-
23/02/15
1
INTERAKSI OBAT Valen-na Meta Srikar-ka, S. Farm, MPH, Apt
Drug Interaction De7inition An interac-on is said to occur when
the eects of one drug are changed by the presence of another drug,
herbal medicine,
food, drink or by some environmental chemical agent (Baxter K,
2008)
Drug
Drug Herbal
Medicine Food Drink Chemical Agent
Incidence of Drug Interactions the reported incidence rates
ranged from 2.2 to 70.3%, and the percentage of pa-ents actually
experiencing problems was less than 11.1% 1
Another review found a 37% incidence of interac-ons among 639
elderly pa-ents 2
Yet another review of 236 geriatric pa-ents found an 88%
incidence of clinically signicant interac-ons, and a 22% incidence
of poten-ally serious and life-threatening interac-ons 3
An Australian study found that about 10% of hospital admissions
were drug-related, of which 4.4% were due to drug interac-ons 4
1. Haumschild MJ, Ward ES, Bishop JM, Haumschild MS.
Pharmacy-based computer system for monitoring and repor-ng drug
interac-ons. Am J Hosp Pharm (1987) 44, 345
2. Manchon ND, Berco E, Lamarchand P, Chassagne P, Senant J,
Bourreille J. Frquence et gravit des interac-on mdicamenteuses dans
une popula-on ge: tude prospec-ve concernant 39 malades. Rev Med
Interne (1989) 10, 5215
3. Lipton HL, Bero LA, Bird JA, McPhee SJ. The impact of
clinical pharmacists consulta-ons on physicians geriatric drug
prescribing. Med Care (1992) 30, 64658. 4. Stanton LA, Peterson GM,
Rumble RH, Cooper GM, Polack AE. Drug-related admissions to an
Australian hospital. J Clin Pharm Ther (1994) 19, 3417.
Mechanism of Drug Interaction Pharmacokine-cs Interac-ons
Pharmacodynamic Interac-ons
Absorp-on
Distribu-on
Metabolism
Excre-on
Addi-ve/synergis-c
Anatagonist
Drug Absorption Interaction For drugs that are given long-term,
in mul-ple doses (e.g. the oral an-coagulants) the rate of
absorp-on is usually unimportant, provided the total amount of drug
absorbed is not markedly altered.
On the other hand for drugs that are given as single doses,
intended to be absorbed rapidly (e.g. hypno-cs or analgesics),
where a rapidly achieved high concentra-on is needed, a reduc-on in
the rate of absorp-on may result in failure to achieve an adequate
eect.
1. Effects of changes in GI pH The passage of drugs through
mucous membranes by simple passive diusion depends upon the extent
to which they exist in the non-ionised lipid-soluble form.
Example: H2 Receptor Antagonist VS Ketoconazole
Example: Tetracycline VS Ca, Al, Mg, Fe
Since most drugs are largely absorbed in the upper part of the
small intes-ne, drugs that alter the rate at which the stomach
emp-es can aect absorp-on.
Example: Metoclopramide VS Paracetamol
2. Chelation mechanism 3. Changes in GI motility
-
23/02/15
2
Drug Distribution Interactions Absorp-on drugs are distributed
around the body by the circula-on.
Some drugs are totally dissolved in the plasma water, but many
others are transported with some propor-on of their molecules in
solu-on and the rest bound to plasma proteins (albumins).
One drug may successfully compete with another and displace it
from the sites it is already occupying. The displaced (and now
ac-ve) drug molecules pass into the plasma water where their
concentra-on rises.
For example, a drug that reduces the binding from 99 to 95%
would increase the unbound concentra-on of free and ac-ve drug from
1 to 5% (a vefold increase). This displacement is only likely to
raise the number of free and ac6ve molecules signicantly if the
majority of the drug is within the plasma rather than the 6ssues,
so that only drugs with a low apparent volume of distribu-on (Vd)
will be aected . such as tolbutamide (96% bound, Vd 10 litres),
oral an-coagulants, such as warfarin (99% bound, Vd 9 litres), and
phenytoin (90% bound, Vd 35 litres).
For Example: Warfarin VS Cloral Hydrate
Drug Metabolism Interactions Enzyme Induc6on. Example: inducers
the cytocrome P450: Carbamazepine, Dexamethasone, Phenobarbital,
Phenitoin, Rifampicin
Example: Rifampicin VS Warfarin The extent of the enzyme
induc-on depends on the drug and its dosage, but it may take days
or even 2 to 3 weeks to develop fully, and may persist for a
similar length of -me when the enzyme inducer is stopped (delayed
in onset and slow to resolve).
Enzyme Inhibi6on. Example of inhibitors the cytocrome P450:
azoles, cime-dine, dil-azem, macrolida
Example: Cime-dine VS Propanolol The clinical signicance of many
enzyme inhibi-on interac-ons depends on the extent to which the
serum levels of the drug rise. If the serum levels remain within
the therapeu-c range the interac-on may not be clinically
important
Drug Excretion Interactions Most drugs are excreted either in
the bile or in the urine. Blood entering the kidneys along the
renal arteries is, rst of all, delivered to the glomeruli of the
tubules where molecules small enough to pass through the pores of
the glomerular membrane (e.g. water, salts, some drugs) are ltered
through into the lumen of the tubules.
Larger molecules, such as plasma proteins, and blood cells are
retained within the blood.
The blood ow then passes to the remaining parts of the kidney
tubules where ac-ve energy-using transport systems are able to
remove drugs and their metabolites from the blood and secrete them
into the tubular ltrate.
The renal tubular cells addi-onally possess ac-ve and passive
transport systems for the reabsorp-on of drugs
1. Changes in Urinary pH Only the non-ionised form is
lipid-soluble and able to diuse back through the lipid membranes of
the tubule cells.
Example: Aspirin VS Urine alkalinize/acidier
Drugs that use the same ac-ve transport systems in the renal
tubules can compete with one another for excre-on
Example: Probenecid VS Penisilin
The ow of blood through the kidney is par-ally controlled by the
produc-on of renal vasodilatory prostaglandins
Example: NSAIDs VS Lithium
2. Changes in Active Renal Tubular Exretion 3. Changes in Renal
Blood Flow
Pharmacodynamics Interactions Addi6ve/synergis6c Interac6ons. If
two drugs that have the same pharmacological eect are given
together the eects can be addi-ve
Addi-ve eects can occur with both the main eects of the drugs as
well as their adverse eects
Example: Methotrexate VS Co-trimoxazole (Bone marrow
megaloblastosis due to folic acid antagonism)
Antagonis6c/opposing Interac6ons. In contrast to addi-ve
interac-ons, there are some pairs of drugs with ac-vi-es that are
opposed to one another.
Example: Coumarin VS dietary vitamin K.
Management of Drug Interactions Obat-obat yang berinteraksi
seringkali tetap bisa
digunakan bersamaan Ada interaksi obat yang menguntungkan
Contoh : probenecid VS penisillin Sifat laporan / informasi IO
Kedalaman informasi Waktu penerbitan literature / current
literature Clinical VS statistical significance
-
23/02/15
3
Management of Drug Interactions terdapat 3 derajat keparahan IO
yait: :
Keparahahan MINOR Bisa terjadi tetapi tidak sigAikan
Keparahan MODERATE Pasien mungkin mengalami sesuat: yang dapat
membuat kondisinya membur:k karena IO Jika kedua obat memang har:s
dig:nakan bersamaan ?
Keparahan MAYOR Bila obat dig:nakan bersamaan, maka kemungkinan
dapat mengancam jiwa (life threatening)
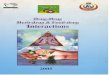
Clinical Signi7icance Grading (Tatro) Tingkat
Signifikasi Keamanan Dokumentasi
1 Major Established, Probable or Suspected
2 Moderate Established, Probable or Suspected
3 Minor Established, Probable or Suspected
4 Major / Moderate Possible
5 Minor / Any Possible/ unlikely
!
Clinical Signi7icance Grading (Tatro) Established adalah
interaksi obat yang memiliki hasil data klinik yang memadai dan
telah terbuk- terjadi dalam beberapa peneli-an yang telah
dilakukan, baik dari segi efek farmakologis dan interaksi
farmakokine-ka.
Probable adalah interaksi obat yang sangat mungkin terjadi,
namun dalam beberapa uji klinis -dak terbuk-.
Suspected adalah interaksi yang kemungkinan teradi, beberapa
interaksi obat telah memiliki data klinik yang baik dan sebagian
interaksi obat membutuhkan peneli-an lebih lanjut.
Possible adalah interaksi dapat terjadi namun data klinik yang
dimiliki sangat terbatas,
Sedangkan unlikely adalah interaksi obat yang memiliki
dokumentasi pada posibble dan suspected, namun karena memiliki
interaksi yang cukup banyak dan -dak memiliki buk- klinis yang baik
sehingga pada akhirnya dikategorikan sebagai unlikely
Conclusion FarSasis sehar:snya siaga terhadap interaksi obat
yang potensial terjadi
Jika kombinasi obat yang potensial menimbulkan interaksi tidak
dapat dihindari : SESUAIKAN DOSIS dan MONITOR PASIEN
Jika terjadi interaksi obat, kombinasi obat yang potensial
menimbulkan interaksi dapat dihindari dengan mengganti obat yang
dicurigai dengan obat lain yang tidak menimbulkan interaksi