-
282 Neurology India | May-Jun 2009 | Vol 57 | Issue 3
Address for correspondence: Dr. Arun George Department of
Neurology, Medical College, Calicut - 673 008, Kerala, India.
E-mail: [email protected]
DOI: 10.4103/0028-3886.53276
Introduction
Guillain Barr syndrome (GBS) affects between one and four per
100,000 of the population annually throughout the world[1] causing
respiratory failure requiring ventilation in approximately 25%,
death in 4-15%[2-4],persistent disability in approximately 20%[5]
and persistent fatigue in 67%.[6] GBS has been classified on a
pathologic basis into demyelinating and axonal forms. Axonal GBS
has been classified further into two groups: Acute motor axonal
neuropathy (AMAN) and acute motor and sensory axonal neuropathy
(AMSAN).[7] The principal clinical method for distinguishing AMAN,
AMSAN, and acute inflammatory demyelinating polyneuropathy (AIDP)
is electrodiagnostic, and clear criteria have been formulated. The
pathology of AMAN and AMSAN is very similar, and both conditions
may follow Campylobacter jejuni enteritis. The clinical picture
AbstractBackground: Guillain-Barr syndrome (GBS) is an acute
neurological illness affecting the peripheral nervous system
causing significant morbidity. The syndrome has been classified
electrophysiologically into demyelinating and axonal forms. The
clinical features of the axonal variant (acute motor axonal
neuropathyAMAN) are not well characterized, particularly in the
Indian context. Objective: To assess the incidence, clinical
presentation and disease course of patients with AMAN. Materials
and Methods: This is an observational study done at a tertiary
referral center in South India. The study period extended from
January 2006 to July 2007. All patients with a clinical diagnosis
of GBS and satisfying the electrophysiological criteria for AMAN
were included. Results: There were 12 cases of AMAN out of a total
of 84 cases of GBS. All AMAN patients showed a characteristic
pattern of hand weakness predominant weakness of finger extensors
with relatively normal power in finger flexors, wrist flexors and
extensors. Proximal limb weakness was mild and was present in 85%
cases. One patient had cranial nerve palsy and one had
hyperreflexia. None of the patients progressed to respiratory
failure. Conclusion: AMAN is a distinct subgroup in GBS showing
certain distinguishing features, the most notable being predominant
weakness of finger extensors.
Key words: AMAn, finger drop, Guillain-Barr syndrome,
hypereflexia, paucity of cranial nerve palsy
Finger drop sign in Guillain-Barr syndrome
Arun George, P. Abdurehiman, Jose James
Department of Neurology, Medical College, Calicut - 673 008,
Kerala, India
Original Article
of AMAN has not been well characterized, particularly in the
Indian context. Here we report 12 consecutive cases of AMAN which
showed a characteristic pattern of predominant finger extensor
weakness.
Materials and Methods
This is an observational study conducted in a tertiary referral
center in south India. The study period extended from January 2006
to July 2007. The purpose of the study was to assess the incidence,
clinical presentation and the disease course of patients with AMAN.
All patients with a clinical diagnosis of GBS and
electrophysiological criteria satisfying AMAN were included.
Electrophysiological studies were performed within 10 days of the
onset of illness in all patients. Nerve conduction studies were
performed by the conventional procedures. Motor conduction studies
were done on the median, ulnar,
-
283Neurology India | May-Jun 2009 | Vol 57 | Issue 3
George, et al.: Finger drop sign
tibial, and peroneal nerves and sensory conduction studies on
the median, ulnar, and sural nerves on both sides. (This is the
standard protocol of nerve conduction study followed in our
institution for GBS irrespective of AMAN or AIDP.) Patients were
classified as having AMAN or AIDP based on the electrodiagnostic
criteria proposed by Hughes and Cornblath recently; i.e. none of
the features of AIDP except one demyelinating feature allowed in
one nerve if distal compound muscle action potential (CMAP) was
less than 10% of lower limit of normal and sensory action potential
amplitudes were normal.[8] Blood cell counts and routine blood
chemistry tests were done at the first neurological examination.
CSF analysis was done before treatment in all patients.
A patient was excluded in the presence of at least one of the
following: (1) marked, persistent asymmetry of the neurological
signs (asymmetry was considered to exist when the MRC grading of
muscle power differed by more than two grades between the
corresponding muscles of the right and left extremity); (2) >10
mononuclear leukocytes in the spinal fluid; (3) conditions such as
diabetic or alcohol neuropathy, neuropathies associated with
industrial agents, metals and drugs, poliomyelitis, and porphyria;
(4) electrodiagnostic study consistent with demyelination. All
patients clinical features including age, sex, presence of
preceding infections, vaccination, cranial nerve involvement,time
to nadir, pattern of limb weakness, Hughes grade and clinical
course were assessed. These patients were followed up monthly for
six months. During the study period we found that the clinical
presentation of AMAN showed certain distinctive features in
comparison to AIDP which also presented to us in the same period.
We then compared the clinical features of patients with AMAN and
AIDP to detect any major differences in their clinical
presentation.
ObservationsOur series had 12 cases of AMAN. During the same
period there were 66 AIDP cases, four cases of Miller Fischer
syndrome and two AMSAN; making a total of 84 cases
of GBS. Thus AMAN represents about 14% of GBS cases presenting
to our department. The clinical features of AMAN patients are given
in Table 1. There were eight males and four females. The mean age
was 33.8 years (range 11-73). Only six patients had a preceding
infection (three gastrointestinal and three respiratory). Nerve
conduction data is given in Table 2. All AMAN patients except two
had a characteristic pattern of distal upper extremity weakness
i.e. severe finger extensor weakness in presence of relatively
normal wrist extension, wrist flexion and finger flexion [Table 3].
Proximal upper extremity weakness (MRC Grade 3-4) was seen in 10
patients. Proximal (MRC Grade 2-4) as well as distal (MRC Grade2-4,
Grade 2 power in only one patient) lower extremity weakness was
seen in all patients. In the lower extremity Grade 2 weakness
occurred proximally in only two patients who were nonambulant at
presentation. Only one patient had bilateral facial palsy. One
patient had hyperreflexia. One patient had hyporeflexia with
extensor plantar response. None of these patients progressed to
respiratory paralysis requiring ventilator support. All patients
were ambulant at the two-month follow up but the finger extension
weakness still persisted, albeit to a lesser degree in eight
patients.
There were 55 AIDP patients for whom complete clinical and
electrophysiologic data [Table 4] are available. There were 31
males and 24 females. A preceding illness was seen in 43.5%. In MRC
grading of the muscle power none of these patients had a selective
finger extensor weakness. Whenever finger extensor weakness
occurred in AIDP patients it was always associated with equally
severe weakness in the finger flexors and much greater weakness in
the proximal muscles of the limb. Cranial nerve palsies were seen
in 32 (58%) patients. Thirteen patients (22%) required ventilator
support. Three patients died.
Discussion
GBS is an acute neurological illness, the course of which may
vary from a self-limiting illness to an acute fulminating illness
with a mortality of approximately
Table 1: Clinical features of patients with AMAN
Age Sex Preceding infection Cranial nerve palsy Hughes grade at
nadir Time to nadir (Days)
17 M Y* N* 3 673 M N N 2 938 M Y N 2 450 F Y N 3 532 M N Y 1 233
M N N 2 428 M Y N 4 623 F N N 3 411 F N N 2 340 F Y N 3 538 M Y N 4
424 M N N 2 3
Y* - Yes, N* - N0
-
284 Neurology India | May-Jun 2009 | Vol 57 | Issue 3
George, et al.: Finger drop sign
Table 2: Electrophysiological parameters on motor nerve
conduction study in AMAN patients
Nerve Mean distal latency (ms)
Mean CMAP amplitude
(mv)
Mean nerve conduction
velocity (m/s)
Median 3.44 (3.7 0.31) 3.2 (7.5 2.4) 55.6 (55.5 4.4)Ulnar 2.8
(2.7 0.5) 3.1 (6.9 2.06) 57 (59.4 5.33)
Common peroneal
4.4 (3.9 0.6) 2.1 (5.8 2.2) 48 (45.7 4.83)
Tibial 4.1 (3.8 0.70) 2.9 (7.1 3.2) 46 (47.2 3.86)
Normative data in our electrophysiology lab are given in
brackets
Table 4: Motor nerve conduction study in patients with AIDP
Nerve Mean distal
latency (Ms)
Mean CMAP amplitude
(mv)
Mean velocity
(m/s)
Conduction block (%)
Median 5.1 6.7 41 20Ulnar 5.06 6.2 38.5 15Common peroneal
6.18 5.3 32.7 17
Tibial 5.9 5.8 33.6 -
Table 3: MRC grading (average) of muscle power in the different
muscle groups in AMAN
Finger flexion
Finger extension
Wrist extension
Wrist flexion
Shoulder abduction
Hip flexion
Hip extension
Foot dorsiflexion
Foot plantar flexion
4 4 4 4 4 3 3 3 3
4 2 4 5 5 4 4 3 34 1 5 5 4 4 4 4 43 0 3 3 3 4 3 3 34 0 3 4 4 4 4
3+ 44 1 3 4 5 4 3 4 43 0 2 3 3 2 3 3 3
4 2 5 5 4 3 3 4 45 2 5 5 4 4 4 4 43 2 3 3 4 4 4 3 33 0 3 3 3 2 3
2 34 2 4 4 4 3 3 4 4
4-15% and permanent disability in about 20%. Patients with AMAN
were considered to have greater long-term disability[9] whereas
patients with AIDP were generally at high risk for rapid
deterioration and need of mechanical ventilation.[10]
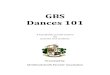
The previous studies have not stressed upon the clinical
features of AMAN. In our small series we found that AMAN patients
had a characteristic pattern of severe distal upper limb weakness
with varying degrees of proximal weakness. This pattern consisted
of severe finger extensor weakness (i.e. at the metacarpophalangeal
and interphalangeal joints) in the presence of relatively normal
power in finger flexion, wrist flexion and wrist extension-the
finger drop sign [Figure 1]. This extensor weakness was not due to
posterior interosseous nerve involvement alone, as to some extent
lumbricals were also involved. But the key feature is the
selectivity i.e. very weak finger extension and reasonably
preserved finger flexion, wrist flexion and extension. This finger
extensor weakness was bilateral in all the AMAN patients. It was
the presenting symptom in four patients. None of our patients with
AMAN had proximal muscle weakness in the absence of distal
involvement. Proximal weakness was mild in comparison to the distal
weakness, particularly in the upper extremity. Only two patients
had severe proximal weakness rendering them non- ambulant. Finger
extensor weakness exceeding MRC Grade 3
was present in 27(49%) patients with AIDP. But this weakness was
never selective i.e. it affected both extensors and flexors equally
and was always associated with severe proximal muscle weakness. It
was neither the presenting symptom nor the dominant symptom. Thus
predominant weakness of finger extensors seems to be relatively
specific for the AMAN variant of GBS.
One of our patients had hyperreflexia. Though this doesnt
satisfy the original clinical criteria where areflexia is a factor
required for making the diagnosis, the clinical course was
consistent with GBS and electrophysiology showed reduced amplitudes
of the CMAP. One patient had hyporeflexia and extensor plantar
response. This does not exclude GBS because in the article by
Asbury[11] it was mentioned that some patients might show a variant
pattern with extensor plantar response. So if the whole clinical
picture fits GBS, the presence of a mere extensor plantar does not
exclude the diagnosis. Deep tendon reflexes may be preserved
throughout the disease course in patients with AMAN and have been
considered indicators of rapid clinical recovery.[12,13] Moreover,
48% of Chinese and 33% of Japanese patients with AMAN showed
hyperreflexia in the recovery phase.[14,15] In Europe, patients
with pure motor GBS had preserved tendon reflexes up to MRC Grade 3
paresis, and more recently, an AMAN patient with hyperreflexia has
been reported.[16] Many believe that the diagnostic criterion of
areflexia should therefore be applied only to the sensory- motor
forms of GBS.
-
285Neurology India | May-Jun 2009 | Vol 57 | Issue 3
George, et al.: Finger drop sign
Fifty-eight per cent of patients with AIDP had cranial nerve
palsy while only one patient with AMAN had cranial nerve palsy
(8%). This paucity of cranial nerve involvement is another
characteristic feature of AMAN. Viser et al.,[17] in their study on
pure motor forms of GBS also observed the same.
All our AMAN patients improved and were ambulant independently
at two months but the finger drop still persisted in eight of the
12, consistent with previous reports of long period to recovery in
patients with axonopathy. There is controversy regarding the
recovery patterns in patients with AMAN. Some studies have shown
rapid clinical recovery whereas others have shown poor recovery
with persistent disability. In those cases showing rapid clinical
recovery authors postulate a distal conduction block at the motor
nerve terminal as the pathologic basis for the low-amplitude CMAP
and the rapid recovery due to reversal of conduction block at the
motor nerve terminals following treatment.[18] Studies employing
motor nerve terminal biopsy have proven this point. Those studies
showing poor clinical recovery suggest a primary axonal
degeneration as the basis for poor recovery. In a pathological
study of three patients with AMAN Feasby et al.,[19] found evidence
of axonal degeneration in the distal segments of the nerves as well
as in the ventral roots and moderate axonal degeneration. McKhann
et al.,[20] in their autopsy study on AMAN patients found
non-inflammatory demyelination and predominant axonal degeneration
in the ventral roots. Thus the pathological basis for the low CMAP
and hence recovery is not uniform in AMAN.
AMAN was recognized as a distinct entity in the early nineties.
McKhann reported a large series of 90 patients from China.[14]
These patients with AMAN were largely children from rural areas.
Bias towards children is due to the fact that this study was done
in a childrens hospital in China. In this study he reported a
rapidly evolving
weakness of proximal muscles and cranial nerve palsies. He did
not highlight any distal involvement. But in that study 25 patients
were followed up till one year in whom 17 patients (all ambulant)
still had distal weakness with mild atrophy of the hands and feet.
This suggests that these patients might have had severe distal
weakness also at initial presentation which may have been
overlooked because of equally severe or greater proximal weakness
and cranial nerve palsies. A second large series of AMAN patients
was reported by Visser et al., from the Dutch Guillain-Barr study
group.17] In this series they found 14 patients as having a pure
motor phenotype clinically. This group had certain specific
features such as shorter time from onset to nadir, predominant
distal weakness, lower incidence of cranial nerve palsies and less
need for ventilatory support. But electrophysiologically their
cases had evidence of distal demyelinating pathology suggesting
that a distal conduction block could have caused the low amplitude
of CMAPs. Our cases did not show any demyelinating features
electrophysiologically. So electrophysiology-wise our cases have
greater similarity to the series from China with normal distal
latencies and markedly reduced CMAP amplitudes. But in that series
there was dominant proximal weakness, the majority had cranial
nerve palsies and many required ventilatory assistance suggesting a
more fulminant entity whereas our clinical picture is milder. So
our cases fall in the middle of this spectrum where the weakness is
predominantly distal, cranial nerve palsies are few, course less
fulminant and electrophysiology suggestive of pure motor
axonopathy. These regional differences observed between the studies
could be due to the different antibodies targeting different sites
along the peripheral nervous system and causing variable degree of
axonal damage or there could be some genetic factor which might
influence the way one responds to an immunological insult and this
might be different in different populations. Future studies may
enhance our knowledge about this very interesting clinical entity
and may offer newer therapeutic strategies.
Figure 1a: Marked weakness of finger extensors Figure 1b: Normal
power in finger flexors
-
286 Neurology India | May-Jun 2009 | Vol 57 | Issue 3
Selectivity of weakness among different muscles or muscle groups
has always fascinated the clinicians in arriving at specific
diagnosis of motor system disease. Whether it is preferential
involvement of anti-gravity muscles in upper motor neuron
disorders, differential involvement of trunk (hypotonic) and limb
(spastic) muscles in cerebral palsy or the affection of specific
group of muscles in muscular dystrophies, these all are the
examples of exploitation of selectivity of muscle involvement for
the purpose of clinical diagnosis. Not much has been said in this
regard about generalized neuropathies except predilection of some
for proximal muscles and of majority for distal muscles. In this
context the article Finger drop sign in Guillain Barre syndrome is
a remarkable piece of work suggesting the diagnosis of AMAN variety
of GB
Sunil Pradhan
Department of Neurology, Institute of Human Behaviour &
Allied Sciences, Dilshad Garden, Delhi
Invited Commentary
syndrome as against AIDP variety whenever predominant weakness
of finger extensors was encountered. With an exception of toxic
neuropathy due to lead exposure, which in any case has a sub-acute
or a chronic presentation, no acute generalized polyneuropathy is
known to have such predilection for extensors of the fingers. With
time and validation finger drop sign is likely to gain popularity
among neurophysicians in the clinical diagnosis of AMAN. Though
finger drop sign has been described in a variety of other
neurological disorders, most of them are focal disorders leading to
unilateral posterior interosseous nerve syndrome and are obviously
out of context due to focal nature of these diseases. Among the
more generalized disorders finger drop sign has been observed with
multifocal motor neuropathy, motor
George, et al.: Finger drop sign
References
1. Hughes RA, Rees JH. Clinical and epidemiological features of
Guillain- Barr syndrome. J Infect Dis 1997;176:S92-8.
2. Van Koningsveld R, Van Doorn PA, Schmitz PI, Ang CW, Van der
Mech FG. Mild forms of Guillain-Barr syndrome in an epidemiologic
survey in The Netherlands. Neurology 2000;54:620-5.
3. Prevots DR, Sutter RW. Assessment of Guillain-Barr syndrome
mortality and morbidity in the United States: Implications for
acute flaccid paralysis surveillance. J Infect Dis
1997;175:S151-5.
4. Rees JH, Thompson RD, Smeeton NC, Hughes RA. An
epidemiological study of Guillain-Barr syndrome in south east
England. J Neurol Neurosurg Psychiatry 1998;64:74-7.
5. Plasma Exchange/Sandoglobulin Guillain-Barr Syndrome Trial
Group. Randomised trial of plasma exchange, intravenous
immunoglobulin, and combined treatments in Guillain-Barr syndrome.
Lancet 1997;349:225-30.
6. Merkies IS, Schmitz PI, Samijn JP, van der Mech FG, van Doorn
PA. Fatigue in immune-mediated polyneuropathies: European
Inflammatory Neuropathy Cause and Treatment (INCAT) Group.
Neurology 1999;53:1648-54.
7. Griffin JW, Li CY, Ho TW, Tian M, Gao CY, Xue P, et al.
Pathology of motor-sensory axonal Guillain-Barr syndrome. Ann
Neurol 1996;39:17-28.
8. Richard AC Hughes, David R. Cornblath Guillain-Barr syndrome.
Lancet 2005;366:1653-66.
9. The Italian Guillain-Barr Study Group. The prognosis and main
prognostic indicators of Guillain-Barr syndrome: A multicentre
prospective study of 297 patients. Brain 1996;119:2053-61.
10. Durand MC, Porcher R, Orlikowski D, Aboab J, Devaux C, Clair
B, et al. Clinical and electrophysiological predictors of
respiratory failure in Guillain-Barr syndrome: A prospective study.
Lancet Neurol
2006;5:1021-8.11. Asbury AK, Cornblath DR. Assessment of current
diagnostic criteria
for Guillain Barr Syndrome. Ann Neurol 1990;27:521.12. Yuki N,
Hirata K. Preserved tendon reflexes in Campylobacter
neuropathy. Ann Neurol 1998;43:546-48.13. Kuwabara S, Mori M,
Ogawara K, Hattori T, Yuki N. Indicators of
rapid clinical recovery in Guillain-Barr syndrome. J Neurol
Neurosurg Psychiatry 2001;70:560-2.
14. McKhann GM, Cornblath DR, Griffin JW, Ho TW, Li CY, Jiang Z,
et al. Acute motor axonal neuropathy: A frequent cause of acute
flaccid paralysis in China. Ann Neurol 1993;33:333-42.
15. Kuwabara S, Ogawara K, Koga M, Mori M, Hattori T, Yuki N.
Hyperreflexia in Guillain-Barr syndrome: Relation with acute motor
axonal neuropathy and anti-GM1 antibody. J Neurol Neurosurg
Psychiatry 1999;67:1804.
16. Podnar S, Vodusek DB. Hyperreflexia in a patient with motor
axonal Guillain-Barr syndrome. Eur J Neurol 2000;7:72730.
17. Visser LH, Van Der Meche A, Van Doorn PA, Meulstee J, Jacobs
BC, Oomes PG, et al. Guillain-Barr syndrome without sensory loss
(acute motor neuropathy): A subgroup with specific clinical,
electrodiagnostic and laboratory features. Brain
1995;118:841-7.
18. Cros D, Triggs WJ. There are no neurophysiologic features
characteristic of Axonal Guillain Barr Syndrome. Muscle Nerve
1994;17:675.
19. Feasby TE, Hahn AF, Brown WF, Bolton CF, Gilbert JJ, Koopman
WJ. Severe axonal degeneration in acute Guillain Barr Syndrome:
Evidence of two different mechanisms? J Neurol Sci 1993;11:185.
20. Griffin JW, Li CY, Ho TW, Xue P, Macko C, Gao CY, et al.
Guillain Barr Syndrome in northern China:The spectrum of
neuropathological changes in clinically defined cases.
Brain1995;118:577-95
Accepted on 25-04-09Source of Support: Nil, Conflict of
Interest: None declared.
MedknowPCRectangle