Embed Size (px)
Citation preview
1
EBV connection to adenotonsillar hypertrophy
Ieva Grīnberga
Mentor: Dr. Jānis Sokolovs
2
EBV also known as the human herpes virus 4, is a member of the herpes
virus family
Prevalent in as much as 90% of the worlds population
The Epstein–Barr virus was named after Michael Anthony Epstein and
Yvonne Barr
Yvonne Barr was a virologist born on 11 March 1932, died at the age of
83 last February
Graduated from University of London in 1966 with a Ph.D.
In 1964 published a study on the existance of the EBV in Lancet
Epstein- Barr virus
3
Extreme fatigue
Fever
Sore throat
Head and body aches
Swollen lymph nodes in the neck and armpits
Swollen liver or spleen or both
Rash
Symptoms
4
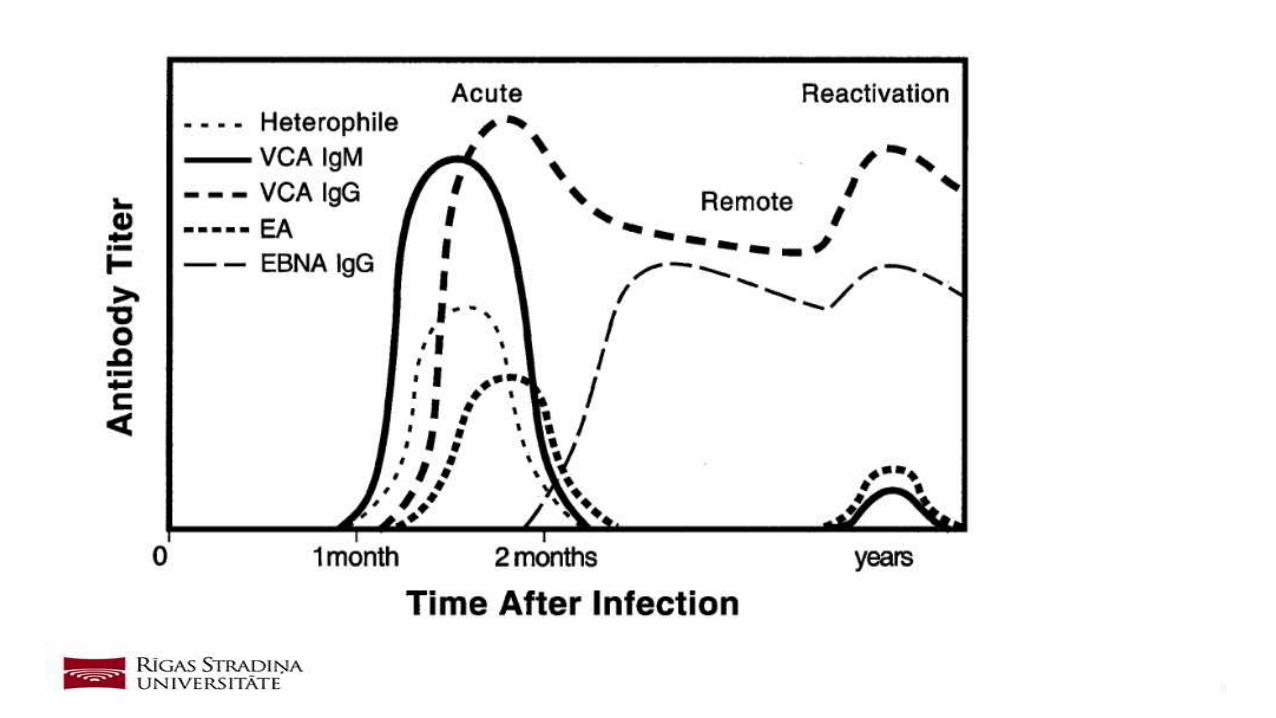
Viral capsid antigen (VCA) Anti-VCA IgM appears early in EBV infection
and usually disappears within 4 to 6 weeks. Anti-VCA IgG appears in the
acute phase of EBV infection, peaks at 2 to 4 weeks after onset, declines
slightly then persists for the rest of a person’s life.
Early antigen (EA)
Anti-EA IgG appears in the acute phase of illness and generally falls to
undetectable levels after 3 to 6 months. In many people, detection of
antibody to EA is a sign of active infection. However, 20% of healthy
people may have antibodies against EA for years.
Laboratory testing [1]
5
EBV nuclear antigen (EBNA)
Antibody to EBNA, determined by the standard immunofluorescent test,
is not seen in the acute phase of EBV infection but slowly appears 2 to 4
months after onset of symptoms and persists for the rest of a person’s
life. Other EBNA enzyme immunoassays may report false positive
results.
Laboratory testing [2]
6
Susceptibility to infection
People are considered susceptible to EBV infection if they do not have
antibodies to the VCA.
Primary (new or recent) infection
People are considered to have a primary EBV infection if they have anti-
VCA IgM but do not have antibody to EBNA. Other results that strongly
suggest a primary infection are a high or rising level of anti-VCA IgG and
no antibody to EBNA after at least 4 weeks of illness. Resolution of the
illness may occur before the diagnostic antibody levels appear. In rare
cases, people with active EBV infections may not have detectable EBV-
specific antibodies.
Result interpretation [1]
7
Past infection
The presence of antibodies to both VCA and EBNA suggests past
infection (from several months to years earlier). Since over 90% of adults
have been infected with EBV, most adults will show antibodies to EBV
from infection years earlier. High or elevated antibody levels may be
present for years and are not diagnostic of recent infection.
Result interpretation [2]
8
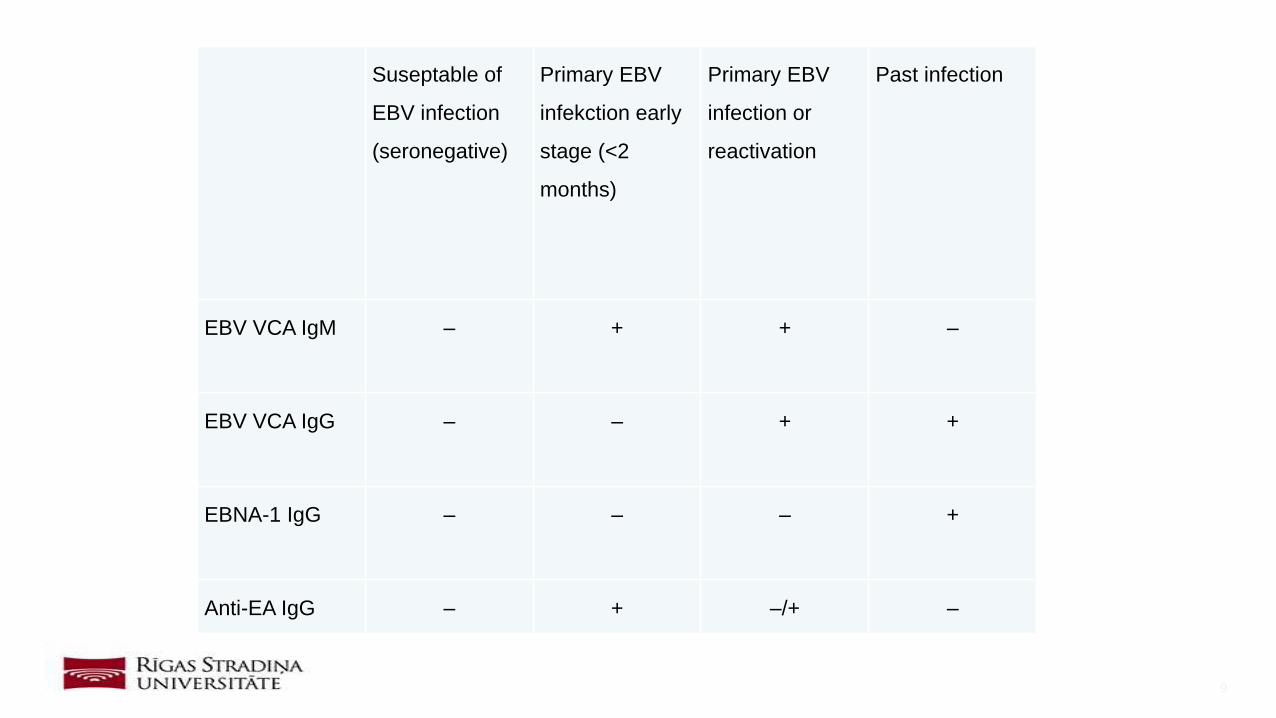
9
Suseptable of
EBV infection
(seronegative)
Primary EBV
infekction early
stage (<2
months)
Primary EBV
infection or
reactivation
Past infection
EBV VCA IgM – + + –
EBV VCA IgG – – + +
EBNA-1 IgG – – – +
Anti-EA IgG – + –/+ –
10
Voice changes: As a result of swollen tissue near the vocal chords, the
voice may be altered slightly.
Difficulty swallowing: The enlarged tissue of the tonsils can become
obstructive and make swallowing certain foods difficult.
Loss of appetite: When swallowing food is difficult or painful, many
children eat less and lose their appetite.
Halitosis: Due to infections of the tonsils, bad breath often affects children
with tonsil hypertrophy.
Tonsillar hypertrophy
11
Obstructive sleep apnea: In severe cases of tonsil hypertrophy, sleep
apnea, a condition indicated by pauses in breathing during sleep, can
occur. This is due to blocked airways. Sleep apnea is a serious condition
that can potentially cause pulmonary hypertension and hypertrophy of the
right side of the heart.
Frequent ear infections: The enlarged tonsils can block the Eustachian
tubes and impede drainage. This can result in fluid build up behind the
eardrum and ear infections.
Chronic Sinusitis: Hypertrophic tonsils and surrounding tissue can
prevent proper drainage from the sinus cavities. The mucous becomes
trapped and infections can develop. Symptoms such as congestion,
pressure and fatigue are common with sinusitis.
12
13
Mouth breathing: As a result of blocked nasal airways, children with
adenoid hypertrophy are often forced to breath through their mouths. If
mouth breathing occurs for a prolonged period of time, orthodontic issues
can arise.
Runny nose: Because mucous cannot drain properly through the back of
the nasal cavity, mucous and secretions exit through the nostrils.
Snoring and sleep apnea: The blocked airways caused by the enlarged
adenoid tissue can interfere with breathing during sleep.
Snoring: Hypertrophic tonsils can obstruct the airways making breathing
during sleep more difficult.
Adenoid hypertrophy
14
Chronic sinusitis: When enlarged adenoids block the nasal passages, the
sinus cavities cannot drain properly. The buildup of mucous leads to
inflammation of the lining and often infections.
Eustachian tube dysfunction: When enlarged adenoids prevent proper
drainage from the Eustachian tubes, fluid collects behind the eardrum.
Adenoid hypertrophy
15
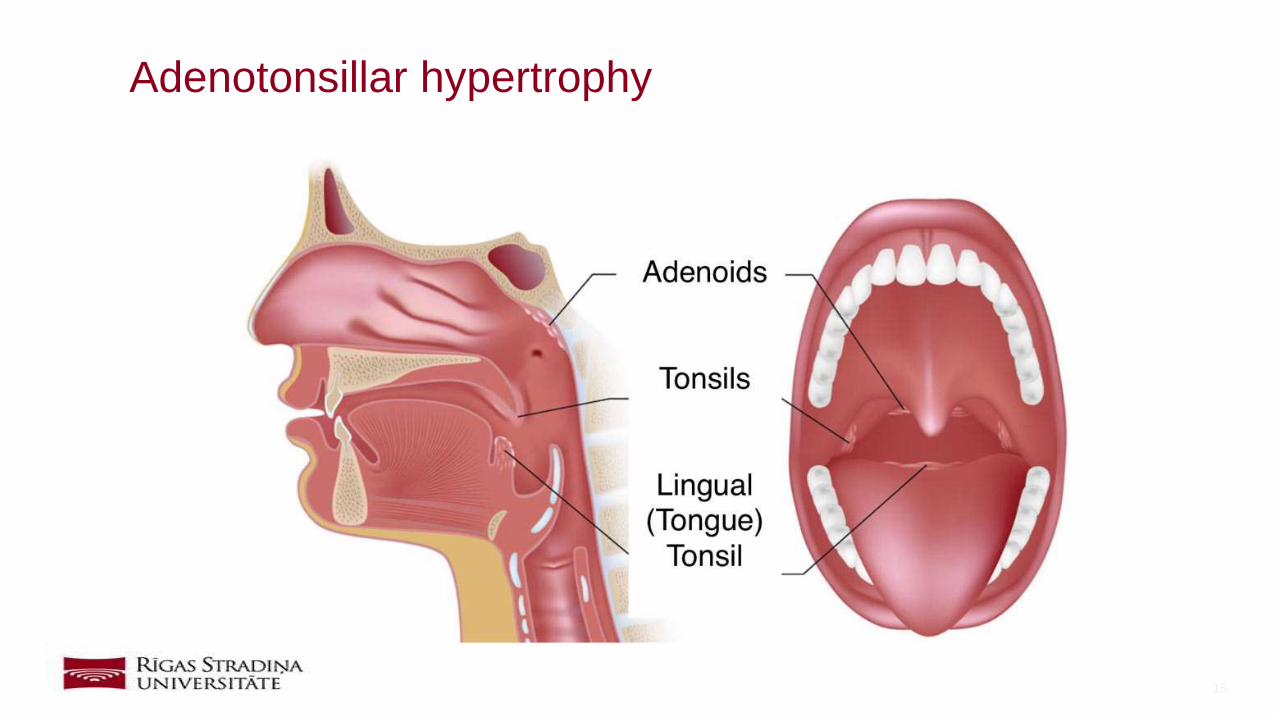
Adenotonsillar hypertrophy
16
The exact cause of tonsil hypertrophy is not always clear, but the
enlargement is typically related to tonsillitis or infection of the tonsils and
surrounding tissue.
Because of the nature of EBV, there have been many discussions about
the connection between adenotonsillar hypertrophy and EBV
Adenotonsillar hypertrophy
17
The aim of this study is to determine the connection between
adenotonsillar hypertrophy and EBV
104 patients were included in this study
Laboratory and objective clinical data was analyzed
Materials and methods
18
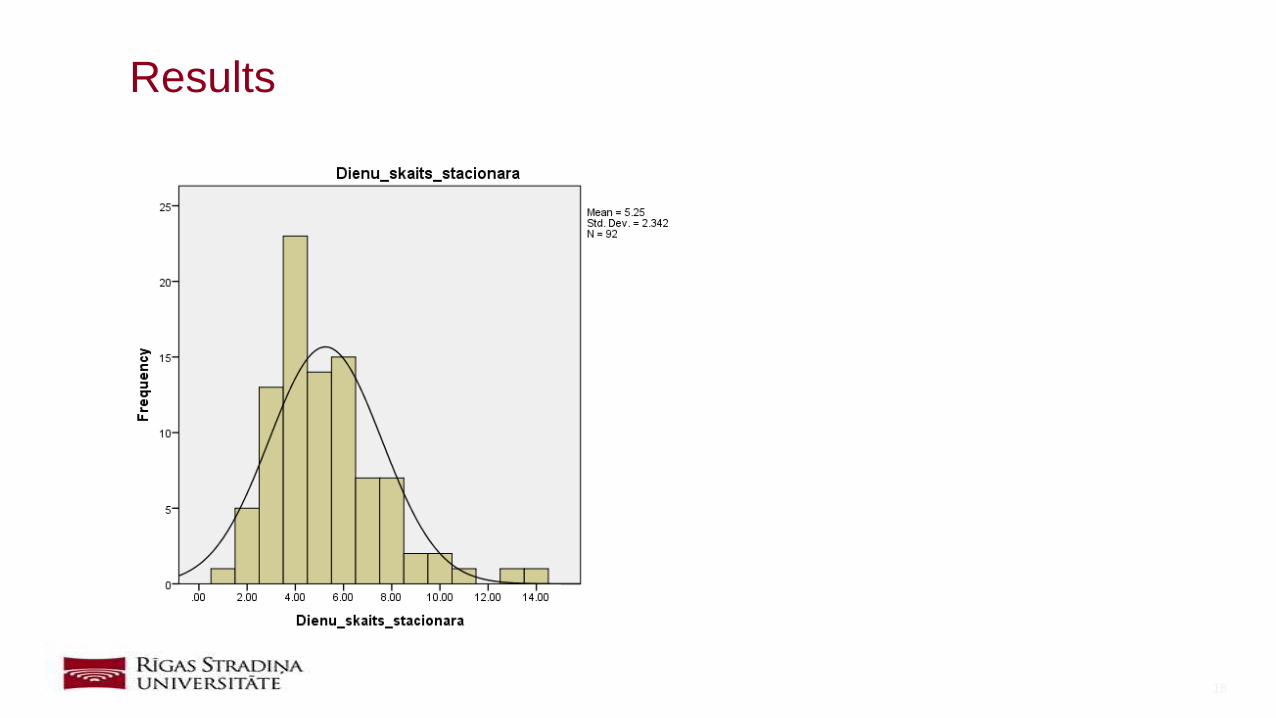
Results
19
20
21
22
23
24
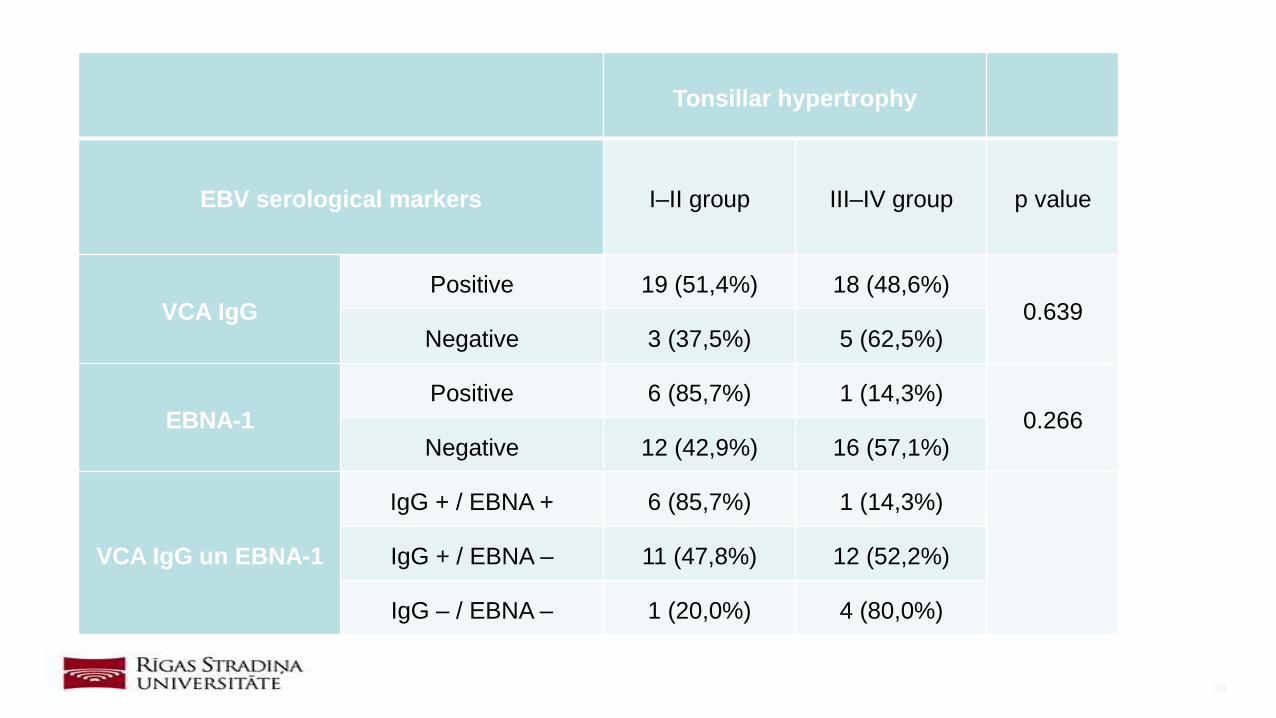
Tonsillar hypertrophy
EBV serological markers I–II group III–IV group p value
VCA IgGPositive 19 (51,4%) 18 (48,6%)
0.639Negative 3 (37,5%) 5 (62,5%)
EBNA-1 Positive 6 (85,7%) 1 (14,3%)
0.266Negative 12 (42,9%) 16 (57,1%)
VCA IgG un EBNA-1
IgG + / EBNA + 6 (85,7%) 1 (14,3%)
IgG + / EBNA – 11 (47,8%) 12 (52,2%)
IgG – / EBNA – 1 (20,0%) 4 (80,0%)
25
26
27
28
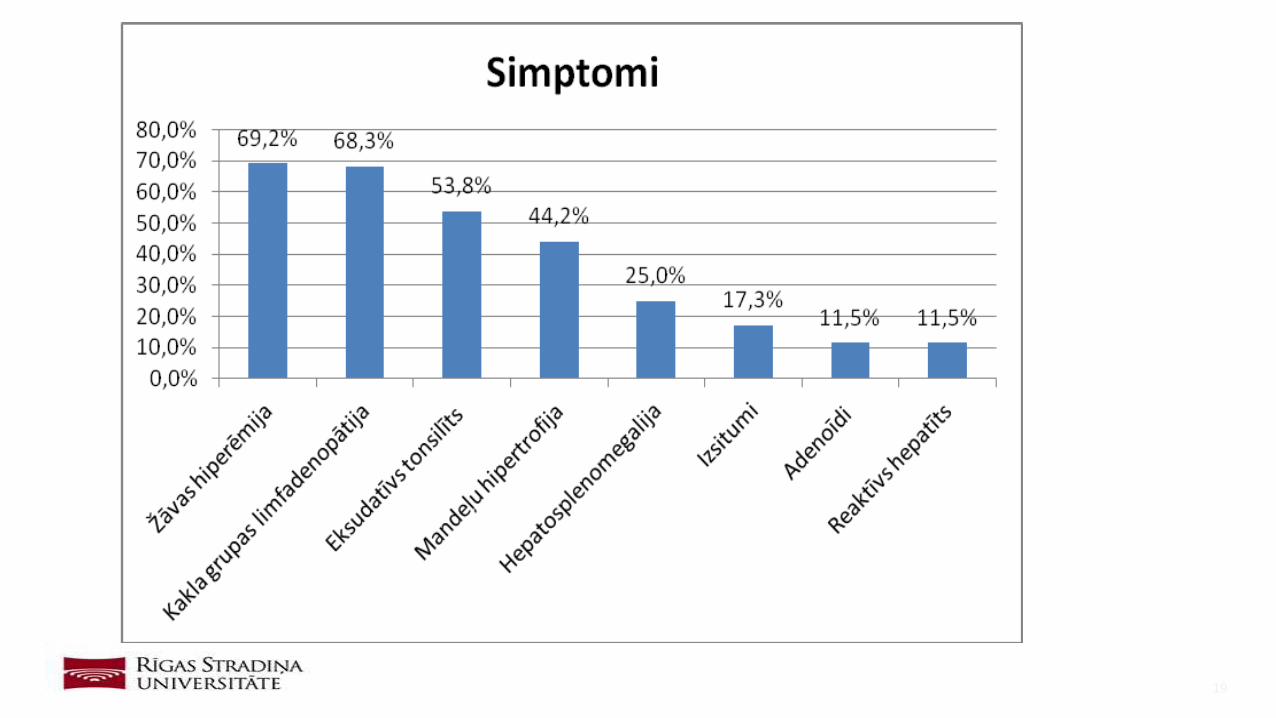
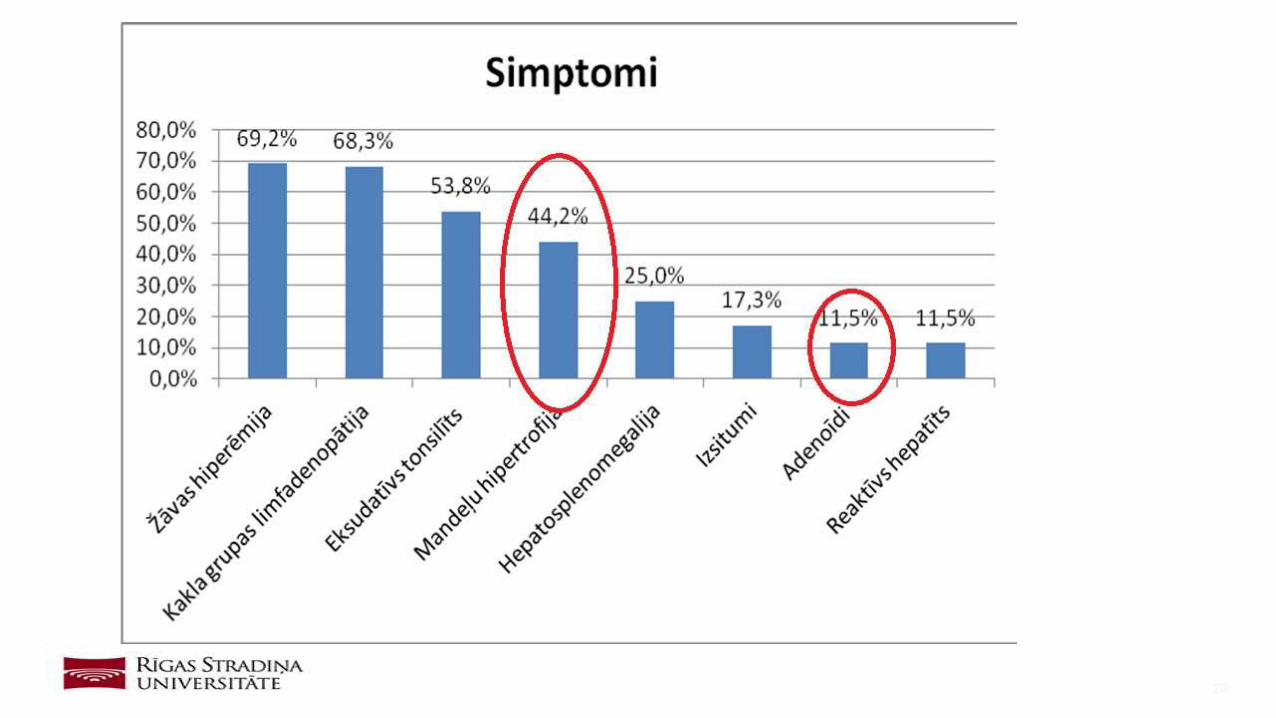
Most commonly diagnosed symptom of EBV infection was throat
hyperaemia
Tonsillar hypertrophy was prevalent in 44,2% of the cases, adenoids
were prevalent in 11,5% cases
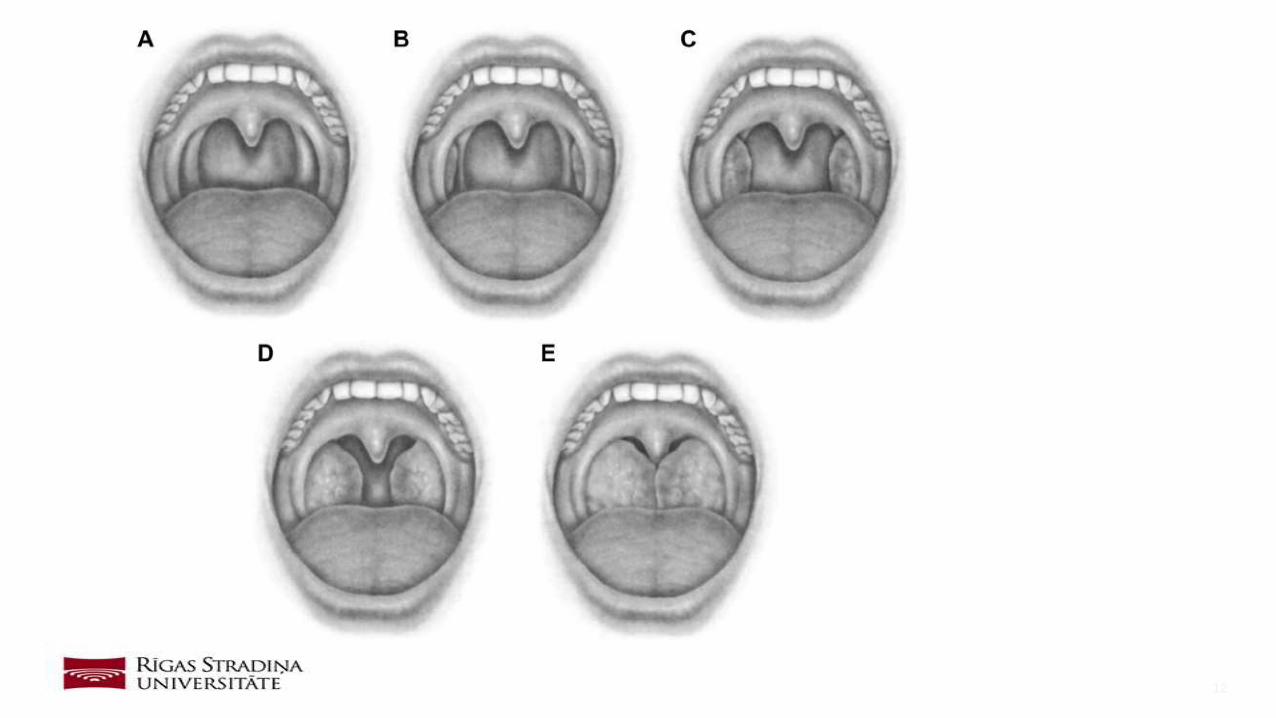
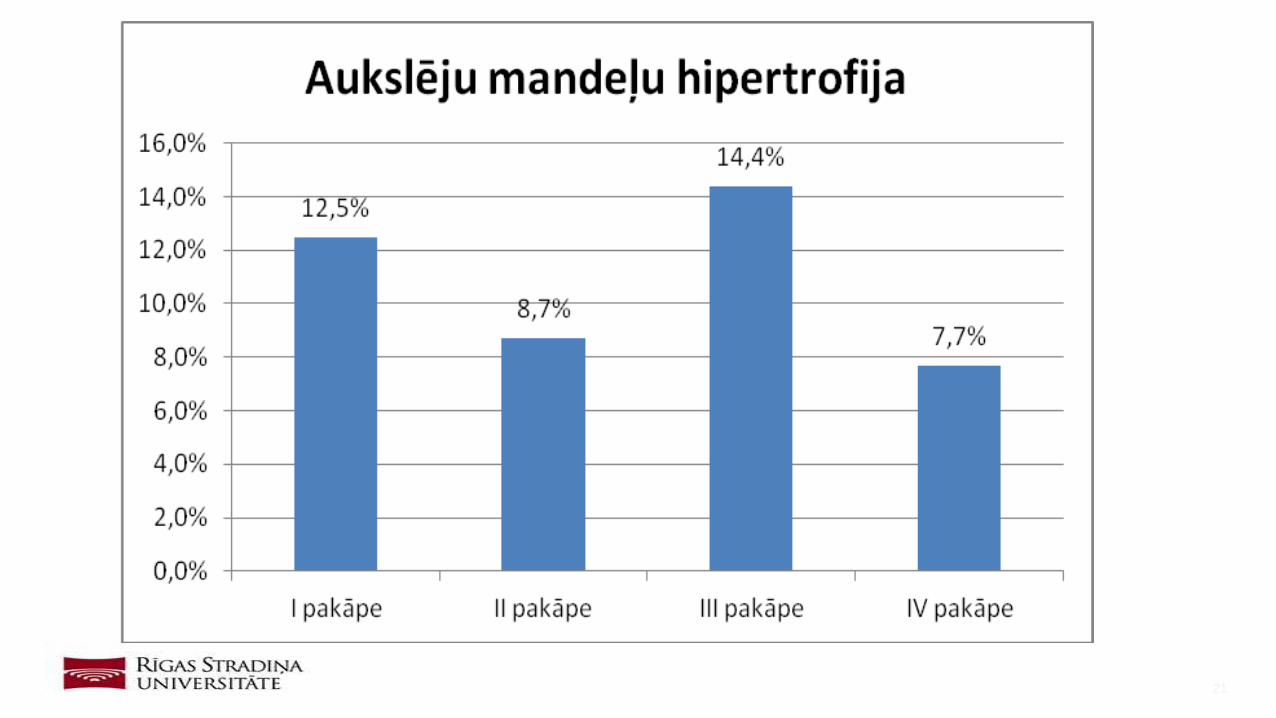
The most common tonsillar hypertrophy grade was III
Patients with VCA IgG and EBNA-1 positive serology had mostly grade I-
II tonsillar hypertrophy
Patients with VCA IgG and EBNA-1 negative serology had mostly grade
III- IV tonsillar hypertrophy
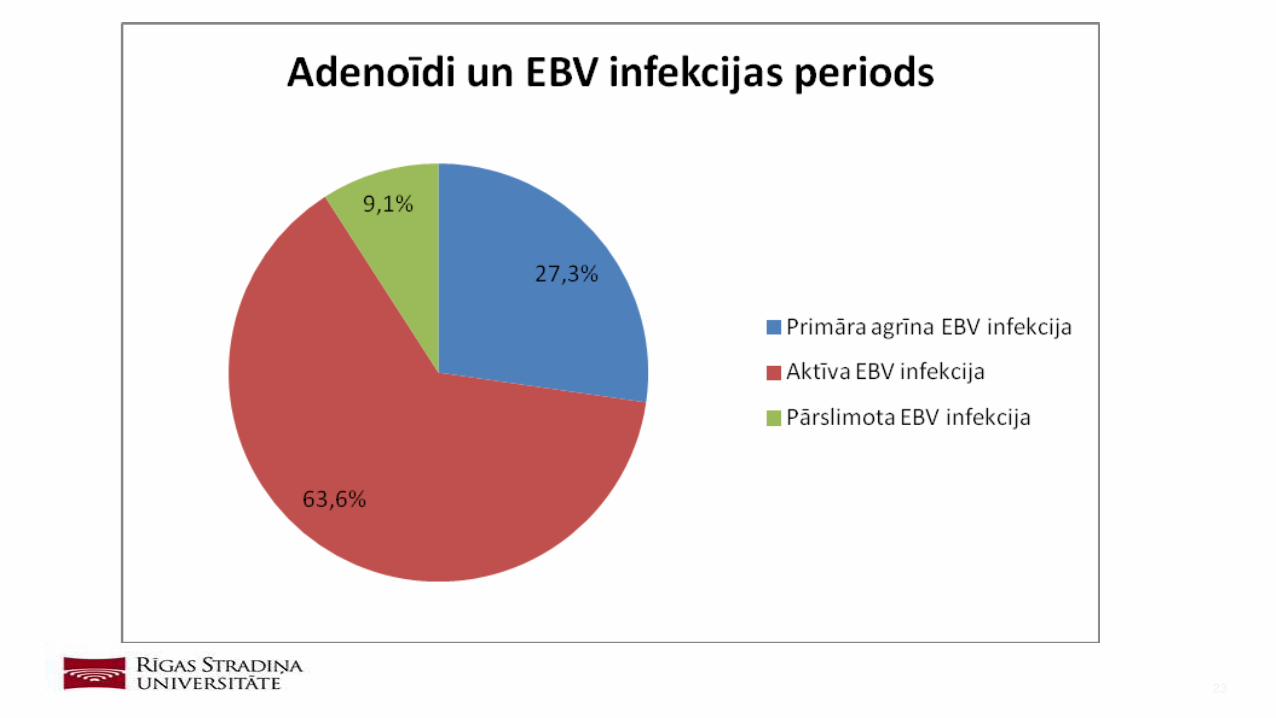
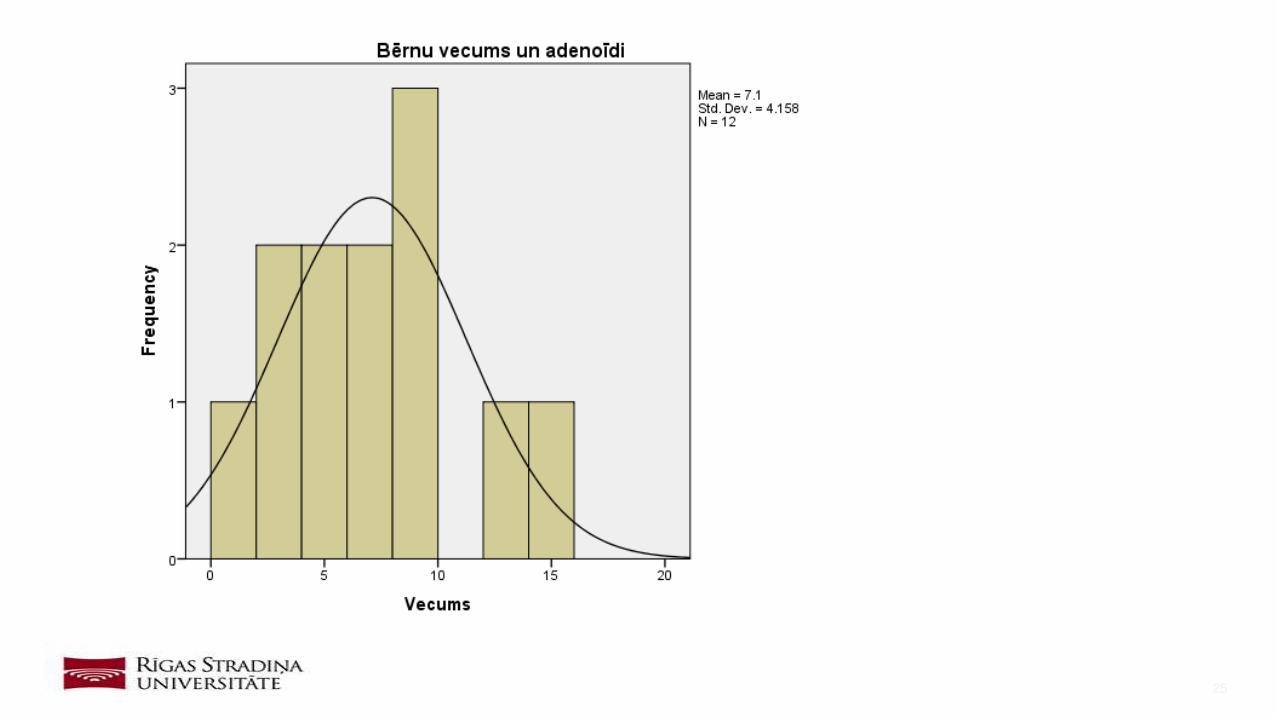
Average age of children with adenoids was 7
Conclusions
29
Akcay A, Kara CO, Dagdeviren E, Zencir M. Variation in tonsil size in 4- to 17-year-old schoolchildren. The Journal of Otolaryngology 2006,N 4,vol. 35, p. 270–4.
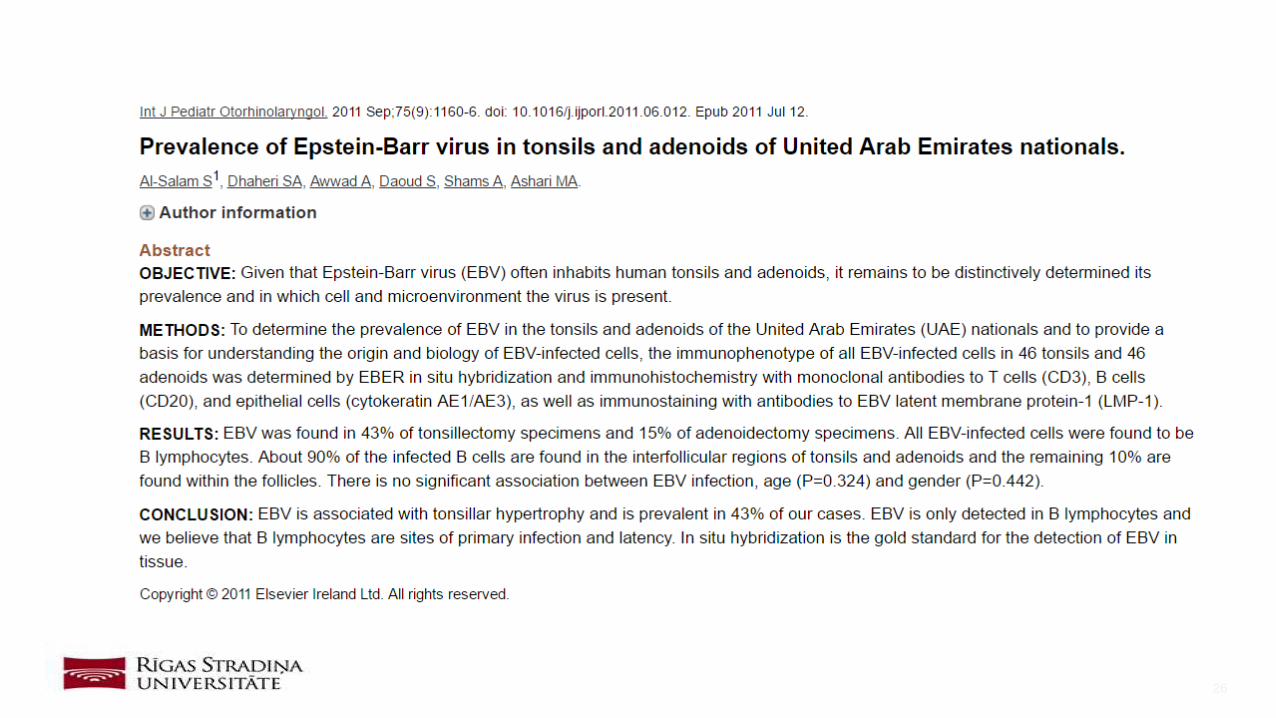
Al-Salam S, Dhaheri S Al, Awwad A, Daoud S, Shams A, Ashari M Al. Prevalence of epstein-barr virus in tonsils and adenoids of united arab emirates nationals. International
Journal of Pediatric Otorhinolaryngology 2011,N 9,vol. 75, p. 1160–6.
Baugh RF, Archer SM, Mitchell RB, Rosenfeld RM, Amin R, Burns JJ, et al. Clinical practice guideline: tonsillectomy in children. Otolaryngology--Head and Neck Surgery : Official
Journal of American Academy of Otolaryngology-Head and Neck Surgery 2011,N 1 Suppl,vol. 144, p. S1-30.
Berger C, Hug M, Gysin C, Molinari L, Frei M, Bossart W, et al. Distribution patterns of beta- and gamma-herpesviruses within Waldeyer’s ring organs. J Med Virol 2007,N 8,vol.
79, p. 1147–52.
Blitzer Andrew, Schwartz Jerome, Song Phillip YM. Oxford Handbook of Otolaryngology. New York: Oxford University Press; 2008.
Brodsky L. Modern assessment of tonsils and adenoids. Pediatric Clinics of North America 1989,N 6,vol. 36, p. 1551–69.
Brooks GF, Carroll KC, Butel JS, Morse SA, Mietzner TA. Jawetz, Melnick & Adelberg’s Medical Microbiology, 26th Edition. 2013.
Capdevila OS, Kheirandish-Gozal L, Dayyat E, Gozal D. Pediatric obstructive sleep apnea: complications, management, and long-term outcomes. Proceedings of the American
Thoracic Society 2008,N 2,vol. 5, p. 274.
Epstein MA, Henle G, Achong BG, Barr YM. Morphological and Biological Studies on a Virus in Cultured Lymphoblasts From Burkitt’S Lymphoma. The Journal of Experimental
Medicine 1965,N 11,vol. 121, p. 761–70.
Fields BN, Knipe DM, Howley PM. Fields Virology, 5th Edition. vol. 2. 2007.
Veres [1]
30
Gulley ML. Molecular diagnosis of Epstein-Barr virus-related diseases. The Journal of Molecular Diagnostics : JMD 2001,N 1,vol. 3, p. 1–10.
Hallberg AC. Tonsillar Disorders: Etiology, Diagnosis and Treatment. New York: Nova Science Publishers, Inc.; 2011.
Havas T, Lowinger D. Obstructive adenoid tissue: an indication for powered-shaver adenoidectomy. Archives of Otolaryngology--Head & Neck Surgery 2002,N 7,vol. 128, p. 789–
91.
Jurijs Markovs. Medicīniskā histoloģija I. Izdevniecība “Eve”; 2003.
Mbata G, Chukwuka J. Obstructive Sleep Apnea Hypopnea Syndrome. Annals of Medical and Health Sciences Research 2012,N 1,vol. 2, p. 74–7.
De Paschale M, Clerici P. Serological diagnosis of Epstein-Barr virus infection: Problems and solutions. World J Virol February World J Virol 2012,N 11,vol. 12, p. 31–43.
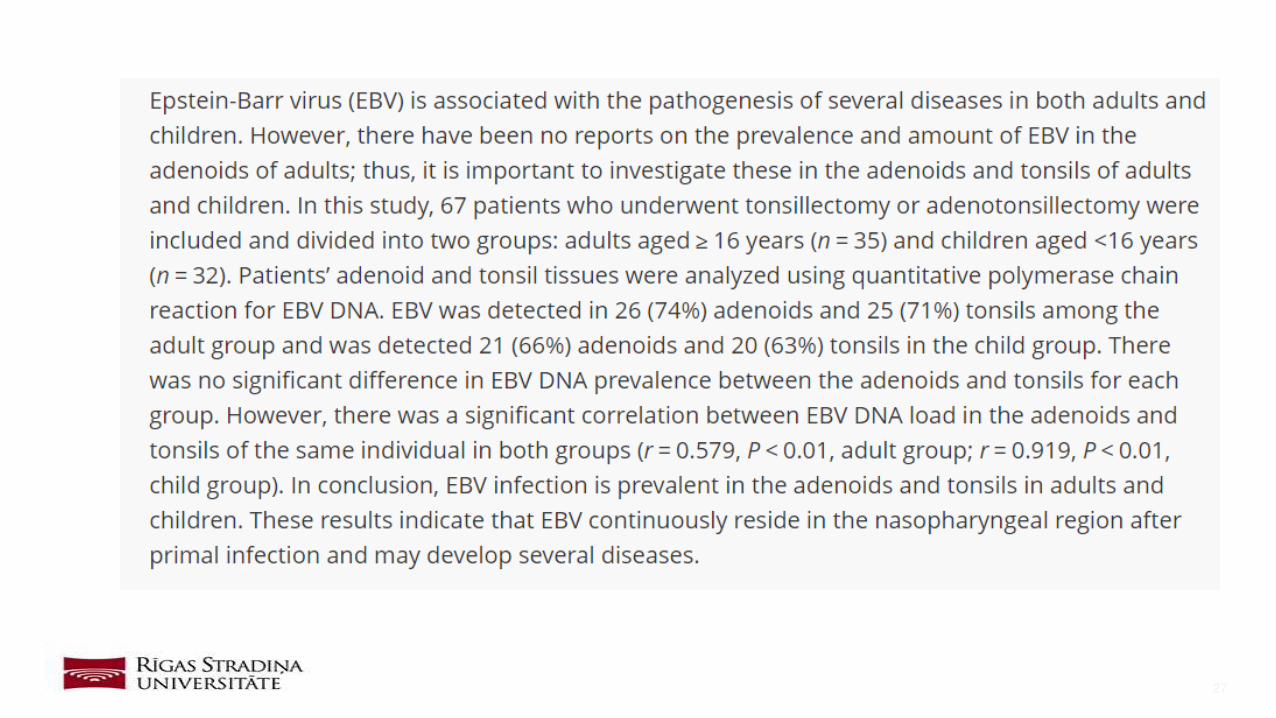
Seishima Noriko, Kondo Satoru, Wakisaka Naohiro, Kobayashi Eiji IT. EBV infection is prevalent in the adenoid and palatine tonsils in adults. Journal of Medical Virology 2016.
Shadfar S, Drake AF, Vaughn B V., Zdanski CJ. Pediatric Airway Abnormalities: Evaluation and Management. Oral and Maxillofacial Surgery Clinics of North America 2012,N
3,vol. 24, p. 325–66.
Sibel Aka, Berna Yayla Özker, Ebru Demiralay smet EC. Role of Ebstein-Barr virus in children with tonsillar hypertrophy. Turk Pediatri Arsivi 2013.
Wood JM, Cho M, Carney a S. Role of subtotal tonsillectomy (’tonsillotomy’) in children with sleep disordered breathing. The Journal of Laryngology and Otology 2014,N Suppl.
S1,vol. 128, p. S3–7.
CDC- Epstein-Barr Virus and Infectious Mononucleosis 2016. https://www.cdc.gov/epstein-barr/hcp.html (accessed March 10, 2017).
Veres [2]
31
Thank you for attention!





























