Embed Size (px)
Citation preview
nursece4less.com nursece4less.com nursece4less.com nursece4less.com 1
Deep Vein Thrombosis:
Prevention And
Prognosis
Jassin M. Jouria, MD
Dr. Jassin M. Jouria is a medical doctor,
professor of academic medicine, and
medical author. He graduated from Ross
University School of Medicine and has
completed his clinical clerkship training in
various teaching hospitals throughout New
York, including King’s County Hospital
Center and Brookdale Medical Center,
among others. Dr. Jouria has passed all
USMLE medical board exams, and has served as a test prep tutor and instructor for
Kaplan. He has developed several medical courses and curricula for a variety of
educational institutions. Dr. Jouria has also served on multiple levels in the academic
field including faculty member and Department Chair. Dr. Jouria continues to serves
as a Subject Matter Expert for several continuing education organizations covering
multiple basic medical sciences. He has also developed several continuing medical
education courses covering various topics in clinical medicine. Recently, Dr. Jouria
has been contracted by the University of Miami/Jackson Memorial Hospital’s
Department of Surgery to develop an e-module training series for trauma patient
management. Dr. Jouria is currently authoring an academic textbook on Human
Anatomy & Physiology.
Abstract
Although there are a number of risk factors associated with deep vein
thrombosis (DVT), it can strike anyone regardless of age, physical
fitness, or other factors. However, DVT has an excellent prognosis
when caught early and treated aggressively. Additionally, there are a
number of strategies for reducing DVT risk. Nurses should familiarize
themselves with these strategies in order to be prepared to advise
their patients on lifestyle adjustments and other actions that can lower
this risk. This course also aims to increase the awareness and clinical
acumen of nurses in their evaluation of deep vein thrombosis.
nursece4less.com nursece4less.com nursece4less.com nursece4less.com 2
Continuing Nursing Education Course Planners
William A. Cook, PhD, Director, Douglas Lawrence, MA, Webmaster,
Susan DePasquale, MSN, FPMHNP-BC, Lead Nurse Planner
Policy Statement
This activity has been planned and implemented in accordance with
the policies of NurseCe4Less.com and the continuing nursing education
requirements of the American Nurses Credentialing Center's
Commission on Accreditation for registered nurses. It is the policy of
NurseCe4Less.com to ensure objectivity, transparency, and best
practice in clinical education for all continuing nursing education (CNE)
activities.
Continuing Education Credit Designation
This educational activity is credited for 1.5 hours. Nurses may only
claim credit commensurate with the credit awarded for completion of
this course activity.
Statement of Learning Need
Patients with DVT may or may not exhibit symptoms. Its important
health professionals help patients understand DVT prevention, risks
and symptoms to avoid future complications.
Course Purpose
To provide nursing professionals with knowledge of DVT prevention,
recognition and treatment options.
nursece4less.com nursece4less.com nursece4less.com nursece4less.com 3
Target Audience
Advanced Practice Registered Nurses and Registered Nurses
(Interdisciplinary Health Team Members, including Vocational Nurses
and Medical Assistants may obtain a Certificate of Completion)
Course Author & Planning Team Conflict of Interest Disclosures
Jassin M. Jouria, MD, William S. Cook, PhD, Douglas Lawrence, MA,
Susan DePasquale, MSN, FPMHNP-BC – all have no disclosures
Acknowledgement of Commercial Support
There is no commercial support for this course.
Activity Review Information
Reviewed by Susan DePasquale, MSN, FPMHNP-BC
Release Date: 1/1/2016 Termination Date: 4/1/2018
Please take time to complete a self-assessment of knowledge,
on page 4, sample questions before reading the article.
Opportunity to complete a self-assessment of knowledge
learned will be provided at the end of the course.
nursece4less.com nursece4less.com nursece4less.com nursece4less.com 4
1. A pulmonary embolism occurs when a clot becomes
dislodged and travels to the ________. a. Respiratory system
b. Lung
c. Digestive system
d. Immune system
2. Compression stockings that will be used to treat DVT
should be a grade ___________. a. 1
b. 2
c. 3
d. 4
3. This is the procedure that injects medication directly into the blood clot via catheter to dissolve the clot.
a. Angioplasty
b. Thrombolytic Therapy
c. Bypass
d. Laparoscopy
4. Which of the following is NOT a risk factor for DVT?
a. Smoking
b. Strength Training
c. Pregnancy
d. Age
5. Which of the following is a long-term complication of DVT
that causes damage to the vein? a. Pulmonary Embolism
b. Heart Attack
c. Post-Thrombotic Syndrome
d. Blockage
nursece4less.com nursece4less.com nursece4less.com nursece4less.com 5
Introduction
Deep vein thrombosis is a blood clot that forms deep in the vein. Most
deep vein thrombosis occurs in the lower extremities, but it can also
occur in other areas of the body. Deep vein thrombosis is typically the
result of lack of movement or vein injury, and is especially common in
patients who have recently had surgery.1
Deep vein thrombosis can cause long term damage if not treated
properly, but has an excellent prognosis when caught early and
treated aggressively.2 While the clot itself is not a concern, the
potential complications that it can cause are of concern. Some patients
will experience a pulmonary embolism if the clot breaks free and
travels to the blood vessels of the lung. When this occurs, the risk of
morbidity is high. In some instances, patients will develop post-
thrombotic syndrome, which impacts the patient’s mobility and level of
basic functioning.
Increasing Patient Awareness Of DVT
Although there are a number of risk factors associated with deep vein
thrombosis, it can strike anyone regardless of age, physical fitness, or
other factors. However, DVT has an excellent prognosis when caught
early and treated aggressively. Additionally, there are a number of
strategies for reducing DVT risk. It is important for health care
providers to familiarize themselves with these strategies in order to be
prepared to advise their patients on lifestyle adjustments and other
actions that can lower this risk. The following fact sheet, produced by
the Vascular Disease Organization, provides a thorough overview of
deep vein thrombosis and the potential complications.3 This fact sheet
nursece4less.com nursece4less.com nursece4less.com nursece4less.com 6
can be distributed to healthcare professionals or patients to increase
awareness of deep vein thrombosis.
Deep Vein Thrombosis Fact Sheet
Overview
Deep vein thrombosis, commonly referred to as “DVT,” occurs when a blood clot or
thrombus, develops in the large veins of the legs or pelvic area. Some DVTs may
cause no pain, whereas others can be quite painful. With prompt diagnosis and
treatment, the majority of DVTs are not life threatening. However, a blood clot
that forms in the invisible “deep veins” can be life threatening. A clot that forms in
the large, deep veins is more likely to break free and travel through the vein. It is
then called an embolus. When an embolus travels from the legs or pelvic areas and
lodges in a lung artery, the condition is known as a “pulmonary embolism,” or PE,
a potentially fatal condition if not immediately diagnosed and treated.
Symptoms
Approximately one-half of those with a DVT never have recognizable symptoms.
The most common symptom is leg pain and tenderness in the calf muscles. One
may also observe swelling or a change in color of one leg to purple or blue. These
signs and symptoms may appear suddenly or may steadily develop over a short
period of time. Symptoms are quite different if the clot breaks loose and travel to
the lungs, causing a pulmonary embolism (PE). The symptoms of PE include chest
pain, shortness of breath, rapid pulse, or a cough. There may also be a feeling of
apprehension, sweating, or fainting. Such symptoms are not specific to a PE, and
can occur with pneumonia, heart attack, and other medical conditions.
Underlying Causes Of DVT
Deep vein thrombosis is typically caused by lack of movement or a
vein injury. In both instances, DVT will develop if an individual does
not take appropriate preventative measures.4
nursece4less.com nursece4less.com nursece4less.com nursece4less.com 7
Lack of Movement
Lack of movement is the most common cause of DVT, yet it is easily
preventable. In most instances, the cause is immobility after surgery
or during extended periods of travel.5 However, any situation that
involves immobility is a potential risk for the development of DVT.
Lack of movement causes blood flow to become sluggish, which can
result in the development of blood clots.6
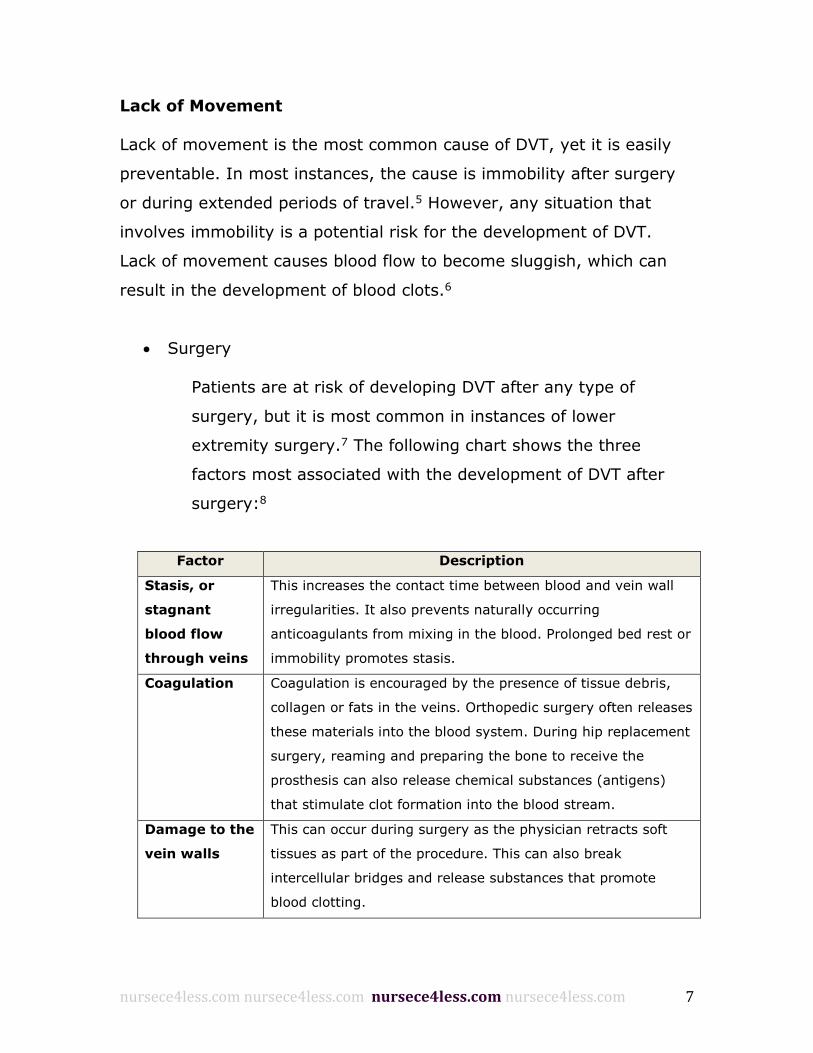
Surgery
Patients are at risk of developing DVT after any type of
surgery, but it is most common in instances of lower
extremity surgery.7 The following chart shows the three
factors most associated with the development of DVT after
surgery:8
Factor Description
Stasis, or
stagnant
blood flow
through veins
This increases the contact time between blood and vein wall
irregularities. It also prevents naturally occurring
anticoagulants from mixing in the blood. Prolonged bed rest or
immobility promotes stasis.
Coagulation Coagulation is encouraged by the presence of tissue debris,
collagen or fats in the veins. Orthopedic surgery often releases
these materials into the blood system. During hip replacement
surgery, reaming and preparing the bone to receive the
prosthesis can also release chemical substances (antigens)
that stimulate clot formation into the blood stream.
Damage to the
vein walls
This can occur during surgery as the physician retracts soft
tissues as part of the procedure. This can also break
intercellular bridges and release substances that promote
blood clotting.
nursece4less.com nursece4less.com nursece4less.com nursece4less.com 8
The above chart provides the three main factors that
contribute to the development of DVT in individuals who have
had surgery. However, there are other factors that may
increase the risk for surgery patients. These factors include
the following:9
o Age
o Previous history of DVT or pulmonary emboli
o Metastatic malignancy
o Vein disease (such as varicose veins)
o Smoking
o Estrogen usage or current pregnancy
o Obesity
o Genetic factors
Long Trips
There is a lower risk of developing DVT during travel, but it is
still a concern. Recent studies have produced conflicting results.
In some instances, studies have shown an increase in the risk of
developing DVT during extended periods of travel, while other
studies have shown no increased risk.2
In most instances of travel related DVT, the individual has other
risk factors that make them more susceptible to DVT, which
include:10
o Age
o Previous history of DVT or pulmonary emboli
o Metastatic malignancy
o Vein disease (such as varicose veins)
o Smoking
nursece4less.com nursece4less.com nursece4less.com nursece4less.com 9
o Estrogen usage or current pregnancy
o Obesity
o Genetic factors
In many travel related DVT cases, the individual may have
asymptomatic, or mild, DVT. This type of DVT tends to resolve
on its own after the patient begins moving again.2
Vein Injury
A patient’s chance of developing DVT increases when the patient’s vein
is already damaged from another cause. Damage to the inside of the
vein increases the risk of blood clot formation.11 In some instances,
damage is caused by a previous DVT. Therefore, a patient who has a
history of DVT is at an increased risk of developing another DVT due to
the permanent damage caused to the vein.12
Vein damage may also occur as the result of increased inflammation
from other health conditions or prescription drugs.13 Another cause of
vein damage is needle injection, which can occur in a healthcare
setting or during injection drug use.3
Diagnosis
Deep vein thrombosis can be difficult to diagnose as it is not easily
identifiable upon an initial exam.14 When a patient is at risk of
developing DVT, or when a patient presents symptoms of DVT,
diagnostic imaging techniques will be used to identify any damage.15
nursece4less.com nursece4less.com nursece4less.com nursece4less.com 10
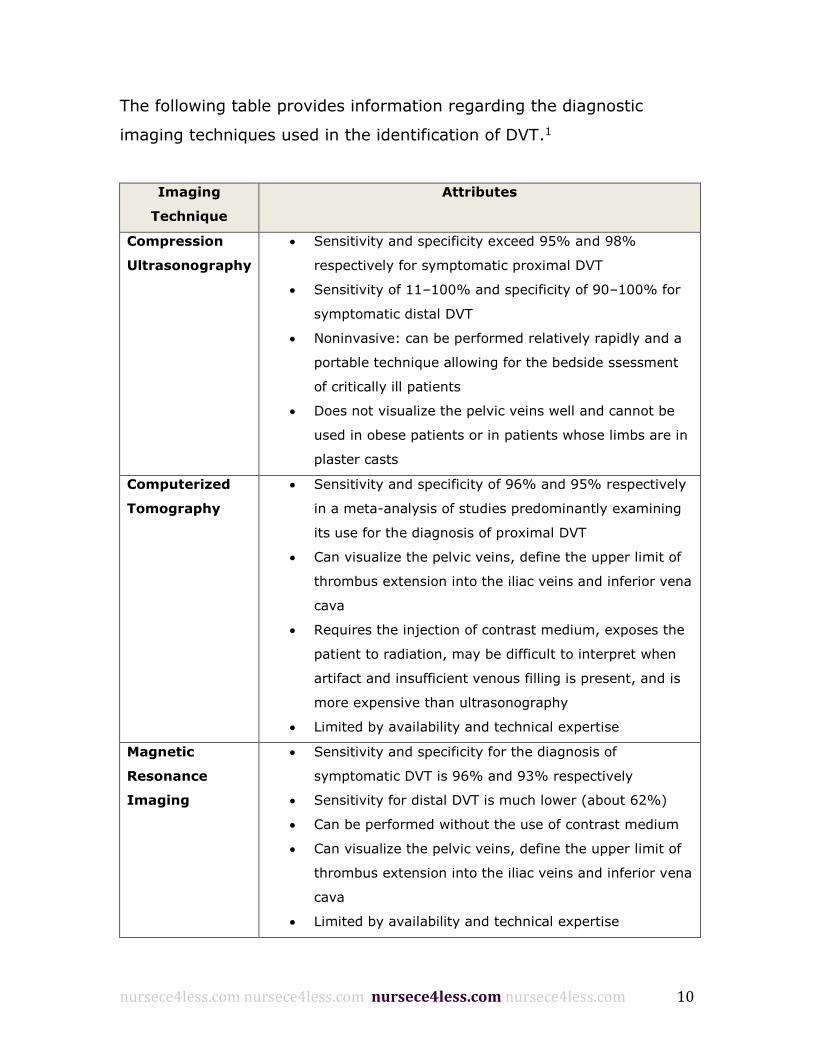
The following table provides information regarding the diagnostic
imaging techniques used in the identification of DVT.1
Imaging
Technique
Attributes
Compression
Ultrasonography
Sensitivity and specificity exceed 95% and 98%
respectively for symptomatic proximal DVT
Sensitivity of 11–100% and specificity of 90–100% for
symptomatic distal DVT
Noninvasive: can be performed relatively rapidly and a
portable technique allowing for the bedside ssessment
of critically ill patients
Does not visualize the pelvic veins well and cannot be
used in obese patients or in patients whose limbs are in
plaster casts
Computerized
Tomography
Sensitivity and specificity of 96% and 95% respectively
in a meta-analysis of studies predominantly examining
its use for the diagnosis of proximal DVT
Can visualize the pelvic veins, define the upper limit of
thrombus extension into the iliac veins and inferior vena
cava
Requires the injection of contrast medium, exposes the
patient to radiation, may be difficult to interpret when
artifact and insufficient venous filling is present, and is
more expensive than ultrasonography
Limited by availability and technical expertise
Magnetic
Resonance
Imaging
Sensitivity and specificity for the diagnosis of
symptomatic DVT is 96% and 93% respectively
Sensitivity for distal DVT is much lower (about 62%)
Can be performed without the use of contrast medium
Can visualize the pelvic veins, define the upper limit of
thrombus extension into the iliac veins and inferior vena
cava
Limited by availability and technical expertise
nursece4less.com nursece4less.com nursece4less.com nursece4less.com 11
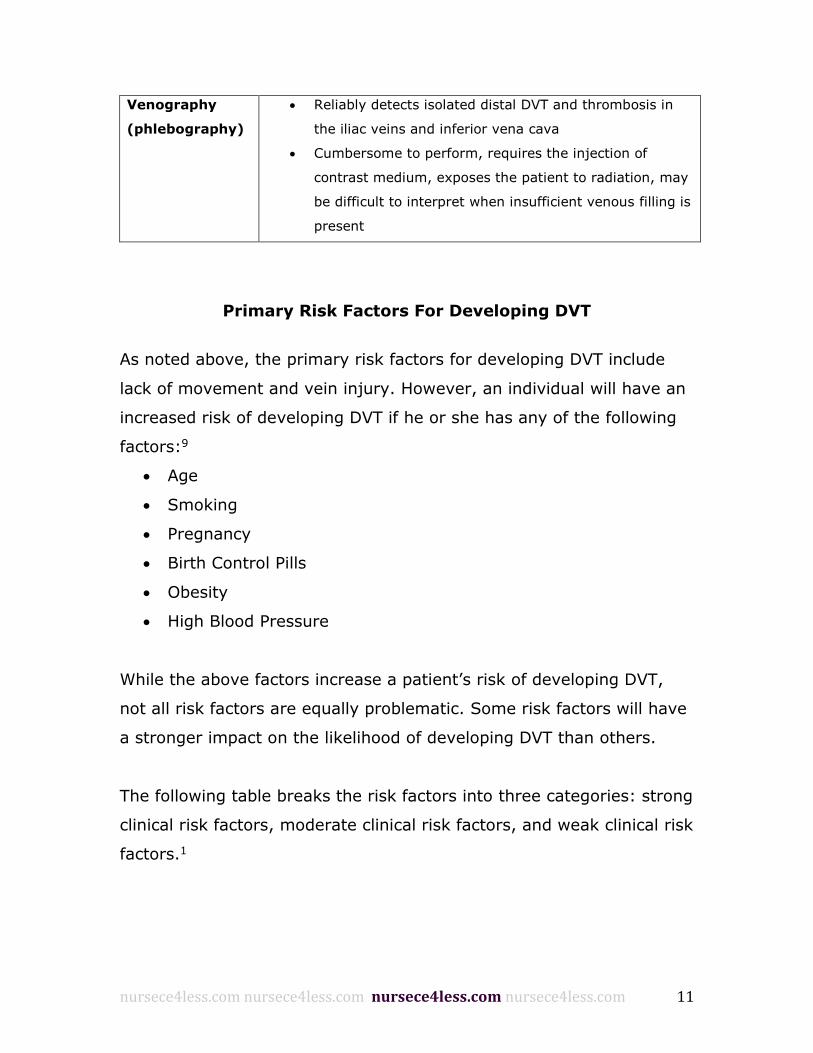
Venography
(phlebography)
Reliably detects isolated distal DVT and thrombosis in
the iliac veins and inferior vena cava
Cumbersome to perform, requires the injection of
contrast medium, exposes the patient to radiation, may
be difficult to interpret when insufficient venous filling is
present
Primary Risk Factors For Developing DVT
As noted above, the primary risk factors for developing DVT include
lack of movement and vein injury. However, an individual will have an
increased risk of developing DVT if he or she has any of the following
factors:9
Age
Smoking
Pregnancy
Birth Control Pills
Obesity
High Blood Pressure
While the above factors increase a patient’s risk of developing DVT,
not all risk factors are equally problematic. Some risk factors will have
a stronger impact on the likelihood of developing DVT than others.
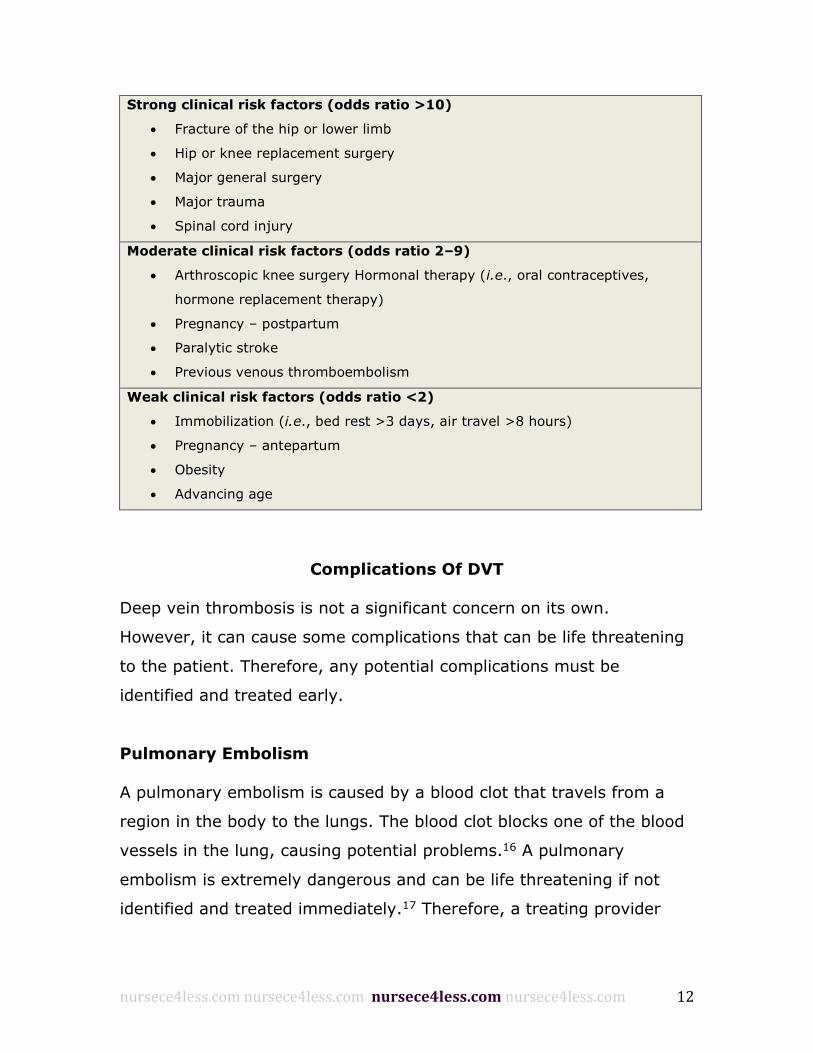
The following table breaks the risk factors into three categories: strong
clinical risk factors, moderate clinical risk factors, and weak clinical risk
factors.1
nursece4less.com nursece4less.com nursece4less.com nursece4less.com 12
Strong clinical risk factors (odds ratio >10)
Fracture of the hip or lower limb
Hip or knee replacement surgery
Major general surgery
Major trauma
Spinal cord injury
Moderate clinical risk factors (odds ratio 2–9)
Arthroscopic knee surgery Hormonal therapy (i.e., oral contraceptives,
hormone replacement therapy)
Pregnancy – postpartum
Paralytic stroke
Previous venous thromboembolism
Weak clinical risk factors (odds ratio <2)
Immobilization (i.e., bed rest >3 days, air travel >8 hours)
Pregnancy – antepartum
Obesity
Advancing age
Complications Of DVT
Deep vein thrombosis is not a significant concern on its own.
However, it can cause some complications that can be life threatening
to the patient. Therefore, any potential complications must be
identified and treated early.
Pulmonary Embolism
A pulmonary embolism is caused by a blood clot that travels from a
region in the body to the lungs. The blood clot blocks one of the blood
vessels in the lung, causing potential problems.16 A pulmonary
embolism is extremely dangerous and can be life threatening if not
identified and treated immediately.17 Therefore, a treating provider
nursece4less.com nursece4less.com nursece4less.com nursece4less.com 13
should be aware of the following signs and symptoms of a pulmonary
embolism:18
Unexplained sudden onset of shortness of breath
Chest pain or discomfort that worsens with a deep breath or
cough
Feeling lightheaded or dizzy, or fainting
Rapid pulse
Sweating
Coughing up blood
A sense of anxiety or nervousness
Deep vein thrombosis is the most common cause of a pulmonary
embolism. Once a clot has formed, usually in the leg, it may
immediately break off and travel to the lungs, or it may not happen for
a number of days after the formation of the clot.19 It is important to
identify the problem as soon as possible as early treatment can reduce
the likelihood that the embolism will be life threatening.20 The
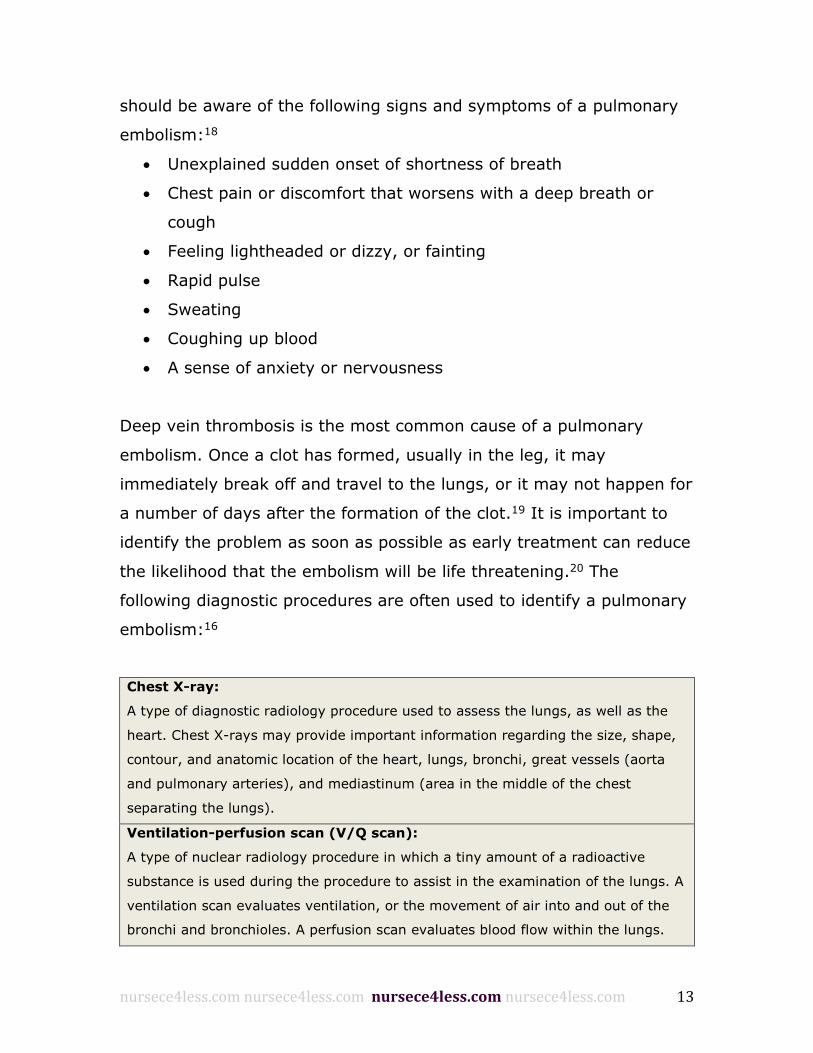
following diagnostic procedures are often used to identify a pulmonary
embolism:16
Chest X-ray:
A type of diagnostic radiology procedure used to assess the lungs, as well as the
heart. Chest X-rays may provide important information regarding the size, shape,
contour, and anatomic location of the heart, lungs, bronchi, great vessels (aorta
and pulmonary arteries), and mediastinum (area in the middle of the chest
separating the lungs).
Ventilation-perfusion scan (V/Q scan):
A type of nuclear radiology procedure in which a tiny amount of a radioactive
substance is used during the procedure to assist in the examination of the lungs. A
ventilation scan evaluates ventilation, or the movement of air into and out of the
bronchi and bronchioles. A perfusion scan evaluates blood flow within the lungs.
nursece4less.com nursece4less.com nursece4less.com nursece4less.com 14
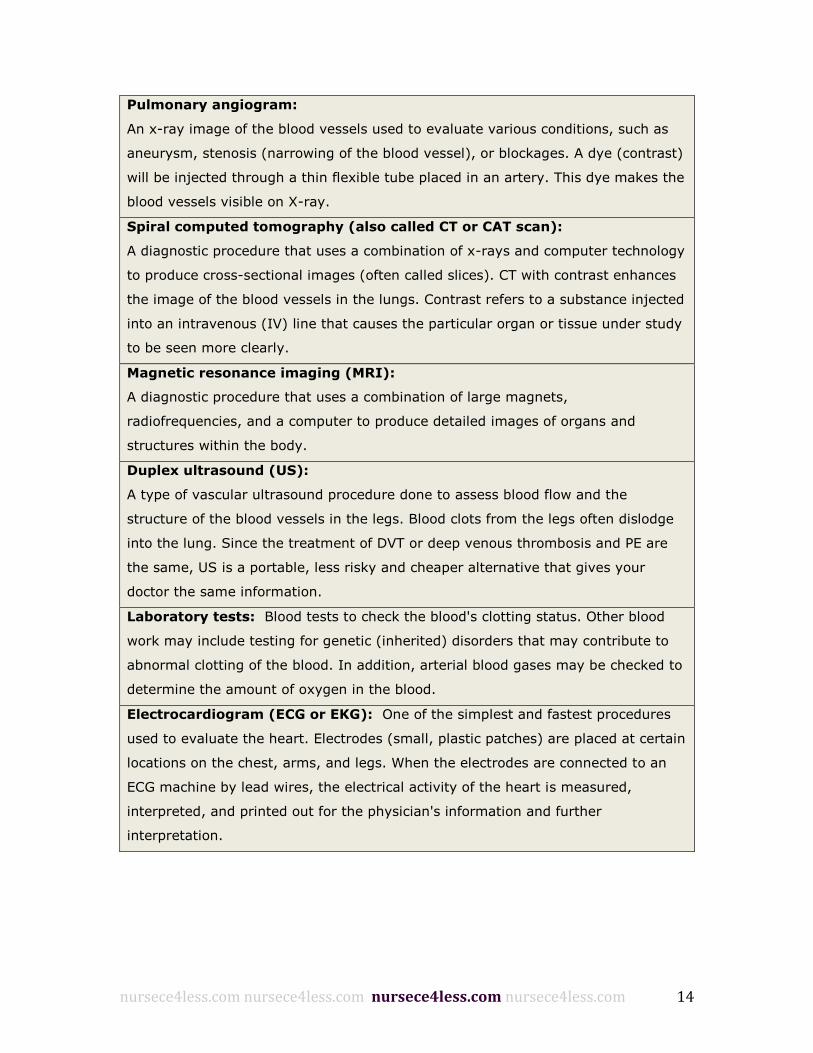
Pulmonary angiogram:
An x-ray image of the blood vessels used to evaluate various conditions, such as
aneurysm, stenosis (narrowing of the blood vessel), or blockages. A dye (contrast)
will be injected through a thin flexible tube placed in an artery. This dye makes the
blood vessels visible on X-ray.
Spiral computed tomography (also called CT or CAT scan):
A diagnostic procedure that uses a combination of x-rays and computer technology
to produce cross-sectional images (often called slices). CT with contrast enhances
the image of the blood vessels in the lungs. Contrast refers to a substance injected
into an intravenous (IV) line that causes the particular organ or tissue under study
to be seen more clearly.
Magnetic resonance imaging (MRI):
A diagnostic procedure that uses a combination of large magnets,
radiofrequencies, and a computer to produce detailed images of organs and
structures within the body.
Duplex ultrasound (US):
A type of vascular ultrasound procedure done to assess blood flow and the
structure of the blood vessels in the legs. Blood clots from the legs often dislodge
into the lung. Since the treatment of DVT or deep venous thrombosis and PE are
the same, US is a portable, less risky and cheaper alternative that gives your
doctor the same information.
Laboratory tests: Blood tests to check the blood's clotting status. Other blood
work may include testing for genetic (inherited) disorders that may contribute to
abnormal clotting of the blood. In addition, arterial blood gases may be checked to
determine the amount of oxygen in the blood.
Electrocardiogram (ECG or EKG): One of the simplest and fastest procedures
used to evaluate the heart. Electrodes (small, plastic patches) are placed at certain
locations on the chest, arms, and legs. When the electrodes are connected to an
ECG machine by lead wires, the electrical activity of the heart is measured,
interpreted, and printed out for the physician's information and further
interpretation.
nursece4less.com nursece4less.com nursece4less.com nursece4less.com 15
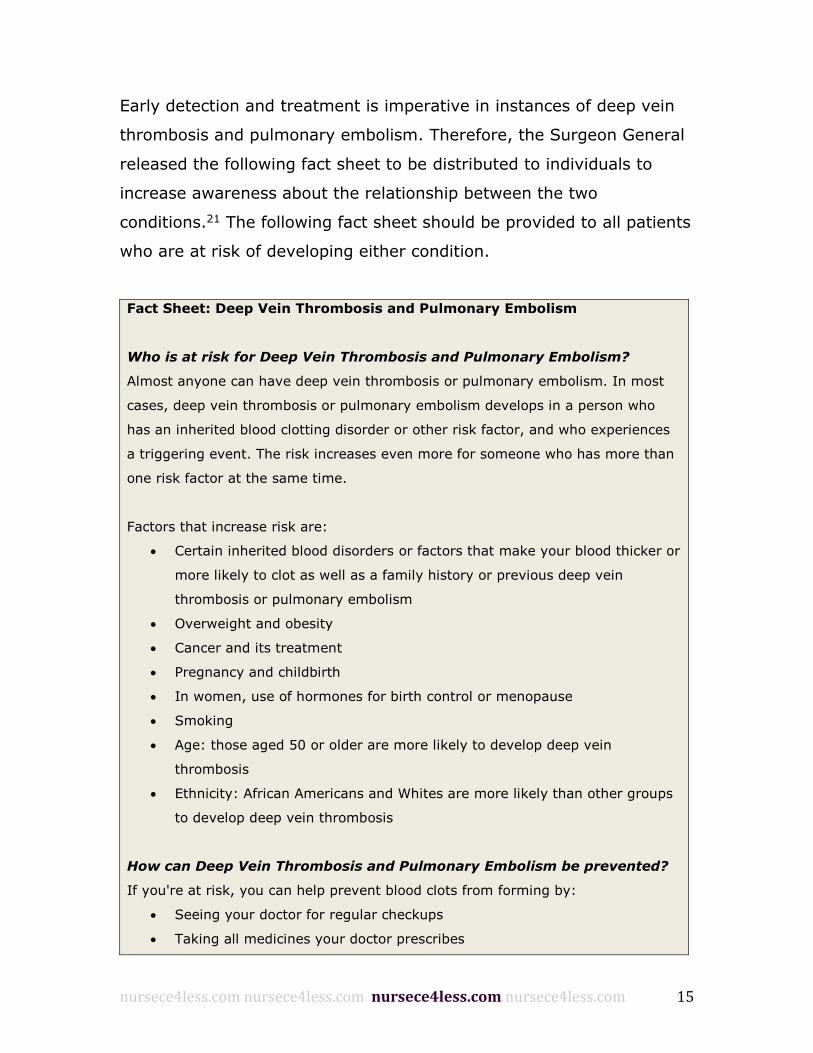
Early detection and treatment is imperative in instances of deep vein
thrombosis and pulmonary embolism. Therefore, the Surgeon General
released the following fact sheet to be distributed to individuals to
increase awareness about the relationship between the two
conditions.21 The following fact sheet should be provided to all patients
who are at risk of developing either condition.
Fact Sheet: Deep Vein Thrombosis and Pulmonary Embolism
Who is at risk for Deep Vein Thrombosis and Pulmonary Embolism?
Almost anyone can have deep vein thrombosis or pulmonary embolism. In most
cases, deep vein thrombosis or pulmonary embolism develops in a person who
has an inherited blood clotting disorder or other risk factor, and who experiences
a triggering event. The risk increases even more for someone who has more than
one risk factor at the same time.
Factors that increase risk are:
Certain inherited blood disorders or factors that make your blood thicker or
more likely to clot as well as a family history or previous deep vein
thrombosis or pulmonary embolism
Overweight and obesity
Cancer and its treatment
Pregnancy and childbirth
In women, use of hormones for birth control or menopause
Smoking
Age: those aged 50 or older are more likely to develop deep vein
thrombosis
Ethnicity: African Americans and Whites are more likely than other groups
to develop deep vein thrombosis
How can Deep Vein Thrombosis and Pulmonary Embolism be prevented?
If you're at risk, you can help prevent blood clots from forming by:
Seeing your doctor for regular checkups
Taking all medicines your doctor prescribes
nursece4less.com nursece4less.com nursece4less.com nursece4less.com 16
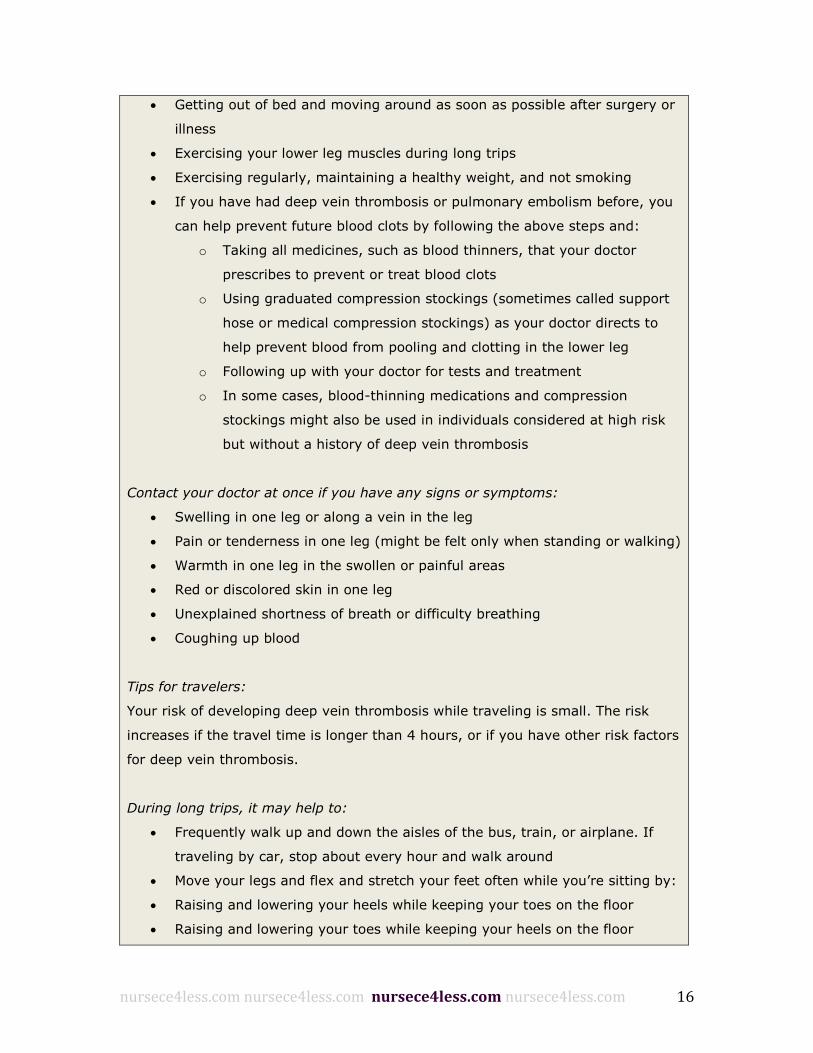
Getting out of bed and moving around as soon as possible after surgery or
illness
Exercising your lower leg muscles during long trips
Exercising regularly, maintaining a healthy weight, and not smoking
If you have had deep vein thrombosis or pulmonary embolism before, you
can help prevent future blood clots by following the above steps and:
o Taking all medicines, such as blood thinners, that your doctor
prescribes to prevent or treat blood clots
o Using graduated compression stockings (sometimes called support
hose or medical compression stockings) as your doctor directs to
help prevent blood from pooling and clotting in the lower leg
o Following up with your doctor for tests and treatment
o In some cases, blood-thinning medications and compression
stockings might also be used in individuals considered at high risk
but without a history of deep vein thrombosis
Contact your doctor at once if you have any signs or symptoms:
Swelling in one leg or along a vein in the leg
Pain or tenderness in one leg (might be felt only when standing or walking)
Warmth in one leg in the swollen or painful areas
Red or discolored skin in one leg
Unexplained shortness of breath or difficulty breathing
Coughing up blood
Tips for travelers:
Your risk of developing deep vein thrombosis while traveling is small. The risk
increases if the travel time is longer than 4 hours, or if you have other risk factors
for deep vein thrombosis.
During long trips, it may help to:
Frequently walk up and down the aisles of the bus, train, or airplane. If
traveling by car, stop about every hour and walk around
Move your legs and flex and stretch your feet often while you’re sitting by:
Raising and lowering your heels while keeping your toes on the floor
Raising and lowering your toes while keeping your heels on the floor
nursece4less.com nursece4less.com nursece4less.com nursece4less.com 17
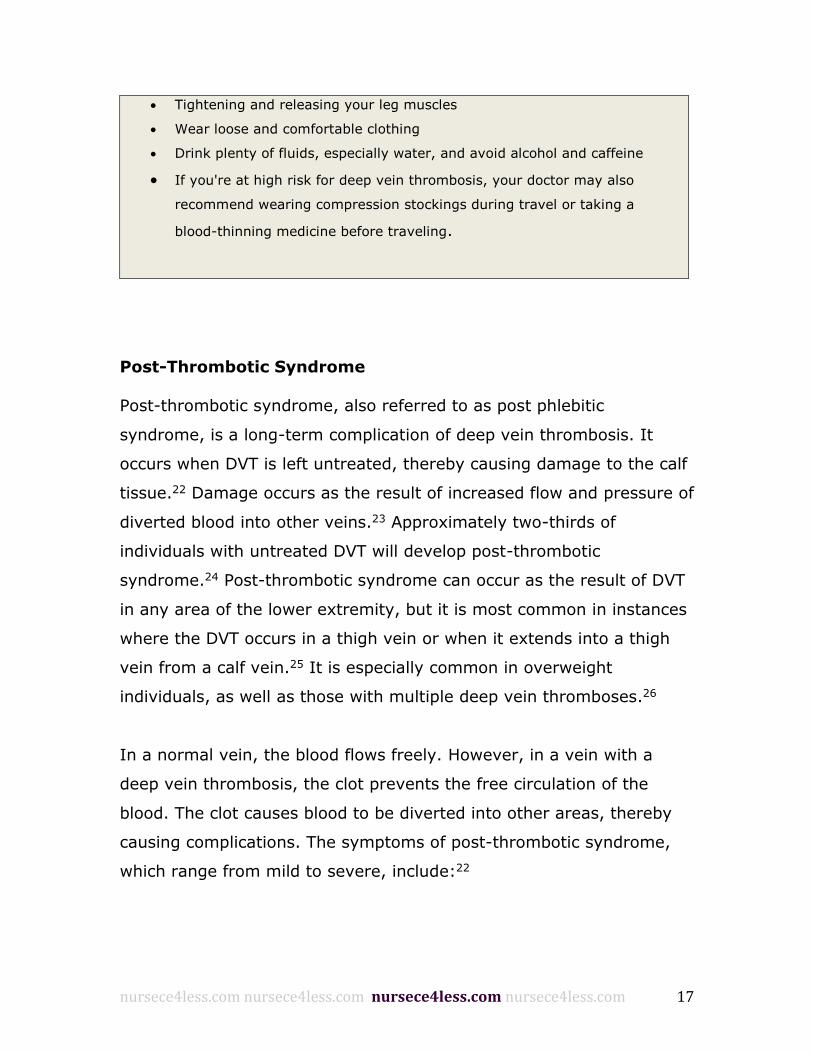
Tightening and releasing your leg muscles
Wear loose and comfortable clothing
Drink plenty of fluids, especially water, and avoid alcohol and caffeine
If you're at high risk for deep vein thrombosis, your doctor may also
recommend wearing compression stockings during travel or taking a
blood-thinning medicine before traveling.
Post-Thrombotic Syndrome
Post-thrombotic syndrome, also referred to as post phlebitic
syndrome, is a long-term complication of deep vein thrombosis. It
occurs when DVT is left untreated, thereby causing damage to the calf
tissue.22 Damage occurs as the result of increased flow and pressure of
diverted blood into other veins.23 Approximately two-thirds of
individuals with untreated DVT will develop post-thrombotic
syndrome.24 Post-thrombotic syndrome can occur as the result of DVT
in any area of the lower extremity, but it is most common in instances
where the DVT occurs in a thigh vein or when it extends into a thigh
vein from a calf vein.25 It is especially common in overweight
individuals, as well as those with multiple deep vein thromboses.26
In a normal vein, the blood flows freely. However, in a vein with a
deep vein thrombosis, the clot prevents the free circulation of the
blood. The clot causes blood to be diverted into other areas, thereby
causing complications. The symptoms of post-thrombotic syndrome,
which range from mild to severe, include:22
nursece4less.com nursece4less.com nursece4less.com nursece4less.com 18
Calf pain
Discomfort
Swelling of the legs (edema)
Leg pain
Skin discoloration
Rashes
Ulcer on the skin of the calf (only in severe instances)
Diagnosis
Post-thrombotic symptoms can be caused by a number of other
unrelated factors, so it is important to properly identify and diagnose
post-thrombotic syndrome before administering treatment.27 Typically,
the syndrome is diagnosed using the following diagnostic techniques:
Compression ultrasound:
Compression ultrasound is a simple and easy test to determine if
there is a clot in the veins. It is generally the first type of test
that a physician will use because it works best soon after
thrombosis has occurred.
Continuous-wave doppler ultrasound:
This test is a simple and fast way to detect whether the valves in
veins are working properly and the blood is flowing normally.
Color duplex scanning:
This test uses color scans to visualize blood vessels and uses
Doppler ultrasound to detect the direction of blood flow. It is a
nursece4less.com nursece4less.com nursece4less.com nursece4less.com 19
test that takes longer than doppler ultrasound but it can also
measure how much damage there is to the veins and exactly
where the damage is located.22
Treatment
When a patient is diagnosed with post-thrombotic syndrome, it is
important to begin treatment immediately to prevent further damage.
Treatment typically includes one or more of the following:28
wearing elastic compression stockings
exercising regularly
elevating leg(s) while resting
medication (aspirin or diuretics), rarely used
Heart Attack and Stroke
Heart attacks and strokes are not commonly associated with deep vein
thrombosis, as they occur as the result of clots in the arteries instead
of the veins.29 However, recent studies have shown that there is a
connection between the development of clots in deep veins and the
development of subsequent clots in arteries.30 When compared to
patients who have never had deep vein thrombosis or a pulmonary
embolism, those who had a history of the conditions showed an
increase in the incidence of heart attack and stroke.31 In fact, the risk
of heart attack or stroke in patients with deep vein thrombosis or
pulmonary embolism was thirty percent higher than it was in those
who had never had the condition.30
nursece4less.com nursece4less.com nursece4less.com nursece4less.com 20
In patients with deep vein thrombosis or pulmonary embolism, heart
attacks and strokes occur most frequently in the first year following an
incident of DVT or pulmonary embolism. Patients are two times more
likely to experience a stroke and three times more likely to experience
a heart attack in the year following a DVT.4 The risk decreases after
the first year, but still remains twenty to forty percent higher than it is
for an individual with no history of DVT or pulmonary embolism.1
DVT Prevention
Once a patient develops deep vein thrombosis, he or she is at risk of
developing additional complications. In addition, both deep vein
thrombosis and pulmonary embolism can be difficult to detect, as they
are often asymptomatic. Therefore, prevention is very important.
Most practitioners will focus on prevention in instances where there is
a risk of DVT or pulmonary embolism, using both pharmaceutical and
mechanical strategies. In instances where preventative strategies are
used, a patient’s risk of developing DVT or pulmonary embolism
decreases from eighty percent to less than twenty percent.25
Prevention is a multifaceted approach and includes both mechanical
and pharmaceutical strategies. In most instances, a number of
strategies will be used together. However, in some situations, a
patient may only require one strategy. Specific strategies will depend
on the level of risk and the type of situation. Some prevention
strategies will be used for a short duration, while other strategies may
extend for a number of months. Common prevention strategies
include:
nursece4less.com nursece4less.com nursece4less.com nursece4less.com 21
Anticoagulants
Movement
Compression stockings
In each situation, the provider will assess the patient and develop a
prevention plan that best meets the patient’s needs.
Anticoagulants
Anticoagulants are often used to prevent clot formation, especially
after surgery. However, while anticoagulants are effective at
preventing clot formation, they also increase the risk of bleeding,
which can be problematic in some patients.32 Therefore, each patient
is assessed before being administered anticoagulants. The following
table provides information regarding the three most common
anticoagulants:8
Anticoagulant Description
Aspirin
Aspirin is easy to administer, costs little, has few bleeding
complications, and does not need to be monitored.
However, it has not been proven more effective than other
agents and may not be advisable for all patients. Studies
have shown that aspirin has a greater protective effect for
men than for women.
Warfarin
(also called
Coumadin)
Warfarin is the most commonly used agent for hip and knee
replacement patients. Warfarin interferes with vitamin K
metabolism in the liver to prevent formation of certain
clotting factors. Because warfarin takes at least 36 hours to
start working, and four to five days to reach its maximum
effectiveness, it is usually started the day before surgery.
nursece4less.com nursece4less.com nursece4less.com nursece4less.com 22
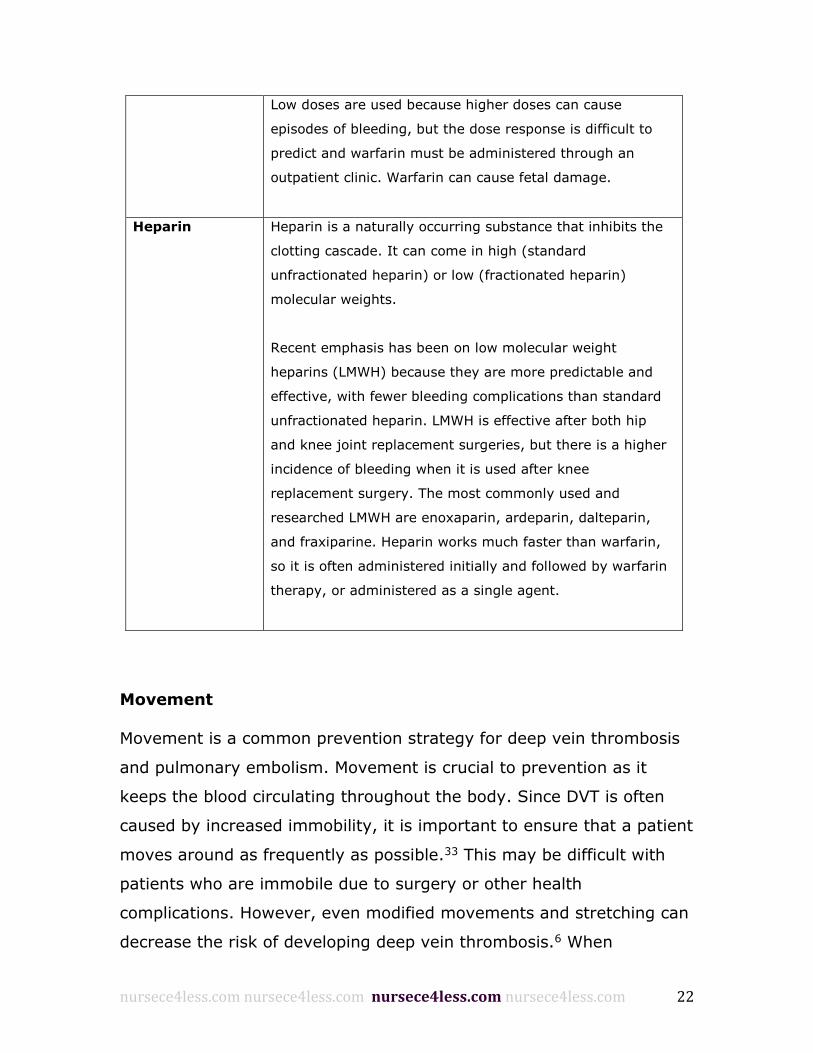
Low doses are used because higher doses can cause
episodes of bleeding, but the dose response is difficult to
predict and warfarin must be administered through an
outpatient clinic. Warfarin can cause fetal damage.
Heparin
Heparin is a naturally occurring substance that inhibits the
clotting cascade. It can come in high (standard
unfractionated heparin) or low (fractionated heparin)
molecular weights.
Recent emphasis has been on low molecular weight
heparins (LMWH) because they are more predictable and
effective, with fewer bleeding complications than standard
unfractionated heparin. LMWH is effective after both hip
and knee joint replacement surgeries, but there is a higher
incidence of bleeding when it is used after knee
replacement surgery. The most commonly used and
researched LMWH are enoxaparin, ardeparin, dalteparin,
and fraxiparine. Heparin works much faster than warfarin,
so it is often administered initially and followed by warfarin
therapy, or administered as a single agent.
Movement
Movement is a common prevention strategy for deep vein thrombosis
and pulmonary embolism. Movement is crucial to prevention as it
keeps the blood circulating throughout the body. Since DVT is often
caused by increased immobility, it is important to ensure that a patient
moves around as frequently as possible.33 This may be difficult with
patients who are immobile due to surgery or other health
complications. However, even modified movements and stretching can
decrease the risk of developing deep vein thrombosis.6 When
nursece4less.com nursece4less.com nursece4less.com nursece4less.com 23
movement is restricted, circulation is interrupted, thereby causing
DVT.34
Compression Stockings
In many instances, a patient will be prescribed compression stockings
as a preventative measure. This is especially true if the patient has a
history of deep vein thrombosis, as compression wear will reduce the
risk of recurrent DVT.35 Most patients are advised to wear compression
stockings for two or more years, or until the risk of developing a clot
has been eliminated.36
Compression stockings are specially made to provide different levels of
pressure at different regions of the leg, which helps move fluid in the
appropriate direction. The stockings use special elastic to apply various
amounts of pressure to the leg. They are available in different grades,
depending on the amount of pressure needed. However, while the
amount of pressure differs between grades, the stockings still use the
same pressure pattern. Stockings are tightest at the ankle, and the
pressure gradually decreases as the stocking moves up the calf. This
helps to move fluid up the leg and prevent it from collecting in
different areas.
Patients will require specially fitted compression stockings that are
intended to prevent the formation of a blood clot. In some instances,
the patient will require a prescription to purchase compression
stockings from a medical supply store. However, some compression
stockings can be purchased over the counter at a pharmacy.37
nursece4less.com nursece4less.com nursece4less.com nursece4less.com 24
There are two different types of compression stockings that are used
to treat or prevent deep vein thrombosis.37
1. To reduce the risk of deep leg vein thrombosis in people who are
at high risk. This kind of compression stocking is less expensive
than those used to help treat existing deep leg vein thrombosis.
2. To relieve symptoms associated with existing deep leg vein
thrombosis, especially swelling and pain, and prevent post-
thrombotic syndrome. This type of stocking may also help
prevent new clots from forming, although this is not its primary
function.
Treatment
Once deep vein thrombosis is identified, it is important to administer
treatment as soon as possible to prevent severe, long-term
complications from developing. The specific treatment will vary
depending on the location of the clot, the severity of the clot and any
other health conditions the patient may have. Typically, treatment will
involve a combination of different therapies specifically tailored to the
patient’s needs.
Some treatment will be administered in an outpatient capacity, while
other forms of treatment will require a short hospital stay with
constant monitoring.20 The primary goal of treatment is to prevent a
pulmonary embolism and reduce the risk of morbidity.5
nursece4less.com nursece4less.com nursece4less.com nursece4less.com 25
Anticoagulants
In addition to helping prevent DVT, anticoagulants are also effective in
treating deep vein thrombosis. Once a clot has formed, anticoagulants
are used to break it apart and increase blood flow.38 However, since
anticoagulants can also cause excessive bleeding, they should be used
with caution.39 The previous table on anticoagulants provides
information regarding the three most common anticoagulants.8
Thrombolytic Therapy
Thrombolytic therapy dissolves blood clots using medications that are
administered via catheter directly into the area where the clot has
formed.40 However, thrombolytic therapy is not used in mild cases of
deep vein thrombosis as the medication must be administered by a
team of trained physicians, nurses and technicians.41 Instead,
thrombolysis is used to treat large clots that are causing severe
symptoms and that pose a risk to the patient. Thrombolytic therapy is
also used to treat clots that cause massive swelling or occur in the
lungs.40 Thrombolytics increase the risk of bleeding, so they should
only be used in extreme situations after a patient has been assessed.42
Thrombolytics are administered via catheter in a catheterization
laboratory using specialized equipment. In most situations, the patient
will be sedated prior to the procedure.43 Once the patient is sedated,
the catheter is inserted into the area where the clot is located, and
thrombolytics are infused directly into the clot, thereby dissolving it.40
It can take a number of hours or a number of days for the clot to
dissolve completely.41 The patient is monitored using a genogram or
duplex ultrasound.40
nursece4less.com nursece4less.com nursece4less.com nursece4less.com 26
Compression
In many instances, compression stockings are used to treat deep vein
thrombosis. Compression stockings reduce the risk of developing post-
thrombotic syndrome, and they also help prevent the patient from
developing additional deep vein thrombosis.44 As mentioned earlier,
typically, treatment with compression stockings will continue for at
least two years to ensure that the deep vein thrombosis has been
resolved and to prevent further complications.36 Some patients may be
advised to wear compression stockings indefinitely after experiencing a
bout of deep vein thrombosis.33
While compression stockings are used for both prevention and
treatment of deep vein thrombosis, the type of stockings used for
treatment differs for each. As stated above, there are two types of
compression stockings that are used to treat or prevent deep vein
thrombosis:37
1. To reduce the risk of deep leg vein thrombosis in people who are
at high risk. This kind of compression stocking is less expensive
than those used to help treat existing deep leg vein thrombosis.
2. To relieve symptoms associated with existing deep leg vein
thrombosis, especially swelling and pain, and prevent post-
thrombotic syndrome. This type of stocking may also help
prevent new clots from forming, although this is not its primary
function.
Patients will require specially fitted compression stockings that are
intended to prevent the formation of a blood clot. Patients should not
nursece4less.com nursece4less.com nursece4less.com nursece4less.com 27
purchase compression stockings for DVT treatment over the counter at
a pharmacy, as accurate sizing and measurement is imperative when
using them for treatment.44 In most instances, patients are advised to
wear grade three strength stockings, as these have the best level of
compression for the reduction of deep vein thrombosis.45 However,
some patients will be unable to tolerate grade three stockings due to
the amount of squeezing force they produce. In these instances,
patients will be prescribed grade two stockings, which are not as
effective as the grade three stockings.44
Prognosis
The prognosis for deep vein thrombosis depends on the severity of the
DVT and the condition of the patient. In most instances, deep vein
thrombosis will resolve quickly and without any additional
complications.10 However, many patients will experience recurring
deep vein thrombosis once they have had an initial case of it.46
Recurring deep vein thrombosis is often the result of vein damage
caused by the initial incidence, but it can also be caused by secondary
health conditions or lifestyle habits.9
Deep vein thrombosis does not pose a risk of morbidity.30 However, if
DVT causes a pulmonary embolism, patients have a high risk of short-
term morbidity.16 Overall, pulmonary embolisms account for 300,000
deaths annually.19 Long-term morbidity is typically associated with
post phlebitic syndrome, which causes a number of complications for
the patient.23
nursece4less.com nursece4less.com nursece4less.com nursece4less.com 28
When treated, the prognosis for deep vein thrombosis is quite positive.
Most patients will experience no long-term complications and will be
able to resume normal activities and level of function quickly.47 Most
patients will recover completely, although the risk of recurrence will
always be a concern. This risk can be minimized if the patient wears
compression stockings. However, if a patient develops a pulmonary
embolism or post phlebitic syndrome, the prognosis is not as positive.
Post Phlebitic Syndrome
Post phlebitic syndrome, also referred to as post-thrombotic
syndrome, is a long-term complication of deep vein thrombosis. It
occurs when DVT is left untreated, thereby causing damage to the calf
tissue.22 Damage occurs as the result of increased flow and pressure of
diverted blood into other veins.23 Approximately two-thirds of
individuals with untreated DVT will develop post phlebitic syndrome.24
Post phlebitic syndrome can occur as the result of DVT in any area of
the lower extremity, but it is most common in instances where the
DVT occurs in a thigh vein or when it extends into a thigh vein from a
calf vein.25 It is especially common in overweight individuals, as well
as those with multiple deep vein thromboses.26
Post phlebitic syndrome typically develops within two years of an
episode of deep vein thrombosis and will range in severity. In extreme
instances, it will cause painful leg ulcers, which will require continuous
medical care.24 Patients with less severe cases will still experience lack
of function and long term mobility issues.23
The risk of developing post phlebitic syndrome increases if any of the
following factors are present:22
nursece4less.com nursece4less.com nursece4less.com nursece4less.com 29
older age
obesity
history of previous ipsilateral DVT
iliac-femoral location of the current thrombosis
failure to recover promptly from the acute symptoms
insufficient quality of oral anticoagulant therapy
Summary
Deep vein thrombosis is a blood clot that forms deep in the vein of the
lower extremity typically as the result of lack of movement or vein
injury. DVT can strike anyone regardless of age, physical fitness, or
other factors; however, it is especially common in patients who have
recently had surgery. It can cause long-term damage if not treated
properly and has an excellent prognosis when caught early and treated
aggressively. While the clot itself is not a concern, the potential
complications that it can cause are of concern. Some patients will
experience a pulmonary embolism if the clot breaks free and travels to
the blood vessels in the lung. When this occurs, the risk of morbidity is
high. In some instances, patients will develop post-thrombotic
syndrome, which impacts the patient’s mobility and level of basic
functioning.
Although there are a number of risk factors associated with deep vein
thrombosis, it can strike anyone regardless of age, physical fitness, or
other factors. However, DVT has an excellent prognosis when caught
early and treated aggressively. Additionally, there are a number of
strategies for reducing DVT risk. It is important for health care

nursece4less.com nursece4less.com nursece4less.com nursece4less.com 30
providers to familiarize themselves with these strategies in order to be
prepared to advise their patients on lifestyle adjustments and other
actions that can lower this risk.
Recent studies have shown that there is a connection between the
development of clots in deep veins and the development of subsequent
clots in arteries. When compared to patients who have never had deep
vein thrombosis or a pulmonary embolism, those who had a history of
the conditions showed an increase in the incidence of heart attack and
stroke. The risk of heart attack or stroke in patients with deep vein
thrombosis or pulmonary embolism has been found to be thirty
percent higher than it was in those who had never had the condition.
There are a number of strategies for reducing DVT risk. It is important
for health care providers to familiarize themselves with these
strategies in order to be prepared to advise their patients on lifestyle
adjustments and other actions that can lower this risk. Prophylaxis for
DVT can often prevent disease and avoid complications later on.
Nurses are able to educate colleagues and patients in health practice
settings where the risk of DVT is known to be at higher risk to occur.
The key to prevent DVT is to recognize who is at risk and to start
preventive measures.
Please take time to help NurseCe4Less.com course planners
evaluate the nursing knowledge needs met by completing the self-assessment of Knowledge Questions after reading the
article, and providing feedback in the online course evaluation.
Completing the study questions is optional and is NOT a course requirement.
nursece4less.com nursece4less.com nursece4less.com nursece4less.com 31
1. A pulmonary embolism occurs when a clot becomes
dislodged and travels to the ________.
a. Respiratory system
b. Lung
c. Digestive system
d. Immune system
2. Compression stockings that will be used to treat DVT
should be a grade ___________.
a. 1
b. 2
c. 3
d. 4
3. This is the procedure that injects medication directly into
the blood clot via catheter to dissolve the clot.
a. Angioplasty
b. Thrombolytic Therapy
c. Bypass
d. Laparoscopy
4. Which of the following is NOT a risk factor for DVT?
a. Smoking
b. Strength Training
c. Pregnancy
d. Age
nursece4less.com nursece4less.com nursece4less.com nursece4less.com 32
5. Which of the following is a long-term complication of DVT
that causes damage to the vein?
a. Pulmonary Embolism
b. Heart Attack
c. Post-Thrombotic Syndrome
d. Blockage
CORRECT ANSWERS:
1. b
2. c
3. b
4. b
5. c
nursece4less.com nursece4less.com nursece4less.com nursece4less.com 33
References Section
The reference section of in-text citations include published works
intended as helpful material for further reading. Unpublished works
and personal communications are not included in this section, although
may appear within the study text.
1. Deep Vein Thrombosis: Risks and Diagnosis [Internet]. Available
from: http://www.williampoh.com/Documents/AFPDVT0710.pdf
2. Kesieme E, Kesieme C, Jebbin N, Irekpita E, Dongo A. Deep vein
thrombosis: a clinical review. J. Blood Med. 2011;2:59–69.
3. Deep Vein Thrombosis [Internet]. Available from:
http://vasculardisease.org/flyers/deep-vein-thrombosis-flyer.pdf
4. Bandyopadhyay G, Roy SB, Haldar S, Bhattacharya R. Deep vein
thrombosis. J. Indian Med. Assoc. 2010;108:866–7.
5. Lottenberg R, Soucie JM, Grant AM, Atrash HK, Raskob GE,
Silverstein R, et al. Surveillance for Deep Vein Thrombosis and
Pulmonary Embolism. Am. J. Prev. Med. 2010. p. S502–S509.
6. Eikelboom JW, Karthikeyan G, Fagel N, Hirsh J. American
Association of Orthopedic Surgeons and American College of
Chest Physicians guidelines for venous thromboembolism
prevention in hip and knee arthroplasty differ: what are the
implications for clinicians and patients? Chest. American College
of Chest Physicians; 2009 Feb 1;135(2):513–20.
7. Yamaki T, Hamahata A, Soejima K, Kono T, Nozaki M, Sakurai H.
Factors predicting development of post-thrombotic syndrome in
patients with a first episode of deep vein thrombosis: preliminary
report. Eur. J. Vasc. Endovasc. Surg. 2011;41:126–33.
nursece4less.com nursece4less.com nursece4less.com nursece4less.com 34
8. Deep Vein Thrombosis -OrthoInfo - AAOS [Internet]. Available
from: http://orthoinfo.aaos.org/topic.cfm?topic=a00219
9. Eichinger S, Heinze G, Jandeck LM, Kyrle PA. Risk assessment of
recurrence in patients with unprovoked deep vein thrombosis or
pulmonary embolism: the Vienna prediction model. Circulation.
2010 Apr 13;121(14):1630–6.
10. Yamaki T, Nozaki M, Sakurai H, Takeuchi M, Soejima K, Kono T.
Presence of Lower Limb Deep Vein Thrombosis and Prognosis in
Patients with Symptomatic Pulmonary Embolism: Preliminary
Report. Eur. J. Vasc. Endovasc. Surg. 2009;37(2):225–31.
11. Halvorson JJ, Anz A, Langfitt M, Deonanan JK, Scott A, Teasdall
RD, et al. Vascular injury associated with extremity trauma:
initial diagnosis and management. J. Am. Acad. Orthop. Surg.
American Academy of Orthopaedic Surgeons; 2011 Aug
1;19(8):495–504.
12. Deroo S, Deatrick KB, Henke PK. The vessel wall: A forgotten
player in post thrombotic syndrome. Thromb. Haemost.
2010;104:681–92.
13. Tovey C, Wyatt S. Diagnosis, investigation, and management of
deep vein thrombosis. BMJ Br. Med. J. 2003;326:1180–4.
14. Scarvelis D, Wells PS. Diagnosis and treatment of deep-vein
thrombosis. CMAJ. 2006 Oct 24;175(9):1087–92.
15. Wells PS, Owen C, Doucette S, Fergusson D, Tran H. Does this
patient have deep vein thrombosis? JAMA. American Medical
Association; 2006 Jan 11;295(2):199–207.
16. Pulmonary Embolism [Internet]. Available from:
http://medicalcenter.osu.edu/patientcare/healthcare_services/lun
g_diseases/lung/embolism/Pages/index.aspx
nursece4less.com nursece4less.com nursece4less.com nursece4less.com 35
17. Acute Pulmonary Embolism — NEJM [Internet]. Available from:
http://www.nejm.org/doi/full/10.1056/NEJMra0907731
18. Headley CM, Melander S. When it may be a pulmonary embolism.
Nephrol. Nurs. J. 2011;38:127–37.
19. Humenberger M, Lang IM. Pulmonary embolism.
Hamostaseologie. 2008;28:40–3.
20. Brenner B, Hoffman R. Emerging options in the treatment of deep
vein thrombosis and pulmonary embolism. Blood Rev.
2011;25:215–21.
21. (OSG) O of the SG. Fact Sheet: Deep Vein Thrombosis and
Pulmonary Embolism.
22. The facts on post-thrombotic syndrome [Internet]. Available
from: http://www.inate.org/en/1/2/6/23/default.aspx
23. Brenner B, Greer IA, Kahn SR. The post thrombotic syndrome.
Thromb. Res. 2011;127:S89–S92.
24. Galanaud JP, Holcroft CA, Rodger MA, Kovacs MJ, Betancourt MT,
Wells PS, et al. Predictors of post-thrombotic syndrome in a
population with a first deep vein thrombosis and no primary
venous insufficiency. J. Thromb. Haemost. 2013 Mar;11(3):474–
80.
25. Guanella R, Kahn SR. Post-thrombotic syndrome: current
prevention and management strategies. Expert Rev. Cardiovasc.
Ther. 2012;10:1555–66.
26. Elman EE, Kahn SR. The post-thrombotic syndrome after upper
extremity deep venous thrombosis in adults: A systematic
review. Thromb. Res. 2006;117(6):609–14.
27. Roumen-Klappe EM, Janssen MCH, Van Rossum J, Holewijn S,
Van Bokhoven MMJA, Kaasjager K, et al. Inflammation in deep
vein thrombosis and the development of post-thrombotic
nursece4less.com nursece4less.com nursece4less.com nursece4less.com 36
syndrome: a prospective study. J. Thromb. Haemost. 2009
Apr;7(4):582–7.
28. Morling JR, Yeoh SE, Kolbach DN. Rutosides for treatment of
post-thrombotic syndrome. Cochrane Database Syst. Rev.
2013;4:CD005625.
29. Rathbun S. Cardiology patient pages. The Surgeon General’s call
to action to prevent deep vein thrombosis and pulmonary
embolism. Circulation. 2009 Apr 21;119(15):e480–2.
30. Goldhaber SZ, Bounameaux H. Pulmonary embolism and deep
vein thrombosis. Lancet. 2012 May 12;379(9828):1835–46.
31. Naccarato M, Chiodo Grandi F, Dennis M, Sandercock PA. Physical
methods for preventing deep vein thrombosis in stroke. Cochrane
database Syst. Rev. 2010 Jan;(8):CD001922.
32. Franchini M, Mannucci PM. A new era for anticoagulants. Eur. J.
Intern. Med. 2009;20:562–8.
33. Galanaud J-P, Laroche J-P, Righini M. The history and historical
treatments of deep vein thrombosis. J. Thromb. Haemost. 2013.
p. 402–11.
34. Friedman RJ, Gallus AS, Cushner FD, FitzGerald G, Jr FAA,
Investigators for the GOR. Physician compliance with guidelines
for deep-vein thrombosis prevention in total hip and knee
arthroplasty. Informa UK Ltd UK; 2007 Nov 19;
35. MJ C, S H, E J, A E, M K. Compression stockings for preventing
deep vein thrombosis (DVT) in airline passengers. John Wiley and
Sons, Ltd. for The Cochrane Collaboration; 2010.
36. Kahn SR, Shbaklo H, Lamping DL, Holcroft CA, Shrier I, Miron MJ,
et al. Determinants of health-related quality of life during the 2
years following deep vein thrombosis. J. Thromb. Haemost. 2008
Jul;6(7):1105–12.
nursece4less.com nursece4less.com nursece4less.com nursece4less.com 37
37. Sachdeva A, Dalton M, Amaragiri S V, Lees T. Elastic compression
stockings for prevention of deep vein thrombosis. Cochrane
database Syst. Rev. 2010 Jan;(7):CD001484.
38. Mavrakanas T, Bounameaux H. The potential role of new oral
anticoagulants in the prevention and treatment of
thromboembolism. Pharmacol. Ther. 2011;130(1):46–58.
39. Gross PL, Weitz JI. New anticoagulants for treatment of venous
thromboembolism. Arterioscler. Thromb. Vasc. Biol. 2008 Mar
1;28(3):380–6.
40. Schermerhorn M, Mewissen MW. Thrombolysis for Lower-
Extremity Deep Vein Thrombosis. Semin. Vasc. Surg.
2010;23(4):228–34.
41. L W, MP A. Thrombolysis for treatment of acute deep vein
thrombosis. John Wiley and Sons, Ltd. for The Cochrane
Collaboration; 2010.
42. Gogalniceanu P, Johnston CJC, Khalid U, Holt PJE, Hincliffe R,
Loftus IM, et al. Indications for Thrombolysis in Deep Venous
Thrombosis. Eur. J. Vasc. Endovasc. Surg. 2009;38(2):192–8.
43. Comerota AJ. Thrombolysis for deep venous thrombosis. J. Vasc.
Surg. 2012;55(2):607–11.
44. Aschwanden M, Jeanneret C, Koller MT, Thalhammer C, Bucher
HC, Jaeger KA. Effect of prolonged treatment with compression
stockings to prevent post-thrombotic sequelae: A randomized
controlled trial. J. Vasc. Surg. 2008;47(5):1015–21.
45. Kahn SR. The post-thrombotic syndrome. Hematology Am. Soc.
Hematol. Educ. Program. 2010 Jan 1;2010(1):216–20.
46. Jiménez D, Aujesky D, Díaz G, Monreal M, Otero R, Martí D, et al.
Prognostic Significance of Deep Vein Thrombosis in Patients
nursece4less.com nursece4less.com nursece4less.com nursece4less.com 38
Presenting with Acute Symptomatic Pulmonary Embolism.
American Thoracic Society; 2012 Dec 20;
47. Spencer FA, Gore JM, Lessard D, Douketis JD, Emery C, Goldberg
RJ. Patient outcomes after deep vein thrombosis and pulmonary
embolism: the Worcester Venous Thromboembolism Study. Arch.
Intern. Med. American Medical Association; 2008 Feb
25;168(4):425–30.
nursece4less.com nursece4less.com nursece4less.com nursece4less.com 39
The information presented in this course is intended solely for the use of healthcare
professionals taking this course, for credit, from NurseCe4Less.com.
The information is designed to assist healthcare professionals, including nurses, in
addressing issues associated with healthcare.
The information provided in this course is general in nature, and is not designed to
address any specific situation. This publication in no way absolves facilities of their
responsibility for the appropriate orientation of healthcare professionals.
Hospitals or other organizations using this publication as a part of their own
orientation processes should review the contents of this publication to ensure
accuracy and compliance before using this publication.
Hospitals and facilities that use this publication agree to defend and indemnify, and
shall hold NurseCe4Less.com, including its parent(s), subsidiaries, affiliates,
officers/directors, and employees from liability resulting from the use of this
publication.
The contents of this publication may not be reproduced without written permission
from NurseCe4Less.com.