Embed Size (px)
Citation preview
Pediatric Hematology/Oncology: Blood, Body, and Beyond
Geoffrey S. Kannan, PhD, MD
Pediatric Neuro-oncology
Pediatric Hematology/Oncology
Disclosures
• Nothing to disclose
• Discuss standard of care for common hematologic disorders
Objectives
• The role of the pediatric hematologist/oncologist
• Discuss common reasons for referral to heme/onc • Disorders of red cells
• Disorders of white cells
• Disorders of platelets
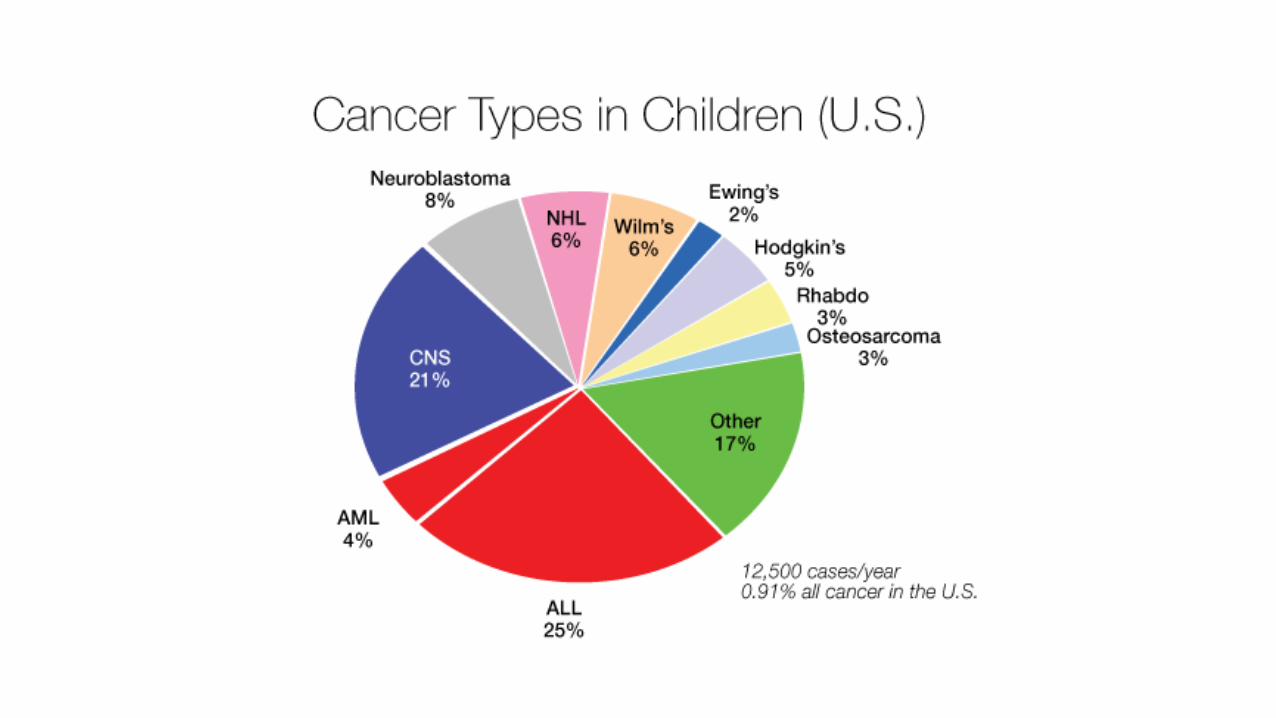
• Brain tumors
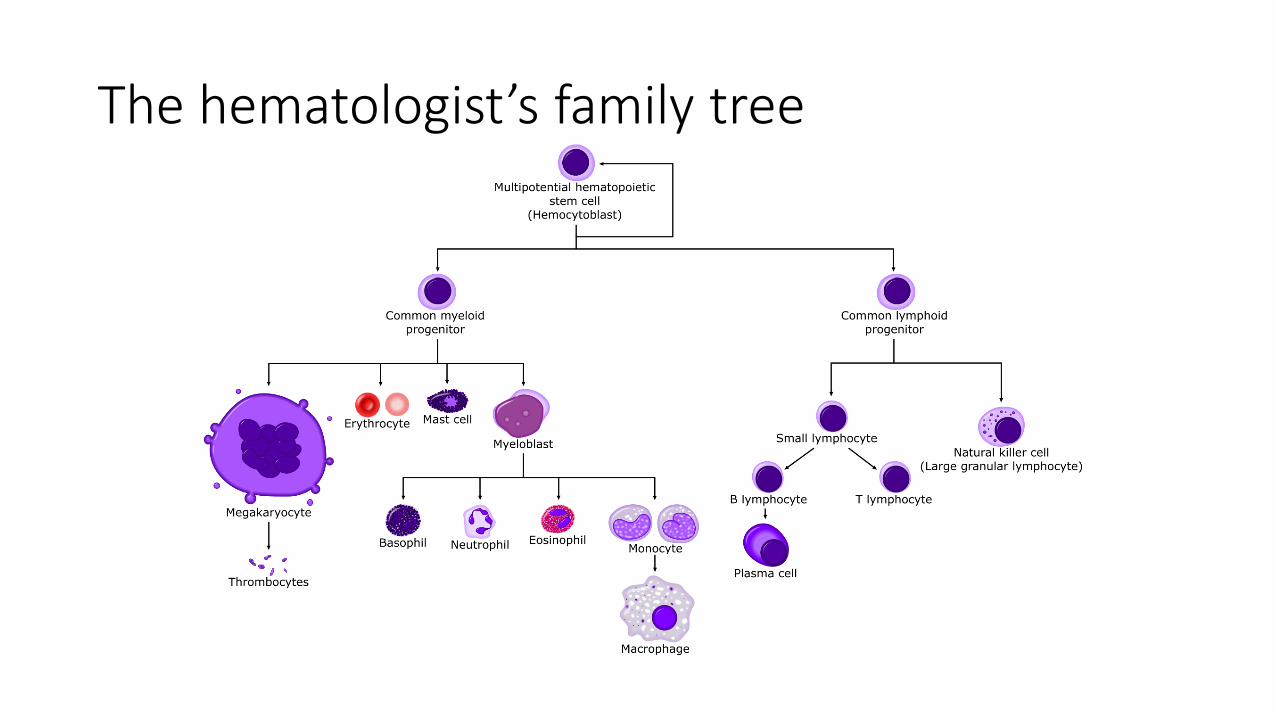
The hematologist’s family tree
Disorders of Red cells
• Red cell production problems
• Red cell destruction problems
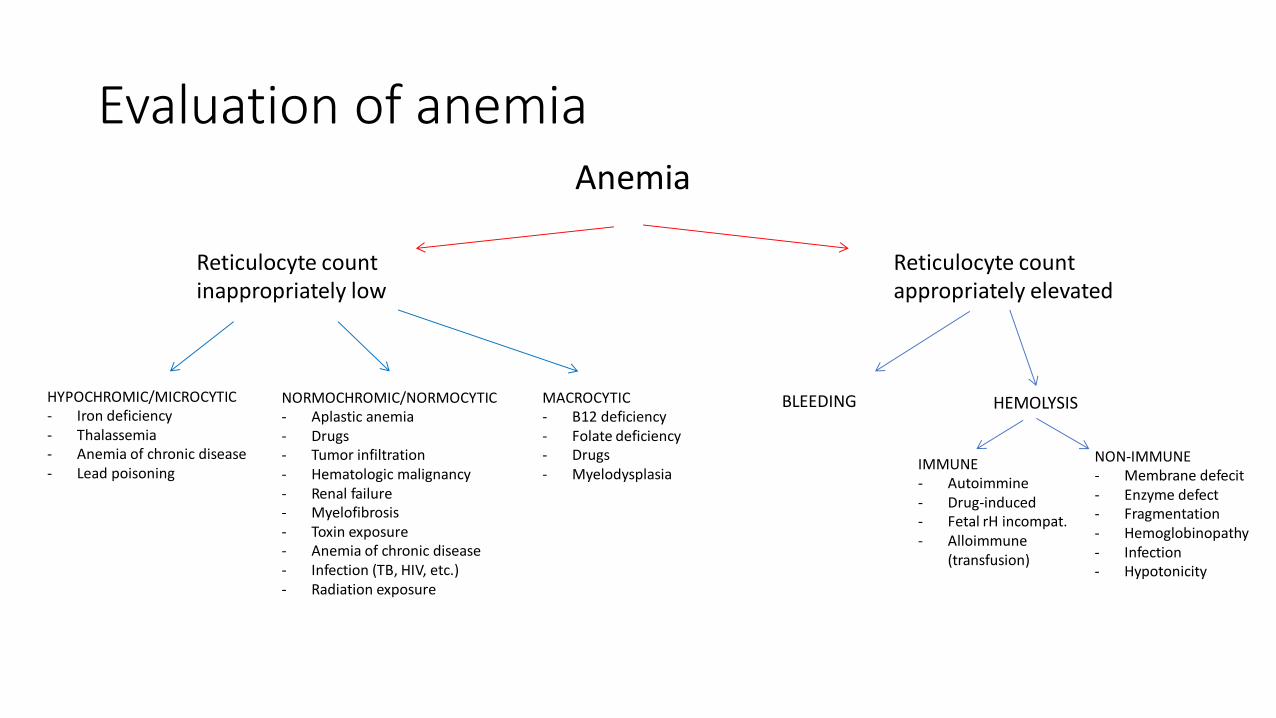
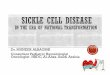
Evaluation of anemia Anemia
Reticulocyte count inappropriately low
Reticulocyte count appropriately elevated
HYPOCHROMIC/MICROCYTIC - Iron deficiency - Thalassemia - Anemia of chronic disease - Lead poisoning
NORMOCHROMIC/NORMOCYTIC - Aplastic anemia - Drugs - Tumor infiltration - Hematologic malignancy - Renal failure - Myelofibrosis - Toxin exposure - Anemia of chronic disease - Infection (TB, HIV, etc.) - Radiation exposure
MACROCYTIC - B12 deficiency - Folate deficiency - Drugs - Myelodysplasia
BLEEDING HEMOLYSIS
IMMUNE - Autoimmine - Drug-induced - Fetal rH incompat. - Alloimmune
(transfusion)
NON-IMMUNE - Membrane defecit - Enzyme defect - Fragmentation - Hemoglobinopathy - Infection - Hypotonicity
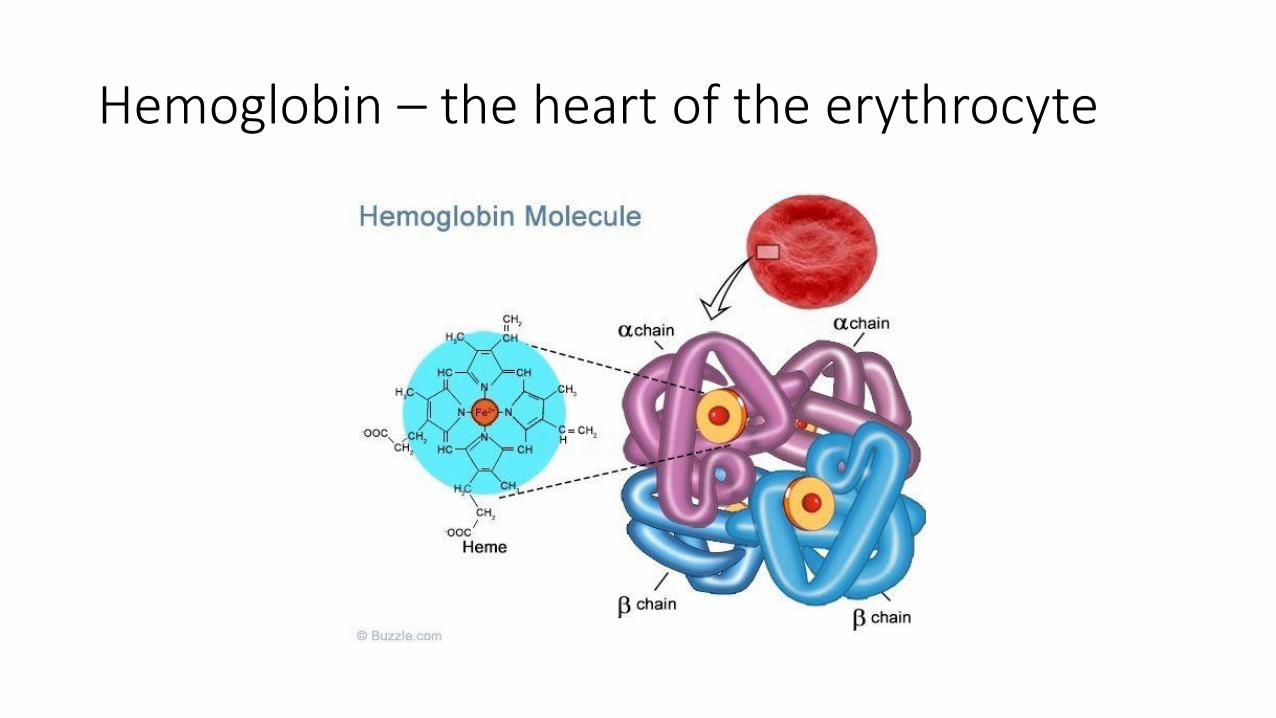
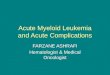
Hemoglobin – the heart of the erythrocyte
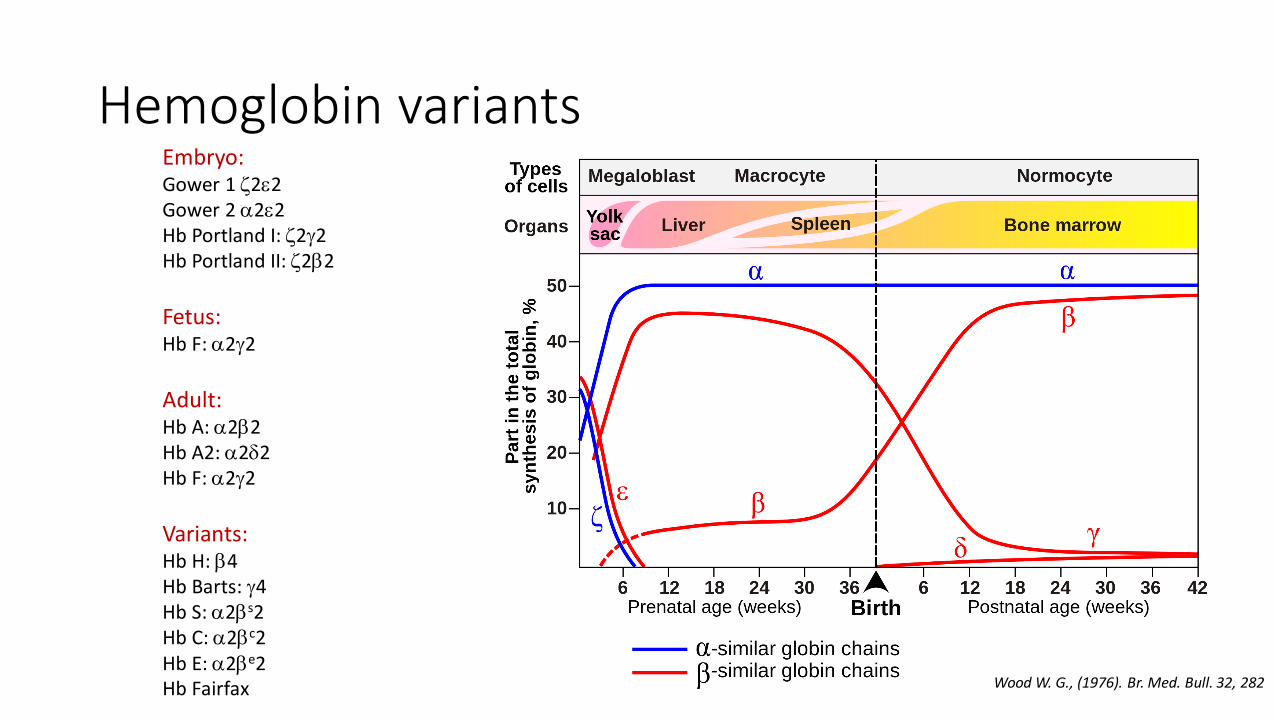
Hemoglobin variants
Wood W. G., (1976). Br. Med. Bull. 32, 282
Embryo: Gower 1 z2e2 Gower 2 a2e2 Hb Portland I: z2g2 Hb Portland II: z2b2
Fetus: Hb F: a2g2
Adult: Hb A: a2b2 Hb A2: a2d2 Hb F: a2g2
Variants: Hb H: b4 Hb Barts: g4 Hb S: a2bs2 Hb C: a2bc2 Hb E: a2be2 Hb Fairfax
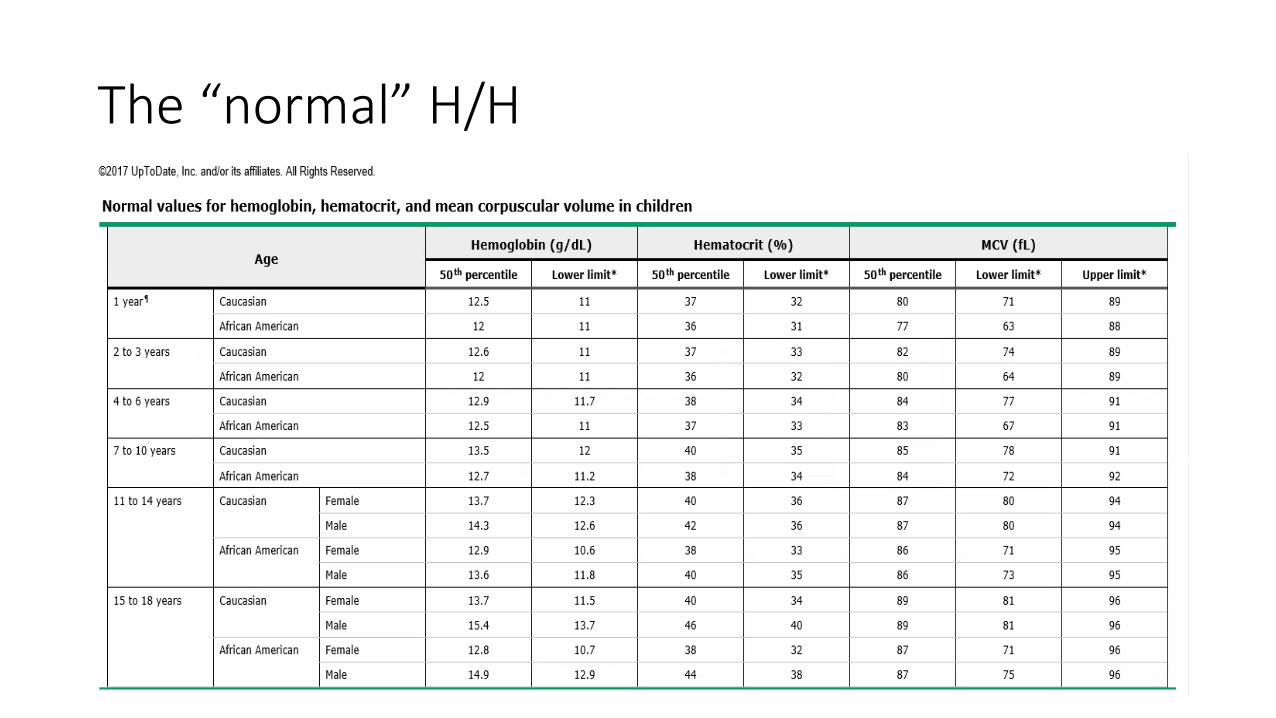
The “normal” H/H
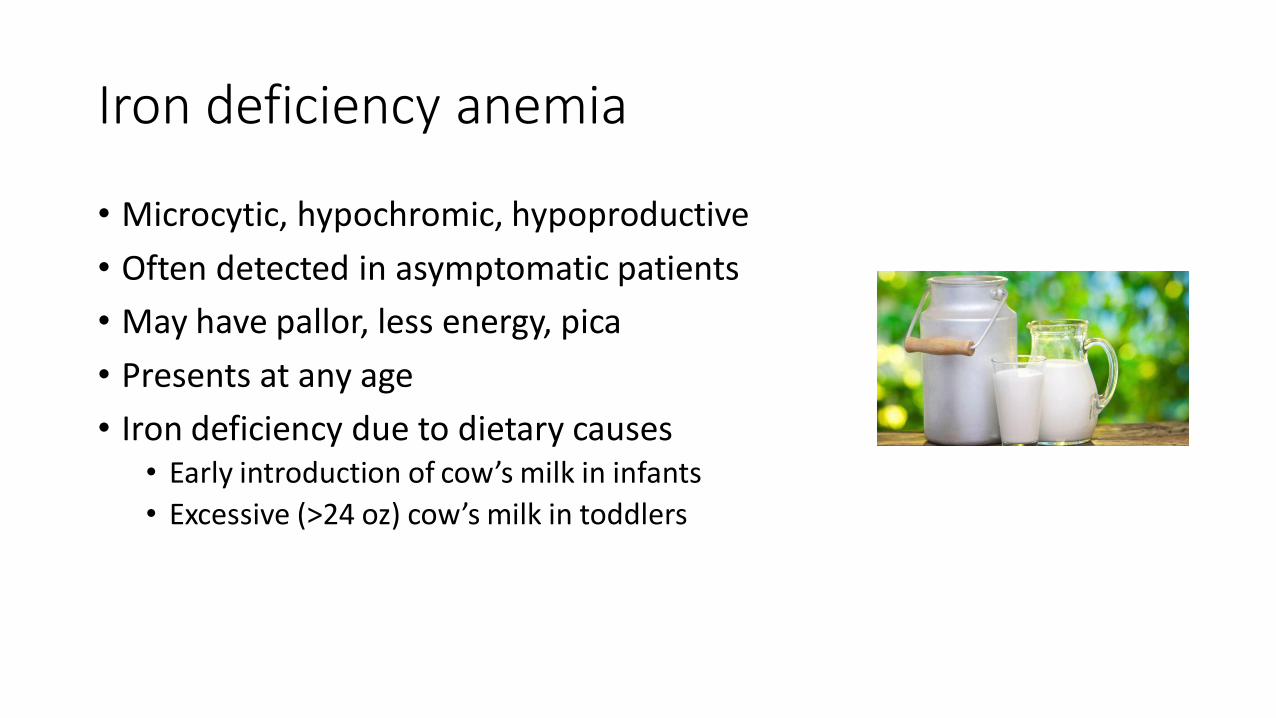
Iron deficiency anemia
• Microcytic, hypochromic, hypoproductive
• Often detected in asymptomatic patients
• May have pallor, less energy, pica
• Presents at any age
• Iron deficiency due to dietary causes • Early introduction of cow’s milk in infants
• Excessive (>24 oz) cow’s milk in toddlers
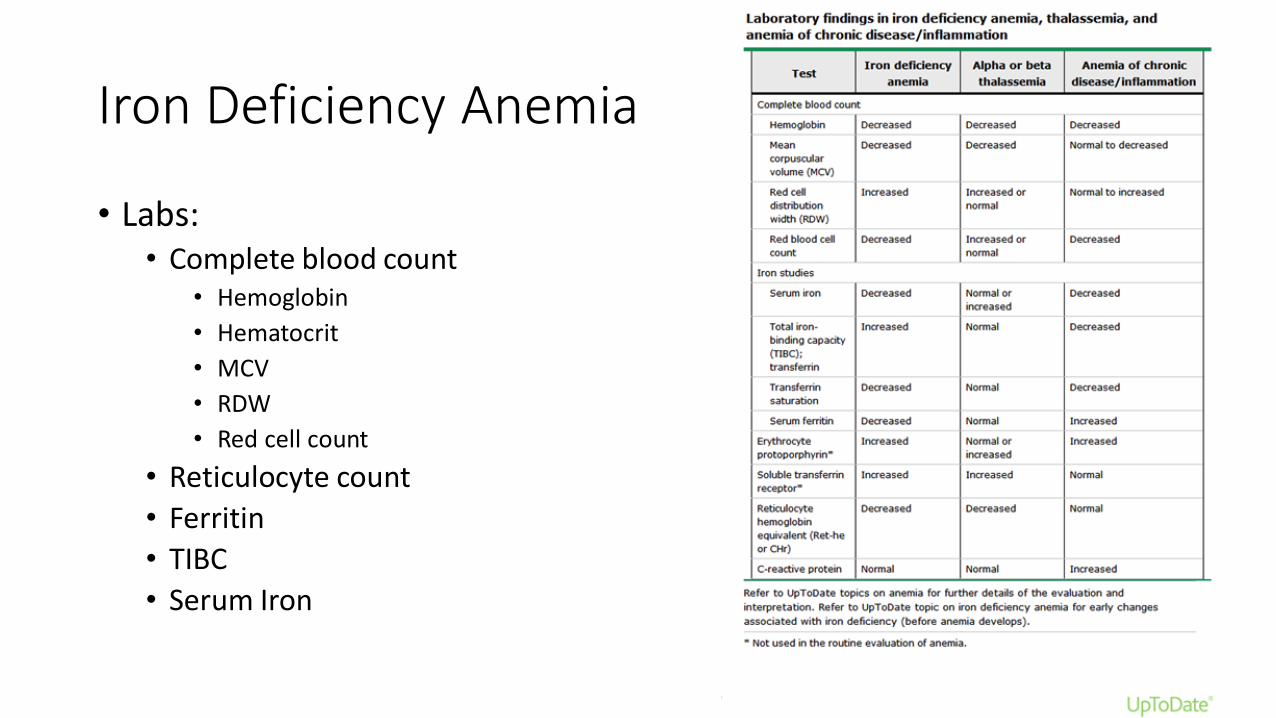
Iron Deficiency Anemia
• Labs: • Complete blood count
• Hemoglobin
• Hematocrit
• MCV
• RDW
• Red cell count
• Reticulocyte count
• Ferritin
• TIBC
• Serum Iron
Iron deficiency anemia
• Treatment is with 3-6 mg/kg/day of elemental iron • Fer-in-sol
• Vitron-C
• Eliminate milk intake (and bottle use, if applicable)
• Increase iron- and vitamin C-rich foods
• 3 months of treatment
• Anemia corrects before iron stores are repleted
• Limited role for IV iron – GI absorption deficiences
• Correct iron deficiency before investigation for thalassemia
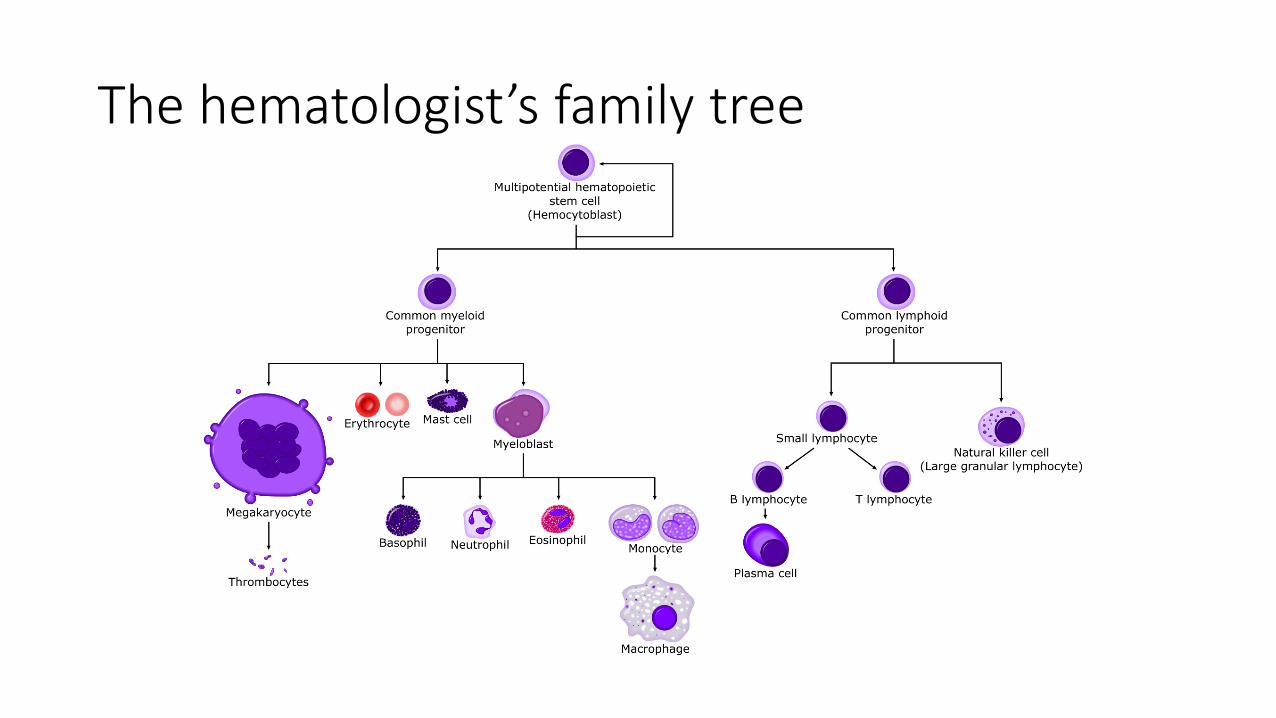
The hematologist’s family tree
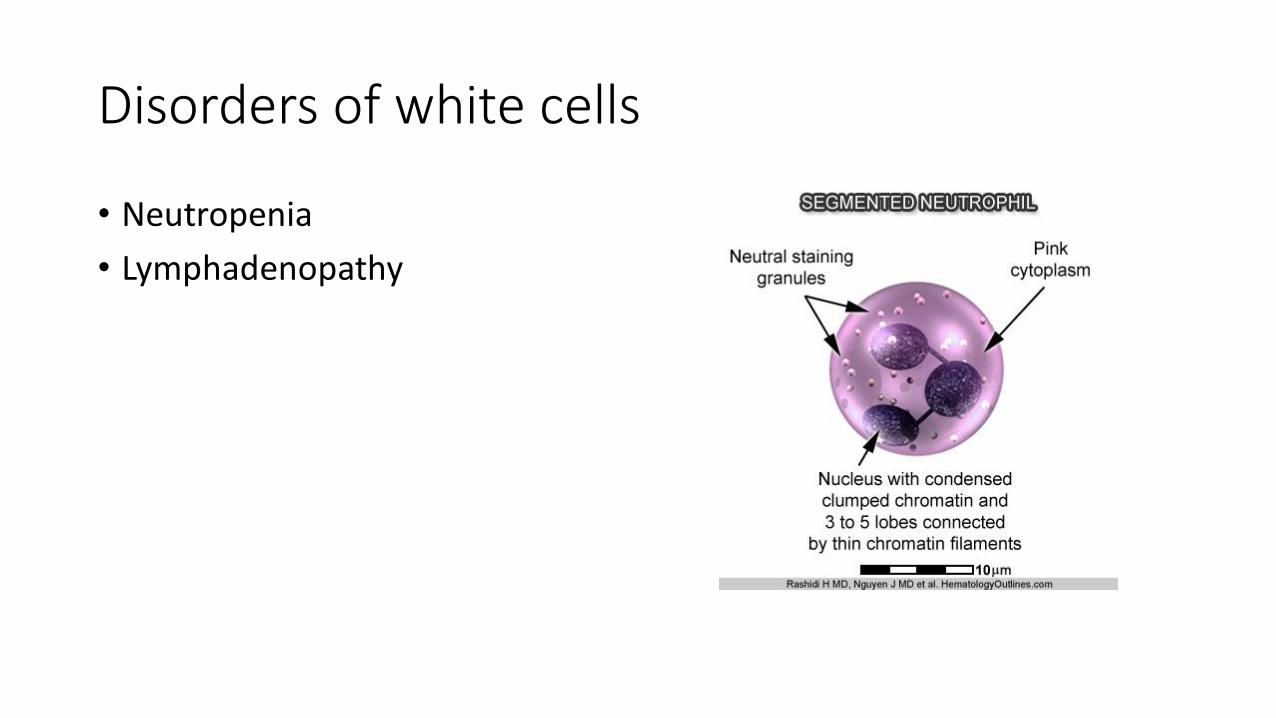
Disorders of white cells
• Neutropenia
• Lymphadenopathy
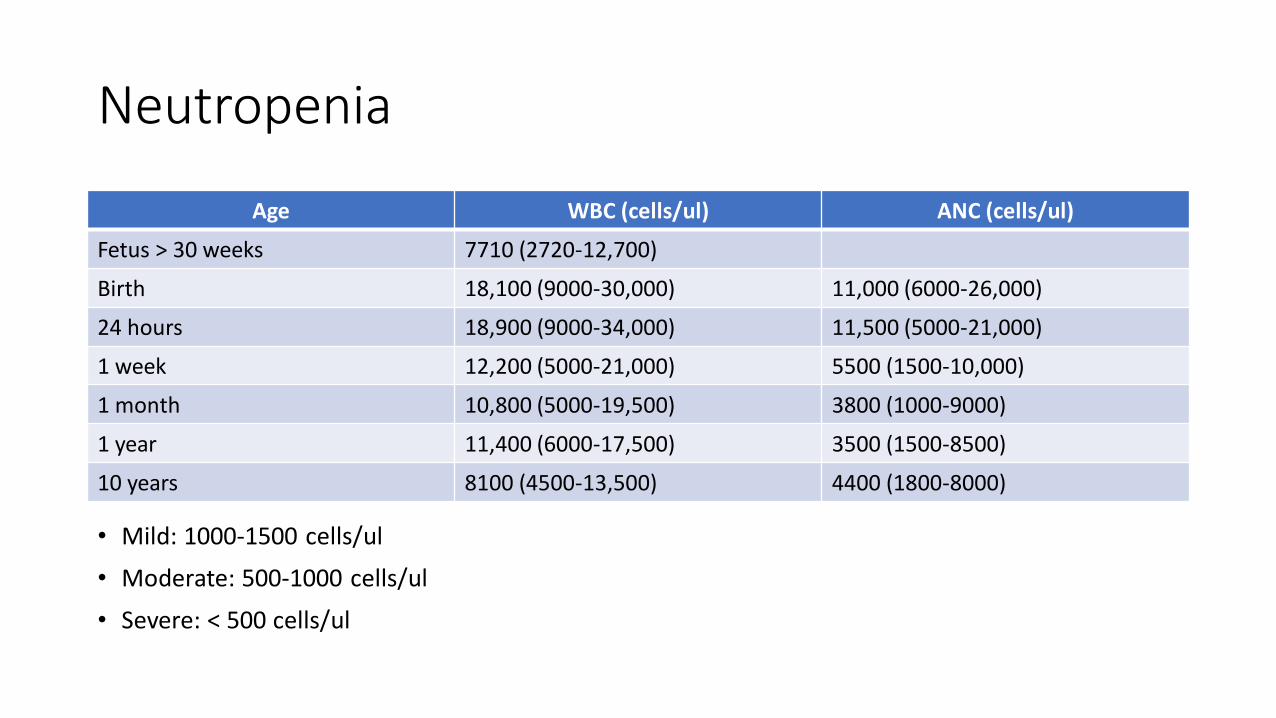
Neutropenia
Age WBC (cells/ul) ANC (cells/ul)
Fetus > 30 weeks 7710 (2720-12,700)
Birth 18,100 (9000-30,000) 11,000 (6000-26,000)
24 hours 18,900 (9000-34,000) 11,500 (5000-21,000)
1 week 12,200 (5000-21,000) 5500 (1500-10,000)
1 month 10,800 (5000-19,500) 3800 (1000-9000)
1 year 11,400 (6000-17,500) 3500 (1500-8500)
10 years 8100 (4500-13,500) 4400 (1800-8000)
• Mild: 1000-1500 cells/ul
• Moderate: 500-1000 cells/ul
• Severe: < 500 cells/ul
Evaluation of neutropenia
• Functional consequence of neutropenia – susceptibility to infection
• CBC samples a very small percentage of the body’s neutrophils
• Key question – how many neutrophils can get to site of infection
• Bone marrow reserve determines ability to respond to infection
• Propensity to infection is related to degree and cause of neutropenia
• Most patients will have adequate bone marrow reserve
• Also consider the APC (neutrophils + monocytes)
Etiologies of neutropenia
• Low to no risk • Chronic benign
• Ethnic
• Post-infectious
• Hypersplenism
• Moderate risk • Transient neonatal
neutropenia • Post-infectious
(decreased marrow reserve)
• Drug-induced • Cyclic • Nutritional • Immune (antibody-
mediated) • Immune (SLE, CVID)
• High risk • Shwachman-Diamond
• Kostmann
• Drug-induced (absent marrow reserve)
• Chemotherapy
• Aplastic anemia
• Marrow infiltration/MDS/leukemia
How can we help with neutropenia?
• Anemia/thrombocytopenia – with neutropenia – call heme
• Repeat CBC with differential; ESR/CRP
• Drugs, temporary bone marrow suppression
• Medical history – bacterial infections (Cyclical? Unusual?)
• Periodontal disease – mouth sores, etc.
• Family history
• Bone marrow biopsy/aspirate
• NK/T cell/Immunoglobulin subsets
• Genetic testing
How can you help with neutropenia?
• We’ll manage together
• Does the child mount a neutrophil response to being sick?
• Chronic benign neutropenia patients can be treated as other children
• Management is related to severity and cause of the (bone marrow) problem
• Most children can be safely vaccinated
• Limited role for growth factors
Lymphadenopathy
• Most often benign as a result of an inflammatory/reactive process
• Cause of great concern for families, especially with family history of hematologic malignancy
• Physical exam to describe extent/character of LN (including testicular exam)
Lymphadenopathy – signs for concern
• Systemic symptoms: fever, night sweats, weight loss
• Supraclavicular lymphadenopathy
• Persistent generalized lymphadenopathy
• Fixed non-tender nodes; matted nodes
• > 1 cm with onset in neonatal period
• >/= 2 cm that increase in size or do not respond to two weeks of abx
• Abnormal CXR
• Abnormal CBC
• Persistently elevated or rising CRP/ESR
Stepwise approach to diagnosis
• Avoid glucocorticoids
• Rule out common causes (Strep, cat-scratch, EBV, CMV, TB (if history suggests))
• Consider 2 week trial of abx
• Consider observation if otherwise well
• No “correct” time to wait for referral in the absence of other symptoms
• Consider chest X-ray, ultrasound of nodes
• Excisional biopsy
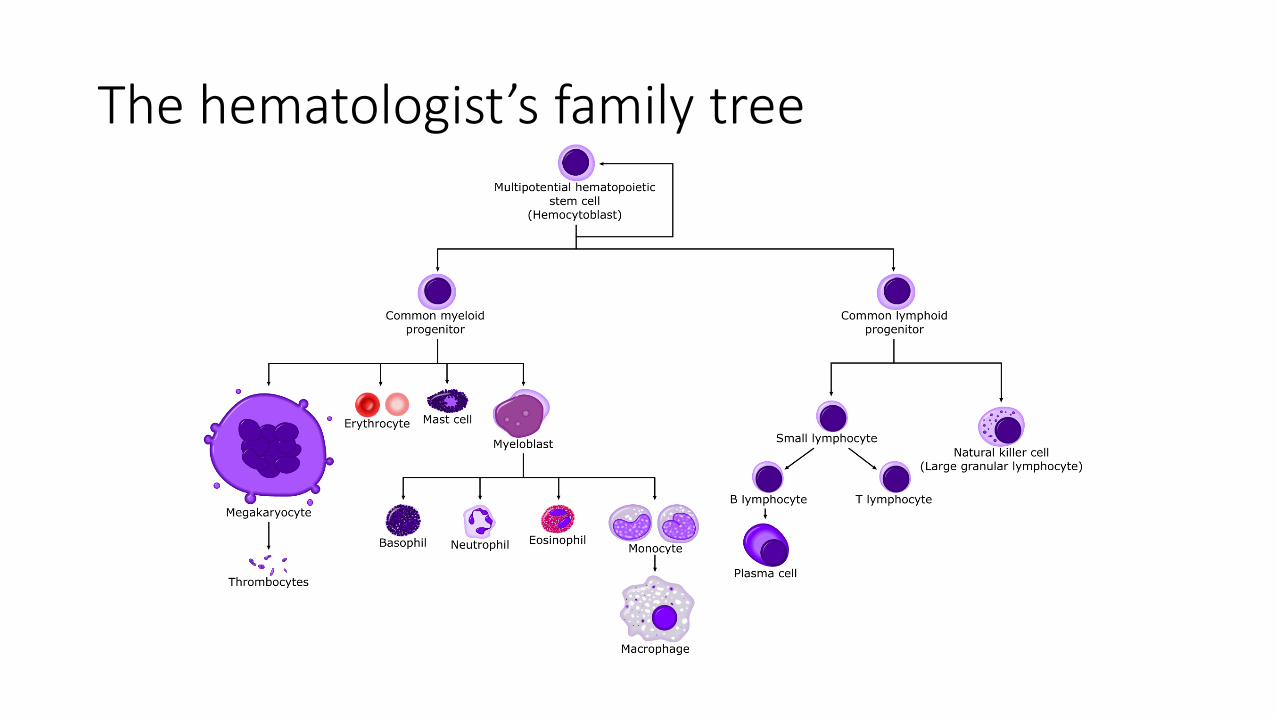
The hematologist’s family tree
Immune Thrombocytopenic Purpura
• (Idiopathic) Thrombocytopenic Purpura
• Immune ThrombocytoPenia
• Isolated thrombocytopenia (<100,000) with rest of BM function normal
• Cause unknown (viral infection, immunologic trigger, environmental)
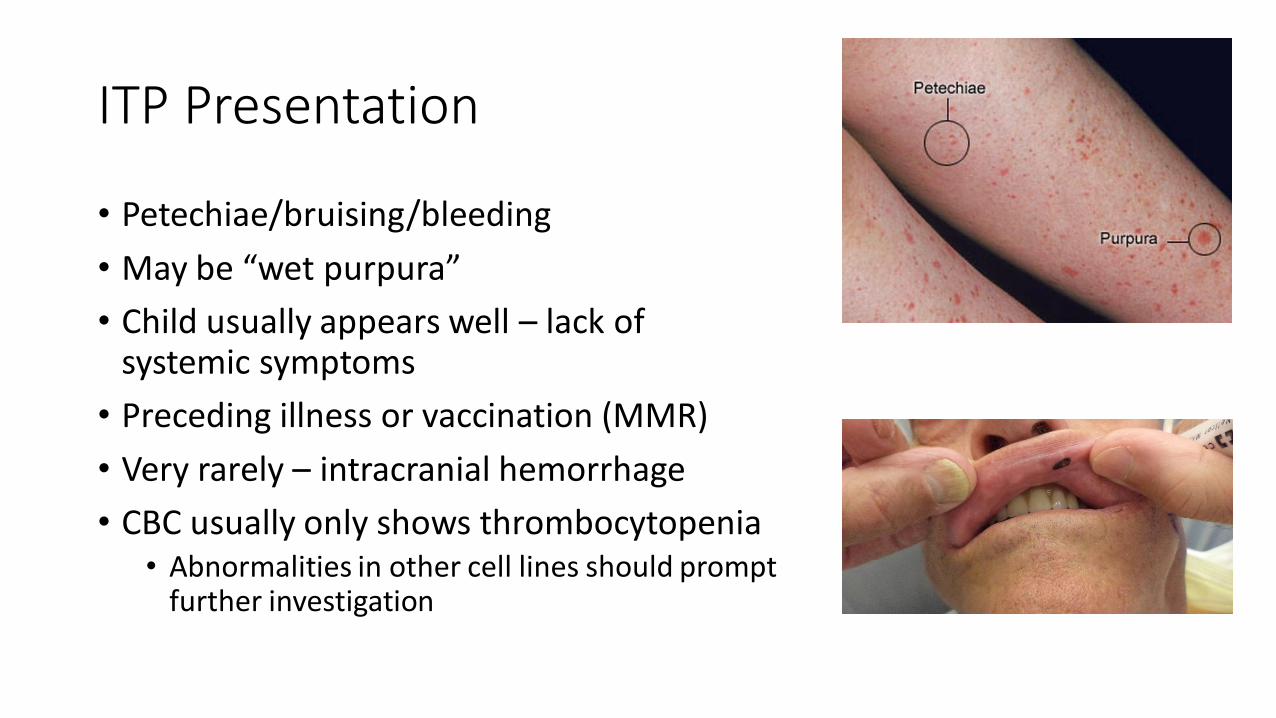
ITP Presentation
• Petechiae/bruising/bleeding
• May be “wet purpura”
• Child usually appears well – lack of systemic symptoms
• Preceding illness or vaccination (MMR)
• Very rarely – intracranial hemorrhage
• CBC usually only shows thrombocytopenia • Abnormalities in other cell lines should prompt
further investigation
ITP management
• Bone marrow examination is not required at diagnosis (may be required for treatment failure)
• No platelet transfusion unless there is life-threatening bleeding
• Activity restriction
• Avoid aspirin/ibuprofen
• Observation
ITP management
• Intravenous immunoglobulin (IVIG) – 1 g/kg
• Anti-D immune globulin (in Rh+, DAT neg patients)
• Glucocorticoids
• Second line – Rituximab, thrombopoeitin receptor agonists (eltrombopag, romiplostim)
• Less used therapies • Recombinant factor VIIa • Vincristine • Aminocaproic acid • Splenectomy
ITP management
• Treatments are not “curative”
• Spontaneous recovery in 3-6 months w/w/o treatment
• Weekly monitoring of platelet count
• Recommendations stratified to age/activity level/patient goals
• First-line therapies usually effective in ~70-80% of patients
• Response may not be sustained, relapses treated same as initial presentation
Chronic ITP
• Thrombocytopenia persisting beyond 12 months after presentation
• 10-20% of cases
• Risk factors • Older age • Less severe thrombocytopenia at presentation • Insidious onset of symptoms • Lack of preceding infection or vaccination
• Evaluate for other causes of thrombocytopenia • Infection • Bone marrow biopsy
• Treatment is similar to acute ITP
• Still expect spontaneous remission (2 years in 30% of children, 5 years in 50%)
• Consider Rituximab, TPO receptor agonists, immune modulating agents (azathioprine, 6MP, danazol, interferon, cyclosporine, dapsone, MMF, rapamycin, cyclophosphamide)
Follow up questions
1. A four-year-old male presents with a 6 week history of persistent anterior cervical lymphadenopathy (3 cm) which has not improved with multiple courses of antibiotics. The infectious disease, ENT, and hematology/oncology teams all agree that a tissue sample is required. Which is the preferred diagnostic procedure for persistent lymphadenopathy?
A. Fine needle aspiration
B. Excisional biopsy
C. Core needle biopsy
Follow up questions
2. You have just diagnosed a 15 month (12 kg) female with iron deficiency anemia. Which dose of ferrous sulfate are you going to start?
A. 12 mg elemental iron per day
B. 24 mg elemental iron per day
C. 60 mg elemental iron per day
D. 90 mg elemental iron per day
Follow up questions
2. Which of the following laboratory values is indicative of iron deficiency anemia?
Hemoglobin MCV Ferritin TIBC
A Low Low High Low
B Low Low Low High
C Low High High Low
D Low High Low High
Follow up questions
4. A 12 month male was incidentally noted to have neutropenia (ANC 400) on a CBC ordered for hemoglobin screening at 9 months. A repeat CBC 2 weeks later was similar—he had a normal platelet count, total WBC count, and hemoglobin/hematocrit but a persistently low ANC. He has been thriving and has not had an unusual number of infections. His test for anti-neutrophil antibodies was positive, and he was diagnosed with autoimmune neutropenia of infancy. Which of the following is true?
A. At his 12 month visit, he should not receive any vaccines
B. At his 12 month visit, he can receive all vaccines except MMR and varicella
C. At his 12 month visit, he can receive all routine vaccines
Follow up questions
5. Which of the following treatment approaches can be used in children with acute ITP?
A. IVIG
B. Systemic steroids
C. Anti-D immunoglobulin
D. Observation
E. All of the above
Brain tumors
• Two major concerns for pediatricians • Increasing head size
• Persistent headache/vomiting
• “Benign” vs “metastatic” when it comes to pediatric brain tumors
• Low grade vs high grade
• CNS is composed of specific cell types
• Tumors arise from these cells
• Metastases to the brain are rare in pediatrics
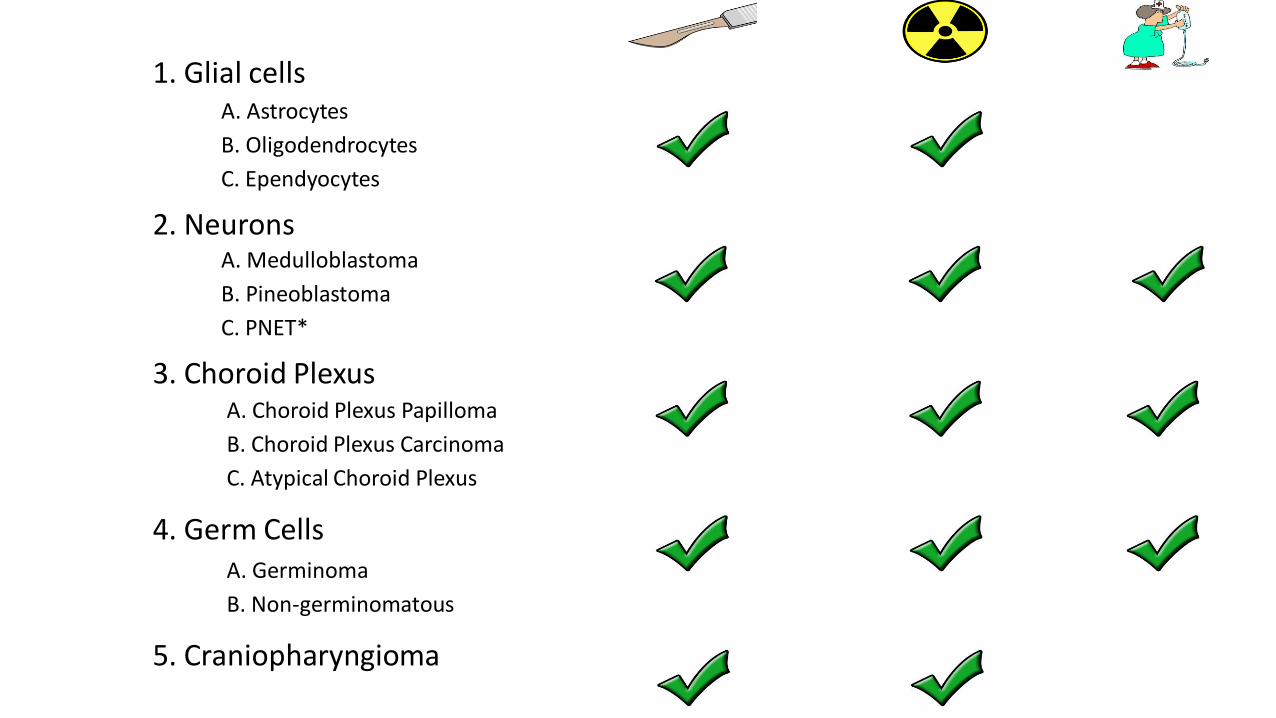
1. Glial cells
2. Neurons
3. Choroid Plexus
4. Germ Cells
5. Craniopharyngioma
B. Oligodendrocytes
C. Ependyocytes
A. Astrocytes
B. Pineoblastoma
C. PNET*
A. Medulloblastoma
B. Choroid Plexus Carcinoma
C. Atypical Choroid Plexus
A. Choroid Plexus Papilloma
B. Non-germinomatous
A. Germinoma

Thank you for your attention
Geoffrey S. Kannan, PhD, MD
Center for Cancer and Blood Disorders
6565 Arlington Blvd, Suite 200
Falls Church, VA 22042
Ph: 703-531-3627
Fax: 703-531-1590
www.psvcare.org