Embed Size (px)
Citation preview

LCA consequences of cancer position statement
Ann Muls, GI Late effects Consultant Nurse, LCA Survivorship Group member

The London Cancer Alliance West and South
Setting the scene
• Number of people diagnosed with cancer (UK): 320,467
• Long term cancer survivors x 3 over last 3 decades
• Increase per year: 3%
• Estimate 2030: 4 million cancer survivors
(Maher & McConnell, 2011; Andreyev et al, 2012; Cancer Research UK, 2012)
The London Cancer Alliance West and South
Cancer survivor: definition
“ someone who is living with or beyond a cancer diagnosis.”

The London Cancer Alliance West and South
Consequences of cancer and its treatments
“the wide range of long-term
physical and psychological changes that seem to be associated with cancer and its treatments, however long ago the diagnosis and the treatment might have been given.”
(Macmillan, 2013)
The London Cancer Alliance West and South
Summary of strategy
• Consequences of cancer and its treatments should be considered at all transition points in the pathway
• Identifying current services available
• Models of care
• Recommendations for adoption by the LCA tumour specific pathways

The London Cancer Alliance West and South
Consequences…what do we mean?
The London Cancer Alliance West and South

The London Cancer Alliance West and South

Current approach across the LCA
• Acute side-effects are routinely discussed at diagnosis
• There are risk factors but they are poorly understood
• There is no way of predicting the nature and likely
onset of consequences and its treatment long-term

Mapping current service provision
17 service providers
• 6 reported that cancer MDTs consider consequences but the extent of content is not known
• Holistic Needs Assessment is widely used
• Agreement that consequences are widespread
• Most teams refer to general services
• Some have cancer specific services: psychological support, physiotherapy, nutritional support
• Established referral pathways for common consequences: pain, bone health, urinary, financial
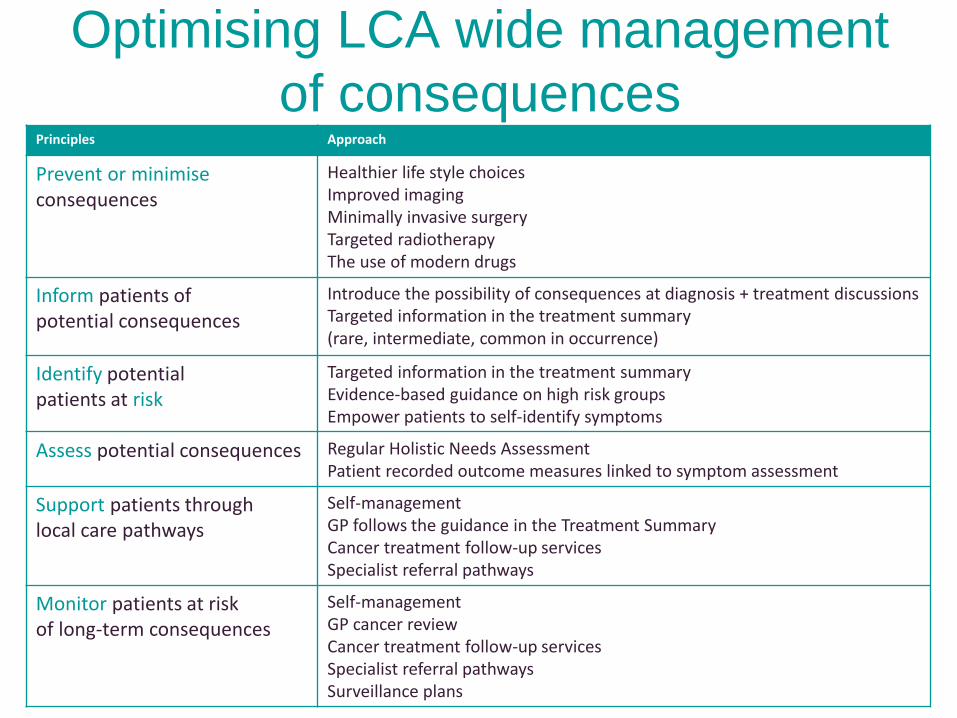
Optimising LCA wide management
of consequences Principles Approach
Prevent or minimise consequences
Healthier life style choices Improved imaging
Minimally invasive surgery
Targeted radiotherapy
The use of modern drugs
Inform patients of potential consequences
Introduce the possibility of consequences at diagnosis + treatment discussions
Targeted information in the treatment summary (rare, intermediate, common in occurrence)
Identify potential patients at risk
Targeted information in the treatment summary Evidence-based guidance on high risk groups Empower patients to self-identify symptoms
Assess potential consequences Regular Holistic Needs Assessment Patient recorded outcome measures linked to symptom assessment
Support patients through local care pathways
Self-management GP follows the guidance in the Treatment Summary
Cancer treatment follow-up services Specialist referral pathways
Monitor patients at risk of long-term consequences
Self-management GP cancer review
Cancer treatment follow-up services Specialist referral pathways Surveillance plans

Integration in the adult
survivorship pathway
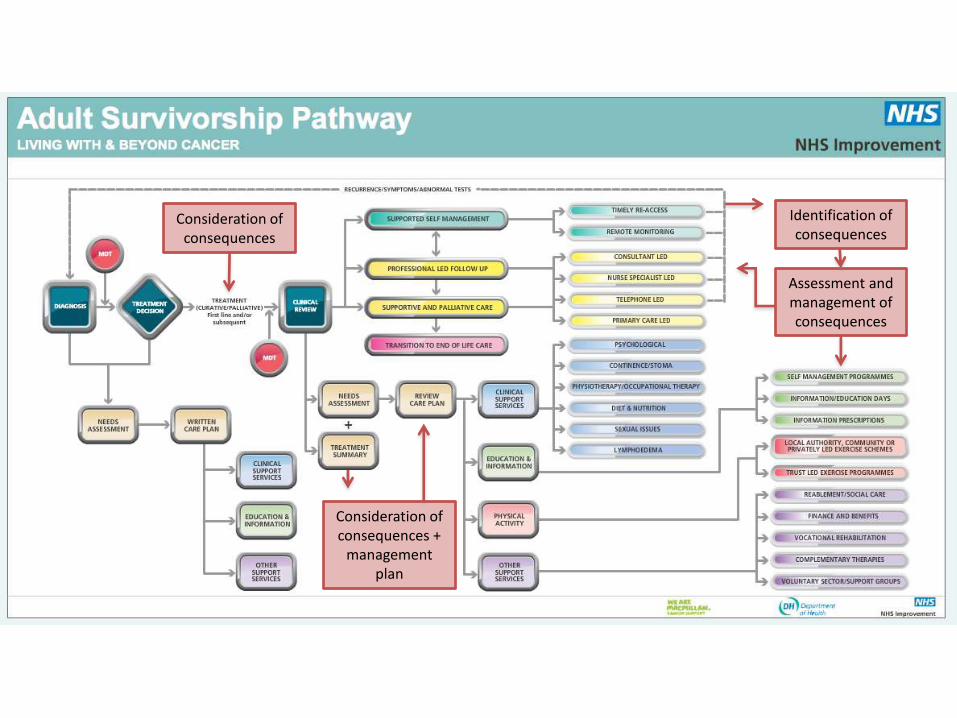
Consideration of consequences
Consideration of consequences +
management plan
Identification of consequences
Assessment and management of consequences

Stratification of need
(Macmillan, 2013)

Recommendations across the LCA
• Adoption of the consequences position paper
• Adoption of the treatment summary as part of the
recovery package
• The role of primary care in recognising, assessing and
addressing consequences
• Review of patient information
• Development of referral pathways and management
strategies in primary, secondary and tertiary care
• Research priorities

References and picture sources
• Andreyev J, Davidson S, Gillespie C, et al. Practice guidance on the management of acute and
chronic gastrointestinal problems arising as a result of treatment for cancer. Gut 2012; 61: 179-
192.
• Cancer Research UK (2012) Incidence of cancer diagnosis in the UK.
Accessed via: http://info.cancerresearchuk.org/cancerstats/incidence/uk-cancer-incidence-statistics
• London Cancer Alliance (in press) Consequences of cancer treatments: A position statement
• Maher J & McConnell H (2011) New pathways of care for cancer survivors: adding the numbers.
British Journal of Cancer, 105: S5-S10.
• ‘Body systems’ by Body Systems Design
Accessed online 08.01.2014 via http://bodysystemsdesign.com/welcome-to-body-systems-design/
• ‘All in your head’ by Julia Gumm
Accessed online 08.01.2014 via http://en.paperblog.com/the-mind-body-connection-534582/
• ‘Money man’ by Invest in the Northeast
Accessed online 08.01.2014 via http://www.investinthenortheast.com/?tag=budget

Breast Radiotherapy Rehabilitation Injury
Service
A national multi-disciplinary service for
consequences of breast radiotherapy
Denise Moorhouse RGN
Service Manager Details and accreditations:
Royal National Hospital for Rheumatic Diseases
NHS Foundation Trust, Upper Borough Walls, Bath, BA1 1RL
• Two million people in the UK with a diagnosis of
cancer - set to grow to 3 million by 2030
• 2007 National Cancer Survivorship Initiative
launched
• “Most modern surgery, radiotherapy,
chemotherapy and biological treatments can
have consequences which develop immediately,
or become apparent years, or even decades
later.” Maher 2013
The Context
www.rnhrd.nhs.uk

Cancer Survivorship
www.rnhrd.nhs.uk

At the end of Cancer treatment…
www.rnhrd.nhs.uk
Individuals receive follow up
according to their needs.
• Most people will manage
with open access to
services
• Some will require shared
care between agencies
• Few will be complex and
require more intensive
input.
Radiotherapy Induced Brachial Plexus Injury
www.rnhrd.nhs.uk
• What is it?
• Radiation damage to the Brachial
nerve
• How many people are affected?
• Severe pain/pins and needles
(neuropathic pain)
• Lymphoedema
• Osteoporosis
• Lung damage
• Reduced quality of life
• Low mood
Facts and Figures Signs and Symptoms
may include

National Collaboration
www.rnhrd.nhs.uk
Bringing together expertise in rehabilitation
and cancer care
• Royal National Hospital for Rheumatic
Diseases, Bath
• The Christie, Manchester
• Barts Health, London

Case Study
www.rnhrd.nhs.uk
Mrs P Aged 79
Breast cancer (L) 1982, aged 47 Lumpectomy, Axillary sampling
Radiotherapy over 3 weeks = 15 fractions. Treatment delivered from 2
different machines with no tattoos or markings. No other adjuvant
treatment given
PMH –Osteoporosis , Scoliosis
Medication – Allendronic Acid 70mgs
Calcium Supplements
Lodine 60 mgs
Omeprozole 20mgs
Retired social worker, likes to eat out, loves travel – Grandchildren live
In Thailand – like to go and see them as often as possible.
Case Study cont…
www.rnhrd.nhs.uk
2003 - ( 21 years later) developed numbness and tingling in
L arm. Eventually unable to lift her arm, became heavy
and numb
2006 - radiotherapy induced brachial plexus diagnosed.
2008 - developed respiratory problems including SOBOE due
to radiotherapy damage and COPD.

Case Study cont…
www.rnhrd.nhs.uk
Presentation at clinic
Weak left shoulder, unable to raise her arm.
Lower back pain, worse with standing and at night.
Worsening neuropathic symptoms in left arm.
Walks with a stick around the house and uses a wheel chair for
going out – which she HATES!
Describes a feeling of loss of purpose/meaning of life
Needs help to dress
Unable to cut up her own food which stops her eating out
Fatigued
Case Study cont…
www.rnhrd.nhs.uk
Attended 2 day clinic at Barts
Alendronic Acid causing gastric irritation - To have IV
Zolendronic Acid 5mg yearly
Amitriptyline 10mgs for neuropathic pain.
Inhalers to mange breathlessness
Declined local Psychology services
Home adaptions and equipment to aid independence
Admit to RNHRD for inpatient programme
Case Study cont…
www.rnhrd.nhs.uk
In patient stay at RNHRD – 2 weeks
Poor posture addressed through physio, developed a
straight posture– no longer SOBOE. Now not starting the
day with a massive productive cough
Progressed form wheelchair to rolator frame for outdoor
use – went shopping by herself!
Developed techniques to manage going out without feeling
overwhelmed( relaxation and desensitisation)
Developed some independence around ADL – washing,
dressing, meal preparation etc.
Why/How did these clinical problems arise?
www.rnhrd.nhs.uk
• Random choices of RT dosages and delivery
• Lack of evidence base, national protocols or
treatment guidelines.
• Lack of modern techniques
• Inconsistent positioning therefore some areas
of breast tissue/ axilla & supraclavicular nodes
were over exposed

National Service – Patient Journey
www.rnhrd.nhs.uk
OR
Referral
Accepted onto caseload
by Prof Candy McCabe,
Clinical lead @ RNHRD
Telephone Assessment by lead nurse at RNHRD
Do not meet criteria
discharged back to
GP or signposted
The Christie
MDT Clinic
RNHRD
MDT Clinic
Bart’s
MDT Clinic
3 month follow up In patient rehab
programme OR
Inpatient Rehabilitation Service
www.rnhrd.nhs.uk
RNHRD specialist
rehabilitation hospital in the
centre of Bath
Two week individualised
programme includes
• Daily physiotherapy, hydrotherapy
and occupational therapy
• Psychology and pain management
available as required

Aims of National Service
www.rnhrd.nhs.uk
3 main clinical outcomes:
• Improvement in daily function
• Improvement in quality of life
• Improvement in pain management
To build a knowledge base about this rare
condition
To provide support and education to health
care providers on safe management of this
condition
Outcomes so far
www.rnhrd.nhs.uk
Early indications suggest:
• Reduced attendance at A&E and
GP
• Improvement in pain
• Improvement in quality of life

www.rnhrd.nhs.uk
• NHS England funding – no costs to GPs
• 3 centres
• RNHRD, Bath
• The Christie, Manchester
• Barts Health, London
• Life long service for this group
• Now recruiting patients into the service
• Service available to everyone registered
with a GP in England

Referrals
www.rnhrd.nhs.uk
Professor Candy McCabe
RNHRD
Upper Borough Walls
Bath
01225 473462