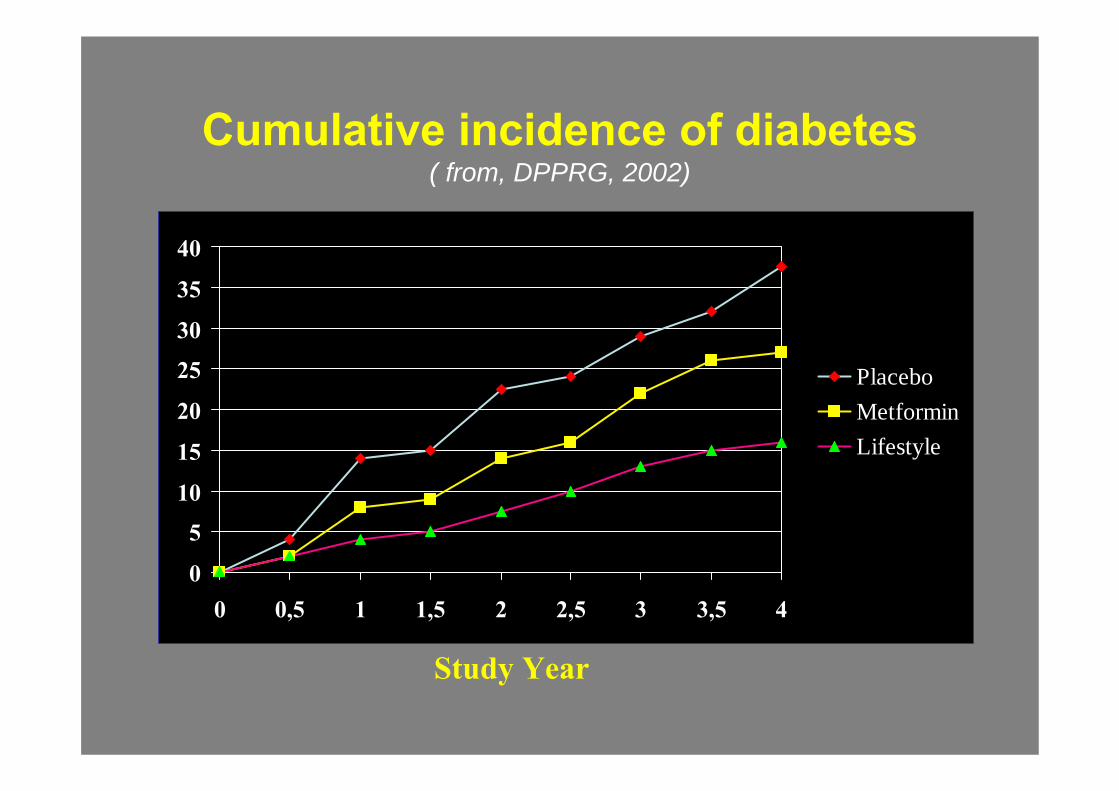
Cumulative incidence of diabetes( from, DPPRG, 2002)
Study Year
0
5
10
15
20
25
30
35
40
0 0,5 1 1,5 2 2,5 3 3,5 4
PlaceboMetforminLifestyle
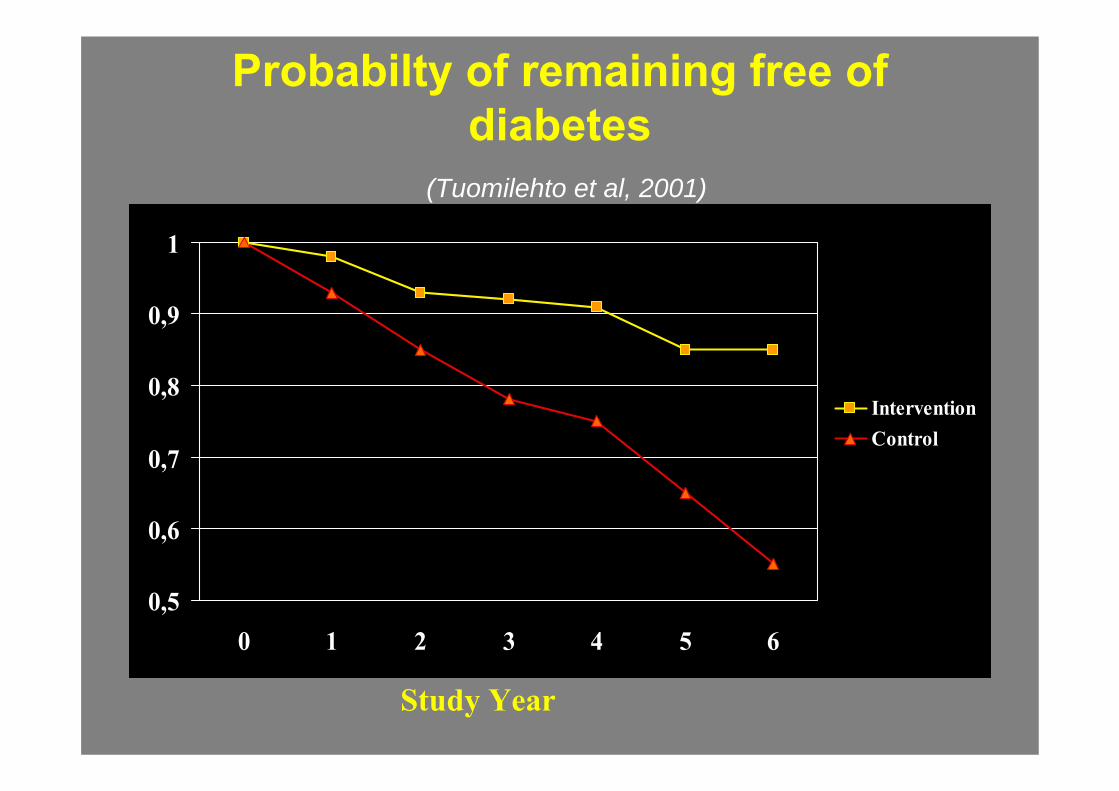
Probabilty of remaining free of diabetes
(Tuomilehto et al, 2001)
0,5
0,6
0,7
0,8
0,9
1
0 1 2 3 4 5 6
InterventionControl
Study Year
DALLA RICERCA AL TERRITORIOIl Rischio
• Ogni anno 270.000 soggetti vengono colpiti da un attacco cardiaco che è fatale nel 50% dei casi e non arriva neanche al ricovero nel 30% dei casi
• Nell’analisi Framingham Study si èrivoluzionato il concetto di rischio: non piùsingoli fattori (fumo, ipertensione, ipercolesterolemia), ma una valutazione del Rischio Assoluto derivante da un’analisi multifattoriale

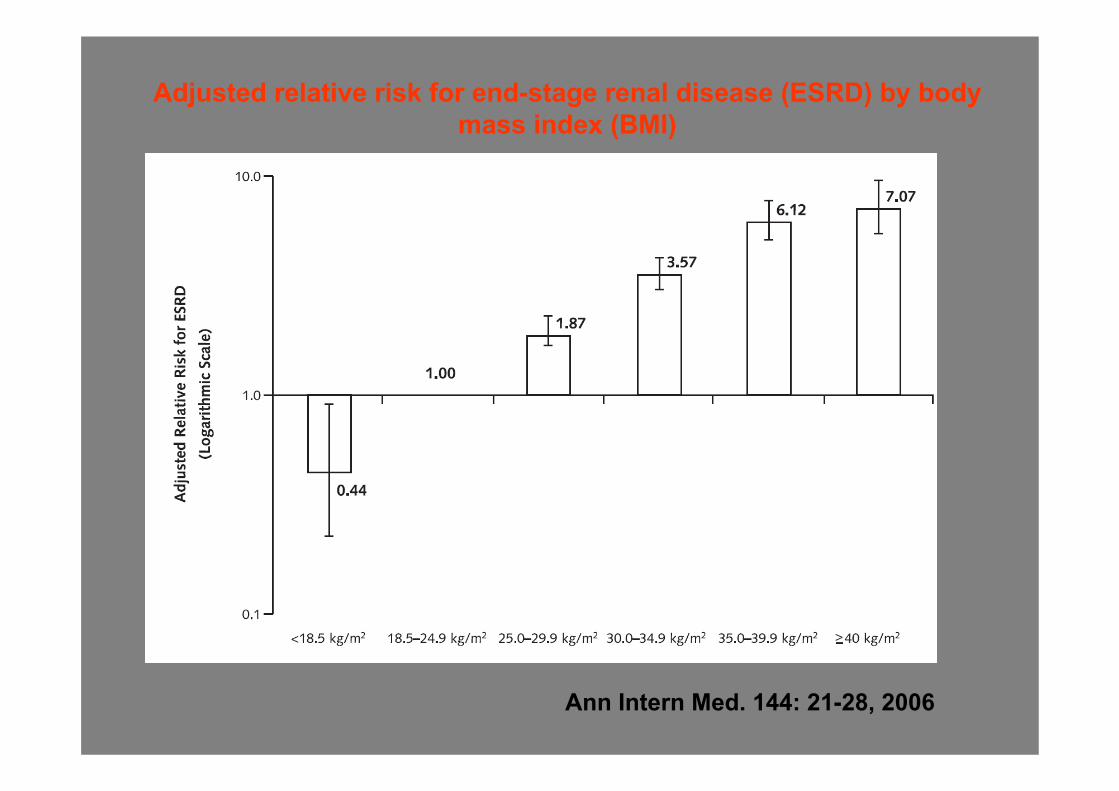
Adjusted relative risk for end-stage renal disease (ESRD) by body mass index (BMI)
Ann Intern Med. 144: 21-28, 2006
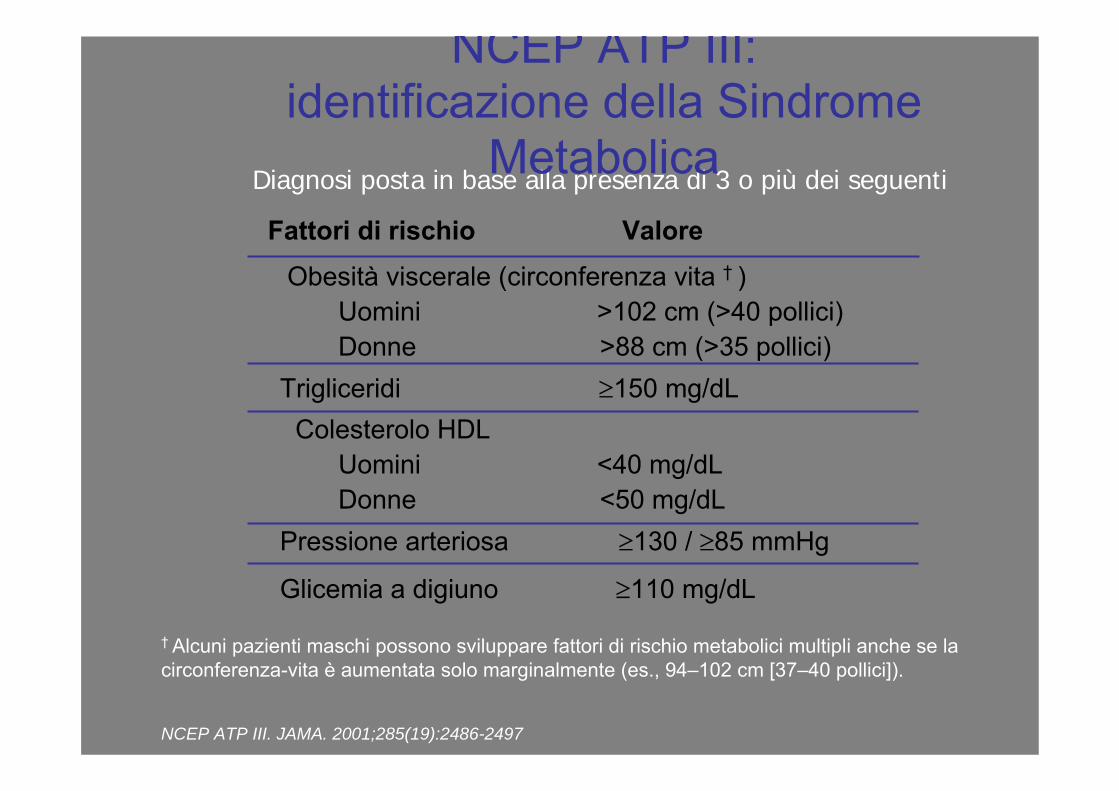
Obesità viscerale (circonferenza vita † )Uomini >102 cm (>40 pollici)Donne >88 cm (>35 pollici)
Trigliceridi ≥150 mg/dLColesterolo HDL
Uomini <40 mg/dLDonne <50 mg/dL
Pressione arteriosa ≥130 / ≥85 mmHg
Glicemia a digiuno ≥110 mg/dL
† Alcuni pazienti maschi possono sviluppare fattori di rischio metabolici multipli anche se la circonferenza-vita è aumentata solo marginalmente (es., 94–102 cm [37–40 pollici]).
NCEP ATP III. JAMA. 2001;285(19):2486-2497
Diagnosi posta in base alla presenza di 3 o più dei seguenti
NCEP ATP III:identificazione della Sindrome
MetabolicaFattori di rischio Valore
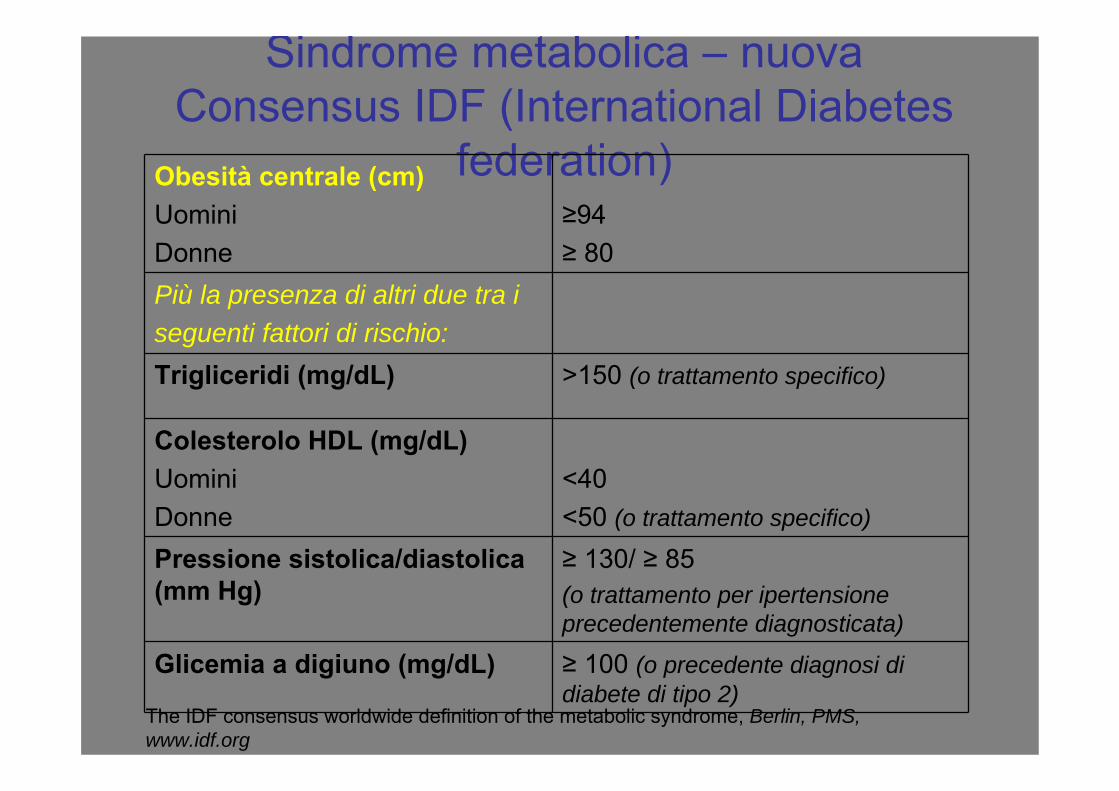
Sindrome metabolica – nuova Consensus IDF (International Diabetes
federation)Obesità centrale (cm)UominiDonne
≥94≥ 80
Più la presenza di altri due tra iseguenti fattori di rischio:Trigliceridi (mg/dL) >150 (o trattamento specifico)
Colesterolo HDL (mg/dL)UominiDonne
<40<50 (o trattamento specifico)
Pressione sistolica/diastolica (mm Hg)
≥ 130/ ≥ 85(o trattamento per ipertensione precedentemente diagnosticata)
Glicemia a digiuno (mg/dL) ≥ 100 (o precedente diagnosi di diabete di tipo 2)
The IDF consensus worldwide definition of the metabolic syndrome, Berlin, PMS, www.idf.org
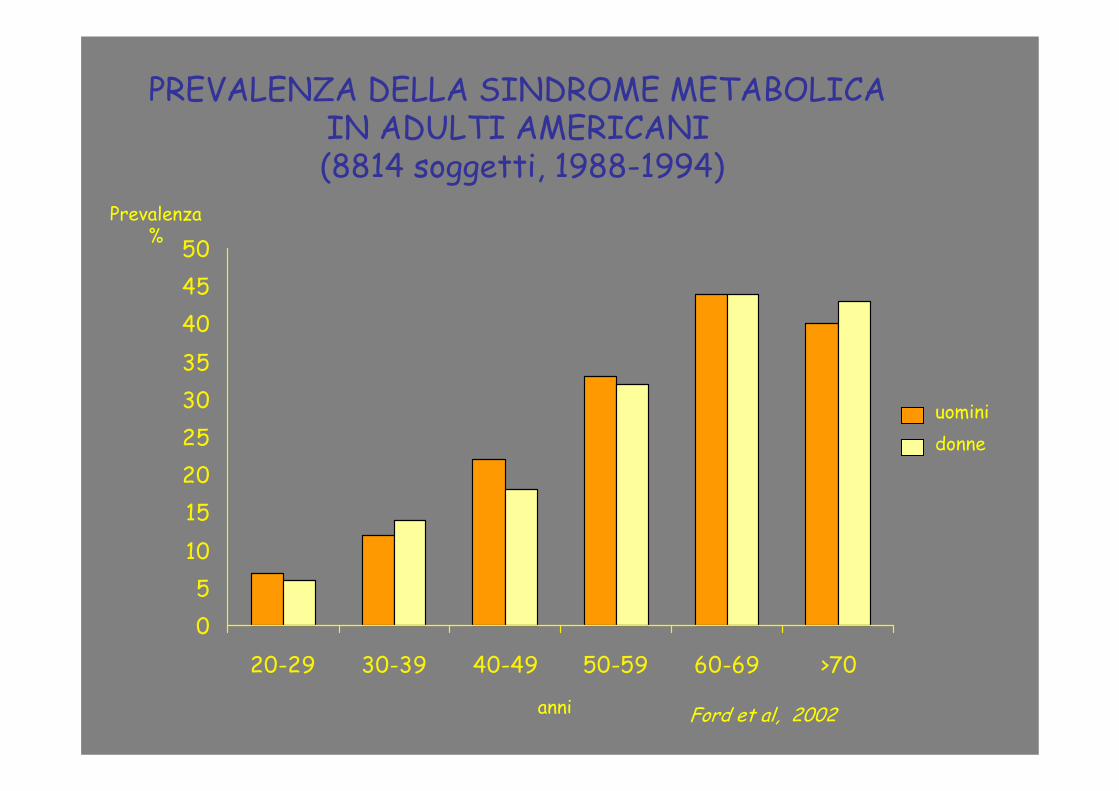
05
101520253035404550
20-29 30-39 40-49 50-59 60-69 >70
uominidonne
Prevalenza%
PREVALENZA DELLA SINDROME METABOLICA IN ADULTI AMERICANI(8814 soggetti, 1988-1994)
anni Ford et al, 2002
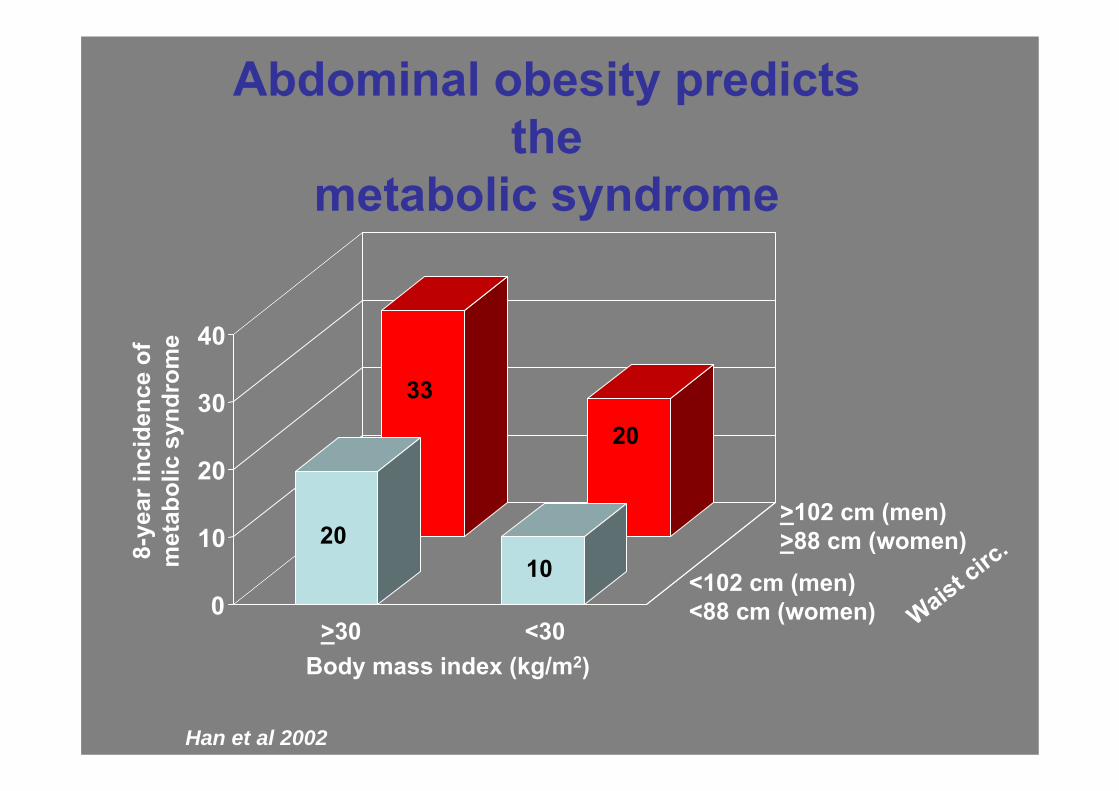
Abdominal obesity predicts the
metabolic syndrome
>30 <30
<102 cm (men)<88 cm (women)
>102 cm (men)>88 cm (women)
Waist circ
.
Body mass index (kg/m2)
8-ye
ar in
cide
nce
ofm
etab
olic
syn
drom
e
Han et al 2002
33
20
2010
0
10
20
30
40
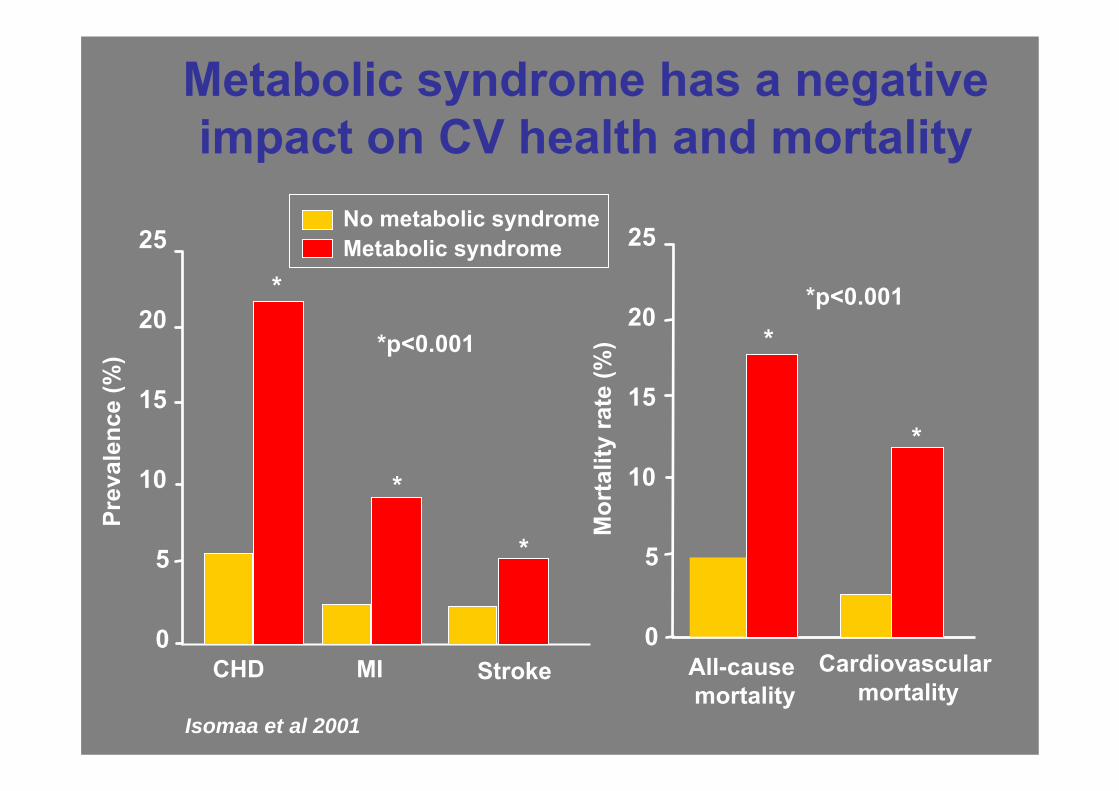
Metabolic syndrome has a negative impact on CV health and mortality
0
5
10
15
20
25
CHD MI Stroke
Prev
alen
ce (%
)
No metabolic syndromeMetabolic syndrome
*p<0.001
Isomaa et al 2001
*
0
5
10
15
20
25
All-cause mortality
Cardiovascular mortality
Mor
talit
y ra
te (%
)
*
*
*
*
*p<0.001
Why is abdominal obesity harmful?
• Abdominal obesity– is often associated with other CV risk factors
– is an independent CV risk factor
• Adipocytes are metabolically active endocrine organs, not simply inert fat storage
Wajchenberg 2000
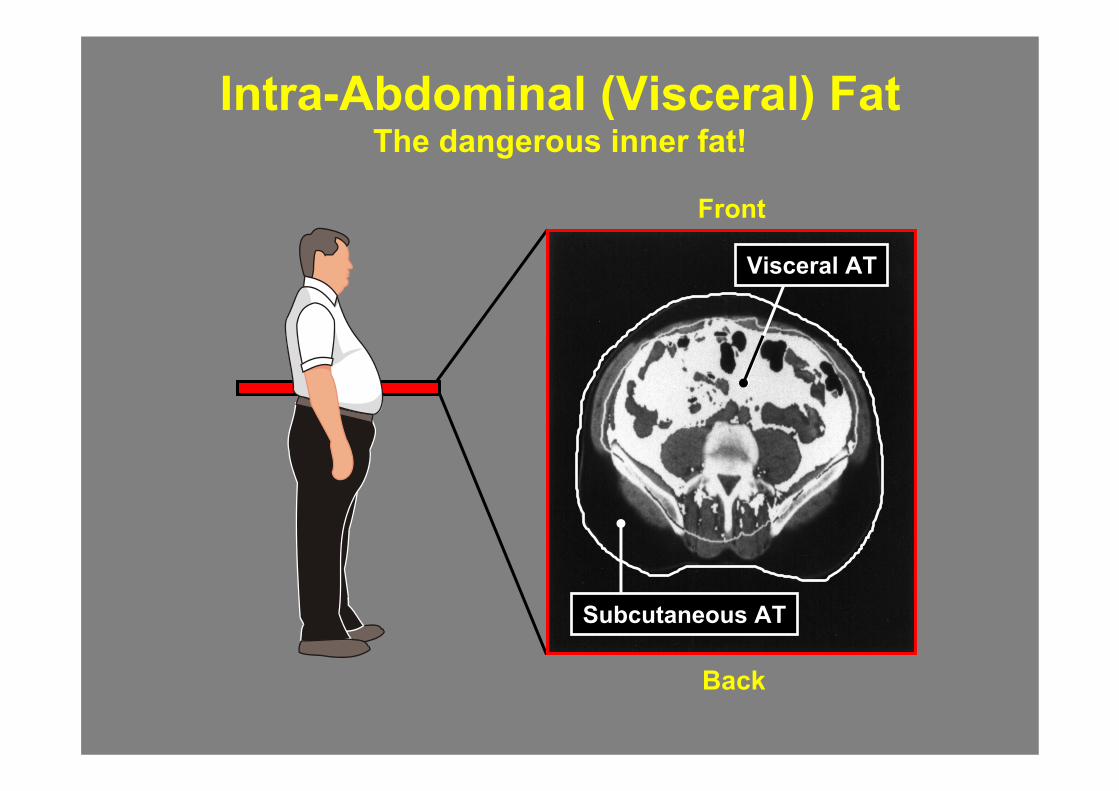
Intra-Abdominal (Visceral) FatThe dangerous inner fat!
Back
Visceral AT
Subcutaneous AT
Front
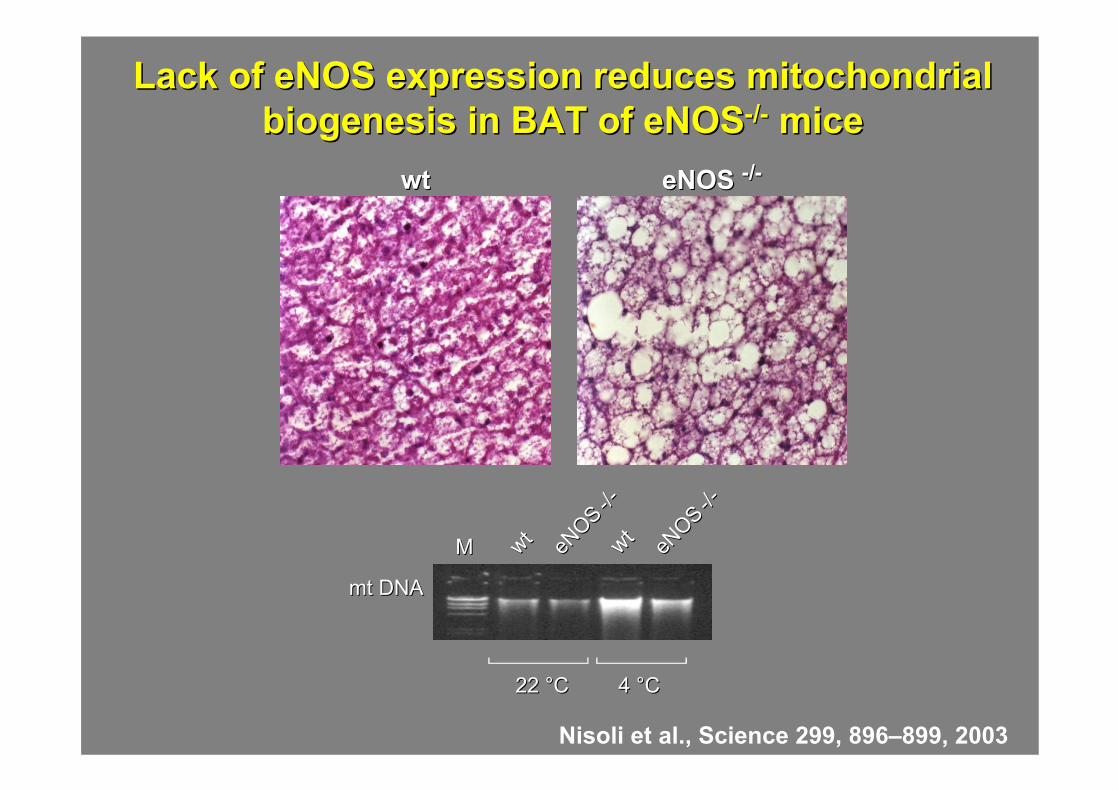
Lack of eNOS expression reduces mitochondrial Lack of eNOS expression reduces mitochondrial biogenesis in BAT of eNOSbiogenesis in BAT of eNOS--//-- micemice
wtwt eNOS eNOS --//--
wtwt wtwteNOS
eNOS --//--
mt DNAmt DNA
eNOS
eNOS --//--
MM
22 22 °°CC 4 4 °°CC
Nisoli et al., Science 299, 896–899, 2003
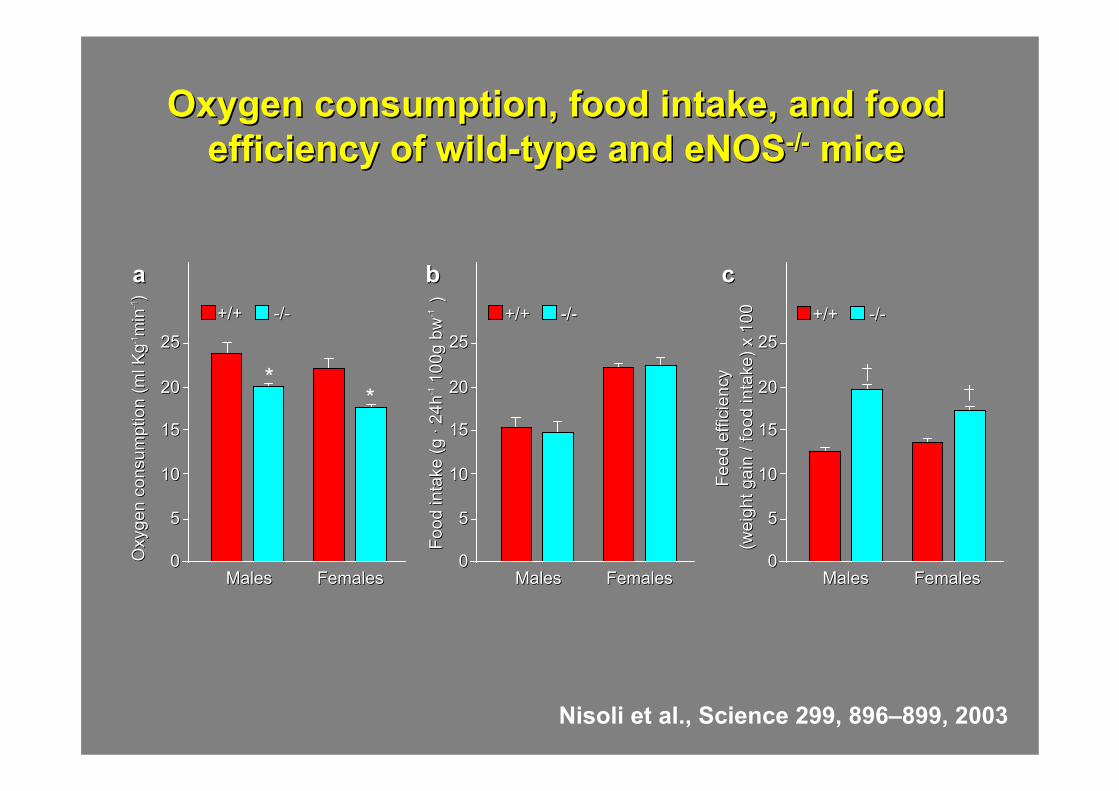
Oxygen consumption, food intake, and food Oxygen consumption, food intake, and food efficiency of wildefficiency of wild--type and eNOStype and eNOS--//-- micemice
Oxy
gen
cons
umpt
ion
(ml K
gO
xyge
n co
nsum
ptio
n (m
l Kg-- 11
min
min
-- 11))
Food
inta
ke (g
Fo
od in
take
(g ··
24h
24h-- 11
100g
bw
100g
bw
-- 11))
Feed
effi
cien
cyFe
ed e
ffici
ency
(wei
ght g
ain
/ foo
d in
take
) x 1
00(w
eigh
t gai
n / f
ood
inta
ke) x
100+/++/+ --//-- +/++/+ --//-- +/++/+ --//--
MalesMales FemalesFemales MalesMales FemalesFemales MalesMales FemalesFemales
aa bb cc
**
2525
2020
1515
1010
55
00
2525
2020
1515
1010
55
00
2525
2020
1515
1010
55
00
Nisoli et al., Science 299, 896–899, 2003
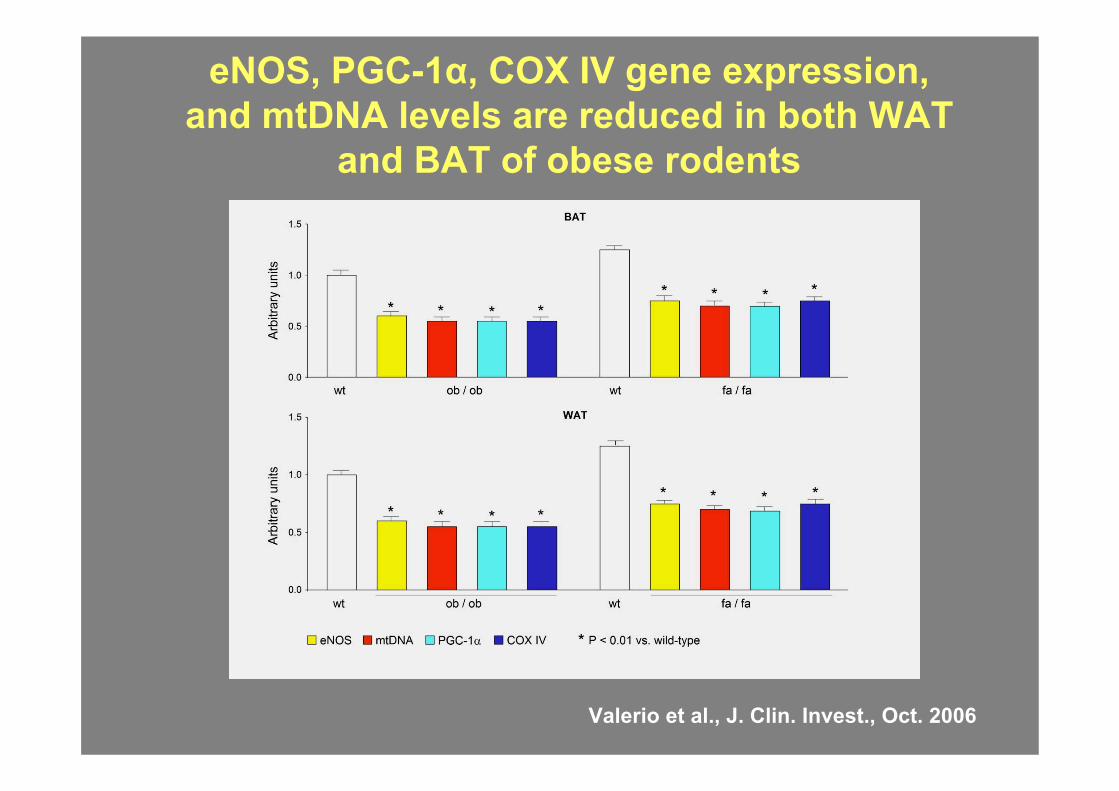
eNOS, PGC-1α, COX IV gene expression, and mtDNA levels are reduced in both WAT
and BAT of obese rodents
Valerio et al., J. Clin. Invest., Oct. 2006
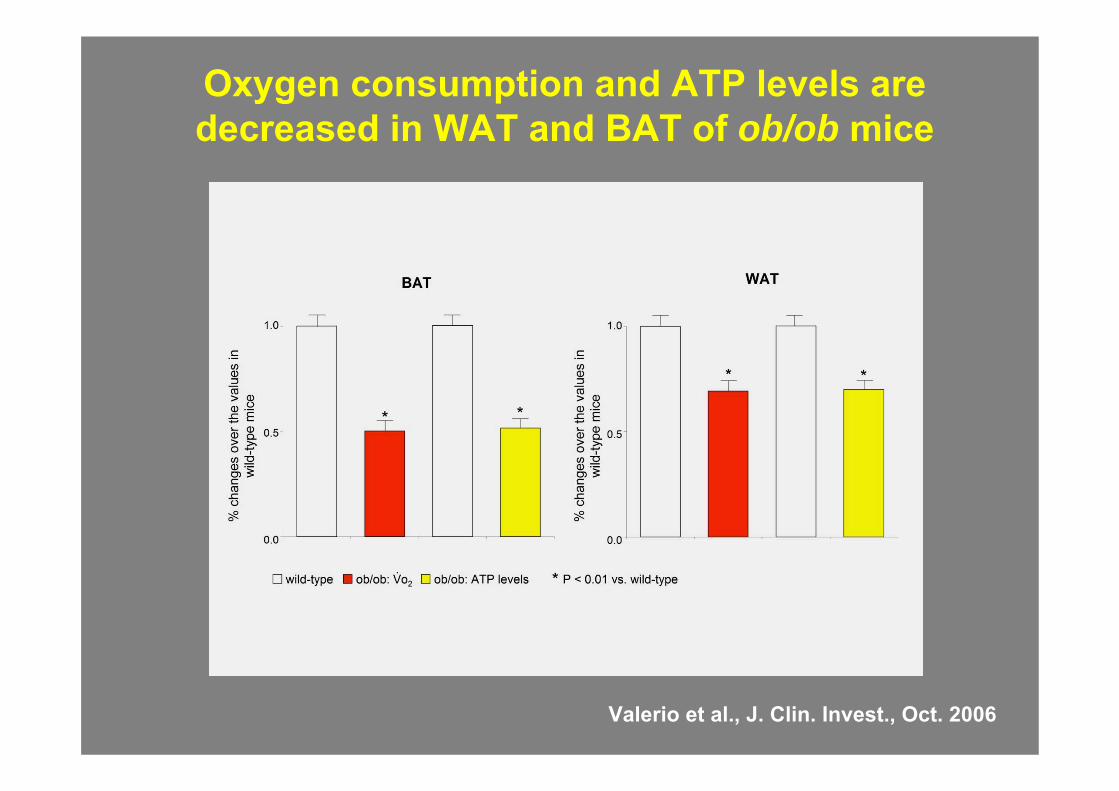
Oxygen consumption and ATP levels are decreased in WAT and BAT of ob/ob mice
Valerio et al., J. Clin. Invest., Oct. 2006
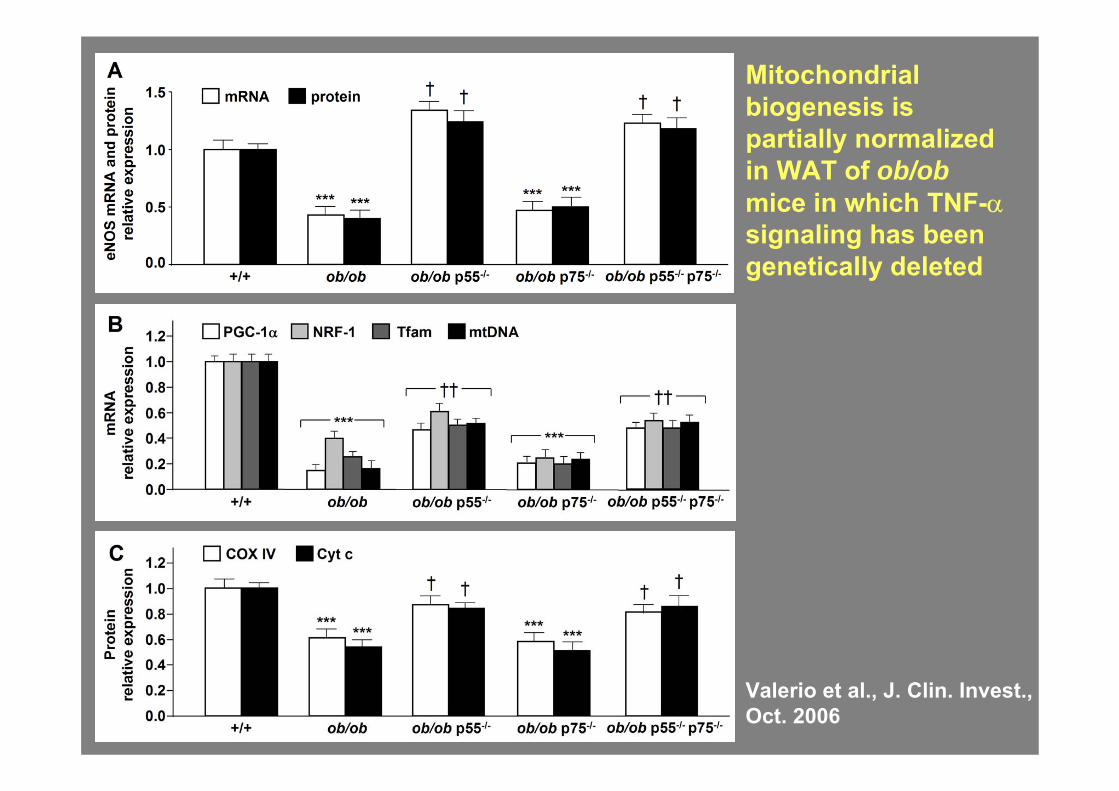
Mitochondrial biogenesis is partially normalized in WAT of ob/obmice in which TNF-αsignaling has been genetically deleted
Valerio et al., J. Clin. Invest., Oct. 2006
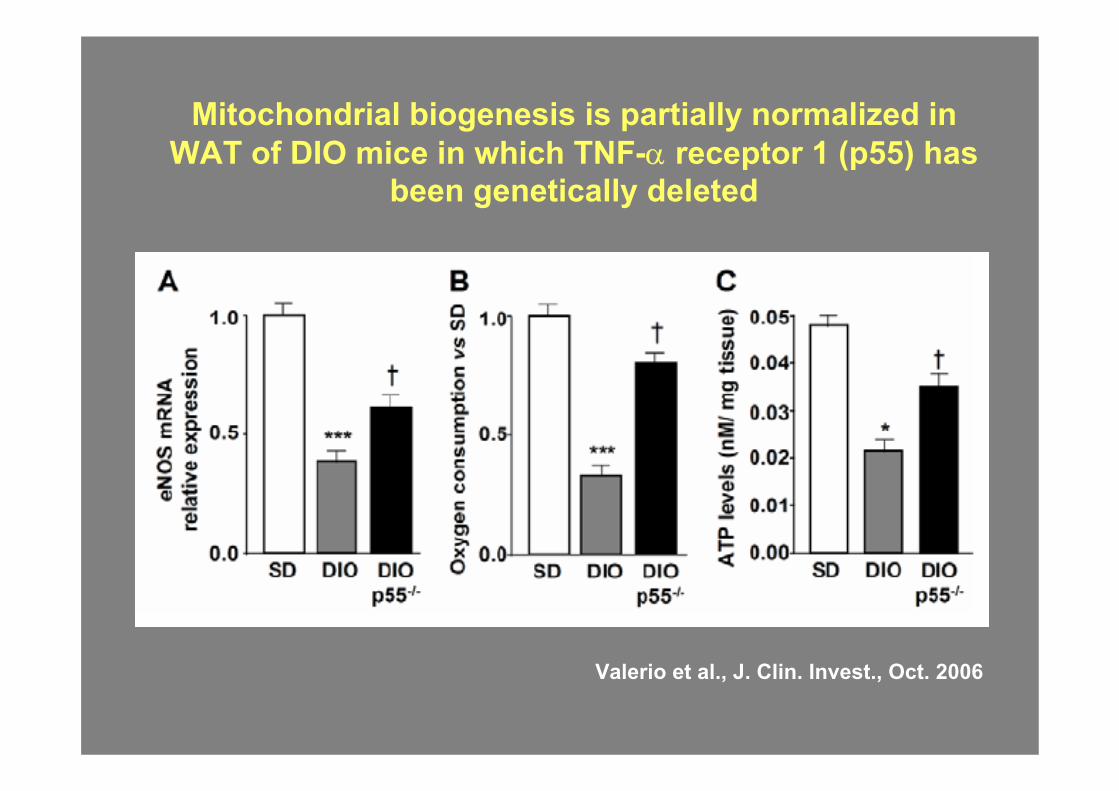
Mitochondrial biogenesis is partially normalized in WAT of DIO mice in which TNF-α receptor 1 (p55) has
been genetically deleted
Valerio et al., J. Clin. Invest., Oct. 2006
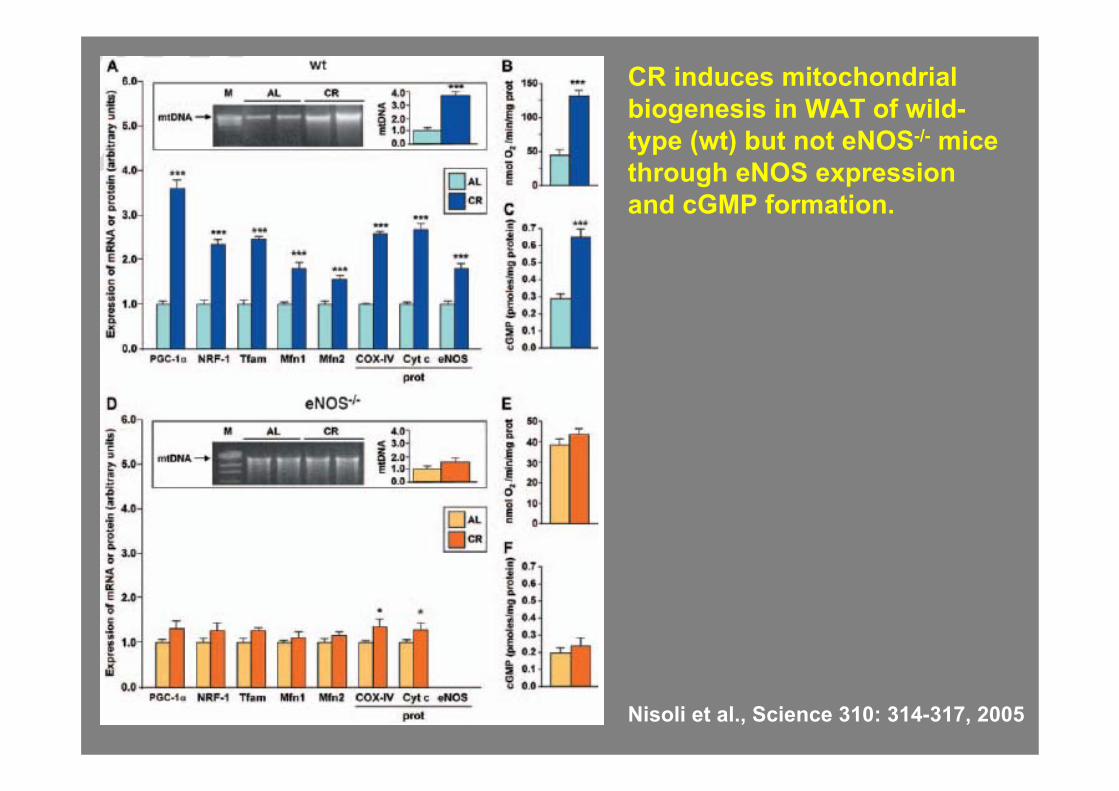
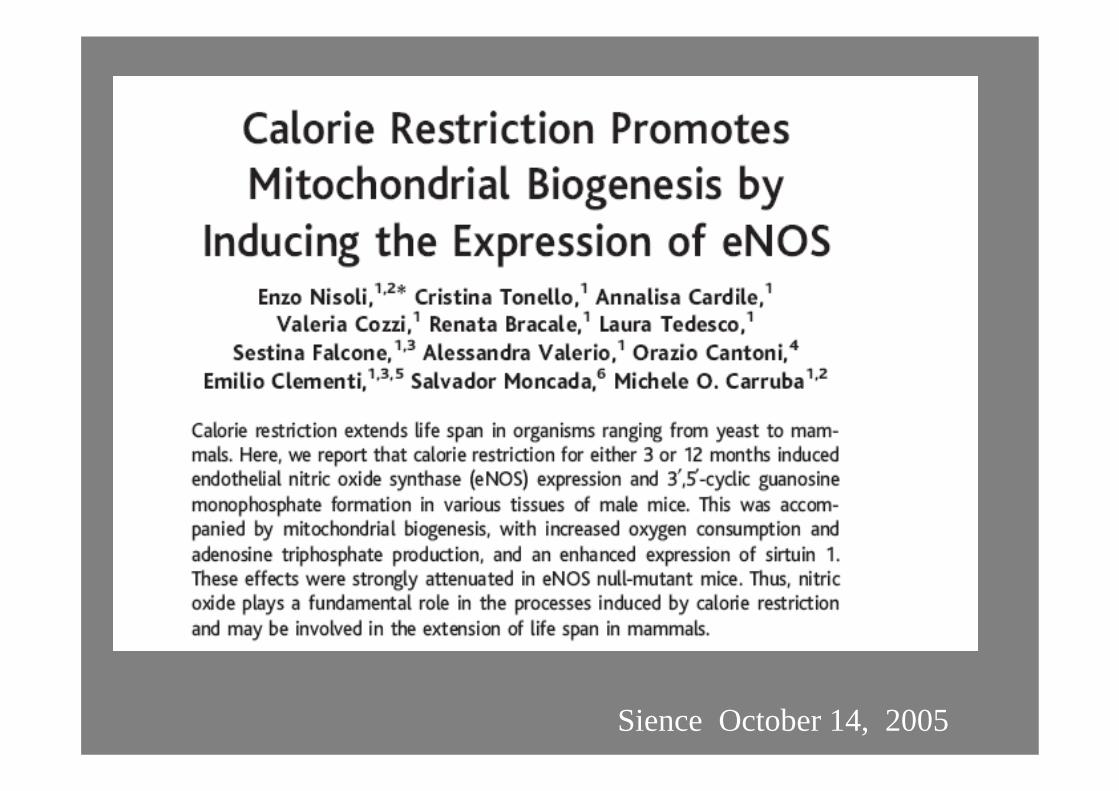
Nisoli et al., Science 310: 314-317, 2005
CR induces mitochondrialbiogenesis in WAT of wild-type (wt) but not eNOS-/- mice through eNOS expression and cGMP formation.

DIETA MEDITERRANEA
• Calorie• Bilanciamento• Carboidrati (IG)• Lipidi (saturi/insaturi)• Fibra• Vitamine e antiossidanti• Numero pasti• Piramide (QB)
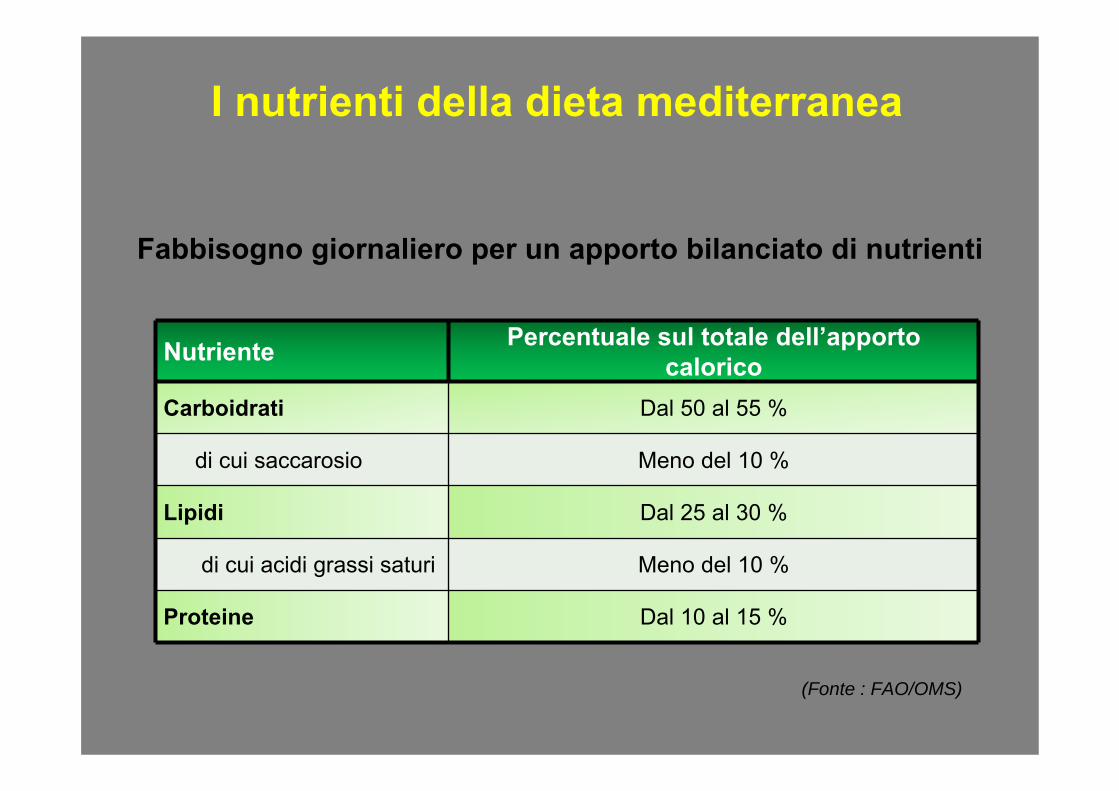
Fabbisogno giornaliero per un apporto bilanciato di nutrienti
I nutrienti della dieta mediterranea
Nutriente Percentuale sul totale dell’apporto calorico
Carboidrati Dal 50 al 55 %
di cui saccarosio Meno del 10 %
Lipidi Dal 25 al 30 %
di cui acidi grassi saturi Meno del 10 %
Proteine Dal 10 al 15 %
(Fonte : FAO/OMS)
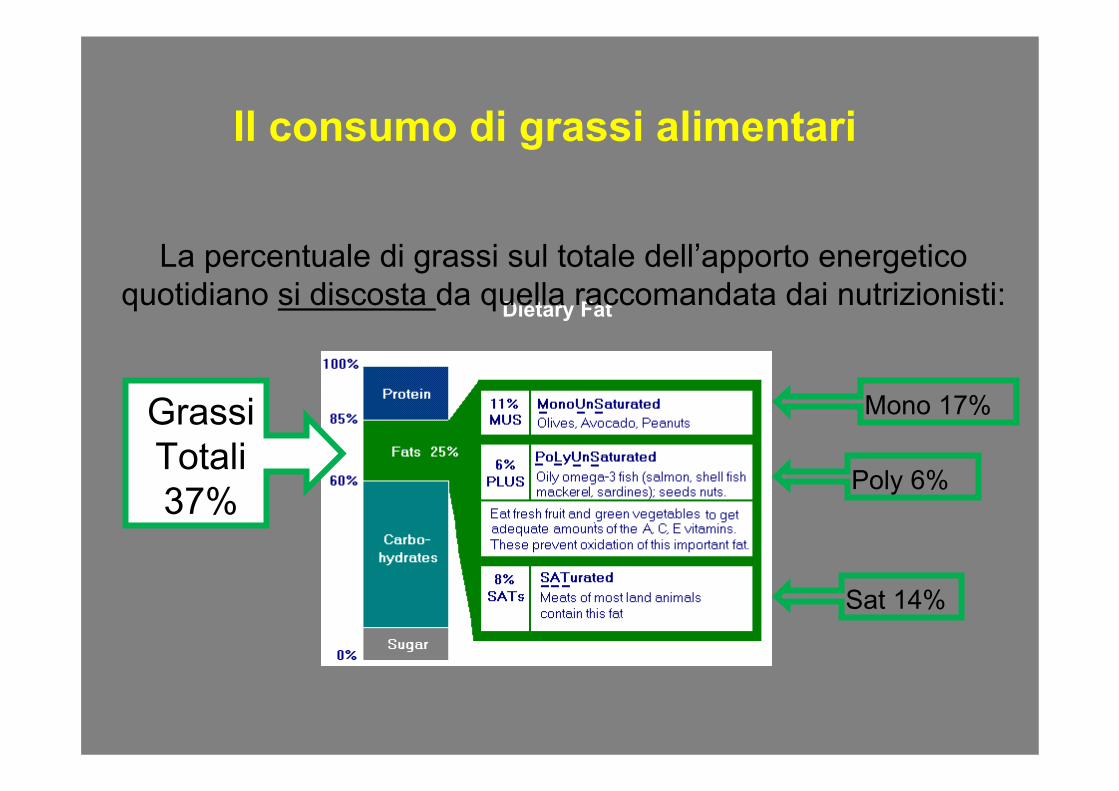
Il consumo di grassi alimentari
Dietary Fat
Grassi Totali 37%
La percentuale di grassi sul totale dell’apporto energetico quotidiano si discosta da quella raccomandata dai nutrizionisti:
Sat 14%
Mono 17%
Poly 6%

Eccessi
Zuccheri sempliciGrassi saturiSaleProteine di origine animalePorzioni troppo abbondantiSpuntini troppo frequenti
Carenze
Frutta e verduraFibre Principi nutritivi fondamentaliCarboidrati complessi

La piramide alimentare
Per un corretto approccio nutrizionale è uso comune classificare gli alimenti in 7 gruppi principali in accordo alle specifiche proprietà nutritive di ogni gruppo.