Embed Size (px)
Citation preview
Delivering Dignity in North Lancashire
Final Report
By Dr Laurence Clark
August 2015
1
Table of Contents
Introduction................................................................................3
Evaluation..................................................................................5
Appreciative Inquiry...................................................................6
Coaching and Mentoring............................................................7
Welcome Values.......................................................................11
Conclusions..............................................................................21
Recommendations...................................................................23
Appendix 1: Definitions of Dignity............................................24
Appendix 2: Delivering Dignity Audit Survey...........................29
Appendix 3: Workshop Dates...................................................56
2
IntroductionAs part of the “Delivering Dignity in North Lancashire” agenda, this project looked at how to improve standards in the care and support of older people. Lancashire County Council and the Clinical Commissioning Groups in North Lancashire worked together to raise awareness of dignity and embed a person-centred ethos across all settings.
Pathways Associates were commissioned to deliver this initiative. A number of distinct pieces of work were delivered:
An overview of the various definitions and understandings of dignity in relation to health and social care (included in appendix 1).
An audit questionnaire around person-centred approaches which was sent to all providers of care and support services to older people in North Lancashire. The providers’ responses are included in appendix 2.
A Delivering Dignity Launch Event which was held at Kirkland and Catterall Memorial Hall on 16 July 2013. It was attended by a total of 25 representatives from providers (although 31 booked to come).
Four Appreciative Inquiry (AI) sessions have been delivered, although more were planned and subsequently cancelled due to poor take-up. Appreciative Inquiry “begins by identifying what is positive and connecting to it in ways that heighten energy and vision for change.…AI recognizes that every organization is an open system that depends on its human capital to bring its vision and purpose to life… The outcome of an AI initiative is a long-term positive change in the organization… AI is important because it works to bring the whole organization together to build upon its positive core.”1 The project delivered AI sessions with 2 providers, Unlimited Care Ltd (4 people with staff) and ARC Community Care (10 people with
1 Cooperrider, David L; Whitney, Diana; and Stavros, Jacqueline M., Appreciative Inquiry Handbook: The First in a Series of AI Workbooks for Leaders of Change, Lakeshore Communications, 2003, Pages XVII – XIX
3

families). It also worked with 2 coaches who then ran an AI event in their own organisations with support.
Three coaching and mentoring cohorts were established. Each cohort attended a series of 6 monthly half-day sessions which explored coaching tools and person-centred approaches to bringing better outcomes for older people. Participants were expected to sign up for all the 6 sessions and co-deliver a small workshop with the focus on the continued development of dignity with the lead coach. Sessions were aimed at managers / owners / supervisors to enable them to develop dignity through team meetings and supervision. Across the 3 cohorts a total of 20 people registered their interest and 14 attended. Please see appendix 3 for workshop dates.
A series of 3 Welcome Values workshops were delivered. The Welcome Values project recruits, trains and supports people who use services, family carers and staff from care providers to visit other people who use services and assess the quality of the care and support they receive. Providers who attended these workshops were the Lancashire In-house Provider, Lake View Nursing Home, Hill Croft Nursing Home and Care Watch Morecambe. A total of 8 people completed the workshops and a further 6 people were visited as part of the reviews. Please see appendix 3 for workshop dates.
An end-of-project celebratory event was organised and subsequently cancelled due to poor take-up.
4
Evaluation
This evaluation will focus on identifying outcomes and positive changes as a result of the project for providers, the local authority and people who use services. In addition, it will identify potential future work to improve the delivery of dignity and person-centred approaches in Lancashire.This is a summative evaluation taking place after the project has been completed. Information was gathered using the following qualitative methods:
Examination of the notes from workshops and other relevant meetings, in addition to the project delivery action plan.
A one-to-one interview with a participant on the Welcome Values workshops.
A bespoke written questionnaire completed by both of the workshop facilitators.
A written questionnaire which identified outcomes from the project distributed via the website Survey Monkey. A total of 7 participants completed this questionnaire.
It proved extremely difficult to get participants to complete the evaluation questionnaire. Nevertheless a total of 10 out of the 63 people (including workshop leaders) who participated took part in this evaluation. None of the people who participated took part in the Appreciative Inquiry. Six of the people had participated in coaching and mentoring sessions; and four had participated in Welcome Values workshops.
5
Appreciative Inquiry
None of the people who participated in the evaluation process took part in the Appreciative Inquiry (AI) workshops. However the workshop facilitator offered some insight into these sessions in their responses to the questionnaire.Appreciative Inquiry enabled staff to meet with older people and family carers and learn from their perspective what matters, what’s working and how they want to move forward being included as a valued partner. The project would have been more beneficial if it had been able to engage more local people and local services. There was a pause in delivering the AI sessions in an attempt to refocus and generate involvement. With more time the facilitator said that would have continued to consistently offer AI as an approach to include older people, there needed to be more of this really.Older people told the facilitator that they had never done anything like this which highlighted that this inclusive way of working in partnership with people and families is not embedded in these services.
6
Coaching and Mentoring
Aims and Objectives
The aims of the coaching and mentoring sessions were:
to enable managers and supervisors to undertake structured, productive sessions with their teams using coaching and mentoring tools
to provide greater understanding, motivation and encourage commitment to person-centred principles that support dignity in older people’s services
to enable managers and supervisors to work in partnership with their teams to deliver dignity in care to older people and their supporters
By the end of the 6 sessions participants should be able to:
Value the uniqueness of every individual
Uphold the responsibility to shape care and support around each individual in a meaningful way from the person’s perspective.
Address issues of communication across different partnerships, communicating and listening to individual’s preferred communication styles.
Understand how an individual’s dignity can be affected.
Recognise and challenge when dignity may be at risk.
Be able to develop workplace cultures that actively promote dignity for everyone.
Be able to use coaching skills in supervision and team meetings in order to create positive actions that have an impact for older people and their families.
7
Develop skilled approaches to finding creative solutions.
Feedback from participants
Asked what new skills they had acquired as a result of the workshops, one participant cited “a variety of tools for solution-focussed problem solving.” Another person said:
“I learnt new skills in coaching the staff team, understanding them better and sharing information as part of appreciative inquiry.”
The facilitator also concurred that participants had learnt variety of new skills:
“Feedback was that the sessions helped learn new skills and confidence to make sure the people they support are at the centre of what they do, also, offered some solutions that we don’t do as frequently as we should because we focus on risk and systems that aren’t about people.”
When asked how the workshops could be improved, 3 people said they were just right and could not think of any improvements:
“The workshops were excellent. Pauline delivered the information with passion and engaged me in all aspects.”
Feedback to the facilitator indicated that the groups did not want the sessions to end and wanted more of them.
Others found the lack of commitment from fellow participants to be a problem:
“There were very few attendees at any of the sessions which meant that there was little sharing of ideas. Times, dates and venues of workshops were not well publicised... It would have been useful to know if the sessions were viable beforehand as some had to travel long distances but there was only 1 other candidate attending.”
“I signed up for the course with Pauline Doyle… Not Pauline’s fault but the course was a non-starter [as] candidates did not turn up; no commitment. For future I
8
suggest a deposit with a refund when completed, as my time was wasted as well as Pauline’s.”
Participants were asked what values they thought were important to people when they are using services. They listed dignity, being treated with respect, being “people-centred”, compassion, empathy, excellence, being listened to, having a voice, having choice and control and having ownership. In terms of how the project had supported their own personal development, participants said:
“I can implement changes I may need to make within my job role.”
“I have a few tools to use.”
“I have a better understanding of sharing information appropriately and listening to others.”
However one participant was less than positive:
“There is always something to learn, however I do not feel that my learning was great in relation to the amount of time I spent travelling and on the course.”
Positive outcomes for respective services identified by participants include being able to provide person-centred care, being able to support the development of other team members to work through issues and having the tools and understanding to keep driving dignity forward. Positive outcomes for the people who use services were identified by participants as having all their needs met in a respectful and dignified manner and feeling that they have a voice and are more actively listened to.
When asked what further action needs to be taken to improve the delivery of dignity to older people in Lancashire who use services, one participant said more people need to do these workshops.
Conclusions
From people’s responses to the questionnaire, there is clear evidence that participants learnt to creatively solve problems
9

and shape care and support around each individual in a meaningful way. Participants said they had a better understanding of how to communicate and listen to individual’s preferred communication styles. There is also evidence of how a person’s dignity can be affected and how and when to challenge when dignity may be at risk. In addition, positive outcomes identified include the ability to use coaching skills in supervision and team meetings.
However it must also be noted that these workshops were hampered considerably by poor attendance and a lack of commitment.
10
Welcome ValuesAims and Objectives
The Welcome Values project recruits, trains and supports people who use services, family carers and staff from care providers to visit other people who use services and assess the quality of the care and support they receive. The assessments focus on:
“…evidence from provider organisations that they and their staff actively seek to welcome people’s friends and extended families into their environment, and where people have no friends and family, that effort is made to support people develop such relationships. We will be looking for the kind of evidence that we value as humans – how it felt, how it smelt, whether people looked happy and contented, whether people were bored and not well supported etc. These are the kind of standards that all of us would want for ourselves and the people we love – do staff think about supporting someone to get changed if their top is dirty or they have food round their mouth etc.? This kind of gentle support makes the most difference and, if it is in place, people are at less risk of being dehumanised to the point where abuse becomes more likely to happen.” (Pathways Associates, 2012)
The results are then fed back to the providers who have the opportunity to respond and make positive changes to provision.
The process has been run a number of times across the UK with different providers. Learning disability providers include Castlebeck (now known as The Danshell Group) across England and Scotland, PossAbilities CIC (Heywood/Rochdale), Shared Approach (Lancashire), Integrate (Lancashire), Castle Support Living Ltd (Lancashire) and SLC Paragon (Lancashire). However
11
this was the first time the project had been run with older people’s services.
The aim of the project was to effect positive changes to the quality of local care services for older people.
The objectives of the project were:
1. To develop a set of standards for services around dignity, respect and community participation in collaboration with older people, family carers and service providers.
2. To train a group of older people, family carers and service providers to carry out reviews.
3. To review local services for older people against these standards through volunteer self-advocates and family carers visiting services.
4. To develop friendships, relationships and community participation for people who use services.
During a Welcome Values review, a team of stakeholders are supported by one or more facilitators to carry out visits to a sample of people who use a particular service over a 12 month period. A stakeholder can be a person who uses services, family member or member of staff from a provider.
At the first workshop the group come together to learn how to conduct a review and collectively come up with a set of values by which the services will be evaluated. Each member of the team then spends time visiting one person who uses a particular service, ideally carrying out four visits including one in the evening visit and one at the weekend.
At the next workshop they discuss what they have found and whether the standards are being met. Support is available at the workshop and in between workshops via phone and email from the facilitator(s).
12
At the third workshop they write action plans for both themselves and the provider to help them work towards achieving the values for that particular service.
During the process used in the Delivering Dignity in Lancashire project, workshops 2 and 3 were combined.
The final half-day workshop is a celebration event where participants assess progress and revisit the action plans. They also make a return visit at the end of the review to discuss their findings with the person and the provider and end the formal process. In order to achieve on-going progress the process may be repeated over and over again.
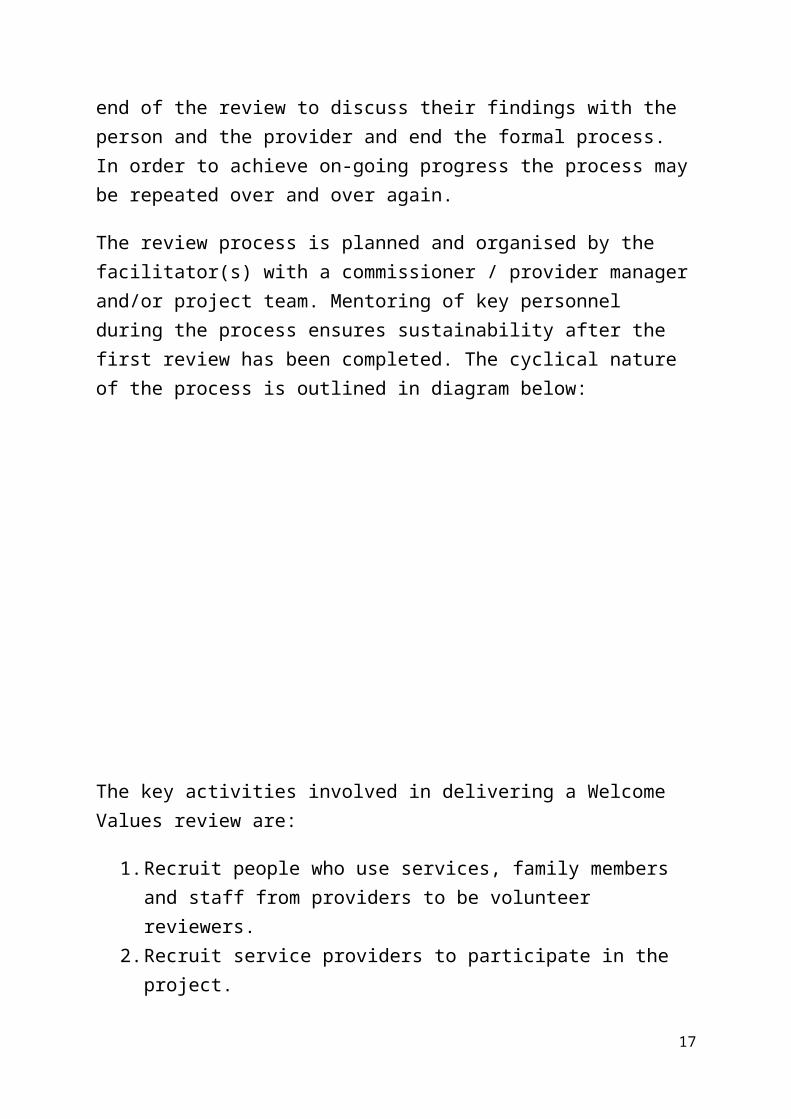
The review process is planned and organised by the facilitator(s) with a commissioner / provider manager and/or project team. Mentoring of key personnel during the process ensures sustainability after the first review has been completed. The cyclical nature of the process is outlined in diagram below:
The key activities involved in delivering a Welcome Values review are:
13
1. Recruit people who use services, family members and staff from providers to be volunteer reviewers.
2. Recruit service providers to participate in the project.3. Co-produce the Welcome Values with people who use
services, family carers and providers.4. Run training courses to prepare participants to carry out
reviews.5. Put policies in place to ensure the safety of participants
and, if they witness abuse, to support them to report it appropriately.
6. Support participants to visit services on a number of occasions at different times of the day and on different days. This will include an introductory visit to explain the purpose of the project, a number of visits to observe how the service is delivered and a final visit to review these observations with users.
7. Feedback the results of the review to the provider and give them the opportunity to respond.
8. Hold regular supervision sessions to support participants to undertake reviews and further develop their skills.
One course of 3 Welcome Values workshops was delivered between March and May 2014 as part of the Delivering Dignity in North Lancashire project. A second course was planned and subsequently cancelled due to poor uptake. Between December 2014 and March 2015 it was intended to work closely with the providers who took part to develop and adapt the process further. However reorganisation activity within Care Watch (including possible redundancy) and the Lancashire In-house Provider service meant this was not possible to the degree planned.
Feedback from participants
The values which were identified as important in relation to dignity in the Welcome Values workshops were:
Zero tolerance towards abuse
14
Respect Treating people as individuals Independence, choice and control Listening and supporting people to express their needs Privacy Feeling that people could complain without fear of
retribution Engagement with family members Assisting people to maintain confidence and positive self-
esteem Need to alleviate people’s loneliness and isolation in
nursing homes and the community.
At the end of the workshops 3 key themes were identified which can be celebrated:
1. There appears to be a lot of respect for people who use services.
2. People who use services are given privacy.3. People who use services are in many ways at the centre of
personal choice and control.
Similarly 3 things were identified by participants that need to change:
1. How people who use services are empowered to have more of a voice and be willing to complain.
2. How to ensure people are safe where they live, especially in relation to living safely and comfortably in large services with other people who may occasionally or regularly be upset angry and unpredictable and have an effect on the wellbeing of others.
3. How to ensure the least restrictive practices are used for people who use services.
It was recognised that generally Older People’s Services would not have the resources to undertake the time allocated for
15
visits and workshops used in this pilot. One evaluation participant said:
“The difficulty with home care as opposed to a care home setting is you’re restricted in terms of time to half-hour or hour slots. So I wanted to see if Welcome Values could work in this setting.”
Therefore a number of adaptations will be required in the future. Visits would need to be generally undertaken by supernumary staff with ideally a high level of input from experts by experience. This is usually how Learning Disability Service Welcome Values reviews are undertaken. In addition, to make the process work for older people’s homecare services, the course could be shorten to just two days and, in between participants would work through a workbook which would guide them through the process. Support from the facilitator would also be available via telephone. In addition, it may be difficult to convince provider organisations to buy into the process:
“Because this training is over and above what staff need to complete to get their Skills for Care certificate and start working, the problem is going to be convincing profit-driven companies that it’s necessary.”
Therefore it may be down to local authorities to drive forward this agenda if improved outcomes around dignity can be demonstrated by Welcome Values.
Participants in the evaluation were asked what new knowledge and skills they had acquired as a result of the workshops:
“I learnt to look at the issue of providing dignity in care through a more holistic approach, not just centring our attention on personal care but also looking at the person’s experiences throughout their daily life.”
16
There was evidence that training participants has taken the new knowledge and skills they had learnt and incorporated them into existing staff training within their organisations:
“It enabled me to develop skills in delivering ‘dignity training’. The most successful to date has been an adaptation of the process we learnt which has been a "dignity focus at mealtimes" document rolled out for all our staff to monitor and improve delivery of care at mealtimes under the key "dignity values" areas. I intend to expand this over further specific areas of care within the home… [This course has] enhanced my ability to support colleagues in looking at their own work practices and strive for continued improvement with an emphasis on looking at their own "dignity needs" as a basis for understanding others.”“The outcomes for me were learning about the Welcome Values process. I’m now going to take what I’ve learnt and incorporate it into the training I already deliver to services up and down the country… [The process] would work well with people with dementia as it’s similar to how we work already. So I would use life stories, the traffic light system and then establish likes and dislikes. It could become part of person-centred planning.”
Participants were generally pleased with the delivery of the workshops:
“The workshops were presented in an informal and friendly manner which made the group interact well and produce some good ideas and thoughts.”
“I enjoyed the training and found it useful. In my head I was trying to see how I could apply it to our workplace.”
However one participant said that, although they found the workshops valuable, they had missed the final workshop and would have appreciated a certificate of attendance at the end.
17
The facilitator said the workshops would have been better with more people turning up and more involvement. In previous Welcome Values project there has been involvement from people who use services and families but only paid staff came to these workshops. The facilitator found it difficult to get people to come; there were attempts to get families involved but this did not happen in the end.
A positive outcome for services identified by one participant was the “consolidation of existing good practice and a deeper understanding by staff of the importance of centring care around dignity values.” A positive outcome for the people who use services identified by the same participant was an “enhanced focus on dignity values which has improved the experience of residents as all staff now have an enhanced appreciation of the need to include these values in the delivery of all care.” Another participant said it was too early to identify outcomes as they were still in the process of implementing the strategies they had learnt.
A positive outcome identified by the facilitator was staff and managers spending more time with people that use services, listening to them and putting themselves in their shoes. People that came were keen and motivated and were owners or leaders in their organisations. However they went on to say that they were not sure if this is now embedded in these organisations as opposed to a one off activity.
In addition, two key issues were identified by the facilitator. The first was around people needing to feel safe not because of abuse from staff but because they had to live in large environments where they really did not want to be. Many are scared of other people who live alongside them taking their things. This must come as a huge shock for people after a lifetime of having choice, power and control over who they live with.
18
The second issue identified was the lack of knowledge and awareness in relation to physical intervention and least restrictive practices:
“It was really alarming – some organisations had little idea of Positive Behaviour Support. They need more training about physical intervention models.”
Conclusions
According to the facilitator, people and organisations usually wholeheartedly take on the Welcome Values process. However in this project, despite the emergence of a few champions, enthusiasm was not widespread in the same way. Although a full course of Welcome Values workshops was eventually delivered, this strand of work was undeniably hampered by poor attendance and lack of commitment. Barriers to delivering this course identified by the facilitator include not getting enough people to take part (particularly families and people using services), difficulty getting providers to release staff for workshops.
19
Conclusions
The workshop facilitators were of the opinion that the workforce is aware of dignity standards but there is little evidence of how they implement those standards in every day practice. They know where the manual is and know what the practice should be but the current systems in place and a general lack of knowledge around how to implement the standards prevents progress.Both facilitators admitted that, at the start of the project they overestimated the level of skills and knowledge around dignity and person-centred thinking within the workforce:
“We did not understand the current practice and had expected that the right values and confidence to work with older people in order to develop practice and policy were in place. Services were good at personal care but when sharing the knowledge there was very little of evidence of how they do that on consistent basis. [We] had to pause and start at much earlier point to examine the value base in services.”“I was shocked and saddened by what they [staff] thought was good.”
Facilitators also thought there was also some tension caused by the amount of activities going on at the same time. People struggled to commit because there were other training courses on offer. Therefore the timing of this project was off.In learning disability services for many years and value the importance of including all stakeholders has been acknowledged, however this is not the case with older people services. This created a barrier to delivering the project in an inclusive, participatory environment.
20
21
Recommendations
Based on the findings of this evaluation, the following recommendations are made to Lancashire County Council:
There needs to be a serious review of systems that are not person centred in organisations.
There needs to be a strong push to make sure that the voices of older people and older carers are valued and incorporated in developing future practice.
There needs to be a serious review of person centred values for the workforce
There is a need to change the model of care for older people with more personalised services and more personal budgets in health and social care.
Basic Values training needs to be delivered across the entire workforce.
There needs to be a long Term strategy around developing new models of services and decommissioning old-fashioned, institutionalised services.
Training on Positive Behaviour Support, physical intervention and least restrictive practices need to be delivered.
The Welcome Values process needs to be condensed down to two workshops and a workbook to make it work more Older People’s services.
22

Appendix 1: Definitions of DignityThere have been numerous papers, reports, consultation documents, policies and even laws around dignity in care over the past few years. This section offers a number of different definitions and ways of viewing dignity to support the Delivering Dignity in North Lancashire project.
Campbell (2009, p. 7) defines dignity as:
“…the quality or state of being worthy of esteem or respect. This means that it is a quality possessed by all human beings, since all are worth respect. But dignity is also about how people are treated. If you treat someone disrespectfully, then you take away their dignity. We often talk of treating someone with dignity, as shorthand for treating them as though they are worthy of respect. One important form of respect is self-respect. If you are not treated with respect by others, it is hard to hold onto your self-respect. It is hard to keep your sense of yourself as an autonomous person with rights to the kind of things that contribute to self-respect, like privacy.”
Campbell goes on to talk about the significance of dignity in health and social care:
“One of the times at which people are most in danger of losing their dignity and their self-respect is when they need help with health and social care. By their nature, health and social care services are provided when people are most vulnerable – when they are feeling at their weakest, when they are afraid and when they have to expose the most intimate and personal parts of themselves (their bodies and their minds) to inspection and handling by others.”
The Commission on Dignity in Care (2012) which looked at securing dignity for older people in hospitals and care homes defines dignity as follows:
23
“Dignity in care means bridging the gap between the principles and rights set out in the NHS Constitution and the reality of being an older person in care. While the Constitution is primarily intended for the health service, it articulates what the whole care sector should be aiming to achieve. The overarching commitment is to help keep us mentally and physically well, to involve us in decisions about our care, to help us get better when we are ill and, when we cannot fully recover, to stay as well as we can and live as independently as we can until the end of our lives.”
The commission goes on to list five ‘Always’ events for dignity in care:
Always treat those in your care as they wish to be treated – with respect, dignity and courtesy.
Always remember nutrition and hydration needs. Always encourage formal and informal feedback from
older people and their relatives, carers and advocates, to improve practice.
Always challenge poor practice at the time – and learn as a team from the error.
Always report poor practice where appropriate – the people in your care have rights and you have professional responsibilities.
The Health and Social Care Advisory Service (undated) state that ‘dignity’ is a term which is used in two major ways:
1. Dignity is a quality of the way we treat others as human beings.
2. Dignity is quality of an older person’s ‘inner self’.
It goes on to elaborate on a number of different types of dignity:
Treating older people as human beings Meeting older people’s human needs:
o Need for personal identityo Need for merits to be recognisedo Need for moral status to be recognised
24
The Royal College of Nursing (2008, p. 8) give the following definition:
“Dignity is concerned with how people feel, think and behave in relation to the worth or value of themselves and others. To treat someone with dignity is to treat them as being of worth, in a way that is respectful of them as valued individuals. In care situations, dignity may be promoted or diminished by: the physical environment; organisational culture; the attitudes and behaviour of the nursing team and others; and the way in which care activities are carried out. When dignity is present people feel in control, valued, confident, comfortable and able to make decisions for themselves. When dignity is absent people feel devalued, lacking control and comfort. They may lack confidence and be unable to make decisions for themselves. They may feel humiliated, embarrassed or ashamed. Dignity applies equally to those who have capacity and to those who lack it. Everyone has equal worth as human beings and must be treated as if they are able to feel, think and behave in relation to their own worth or value.”
The Social Care Institute for Excellence offers the following definition:
“Dignity in care means the kind of care, in any setting, which supports and promotes, and does not undermine, a person’s self-respect, regardless of difference” (SCIE, 2010)
The Dignity in Care campaign from the Social Care Institute for Excellence conducted numerous focus groups around the country to find out what Dignity in Care meant to people. The issues raised at these events resulted in the development of the 10 Point Dignity Challenge (SCIE, 2013). The challenge describes values and actions that high quality services that respect people's dignity should:
1. Have a zero tolerance of all forms of abuse 2. Support people with the same respect you would want
for yourself or a member of your family
25
3. Treat each person as an individual by offering a personalised service
4. Enable people to maintain the maximum possible level of independence, choice and control
5. Listen and support people to express their needs and wants
6. Respect people's right to privacy 7. Ensure people feel able to complain without fear of
retribution 8. Engage with family members and carers as care
partners 9. Assist people to maintain confidence and positive self-
esteem 10. Act to alleviate people's loneliness and isolation
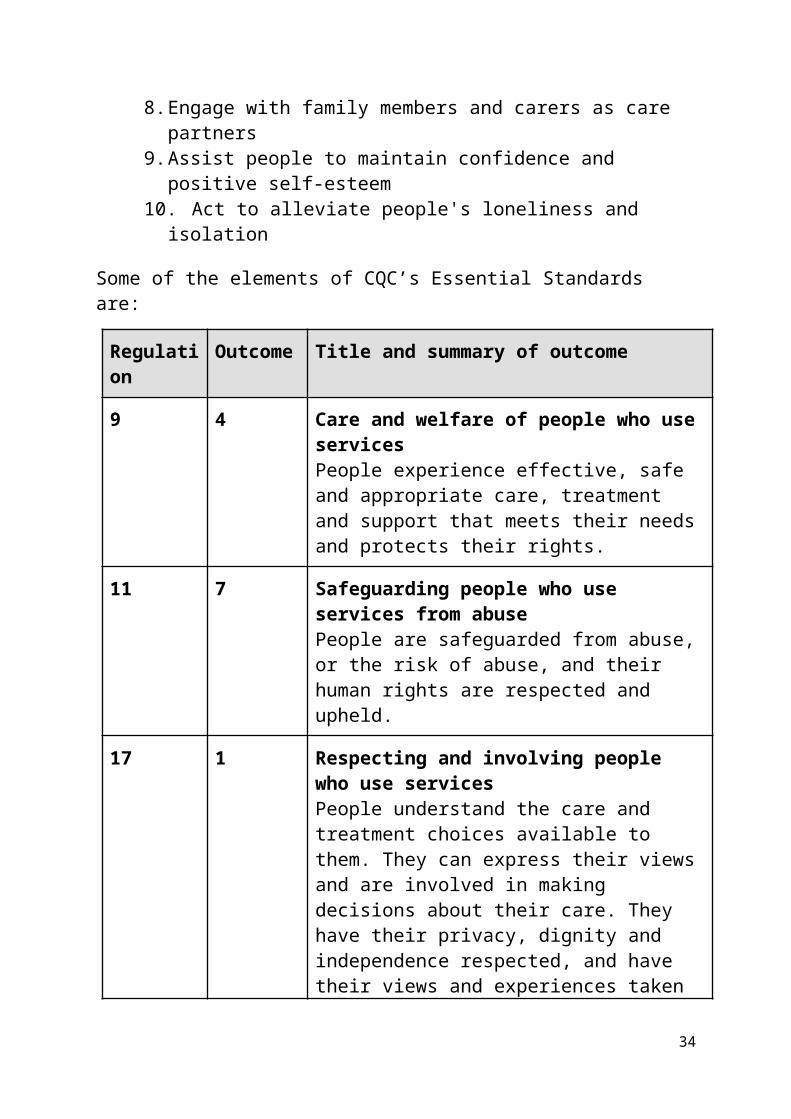
Some of the elements of CQC’s Essential Standards are:
Regulation
Outcome
Title and summary of outcome
9 4 Care and welfare of people who use servicesPeople experience effective, safe and appropriate care, treatment and support that meets their needs and protects their rights.
11 7 Safeguarding people who use services from abusePeople are safeguarded from abuse, or the risk of abuse, and their human rights are respected and upheld.
17 1 Respecting and involving people who use servicesPeople understand the care and treatment choices available to them. They can express their views and are involved in making decisions about their care. They have their privacy, dignity and independence respected, and have their views and experiences taken into account in the way in which the service is
26
delivered.
27

Appendix 2: Delivering Dignity Audit Survey
A questionnaire for providers around delivering dignity was developed by Pathways Associates in consultation with the commissioners. It was distributed via email to 193 providers, who were given the option of completing the form via the Survey Monkey website or an attached Microsoft Word document. In total 24 questionnaires were returned, 9 via Survey Monkey and 15 via email, giving a response rate of 12.5%.Respondents were asked to complete their questionnaires by 30th September 2013. This deadline was later extended to 7th October. The final questionnaire we received was sent on 1st November.Some people responded by cutting and pasting lengthy policy documents into the form. It was difficult to see how this answered the questions and these responses have not been included here.
28
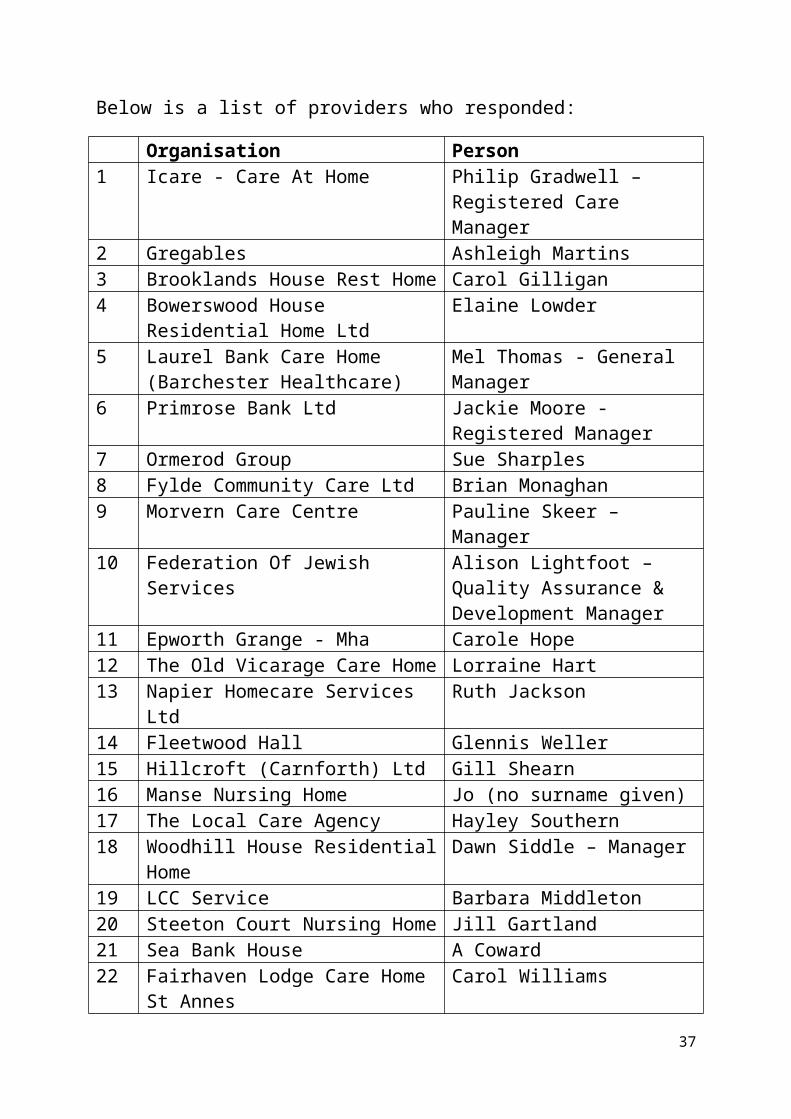
Below is a list of providers who responded:Organisation Person
1 Icare - Care At Home Philip Gradwell –Registered Care Manager
2 Gregables Ashleigh Martins3 Brooklands House Rest Home Carol Gilligan4 Bowerswood House
Residential Home LtdElaine Lowder
5 Laurel Bank Care Home (Barchester Healthcare)
Mel Thomas - General Manager
6 Primrose Bank Ltd Jackie Moore - Registered Manager
7 Ormerod Group Sue Sharples8 Fylde Community Care Ltd Brian Monaghan9 Morvern Care Centre Pauline Skeer – Manager10 Federation Of Jewish Services Alison Lightfoot – Quality
Assurance & Development Manager
11 Epworth Grange - Mha Carole Hope12 The Old Vicarage Care Home Lorraine Hart13 Napier Homecare Services Ltd Ruth Jackson14 Fleetwood Hall Glennis Weller15 Hillcroft (Carnforth) Ltd Gill Shearn16 Manse Nursing Home Jo (no surname given)17 The Local Care Agency Hayley Southern18 Woodhill House Residential
HomeDawn Siddle – Manager
19 LCC Service Barbara Middleton20 Steeton Court Nursing Home Jill Gartland21 Sea Bank House A Coward22 Fairhaven Lodge Care Home St
AnnesCarol Williams
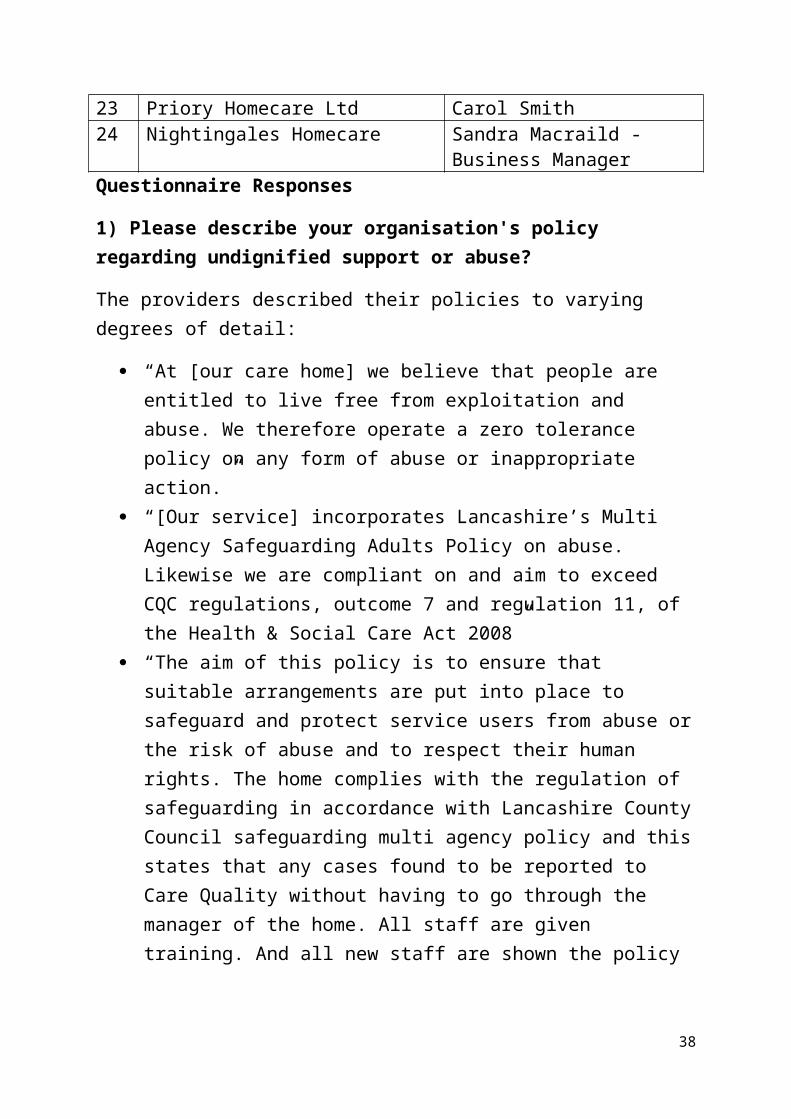
23 Priory Homecare Ltd Carol Smith24 Nightingales Homecare Sandra Macraild -
Business ManagerQuestionnaire Responses
1) Please describe your organisation's policy regarding undignified support or abuse?
29
The providers described their policies to varying degrees of detail:
“At [our care home] we believe that people are entitled to live free from exploitation and abuse. We therefore operate a zero tolerance policy on any form of abuse or inappropriate action.”
“[Our service] incorporates Lancashire’s Multi Agency Safeguarding Adults Policy on abuse. Likewise we are compliant on and aim to exceed CQC regulations, outcome 7 and regulation 11, of the Health & Social Care Act 2008”
“The aim of this policy is to ensure that suitable arrangements are put into place to safeguard and protect service users from abuse or the risk of abuse and to respect their human rights. The home complies with the regulation of safeguarding in accordance with Lancashire County Council safeguarding multi agency policy and this states that any cases found to be reported to Care Quality without having to go through the manager of the home. All staff are given training. And all new staff are shown the policy and used in their induction. All training is reviewed annually or if any changes occur.”
“At [our care home] all the staff are trained, at the start of their employment in the Induction Programme and then throughout the year, attending regular training sessions at the home. All the Staff recognises and respect resident’s individual differences and staff encourage and enable residents to make choices and respect the choice they have made.”
“To ensure the dignity and wellbeing of our residents all our staff are trained and are aware of our safeguarding policy. We have a notice up in our office and in the staff room providing details of how to contact the safeguarding team and raise a safeguarding alert.”
“The abuser, if it is a staff member, is suspended from duty pending investigation. A safeguarding is raised with LCC. The responsible funding body is informed and the
30
next of kin. If necessary the GP is contacted. The CQC are informed via the appropriate notification.”
“We have policies and procedures as part of our ISO9001 management system to formalise our monitoring of abuse. We use No Secrets as our code of practice and adhere to CQC’s outcome 7 – Safeguarding people who use services from abuse. All staff are familiar with these. Anyone witnessing undignified support or abuse is required to report it to their line manager for appropriate action to be taken.”
“Appropriate action may include an investigation, notification to the appropriate authorities, suspension, disciplinary, additional staff training and a change to our current policies and procedures.”
“When service users join our organisation, we familiarise them with our policy.”
“We promote dignity and do not tolerate undignified support or abuse”
“Where abuse is suspected, or alleged by a resident or advocate, this will be reported immediately to the Manager/Proprietor, Staff are not to ask questions, staff are to write down any disclosure/incident information you have as soon as possible, sign and date it. The Manager/Proprietor will make an alert to The Safeguarding Adults team.”
“Our policy sets out the procedures which are designed to benefit clients at risk, protect staff, visitors and reflects legislation.”
“We do not tolerate any abuse in our home, staff are able to talk to the manager at any time, with their concerns. We also encourage "whistle blowing policy". Any staff found to be giving unprofessional help will be disciplined.”
“Company policy updated 3 yearly for signs/actions/who to report to. Very in depth. Also follow local policy and whistleblowing”
31
“[Our care home] operates a zero tolerance policy on all forms of abuse and operates a robust safeguarding procedure which is audited annually”
“We have a dignity policy and a safeguarding policy, both of which stress that any breach of the required standard will be taken seriously and dealt with as a performance/disciplinary matter. Staff are made aware of the safeguarding procedures”
“It is the responsibility of all staff to look for abuse, and where abuse is suspected to report it to the appropriate person.”
“We have a clear Safeguarding Policy in place with a simplified flowchart for staff to follow. We run in-house safeguarding training for all staff. We include Dignity & Respect in a course that we run titled ‘The Role of the Social Care Worker’ and we are currently designing an ‘Exceptional Customer Service’ course that also looks at how we can ensure dignity & respect when assisting our residents.”
2) What measures are in place to ensure that service users, family members and staff can raise concerns comfortably and safely?
Providers described the following measures: “On assessment and introduction to our services, service
users meet with a care manager and are made aware of our quality assurance document whereby we give them assurance of a named care manager who is responsible for the overall welfare, together with our 24 hour Helpline number – see below our complaints procedure and our Promise to You document. Service users are given a ‘Welcome’ pack which clearly states our contact number and includes the named documents for easy reference as well as other documents.”
32
“A copy of the complaints notice is placed in each of the service users rooms, this is available for both family members and service users with direction of who to go to if they have any concerns. Staff have regular safeguarding training which covers all aspects including raising concern. Regular service user meetings and one-to-one discussions take place also.”
“We have a complaints procedure easily accessible to residents, relatives and staff. Whistleblowing policies are in place to support residents and staff. We also have a Grievance Policy for staff to raise concerns.”
“All the information is in the welcome pack that a new service user /family are given where there are phone no’s and names of who can apply. Also a poster up in the hall way with the same no’s on. All staff are trained and have annual refreshers.”
“At the outset of a care package, our supervisors explain our policies and procedures to service users and their family members/advocates/personal carers. All concerns raised are dealt with immediately and the person raising them is kept informed of progress. Matters are dealt with confidentially and the person raising the concern is listened to right from the start to give them confidence that everything necessary is being done.”
“People can raise concerns in a variety of forms – telephone conversation, email, letter, attending a one-to-one meeting or a group meeting if required.”
“A firm and robust whistleblowing policy is in place, carers are always given time to speak to any of the management team. Family members are able to visit the office, pick up the telephone or return any of the concern, complaints slips or write on the survey forms.”
“Policies, procedures, word of mouth, visitors questionnaires.”
“Complaints policy is on display in the main entrance of the home. We have an 'open door' policy. These policies
33
are also highlighted in the homes Statement of Purpose and Service user guide.”
“The manager lives on site so is available to talk to Service Users and their families at any time. If Service Users or their family wish to make an appointment to see the manager, this can be arranged for a mutual time. There are questionnaires sent out for feedback on all different aspects of the care process. All concerns will be considered and feedback given. All concerns will be treated with the utmost confidentiality”
“Phone nos and contact details in each resident’s room and also displayed in reception. Manager has open door policy and relatives etc are free to speak to her at any time”
“We operate an open door system for all service users, staff and visitors. Satisfaction questionnaires are sent out regularly which can be returned anonymously if necessary. We have clear complaints procedure on display in the reception area and complaints forms available at all times in the reception area.”
“All stakeholders are informed of the process, including who to contact internally and externally. We have recently provided relevant training for the service users’ forum.”
“Open door policy - safeguarding advice and training. Safeguarding policy and procedures.”
“Anyone who feels dissatisfied with any aspect of the company or delivery of care should raise the matter with the responsible member of staff. It may be that the staff member can deal with the point and if necessary apologise. If the complainant feels uncomfortable about this then a complaint should be made to the Manager or Director, contactable through the company.”
“We follow safeguarding and whistle blowing policy. All allegations are reported and investigated. Complaints policy in residents’ rooms SUG and SOP, dotted around the home on notice boards, together with the whistle blowing policy and posters.”
34

3) What are the opportunities for people who use your services, their families and your staff to shape and influence services?
Typically feedback from service users and families came from questionnaires and surveys, with little evidence of co-production happening:
“We have a 360 degree supervision procedure whereby we use direct feedback from the service user. This is having a positive effect on developing care workers to ensure that service users get the care they expect.”
“[Our care home] is constantly monitoring and reviewing the service via service user’s and staff complaint procedures, satisfaction questionnaires, service user’s care plan meetings, preference discussions, handovers, formal supervisions, formal and informal meetings.”
“At the home we hold regular Residents and Relatives meeting and at the meetings all who attends are encourage to have their say in the running of the home, or if they have any ideas, complaints or issues. Surveys and Questionnaires go out to residents, staff and family members on regular intervals throughout the year, and the home holds regular staff meetings of which are very well attended.”
“[Our care home] holds regular meetings for resident, Families and staff. We also hold open evening for families and friends to come along and discuss any issues. Again we do have an open door policy and are open to suggestions from anyone. We give feedback from questionnaires, which have been distributed to families and to residents.”
“We undertake a minimum of annual reviews of our service provision, giving all stakeholders the opportunity of giving us feedback. Feedback may be completing an
35
evaluation form, one-to-one meetings or telephone conversations.”
“Our staff attend regular briefing sessions and training and are aware that they can raise concerns, ideas, new initiatives, etc., at any time. We find that briefing sessions usually provide the type of opportunity which staff like to discuss and put forward ideas.”
“We have post admission meetings. Twice a year we have a buffet lunch at a central location to which families are invited. This is attended by the matron and directors.”
“We meet regularly with service users and their families to give them the opportunity to shape and improve our services.”
“Any outcomes from investigations are considered as part of our holistic approach to reviewing our services, changes being made wherever we find things could be improved.”
“Our supervisors review care plans on a regular basis and these are discussed with service users and their families. Anything which is highlighted which is not currently addressed would be considered as forming part of our service.”
“The information received will be looked into and any improvements that can be made will be adapted into our working practice. This information may come from surveys or questionnaires”
“Currently offering dementia awareness training offered to all family members, one to one time with their family member, offers of inclusion to care plans and care given.”
“All families and visitors to the home are invited to resident meetings which are held quarterly. It is mainly at these meetings that people can voice their views and suggestions to improve our services. We also have Quality Assurance surveys that go out to families, staff, visitors and Professional representatives. In the main entrance to the home we have a suggestion box. Again our' Open door policy' always works. I find that families, staff and visitors feel comfortable to approach me about
36
concerns and suggestions for improvements. I feel that being the Proprietor/Manager on site makes a huge difference to all people who use our service. Staff meetings are held quarterly. Appraisals for staff twice a year. Supervisions every six to eight weeks. These are also a means for staff to shape and influence the service.”
“Staff meetings are carried out, so staff can have an input into all aspects of how the home is run. Service User questionnaires are sent out six monthly and an audit carried out on the feedback. We hold Service User meetings monthly, so any problems, concerns, suggestions they may have can be looked at and changes put into place if needed.”
“Residents and relatives meetings. Staff meetings and supervision sessions bi-monthly”
“Meetings are held for staff, residents and NOK. Posters are put up in advance inviting contributions for the agenda and asking all to attend. their input is encouraged as much as possible”
“Service user forum ; Family forum; Involvement in recruitment and selection; Staff consultation group; Surveys and questionnaires; Feedback re staff performance; Person Centred Plans; Trustee surgeries; Consultation re organisational strategy.”
“Open door policy; Residents meetings; Staff meetings; Staff supervisions and appraisals”
“We will continue to monitor our service delivery in order to maintain high standards. A comment form will be sent to each client and report formulated. We welcome ideas and comments from our clients to assist in improving the service provided. We aim to develop good working partnerships with our clients, employees and other service providers. All of [our] Policies and Procedures can be sighted by any of our clients at any time and we welcome any suggestions to help improve our Quality System and the way in which the company operates.”
37
“Each ‘Have your say’ and question raised from staff forum are answered with feedback directly from our Senior Management Team. There is openness in our responses. Feedback is valued and has helped us to review and sometimes change how we do things at [our care home]. We also hold regular presentations to involve everyone and gain direct feedback.”
“Any suggestions from staff and service user families are taken into account when changes are being planned”
“Regular residents forums, regular surveys staff, residents and families on topics such as quality and food. Monthly dementia café.”
4) How many complaints concerning lack of dignity have you received in the past 12 months?
2 providers reported receiving a total of 6 complaints from people who use services.
7 providers reported receiving a total of 13 complaints from families.
1 provider reported receiving 1 complaint from a member of staff.
1 provider reported receiving 1 complaint from other people.
5) How does your organisation use Person-Centred Approaches to deliver care and support?
Some responses indicate a lack of knowledge around what constitutes person-centred planning:
All our Care Files and Plans are completed on person centred care, with full input from the resident, family members and care staff. This starts on admission to the home, with regular reviews and meeting throughout the
38
year or when necessary. All the care staff have daily input in these.”
“Person centred care planning involving services users and relatives in developing care plans on their needs, opinions and own choices.”
“We focus on Person Centred approaches throughout our home by researching our resident's life history. On admission we also take a detailed inventory of their likes and dislikes. We continually offer choices for example with meals and time that they would like to go to bed and get up in a morning. We always follow each individual's uniqueness from their past history “
“Each resident has an individual assessment, pre-admission and post admission, this is reviewed within 48 hrs and again after 4 weeks to ensure care needs are appropriate to each resident. Residents and family are encouraged to contribute to the planning of care. Once an individual care plan has been constructed it is reviewed monthly or more frequently depending upon residents’ circumstances. Al residents PC care plans are available for all staff to access to ensure continuity when delivering care to each resident”
“On admission a ‘This is me’ document is completed and the information is used to determine what is important to that person during their stay. We arrange activities on an individual basis as well as a group. We offer choice and inclusion to residents, involving families and representatives.”
However there is also evidence that some providers have received training and practice person-centred planning:
“A cross-section of our staff have attended a range of training, workshops and conferences specifically on personalisation. The tools and approaches we use are in line with Helen Sanderson Training.”
39
“All our staff undertake the Skills for Care Common Induction Standards training. A person-centred approach spans all of the training. Our staff have specific assignments to do to familiarise themselves with what each individual service user’s likes/dislikes/preferences on the care approach and what is important to them. Our care plans incorporate, where possible, specifics for the individual service user. We believe that our excellent rapport with families/advocates and personal carers enables us to personalise our services, within the limitations of our assigned hours. We keep our care plans up-to-date to reflect changes in the service user’s requirements and build in any additional information which can personalise the service we offer.”
“All of our care planning is carried out with the service user and their families, or representative, and is built taking with the involvement and wishes and aspirations of them. We no longer tell them what we will be doing, but work in partnership with them to achieve outcomes”
“Any decisions on care is centred round the service user, they and their family have full input into the care they receive. The service user is the one who decides on how they are cared for.”
“Person Centred approaches training is provided to all staff and is embedded within all contact with people that we support. People are given choice and control over the activities that they take part in, including where they live and who they live with.”
“Each of our residents has an individualised person centred care plan that is reviewed with the resident and/or family. We have a Wellbeing team who obtain life history information with the help of the resident and/or family. It can sometimes to be difficult to meet each individual request, but every effort is made by the team to provide care and activity in a way that meets each person’s needs.”
40
6) Please give examples of the person centred tools and approaches used
Again some responses indicate a lack of knowledge around person-centred tools:
“Care managers have been trained to assess service users, and, with their permission, access relevant information from other professionals (multi-disciplinary team), family members, friends and people the service user wants to have involved in their person-centred plan.”
“Care Files and Care Plans, Activities and Social Programmes, Quality Audit Monitoring and Tools, Questionnaires, Surveys and general daily observations and walking round the home on a daily basis.”
“Choice of care, foods, whether or not they require a doctor, invited to meetings.”
“Care planning. Social activities.” “Care plans. Audit by managers of sitting and observing
practice quarterly regulation visits by regional managers on a monthly basis”
“Pre admission assessment; individual care plans, person centred plans for daily use for each resident all care plans reviewed and revised monthly daily plans are reviewed and revised weekly”
“Life Histories Getting to know family and friends Memory Boxes”
“One example: Spending time with family and friends, Cultural or spiritual activities, Leisure activities : Offering transport accompanied with a carer”
“Our initial ‘Residents & Relatives Key Questions List’ on admission and life history books obtain relevant information to help staff ensure a personalised approach to meet their choice and need. Personalised care plans are also written involving the resident and/or family.”
41

However there was also some evidence of person-centred approaches and tools:
“We work alongside the training techniques of Helen Sanderson Associates which gives us the tools to work with the residents which enable us to monitor each individual’s wellbeing at that time. We are also using memory boxes outside the individual's bedroom, where we place items which belonging to each individual. This is helping the residents to recognise their own bedroom. We also have menus choices which are written on the boards on the units. Staff also communicates these choices to the resident and discussions take place with them when the meals are being served.”
“The ‘This is me’ determines what is important to that person, likes and dislikes, how can they be supported and what do people say about them. Individual assessment of abilities and activities geared to individual taste. “
“Introducing new Namaste Care. (Sensory approach for advanced dementia) Choice given for every aspect of care. 1 page profiles used ‘This is Me’. All staff know residents very well. In depth person-centred care plans, Kitwood Flower and Wish Tree.”
“One page profiles Learning logs Important to/for Good day/bad day What's working/not working Positive and productive teams”
7) How does your organisation enable people to maintain the maximum possible level of independence, choice and control?
Providers responded: The goal of the home is to promote independence
wherever possible. Individual care plans giving this type of information. Choice of room colour when being admitted, Meal times, Times that they rise and go to bed, What they
42

watch on TV. Choice to go out independently or with family and friends. What they wear on a daily basis.”
“Staff are instructed to treat service users at all times with sensitivity and respect. Always knock before entering a service users room and will respect not to disturb except in cases of emergency. Every service user has a secure lockable storage space. Service user will have facilities for entertaining personal and professional visits in private. Will offer help as appropriate and will sensitively assist service users in the performance of personal tasks and their individual presentation but will always allow them as much independence as they wish.”
“By facilitating access to the wider community, as well as bringing the community into the home in the form of visitors, volunteers and entertainment.”
“We work with the service user to maintain or improve their current level of independence. We do this by involving them in small tasks, working alongside them to undertake other tasks and by encouraging them to make telephone calls themselves. We help them write cards, pay bills, make up shopping lists and have memory prompts to give them as much independence as possible.”
“By doing everything possible to ensure it’s the way in which the resident wants it.”
“The resident’s charter is outlined in the homes brochure. Staff training upholds the principles of care by acknowledging and respecting the rights of the residents. Every attempt is made to ensure that our home provides adequately for all the residents needs so that people can lead a normal life as they are able, both within and outside the boundaries of the home. Residents have the freedom to be as independent, have choice and control of their daily living needs. This is all laid out in individual care plans.”
“Staff are trained to encourage service users to carry out as many tasks for themselves as they are able, and only
43
to step in when:- there is a problem , the service user asks for help or they are having difficulty with tasks.”
“Individualised care plans. Life histories. Enabling residents to carry on with hobbies etc”
“Through the use of good care planning individual residents are asked about their preferences and given the opportunity to choose their preferred choices these are all noted within the care plan. The promotion of independence is paramount in all that we do and this too is recorded within the care plan and PC plan of care.”
“Supporting the development of skills so that pople have the capacity to make choices and have control over their lives. Using a range of communication methods to assist empowerment. Providing information and guidance to assist choice and decision making”
“Risk Assessments Giving Choices Detailed person centred care profiles”
“By following the dignity in care charter” “Each resident is involved in their own personalised care
plan to state their individual choice. Staff are encouraged to assist residents to complete tasks, not do for them. We have an onsite Physiotherapist who runs in-house Falls Prevention classes to strengthen residents’ stamina, balance and co-ordination. These are also run by members of our Wellbeing team.”
“Empower them. Choice in all aspects of daily living. Newsletter sent monthly to families and residents.”
8) How does your organisation respect people's right to privacy?
Some privacy measures, such as “specific visiting times” seemed to be at odds with the previous question on choice and control. Other responses included:
“We follow the data protection act in relation to any paperwork all our workings are carried out in a
44
confidential manner. Residents can choose to lock their bedroom doors, if they so wish. They can have their own bedroom key so that they can 0go in and out of their bedroom as they please. We have separate lounges for when families come to visit so they can do so in private if they wish to do so. Staff will always knock on a resident's bedroom door and wait before entering, same when a resident is receiving personal care staff will always ask the resident how they would like a task to be carried out.”
“They all have their own en suite rooms and staff knock prior to entry. Confidentiality is maintained with regards to personal details. GP visits are held in their own rooms. Personnel files are stored securely.”
“All staff are taught to recognise the need for privacy of our residents. Each resident has their own personalised room that includes a bedroom and living space. All staff ensure knocking and introduction before entering a residents room. Time and space is also notably important when their visitors arrive.”
“Choice of locks on doors, choice not to be checked throughout the night, room available for private parties, meetings, practice nurses, end of life.”
“All our staff are trained to respect people’s right to privacy. This covers all aspects of personal care, the service users’ environments and confidentiality. We do, of course, advise service users and their families if anything comes to our attention which would require us to report it.”
“Privacy when needed, shutting room doors, knocking on residents’ door.”
9) How are people’s friends and family members made to feel welcome?
“Introduction of all new members of staff. Family and friends are encouraged to attend and join in with
45
entertainment and activities in and out of the home. Input and participation within the service user’s daily living is encouraged with family, next of kin and representatives. The appropriate persons are fully informed and provided with relevant information regarding the individual service user.”
“Friends and family members take part in initial discussions if this is appropriate and if this is what the service user wants or requires. We establish a good rapport with anyone involved with the service user and our carers build up a relationship with anyone who visits the service user. Our supervisors, care co-ordinators and all head office staff ensure that all enquiries are dealt with efficiently and effectively and in a friendly and helpful manner. We advise all our service users and their support network that we are here to help and that they only need to contact us to let us know what they require.”
“Involvement in the care planning and package of care” “A welcome at the door, an offer of tea or coffee, an
update on recent care given, taken through to relative offered privacy.”
“Good greetings and the welcome on the door mat is the most important task when you greet visitors. A good hand shake and a smile. Offer drinks and snacks. We have a large glass bowl of a variety of sweets by the visitors book that always welcomes a smile and a treat. Taking time at the front door to make people feel welcome and not feel rushed. At times it’s nice to ask relatives and friends would they like to stay for lunch, tea or supper, depending on the time of their visit.”
“Visitors are welcomed by staff, and are offered refreshments while they are visiting if they wish to speak to someone about their friend/relative the senior on duty will be pleased to see them.”
“Encouraged to visit and welcomed into home. Refreshments offered. Invites to events in home.”
46
“All visitors are greeted warmly by all levels of staff; this is monitored by random customer satisfaction survey. Staff are taught how to greet visitors and how to answer the telephone in a welcoming manner. Visitors are encouraged to attend meeting and to contribute their ideas towards the running of & improvement of the home.”
“Family and friends are very involved in every aspect of our service provision. They are kept informed about their relatives care and support and are free to visit them at home whenever they wish. We encourage people to have social gathering to which family and friends can be invited”
“Open door policy. Meals Resident and family meetings Involvement in care planning Social Events”
“We arrange a home visit with our senior carer inviting any family member who would like to attend”
“They initially link with our Admissions Officer as a point of contact who is with them each step of the way through to admission of their relative and is thereafter accessible as a point of contact. Other staff are involved in a ‘meet and greet’ of the resident and family. A pre-admission pack of information is provided and a welcome pack on arrival.”
“Greeted at the door, offered refreshments, no restrictions on visiting, can have meals at any time with residents, manager has open door policy for all.”
“We have open visiting and a Hostess lady who offer light refreshment.”
10) Are people told in advance about any changes to the service they receive?
All of the providers answered “yes” to this question.
11) Have your staff members been made aware of the 10 Dignity Challenges from the Social Care Institute for Excellence (SCIE)?
47
16 providers (66%) answered “yes” to this question.
12) Are posters and cards with the 10 Dignity Challenges on display in your premises?
14 providers (58%) answered “yes” to this question.
13) What opportunities are there for staff to discuss the 10 Dignity Challenges and how they apply to the delivery of your services?
Common opportunities included one-to-one supervision sessions, induction, appraisals, on-going training, Common Induction Standards training, and pocket cards. Comments included:
“Much work has been done with the care workers around the dignity challenge whereby a rotation of 1 of the 10 statements are discussed and evidence sought at care workers’ supervisions.”
“The 10 dignity challenges are discussed at induction, through safeguarding / Person-Centred training and at meetings.”
“Staff can discuss these during the Common Induction Standard Training, any other training provided, briefing sessions, when they call in to the office or when they have supervision and appraisals.”
“Dignity training is encompassed with our individual care plan training, Dementia training, Mental Capacity training, Moving and handling training. Medication training. I would say that there is dignity training in all aspects of all our training.”
48
14) Please give a breakdown of the numbers of staff managed by you with details of how many have completed any dignity training?
Not everyone put down the total number of staff they managed, so it was impossible to always work out the percentage of staff that had been trained. Also some respondents chose not to answer that question at all. However from the information given:
1 provider (Gregables) said that none of their staff had received training.
11 out of the 16 providers who answered the question had trained at least 90% of their staff.
5 out of the 16 providers who answered the question had trained 100% of their staff.
15) Have any of your staff become Dignity Champions?
Only 12 (50%) of the providers had dignity champions amongst their staff.
16) If yes, how does your organisation support its Dignity Champions?
Responses ranged from “not specifically” to a number of initiatives including:
“We have a Dignity lead and meetings are held with the Champions. Minutes are circulated to the home managers. Time is given to attend meetings and to action incentives.”
“Staff are enabled to access Dignity update bulletins regularly.”
“Letting her voice opinions [and] work on behalf of the resident to promote their rights if needed.”
49
“Our Dignity Pledges are displayed in the entrance to the home accompanied by the name of the Dignity champions and their telephone numbers for any support required.”
“We attend meetings. Dignity Board in situ. Staff Meetings”
“They have access to in-house training delivery and updates.”
17) Dignity Action Day on 1st February gives everyone the opportunity to contribute to upholding people's rights to dignity and provide a truly memorable day for people receiving care. How has your organisation celebrated this day in the past?
Only 5 (21%) of the providers said that they celebrated Dignity Action Day. Amongst these providers the day is celebrated in the following ways:
“Every year we have held a celebration day to recognise all carers who have achieved their Skills for Care Diploma and training awards during the year. This is combined with an awareness day offering dignity to our service users and celebrating Michael Parkinson’s work in supporting dignity.”
“Each home will do their own presentation along with looking for new ideas and suggestions. Dignity Day is a special day in our calendar and events take place throughout the day.”
“Open day. Display in reception and information leaflets out with refreshments.”
“The Activities Co-ordinators arranged an open day coffee morning with homemade biscuits, cakes and cupcakes, sweets and toffees the resident made. This was attended well by the staff and family members.”
“Had a theme party”One provider now intends to celebrate the day in the future:
50
“We have not celebrated Dignity Action Day but we intend to in 2014, it will be discussed with the staff and request their involvement with suggestions and input to provide an enjoyable day for all”
18) Any other comments/suggestions or positive stories you wish to share?
The following comments were received: “We have a Dignity Tree in reception. Staff, residents and
relatives are invited to comment on their ideas, suggestions and experiences. These are written on tags and hung on the tree and displayed for all to read.”
“We believe that focusing on our service users as individuals and taking their needs and wants into account, provides the level of care and support which they desire. We have booked staff on to the launch event of Skills for Care Common Core Principles for Dignity. We intend to incorporate the toolkit into our training in the future.”
“At [our care home] we integrate some staff and resident meetings together, to encourage better understanding of everyone's perspective on care and living or working within the home. This works well and promotes a feeling of family and greater understanding.”
“The Wish Tree was a great success; all wishes were granted! One of the residents has been given a badge and is now a resident helper which gives him a feeling of self-worth and belonging. Residents are empowered to assist with personal dressing, bathing, housework, laying of tables, gardening, hovering, even assisting with making sandwiches for their teas.”
51
Appendix 3: Workshop Dates
Appreciative Inquiry WorkshopsNeed dates
Coaching and Mentoring SessionsAll sessions took place in the Blackpool Enterprise Centre.
Cohort 1 – 7 people registered, 5 attendedDates:
11th October 2013 15th November 2013 9th December 2013 10th January 2014 20th February 2014 28th March 2014
Cohort 2 – 7 people registered, 3 attended 7th February 2014 3rd March 2014 4th April 2014 2nd May 2014 6th June 2014 4th July 2014
Cohort 3 – 6 people registered, all attendedNeed dates
Welcome Values Workshops
Providers who attended were the Lancashire In-house Provider, Lake View Nursing Home, Hill Croft Nursing Home and Care Watch Morecambe:
Workshop 1 – 12TH March 2014 Workshop 2 – 25th April 2014 Workshop 3 – 21st May 2014
52

Bibliography
Campbell, F. (2009) Walk a mile in my shoes, London: Centre for Public Scrutiny.
Commission on Dignity in Care (2012) Delivering dignity: Securing dignity in care for older people in hospitals and care homes. Final report, London: Local Government Association, the NHS Confederation and Age UK.
Health and Social Care Advisory Service (undated) Introduction to the Dignity through Action Workshop. Basingstoke: HASCAS.
Royal College of Nursing (2008) Defending Dignity: challenges and opportunities for nurses. London: Royal College of Nursing.
SCIE (2010) SCIE Guide 15: Dignity in care. London: SCIE.
SCIE (2013) The 10 Point Dignity Challenge. London: SCIE.
53