Embed Size (px)
Citation preview
Received: 5 February 2002Revised: 25 June 2002Accepted: 25 June 2002Published online: 10 August 2002© Springer-Verlag 2002
Abstract Tuberculosis, more thanany other infectious disease, has al-ways been a challenge, since it hasbeen responsible for a great amountof morbidity and mortality in hu-mans. After a steady decline in thenumber of new cases during thetwentieth century, due to improvedsocial and environmental conditions,early diagnosis, and the developmentof antituberculous medication, astagnation and even an increase inthe number of new cases was notedin the mid-1980s. The epidemiologi-cal alteration is multifactorial: globalincrease in developing countries; mi-nority groups (HIV and other immu-nocompromised patients); and elder-ly patients due to an altered immunestatus. Other factors that may be re-sponsible are a delayed diagnosis,especially in elderly patients, incom-plete or inadequate therapy, and theemergence of multidrug-resistant tu-berculosis. The course of the diseaseand its corresponding clinicoradio-logical pattern depends on the inter-action between the organism and the
host response. Classically, pulmona-ry tuberculosis has been classified inprimary tuberculosis, which occurredpreviously in children, and postpri-mary tuberculosis, occurring in adultpatients. In industrialized countries,however, there seems to be a shift ofprimary tuberculosis towards adults.Furthermore, due to an altered im-munological response in certaingroups, such as immunocompro-mised and elderly patients, an atypi-cal radioclinical pattern may occur.The changing landscape, in whichtuberculosis occurs, as well as theglobal resurgence, and the changedspectrum of the clinical and radio-logical presentation, justify a re-newed interest of radiologists for the imaging features of pulmonarytuberculosis. This article deals withthe usual imaging features of pulmonary tuberculosis as well asthe atypical patterns encountered inimmunodepressed and elderly pa-tients.
Keywords Pulmonary tuberculosis
Eur Radiol (2003) 13:1771–1785DOI 10.1007/s00330-002-1612-y C H E S T
P. Van DyckF. M. VanhoenackerP. Van den BrandeA. M. De Schepper
Imaging of pulmonary tuberculosis
Introduction
During the twentieth century, in industrialized coun-tries, tuberculosis (TB) has evolved from a frequentand possible lethal disease to a treatable, preventable,and eradicable disease [1]. For this reason, TB has disappeared from the spotlight. Together with the de-crease in TB incidence, the control programs becamevictims of their own success: in the U.S., the number of
TB clinics and TB beds decreased to one-third in 1988[2].
However, since the mid-1980s, the decrease of manyyears’ standing of TB infection has come to an end, andin some countries there has been a slight increase [3]. In1993 the World Health Organization (WHO) declaredTB a “global emergency”: 1.7 billion of people were in-fected with M. tuberculosis, every year 3 million of peo-ple died from TB, and approximately 8 million new
P. Van Dyck · F.M. Vanhoenacker (✉)A.M. De SchepperDepartment of Radiology, University Hospital Antwerp, Wilrijkstraat 10, 2650 Edegem, Belgiume-mail: [email protected].: +32-3-8213532Fax: +32-3-8252026
F.M. VanhoenackerDepartment of Radiology, AZ St. Maarten,Rooienberg 25, 2570 Duffel, Belgium
P. Van den BrandeDepartment of Pneumology, AZ St. Maarten, Rooienberg 25, 2570 Duffel, Belgium
cases occurred. In developed countries, 80% of patientsare 50 years or older. There is no doubt, however, thatthe HIV epidemic has played an important role in the re-surgence of TB [3]. Furthermore, these patients oftenpresent with atypical clinical and radiological presenta-tions, often resulting in late – even postmortem – diag-nosis and hence therapy [4].
In developing countries, in which almost more than90% of the TB cases worldwide occur, the situation isdramatic, and TB is still an evolving disease [5]. Thenumber of cases continues to increase: between1984–1986 and 1989–1991, the number of cases in-creased with more than 20 and 80% of cases involvingpersons in their productive years (15–59 years) [6]. Alsoin developing countries, TB is related mainly to povertyand HIV epidemic [7].
Finally, global emergence of multidrug-resistant(MDR) strains of M. tuberculosis in recent years hasgreatly complicated the management and control oftransmission of active cases [8].
A thorough understanding of the pathogenesis of TBis a prerequisite to the interpretation of the clinical andradiographic behavior. Pulmonary tuberculosis (PTB)can be classically divided into primary and postprimary(or reactivation) TB, each with corresponding radiologi-cal patterns. This classification, however, refers to a pe-riod of high TB prevalence (in the pre-antibiotic era).Due to the changing epidemiology, considerable overlapin the radiological presentations of those entities may ex-ist. For didactical reasons, pathogenesis and correspond-ing radiographic patterns are discussed, followed by adiscussion of atypical patterns.
Pathogenesis of tuberculosis
Primary tuberculosis
After eradication of bovine TB by pasteurization of milk,enterogenous TB infection in developed countries is al-most nonexistent, and primary TB infections are respira-tory of origin, due to inhalation of droplets, producedwhen persons with pulmonary or laryngeal TB sneeze,cough, speak, or sing [1]. These droplets (2–10 µm), lad-en with a few bacilli (1–4 µm), are carried by cilia to theterminal bronchioles. Inoculation takes place most oftenin the best ventilated areas of the lungs, most frequentlyin the anterior segments of the upper lobes, middle lobe,and lingula, and the basal segments of the lower lobes.Local alveolar macrophages orchestrate a complex im-munopathological process and this results, after a fewweeks, in formation of epitheloid granulomas, which candevelop into larger tuberculomas. Delayed hypersensitiv-ity becomes manifest approximately 4–10 weeks afterinitial infection. At this moment, the tuberculin reactionbecomes positive. Primary tuberculosis is a condition
that reflects an individual’s conversion from insensitivityto the antigens of the tubercle bacilli [9].
The macroscopic hallmark of hypersensitivity is thedevelopment of caseous necrosis in the pulmonary focusand/or in the involved lymph nodes. The primary paren-chymal focus is known as the Ghon focus [9]. The com-bination of the Ghon focus and the enlarged draininglymph nodes form the primary complex: the Ranke orGhon complex [10].
The further extent of the primary infection, occurringafter inhalation of TB bacilli, is dependent on differentfactors such as number and virulence of the agens, natu-ral and acquired resistance of the host, and hypersensi-tivity [11].
Finally, many exogenous and endogenous factors maycontribute to immunodepression: diabetes mellitus; HIV;malignancy; corticotherapy; alcoholism; and malnutri-tion.
In the immunocompetent patient, development of spe-cific immunity is usually adequate to limit further multi-plication of bacilli, the host remains asymptomatic, andlesions heal [12]. In the clinical and radiographic occultcases, conversion from a previously negative to positivetuberculin skin test may be the only witness of primaryinfection. This is the case in 95% in immunocompetentpatients. Healing of TB occurs with resorption of case-ous necrosis, accompanied by deposition of collagen (fi-brosis) and calcification [13].
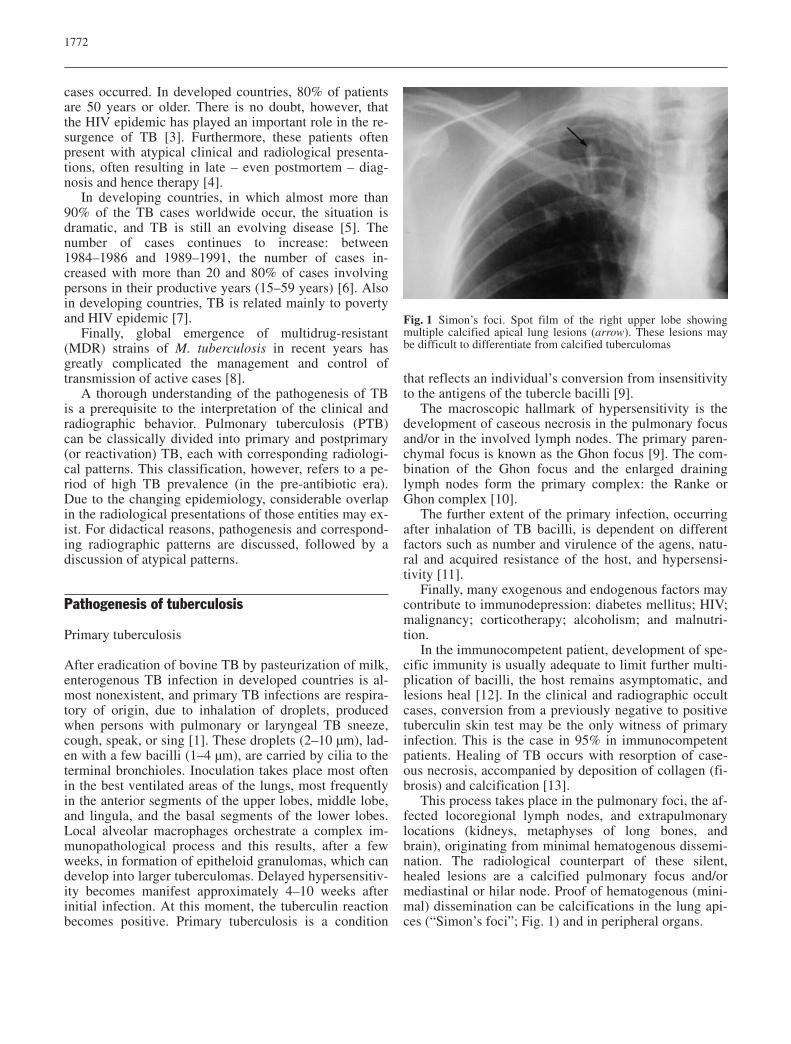
This process takes place in the pulmonary foci, the af-fected locoregional lymph nodes, and extrapulmonarylocations (kidneys, metaphyses of long bones, andbrain), originating from minimal hematogenous dissemi-nation. The radiological counterpart of these silent,healed lesions are a calcified pulmonary focus and/ormediastinal or hilar node. Proof of hematogenous (mini-mal) dissemination can be calcifications in the lung api-ces (“Simon’s foci”; Fig. 1) and in peripheral organs.
1772
Fig. 1 Simon’s foci. Spot film of the right upper lobe showingmultiple calcified apical lung lesions (arrow). These lesions maybe difficult to differentiate from calcified tuberculomas
These healed pulmonary and extra-pulmonary lesionsharbor bacilli in dormant position, at low metabolic rate,but causing continuous antigenic stimulation for mainte-nance of hypersensitivity to tuberculous antigen. In situ-ations of immunodepression, these bacilli can reactivate.
In immunocompromised patients (HIV, alcoholics, di-abetics, chronic renal insufficiency), more widespreadlymphogenic and hematogenous dissemination can occurand frequently results in adenopathy and peripheral loca-tions, respectively.
If immunity is inadequate, clinically active diseasecan develop within 5 years after infection, called pro-gressive primary tuberculosis [12, 14].
Postprimary disease
Postprimary disease results from reactivation of dormantresidual foci, in which the T-cell-mediated tissue re-sponse is directed towards caseation of those foci [9]. Ingeneral, there is clinical, radiological, and epidemiologi-cal evidence that postprimary disease can occur fromfour possible pathways, linking primary infection topostprimary disease. These pathways can occur isolatedor combined:
1. Postprimary disease can develop from reactivation ofbacilli in the lung apices. These apical lung lesionsare the result of hematogenous spread during primaryinfection a few years earlier, after a symptom-free pe-riod. Hematogenous spread and reactivation occurspreferentially in the apical, posterior segments of theupper lobes, and apical segment of the lower lobe, be-cause the oxygen tension is highest in the upper lungzones. Another explanation for this anatomical distri-bution is the impaired lymphatic clearance. Thelymph flow may be restricted in the upper lung zonesof the erect lung or in the posterior aspects of the lungdue to the relatively greater bellows action of the an-terior rib cage during respiratory excursion [9, 10].These apical lung sites are called Simon’s foci(Fig. 1). After reactivation, these lesions reach conflu-ence, liquefy, and excavate. This form of postprimaryPTB is usually described as hematogenous phtysis[15].
2. Perforation of a lymph node into a bronchus or a tu-berculous bronchitis (well-known complications ofgangliopulmonary TB) may cause ulcerations of prin-cipal and/or segmental bronchi [5]. Localization ofthose bronchial anomalies are determined by the lo-calization of the involved bronchopulmonary and tra-cheobronchial lymph nodes. Frequently, the anteriorsegment bronchus of the upper lobe and middle lobebronchus are affected. Other lesions can be bronchi-ectasis, which are typically central. Aspiration of ba-cilli in the bronchial lumina cause bronchogenic dis-
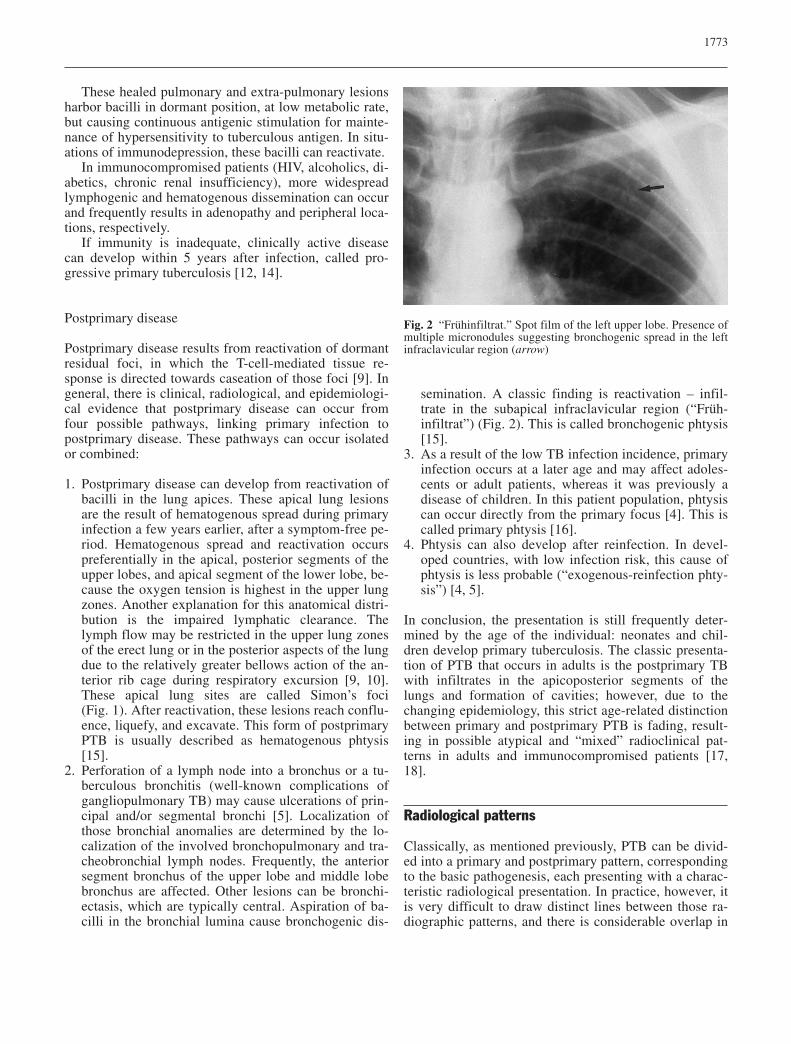
semination. A classic finding is reactivation – infil-trate in the subapical infraclavicular region (“Früh-infiltrat”) (Fig. 2). This is called bronchogenic phtysis[15].
3. As a result of the low TB infection incidence, primaryinfection occurs at a later age and may affect adoles-cents or adult patients, whereas it was previously adisease of children. In this patient population, phtysiscan occur directly from the primary focus [4]. This iscalled primary phtysis [16].
4. Phtysis can also develop after reinfection. In devel-oped countries, with low infection risk, this cause ofphtysis is less probable (“exogenous-reinfection phty-sis”) [4, 5].
In conclusion, the presentation is still frequently deter-mined by the age of the individual: neonates and chil-dren develop primary tuberculosis. The classic presenta-tion of PTB that occurs in adults is the postprimary TBwith infiltrates in the apicoposterior segments of thelungs and formation of cavities; however, due to thechanging epidemiology, this strict age-related distinctionbetween primary and postprimary PTB is fading, result-ing in possible atypical and “mixed” radioclinical pat-terns in adults and immunocompromised patients [17,18].
Radiological patterns
Classically, as mentioned previously, PTB can be divid-ed into a primary and postprimary pattern, correspondingto the basic pathogenesis, each presenting with a charac-teristic radiological presentation. In practice, however, itis very difficult to draw distinct lines between those ra-diographic patterns, and there is considerable overlap in
1773
Fig. 2 “Frühinfiltrat.” Spot film of the left upper lobe. Presence ofmultiple micronodules suggesting bronchogenic spread in the leftinfraclavicular region (arrow)

the radiological manifestations. The disease and its ra-diological patterns are rather to interpret as a continuousinteraction between the individual patient, with his ownimmune status and M. tuberculosis [19].
Recognizing the limitations of this radiographic pat-tern categorization, we discuss firstly the usual radiolog-ical presentation of primary (gangliopulmonary TB) andpostprimary (phtysis) TB. It is emphasized, however,that the different radiological patterns can present as iso-lated, combined, or successive in the same patient; there-fore, a specific subsection is dedicated to radiologicalpatterns that can be seen in both primary and postprima-ry PTB.
Finally, we focus on some atypical patterns of PTB,as observed in some groups.
Typical radiological patterns of primary PTB
In Western countries, in the pre-antibiotic era, primaryPTB occurred predominantly in children and was partic-ularly prevalent in areas where control measures were in-adequate; however, primary TB in the adult is increasingin incidence as a result of new infection being acquiredby people residing in areas where prophylactic and thera-peutic measures have resulted in low incidence of infec-tion during childhood [20].
Classically, four entities have been described: gan-gliopulmonary TB; tuberculous pleuritis; miliary TB;and tracheobronchial TB. In this section, only ganglio-pulmonary TB is discussed and the other entities are dis-cussed in the section “Radiological patterns encounteredin both primary and/or postprimary PTB”, since they areencountered in primary as well as in postprimary PTB.
Gangliopulmonary TB is characterized by the presenceof mediastinal and/or hilar adenopathies and less conspic-uous parenchymal abnormalities (Ghon focus). Because ofits preferential occurrence in children, it has been desig-nated as “childhood”-type PTB; however, in regions withlow incidence of TB, it is now a rare entity in children ex-cept for nonindigenous children and has been increasinglyencountered in adults and elderly patients [4]. Right para-tracheal and hilar localizations are the most common sitesof nodal involvement in primary PTB, although othercombinations have been described (bilateral hilar, isolatedmediastinal). The prevalence of adenopathies decreaseswith age [21]. On contrast-enhanced CT scan, tuberculousadenopathies, often measuring more than 2 cm, show avery characteristic, but not pathognomonic, “rim sign”consisting of a low-density center surrounded by a periph-eral enhancing rim (Fig. 3) [22]. This rim sign has alsobeen found with atypical mycobacteria [23], lymphoma[24], and testis carcinoma [25].
Associated parenchymal infiltrates are encountered onthe same side as nodal enlargement in approximatelytwo-thirds of pediatric cases of primary PTB [21].
Parenchymal opacities are typically located in the pe-riphery of the lung, especially in the subpleural areas.They are usually difficult to see on conventional radio-graphs, because of their small volume; therefore, CT isoften necessary to detect these subtle parenchymal infil-trates [26].
In contrast to the age-related occurrence observedwith lymphadenopathy, Leung et al. [21] found that theprevalence of radiographically detectable parenchymalinvolvement was significantly lower in children up to3 years of age (51%) as compared with that in older chil-dren (78%) in whom the prevalence is similar to the pre-viously reported 80% in adults [27].
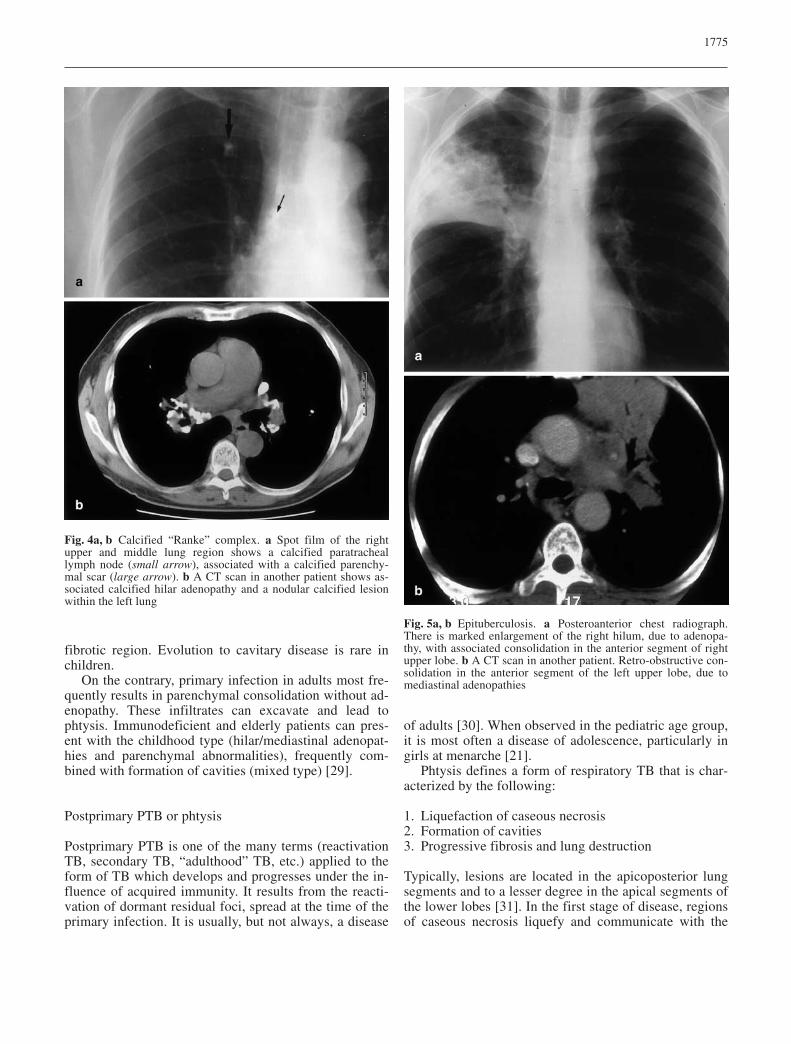
Generally, the disease is self-limiting and immuno-competent patients remain usually asymptomatic. Fre-quently, the only radiological evidence is the so-calledRanke complex: the combination of a parenchymal scar(whether calcified or not) – the Ghon lesion – and calci-fied hilar and/or paratracheal lymph nodes (Fig. 4). Fre-quently, physical examination reveals no abnormalities.
Gangliopulmonary TB may be complicated by perfo-ration of an adenopathy in a bronchus (cfr. supra), retro-obstructive pneumonia, and/or atelectasis (epituberculo-sis; Fig. 5). A retro-obstructive infiltrate in primary TBmost commonly appears as an area of homogenous con-solidation. Obstructive atelectasis or overinflation result-ing from compression by an adjacent enlarged node havebeen reported to occur in 9–30% and 1–5% of childrenwith primary TB, respectively [21]. Distribution is typi-cally right sided, with obstruction occurring at the levelof the right lobar bronchus or bronchus intermedius [28].
In these complicated cases, symptoms such as coughor wheezing are frequent. Retro-obstructive inflamma-tion may resorb and evolve to a fibrotic and/or calcifiedlesion. Destruction and fibrosis of the lung parenchymaresult in formation of traction bronchiectasis within the
1774
Fig. 3 Tuberculous adenopathy. Contrast-enhanced CT scan dem-onstrating an enlarged tuberculous lymph node in the upper medi-astinum, with peripheral rim enhancement and low-density center
fibrotic region. Evolution to cavitary disease is rare inchildren.
On the contrary, primary infection in adults most fre-quently results in parenchymal consolidation without ad-enopathy. These infiltrates can excavate and lead tophtysis. Immunodeficient and elderly patients can pres-ent with the childhood type (hilar/mediastinal adenopat-hies and parenchymal abnormalities), frequently com-bined with formation of cavities (mixed type) [29].
Postprimary PTB or phtysis
Postprimary PTB is one of the many terms (reactivationTB, secondary TB, “adulthood” TB, etc.) applied to theform of TB which develops and progresses under the in-fluence of acquired immunity. It results from the reacti-vation of dormant residual foci, spread at the time of theprimary infection. It is usually, but not always, a disease
of adults [30]. When observed in the pediatric age group,it is most often a disease of adolescence, particularly ingirls at menarche [21].
Phtysis defines a form of respiratory TB that is char-acterized by the following:
1. Liquefaction of caseous necrosis2. Formation of cavities3. Progressive fibrosis and lung destruction
Typically, lesions are located in the apicoposterior lungsegments and to a lesser degree in the apical segments ofthe lower lobes [31]. In the first stage of disease, regionsof caseous necrosis liquefy and communicate with the
1775
Fig. 4a, b Calcified “Ranke” complex. a Spot film of the rightupper and middle lung region shows a calcified paratracheallymph node (small arrow), associated with a calcified parenchy-mal scar (large arrow). b A CT scan in another patient shows as-sociated calcified hilar adenopathy and a nodular calcified lesionwithin the left lung
Fig. 5a, b Epituberculosis. a Posteroanterior chest radiograph.There is marked enlargement of the right hilum, due to adenopa-thy, with associated consolidation in the anterior segment of rightupper lobe. b A CT scan in another patient. Retro-obstructive con-solidation in the anterior segment of the left upper lobe, due tomediastinal adenopathies
tracheobronchial tree to form cavities. Higher oxygentension results in exponential growth of bacilli. Cough-ing may result in bronchogenic spread in the ipsi- orcontralateral lung segments and/or contamination of oth-er patients, via inhalation of bacilli-laden droplets.
The whole process can take months to years. Theclinical presentation is variable and ranges from asymp-tomatic to insidious or acute. Cough, anorexia, weightloss, fatigue, and fever are nonspecific complaints,which are frequently disregarded by patient or his envi-
ronment, and are attributed to senile decay (patient’s de-lay). Hemoptysis is sometimes the first alarming symp-tom and diagnosis is suggested on radiographs. Symp-toms can be more acute when phtysis occurs immediate-ly after primary infection or exogenic reinfection or re-activation: patients present with a “flu-like” syndrome,e.g., fever, sputa, and night sweats. This variety of non-specific symptoms can mimic more frequent pathologysuch as bacterial–viral pneumonia, neoplasia, orthrombo-embolic disease; therefore, recognition by phy-
1776
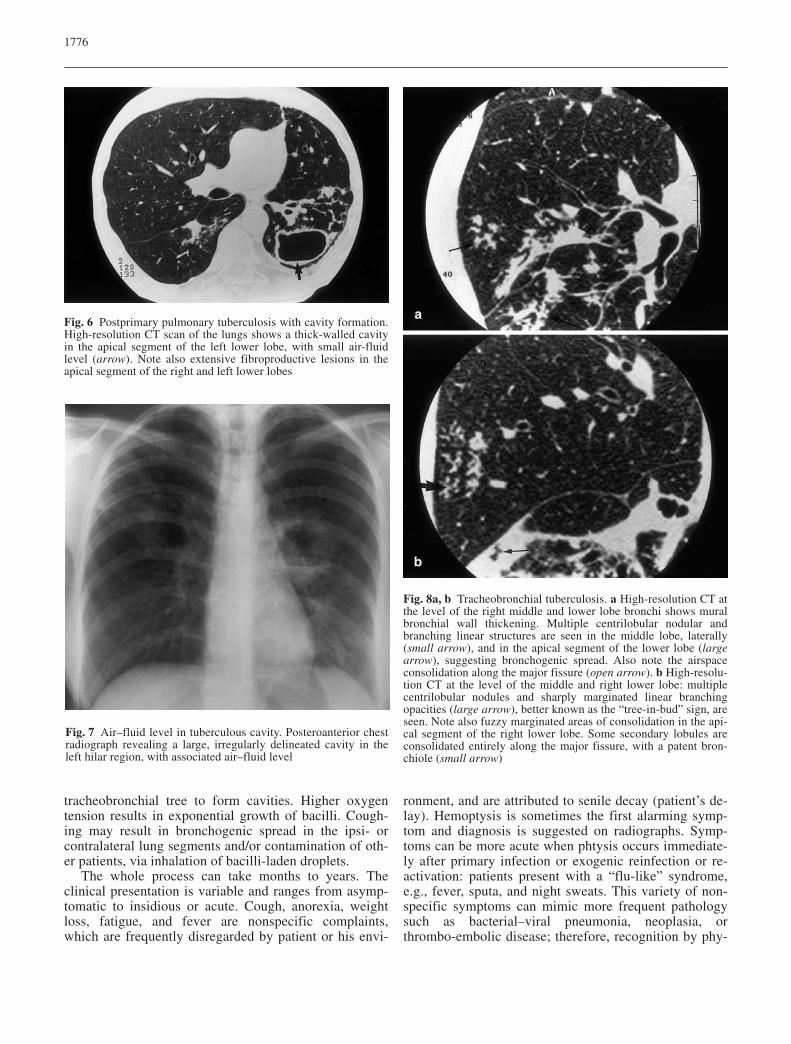
Fig. 6 Postprimary pulmonary tuberculosis with cavity formation.High-resolution CT scan of the lungs shows a thick-walled cavityin the apical segment of the left lower lobe, with small air-fluidlevel (arrow). Note also extensive fibroproductive lesions in theapical segment of the right and left lower lobes
Fig. 7 Air–fluid level in tuberculous cavity. Posteroanterior chestradiograph revealing a large, irregularly delineated cavity in theleft hilar region, with associated air–fluid level
Fig. 8a, b Tracheobronchial tuberculosis. a High-resolution CT atthe level of the right middle and lower lobe bronchi shows muralbronchial wall thickening. Multiple centrilobular nodular andbranching linear structures are seen in the middle lobe, laterally(small arrow), and in the apical segment of the lower lobe (largearrow), suggesting bronchogenic spread. Also note the airspaceconsolidation along the major fissure (open arrow). b High-resolu-tion CT at the level of the middle and right lower lobe: multiplecentrilobular nodules and sharply marginated linear branchingopacities (large arrow), better known as the “tree-in-bud” sign, areseen. Note also fuzzy marginated areas of consolidation in the api-cal segment of the right lower lobe. Some secondary lobules areconsolidated entirely along the major fissure, with a patent bron-chiole (small arrow)
sicians is often delayed (“doctor’s delay”). Physical ex-amination is nonspecific as well.
Radiographs may show extensive abnormalities, suchas apicoposterior infiltrates, cavities, pleural exudates, fi-bro-productive lesions causing distortion of lung paren-chyma, elevation of fissures and hila, pleural adhesions,and formation of traction bronchiectasis [19].
Cavitation in one or multiple sites is radiographicallyevident in 40% of cases of postprimary disease (Fig. 6).The cavity walls may range from thin and smooth tothick and nodular. It can be difficult to distinguish thin-walled cavities from bullae, cysts, or pneumatoceles[32]. When multiple apical cavities are encountered, thepossibility that cystic bronchiectases are present in addi-tion to necrotic cavities must be considered [32].
Air-fluid levels in the cavity occur in 10% of cases(Fig. 7) [25]. According to some authors, air-fluid levelscan be due to superimposed bacterial or fungal infectionof the cavity [33].
Bronchogenic spread is radiographically identified in20% of cases of postprimary TB and manifests as multi-ple, ill-defined micronodules, distributed in a segmentalor lobar distribution, distant from the site of the cavityformation and typically involving the lower lung zones[34]. On CT scan, it is identified in 95% of cases [35].High-resolution (HR) CT is the imaging technique ofchoice to reveal early bronchogenic spread [36] and typi-cal findings are 2- to 4-mm centrilobular nodules andsharply marginated linear branching opacities which havebeen shown to represent caseous necrosis containing ba-cilli within and around terminal and respiratory bronchi-oles (“tree-in-bud” sign; Fig. 8b) [36]. Ascending con-taminations producing tracheitis and laryngitis can beseen (Fig. 9).
Because of effective antituberculous treatment of pri-mary TB during the 1960s, the overall incidence of en-dobronchial TB has decreased in western Europe [4];
1777
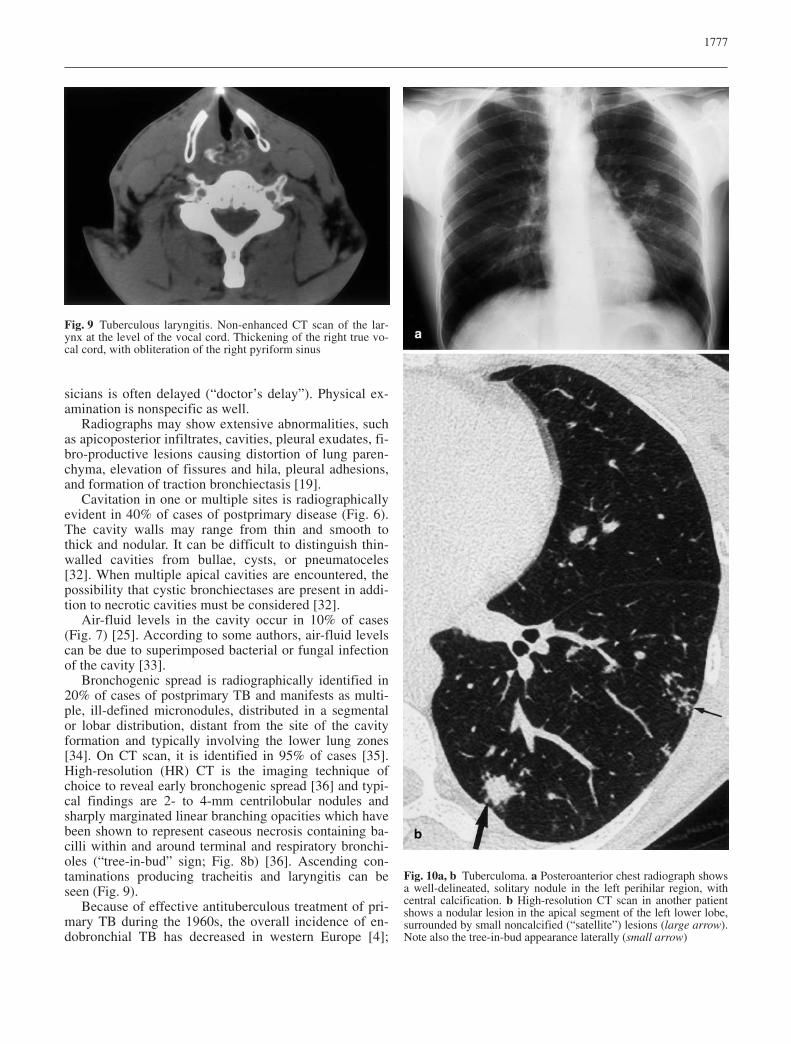
Fig. 9 Tuberculous laryngitis. Non-enhanced CT scan of the lar-ynx at the level of the vocal cord. Thickening of the right true vo-cal cord, with obliteration of the right pyriform sinus
Fig. 10a, b Tuberculoma. a Posteroanterior chest radiograph showsa well-delineated, solitary nodule in the left perihilar region, withcentral calcification. b High-resolution CT scan in another patientshows a nodular lesion in the apical segment of the left lower lobe,surrounded by small noncalcified (“satellite”) lesions (large arrow).Note also the tree-in-bud appearance laterally (small arrow)
however, recently, there has been an increased incidenceof endobronchial TB in HIV-positive patients [37] and inelderly subjects [38].
Although pulmonary tuberculomas are most often theresult of healed primary TB, they are seen in 3–6% ofcases of postprimary tuberculosis as the main or only ab-normality on chest radiographs (Fig. 10a) [39]. This isdiscussed later in “Radiological patterns encountered inboth primary and/or postprimary PTB”.
Cicatrization atelectasis is a common finding afterpostprimary TB. Up to 40% of patients with postprimaryTB have a marked fibrotic response, which manifests asatelectasis of the upper lobe, retraction of hilum, com-pensatory lower lobe hyperinflation, and mediastinalshift towards the fibrotic lung. Apical pleural thickeningassociated with fibrosis may reveal proliferation of ex-trapleural fatty tissue and peripheral atelectasis on CT[40].
Complete destruction of a whole lung or a major partof a lung is not uncommon in the end stage of TB. Suchdamage results from a combination of parenchymal andairway involvement. Secondary pyogenic or fungal infec-tion may supervene. Once the lung is destroyed, the ac-tivity is difficult to assess with radiological studies [32].
Diagnosis of postprimary TB is made bacteriological-ly. After antituberculous therapy, radiographs show dis-appearance of infiltrates and fibrosis develops. Fibrosiscan be stable or regress. When sputum is negative, butwith CT findings suggestive of bronchogenic spread, aguided fibroscopy may be proposed to assess the correctdiagnosis of active TB. If staining and/or culture remainnegative and the imaging features remain stable, the pro-cess can be considered as “inactive” TB.
Radiological patterns encountered in both primaryand/or postprimary PTB
Several radiological patterns are not exclusively seen ineither primary or postprimary TB. For didactical reasons,these patterns are discussed in detail separately.
Miliary tuberculosis
Miliary tuberculosis results from the acute hematoge-nous dissemination of TB bacilli in lungs and other or-gans, where innumerable small tuberculous granulomasdevelop. It can be seen in primary or postprimary dis-ease. Although classically seen in children, within a fewmonths after first contact, there is increasing incidenceof miliary TB in adults and elderly subjects [41].
The clinical presentation varies with age and immu-nological situation. Children mostly present with acuteillness: fever; malaise; anorexia; dyspnea; and some-times meningeal symptoms. Adults can present with a
more insidious clinical image. Immunodeficient adultsand elderly patients can present with variable clinicalfindings, ranging from hyperacute–respiratory insuffi-ciency to slowly, insidious, and progressive clinical pre-sentation, and diagnosis is often made only post mortem[4]. Physical examination may reveal hepatosplenomega-ly, lung crepitations, and choriodeal tubercles. The tuber-culin skin test is usually positive, but in severe, hyper-acute cases, it can remain negative.
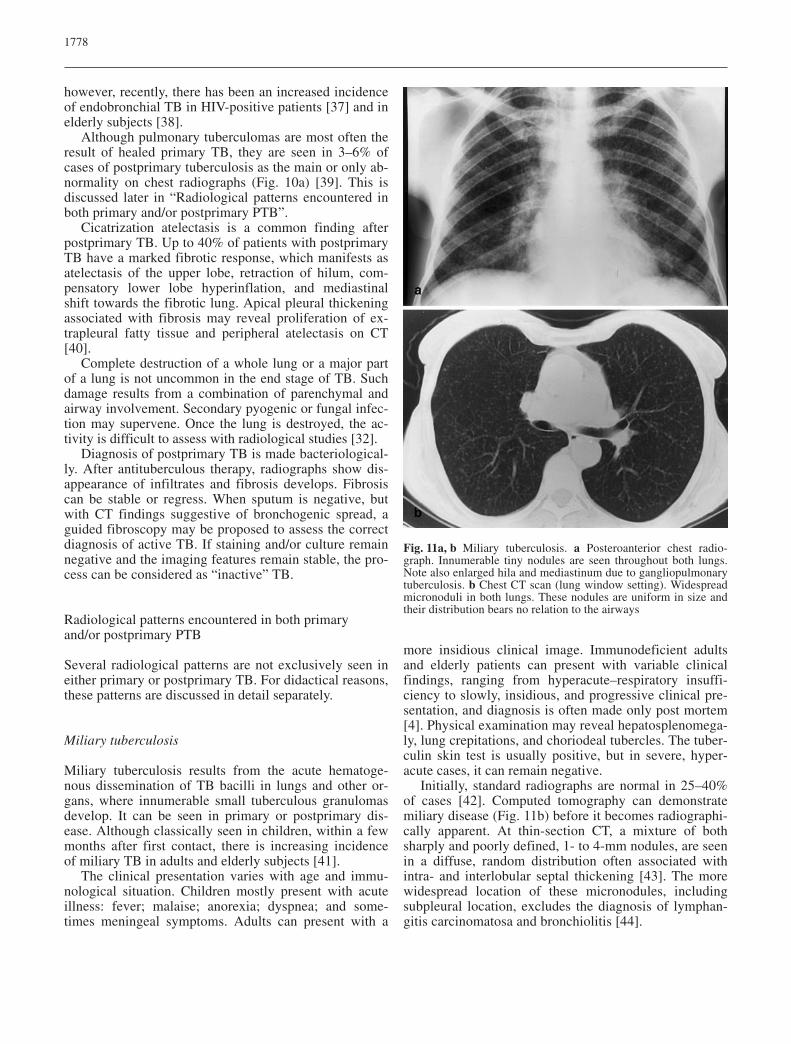
Initially, standard radiographs are normal in 25–40%of cases [42]. Computed tomography can demonstratemiliary disease (Fig. 11b) before it becomes radiographi-cally apparent. At thin-section CT, a mixture of bothsharply and poorly defined, 1- to 4-mm nodules, are seenin a diffuse, random distribution often associated withintra- and interlobular septal thickening [43]. The morewidespread location of these micronodules, includingsubpleural location, excludes the diagnosis of lymphan-gitis carcinomatosa and bronchiolitis [44].
1778
Fig. 11a, b Miliary tuberculosis. a Posteroanterior chest radio-graph. Innumerable tiny nodules are seen throughout both lungs.Note also enlarged hila and mediastinum due to gangliopulmonarytuberculosis. b Chest CT scan (lung window setting). Widespreadmicronoduli in both lungs. These nodules are uniform in size andtheir distribution bears no relation to the airways
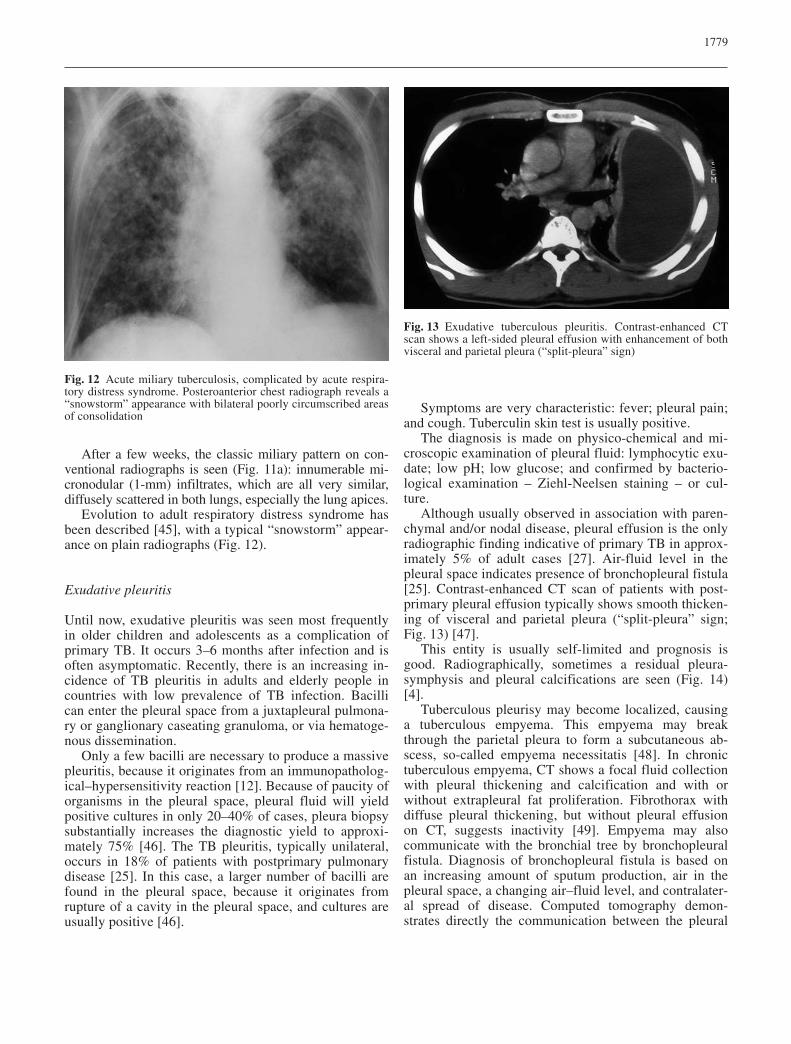
After a few weeks, the classic miliary pattern on con-ventional radiographs is seen (Fig. 11a): innumerable mi-cronodular (1-mm) infiltrates, which are all very similar,diffusely scattered in both lungs, especially the lung apices.
Evolution to adult respiratory distress syndrome hasbeen described [45], with a typical “snowstorm” appear-ance on plain radiographs (Fig. 12).
Exudative pleuritis
Until now, exudative pleuritis was seen most frequentlyin older children and adolescents as a complication ofprimary TB. It occurs 3–6 months after infection and isoften asymptomatic. Recently, there is an increasing in-cidence of TB pleuritis in adults and elderly people incountries with low prevalence of TB infection. Bacillican enter the pleural space from a juxtapleural pulmona-ry or ganglionary caseating granuloma, or via hematoge-nous dissemination.
Only a few bacilli are necessary to produce a massivepleuritis, because it originates from an immunopatholog-ical–hypersensitivity reaction [12]. Because of paucity oforganisms in the pleural space, pleural fluid will yieldpositive cultures in only 20–40% of cases, pleura biopsysubstantially increases the diagnostic yield to approxi-mately 75% [46]. The TB pleuritis, typically unilateral,occurs in 18% of patients with postprimary pulmonarydisease [25]. In this case, a larger number of bacilli arefound in the pleural space, because it originates fromrupture of a cavity in the pleural space, and cultures areusually positive [46].
Symptoms are very characteristic: fever; pleural pain;and cough. Tuberculin skin test is usually positive.
The diagnosis is made on physico-chemical and mi-croscopic examination of pleural fluid: lymphocytic exu-date; low pH; low glucose; and confirmed by bacterio-logical examination – Ziehl-Neelsen staining – or cul-ture.
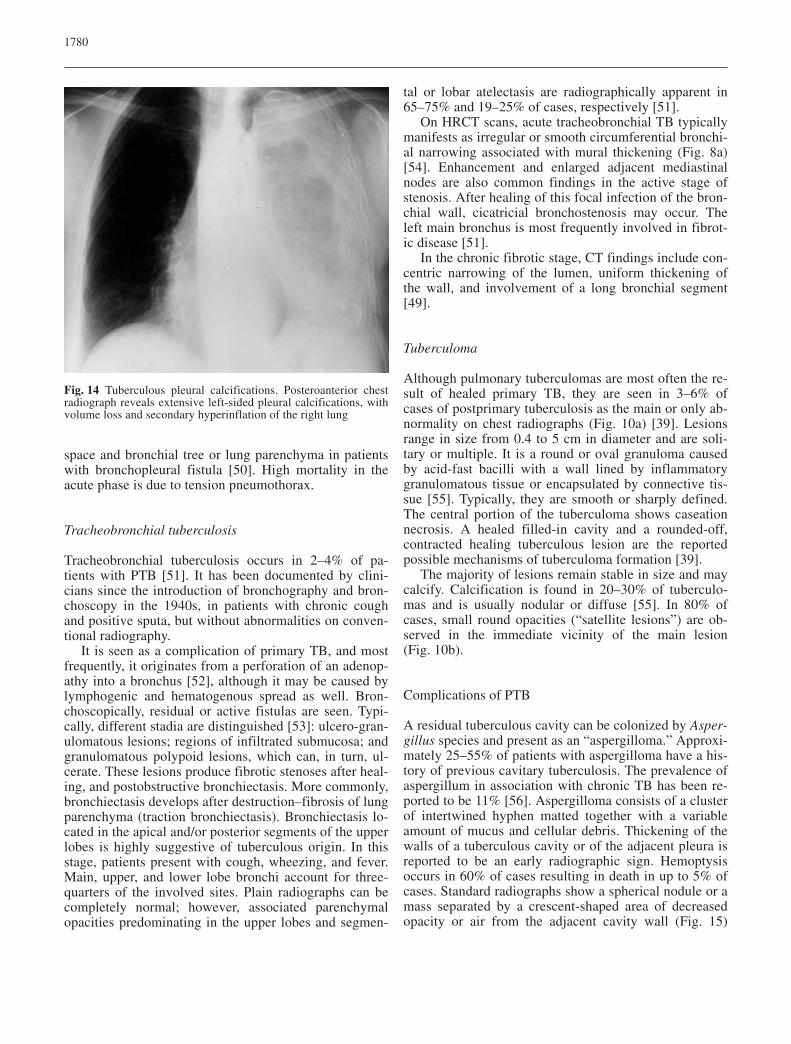
Although usually observed in association with paren-chymal and/or nodal disease, pleural effusion is the onlyradiographic finding indicative of primary TB in approx-imately 5% of adult cases [27]. Air-fluid level in thepleural space indicates presence of bronchopleural fistula[25]. Contrast-enhanced CT scan of patients with post-primary pleural effusion typically shows smooth thicken-ing of visceral and parietal pleura (“split-pleura” sign;Fig. 13) [47].
This entity is usually self-limited and prognosis isgood. Radiographically, sometimes a residual pleura-symphysis and pleural calcifications are seen (Fig. 14)[4].
Tuberculous pleurisy may become localized, causinga tuberculous empyema. This empyema may breakthrough the parietal pleura to form a subcutaneous ab-scess, so-called empyema necessitatis [48]. In chronictuberculous empyema, CT shows a focal fluid collectionwith pleural thickening and calcification and with orwithout extrapleural fat proliferation. Fibrothorax withdiffuse pleural thickening, but without pleural effusionon CT, suggests inactivity [49]. Empyema may alsocommunicate with the bronchial tree by bronchopleuralfistula. Diagnosis of bronchopleural fistula is based onan increasing amount of sputum production, air in thepleural space, a changing air–fluid level, and contralater-al spread of disease. Computed tomography demon-strates directly the communication between the pleural
1779
Fig. 12 Acute miliary tuberculosis, complicated by acute respira-tory distress syndrome. Posteroanterior chest radiograph reveals a“snowstorm” appearance with bilateral poorly circumscribed areasof consolidation
Fig. 13 Exudative tuberculous pleuritis. Contrast-enhanced CTscan shows a left-sided pleural effusion with enhancement of bothvisceral and parietal pleura (“split-pleura” sign)
space and bronchial tree or lung parenchyma in patientswith bronchopleural fistula [50]. High mortality in theacute phase is due to tension pneumothorax.
Tracheobronchial tuberculosis
Tracheobronchial tuberculosis occurs in 2–4% of pa-tients with PTB [51]. It has been documented by clini-cians since the introduction of bronchography and bron-choscopy in the 1940s, in patients with chronic coughand positive sputa, but without abnormalities on conven-tional radiography.
It is seen as a complication of primary TB, and mostfrequently, it originates from a perforation of an adenop-athy into a bronchus [52], although it may be caused bylymphogenic and hematogenous spread as well. Bron-choscopically, residual or active fistulas are seen. Typi-cally, different stadia are distinguished [53]: ulcero-gran-ulomatous lesions; regions of infiltrated submucosa; andgranulomatous polypoid lesions, which can, in turn, ul-cerate. These lesions produce fibrotic stenoses after heal-ing, and postobstructive bronchiectasis. More commonly,bronchiectasis develops after destruction–fibrosis of lungparenchyma (traction bronchiectasis). Bronchiectasis lo-cated in the apical and/or posterior segments of the upperlobes is highly suggestive of tuberculous origin. In thisstage, patients present with cough, wheezing, and fever.Main, upper, and lower lobe bronchi account for three-quarters of the involved sites. Plain radiographs can becompletely normal; however, associated parenchymalopacities predominating in the upper lobes and segmen-
tal or lobar atelectasis are radiographically apparent in65–75% and 19–25% of cases, respectively [51].
On HRCT scans, acute tracheobronchial TB typicallymanifests as irregular or smooth circumferential bronchi-al narrowing associated with mural thickening (Fig. 8a)[54]. Enhancement and enlarged adjacent mediastinalnodes are also common findings in the active stage ofstenosis. After healing of this focal infection of the bron-chial wall, cicatricial bronchostenosis may occur. Theleft main bronchus is most frequently involved in fibrot-ic disease [51].
In the chronic fibrotic stage, CT findings include con-centric narrowing of the lumen, uniform thickening ofthe wall, and involvement of a long bronchial segment[49].
Tuberculoma
Although pulmonary tuberculomas are most often the re-sult of healed primary TB, they are seen in 3–6% ofcases of postprimary tuberculosis as the main or only ab-normality on chest radiographs (Fig. 10a) [39]. Lesionsrange in size from 0.4 to 5 cm in diameter and are soli-tary or multiple. It is a round or oval granuloma causedby acid-fast bacilli with a wall lined by inflammatorygranulomatous tissue or encapsulated by connective tis-sue [55]. Typically, they are smooth or sharply defined.The central portion of the tuberculoma shows caseationnecrosis. A healed filled-in cavity and a rounded-off,contracted healing tuberculous lesion are the reportedpossible mechanisms of tuberculoma formation [39].
The majority of lesions remain stable in size and maycalcify. Calcification is found in 20–30% of tuberculo-mas and is usually nodular or diffuse [55]. In 80% ofcases, small round opacities (“satellite lesions”) are ob-served in the immediate vicinity of the main lesion(Fig. 10b).
Complications of PTB
A residual tuberculous cavity can be colonized by Asper-gillus species and present as an “aspergilloma.” Approxi-mately 25–55% of patients with aspergilloma have a his-tory of previous cavitary tuberculosis. The prevalence ofaspergillum in association with chronic TB has been re-ported to be 11% [56]. Aspergilloma consists of a clusterof intertwined hyphen matted together with a variableamount of mucus and cellular debris. Thickening of thewalls of a tuberculous cavity or of the adjacent pleura isreported to be an early radiographic sign. Hemoptysisoccurs in 60% of cases resulting in death in up to 5% ofcases. Standard radiographs show a spherical nodule or amass separated by a crescent-shaped area of decreasedopacity or air from the adjacent cavity wall (Fig. 15)
1780
Fig. 14 Tuberculous pleural calcifications. Posteroanterior chestradiograph reveals extensive left-sided pleural calcifications, withvolume loss and secondary hyperinflation of the right lung

[57]. On supine and prone positions, it is obvious thatthe nodule is often mobile.
Bronchogenic carcinoma and PTB often coexist, cre-ating a difficult diagnostic problem. Manifestations ofcarcinoma can mimic or can be misinterpreted as pro-gression of TB. Tuberculosis may favour the develop-ment of bronchogenic carcinoma by local mechanisms(scar cancer), or TB and carcinoma may be coincidental-ly associated. In addition, carcinoma may lead to reacti-vation of TB, both by eroding into an encapsulated focusand by affecting the patient’s immunity; therefore, anypredominant or growing nodule should be suspicious forcoexisting lung cancer in patients with TB [58].
Pulmonary arteries and veins in an area of active TBinfection may demonstrate vasculitis and thrombosis.Bronchial arteries may be enlarged in bronchiectasis as-sociated with TB or in parenchymal TB itself. In patientswith bronchiectasis, nodular and tubular structures there-fore are suggestive for hypertrophied bronchial arteries(Fig. 16) on HRCT scan. Spiral-CT angiography may bea useful technique to confirm these hypertrophied arte-ries.
A Rasmussen aneurysm is a pseudoaneurysm of apulmonary artery caused by erosion from an adjacent tu-berculous cavity [59]. A review of autopsy findings inpatients with a history of chronic cavitary TB showed aprevalence of Rasmussen aneurysms of 5%. Hemoptysisis the usual presenting symptom, which may be minimal,but also massive and life threatening. Arterial emboliza-tion has been demonstrated as an effective method toachieve control of bleeding.
Broncholithiasis is an uncommon complication,caused by rupture of a calcified pulmonary-peribronchialnode into an adjacent bronchus. Cough, wheezing, andrecurrent pneumonia can be presenting symptoms.
Right-sided lobar or segmental bronchi are most fre-quently involved [60]. CT scan shows a calcified lymphnode that is either endobronchial or peribronchial and isassociated with findings of bronchial obstruction, suchas atelectasis, obstructive pneumonitis, branching opaci-ties in V- or W-shaped configuration (obstructive bron-choceles), focal hyperinflation, or bronchiectasis [61].
The most common cause of esophageal TB is second-ary involvement from adjacent tuberculous adenitis. Itcan result in strictures (due to active granulomatous in-flammatory tissue and scar tissue after healing), inesophago-tracheobronchial or mediastinal fistulas, and intraction diverticulas [56]. The subcarinal region is pref-erentially involved, because of the anatomic proximity ofthe esophagus to the diseased lymph nodes. Presentingsymptoms may be fever, cough, dysphagia, and chestpain [62].
Tuberculous pericarditis is reported to complicate 1%of cases of TB. It is commonly caused by extranodal ex-tension of tuberculous adenitis into the pericardium dueto the close anatomical relationship between the lymphnodes and the posterior pericardial sac. The pericardiumcan also be involved in miliary spread of the disease. OnCT, adenopathies and a pericardial thickening (with orwithout effusion) is seen. Constrictive pericarditis withfibrous or calcified constrictive thickening of the pericar-dium of more than 3 mm occurs as a delayed complica-tion in approximately 10% of patients with tuberculouspericarditis [49].
Pneumothorax secondary to TB occurs in approxi-mately 5% of patients with postprimary TB, usually insevere cavitary disease. It heralds severe and extensive
1781
Fig. 15 Aspergilloma. Spot film of the left upper lobe. A nodularmass is seen within a thick-walled cavity in the left upper lobe.The residual air within the apical region of the cavity creates a so-called crescent air sign (arrow)
Fig. 16 Hypertrophied bronchial arteries associated with paren-chymal TB. Spot view of the right upper lung after selective bron-chial angiography reveals large, hypertrophied bronchial arterieswithin a pulmonary consolidation area
pulmonary involvement by the infectious process, andthe onset of bronchopleural fistula and empyema; there-fore, if any apical abnormality is seen after reexpansionof a spontaneous pneumothorax, active TB should beconsidered [63].
Tuberculous fibrosing mediastinitis is an uncommoncomplication and progresses insidiously without signifi-cant clinical symptoms. The mediastinal granulomatouslymph nodes coalesce, and the development of multipletuberculous granulomas creates both acute inflammatorychanges and reactive fibrosis in the mediastinum. TheCT findings include a mediastinal or hilar mass, calcifi-cation in the mass, tracheobronchial narrowing, pulmo-nary vessel encasement, and sometimes a superior venacava syndrome [64].
Tuberculous spondylitis (Pott’s disease) is a well-known complication and most commonly affects thelower thoracic and upper lumbar spine.
Atypical patterns
In developed countries, TB mainly affects the nonindige-nous population and risk groups of the indigenous popu-lation; among the latter, elderly patients constitute one-third of total TB prevalence, whereas they represent onlyone-tenth of the total population and an increase in TBincidence in elderly subjects is still to be expected. Fur-thermore, diagnosis is frequently delayed or even madepost mortem. Causes of this delayed diagnosis are non-specific symptomatology, negative tuberculin skin tests,atypical radiological presentations, and associated dis-eases mimicking TB [65, 66, 67, 68, 69].
It could be expected that elderly patients present withtypical radiological features of postprimary reactivationtuberculosis, i.e., apicoposterior infiltrates and cavitarydisease; however, because of the altered cellular immuneresponse in the ×, unusual pathogenetic mechanisms andatypical presentations for this age group may occur [70].Several factors may influence the pathogenesis of atypi-cal patterns in the elderly. Firstly, there is deficient cellu-lar immunity in the elderly subject that promotes reacti-vation TB (typical pattern). Secondly, an exogenic rein-fection or “second” primary infection can take place: el-derly patients may have outlived their initial infectingorganisms, as manifested by the negative tuberculin skintest, and become vulnerable to a “second primary infec-tion” [71]. Thirdly, elderly subjects can also be infectedfor the first time in their life. In cases of exogenic rein-fection or primary infection, a shift should be expectedfrom the usual pathogenetic pathway (reactivation) to anunusual pathway for adults, with a presentation similarto that found in children [72, 73, 74].
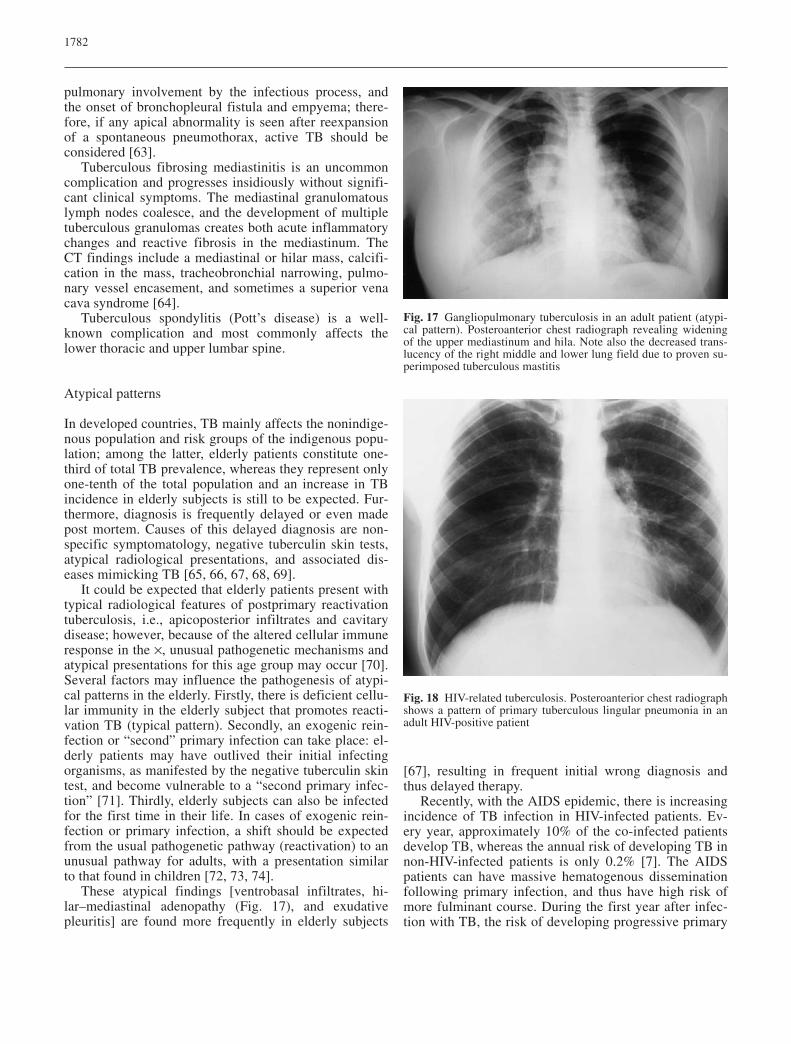
These atypical findings [ventrobasal infiltrates, hi-lar–mediastinal adenopathy (Fig. 17), and exudativepleuritis] are found more frequently in elderly subjects
[67], resulting in frequent initial wrong diagnosis andthus delayed therapy.
Recently, with the AIDS epidemic, there is increasingincidence of TB infection in HIV-infected patients. Ev-ery year, approximately 10% of the co-infected patientsdevelop TB, whereas the annual risk of developing TB innon-HIV-infected patients is only 0.2% [7]. The AIDSpatients can have massive hematogenous disseminationfollowing primary infection, and thus have high risk ofmore fulminant course. During the first year after infec-tion with TB, the risk of developing progressive primary
1782
Fig. 17 Gangliopulmonary tuberculosis in an adult patient (atypi-cal pattern). Posteroanterior chest radiograph revealing wideningof the upper mediastinum and hila. Note also the decreased trans-lucency of the right middle and lower lung field due to proven su-perimposed tuberculous mastitis
Fig. 18 HIV-related tuberculosis. Posteroanterior chest radiographshows a pattern of primary tuberculous lingular pneumonia in anadult HIV-positive patient

disease is almost 30%, in contrast with the 3% risk ofimmunocompetent patients [75]. Because of deficientcellular immunity, they are also prone to reactivation TB.Most of the TB infections in HIV patients are postprima-ry TB.
The radiographic appearance of HIV-associated PTBis dependent on the level of immunosuppression at thetime of overt disease [76]. In the early stages of dis-ease, radiographic findings are similar to those found inimmunocompetent patients [77]. At severe level of im-munosuppression, 10–20% of patients have normalchest films [78] or demonstrate findings usually associ-ated with primary disease, regardless of prior TB expo-sure status (Fig. 18) [70]. A miliary pattern of diseasehas also been reported to be associated with severe im-munosuppression [79]. Mediastinal and hilar adenopa-thy occur in 75% of cases [80]. Extrapulmonary local-izations are frequent in HIV-infected patients and in-volve brain, pericardium, intestine, peritoneum, andtestes. Cryptogenic miliary TB is the term used for pa-tients with normal chest films, positive sputum, anddisseminated TB [77].
Conclusion
Because of the global increase of TB incidence, especial-ly due to the AIDS epidemic and progressive increase ofthe geriatric population, the problem of TB has regainedactual importance.
There is a changing radiological pattern of PTB, withfading of the strict classical distinction between primaryand postprimary disease. Atypical presentations are nowseen, especially in HIV-infected and elderly subjects,e.g., exudative pleuritis in the elderly, gangliopulmonaryforms of TB in HIV-infected adults. This results in latediagnosis and delayed therapy.
Chest film is the mainstay in radiographic evaluationof suspected or proven PTB.
The HRCT scan has no impact on patient management,but typical findings should suggest diagnosis, e.g., tubercu-lous adenopathy (“rim sign”), tuberculoma, and endobron-chial TB (“tree-in-bud” sign). The CT evaluation may behelpful in determination of disease activity in some patients,but definitive diagnosis still requires isolation and identifi-cation of M. tuberculosis species in the clinical specimen.
1783
References
1. Styblo K (1989) Eradication of tuber-culosis in developed countries in theHIV era. Bull Int Union Tuberc LungDis 64:58–64
2. Snider GL (1997) Tuberculosis thenand now: a personal perspective on thelast 50 years. Ann Intern Med126:237–243
3. Rieder HL, Cauthen GM, Kelly GD et al. (1989) Tuberculosis in the UnitedStates. J Am Med Assoc 262:385–389
4. Gyselen A, Uydebroeck M, Weyler J(1992) Epidemiologie. In: Demedts M,Gyselen A, Van den Brande P (eds) Tuberculosis. Een blijvende uitdaging.Garant, Leuven-Apeldoorn, pp 17–30
5. Styblo K (1991) Epidemiology of tu-berculosis. Selected papers. KNCV24:1–136
6. Raviglione MC, Snider DE, Kochi A(1995) Global epidemiology of tuber-culosis. Morbidity and mortality of aworld-wide epidemic. J Am Med Assoc 273:220–226
7. Narain JP, Raviglione MC, Kochi A(1992) HIV-associated tuberculosis indeveloping countries: epidemiologyand strategies for prevention. TubercLung Dis 73:311–321
8. Bradford WZ, Daley CL (1998) Multi-ple drug-resistant tuberculosis. InfectDis Clin North Am 12:157–172
9. Agrons GA, Markowitz RI, Kramer SS(1993) Pulmonary tuberculosis in children. Semin Roentgenol28:158–172
10. Goodwin RA, DesPrez RM (1983)Apical localization of pulmonary tu-berculosis, chronic pulmonary histo-plasmosis and progressive massive fibrosis of the lung. Chest 83:801–805
11. Rich AR (1944) The pathogenesis oftuberculosis. Blackwell, Oxford
12. Bass JB Jr, Farer LS, Hopewell PC etal. (1994) Treatment of tuberculosisand tuberculosis infection in adults andchildren. American Thoracic Societyand The Centers for Disease Controland Prevention. Am J Respir Crit CareMed 149:1359–1374
13. Pratt PC (1979) Pathology of tubercu-losis. Semin Roentgenol 14:196–203
14. McAdams HP, Erasmus J, Winter JA(1995) Radiologic manifestations ofpulmonary tuberculosis. Radiol ClinNorth Am 33:655–678
15. Stead WW (1984) Tuberculosis in theelderly. J Am Geriatr Soc 32:82–83
16. Sutherland I, Svandova E, RadhakrishnaS (1982) Development of clinical tu-berculosis following infection with tu-bercle bacilli. Tubercle 63:255–268
17. Stead WW (1998) Tuberculosis amongelderly persons, as observed amongnursing home residents. Int J TubercLung Dis 2:S64–S70
18. Chaisson RE, Schecter GF, Theuer CP,Rutherford GW, Echenberg DF, Hopewell PC (1987) Tuberculosis inpatients with AIDS. Am Rev RespirDis 136:570–574
19. Palmer PE (1979) Pulmonary tubercu-losis: usual and unusual radiographicpresentations. Semin Roentgenol14:204–242
20. Fraser RG, Pare JAP (1989) Mycobac-terial infections of the lung. In: Fraser RG, Pare JAP (eds) Diagnosisof diseases of the chest. Saunders, Philadelphia, pp 614–642
21. Leung AN, Muller NL, Pineda PR,FitzGerald JM (1992) Primary tubercu-losis in childhood: radiographic mani-festations. Radiology 182:87–91
22. Kim WS, Moon WK, Kim IO et al.(1997) Pulmonary tuberculosis in chil-dren: CT evaluation. Am J Roentgenol168:1005–1009
23. Hartman TE, Primack SL, Muller NL,Staples CA (1994) Diagnosis of thorac-ic complications in AIDS: accuracyof CT. Am J Roentgenol 162:547–553
24. Im JG, Song KS, Kang HS et al. (1987)Mediastinal tuberculous lymphadenitis:CT manifestations. Radiology164:115–119
25. Woodring JH, Vandiviere HM,Fried AM, Dillon ML, Williams TD,Melvin IG (1986) Update: radiographicfeatures of pulmonary tuberculosis.Am J Roentgenol 146:497–506
26. Naidich DP, McCauley DI, LeitmanBS, Genieser NB, Hulnick DH (1984)CT of pulmonary tuberculosis. In:Siegelmann SS (ed) Computed tomog-raphy of the chest. Churchill Living-stone, New York, pp 175–217
27. Choyke PL, Sostman HD, Curtis AMet al. (1983) Adult-onset pulmonary tu-berculosis. Radiology 148:357–362
28. Weber AL, Bird KT, Janower ML(1968) Primary tuberculosis in child-hood with particular emphasis onchanges affecting the tracheobronchialtree. Am J Roentgenol Radium TherNucl Med 103:123–132
29. Kent DC, Elliot RC (1967) Hilar aden-opathy in tuberculosis. Am Rev RespirDis 96:439–450
30. Lamont AC, Cremin BJ, Pelteret RM(1986) Radiologic patterns of pulmo-nary tuberculosis in the paediatric agegroup. Paediatr Radiol 16:2–7
31. Van den Brande P, Demedts M (1992)Pulmonary tuberculosis in the elderly:diagnostic difficulties. Eur J Med1:224–229
32. Winer-Muram HT, Rubin SA (1990)Thoracic complications of tuberculosis.J Thorac Imaging 5:46–63
33. Kuhlman JE, Deutsch JH, Fishman EK,Siegelman SS (1990) CT features ofthoracic mycobacterial disease. Radio-graphics 10:413–431
34. Hadlock FP, Park SK, Awe RJ, RiveraM (1980) Unusual radiographic find-ings in adult pulmonary tuberculosis.Am J Roentgenol 134:1015–1018
35. Im JG, Itoh H, Han MC (1995) CT ofpulmonary tuberculosis. Semin Ultra-sound CT MR 16:420–434
36. Im JG, Itoh H, Shim YS et al. (1993)Pulmonary tuberculosis: CT findings –early active disease and sequentialchange with antituberculous therapy.Radiology 186:653–660
37. Wasser LS, Shaw GW, Talavera W(1988) Endobronchial tuberculosis inAIDS. Chest 94:1240–1244
38. Van den Brande P, Van de Mierop F,Verbeken EK, Demedts M (1990) Clin-ical spectrum of endobronchial tuber-culosis in elderly patients. Arch InternMed 150:2105–2108
39. Sochocky S (1958) Tuberculoma of thelung. Am Rev Tuberc 78:403–410
40. Im JG, Webb WR, Han MC, Park JH(1991) Apical opacity associated withpulmonary tuberculosis: high-resolu-tion CT findings. Radiology178:727–731
41. Proudfoot AT, Akhtar AJ, Douglas AC,Home NW (1969) Miliary tuberculosisin adults. Br Med J 2:273–276
42. Kwong JS, Carignan S, Kang EY,Muller NL, FitzGerald JM (1996) Mili-ary tuberculosis: diagnostic accuracyof chest radiography. Chest110:339–342
43. Leung AN (1999) Pulmonary tubercu-losis: the essentials. Radiology210:307–322
44. Webb WR, Müller NL, Naidich DP(2001) Diseases characterized primari-ly by nodular or reticulonodular opaci-ties. In: Webb WR, Müller NL, NaidichDP (eds) High-resolution CT of thelung. Lippincott Williams and Wilkins,Philadelphia, pp 319–321
45. Piqueras AR, Marruecos L, Artigas A,Rodriguez C (1987) Miliary tuberculo-sis and adult respiratory distress syn-drome. Intensive Care Med13:175–182
46. Hopewell PC (1995) A clinical reviewof tuberculosis. Radiol Clin North Am33:641–653
47. Yilmaz MU, Kumcuoglu Z, Utkaner G,Yalniz O, Erkmen G (1998) CT find-ings of tuberculous pleurisy. Int JTuberc Lung Dis 2:164–167
48. Glicklich M, Mendelson DS, Gen-dal ES, Teirstein AS (1990) Tubercu-lous empyema necessitatis: CT find-ings. Clin Imaging 14:23–25
49. Kim Y, Song KS, Goo JM, Lee JS,Lee KS, Lim TH (2001) Thoracic se-quelae and complications of tuberculo-sis. Radiographics 21:839–858
50. Westcott JL, Volpe JP (1995) Peripher-al bronchopleural fistula: CT evalua-tion in 20 patients with pneumonia,empyema or postoperative air leak. Radiology 196:175–181
51. Lee KS, Kim YH, Kim WS, HwangSH, Kim PN, Lee BH (1991) Endo-bronchial tuberculosis: CT features.J Comput Assist Tomogr 15:424–428
52. Auerbach O (1949) Tuberculosis of thetrachea and the major bronchi. Am RevTuberc 60:604–620
53. Smith L, Schillaci R, Sarlin R (1987)Endobronchial tuberculosis. Serial fi-beroptic bronchoscopy and natural his-tory. Chest 91:644–647
54. Moon WK, Im JG, Yeon KM, Han MC(1997) Tuberculosis of central airways:CT findings of active and fibrotic dis-ease. Am J Roentgenol 169:649–653
55. Lee KS, Song KS, Lim TH, Kim PN,Kim IY, Lee BH (1993) Adult-onsetpulmonary tuberculosis: findings onchest radiographs and CT scans. AmJ Roentgenol 160:753–758
56. Fraser RS, Müller NL, Colman N,Pare PD (1999) Diagnosis of diseasesof the chest. Saunders, Philadelphia,pp 798–873
57. Fraser RS (1993) Pulmonary aspergil-losis: pathologic and pathogenetic fea-tures. Pathol Annu 28:231–277
58. Snider GL, Placik B (1969) The rela-tionship between pulmonary tuberculo-sis and bronchogenic carcinoma: a to-pographic study. Am Rev Respir Dis99:229–236
59. Santelli ED, Katz DS, Gold-schmidt AM, Thomas HA (1994) Em-bolization of multiple Rasmussen an-eurysms as a treatment of hemoptysis.Radiology 193:396–398
60. Conces DJ Jr, Tarver RD, Vix VA(1991) Broncholithiasis: CT features in15 patients. Am J Roentgenol157:249–253
61. Adler O, Peleg H (1987) Computed to-mography in diagnosis of broncholithi-asis. Eur J Radiol 7:211–212
62. Im JG, Kim JH, Han MC, Kim CW(1990) Computed tomography ofesophagomediastinal fistula in tubercu-lous mediastinal lymphadenitis. J Com-put Assist Tomogr 14:89–92
63. Ihm HJ, Hankins JR, Miller JE,McLaughlin JS (1972) Pneumothoraxassociated with pulmonary tuberculo-sis. J Thorac Cardiovasc Surg64:211–219
64. Lee JY, Kim Y, Lee KS, Chung MP(1996) Tuberculous fibrosing mediasti-nitis: radiological findings. AmJ Roentgenol 167:1598–1599
65. McCray E, Weinbaum CM,Braden CR, Onorato IM (1997) Theepidemiology of tuberculosis in theUnited States. Clin Chest Med18:99–113
66. Alvarez S, Shell C, Berk SL (1987)Pulmonary tuberculosis in elderly men.Am J Med 82:602–606
67. Fulton JH et al. (1987) Tuberculosis:diagnostic difficulty in the elderly.J Clin Exp Gerontol 9:303–311
68. Bobrowitz ID (1982) Active tuberculo-sis undiagnosed until autopsy. AmJ Med 72:650–658
69. Van den Brande P, Vijgen J, DemedtsM (1991) Clinical spectrum of pulmo-nary tuberculosis in older patients:comparison with younger patients.J Gerontol Med Sci 46:M204–M209
70. Pitchenik AE, Rubinson HA (1985)The radiographic appearance of tuber-culosis in patients with AIDS and pre-AIDS. Am Rev Respir Dis131:393–396
71. Stead WW, Lofgren JP, Warren E, Thomas C (1985) Tuberculosis as anendemic and nosocomial infectionamong the elderly in nursing homes. N Engl J Med 312:1483–1487
72. Iseman MD (1980) Tuberculosis in theelderly: treating the “white plague”.Geriatrics 35:90–107
73. Korzeniewska-Kosela M, Krysl J,Muller N, Black W, Allen E, FitzGerald JM (1994) Tuberculosis inyoung adults and the elderly: a pro-spective comparison study. Chest106:28–32
74. Umeki S (1989) Comparison of young-er and elderly patients with pulmonarytuberculosis. Respiration 55:75–83
1784

75. Daley CL, Small PM, Schecter GF et al. (1992) An outbreak of tuberculo-sis with accelerated progression amongpersons infected with HIV. An analysisusing restriction–fragment–lengthpolymorphisms. N Engl J Med326:231–235
76. Goodman PC (1990) Pulmonary tuber-culosis in patients with AIDS. J ThoracImaging 5:38–45
77. Hopewell PC (1989) Tuberculosis andHIV infection. Semin Respir Infect4:111–122
78. Perlman DC, el-Sadr WM, Nelson ETet al. (1997) Variation of chest radio-graphic patterns in pulmonary tubercu-losis by degree of HIV-related immu-nosuppression. The Terry Beirn Com-munity Programs for Clinical Researchon AIDS (CPCRA). The AIDS ClinicalTrials Group (ACTG). Clin Infect Dis25:242–256
79. Raviglione MC, Narain JP, Kochi A(1992) HIV-associated tuberculosis indeveloping countries: clinical features,diagnosis and treatment. Bull WorldHealth Organ 70:515–526
80. Haramati LB, Jenny-Avital ER, Alterman DD (1997) Effect of HIV status on chest radiographic and CTfindings in patients with tuberculosis.Clin Radiol 52:31–35
1785

Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.