Embed Size (px)
Citation preview

O
Kl
CA
F
iQdscitFfntaaaptmtif
o
Md
1d
Operative Techniques in Otolaryngology (2005) 16, 209-212
RIGINAL CONTRIBUTIONS
ey principles to minimize mucoperichondrial flapacerations during nasal septal surgery
hristopher Low, MBChB, MRCS, Nadarajah Sanjeevan, MBChB, MRCS,lessandro Panarese, FRCS, MD, Stephen Hone, FRCS, MD
rom the Department of Otorhinolaryngology, Royal Liverpool University Hospital, Liverpool, United Kingdom.
Septal perforation, an unpleasant complication of septal surgery, is a direct result of compromisedvascular supply to the septum caused by substantial mucoperichondrial flap laceration during surgery.Blue silicone nasal splints can be used to assist surgeons in the early detection of a small mucoperi-chondrial flap laceration, thus minimizing the risk of converting it into a larger and more substantialtear. The splints can also be used to protect the mucoperichondrial flap from inadvertent iatrogenictrauma. These techniques are useful adjuncts for minimizing mucoperichondrial flap lacerations, whichultimately reduce the risk of septal perforation.© 2005 Elsevier Inc. All rights reserved.
KEYWORDSSeptoplasty;Intranasal splints;Mucoperichondrialflap;Laceration
etptdep1
owfOs
ttcarflvdsbtm
Septal surgery has been described since the ancient timesn Egypt. During the 18th century, a physician nameduelmatz recognized and addressed the problems of septaleformities by recommending daily digital pressure on theeptum.1 During the late 19th century, Ingals, who wasoined the father of modern septal surgery, used cocaine andnnovatively performed small en bloc resections of the sep-al cartilage.2 It was not until the early 20th century whenreer3 and Killian4 described the submucus resection, whichormed some of the basis of the current septoplasty tech-ique. In 1929, Metzenbaum described the swinging doorechnique.5 Because the classic submucus resection did notccount for correction of the caudal septum, in 1937, Peerdvocated removal of the caudal septum, straightening it,nd replacing the straightened cartilage onto the midlineosition.6 The submucus resection resulted in complica-ions, including septal perforation and unacceptable cos-etic deformities such as dorsal saddling, columella retrac-
ion, and alar widening. Therefore, in 1948, Cottlentroduced conservative resections in septal surgery,7 whichormed the basic principles of today’s septoplasty.
Septoplasty is now considered the operation of choice,8
ver and above submucus resection because of better pres-
Address reprint requests and correspondence: Christopher Low,BChB, MRCS, 3 Edinburgh Road, Liverpool L7 8RD, United King-
om.
sE-mail address: [email protected]043-1810/$ -see front matter © 2005 Elsevier Inc. All rights reserved.oi:10.1016/j.otot.2005.08.003
rvation of cosmetic results, and the rate of septal perfora-ion is lower.9 However, submucus resections are still beingerformed because some believe that septoplasty may leado residual or recurrent nasal obstruction, and there is noifference in the septal perforation rate between the 2 op-rations.10 A recent article showed significant overall septalerforation rates of 2% to 8% for submucus resection and.6% to 5.4% for septoplasty.11
The main indications for septoplasty are to relieve nasalbstruction or unblock the osteomeatal complex of sinuseshen medical treatment has failed. It is sometimes per-
ormed in conjunction with rhinoplasty to harvest a graft.ccasionally, it is performed to ameliorate posterior epi-
taxis.There are various approaches in septoplasty, and the
echnique used is dependent on the septal deformity encoun-ered. Regardless of the approach, raising the mucoperi-hondrial flaps is an essential step in the operation to gainccess to the septal deformity. During this step, the inexpe-ienced eye of residents and trainees may fail to detect smallap lacerations, and may even extend the lacerations inad-ertently. Substantial mucoperichondrial flap lacerationsevoid the septum of its vascular supply, thus leading toeptal necrosis and perforation.12 With the application of alue silicone intranasal splint for color contrast, early de-ection of small mucoperichondrial flap lacerations can beade effectively, thus minimizing the lacerations. The
plint can also be used to prevent incidental iatrogenic

tpm
S
Tfiornpit
ec
cctisrflbsptdv
Fl
Ffl
210 Operative Techniques in Otolaryngology, Vol 16, No 3, September 2005
rauma to the flaps. This article describes a standard septo-lasty technique, highlighting key principles to minimizeucoperichondrial flap laceration.
urgical technique
he patient is positioned supine, with 30° upward anglerom the hips. General anesthetic is usually used, althought is possible to perform septoplasty with local anestheticnly. The patient is draped, and 3 mL of 1:10,000 epineph-ine on ribbon gauze or cotton strips is applied into eachasal cavity. Further vasoconstriction and analgesia are ap-lied with 2 mL of 1% lidocaine, and 1:80,000 epinephrinenjection into the columella soft tissue at the caudal edge ofhe septum and into the submucoperichondrial plane bilat-
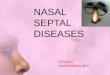
igure 2 The tip of a septal spur is where the thinned and stret
igure 1 Blue splint in right nasal cavity providing good color cap laceration. (Color version of figure is available online.)
eads to a tear during dissection of the flap.
rally. Infiltration into the submucoperichondrial plane fa-ilitates dissection of the mucoperichondrial flap.
A vertical skin incision of the left vestibule is made at theaudal septal edge (left hemi-transfixion incision). This pro-edure allows good access to the entire septum; posteriorlyo the perpendicular plate of ethmoid bone and vomer, andnferiorly to the maxillary crest, including the anterior nasalpine. A blue intranasal silicone splint is inserted into theight nasal cavity before raising the right mucoperichondrialap (Figure 1). Dissection of the subperichondrial planeegins at the caudal edge of the septal cartilage with theharp tip of a curved scissors. When the subperichondriallane is undermined, a Freers dissector is then used to raisehe flap as much as it is necessary to gain access to theeformities. During this process, 3 areas are potentiallyulnerable to mucosal flap tear: (1) between the septal
ucoperichondrial flap has a potential weakness, which inevitably
t to assist surgeons during early detection of a mucoperichondrial
ched m
ontras

clfllaaslpdnfl
i
acembotdoo
bpbsopc
(esmtandscoTr
C
Ta
Fah
Fp
211Low et al Key Principles to Minimize Mucoperichondrial Flap Lacerations
artilage and maxillary crest; (2) between the septal carti-age and vomer; and (3) at the tip of a septal spur, where theap is thinned and stretched (Figure 2). When mucosal flap
aceration occurs, the blue intranasal splint is readily seen asresult of the contrast of colors between the splint (blue)
nd the flap (red hue) (Figure 3). This contrast alerts theurgeon to the tear, thereby reducing the risk of furtheraceration. It also provides good orientation of the tissuelanes, which helps the surgeon in relocating the plane ofissection. The blue splint is then transferred into the leftasal cavity for dissection of the left mucoperichondrialap.
Once both flaps are raised adequately, the septal cartilages dislocated from its attachment to the vomer (posteriorly)
igure 3 Early exposure of mucoperichondrial flap laceration asresult of good color contrast between the blue splint and the redued mucosa. (Color version of figure is available online.)
igure 4 Blue splint in right subperichondrial plane protecting
roviding good color contrast when the cartilage has been cut through.nd maxillary crest (inferiorly) with a Freer dissector. Ex-ess cartilage on the vertical plane is trimmed at the inferiordge of the cartilage. Bony spurs and deviations are re-oved with straight cutting forceps. Using a small surgical
lade, deviations of the septal cartilage can be treated by 1r a combination of the following methods: (1) scoring onhe concave aspect of the deviation; (2) excision of theeviated portion of the cartilage, leaving behind 1-cm stripf caudal and dorsal strut; and (3) partial thickness excisionf the convex surface of the deviation.
If excision of the cartilage is performed with a blade, alue splint should be placed into the submucoperichondriallane to shield the ipsilateral mucosal flap from the surgicallade when it cuts through the cartilage from the oppositeide. This procedure should also be used during the harvestf septal cartilage for grafting purposes. The blue splintrovides effective visual assistance to the surgeon when theartilage is cut through (Figure 4).
The hemitransfixion incision is closed with a 3-0 Vicrylabsorbable) suture (Ethicon, Inc, Johnson & Johnson, Som-rville, NJ). A mattress suture is fashioned with the sameuture by sandwiching the residual cartilage between bothucoperichondrial flaps to prevent septal hematoma forma-
ion. Studies have shown that there is no advantage inpplying intranasal splints to prevent synechiae formation ifasal douching is advocated postoperatively for 7-10ays.13-16 This result is no evidence that splints providetability to the septum postoperatively. Furthermore, theyan cause increased morbidity in patients. Nasal packs arenly applied if there is excessive bleeding from the nose.hese reasons deter us from applying intranasal splints
outinely. Nasal packs are also not applied routinely.
omments
he described septoplasty technique is one of many standardpproaches, which allows safe and effective correction of clin-
ight mucoperichondrial flap from inadvertent scalpel injury and
the r (Color version of figure is available online.)
icfsdctmsa
R
1
1
1
1
1
1
1
212 Operative Techniques in Otolaryngology, Vol 16, No 3, September 2005
cally significant septal deformities. Preserving the mucoperi-hondrial flaps or minimizing inevitable lacerations is the keyor reducing the risk of septal perforation. A blue intranasalilicone splint can be a useful tool for residents or traineesuring the early stages of their training to enhance their appre-iation of the surgical planes and minimize their flap lacera-ions. This tool can only inspire confidence in the trainee. Thisethod can be used to facilitate operative demonstration of
eptal surgery. The splints can be purchased in different colorsnd sizes to accommodate the surgeon’s preference.
eferences
1. Quelmatz E: Haller’s disputat ad nosbraum. Paris, Historian, 17572. Ingals EF: Deflections of the septum narium. Arch Laryngol 3:291-
313, 18823. Freer OT: The correction of deflections of the nasal septum with a
minimum of traumatism. JAMA 38:636, 19024. Killian G: Die submucose fensterresektion der nasenscheidewand.
Arch Laryngologie 16:362-394, 19045. Metzenbaum M: Replacement of the lower end of the dislocated
cartilage versus submucous resection of dislocated end of the septal
cartilage. Arch Otolaryngol Head Neck Surg 9:282-311, 19296. Peer LA: An operation to repair lateral displacement of the lowerborder of the septal cartilage. Arch Otolaryngol Head Neck Surg25:475-489, 1937
7. Cottle MH, Loring RM: Newer concepts of septum surgery: Presentstatus. Eye Ear Nose Throat Mon 27:403-429, 1948
8. Chuden H: SMRs, septoplasty and the surgical treatment of septalperforations. Laryngol Rhinol Otol (Stuttg) 55:264-269, 1976
9. Haraldsson PO, Nordemar H, Anggard A: Long-term results afterseptal surgery–Submucous resection versus septoplasty. ORL J Oto-rhinolaryngol Relat Spec 49:218-222, 1987
0. Low WK, Willatt DJ: Submucous resection for deviated nasal septum:A critical appraisal. Singapore Med J 33:617-619, 1992
1. Bateman ND, Woolford TJ: Informed consent for septal surgery: Theevidence-base. J Laryngol Otol 117:186-189, 2003
2. Fairbanks DN, Fairbanks GR: Nasal septal perforation: Prevention andmanagement. Ann Plast Surg 5:452-459, 1980
3. Cook JA, Murrant NJ, Evans KL, et al: Intranasal splints and theireffects on intranasal adhesions and septal stability. Clin Otolaryngol17:24-27, 1992
4. von Schoenberg M, Robinson P, Ryan R: The morbidity from nasalsplints in 105 patients. Clin Otolaryngol 17:528-530, 1992
5. Malki D, Quine SM, Pfleiderer AG: Nasal splints, revisited. J LaryngolOtol 113:725-727, 1999
6. Al-Mazrou KA, Zakzouk SM: The impact of using intranasal splintson morbidity and prevalence of adhesions. Saudi Med J 22:616-618,
2001