Embed Size (px)
Citation preview
Cardiac dysfunctionFocus on echocardiographic assessment
Drude Fugelseth
Professor/Consultant
Institute of Clinical Medicine,
University of Oslo
Dept. of Neonatal Intensive Care,
Oslo University Hospital, Ullevål
Oslo, Norway
Cardiac dysfunction in newborn infants
• Normal cardiac-/myocardial function
• Maturation of the myocardium
• Etiology of cardiac dysfunction in neonates
• Echocardiographic assessment of cardiac dysfunction in neonates
– cavity measurements
– longitudinal and regional ventricular wall measurements
• Summary/Conclusion
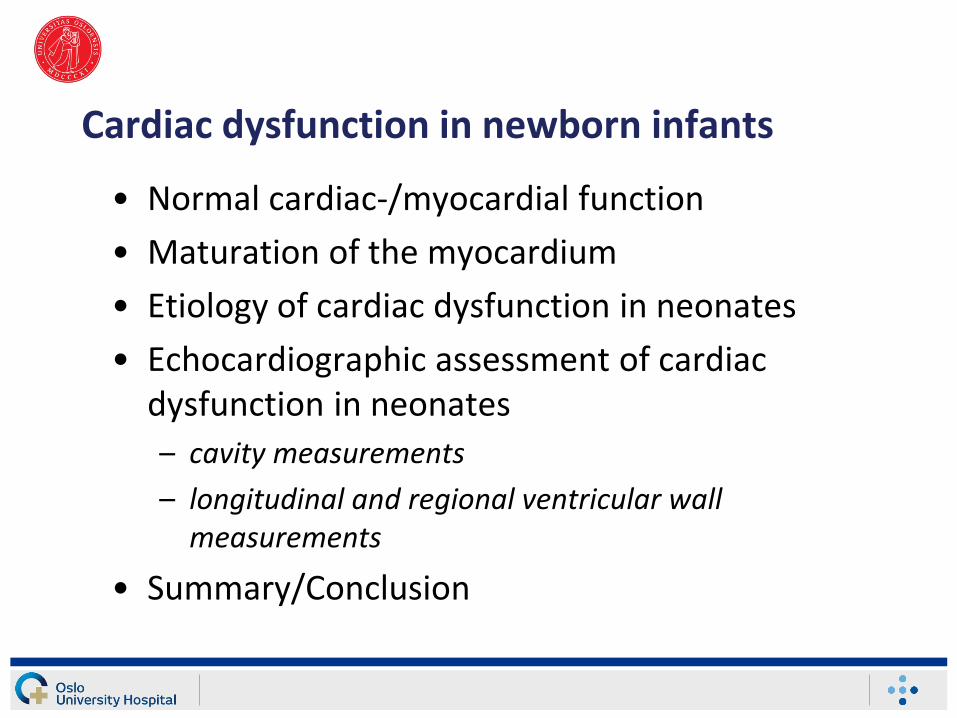
Normal cardiac functionNecessary for adequate macrocirculation
Blood- and oxygen-supply to all organ systems
Cardiac output and blood pressure
Sufficient to supply organs on higher level than the heart
Sufficient during physical work
Contractility Preload Afterload
HR SV
CO
TPR
BP
SVHR
CO
BP
SVR
+-
HR (heart rate)
SV (stroke volume)
CO (cardiac output)
SVR (systemic vascular resistance)
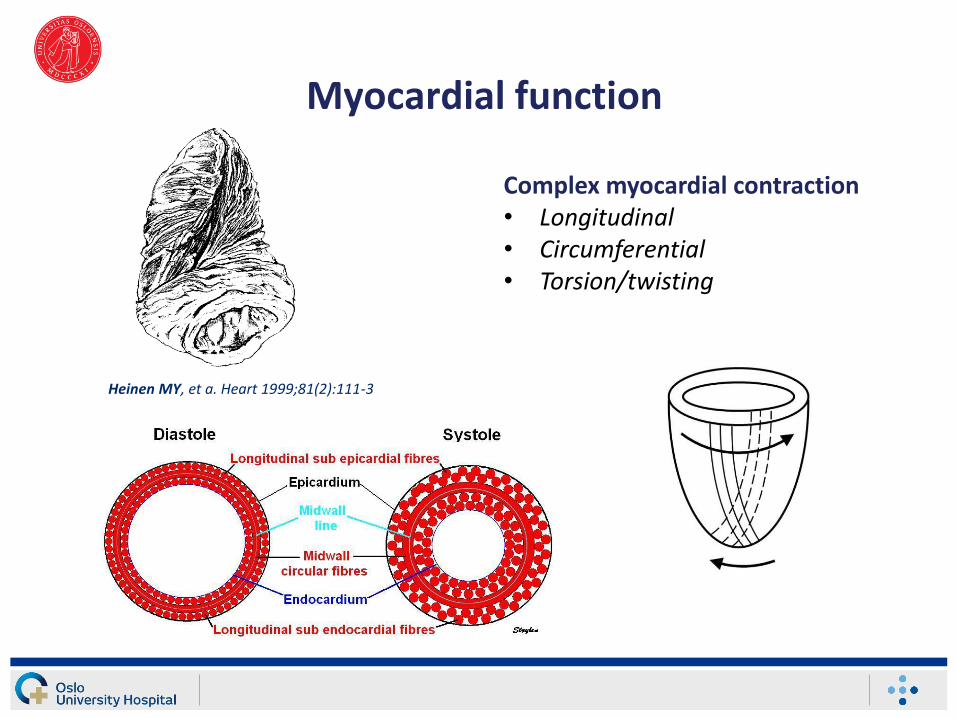
Myocardial function
Complex myocardial contraction• Longitudinal • Circumferential • Torsion/twisting
Heinen MY, et a. Heart 1999;81(2):111-3
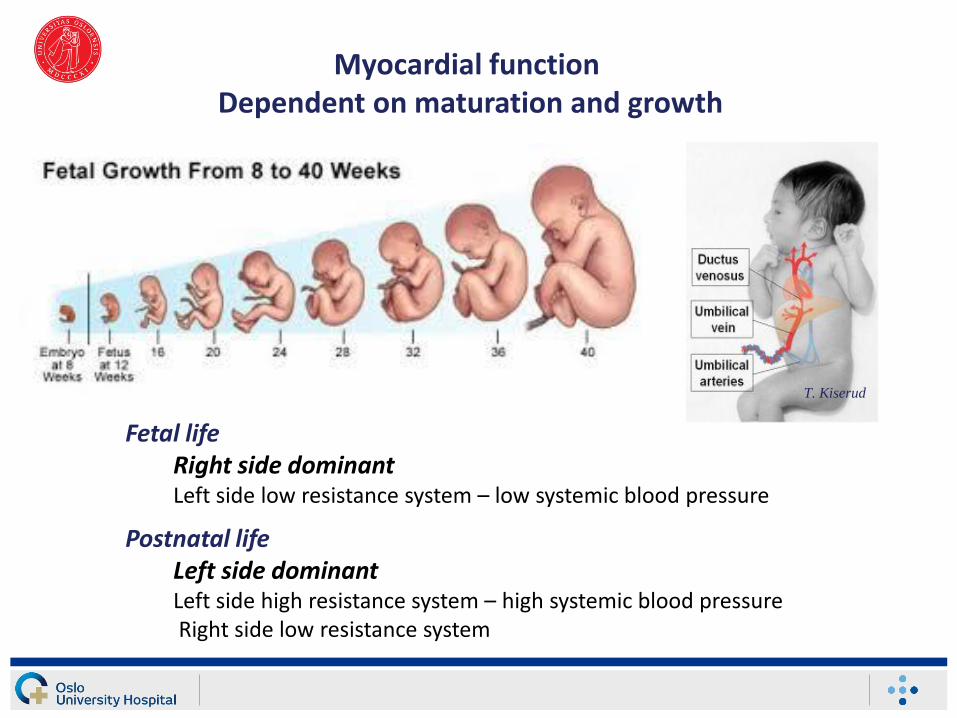
Myocardial function Dependent on maturation and growth
T. Kiserud
Fetal lifeRight side dominantLeft side low resistance system – low systemic blood pressure
Postnatal lifeLeft side dominant Left side high resistance system – high systemic blood pressureRight side low resistance system
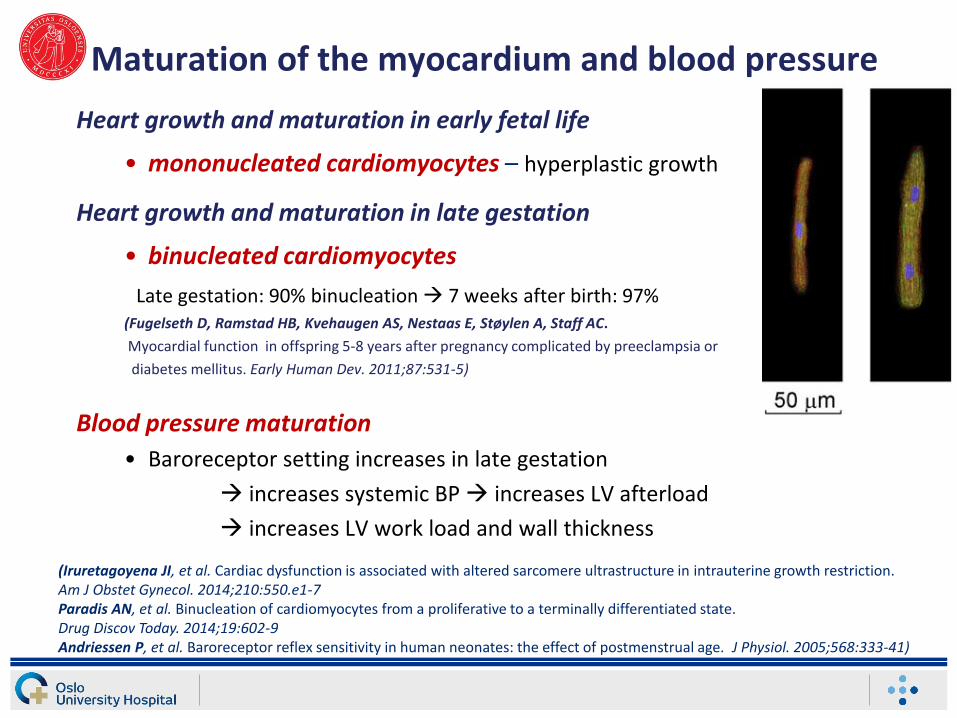
Maturation of the myocardium and blood pressure
Heart growth and maturation in early fetal life
• mononucleated cardiomyocytes – hyperplastic growth
Heart growth and maturation in late gestation
• binucleated cardiomyocytes
Late gestation: 90% binucleation 7 weeks after birth: 97%(Fugelseth D, Ramstad HB, Kvehaugen AS, Nestaas E, Støylen A, Staff AC.
Myocardial function in offspring 5-8 years after pregnancy complicated by preeclampsia or
diabetes mellitus. Early Human Dev. 2011;87:531-5)
Blood pressure maturation
• Baroreceptor setting increases in late gestation
increases systemic BP increases LV afterload
increases LV work load and wall thickness
(Iruretagoyena JI, et al. Cardiac dysfunction is associated with altered sarcomere ultrastructure in intrauterine growth restriction.Am J Obstet Gynecol. 2014;210:550.e1-7Paradis AN, et al. Binucleation of cardiomyocytes from a proliferative to a terminally differentiated state. Drug Discov Today. 2014;19:602-9Andriessen P, et al. Baroreceptor reflex sensitivity in human neonates: the effect of postmenstrual age. J Physiol. 2005;568:333-41)
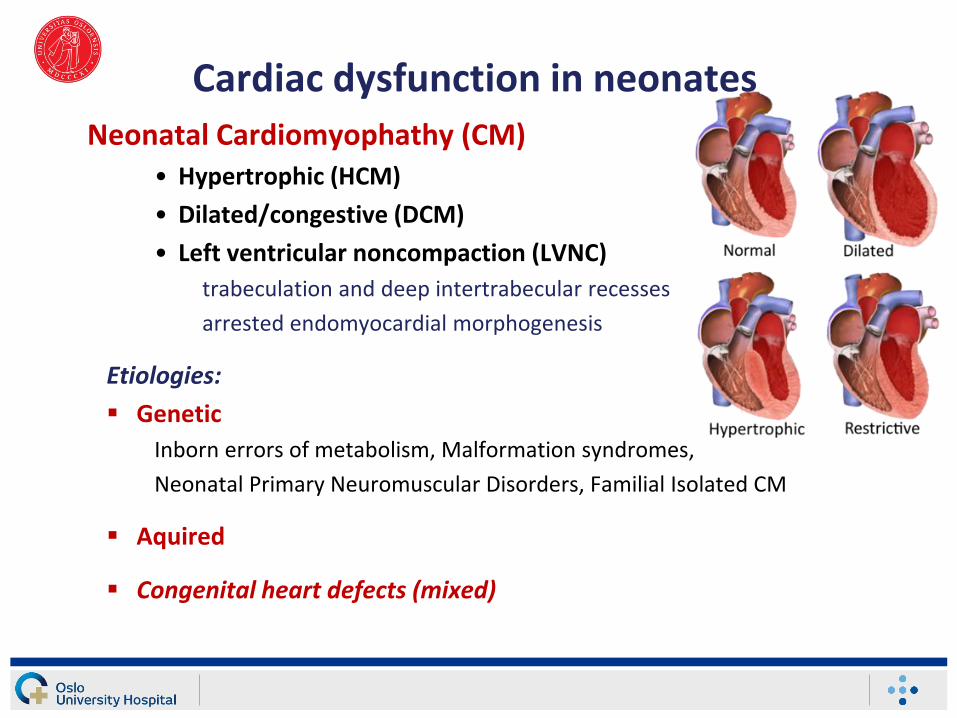
Cardiac dysfunction in neonates
Neonatal Cardiomyophathy (CM) • Hypertrophic (HCM)
• Dilated/congestive (DCM)
• Left ventricular noncompaction (LVNC)
trabeculation and deep intertrabecular recesses
arrested endomyocardial morphogenesis
Etiologies:
Genetic
Inborn errors of metabolism, Malformation syndromes,
Neonatal Primary Neuromuscular Disorders, Familial Isolated CM
Aquired
Congenital heart defects (mixed)
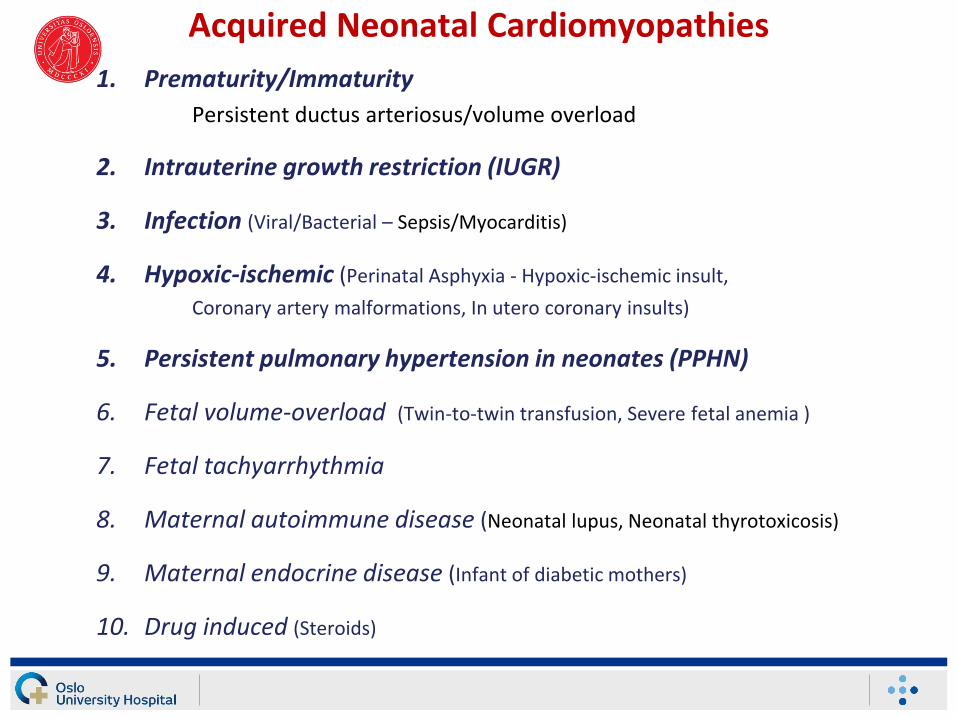
Acquired Neonatal Cardiomyopathies
1. Prematurity/Immaturity
Persistent ductus arteriosus/volume overload
2. Intrauterine growth restriction (IUGR)
3. Infection (Viral/Bacterial – Sepsis/Myocarditis)
4. Hypoxic-ischemic (Perinatal Asphyxia - Hypoxic-ischemic insult,
Coronary artery malformations, In utero coronary insults)
5. Persistent pulmonary hypertension in neonates (PPHN)
6. Fetal volume-overload (Twin-to-twin transfusion, Severe fetal anemia )
7. Fetal tachyarrhythmia
8. Maternal autoimmune disease (Neonatal lupus, Neonatal thyrotoxicosis)
9. Maternal endocrine disease (Infant of diabetic mothers)
10. Drug induced (Steroids)
Assessment of cardiac dysfunction in neonates
Neonatologist performed echocardiography (NPE)
Most evident scenarios for recommending functional
echocardiography in neonates are:
• The transitional circulation period in very premature infants
• Assessment of PDA beyond the early transitional period
• To explore the reasons for circulatory compromise and hypotension
• To diagnose and follow treatment for PPHN
In all situations the exclusion of congenital heart defects are of considerable importance
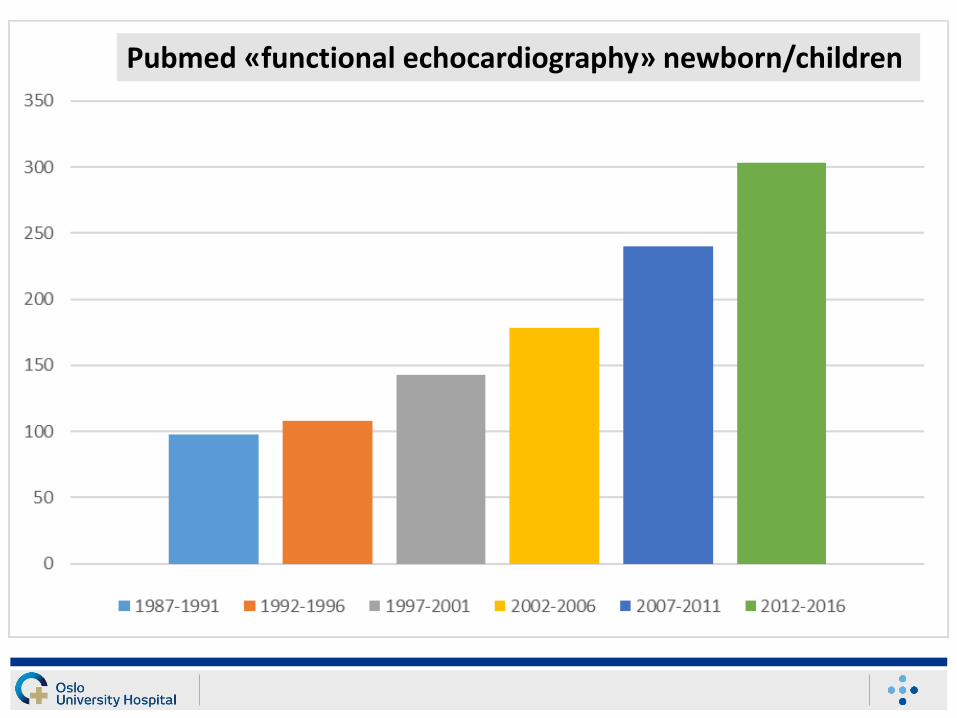
Pubmed «functional echocardiography» newborn/children
Pediatric Research 2016
Echocardiographic assessment of Cardiac dysfunction in neonates
Blood flow measurements
• Cardiac output(RVCO/LVCO)
• Cardiac input (SVC)
Cavity measurements• Dimensional and
volume changes
Time indices
• Tei index
Global longitudinal wallmeasurements• AV-plane excursion/displacement
and strain
• AV-plane velocity and strain rate
Regional wall measurements• Longitudinal strain and strain rate
• Circumferential strain and strain rate
• Radial strain and strain rate
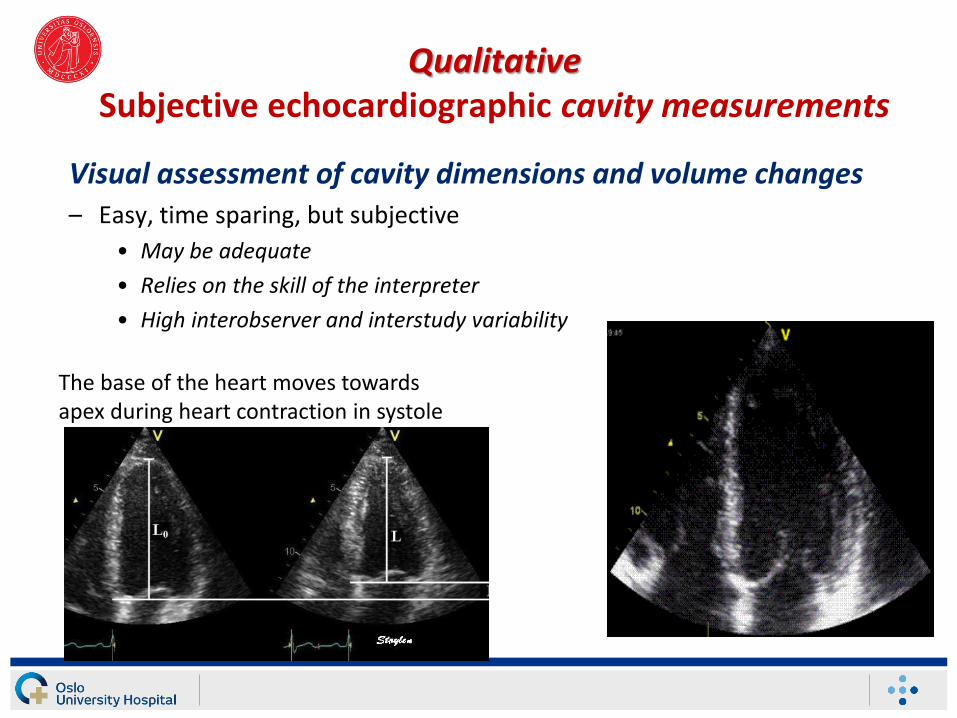
QualitativeSubjective echocardiographic cavity measurements
Visual assessment of cavity dimensions and volume changes– Easy, time sparing, but subjective
• May be adequate
• Relies on the skill of the interpreter
• High interobserver and interstudy variability
The base of the heart moves towards apex during heart contraction in systole
Quantitative echocardiographic cavity assessments
• Cavity changes measurements – One-dimensional (1D), 2D or 3D echocardiographic parameters
– End-diastole• frame after mitral valve closure / the largest LV-dimension or volume
– End-systole• frame after aortic valve closure / smallest dimension or volume
• Fractional shortening (FS)
• Ejection fraction (EF)
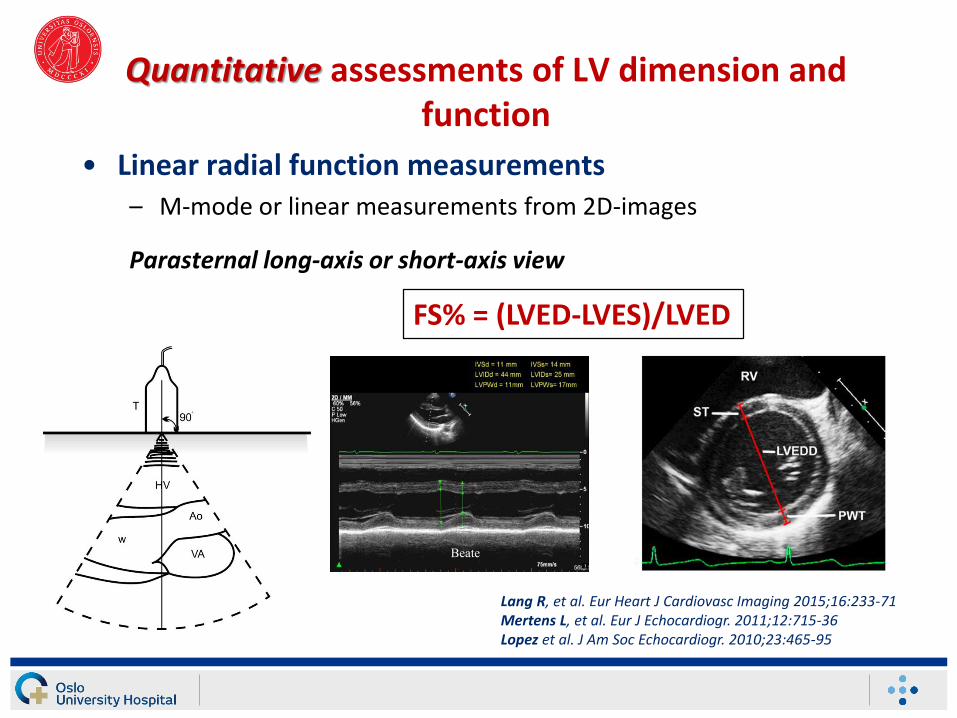
Quantitative assessments of LV dimension and function
• Linear radial function measurements– M-mode or linear measurements from 2D-images
Parasternal long-axis or short-axis view
Lang R, et al. Eur Heart J Cardiovasc Imaging 2015;16:233-71Mertens L, et al. Eur J Echocardiogr. 2011;12:715-36Lopez et al. J Am Soc Echocardiogr. 2010;23:465-95
Beate
FS% = (LVED-LVES)/LVED
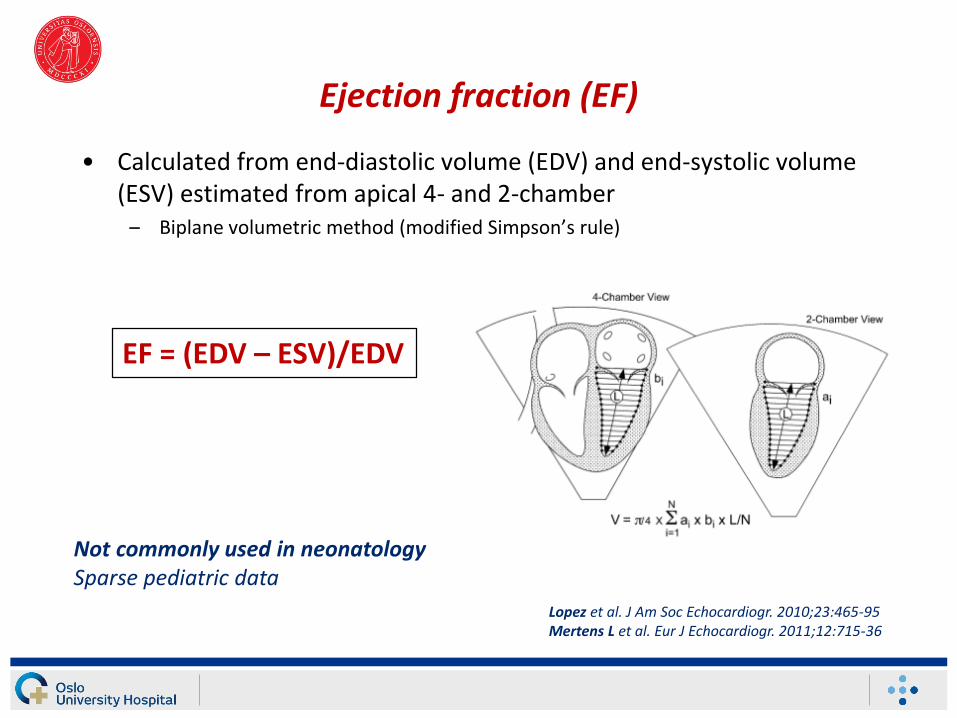
Ejection fraction (EF)
• Calculated from end-diastolic volume (EDV) and end-systolic volume (ESV) estimated from apical 4- and 2-chamber
– Biplane volumetric method (modified Simpson’s rule)
Not commonly used in neonatologySparse pediatric data
EF = (EDV – ESV)/EDV
Lopez et al. J Am Soc Echocardiogr. 2010;23:465-95Mertens L et al. Eur J Echocardiogr. 2011;12:715-36
Echocardiographic measurements of cardiac function
Global longitudinal wall measurements• AV-plane excursion/displacement and strain
MAPSE/TAPSE
Colour TDI (cTDI)
Global longitudinal strain by TDI/STE
• AV-plane velocity and strain ratePulse wave TDI/cTDI
Global longitudinal strain rate (TDI/STE)
Regional wall measurements
• Longitudinal strain and strain rate
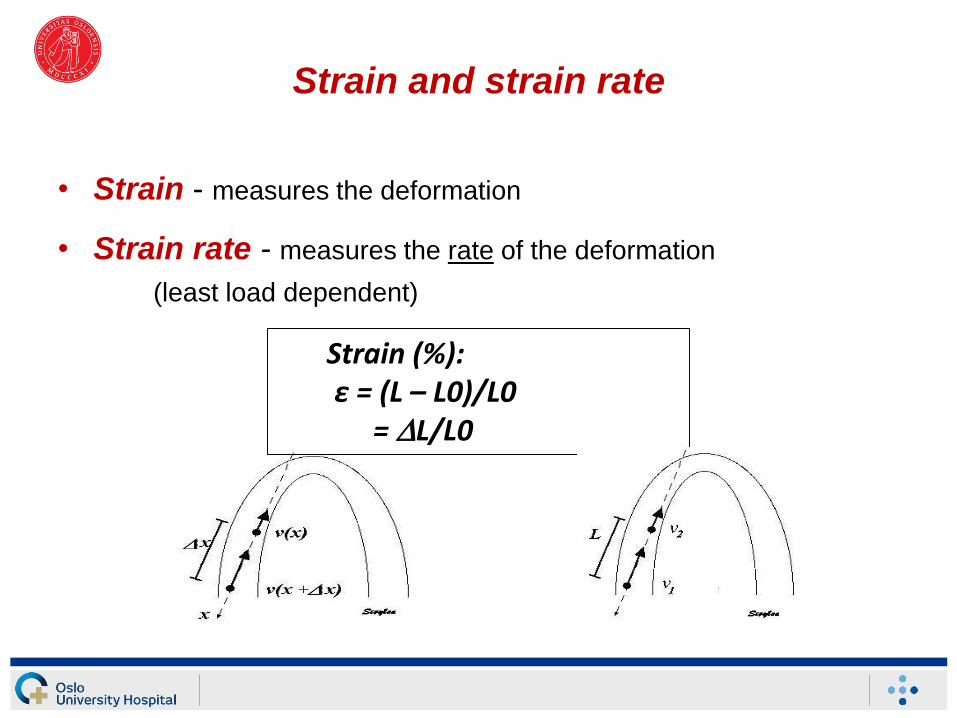
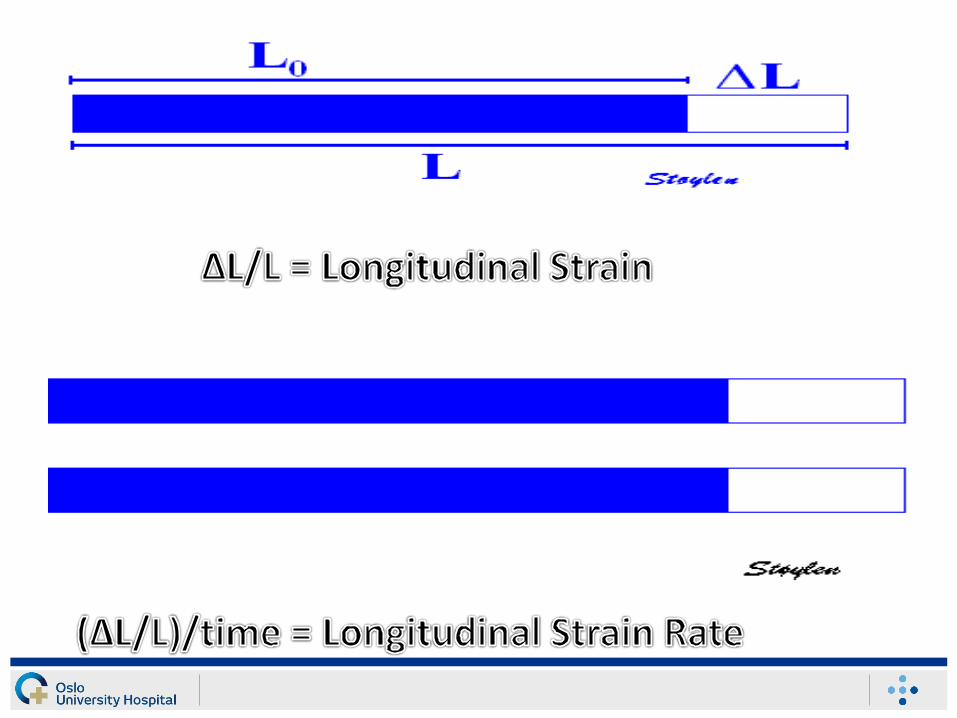
Strain and strain rate
• Strain - measures the deformation
• Strain rate - measures the rate of the deformation
(least load dependent)
Strain (%): ε = (L – L0)/L0
= L/L0
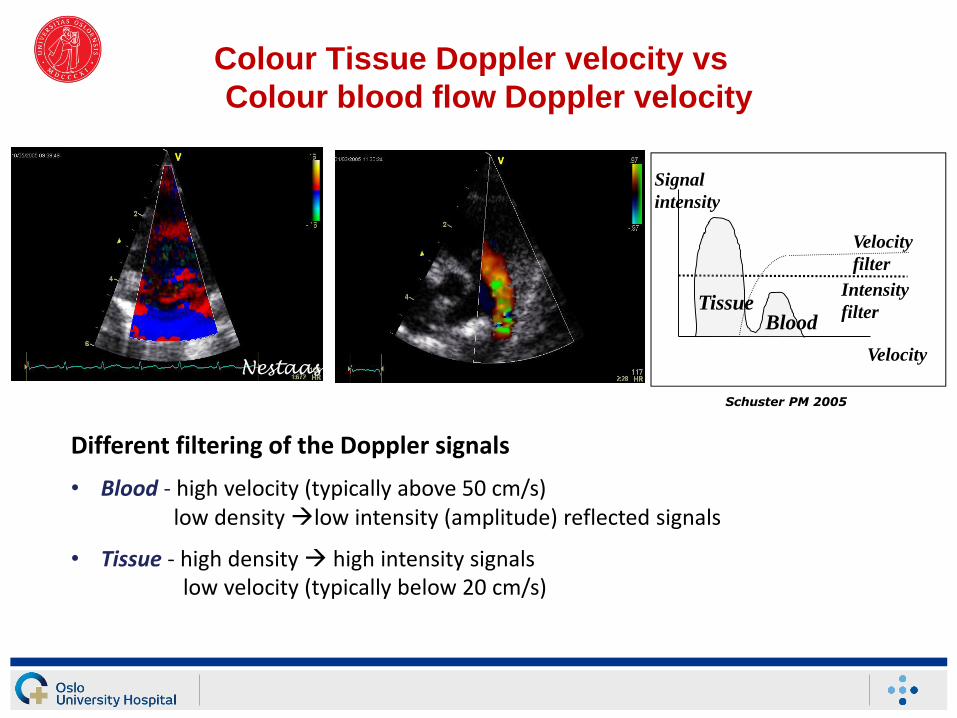
Colour Tissue Doppler velocity vs
Colour blood flow Doppler velocity
Different filtering of the Doppler signals
• Blood - high velocity (typically above 50 cm/s) low density low intensity (amplitude) reflected signals
• Tissue - high density high intensity signalslow velocity (typically below 20 cm/s)
Signal
intensity
Velocity
Intensity
filter
Velocity
filter
Tissue Blood
Schuster PM 2005
Nestaas
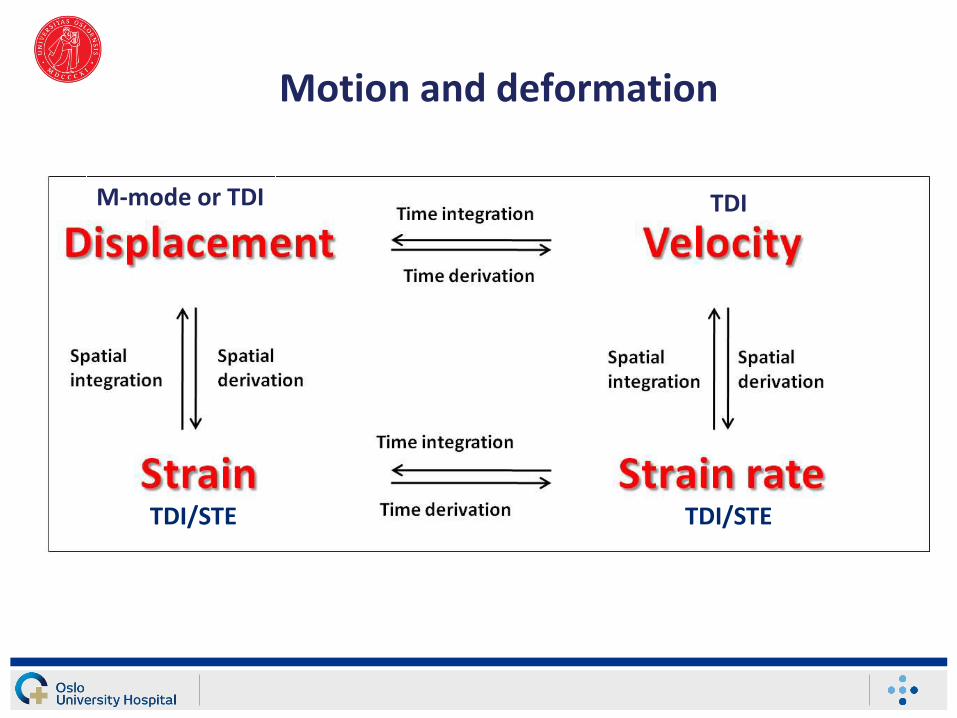
Motion and deformation
M-mode or TDI TDI
TDI/STE TDI/STE
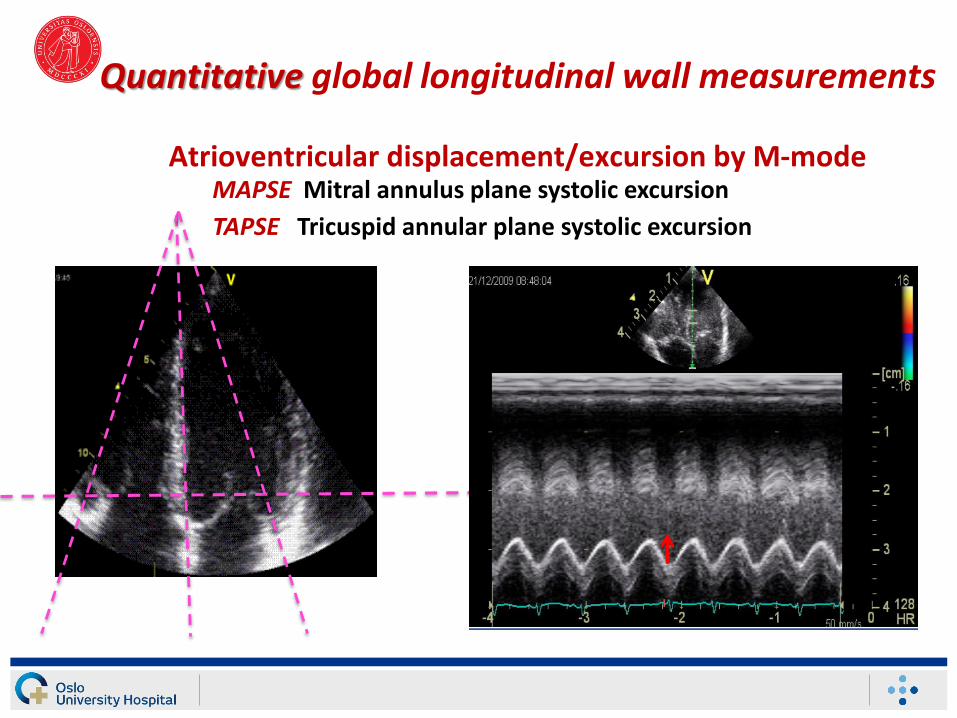
Quantitative global longitudinal wall measurements
Atrioventricular displacement/excursion by M-modeMAPSE Mitral annulus plane systolic excursion
TAPSE Tricuspid annular plane systolic excursion
MAPSE and TAPSEGlobal longitudinal wall measurements
• Koestenberger M, et al. Longitudinal systolic left ventricular function in preterm and term neonates: reference values of the mitral annular plane systolic excursion (MAPSE) and calculation of z-scores. Pediatr Cardiol. 2015;36:20-6
• Jain A, et al. A comprehensive Echocardiographic Protocol for Assessing Neonatal Right Ventricular Dimensions and Function in the Transitional Period: Normative Data and Z Scores. J Am Soc Echocardiogr. 2014;27:1293-304
• Grangl G, et al. Tricuspid Annular Plane Systolic Excursion Is Reduced in Infants with Pulmonary Hypertension. Echocardiography. 2015;32:883-4
• Eriksen BH, Nestaas E, Hole T, Liestøl K, Støylen A, Fugelseth D. Longitudinal assessment of atrioventricular annulus excursion by grey-scale m-mode and colour tissue Doppler imaging in premature infants. Early Hum Dev. 2013;89:977-82
• Eriksen BH, Nestaas E, Hole T, Liestøl K, Støylen A, Fugelseth D. Myocardial function in term and preterm infants. Influence of heart size, gestational age and postnatal maturation. Early Hum Dev. 2014;90: 359-64
GA, postnatal age and heart size have to be taken into consideration when assessing indices of myocardial function in infants
References in newborn infants
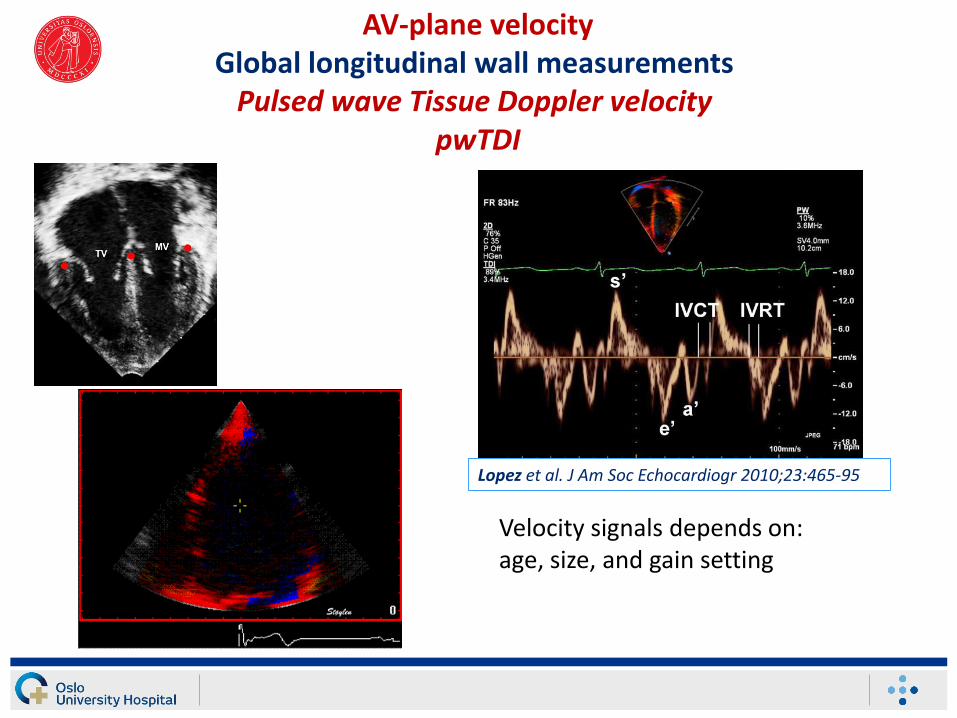
AV-plane velocityGlobal longitudinal wall measurements
Pulsed wave Tissue Doppler velocity pwTDI
Velocity signals depends on: age, size, and gain setting
Lopez et al. J Am Soc Echocardiogr 2010;23:465-95
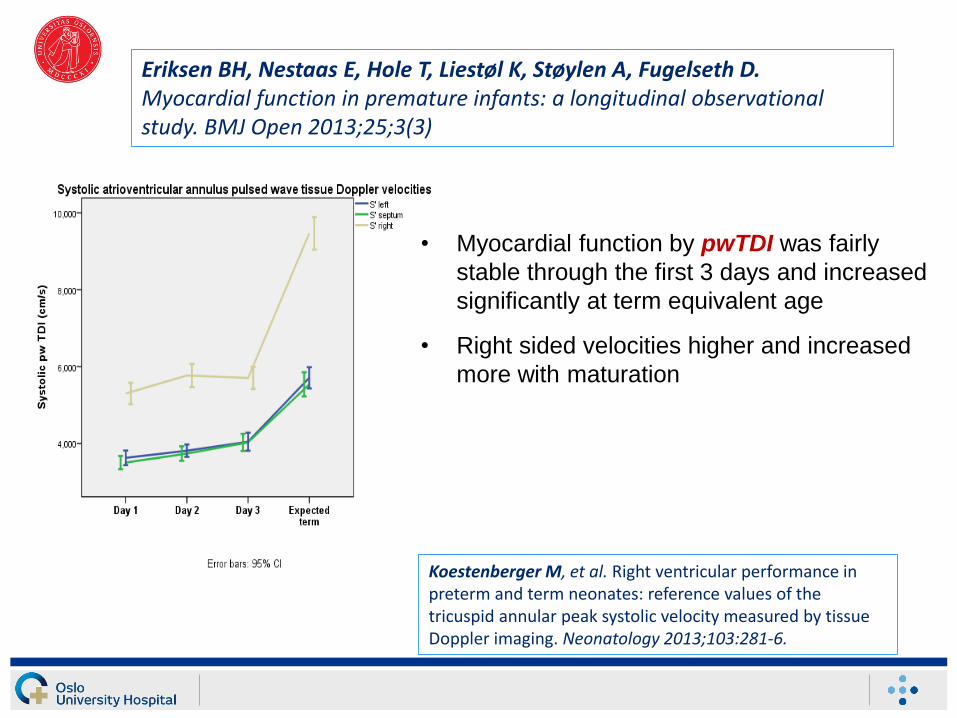
• Myocardial function by pwTDI was fairly
stable through the first 3 days and increased
significantly at term equivalent age
• Right sided velocities higher and increased
more with maturation
Koestenberger M, et al. Right ventricular performance in preterm and term neonates: reference values of the tricuspid annular peak systolic velocity measured by tissue Doppler imaging. Neonatology 2013;103:281-6.
Eriksen BH, Nestaas E, Hole T, Liestøl K, Støylen A, Fugelseth D. Myocardial function in premature infants: a longitudinal observational study. BMJ Open 2013;25;3(3)
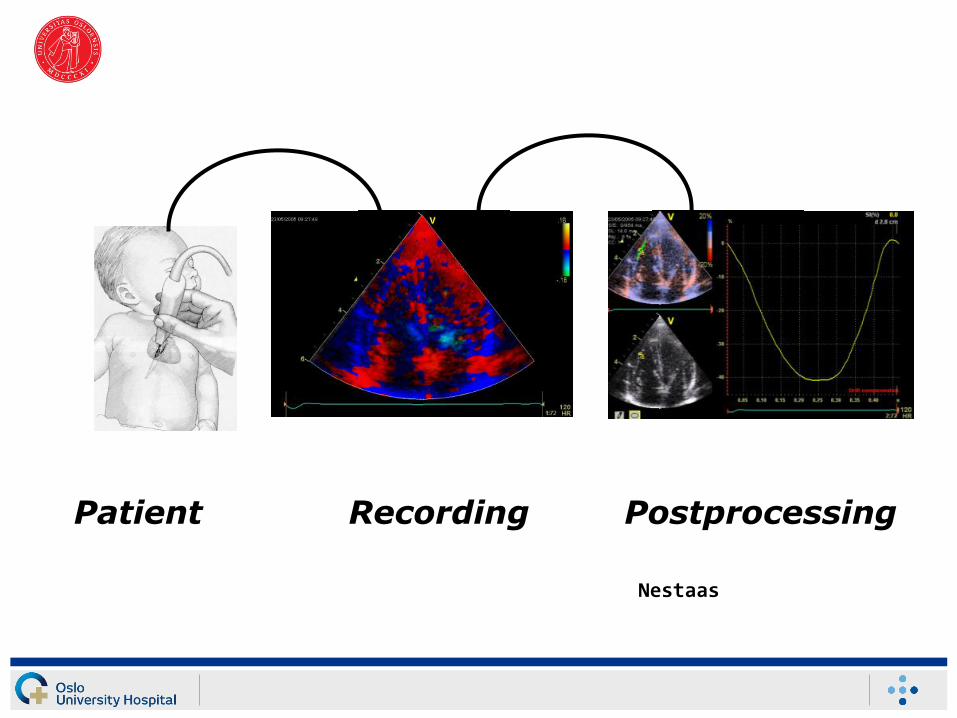
Nestaas
Recording PostprocessingPatient
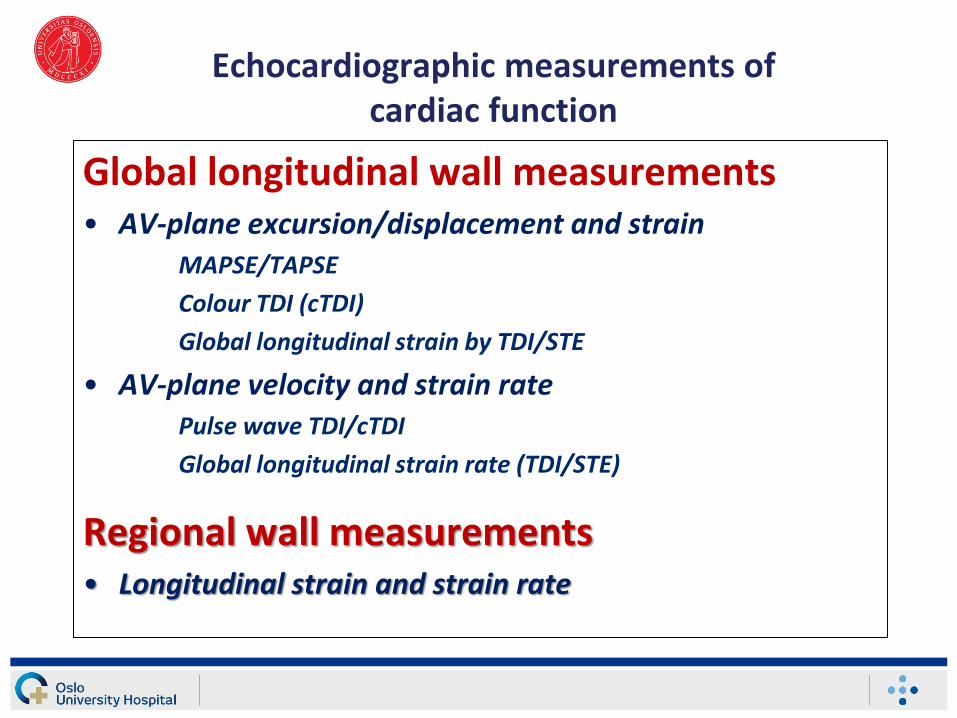
Echocardiographic measurements of cardiac function
Global longitudinal wall measurements• AV-plane excursion/displacement and strain
MAPSE/TAPSE
Colour TDI (cTDI)
Global longitudinal strain by TDI/STE
• AV-plane velocity and strain ratePulse wave TDI/cTDI
Global longitudinal strain rate (TDI/STE)
Regional wall measurements• Longitudinal strain and strain rate
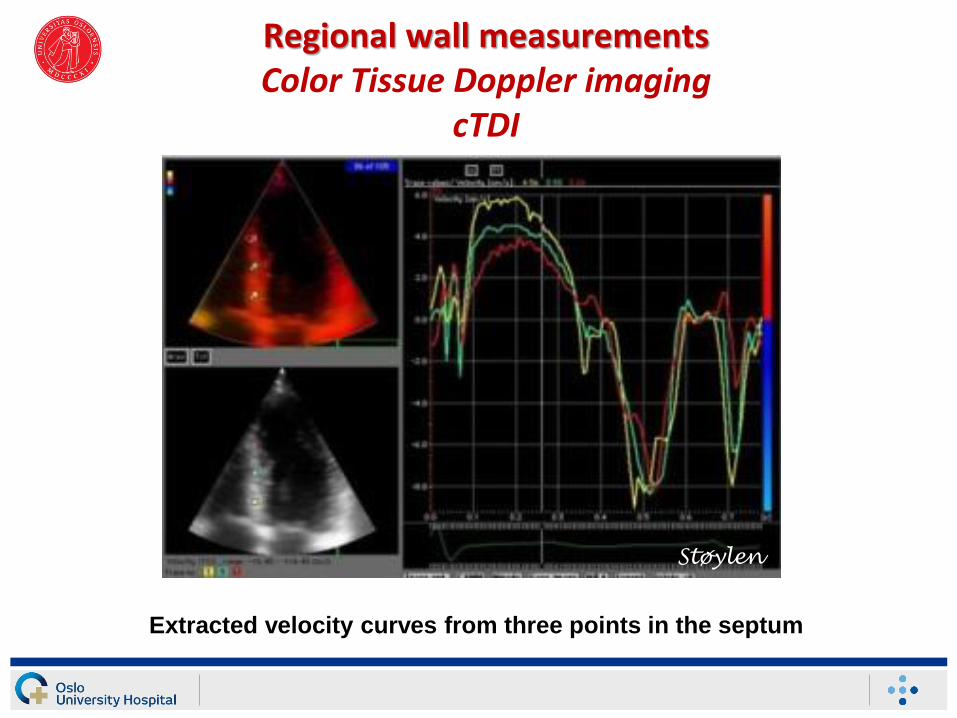
Regional wall measurementsColor Tissue Doppler imaging
cTDI
Extracted velocity curves from three points in the septum
Støylen
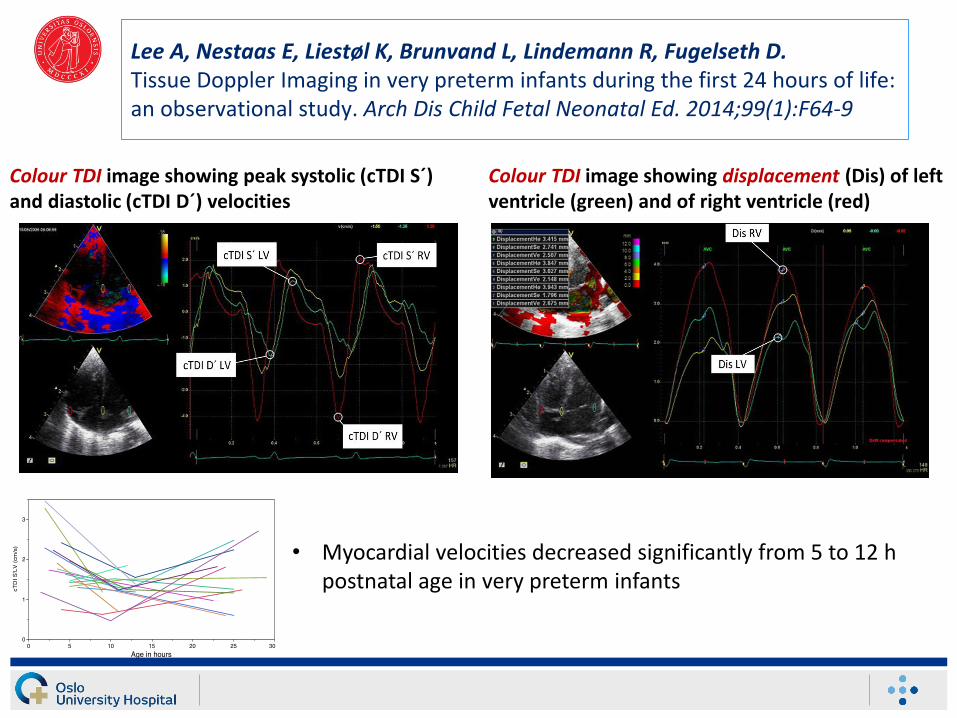
Lee A, Nestaas E, Liestøl K, Brunvand L, Lindemann R, Fugelseth D. Tissue Doppler Imaging in very preterm infants during the first 24 hours of life: an observational study. Arch Dis Child Fetal Neonatal Ed. 2014;99(1):F64-9
• Myocardial velocities decreased significantly from 5 to 12 h postnatal age in very preterm infants
Colour TDI image showing peak systolic (cTDI S´) and diastolic (cTDI D´) velocities
Colour TDI image showing displacement (Dis) of left ventricle (green) and of right ventricle (red)
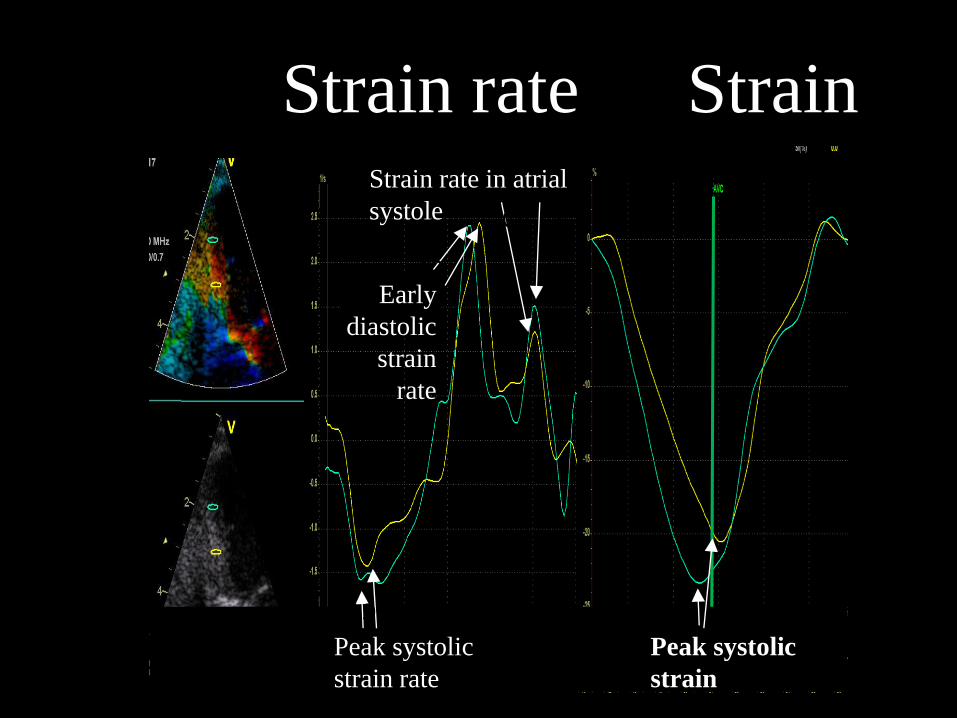
Peak systolic
strain
Peak systolic
strain rate
CV
Early
diastolic
strain
rate
CVCV
Strain rate in atrial
systole CV CV
Strain rate Strain
Strain and strain rate by TDI
1. Nestaas E, Stoylen A, Sandvik L, Brunvand L, Fugelseth D. Feasibility and reliability of strain and strain rate measurement in neonates by optimizing the analysis parameters settings. Ultrasound in Med Biol. 2007;33:270-8
2. Nestaas E, Stoylen A, Fugelseth D. Optimal types of probe, and tissue Doppler frame rates, for use during tissue Doppler recording and off-line analysis of strain and strain rate in neonates at term. Cardiol Young. 2008; 18(5):502-11
3. Nestaas E, Støylen A, Brunvand L, Fugelseth D. Tissue Doppler derived longitudinal strain and strain rate during the first 3 days of life in healthy term neonates. Pediatr Res. 2009;65(3):357-62
4. Nestaas E, Støylen A, Brunvand L, Fugelseth D. Longitudinal strain and strain rate by tissue Doppler are more sensitive parameters than fractional shortening for assessing the reduced myocardial function in asphyxiated neonates. CardiolYoung. 2011;21(1):1-7
5. Fugelseth D, Ramstad HB, Kvehaugen AS, Nestaas E, Støylen A, Staff AC. Myocardial function in offspring 5-8 years after pregnancy complicated by preeclampsia or diabetes mellitus. Early Human Dev. 2011;87(8):531-5
6. Nestaas E, Støylen A, Fugelseth D. Myocardial assessment in neonates by one-segment strain and strain rate analyses by tissue Doppler – a quality improvement study. BMJ Open. 2012;2(4):415-9
7. Nestaas E, Skranes JH, Støylen A, Brunvand L, Fugelseth D. The myocardial function during and after therapeutic hypothermia for hypoxic-ischemic encephalopathy, a cohort study. Early Hum Dev. 2014;90(5):247-52
8. Nestaas E, Fugelseth D, Støylen A. Automated, objective and expert-independent assessment of the analyzability of strain and strain rate in tissue Doppler images in term neonates by assessing the strain and strain rate beat-to-beat variation. Ultrasound Med Biol. 2014;40(3):637-42
9. Brunvand L, Fugelseth D, Stensaeth KH, Dahl-Jørgensen K, Margeirsdottir HD. Early reduced myocardial diastolic function in children and adolescents with type 1 diabetes mellitus – a population based study. BMC Cardiovasc Disord. 2016;16:103
10. Brunvand L, Heier M, Brunborg C, Hanssen KF, Fugelseth D, Stensaeth KH, Dahl-Jørgensen K, Margeirsdottir HD. Advanced glycation end products in children with type 1 diabetes and early reduced diastolic heart function. BMC Cardiovasc Disord. 2017;17(1):133
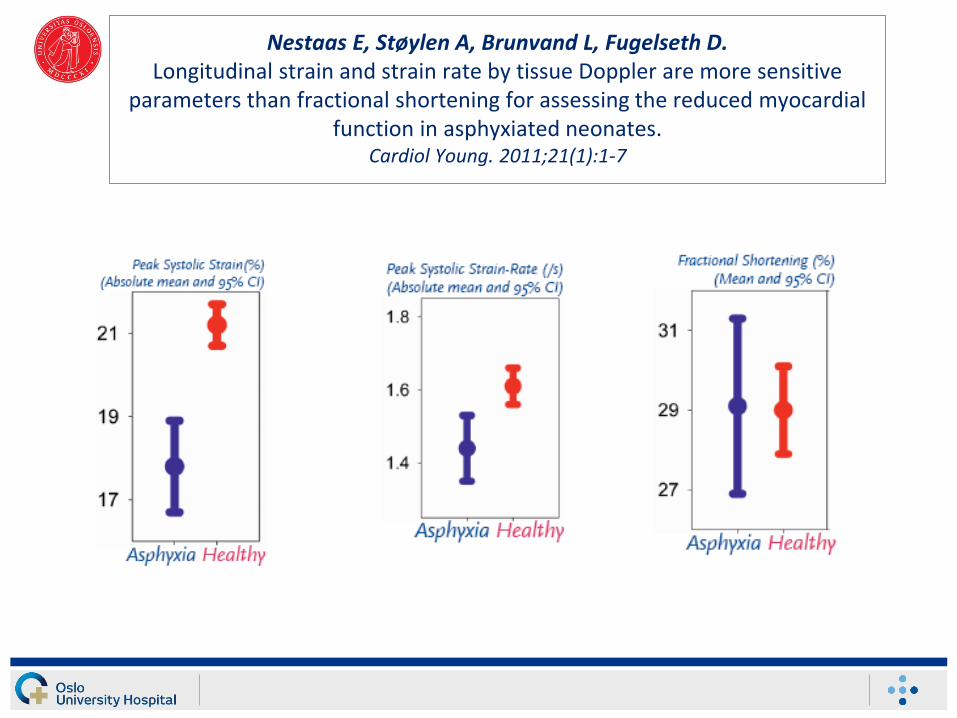
Nestaas E, Støylen A, Brunvand L, Fugelseth D. Longitudinal strain and strain rate by tissue Doppler are more sensitive
parameters than fractional shortening for assessing the reduced myocardial function in asphyxiated neonates.
Cardiol Young. 2011;21(1):1-7
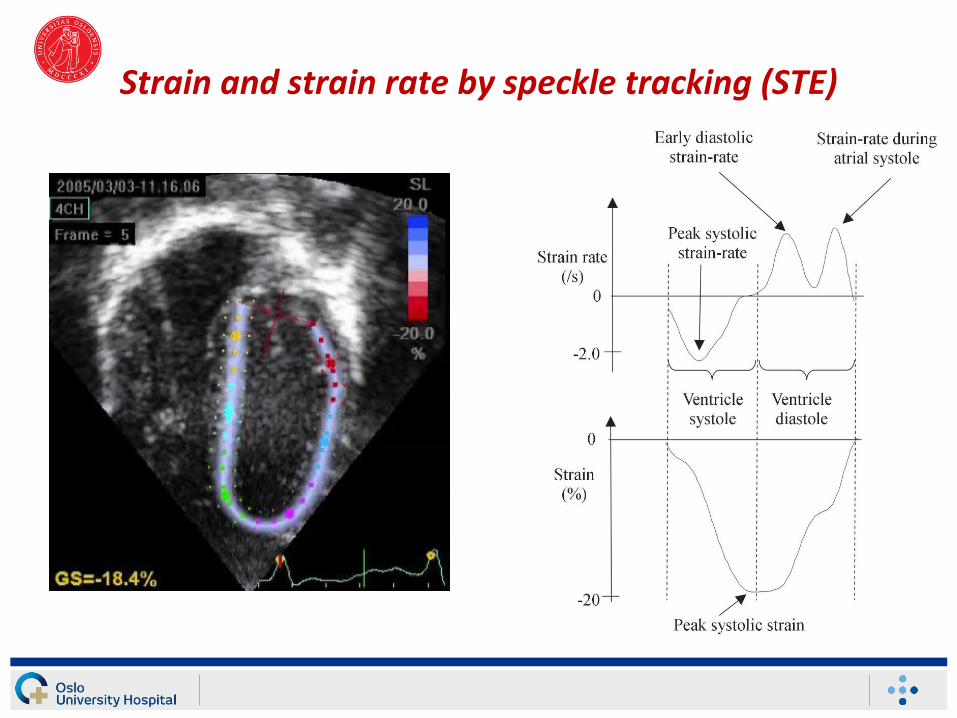
Strain and strain rate by speckle tracking (STE)
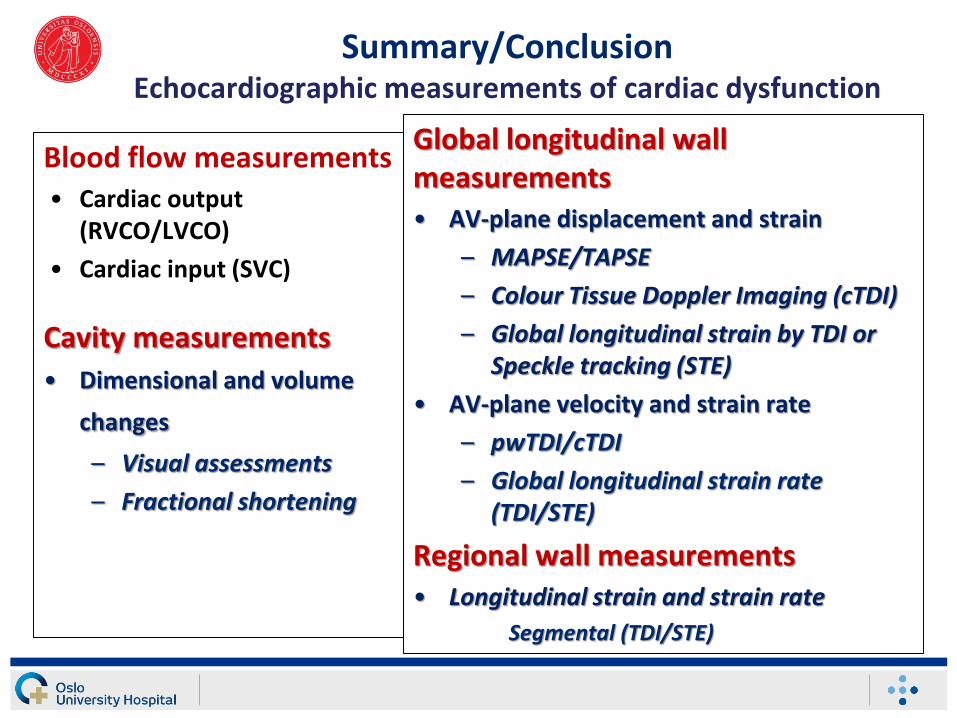
Summary/ConclusionEchocardiographic measurements of cardiac dysfunction
Blood flow measurements• Cardiac output
(RVCO/LVCO)
• Cardiac input (SVC)
Cavity measurements
• Dimensional and volume
changes
– Visual assessments
– Fractional shortening
Global longitudinal wallmeasurements• AV-plane displacement and strain
– MAPSE/TAPSE
– Colour Tissue Doppler Imaging (cTDI)
– Global longitudinal strain by TDI or Speckle tracking (STE)
• AV-plane velocity and strain rate
– pwTDI/cTDI
– Global longitudinal strain rate (TDI/STE)
Regional wall measurements• Longitudinal strain and strain rate
Segmental (TDI/STE)