Embed Size (px)
Citation preview
EFFECT OF EFFECT OF ANAESTHETIC AGENTS ANAESTHETIC AGENTS ON CARDIOVASCULAR ON CARDIOVASCULAR
SYSTEMSYSTEM
www.anaesthesia.co.in

CARDIOVASCULAR SYSTEM
• Cardiac output (Stroke volume x Heart rate)
• Systemic vascular resistance (B.P. / C.O.)
• Coronary blood flow & autoregulation
• Arrhythmogenicity
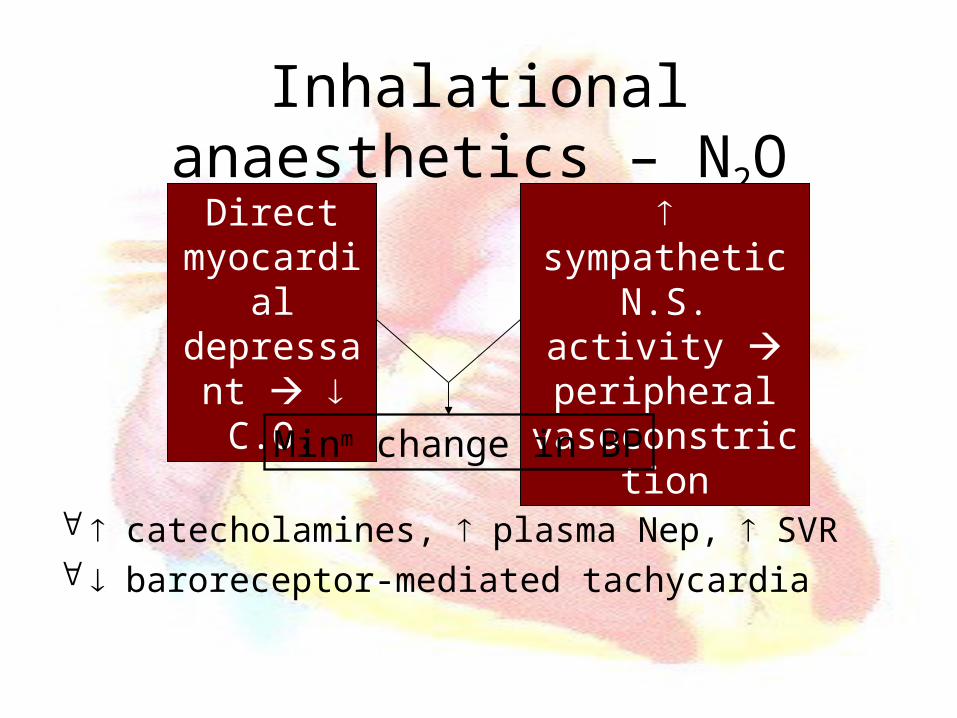
Inhalational anaesthetics – N2O
catecholamines, plasma Nep, SVR baroreceptor-mediated tachycardia
sympathetic N.S. activity
peripheral vasoconstriction
Direct myocardial depressant C.O.
Minm change in BP
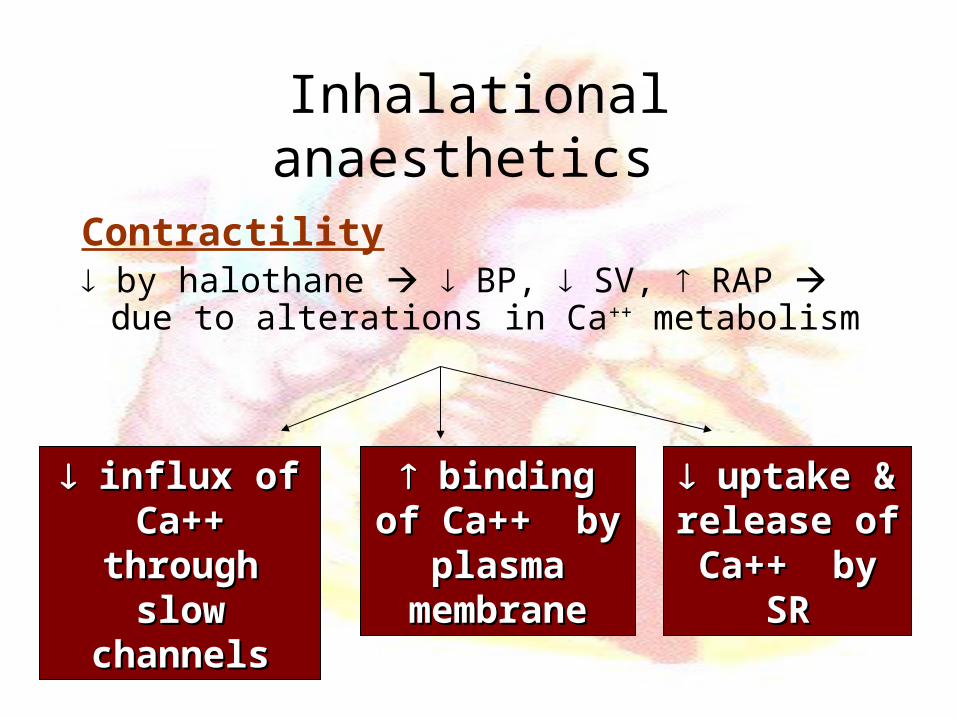
Inhalational anaesthetics
Contractility by halothane BP, SV, RAP due
to alterations in Ca++ metabolism
influx of Ca++ influx of Ca++ through slow through slow
channelschannels
binding of binding of Ca++ by Ca++ by plasma plasma
membranemembrane
uptake & uptake & release of Ca+release of Ca+
+ by SR+ by SR
Inhalational anaesthetics
Contractility by isoflurane in isolated hearts C. O.
maintained in vivo with minimal myocardial depression till 2 MAC ; SV, HR, Normal C. O.
• Sevoflurane dose-dependent myocardial depression through direct effect on Ca++ channels
• Desflurane dose-dependent myocardial depression
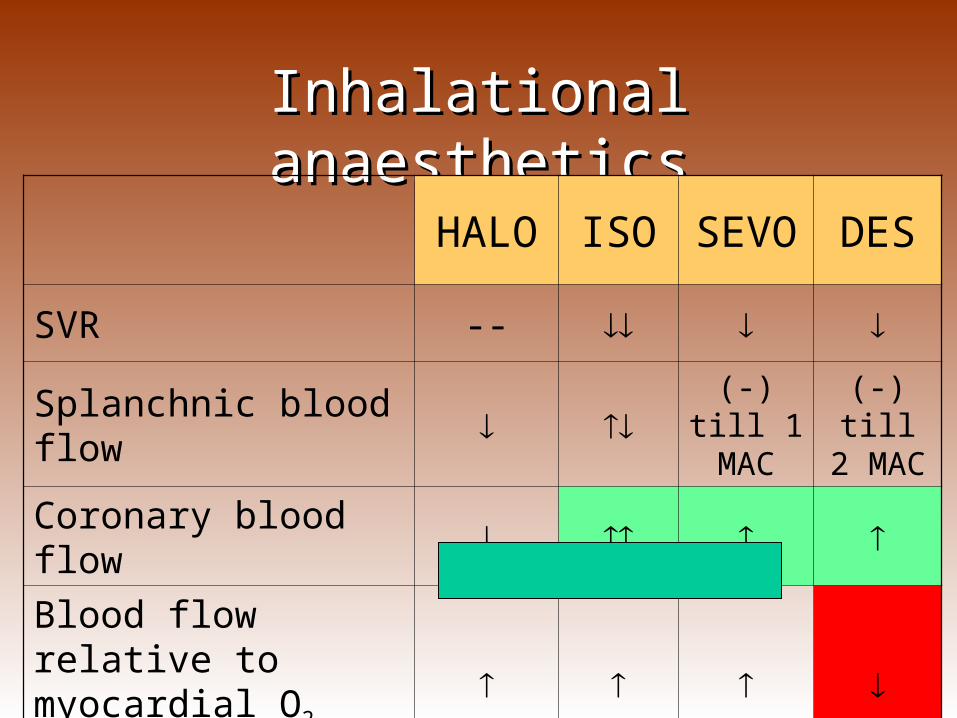
Inhalational anaestheticsInhalational anaesthetics
HALO ISO SEVO DES
SVR --
Splanchnic blood flow (-) till 1 MAC
(-) till 2 MAC
Coronary blood flow
Blood flow relative to myocardial O2 demand
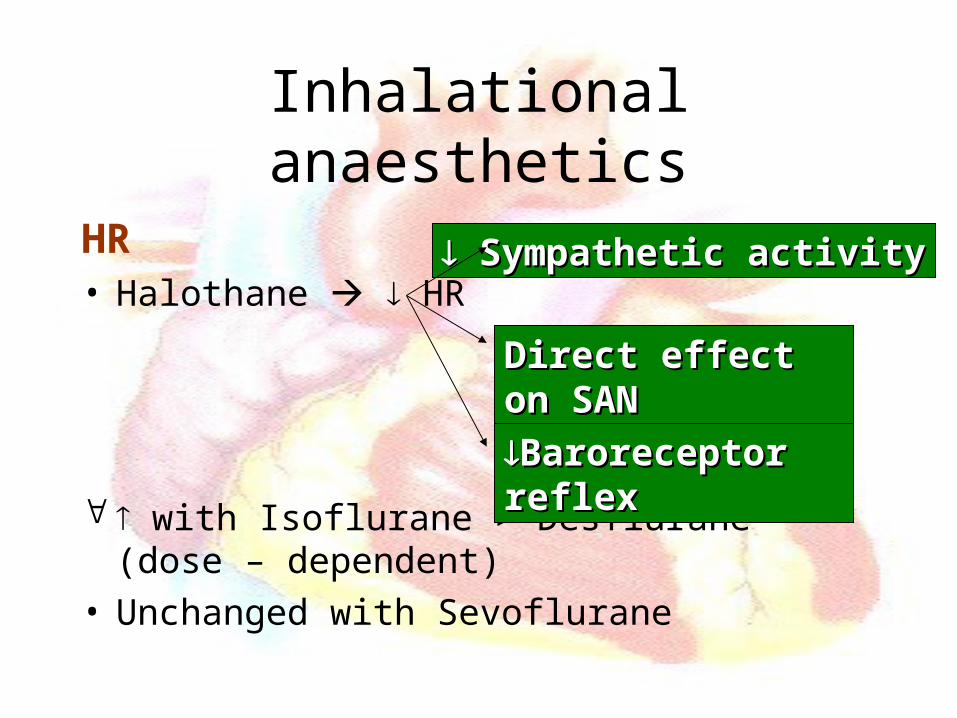
Inhalational anaesthetics
HR• Halothane HR
with Isoflurane > Desflurane (dose – dependent)• Unchanged with Sevoflurane
Sympathetic activitySympathetic activity
Direct effect on SANDirect effect on SAN
Baroreceptor reflexBaroreceptor reflex
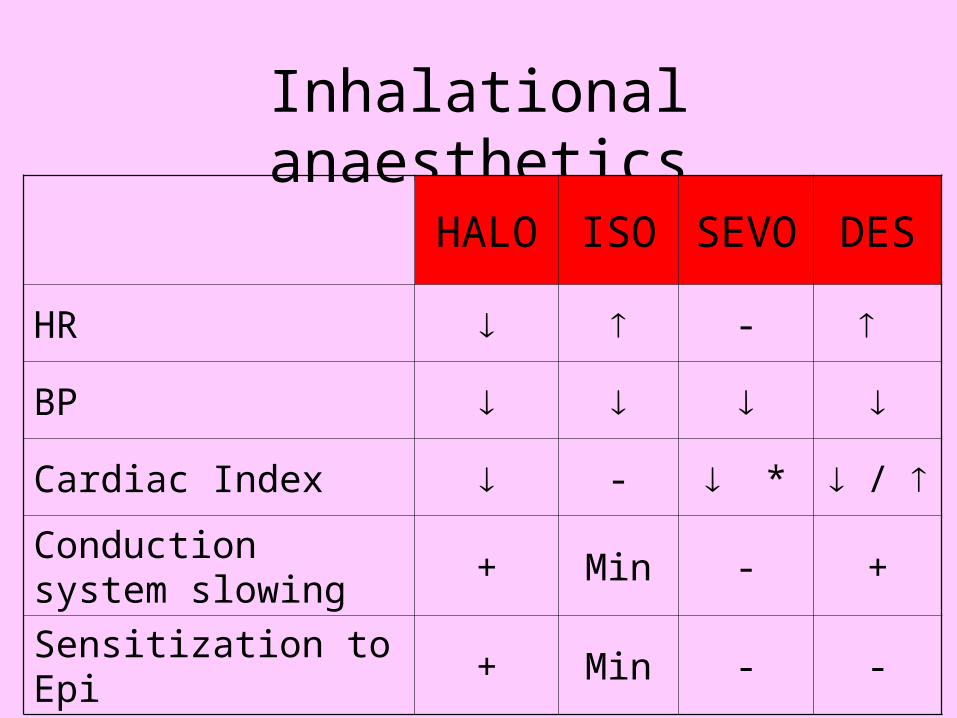
Inhalational anaesthetics
HALO ISO SEVO DES
HR -
BP
Cardiac Index - * /
Conduction system slowing
+ Min - +
Sensitization to Epi + Min - -
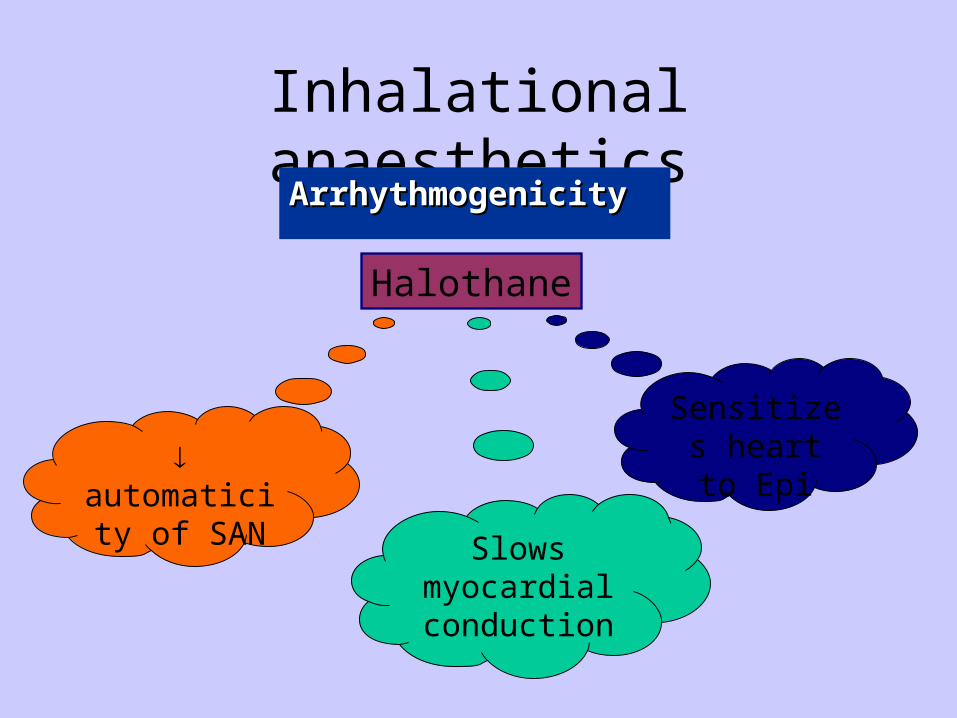
Inhalational anaestheticsArrhythmogenicity Arrhythmogenicity
automaticity of SAN
Slows myocardial conduction
Sensitizes heart to Epi
Halothane
Inhalational anaesthetics
Coronary steal phenomenonCoronary stenosis + coronary perfusion pressure
Detrimental redistribution of coronary blood flow with Isoflurane Contractile dysfunction; more in region distal to a critical coronary stenosis Avoided if CPP restored

Inhalational anaesthetics: Coronary autoregulation
Inhalational anaesthetics
• Protection against myocardial ischemia All except Des
• Interaction with CCBs En > Halo > Iso
• Rapid in concentration of Des & Iso HR & BP
Xenon
• Good haemodynamic stability
• Little change in BP
• No change in LV function with 65% Xe (MAC – 71%)
• Slight in HR
Intravenous Induction Agents- Thiopentone sodium
• Venodilation preload
• Direct myocardial depression at high doses
• SVR relatively unaltered after normal induction dose in healthy adults
• HR due to baroreceptor reflex
• Myocardial O2 consumption
Intravenous Induction Agents- Propofol
BP SVR - sympathetic activity + direct in
vascular S.M. tone / unchanged HR coronary perfusion pressure
• Unchanged global O2 supply-demand ratio
Intravenous Induction Agents - Etomidate
• Unchanged myocardial function
• Minm effect on haemodynamic stability
• No effect on symp N. S. & baro-R fncn
coronary vascular resistance, coronary perfusion well-maintained myocardial O2 supply-demand ratio
Intravenous Induction Agents - Ketamine
HR, BP, CO, SVR, PVR
• Can be attenuated by prior BDZs, other inhal or i/v anaes agents, adrenergic ATs
• Centrally mediated symp tone, not dose dependent; overrides direct myocardial depressant effect except at high doses
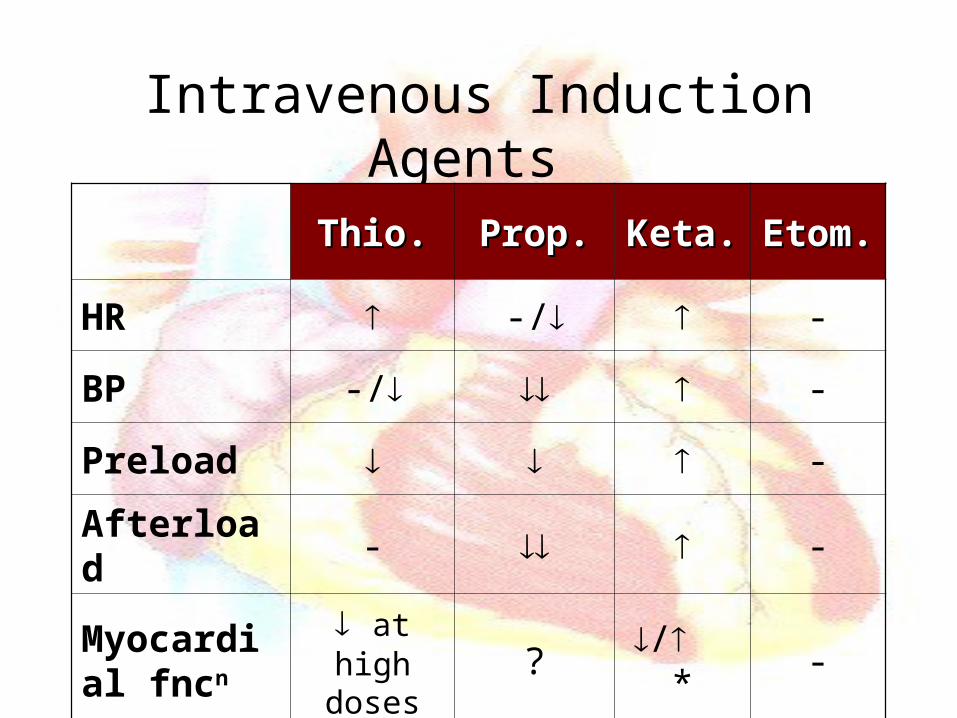
Intravenous Induction Agents
Thio.Thio. Prop.Prop. Keta.Keta. Etom.Etom.
HR -/ -
BP -/ -
Preload -
Afterload - -
Myocardial fncn
at high doses
? / * -
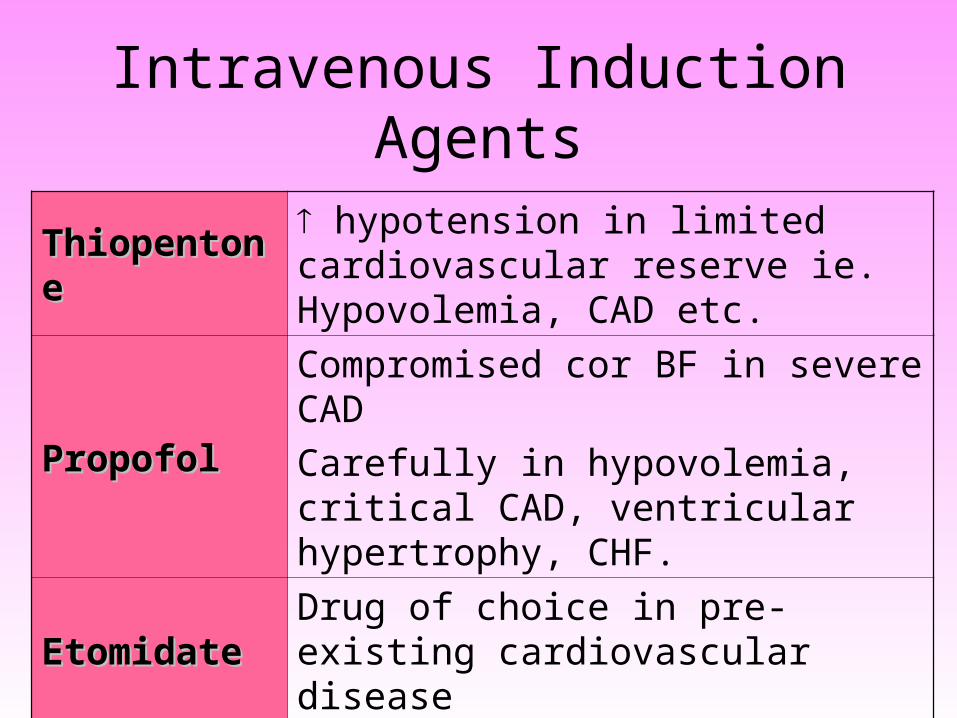
Intravenous Induction Agents
ThiopentoneThiopentone hypotension in limited cardiovascular reserve ie. Hypovolemia, CAD etc.
PropofolPropofolCompromised cor BF in severe CAD
Carefully in hypovolemia, critical CAD, ventricular hypertrophy, CHF.
EtomidateEtomidateDrug of choice in pre-existing cardiovascular disease
KetamineKetamineC.I. in IHD, vascular aneurysms
Avoided in shock, critical illness

Opioids
HR• Fent analogs HR by vagomimetic action;
severe bradycardia /asystole possible with Fent analogues; usually have favourable effect on myocardial O2 supply-demand ratio in CAD patients
• Pethidine HR by anticholinergic action
• Morphine /
Opioids
• Histamine release HR, MBP; Peth > Morph (less with slower administration); negligible with Fent analogues
contractility of isolated cardiac muscle, but blood concn insufficient; Morph & Fent both cardiostable at clinical concns
• Minor in BP with Fent analogs possibly by a centrally mediated in sympathetic tone
Opioids
Potency : Sufent > Fent > Morph > Peth
C.V. S/Es : Peth > Morph > Fent > Sufent
Cardiovascular side effects 1
Potency
Opioid AG - ATs
• Nalbuphine, Pentazocine HR, BP, SVR, PAP, LVEDP
• Butorphanol Small in PAP
• Newer agents Minimal effects, except meptazinol, dezocine
Opioids
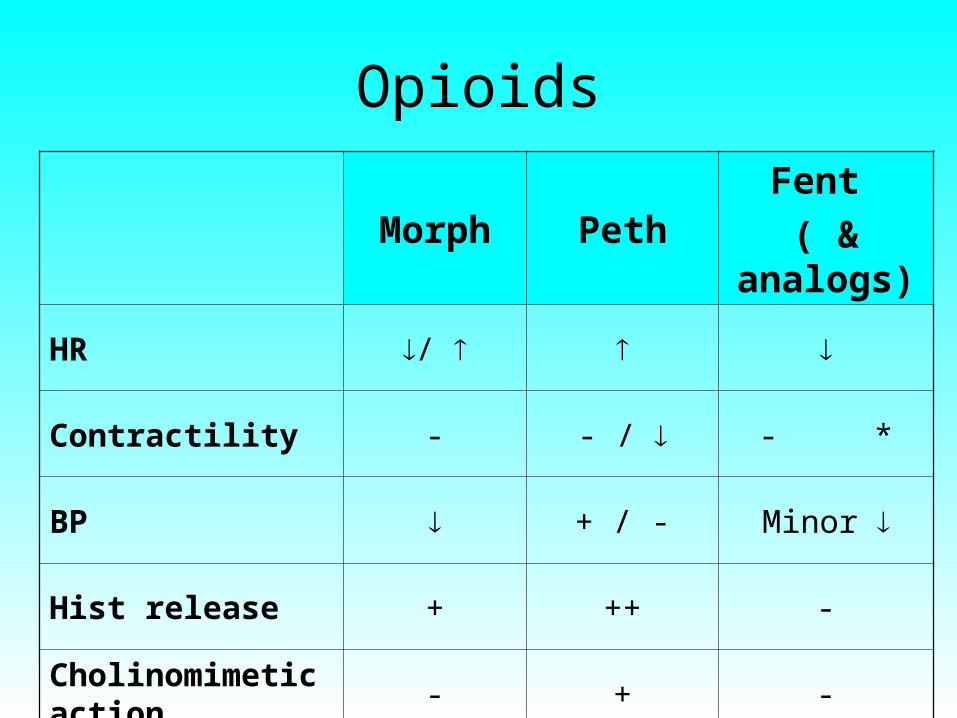
Morph PethFent
( & analogs)
HR /
Contractility - - / - *
BP + / - Minor
Hist release + ++ -
Cholinomimetic action
- + -
Benzodiazepines
• Mild, transient, dose-related fall in ABP, associated with catecholamine concn and sympathetic tone
• Dangerously exaggerated fall in BP with concurrent hypovolemia, coadministered i/v or inhaln anaesthetics or opioids

Interactions
• Opioids / BDZs + Ketamine sympathomimetic effects
• Opioids + BDZs MBP due to SVR, probably due to sympathetic tone
• Propofol / Opioids + NMBs fent analogs + vec bradycardia & asystole, no change in HR with pancuronium
Neuromuscular Blockers - Succinylcholine
• Low doses negative inotropism & chronotropism
• Large doses tachycardia
• Arrhythmias
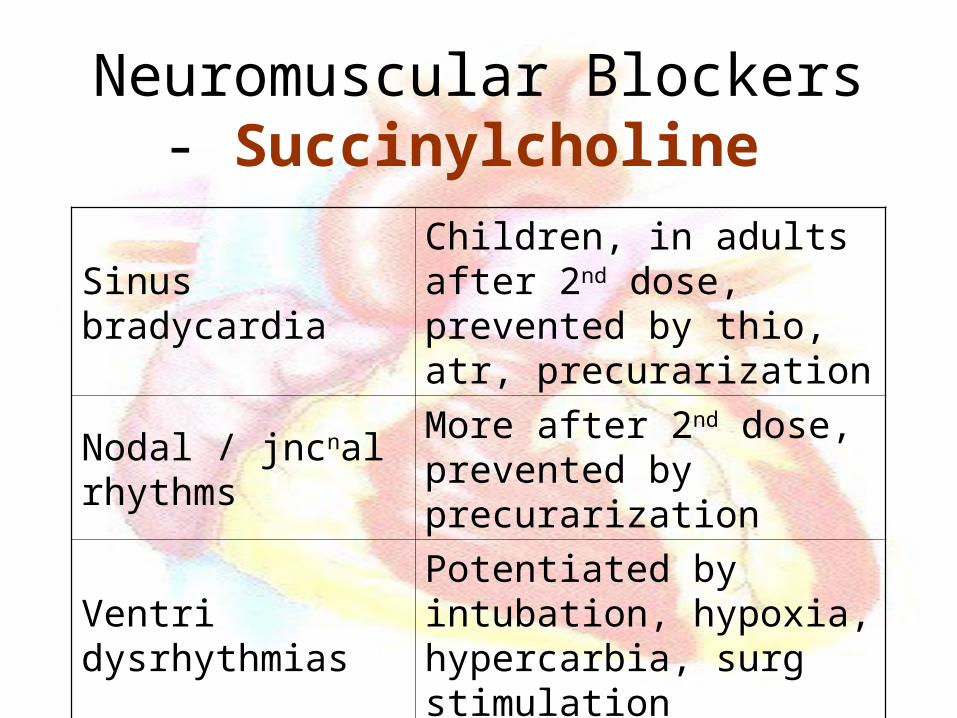
Neuromuscular Blockers - Succinylcholine
Sinus bradycardiaChildren, in adults after 2nd dose, prevented by thio, atr, precurarization
Nodal / jncnal rhythms
More after 2nd dose, prevented by precurarization
Ventri dysrhythmiasPotentiated by intubation, hypoxia, hypercarbia, surg stimulation
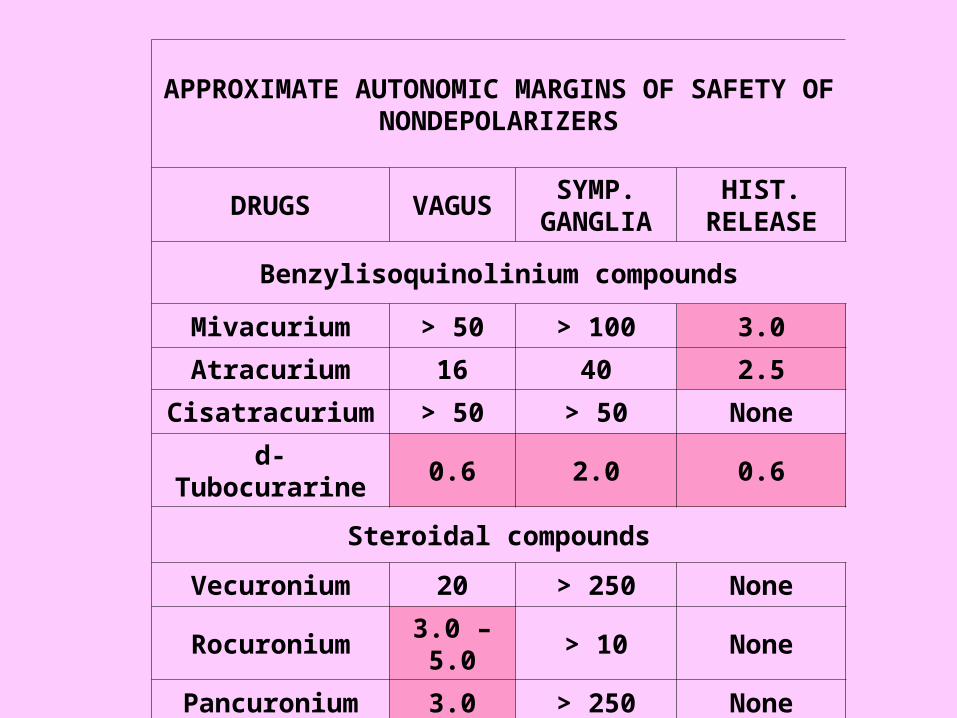
APPROXIMATE AUTONOMIC MARGINS OF SAFETY OF NONDEPOLARIZERS
DRUGS VAGUSSYMP.
GANGLIAHIST.
RELEASE
Benzylisoquinolinium compounds
Mivacurium > 50 > 100 3.0
Atracurium 16 40 2.5
Cisatracurium > 50 > 50 None
d-Tubocurarine 0.6 2.0 0.6
Steroidal compounds
Vecuronium 20 > 250 None
Rocuronium 3.0 – 5.0 > 10 None
Pancuronium 3.0 > 250 None
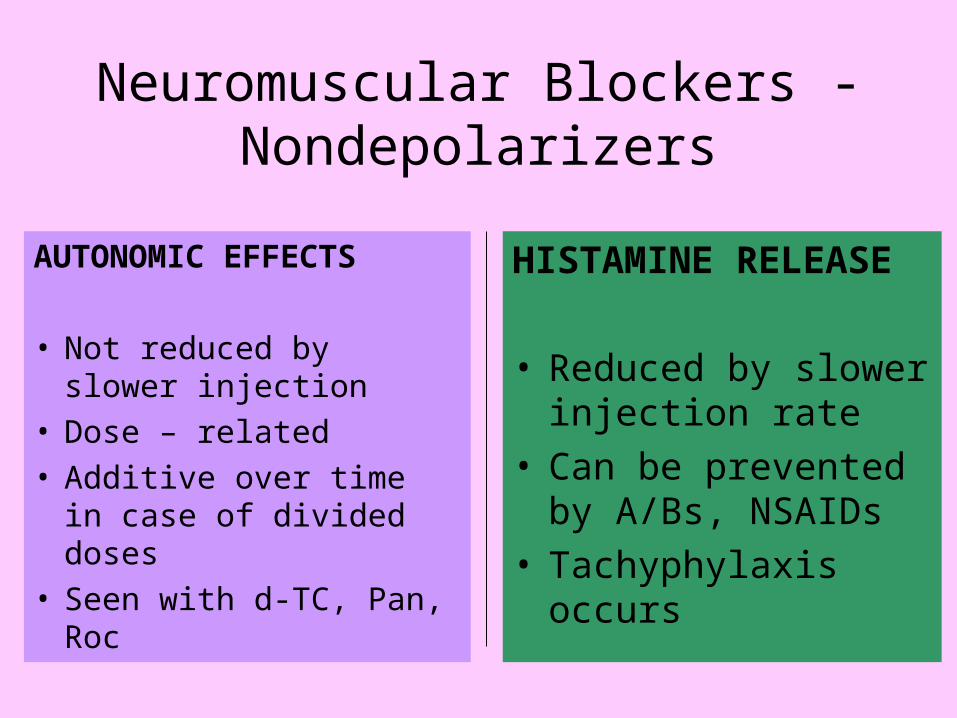
Neuromuscular Blockers - Nondepolarizers
AUTONOMIC EFFECTS
• Not reduced by slower injection
• Dose – related• Additive over time in
case of divided doses• Seen with d-TC, Pan, Roc
HISTAMINE RELEASE
• Reduced by slower injection rate
• Can be prevented by A/Bs, NSAIDs
• Tachyphylaxis occurs
Neuromuscular Blockers - Nondepolarizers
HISTAMINE RELEASE• Erythema of face, neck, torso; moderate BP, HR; rarely bronchospasm; degranulation of serosal mast cells in skin, conn. tissue & near blood vessels & nerves.
• Mainly with mivacurium, atracurium, doxacurium, d-TC, metocurine

Neuromuscular Blockers - Nondepolarizers
Panc.Panc. Vec.Vec. Atrac.Atrac. Roc.Roc.
HR -
BP - -
Autonomic effects
+ - - +
Histamine release
- - ++ -
Local Anaesthetics
rate of depolarization in fast-conducting tissue of Purkinje bundle & ventricular myocardium ( fast Na+ conductance depresses rapid phase of depolarization)
contractility, BP, HR, asystole resistant to pacing
Local Anaesthetics
• Prolonged PR-interval, duration of QRS - complex
spontaneous pacemaker activity in SAN sinus bradycardia, sinus arrest
• Dose dependent (-)ive inotropic action on heart
Local Anaesthetics
• Biphasic action on vascular smooth muscle (low concn – vasoconstriction; high concn – vasodilation)
• Indirect action – due to autonomic blockade
• CC / CNS ratio –
Lignocaine > Etidocaine > Bupivacaine
Local Anaesthetics
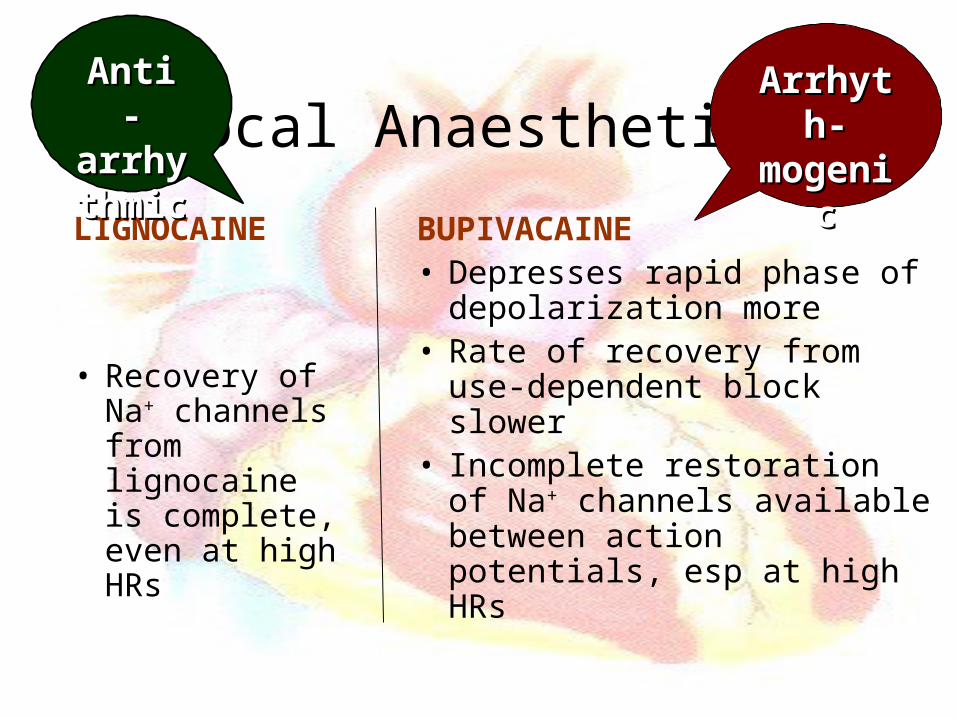
LIGNOCAINE
• Recovery of Na+ channels from lignocaine is complete, even at high HRs
BUPIVACAINE• Depresses rapid phase of
depolarization more• Rate of recovery from use-
dependent block slower• Incomplete restoration of Na+
channels available between action potentials, esp at high HRs
Anti - Anti - arrhytarrhythmichmic
ArrhythArrhyth--
mogenicmogenic
Local Anaesthetics
Bupivacaine : R- bupi more cardiotoxic.
Prolonged PR-interval & QRS complex, predisposition to re-entrant arrhythmias, VT / VF / Heart blocks / CHF (due to loss of contractility) resistant to defibrillation
Cardiovascular stability
• Careful selection of agent• Titrated doses * To patient & comorbid conditions
* To surgery
• Slow rate of administration
• Knowledge of cardiovascular effects
• Prompt recognition & appropriate treatment in case of problems