Embed Size (px)
Citation preview

From the Card
of Ulsan Colle
Reprint reque
Center Hear
Poongnap-do
seoul.kr).
0894-7317/$3
Copyright 201
http://dx.doi.o
Prognostic Implications of Initial EchocardiographicFindings in Adolescents and Adults with Supracristal
Ventricular Septal Defects
Min Soo Cho, MD, Sun-Joo Jang, MD, Byung Joo Sun, MD, Jeong Yoon Jang, MD, Jung-Min Ahn, MD,Dae-Hee Kim, MD, Jong-Min Song, MD, Duk-Hyun Kang, MD, and Jae-Kwan Song, MD, Seoul, South Korea
Background: Although surgery is recommended for pediatric patients with supracristal ventricular septaldefects (sVSDs) to prevent progression of aortic regurgitation (AR), outcomes in adolescents and adultswith sVSDs are not known.
Methods: In this retrospective observational study, clinical data without surgery were obtained in 60 patientswith sVSDs (group 1; mean age, 366 13 years), 120 age- and defect size–matched patients with perimembra-nous ventricular septal defects (group 2), and 52 patients with sVSDs who underwent surgery (group 3; meanage, 32 6 11 years).
Results: Aortic sinus wall prolapse (38% vs 3%, P < .0001) and moderate to severe AR (7% vs 0%, P = .012)were more frequently observed in group 1 than in group 2. Five, three, and two patients in group 1 hadsurgery during follow-up because of rupture of the aneurysm of the sinus of Valsalva, endocarditis, and heartfailure, respectively. Group 1 had a lower 12-year clinical event-free (surgery and endocarditis) rate (766 9%vs 94 6 4%, P = .031) but an equivalent overall survival rate (100% vs 94 6 3%, P = .143) compared withgroup 2. Patients with maximal prolapsing aortic sinus wall length > 7 mm showed a higher frequency ofaneurysm of the sinus of Valsalva rupture than those with no prolapse or maximal prolapsing length# 7 mm (80% [four of five] vs 2% [one of 55], P < .001). The event-free and overall survival rates were com-parable between groups 1 and 3, with equivalent 10-year AR progression–free survival rates (94 6 5% vs91 6 5%, P = .301).
Conclusions: Aneurysm of the sinus of Valsalva rupture, rather than AR progression, was the main clinicalevent. Watchful monitoring of patients with high-risk echocardiographic features may be a rational option.(J Am Soc Echocardiogr 2014;27:965-71.)
Keywords: Subarterial ventricular septal defect, Aortic regurgitation, Aneurysm of sinus of Valsalva, Echocar-diography
The association between ventricular septal defect (VSD) and aorticregurgitation (AR) was recognized as an important disease entitymany years ago. Supracristal VSD (sVSD) is strongly associatedwith this disease entity, which is characterized by a totally deficientinfundibular septum1 and a lack of continuity between the aorticmedia, annulus, and ventricular septum.2 Aortic valve prolapsethat results in AR and aneurysm of the sinus of Valsalva (ASV) arecommon aortic complications of sVSD and are reported to progressonce they develop.3-6 Therefore, it has been recommended to repairthe defect surgically as soon as these aortic complications are
iac Imaging Center, Asan Medical Center Heart Institute, University
ge of Medicine, Seoul, South Korea.
sts: Jae-Kwan Song, MD, Cardiac Imaging Center, Asan Medical
t Institute, University of Ulsan College of Medicine, 388-1
ng Songpa-gu, Seoul, 138-736, South Korea (E-mail: jksong@amc.
6.00
4 by the American Society of Echocardiography.
rg/10.1016/j.echo.2014.05.016
detected.2,7-9 However, this recommendation is based onobservational studies of young pediatric patients (mean age < 10years),5,8,9 and the natural history of patients with sVSDs whohave reached adolescence or adulthood is poorly understood.Given that the aorta and cardiac chambers grow only duringchildhood and stop expanding significantly after 15 years of age,10
it is possible that the progression or pattern of these aortic complica-tions in adult patients with sVSDs may differ from those in children,and even in young pediatric patients, the role of prophylactic surgeryfor patients without aortic complications remains controversial.11,12
We aimed to evaluate the natural histories of adolescents and adultswith sVSDs and to determine factors associated with thedevelopment of aortic complications, including AR progressionand ASV rupture. The clinical outcomes of those adolescent oradult patients with sVSDs, who were followed conservatively andtreated surgically only when necessary, were compared with thoseof adult patients with perimembranous VSDs (pmVSDs), forwhom the same watchful monitoring strategy has been acceptedas the standard approach, and those of patients with sVSDs whounderwent initial surgery.
965

Abbreviations
AR = Aortic regurgitation
ASV = Aneurysm of the sinus
of Valsalva
pmVSD = Perimembranousventricular septal defect
sVSD = Supracristalventricular septal defect
VSD = Ventricular septaldefect
966 Cho et al Journal of the American Society of EchocardiographySeptember 2014
METHODS
Study Population
Between January 1990 andNovember 2009, 134 patients>16 years of age were confirmedto have isolated sVSDs withoutcomplex congenital lesions inour institution. The routine evalu-ation included transthoracicechocardiography and a single-pass heart scan using 99mTc-dieth-ylenetriamene penta-acetate to
measure Qp/Qs. Patients were excluded if they had Eisenmengersyndrome (n = 2) or were not followed up after the initial visit(n = 20). The subjects thus consisted of the remaining 60 patientswith sVSDs who were followed conservatively and whose follow-updata were available (group 1) and 52 who underwent initial surgery(group 3). In group 3, the development of complications (ASV rupture[n = 11] and infective endocarditis [n = 6]) or heart failure (n = 5) wasmain indication for surgery, and the remaining 30 stable patientswithout symptoms underwent surgery under attending physicians’discretion. As a control group, 120 age- and defect size–matched pa-tients with pmVSDs who were also followed conservatively for thedevelopment of symptoms or complications before surgical interven-tion were selected from the database of our echocardiography labora-tory (group 2). This retrospective study conformed to the ethicalguidelines of the 1975 Declaration of Helsinki as reflected in a prioriapproval by our institutional review board. The requirement forinformed consent was waived by the board for this study.
Echocardiography
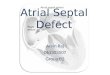
The diagnoses of sVSD and pmVSD were based on the echocardio-graphic observations,13,14 and transesophageal echocardiography wasgenerally recommended for detailed evaluation of sVSDs andassociated anatomic abnormalities, which was performed in >70%of patients. The echocardiographic images were reviewed todetermine whether significant aortic sinus wall prolapse was presentbecause of herniation of the aortic wall through the VSD(Figures 1A–1D). The size of the remnant VSD showing flowcommunication through the defect was measured at mid-systole inthe magnified view (Figure 1). In patients with aortic sinus wall pro-lapse, the maximal length of the prolapsed wall was measured at dias-tole; the maximal distance between the crest of interventricularseptum and beginning of the aortic sinus wall prolapse at systolewas defined as presumptive true VSD size (Figures 1E–1H).Parasternal long-axis images on transthoracic echocardiographywere used for VSD size measurement; in patients with poor resolu-tion, the long-axis image on transesophageal echocardiography wasused. The degree of AR was assessed by comprehensive Dopplerechocardiographic measurements using jet width, jet cross-sectionalarea in the left ventricular outflow tract, and Doppler tracing of theaortic flow and classified as mild, moderate, or severe.15 Cardiacchamber dimensions and left ventricular ejection fraction weremeasured according to the recommendations of the AmericanSociety of Echocardiography.16
Data Collection and Analysis
A chart review was performed, and the data were collected by us-ing a standardized form that recorded the information regarding
patient demographics, medical history, clinical presentation, resultof imaging studies, and adverse clinical events. Adverse clinicalevents included a composite of open-heart surgery for any cause,including reoperation after the initial surgery in group 3, cardiacdeath, and the development of infective endocarditis.9 Follow-up data were collected by a direct telephone interview and adetailed review of all medical records. The causes and dates ofany deaths were confirmed by information gathered from theNational Population Registry of the Korean National StatisticalOffice, together with a review of all available clinical records atthe time of death. The median follow-up durations were 78months in the sVSD group (interquartile range, 37–137 months)and 71 months in the pmVSD group (interquartile range,39–115 months).
Statistical Analysis
All statistical analyses were performed by using SPSS version 18.0(SPSS, Inc, Chicago, IL). Summary statistics are presented as fre-quencies and percentages or as mean 6 SD. Differences betweentwo groups in terms of continuous variables were tested by using un-paired Student t tests and the Mann-Whitney U test and differencesamong three groups by using analysis of variance and the Tukeymethod for post hoc analysis. The c2 test or Fisher exact test wasused to compare the frequencies of categorical variables betweengroups. Bonferroni correction was used for multiple comparisons.The Spearman rank correlation test was performed to evaluate anassociation between AR severity and the maximal length of the pro-lapsing aortic wall. To determine the cutoff value of the maximallength of the prolapsing aortic wall for predicting the developmentof ASV rupture, a receiver operating characteristic curve was used.To identify factors that were associated with the development of clin-ical events in groups 1 and 2, univariate and multivariate Coxproportional-hazard models were used. In multivariate analysis,VSD type, left atrial size, and left ventricular size were used in thebackward linear regression method. Cumulative survival and event-free survival rate curves were generated with the Kaplan-Meiermethod and compared by using the log-rank test. All P values weretwo sided, and P values < .05 were considered significant.Intraobserver and interobserver variability for the measurement ofVSD size were assessed by Bland-Altman analysis, with interobservervariability by intraclass correlation coefficients between two indepen-dent observers for 20 randomly selected patients. The two indepen-dent observers achieved interobserver variability of 0.92 to 0.98 andintraobserver variability of 0.94 to 0.98.
RESULTS
The baseline characteristics of the patients are summarized inTable 1. Groups 1 and 2 did not differ with regard to age at initialdiagnosis, mean size of the remnant VSD, left ventricular size, orQp/Qs. Compared with group 2, group 1 had a significantly higherprevalence of aortic sinus wall prolapse (P < .0001) and moderate tosevere AR (P = .012). Moderate to severe AR was observed only inthe sVSD group. There was no significant association between ARseverity and the maximal length of the prolapsing aortic sinus wallin the group 1 (r = –0.115, P = .603). The presumptive true VSDsize (6.1 6 4.1 vs 8.7 6 5.6 mm, P = .010) and remnant VSD size(3.5 6 0.9 vs 5.1 6 3.3 mm, P < .001) were larger in group 3compared with group 1. This trend was also observed in patients

Figure 1 Representative transthoracic echocardiographic images (A–D) of sVSDs (arrow) with (A,B) and without (C,D) a prolapsingaortic sinus wall (dotted line). In the magnified images (B,D), the sizes of the remnant VSDs are measured (double-headed arrows).Transesophageal echocardiographic images (E–H) shows how the maximal length of a prolapsing aortic sinus wall (white arrow) andthe presumptive true VSD size (dotted arrow) are measured. Ao, aorta; LA, left atrium; LV, left ventricle; RV, right ventricle.
Table 1 Baseline characteristics of the subjects
Variable Group 1 (n = 60) Group 2 (n = 120) Group 3 (n = 52) P
Age (y) 36.3 6 12.6 36.5 6 14.2 32.2 6 10.9 .127
Men 29 (48.3%) 56 (46.7%) 33 (63.5%) .116
Diabetes 3 (5.0%) 5 (4.2%) 0 (0%) .290
Hypertension 9 (15.0%) 20 (16.7%) 2 (3.8%) .069
Qp/Qs on heart scan 1.35 6 0.15 1.32 6 0.18 1.79 6 0.76* .353
Echocardiographic data
Remnant defect size (mm) 3.5 6 0.9 3.6 6 1.3 5.1 6 3.3 <.001
LV diastolic dimension (mm) 52.2 6 5.9 51.3 6 6.3 56.7 6 8.5* <.001
LA dimension (mm) 37.3 6 5.7 37.7 6 5.9 41.4 6 7.5* <.001
Trans-VSD PG (mm Hg) 117.0 6 32.6 109.5 6 31.2 102.5 6 26.5 .076
RV-RA PG (mm Hg) 22.0 6 5.4 24.3 6 8.5 36.4 6 17.6* <.001
LV ejection fraction (%) 62.3 6 5.8 61.7 6 7.2 61.5 6 7.7 <.001
AR 24 (40.0%) 10 (8.3%)* 39 (75.0%)* <.001
Mild 20 10 28
Moderate 3 0 7Severe 1 0 4
Prolapse of aortic sinus wall 23 (38.3%) 3 (2.5%)* 28 (53.8%) <.001
LA, Left atrial; LV, left ventricular; PG, pressure gradient; RA, right atrium; RV, right ventricular.
Data are expressed as mean 6 SD or number (percentage).
*P < .05 versus group 1.
Journal of the American Society of EchocardiographyVolume 27 Number 9
Cho et al 967
with sVSDs and aortic wall prolapse (10.36 4.0 and 12.86 4.8 mmin groups 1 and 3, respectively, P = .052). Compared with group 1,group 3 showed larger left ventricles and left atria and a higher
prevalence of AR. Sixteen patients underwent additional aorticvalve procedures during initial surgery for sVSDs, with valve repairin nine and replacement in seven patients.

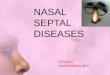
Figure 2 Representative echocardiographic images of a patient with a sVSD before (A–D) and after (E–H) the ASV ruptured. At thetime of the initial diagnosis in 1999, prolapse of the aortic sinus (dotted line in A) wall was present, but there was no evidence of AR oraorta–right ventricular shunt (D). Eleven years later, the patient reported the sudden onset of dyspnea, and echocardiography showeda prominent aneurysmal change (E). Color Doppler flow mapping revealed continuous shunt flow from the aorta to the right ventricle(H) in addition to the shunt through the VSD (G).
968 Cho et al Journal of the American Society of EchocardiographySeptember 2014
During follow-up, ASV rupture into the right ventricle occurred infive patients in group 1 (Figure 2), and urgent surgical correction wasrequired. Three patients in group 1 developed infective endocarditis,which also required open-heart surgery. One patient developed ASVrupture and infective endocarditis simultaneously. Vegetations devel-oped in the right ventricular side of the sVSD in two patients and inthe aortic valve in one patient. The other indication for open-heartsurgery during follow-up was the development of heart failure symp-toms, which occurred in two patients. One of these patients refusedsurgical intervention for severe AR at the time of the initial diagnosis,developed progressive dyspnea, and underwent open-heart surgery.The other patient exhibited a progressive increase in Qp/Qs (from1.4 to 1.6) and a decrease in left ventricular ejection fraction (from66% to 53%) 10 years after diagnosis, and surgery was recommendedbecause of the development of symptoms. None of the patientsunderwent surgery because of progression to severe AR. In group2, two patients underwent open-heart surgery because of infectiveendocarditis and the development of heart failure symptoms.Another two patients with pmVSDs also developed infective endo-carditis and recovered without surgical intervention. None of thepatients in the sVSD group died, whereas four patients in thepmVSD group had noncardiac deaths.
Adverse clinical events occurred more frequently in group 1 (15.0%[nine of 60] vs 3.3% [four of 120], P = .011). Univariate analysisrevealed that VSD type, left atrial size, left ventricular end-diastolicdimension, aortic sinus wall prolapse, and AR were significantlyassociated with the development of adverse clinical events. A multivar-iate Cox proportional-hazard model revealed that sVSD (hazard ratio,
4.55; 95% confidence interval, 1.17–17.74; P = .029) and left atrial size(hazard ratio per millimeter, 1.18; 95% confidence interval, 1.07–1.30;P= .001)were independent risk factors for the development of adverseclinical events. The 12-year adverse event-free survival rate was lowerin the sVSD group (766 9%vs 946 4%, P= .031), but the two groupsdid not differ in 12-year overall survival rate (100% vs 94 6 3%,P = .143; Figure 3).
ASV rupture in the sVSD group developed suddenly, without anypreceding symptoms or signs. Except for one patient, all patientsshowed prominent prolapse of the aortic sinus wall at the time ofthe initial diagnosis, and the duration from the diagnosis of sVSD toASVrupture was longer than the durations from diagnosis to all otherclinical events (median, 142 months [range, 85–165 months] vs 48months [range, 9–120 months]; P = .014). Of 23 patients with aorticsinus wall prolapse at the initial diagnosis, four (17%) developed ASVrupture, whereas only one of 37 patients (3%) without aortic sinuswall prolapse developed ASV rupture (P = .066). ASV rupture wascritically dependent on the maximal length of the prolapsing aorticsinus wall: patients with maximal prolapsing aortic sinus wall length> 7 mm showed a higher frequency of ASV rupture than thosewith no prolapse or maximal prolapsing length # 7 mm (80%[four of five] vs 1.8% [one of 55], P < .001). The positive and negativepredictive values were 80% and 98%, respectively.
During follow-up period, two patients in group 3 died of suddencardiac death and infective endocarditis. The 12-year event-free andoverall survival rates were comparable between groups 1 and 3(Figure 3). Of the nine patients in group 1 who developed adverseclinical events, initial evaluation showed mild, moderate, and severe

Figure 3 Comparison of event-free and overall survival rates between the groups.
Figure 4 Diagrams showing the severity of AR in patients withsVSDs during follow-up with (lower panel, B) and without (upperpanel, A) initial surgery.
Journal of the American Society of EchocardiographyVolume 27 Number 9
Cho et al 969
AR in two, two, and one patient, respectively. Two patients whounderwent open-heart surgery because of progressive dyspneaand did not show any change in AR severity during follow-up.Among five patients who developed ASV rupture, AR progressionwas observed in two (from mild to moderate AR in one patientand from no AR to moderate AR in the other). AR progressionfrom no AR to severe AR happened in one patient who developedinfective endocarditis involving the aortic valve, whereas the otherpatients who developed endocarditis not involving the valve didnot show any AR progression.
Of the 51 patients with sVSDs who did not develop events, follow-up echocardiographic data showing whether the severity of AR hadchanged over time were available for 38 patients (74.5%) duringfollow-up (median follow-up, 86 months; interquartile range,31–140 months). Only two of the patients showed changes in theseverity of AR (Figure 4A). None of the 38 patients developed severeAR during follow-up. Long-term echocardiographic follow-up data(median follow-up, 62 months; interquartile range, 23–106 months)were available in 41 patients (78.8%) in group 3, and three patientsshowed AR progression (Figure 4B), but none underwent the repeatsurgery to control AR. Interestingly, these three patients all underwentaortic valve repair procedures at the time of initial sVSD closuresurgery. The 10-year AR progression-free survival rate was notdifferent between groups 1 and 3 (94 6 5% vs 91 6 5%, P = .301).
DISCUSSION
This retrospective analysis of clinical outcomes of sVSD and pmVSDrevealed that open-heart surgery was more frequently performed dur-ing the watchful monitoring of adult patients with sVSDs than duringthe watchful monitoring of adult patients with pmVSDs. However, asdiscussed in more detail below, these events did not develop asfrequently in adolescent or adult patients with sVSDs as in pediatricpatients with sVSDs. Moreover, these events did not translate directlyinto excess mortality; indeed, the overall survival rates were excellent.
AR progression was rare, and ASV rupture and infective endocarditiswere the main causes that necessitated surgical intervention. Ruptureof the ASV was the most frequent clinical event and was associatedwith prolapse of the aortic sinus wall through the sVSD. It was foundto be critically dependent on the maximal length of the prolapsingwall. Thus, watchful waiting and closemonitoring of patients with thesehigh-risk echocardiographic features can be a rational managementoption for adult patients with sVSDs.
Natural History of sVSD: Age, Defect Size, and OtherEchocardiographic Findings
Supporting the idea of early or prophylactic surgery in patients withsVSDs is that longer durations from the onset of AR to surgical

970 Cho et al Journal of the American Society of EchocardiographySeptember 2014
intervention are associated with persistent AR after repair surgery.8
However, other investigators have not found that surgery performedbefore the onset of AR is beneficial.17,18 Moreover, the clinical factorsthat determine the development of these serious aortic complicationshave not been investigated fully.
The currently available data regarding the natural history of sVSDare based on retrospective analyses of pediatric patients. These ana-lyses show that the prevalence rates of aortic wall prolapse and ARincrease gradually in a linear fashion as the age of the patientincreases5 and that >80% of pediatric patients with sVSDs neededsurgical intervention, with a high rate of AR progression duringfollow-up.5,9 These findings differ markedly from our finding thatadolescent or adults with sVSD who were followed conservativelyhad a frequency of surgical intervention of 15% (nine of 60) andnegligible AR progression.
Two possible answers may explain this large difference. VSD sizecould be an important factor determining the prognosis: the defectsobserved in our group 1 were <5 mm in size (3.5 6 0.9 mm),whereas the largest series of pediatric patients with sVSDs to datehas shown that 82% (176 of 214) had sVSDs defect that were$5 mm in size, with significantly larger Qp/Qs values.9 Because theamount of shunt during systole is believed to be an important hemo-dynamic factor that contributes to the progression of the syndrome ofsVSD and AR,2 it is conceivable that the small defects seen in adultsare more likely to be associated with a lower incidence of aortic com-plications. Supporting the prognostic value of defect size is that someinvestigators have recommended that even young asymptomaticpatients with small defects (<5 mm) can be managed conservatively.9
However, it is also well known that sVSD should be restrictive withregard to the development of prolapse of the adjacent aortic sinuswall and AR. The Venturi effect is believed to be the predominantmechanism behind aortic valve cusp deformity and subsequentAR,19,20 a notion that is supported by the finding that pediatricpatients with sVSDs and AR syndrome are nearly always older andseldom have congestive heart failure episodes in infancy, which arecharacteristic of large VSD. The average Qp/Qs of patients withthis syndrome is <2, and pulmonary artery pressures are at mostonly mildly elevated.20 Thus, the VSD must be restrictive but of suf-ficient size to produce aortic valve cusp distortion.
The other explanation for the difference between adult and pedi-atric patients with sVSDs in terms of surgery and AR progressionrates relates to the normal growth pattern of the aorta. The aortaand cardiac chambers grow in unison and at a predictable rate afterbirth: their dimensions at birth are 50% of those in adulthood, andthis rises to 75% at 5 years of age and 90% at 12 years of age. Afterpuberty, the growth rate slows even further, with significant in-creases no longer seen after 15 years of age.10 Several studies alsoshow that the cumulative development of aortic complications inpediatric patients with sVSDs is age dependent.4,6,9 Notably, afollow-up echocardiographic study revealed that 65% (17 of 26)of neonates or young infants with sVSDs who did not exhibit ARsubsequently developed AR,5 which suggests that AR in associationwith sVSD is an acquired lesion.20 Moreover, several studies suggestthat the peak age for aortic wall prolapse is about 7 years, while thepeak age for AR is between 5 and 10 years.6,21-23 All of thesefindings suggest strongly that the normal rapid growth of the aortaand cardiac chambers in the childhood or infancy plays a criticalrole in the development of aortic complications in sVSD. Becauseprogressive aortic enlargement is expected to occur mainly duringchildhood, this could explain why patients with sVSDs tend todevelop aortic complications in childhood. Thus, our findings
support the notion that not only VSD size but also age is animportant clinical variable that determines the development ofaortic complications and the prognosis of patients with sVSDs.
ASV Rupture versus AR Progression
ASV rupture is another well-known aortic complication of sVSD, andsVSD is the most common underlying disease associated with thedevelopment of ASVrupture.24-26 According to one large-scale study,the incidence of ASV in pediatric patients with sVSDs was less thanhalf that of aortic valve prolapse and AR in patients with sVSDs(9.1% [36 of 395] vs 24.1% [95 of 395]).4 Thus, ASV rupture hasnot been described as an important complication in pediatric patientswith sVSDs. However, in the present study, it was the most commoncause of late surgery, and none of our patients underwent surgery forAR progression alone. This apparent discrepancy can again be ex-plained by the different peak age of these complications: prolapseand regurgitation of the aortic valve develop most frequently be-tween 5 and 8 years of age, whereas ASV is not found before theage of 10 years, only begins to develop during the teenage years,and is most frequently diagnosed in patients aged >20 years.4 Thus,the development of adverse clinical events associated with aorticcomplications in patients with sVSDs is highly dependent on patientage. Our finding showing a close relationship between ASV ruptureand the maximal prolapsing aortic sinus wall length at the initial diag-nosis reinforces the prognostic implication of echocardiographic find-ings. However, because of its retrospective study setting and relativelysmall number of patients with ASV rupture, we could not concludethat prophylactic surgery would be beneficial for selected patientswith aortic sinus wall prolapse. Further study is necessary to deter-mine the indication for surgery for patients with sVSDs and aorticsinus wall prolapse to prevent ASV rupture.
Limitations
This was an observational study at a single center, which lends itself topotential bias. Lack of established guidelines for the management ofadolescent and adult patients with sVSDs contributed to inhomoge-neity of surgical indications for patients with sVSD and baseline differ-ences between groups in our study, which might affect the long-termoutcomes. This, together with the fact that Asians and Caucasiansdiffer in the relative incidence of sVSD, means that the findings ofthe present study should be generalized with caution. The patientswho did not visit our institution after the first visit were excludedfrom analysis, and follow-up echocardiographic data were not avail-able in all of the patients who did not show clinical events. Thus,the frequency with which significant AR developed may have beenunderestimated. However, because events such as hospital admission,mortality, and surgery could be assessed in all study subjects, webelieve our main findings are valid despite these limitations.Because those excluded from analysis had comparable age, Qp/Qs,prevalence of AR, and sinus wall prolapse, we may expect a similarfavorable prognosis.
CONCLUSIONS
Clinical outcomes of adolescent and adult patients with sVSDs are char-acterized by low complication rates and different patterns of complica-tion development. Older patients with sVSDs are at risk for ASVrupture, which is higher than the risk for AR progression. A strong asso-ciation is present between ASV rupture and aortic sinus wall prolapse.

Journal of the American Society of EchocardiographyVolume 27 Number 9
Cho et al 971
The role of prophylactic surgery for patients at high risk (maximalprolapsing aortic sinus wall length > 7 mm) needs to be clarified.
REFERENCES
1. Soto B, Becker AE, Moulaert AJ, Lie JT, Anderson RH. Classification ofventricular septal defects. Br Heart J 1980;43:332-43.
2. YacoubMH, Khan H, Stavri G, Shinebourne E, Radley-Smith R. Anatomiccorrection of the syndrome of prolapsing right coronary aortic cusp,dilatation of the sinus of Valsalva, and ventricular septal defect. J ThoracCardiovasc Surg 1997;113:253-61.
3. Plauth WH, Braunwald E, Rockoff SD, Mason DT, Morrow AG. Ventricu-lar septal defect and aortic regurgitation. Am J Med 1965;39:552-67.
4. Momma K, Toyama K, Atsuyoshi T, Ando M, Nakazawa M, Hirosawa K,et al. Natural history of subarterial infundibular ventricular septal defect.Am Heart J 1984;108:1312-7.
5. Schmidt KG, Cassidy SC, Silverman NH, Stanger P. Doubly committedsubarterial ventricular septal defect: echocardiographic features and surgi-cal implications. J Am Coll Cardiol 1988;12:1538-46.
6. Tohyama K, Satomi G, Momma K. Aortic valve prolapse and aortic regur-gitation associated with subpulmonic ventricular septal defect. Am J Car-diol 1997;79:1285-9.
7. Hitchcock JF, Suijker WJL, Ksiezycka E, Harinck E, van Mill GJ, Ruzyllo W,et al. Management of ventricular septal defect with associated aortic regur-gitation. Ann Thorac Surg 1991;52:70-3.
8. Komai H, Naito Y, Fujiwara K, Noguchi Y, Nishimura Y, Uemura S. Surgi-cal strategy for doubly committed subarterial ventricular septal defect withaortic cusp prolapse. Ann Thorac Surg 1997;64:1146-9.
9. Lun KS, Li H, Leung MP, Yung TC, Chiu CSW, Cheung YF. Analysis ofindications for surgical closure of subarterial ventricular septal defectwithout associated aortic cusp prolapse and aortic regurgitation. Am J Car-diol 2001;87:1266-70.
10. Nidorf SM, Picard MH, Triulzi MO, Thomas JD, Newell J, King ME, et al.New perspectives in the assessment of cardiac chamber dimensions duringdevelopment and adulthood. J Am Coll Cardiol 1992;19:983-8.
11. Backer CL, Winters RC, Zales VR, Takami H, Muster AJ, BensonW Jr, et al.Restrictive ventricular septal defect: how small is too small to closure? AnnThorac Surg 1993;56:1014-9.
12. Santini F, MazzuccoA. Timing of surgical closure of subpulmonary ventric-ular septal defect in infancy. Am J Cardiol 1997;80:976-7.
13. Griffin ML, Sullivan ID, Anderson RH, Macartney FJ. Doubly committedsubarterial ventricular septal defect: newmorphological criteria with echocar-diographic and angiocardiographic correlation. Br Heart J 1988;59:474-9.
14. Van Praagh R, Geva T, Kreutzer J. Ventricular septal defect: how shallwe describe, name and classify them? J Am Coll Cardiol 1989;14:1298-9.
15. Zoghbi WA, Enriquez-Sarano M, Foster E, Grayburn PA, Kraft CD,Levine RA, et al. Recommendations for evaluation of the severity of nativevalvular regurgitation with two-dimensional and Doppler echocardiogra-phy. J Am Soc Echocardiogr 2003;16:777-802.
16. Lang RM, Bierig M, Devereux RB, Flachskampf FA, Foster E, Pellikka PA,et al. Recommendations for chamber quantification: a report from theAmerican Society of Echocardiography’s Guidelines and Standards Com-mittee and the Chamber Quantification Writing Group, developed inconjunctionwith the European Association of Echocardiography, a branchof the European Society of Cardiology. J Am Soc Echocardiogr 2005;18:1440-63.
17. Keane JF, PlauthWH,Nadas AS. Ventricular septal defect with aortic regur-gitation. Circulation 1977;56(Suppl I):I-72-7.
18. Karpawich PP, Duff DF, Mullins CE, Cooley DA, McNamara DG. Ventric-ular septal defect with associated aortic valve insufficiency: progression ofinsufficiency and operative results in young children. J Thorac CardiovascSurg 1981;82:182-9.
19. Tatsuno K, Konno S, Ando M, Sakakibara S. Pathogenetic mechanisms ofprolapsing aortic valve and aortic regurgitation associated with ventricularseptal defect: anatomical, angiographic, and surgical considerations. Circu-lation 1973;48:1028-37.
20. Tweddel JS, Pelech AN, Frommelt PC. Ventricular septal defect and aorticvalve regurgitation: pathophysiology and indications for surgery. SeminThorac Cardiovasc Surg Pediatr Card Surg Ann 2006;9:147-52.
21. Lue HC, Sung TC, Hou SH, Wu MH, Cheng SJ, Chu SH, et al. Ventricularseptal defect in Chinese with aortic valve prolapse and aortic regurgitation.Heart Vessels 1986;2:111-6.
22. Mori K, Matsuoka S, Tatara K, Hayabuchi Y, Nii M, Kuroda Y. Echocardio-graphic evaluation of the development of aortic valve prolapse in supra-cristal ventricular septal defect. Eur J Pediatr 1995;154:176-81.
23. Chiu SN, Wang JK, Lin MT, Wu ET, Lu FL, Chang CI, et al. Aortic valveprolapse associated with outlet-type ventricular septal defect. Ann ThoracSurg 2005;79:1366-71.
24. Chu SH, Hung CR, How SS, Chang H, Wang SS, Tsai CH, et al. Rupturedaneurysms of the sinus of Valsalva in Oriental patients. J Thorac Cardio-vasc Surg 1990;99:288-98.
25. Choudhary SK, Bhan A, Sharma R, Airan B, Kumar AS, Venugopal P.Sinus of Valsalva aneurysms: 20 years’ experience. J Card Surg 1997;12:300-8.
26. Jung SH, Yun TJ, Im YM, Park JJ, Song H, Lee JW, et al. Ruptured sinus ofValsalva aneurysm: transaortic repair may cause sinus of Valsalva distor-tion and aortic regurgitation. J Thorac Cardiovasc Surg 2008;135:153-8.