Embed Size (px)
Citation preview

IN ADPKD FIND OUT WHY
SEEING IS BELIEVINGADPKD=autosomal dominant polycystic kidney disease.
INDICATION: JYNARQUE® (tolvaptan) is indicated to slow kidney function decline in adults at risk of rapidly progressing autosomal dominant polycystic kidney disease (ADPKD).
WARNING: RISK OF SERIOUS LIVER INJURY• JYNARQUE (tolvaptan) can cause serious and potentially fatal liver injury. Acute liver failure requiring liver transplantation has been reported• Measure transaminases (ALT, AST) and bilirubin before initiating treatment, at 2 weeks and 4 weeks after initiation, then monthly for the
first 18 months and every 3 months thereafter. Prompt action in response to laboratory abnormalities, signs, or symptoms indicative of hepatic injury can mitigate, but not eliminate, the risk of serious hepatotoxicity
• Because of the risks of serious liver injury, JYNARQUE is available only through a Risk Evaluation and Mitigation Strategy program called the JYNARQUE REMS Program
Please see IMPORTANT SAFETY INFORMATION on pages 9-10.
Patient image and patient case are fictional.

2
Peter, a 49-year-old accountant with ADPKD
Patient image and patient case are fictional.
Kidney function is an important measure of disease progression, especially in patients with more advanced disease1
Imaging the kidneys to measure total kidney volume (TKV) can help identify rapidly progressing ADPKD and reveal the extent of disease progression.2-4
SELECT IMPORTANT SAFETY INFORMATION:CONTRAINDICATIONS: • History, signs or symptoms of
significant liver impairment or injury. This contraindication does not apply to uncomplicated polycystic liver disease
• Taking strong CYP3A inhibitors
• With uncorrected abnormal blood sodium concentrations
• Unable to sense or respond to thirst• Hypovolemia
• Hypersensitivity (e.g., anaphylaxis, rash) to JYNARQUE® (tolvaptan) or any component of the product
• Uncorrected urinary outflow obstruction• Anuria
REALLY SEE ADPKD
UNDERSTANDING RISK FACTORS ASSOCIATED WITH RAPID PROGRESSION CAN HELP YOU

Please see IMPORTANT SAFETY INFORMATION on pages 9-10.3
PETER’S MEDICAL HISTORY CAN HELP IDENTIFY RAPIDLY PROGRESSING ADPKD
CKD=chronic kidney disease.eGFR=estimated glomerular filtration rate.ESRD=end-stage renal disease.
Identifying certain risk factors associated with rapid progression can start to give you a better understanding of a patient’s disease5
Vitals• Age: 49• Height: 5 feet, 8 inches (1.7 m)• Weight: 165 lb• BMI: 25• Blood pressure: 128/85 mm Hg
(managed with antihypertensive therapy)
ADPKD diagnosis• 13 years ago Peter’s PCP was
concerned about Peter’s early onset hypertension and family history of ADPKD and referred him to a nephrologist who used an ultrasound to confirm diagnosis of ADPKD
Family history• Mother diagnosed with ADPKD in
mid-30s with CKD stage 3A and started dialysis at age 45
Medical history• CKD stage 3A• Hypertension (presented with a
blood pressure of 153/95 mm Hg) • Serum creatinine: 1.5 mg/dL• eGFR: 54 mL/min/1.73 m2
(5.2 mL/min/1.73 m2 decline in 12 months)
Risk factor: eGFR decline
An eGFR decline ≥5 mL/min/1.73 m2 within 1 year is a risk factor associated with rapidly progressing ADPKD.6
Risk factor: Family history
A family history of ESRD before age 58 is a risk factor associated with rapid disease progression.6

4
SELECT IMPORTANT SAFETY INFORMATION:Serious Liver Injury: JYNARQUE® (tolvaptan) can cause serious and potentially fatal liver injury. Acute liver failure requiring liver transplantation has been reported in the post-marketing ADPKD experience. Discontinuation in response to laboratory abnormalities or signs or symptoms of liver injury (such as fatigue, anorexia, nausea, right upper abdominal discomfort, vomiting, fever, rash, pruritus, icterus, dark urine or jaundice) can reduce the risk of severe hepatotoxicity. To reduce the risk of significant or irreversible liver injury, assess ALT, AST and bilirubin prior to initiating JYNARQUE, at 2 weeks and 4 weeks after initiation, then monthly for 18 months and every 3 months thereafter.
History of symptoms• Hematuria: Yes• Abdominal/flank pain: Yes• Kidney stones: No• Urinary tract infection: No• Liver cysts: Yes• Kidney cyst infections: Yes
Diagnosis: At risk for rapid progression of ADPKD
Peter’s family history, symptoms, and eGFR decline led his nephrologist to suspect rapidly progressing ADPKD.

5Please see IMPORTANT SAFETY INFORMATION on pages 9-10.
IMAGING PETER’S KIDNEYS HELPED REVEAL THE EXTENT OF HIS DISEASEImaging the kidneys to determine TKV can help confirm a risk of rapidly progressing ADPKD—and predict future decline of kidney function7
After confirming a diagnosis of rapidly progressing ADPKD, Peter’s nephrologist ordered an abdominal CT scan to see the extent of his disease.
CT scan to evaluate TKV helped confirm a high risk of rapid progression and future decline of kidney function. Imaging the kidneys can help predict the risk of rapid kidney function decline.2
Imaging results Risk factor: TKV greater than expected for age
Continuous cyst growth in both kidneys increases TKV and eventually leads to ESRD.3
In patients like Peter with more advanced disease, reduced eGFR (<60 mL/min/1.73 m2) can be informative in identifying patients at risk of rapidly progressing ADPKD. Imaging remains important in this setting to rule out other contributing factors.1

6
CALCULATING PETER’S TKV
SELECT IMPORTANT SAFETY INFORMATION: Hypernatremia, Dehydration and Hypovolemia: JYNARQUE® (tolvaptan ) therapy increases free water clearance which can lead to dehydration, hypovolemia and hypernatremia. Instruct patients to drink water when thirsty, and throughout the day and night if awake. Monitor for weight loss, tachycardia and hypotension because they may signal dehydration. Ensure abnormalities in sodium concentrations are corrected before initiating therapy. If serum sodium increases above normal or the patient becomes hypovolemic or dehydrated and fluid intake cannot be increased, suspend JYNARQUE until serum sodium, hydration status and volume status parameters are within the normal range.
CT=computed tomography.
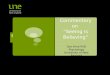
Peter’s TKV can be calculated using CT measurements of kidney length, width, and depth using the ellipsoid equation8
Height-adjusted (ht) TKV4,7
Peter’s htTKV can be used to estimate his future renal declineTKV: 4490 mLHeight: 1.7 m Peter’s htTKV: 2641.2 mL/m
L=length; W=width; D=depth.Units for kidney dimensions are in mm. To get kidney volume in mL, multiply by 0.001.
LEFT KIDNEY RIGHT KIDNEY
x (LxWxD)6π TKVx (LxWxD)6
π+ =
hTKV htTKV=
WidthDepth
LengthLength
Depth Width

7Please see IMPORTANT SAFETY INFORMATION on pages 9-10.
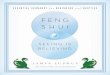
Plotting htTKV and age predicts the change in eGFR over time in patients with typical* ADPKD7
*Bilateral and diffuse distribution, with mild, moderate, or severe replacement of kidney tissue by cysts, where all cysts contribute similarly to TKV.7 Republished with permission of the American Society of Nephrology, from Imaging classification of autosomal polycystic kidney disease: a simple model for selecting patients for clinical trials. J Am Soc Nephrol. 2015;26(1):160-172.
PREDICTING CHANGES IN PETER’S KIDNEY FUNCTION
Patient Age (Years)
HtTK
V (m
L/m
)
200
400
600800
1000
2000
4000
60008000
10000
16000
15 20 25 30 35 40 45 50 55 60 65 70 75 80
Class 1E
Class 1C
Class 1B
Class 1A
Class 1D
Estimated kidney growth rate:
yearly percentage increase
1A
Low risk
<1.5% 3%–4.5%1.5%–3%
Intermediate risk High risk High risk High risk
4.5%–6%
1B 1C 1D 1E
>6%
Class
Risk for eGFR decline
Peter

8
Patient Age (Years)
HtTK
V (m
L/m
)200
400
600800
1000
2000
4000
60008000
10000
16000
15 20 25 30 35 40 45 50 55 60 65 70 75 80
Class 1E
Class 1C
Class 1B
Class 1A
Class 1D
Estimated kidney growth rate:
yearly percentage increase
1A
Low risk
<1.5% 3%–4.5%1.5%–3%
Intermediate risk High risk High risk High risk
4.5%–6%
1B 1C 1D 1E
>6%
Class
Risk for eGFR decline
A patient’s ADPKD imaging classification† can help estimate their disease progression7
SELECT IMPORTANT SAFETY INFORMATION:Inhibitors of CYP3A: Concomitant use of JYNARQUE with drugs that are moderate or strong CYP3A inhibitors (e.g., ketoconazole, itraconazole, lopinavir/ritonavir, indinavir/ritonavir, ritonavir, and conivaptan) increases tolvaptan exposure. Use with strong CYP3A inhibitors is contraindicated; dose reduction of JYNARQUE is recommended for patients taking moderate CYP3A inhibitors. Patients should avoid grapefruit juice beverages while taking JYNARQUE.
†Classification only applies to patients with typical morphology of ADPKD as defined by diffuse bilateral cystic involvement of the kidneys.7
In ADPKD
Seeing is BelievingImaging the kidneys can help you see the extent of disease progression in rapidly progressing ADPKD, and help you identify patients, like Peter, who may benefit from treatment with JYNARQUE® (tolvaptan)2-4

9(Continued on next page)
INDICATION: JYNARQUE is indicated to slow kidney function decline in adults at risk of rapidly progressing autosomal dominant polycystic kidney disease (ADPKD).
IMPORTANT SAFETY INFORMATION:WARNING: RISK OF SERIOUS LIVER INJURY
• JYNARQUE (tolvaptan) can cause serious and potentially fatal liver injury. Acute liver failure requiring liver transplantation has been reported
• Measure transaminases (ALT, AST) and bilirubin before initiating treatment, at 2 weeks and 4 weeks after initiation, then monthly for the first 18 months and every 3 months thereafter. Prompt action in response to laboratory abnormalities, signs, or symptoms indicative of hepatic injury can mitigate, but not eliminate, the risk of serious hepatotoxicity
• Because of the risks of serious liver injury, JYNARQUE is available only through a Risk Evaluation and Mitigation Strategy program called the JYNARQUE REMS Program
CONTRAINDICATIONS:• History, signs or symptoms of significant liver impairment or injury. This contraindication does not apply to uncomplicated
polycystic liver disease• Taking strong CYP3A inhibitors• With uncorrected abnormal blood sodium concentrations• Unable to sense or respond to thirst• Hypovolemia• Hypersensitivity (e.g., anaphylaxis, rash) to JYNARQUE or any component of the product• Uncorrected urinary outflow obstruction• Anuria Serious Liver Injury: JYNARQUE can cause serious and potentially fatal liver injury. Acute liver failure requiring liver transplantation has been reported in the post-marketing ADPKD experience. Discontinuation in response to laboratory abnormalities or signs or symptoms of liver injury (such as fatigue, anorexia, nausea, right upper abdominal discomfort, vomiting, fever, rash, pruritus, icterus, dark urine or jaundice) can reduce the risk of severe hepatotoxicity. To reduce the risk of significant or irreversible liver injury, assess ALT, AST and bilirubin prior to initiating JYNARQUE, at 2 weeks and 4 weeks after initiation, then monthly for 18 months and every 3 months thereafter.
INDICATION and IMPORTANT SAFETY INFORMATION for JYNARQUE® (tolvaptan)

Hypernatremia, Dehydration and Hypovolemia: JYNARQUE therapy increases free water clearance which can lead to dehydration, hypovolemia and hypernatremia. Instruct patients to drink water when thirsty, and throughout the day and night if awake. Monitor for weight loss, tachycardia and hypotension because they may signal dehydration. Ensure abnormalities in sodium concentrations are corrected before initiating therapy. If serum sodium increases above normal or the patient becomes hypovolemic or dehydrated and fluid intake cannot be increased, suspend JYNARQUE until serum sodium, hydration status and volume status parameters are within the normal range.Inhibitors of CYP3A: Concomitant use of JYNARQUE with drugs that are moderate or strong CYP3A inhibitors (e.g., ketoconazole, itraconazole, lopinavir/ritonavir, indinavir/ritonavir, ritonavir, and conivaptan) increases tolvaptan exposure. Use with strong CYP3A inhibitors is contraindicated; dose reduction of JYNARQUE is recommended for patients taking moderate CYP3A inhibitors. Patients should avoid grapefruit juice beverages while taking JYNARQUE.Adverse Reactions: Most common observed adverse reactions with JYNARQUE (incidence >10% and at least twice that for placebo) were thirst, polyuria, nocturia, pollakiuria and polydipsia. Other Drug Interactions:• Strong CYP3A Inducers: Co-administration with strong CYP3A inducers reduces exposure to JYNARQUE. Avoid concomitant use
of JYNARQUE with strong CYP3A inducers• OATP1B1/3 and OAT3 Transporter Substrates: Patients who take JYNARQUE should avoid concomitant use with OATP1B1/
B3 and OAT3 substrates (e.g., statins, bosentan, glyburide, nateglinide, repaglinide, methotrexate, furosemide), as the plasma concentrations of these substrates may be increased
• BCRP Transporter Substrates: Tolvaptan is an inhibitor of BCRP. Patients who take JYNARQUE, should avoid concomitant use with BCRP substrates (e.g., rosuvastatin)
• V2-Receptor Agonist: Tolvaptan interferes with the V2-agonist activity of desmopressin (dDAVP). Avoid concomitant use of JYNARQUE with a V2-agonist
Pregnancy and Lactation: Based on animal data, JYNARQUE may cause fetal harm. In general, JYNARQUE should be discontinued during pregnancy. Advise women not to breastfeed during treatment with JYNARQUE.To report SUSPECTED ADVERSE REACTIONS, contact Otsuka America Pharmaceutical, Inc. at 1-800-438-9927 or FDA at 1-800-FDA-1088 (www.fda.gov/medwatch).Please see FULL PRESCRIBING INFORMATION, including BOXED WARNING.
10
INDICATION and IMPORTANT SAFETY INFORMATION for JYNARQUE® (tolvaptan) (Cont’d)

Manufactured by Otsuka Pharmaceutical Co., Ltd., Tokyo, 101-8535 Japan.Distributed and marketed by Otsuka America Pharmaceutical, Inc., Rockville, MD 20850 USA.JYNARQUE is a registered trademark of Otsuka Pharmaceutical Co., Ltd., Tokyo, 101-8535 Japan.All rights reserved.
©2019 Otsuka America Pharmaceutical, Inc. October 2019 10US19EBP0187
References: 1. Chebib FT, Perrone RD, Chapman AB, et al. J Am Soc Nephrol. 2018;29(10):2458-2470. doi:10.1681/ASN.2018060590 2. Grantham JJ, Chapman AB, Torres VE. Clin J Am Soc Nephrol. 2006;1(1):148-157. 3. Grantham JJ, Torres VE. Nat Rev Nephrol. 2016;12(11):667-677. 4. Chapman AB, Bost JE, Torres VE, et al. Clin J Am Soc Nephrol. 2012;7(3):479-486. 5. Schrier RW, Brosnahan G, Cadnapaphornchai MA, et al. J Am Soc Nephrol. 2014;25(11):2399-2418. doi:10.1681/ASN.2013111184 6. Gansevoort RT, Arici M, Benzing T, et al. Nephrol Dial Transplant. 2016;31(3):337-348. 7. Irazabal MV, Rangel LJ, Bergstralh EJ, et al. J Am Soc Nephrol. 2015;26(1):160-172. 8. Magistroni R, Corsi C, Martí T, Torra R. Am J Nephrol. 2018;48(1):67-78. doi:10.1159/000491022
Talk to your Otsuka Sales Representative about watching an interactive video featuring
Peter and visit JYNARQUEhcp.com to learn more about why
Seeing is Believing
Please see FULL PRESCRIBING INFORMATION, including BOXED WARNING.