Embed Size (px)
Citation preview

PEDIATRIC ANEMIAS
Gábor Kovács MD, PhD
Semmelweis University
2nd Dep. of Pediatrics


Diagnosis of anemia
Age Hemoglobin (g/l)
6 mo - 2 years < 100
< 110
6 - 14 years < 120
Adult women < 120
Adult man < 130
2 - 5 years

CLASSIFICATION OF ANEMIAS
MICROCYTAER
HYPOCHROM
NORMOCYTAER
NORMOCHROM
MACROCYTAER
(MCV<75 fl
MCH<27 pg)
(MCV 75-90 fl
MCH>26 pg)
(MCV>90 fl)
Iron deficiency hemolysis megaloblastosis
(B12-, folic acid def.)
Thalassemia secunder anemia alcohol, liver disease
Chronic. Illnes Blood loss MDS, aplastic anemia
Plumb intox. Bone marrow insuff. CDA
sideroblastyc (B6) Renal failure gravidity, myxoedema

Reticulocyte
Increased: hemolytic anemias, blood loss,
regeneration
Decreased: bone marrow diseases,
erythropoietine deficiency, other
deficiencies (iron, Vitamin B12, folic acid)
„Normal”: ineffective erythropoesis
(thalassemia, MDS, CDA, myelofibrosis),
chr. inflammation, malignancy

RDW
Red cell distribution width (SD)
Normal: 10-14 %
increased: iron deficiency, cong. membrane
disorders, burn, thrc. aggregation-s./DIC

Microcytaer anemias
Iron Protoporphyrine
iron deficiency anemia
chr. infection sideroblastic
malignancy anemia
thalassemia
Hem + globin
Hemoglobin

DD of hypochrom (mikrocytaer)
anemias
iron def. inf, tumor thalassemia siderobl.
MCV
MCH
MCHC
all
decreased
slightly
decreased
all
decreased
decreased
(MCV might
be increased)
SeFe decreased decreased norm. increased
TVK increased decreased norm. norm.
ferritin decreased norm. or
increased
norm. increased
iron reserve decreased norm. or
increased
norm. norm. or
increased
Hb electro-
phoresis
norm. norm. pathol. norm.

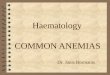
Thalassemia

Thalassemia


Iron deficiency anemia

Hypochrom anemia
(iron deficiency)

Daily iron requirement
4 mo - 1 year 1.0 mg
2 - 10 years 0.5-1.0 mg
Puberty 2.0 mg
Adult man 1.1 mg
Adult women 2.4 mg
Pregnant women -6 mg

Stages of iron deficiency
Iron depot
Transport
iron
Hb-iron
Normal iron homeostasis:
Malt train med II/3

Stages of iron deficiency
Prelatent iron deficiency:
Iron stores
are empty
Decreased serum ferritine; decreased
transferrine saturation; increased IBC;
hemoglobin normal
Iron depotTransport iron
Hb-iron
Malt train med II/5

Stages of iron deficiency
Latent iron deficiency:
Transport
iron
decreased
Decreased serum ferritine; decreased transferrine
saturation; decreased serum iron, increased IBC;
increased erythrocyte protoporphyrine, hemoglobin
normal
Iron depotTransport iron
Hb-iron
Malt train med II/6

Stages of iron deficiency
Iron deficiency anemia:
Iron depotTransport iron
Hb-iron
Microcytaer, hypochrom anemia
Malt train med II/7
Decreased serum ferritine; decreased transferrine
saturation; decreased serum iron, increased IBC;
increased erythrocyte protoporphyrine, decreased
hemoglobin and MCH

Iron deficiency
Hb low
MCV<75 fl
MCH<27 pg
RDW>14 %
Anisocytosis
Thr>400
No infections
+ anamnesis
PS: in Down-s: MCV and MCH higher

Iron def.

Significance of iron
Important for the synthese of
hemoglobin and myoglobin.
Basic for the oxydative phosphorilation
(energy supply).
Important for the normal mental
functions and for the immune system.

The dopaminerg system
normal: Iron def.:
D-2 rec. sensitivity
dopamine effect
opiate effect
Learning
capacity
dopamine
opiate effect
Learning
capacity
Malt train med II/46

Iron and the immune system
Iron def.
Lymphocyte proliferation
Interleukin-2
Immune response
Malt train med II/54

Causes of iron deficiency 1.
Decreased iron intake:
Nutritional intake insufficient: not
enough iron in the meal, breast-feeding
after 6 months.
Decreased absorption: gastrointestinal
diseases, malabsorption

Causes of iron deficiency 2.
Increased iron need:
Chronic blood loss: ulcus, varix, GI
malignancy, colitis, diverticulosis,
menstruation, parasitosis, hematuria.
Increased need: prematurity, growth,
gravidity, breast feeding.
Acute bleedings: Hemorrhagic
diathesis, coagulation disorders.

Incidence of iron deficiency - USA
•Infants: 14 %
•3-5 y: 4 %
•Adolescents (girls): 9-11 %
•Women, 20-49 y: 9 %

AAP guideline 2010
Preterm infants
1 mo-12 mo: 2 mg/kg Fe/day
(drug or Fe-rich formula)
Pediatrics: 2010, 126: 1040-1051

AAP guideline 2010
Brest-feeding infants
>4 mo: 1 mg/kg/day extra Iron
Until, half of the daily food is Fe-rich-
food or Fe-rich-formula

AAP guideline 2010
Formula-feed infants
Need: 10-11 mg/day iron
In formula Iron m in. 10-12 mg/l
Until, half of the daily food is Fe-rich-
food.
NO cow milk until 1 year!!

AAP guideline 2010
1-3 years
Daily need: 7-8 mg
Iron-rich food!
Screening at 1 year: ferritin, CRP, Hb
Later screening: for risk groups (14 %)

Risk groups
•Preterm infants, SGA newborns
•Only breast feeding after 4 mo (!)
•Cow milk <1 y
•Low iron intake
•Growth retardation
•Nutritional and absorption
problems
•Girls at puberty, heavy menses
bleedings

AAP guideline 2011 for adolescents
12-15 y: 9 % iron deficiency, 2 % anemia
26-29 y: 11 % iron deficiency, 3 % anemia
Boys< 1 % (more iron needed at puberty)
Risk group: strong menses bleeding, chr.
illness, malabsoprtion, obesity, sportsmen,
veggie diet (veganism)

AAP guideline 2011 for adolescents
Daily need: 9-13 y: 9 mg, 14-18 y: girls 15
mg, boys 11 mg
Gravid adolescents: 27 mg
For girls: yearly blood picture vérkép
(ferritin, CRP, Hb)! (in boys only 1x)
If Hb< 110 g/l, treatment!!: 3-6 mg/kg
per os iron

Treatment of iron deficiency
Malt train med II/40

Treatment of iron deficiency 1.
Disadvantage: gastrointestinal
intolerance (nausea, vomitus, diarrhoea,
obstipation)
Uncontrolled absorption.
Benefit: cheap, good absorption,
quick effect.
Iron-salts (sulfate)

Receptor-mediated, controlled absorption.
Advantage:
Few side effects.
Decreased risk for free radicals.
But slower and lower effect!
Iron-carbohydrate-complex
Treatment of iron deficiency 2.

Iv: 1-2 mg/kg/d for 5 days
Dose: 5-6 mg/kg/d orally
Timing: orally for 4-6 months (!)
Treatment of iron deficiency 3.


Normocytaer anemias

Classification of anemias 2.
B. Hemolysis
1. Intracorpuscular or intrinsic
membrane-defects (spherocytosis, elliptocytosis,
stomatocytosis PNH)
hemoglobinopathy (sickle cell anemia, thalassemia)
enzyme-defekts (pentóz-monofoszfát ciklus
zavarai, glutation szint. zavarai)

Classification of anemias 3.
B. Hemolysis
2. Extracorpuscular or extrinsic
immunmechanisms:
natural isoagglutinins (transzfusion rection)
aquired antibodies (autoimmun hemol. anemias)
drugs
infection diseases (mononucleosis, mycoplasma)
autoimmune or malignant diseases

Clinical signs of hemolysis
Pallor, collapse
Icterus
Splenomegaly
Cholelithiasis
Others: ulcus cruris, aplastic crisis, cyanosis, cardiopulmonal dysfunktion, colica, waist pain, fever, adenopathy,
Emergency!!!

Laboratory signs of hemolysis
serum indirect bilirubin increased
urinary urobilinogene increased
hemoglobinuria
serum haptoglobine decreased
reticulocytosis (10-20%)
elevated serum LDH
fragmented RBC-s
erythroid hyperplasia in the bone marrow

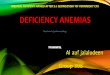
Spherocytosis

Elliptocytosis

Stomatocytosis

Sickle cell disease

Cold agglutination

RBC fragmentation (DIC)

Treatment of hemolytic anemias
Spherocytosis – ery transfusions, splenectomy
Immune hemolysis – IVIG (warm AIHA),
steroid, rituximab (cold AIHA)
Sickle cell – fluid, analgetic
Thalassemia: transfusion, chelate, BMT
DIC – fresh frozen plasma (+treatment of the
etiology)

Drug-induced hemolysis
Immune complex binding
quinine, phenacetin
Drug-adsorption
penicillin, cefalosporins
Non-specific adsorption
Membrane disturbances, decreased ery
lifespan
Auto-antibodies (Coombs positive)
alfa-metildopa, pentostatin, fludarabin,
tacrolimus, alfa-interferon

Other secunder hemolytickus állapotok
INFECTIONS
malária, clostridium, viruses
CHEMICAL, PHYSICAL FACTORS
drugs, chemicals, heavy metals (lead, cupper,
iron), burn
SECUNDER
liver-, kidney diseases

SUMMARY
All non-mikrocyter anemia should
be treated in hematological centers!
All microcyter anemia, not-
responding for a 2-4 weeks of iron
therapy, should be admitted to the
center!


Macrocytaer anemias

Macrocytosis

Bone marrow insufficiency
Hypoplastic anemia: only anemia
(decreased erythropoesis)
Aplastic anemia: pancytopenia (decreased
erythro-, myelo, thrombopoesis)

Cong. aplastic anemias
Fanconi anemia
Dyskeratosis congenita
Shwachmann-Diamond s.
Constitucional aplastic anemia

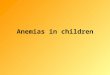
Fanconi anemia
DNS repair defect
(AR, chr. 9 and 20)
Multiple anomalies:
growth stunting,
ment. ret, bone,
kidney, heart, gonad,
skin pigmentation


Dyskeratosis congenita
X-rec. inheritance
In 90% aplastic anemia
Nail dystrophy, mucosal leukoplakia,
hyperpigmentation etc.
Mental retardation
Frequent carcinom

Dyskeratosis congenita

Shwachman-Diamond sy.
AR inheritance
Neutropenia
In 25% aplastic anemia
Metaphyseale chondrodysplasia
Exocrine pancreas insufficiency

Hypoplastic anemias
Cong. red cell aplasia (Diamond-
Blackfan anemia)
Transient eryhtroblastopenia
Parvovirus-induced eryhtroblastopenia
Pure red cell aplasia

Diamond-Blackfan anemia
AD, AR inheritance
Anemia in the 1st year of life
Cong. malformations in 25 %
Normochrom, macrocyter anemia, low
reticulocyte, HbF and EPO increased
In the BM: E:M=1:50


Treatment of congenital anemias
glucocorticoid
ATG
Bone marrow transplantation