-
7/25/2019 Cystic degeneration in fibrous dysplasia of the
jaws.pdf
1/6
-
7/25/2019 Cystic degeneration in fibrous dysplasia of the
jaws.pdf
2/6
approximately 5 cm in diameter and was lined by a thick,
fibrous tissue layer.
Histologic examination of the decalcified sections showed
a thin layer of cortical and cancellous bone, which merged
with a fibro-osseous lesion consisting of hypercellularfibrous
connective tissue containing scattered irregular foci
of osteoid and thin trabeculae of woven bone; some of this
woven bone showed osteoblastic rimming (Fig 5). The
fibrous connective tissue was composed of plump,
ovaltospindle-shaped fibroblasts with vesicular nuclei.
Scattered multinucleated, osteoclastlike giant cells were
present. On the innermost aspect of the biopsy specimen, an
irregular cystlike cavity was present; it was lined by a
thick
layer of fibrous connective tissue and in places by inflamed
granulation tissue. There was no epithelial lining (Fig 6).
The
histologic features were not pathognomonic; they were
essentially those of a benign fibro-osseous lesion. The
differ-
ential diagnosis included a reparative/reactive process,
fibrous dysplasia, juvenile cemento-ossifying fibroma, and
osteoblastoma.
In view of the poor circumscription of the lesion radi-
ographically, the intraoperative finding of a soft, fibrous
lesion with no plane of cleavage, and the absence of any
history of trauma (although it should be noted that in
approx-
imately 50% of cases subsequently diagnosed as traumatic
bone cyst, there has been no previous trauma to the area),
the
lesion was signed out as fibrous dysplasia with a secondary
degenerative cyst. The case was referred for consultation to
a
pathologist, who subsequently agreed with our diagnosis(personal
communication, Dr K. Unni, Rochester, Minn).
A coronoidectomy and enucleation of the cyst were
performed through use of a combined submandibular and
intraoral approach. Lack of circumscription of the lesion
was
again confirmed at this time. No attempt was made to remove
the entire lesion. Postoperative healing was uneventful, and
the patient was maintained on a rigorous home physiotherapy
program. Six months postoperatively, the patient maintained
a mouth opening of 30 mm, and there was no increase in the
size of the lesion. The patient has subsequently been lost
to
follow-up, and all attempts to recall him have failed (he
lives
in a rural community). However, his father has reported that
2 years after the operation there has been no increase in
the
size of the lesion and the patient has not been experiencingany
functional problems.
DISCUSSIONAneurysmal and simple bone cysts (the latter also
referred to as a unicameral bone cyst, solitary bone
cyst, and traumatic bone cyst) are well-defined clinico-
pathologic entities that sometimes occur as secondary
phenomena in many benign and malignant bone
tumors and tumorlike lesions. In addition, secondary
cystic lesions of bone are encountered that fail to meet
the histologic criteria for a diagnosis of either
aneurysmal or simple bone cyst.19,20 These cysts
consist of blood-filled cavities in bone that are lined by
a thick layer of fibrous tissue; they have been referred
to as nonspecific cystic degenerations.4,17 They do not
appear to represent yet another distinct pathologic
lesion and have not been classified as such by various
authorities.21-23 More probably, they form part of the
clinicopathologic spectrum of nonepithelial-lined
cysts of bone.
The pathogenesis of nonepithelial-lined bone cysts
338 Ferretti, Coleman, and Altini ORAL SURGERY ORAL MEDICINE
ORAL PATHOLOGYSeptember 1999
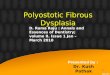
Fig 2. Panoramic radiograph shows ill-defined, diffuse,
ground glass, radiopaque lesion occupying ramus, angle,
and body of mandible and causing massive expansion of coro-
noid process (arrows).
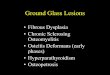
Fig 1. Frontal view shows large, diffuse swelling of right
side
of face and limited mouth opening.
-
7/25/2019 Cystic degeneration in fibrous dysplasia of the
jaws.pdf
3/6
remains unknown. However, there is growing accep-
tance of the postulate that aneurysmal and simple bone
cysts are 2 histologic expressions of a related process.24
It has been proposed that these cystic lesions arise from
an intrabony vascular defect, such as an arteriovenous
malformation that results in intramedullary hemor-
rhage.8,13,15,25 Direct circulatory connection with thehematoma
may lead to the formation of an aneurysmal
bone cyst, whereas complete interruption of the blood
supply may lead to simple bone cyst formation. It is an
attractive concept to include nonspecific cystic degener-
ations in this spectrum and to consider them as repre-
senting another manifestation of this pathogenetic
process. The clinical findings of a cavity filled with
blood and lined by a vascular connective tissue provide
support for this proposal. Support for the origin of
nonepithelial-lined bone cysts from vascular defects
has been provided by the finding that aneurysmal bone
cysts had elevated intracystic pressure consistent with
an arteriovenous communication.8
It remains difficult, however, to explain why certain
of these nonepithelial-lined bone cysts occur more
frequently in some fibro-osseous lesions than in
others,13-15 and it should be pointed out that unlike the
aneurysmal and simple bone cysts, nonspecific cystic
degeneration does not appear to occur as a primary
phenomenon. This suggests that other factors may be
involved in the pathogenesis.
The first reports of fibrous dysplasia complicated
by nonspecific cystic degeneration have been attrib-
uted to Jaffe26 and Schlesinger, Keats, and Ruoff.27
Their cases occurred in the rib and proximal tibia,
respectively. A comprehensive review of 42 cases of
extragnathic fibrous dysplasia2 revealed 13 examples
of nonspecific macrocystic and microcystic degenera-
tion. An additional 3 cases of nonspecific cystic
degeneration occurring in fibrous dysplasia of the
ribs, vertebra, and tibia have been described.3 In
theseinstances, the rapid swelling associated with the
cystic degeneration raised concerns about possible
malignant transformation.
Nonspecific cystic degeneration occurring in
fibrous dysplasia of the jaws has rarely been reported
in the literature. Obwegeser, Freihofer, and Horejs5
reported 2 cases of fibrous dysplasia that demon-
strated radiographic and clinical evidence of cyst
formation. In one of these cases, which presented as a
unilocular radiolucency of the mandible associated
with several impacted teeth, the cyst wall was
composed of highly cellular connective tissue with no
epithelial lining. The cyst recurred after treatment; in
addition, the patient subsequently developed several
similar cystic lesions in the maxilla. Fisher17 reported
2 cases of bone cavities in fibro-osseous lesions in the
maxillofacial skeleton. One of these lesions, which
presented as a nontender expansion of the mandible
and radiographically as a well-defined radiolucency,
was characterized by a cystic cavity lined by dense
fibrous tissue.
ORAL SURGERY ORAL MEDICINE ORAL PATHOLOGY Ferretti, Coleman, and
Altini 339Volume 88, Number 3
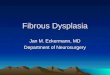
Fig 3. Coronal CT scan shows buccal and lingual expansion
of coronoid process of right mandible extending into
infratemporal fossa. At center of lesion is a large, well-
circumscribed unilocular cyst.
Fig 4. Axial CT scan shows expanded ramus of right mandible
causing lateral displacement and thinning of right zygomatic
arch. Central cyst is surrounded by a layer of poorly
mineral-
ized bone, which in parts has replaced cortex. In
condylarregion, lesional tissue merges with surrounding bone.
-
7/25/2019 Cystic degeneration in fibrous dysplasia of the
jaws.pdf
4/6
-
7/25/2019 Cystic degeneration in fibrous dysplasia of the
jaws.pdf
5/6
osseous jaw lesions.6,17 Careful follow-up is there-
fore advised.
We thank Dr Krishnan Unni of the Mayo Clinic, Rochester,
Minn, for reviewing the case.
REFERENCES1. Hara H, Ohishi M, Higuchi Y. Fibrous dysplasia of
the mandible
associated with large solitary bone cyst. J Oral Maxillofac
Surg1990;48:88-91.
2. Martinez V, Sissons HA. Aneurysmal bone cyst: a review of
123cases including primary lesions and those secondary to otherbone
pathology. Cancer 1988;61:2291-304.
3. El-Deeb M, Sedano HO, Waite DE. Aneurysmal bone cyst of
thejaws: report of a case associated with fibrous dysplasia
andreview of the literature. Int J Oral Surg 1980;9:301-11.
4. Simpson AHRW, Creasy TS, Williamson DM, et al. Cystic
degeneration of fibrous dysplasia masquerading as sarcoma. JBone
Joint Surg 1989;71B:434-6.
5. Obwegeser HL, Freihofer HPM, Horejs J. Variations of
fibrousdysplasia in the jaws. J Maxillofac Surg 1973;1:161-71.
6. Oliver LP. Aneurysmal bone cyst: report of a case. Oral
SurgOral Med Oral Pathol 1973;35:67-76.
7. Diercks RL, Sauter AJM, Mallens WMC. Aneurysmal bone cystin
association with fibrous dysplasia. J Bone Joint
Surg1986;68B:144-6.
8. Biesecker JL, Marcove RC, Huvos AG, et al. Aneurysmal
bone
cysts: a clinicopathologic study of 66 cases. Cancer
1970;26;615-25.
9. Waldron CA. Fibro-osseous lesions of the jaws. J Oral
Maxillofac Surg 1985;43:249-62.10. Makek MS. So-called
fibro-osseous lesions of tumorous
origin. Biology confronts terminology. J Craniomaxillofac
Surg1987;15:154-68.
11. Svensson B, Isacsson G. Benign osteoblastoma associated
withan aneurysmal bone cyst of the mandibular ramus and
condyle.Oral Surg Oral Med Oral Pathol 1993;76:433-6.
12. Saito Y, Hoshina Y, Nagamine T, et al. Simple bone cyst: a
clin-ical and histopathological study of fifteen cases. Oral Surg
OralMed Oral Pathol 1992;74:487-91.
13. Higuchi Y, Nakamura N, Tashiro H. Clinicopathologic study
ofcemento-osseous dysplasia producing cysts of the mandible.Oral
Surg Oral Med Oral Pathol 1988;65:339-42.
14. Ackerman GL, Altini M. The cementomas: a
clinico-patholog-ical reappraisal. Journal of the Dental
Association of SouthAfrica 1992;47:187-94.
15. Melrose RJ,Abrams AM, Mills BG. Florid osseous dysplasia:
a
clinicopathologic study of thirty-four cases. Oral Surg Oral
MedOral Pathol 1976;41:62-82.
16. Buraczewski J, Dabska M. Pathogenesis of aneurysmal
bonecyst: relationship between the aneurysmal bone cyst and
fibrousdysplasia of bone. Cancer 1971;28:597-604.
17. Fisher AD. Bone cavities in fibro-osseous lesions. Br J Oral
Surg1976;14:120-7.
18. Struthers PJ, Shear M. Aneurysmal bone cyst of the jaws:
patho-genesis. Int J Oral Surg 1984;13:92-100.
19. Rushton MA. Solitary bone cysts in the mandible. Br Dent
J1946;81:37-49.
ORAL SURGERY ORAL MEDICINE ORAL PATHOLOGY Ferretti, Coleman, and
Altini 341Volume 88, Number 3
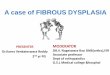
Fig 6. High-power view shows cyst consisting of dense,
hyalinized fibrous tissue without any epithelial lining
(hematoxylin-eosin, original magnification 40).
-
7/25/2019 Cystic degeneration in fibrous dysplasia of the
jaws.pdf
6/6
20. Jaffe HL, Liechtenstein L. Solitary unicameral bone cyst
withemphasis on the roentgen picture, the pathologic appearance
andthe pathogenesis. Arch Surg 1942;44:1004-25.
21. Shear M. Cysts of the oral regions 3rd ed. Oxford: Wright;
1992.p 171-86.
22. Unni KK. Dahlins bone tumours: general aspects and data
on11087 cases 5th ed. Philadelphia: Lippincott-Raven; 1996.
p382-93.
23. Kramer IRH, Pindborg JJ, Shear M. The WHO histologicaltyping
of odontogenic tumours. Cancer 1992;70:2988-94.
24. Hillerup S, Hjorting-Hansen E. Aneurysmal bone
cystsimplebone cyst: two aspects of the same pathological entity?
Int J OralSurg 1978;7:16-22.
25. Jaffe HL. Giant-cell reparative granuloma, traumatic bone
cyst,
and fibrous (fibro-osseous) dysplasia of the jaw bones. OralSurg
Oral Med Oral Pathol 1953;6:159-75.
26. Jaffe HL. Fibrous dysplasia of bone. Bulletin of the New
YorkAcademy of Medicine 1946;22:588-604.
27. Schlesinger PT, Keats S, Ruoff AC III. Fibrous dysplasia:
reportof a case. J Bone Joint Surg Am 1949;31A:187-91.
28. Schwartz DT, Alpert M. The malignant transformation of
fibrousdysplasia. Am J Med Sci 1964;247:1-20.
29. Eversole LR, Sabes WR, Rovin S. Fibrous dysplasia: a
noso-logic problem in the diagnosis of fibro-osseous lesions of
the
jaws. J Oral Pathol 1972;1:189-220.30. Waldron CA. Fibro-osseous
lesions of the jaws. J Oral
Maxillofac Surg 1993;51:828-35.
Reprint requests:
Hedley Coleman, BDS, BChD(Hons), M DentDivision of Oral
PathologyPrivate Bag 3WITS 2050South Africa
342 Ferretti, Coleman, and Altini ORAL SURGERY ORAL MEDICINE
ORAL PATHOLOGYSeptember 1999
Dont miss a single issue of the journal! To ensure prompt
service when you change your address, pleasephotocopy and complete
the form below.
Please send your change of address notification at least six
weeks before your move to ensure continued service.
We regret we cannot guarantee replacement of issues missed due
to late notification.
JOURNAL TITLE:Fill in the title of the journal here.
OLD ADDRESS:Affix the address label from a recent issue of the
journal here.
NEW ADDRESS:Clearly print your new address here.
Name
Address
City/State/ZIP
COPY AND MAIL THIS FORM TO: OR FAX TO: OR PHONE:Journal
Subscription Services 314-432-1158 1-800-453-4351Mosby, Inc Outside
the USA, call11830 Westline Industrial Dr 314-453-4351St Louis, MO
63146-3318
Send us your new address at least six weeks aheadON T H E M O V
E ?