Embed Size (px)
Citation preview
Overview of Cancer SurvivorshipOverview of Cancer Survivorship
Patricia A. Ganz, M.D.Professor, UCLA Schools of Medicine & Public Health
Director, UCLA-LIVESTRONG SurvivorshipCenter of ExcellenceCenter of Excellence
Jonsson Comprehensive Cancer Center
Who are the Cancer S r i ors?Survivors?
• More than 1 in 3 Americans willMore than 1 in 3 Americans will be diagnosed with cancer in their lifetime et e
• 11.1 million Americans have a personal history of cancerpersonal history of cancer
• The number of cancer survivors ill i h l d i thwill increase sharply during the
next 25 yrs
IOM t f th t t t tIOM report focuses on the post-treatment and pre-recurrence/end-of-life phase of care
American Cancer SocietyAmerican Cancer Society
Public Service Advertisement ca. 1988
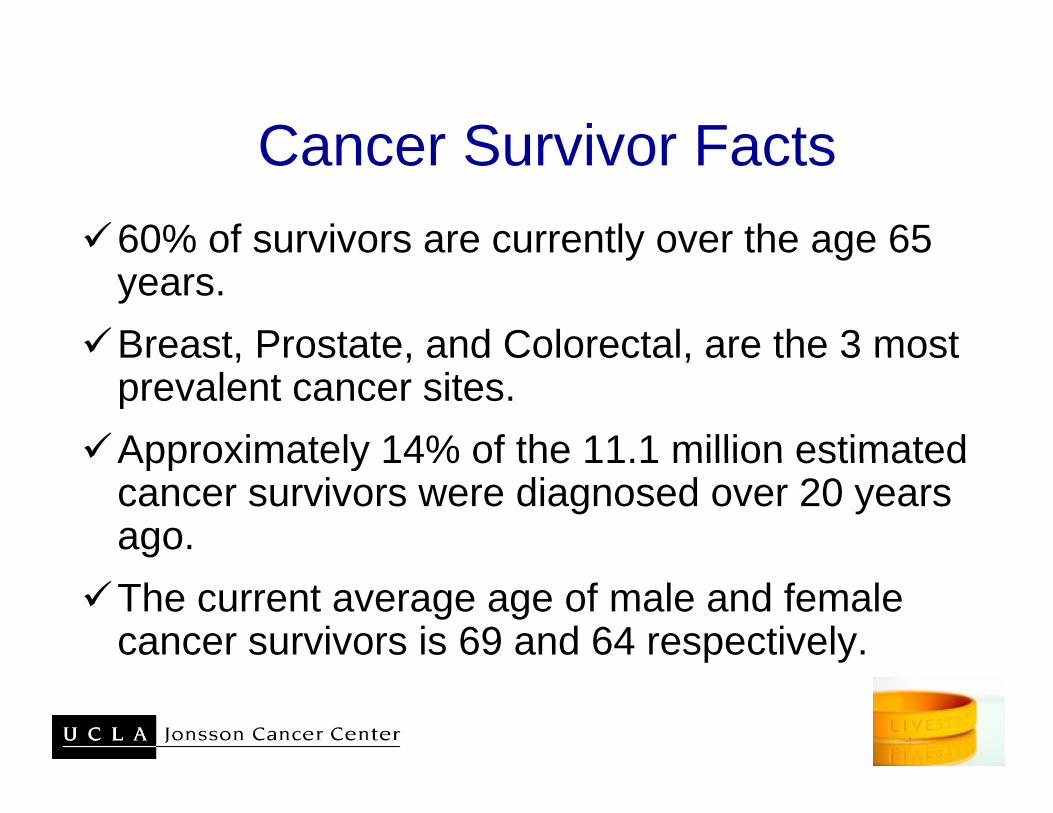
Cancer Survivor FactsCancer Survivor Facts60% of survivors are currently over the age 65 % y gyears.Breast, Prostate, and Colorectal, are the 3 mostBreast, Prostate, and Colorectal, are the 3 most prevalent cancer sites.Approximately 14% of the 11 1 million estimatedApproximately 14% of the 11.1 million estimated cancer survivors were diagnosed over 20 years ago.The current average age of male and female cancer survivors is 69 and 64 respectively.
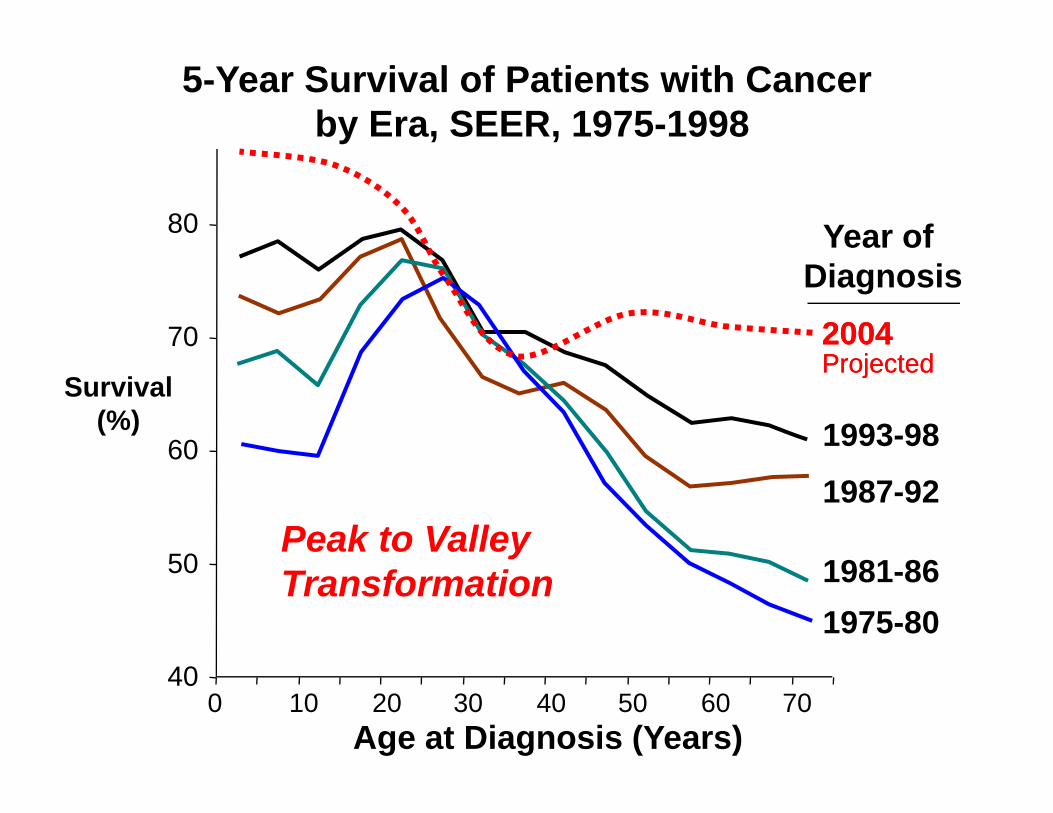
5-Year Survival of Patients with Cancer by Era, SEER, 1975-1998
80 Year of
70
Diagnosis20042004P j t dP j t d
60 1993-98Survival
(%)
ProjectedProjected
50
601987-92
1981 86Peak to Valley
50 1981-861975-80
Transformation
Age at Diagnosis (Years)
400 10 20 30 40 50 60 70
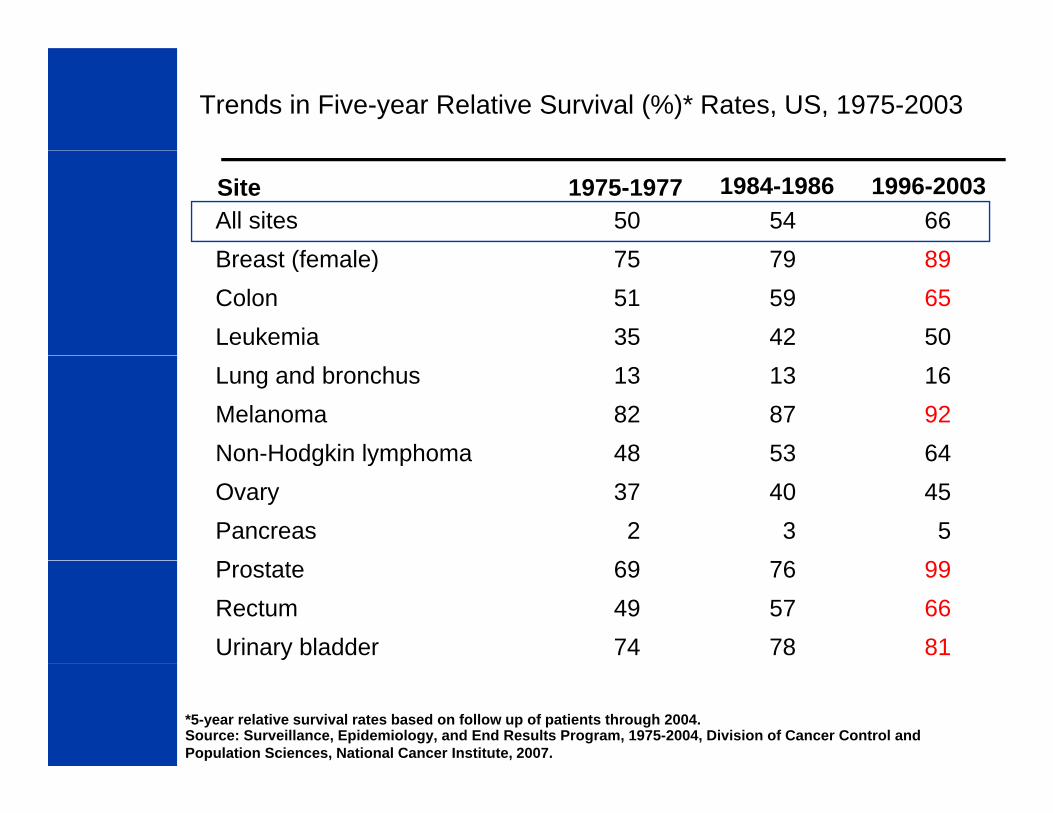
Trends in Five-year Relative Survival (%)* Rates, US, 1975-2003
Site 1975-1977 1984-1986 1996-2003All sites 50 54 66B t (f l ) 75 79 89Breast (female) 75 79 89Colon 51 59 65Leukemia 35 42 50Lung and bronchus 13 13 16Melanoma 82 87 92Non-Hodgkin lymphoma 48 53 64Non Hodgkin lymphoma 48 53 64Ovary 37 40 45Pancreas 2 3 5P 69 6 99Prostate 69 76 99Rectum 49 57 66Urinary bladder 74 78 81
*5-year relative survival rates based on follow up of patients through 2004. Source: Surveillance, Epidemiology, and End Results Program, 1975-2004, Division of Cancer Control andPopulation Sciences, National Cancer Institute, 2007.
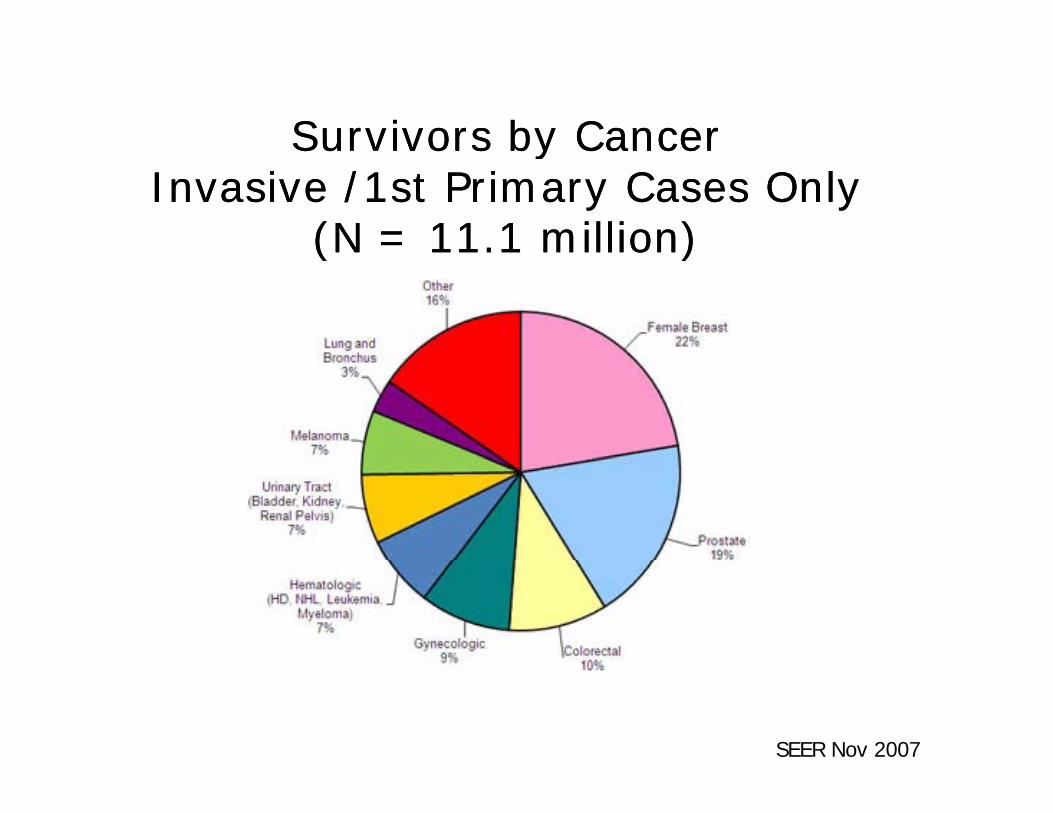
Survivors by Cancer Survivors by Cancer Survivors by Cancer Survivors by Cancer Invasive /1st Primary Cases Only Invasive /1st Primary Cases Only
(N = 11.1 million)(N = 11.1 million)( )( )
SEER Nov 2007
How did we make such incredible strides?
E li d t ti• Earlier detection• New drugs and other treatments• Combined modality therapy• Prolonged adjuvant and/or maintenanceProlonged adjuvant and/or maintenance
therapies• High dose chemotherapy with HCT• High dose chemotherapy with HCT• Prevention of second malignancies
But there is a costBut there is a cost…
• TimeTime• Money
H• Human• Interpersonal• Existential
For many individuals cancer is For many individuals, cancer is now a chronic disease…..
• Comparison of cancer survivors and age-• Comparison of cancer survivors and age-matched individuals from the National Health Interview Survey (NHIS) in 2000Health Interview Survey (NHIS) in 2000
• Multiple measures of burden embedded within the surveywithin the survey
JNCI 96:1322, 2004
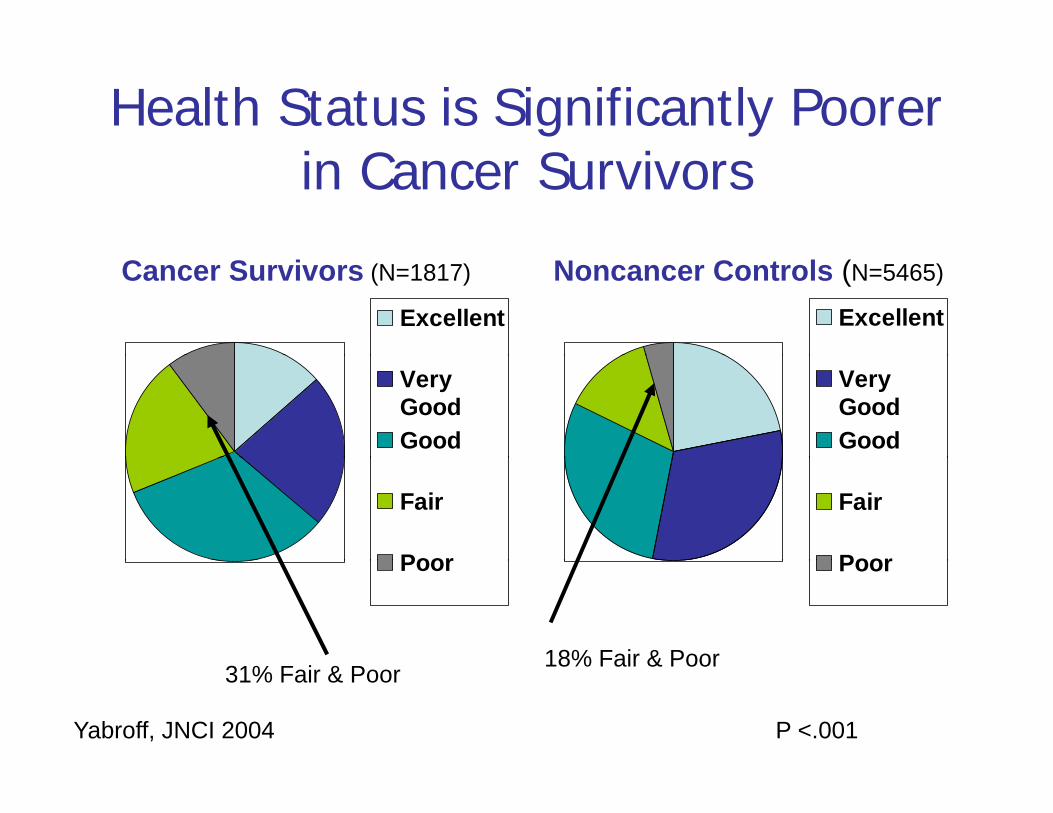
Health Status is Significantly Poorer i C S iin Cancer Survivors
Excellent Excellent
Cancer Survivors (N=1817) Noncancer Controls (N=5465)
VeryGoodGood
VeryGoodGood
Fair
Poor
Fair
PoorPoor Poor
18% Fair & Poor
Yabroff, JNCI 2004 P <.001
18% Fair & Poor31% Fair & Poor
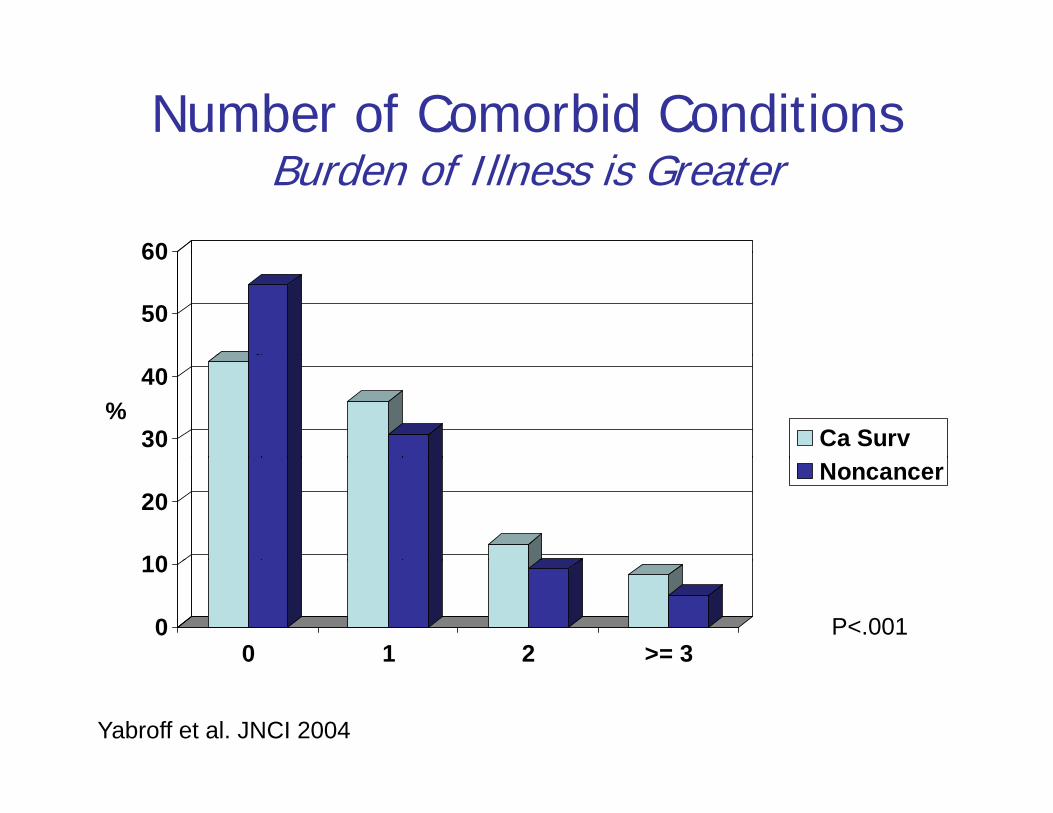
Number of Comorbid ConditionsBurden of Illness is Greater
60
50
60
30
40
Ca Surv%
10
20Noncancer
0
10
0 1 2 >= 3P<.001
Yabroff et al. JNCI 2004
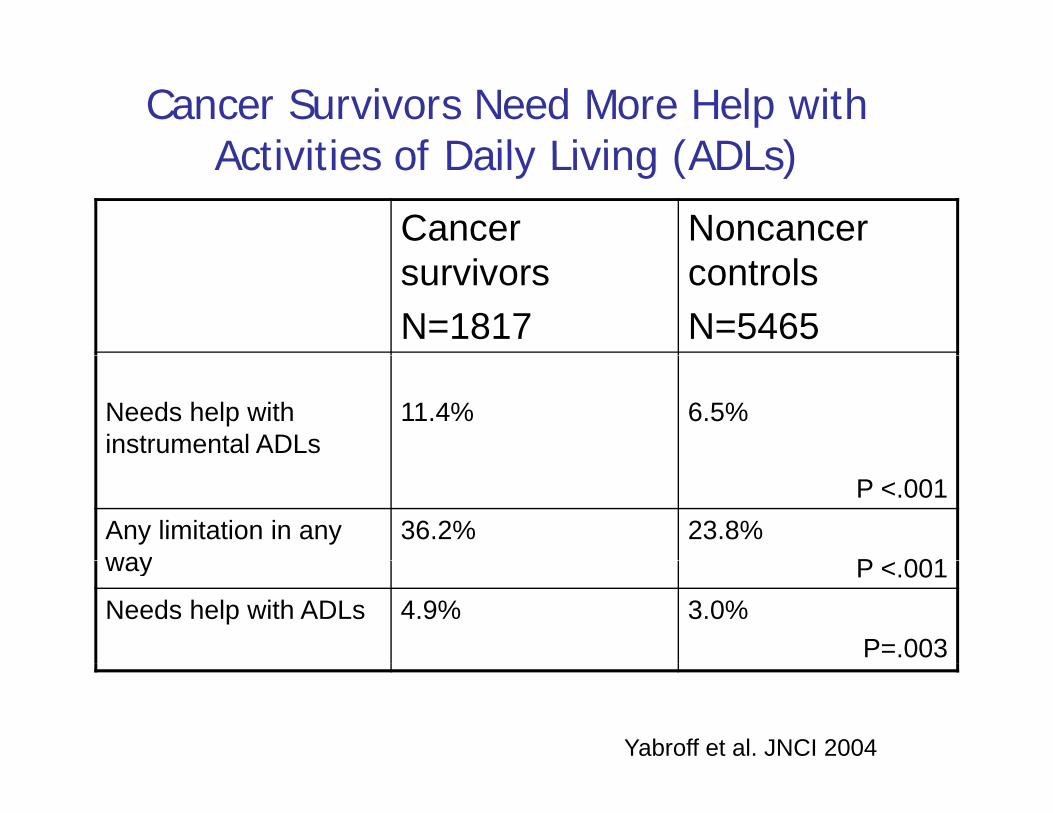
Cancer Survivors Need More Help with Activities of Daily Living (ADLs)
Cancer Noncancer
Activities of Daily Living (ADLs)
survivorsN=1817
controlsN=5465
Needs help with instrumental ADLs
11.4% 6.5%
P <.001Any limitation in any way
36.2% 23.8%P 001way P <.001
Needs help with ADLs 4.9% 3.0%P=.003
Yabroff et al. JNCI 2004
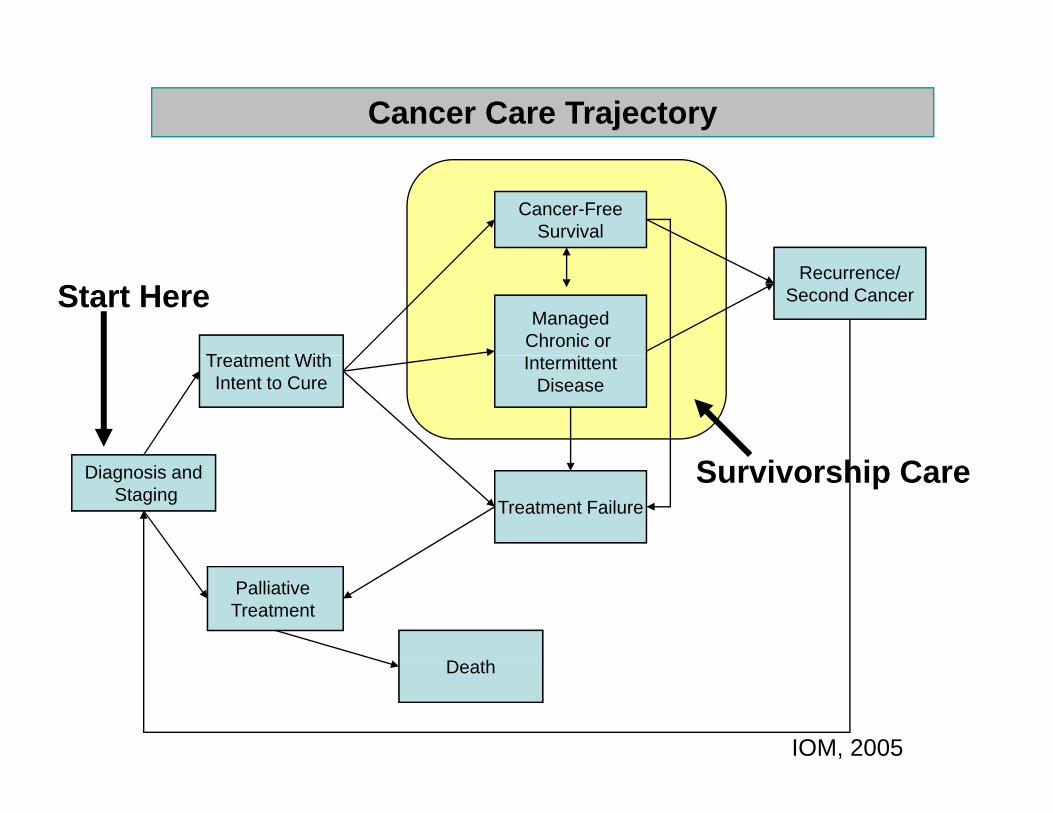
Cancer Care Trajectory
Cancer-FreeSurvival
T t t With
ManagedChronic or
Recurrence/Second CancerStart Here
Treatment With Intent to Cure
IntermittentDisease
Diagnosis andStaging
Treatment Failure
Survivorship Care
Palliative Treatment
D thDeath
IOM, 2005
IOM Findings:S i hi CSurvivorship Care• Survivorship care is a neglected phase of the cancer care trajectory
• Cancer recurrence, second cancers, and treatment late effectstreatment late effects concern survivors
• Few guidelines on• Few guidelines on follow-up care
• Providers lack• Providers lack education and training
IOM Findings:S i hi CSurvivorship Care
• Survivors may:• Survivors may:
– be unaware of risk
– have no plan forhave no plan for follow-up
• Opportunities to ppintervene may be missed
• Cancer care is often not coordinated
• Models of• Models of survivorship care not tested
IOM Findings:Quality Survivorship Q y pCareCh i• Chronic care model applies
• Essential care components
–Prevention
–SurveillanceSurveillance
–Intervention
Coordination–Coordination
Why is cancer different from other chronic diseases?
• Cancer treatment is….Cancer treatment is….– Complex– Multi-modalMulti-modal– Multi-disciplinary
Toxic– Toxic– Expensive
And often poorly coordinated– And often poorly coordinated• Cancer treatment usually occurs in isolation
from primary health care deliveryfrom primary health care delivery
Other Challenges
• Limited systematic study of the late effects of cancer therapy
• Follow-up care plans have been ad hoc, p p ,with focus on surveillance for recurrence
• When should health promotion andWhen should health promotion and chronic disease prevention become the focus?focus?
• Infertility? “Dear, you should just be happy to be alive ”to be alive.
Why does cancer care present such a challenge?
• An average of 3 specialists/patient, with treatments across time and space…outpatient, inpatient, specialized treatment facilities…. limited communication among treating physicians, multiple medical records
• In addition, aging of the population AND work force shortageg
Proposed Strategies to Address these Challenges
• Integrated, electronic medical recordsIntegrated, electronic medical records• Patient navigators• Consultation planning• Consultation planning
N f th t t iN f th t t i id lid lNone of these strategies areNone of these strategies are widely widely available for patients receiving active available for patients receiving active treatment!treatment!treatment!treatment!
What happens when treatment ends?What happens when treatment ends?
Why do we need a survivorship care plan?
• To summarize and communicate whatTo summarize and communicate what transpired during cancer treatment
• To describe known and potential late effects of pcancer treatments, with expected time course
• To communicate to the survivor and other health care providers what has been done and what needs to be done in the futureT t h lth lif t l t t• To promote a healthy lifestyle to prevent recurrence and reduce the risk of other comorbid conditionscomorbid conditions
Survivorship Care Plan flows from h IOM R d iother IOM Recommendations
• Continuous healing relationshipsg p• Customization based on needs and values• Patient as the source of control• Shared knowledge and free flow of information• Evidence-based decision making
S f t t t• Safety as a system property• Need for transparency• Anticipation of needs• Anticipation of needs• Decrease in waste• Cooperation among physiciansp g p y
Key Elements Included in Survivorship C PlCare Plan
• Specific tissue diagnosis and stage• Specific tissue diagnosis and stage• Initial treatment plan and dates of treatment• Toxicities during treatment• Toxicities during treatment• Expected short- and long-term effects of RX• Late toxicity monitoring neededLate toxicity monitoring needed• Surveillance for recurrence or second cancer• Who will take responsibility for survivorship careWho will take responsibility for survivorship care• Psychosocial and vocational needs• Recommended preventive behaviors/interventionsRecommended preventive behaviors/interventions
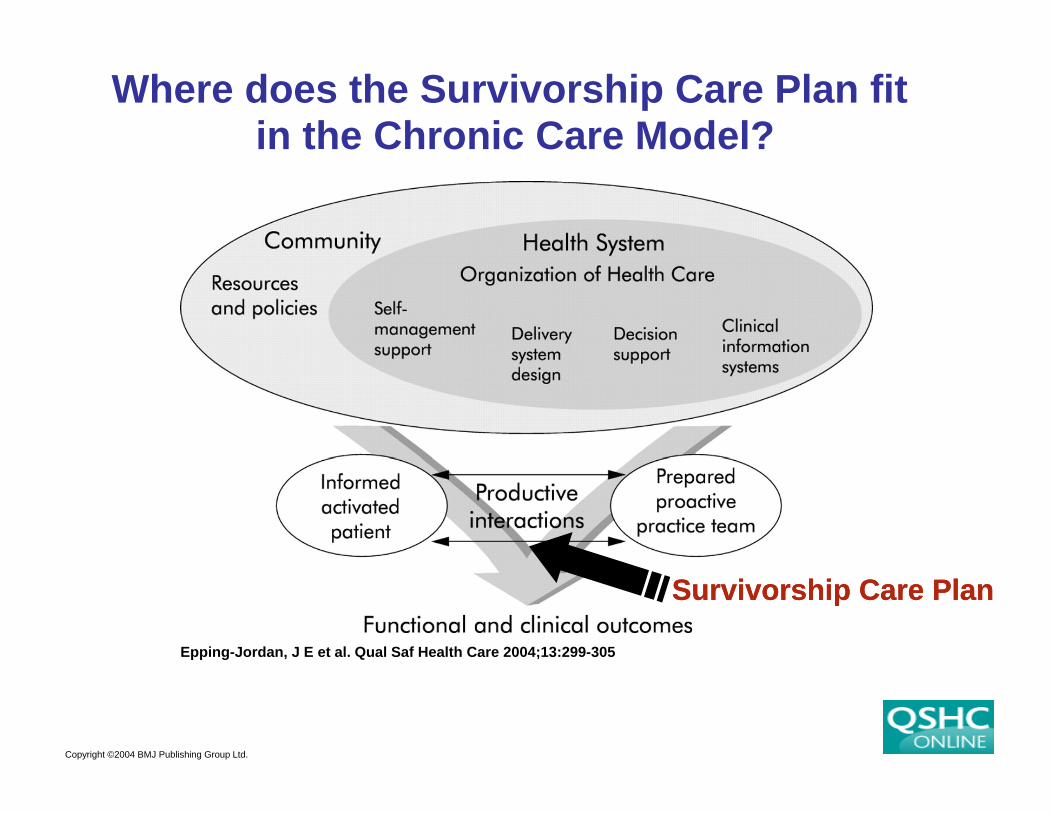
Where does the Survivorship Care Plan fitin the Chronic Care Model?
Epping-Jordan, J E et al. Qual Saf Health Care 2004;13:299-305
Survivorship Care PlanSurvivorship Care Plan
Copyright ©2004 BMJ Publishing Group Ltd.
What are the barriers to routine generation of a treatment summary andgeneration of a treatment summary and
survivorship care plan?
• An expectation in some specialties and not others (e.g. radiation therapy vs. medical ( g pyoncology)
• Lack of appreciation of the need and value added
• Lack of time/reimbursement• Lack of awareness that survivors and primary
care physicians need improved communicationcommunication
Oncology Community’s Response to h IOM Rthe IOM Report
• American Society of Clinical Oncology (ASCO)American Society of Clinical Oncology (ASCO) has developed templates for patients finishing adjuvant therapy for breast and colon cancer
• Generic template and lung cancer templates also available
• ASCO has worked with electronic health record vendors to extract treatment plan and treatment
di l f h l i dsummary directly from the electronic record• See www.asco.org/treatmentsummary
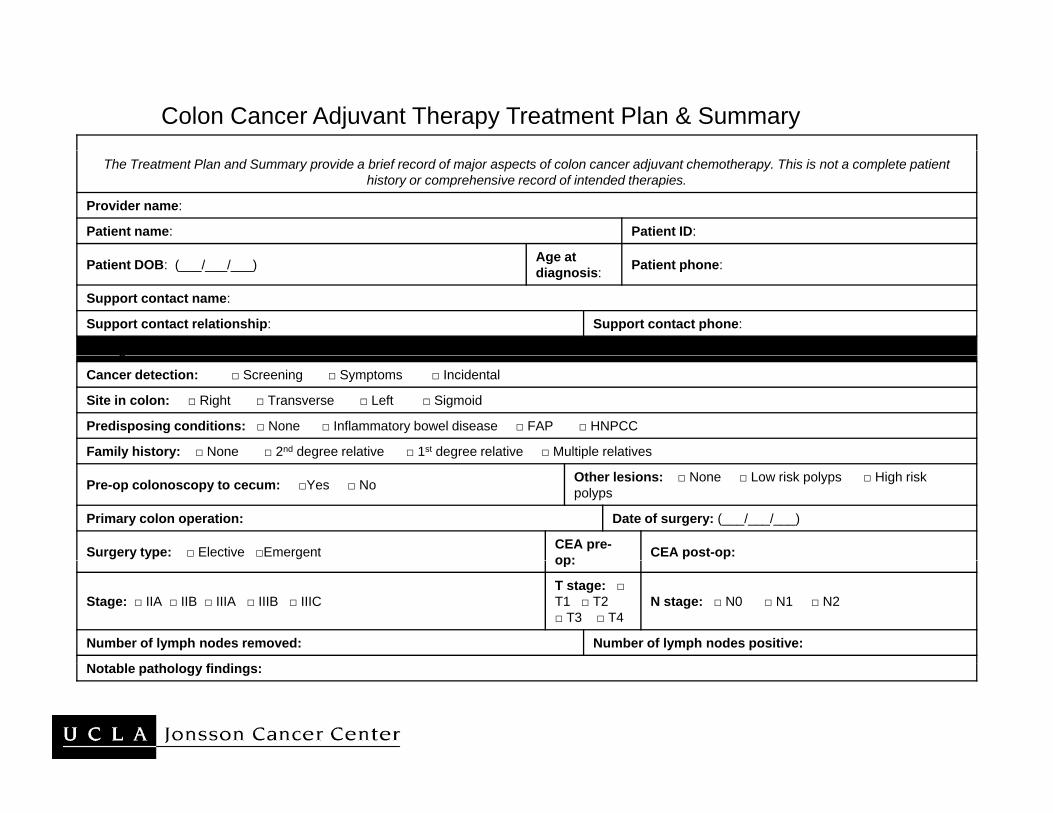
Colon Cancer Adjuvant Therapy Treatment Plan & Summary
The Treatment Plan and Summary provide a brief record of major aspects of colon cancer adjuvant chemotherapy. This is not a complete patient history or comprehensive record of intended therapies.
Provider name:
Patient name: Patient ID:
A tPatient DOB: (___/___/___) Age at diagnosis: Patient phone:
Support contact name:
Support contact relationship: Support contact phone:
Background Informationg
Cancer detection: □ Screening □ Symptoms □ Incidental
Site in colon: □ Right □ Transverse □ Left □ Sigmoid
Predisposing conditions: □ None □ Inflammatory bowel disease □ FAP □ HNPCC
Family history: □ None □ 2nd degree relative □ 1st degree relative □ Multiple relativesy y g g p
Pre-op colonoscopy to cecum: □Yes □ No Other lesions: □ None □ Low risk polyps □ High risk polyps
Primary colon operation: Date of surgery: (___/___/___)
Surgery type: □ Elective □Emergent CEA pre-op: CEA post-op:op:
Stage: □ IIA □ IIB □ IIIA □ IIIB □ IIIC T stage: □T1 □ T2 □ T3 □ T4
N stage: □ N0 □ N1 □ N2
Number of lymph nodes removed: Number of lymph nodes positive:
Notable pathology findings:
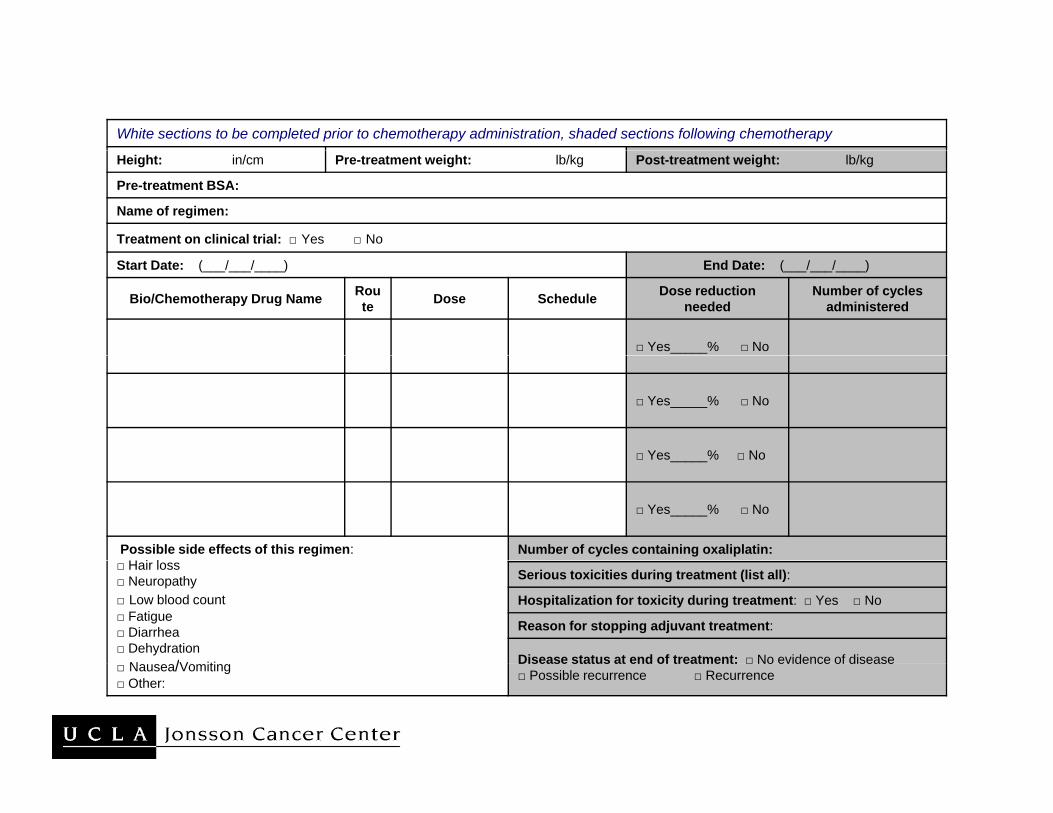
White sections to be completed prior to chemotherapy administration, shaded sections following chemotherapy
Height: in/cm Pre-treatment weight: lb/kg Post-treatment weight: lb/kg
Pre-treatment BSA:
Name of regimen:
Treatment on clinical trial: □ Yes □ No
Start Date: (___/___/____) End Date: (___/___/____)
Bio/Chemotherapy Drug Name Route Dose Schedule Dose reduction
neededNumber of cycles
administered
□ Yes_____% □ No
□ Yes_____% □ No
□ Yes % □ No□ Yes_____% □ No
□ Yes_____% □ No
Possible side effects of this regimen:H i l
Number of cycles containing oxaliplatin:□ Hair loss □ Neuropathy □ Low blood count □ Fatigue □ Diarrhea □ Dehydration
N /V iti
Serious toxicities during treatment (list all):
Hospitalization for toxicity during treatment: □ Yes □ No
Reason for stopping adjuvant treatment:
Disease status at end of treatment: □ No evidence of disease□ Nausea/Vomiting□ Other:
Disease status at end of treatment: □ No evidence of disease□ Possible recurrence □ Recurrence
Current status:I l i d E l iImplementation and Evaluation
• In 2008, ASCO introduced treatmentIn 2008, ASCO introduced treatment summary & care plan as a quality improvement measure p
• Increasing visibility of cancer survivorship and survivorship programs using some p p g gform of treatment summary
• LIVESTRONG Survivorship Centers of pExcellence
• Other efforts – www.journeyforward.orgj y g
When does long-term survivorship begin?• Definitional problems should it begin• Definitional problems…should it begin
at the moment of diagnosis when treatment decisions are being made?treatment decisions are being made?
• The eye is in the beholder…for some ti t d id it i lpatients and providers, it is only many
years later, or after some of the late ff t teffects are apparent
• Problem of labeling
Survivorship Health Care DeliverySurvivorship Health Care Delivery
• Ganz’s Three P’s of Survivor Care• Ganz s Three P s of Survivor Care–Palliation–Prevention
Health Promotion–Health Promotion
Symptom Management/Palliative Care:A I t l P t f S i hi CAn Integral Part of Survivorship Care
• Definition of Palliative Care:Definition of Palliative Care: – Medical care or treatment that concentrates
on reducing the severity of disease symptoms g y y p(particularly if there is not a curative medical treatment)
– Goal is to prevent and relieve suffering and to improve QOL for people facing complex illillness
• Focus on the most severe and prolonged tsymptoms
Common Palliative Care Concerns• Pain
F ti• Fatigue• Depression
Ph i l li it ti• Physical limitations• Cognitive changes
L h d• Lymphedema• Sexual dysfunction• Menopause related symptoms• Body Image
Consultant Specialists Required
• Mental healthMental health• Pain management• Physical medicine/vocational rehab• Physical medicine/vocational rehab• Endocrinology
C di l• Cardiology• Gynecology/fertility• Pulmonary• Neurology/neuropsychology
PreventionPrevention
• Systematic ongoing follow-up required forSystematic ongoing follow up required for screening
Goal: early detection and early intervention for– Goal: early detection and early intervention for potentially serious late-onset complications e.g., cataracts, osteoporosis, cardiac diseaseg , , p ,
– Chemoprevention when available– Life style modification to prevent secondLife style modification to prevent second
cancers
Health PromotionHealth Promotion
• Health promotion counselingHealth promotion counseling – Goal: promote risk reduction for health
problems that commonly present during adulthood ( esp. for childhood cancer survivors)Avoid weight gain– Avoid weight gain
– Increase physical activityAvoidance of exposures that are harmful– Avoidance of exposures that are harmful
– Decrease risk of other chronic diseases, e.g. diabetes, heart diseasediabetes, heart disease
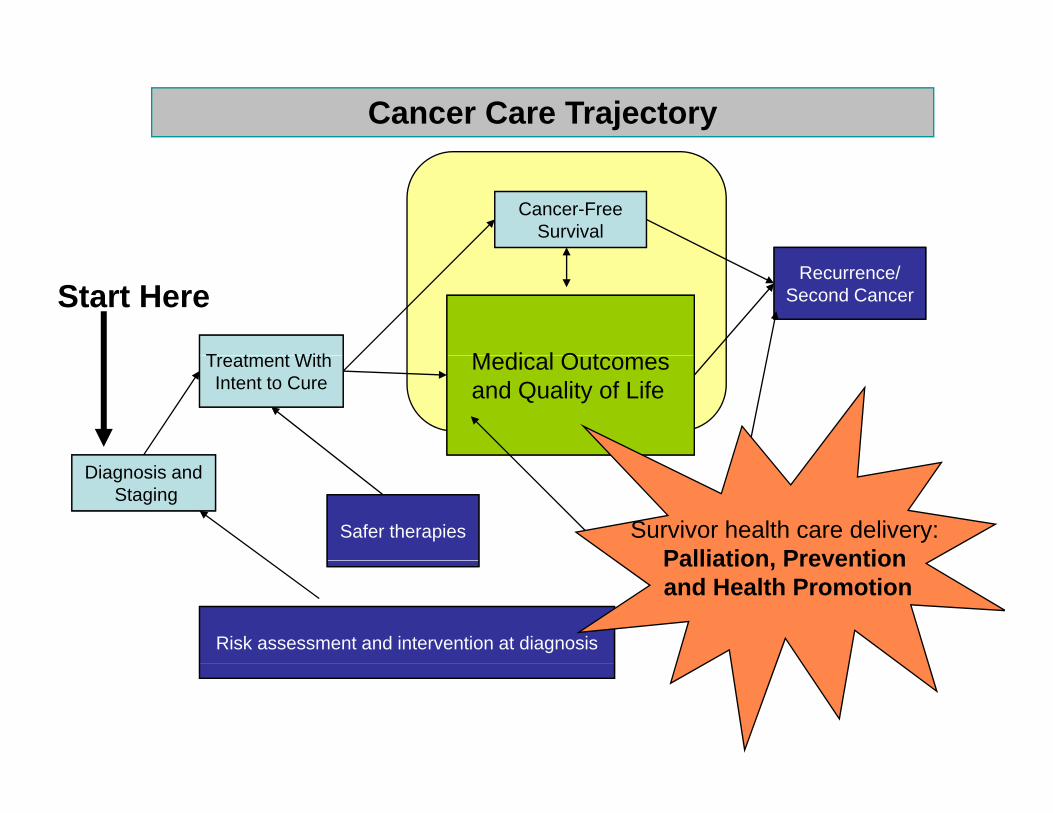
Cancer Care Trajectory
Cancer-FreeSurvival
T t t With M di l O t
Recurrence/Second CancerStart Here
Treatment With Intent to Cure
Medical Outcomesand Quality of Life
Diagnosis andStaging
Safer therapies Survivor health care delivery: Palliation Prevention
Risk assessment and intervention at diagnosis
Palliation, Prevention and Health Promotion
Opportunitiespp• At the minimum, we must prepare a
treatment summary on every patienttreatment summary on every patient completing curative-intent therapy…
• Focus on primary secondary and tertiary• Focus on primary, secondary and tertiary prevention of long-term and late effects
• Use treatment summary & care plan to• Use treatment summary & care plan to facilitate sharing and coordination of care
Outcomes & MetricsOutcomes & Metrics
• Adherence to cancer surveillanceAdherence to cancer surveillance• Adherence to cancer therapies (e.g.
adjuvant endocrine therapy)adjuvant endocrine therapy)• Other health maintenance and promotion,
e.g. smoking cessation, weight control,e.g. smoking cessation, weight control, physical activity, immunizations
• Management of psychosocial distress,Management of psychosocial distress, depression
• Prevention of second cancersPrevention of second cancers
ResourcesIOM: Lost in Transition report from 2005IOM: Implementing the Survivorship CareIOM: Implementing the Survivorship Care Planning, Workshop Report, 2006JCO Special Review Issue: CancerJCO Special Review Issue: Cancer Survivorship, November 10, 2006M. Feuerstein (ed.) Handbook of CancerM. Feuerstein (ed.) Handbook of Cancer Survivorship, Springer, 2007P. Ganz (ed.) Cancer Survivorship: TodayP. Ganz (ed.) Cancer Survivorship: Today and Tomorrow, Springer, 2007
VITA stands for....“Vital Information and Tailored Assessment”Vital Information and Tailored Assessment
The VITA Program is the clinical arm ofThe VITA Program is the clinical arm ofUCLA-LIVESTRONG Survivorship COE
http://vita.mednet.ucla.edu/
What is needed to implementWhat is needed to implement the survivorship care plan?
Acceptance of cancer as a chronic disease—following an initial period of extraordinarily complex therapy!therapy!Reimbursement for evaluation and management time required to prepare and communicate the planExpand the evidence-base of knowledge re: late effects, follow-up needs and survivorship careTrain all health professionals in the needs of theTrain all health professionals in the needs of the growing number of cancer survivors—how to act on the care plan recommendations
Cancer Survivorship Care Plans:pA model for integration of QOL & QOC
Quality of Life Quality of Care