Embed Size (px)
Citation preview

Magnetic Resonance Venography & Venous Ultrasonography for Diagnosing Deep Venous Thrombosis:A Prospective Blinded Comparative Study
Prof. Shad Salim AkhtarMBBS, MD, MRCP(UK), FRCP (Edin), FACP(USA)
Consultant Medical OncologistMedical DirectorKFSH, PFOCBuraidah, Al-Qassim, Saudi Arabia

Scenario
45 female attends A & E Swelling left legPainful2 days duration
No other illnessNo drugsO/E
Left leg ?swollen, non tender, not hot

Questions?
Does she have DVT?Admit?Review latter?What test to ask for?Shall I anticoagulate her?

Deep Vein Thrombosis
Usually originates in deep veins of calf Venous sinuses of soleus & gastrocnemius
Rarely popliteal, femoral, iliac Symptoms and signs are not characteristic
Qaseem A et al: Ann Fam Med 2007; 5:57Cantwell CP et al: J Vasc Interv Radiol 2006; 17:163
Only 20-30% have actually DVT>50% are never diagnosed

Deep Vein Thrombosis
Incorrect diagnosis!Misdiagnosis
Increased risk of PEPost-thrombotic syndrome
Over diagnosisAnticoagulation related bleeding
Qaseem A etal: Ann Fam Med 2007; 5:57Cantwell CP etal: J Vasc Interv Radiol 2006; 17:163

Wells Prediction Rule for Predicting Pretest Probability of Deep Vein Thrombosis
low ≤0; intermediate 1-2; high ≥3: If symptoms in 2 legs assess more symptomatic leg
Wells PS et al: Lancet 1997; 350:1795

Deep Venous Thrombosis
Objective diagnosis is
essential

Ho WK et al: Med J Aust 2005; 182:476

DVT Diagnostic Tools
D-dimer assayContrast venography
Gold standardNot appropriate as the first test
Venous ultrasonographyComputed tomographic venographyMagnetic resonance imaging
Merli G: Am J Med 2005; 118 (8A):3S

Venous Ultrasonography-Accuracy
Site Sensitivity% Specificity%Proximal 94-100 98-99Distal 60-70 60
Kyrle PA, Eichenger S: Lancet 2005; 365: 1163–74

Venous Ultrasonography-Limitations
3-34% need repeated study at 1 wkLess accurate diagnosis below kneeLimited visualization of pelvic veinsDifficulty in diagnosing recurrencePoor sensitivity in asymptomatic
patients
Lensing AW et al: Lancet 1999; 353: 479

Venous Ultrasonography-Limitations
TechnicalOedemaWound Immobilization devicesTendernessObesity
DiagnosticOperator dependentRecannalized vs fresh thrombus!!
Kearon C et al; Ann Intern Med 1998; 128:663

MRV vs Venous USG Study
King Fahd Specialist Hospital/Prince Faisal Oncology Centre
ProspectiveBlindedNon randomizedApproved by institute research/ethics
committee

Patients & Methods
Inclusion criteriaPatients admitted with suspected DVTAge >=18 years age
Exclusion criteriaContraindications for MRVSymptoms for more than 2 weeksHistory of ipsilateral DVT

Patients & Methods
A data abstraction form was designedDetailed history takenPhysical examination conducted Procedures were explained to the patientInformed consent was soughtVU & MRV were performed within 48 hrs
of admission

Patients & Methods-Imaging Techniques
MRV Performed by trained radiographersSuperconducting magnet 1.5 Tesla unit
(GE, Signa Horizon, USA)45 cms body coil Time of flight with fat saturationThree imaging blocks from ankle to IVCBoth legs were examined simultaneouslyAcquisition time 45 minutes

Patients & Methods-Imaging Techniques
Venous ultrasonography Qualified radiologist
Blinded to the result of MRV Symptomatic limb examined 5-7 MHZ linear array transducer
(GE Logic 400, USA) Examination procedure
Compression Augmentation manoeuvres Colour doppler evaluation of whole limb Calf to iliac veins

Patients & Methods-Imaging Analysis
VU and MRV analysed by two radiologists BLINDED to other modality
MRV Venous segments read Coronal source data Standard imaging reconstruction techniques Patency normal flow Thrombosis low signal intensity in venous lumen

VUThrombosis
non compressibilityAbsent flowVisibility of thrombus in lumen
Findings recorded in a standard format
Patients & Methods-Imaging Analysis

Patients & Methods-Statistical analysis
Data computerizedCompared by Chi square test for paired
variables with Yate’s correctionP value <0.05 was considered significant

Results
No of patients 40Exclusions 9
Previous ipsilat DVT 2Symptoms > 2wks 2Pregnant 2 Implanted met device 1Refusal to consent 1VU technically difficult 1

Results
Male:Female::10: 21Age
Range 18-85 yrsMean females 33 (14.5)Mean males 44 (23.8)

Results-Symptoms
Pain 29 (93.5%)Swelling 26 (83.6%)
Duration of symptoms = 1-14 days (median 6 days)Duration of symptoms 1-14 days, median 6 days

Results-Signs
Sign No (%)Increase temp 14 (45.2) 3 cm difference in diameter Above knee 17 (54.8) Below knee only 8 (25.8) Redness 3 (9.7)

Results-Co morbidity
Co morbidity No (%)Surgery 6 (19.4)Post partum 4 (12.9)Malignancy 2 (6.4)Varicosities 2 (6.4)Trauma 1 (3.2)

Results-Detection of thrombus
Venous segment
Imaging Study
MRV (%) VU (%)
+ve -ve +ve -ve p value
Calf vein 12 (38.7) 19 (61.3) 8 (25.8) 23 (74.2) 0.42
Popliteal 14 (45.2) 17 (54.8) 15 (48.4) 16 (51.6) 1.00
Femoral 20 (64.5) 11 (35.4) 19 (61.3) 12 (38.7) 1.00
Iliac 19 (61.3) 12 (38.7) 7 (22.6) 24 (77.4) <0.05
IVC 5 (16.1) 26 (83.9) Not assessed

Top
a
Venous segment
Imaging Study
MRV (%) VU (%)
+ve -ve +ve -ve p value
Calf vein 12 (38.7) 19 (61.3) 8 (25.8) 23 (74.2) 0.42
Popliteal 14 (45.2) 17 (54.8) 15 (48.4) 16 (51.6) 1.00
Results-Detection of thrombus

Top
b
Venous segment
Imaging Study
MRV (%) VU (%)+ve -ve +ve -ve p value
Femoral 20 (64.5)
11 (35.4)
19 (61.3)
12 (38.7)
1.00
Results-Detection of thrombus

c
Top
Venous segment
Imaging Study
MRV (%) VU (%)+ve -ve +ve -ve p value
Iliac 19 (61.3)
12 (38.7)
7 (22.6)
24 (77.4)
<0.05
IVC 5 (16.1)
26 (83.9)
Not assessed

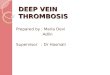
Venography MRDTI VU
Fraser DGW et al: Ann Intern Med. 2002;136:89-98

Cantwell CP etal: J Vasc Interv Radiol 2006; 17:163
Soleus muscle venous thrombosis
Axial true FISP image

Sensitivity and Specificity of True FISP MRV for DVT Detection by Segment and Overall
Venous Segment
Sensitivity (%) Specificity (%)
Iliac 100 100Femoral 100 98Popliteal 100 100Tibial & others 68 94Overall 87 98
Cantwell CP etal: J Vasc Interv Radiol 2006; 17:163

Conclusion
Missing true gold standard for DVTContrast venography most reliable Difficult & invasive
Can MRV be the “gold standard”Non-invasive No radiationAccurateComprehensive imaging Reproducible

Conclusion
Barriers to MRVLack of availability High costLong examination time
FutureScanners becoming plentiful CheaperRapid scanning speedCosts may decrease

Zahid Nabi MRCP (I), FCPS, Khalida Parveen Salim MD, MRCR (UK), Ahmad Salamah Balah MBBCh, MD, Mohammed Kamel Al Adli MD, CES
Prince Faisal Oncology Centre, King Fahd Specialist Hospital,
Buraidah Al-Qassim, Kingdom of Saudi Arabia
Co-Investigators