Embed Size (px)
DESCRIPTION
papilomatosis laring pada anak
Citation preview

GOOD AFTERNOON

DIAGNOSIS AND MANAGEMENT OF
JUVENILE-ONSET LARYNGEAL PAPILLOMATOSIS
SCIENTIFIC ADVISORDR. I GDE ARDIKA NUABA,SP.THT-KL [K]
PUTU DEWI PRAMUSITA

INTRODUCTION
A common proliferative benign tumor in children
It is also known as respiratory papillomatosis It is also known as respiratory papillomatosisor recurrent respiratory papillomatosis
Divided into 2 categories :
• Juvenile-onset laryngeal papillomatosis
• Adult-onset laryngeal papillomatosis

INTRODUCTION
Donalus (17th Century) : warts in the throat
McKenzie (19th Century) : laryngeal papilloma McKenzie (19th Century) : laryngeal papilloma
Ullman (1923) : virus as the etiology
1982 : HPV is identified
Most often : HPV types 6 & 11

INTRODUCTIONjuvenile-onset laryngeal papillomatosis
The most common laryngeal neoplasm identified in children
♂ : ♀ = 1: 1 ♂ : ♀ = 1: 1
Diagnosis is based on anamnesis, physical examination, biopsy, and other ancillary services
Management modalities are surgery and adjuvant therapies

INTRODUCTIONjuvenile-onset laryngeal papillomatosis
obstruction of the airway, high recurrent rate, no single effective modality of therapy &
complications
potential for morbid consequences
acknowledgement of
diagnosis & management is a necessity

EMBRIOLOGY OF LARYNX
Basic Otorhinolaryngology : A Step by Step Learning Guide, 2006
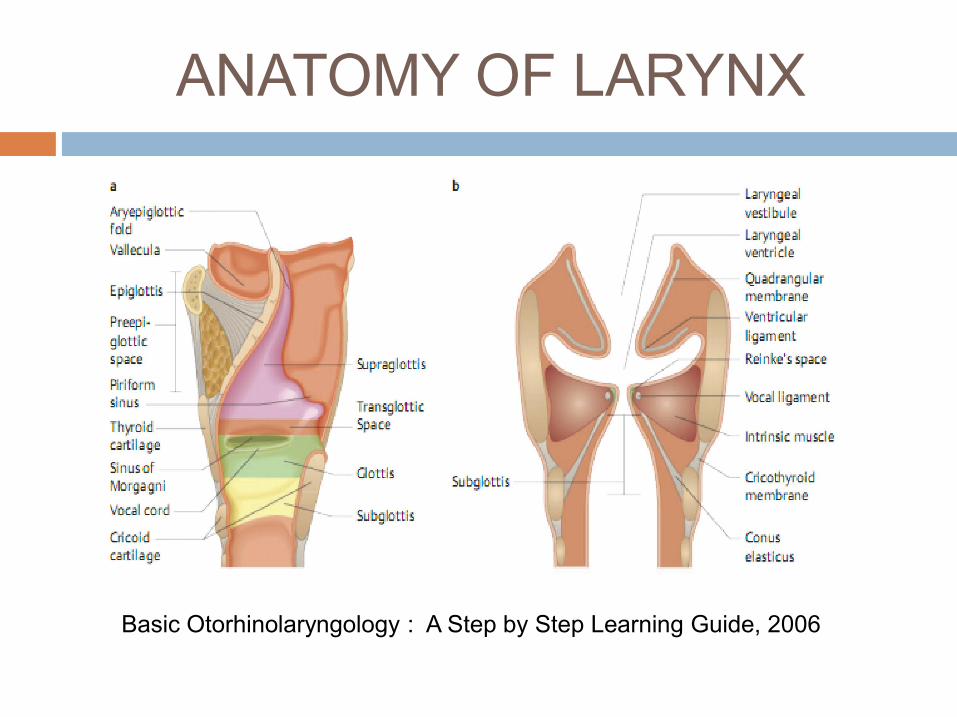
ANATOMY OF LARYNX
Basic Otorhinolaryngology : A Step by Step Learning Guide, 2006

EPIDEMIOLOGY
The most common laryngeal neoplasm & second most frequent cause of hoarseness in children
Diagnosed at 2-4 years old ( 75% are Diagnosed at 2-4 years old ( 75% are diagnosed before 5 years old), with a 1-year delay in diagnosis
Estimated 1500-2500 new cases/year in USA
Incidence (USA ): 4,3/100.000 children whom requires over 15.000 surgeries & US $ 100 million per year

EPIDEMIOLOGY
♂ : ♀ = 1: 1
A mean number of 19,7 surgeries/children (4,4/year) in USA
Children diagnosed before 3 years old are :
• 3,6 times more likely to require more than
4 surgery/year
• 2,1 times more likely to have 2/more
anatomic sites affected after 4 years old

EPIDEMIOLOGY
younger children whom affected & diagnosed
are often :
• with disease progression
• have persistent disease
• experience increased number of surgeries
in the 1st year following diagnosis

ETIOPATHOGENESIS
HPV type
6 & 11
lesions on respiratory tract

ETIOPATHOGENESIS
HPV
• Non enveloped icosahedral capsid• Non enveloped icosahedral capsidvirus
• Double stranded circular DNA 7900 base pair long
• 3 regions : upstream regulatory, early and later

ETIOPATHOGENESIS
ETIOPATHOGENESIS
lesions on respiratory tract
• Sessile / exophytic• Sessile / exophytic• Pink / white• Pedunculated masses with fingerlike
projections of non-keratinized stratified squamous epithelium
• Supported by a core of highly vascularized connective tissue stroma

ETIOPATHOGENESIS
lesions on respiratory tract
• Basal layer normal / hyperplastic with mitotic figures
• Basal layer normal / hyperplastic with mitotic figures
• Cellular differentiation is abnormal• Degree of atypia sign of premalignant
tendency• HPV type 11 more obstructive airway
early in the disease & greater need for tracheotomy

ETIOPATHOGENESIS
common anatomic sites
where ciliated & squamous epithelium are juxtaposed
• Limen vestibuli• Nasopharyngeal surface of soft palate• Midline laryngeal surface of epiglottis• Upper & lower margins of the ventricle• Undersurface of vocal folds• Carina• Bronchial spurs

ETIOPATHOGENESIS
Laryngeal Papillomatosis

ETIOPATHOGENESIS
Histopathology of Laryngeal Papillomatosis

TRANSMISSION
Remains unclear
Several studies linked juvenile-onset laryngeal Several studies linked juvenile-onset laryngeal papillomatosis to mothers with genital HPV infection (vertically through birth canal)
Kashima : more likely to be first born & vaginally delivered

PREDISPOSITION FACTORS
Child whose mothers are with genital condylomatascondylomatas
Child with bronchopulmonary dysplasia who needs prolonged endotracheal intubation

DIAGNOSIS
• History of the patientAnamnesis
• Signs and symptoms• Indirect laryngoscopy
Physical examination
• Histopathology• Identification of HPV &
extention of lesions
Biopsy and Other ancillary
services
DIAGNOSIS
ANAMNESIS & PHYSICAL EXAMINATION
triad of progressive hoarseness, stridor, and respiratory distress
other symptoms :
hoarseness + obstructive
airway symptoms laryngoscopy
inspiratory stridor biphasic
other symptoms :
chronic cough, recurrent
pneumonia, failure to thrive,
dyspnea, dysphagia

DIAGNOSIS
ANAMNESIS & PHYSICAL EXAMINATION
• when respiratory distress is absent : careful history of onset, possible airway trauma, history of onset, possible airway trauma, characteristic of the cry
• Subglottic lesion : low/high-pitched, coarse, fluttering voice
• Glottic lesion : high-pitched, cracking voice, aphonia
• Neonatus with stridor consider papillomatosis

DIAGNOSIS
PHYSICAL EXAMINATION & BIOPSY
• Thorough & organized examination • Thorough & organized examination • Frequent visits to establish agressiveness• Evaluation of : signs of respiratory distress, level of
obstruction, level of oxygenation• Clinic setting / operating room setting• With indirect laryngoscopy : rigid / flexible (flexible
is considered superior to rigid)• Biopsy is the gold standard

DIAGNOSIS
OTHER ANCILLARY SERVICES
• Identification of HPV on lesions : IHC, isolation of DNA virus, in situ hybridisation, PCR
• Chest X-Ray & CT Scan of neck & chest : will demonstrate extent of the lesions

STAGING
Most clinicians find that tracking a child’s disease progression in a uniform protocol is necessarynecessary
A such universal yet simple protocol is not yet accepted
Coltrera & Derkay have proposed a staging system to overcome the issue

STAGING ASSESSMENT FOR RECURRENT LARYNGEAL PAPILLOMATOSIS
Patient initials__ Date of Surgery__ Surgeon__ Patient ID#___Institution__
1. How long since the last papilloma surgery? __days,__weeks,__months,__years,__don’t know,__this is the child first surgery
2. Counting today’s surgery, how many papilloma surgery in the past 12 months? ___
3. Describe the patient’s voice today:Normal__ (0), abnormal__ (1), aphonic__ (2)Normal__ (0), abnormal__ (1), aphonic__ (2)
4. Describe the patient’s stridor today:Absent__ (0), present with activity__ (1), present at rest__ (2)
5. Describe the urgency of today’s intervention: Scheduled__(0), elective__ (1), urgent__ (2), emergent__ (3)
6. Describe today’s level of respiratory distress: None__ (0), mild__(1), moderate__(2), severe__(3), extreme__(4)
Total score for questions 3-6=_______________

FOR EACH SITE, SCORE AS 0=NONE, 1=SURFACE LESION, 2=RAISED LESION, 3=BULKY LESION
LARYNX: Epiglottis
Lingual surface__laryngeal surface__Aryepiglottic folds right__ left__False vocal folds right__ left__True vocal folds right__ left__Arytenoids right__ left__Anterior commisure ___Anterior commisure ___Posterior commisure ___Subglottis ___
TRACHEA: Upper one-third ___Middle one-third ___Lower one-third ___Bronchi right__ left__Tracheotomy stoma___

FOR EACH SITE, SCORE AS 0=NONE, 1=SURFACE LESION, 2=RAISED LESION, 3=BULKY LESION
OTHER:Nose ___Palate ___Pharynx ___Esophagus ___Esophagus ___Lungs ___Other ___
TOTAL SCORE ALL SITES :_____
TOTAL CLINICAL SCORE :_____

DIFFERENTIAL DIAGNOSIS
Laryngotracheobronchitis
Asthma
Laryngomalacia
Vocal fold paralysis
Vocal fold nodules
Congenital laryngeal cyst

MANAGEMENT
No single effective modality of therapy
Recent modalities: surgery & adjuvant therapies
When respiratory distress is present When respiratory distress is present tracheotomy probably necessary to secure the airway
Several experts : tracheotomy should be avoided & decannulation as soon as the disease is managable by endoscopic procedures

MANAGEMENT
SURGERY
• Goals : optimal erradication of papillomatosis, preservation of normal structures, maintain voice qualityquality
• In aggressive disease : reducing disturbances due to tumor, reducing extention rate, maintain patency of airway, increasing time interval between procedures
• Modalities : forceps, CO2 laser, phonomicrosurgical, KTP/Nd:YAG laser, flash scan laser, microdebrider

MANAGEMENT
Forceps
Early modality
CO2 laser
Favored over cold instruments
Emission wave length of 10.600 nm
Controlled destruction of pathologic tissue & hemostasis
Convert light to thermal energy vaporizes the lesions
Several procedures & intervals
Beware of potential post op scar formation

MANAGEMENT
Phonomicrosurgical
Cold steel excision + principles of phonomicrosurgery, submucosal infusion & phonomicrosurgery, submucosal infusion & microinstrumentation minimize the risk of scar formation
KTP/Nd:YAG laser
532 nm wave
Found to be safe & effective

MANAGEMENT
Flash scan laser
Good early result
Microdebrider Microdebrider
Quickly debulking laryngeal papilloma
Smaller shaver blades (< 2 mm)
Reduced laryngeal scarring, adding safety compare to CO2 laser, shorter operating time, less expense
MANAGEMENT
ADJUVANT
> 4 surgeries/year, distal multisite spread &/or rapid regrowth with airway compromise
• Cidofovir• Cidofovir• Interferon α
• Photodynamic• Indole-3-carbinol• Acyclovir• Chemoterapy & hormon therapy

MANAGEMENT
Cidofovir
Most commonly recommended
Apoptosis induction on HPV-positive cellsApoptosis induction on HPV-positive cells
Improve airway & increase interval period
Nefrotoxicity & carcinogenesis
Repetitive procedures increase risk of airway compromise, cost, and morbidity

MANAGEMENT
Interferon αProteins manufactured by cellsEnzymes block DNA & RNA virus
replication + altering cell membrane less susceptible to viral penetrationsusceptible to viral penetration
The exact mechanism remains unclearSide effects : acute & chronic reactionsDose: 5 million unit/m2 (s.c) for 28 days 3
days/week for at least 6 months if excellent response, severe side effects 3 million unit/m2 days per week & slow weaning afterward

MANAGEMENT
Photodynamic
Transfer of energy to a photo-sensitive drug (dyhematoporphyrin ether/DHE)
Dose : 4,25 mg/kg (iv) prior to photoactivationwith argon pump dye laser
Significant decrease of disease growth
Drawback : markedly photosensitive for 2-8 weeks

MANAGEMENT
Indole-3-carbinol (I3C)
dietary supplement (high concentration in cabbage,brocoli, cauliflower)cabbage,brocoli, cauliflower)
inhibit papilloma formation in mice
dosage of active drug in human is still a controversy

MANAGEMENT
Acyclovirdependent on the precense of thymidine
kinase coded by virus still unknown for HPV, but conflicting clinical still unknown for HPV, but conflicting clinical
results in several studies (+) may be effective when there are codisease
factors
Chemoterapy & hormonal therapy not yet proven to be effective

MANAGEMENT
VACCINE
• Quadrivalent vaccine (HPV type 6,11,16,18) is undergoing phase III clinical studies
• Goal : a reduction in the susceptibility of neonates to the virus among vaccinated mothers

COMPLICATIONS
MORBID CONCEQUENCES
AIRWAY OBSTRUCTION
PROGRESSION TO SCC

COMPLICATIONS
• Distal spreading to trachea (±26%)
• Distal spreading to bronchi & lungs (±5%)
AIRWAY OBSTRUCTION
lungs (±5%)
• Rare• Commonly with lungs involvement• Etiology of progression is still
unknown
PROGRESSION TO SCC

COMPLICATIONS
COMPLICATIONS DUE TO SURGERY
• Pneumothorax• Pneumothorax• Tracheal or lung injury• Posterior glottic stenosis• Anterior glottic stenosis• Subglottic stenosis• Tracheal stenosis

PROGNOSIS
Is unpredictable
Significance recurrence rate (70%)
Most children require surgical procedures as often as 1 every 2-4 weeks (total of average 150 times before adolescent)

PROGNOSIS
Most children whom severely affected are with complications
Laryngeal papillomatosis in neonatus has a poor prognosisa poor prognosis
Death is often associated with complications caused by surgical procedures and distal course of disease’ spreading

PROGNOSIS
careful & sequential inspections are necessary to establish
the disease’ aggressivenessthe disease’ aggressiveness
• Some clinicians conduct it at their clinic• Others suggest early routine bronchoscopy in
operating theatre with 4-6 weeks interval in children with presumably aggressive disease

DISCUSSION
Proliferative benign tumor
Age 1 day to 84 years old
Quite common in children Quite common in children
Synonim : respiratory papillomatosis or recurrent respiratory papillomatosis
Divided into 2 categories :
• Juvenile-onset laryngeal papillomatosis
• Adult-onset laryngeal papillomatosis
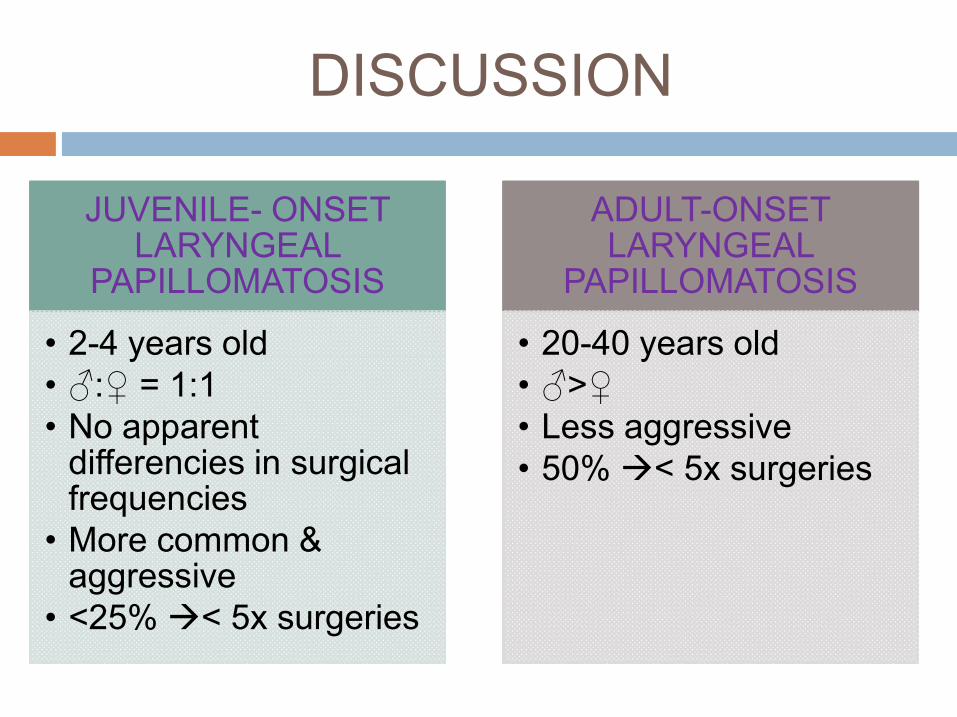
DISCUSSION
JUVENILE- ONSET LARYNGEAL
PAPILLOMATOSIS
• 2-4 years old
ADULT-ONSET LARYNGEAL
PAPILLOMATOSIS
• 20-40 years old• 2-4 years old• ♂:♀ = 1:1• No apparent
differencies in surgical frequencies
• More common & aggressive
• <25% < 5x surgeries
• 20-40 years old• ♂>♀• Less aggressive• 50% < 5x surgeries

DISCUSSION
AGENT
• HPV type 6 & 11• Transmission is presumably vertically through birth
canal from mothers with genital HPV infection• More likely to be first born & vaginally delivered
because of long second stage of labor (Kashima)

DISCUSSION
AGENT
• Risk of a child contracting the disease from a mother with active condylomatous lesion & vaginally delivered = 1/400 (Shah, et al)
• In utero process & SC not yet proven to be effective to overcome the issue
NEEDS FURTHER RESEARCH

DISCUSSION
Hallmark of anamnesis : triad of progressivehoarseness, stridor, respiratory distress
Thorough, organized, frequent examination in clinical / operating room setting clinical / operating room setting
Examination with indirect laryngoscopy : flexible is considered superior to rigid
Biopsy is the gold standard
Coltrera & Derkay staging system : unified protocol to evaluate disease progression

DISCUSSION
Frequently detected after signs of respiratory distress are present need for tracheotomy
Prolonged tracheotomy + subglottic papilloma Prolonged tracheotomy + subglottic papilloma higher risk for distal spreading
Therefore tracheotomy should be avoided

DISCUSSION
When tracheotomy can not be avoided decannulation as soon as disease is managed by endoscopic proceduresby endoscopic procedures
Other studies : tracheotomy do not lead the spread
Other extralaryngeal structures which most affected : oral cavity, trachea, bronchi

DISCUSSION
THERAPY
• No single effective modality of therapy• No single effective modality of therapy• Surgery procedures requires skilled team &
properly equipped facility• Primary goals : optimal erradication of
papillomatosis, preservation of normal structures, & maintain voice quality
• Recently microdebrider is more favorable to CO2 laser

DISCUSSION
THERAPY
• Adjuvant therapy is required in ± 20% of all cases
• Frequently recommended : cidofovir & interferon-α
• Consideration on adjuvant therapy : indication & side effects
CONCLUSION
Juvenile-onset laryngeal papillomatosis is a disease with potential morbid consequences
No single effective modality of therapy
On-progress current modalities of therapy are On-progress current modalities of therapy are surgery and adjuvant therapies
Future research on its clinical course and predisposition factors are still needed
Alert, supportive, and educated parents or family is invaluable to the child’s safety

THANK YOU