Embed Size (px)
Citation preview
8/4/2019 Mastectomy Auto Saved)
http://slidepdf.com/reader/full/mastectomy-auto-saved 1/5
UPH – Dr. Jose G. Tamayo Medical UniversitySto. Niño, Biñan, Laguna
COLLEGE OF NURSING
MASTECTOMY(Breast Cancer)
SANTE, Kevin B
BSN – IV Sect. 6 / Gr.24
Dexter Mirabueno, RN
8/4/2019 Mastectomy Auto Saved)
http://slidepdf.com/reader/full/mastectomy-auto-saved 2/5
Breast Cancer
The most common cancer in FEMALES
I. Risk Factors
Female gender – 99% of cases occur in women.
Increasing age – Increasing age is associated with an increased risk.
Personal history of breast cancer – Once treated for breast cancer, the risk of developing breast
cancer in same or opposite breast is significantly increased.
Family history of breast cancer – Having first-degree relative with breast cancer (mother, sister,
and daughter) increases the risk twofold; having two first degree relatives increases the risk
fivefold. The risk is higher if the relative was premenopausal at the time of diagnosis. The risk is
increased if a father or brother had breast cancer (exact risk is unknown).
Genetic mutation – BRCA1and BRCA2 mutations account for the majority of inherited cases of
breast cancer.
Hormonal Factors
Early menarche – Before 12 years of age
Late menopause – After 55 years of age
Nulliparity – No full-term preganancies
Late age at first full-term pregnancy – After 30 years of age
Hormone therapy – estrogen and progesterone
Exposure to ionizing radiation
Obesity
High-fat diet
Alcohol intake (beer, wine, liquor)
II. Epidemiology
It is estimated that there will be a total of 12, 262 new breast cancer cases in 2010 with 4,371deaths. Latest data reveals that three out of every 100 Filipinas are likely to develop breast cancer
in their lifetime and that one out of every 100 are likely to die from the disease before age 75
(Philippine Cancer Facts and Estimates 2010).
III. Anatomy and Physiology Male and female breasts mature comparably until puberty, when in females estrogen and
other hormones initiate breast development. This development usually occurs from 10 to 16 years
of age, although the range can vary from 9 to 18 years. Stages of breast development are
described as Tanner stages 1 through 5.
Stage 1 describes a prepubertal breast
Stage 2 is breast budding, the first sign of puberty in female. Stage 3 involves further enlargement of breast tissue and the areola (a darker
tissue ring around the nipple).
Stage 4 occurs when the nipple and areola from a secondary mound on top of the
breast tissue.
Stage 5 is the continued development of a larger breast with a single contour.
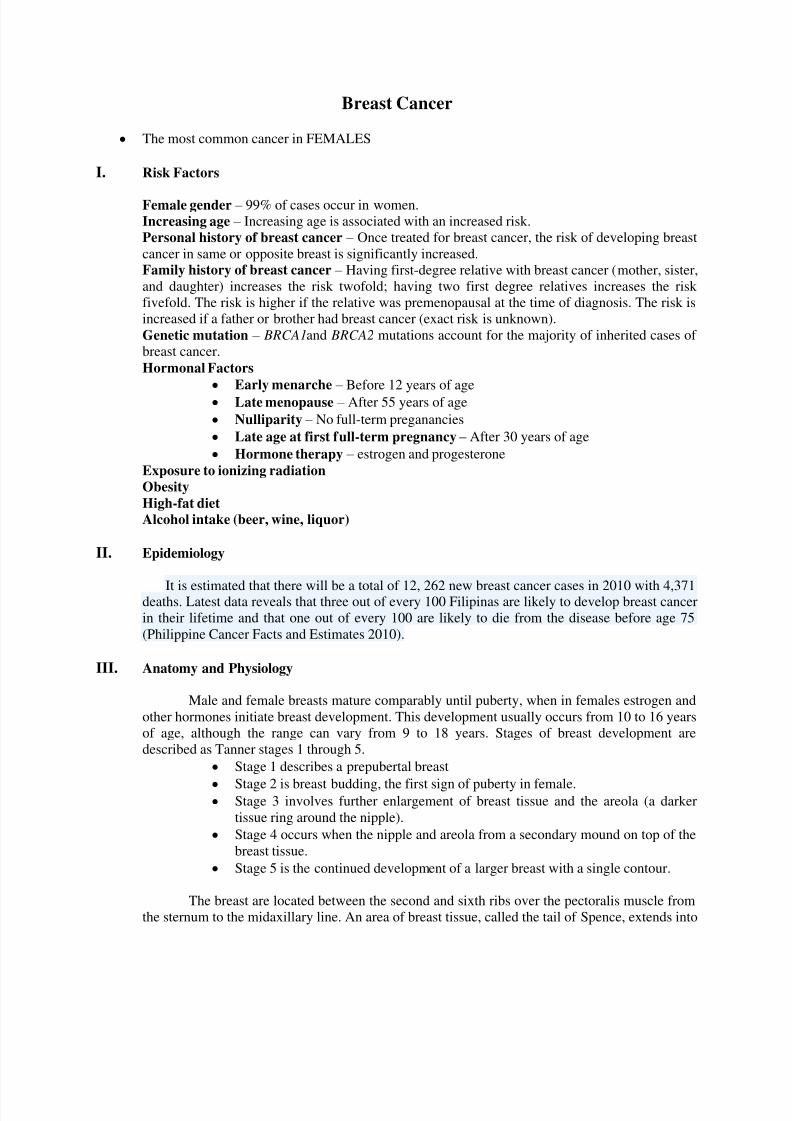
The breast are located between the second and sixth ribs over the pectoralis muscle from
the sternum to the midaxillary line. An area of breast tissue, called the tail of Spence, extends into
8/4/2019 Mastectomy Auto Saved)
http://slidepdf.com/reader/full/mastectomy-auto-saved 3/5
the axilla. Fascial bands, called Cooper’s ligaments, support the breast on the chest wall. Theinframammary fold (or crease) is a ridge of fat at the bottom of the breast.
Each breast contains 12 to 20 cone-shaped lobes, which are made up of glandular
elements (lobules and ducts) and separated by fat and fibrous tissue that binds the lobes together.
Milk is produced in the lobules and then carried through the ducts to the nipple.
IV. Clinical Manifestations Firm, nontender, nonmobile mass
Solitary, irregularly shaped mass
Adherence to muscle or skin, causing dimpling effect
Involvement of upper outer quadrant or central nipple portion of the breast.
Asymmetry of the breasts
“Orange peel” skin (Peau d’ Orange)
Retraction of the nipple
Abnormal discharge from the nipple
V. Assessment and Diagnostic Findings
Laboratory Findings Biopsy
Mammography
Staging
Stage I – Tumors that are 2 cm or less with no involvement of axillary lymphnodes Stage II – Tumors that are 2cm to 5 cm with involvement of axillary lymphnodes
Stage III – Tumors greater than 5cm with involvement of axiallary lymphnodes
Stage IV – Tumor of any size, with distant metastases
8/4/2019 Mastectomy Auto Saved)
http://slidepdf.com/reader/full/mastectomy-auto-saved 4/5
VI. Management
Medical Management Chemotherapy Tamoxifen therapy Radiation therapy
Surgical Management
MASTECTOMY Removal of the breast, with or without surrounding structures.
Surgical treatment for breast cancer.
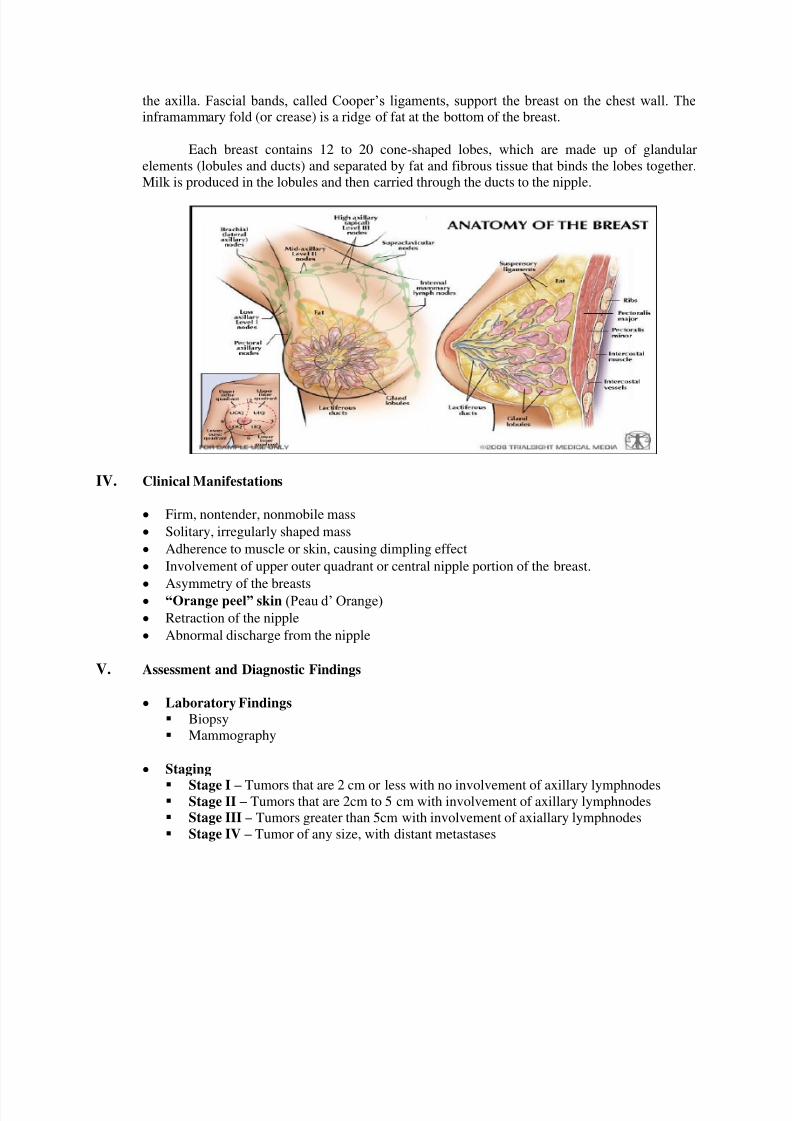
Mastectomies can be performed in four distinct methods, depending on the
diagnosis and the extent of the pathologic findings.
Lumpectomy (Tylectomy) - is a common surgical procedure designed to remove a
discrete lump, usually a benign tumor or breast cancer, from an affected man or
woman's breast.
Subcutaneous Mastectomy - Removal of all breast tissue. Overlying the skin and
nipple are left intact.
Simple Mastectomy – Removal of entire breast, pectoralis muscles, and the nipples
remain intact. Modified Radical Mastectomy – Removal of breast, pectoralis major and axillary
lymphnodes.
Radical Mastectomy – MRM with removal of pectoralis muscles, axillary and neck
lymphnodes, followed by skin grafting.
Stage I and II
Options
1. Breast conservative surgery
(lumpectomy/quadrandectomy/segemental mastectomy with separate axillary
node dissection and irradiation)
2. Modified radical mastectomy
(Total mastectomy with axillary dissection)
Stage IIIA
Options
1. Modified radical mastectomy
8/4/2019 Mastectomy Auto Saved)
http://slidepdf.com/reader/full/mastectomy-auto-saved 5/5
2. Induction chemotherapy + MRM + Radiation
Stage IIIB
1. Induction chemotherapy first then with
- Good Response – MRM – Radiation
- Poor response – Radiation – MRM
Stage IV 1. Radiation and/or palliative (hygienic mastectomy) + chemotherapy and/or
hormonal therapy
Complications of surgery1. Lymphedema2. Hematoma
3. Infection
Nursing Management
PRE-Operative Care Psychological support – involve the husband as necessary.
Teach arm exercises to prevent lymphedema. Inform about wound section drainage.(Hemovac, Jackson-Pratt)
Deep breathing exercise to prevent post-operative respiratory complications
POST-Operative Care Place on semi-fowlers position with affected arm elevated on pillows
abducted, to promote venous return and prevent edema.
Monitor hemovac output (serosanguinous for the first 24 hours)
Check behind for bleeding Post signs warning against taking BP, starting IV line or drawing blood on
affected side. Reinforce special mastectomy exercise as prescribed. Provide adequate analgesia to promote ambulation and exercise.
Encourage regular coughing and deep breathing exercises. Prepare for size and appearance of the incision and provide support when
incision is viewed for the first time. Provide with detailed information concerning breast prosthesis. Fitting is not
possible for 4 to 6 weeks.
A temporary prosthesis or lightly padded bras worn until healing iscompleted. Avoid constructive clothing and report persistent edema, redness
or infection of incision. Teach the importance of continuing monthly BSE on the remaining breast.


![Controlling Auto Saved]](https://img.pdfslide.us/doc/110x75/577d35171a28ab3a6b8f9027/controlling-auto-saved.jpg)


![FORTUNE....Pptx Auto Saved]](https://img.pdfslide.us/doc/110x75/577d20cd1a28ab4e1e93c8a4/fortunepptx-auto-saved.jpg)
![Incentive Auto Saved]](https://img.pdfslide.us/doc/110x75/577d33c51a28ab3a6b8bb269/incentive-auto-saved.jpg)


![OB Notes.pptx Auto Saved]](https://img.pdfslide.us/doc/110x75/577d1e601a28ab4e1e8e64ef/ob-notespptx-auto-saved.jpg)



![Apollo Tyres_1 Auto Saved]](https://img.pdfslide.us/doc/110x75/577d279e1a28ab4e1ea45eea/apollo-tyres1-auto-saved.jpg)


![fINALsEMINAR.ppt Auto Saved]](https://img.pdfslide.us/doc/110x75/577d29e21a28ab4e1ea8234f/finalseminarppt-auto-saved.jpg)



![Proposal Kewirausahaan Auto Saved]](https://img.pdfslide.us/doc/110x75/5571ff1f49795991699caf1f/proposal-kewirausahaan-auto-saved.jpg)

![Embedded System Auto Saved]](https://img.pdfslide.us/doc/110x75/577d208b1a28ab4e1e932aa3/embedded-system-auto-saved.jpg)


![TETRA Auto Saved]](https://img.pdfslide.us/doc/110x75/577d25121a28ab4e1e9dfd04/tetra-auto-saved.jpg)


![Crypto Ppt Auto Saved]](https://img.pdfslide.us/doc/110x75/577d20f21a28ab4e1e941a72/crypto-ppt-auto-saved.jpg)
