Embed Size (px)
Citation preview
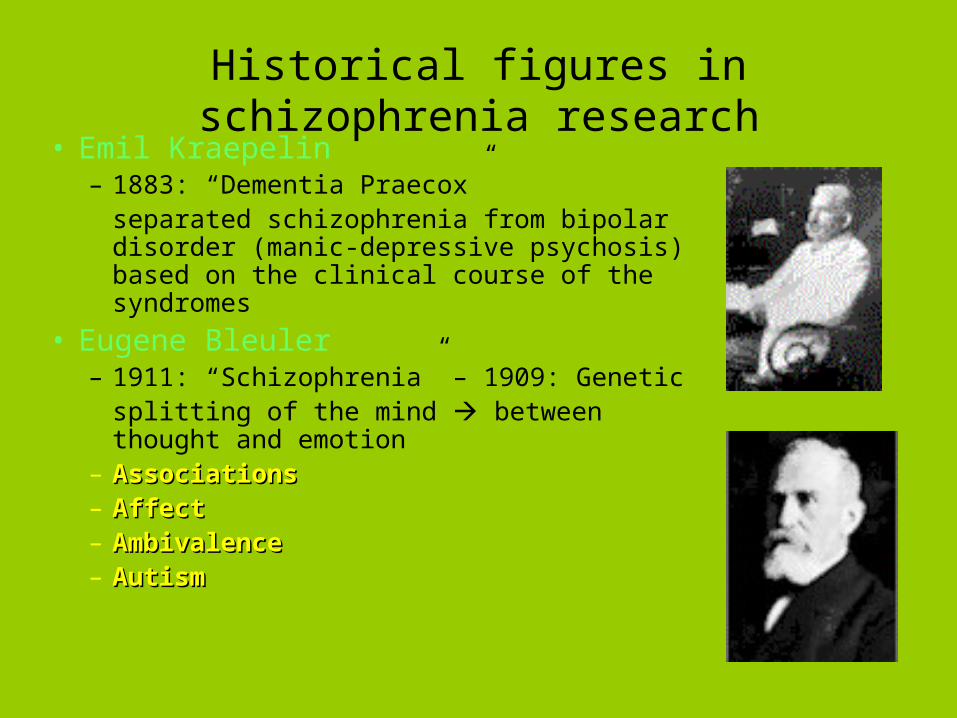
Historical figures in schizophrenia research• Emil Kraepelin
– 1883: “Dementia Praecox”separated schizophrenia from bipolar disorder (manic-depressive psychosis) based on the clinical course of the syndromes
• Eugene Bleuler– 1911: “Schizophrenia” – 1909: Genetic
splitting of the mind between thought and emotion
– AssociationsAssociations– AffectAffect– AmbivalenceAmbivalence– AutismAutism
Epidemiology
• Prevalence ~1%; male = female
Right now over 2 million adult Americans have schizophrenia
• Seen in all cultures at similar frequency • Onset usually late adolescence to young
adulthood, earlier in males than females
(reactive: leaving home, loss of parent, 1st sex experience)
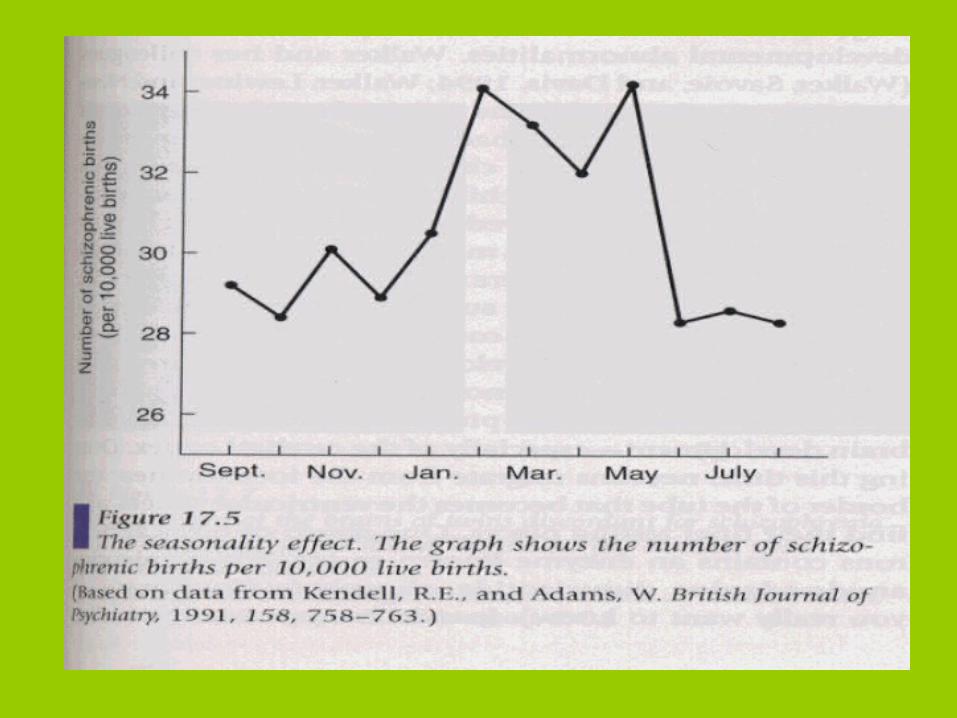
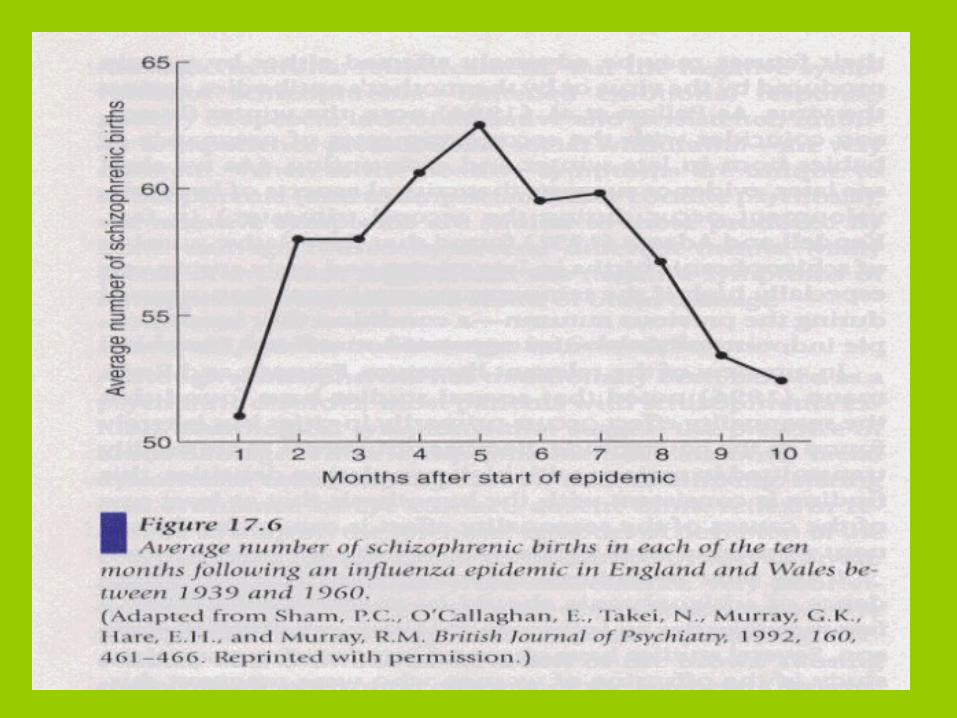
• Increased chance of being born in the winter or early spring
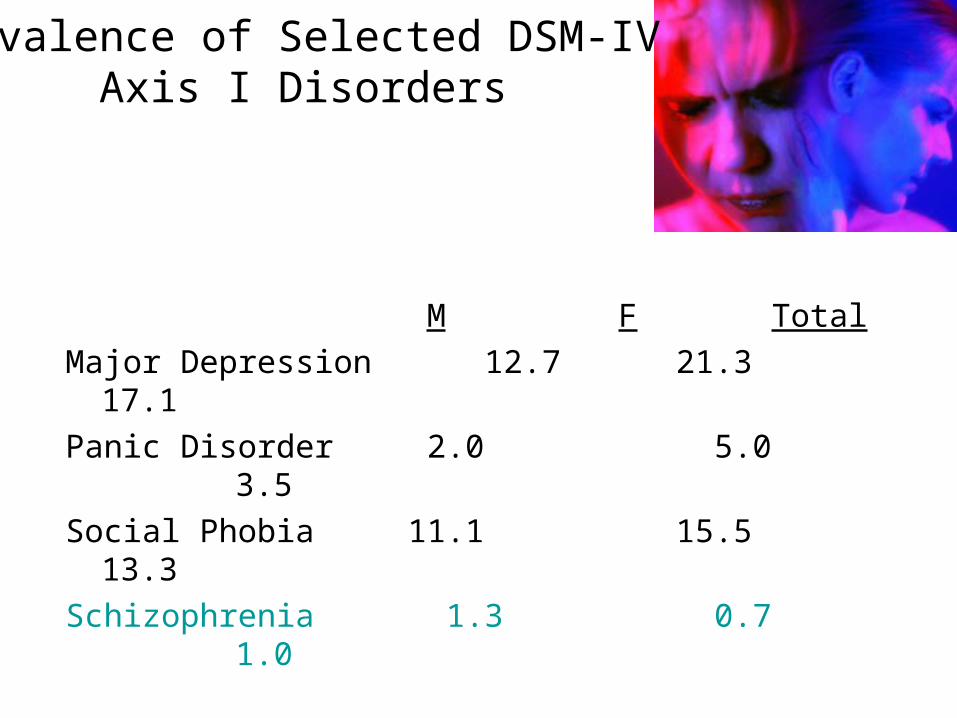
Prevalence of Selected DSM-IV Axis I Disorders
M F Total
Major Depression 12.7 21.3 17.1
Panic Disorder 2.0 5.0 3.5
Social Phobia 11.1 15.5 13.3
Schizophrenia 1.3 0.7 1.0
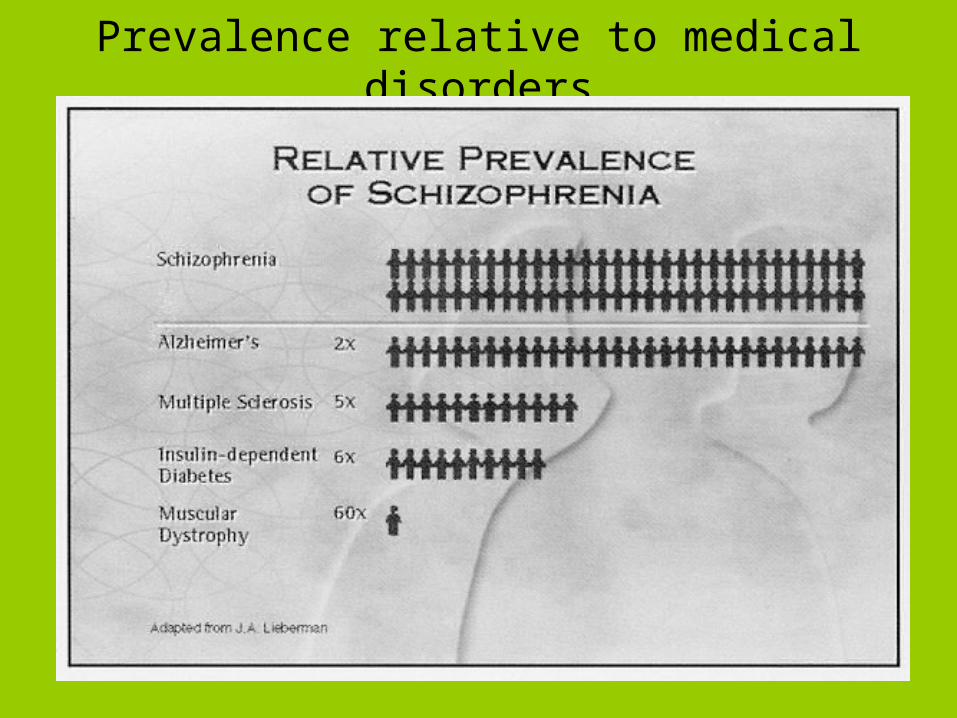
Prevalence relative to medical disorders
Schizophrenics have:
• Increased mortality rate from accidents and natural causes:– life span is shortened by about a decade– some under-diagnosis of medical illness is present
• ~10-15% suicide; ~50% attempt– early in illness and young age– high premorbid function– depression– the latter two often contributing to demoralization
• Illness seems concentrated in urban settings, i.e., it is somewhat correlated with population density in larger cities
• Illness seems concentrated in lower socioeconomic classes (1/3 of homeless)
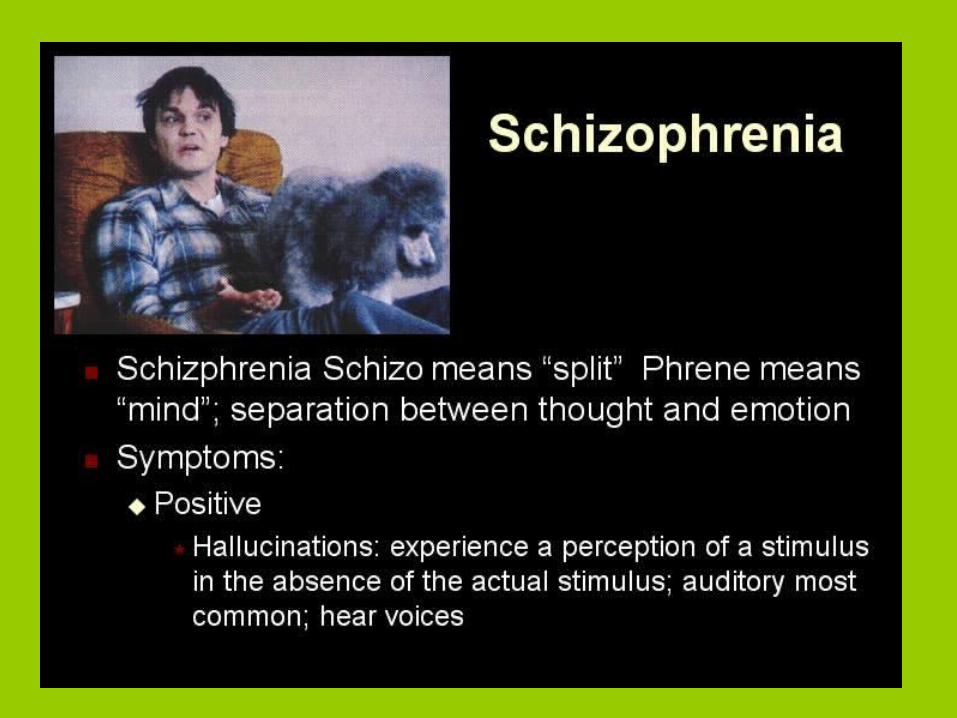
Diagnosis of Schizophrenia
A. Characteristic symptoms: > 2 of 5 (active phase symptoms – Criterion A)
(1) delusions
(2) hallucinations
(3) disorganized speech (incoherence-”word salad”)
(4) grossly disorganized or catatonic behavior
(5) negative symptoms, i.e., affective flattening, alogia, or avolition
* bizarre delusions or running commentary voices or voices conversing with each other
Diagnosis of Schizophrenia
B. Social/occupational dysfunction (50% unemployed)
C. Duration: at least 6 mo. (include at least 1 month of symptoms from Criterion A)
D&E. Mood Disorder, Substance/general medical condition exclusion
F. No Pervasive Developmental Disorder: (ex:Autism) (only if prominent delusions or hallucinations are also present for at least a month)
Subtypes
– Catatonic• Catatonic behavior dominates (catalepsy-muscle
rigidity/agitation)• Less common nowadays
– Disorganized (hebephrenic)• Disorganized speech, behavior, and affect (flat or
inappropriate)
– Paranoid• Delusions and/or auditory hallucinations• Not limited to persecutory themes• Tends to have a later onset and better course
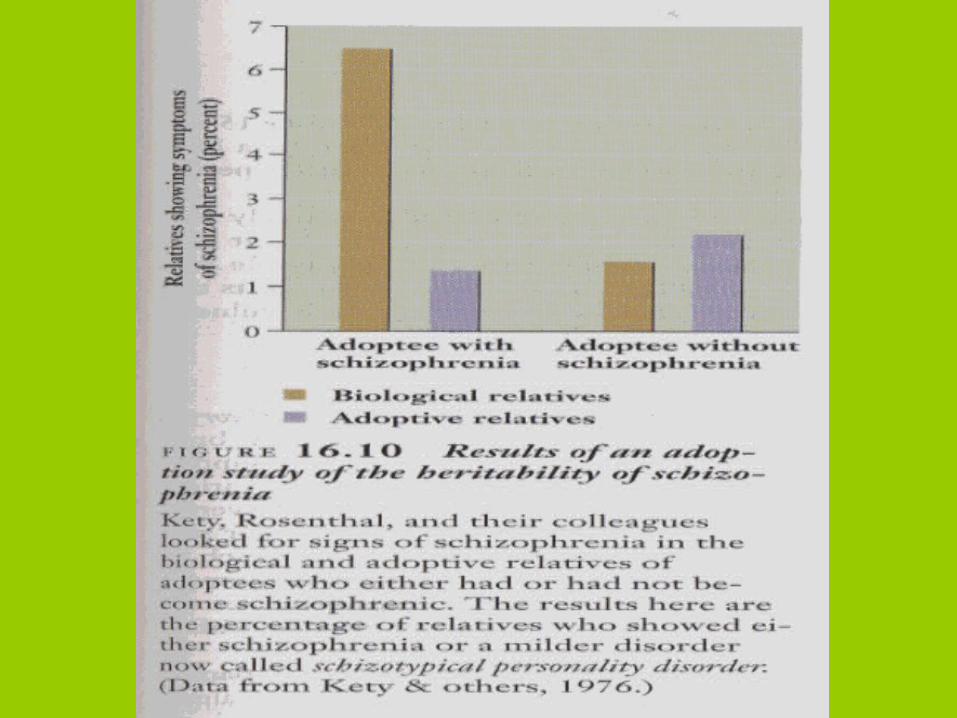
Etiology of Schizophrenia
Genetic Influences
Implies genetic factors not environmental
Adoption Studies
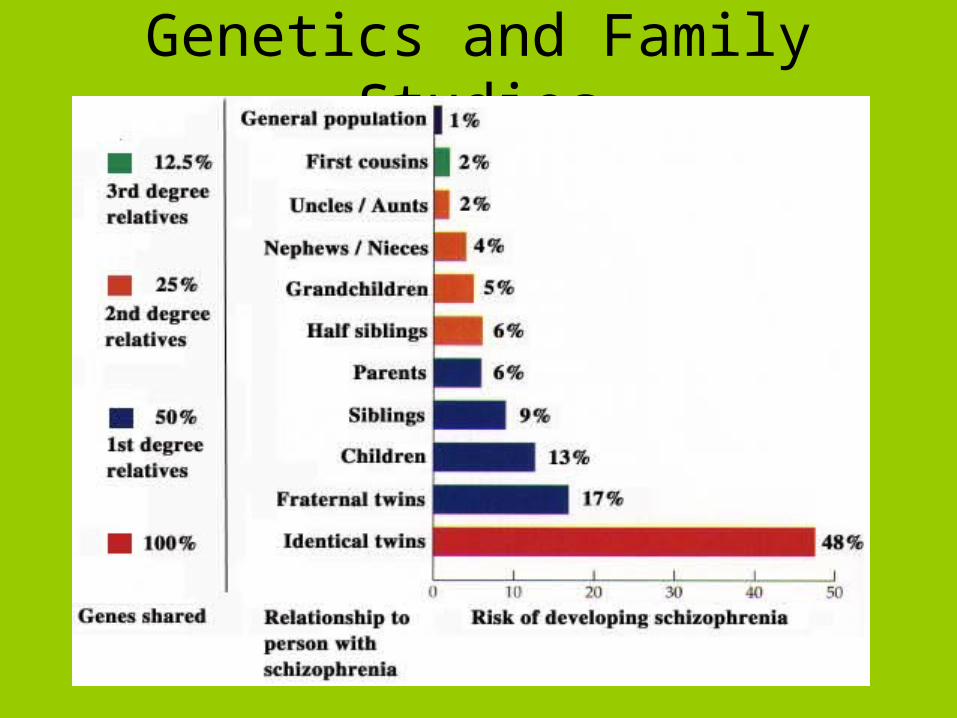
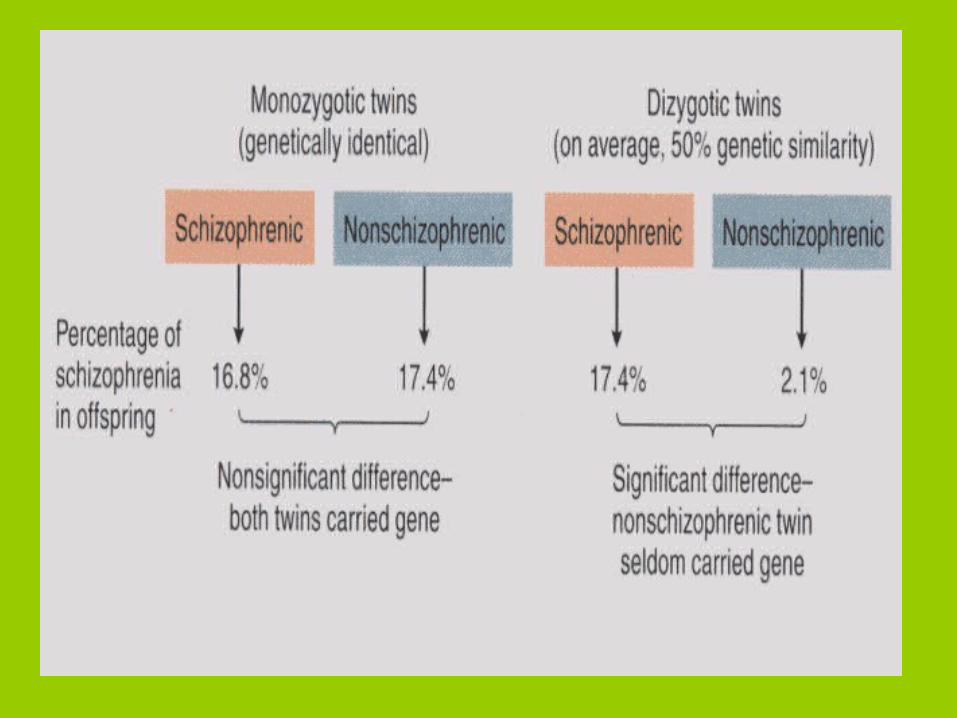
Genetics and Family Studies
Etiology of Schizophrenia
Brain Abnormalities
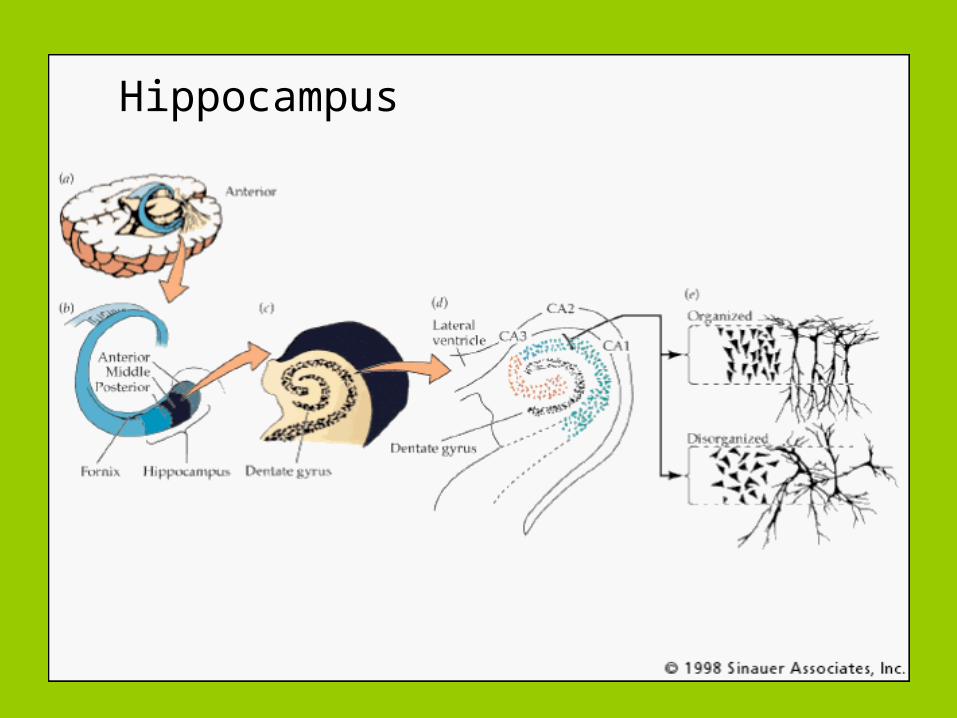
Hippocampus
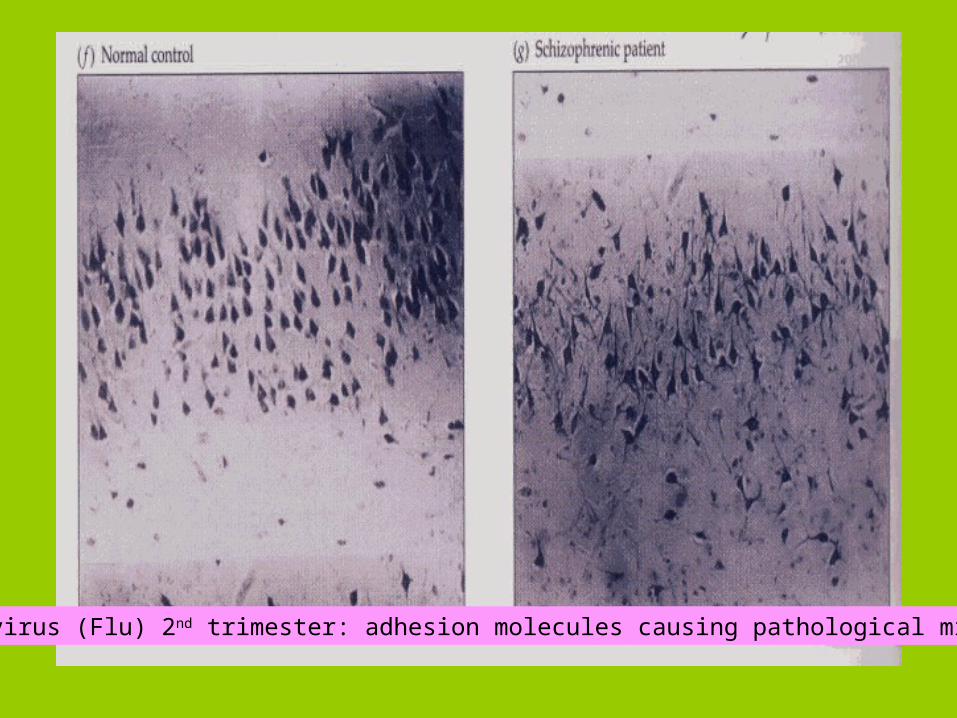
Due to virus (Flu) 2nd trimester: adhesion molecules causing pathological migration
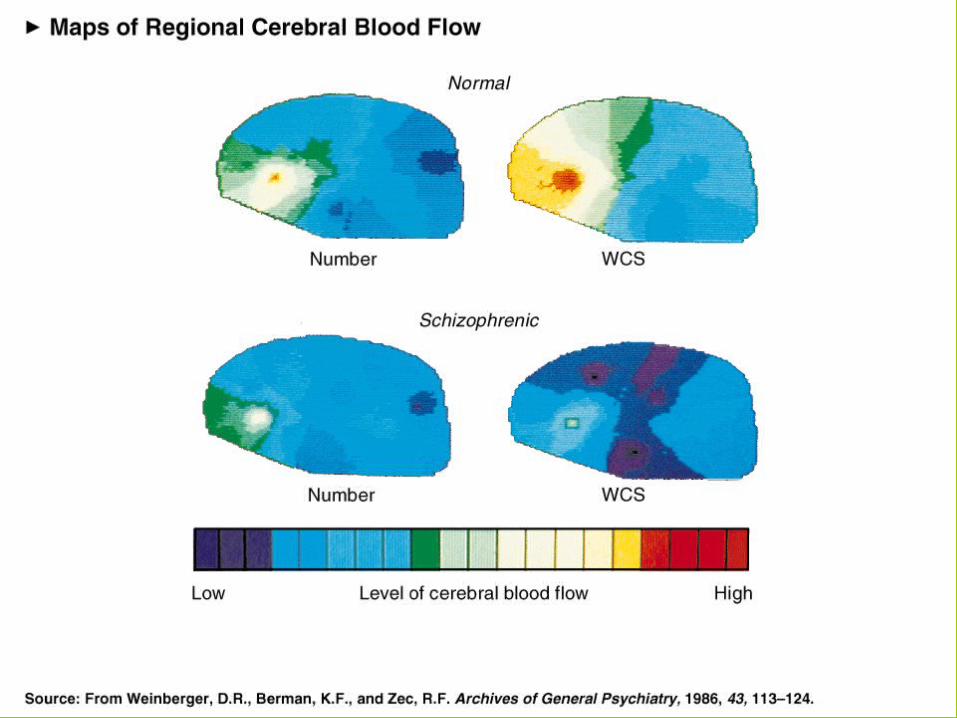
Frontal Lobe Issues Functional brain imaging (PET, rCBF)
• Failure to increase blood flow to the dorsolateral prefrontal cortex while performing the activation task of the Wisconsin Card Sorting Test
• Reduced blood flow to the left globus pallidus (an even earlier finding in the course of illness) suggests a problem in the system connecting the basal ganglia to the frontal lobes
• Correlation with severity of disease present
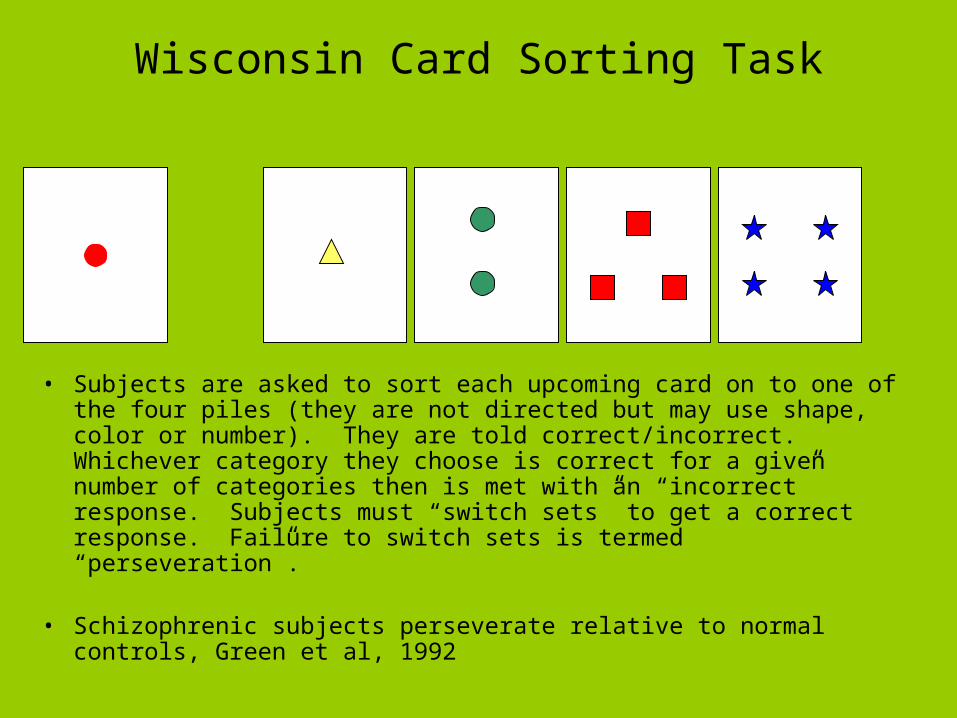
Wisconsin Card Sorting Task
• Subjects are asked to sort each upcoming card on to one of the four piles (they are not directed but may use shape, color or number). They are told correct/incorrect. Whichever category they choose is correct for a given number of categories then is met with an “incorrect” response. Subjects must “switch sets” to get a correct response. Failure to switch sets is termed “perseveration”.
• Schizophrenic subjects perseverate relative to normal controls, Green et al, 1992
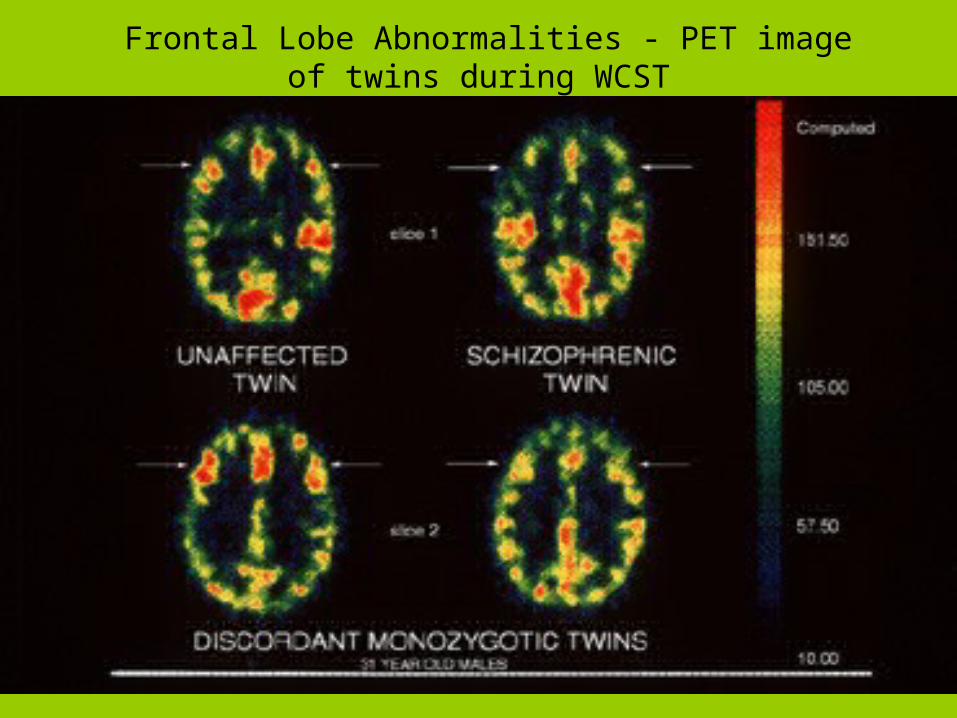
Frontal Lobe Abnormalities - PET image of twins during WCST
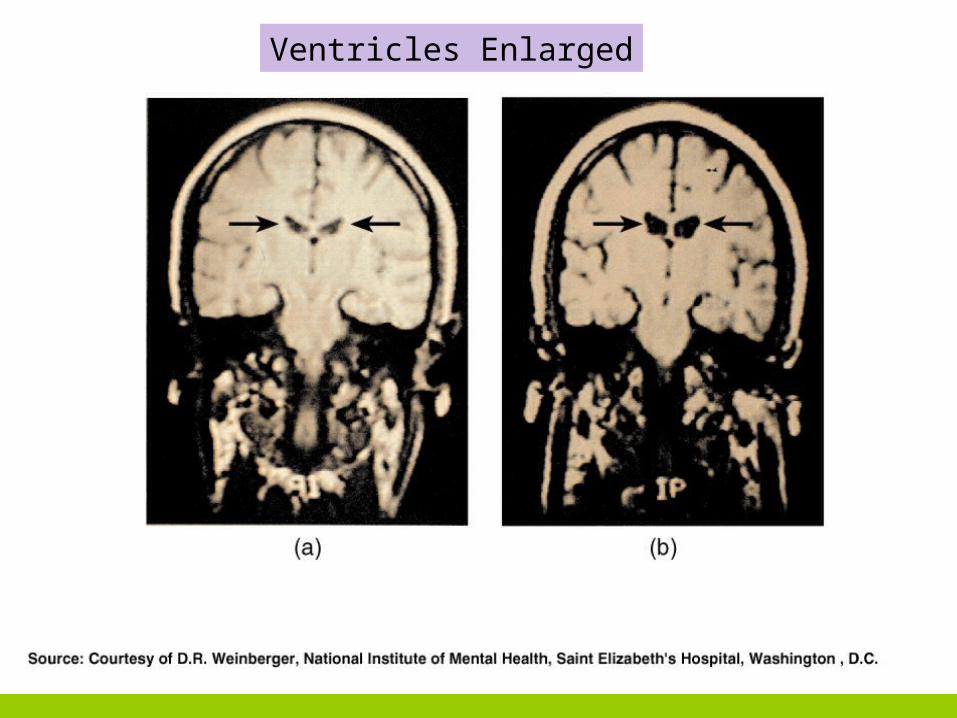
Ventricles Enlarged
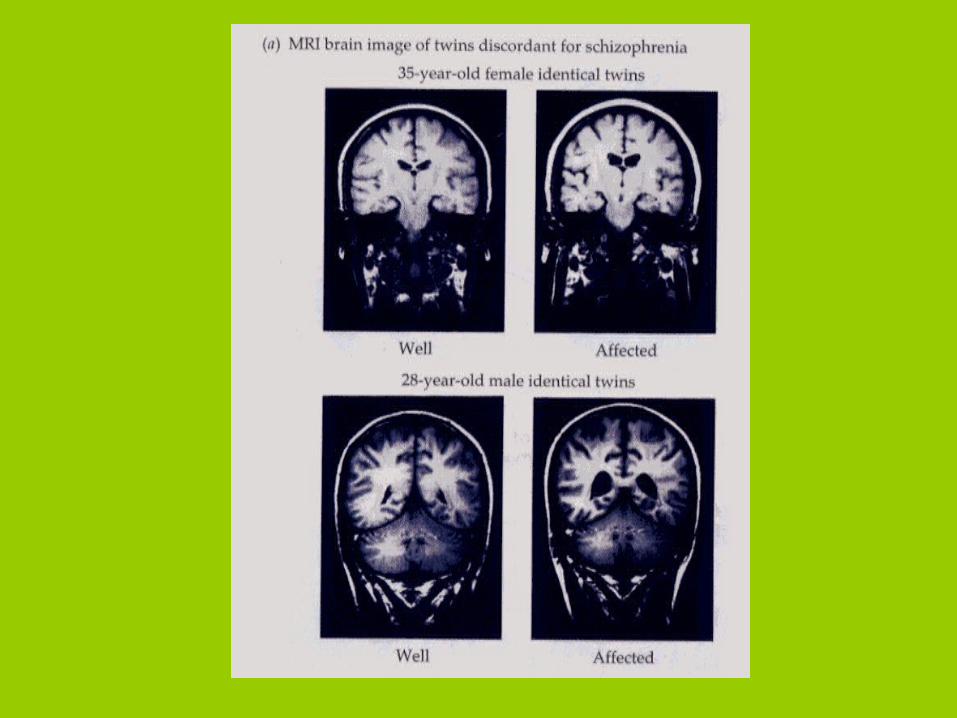
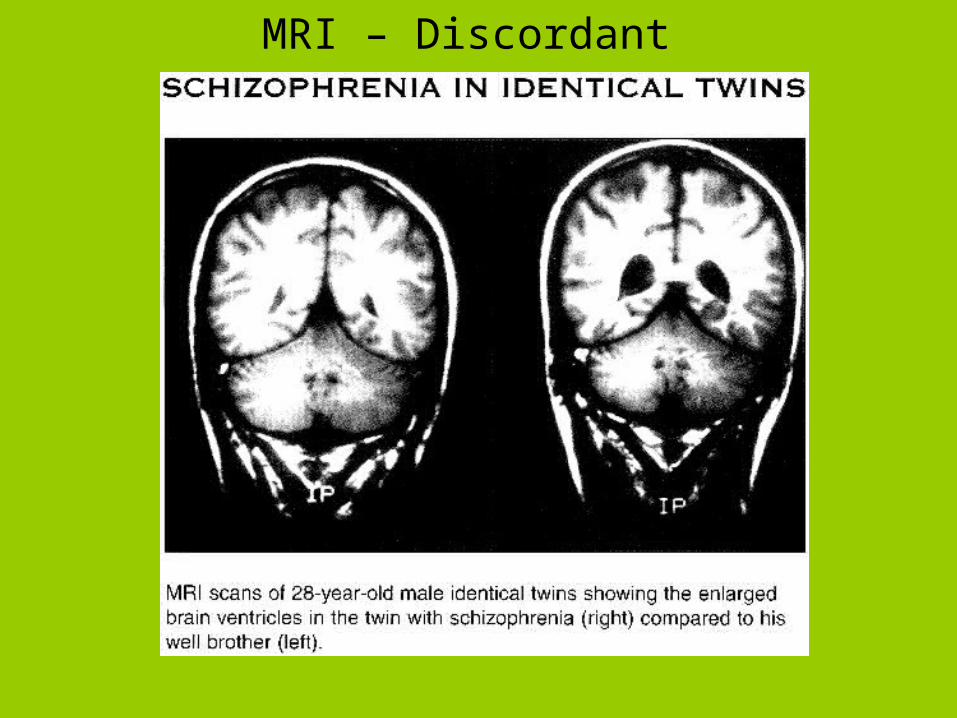
MRI – Discordant
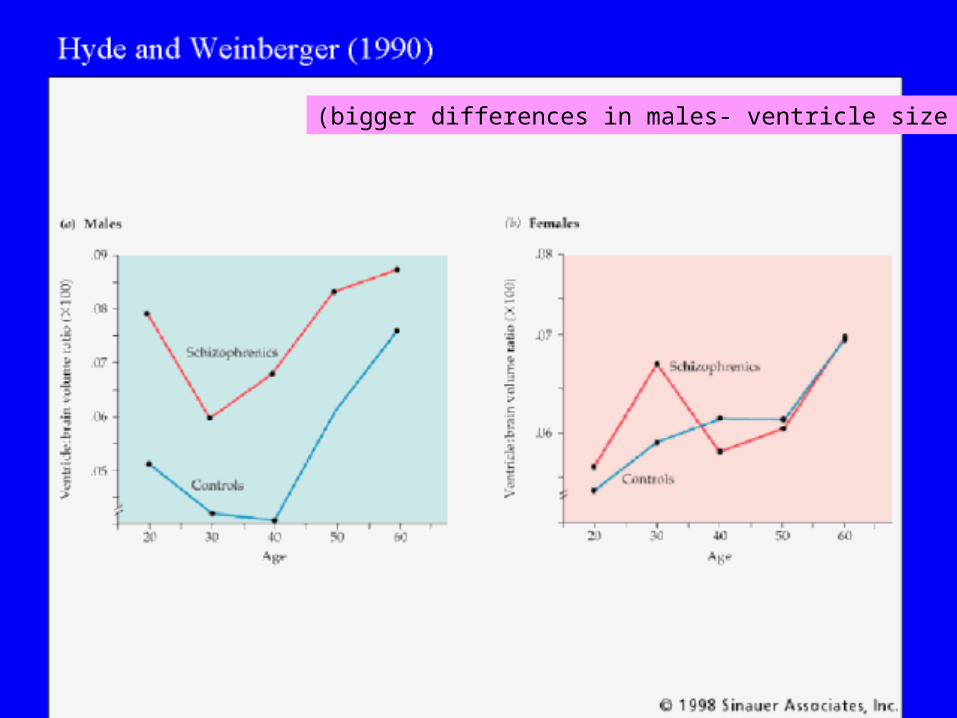
(bigger differences in males- ventricle size
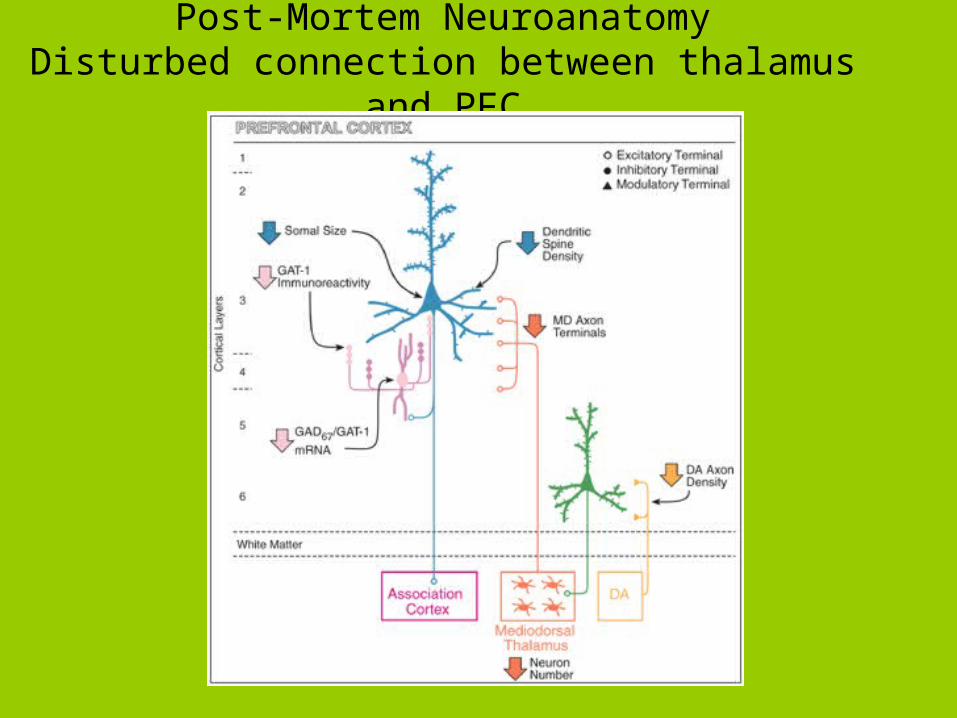
Post-Mortem NeuroanatomyDisturbed connection between thalamus and PFC
Serendipity Strikes Again!!!!
1960 – discovery that striatums (caudate putamens) depleted of Dopamine
Dopamine Hypotheses of Schizophrenia
• Dopamine– Schizophrenia due to over activity
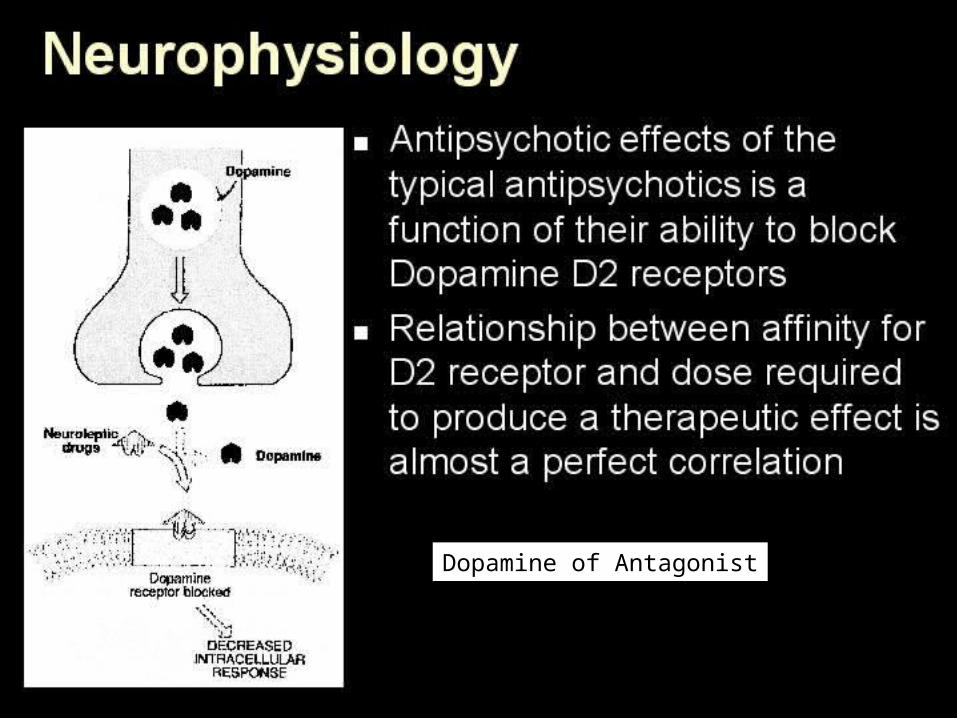
Dopamine of Antagonist
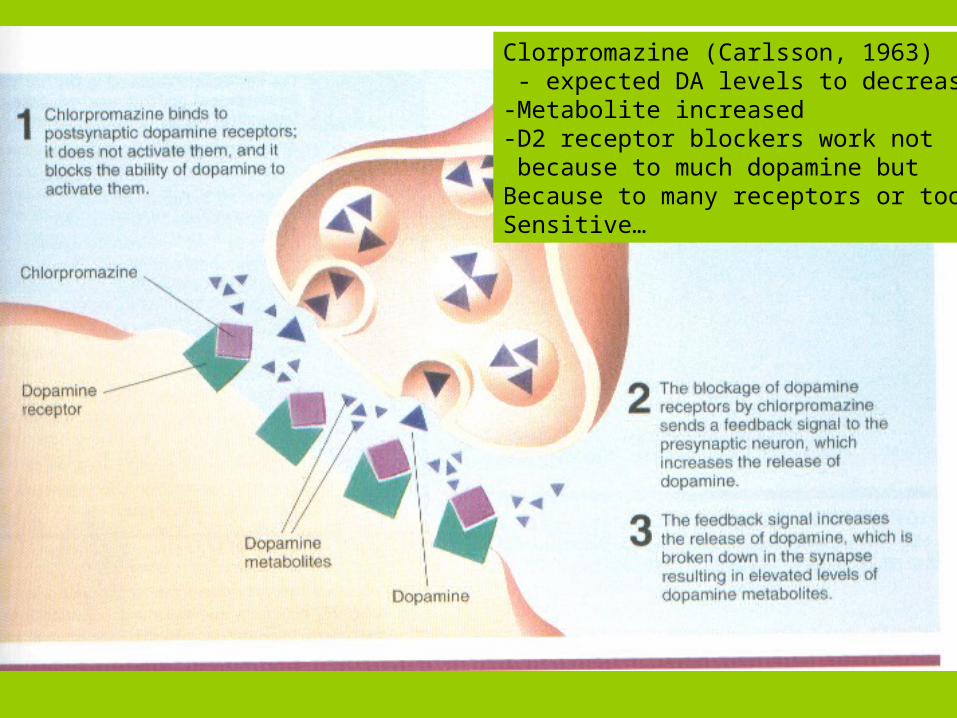
Clorpromazine (Carlsson, 1963) - expected DA levels to decrease-Metabolite increased-D2 receptor blockers work not because to much dopamine but Because to many receptors or tooSensitive…
Dopamine Hypotheses of Schizophrenia (revised)
• Dopamine– Positive symptoms of schizophrenia
attributed to hyperdopaminergic function (more receptors or increased sensitivity, etc, D2)

Evidence in Support
•Dopamine hypothesis - weaknesses:
–Some atypical antipsychotics such as clozapine are not as well correlated with respect to D2 dopamine receptor binding and clinical potency
–Does not account for negative symptoms of schizophrenia
•Evidence against DA hypothesis of
Schizophrenia – Glutamate???
–Disorganized thought symptoms of schizophrenia attributed to hypofunctional glutamate system
–Glutamate antagonists such as PCP and ketamine mimic disorganized thought, may also cause psychosis and negative symptoms?