Embed Size (px)
Citation preview

CVP AND PCWP MONITORING
Dr RANDEEP SINGH DHALIWAL
MODERATED BY
Dr HARSH MADHOKwww.anaesthesia.co.in [email protected]

CENTRAL VENOUS CANNULATION MONITORING
INDICATION:CVP MONITORING.PA CATHETERISATION & MONITORING.TRANSVENOUS CARDIAC PACING.TEMPORARY HEMODIALYSIS.DRUG ADMINISTRATIONASPIRATION OF AIR EMBOLISAMPLING SITE FOR REPEATED BLOOD TESTING

CENTRAL VENOUS CANNULATION SITES.
RT IJV.RT SUBCLAVIANLT IJV.EXT JUGULAR VEIN .FEMORAL VEIN.AXILLARY ND PERIPHERAL EINS.PICC CATHETERS.

PHYSIOLOGICAL CONSIDERATION(WAVEFORMS & CARDIAC CYCLE)
Early Diastole Late Systole.(y wave) (v wave)
Mid Diastole. Mid Systole.(h wave) (x wave)
Late Diastole. Early Systole. (a wave) (C wave)

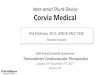
Central Venous Pressure Waveform Components
WAVEFORM PHASE OF CARDIAC CYCLE
MECHANICAL EVENTS
a wave End diastole Atrial contraction
c wave Early systoleIsovolumic ventricular contraction, tricuspid motion toward the right atrium
v wave Late systole Systolic filling of the atrium
h wave Mid to late diastole Diastolic plateau
x descent Mid systoleAtrial relaxation, descent of the base, systolic collapse
y descent Early diastoleEarly ventricular filling, diastolic collapse

CORRELATION BETWEEN ECG WAVE AND THE CVP WAVE.

1,ATRIAL FIBRILLATION.
ATRIUM IS UNABLE TO UNDERGO SYSTOLE AND HENCEABSENT A WAVE
PROMINENT C WAVE
ABNORMAL CVP WAVE FORMS AND ITS INTERPRETATIONS

2,NODAL RHYTHM, A.V DISSOCIATION
BOTH ATRIUM AND VENTRICLE CONTRACT AT THERE OWN RATE.
CANNON A WAVE,

TRICUSPID RGURGITATIONREFLUX OF BLOOD DURING VENTRICULAR SYSTOLE WILL RESULT IN.
TALL C WAVE. TALL V WAVE LOSS OF X DESEND ( AS THE REGURGITENT FLOW OF BLOOD ALREADY HAS FILLD THE RELAXING ATRIUM HENCE THE X DESEND STEEP IS LOST

TRICUSPID STENOSIS
• TALL A WAVE • ATTENUATED Y DESEND.
CARDIAC TEMPONADE. DOMINANT X DESEND
ATTENUTED Y DESEND

RT VENTRICULAR ISCHEMIA AND PERICARDIAL CONSTRICTION
• TALL A AND WAVES ( SYSTOLIC DYSFUCTION)• STEEP X AND Y DESEND (DIASTOLIC
DYSFUNCTION)

Complications of Central Venous Pressure Monitoring
MECHANICAL:
Vascular injury Arterial Venous Hemothorax Cardiac tamponade
Respiratory compromise Airway compression from hematoma Tracheal, laryngeal injury Pneumothorax
Nerve injury Arrhythmias Subcutaneous/mediastinal emphysema

Thromboembolic I. Venous thrombosis II. Pulmonary embolism III. Arterial thrombosis and embolism (air, clot) IV. Catheter or guidewire embolism
Infectious I. Insertion site infection II. Catheter infection III. Bloodstream infection IV. Endocarditis
Misinterpretation of data Misuse of equipment

PRESSURE VALUES AT EACH CHAMBER
Cardiac chamber Systolic (mm Hg) Diastolic (mm Hg)
Right Atrium Mean = 3Right Ventricle 25 06Pulmonary Artery
25 09
Pulmonary Artery Wedge
Mean = 9
Left Atrium Mean =8Left Ventricle 130 08


SPECIFICATIONS OF P.A CATHETER7.0 TO 9.0 FRECH CIRCUMFERENCE.110 cm length.volume of cuff(Balloon) 1.5 cm of air.4 Ports.Distal most for measurment of PAWP.30 cm from 1st Proximally for measuring CVPPort for balloon inflation.Thermioster for temperature and cardiac output measurement

Indications for Pulmonary Artery Catheterization
• The most recent recommendations governing the use of PACs are the American Society of Anesthesiologists practice guideline published in 2003.
• Surgical patients undergoing procedures associated with a high risk of complications from hemodynamic changes (e.g., cardiac surgery).
• Patients with advanced cardiopulmonary diseases that would place them at increased risk for adverse perioperative events.

Guidelines for PA catheter Placement.
From I.J.V PUNCTURE SITE
DISTANCE IN cm
RT ATRIUM 20 TO 25
RT VENTRICLE 30 TO 35
PULMONARY ARTERY 40 TO 45
WEDGE SITE 45 TO 50

Abnormal Pulmonary Artery and Wedge Pressure Waveforms
• Artifactual pressure peaks and troughs in the pulmonary artery pressure (PAP) waveform caused by catheter motion.
• when the balloon is overinflated and occludes the lumen orifice. This phenomenon is termed overwedging and is usually caused by distal catheter migration and eccentric balloon inflation, which forces the catheter tip against the vessel wall

PATHOLOGICAL CHANGES IN PCWP WAVE FORMS
1. Severe mitral regurgitation. A tall systolic v wave is inscribed in the pulmonary artery
wedge pressure (PAWP) trace and also distorts the pulmonary artery pressure (PAP) trace, thereby giving it a bifid appearance.
mean PAWP exceeds left ventricular end-diastolic pressure in this condition.
V wave height is an indicator of the severity of mitral regurgitation

2.MITRAL STENOSIS.
• Mean pulmonary artery wedge pressure (PAWP) is increased (35 mm Hg)
• The diastolic y descent is markedly attenuated.
• A waves are not seen in the PAWP or CVP traces because of atrial fibrillation

3.Myocardial ischemia
• Pulmonary artery pressure (PAP) is relatively normal
• Mean pulmonary artery wedge pressure (PAWP) is only slightly elevated (15 mm Hg).
• PAWP morphology is markedly abnormal, with tall a waves (21 mm Hg) resulting from the diastolic dysfunction seen in this condition.

4.Pericardial constriction.
• This condition causes elevation and equalization of diastolic filling pressure in the pulmonary artery pressure (PAP), pulmonary artery wedge pressure (PAWP), and central venous pressure (CVP) traces.
• The CVP waveform reveals tall a and v waves with steep x and y descents and a mid-diastolic plateau wave or h wave.

5.CARDIAC TEMPONADE.• Like pericardial constriction, cardiac tamponade impairs cardiac
filling, but in the case of tamponade, a compressive pericardial fluid collection produces this effect. This fluid collection results in a marked increase in CVP and reduced diastolic volume, stroke volume, and cardiac output. Despite many similar hemodynamic features, tamponade and constriction may be distinguished by the different CVP waveforms seen in these two conditions. In tamponade, the venous pressure waveform appears more monophasic and is dominated by the systolic x pressure descent. The diastolic y pressure descent is attenuated or absent because early diastolic flow from the right atrium to the right ventricle is impaired by the surrounding compressive pericardial fluid collection

IF THE SITE OF INSERTION IS DIFFERENT
• Extra 5 to 10 cm from the left internal jugular and left and right external jugular veins,
• 15 cm from the femoral veins,• 30 to 35 cm from the antecubital veins.• tip of the PAC should be within 2 cm of the cardiac
silhouette on a standard anteroposterior chest film.• right ventricular waveform is not observed after
inserting the catheter 40 cm, coiling in the right atrium is likely.

COMPLICATION OF PCWP
1. CATHETER RELATED Catheter knots, Thrombo embolism pulmonary Infaction Infective endocarditis. Pulmonary Artery Rupture.

2.DURING CATHETERISATION. Arrythemias R.B.B.B Complete heart Block( in pre existing LBBB) 3. MIS INTEPRETATION OF DATA
4. MISUSE OF EQUIPMENT.

THANK YOU
www.anaesthesia.co.in