Embed Size (px)
Citation preview
SYSTEMIC THERAPY FOR UNRESECTABLE STAGE III OR
METASTATIC CUTANEOUS MELANOMA
Sarkheil MehdiHematologist- oncologist
Epidemiology
• Metastatic melanoma accounts for less than 5% of all cases of melanoma• associated with a poor rate of survival at 5 years (13%). • Common sites of metastases include distant skin, lymph nodes, liver,
lungs, bone, and brain.
Treatment is based on Staging
• MM staging is done with a combination of 2 systems:• Breslow’s Depth: A depth measurement made by the pathologist, reported in
millimeters (mm.) The single most important factor in determining prognosis.• Clark’s Level: A method of staging based on anatomical levels in the skin;
becomes more important prognostic indicator in thinner lesions. (Example: A 0.19mm lesion still confined to the epidermis has a better prognosis than a 0.19mm lesion penetrating into the papillary dermis.
Stages of Melanoma
• Stage 0: The melanoma involves only the top layerof skin. It is called melanoma in situ.• Stage I: The tumor is no more than 1 millimeterthick The surface may appear broken down. Or tumor is between 1 and 2 millimeters thick, and surface is not broken down.• Stage II: The tumor is between 1 and 2 millimetersthick, and the surface appears broken down. Orthickness of the tumor is more than 2 millimeters,and the surface may appear broken down.
Stages of Melanoma• Stage III: The melanoma cells have spread to atleast one nearby lymph node Or to tissuesnearby.• Stage IV: Cancer cells have spre ad to the lung orother organs, skin areas, or lymph nodes far awayfrom the original growth.
Melanoma commonlyspreads to other parts of the skin, tissue under theskin, lymph nodes, and lugs, liver, brain, bones, and other organs
Treatment is based on Staging
• In situ melanomas (confined to epidermis) are excised with 5mm margins. Patients gets yearly skin exams for life.
• Invasive melanomas < 0.75mm depth get re-excised with 1cm margins.
• Secondary characteristics of the tumor can infer additional risk for metastasis: Ulceration; lymphatic, perineural or vascular invasion; regression, etc. These patients get skin exams q3months x 1 year, then q6months x 1 year, and then yearly.
Treatment is based on Staging
• Invasive melanomas > 0.75mm Breslow’s depth get referred to surgical oncology for Sentinel Lymph Node (SNL) biopsy.
• Dye is injected near site of tumor and taken up by first (sentinel) lymph node in drainage network. This node is then excised and sent to path. Melanoma cells in node indicate metastatic disease.
• Usually the remainder of the affected lymphatic drainage basin is dissected and removed and patient is referred to oncology for adjuvant chemo, radiation or interferon treatment.
metastatic melanomas
• Surgery is the preferred option for the management of metastatic melanoma with resectable solitary sites of disease in selected patients.
• Following complete resection, adjuvant systemic treatment in the context of clinical trial can be considered.
• Patients with residual disease should be treated with systemic therapy for metastatic melanoma.
metastatic melanomas
• Most metastatic melanomas are not amenable to surgery; systemic therapy is often the best option.
• Optimal selection of systemic agents depends on : mutation status of cancer, volume and tempo of disease, and presence of symptoms and host performance status.
• Certain agents may be better suited for selected subgroups of patients as well.
Other useful tests
• Patients with unresectable stage III and stage IV cutaneous melanoma should undergo BRAF biomarker testing to determine whether they are candidates for vemurafenib.
• Molecular validation should be performed using parallel testing with early access program testing kits; a reasonable number of duplicate test cases (i.e. 40 samples) should be performed.
First-line systemic therapy:
BRAF-positive patients :
• 1. Clinical trials.
• 2. Vemurafenib (960 mg orally, twice per day) in patients with high volume, symptomatic disease, or who are poor candidates to receive immunotherapy with ipilimumab.• 3. Ipilimumab in patients with low volume, asymptomatic disease.
• 4. Dacarbazine- or paclitaxel-based systemic chemotherapy.
BRAF-negative patients :
• 1. Clinical trials.
• 2. Ipilimumab.
• 3. Targeted therapy based on tumour mutational status (based on probability of clinical benefit).
• 4. Dacarbazine- or paclitaxel-based systemic chemotherapy.
Second-line systemic therapy
Patients who are intolerant or who have progressed after first-line therapy may be considered for:
• 1. Clinical trials.
• 2. Treatment with a different agent not used from the first-line list.
• 3. Ipilimumab, if vemurafenib was given as first-line.
B-RAF Inhibitors
• The BRAF gene is responsible for encoding the B-Raf protein• it plays a role in cell signaling and cell growth
• it is mutated in about 50% of individuals with cutaneous melanoma.• The most common variants are BRAF V600E, BRAF V600K, and BRAF
V600R.
• Vemurafenib (PLX4032) is a BRAF inhibitor that is active against the BRAF V600E mutation.
B-RAF Inhibitors
• A phase III trial by Chapman, et al. compared vemurafenib (960 mg orally, twice per day) with dacarbazine (1000 mg/m2, every 3 weeks)
in previously untreated patients (n=675) with metastatic melanoma who tested positive for the BRAF V600E mutation and demonstrated a hazard ratio for tumor progression of 0.26 (95% CI 0.20-0.33; p<.001) for vemurafenib with an estimated median progression-free survival time was 5.3 months versus 1.6 months for dacarbazine.
B-RAF Inhibitors
Vemurafenib produced a 20% increase in overall survival at 6 months (84%, 95% CI 78-89% versus 64%, 95% CI 56-73%• relative risk of death 63%, p<.001)Among previously treated patients with BRAF V600–mutant metastatic melanoma• vemurafenib has been shown to produce an overall response rate of
53% (8 complete and 62 partial responses) • median duration of 6.7 months• median progression-free survival in this cohort was 6.8 months.
B-RAF Inhibitors
• Other BRAF inhibitors include sorafenib, GDC-0879, PLX-4720, and dabrafenib
B-RAF Inhibitors
• Dabrafenib has been the most successful of these agents.
• BREAK-3 open-label trial compared dabrafenib (150 mg 2 times per day) with dacarbazine (1000 mg/m2 IV q 3 wks)
in patients with stage IV or unresectable BRAF V600+ melanoma (N=250) demonstrated a PFS advantage with dabrafenib (median PFS 5.1 months vs. 2.7 months; HR 0.30; 95% CI 0.18-0.51; p<.001).
CTLA-4 Blockers
• Ipilimumab is a human monoclonal antibody that blocks the action of cytotoxic T lymphocyte-associated antigen 4 (CTLA-4). • By blocking CTLA-4, ipilimumab promotes an immune response
against tumours. • Clinical trials have demonstrated overall survival rates of 13 to 47% at
one year and 24 to 33% at two years in patients treated with ipilimumab (10 mg/kg, every three weeks for four cycles, then every 12 weeks as maintenance) as second line therapy.
CTLA-4 Blockers
• A phase III clinical trial by Robert, et al. (2011), among previously untreated patients (n=502) with metastatic melanoma
compared ipilimumab (10 mg/kg every three weeks for four cycles) plus dacarbazine (850 mg/m2 every three weeks through week 22) with dacarbazine alone
both regimens included an induction phase followed by a maintenance phase.
CTLA-4 Blockers
• The overall survival rates at one year and two years were 47.3% and 28.5% for ipilimumab combination therapy and 36.3% and 17.9% for dacarbazine monotherapy, respectively.
• Ipilimumab + dacarbazine combination therapy was also shown to produce better overall survival rates than ipilimumab alone (62% and 45%, respectively, at one year; 24% and 21%, respectively, at two years; 20% and 9%, respectively, at three years).
Other Biologic Agents
• Imatinib is a tyrosine kinase inhibitor that targets Abl, c-Kit, and platelet-derived growth factor receptor
• it may be effective in patients with metastatic melanoma who have c-kit mutations.
imatinib mesylate
• A phase II clinical trial among patients with metastatic melanoma and c-Kit aberrations showed that
administration of imatinib mesylate at 800 mg per day, orally (in six-week cycles) resulted in durable response rate (i.e., CR and PR) of 16% (4 of 24 patients), with a median OS= 10.7 months.
MEK inhibitors
• trametinib and selumetinib have been studied in the setting of advanced/unresectable melanoma. • METRIC study compared trametinib (2 mg per day orally) with
standard dacarbazine in BRAFV600E/K mutant patients (N=322) and was able to demonstrate better median PFS for trametinib
(4.8 months vs. 1.5 months; HR progession/death 0.45, 95% CI 0.33-0.63; p<.001), as well as better OS at 6 months (81% vs. 67% for chemo despite crossover; HR death 0.54, 95% CI 0.32-0.92; p=.01).
Anti-angiogenesis
• Phase II data on bevacizumab has shown some benefit in survival, when this agent is combined with chemotherapy.
• A double-blind trial of bevacizumab (15 mg per kg IV) and carboplatin/ paclitaxel, compared with carboplatin/paclitaxel alone, in patients with previously untreated metastatic melanoma (N=214)
Anti-angiogenesis
• produced better median OS at 13 months (12.3 months vs. 8.6 months; HR 0.67; p=.0366)
but not PFS (5.6 months vs. 4.2 months; HR 0.78; p=.1414).
• At 17 months, however, the median OS difference was no longer significant (12.3 months vs. 9.3 months; HR 0.79; p=.1916).
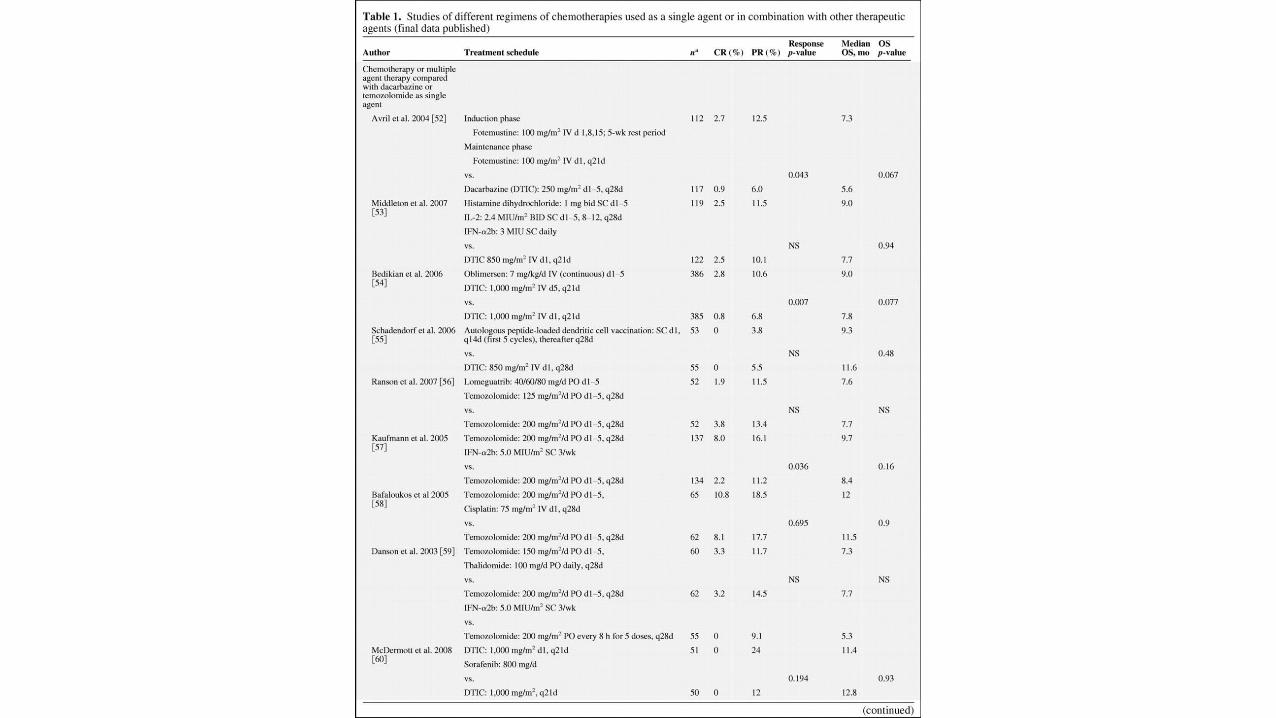
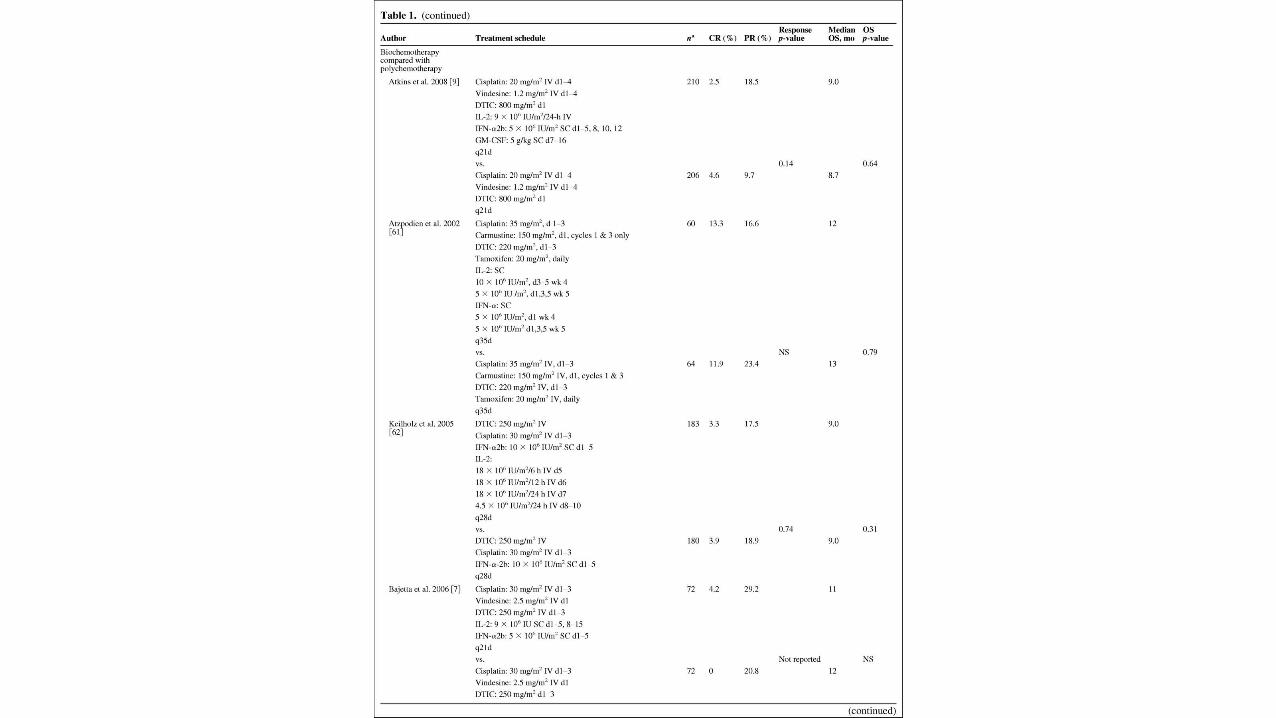
Chemotherapy
• Prior to the development of novel agents such as ipilimumab and vemurafenib
standard therapy for metastatic melanoma has been dacarbazine (DTIC) chemotherapy alone or in combination with other cytotoxic agents and/or interferon-alpha (IFN-α), or high-dose interleukin-2 (IL-2) alone or in combination with other agents.
Chemotherapy
• these regimens have produced only minimal gains in overall survival.
• In phase III clinical trials, combination therapy using DTIC has
• produced response rates of 16 to 27% with median overall survival ranging from 6 to 16 months.
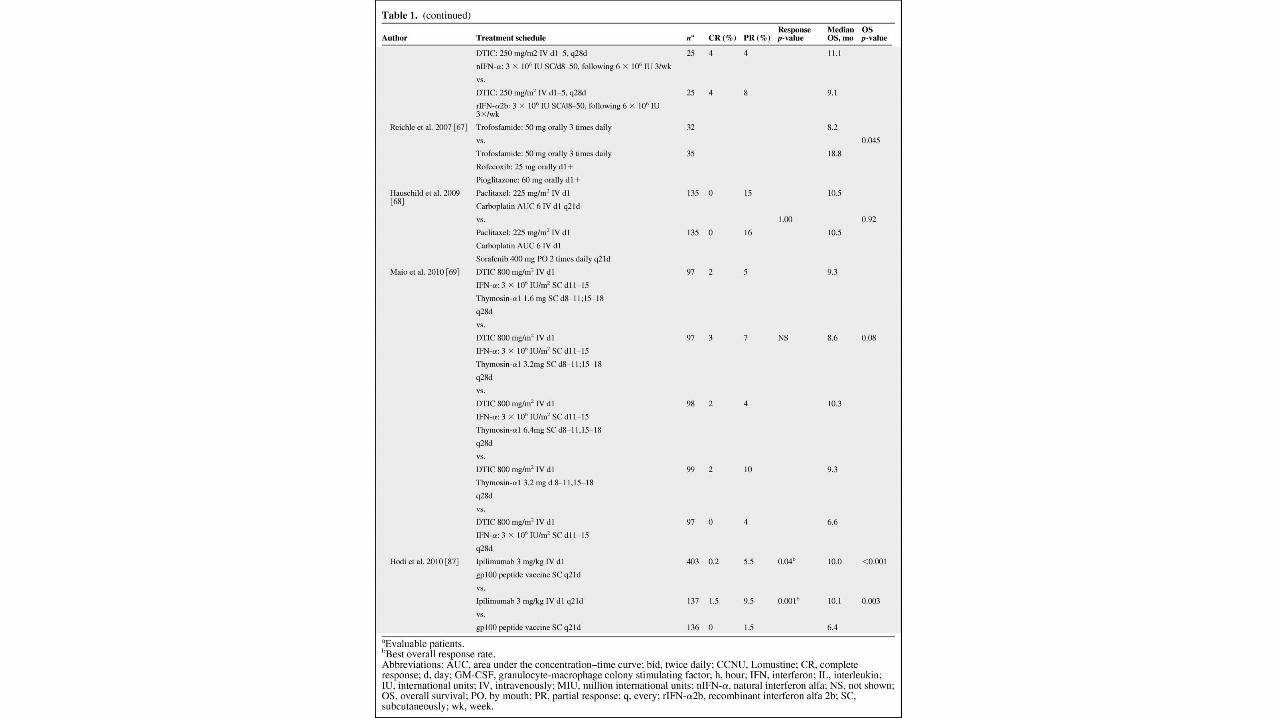
Chemotherapy
• Phase III data on high-dose IL-2 is similar: response rates of 5 - 33%, with median OS= 9 - 11 months
with the exception of high-dose IL-2 and gp100 peptide vaccination, which was recently shown to result in a median OS of 18 months (p=.06, versus high-dose IL-2 alone).
chemotherapy
• A meta-analysis comparing biochemotherapy (i.e., chemotherapy+ IFN-α +/- IL-2) with chemotherapy alone
among 2600 patients with metastatic melanoma
revealed a better response rate with biochemotherapy (27.9% versus 18.6%; p<.001) but no difference in OS (17.2% versus 17.5%).