Embed Size (px)
Citation preview

KEMENTRIAN PENDIDIKAN DAN KEBUDAYAANFAKULTAS KEDOKTERAN UNIVERSITAS RIAU
SMF/BAGIAN SARAFSekretariat : Gedung Kelas 03, RSUD Arifin Achmad Lantai 04
Jl. Mustika, Telp. 0761-7894000E-mail : [email protected]
P E K A N B A R U
I. PATIENT’S IDENTITY
Name Mr. S
Age 51 years 10 months
Gender Male
Address Matoluok Village, Bangkinang
Religion Moslem
Marital Status Married
Occupation Driver
Date of Admission December, 27th 2015
Medical Record 88 93 xx
II. ANAMNESIS
Autoanamnesis and alloanamnesis with patient’s wife (December, 28th
2015)
Chief Complaint
The weakness on the right limbs
Present Illness History
Since 4 hours before admission, the patient has complained the weakness on
his right limbs. At first, the patient has complained weakned on the right
limbs suddenly when he woke up in the morning. He never complained the
numbness before.
Furthermore, the patient’s speech became nonfluent or lisp.
No history of headache, vomiting, losing of vision and decreasing of
consciousness. No history of trauma.
Past Illness History
1

Patient had an uncontrolled hypertension since 6 years ago
Unknown history of Diabetes mellitus and Cardiovascular disease
No history of obesity
Family Illness History
His father had a hypertension
His nephew had a stroke
No history of Diabetes mellitus
No history of Cardiovascular disease
Socioeconomic History
He is a smoker since 30 years ago
He never consumed alcohol and drugs
Dietary habit is irregular
THE SUMMARY OF ANAMNESIS
Mr. S, 51 years old admitted to the hospital on December, 27th 2015. The
patient has complained the sudden weakness on the right limbs since 4 hours
before admission. The patient’s speech nonfluent or lisp. Patient had an
uncontrolled hypertension since 6 years ago, his family had a history of
hypertension and stroke. He is a smoker since 30 years ago and dietary habit is
irregular.
III. PHYSICAL EXAMINATION
A. General status
Blood Pressure : 210/90 mmHg
Heart Rate : 88 bpm
Respiratory Rate : 20 times per minute
Temperature : 36,5°C
Weight : 70 kg Height : 165 cm
2

B. Neurological status
1) Consciousness : Alertness GCS : E4M6V5
2) Cognitive Function : Normal
3) Neck Stiffness : Negative
4) Cranial Nerves
1. Cranial nerve I (Olfactory)Right Left Interpretation
Sense of Smell Normal Normal Normal
2. Cranial nerve II (Optic)Right Left Interpretation
Visual Acuity Normal Normal
NormalVisual Fields Normal NormalColour Recognition Normal Normal
3. Cranial nerve III (Oculomotor)Right Left Interpretation
PtosisPupil Shape SizeExtraocular movementsPupillary reactions to light Direct Indirect
(-)
RoundΦ3 mmNormal
(+)(+)
(-)
RoundΦ3 mmNormal
(+)(+)
Normal
4. Cranial nerve IV (Trochlear)Right Left Interpretation
Extraocular movements Normal Normal Normal
5. Cranial nerve V (Trigeminal)Right Left Interpretation
MotorSensoryCorneal reflex
NormalNormal
(+)
NormalNormal
(+)Normal
6. Cranial nerve VI (Abducens)Right Left Interpretation
Extraocular movements
Normal(-)
Normal(-)
Normal
3

StrabismusDeviation (-) (-)
7. Cranial nerve VII (Facial)Right Left Interpretation
TicMotor- corners of
the mouth- folds
nasolabialis- frowning- Raise
eyebrows- Closed eyes
Sense of TasteChvostek Sign
(-)
Decrease
Shallow
(+)(+)
(+)(+)(-)
(-)Normal
(+)
(+)
(+)(+)
(+)(+)(-)
Paresis N VII dextra central type
8. Cranial nerve VIII (Acoustic)Right Left Interpretation
Sense of Hearing (+) (+) Normal
9. Cranial nerve IX (Glossopharyngeal)Right Left Interpretation
Pharyngeal ArchSense of TasteGag Reflex
Normal Normal
(+)
NormalNormal
(+)Normal
10. Cranial nerve X (Vagus)Right Left Interpretation
Pharyngeal ArchDysphonia
Normal (-)
Normal
(-)Normal
11. Cranial nerve XI (Accessory)Right Left Interpretation
MotorTrophy
NormalEutrophy
NormalEutrophy Normal
4

12. Cranial nerve XII (Hypoglossal)Right Left Interpretation
MotorTrophyTremorDysarthria
Tongue compelledEutrophy
(-)(+)
NormalEutrophy
(-)(+)
Parese N XII dextra
IV. MOTOR SYSTEM
Right Left Interpretation
Upper Extremity Strength
DistalProximal
Tone Trophy Involuntary movements Clonus
44
Normal Eutrophy
(-)(-)
55
NormalEutrophy
(-)(-)
Lower Extremity Strength
DistalProximal
Tone Trophy Involuntary movements Clonus
44
Normal Eutrophy
(-)(-)
55
NormalEutrophy
(-)(-)
Hemiparesis dextra (UMN
Type)
Body Trophy Involuntary movements Abdominal Reflex
Eutrophy(-)(-)
Eutrophy(-)(-)
Normal
V. SENSORY SYSTEMRight Left Interpretation
Touch
Pain
Temperatur
Propioseptif
(+)
(+)
(+)
(+)
(+)
(+)
(+)
(+)
Normal
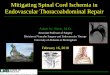
VI. REFLEX
Right Left Interpretation
5

PhysiologicBicepsTricepsKneeAnkle
(+)(+)(+)(+)
(+)(+)(+)(+)
Physiologic reflex (+)
Pathologic Babinsky Chaddock Hoffman Tromer Openheim SchaeferPrimitive Reflex Palmomental Snout
(-)(-)(-)(-)(-)
(-)(-)
(-)(-)(-)(-)(-)
(-)(-)
Pathologic reflex (-)
Primitive Reflex (-)
VII. COORDINATION
Right Left InterpretationPoint to point movementsWalk heel to toeGaitTandemRomberg
NormalNormalNormalNormalNormal
NormalNormalNormalNormalNormal
Normal
VIII. AUTONOMY SYSTEM
Urination : Normal
Defecation : Normal
IX. Others Examination
a. Laseque : Unlimited
b. Kernig : Unlimited
c. Patrick : -/-
d. Kontrapatrick : -/-
e. Valsava test : -
f. Brudzinski : -
GAJAH MADA ALGORITHM
Loss of consciousness (-), headache (-), pathology reflex (-) Non-
Hemorrhagic stroke
6

SIRIRAJ SCORE
(2.5 x level of consciousness (0)) + (2 x Vomit (0)) + (2 x headache (0)) + (0.1 x
diastolic (100)) – (3x atheroma factor (1)) – 12 = - 5 Non-Hemorrhagic stroke
X. THE SUMMARY OF EXAMINATION
General Status : Hypertension (210/90 mmHg)
Cognitive Function : Normal
Neck Stiffness : Negative
Cranial Nerves : Parese N VII dextra central typeParese N XII dextra
Motoric : Hemiparesis dextra (UMN Type)
Sensory : Normal
Coordination : Normal
Autonomy : Normal
Reflex : Normal
Gajah Mada Algorithm: Non-hemorrhagic stroke
Siriraj Score : Non-hemorrhagic stroke
XI. WORKING DIAGNOSIS
CLINICAL DIAGNOSIS : Stroke
TOPICAL DIAGNOSIS : Carotid system
ETIOLOGICAL DIAGNOSIS : Ischemic stroke
DIFFERENTIAL DIAGNOSIS : Hemorrhagic stroke
XII. SUGGESTION EXAMINATION
Blood routine
Blood chemistry
Electrocardiography
Chest X-ray
Head CT Scan
7
XIII. SUGGESTION FOR MANAGEMENT THERAPY
General
- Immobilization and head up 20-30
- Monitoring of vital sign
- Medical rehabilitation
- IVFD (30ml/kgBB/day) Ringer Lactate 20 dpm
Special
- Citicoline 3 x 500 mg per IV
- Aspilet 2 x 80 mg per oral
- Folic acid 2 x 400 µg tab per oral
XIV. LABORATORY AND RADIOLOGY FINDINGS
1. Blood Routine (December, 27th 2015)
- Hemoglobin : 14,1 g/dL
- Hematocrit : 42,9 %
- Leukocyte : 6.700/mm3
- Thrombocyte : 280.000/mm3
Interpretation: Normal
2. Blood Chemistry
(December, 29th 2015)
- Glucose : 112 mg/dL
- Choresterol : 295 mg/dL
- HDL : 70,9 mg/dL
- Triglyceride : 107 mg/dL
- Uric acid : 7,6 mg/dL
- LDL Cholesterol : 203 mg/dL
- Ureum : 32 mg/dL
- Creatinin : 1,50 mg/dL
- AST : 23 U/L
- ALT : 17 U/L
- Albumin : 4,07 g/dL
8

3. Electrocardiography
Interpretation : synus rithm, no abnormal morphology waves.
4. Head CT Scan without contrast
Interpretation: ischemic on the left paraventricel hemisphere cerebri
XV. FINAL DIAGNOSIS
9

- Ischemic stroke
- Hypertension
- Hyperlipidemia
FOLLOW UP
December, 29th 2015
S : weakness of the right limbs, lisp.
O :
GCS E4M6V5
Blood Pressure180/90 mmHg
Heart Rate 80 bpm
Respiratory Rate 20 tpm
Temperature 36,8°C
Cognitive Function : Normal
Neck Stiffness : Negative
Cranial Nerves : Paresis N VII dextra central type
Paresis N XII dextra
Motoric : Right extremity hemiparesis
Sensory : Normal
Coordination : Normal
Autonomy : Normal
Reflex : Normal limit
A : Ischemic stroke + Hypertension
P :
IVFD RL 20 dpm
Citicolin 3 x 500 mg per IV
Aspilet 2 x 80 mg per oral
Folic acid 2 x 400 µg per oral
December, 30st 2015
S : weakness of the right extremity, lisp.
10

O :
GCS E4M6V5
Blood Pressure170/100 mmHg
Heart Rate 76 bpm
Respiratory Rate 20 tpm
Temperature 36,5°C
Cognitive Function: Normal
Neck Stiffness : Negative
Cranial Nerves : Paresis N VII dextra central type
Paresis N XII dextra
Motoric : Right extremity hemiparesis
Sensory : Normal
Coordination : Normal
Autonomy : Normal
Reflex : Normal
A : Ischemic stroke + Hypertension + Hyperlipidemia
P :
IVFD RL 20 dpm
Citicolin 3 x 500 mg per IV
Aspilet 2 x 80 mg tab per oral
Folic acid 2 x 400 µg tab per oral
Amlodipine 1 x 10 mg per oral
Simvastatin 1 x 10 mg per oral
11

Discussion
ISCHEMIC STROKE
1. Definition
Stroke is applied to a sudden focal neurologic syndrome, specifically the
type due to cerebrovascular disease. The term cerebrovascular disease designates
any abnormality of the brain resulting from a pathologic process of the blood
vessels. Pathologic process is given an inclusive meaning namely, occlusion of
the lumen by embolus or thrombus, rupture of a vessel, an altered permeability of
the vessel wall, or increased viscosity or other change in the quality of the blood
flowing through the cerebral vessels. The vascular pathologic process may be
considered not only in its grosser aspects embolism, thrombosis, dissection, or
rupture of a vessel but also in terms of the more basic or primary disorder, i.e.,
atherosclerosis, hypertensive arteriosclerotic change, arteritis, aneurysmal
dilation, and developmental malformation. Equal importance attaches to the
secondary parenchymal changes in the brain resulting from the vascular lesion.
These are of two main types ischemia, with or without infarction, and hemorrhage
and unless one or the other occurs, the vascular lesion usually remains silent. The
only exceptions to this statement are the local pressure effects of an aneurysm,
vascular headache (migraine, hypertension, temporal arteritis), multiple small
vessel disease with progressive encephalopathy (as in malignant hypertension or
cerebral arteritis), and increased intracranial pressure (as occurs in hypertensive
encephalopathy and venous sinus thrombosis). Also, persistent acute hypotension
may cause ischemic necrosis in regions of brain between the vascular territories of
cortical vessels, even without vascular occlusion.1
More than any other organ, the brain depends from moment to moment on
an adequate supply of oxygenated blood. Constancy of the cerebral circulation is
assured by a series of baroreceptors and vasomotor reflexes under the control of
12

centers in the lower brainstem. Obstruction of an artery by thrombus or embolus is
the usual cause of focal ischemic damage, but failure of the circulation and
hypotension from cardiac decompensation or shock, if severe and prolonged
enough, can produce focal as well as diffuse ischemic changes.1
Focal cerebral ischemia differs fundamentally from global ischemia. In the
latter state, if absolute, there is no cerebral blood flow of the entire brain and
irreversible destruction of neurons occurs within 4 to 8 min at normal body
temperature. In focal ischemia, there is nearly always some degree of circulation
(via collateral vessels), permitting to a varying extent the delivery of oxygenated
blood and glucose.
The effects of a focal arterial occlusion on brain tissue also vary depending
on the location of the occlusion in relation to available collateral and anastomotic
channels. If the obstruction lies proximal to the circle of Willis (toward the heart),
the anterior and posterior communicating arteries of the circle are often adequate
to prevent infarction. In occlusion of the internal carotid artery in the neck, there
may be anastomotic flow from the external carotid artery through the ophthalmic
artery or via other smaller externalinternal connections. With blockage of the
vertebral artery, the anastomotic flow may be via the deep cervical, thyrocervical,
or occipital arteries or retrograde from the other vertebral artery. If the occlusion
is in the stem portion of one of the cerebral arteries, i.e., distal to the circle of
Willis, a series of meningeal interarterial anastomoses may carry sufficient blood
into the compromised territory to lessen (rarely to prevent) ischemic damage.
There is also a capillary anastomotic system between adjacent arterial branches,
and although it may reduce the size of the ischemic field, particularly of the
penetrating arteries, it is usually not significant in preventing infarction. Thus,
in the event of occlusion of a major arterial trunk, the extent of infarction ranges
from none at all to the entire vascular territory of that vessel. Between these two
extremes are all degrees of variation in the extent of infarction and its degree of
completeness.1
Additional ischemia-modifying factors determine the extent of necrosis.
The speed of occlusion assumes importance; gradual narrowing of a vessel allows
time for collateral channels to open. The level of blood pressure may influence the
13

result; hypotension at a critical moment may render anastomotic channels
ineffective. Hypoxia and hypercapnia are presumed to have deleterious effects.
Altered viscosity and osmolality of the blood and hyperglycemia are potentially
important factors but difficult to evaluate. Finally, anomalies of vascular
arrangement (of neck vessels, circle of Willis, and surface arteries) and the
existence of previous vascular occlusions must influence the outcome.1
The specific neurologic deficit obviously relates to the location and size of
the infarct or focus of ischemia. The territory of any artery, large or small, deep or
superficial, may be involved. When an infarct lies in the territory of a carotid
artery, as would be expected, unilateral signs predominate: hemiplegia,
hemianesthesia, hemianopia, aphasia, and agnosias are the usual consequences. In
the territory of the basilar artery, the signs of infarction are frequently bilateral
and occur in conjunction with cranial nerve palsies and other segmental brainstem
and cerebellar signs; quadriparesis, hemiparesis, and/or unilateral or bilateral
sensory impairment are typical, coupled with diplopia, dysarthria, and vertigo in
various combinations.1
2. Risk factor
According to the American Heart Association (AHA), the risk factors of
stroke are divided into two, that are not modifiable risks factors and modifiable
risk factors. Not modifable risk factors include: age, sex, low birth weight, race or
ethnicity, and genetic factors. Modifiable risk factors include: hypertension,
smoking, diabetes, nutritional imbalance, lack of physical activity, alcohol
consumption, and drug abuse. Incidence of stroke can occur with one or more risk
factors (multifactor).1-3
Table 3. Stroke risk factors1-3
Not Modifable Modifable
1. Age
2. Gender
3. Genetic
4. Ethnic
1. Stroke history 10. Smoking
2. Hypertension 11. Alcohol
3. Heart disease 12. Drug abuse
4. Diabetes melitus 13. Hyperhomosisteinemia
5. Carotid stenosis 14. Antibody anti fosfolipid
6. TIA 15. Hyperurisemia
14

7. Hypercholesterolemia 16. Elevation of hematocrit
8. Oral contraception 17. Elevation of fibrinogen
9. Obesity
3. Clinical Manifestation
The specific neurologic deficit obviously relates to the location and size of
the infarct or focus of ischemia. The territory of any artery, large or small, deep or
superficial, may be involved. When an infarct lies in the territory of a carotid
artery, as would be expected, unilateral signs predominate: hemiplegia,
hemianesthesia, hemianopia, aphasia, and agnosias are the usual consequences. In
the territory of the basilar artery, the signs of infarction are frequently bilateral
and occur in conjunction with cranial nerve palsies and other segmental brainstem
and cerebellar signs; quadriparesis, hemiparesis, and/or unilateral or bilateral
sensory impairment are typical, coupled with diplopia, dysarthria, and vertigo in
various combinations.1,2
4. Management
Stroke patients should be handled by a multidisciplinary team.
Management stroke be done by improving the general state of the patient, treat the
risk factors, and prevent complications.3-6
4.1 Hyperacute stadium
Action at this stadium is done at the Emergency Room, the aim is to
prevent the widespread of brain tissue damaging. At this stage, patients were
given oxygen 2 L / min and crystalloid/colloid fluid, avoid administration of
dextrose. Brain CT scan examination, electrocardiography, chest X-ray, complete
peripheral blood and platelet count, prothrombin time / INR, APTT, blood
glucose, blood chemistry (including electrolytes), and if hypoxia, do the blood gas
analysis. Other actions in the Emergency Room are providing mental support to
patients and provide an explanation to the family to remain calm.3-6
4.2 Acute stadium
4.2.1 General treatment
15

Place the patient’s head in 30o positions, head an chest in a field, change
the sleep position every 2 hours. Mobilization began gradually when
hemodynamically stable. Furthermore, free the airway, give oxygen 1-2 liters /
min. If necessary, intubation. Fever overcome with compresses and antipyretic,
then look for the cause, when the bladder is full, emptied (preferably with
intermittent catheters).3-6
Fluid nutrition with 1500-2000 isotonic cristalloid or colloid and
electrolyte as needed, avoid fluids containing glucose or isotonic saline. Nutrition
orally only if swallowing function well, if there is swallowing disorders or
decreased consciousness, nasogastric tube is recommended. 3-6
Blood glucose levels > 150 mg% should be corrected with continuous
intravenous drip insulin during 2-3 days. Hipoglikemia (blood glucose < 60 mg%
or < 80mg% with symptoms) should be corrected immediatelywith dextrose 40%
iv until return to normal and the cause must be sought. 3-6
Headache, nausea, and vomiting treated according to the symptoms. Blood
preassure doesn’t need taken down immediately, except when the systolic
pressure ≥ 220 mmHg and diastolic pressure ≥120 mmHg, Mean Arterial Blood
Pressure (MAP) ≥ 130 mmHg (the two measurements with an interval of 30
minutes), or obtained acute myocardial infarction, congestive heart failure as well
as kidney failure. Maximal blood pressure reduction was 20%, and the
recommended drugs are sodium nitroprusside, alpha-beta receptor blockers, ACE
blockers, or antagonists calsium. 3-6
If hypotension occurs, the systolic pressure ≤ 90 mmHg, diastolic ≤70 mm
Hg, the patient should be given 250 mL of 0.9% NaCl for 1 hour, followed by 500
mL for 4 hours and 500 mL for 8 hours or until hypotension treated. If not
corrected, that is systolic blood pressure still <90 mmHg, dopamine 2-20 mcg / kg
/ minute can be given until the systolic blood pressure ≥110 mmHg. 3-6
If there is seizure, give diazepam 5-20 mg iv slowly for 3 minutes, the
maximum dosage is 100 mg per day, followed by oral administration of
anticonvulsants such as phenytoin, carbamazepine. If the seizure appeared after 2
weeks, given orally long-term anticonvulsant. 3-6
16

If there is an increased of intracranial pressure, bolus mannitol were given
an of 0.25 to 1 g / kg per 30 minutes intravenously, and if rebound phenomenon
suspected, or general condition deteriorated, followed by 0,25g / kg per 30
minutes every 6 hours for 3-5 days. Monitoring of the osmolarity should be
performed (<320 mmol), alternatively can be administered hypertonic solutions
(NaCl 3%) or furosemid. 3-6
4.2.2 Special treatment
The goal is to reperfusion by administration of antiplatelet agent such as
aspirin and anticoagulant, or with trombolytic rt-PA (combinant tissue
Plasminogen Activator), and neuroprotective agent, such as citicoline or
piracetam. 3-6
4.3 Subacute Stadium
Medical measures may include cognitive therapy, behavior, swallowing,
speech therapy, and bladder training (including physical therapy). Given the long
course of the disease, it takes a special intensive treatment of post-stroke in the
hospital with the goal of independence of the patient, understand, comprehend and
implement primary and secondary prevention programs.6
Subacute phase treatment:6
- Continuing the appropriate treatment of acute conditions before
- The management of complications
- Restoration / rehabilitation (as needed of patients), which is
physiotherapy, speech therapy, cognitive therapy, and occupational
therapy
- Secondary Prevention
- Family education and discharge planning
THE BASIC OF DIAGNOSIS
1. Basic of clinical diagnosis
From the history taking, a 51 years old man had a sudden weakness on the
right arm and leg (Hemiparesis). And his speech became nonfluent. No history of
17

trauma. It is consistent with the WHO’s definition that clinical symptoms of stroke
is cerebral disorders, either focal or global attack in 24 hours or more, no illness is
found other than vascular disorders. And elderly is a risk factor of stroke.
2. Basic of topical diagnosis
Carotid system had been considered in this patient because there is
hemiparesis, paresis N. VII dextra central type, and paresis N. XII dextra.
Hemiparesi, and paresis N. VII dextra central type and paresis N. XII dextra is
symptoms of middle cerebral artery occlusion. Middle cerebral artery is the
greatest branch of internal carotid artery. From the physical examination there is
right hemiparesis, so the lesion is on the left hemisphere because a lesion in one
side of carotid system will lead to contralateral neurological deficit. and there is
parese N.XII dextra, so the lession thought in the left hemisphere.
3. Basic of etiological diagnosis
Basic etiological diagnosis of this patient has been leaded to ischemic
stroke, because on this patient there are no losing of consciousness, no projectil
vomiting, no headache, no increasing of diastolic blood pressure and hemiparesis.
It is also supported by Siriraj score and Gajah Mada Algorithm that give the
impression of the non-hemorrhage stroke.
4. Basic of differential diagnosis
The gold standard examination for diagnosing the non hemorrhagic or
hemorrhagic stroke is CT Scan. The consideration of the hemorrhagic stroke
because of it almost has the same manifestation, like the immediate onset, the
patient was not in severe activity, and there is neurological deficit.
5. Basic of secondary diagnosis
From history taking, this patient had uncontrolled hypertension since 6
years ago and from the physical examintaion the blood pressure is 210/90 mmHg.
This is appropriate with JNC 8 criteria that in patient’s <60 years old the diagnose
of hypertension is when the sistolic blood pressure ≥ 140 mmHg or the diastolic
blood pressure ≥ 90 mmHg. Hyperlipidemia refers to increased levels of lipids
(fats) in the blood, including an triglycerides. And from history sosioeconomic
patient had dietary habit irregular, overweight, and from laboratory finding
18

cholesterol total increased (295 mg/dL) and LDL cholesterol is 203 mg/dL this
appropriate with Hyperlipidemia.
6. Basic of final diagnosis
The final diagnosis of this patient is ischemic stroke. This diagnosis is
based on history taking, physical examination and supporting examination.
7. Basic of supporting examination
1. Laboratory to find the risk factor for stroke and general condition of
patient.
2. Head CT-scan to know the final diagnose from the location and the wide
of the lesion.
8. Basic of treatment
a. The aim of Bed rest with head position elevated 300 is to maintain the
adequate circulation to the brain.
b. The aim of IVFD (30ml/kgbb/day) Ringer Lactate 20 dpm is to
maintain the euvolemic condition and glucose level needed.
c. The aim of Inj aspilet 2 x 80 mg is to prevent from recurrent stroke attack
d. The aim of Inj citicoline 2 x 500 mg is as the neuroprotector
e. The aim of amlodipine 1 x 10 mg is for control hypertension
f. The aim of simvastatin 1 x 10 mg is for control cholesterol
19

REFFERENCE
1. Ropper AH, Brown RH. Adams and Victor’s Principles of Neurology. 8th Ed. New York: McGraw-Hill Companies, Inc. 2005. Chapter 34, Cerebrovascular Disease; p.660-770.
2. Rumantir CU. Gangguan Peredaran Darah Otak. Pekanbaru: SMF Saraf RSUD Arifin Achmad/FK UNRI. Pekanbaru. 2007.
3. Warlow C, van Gijn J, Dennis M, Wardlaw J, Bamford J, Hankey G. Stroke Practical Management. 3th Ed. 2008. Blackwell Publishing. p.39-40.
4. Guideline Stroke Tahun 2011. Pokdi Stroke. Perhimpunan Dokter Spesialis Saraf Indonesia (PERDOSSI). Jakarta. 2011.
5. Powers WJ. AHA/ASA Guideline 2015 AHA/ASA Focused Update of the 2013 Guidelines for the Early Management of Patients With Acute Ischemic Stroke Regarding Endovascular Treatment. AHA journals. 2015;46:000-000.
6. Setyopranoto I. Stroke: Gejala dan Penatalaksanaan. CDK 185/Vol.38 no.4/Mei-Juni 2011; hal.247-250.
20
21