Embed Size (px)
Citation preview

I N T E R - AT R I A L S E P TA L P U N C T U R E
T E C H N I Q U E S
B A L A K U M A R A N . J
P G I M E R & D R . R . M . L H O S P I TA L
N E W D E L H I .
TRANSEPTAL PUNCTURE (TP)
History of septal puncture
Embyrology and Anatomy of septum.
Methods of septal puncture.
Landmarks.
Septal puncture technique
TP in abnormal hearts.
TP in special circumstances.
Complications of TP and Management.
Atrial septostomy
HISTORY OF SEPTAL PUNCTURE
1956- Ross – a surgical intern in John Hopkins under Blalock.
Went to NHI- worked under Dr. Morrow in maryland.
Saw some demonstrations.
Suprasternal approach (a long needle passed retrosternally through the
great vessels and into the left atrium [LA]) (Radner technique)
Posterior transthoracic method (a needle passed lateral to the vertebral
column into the LA).
Transbronchial approach to the LA and direct puncture of the left ventricle
by the subxyphoid or apical approaches.
J Am Coll Cardiol 2008;51:2107–15
HISTORY OF SEPTAL PUNCTURE
Ross - used a long curved needle inserted through the dog’s saphenous
vein to access the left atrium via the interatrial septum.
These animal experiments followed the first clinical application in man
published in1959.
Dr. Brockenbrough, also working at the National Institute of Health,
modified the transseptal needle to allow insertion via the Seldinger
technique and published his data in 1960 and 1962 .
Am J Cardiol 1959; 3: 653–5
1960, Brockenbrough and Braunwald-needle.
1979, Duff and Mullins- sheath, dilator.
Croft - found the use of the RAO projection (RAO 45°–50°)-for IAS / pig tail use
in Ascending Aorta.
Transseptal catheterization became routine during mitral valve balloon
valvuloplasty and presently is part of the armamentarium of the
interventional electrophysiologist.
Clin. Cardiol. 18,217-220 (1995)

Embryology of septum
The primitive sinuatrium is separated into right and left atria by the downward
growth of the septum primum (develops at fifth week of gestation) from the
roof of the sinuatrium toward the atrioventricular (AV) canal, thereby creating
an inferior interatrial opening known as the ostium primum (between SP and
endocardial cushion).
Soon after, numerous perforations form in the anterior–superior portion of the
septum primum, eventually coalescing to form the ostium secundum..
The Journal of Innovations in Cardiac Rhythm Management, (2013), 1415–1427
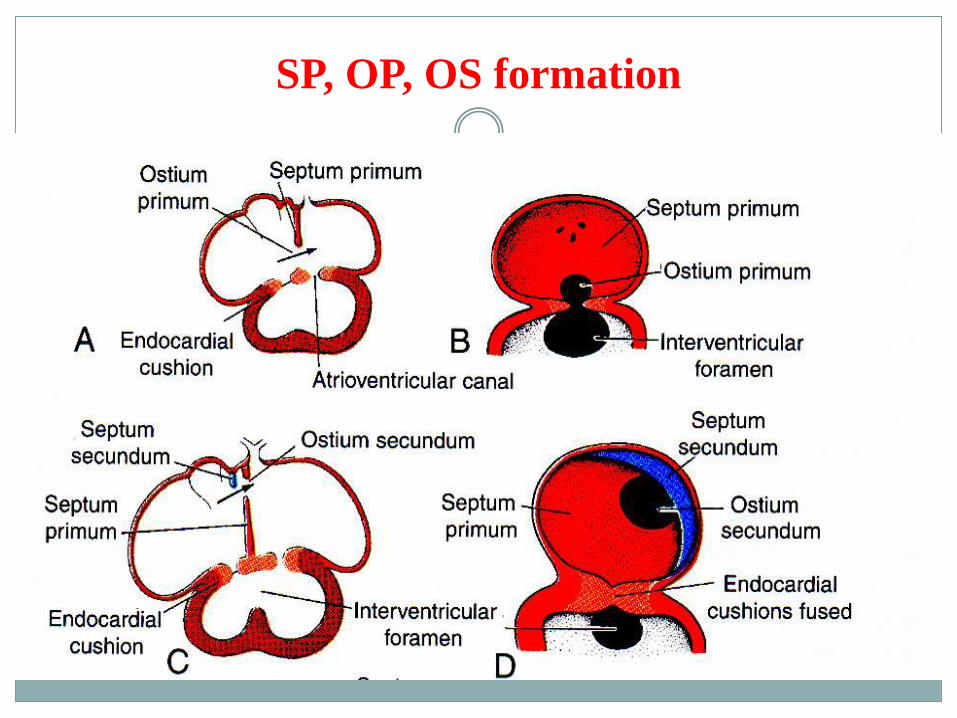
SP, OP, OS formation

The septum secundum begins to develop to the right of the septum primum – stops growing at seventh
week – leads to posterior and inferior gap known as fossa ovalis (FO).
The area of fusion of the muscular septum secundum and the thinner portion of the septum primum is
known as the limbus, which forms a raised margin around the superior aspect of the FO. The FO is
covered by thin, fibrous tissue from the septum primum, forming the valve of the foramen ovale
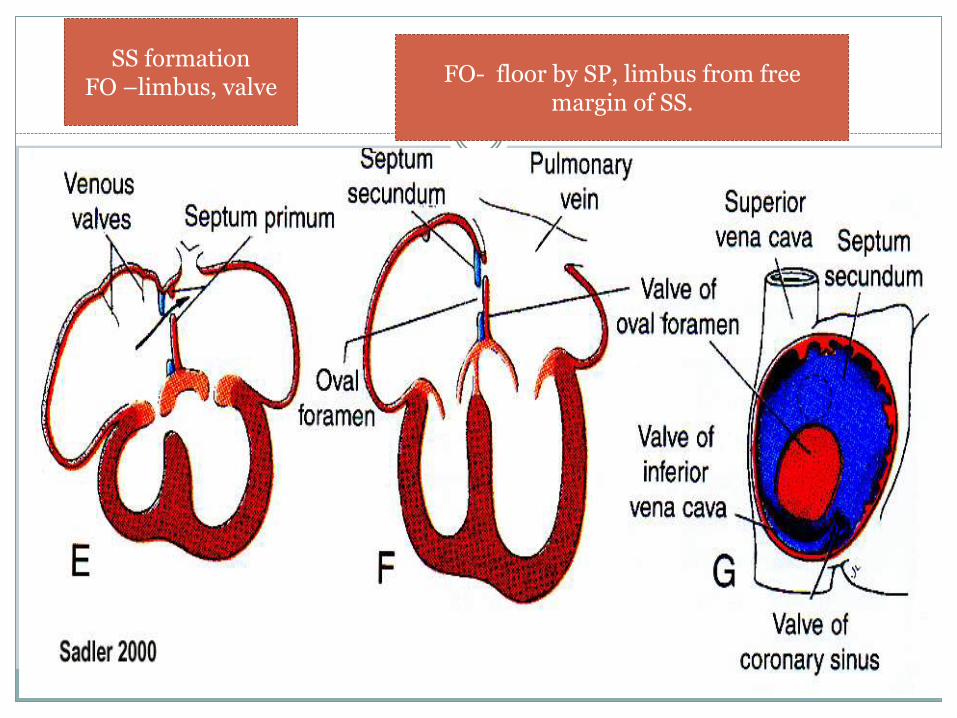
SS formationFO –limbus, valve
FO- floor by SP, limbus from free margin of SS.
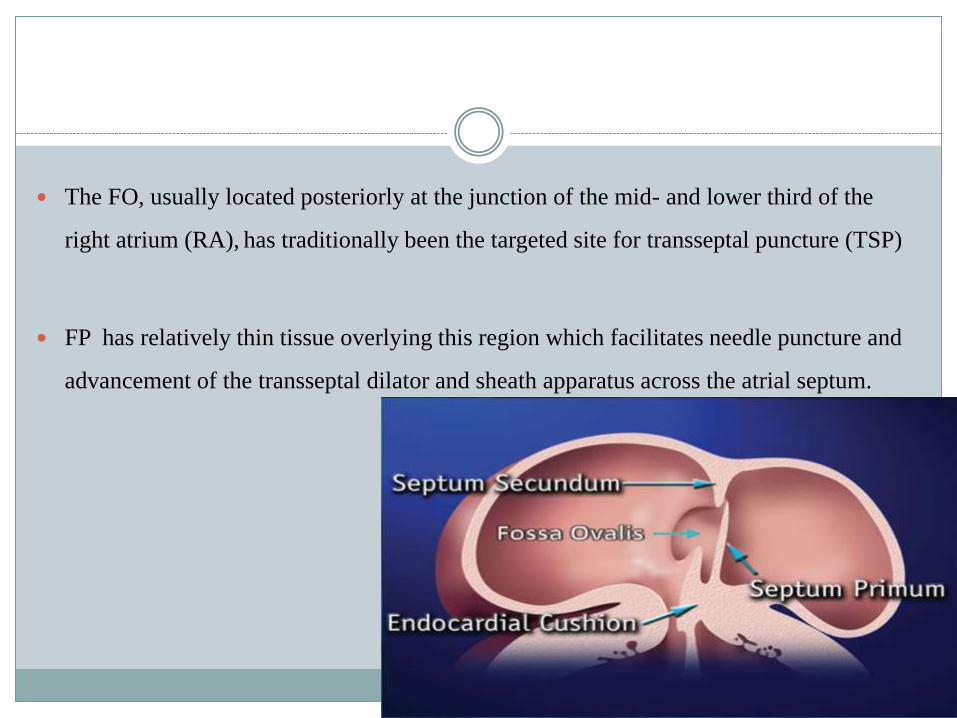
The FO, usually located posteriorly at the junction of the mid- and lower third of the
right atrium (RA), has traditionally been the targeted site for transseptal puncture (TSP)
FP has relatively thin tissue overlying this region which facilitates needle puncture and
advancement of the transseptal dilator and sheath apparatus across the atrial septum.
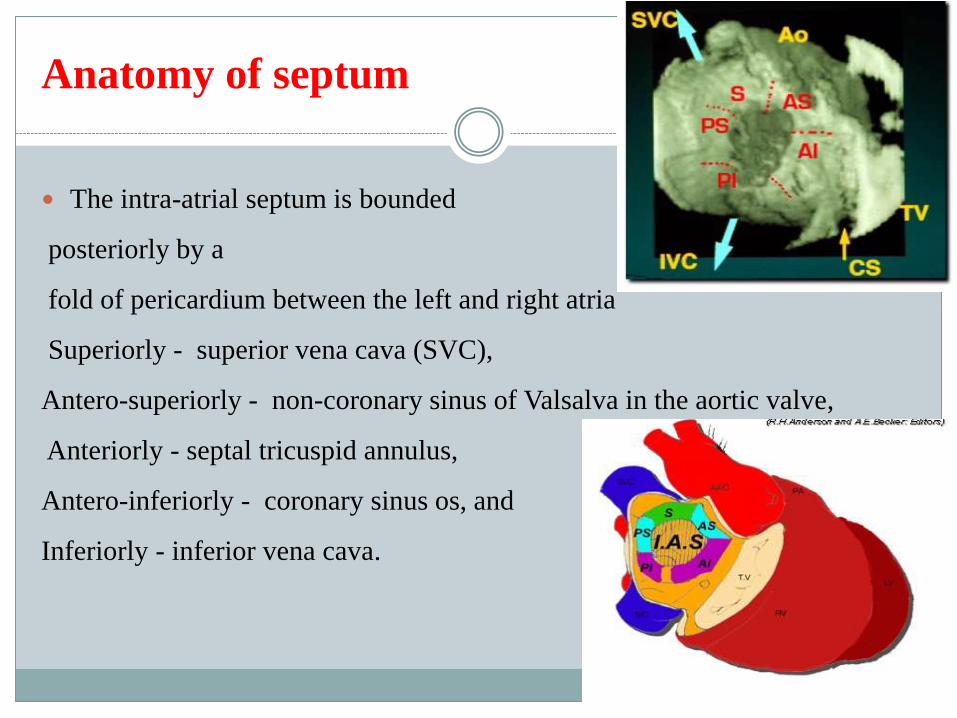
Anatomy of septum
The intra-atrial septum is bounded
posteriorly by a
fold of pericardium between the left and right atria
Superiorly - superior vena cava (SVC),
Antero-superiorly - non-coronary sinus of Valsalva in the aortic valve,
Anteriorly - septal tricuspid annulus,
Antero-inferiorly - coronary sinus os, and
Inferiorly - inferior vena cava.
The atrial septum is a blade-shaped structure with a concave anterior
margin that reflects the curve of the ascending aorta, a convex
posterior margin, and an inferior margin along the mitral annulus.
The Fossa ovalis comprises an average of 28 per cent of the total
septal area, or 43 mm2 in infants and 240 mm2 in adults.
Am Heart J.1979 Aug;98(2):194-9
INDICATIONS OF IAS PUNCTURE
PTMC
EP STUDY
CONGENITAL DISEASES
AORTIC VALVE GRADIENT.
PERCUTANEOUS AORIC VALVE REPLACEMENT/MITRAL VALVE
REPAIR.
And also most important is that it needs site specific puncture in some special
circumstances.
cardiac interventions Today, March/April 2014
TRANSEPTAL PUNCTURE
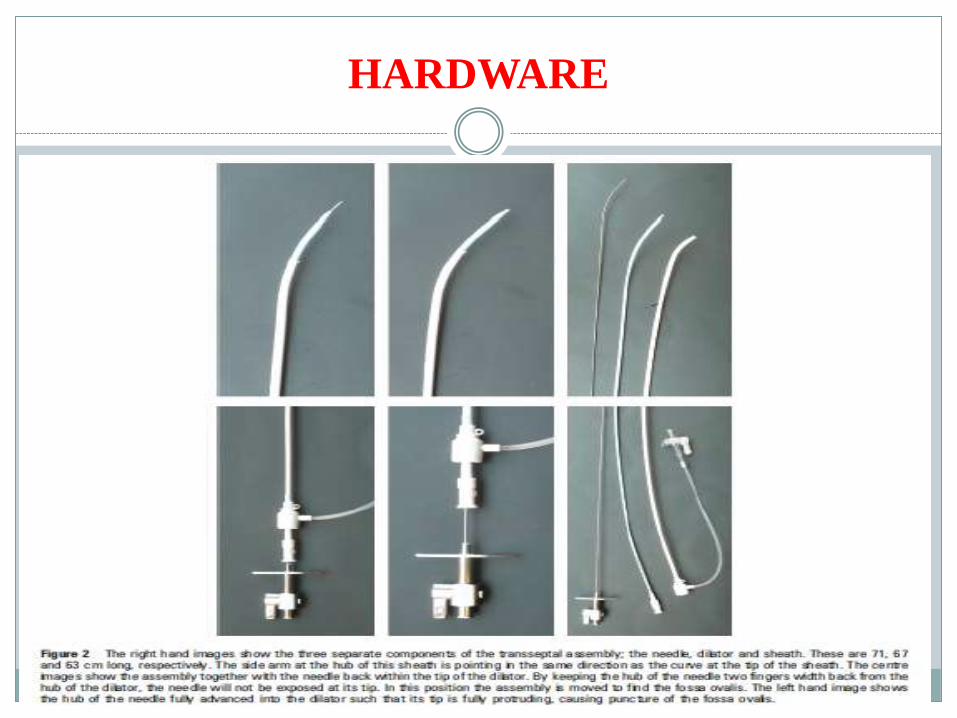
HARDWARE
TRANSEPTAL NEEDLE
MEDTRONIC
Brockenbrough needle.
The Medtronic Brockenbrough curved needle is made up of an outer
cannula and an inner stylet.
The outer cannula is made of flexible thin-walled tubing.
The inner stylet is solid, much stiffer and closely fitting, whose
sharpened end protrudes 2-3 mm beyond the tip of the cannula.
ADULT- 18 guage tapering to 21 gauge tip.(71 cm).
PAEDIATRIC- 19 guage tapering to 22 guage tip (56 cm).
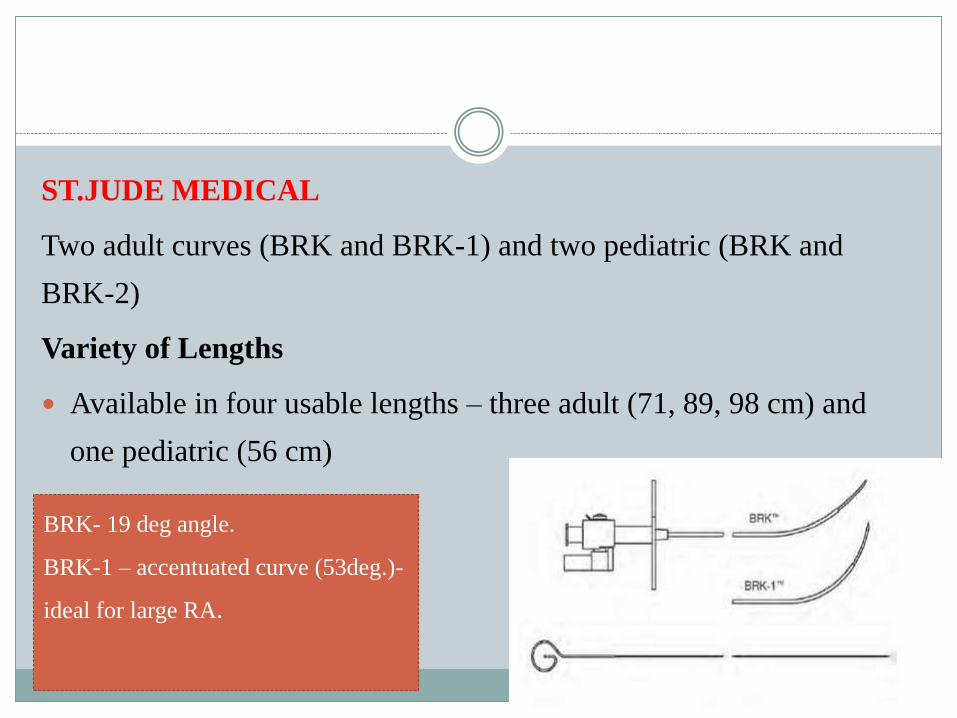
ST.JUDE MEDICAL
Two adult curves (BRK and BRK-1) and two pediatric (BRK and
BRK-2)
Variety of Lengths
Available in four usable lengths – three adult (71, 89, 98 cm) and
one pediatric (56 cm)
BRK- 19 deg angle.
BRK-1 – accentuated curve (53deg.)-
ideal for large RA.

ROUTE OF PUNCTURE
TRANSFEMORAL
RIGHT
LEFT
TRANSJUGULAR
RIGHT
LEFT
TRANSHEPATIC
Methods of septal puncture
FLUOROSCOPIC METHOD (Based on various landmarks)
Trans Esophageal Echo GUIDED
INTRACARDIAC Echo GUIDED.
Mechanical
Phase Array
MDCT GUIDED
MRI GUIDED (ANIMALS)Heart 2009;95;85-92

LANDMARKS FOR SEPTAL PUNCTURE
Various methods available.
1. Inoue angiographic method.
2. Hung modified fluoroscopic method.
Above for identification of midline (vertical and horizontal).
Via
Pigtail catheter.
EP catheters (CS and His bundle catheters).
Catheterization and Cardiovascular Diagnosis 26:275284 (1992)
Inoue's angiographic method
VERTICAL MIDLINE
Inoue has devised a specific transseptal puncture technique designed for
the Inoue-balloon BMV, incorporating the concept of a vertical “mid-line,”
a line assumed to divide the intra-atrial septum into anterior and posterior
halves.
This line is defined based on the landmarks obtained from right atrial
angiography (with levophase) during normal respiration in the frontal
plane.
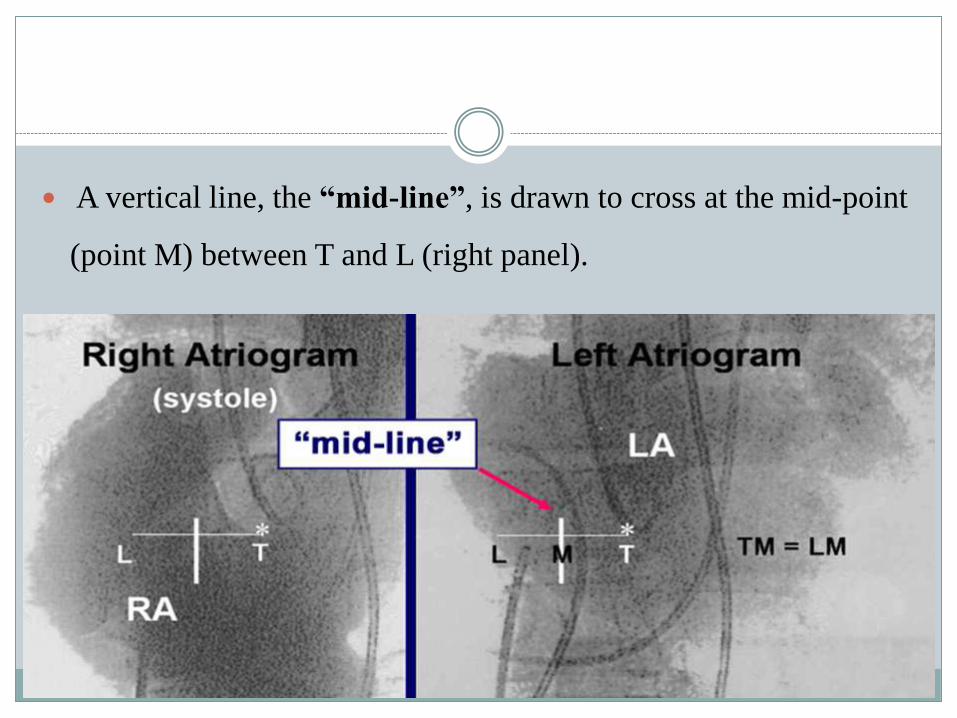
A vertical line, the “mid-line”, is drawn to cross at the mid-point
(point M) between T and L (right panel).
Hung's modified fluoroscopic method
VERTICAL MIDLINE
In this method, the aortic valve instead of the tricuspid valve is used as a landmark
because of their proximity. Therefore, point T is substituted with the tip of a pigtail
catheter touching the aortic valve (usually the non-coronary sinus of Valsalva) in
the frontal view.
A horizontal line is drawn from point A to L, where the line intersects the right
lateral edge of the left atrium.
The "mid-line" thus derived is usually identical to that from the Inoue's
angiographic method
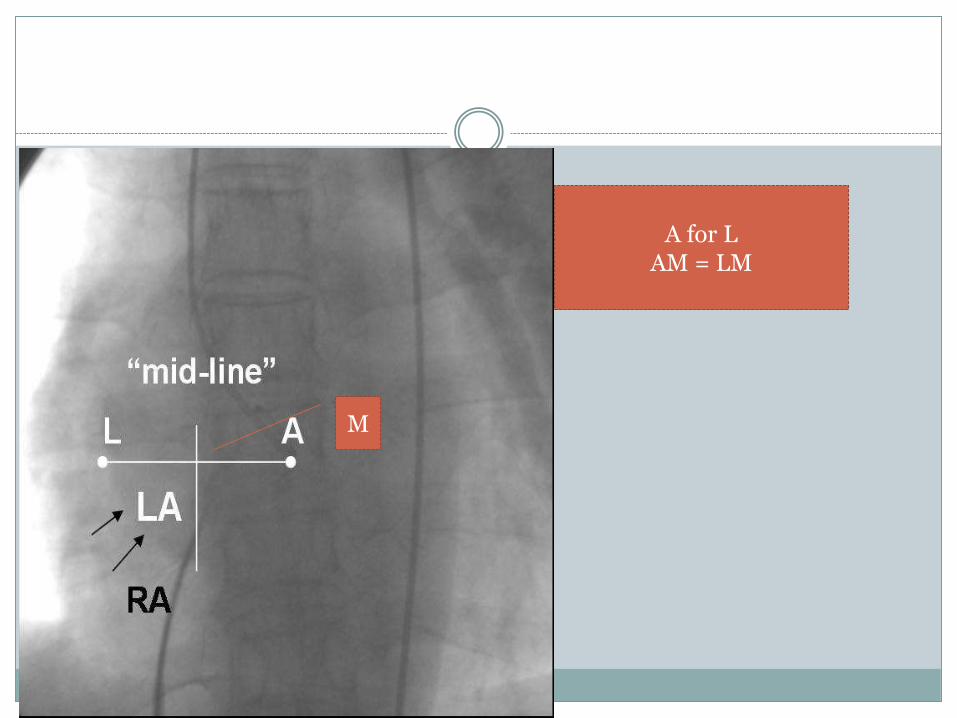
A for LAM = LM
M

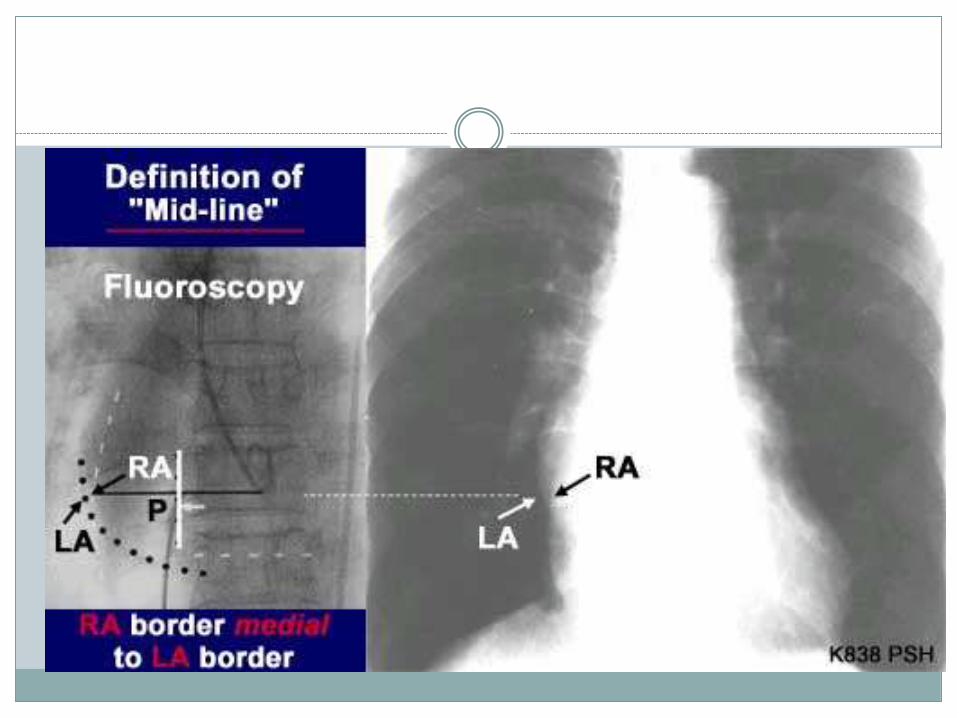
Posterior Limit of Atrial Septum -- Left vs. Right
Atrium
The posterior limit of septum is the lateral border of the medial
atrium, usually the left atrium.
Infrequently (such as in patients with giant left atria), the lateral
border of the right atrium is medial to that of the left atrium, and thus
the posterior limit is the right atrium.
In the case with a giant left atrium, if the left atrial border is used as the
posterior septal limit, the mid-line would be outside or near the right Giant
Atrium.
Puncture on this false “mid-line” would result in cardiac perforation and
tamponade.
Inoue's Angiographic Method vs. Fluoroscopic
Method
Because in most cases of mitral stenosis, the left atrial silhouette is visible under
fluoroscopy, the “septal line” and “mid-line”can be determined without angio.
However, angiography is recommended in the following situations:
1) For operators inexperienced with the transseptal puncture technique.
2) In cases in which atrial silhouettes are not well visualized under
fluoroscopy
3) In extremely difficult cases of transseptal puncture, e.g.in the presence of
a giant left atrium or severe kyphoscoliosis
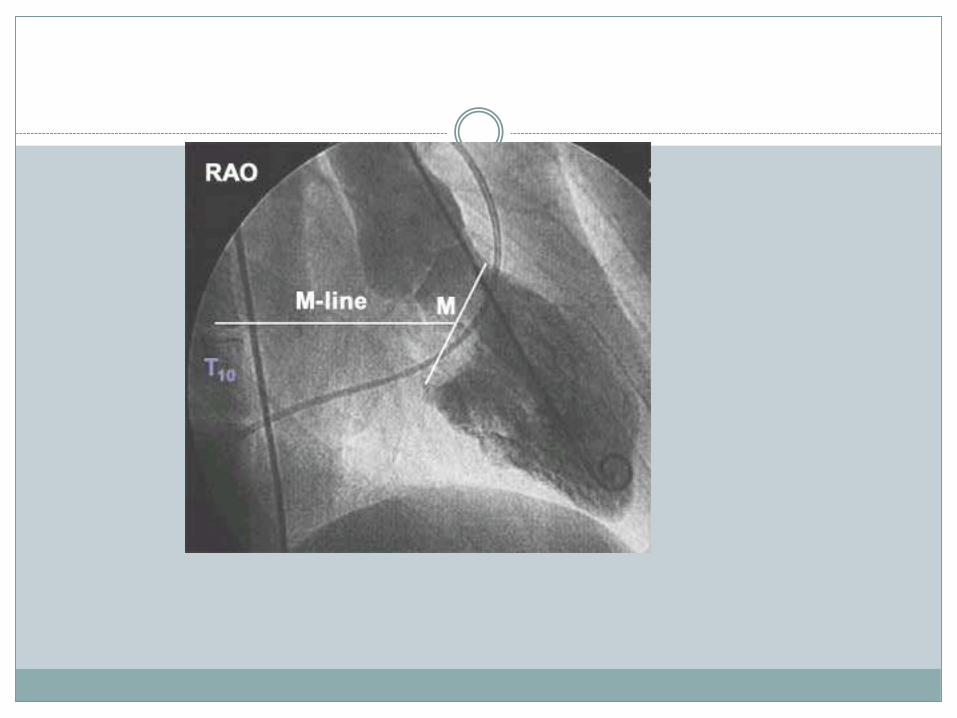
Definition of the Horizontal "M-line"
The "M-line" is a horizontal line crossing the center of the mitral annulus (point M). It
is derived from a diastolic stop frame of diagnostic left ventriculography obtained in
30-degree RAO projection.
The latter is identical to the projection used when manipulating the catheter
balloon across the mitral valve. This line is memorized in relation to the vertebral
body (T10).
The stop frame angiogram is also used as a road map during transseptal puncture
and balloon catheter manipulation.
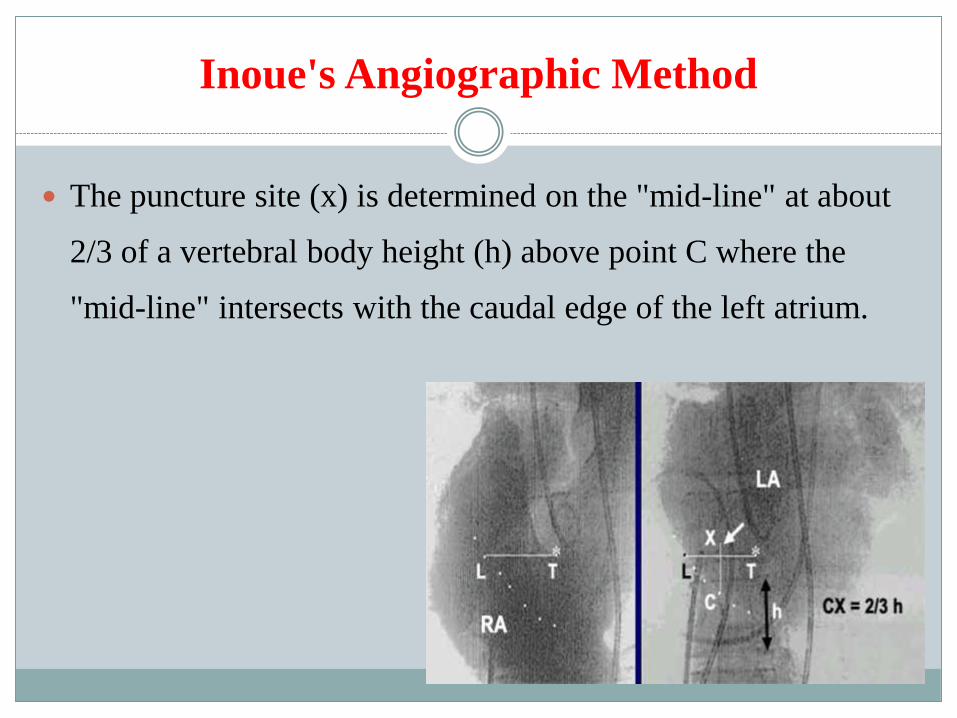
Inoue's Angiographic Method
The puncture site (x) is determined on the "mid-line" at about
2/3 of a vertebral body height (h) above point C where the
"mid-line" intersects with the caudal edge of the left atrium.
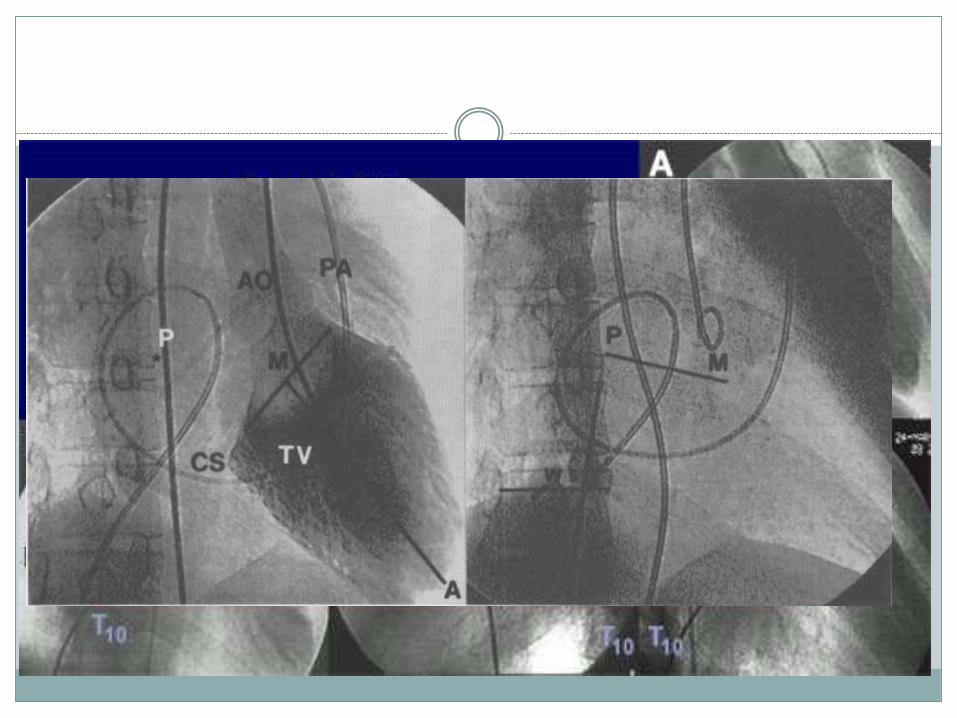
Modified method
The puncture is usually made also on the "mid-line", but on the level of horizontal
"M-line" derived from left ventriculogram.
Usually the distance (PM) is about 1.2 times the vertebral width (w) and the puncture
site (P) is slightly higher than the M point.
However, in individual cases the puncture site on the "mid-line" may have to be
adjusted. For example, in a patient with a giant left atrium, the operator often is forced
to make septal puncture more caudally to the "M-line" because the septum begins its
curviliniear shape more caudally.
EP LANDMARKS FOR TRANSEPTAL PUNCTURE
These catheter options include:
HIS Catheter (positioned on the HIS bundle)-Replaces Pigtail in aorta.
CS Catheter (located in the coronary sinus)-The usual puncture site is
approximately 10–14 mm from the ostium of the CS and superior and
posterior in the RAO view or superior in the LAO view
The Journal of Innovations in Cardiac Rhythm Management, June 2011

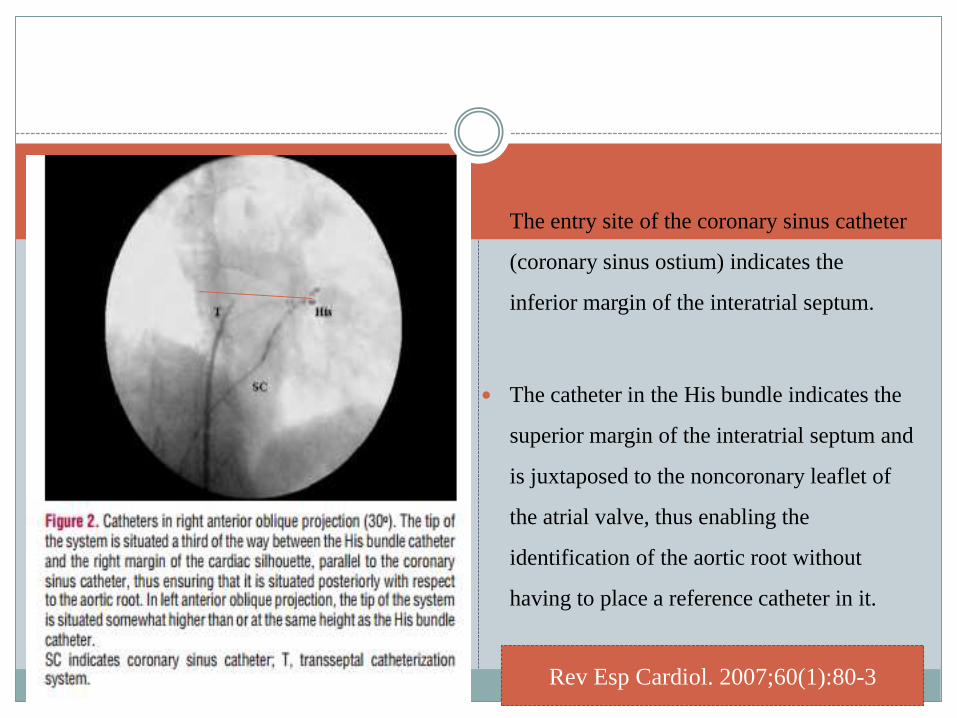
The entry site of the coronary sinus catheter
(coronary sinus ostium) indicates the
inferior margin of the interatrial septum.
The catheter in the His bundle indicates the
superior margin of the interatrial septum and
is juxtaposed to the noncoronary leaflet of
the atrial valve, thus enabling the
identification of the aortic root without
having to place a reference catheter in it.
Rev Esp Cardiol. 2007;60(1):80-3
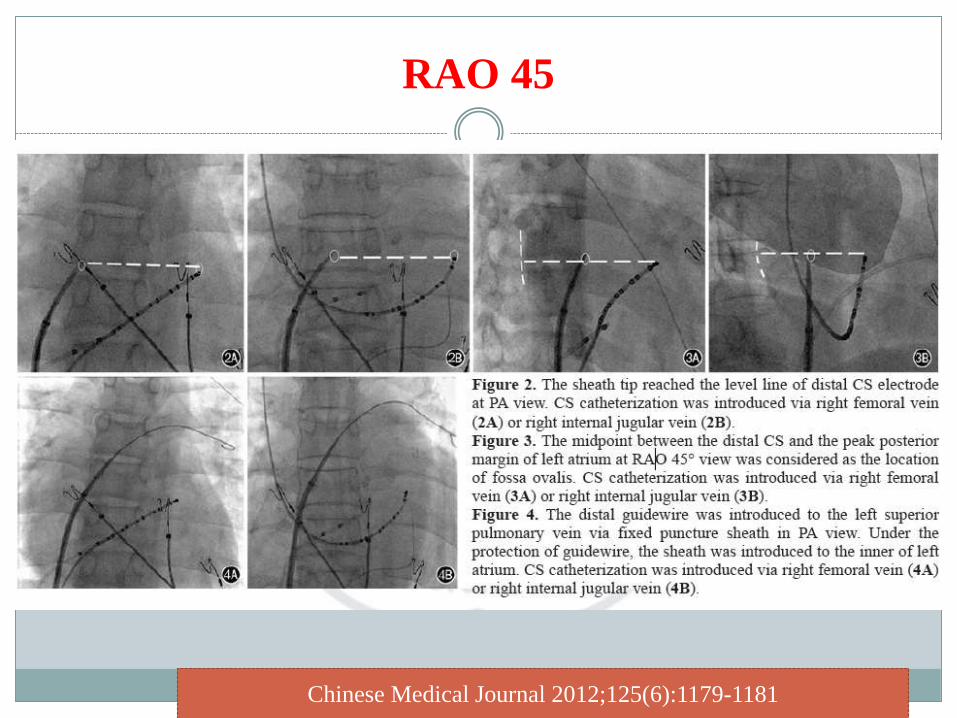
RAO 45
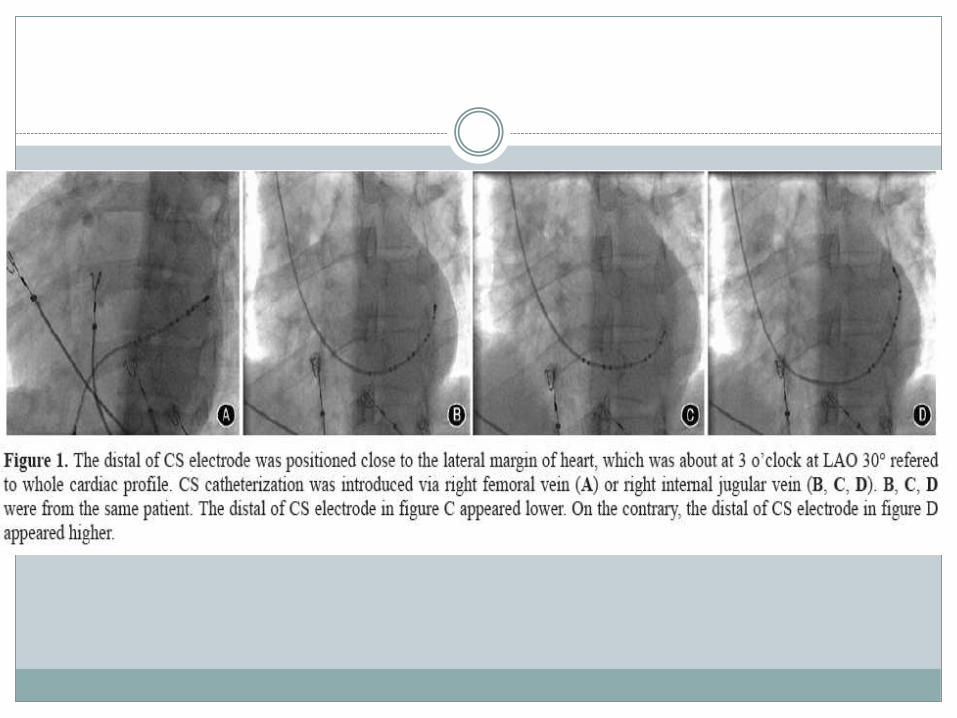
Chinese Medical Journal 2012;125(6):1179-1181
MDCT GUIDED FLOUROSCOPY
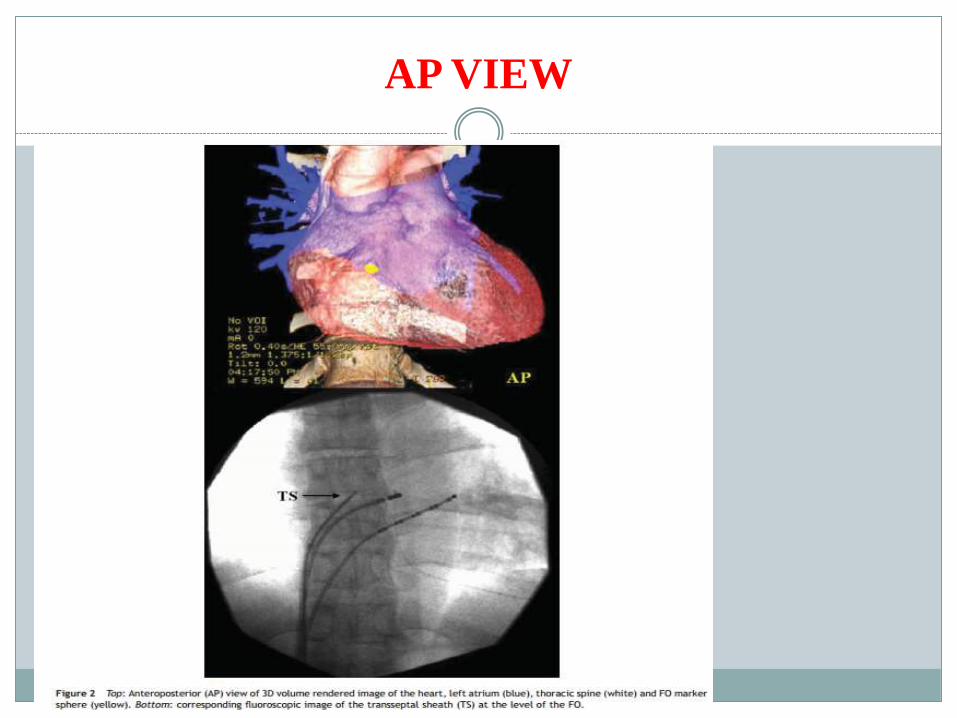
AP VIEW
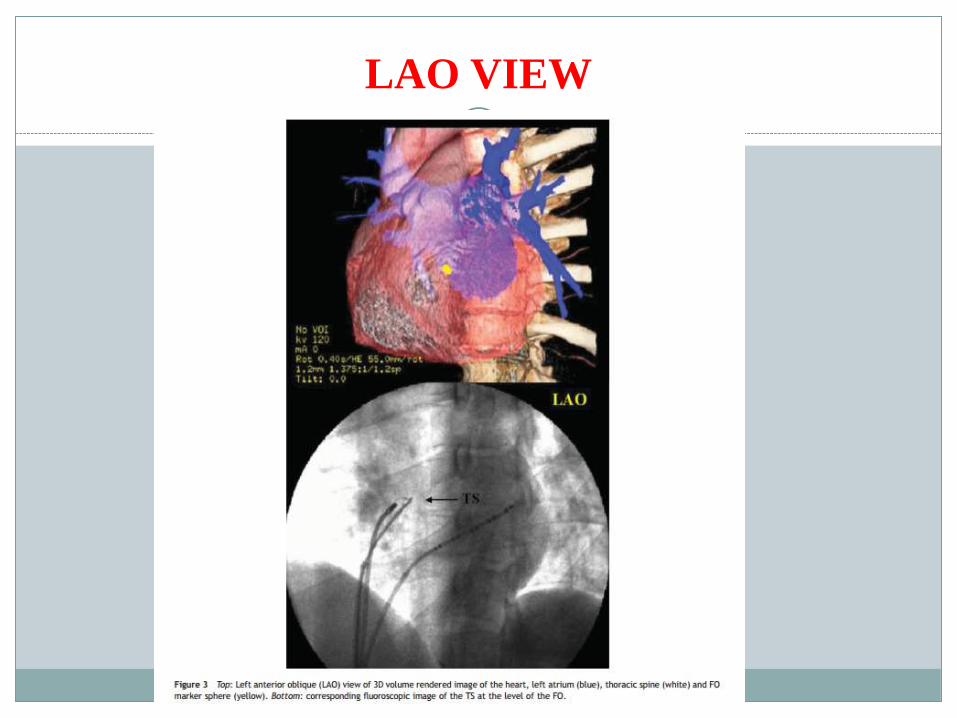
LAO VIEW

Real-Time MRI Guided Atrial Septal Puncture and
Balloon Septostomy in SwineAmish N. Raval, MD, Parag V. Karmarkar, MSc, [...], and Robert J. Lederman, MD
Catheter Cardiovasc Interv. 2006 April ; 67(4): 637–643.
rtMRI permits rapid and robust transcatheter
ASP and BAS by virtue of superior
visualization of complex anatomy in any
orientation.
Additional advantages include online
hemodynamic assessment and freedom from
exposure to ionizing radiation or nephrotoxic
contrast agents. Further technical development
may enable more novel applications.
PTMC TECHNIQUE
Preoperative fasting required.
Iv fluids
Peripheral iv cannula checked.
Prepare both the groins.
Two venous access.
To keep in mind about cardiac tamponade is a dreaded
complication and be prepared for that.
Heart 2009;95:85–92.
PTMC TECHNIQUE
The basic technique involves right (7 F) and left femoral
vein(6 F) access.
A 0.032 inch small guide wire is needed.
Take right femoral arterial access(6F). A pigtail catheter is
placed in the aortic root (non-coronary cusp) to better define
the location of the aortic valve.
LV angio (30 RAO view) - to look for MR
STEPS IN SEPTAL PUNCTURE
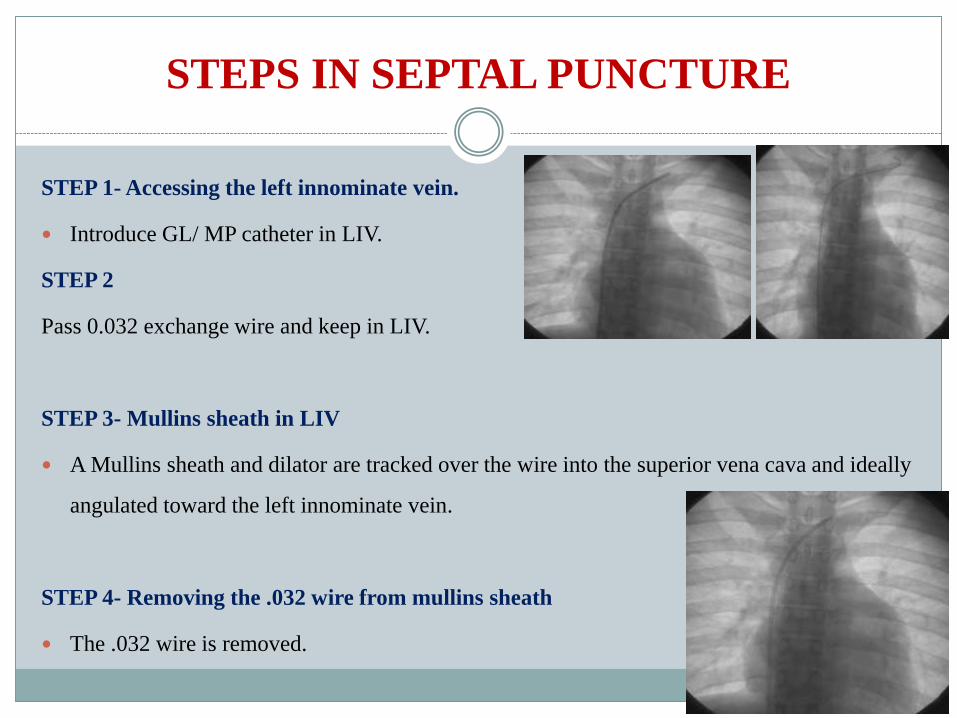
STEP 1- Accessing the left innominate vein.
Introduce GL/ MP catheter in LIV.
STEP 2
Pass 0.032 exchange wire and keep in LIV.
STEP 3- Mullins sheath in LIV
A Mullins sheath and dilator are tracked over the wire into the superior vena cava and ideally
angulated toward the left innominate vein.
STEP 4- Removing the .032 wire from mullins sheath
The .032 wire is removed.
STEP 5-Introduction of Brockenbrough needle.
Check the needle -sheath assembly. Length of the needle in relation to the
dilator is checked. When fully inserted, needle protrude beyond 3-5 mm
from tip of dilator.
Connect the three way with syringe with saline.
It is better to flush the saline while the needle is being tracked through the
mullins.
Allow free movement of needle.
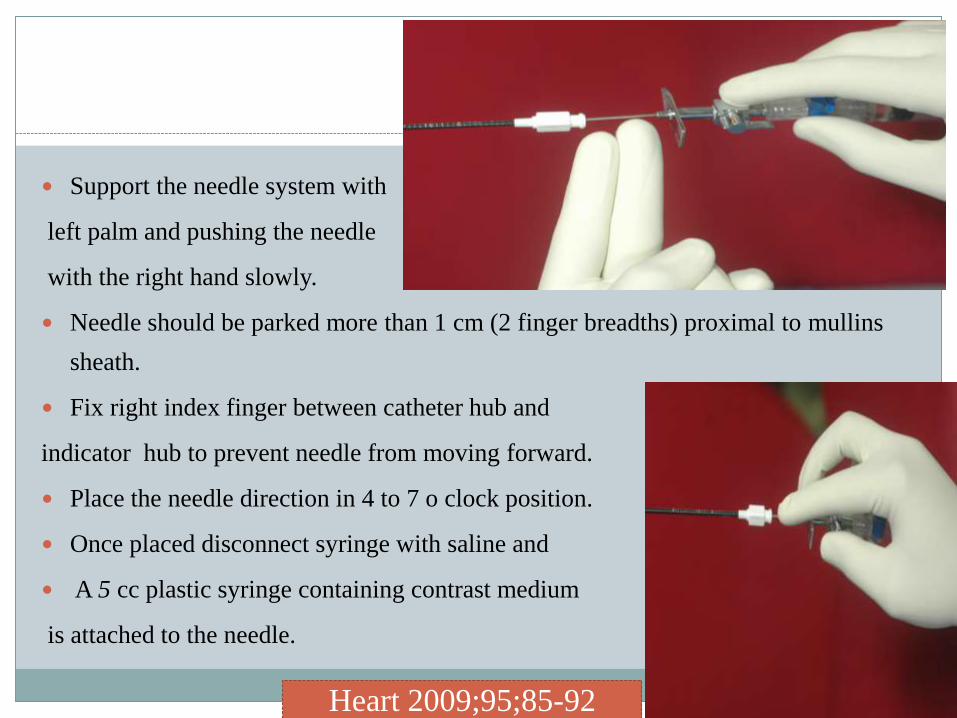
Support the needle system with
left palm and pushing the needle
with the right hand slowly.
Needle should be parked more than 1 cm (2 finger breadths) proximal to mullins
sheath.
Fix right index finger between catheter hub and
indicator hub to prevent needle from moving forward.
Place the needle direction in 4 to 7 o clock position.
Once placed disconnect syringe with saline and
A 5 cc plastic syringe containing contrast medium
is attached to the needle.
Heart 2009;95;85-92
STEP 6 –Adjust the pigtail in aortic sinus (lower most cusp-non-coronary cusp).
STEP 7- Descent to the FO region.
In LAO or AP view.
Keep the pointer of the needle in 5 o cock position.
Take care that the components should not rotate.
Falling from SVC to RA-first movement
Falls over the limbic edge of FO-second subtle movement. (sometimes not possible to
feel-see for RA ectopics)
Sometimes it can enter CS also.
Confirm in other views.
Connect the pressure transducer and look for pressure curve
variations.
For the puncture the needle should be held in the fingers of the
right hand, with the left hand holding the sheath and dilator
controlling movement of the whole assembly.
Under frontal fluoroscopic view, the needle-fitted transseptal
catheter with its direction indicator pointing about 4 o’clock is
slowly withdrawn downward (caudally) from the superior vena
cava.
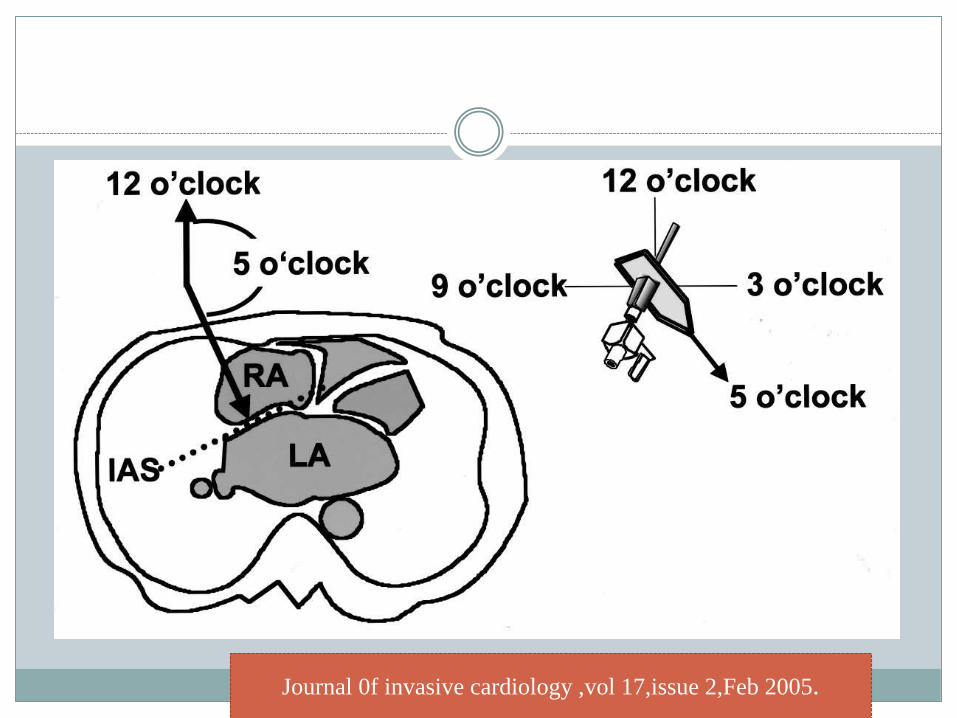
Journal 0f invasive cardiology ,vol 17,issue 2,Feb 2005.
As it is withdrawn caudally to the primary target site, the
catheter tip is aligned with the “midline.”
In general, it is at 4 o’clock in relatively small left atrium
(< 4 cm), between 4 and 5 o’clock in a usual-size left
atrium, and at 6 o’clock in a large left atrium (> 5 cm).
Catheterization and Cardiovascular Diagnosis 26:275284 (1 992)
If atrial septum bulges towards the right atrium, especially in cases
of a giant left atrium, it is difficult to align the catheter tip with the
“midline” and perpendicular to the septum.
The catheter tip faces a strong resistance at 4 o’clock when it
touches the bulged septal surface. As the needle is being rotated
clockwise, the catheter needle will give way suddenly (ceiling of the
room is 12 o’clock orientation, floor is 6 o’clock orientation)
In effect, the needle tip flips over the crest of the bulge and towards the right side of the
patient pointing to 9 o’clock.
To prevent this, the catheter should be pressed slightly against the septum as the needle is
being rotated clockwise to 6 to 7 o’clock.
At the same time, a slight counterclockwise twist is applied to the catheter with the left hand
to counter any excessive clockwise rotation of the needle. If the crest of the bulge happens to
be at the “midline,” it is not possible to make a puncture on the line. In this case the puncture
site is settled in the region slightly lateral to “the midline.”
STAINING OF SEPTUM
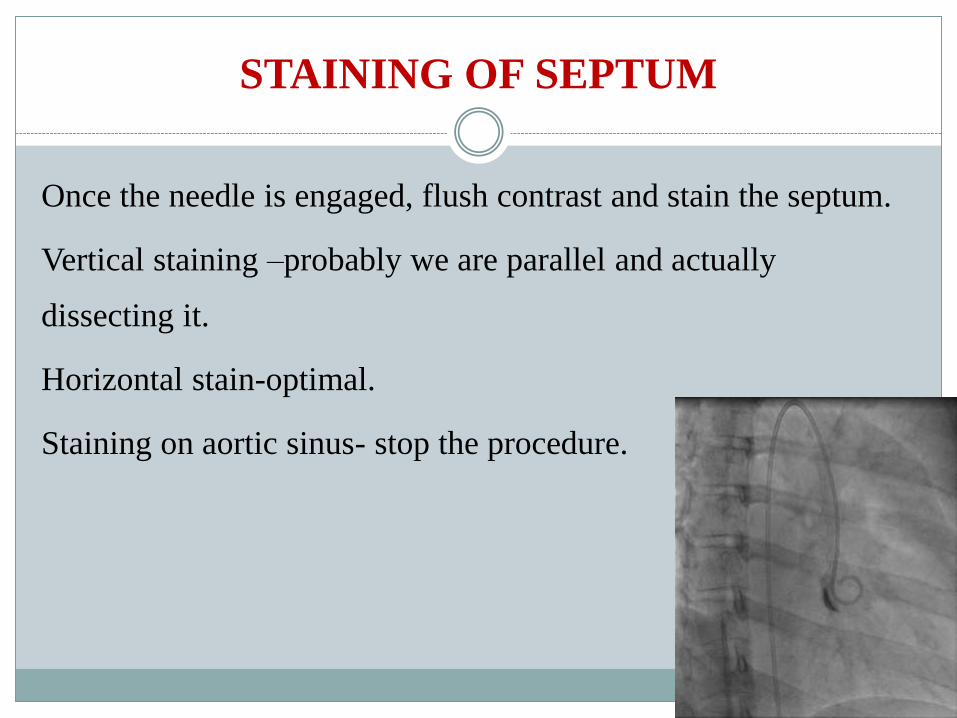
Once the needle is engaged, flush contrast and stain the septum.
Vertical staining –probably we are parallel and actually
dissecting it.
Horizontal stain-optimal.
Staining on aortic sinus- stop the procedure.
If no blood is aspirated, the needle either has dissected the high septum or is caught
in the thickened septum. Staining of the septum with injection of a small amount of
contrast medium easily distinguishes the two. When the high septum is dissected, it
is stained in more vertical fashion .
In this situation the needle is withdrawn and septal puncture is made at a lower
(caudal) site. When the needle is caught in the thick septum, the stain takes more
horizontal orientation . In this case the catheter/ needle is carefully forced across
the septum as described below or the puncture is attempted at another site.
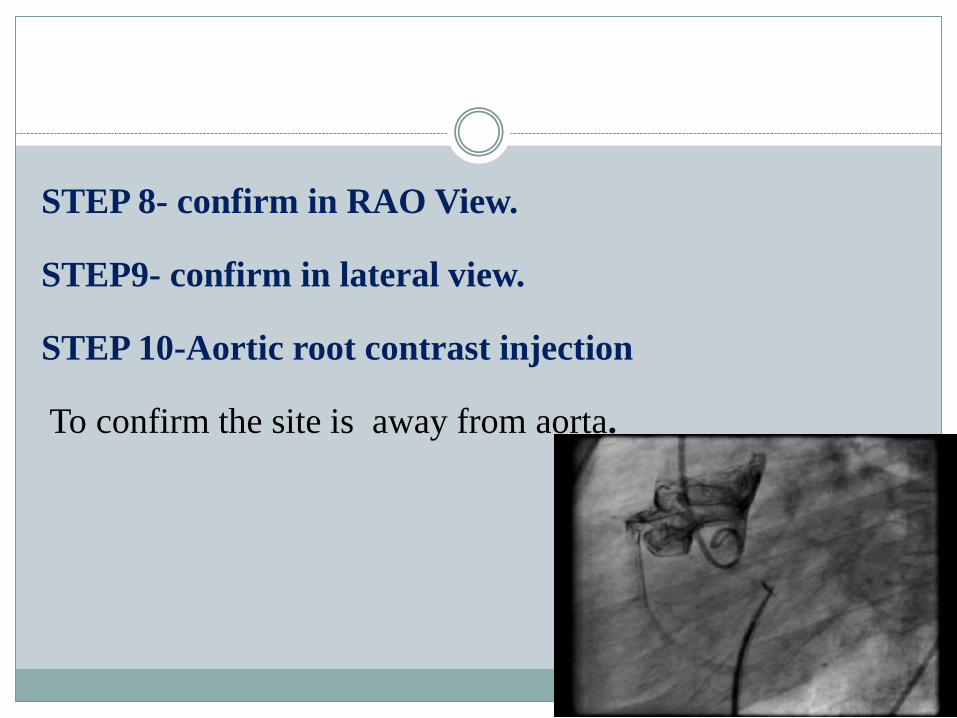
STEP 8- confirm in RAO View.
STEP9- confirm in lateral view.
STEP 10-Aortic root contrast injection
To confirm the site is away from aorta.
STEP 11- PUNCTURE- FINALLY?
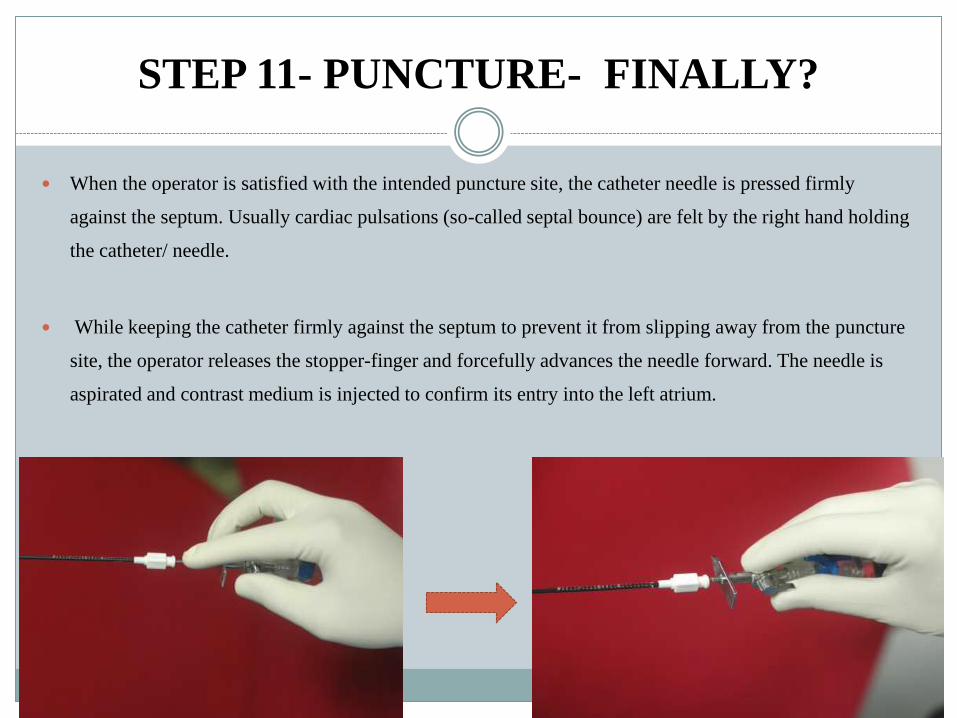
When the operator is satisfied with the intended puncture site, the catheter needle is pressed firmly
against the septum. Usually cardiac pulsations (so-called septal bounce) are felt by the right hand holding
the catheter/ needle.
While keeping the catheter firmly against the septum to prevent it from slipping away from the puncture
site, the operator releases the stopper-finger and forcefully advances the needle forward. The needle is
aspirated and contrast medium is injected to confirm its entry into the left atrium.

TO CONFIRM IN LA
-presssure waveform
-blood colour.
-left main bronchus in LAO forms the roof of LA.
-contrast injection in lateral view.
If there is no or little resistance, the catheter needle is advanced forward
about 2 cm into the left atrium.
During the process the operator must be prepared to withdraw the needle as soon
as the catheter enters the left atrium, lest the excessive forward momentum carries
the needle forward and perforate the left atrial wall causing cardiac tamponade.
Upon removing the needle after the catheter is placed in the left atrium, heparin,
100 units/kg body weight, should be given immediately through the catheter.
After baseline hemodynamic studies, including simultaneous measurement of
cardiac output, PTMC is performed.
There is much anatomical variation in the intra-atrial septum
and consequently the transseptal needle may not always fall
into the fossa ovalis. If patients have a large RA it is usually
necessary to reshape the needle to give it a greater curvature.
Many operators routinely do this for all transseptal punctures
and needles with a greater curvature than the standard are
available.
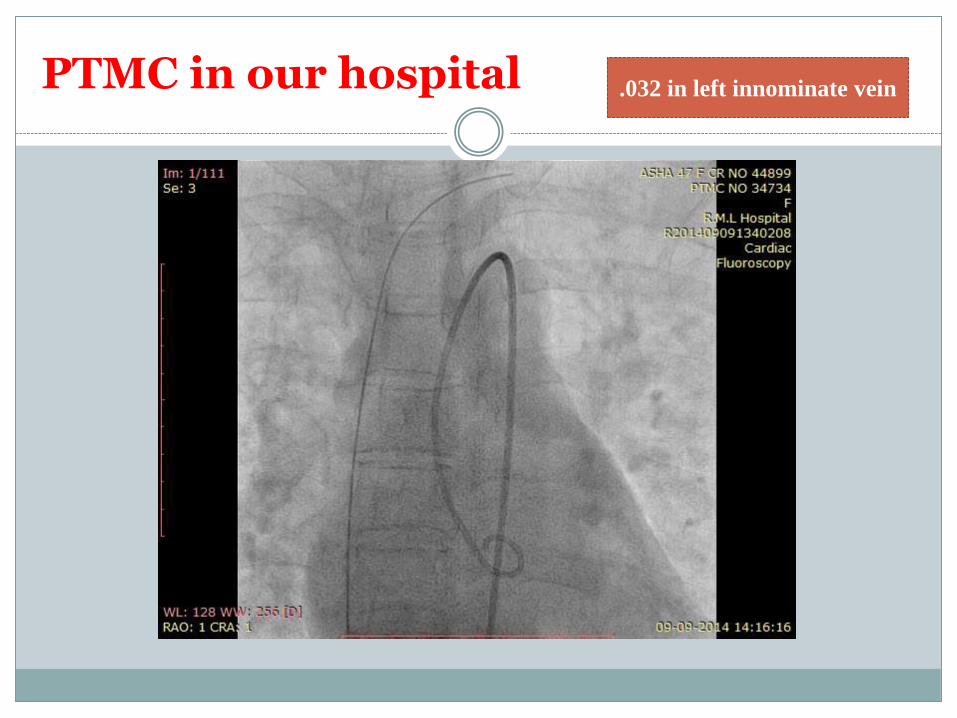
PTMC in our hospital .032 in left innominate vein
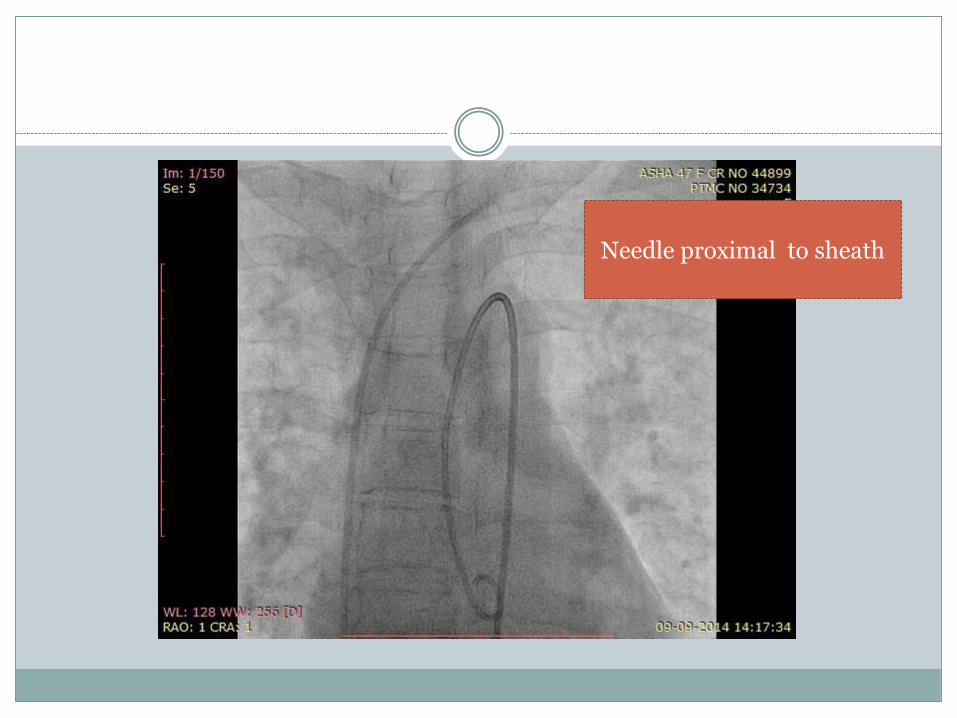
Needle proximal to sheath
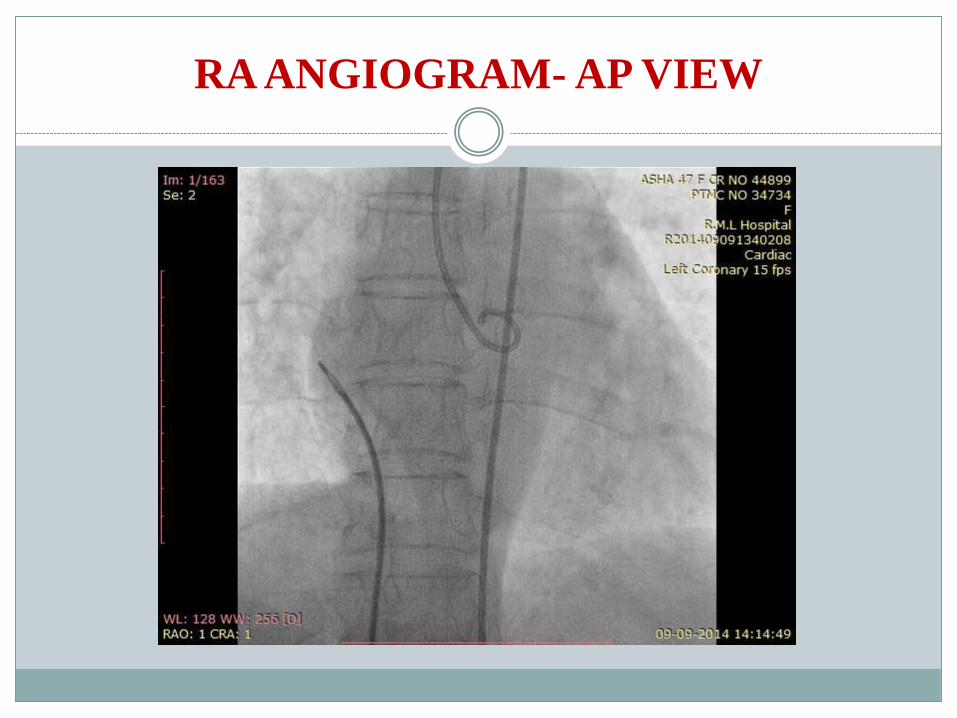
RA ANGIOGRAM- AP VIEW
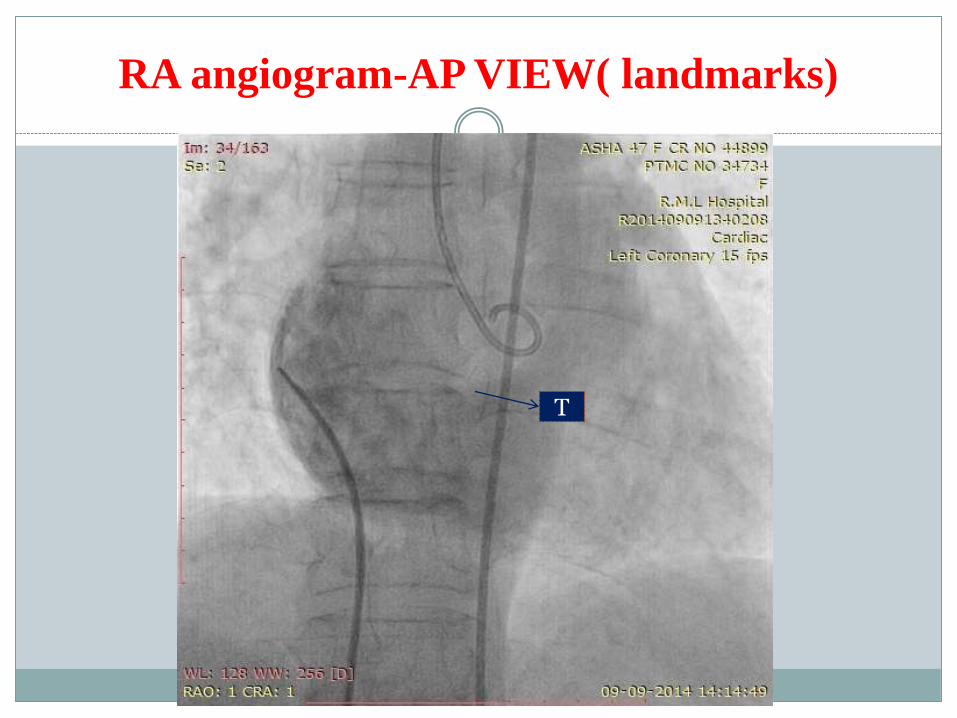
RA angiogram-AP VIEW( landmarks)
T
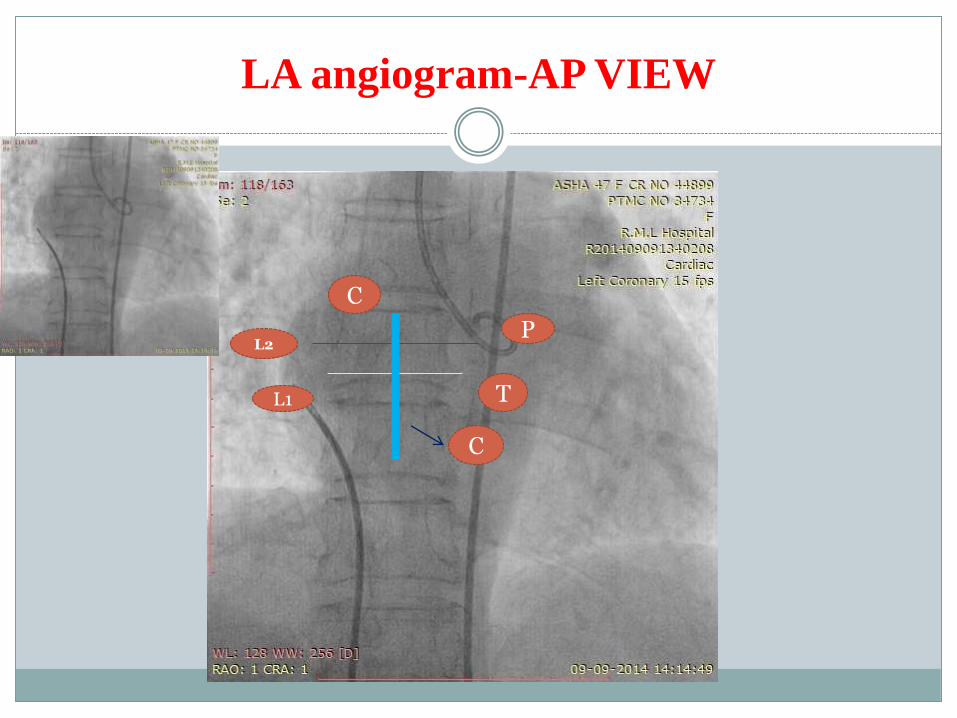
LA angiogram-AP VIEW
P
TL1
L2
C
C

LA ANGIOGRAM - AP VIEW
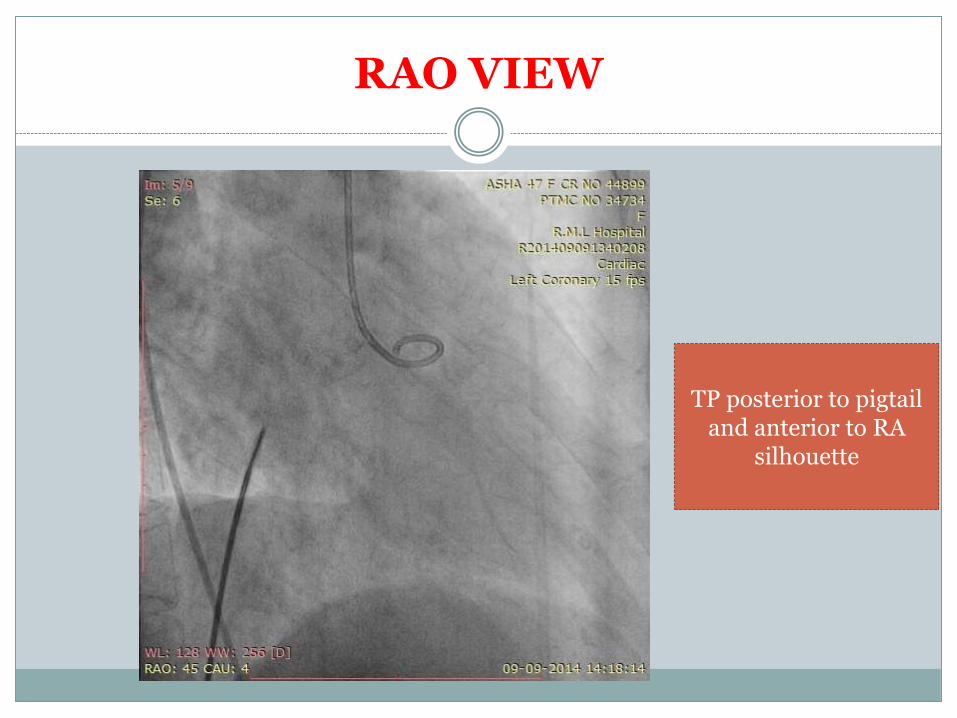
RAO VIEW
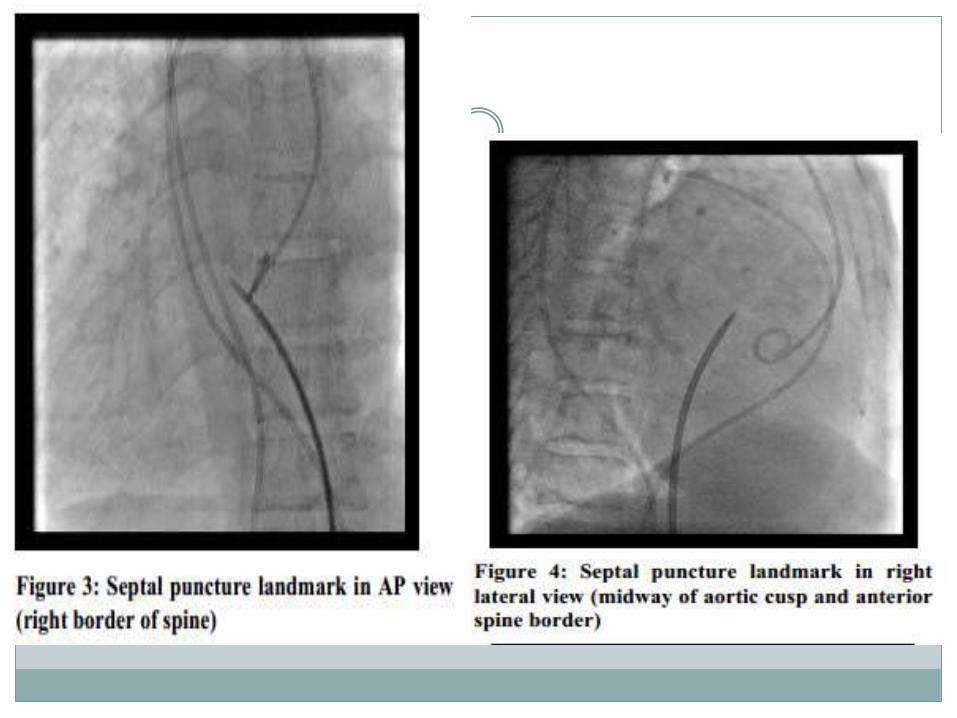
TP posterior to pigtail and anterior to RA
silhouette
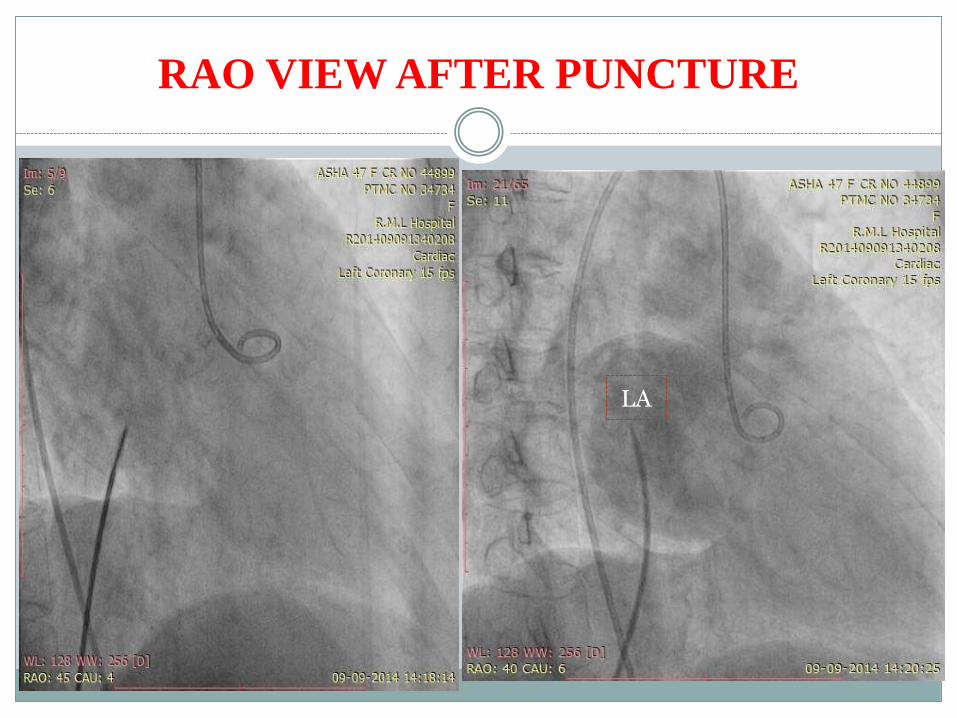
RAO VIEW AFTER PUNCTURE
LA
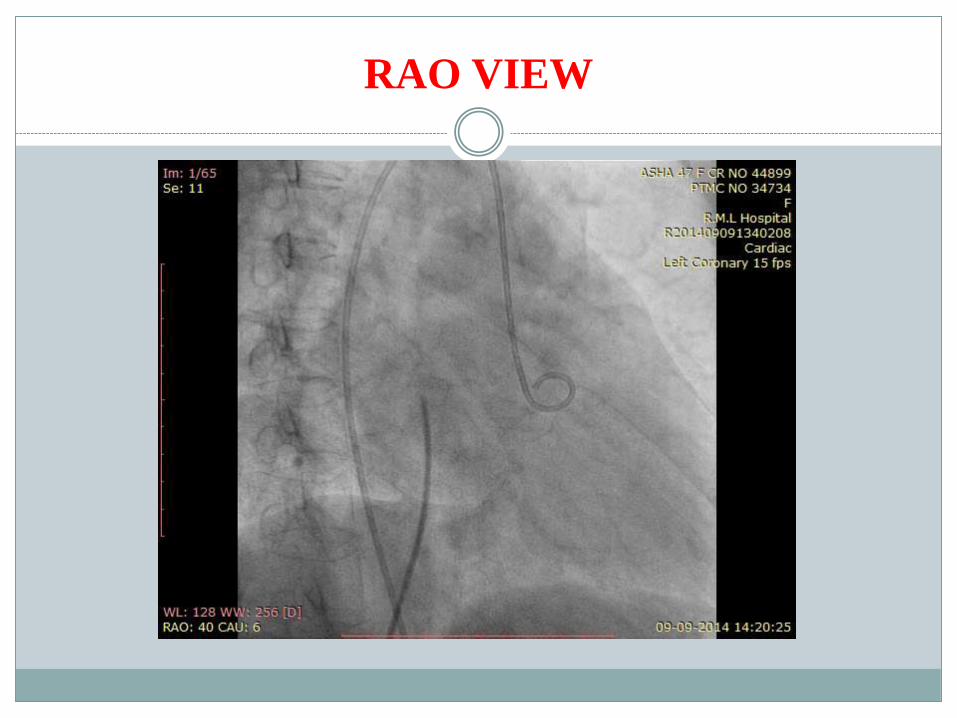
RAO VIEW

LATERAL VIEW
LA
The fossa ovalis in the lower third of the imaginary line connecting the pigtail
catheter (aortic valve) and the posterior wall of the left atrium .
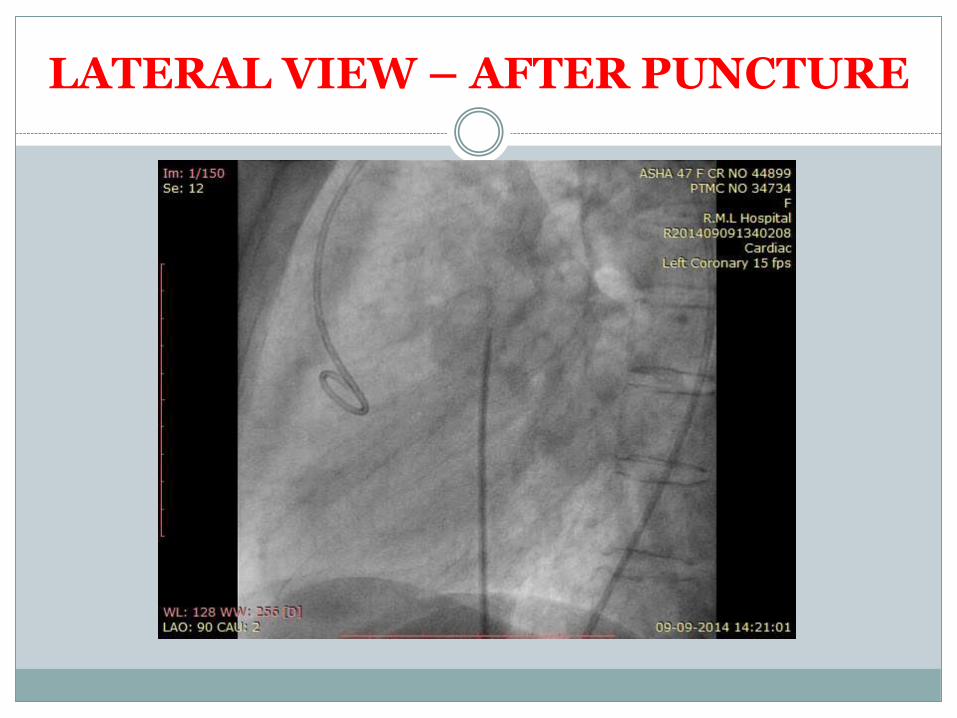
LATERAL VIEW – AFTER PUNCTURE

RAO VIEW LV ANGIO
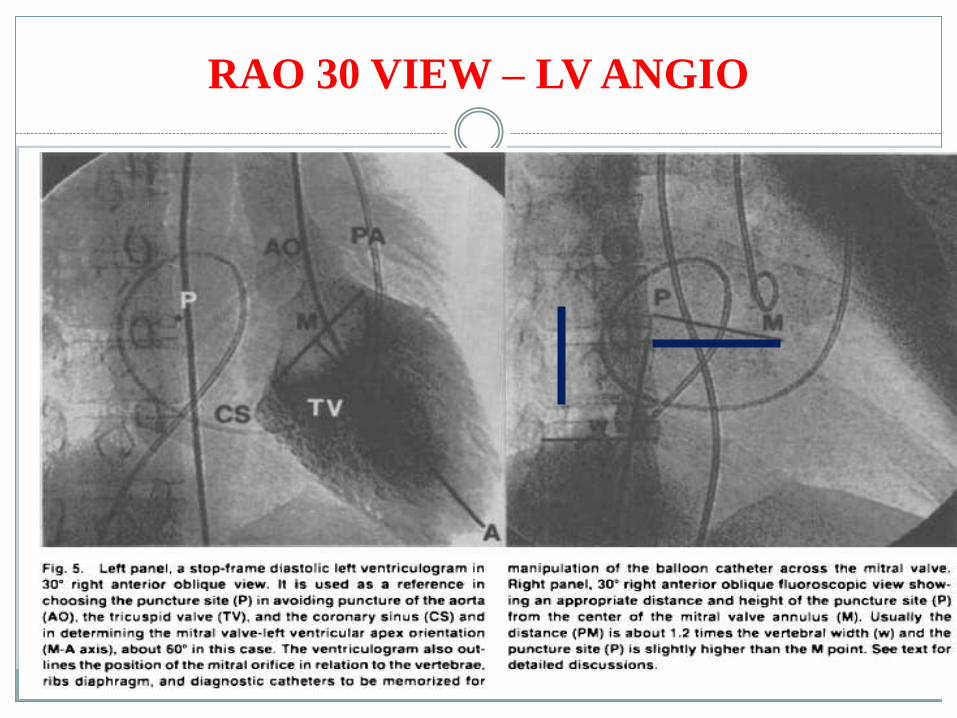
RAO 30 VIEW – LV ANGIO

RAO -45 VIEW- LV ANGIO
P
Best is RAO - 30
TRANSEPTAL PUNCTURE IN SPECIAL
CIRCUMSTANCES
Interrupted IVC
IVC filter
Unable to access left femoral vein
OPTIONS1. Jugular2. Hepatic3. Left femoral
Transhepatic approach to septal puncture
No other access available.
Single balloon technique if for BMV.
The puncture site was identified by fluoroscopy in the midaxillary
line, midway between the diaphragm and the lower margin of the
liver/Puncture in lateral and right side of liver.
Hepatic vein –IVC-RA-Septum (usually perpendicular and caudal
part of septum).
Distal end of needle 10 degree curve.
Mainly for pediatric interventions.
Circulation. 1995; 92: 1526-1530
8F to 14 F can be used via hepatic vein.
Can be used if femoral venous, jugular access not
possible.
Catheterization and Cardiovascular Diagnosis 39:204-206 (1 996)
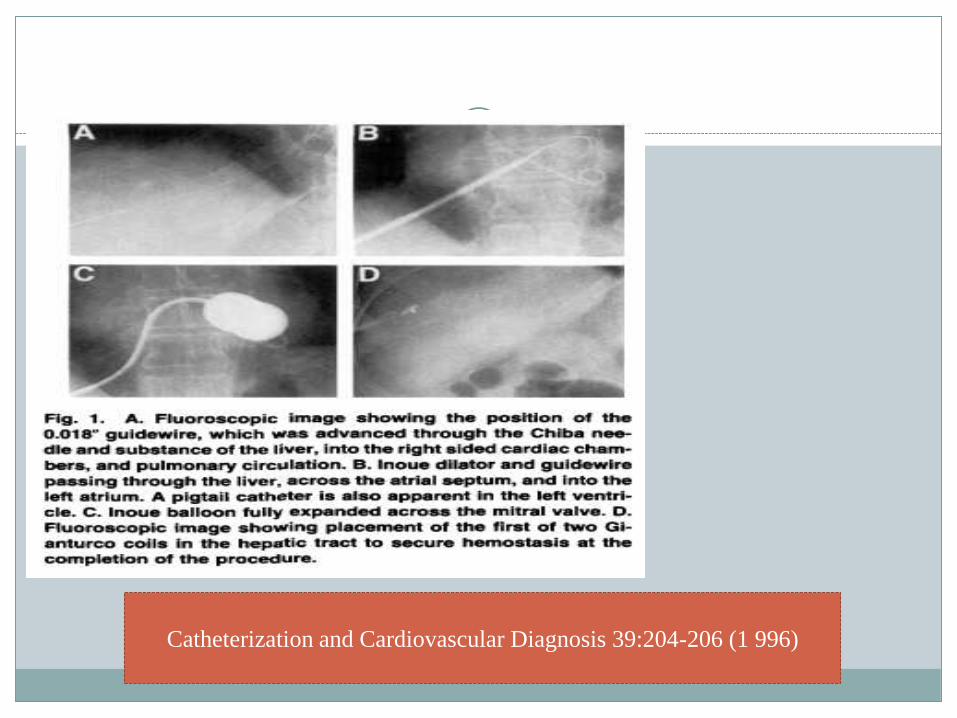
Catheterization and Cardiovascular Diagnosis 39:204-206 (1 996)
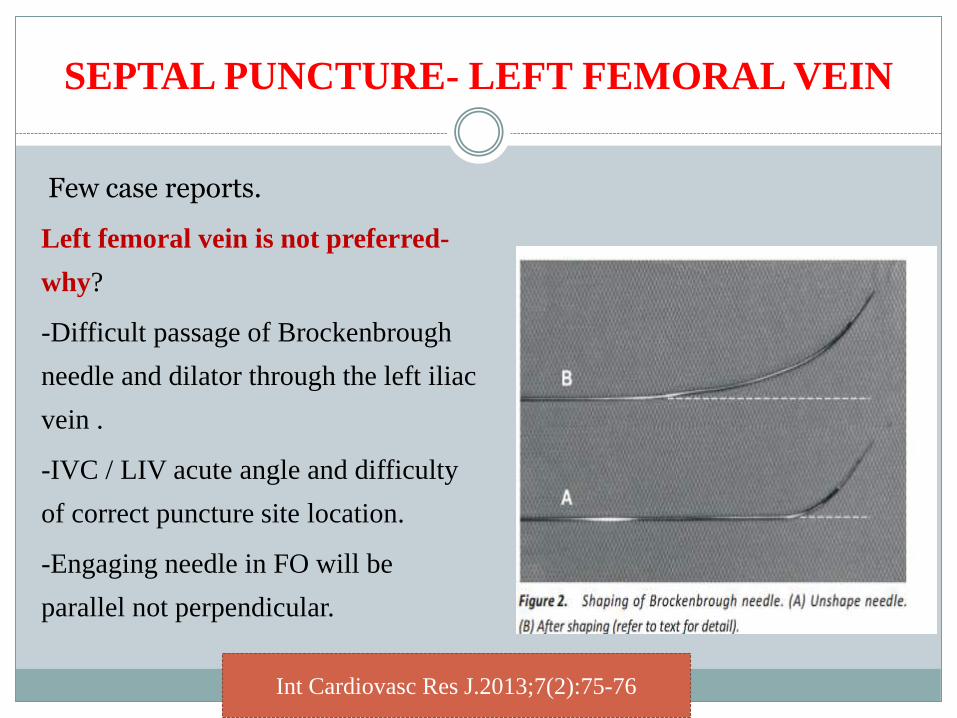
SEPTAL PUNCTURE- LEFT FEMORAL VEIN
Few case reports.
Left femoral vein is not preferred-
why?
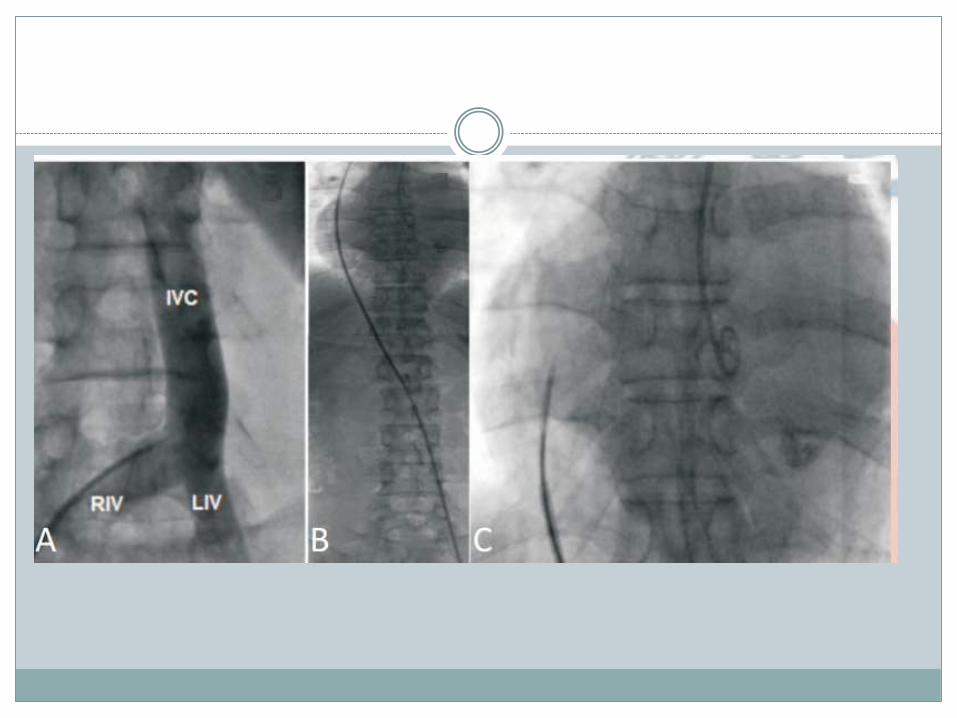
-Difficult passage of Brockenbrough
needle and dilator through the left iliac
vein .
-IVC / LIV acute angle and difficulty
of correct puncture site location.
-Engaging needle in FO will be
parallel not perpendicular.
Int Cardiovasc Res J.2013;7(2):75-76
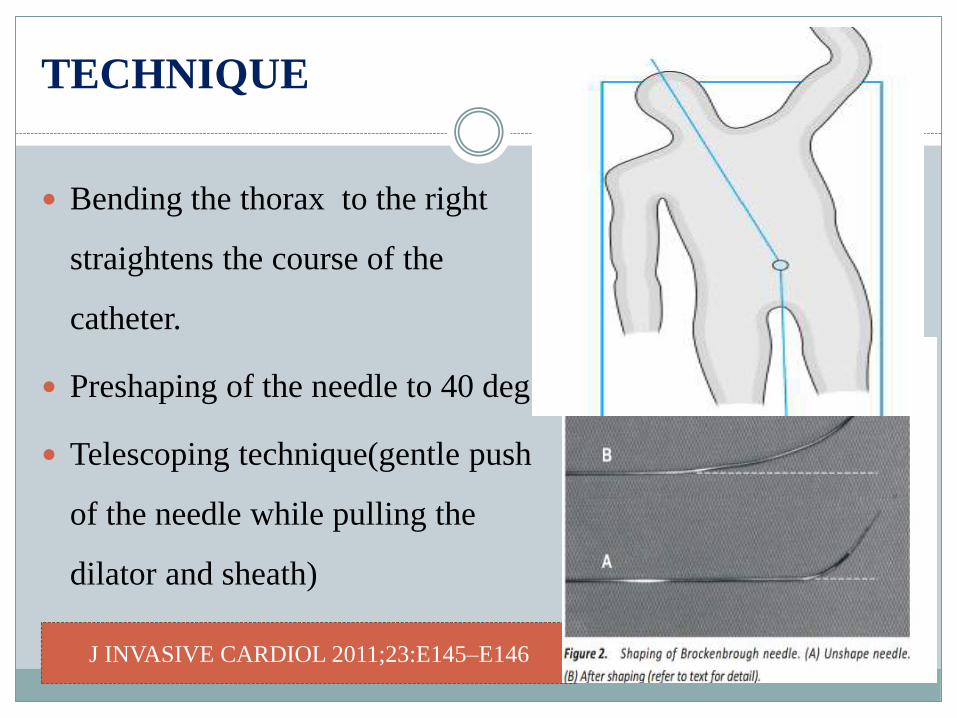
TECHNIQUE
Bending the thorax to the right
straightens the course of the
catheter.
Preshaping of the needle to 40 deg.
Telescoping technique(gentle push
of the needle while pulling the
dilator and sheath)
J INVASIVE CARDIOL 2011;23:E145–E146
TRANSJUGULAR APPROACH
Landmark is different.
RAO -45
Stop-frame of levophase left atrial image from PA angio is the
reference.
Puncture site is 2 cm below the roof of left atrial image and midway
between imaginary vertical line from pigtail and anterior border of
spine.
Better is high atrial septal puncture for facilitating balloon across the
LV.
CHAPTER 38- by Boonjong saejueng,Tansuphaswadikul.
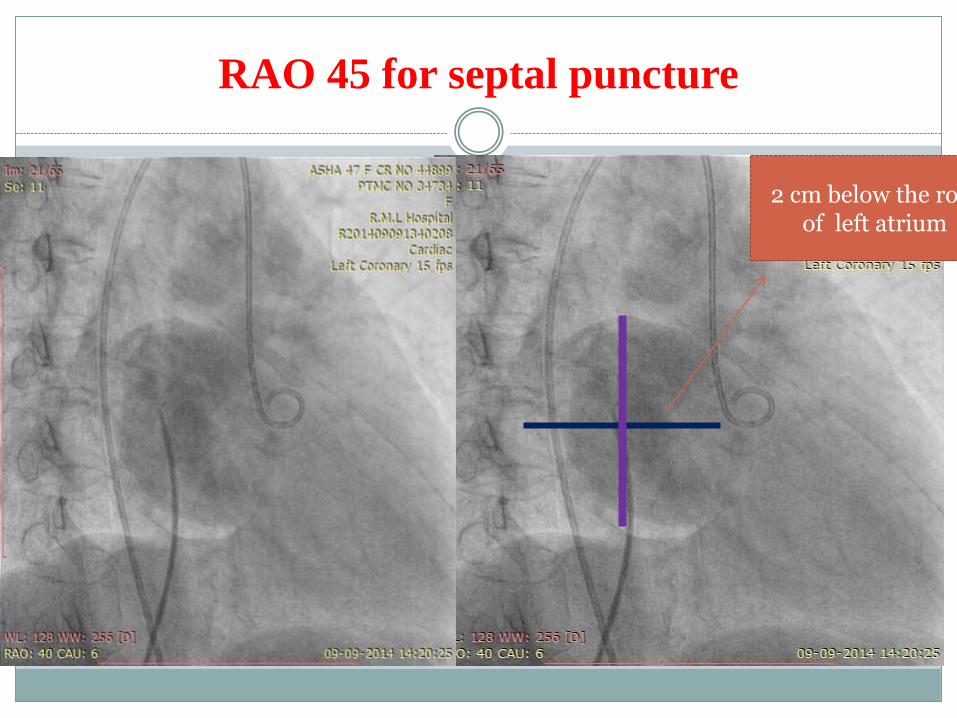
RAO 45 for septal puncture
2 cm below the roof of left atrium
The adult Brokenborough needle may be too long for transjugular PTMC hence, a
shorter needle would make transseptal puncture easier through the jugular
approach.
Endry’s pediatric transseptal puncture needle can be used.(30 cm in length) or
paediatric brockenbrough needle (51 cm ) can be used.
The direction indicator of the puncture needle must point in the 7-8 o’clock
position instead of the conventional 5 o’clock position; and after septal puncture,
the balloon must be rotated in a clockwise manner to facilitate entry into the LV,
unlike the conventional anticlockwise approach.
The bulge on the atrial septum creates a shelf in the lower end of the septum.
RIGHT IJV
The course from right IJV is a straight line making the impingement of
septum straight forward.
The curve at the distal end of brockenbrough neddle straightened to a very
slight 10 deg curve.
LEFT IJV
Increased curvature is needed to avoid oblique passage causing septal
dissection.
Needle kept pointing 7-8 o clock.
J Am Coll Cardiol Intv. 2012;5(2):243-244.

TEE GUIDED SEPTAL PUNCTURE
Always an guide for TP along with fluoroscopy.
(TEE) is more useful, particularly when visualizing a specific area of the fossa
ovalis to be punctured.(with 3D).
Superior/ inferior localization is seen best in the bicaval view (90°), and
anterior/posterior localization is seen best in the 4-chamber view (0°).
Tenting of the fossa ovalis (the thin septum) by the TS catheter tip indicates
correct positioning, even if the needle or catheter cannot be visualized.
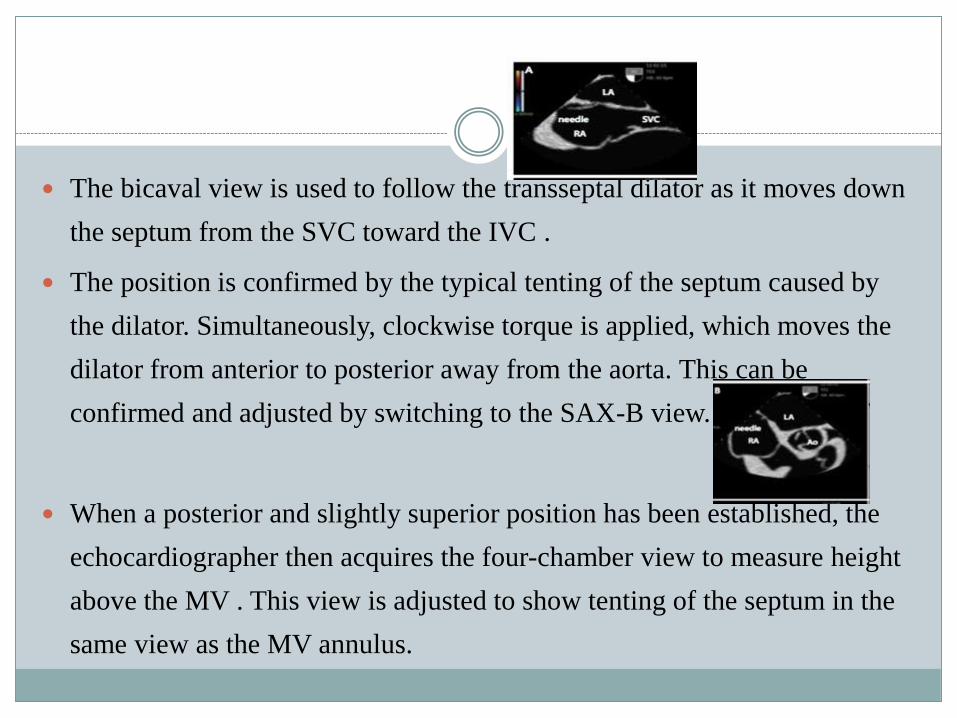
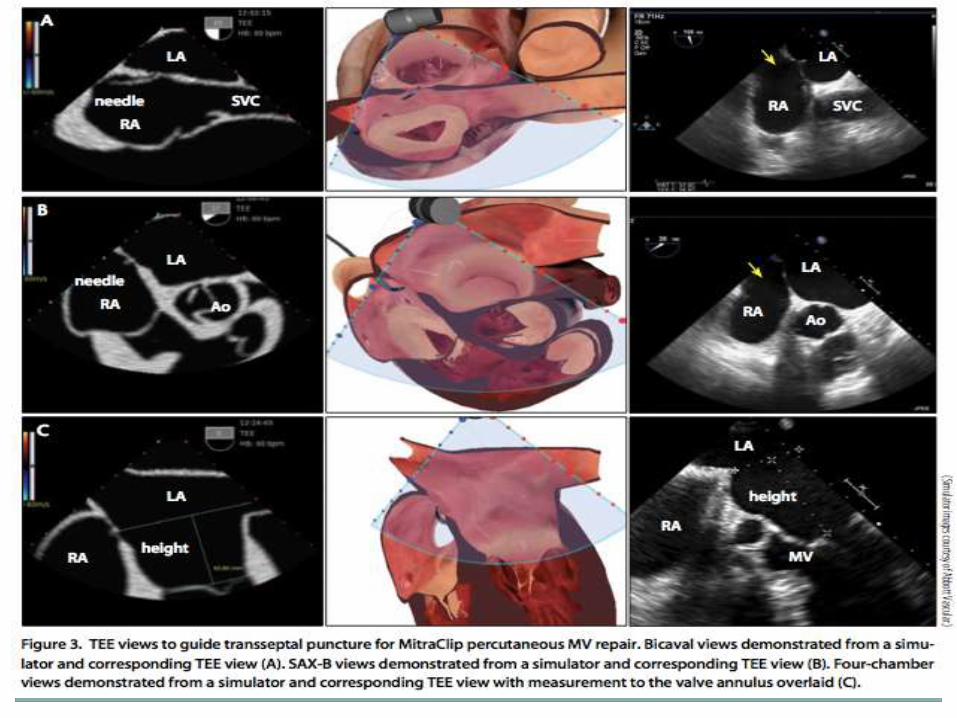
The bicaval view is used to follow the transseptal dilator as it moves down
the septum from the SVC toward the IVC .
The position is confirmed by the typical tenting of the septum caused by
the dilator. Simultaneously, clockwise torque is applied, which moves the
dilator from anterior to posterior away from the aorta. This can be
confirmed and adjusted by switching to the SAX-B view.
When a posterior and slightly superior position has been established, the
echocardiographer then acquires the four-chamber view to measure height
above the MV . This view is adjusted to show tenting of the septum in the
same view as the MV annulus.
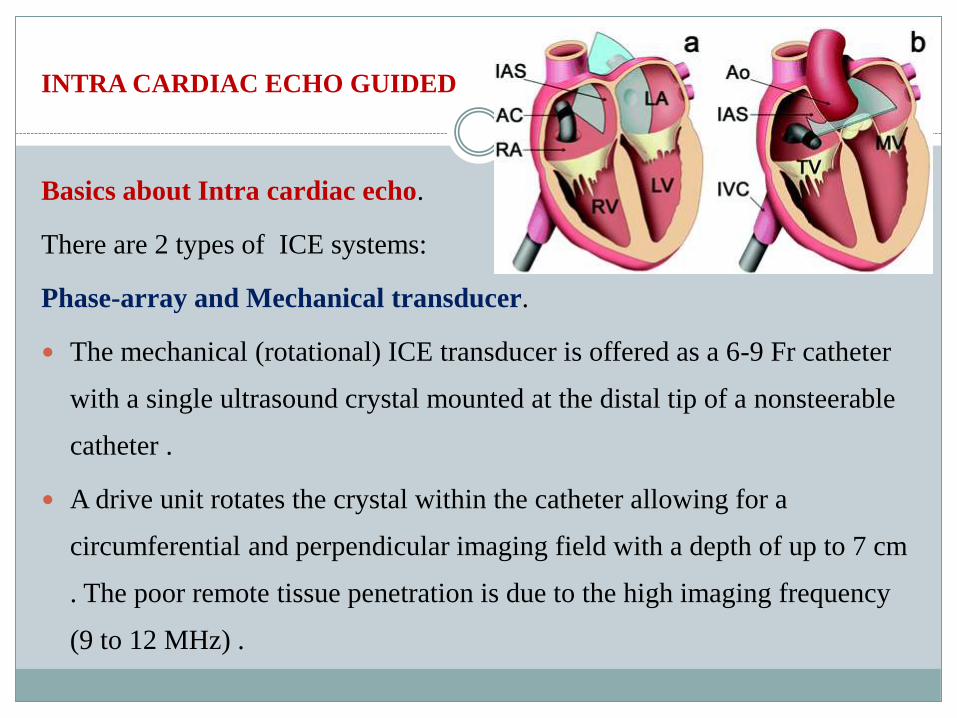
INTRA CARDIAC ECHO GUIDED
Basics about Intra cardiac echo.
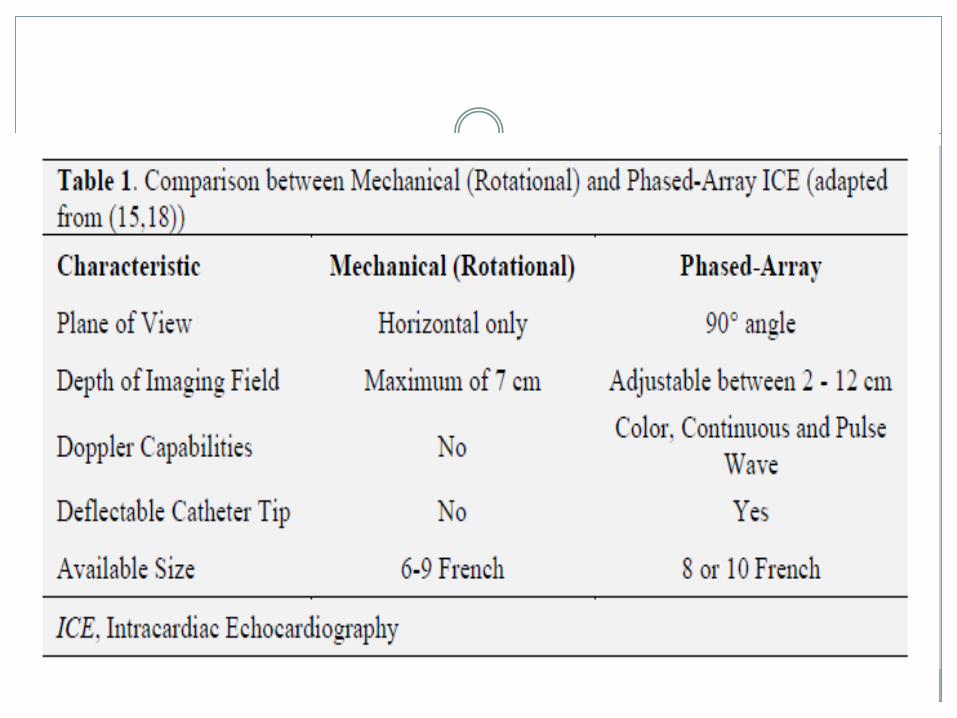
There are 2 types of ICE systems:
Phase-array and Mechanical transducer.
The mechanical (rotational) ICE transducer is offered as a 6-9 Fr catheter
with a single ultrasound crystal mounted at the distal tip of a nonsteerable
catheter .
A drive unit rotates the crystal within the catheter allowing for a
circumferential and perpendicular imaging field with a depth of up to 7 cm
. The poor remote tissue penetration is due to the high imaging frequency
(9 to 12 MHz) .
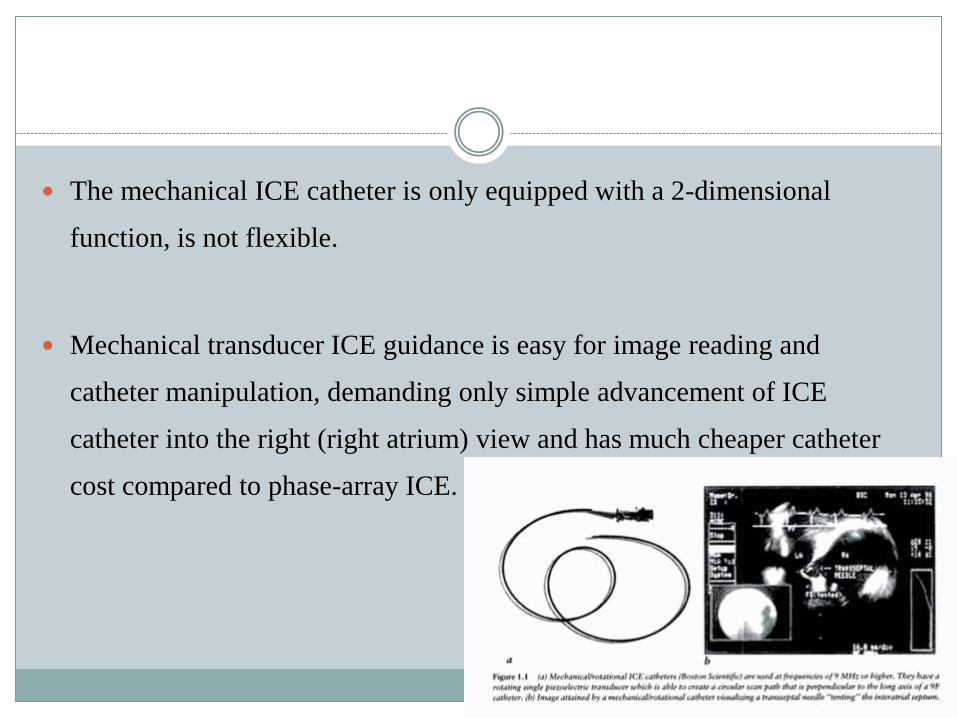
The mechanical ICE catheter is only equipped with a 2-dimensional
function, is not flexible.
Mechanical transducer ICE guidance is easy for image reading and
catheter manipulation, demanding only simple advancement of ICE
catheter into the right (right atrium) view and has much cheaper catheter
cost compared to phase-array ICE.
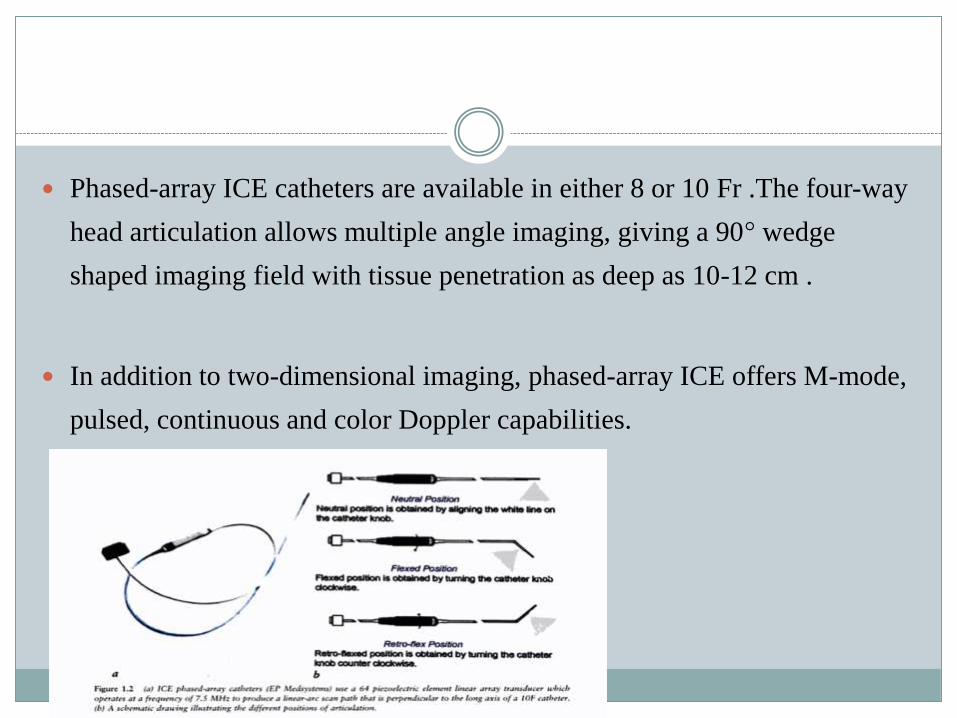
Phased-array ICE catheters are available in either 8 or 10 Fr .The four-way
head articulation allows multiple angle imaging, giving a 90° wedge
shaped imaging field with tissue penetration as deep as 10-12 cm .
In addition to two-dimensional imaging, phased-array ICE offers M-mode,
pulsed, continuous and color Doppler capabilities.
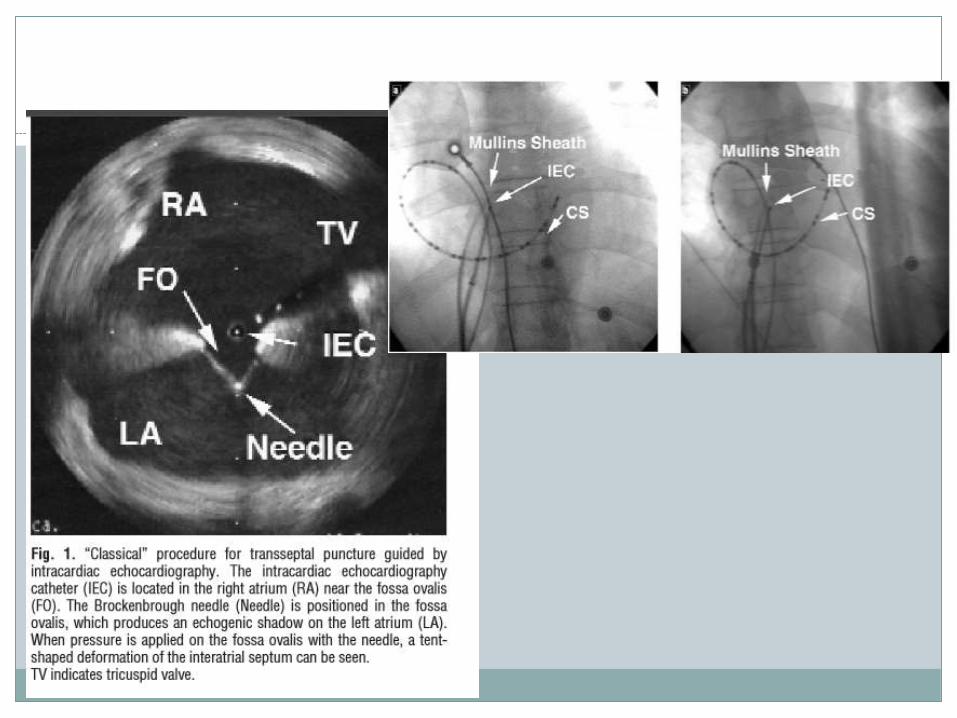
Intracardiac echocardiography (ICE) can help better delineate the border of the
septum, clearly visualize the relative positions of the catheter, needle, and septum,
and confirm entry into the left atrium.
It also eliminates the need for contrast medium exposure, and spares unnecessary
multiple or false punctures.
ICE-guided transseptal puncture preserves the advantages of transesophageal
echocardiography guidance while eliminating the need for intravenous sedation or
prolonged oral scope intubation, and improves patient comfort.
J Chin Med Assoc 2010;73(9):
INTRA CARDIAC ECHO GUIDED.
The right femoral vein was cannulated with an 11 F introducer sheath and a 60-cm sheath
with a 55° angle was advanced through it.
A 9 F intracardiac echocardiography catheter (EP Technologies, Boston Scientific Corp; San
Jose, California) was introduced via the sheath from left femoral vein, which was withdrawn
by clockwise rotation until it was in contact with the fossa ovalis.
For transseptal catheterization, the Brockenbrough needle was placed within a dilator
introduced into an 8 F sheath (Mullins) from right femoral vein.
Rev Esp Cardiol. 2004;57:359-62. - Vol. 57 Num.04
The ICE catheter is advanced from the femoral vein to the
‘‘home’’ view in the body of the RA facing the tricuspid valve.
From this position, a posterior tilt of the transducer and a
clockwise rotation of the catheter brings the IAS and FO into
view in the near field with the body of the LA visible in the far
field.
The Journal of Innovations in Cardiac Rhythm Management, October 2013
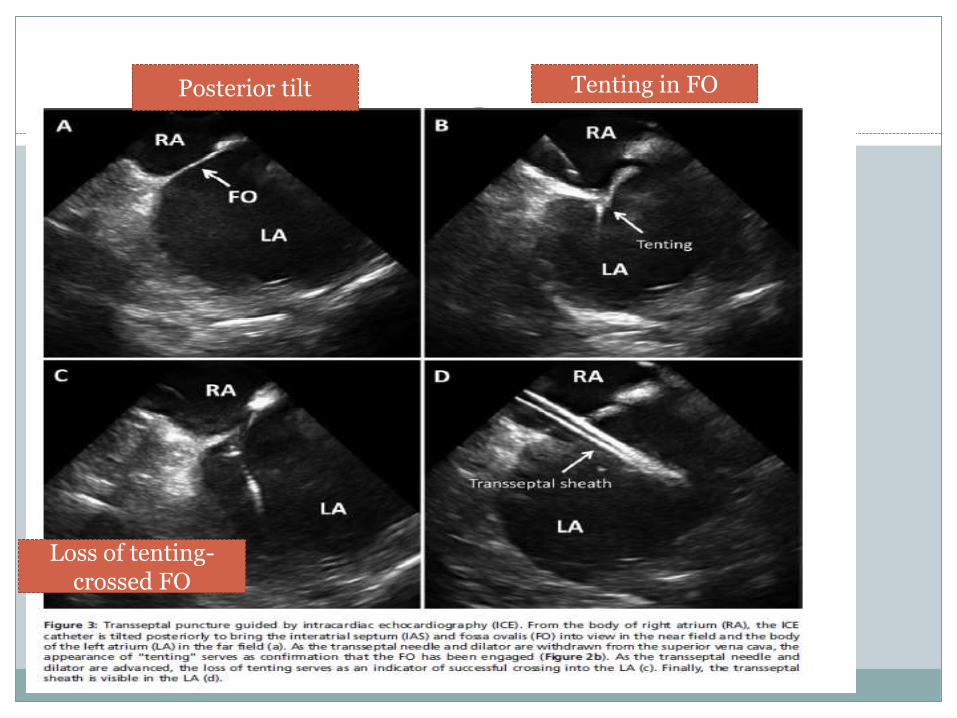
Posterior tilt Tenting in FO
Loss of tenting-crossed FO
Newer Methods for Atrial Septal Puncture
RF ASSISTED PUNCTURE
In an attempt to improve the TS technique, a new system that uses
radiofrequency (RF) energy has been used to puncture the septum
(Radiofrequency Transseptal System, Baylis Medical, Montreal, Canada).
Instead of a needle, an RF catheter is introduced into the dilator sheath
assembly.
This catheter delivers 5 W energy for 2 to 5 s and can perforate
the atrial septum after 1 to 4 pulses.
Added advantage in thick, scarred, calcified, or patched atrial
septa, where excess force could result in unsuccessful puncture
or in perforation of the LA free wall secondary to catheter
momentum.
RF ABLATIVE NEEDLES
NRG RF Transseptal needle (Baylis Inc).
Predictably crosses all types of septa
Can cross an aneurysmal septum in a controlled manner
Can effectively cross a fibrotic septum
Compatible with standard sheaths / dilators
Proximal Gauge: 18 Ga
Distal Gauge: 21 Ga
The curves of the NRG™ RF
Transseptal Needles mimic those of conventional needles
Inner lumen for fluid injection and pressure waveforms
Electrically insulated.
INFRA RED ASSISTED TP
CardioOptics (Boulder, Colorado) manufactures a catheter that emits infrared light
and can image through flowing blood in real time.
In infrared imaging, an infrared wavelength in low-absorptive wavelength regions
provides direct images of structures, through flowing blood to about two
centimeters in an 80 deg field of view, much like an endoscope. It permits the fossa
ovalis or septal defect to be seen directly at distances ranging ' from 0.2 — 2 cm.
This catheter may be useful in TS catheterization, allowing direct visualization of
the fossa ovalis. Animal testing has been completed, and Phase I human trials are
pending.J Am Coll Cardiol 2008;51:2116–22
GUIDEWIRE TECHNIQUE
0.014 inch PTCA guidewire is usefeul
Before the procedure, try to move the guidewire through the sharp edge of the
needle two or three times, and obtained confirmation of safety.
Successful left atrial puncture can be confirmed by simply advancing the
guidewire. If the tip of the needle is not in the left atrium, advancing the guidewire
is impossible.
Second, the needle-dilator combination is safely advanced into the left atrium over
the guidewire. For the Inoue balloon technique, since the target atrial septum of the
large left atrium may be thick, it would be very difficult to advance the Mullins
dilator alone into the left atrium over the needle.
JIVC vol.17,issue 2,feb 2008
SafeSept Transseptal guidewire
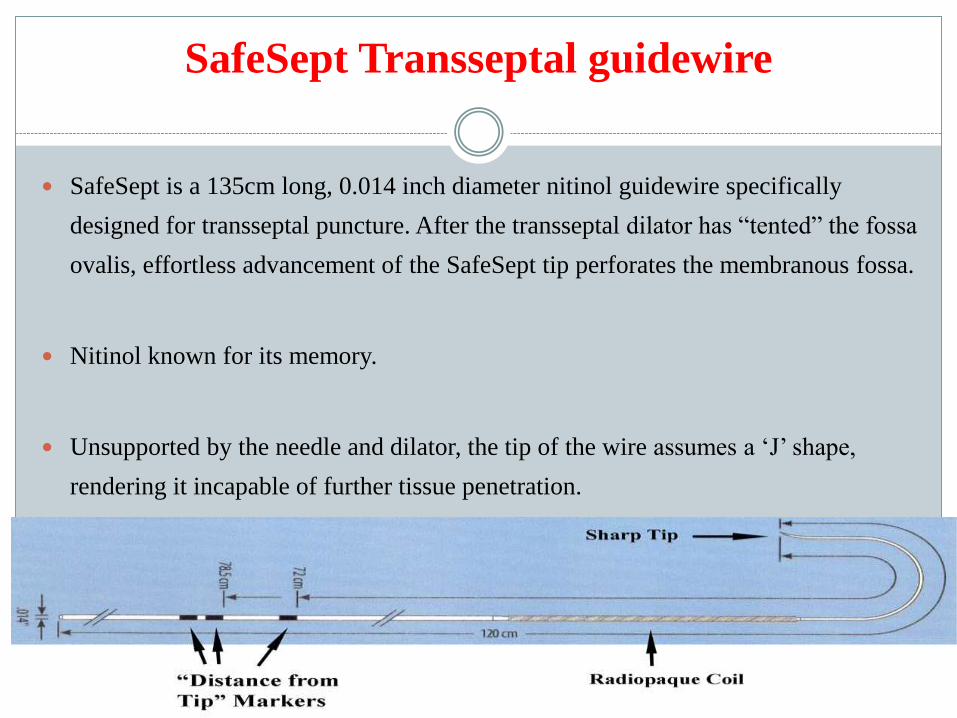
SafeSept is a 135cm long, 0.014 inch diameter nitinol guidewire specifically
designed for transseptal puncture. After the transseptal dilator has “tented” the fossa
ovalis, effortless advancement of the SafeSept tip perforates the membranous fossa.
Nitinol known for its memory.
Unsupported by the needle and dilator, the tip of the wire assumes a ‘J’ shape,
rendering it incapable of further tissue penetration.
A TSGW (SafeSeptTM, Pressure Products Inc., San Pedro,
CA, USA) was then inserted into the Brockenbrough needle
and advanced to the unexposed tip.
The position of the sheath assembly was examined in the right
anterior oblique projection to ensure it lies centrally on the
interatrial septum posterior to the coronary sinus catheter and
anterior to the posterior heart border.
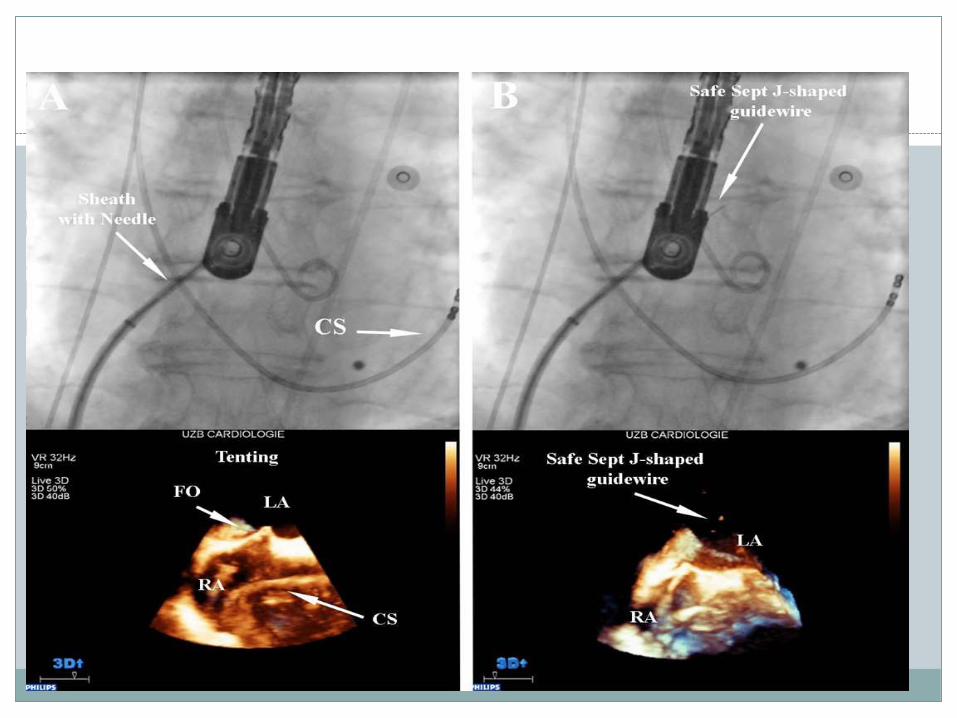
If the wire is pushed in an incorrect position outside the fossa
ovalis, crumpling and resistance is encountered, and an
attempt using a different orientation is required, thus acting as
a probing wire.
If passage through the septum into the LA is achieved, the
guidewire passes effortlessly without resistance in its pre-
formed ‘J’ shape through the left atrial chamber.
Europace Advance Access published August 8, 2011

EXCIMER LASER
Another new technology that also may improve the safety of
TS puncture is the excimer laser catheter (0.9-mm Clirpath X-
80, Spectranetics, Colorado Springs, Colorado).
The laser catheter is inserted via a modified Mullins sheath
and dilator (inner lumen compatible with a0.038-inch wire)
and can puncture the septum after a brief (2 to 5 s) application
of laser energy.
The laser catheter requires less force (10-fold) to cross the
septum compared with the Brockenbrough needle, and can
then be used as a rail over which the Mullins sheath and dilator
can be advanced.
Currently, only data from animal studies are available,
although the technology seems promising and can be used “off
the shelf”.

JUGULAR VEIN APPROACH-NEWER
The LA-Crosse system (St. Jude Medical, St. Paul, Minnesota) is
composed of 3 parts: a stabilizer sheath, a guide catheter, and a flexible
puncture screw.
The stabilizer sheath is placed from the right internal jugular vein such that
the distal end lies in the inferior vena cava and the side opening faces the
mid RA. A guide catheter is advanced through the stabilizer sheath and out
the side opening until its distal end is in contact with the fossa ovalis
J Am Coll Cardiol 2008;51:2116–22
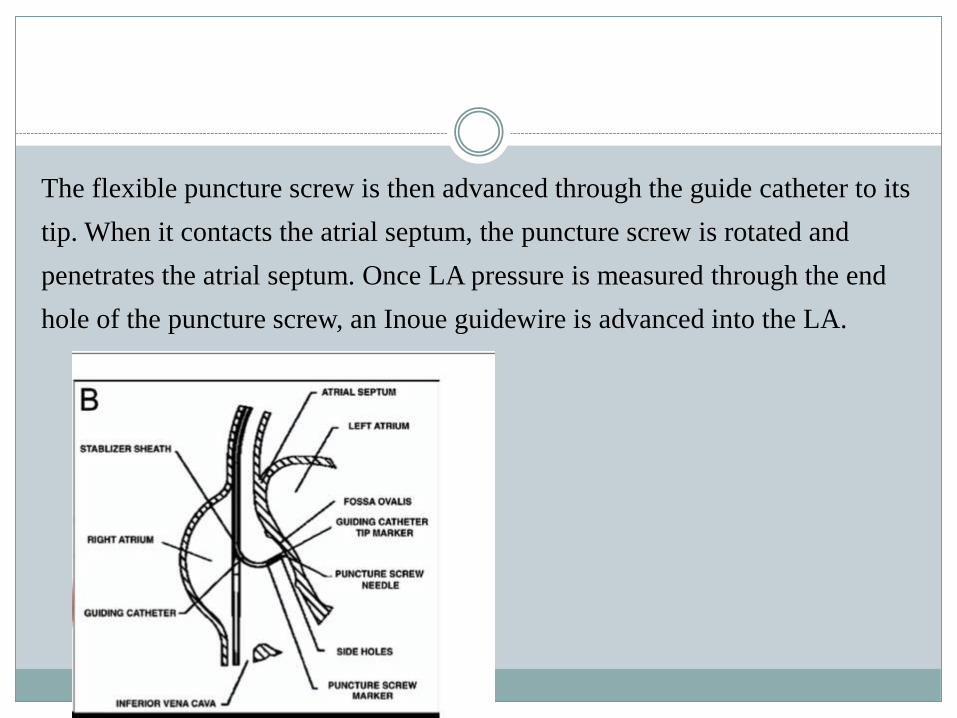
The flexible puncture screw is then advanced through the guide catheter to its
tip. When it contacts the atrial septum, the puncture screw is rotated and
penetrates the atrial septum. Once LA pressure is measured through the end
hole of the puncture screw, an Inoue guidewire is advanced into the LA.
This system has been 100% successful in animal models
guided by fluoroscopy, and can be used to perform multiple
punctures in selective portions of the atrial septum.
Human evaluation is pending.
TRANSEPTAL PUNCTURE IN ABNORMAL
HEARTS.
Dextrocardia
Dextrocardia represents a significant challenge to transseptal puncture.
Distorted cardiac anatomy provides technical difficulties during fluoroscopy-
guided transcatheter procedures.
However, cases have been reported of successful access to the right atrium
(RA) using a mirror image technique with successful outcomes.

PTMC IN DEXTROCARDIA WITH SI
The radiographic images were acquired in the inverted position
and were used as fluoroscopic guidance for the septal puncture, as
previously described by Nallet et al .
Transseptal catheterization was performed from the left groin to
reduce the puncture needle angulation at the confluence of the iliac
veins to the left-sided inferior vena cava.
Cathet Cardiovasc Diagn 1996; 39: 85– 88
Fluoroscopic imaging can be inverted .This created a pseudo-AP view when the
C-arm was in the AP position and a pseudo-right anterior oblique (RAO)
30º view when the C-arm was in left anterior oblique (LAO) 30º view.
Septal descent was performed in the pseudo-AP view with the needle kept in the
7 o’clock position. After achieving the standard fluoroscopic
positions in pseudo-RAO, pseudo-AP and lateral views,
the septum, along with the interatrial septal aneurysm, were
stained with contrast injection into the septum.
J Invasive Cardiol 2008; 20(1): E33-E35.
IN RIGHT SIDED ARCH
The usual technique for transseptal puncture described in
this text does not need to be modified in patients with a
right-sided aortic arch.
The Journal of Innovations in Cardiac Rhythm Management, June 2011
Emerging Indications for TS Puncture
TS catheterization in electrophysiology (EP).
Even if a PFO is present, transseptal puncture may still be preferred.
This is because the PFO tends to be superior and superiorly directed,
sometimes creating difficulty for accessing the inferior pulmonary veins
and the posteroinferior mitral annulus.
USES
RF ablation for atrial fibrillation..Ablation of accessory pathways located
along the mitral annular region, LA tachycardias and flutters.
J Am Coll Cardiol 2008;51:2116–22
Percutaneous mitral valve repair
The MitraClip device (Evalve Inc., Menlo Park, California),
requires the introduction of a 22-F device via TS puncture.
Puncture should be 3.5 to 4 cm above mitral annulus.
Adequate height above the valve ensures that the MitraClip
system has room to create a straight downward trajectory to
the apex of the ventricle with a minimum of manipulation
PFO and atrial septal defect (ASD) repair.
The second most common use for TS catheterization is percutaneous repair
of ASD and PFO.
In rare occasions, atrial septal aneurysms may “pocket” the catheter tip
and wire, preventing the cannulation of a small ASD or PFO. In this
situation and in the long-tunnel variant PFO, TS puncture has been used to
place a catheter in the LA, and deploy a closure device to seal the defect .
Catheter Cardiovasc Interv. 65 2005:295-300.
LA appendage closure
The LA appendage is positioned in the anterior-superior portion of the LA,
above the mitral valve. The Watchman device (Atritech Company,
Plymouth, Minnesota) is a nitinol cage with a polyethylene membrane that
can be implanted into the LA appendage of patients with atrial fibrillation
to prevent stroke.
For placement of this device, TS puncture is performed in the superior
fossa ovalis so that the delivery sheath is coaxial with the LA appendage,
and device deployment is facilitated.
Percutaneous left ventricular assist device
The TandemHeart Device (CardiacAssist, Pittsburgh,
Pennsylvania) is a circulatory assist device that retrogradely
perfuses the aorta with oxygenated blood from the LA.
After TS puncture, a 21-F cannula is advanced across the atrial
septum from the femoral vein.
Paravalvular leak (PVL) closure
Paravalvular leak of mitral prostheses can be repaired percutaneously from a TS
approach, particularly if the leak is along the lateral aspect of the LA.
The TS puncture should be in the middle or inferior fossa ovalis to direct a right
Judkins catheter to the lateral wall of the atrium at the level of the mitral valve.
A PVL along the medial aspect of mitral prostheses is technically more difficult to
repair because the acute angle needed to access the PVL. Such leaks might be
approached from a TS puncture performed from the right internal jugular vein.
Other procedures. The TS technique has been used in a
variety of other procedures, including pulmonary vein stenosis
intervention, antegrade VSD closure and atrial septostomy.
Transseptal access for ablation of non-AF arrhythmias
Transseptal access is often required for ablation of arrhythmias other
than AF. Two frequently encountered scenarios include ablation of
left-sided atrioventricular bypass tracts located along the mitral
annulus and ablation of ventricular arrhythmias via the transseptal
approach.
For ablation of bypass tracts, an anterior TSP can be particularly
helpful by directing the transseptal sheath and ablation catheter
directly toward the mitral annulus.
Catheter ablation of atrial fibrillation
The use of site-specific TSC can play an important role in achieving
success during AF ablation. The PVs are posterior structures in the LA and
assuring adequate ‘‘reach’’ of the RF or cryoballoon catheter is particularly
important, especially when addressing the right-sided veins.
For the purpose of RF catheter ablation of AF, in our laboratory, a
relatively anterior crossing of the IAS is preferred in order to allow
adequate room for deflectable sheaths and catheters to freely reach around
to the posterior wall and PVs.
For cryoballoon ablation, a more anterior crossing of the IAS has been
recommended, and our experience also suggests that this provides the most
favorable approach for accessing all PVs with the cryoballoon, particularly
the right inferior vein.
Regardless of the modality of ablation (RF or cryoballoon) or the
operator’s preferred site of transseptal crossing (anterior or posterior), ICE
provides a powerful tool for performing a safe site-specific TSP and
improving the chances of a successful AF ablation procedure.
Site specific puncture
Site-specific transseptal puncture is an essential skill to guide
many interventional structural heart.
As with most interventional procedures, proper guide position
is the foundation upon which the success of the procedure
depends.
Accomplishing this requires not only an understanding of
intracardiac anatomy, but also seamless communication
between the echo and flouroscopy.
March/April 2014 cardiac interventions Today
COMPLICATIONS
Relevant anatomy to procedural risks
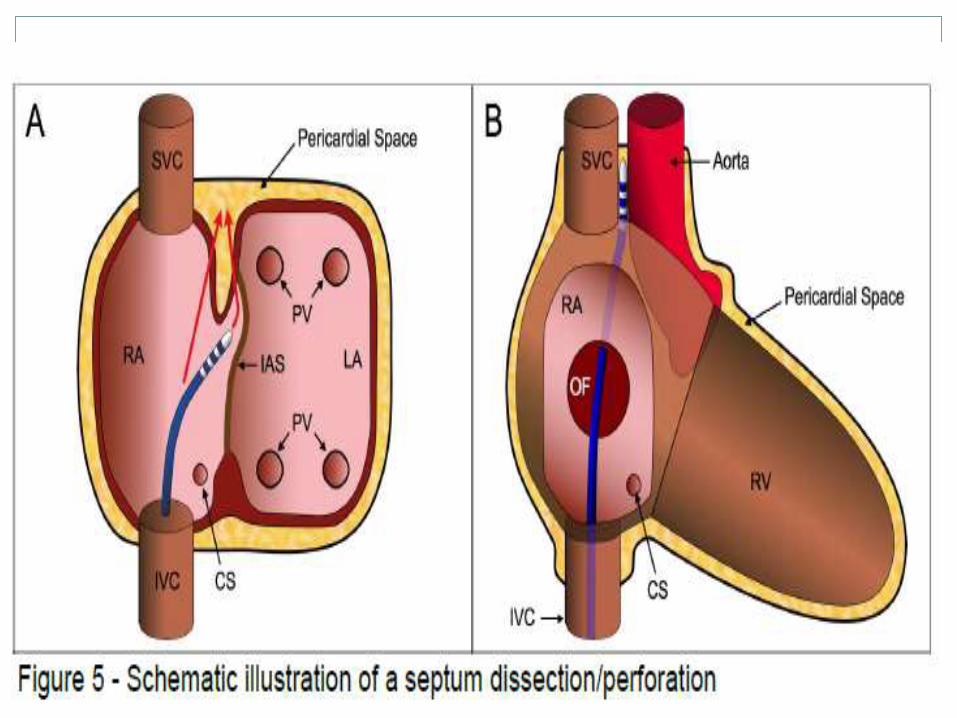
POSTERIOR
The posterior component of the FO is bordered by the atrial infolding,
comprising two muscular layers, and an inner adipose layer.
Puncture through this area would lead to a pericardial location.
In addition, with sufficient forward motion, the needle may pass between
the two layers and into the LA. This could be mistaken as a successful
puncture and the sheath advanced. This should be suspected if cardiac
tamponade develops as the transseptal sheath is withdrawn.
Cardiac tamponade
Incidence is 1.5 to 4.7 percent (3.2%).
Always have pre procedure echo to confirm whethr it is
new effusion or fat.
Any unexplained hypotension afer septal puncture
tamponade is more likely.
Clin Cardiol. 1986:21-26.
Think before pulling out
MANAGEMENT.
Only a needle puncture-wait and watch.defer the procedure and repeat echo in regular intervals.
If effusion is small and Balloon in left atrium,
do BMV as reduction in LA pressure will decreases the leak.
If septum is dilated, don’t remove the dilator.
Pigtail insertion and SHIFT TO CTVS with dilator in situ.
Reverse Heaprin (1 mg protamine per 100 U of UFH).
Autotransfusion
PREVENTION
Keep left femoral vein access.
After septal puncture-wait for 2 minutes and give heparin.
Heparin less than 30 min- full dose.
30 min to 2 hrs–use half dose.More than 2 hrs- quarter dose.
If 5000 U GIVEN< 2 hrs-25 mg >2hrs-12.5 mg
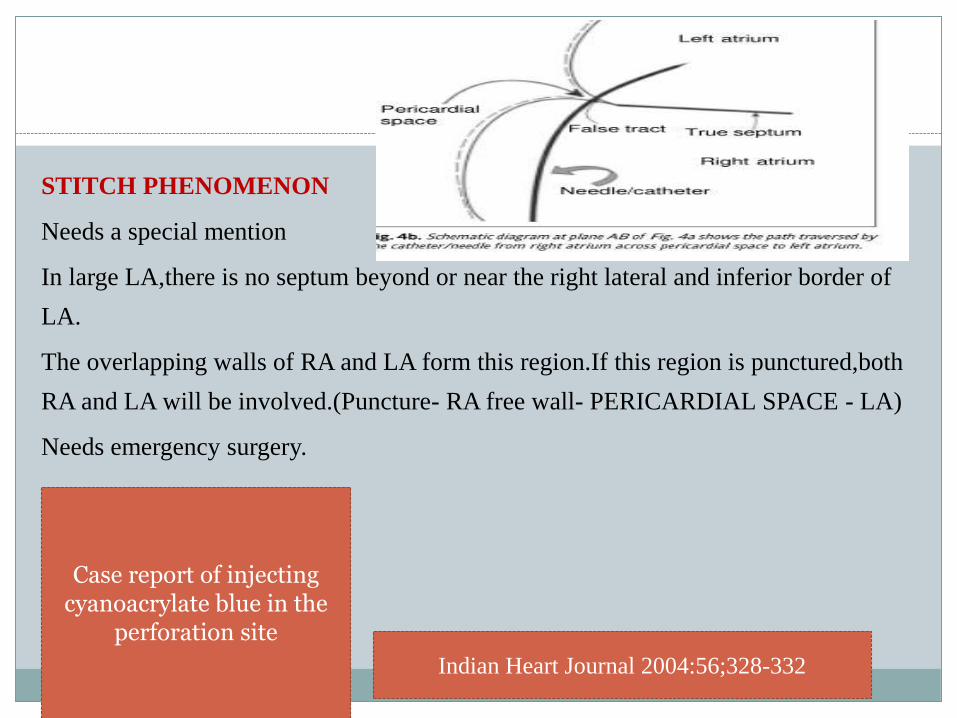
STITCH PHENOMENON
Needs a special mention
In large LA,there is no septum beyond or near the right lateral and inferior border of
LA.
The overlapping walls of RA and LA form this region.If this region is punctured,both
RA and LA will be involved.(Puncture- RA free wall- PERICARDIAL SPACE - LA)
Needs emergency surgery.
Indian Heart Journal 2004:56;328-332
Case report of injecting cyanoacrylate blue in the
perforation site
Keep in mind
Sometimes there will thin walled RV, so pericardial
puncture will enter RV also, hence pass a guide wire and see
its free movement ,check for pressure and for ectopics.
Complication
ANTERIOR
The most feared complication of transseptal puncture is penetration of the needle into the
aortic root. Puncture into the non-coronary cusp can be recognized by injection of contrast
and changes in the pressure waveform.
If this complication is not recognized and the sheath advanced into the aortic root, then
surgical repair is mandated.
Removal of the sheath should only be performed under direct surgical guidance and not prior
to operation, as tamponade is likely to result.
PREVENTION
Inject contrast in aorta before septal puncture.
Atrial septosotomy
In 1966 Rashkind and Miller described a nonsurgical
procedure to create an atrial septal defect, using a balloon
catheter.
Since then it has remained an integral part of cardiac
catheterisation in neonates.
The use of two-dimensional transthoracic echocardiography to
monitor the procedure, and the possibility of using the
umbilical vein as an access site have simplified this procedure
dramatically, so that it can be performed at the bedside in the
neonatal intensive care unit.
Used primarily in newborn children under six weeks of age
Indications for balloon atrial septostomy
Transposition of the great arteries with or without associated cardiac defects .
Tricuspid atresia with restrictive ASD,
Pulmonary atresia with intact ventricular septum
Total anomalous pulmonary venous connection with restrictive ASD.
It may be indicated in patients with hypoplastic left heart syndrome for emergency
relief of the transseptal atrial gradient in neonates with a severely restrictive interatrial
defect.
Balloon atrial septostomy is an effective treatment in infants less than six weeks. It is
inappropriate in children older than 1-2 months.
Balloon atrial septostomy has limitations in older infants,
due to the increased thickness of the atrial septum.
In these cases blade septostomy and static balloon
dilation of the atrial septum are prefered to enlarge the
interatrial communication.
Catheter description
A variety of catheters are in use for balloon atrial septostomy.
The most commonly used catheter at the present time, the 5F Miller
balloon atrial septostomy catheter (Edwards Lifesciences, Irvine,
CA, USA), needs an 7F to 8F introducer.
The low profile, dual lumen Z-5 atrioseptostomy catheter (Numed,
Cornwall, ON, Canada), comes in 4F or 5F sizes, depending on the
balloon diameter, and requires a 5 or 6F introducer, respectively.
The procedure can be performed under sedation or general anaesthesia.
The access can be achieved via the femoral or the umbilical vein.
The femoral vein is punctured in the typical way, an 4 or 5F introducer is
placed in the vessel, and then exchanged for a 7F or 8F introducer, when
the Miller catheter is used.
The balloon catheter is advanced into the right atrium. Then the foramen
ovale is crossed and the catheter is positioned in the left atrium.
Correct position is documented via biplane fluoroscopy or
two-dimensional echocardiography.
In the anteroposterior fluroscopic projection, it is
sometimes advantageous to position the catheter tip in the
orifice of the left upper pulmonary vein (outside the
cardiac silhouette), to confirm its left atrial location.
The balloon is quickly inflated with 3-4 ml of dilute radiopaque solution, locked,
and then sharply withdrawn into the right atrium down to the junction of the
inferior caval vein.
The catheter is then advanced into the body of the right atrium, so as not to
obstruct inferior caval return, and then deflated rapidly. This maneuver may be
repeated two to three times.
The size of the interatrial communication can be measured directly by
echocardiography at the table. The efficacy is usually immediately obvious, from
the rise in systemic arterial saturation
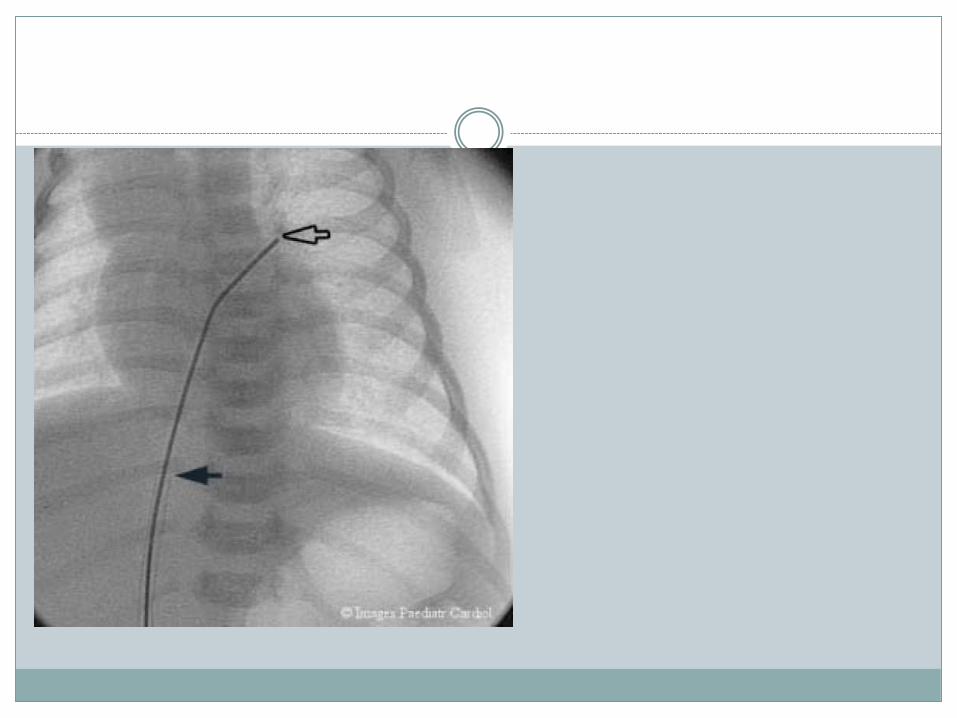
Using the umbilical venous approach, the umbilical cord is cut
transversely, flush with the skin, the vein is identified, and the catheter
directly inserted into the vessel with the aid of a forceps.
The progress of the catheter through the ductus venosus can be monitored
either by fluroscopy (in which case the catheter passes from the right of
the midline superiorly towards the right atrium in the anteroposterior
projection, and from front to back in the lateral projection), or by cross
sectional echocardiography.
Complications are rhythm disturbances (premature ectopic beats,
supraventricular tachycardia, atrial flutter and fibrillation, partial or
complete heart block, ventricular arrhythmias), perforation of the
heart, balloon fragment embolization, laceration of atrioventricular
valves, systemic or pulmonary veins and failure of balloon deflation.

THANK YOU