Embed Size (px)
Citation preview
HYPERACUTE STROKE CASE STUDIES
By Mady Roman Hyper Acute Stroke Nurse
Practitioner RHH
MC Case study 82 years old, lady
• 9:30 well, in touch with her son
• 11:30 hairdresser came to her house and found her slumped in chair with left side weakness, unable to move, confused.
• GCS=14/15, NIHSS=16
MC Case study NIHSS on arrival= 16
• confused
• partial gaze to right
• complete left hemianopia
• left minor facial paresis
• no movement to left arm
• no effort against gravity on left leg
• severe sensory loss on left side
• mild slurring of words
• complete neglect on left side
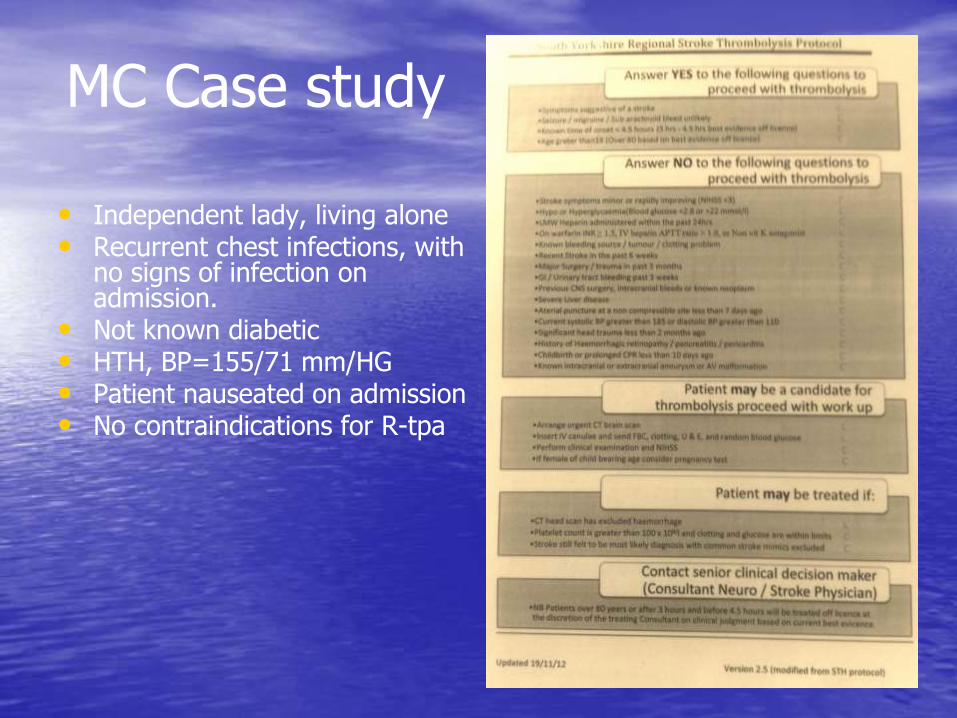
• Independent lady, living alone • Recurrent chest infections, with
no signs of infection on admission.
• Not known diabetic • HTH, BP=155/71 mm/HG • Patient nauseated on admission • No contraindications for R-tpa
MC Case study
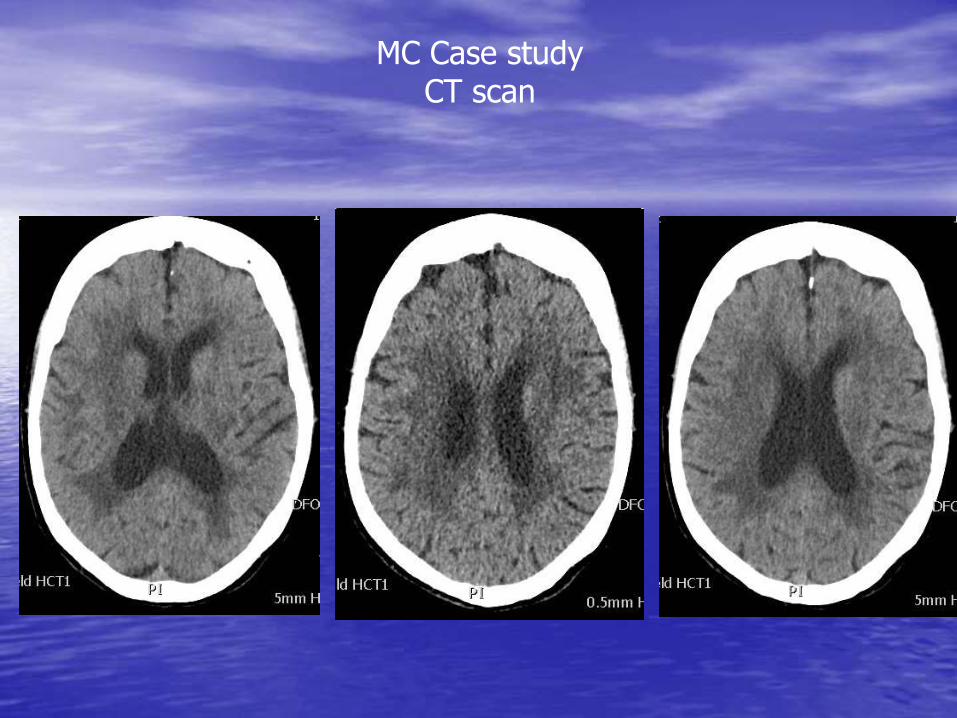
MC Case study CT scan
MC Case Study
Would you thrombolyse?
MC Case study CT scan reported:
• There is low attenuation within the right basal ganglia, it is not possible to be certain whether this is an acute or area of infarction or long standing ischaemia.
• There is increased density to the right MCA.
• Ischaemia is also noted within the brainstem.
• No acute haemorrhage.
MC Case study
• Considered for thrombolysis.
• Consent received from
family and patient. • Proceeded to
thrombolyse @13:10, 3h40’ from last seen well and
48’ from arrival to hospital
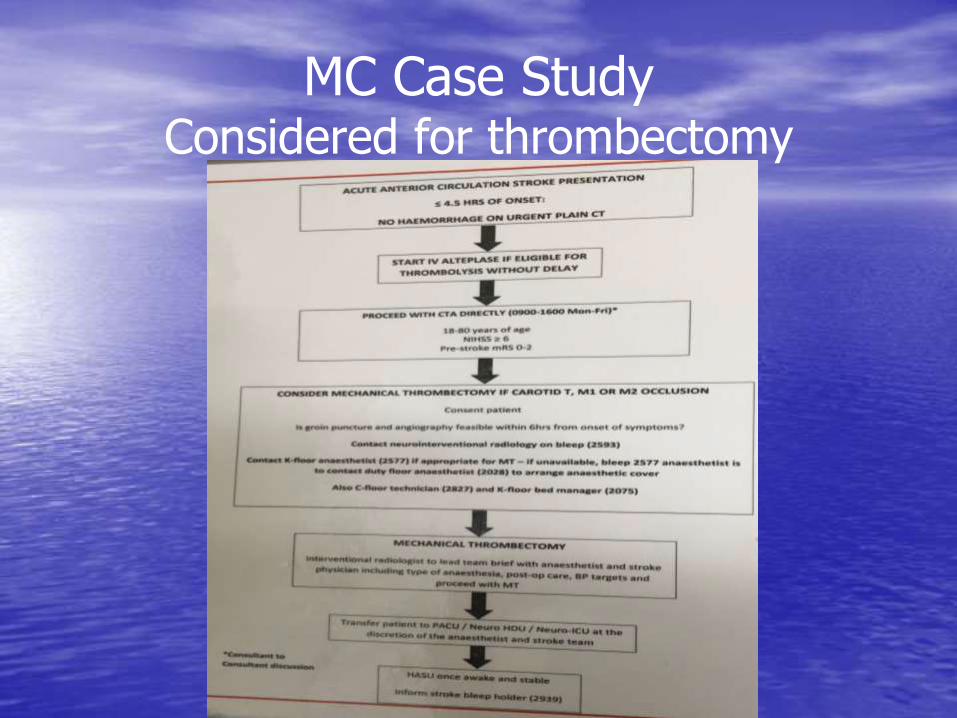
MC Case Study Considered for thrombectomy
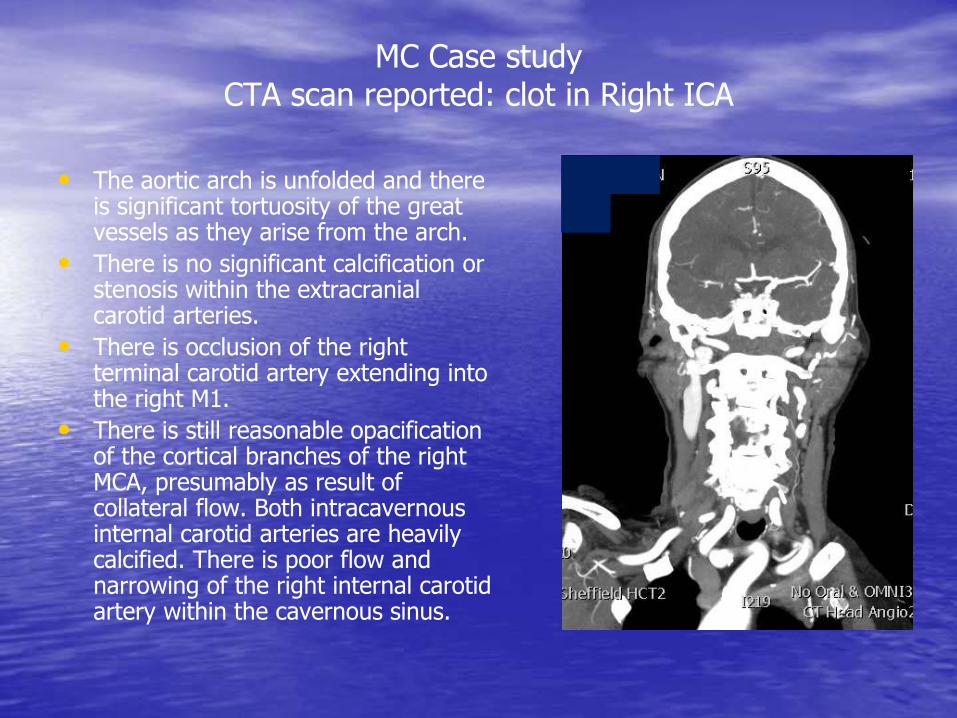
• The aortic arch is unfolded and there is significant tortuosity of the great vessels as they arise from the arch.
• There is no significant calcification or stenosis within the extracranial carotid arteries.
• There is occlusion of the right terminal carotid artery extending into the right M1.
• There is still reasonable opacification of the cortical branches of the right MCA, presumably as result of collateral flow. Both intracavernous internal carotid arteries are heavily calcified. There is poor flow and narrowing of the right internal carotid artery within the cavernous sinus.
MC Case study CTA scan reported: clot in Right ICA
MC Case Study
• Would you proceed to thrombectomy?
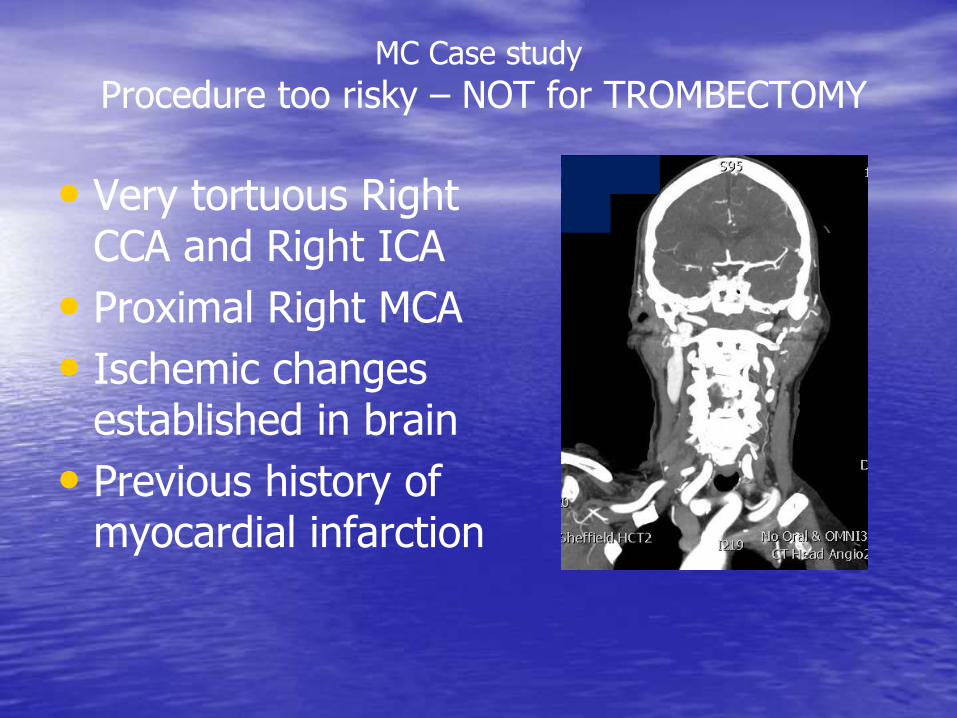
• Very tortuous Right CCA and Right ICA
• Proximal Right MCA
• Ischemic changes established in brain
• Previous history of myocardial infarction
MC Case study
Procedure too risky – NOT for TROMBECTOMY
14:35 Patient arrived in HASU from x-Ray department;
On arrival to HASU:
• GCS=15/15, NIHSS=13, confusion cleared, improving heminopia and left side weakness, improving speech.
• R-tpa infusion finished
• BP=201/100 mmHG, nausea still present.
• Bleed suspected by nursing staff
MC Case study
MC Case Study
• What would you do?
MC Case study
• Suspected bleed dismissed by medical staff on basis of improving neurology and long standing nausea.
• Labetalol given with success, BP=166/77 mgHG
MC Case study
• 3:00 am next day – nursing staff found patient vomiting, BP:201/100 mmHG
• 3:05 am patient become unresponsive, GCS dropped from 14/15 to 9/15
• H@N called and F1 doctor sent to review patient.
• NIHSS=23: patient not responding to voice, making incomprehensive sounds, withdrawing to pain on left side, pupils equal reacting to light.
• SNP ordered urgent CT head
• F1 requested SPR advice
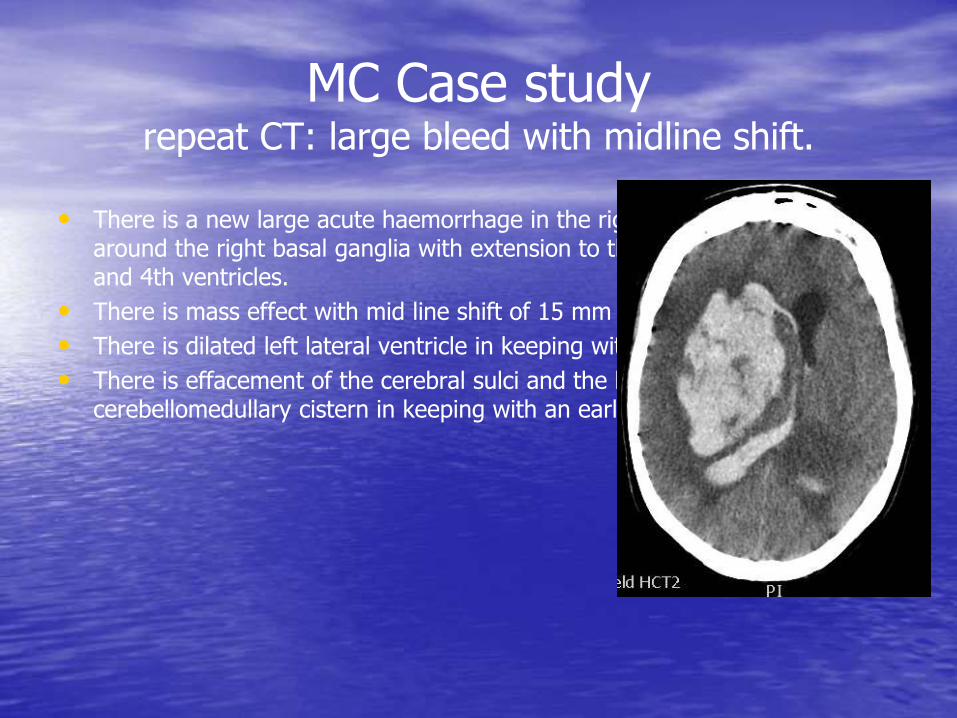
MC Case study repeat CT: large bleed with midline shift.
• There is a new large acute haemorrhage in the right hemisphere centered around the right basal ganglia with extension to the lateral ventricles, 3rd and 4th ventricles.
• There is mass effect with mid line shift of 15 mm to the left.
• There is dilated left lateral ventricle in keeping with hydrocephalus.
• There is effacement of the cerebral sulci and the basal cisterns apart from cerebellomedullary cistern in keeping with an early cerebral herniation.
MC case study
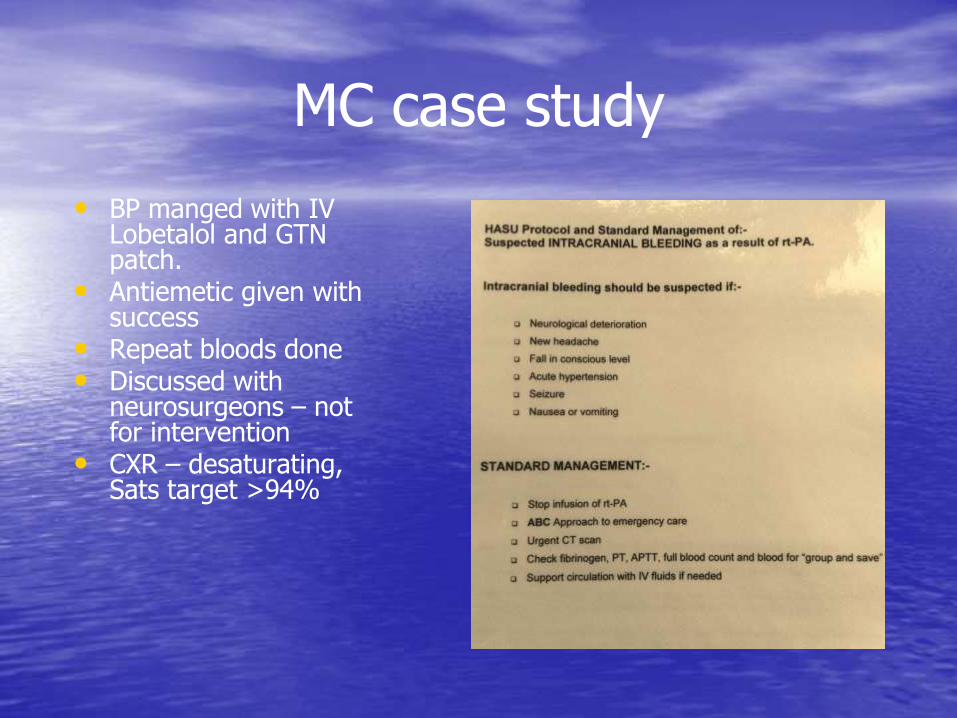
• BP manged with IV Lobetalol and GTN patch.
• Antiemetic given with success
• Repeat bloods done • Discussed with
neurosurgeons – not for intervention
• CXR – desaturating, Sats target >94%
MC case study
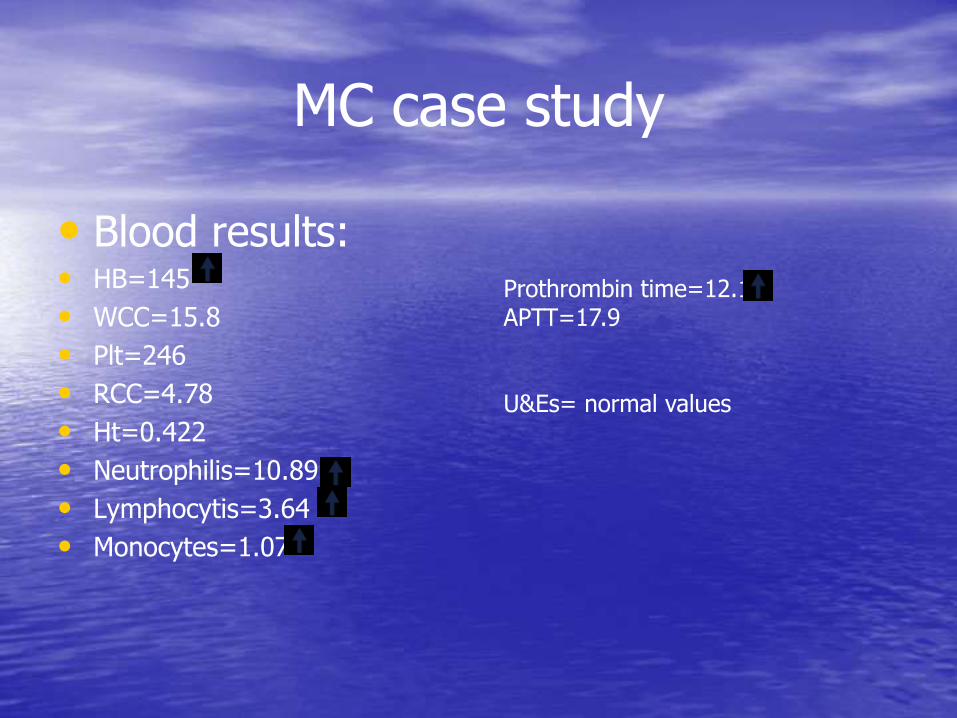
• Blood results: • HB=145
• WCC=15.8
• Plt=246
• RCC=4.78
• Ht=0.422
• Neutrophilis=10.89
• Lymphocytis=3.64
• Monocytes=1.07
Prothrombin time=12.1 APTT=17.9 U&Es= normal values
MC Case Study
• What would you do?
MC study case Abnormal blood results recommendations
• For major bleeding (e.g. intracerebral) within 48 h of administration of R-tpa we recommend:
• All patients should be discussed with haematology team urgently
• Stop infusion of fibrinolytic drugs and other antithrombotic drugs .
• Administer FFP 12 ml/kg.
• Administer intravenous tranexamic acid 1 g tds .
• If there is depletion of fibrinogen, administer cryoprecipitate or fibrinogen concentrate.
• Further therapy should be guided by results of coagulation tests
MC study case Outcome
• Catastrophic bleed
• DNR agreed with family
• MC passes away at 16:00h same day.
• May RIP
KW Case Study 82 year old gentleman
• 11:50 am while having lunch with his wife developed sudden L side weakness and dropped his cutlery.
• GCS= 13/15
• 50 minutes later arrives in NAU via emergency ambulance.
NIHSS=21
• severe L side weakness and inattention,
• complete heminopia
• partial facial palsy
• dysarthria
BP=153/65 mm/Hg, pulse=53, sat=94%
BM=5.3, not known diabetic
PMH: IHD, MI
KW Case Study
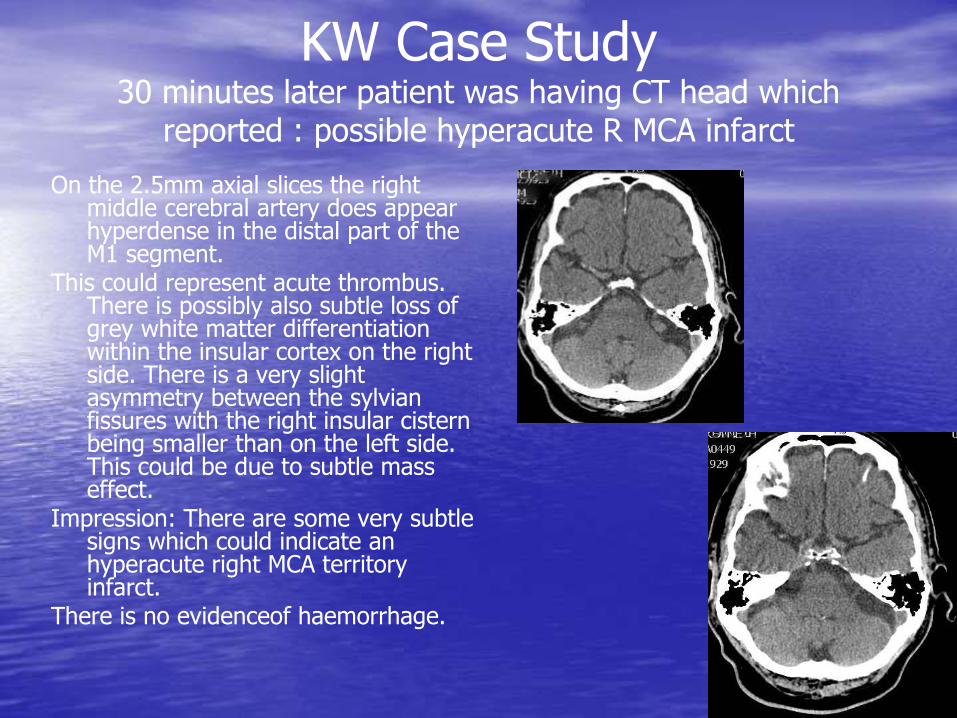
On the 2.5mm axial slices the right middle cerebral artery does appear hyperdense in the distal part of the M1 segment.
This could represent acute thrombus. There is possibly also subtle loss of grey white matter differentiation within the insular cortex on the right side. There is a very slight asymmetry between the sylvian fissures with the right insular cistern being smaller than on the left side. This could be due to subtle mass effect.
Impression: There are some very subtle signs which could indicate an hyperacute right MCA territory infarct.
There is no evidenceof haemorrhage.
KW Case Study 30 minutes later patient was having CT head which
reported : possible hyperacute R MCA infarct
KW Case Study
Would you thrombolyse?
KW Case Study
• Consultant decided to thrombolyse.
• 2 hours after thrombolysis patient improving
• NIHSS=13.
L limb weakness now mild
More alert
Improving dysarthria.
• BP=146/65 mm/Hg
• Blood results normal
KW Case Study
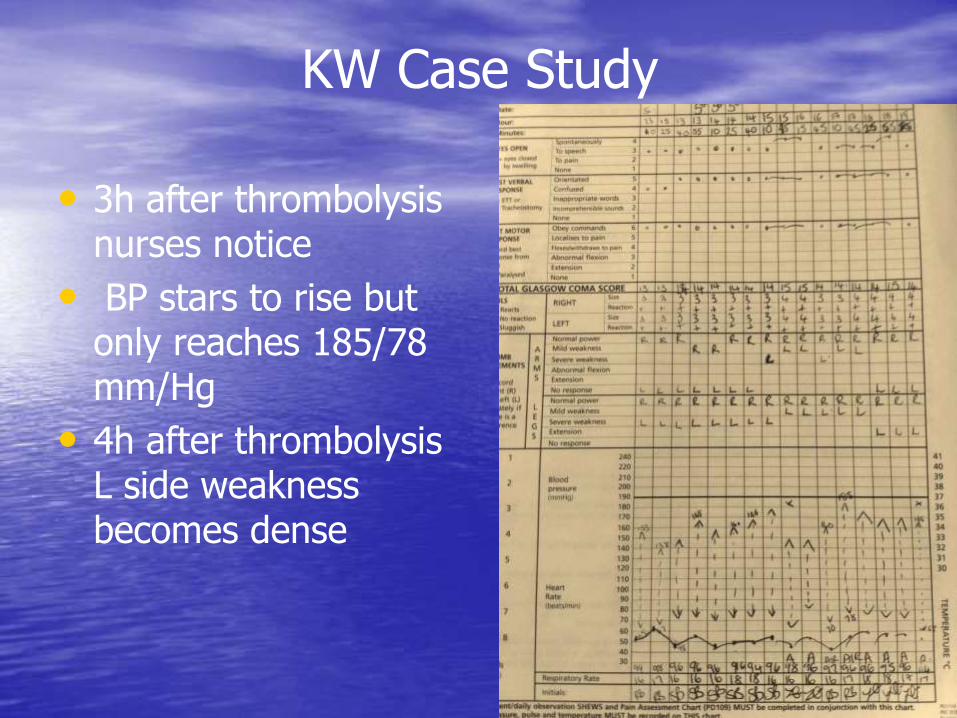
• 3h after thrombolysis nurses notice
• BP stars to rise but only reaches 185/78 mm/Hg
• 4h after thrombolysis L side weakness becomes dense
KW Case Study
• What would you do?
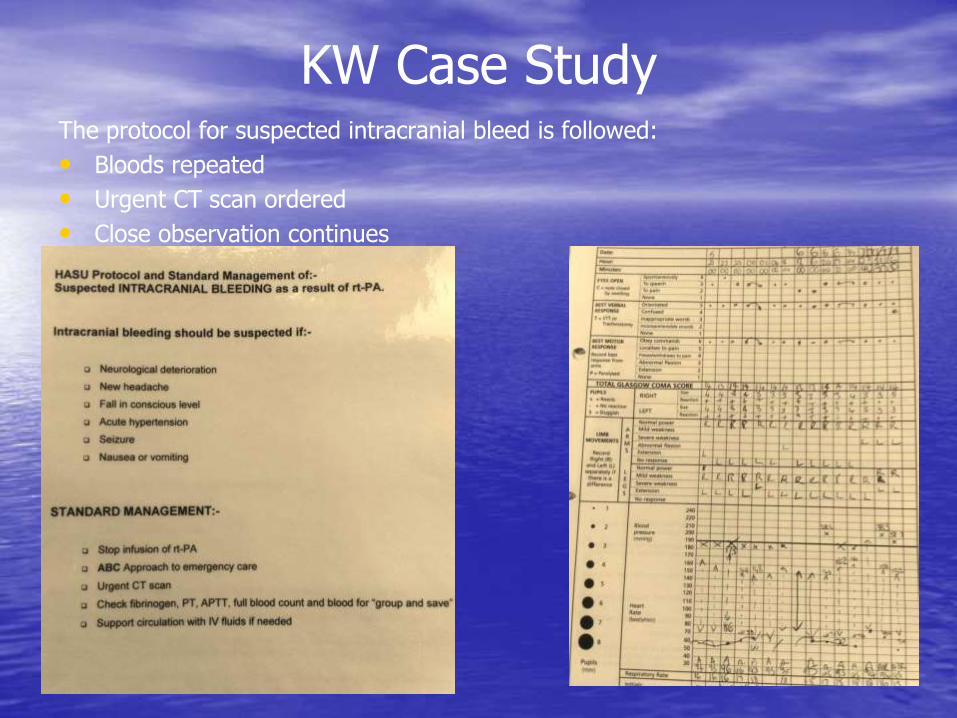
KW Case Study The protocol for suspected intracranial bleed is followed:
• Bloods repeated
• Urgent CT scan ordered
• Close observation continues
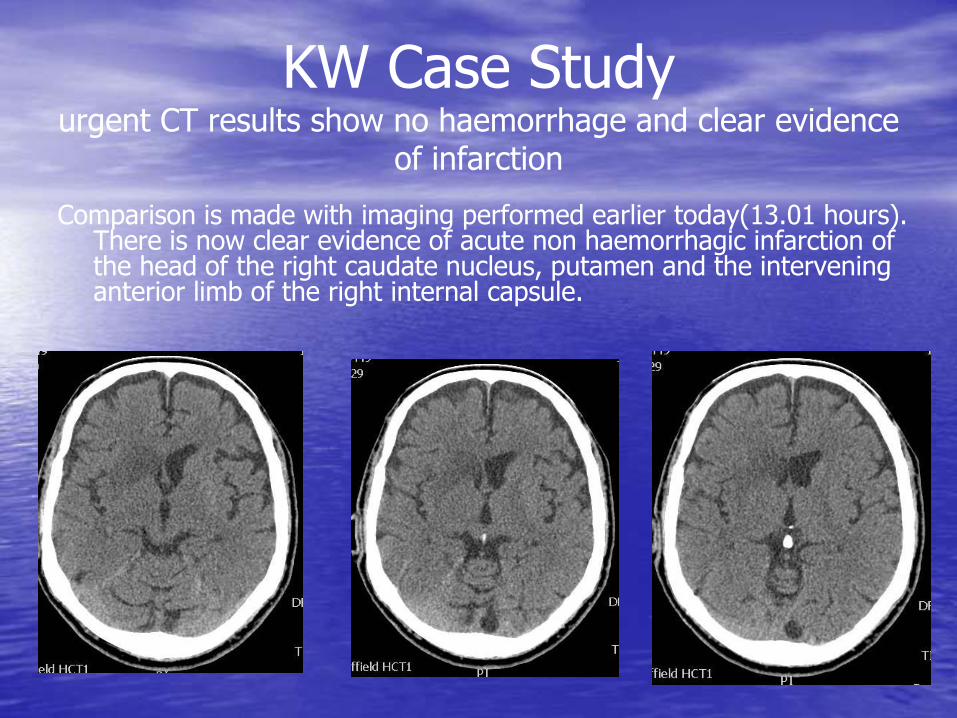
Comparison is made with imaging performed earlier today(13.01 hours). There is now clear evidence of acute non haemorrhagic infarction of the head of the right caudate nucleus, putamen and the intervening anterior limb of the right internal capsule.
KW Case Study urgent CT results show no haemorrhage and clear evidence
of infarction
• Patient’s condition continues to deteriorate
• NIHSS: 16, with L limbs back to severe weakness
• Fluctuating GCS: 10-13/15
• Patient agitated and failed dysphagia screen
• Repeat CT head done
KW Case Study 24h after thrombolysis
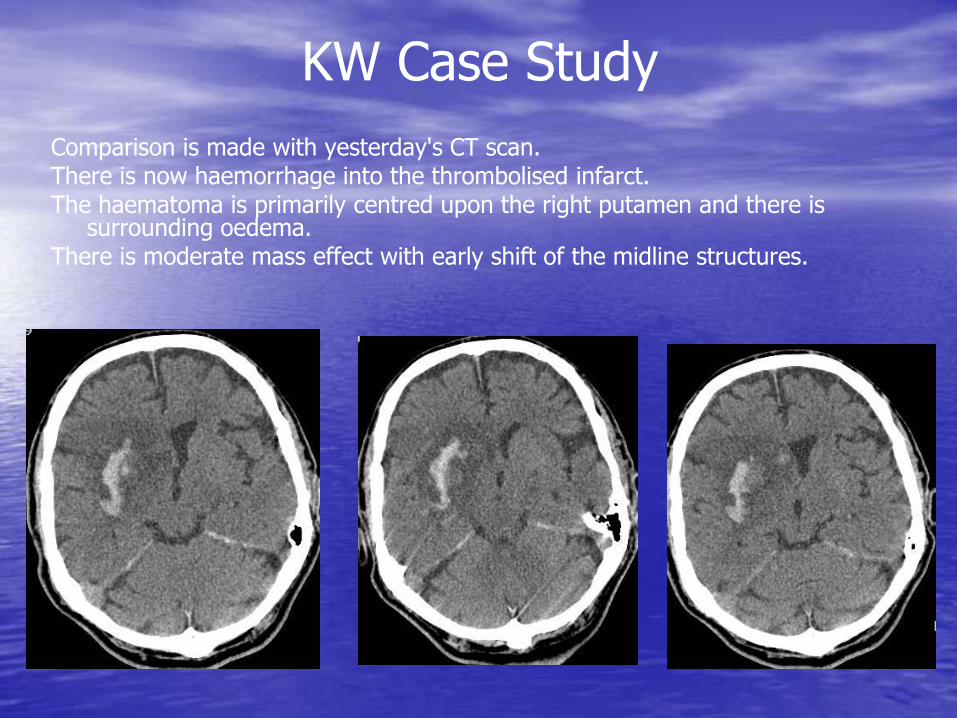
Comparison is made with yesterday's CT scan. There is now haemorrhage into the thrombolised infarct. The haematoma is primarily centred upon the right putamen and there is
surrounding oedema. There is moderate mass effect with early shift of the midline structures.
KW Case Study
• Not a candidate for surgical intervention due to his age and disability
• Next day patient becomes pyrexic and condition starts to deteriorate
• Blood cultures done and treatment started
• NG tube and CBD inserted
• Patient DNAR
• Transferred to ASU a few days later
KW Case Study
• Patients condition fluctuated a lot but he remains paraxial at all times
• 2 weeks later diagnosed with endocarditis
• 18 days later after thrombolysis patient died of complications.
• May he RIP
KW Case Study outcome
• Working together can be the key to improving stroke services
• Applying CONSISTENCY in medical treatment following our protocols and recognising the role and experience of the SNP and HASU nurses would be beneficial.
• Developing a single practice through out region to approach strokes with all their complications in the acute phase, with good protocols in place can also help.
• This will require good communication and information sharing.
• Thank you for your attention and participation.
Conclusions



















![Case Study of Stroke[1]](https://img.pdfslide.us/doc/110x75/5512d1a14a7959c4028b4ac1/case-study-of-stroke1.jpg)