Embed Size (px)
Citation preview
Rehabilitation Issues In Breast Cancer Survivorship
Maryam B Lustberg, MD MPH Medical Director of Survivorship
The OSU Comprehensive Cancer Center
Outline
Recent updates in breast cancer management Common symptoms faced by breast cancer survivors:
- Chemotherapy induced neuropathy - Chemobrain - Arthralgias
Exercise prescription Current challenges and future direction in Oncorehab and breast
cancer survivorship
Recent Updates in Breast Cancer Management
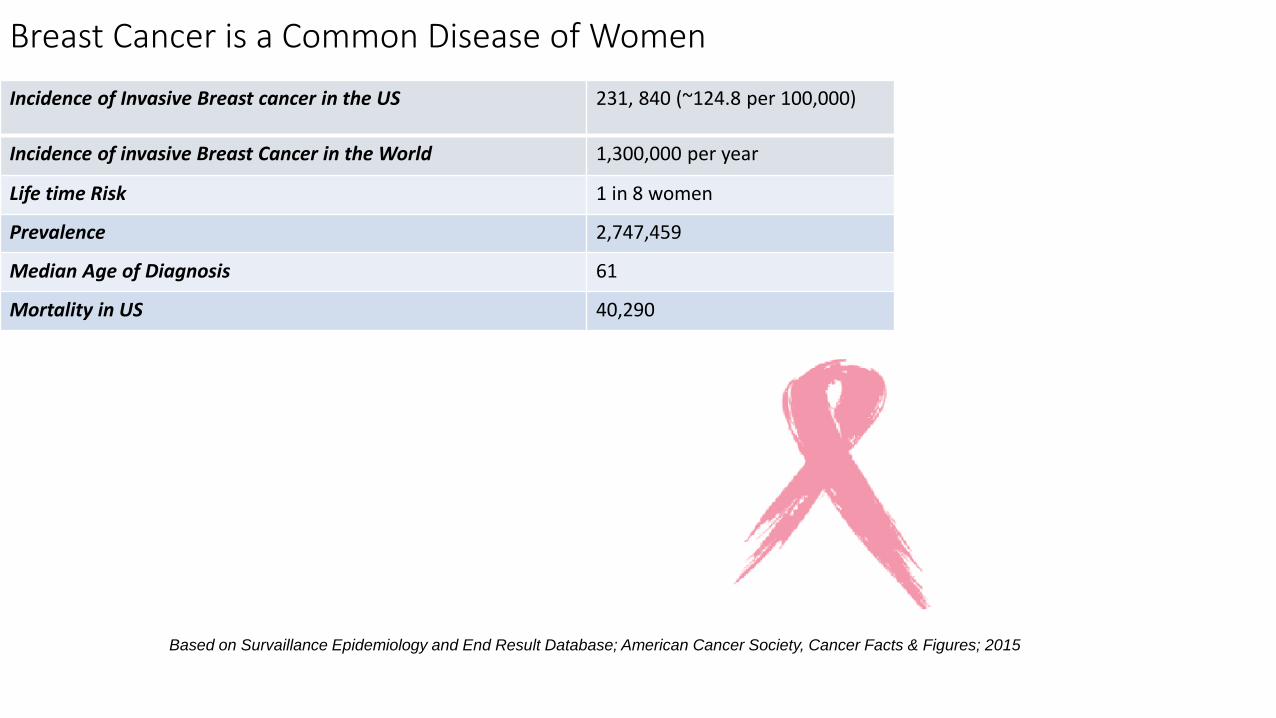
Breast Cancer is a Common Disease of Women
Incidence of Invasive Breast cancer in the US 231, 840 (~124.8 per 100,000)
Incidence of invasive Breast Cancer in the World 1,300,000 per year
Life time Risk 1 in 8 women
Prevalence 2,747,459
Median Age of Diagnosis 61
Mortality in US 40,290
Based on Survaillance Epidemiology and End Result Database; American Cancer Society, Cancer Facts & Figures; 2015
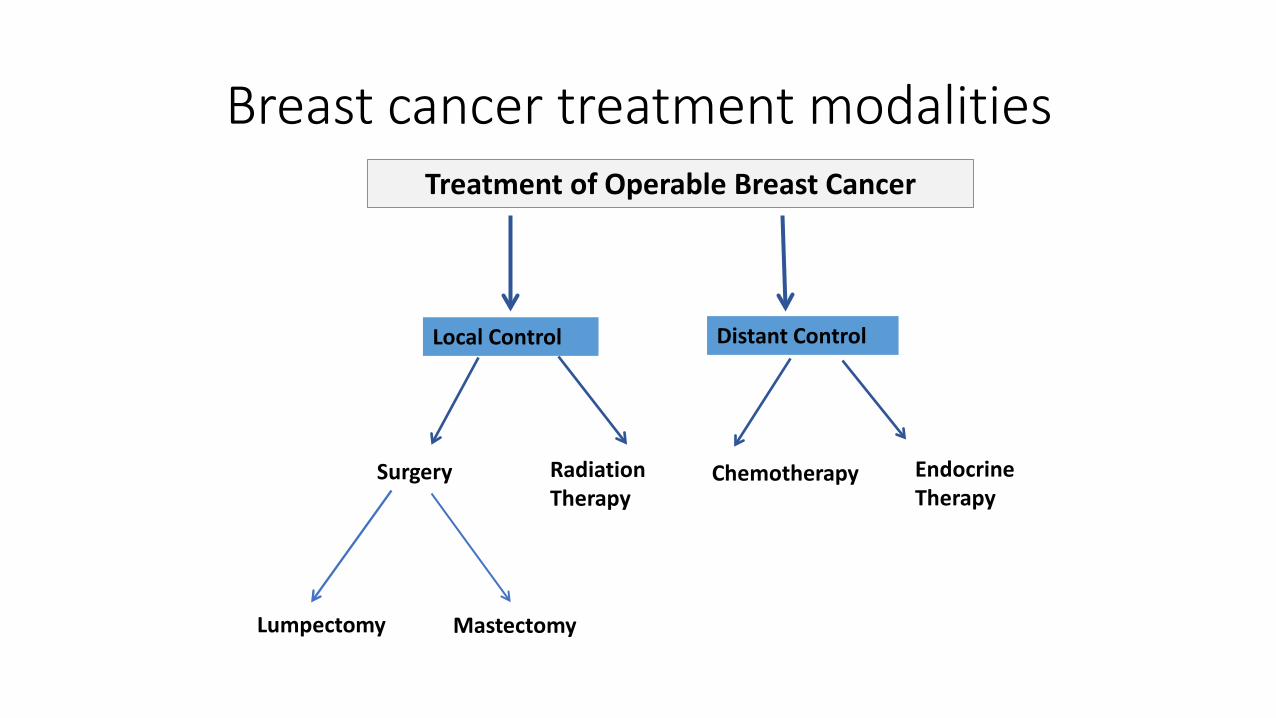
Breast cancer treatment modalities Treatment of Operable Breast Cancer
Surgery Chemotherapy
Local Control
Radiation Therapy
Distant Control
Endocrine Therapy
Lumpectomy Mastectomy
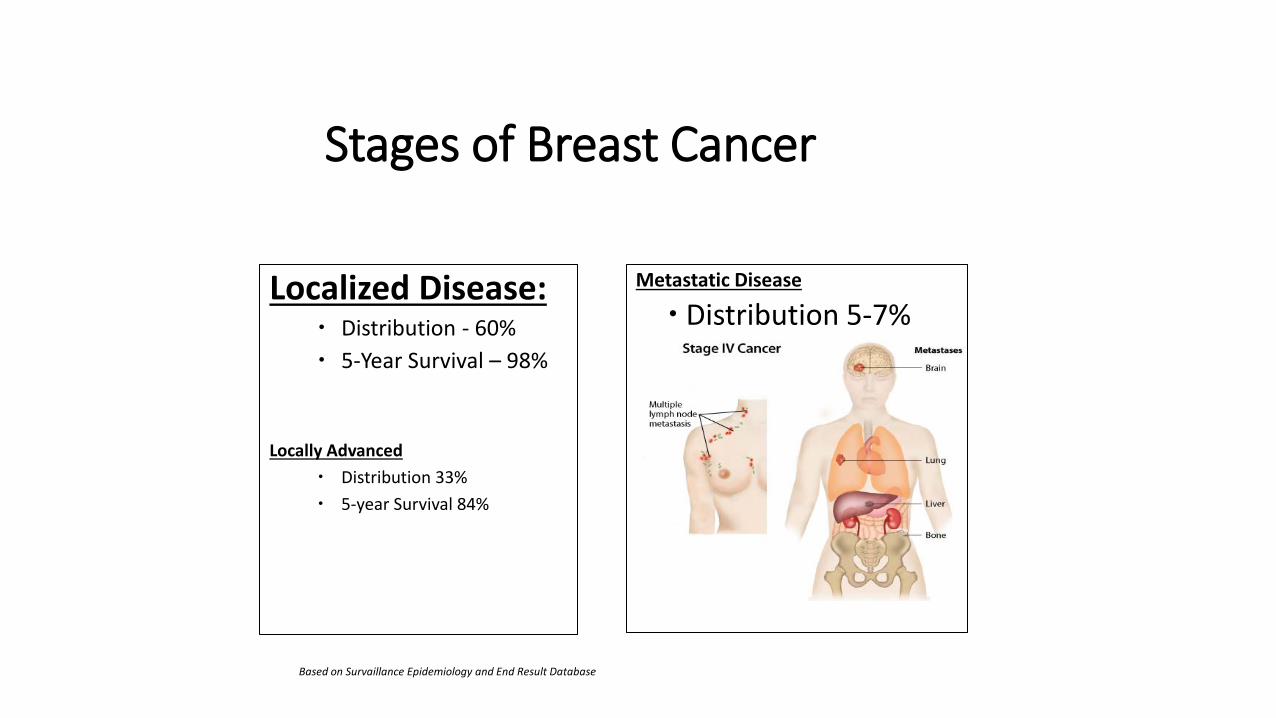
Stages of Breast Cancer
Localized Disease: Distribution - 60% 5-Year Survival – 98%
Locally Advanced
Distribution 33% 5-year Survival 84%
Metastatic Disease
Distribution 5-7% 5-year survival 23%
Based on Survaillance Epidemiology and End Result Database
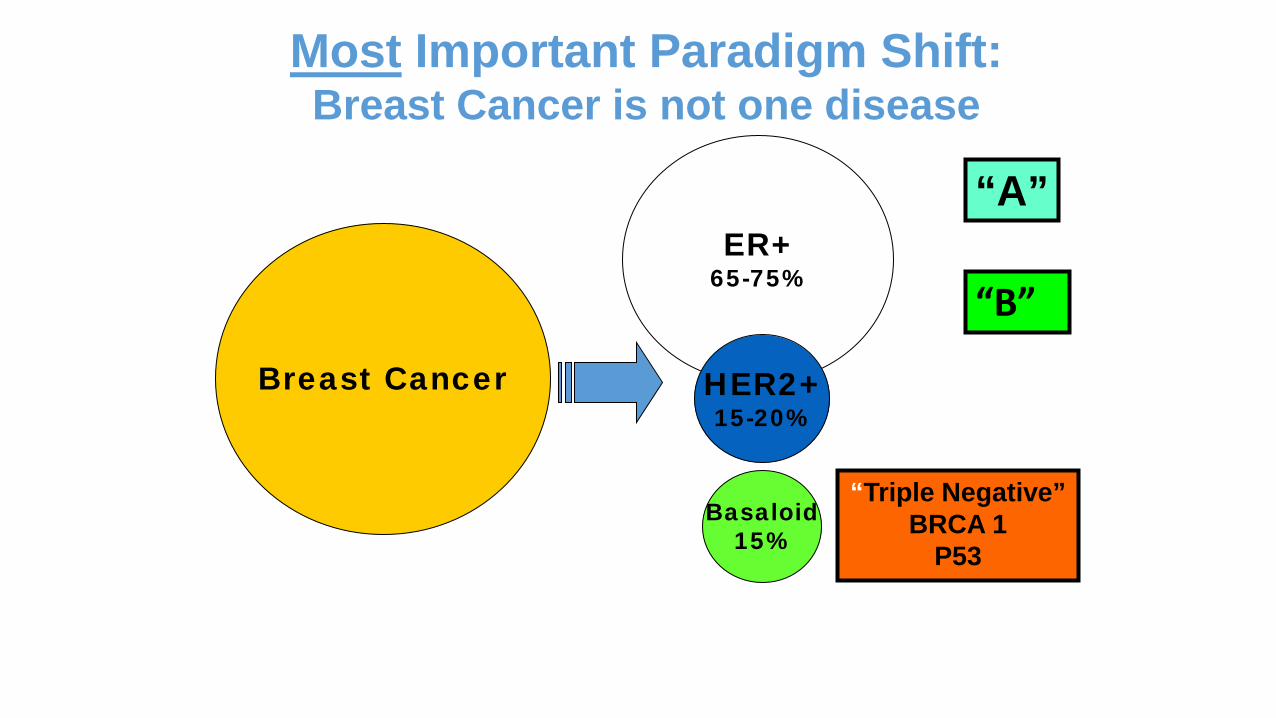
Breast Cancer
ER+ 65-75%
HER2+ 15-20%
Basaloid 15%
Most Important Paradigm Shift: Breast Cancer is not one disease
“Triple Negative” BRCA 1
P53
“A”
“B”
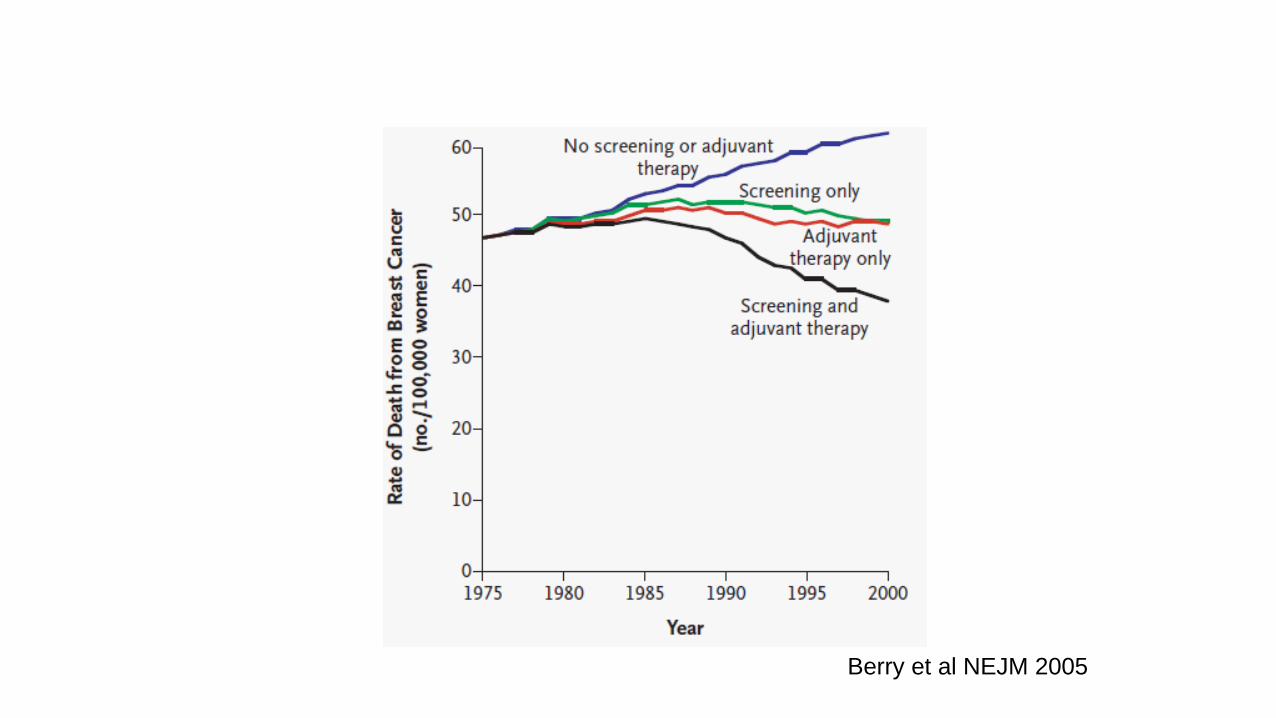
Berry et al NEJM 2005
Breast Cancer: Then and Now
Then ~75% of women survived ≥5 years Mastectomy was the only surgical option Single-agent chemotherapy was standard of
care Hormonal therapy with tamoxifen was
under investigation only Genes involved in breast cancer
development have not yet been identified
Now ~95% of women survive ≥5 years Lumpectomy is available Combination chemotherapy is the standard
of care Hormonal therapy is widely used Receptor-based therapy is widely used Understanding of genetic components have
expanded
National Cancer Institute. Available at: http://www.cancer.gov/cancertopics/cancer-advances-in-focus/breast.
Breast Cancer Systemic Therapy Options
Endocrine Therapy Chemotherapy Biologics (trastuzumab, pertuzumab)
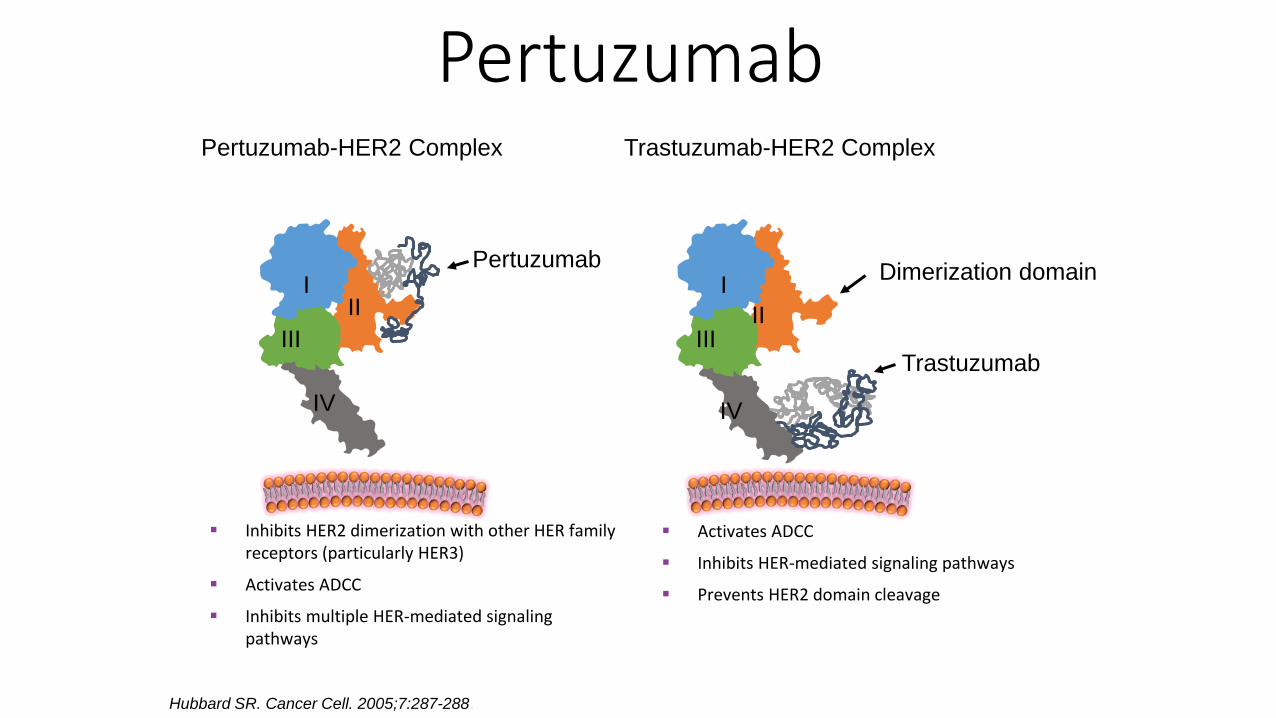
Pertuzumab
Hubbard SR. Cancer Cell. 2005;7:287-288.
Pertuzumab-HER2 Complex Trastuzumab-HER2 Complex
Pertuzumab Dimerization domain
Trastuzumab III
II I
Inhibits HER2 dimerization with other HER family receptors (particularly HER3)
Activates ADCC
Inhibits multiple HER-mediated signaling pathways
Activates ADCC
Inhibits HER-mediated signaling pathways
Prevents HER2 domain cleavage
III II
I
IV IV
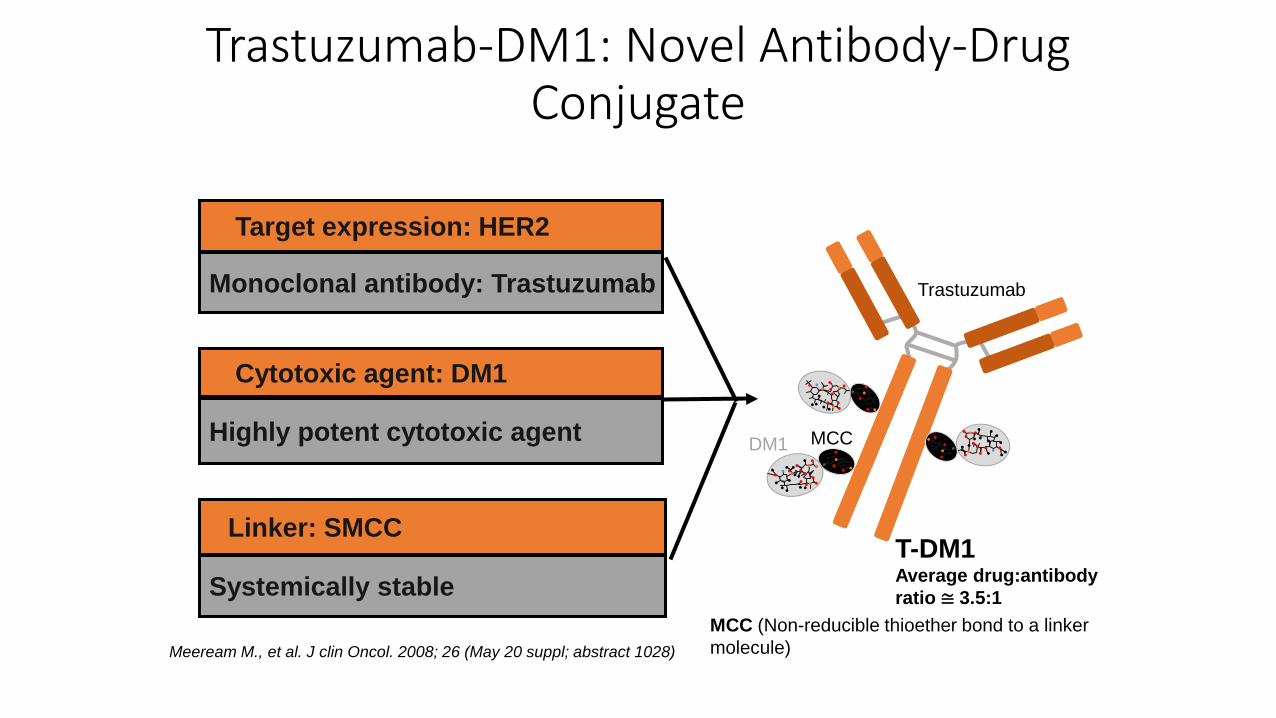
Highly potent cytotoxic agent
Cytotoxic agent: DM1
Monoclonal antibody: Trastuzumab
Target expression: HER2
Systemically stable
Linker: SMCC T-DM1 Average drug:antibody ratio ≅ 3.5:1
Trastuzumab-DM1: Novel Antibody-Drug Conjugate
Trastuzumab
MCC DM1
MCC (Non-reducible thioether bond to a linker molecule) Meeream M., et al. J clin Oncol. 2008; 26 (May 20 suppl; abstract 1028)
Good news
We are using less chemotherapy and smarter targeted therapies Selecting for higher risk tumors using tissue profiling (Oncotype Dx)
Bad news
Our newer endocrine therapy options are more toxic than tamoxifen More arthralgias More fatigue More weight gain
Bad news
When we do use chemotherapy, our regimens in some ways have become more dose dense and toxic Longer duration of therapy: 1 year for Her2 + disease
Good news
We know more about the benefits of lifestyle modifications- nutrition and exercise than ever before Cancer diagnosis and treatment are filled with teachable moments
and opportunities for change
Bad news
It’s not so easy to change Many survivors continue to struggle and are not facing the effects of
treatment related toxicities (neuropathy, chemobrain, fatigue etc)
Common symptoms faced by breast cancer survivors
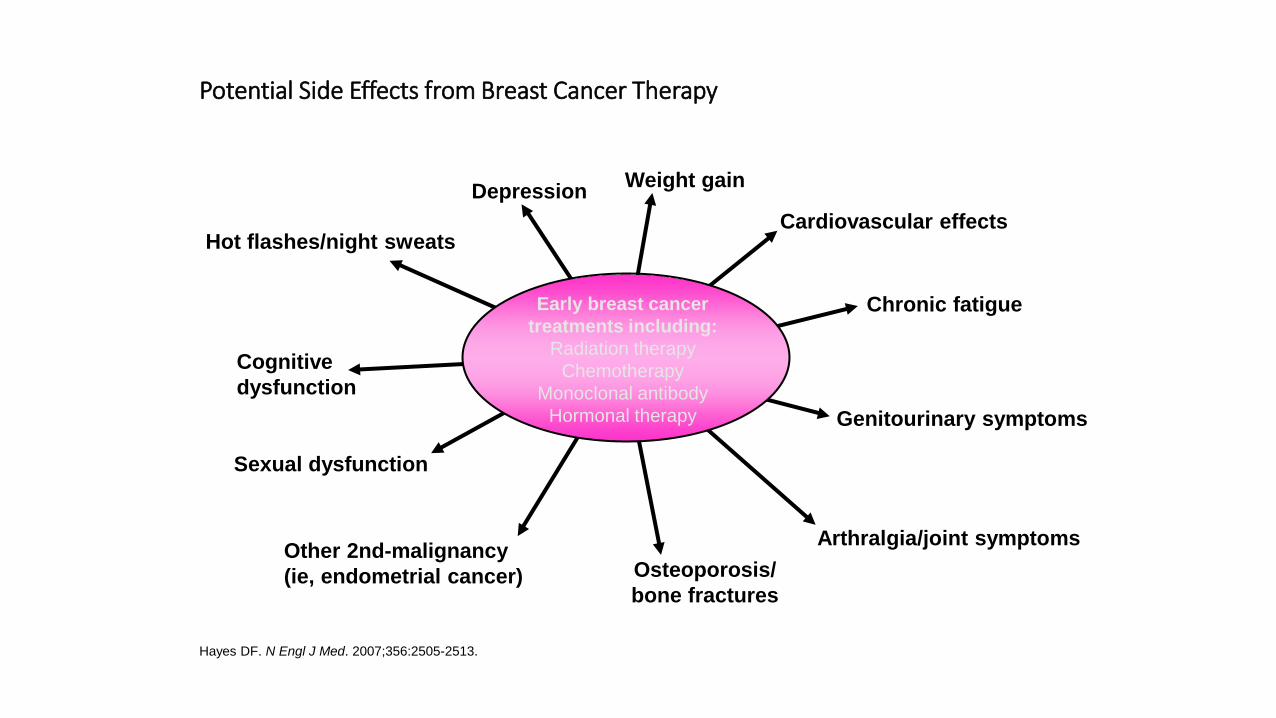
Potential Side Effects from Breast Cancer Therapy
Hayes DF. N Engl J Med. 2007;356:2505-2513.
Hot flashes/night sweats
Arthralgia/joint symptoms
Sexual dysfunction
Cognitive dysfunction
Depression
Genitourinary symptoms
Other 2nd-malignancy (ie, endometrial cancer)
Chronic fatigue
Cardiovascular effects
Osteoporosis/ bone fractures
Early breast cancer treatments including:
Radiation therapy Chemotherapy
Monoclonal antibody Hormonal therapy
Weight gain
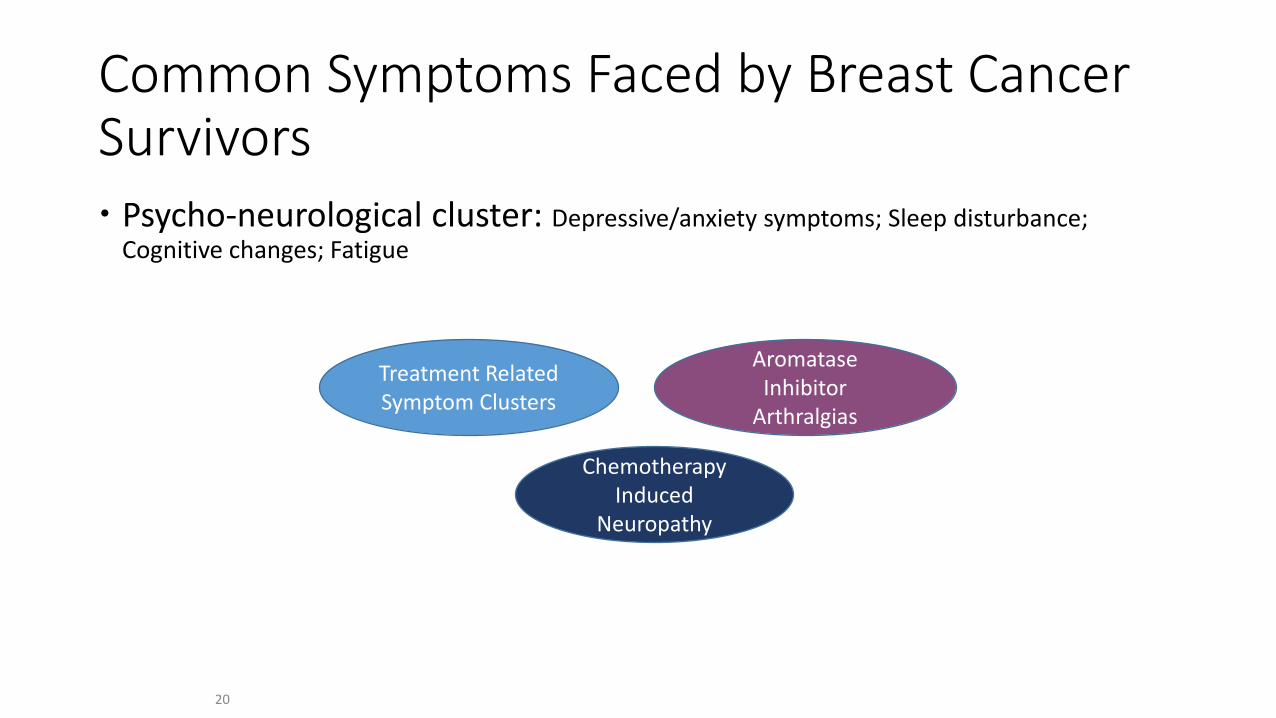
Common Symptoms Faced by Breast Cancer Survivors Psycho-neurological cluster: Depressive/anxiety symptoms; Sleep disturbance;
Cognitive changes; Fatigue
20
Treatment Related Symptom Clusters
Chemotherapy Induced
Neuropathy
Aromatase Inhibitor
Arthralgias
Mechanistic Biologic Rationale of Symptom Toxicities
21
Is still missing. We began to look at chemotherapy effects in mice and humans to better understand the role of central inflammation in symptom cluster as well in chemotherapy induced neuropathy.
Mouse model of chemotherapy Human clinical trials; natural history and Intervention studies
Overarching Hypothesis of our group’s research Neuroinflammation resulting from chemotherapy administration
promotes: Depression Anxiety Cognitive deficits Fatigue. Neuropathy
22
Chemotherapy induced neuropathy
Chemotherapy induced neuropathy (CIPN)
Common and can be debilitating Associated with a variety of
chemotherapeutic agents In breast population: taxanes,
eribulin and platinums Impacts ability to give drug, and
has huge impact on function and quality of life
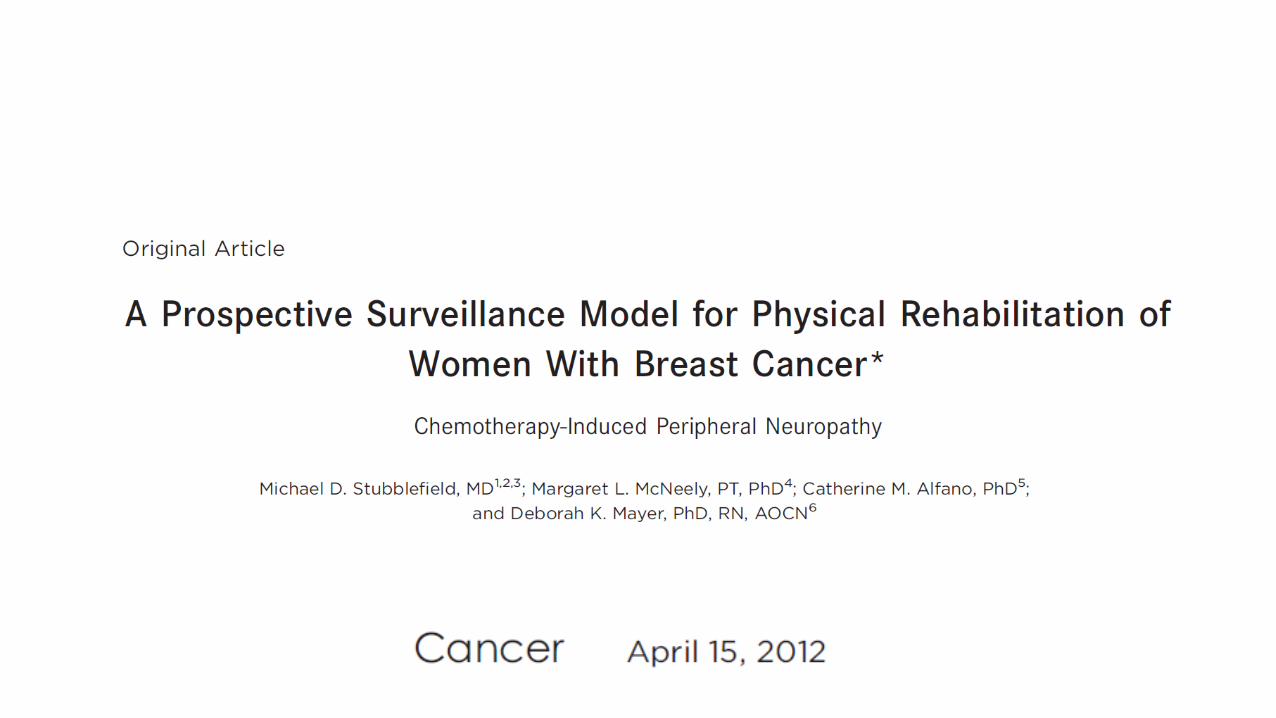
Gaps in Knowledge: CIPN
How severe are quantitative functional effects of CIPN on gait and balance in patients undergoing chemotherapy? Are early changes in these measures predictors of more severe CIPN
with additional therapy? By intervening earlier on functional deficits, can we change the course
of CIPN?
25
CIPN Challenges So common yet so little is known about
*the mechanism of injury **Who is most at risk ***How to prevent it?
****How to treat it?
Summary of preventative strategies for CIPN
There are no agents recommended for the prevention of CIPN.
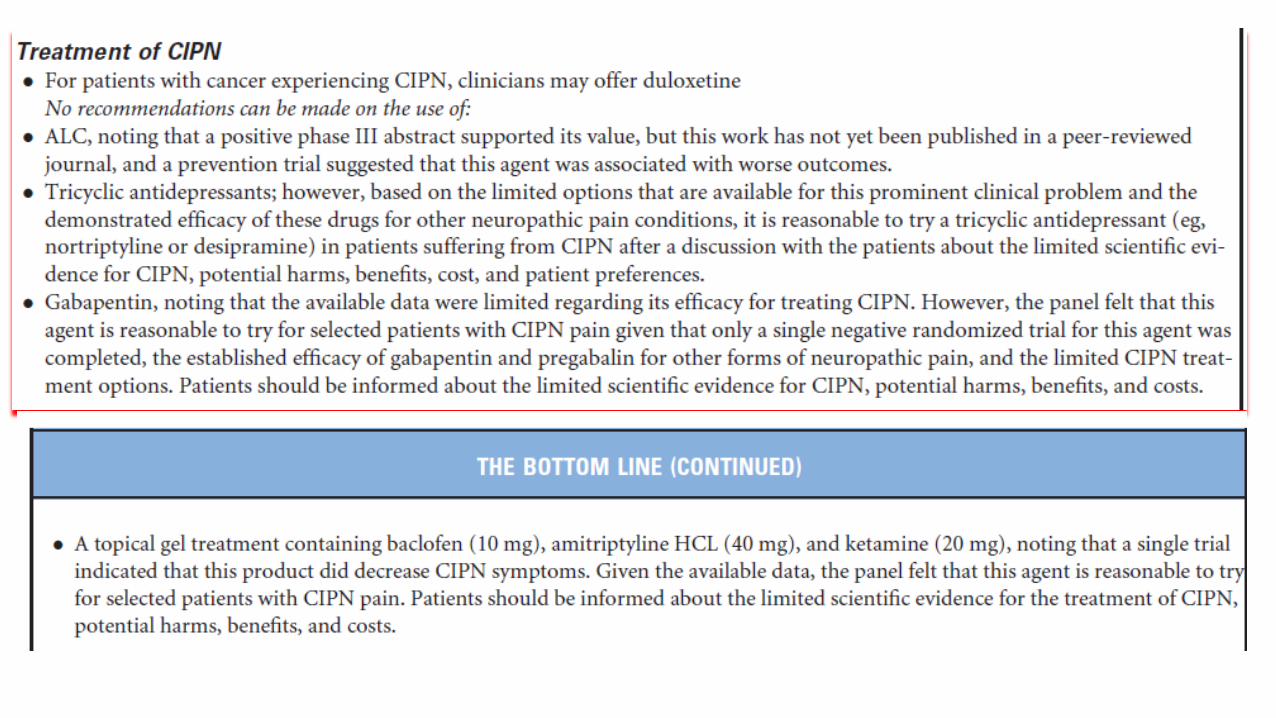
Summary of therapeutic strategies for CIPN
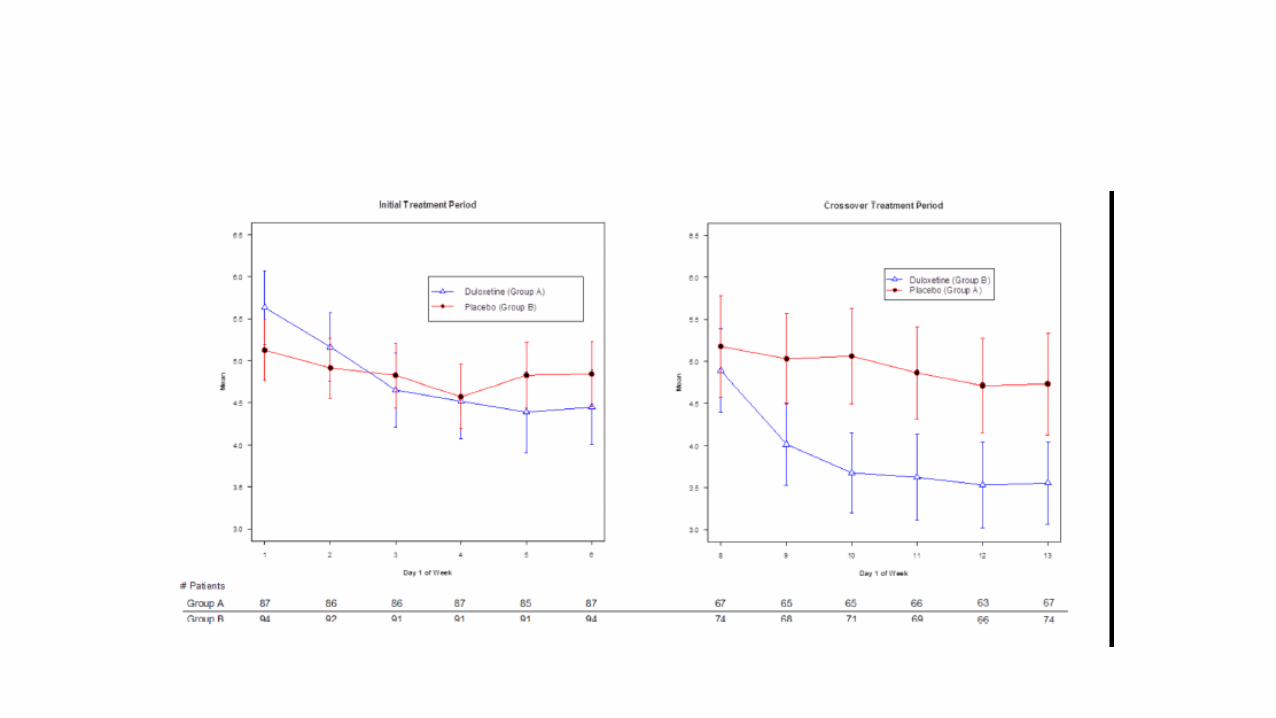
Moderate recommendation for use of duloxetine Based on limited options that are available for this prominent clinical
problem and the demonstrated efficacy of the following agents in other neuropathic conditions, it is reasonable to try
*tricyclic antidepressant such as nortriptyline and amitriptyline *gabapentin *A topical agent including baclofen, amitriptyline, ketamine Discuss with patients limited scientific evidence in patients suffering from
CIPN, potential harms and benefits.
Duloxetine
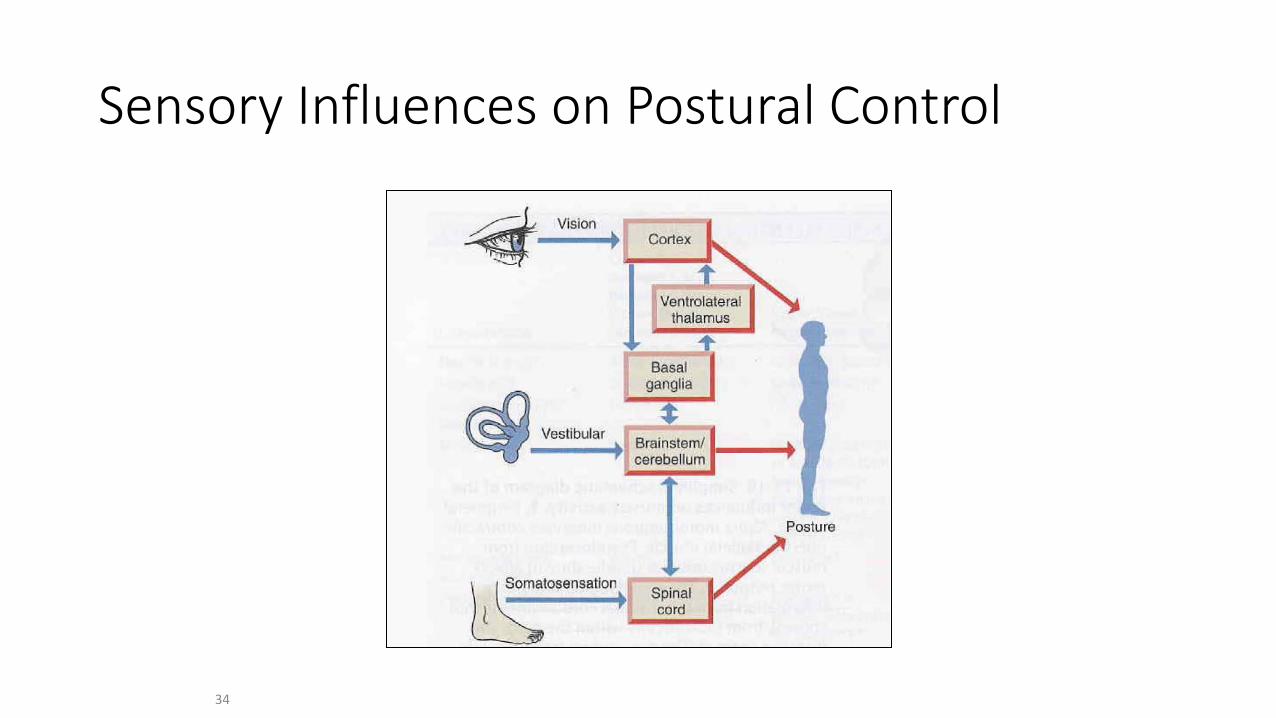
Sensory Influences on Postural Control
34
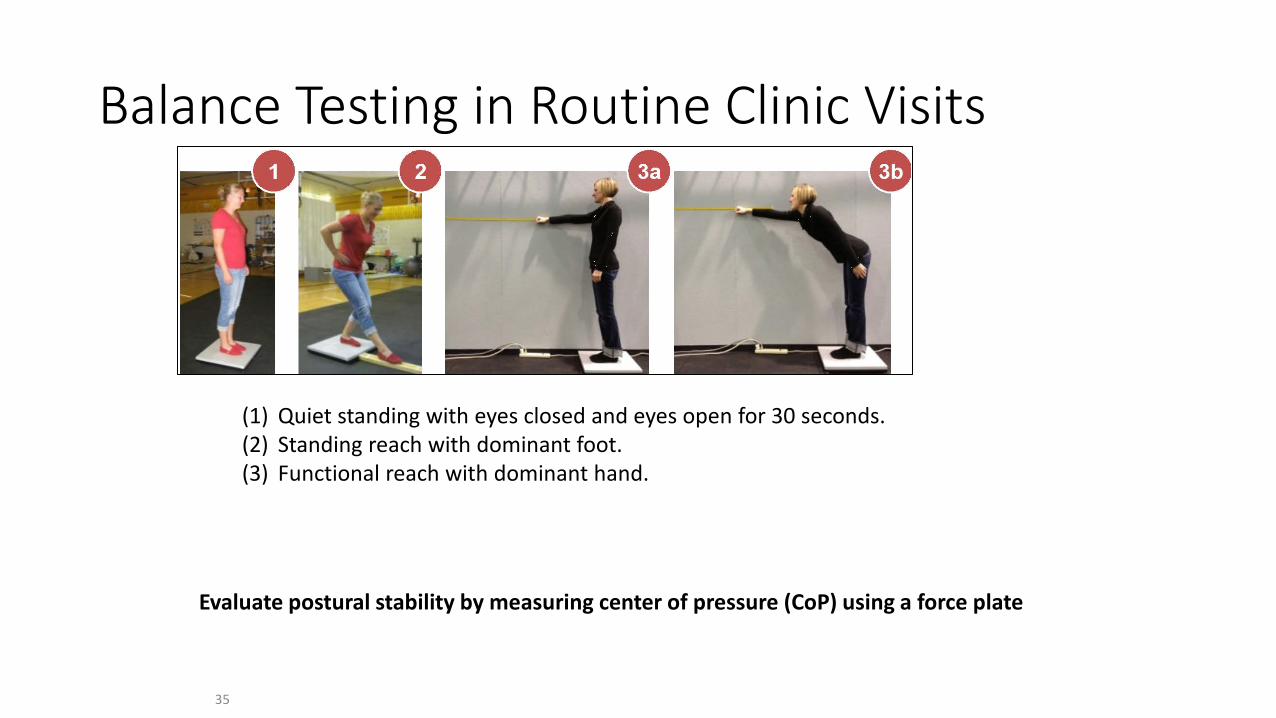
Balance Testing in Routine Clinic Visits
35
(1) Quiet standing with eyes closed and eyes open for 30 seconds. (2) Standing reach with dominant foot. (3) Functional reach with dominant hand.
Evaluate postural stability by measuring center of pressure (CoP) using a force plate
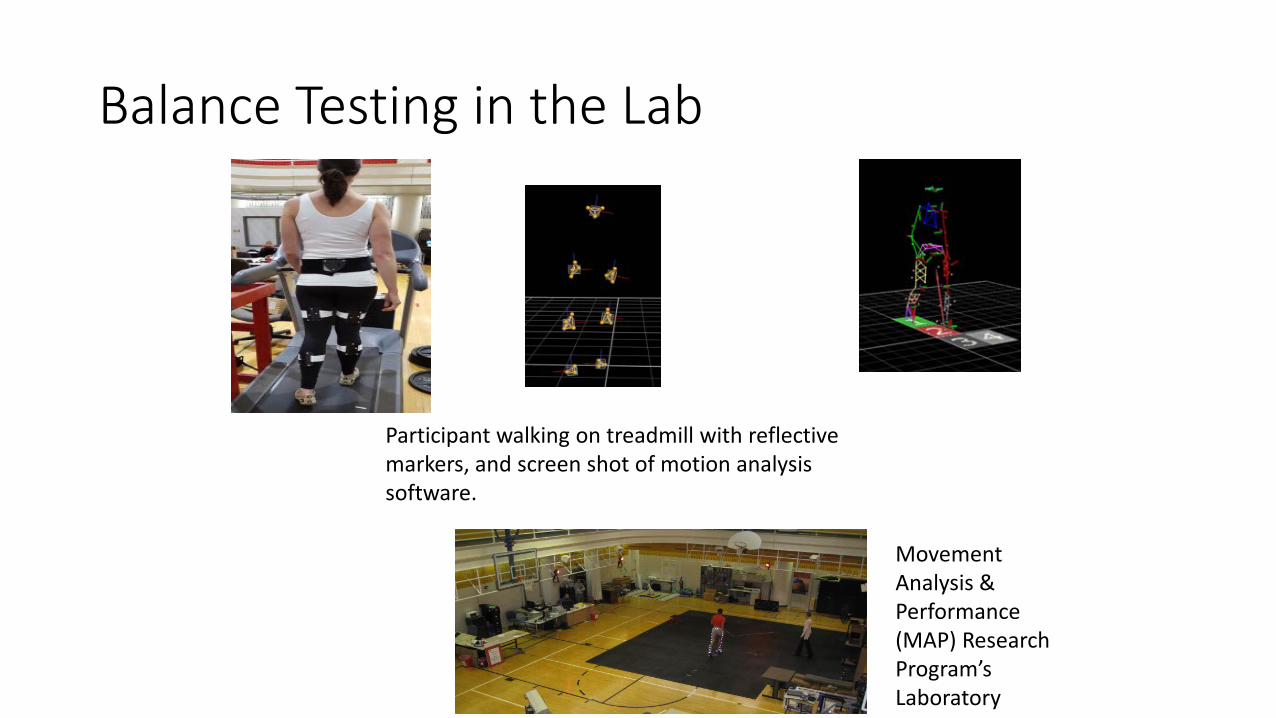
Balance Testing in the Lab
Participant walking on treadmill with reflective markers, and screen shot of motion analysis software.
Movement Analysis & Performance (MAP) Research Program’s Laboratory
OSU 13010 Current NCI R03 (Lustberg, Chaudhari Co-PIs) 30 breast cancer patients accrued Recruited at the time of initiating taxane therapy 30 additional colon cancer patients initiating oxaliplatin therapy will be
accrued next for comparison
38
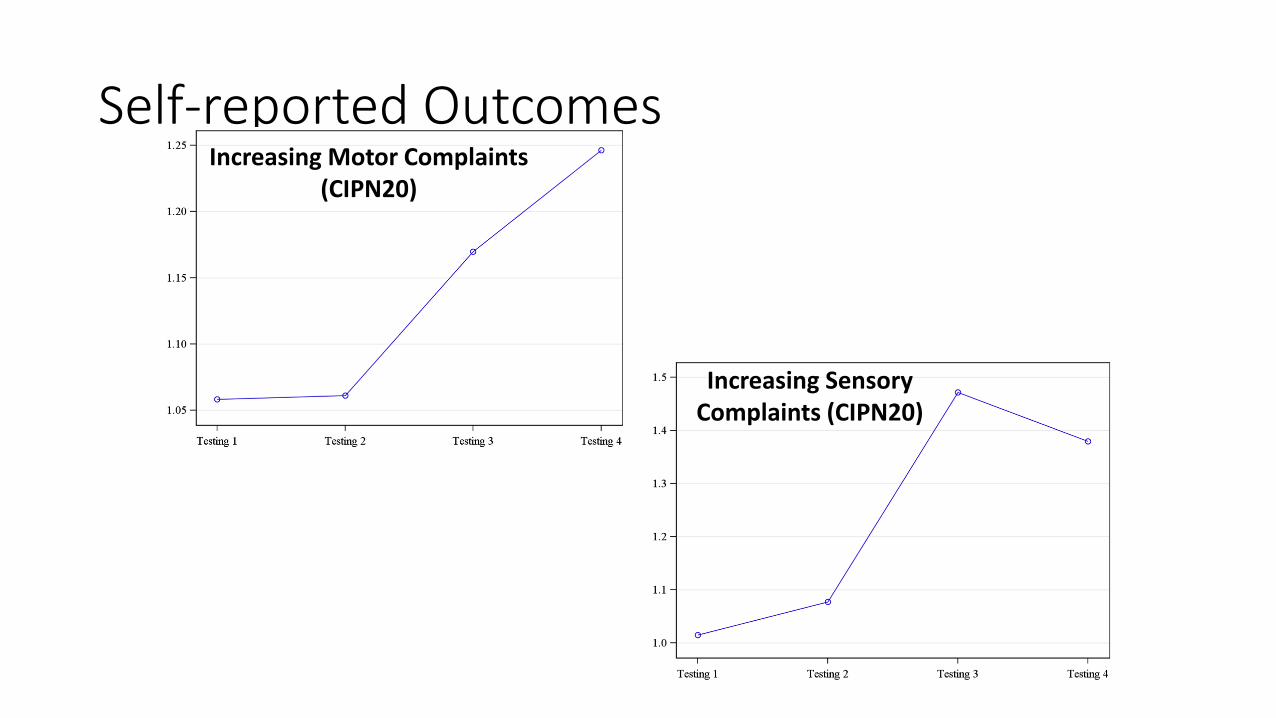
Self-reported Outcomes Increasing Motor Complaints
(CIPN20)
Increasing Sensory Complaints (CIPN20)
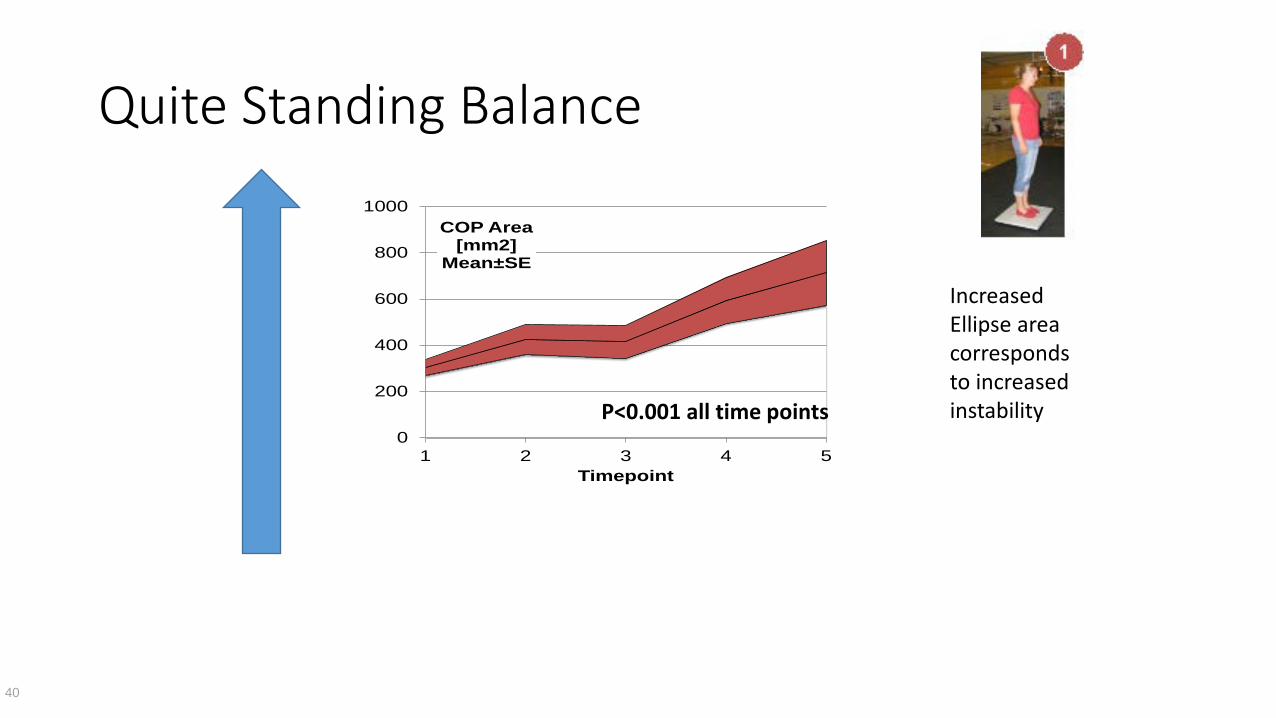
Quite Standing Balance
40
Increased Ellipse area corresponds to increased instability P<0.001 all time points
0
200
400
600
800
1000
1 2 3 4 5
COP Area [mm2]
Mean±SE
Timepoint
Interim Analysis Results
For most of these parameters, the significant changes were observed as early as the 2nd treatment. Pain interference from the BPI-SF did not show any significant
changes throughout the study. Balance and gait testing are feasible in the clinical setting Balance, function and physical functions may all be affected even
without pain symptoms.
Next Steps: Future Clinical Trial Intervene on Early Balance Changes Preclinical evidence is emerging that rigorous treadmill exercise
prevents the development of CIPN in a mouse model by reduction of axonal degeneration. Animals undergoing exersise had normal tubulin levels suggesting
that exercise interferes with paclitaxel’s ability to alter microtubule dynamics in long axons. Upregulated BDNF and other neurotropic factors which may also be
beneficial in mitigating CIPN
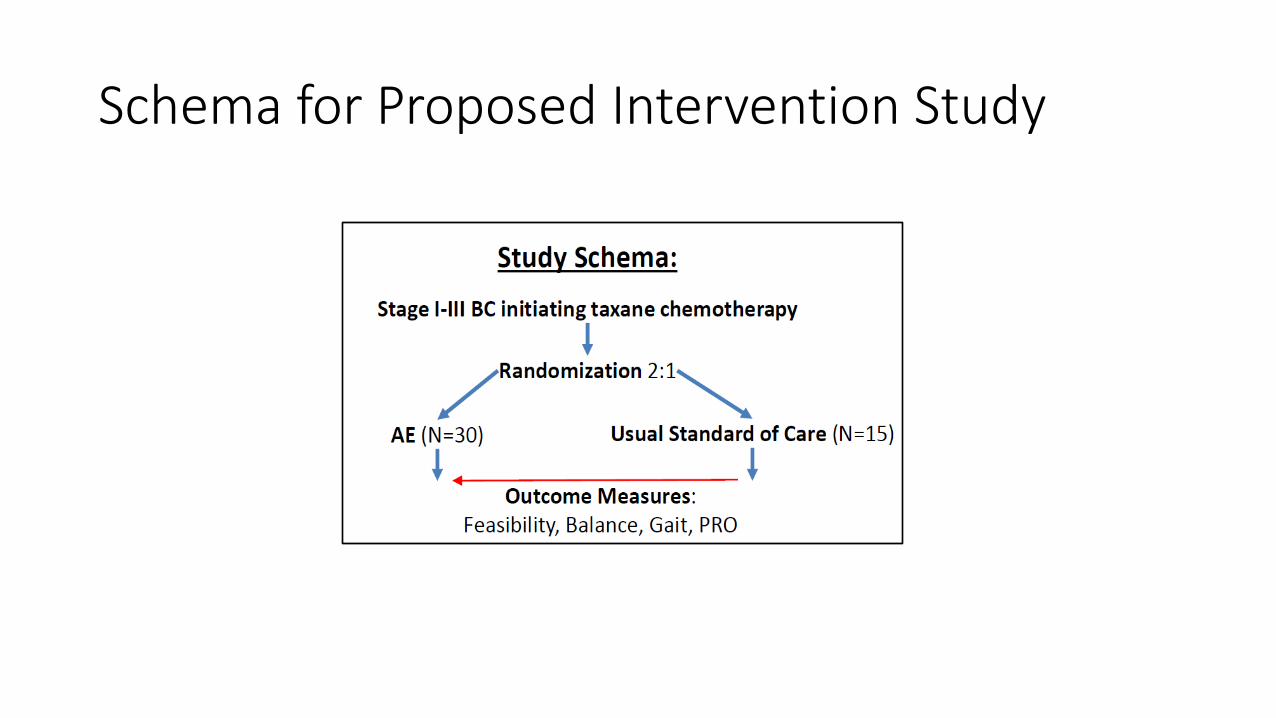
Schema for Proposed Intervention Study
Next Steps: Back to the LabWhat is the Mechanism of Balance Changes? Neurotoxicity is impacting peripheral nervous system Additional mechanistic information and exact role of central neuro-
inflammation not known Role of microglia in spinal cord and brain? Contribution of other symptom clusters to neuropathy symptoms and
vice versa
44
Conceptual Model of Neuropathy
?
Cancer Treatment
Host Factors
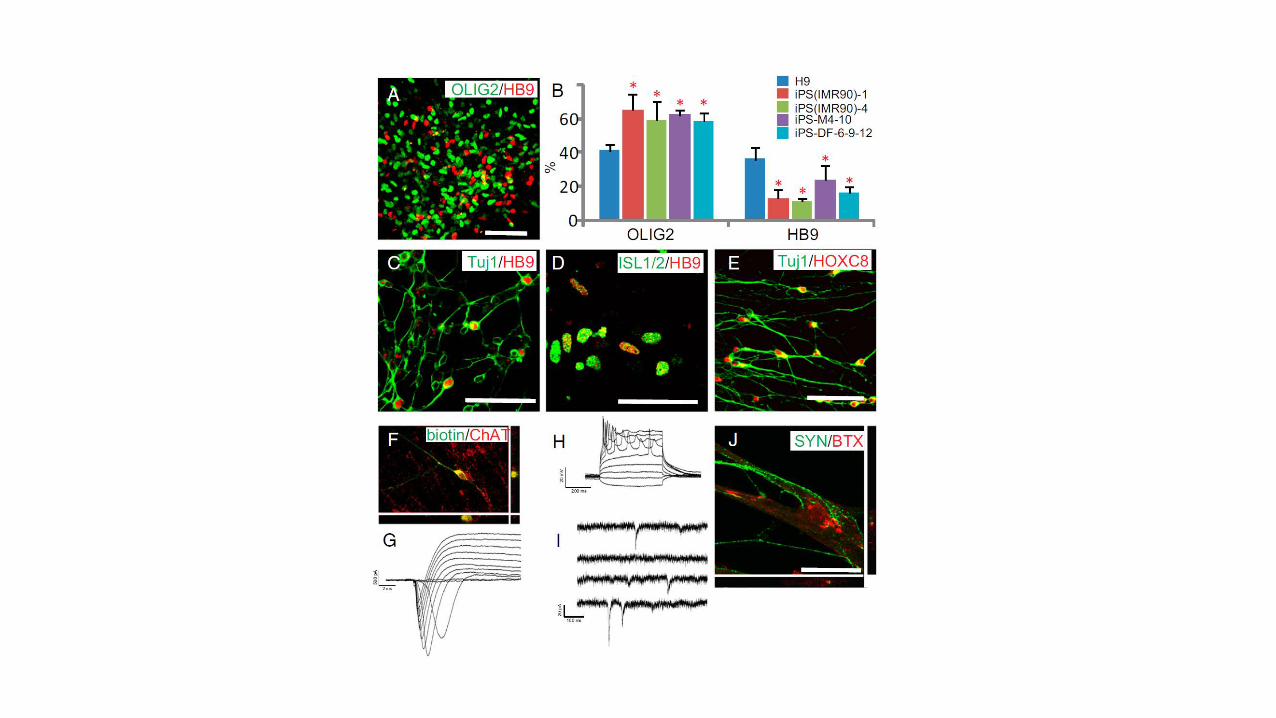
Growing a neuron
Study Design
Case controlled study 20 patients who developed grade 3 CIPN 20 patients who have no recorded symptoms of CIPN
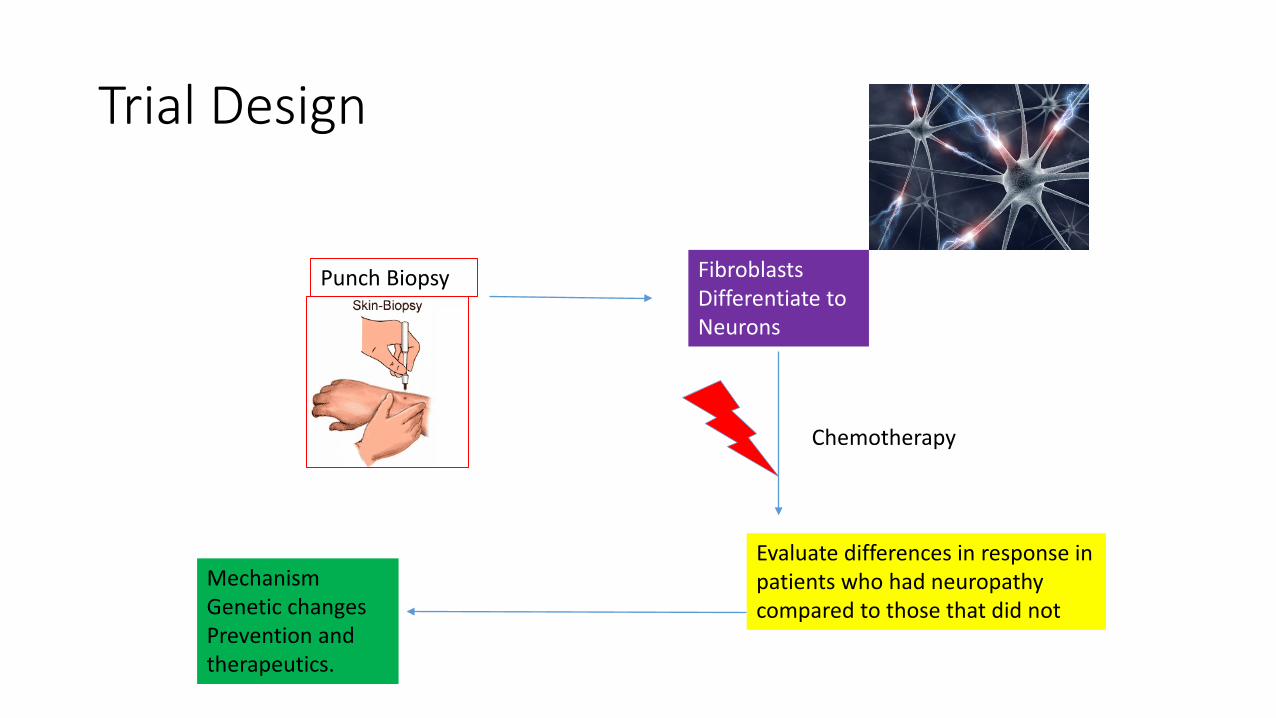
Trial Design
Punch Biopsy Fibroblasts Differentiate to Neurons
Evaluate differences in response in patients who had neuropathy compared to those that did not
Chemotherapy
Mechanism Genetic changes Prevention and therapeutics.
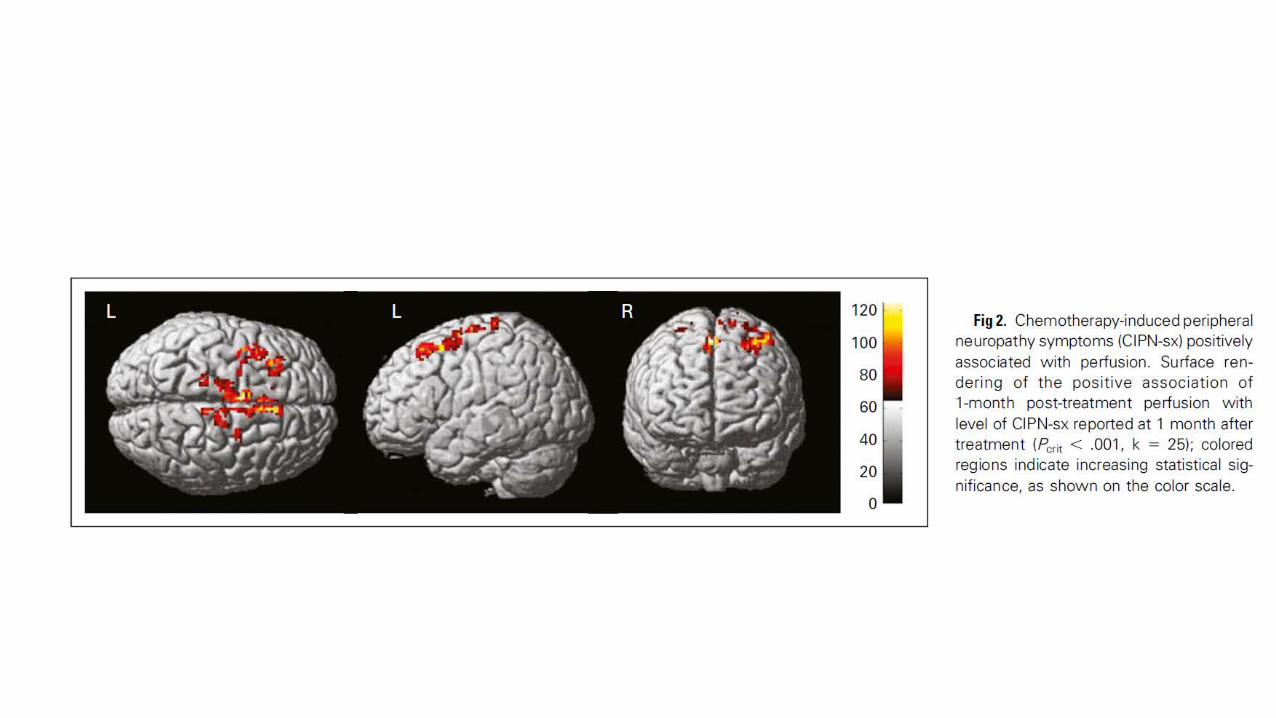
Peripheral neuropathy: what are the central effects Increasing evidence that effects are not all peripheral Peripheral neuropathy symptoms after systemic chemotherapy for
breast cancer are associated with changes in cerebral perfusion and gray matter Additional studies are needed for potential diagnostic and
therapeutic implications.
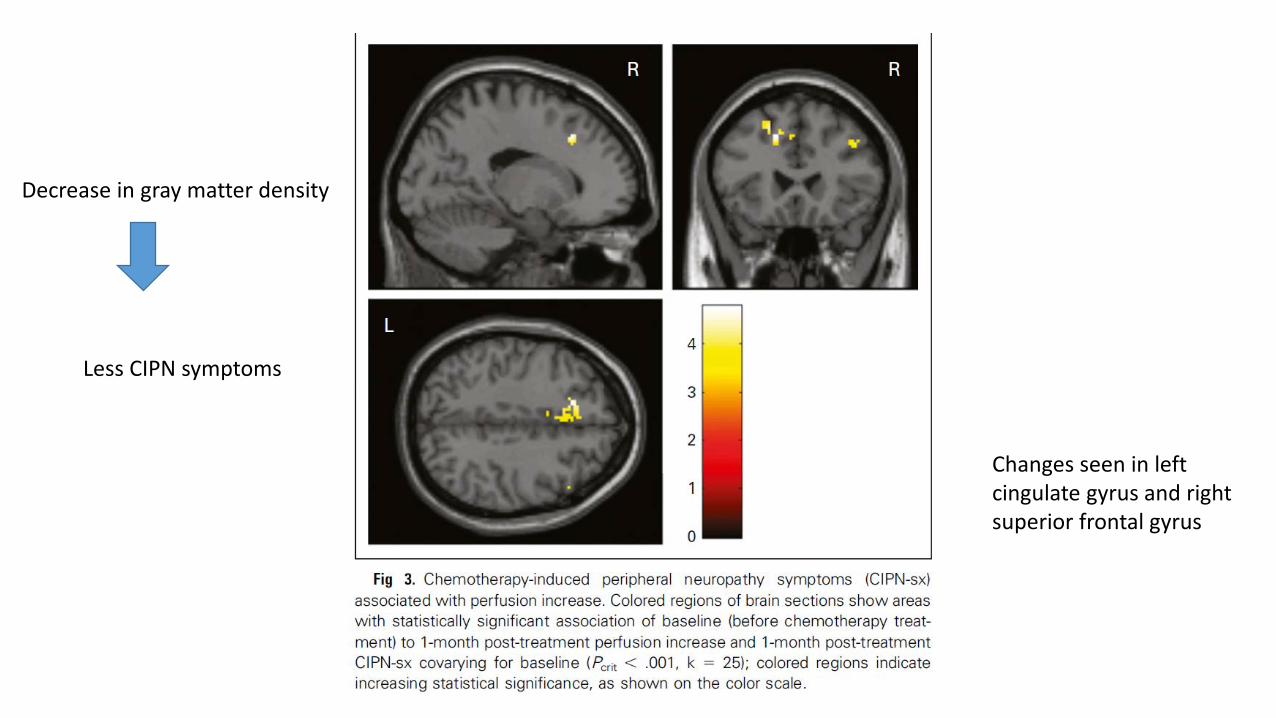
Decrease in gray matter density
Less CIPN symptoms
Changes seen in left cingulate gyrus and right superior frontal gyrus
Chemobrain
Chemotherapy and Cognitive Function
Anthracyclines: [Adriamycin (ADR), Doxorubicin (DOX)] frequently used treatment in breast cancer patients Impact greater than 30% of patients Symptoms last 12-24 months in most No effective preventative or treatment options
Cognitive impairement defined
Chemobrain is a common term used by cancer survivors to describe thinking and memory problems that can occur after cancer treatment. Other terms included chemo fog, cognitive changes or cognitive
dysfunction.
Memory
Concentration (Processing time)
Language (Verbal Fluency
Neurocognitive Changes
What patients say about cognitive effects of chemotherapy: “I just don’t feel as sharp as I was before I started my treatment.” “I forget things more easily.” “I have to work really hard to remember what I did all day.”
What patients say….
I used to run on automatic, now I have to really think and process things before I do them. I find myself checking and re-checking before going through a stop
sign.” “It’s a very shaky feeling that makes me unsure of myself.”
Factors Affecting Cognitive Functioning
Age and menopausal status Fatigue Depression, anxiety, stress Pain and pain medications Other physical illnesses No baseline assessment prechemo Above complicates the studies plus biologic mechanism not well-
understood
Proposed Mechanisms
Inflammation Oxidative stress
Neuronal damage
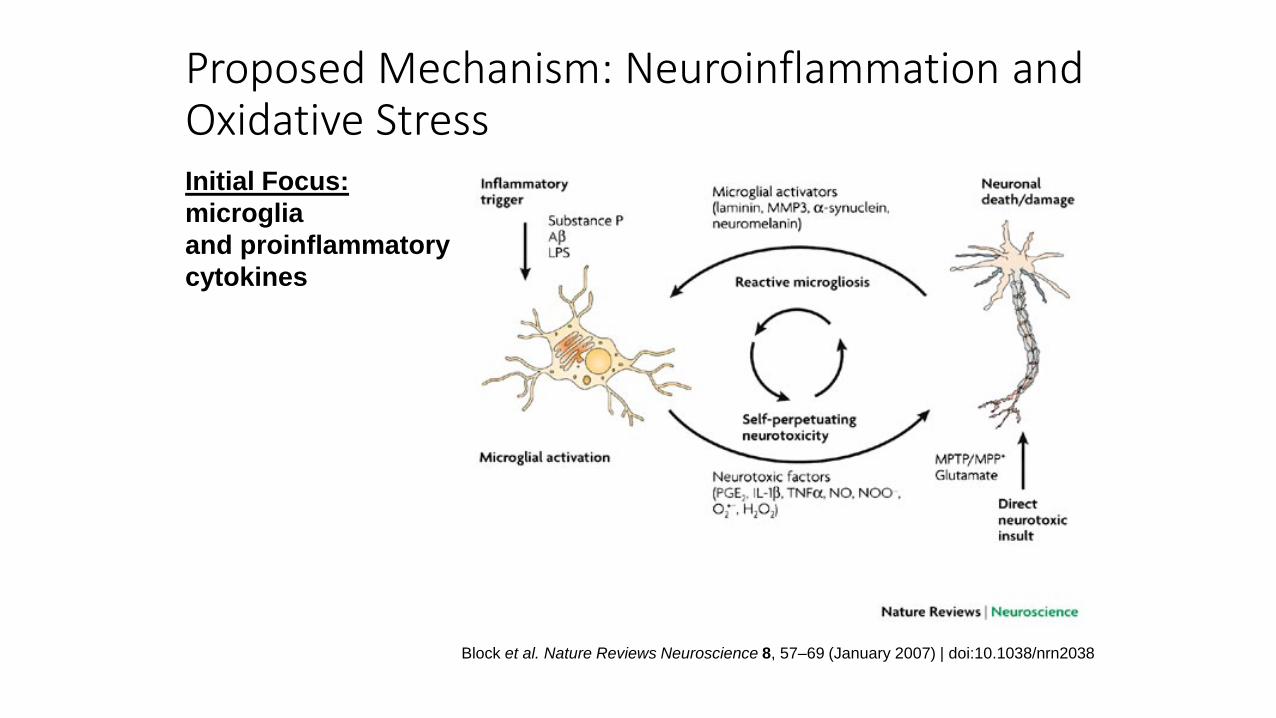
Proposed Mechanism: Neuroinflammation and Oxidative Stress
Block et al. Nature Reviews Neuroscience 8, 57–69 (January 2007) | doi:10.1038/nrn2038
Initial Focus: microglia and proinflammatory cytokines
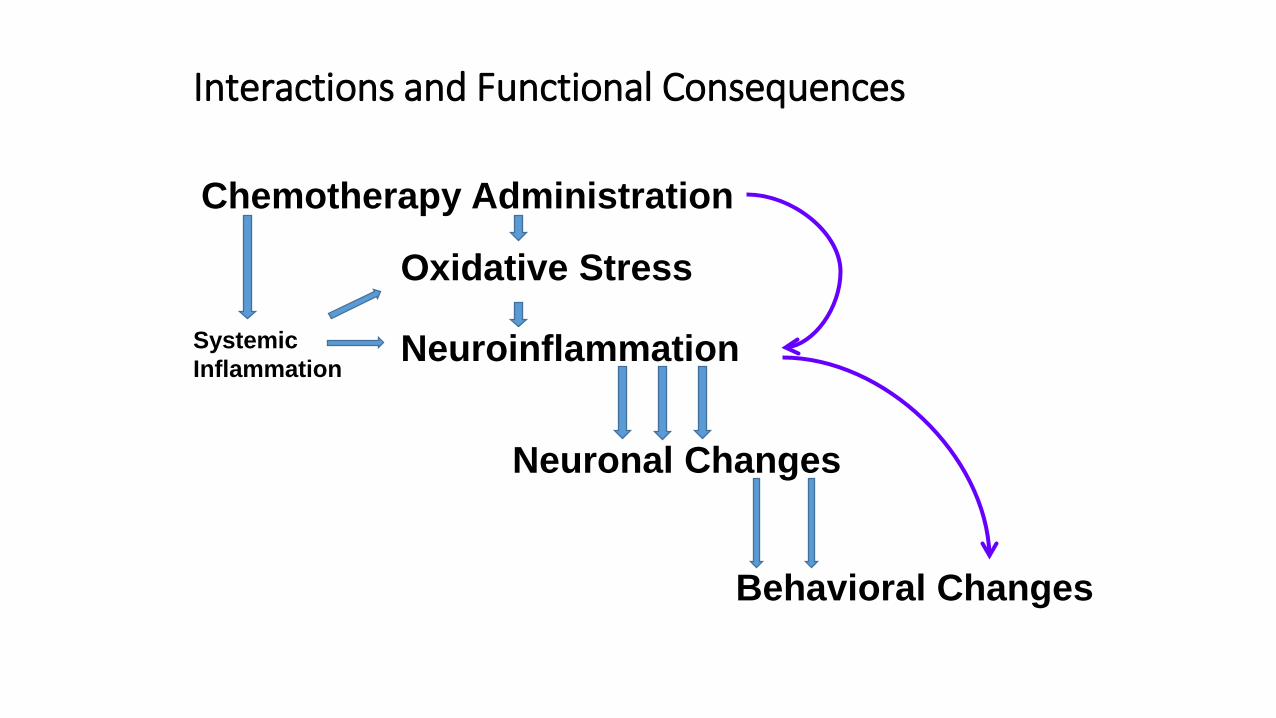
Interactions and Functional Consequences
Chemotherapy Administration
Neuroinflammation
Neuronal Changes
Behavioral Changes
Systemic Inflammation
Oxidative Stress
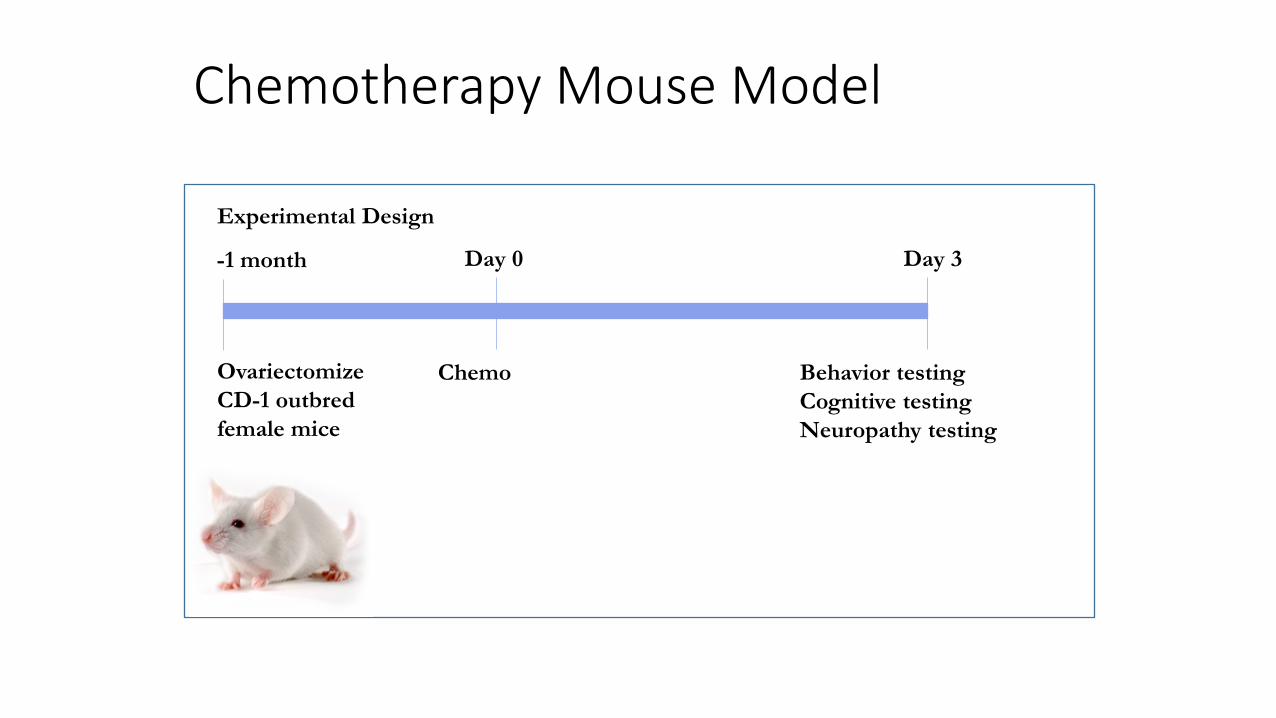
Chemotherapy Mouse Model
Experimental Design
-1 month
Ovariectomize CD-1 outbred female mice
Day 0
Chemo
Day 3
Behavior testing Cognitive testing Neuropathy testing
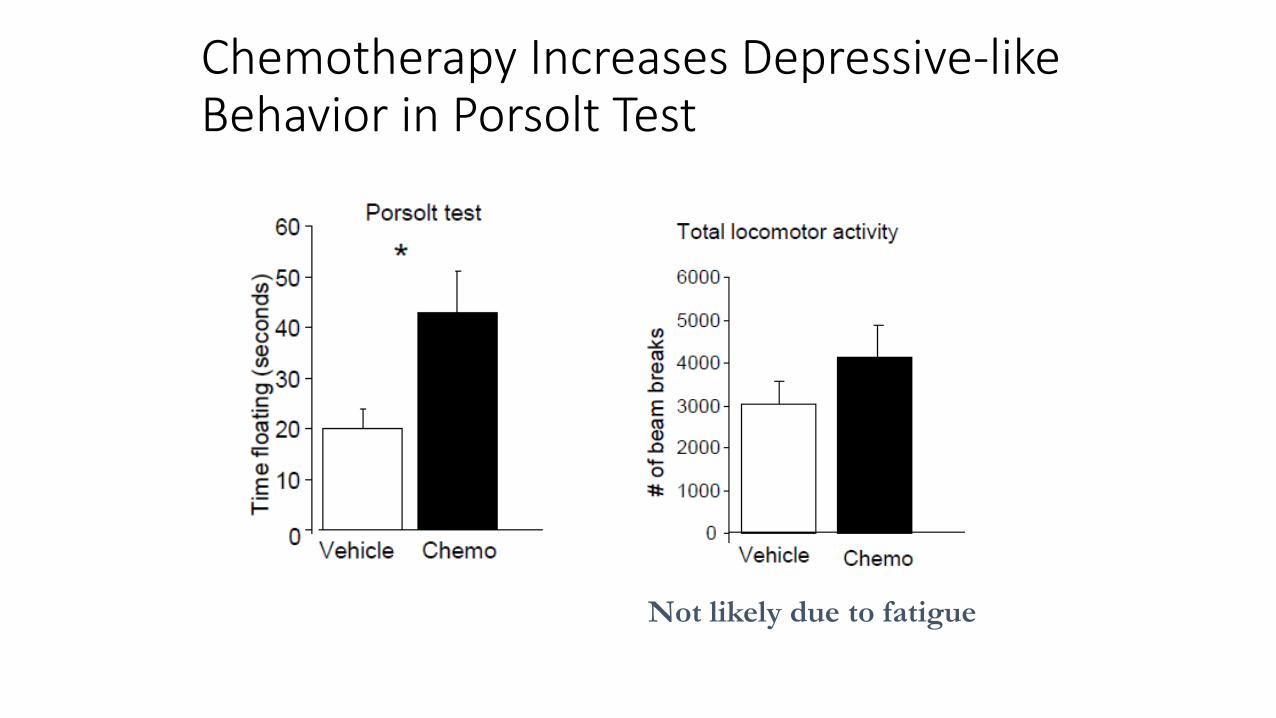
Chemotherapy Increases Depressive-like Behavior in Porsolt Test
Not likely due to fatigue
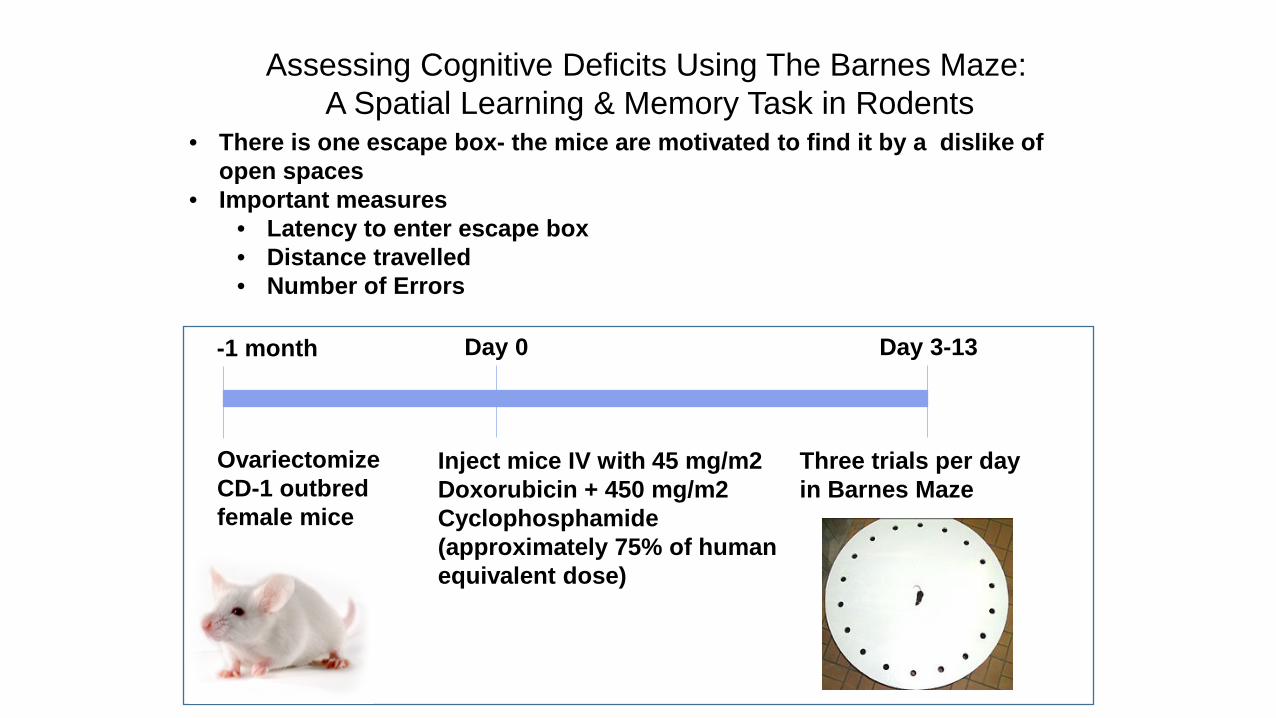
Assessing Cognitive Deficits Using The Barnes Maze: A Spatial Learning & Memory Task in Rodents
• There is one escape box- the mice are motivated to find it by a dislike of open spaces
• Important measures • Latency to enter escape box • Distance travelled • Number of Errors
Increased latency and errors are associated with a cognitive deficit.
-1 month
Ovariectomize CD-1 outbred female mice
Day 0
Inject mice IV with 45 mg/m2 Doxorubicin + 450 mg/m2 Cyclophosphamide (approximately 75% of human equivalent dose)
Day 3-13
Three trials per day in Barnes Maze
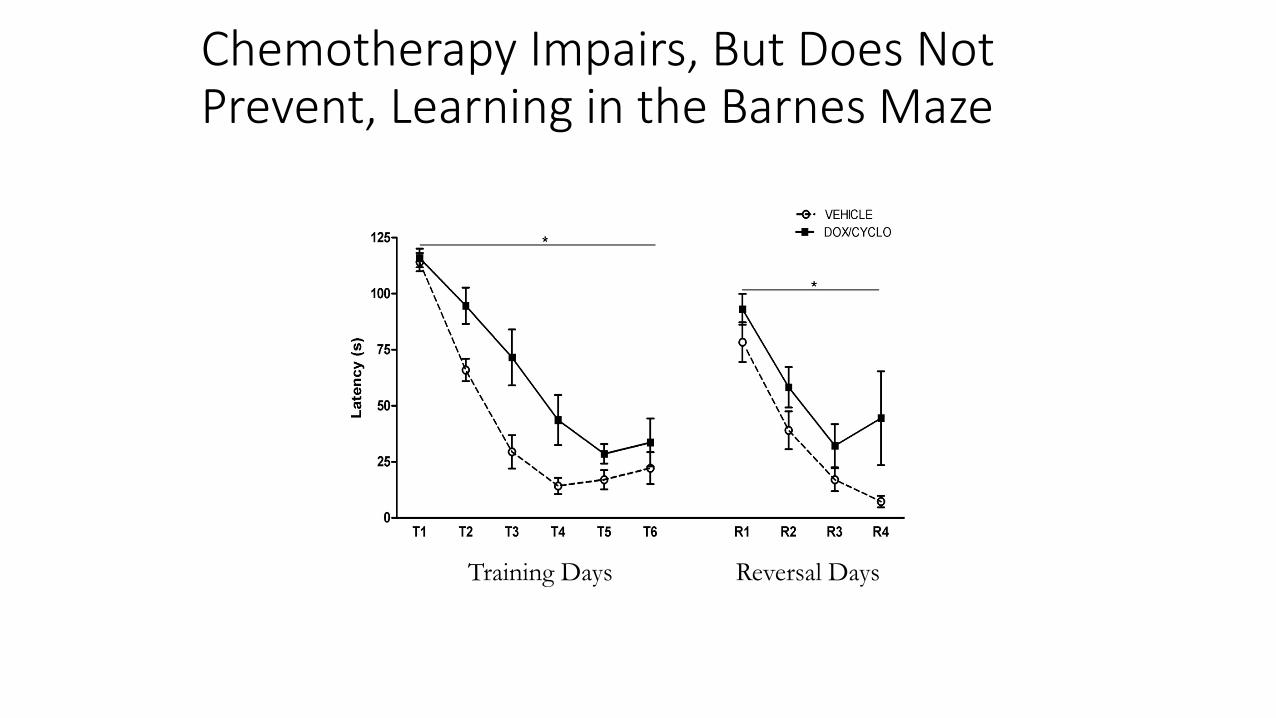
Chemotherapy Impairs, But Does Not Prevent, Learning in the Barnes Maze
* *
Training Days Reversal Days
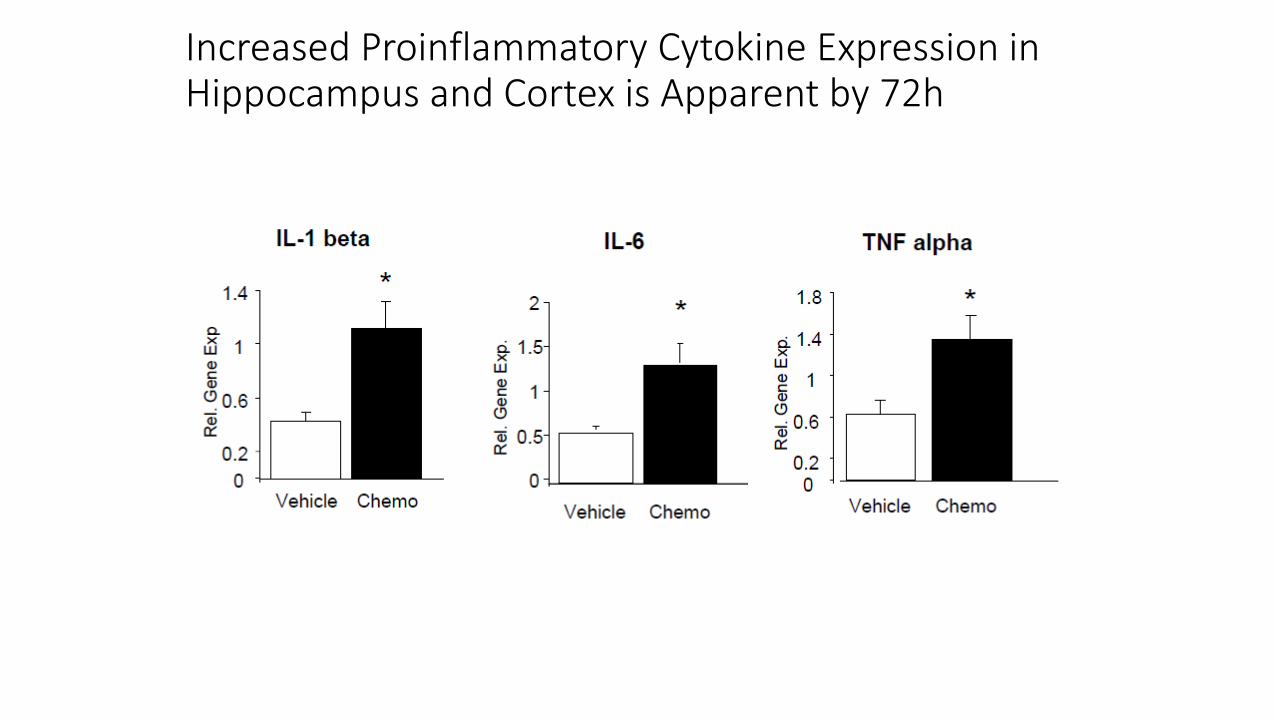
Increased Proinflammatory Cytokine Expression in Hippocampus and Cortex is Apparent by 72h
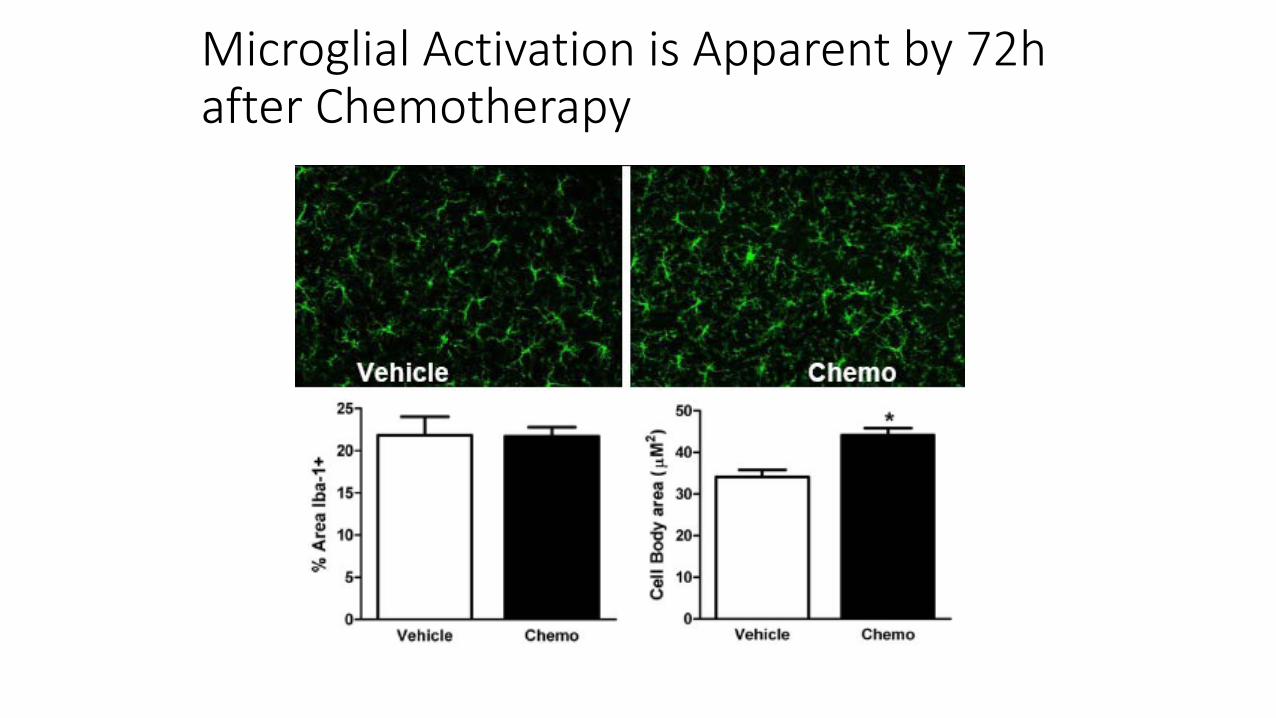
Microglial Activation is Apparent by 72h after Chemotherapy
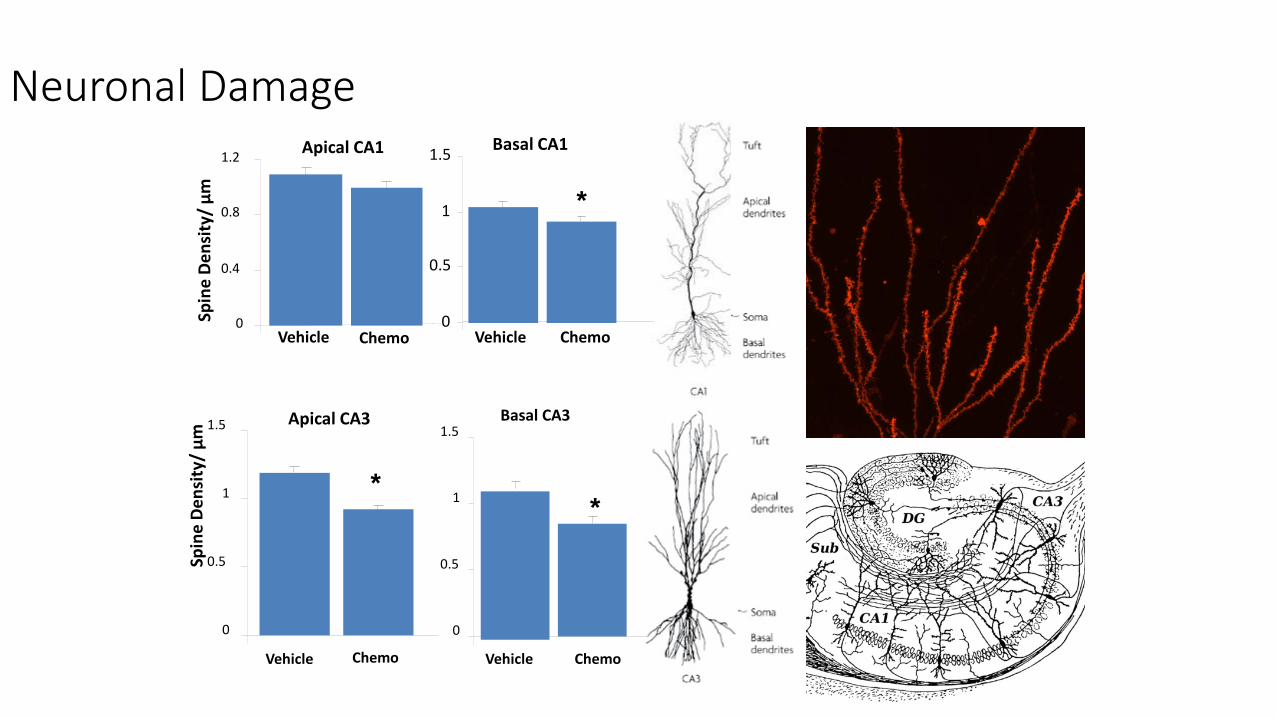
Neuronal Damage Basal CA1
0
0.5
1
1.5
Vehicle Chemo
Spin
e D
ensi
ty/
µm
*
*
Apical CA3
0
0.5
1
1.5
Vehicle Chemo
Spin
e De
nsity
/ µm
Apical CA1
0
0.4
0.8
1.2
Chemo Vehicle
Basal CA3
0
0.5
1
1.5
*
Vehicle Chemo
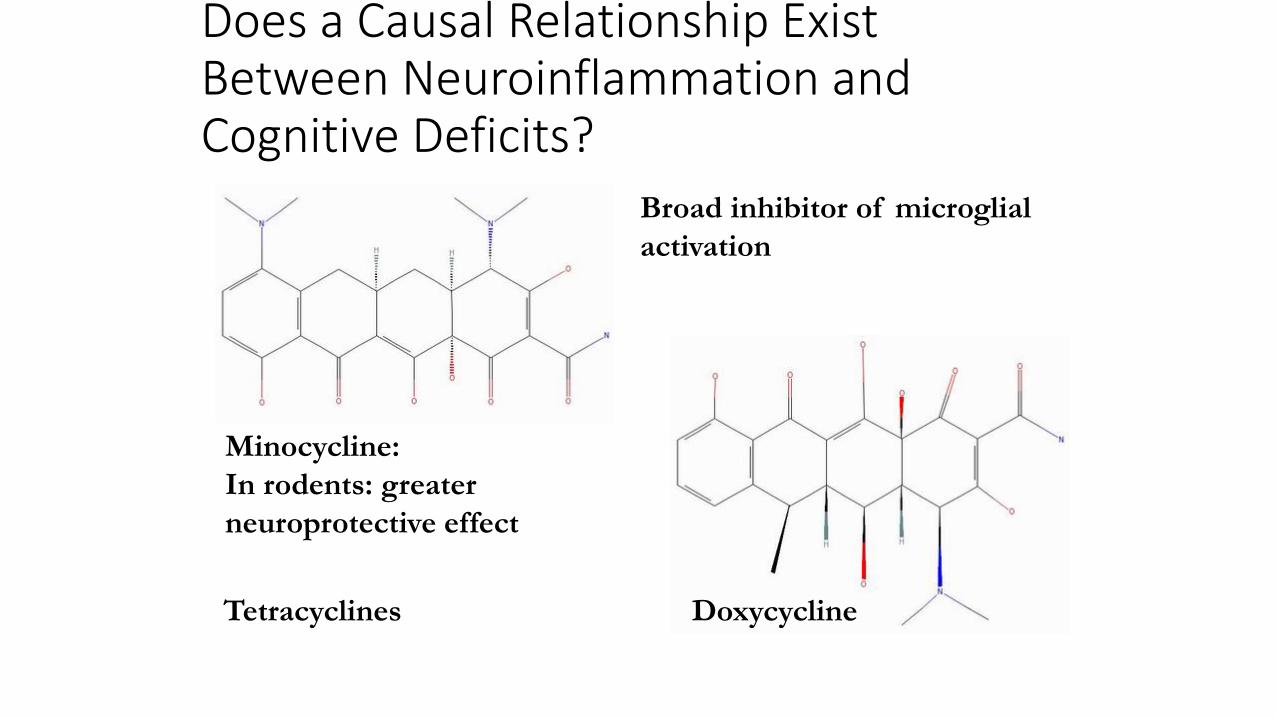
Does a Causal Relationship Exist Between Neuroinflammation and Cognitive Deficits?
Minocycline: In rodents: greater neuroprotective effect
Doxycycline Tetracyclines
Broad inhibitor of microglial activation
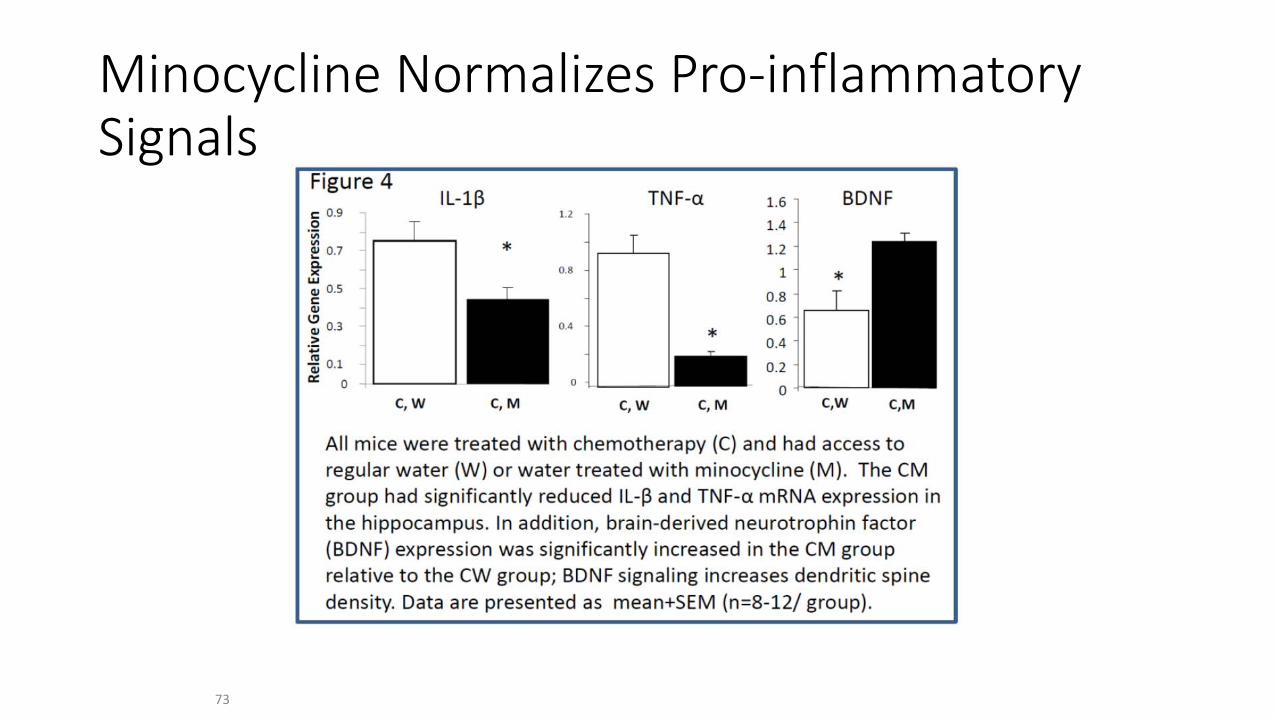
Minocycline Normalizes Pro-inflammatory Signals
73
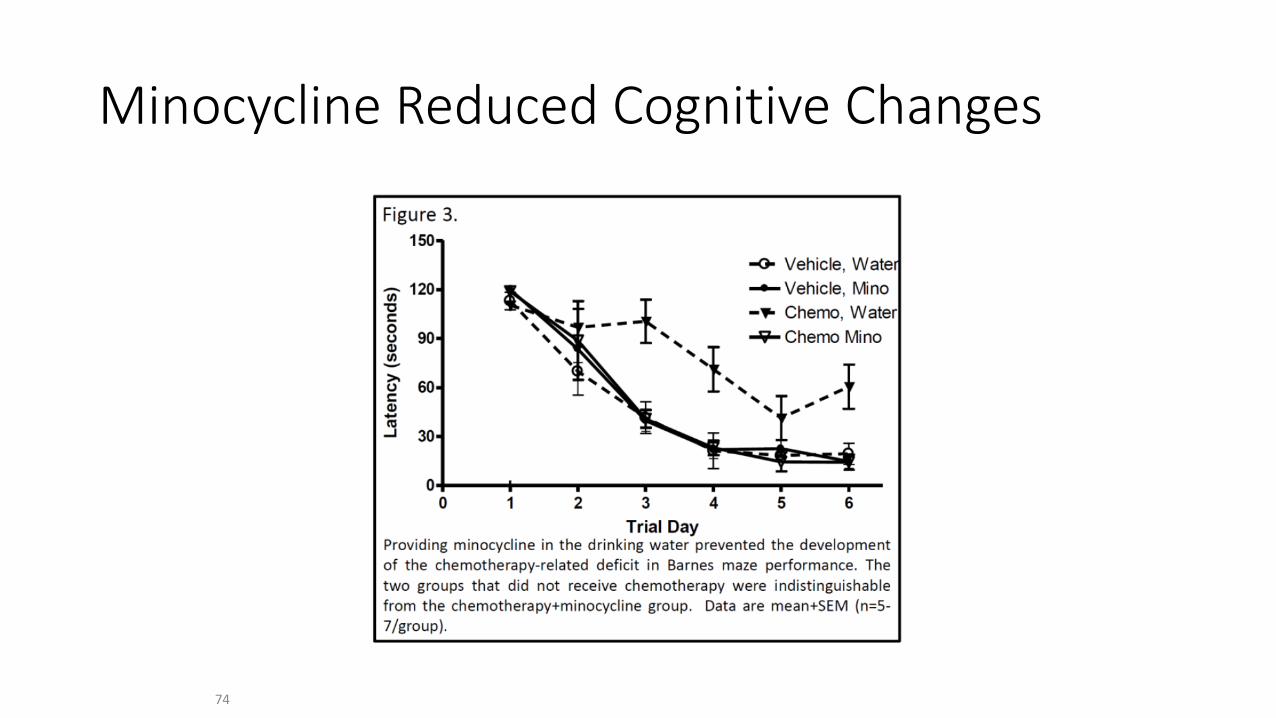
Minocycline Reduced Cognitive Changes
74
Lots to Do….. Other agents like Omega 3 supplements– Recent R01
funding to conduct these experiments in mice Additional studies investigating CIPN and microglia
peripherally and centrally and whether these are mitigated by different interventions such as exercise, minocycline, Omega 3 supplementation Additive effects of tumor and chemotherapy on
inflammation Social and stress influences on chemo-induced
neuroinflammation and behavioral consequences
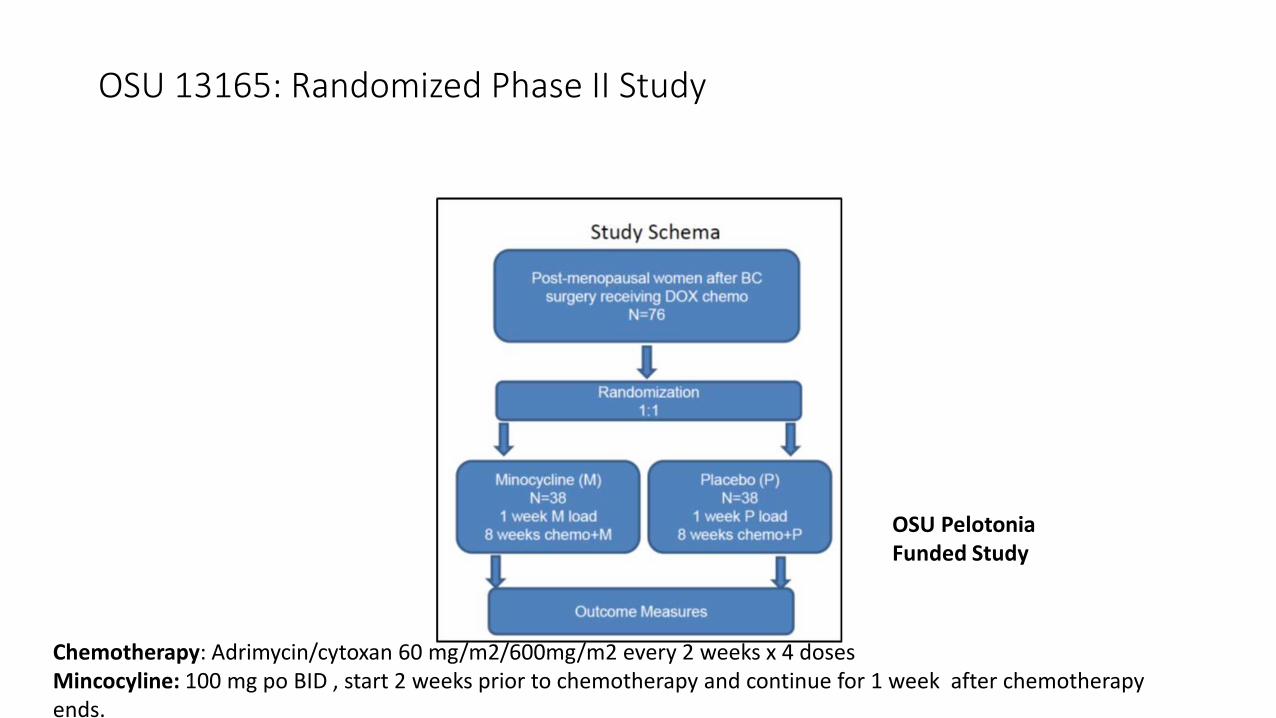
OSU 13165: Randomized Phase II Study
Chemotherapy: Adrimycin/cytoxan 60 mg/m2/600mg/m2 every 2 weeks x 4 doses Mincocyline: 100 mg po BID , start 2 weeks prior to chemotherapy and continue for 1 week after chemotherapy ends.
OSU Pelotonia Funded Study
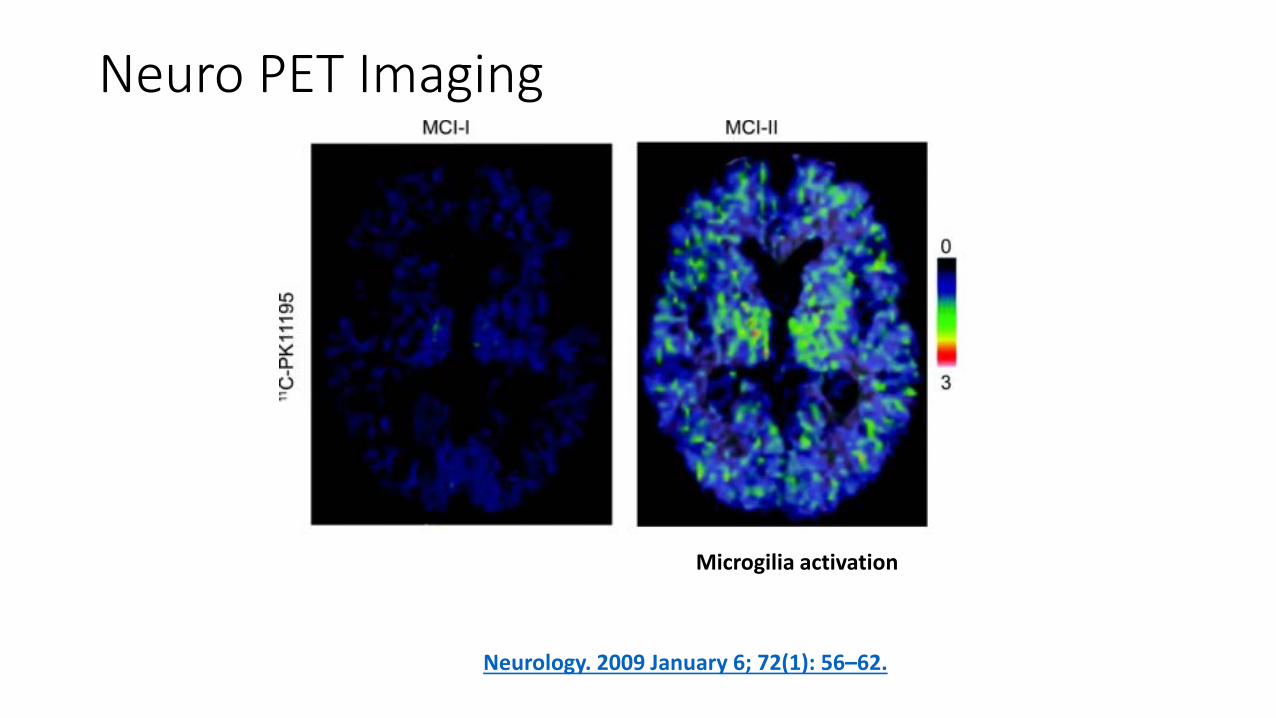
Neurology. 2009 January 6; 72(1): 56–62.
Microgilia activation
Neuro PET Imaging
n-3 PUFA and neuroinflammation
Reduce markers of oxidative stress 4- hydroxynonenal (4-HNE), malondialdehyde (MDA) Produced when free radicals react with double bonds of
phospholipids -> mitochondrial damage
Decrease inflammatory cytokines TNFα, IL-1β, IL-6
Decrease post-ischemic/traumatic neuronal damage
Prevents microglial activation
Eicosapentaenoic acid (EPA); Docosahexaenoic acid (DHA) DHA is most abundant n-3 PUFA in brain tissue
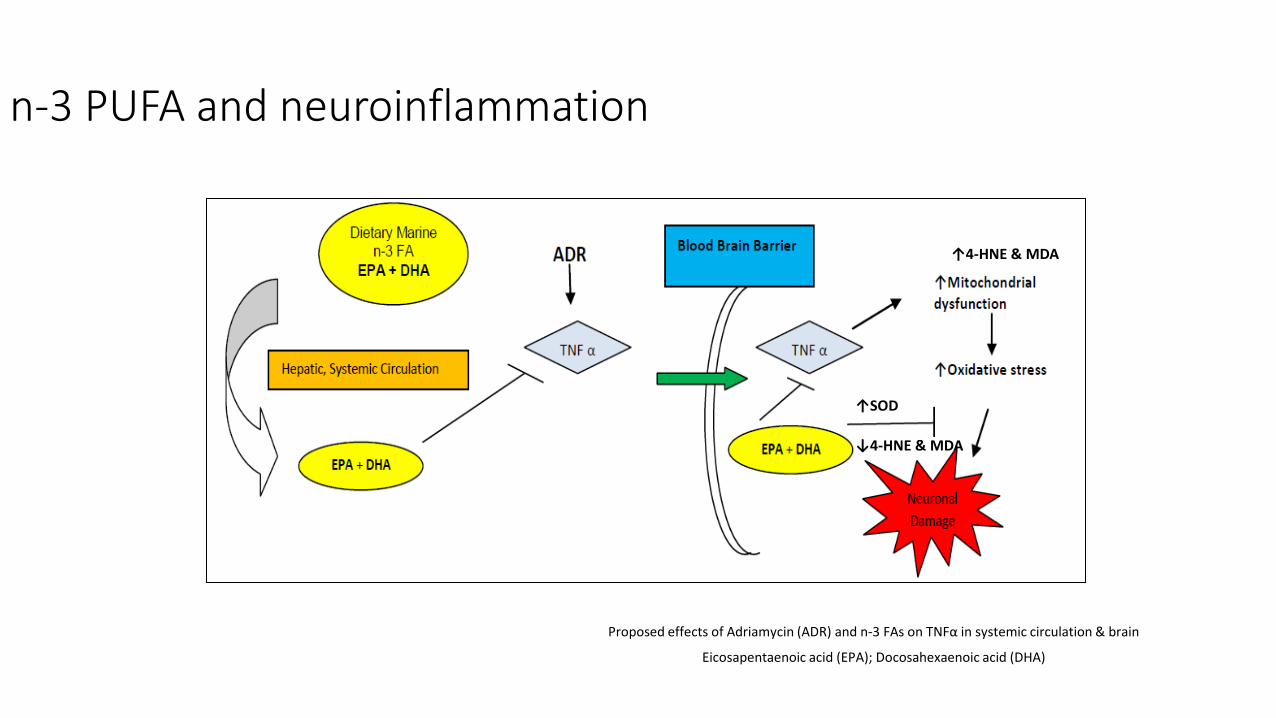
n-3 PUFA and neuroinflammation
Proposed effects of Adriamycin (ADR) and n-3 FAs on TNFα in systemic circulation & brain
Eicosapentaenoic acid (EPA); Docosahexaenoic acid (DHA)
↑4-HNE & MDA
↑SOD
↓4-HNE & MDA
n-3 PUFA may preserve cognitive function
EPA+DHA supplementation/enrichment increases brain tissue EPA+DHA, decreases n-6:n-
3 ratio in rodents
Short-term feeding of DHA (pre or post injury) enhances cognitive function in rodent models of traumatic brain injury
Long-term feeding of EPA+DHA decreases neuronal damage post-ischemic injury in rodents
DHA alone or in combination with EPA improves cognitive function (verbal fluency, recognition and memory) and reduces depression in healthy or mildly cognitively impaired adults
Hypothesis
A DHA enriched diet will decrease chemotherapy-induced proinflammatory cytokine expression and markers of oxidative stress in brain tissue, also decreasing microglial activation, which in turn will reduce the ADR associated cognitive decline.
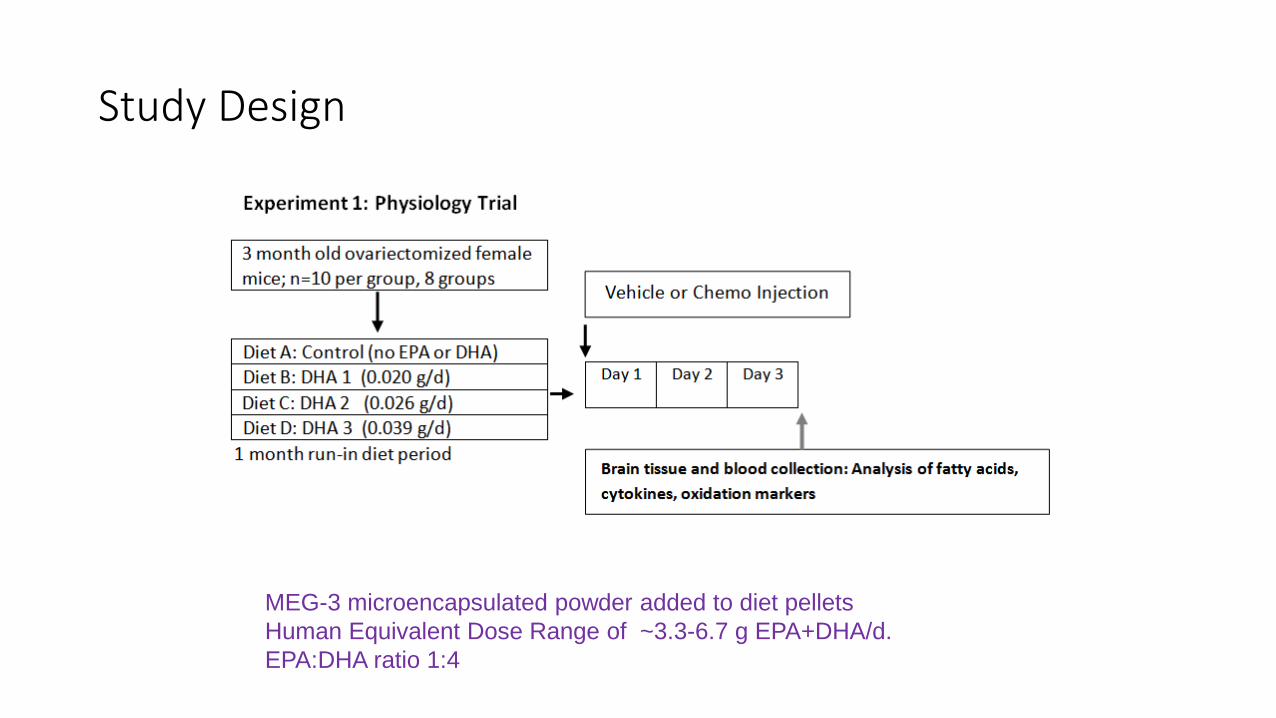
Study Design
MEG-3 microencapsulated powder added to diet pellets Human Equivalent Dose Range of ~3.3-6.7 g EPA+DHA/d. EPA:DHA ratio 1:4
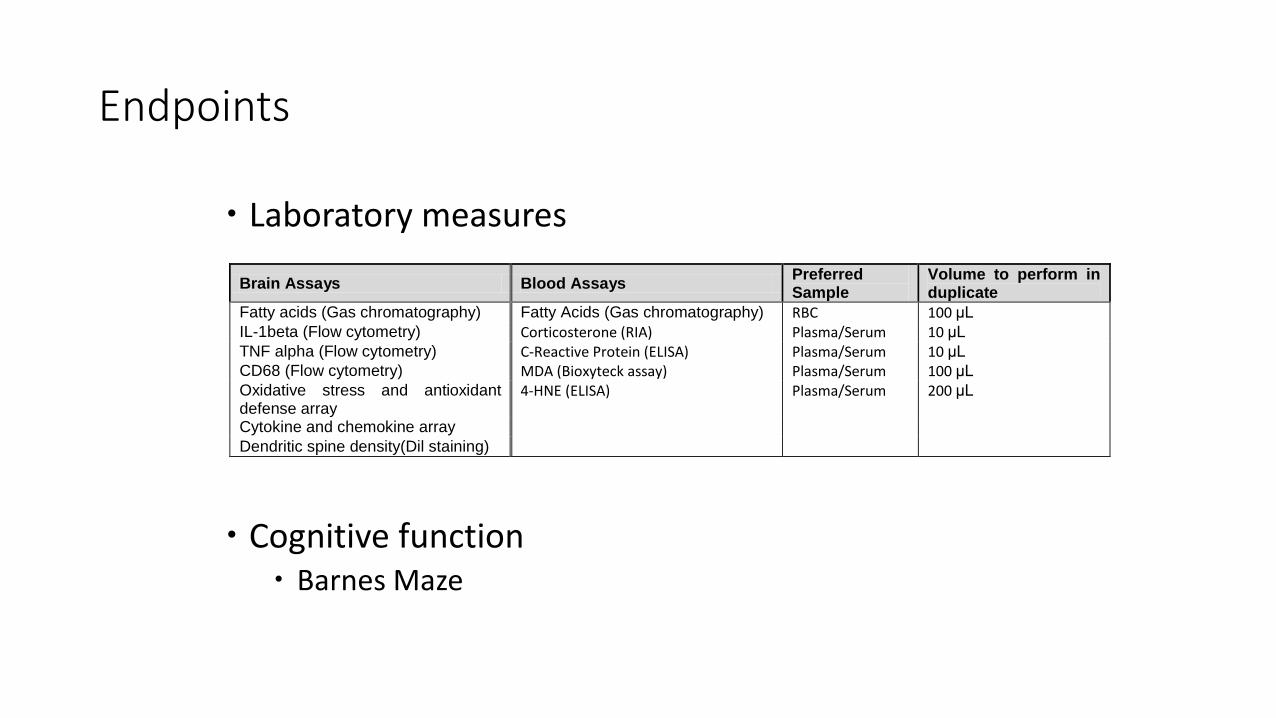
Endpoints
Laboratory measures Cognitive function
Barnes Maze
Brain Assays Blood Assays Preferred Sample
Volume to perform in duplicate
Fatty acids (Gas chromatography) Fatty Acids (Gas chromatography) RBC 100 μL IL-1beta (Flow cytometry) Corticosterone (RIA) Plasma/Serum 10 μL TNF alpha (Flow cytometry) C-Reactive Protein (ELISA) Plasma/Serum 10 μL CD68 (Flow cytometry) MDA (Bioxyteck assay) Plasma/Serum 100 μL Oxidative stress and antioxidant defense array
4-HNE (ELISA) Plasma/Serum 200 μL
Cytokine and chemokine array Dendritic spine density(Dil staining)
Significance
Understanding the mechanisms by which chemotherapy causes cognitive changes and intervening with DHA to potentially alleviate these deficits, could vastly improve the quality of life for breast cancer survivors. Additional studies with non pharmacologic interventions are needed
including exercise intervention studies
Arthralgias
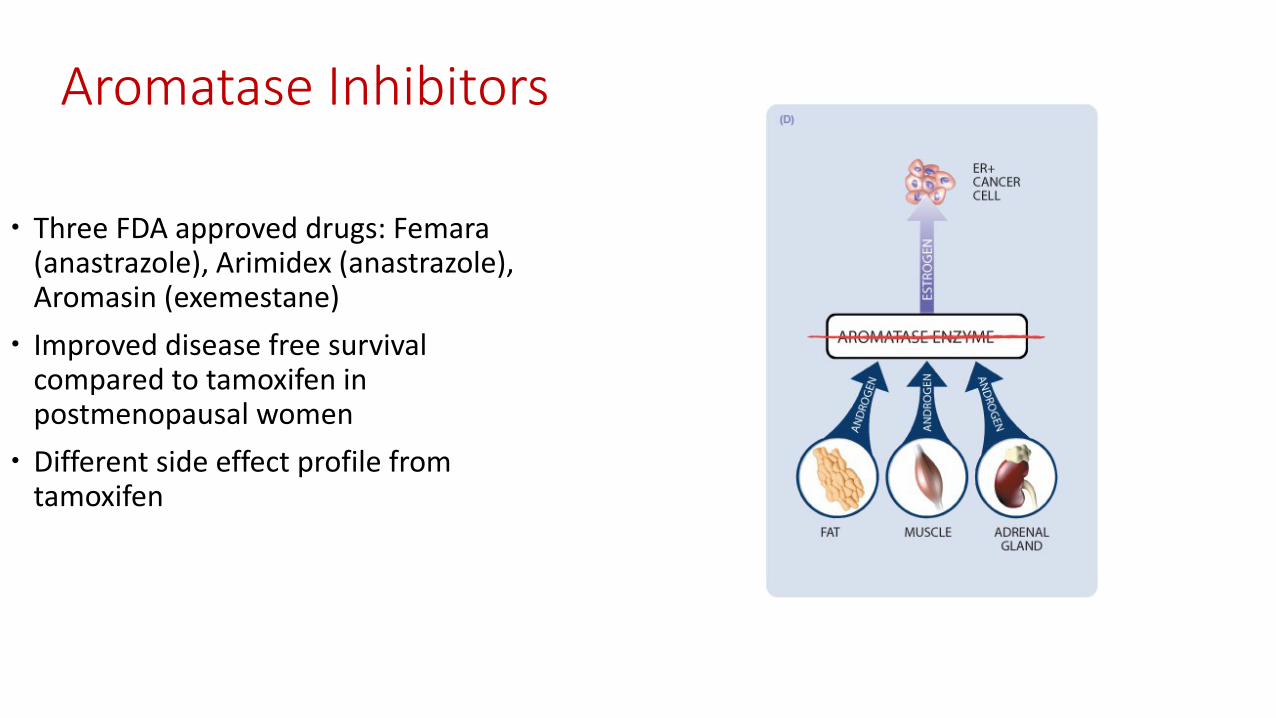
Aromatase Inhibitors
Three FDA approved drugs: Femara (anastrazole), Arimidex (anastrazole), Aromasin (exemestane)
Improved disease free survival compared to tamoxifen in postmenopausal women
Different side effect profile from tamoxifen
Side-effects of Aromatase Inhibitors
Hot flashes and other low estrogen symptoms Bone loss: recommend regular bone density monitoring
every 2 years while on therapy Joint pain -20-47% of women develop joint symptoms -Limited treatment options: interruptions in
therapy and nonsteroidal anti-inflammatory drugs (NSAIDs)
-Not effective in all patients: leads to alteration or termination of therapy in up to 20% of women.
Background: Why? Why do arthralgias occur? ? Estrogen deprivation directly mediated by AIs is implicated
Pro-inflammatory cytokines may also be regulated by estrogen
Background: Prevention Fish and fish oil supplement contain long chain n-3 polyunsaturated
fatty acids (n-3 PUFAs). A recent meta-analysis of randomized trials showed reduced joint pain
intensity, morning stiffness, and analgesic use in patients with rheumatoid arthritis supplemented with these n-3 PUFAs.
The efficacy of n-3 PUFAs in the prevention of AIIAs was reported as a
feasibility study by our group at the 2014 San Antonio Breast Cancer symposium:
Although promising trends were demonstrated by this
investigation, conclusive results were not seen.
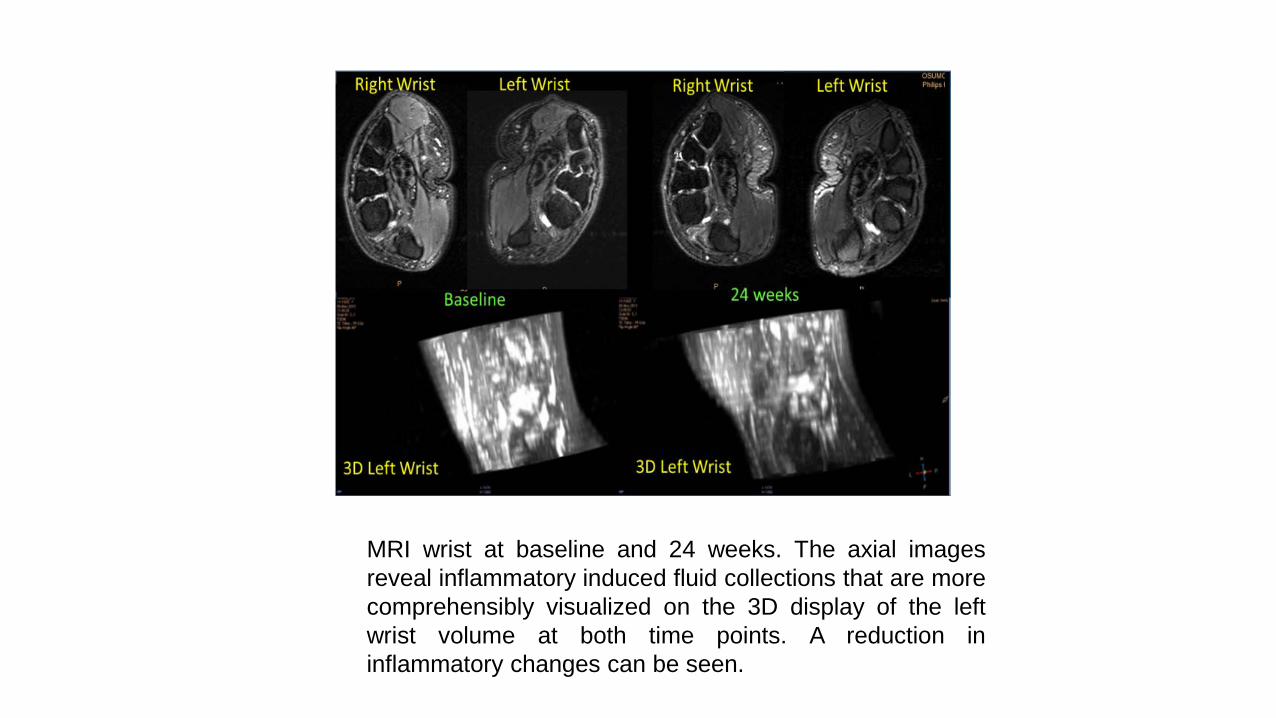
MRI wrist at baseline and 24 weeks. The axial images reveal inflammatory induced fluid collections that are more comprehensibly visualized on the 3D display of the left wrist volume at both time points. A reduction in inflammatory changes can be seen.
Hypothesis Based on observations that n-3 PUFAs have anti-inflammatory effects and
that the mechanism of AIIAs may be in part due to inflammation, we posit women taking n-3 PUFA supplements will be less likely to develop AIIAs compared to women on placebo.
We hypothesize that a woman’s risk for AIIAs and her response to n-3 PUFA supplementation can be predicted by multi-SNP analysis and modeling.
This is the first randomized study assessing the efficacy of preventing AIIAs with n-3 PUFA supplementation while validating genomic predictors of AI-induced toxicity and response to therapy.
Funded by Gateway Foundation
Objectives
Objective 1. To determine the efficacy of the complementary therapy n-3 PUFA supplementation in preventing AIIAs. Hypothesis. Women receiving n-3 PUFA supplementation will experience significantly less AIIAs compared to women receiving placebo.
Objectives
Objective 2. To prospectively define the population most at risk for developing AIIAs by the identification and validation of genetic risk predictors and to develop an SNP/gene profile predictive of treatment intervention response. Hypothesis. In the control group, expanded genomic analysis of germ line DNA will differentiate patients who develop significant AIIAs from those patients without symptoms. Among women receiving n-3 PUFA supplementation, treatment response will be predicted by the identification of an SNP-based Bayesian network from peripheral blood-sourced DNA. We further hypothesize that the genes associated with the SNPs defined in our predictive network will be associated with inflammatory pathways.
Eligibility Criteria Inclusion criteria Women diagnosed with breast cancer stages I-III initiating first line adjuvant AI
therapy with any of the FDA-approved AIs (anastrazole, exemestane, letrozole)
Concurrent GnRH agonist therapy is allowed. Concurrent breast related radiation therapy is allowed.
Prior tamoxifen use is allowed.
Prior chemotherapy is allowed.
Age >18 years.
Ability to understand and the willingness to sign a written informed consent document.
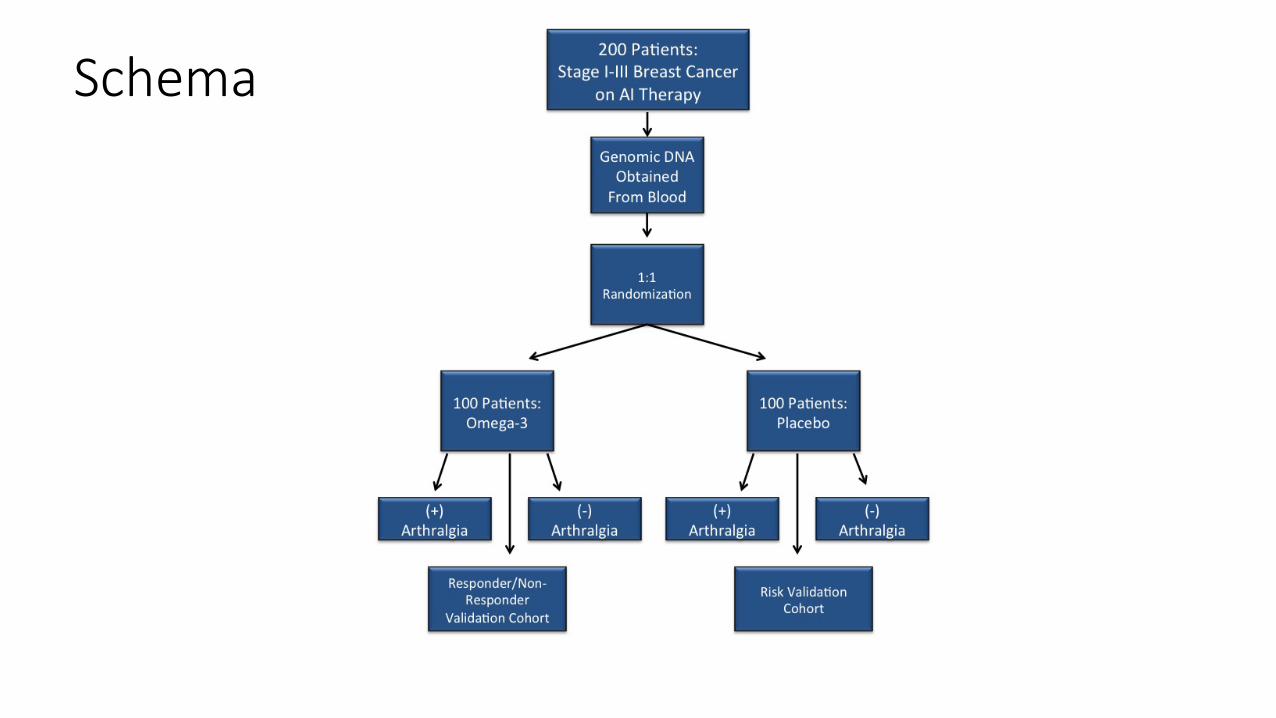
Schema
Design This is a double-blinded, randomized study of postmenopausal women
with breast cancer stages I-III who are initiating adjuvant endocrine therapy with FDA approved third generation AIs (letrozole, anastrozole, or exemestane)
Enrollment goal: 200 patients with collaboration from The Cleveland Clinic
Upon study enrollment, peripheral blood samples will be collected from these patients in order to obtain genomic DNA.
Using a fixed-block 1:1 randomization, each subject will then be randomized to a 6-month treatment period with either oral administration of n-3 PUFA supplements or a placebo of a mixture of oils typical of the American diet (TAD) fatty acid ratio.
Evaluation RBC n-3 PUFAs levels: these are important for capturing long-term (~3
month) n-3 PUFAs intake Inflammatory markers: IL-1β, IL-6, IL-17, TNF-RI and TNF-RII Arthralgia Assessment: validated instruments that have been used to
evaluate joint symptoms, functional capacity, and quality of life in our target population.
Brief Pain Inventory (BPI) FACT-B and endocrine subscale (FACT-ES) Western Ontario and McMaster Universities Osteoarthritis Index
(WOMAC) Modified Score for the Assessment and Quantification of Chronic
Rheumatoid Affections of the Hands (M-SACRAH)
Trial to open Summer 2016
Funding: The Gateway For Cancer Research Collaboration with The Cleveland Clinic
The Exercise Prescription
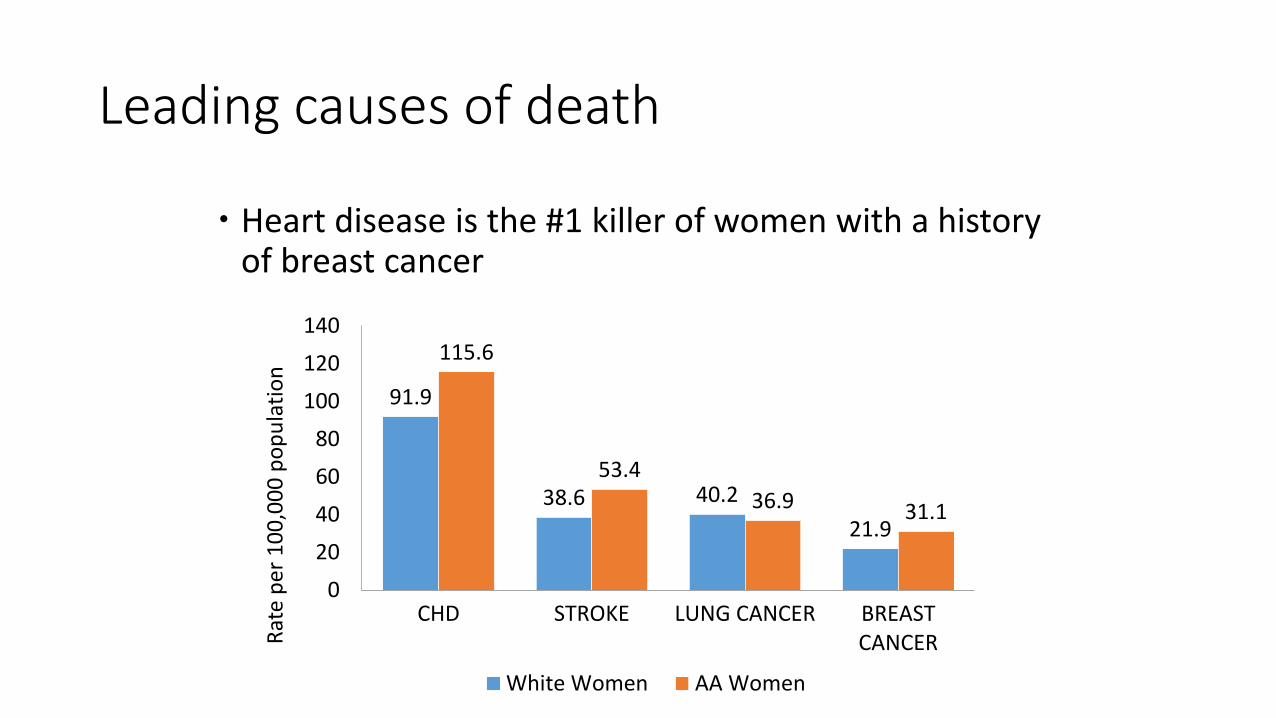
Leading causes of death
Heart disease is the #1 killer of women with a history of breast cancer
91.9
38.6 40.2 21.9
115.6
53.4 36.9 31.1
020406080
100120140
CHD STROKE LUNG CANCER BREASTCANCER
White Women AA Women
Rate
per
100
,000
pop
ulat
ion
Cancer treatments can increase the risk of CHD Radiation
Increases risk of coronary artery disease and myocardial infarction
Anthracyclines Increases risk of heart failure in the subsequent 10 years
Herceptin (Tratuzumab) Increases risk of hypertension or low-normal heart function
Combination therapy (anthracycline + herceptin) Increases risk of heart disease up to 7 times
Common risk factors
Smoking, unhealthy diet, physical inactivity
Breast Cancer
Cardiovascular Disease
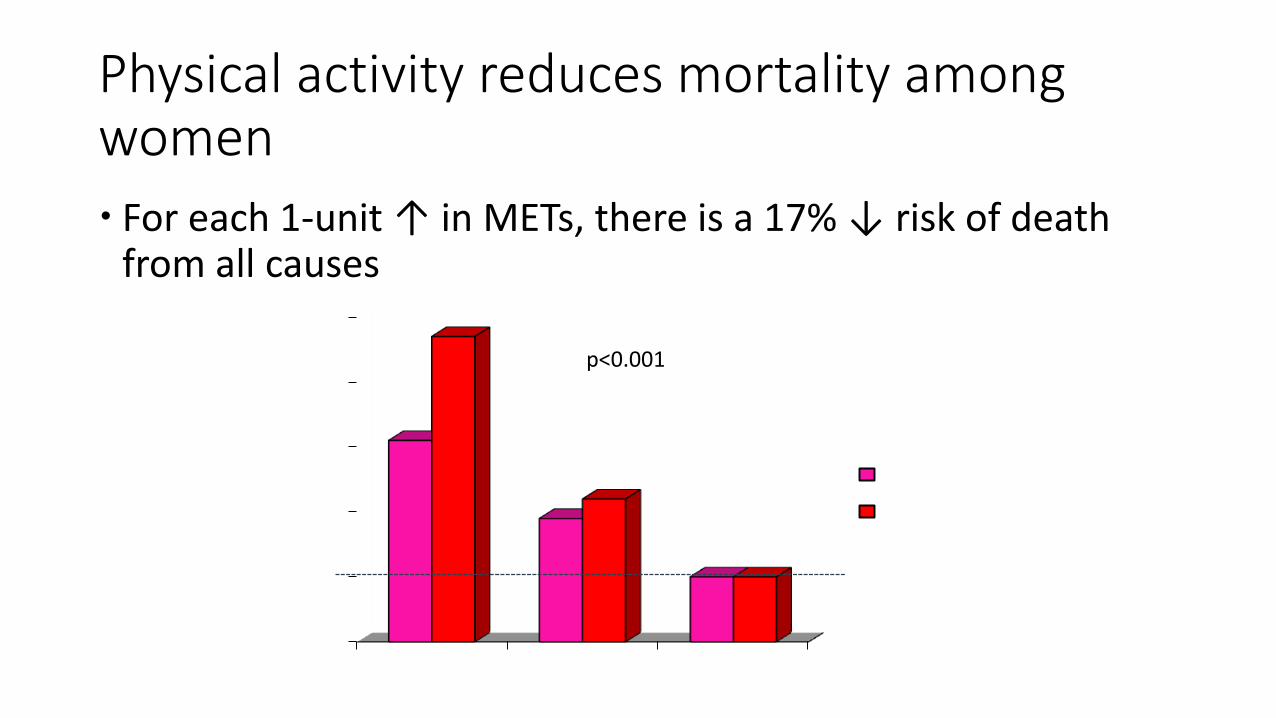
Physical activity reduces mortality among women For each 1-unit ↑ in METs, there is a 17% ↓ risk of death
from all causes
0
1
2
3
4
5
<5 MET 5-8 MET >8 MET
Haza
rds R
atio
of D
eath
All-CauseCardiac
p<0.001
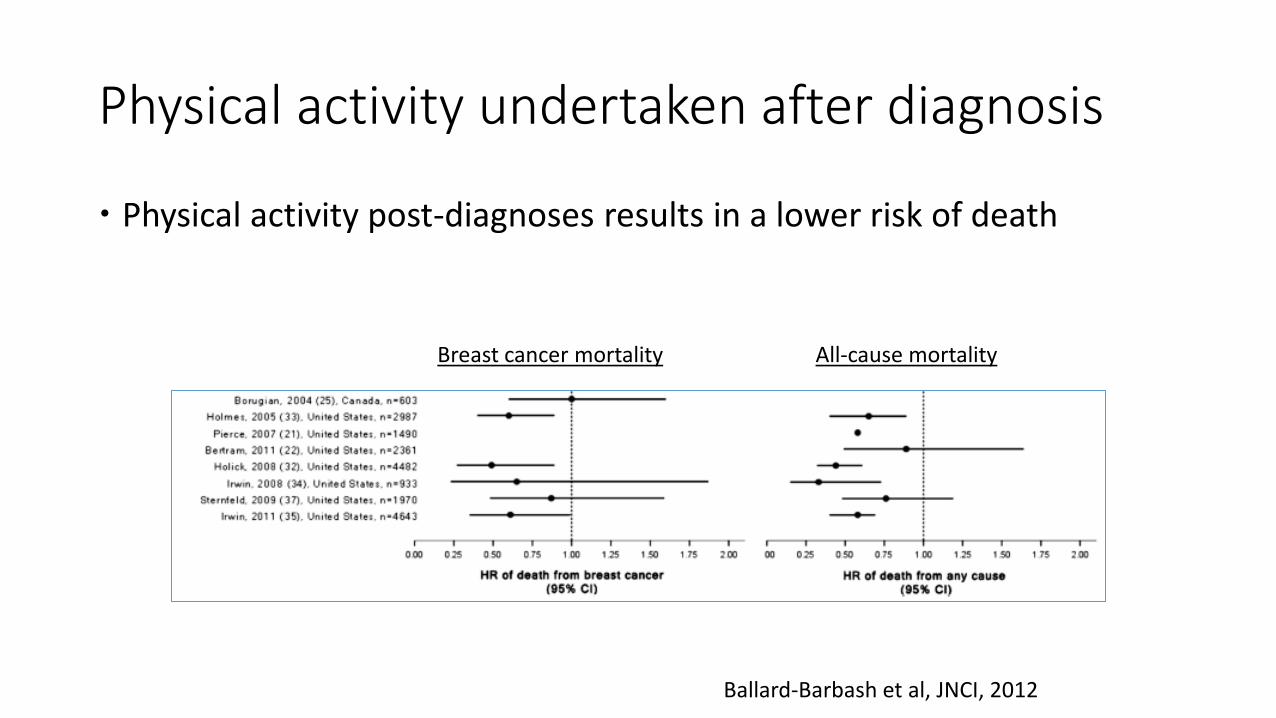
Physical activity undertaken after diagnosis
Physical activity post-diagnoses results in a lower risk of death
Ballard-Barbash et al, JNCI, 2012
Breast cancer mortality All-cause mortality
Few women meet physical activity guidelines
Only 16% of women met physical activity guidelines in 2008 19% of white women 11% of black women
Up to 90% of breast cancer survivors post-treatment do not exercise regularly
Source: National Health Interview Survey, 2010
Existing research on exercise
Weaknesses of existing exercise studies include a lack of evidence-based protocol for exercise prescriptions and inconsistent adherence to the principles of exercise (frequency, intensity, and duration) CR is designed to induce changes in the cardiovascular risk profile of
participants Includes education on the topics of stress management, smoking cessation,
nutrition, and weight loss Exercise prescriptions can be modified for survivors with treatment side-
effects such as lymphedema
Cardiac rehabilitation (CR)
CR programs have substantial extant infrastructure and may improve morbidity and mortality from both cardiovascular disease and cancer among breast cancer patients post-treatment CR programs, comprising exercise and education, are efficacious in
improving cardiorespiratory fitness, reducing modifiable risk factors, and improving quality of life (QoL) among high-risk female cardiac patients It remains unknown if a CR program would be efficacious among
lower-risk breast cancer patients
Study aims
1. Assess the feasibility of conducting a 14-week CR program in women after completion of acute therapy for breast cancer
2. Preliminarily evaluate the efficacy of CR in improving cardiorespiratory fitness (peak oxygen uptake, VO2 max) at 14 weeks.
3. Explore changes in risk factors (blood pressure, cholesterol, fasting glucose, and body mass index) between baseline and 14-week follow-up.
4. Quantify the difference in QoL between baseline and 14 weeks, adjusting for baseline QoL values.
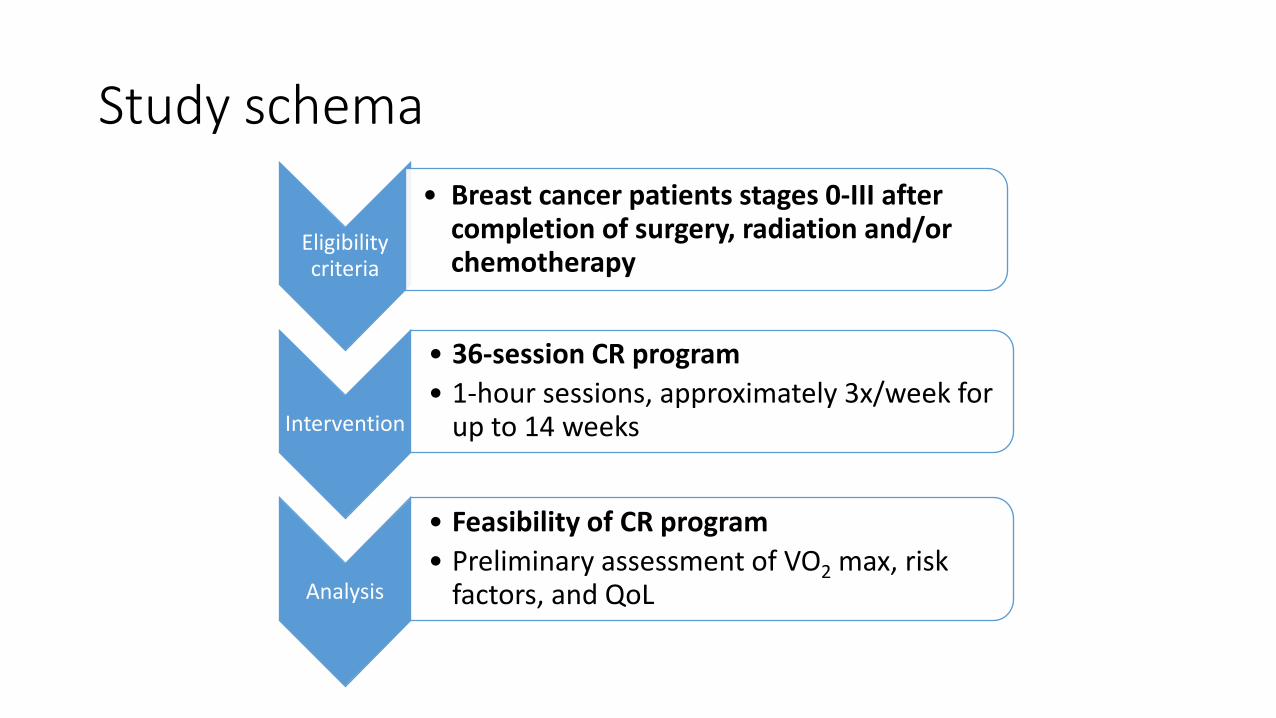
Study schema
Eligibility criteria
• Breast cancer patients stages 0-III after completion of surgery, radiation and/or chemotherapy
Intervention
• 36-session CR program • 1-hour sessions, approximately 3x/week for
up to 14 weeks
Analysis
• Feasibility of CR program • Preliminary assessment of VO2 max, risk
factors, and QoL
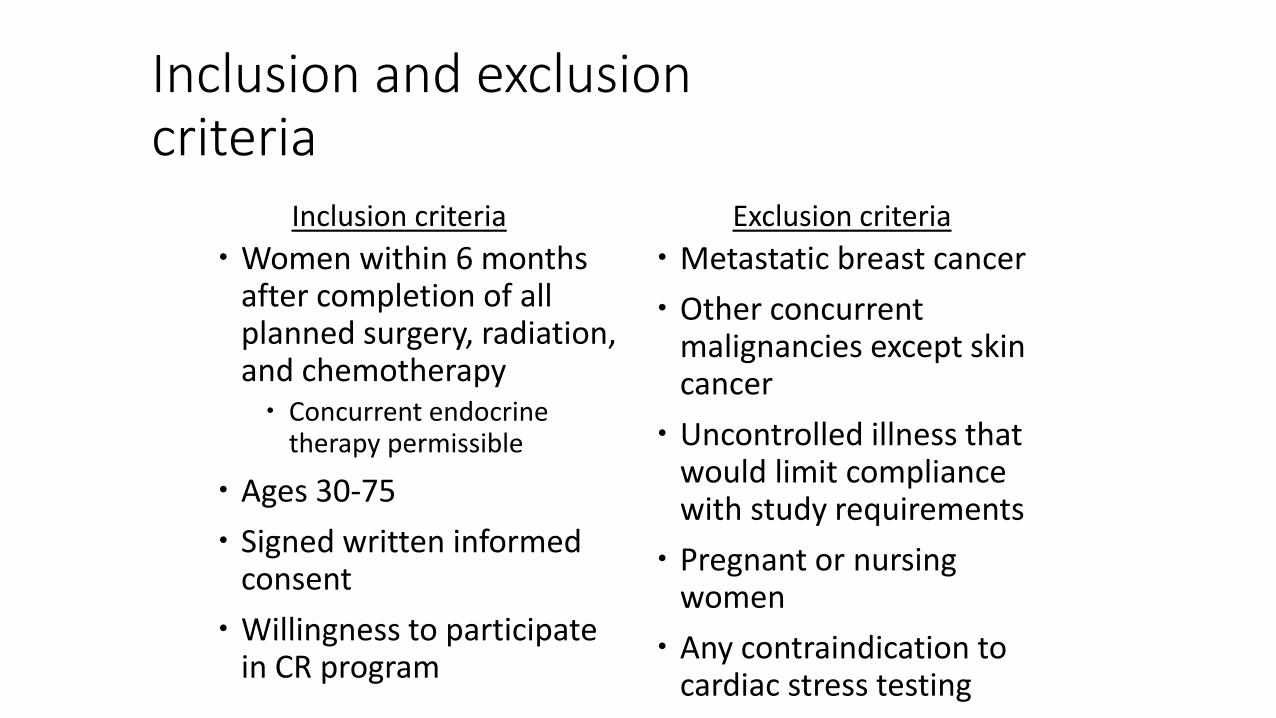
Inclusion and exclusion criteria
Women within 6 months after completion of all planned surgery, radiation, and chemotherapy Concurrent endocrine
therapy permissible
Ages 30-75 Signed written informed
consent Willingness to participate
in CR program
Metastatic breast cancer Other concurrent
malignancies except skin cancer
Uncontrolled illness that would limit compliance with study requirements
Pregnant or nursing women
Any contraindication to cardiac stress testing
Inclusion criteria Exclusion criteria
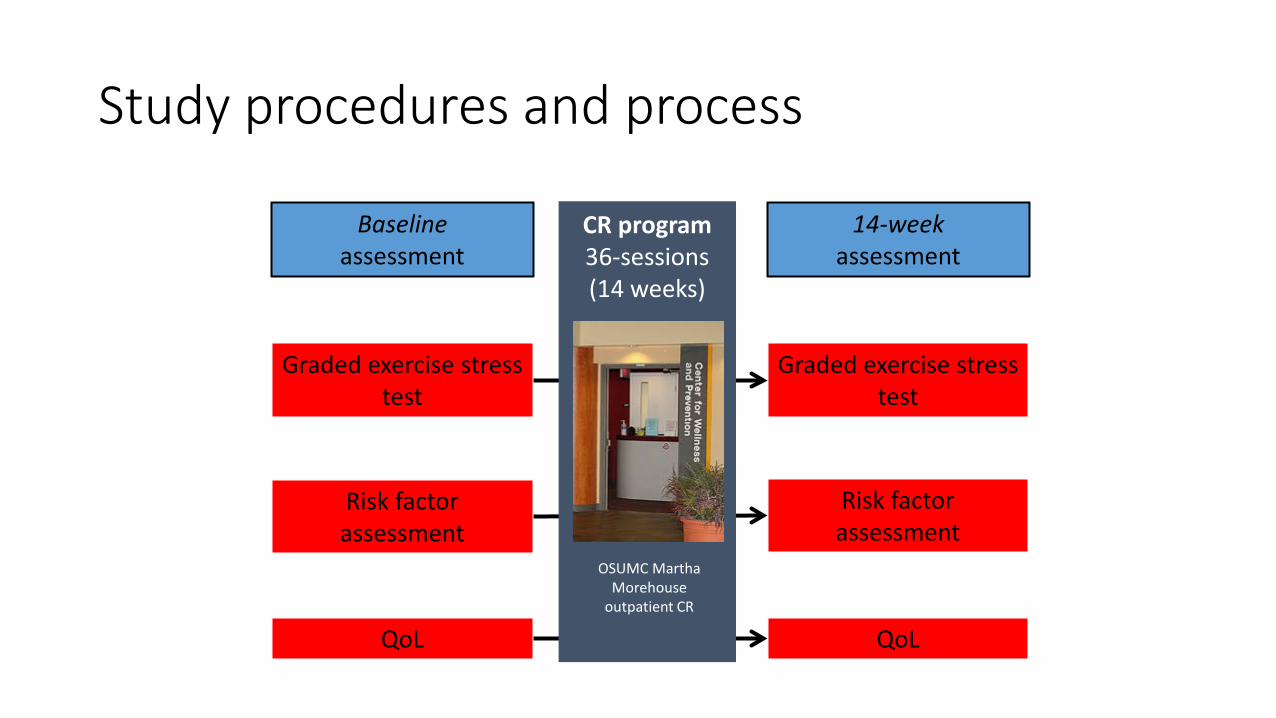
Study procedures and process
Graded exercise stress test
Graded exercise stress test
Risk factor assessment
Baseline assessment
14-week assessment
Risk factor assessment
QoL QoL
CR program 36-sessions (14 weeks)
OSUMC Martha Morehouse
outpatient CR
OSU 14060
10 out of 20 women currently enrolled General satisfaction with program is high Logistical issues/barriers to exercise remain for many women
Current challenges and future direction in Oncorehab and breast cancer survivorship
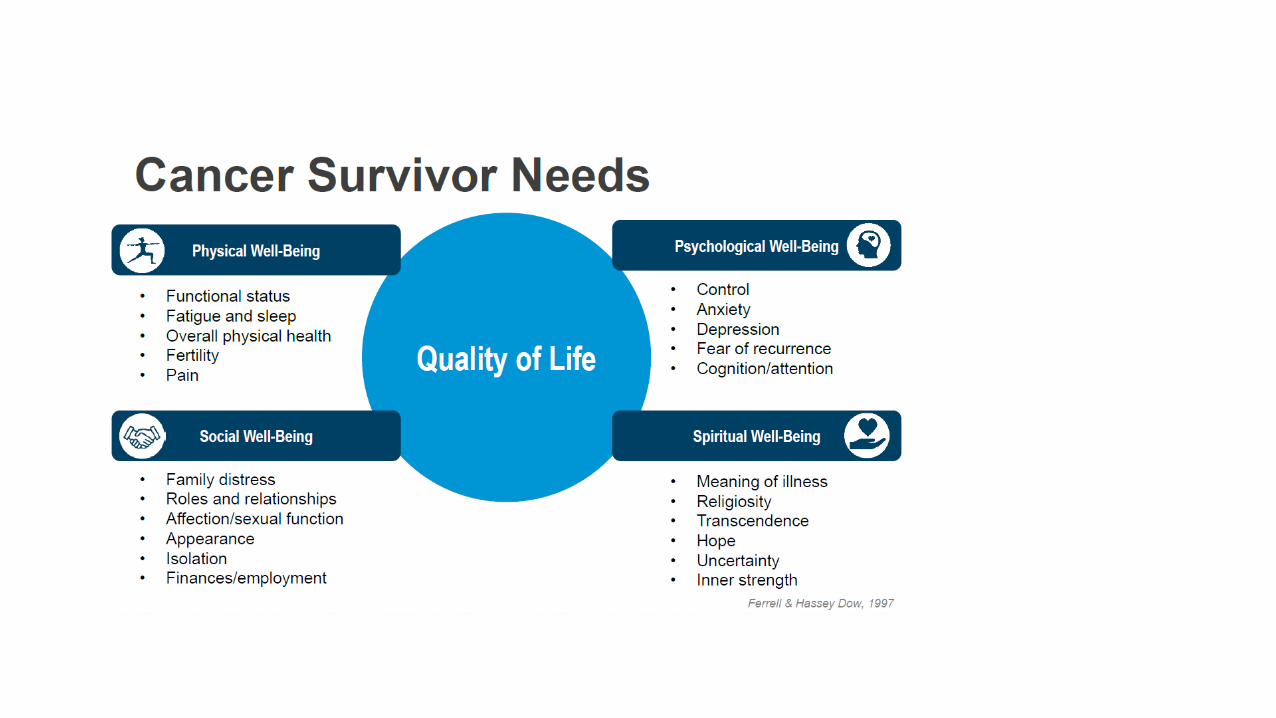
Survivorship Care: Why now?
• Rapidly growing population of survivors • Promote optimal health for survivors • Increasing expectations for a better quality of life • Greater emphasis on patient-centered issues
Definition of Cancer Survivor – Individuals living after (or with) cancer, their families as
well as their care givers, “From the day of diagnosis through the remainder of their lives”*
– Survivorship as a continuum, integrated into cancer care
*National Coalition for Cancer Survivorship (NCCS) NCI Office of Survivorship, Centers for Disease Control and Prevention and Lance Armstrong Foundation
Institute of Medicine (IOM) 2006: Lost in Translation
Prevention of recurrent and new cancer Management of late effects Assessment of medical and psychosocial late effects Interventions for consequences of cancer and treatment Coordination of care among providers
Hewitt M, et al. eds. From Cancer Patient to Cancer Survivor: Lost in Transition. Washington DC; The National Academies Press; 2005.
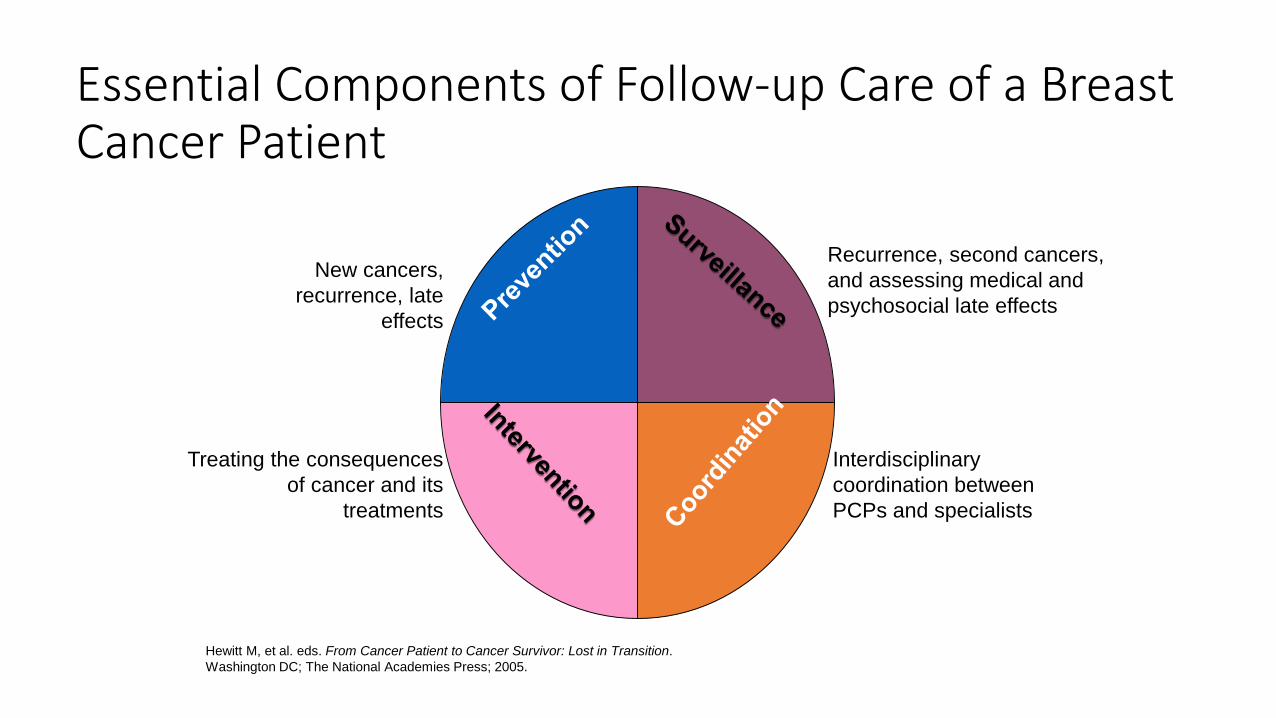
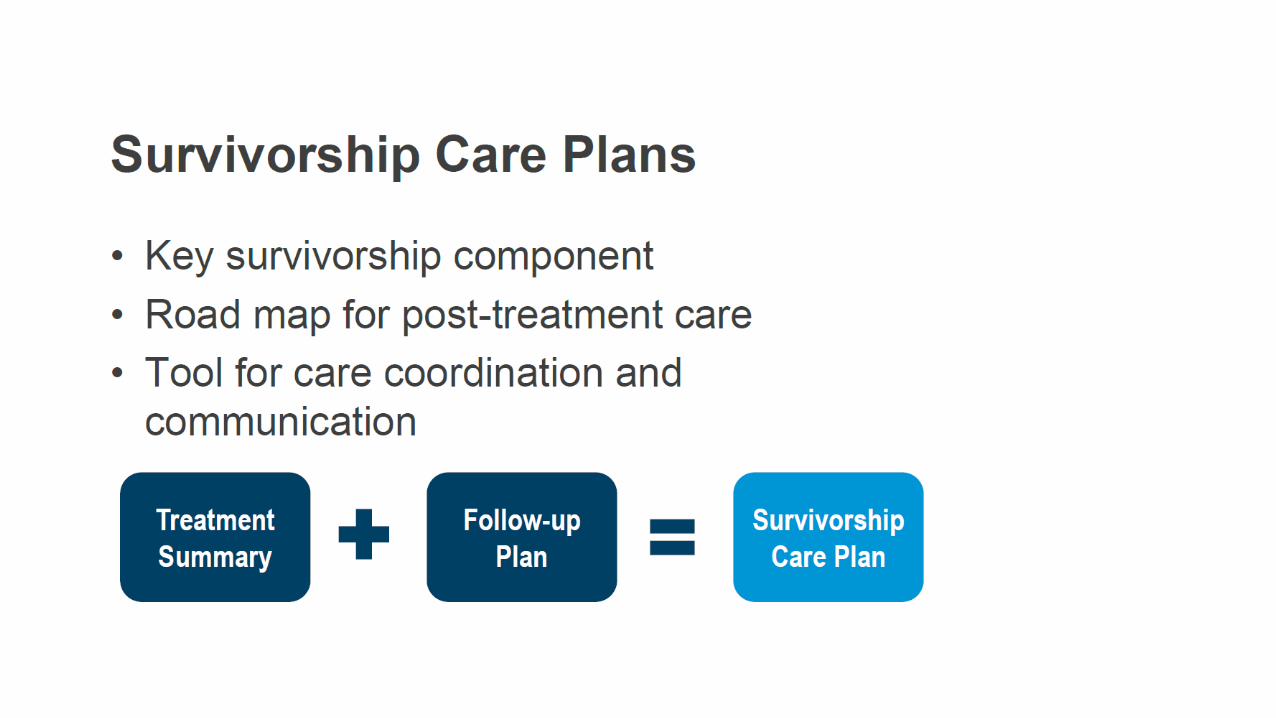
Essential Components of Follow-up Care of a Breast Cancer Patient
Treating the consequences of cancer and its
treatments
New cancers, recurrence, late
effects
Recurrence, second cancers, and assessing medical and psychosocial late effects
Interdisciplinary coordination between PCPs and specialists
Distress Assessment: James Supportive Care Screening Tool Use of the James Supportive Care Screening (SCS):
A patient self-report instrument designed to capture the most common symptoms reported by cancer survivors
When combined with targeted referrals, our tool will allow cancer programs to meet: The screening standards of the NCCN
ACS Accreditation Standards
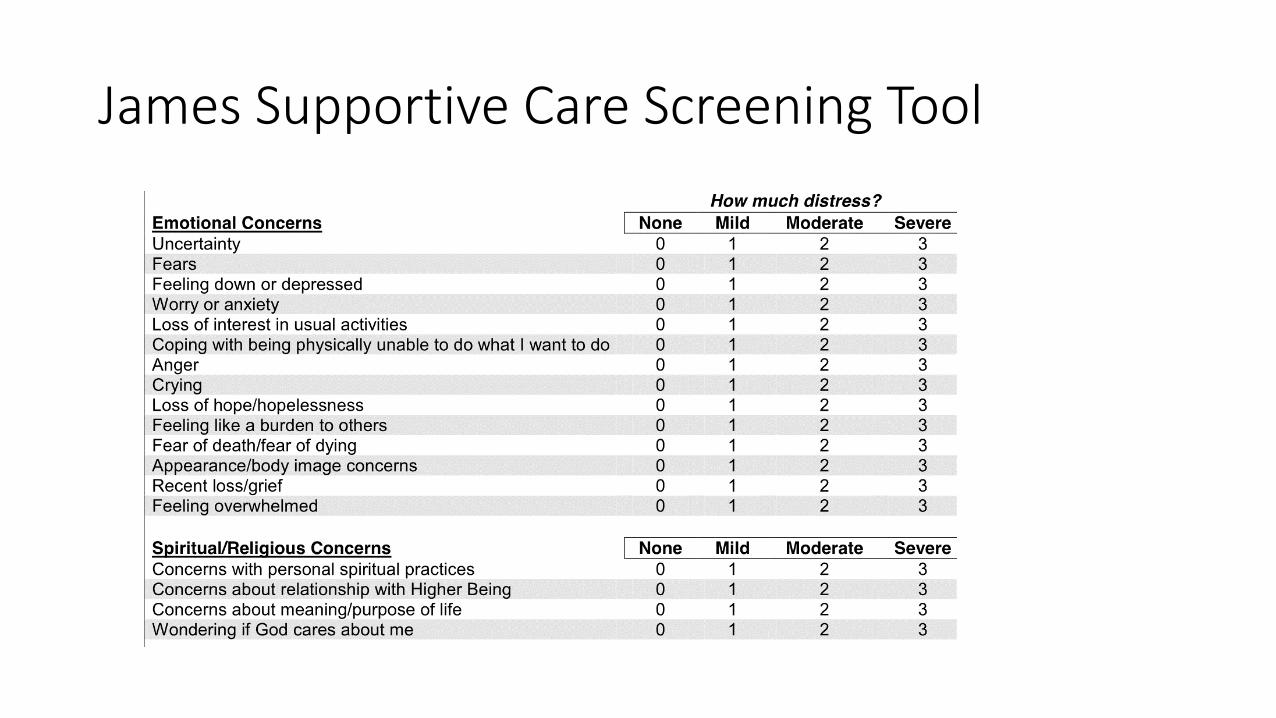
James Supportive Care Screening Tool
Goals
100% of all nonmetastatic cancer patietns will have a survivorship care plan 100% will have distress screening Currently at 60-70% at the Stefanie Spielman Breast Center
Rehabilitation Needs of Breast Cancer Survivors We oncologists cannot do this alone Many challenges Many opportunities Landscape will be changed in the next decade
More research is needed Understand the biological basis of the symptoms patients experience as a
consequence of treatment Evidence based approaches on how to best intervene How to coordinate care and referrals
How to individualize care for reach patient, survivor, thriver
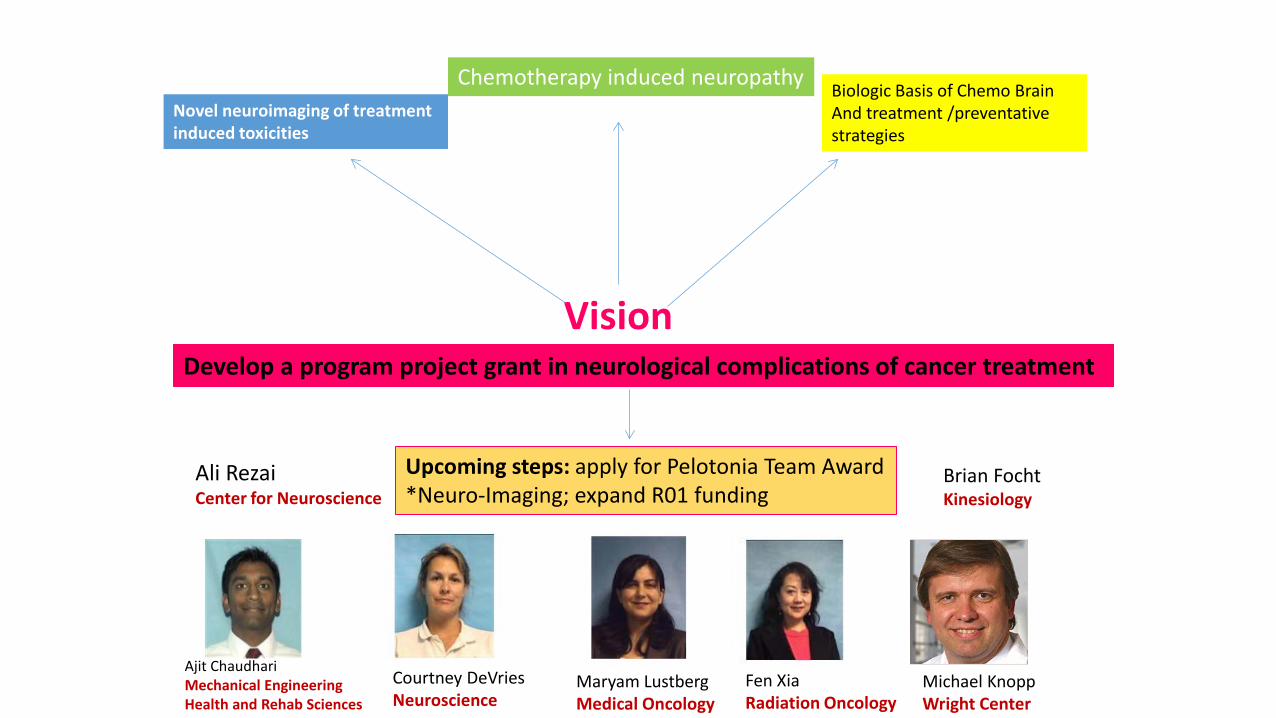
Vision Develop a program project grant in neurological complications of cancer treatment
Biologic Basis of Chemo Brain And treatment /preventative strategies
Novel neuroimaging of treatment induced toxicities
Upcoming steps: apply for Pelotonia Team Award *Neuro-Imaging; expand R01 funding
Chemotherapy induced neuropathy
Ajit Chaudhari Mechanical Engineering Health and Rehab Sciences
Courtney DeVries Neuroscience
Maryam Lustberg Medical Oncology
Fen Xia Radiation Oncology
Brian Focht Kinesiology
Michael Knopp Wright Center
Ali Rezai Center for Neuroscience
DeVries Laboratory Chaudhari Laboratory Michael Knopp Rebecca Andridge Rebecca Jackson Charles Shapiro Janice Kiekolt-Glaser SSCBC Breast medical oncology
colleagues Patients and families
CCTS funding Pelotonia funding (Idea Award
2012) Spielman Fund NCI: R01CA189947 R01CA194924 R03CA182165
Acknowledgements
Thank You
134





























