Embed Size (px)
Citation preview

Postmortem Studies in Schizophreniaby Peter Powchik, Michael Davidson, Vahram Haroutunian,
Stephen M. Qabriel, Dushyant P. Purohit, Daniel P. Perl, Philip D. Harvey,and Kenneth L. Davis
Abstract
The past decade has seen renewed interest in the neu-ropathology of schizophrenia. The advent of new post-mortem techniques and functional imaging, along witha greater understanding of the neuropsychology ofschizophrenia, have provided many new clues to thenature of the underlying brain dysfunction in this dis-order. There has also been a greater understanding ofthe presence of severe cognitive dysfunction amongmany elderly persons with schizophrenia. In this arti-cle, a series of investigations are described that seek toanswer basic questions about the neuropathology ofschizophrenia, hi particular as it pertains to cognitiveimpairment. The first study describes neuropathologi-cal findings in 100 consecutively autopsied personswith schizophrenia, the majority of whom had haddetailed antemortem assessments. Results from thisfirst study nrompted the conclusion that schizophreniais not characterized by classical, histologically identifi-able neuropathology. Moreover, most cases of demen-tia in schizophrenia are probably not the result of neu-ropathologically identifiable dementing illnesses. Thenext four studies examined chemical markers that arealtered in Alzheimer's disease and some other dement-ing conditions and have also been suggested to beabnormal hi schizophrenia: choline acetyltransferase,catecholamines and indolamines, neuropeptides, andsynaptic proteins. Schizophrenia cases as a group didnot show a cholinergic deficit; nor did they differ fromelderly comparison cases with respect to cortical cate-cholamines and indolamines. Among the schizophreniacases, however, cognitive impairment was negativelycorrelated with choline acetyltransferase activity.Those with cognitive impairment showed evidence ofcortical noradrenergic and serotonergic deficits.Neuropeptide deficits were also present In schizophre-nia, but their pattern differed from that seen inAlzheimer's disease. Increased synaptic protein activ-
ity was found in the cingulate cortex of persons withschizophrenia, and this activity was correlated withschizophrenia symptoms. From this second series ofstudies, it was concluded that some biological meas-ures in schizophrenia may be related to cognitiveimpairment (e.g., cortical amines), whereas others maybe related to diagnosis (eg., neuropeptide deficits). Inaddition, synaptic organization may correlate withschizophrenia symptoms.
Key words: Brain pathology, dementia, serotonin,norepinephrine, synaptic proteins.
Schizophrenia Bulletin, 24(3):325-341,1998.
Over the past three decades, our understanding of the clin-ical boundaries of schizophrenia, its associated cognitiveimpairments, and even its treatment has advanced signifi-cantly. Unfortunately, a fundamental understanding of thebiological underpinnings of schizophrenia has proven elu-sive. The "challenge study" paradigm of the 1970s and1980s, although still useful in advancing the understand-ing of some psychiatric disorders, has generally fallen outof favor as a tool to investigate the biology of schizophre-nia. Replacing these methods are advances in functionalimaging that can indirectly reveal differences in brainfunction between patients with schizophrenia and con-trols. Despite the knowledge that can be gained, however,functional neuroimaging remains a collection of indirectmethods. To fully understand the abnormal brain structureor functional connections that are presumed to be presentin and responsible for schizophrenia, more direct methodsmust be employed. The most direct methods use post-mortem brain tissue.
As reviewed by Bogerts (1993), there were nearly200 neuropathological studies of schizophrenia before1957 and then, from the mid-1950s to 1990, the topic
Reprint requests should be sent to Dr. P. Powchik, Pfizer, Inc., 235-10-50,235 East 42nd St., New York, NY 10017.
325
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/24/3/325/1839746 by guest on 17 February 2022

Schizophrenia Bulletin, Vol. 24, No. 3, 1998 P. Powchik et al.
remained conspicuously absent from the international aca-demic venue. A major discouragement to continued neuro-pathological studies was the fact that classical techniqueswere unable to identify any consistent abnormalities inbrain tissue derived from persons with schizophrenia.
The advent of powerful new neuroscience techniquessparked a renewed interest in the field (Kleinman et al.1988; Shapiro 1993). There are even trends in findingsthat suggest the presence of temporal lobe (Akbarian19936), thalamic (Pakkenberg 1992), hippocampal(Arnold et al. 1995a), or cingulate (Benes 1993) abnor-malities in schizophrenia. However, despite technicaladvances, consistently replicable findings with respect tothe neuropathology of schizophrenia are still lacking.
Recently, several clearly definable methodologicalproblems hampering progress in neuropathological stud-ies of schizophrenia have been pointed out (Arnold et al.\995b). Among those problems are tissue acquisition dif-ficulties, which translates into a small number of cases;unreliability of clinical information; inadequate orimproper comparison groups; inconsistent tissue han-dling; qualitative rather than quantitative neuropathologi-cal descriptions; and the generally well-recognized limita-tions of classical neuropathological techniques. The seriesof studies described here attempted to address all of theseissues and shed some additional light on the neuropathol-ogy of schizophrenia.
Study Background
Our group has maintained an active role in developing abrain bank for the study of neuropsychiatric disorderssince the early 1980s. In 1988, we entered into an acade-mic association with the Pilgrim Psychiatric Center (PPC,a facility operated by the New York State Office ofMental Health) and the opportunity to develop a brainbank for schizophrenia presented itself. PPC was arguablyone of the largest psychiatric hospitals in the UnitedStates, if not the world. It was originally planned to houseup to 35,000 patients but at its maximum census in theearly 1960s housed about 17,000 patients. In 1988, as aresult of "deinstitutionalization," the patient population ofPPC was approximately 2,300, with nearly 1,000 patientsover 65. The striking features of the elderly populationwere the high prevalence of moderate to severe cognitiveimpairment (> 60%) and the fact that many of the caseswere not easily cross-sectionally distinguishable from per-sons with moderate to severe Alzheimer's disease (AD).Although the prevalence of AD increases with age andthus might have provided an explanation for the cognitiveimpairment in this population of psychiatric patients, thepossibility of another etiology needed to be investigated.
As part of a clinical program instituted at PPC, allpatients over 65 underwent complete diagnostic reviewsand symptomatic and cognitive assessments conducted byexperienced clinicians (Harvey et al. 1992; Davidson etal. 1995). These clinicians were trained in structured eval-uations and periodically assessed to ensure interrater reli-ability. These prospectively collected, antemortem clinicaldata constituted a reliable source of clinical informationcollected in a standardized way, thus addressing one ofthe main concerns of postmortem studies.
Another clinical improvement at PPC was the devel-opment of an efficient, yet compassionate approach toobtaining autopsies. Prior to the development of theautopsy retrieval program, the autopsy rate at PPC wasless than 20 percent, with the vast majority of autopsiesobtained with the permission of the medical director 72 to168 hours after death. Such postmortem intervals (PMIs)make tissue usable only for the most rudimentary histo-logical and neuropathological investigations. Within 2years of the program's initiation, the autopsy rateincreased to more than 50 percent, with nearly half theautopsies obtained in less than 24 hours. Since 1989,more than 170 autopsies have been obtained. Of these,103 were from persons with schizophrenia, 72 of whomhad detailed antemortem assessments. These have beenresearch-quality autopsies, and tissue handling is con-sistent for all samples. Thus, we were able to develop anautopsy retrieval system that addresses the issues ofobtaining sufficient quantities of tissue and uniform tissuehandling.
The studies described below, which focused primarilyon cortical structures, were spurred by a series of ques-tions related to schizophrenia in general and cognitiveimpairment in particular:
• Is schizophrenia characterized by classically identi-fiable cortical neuropathology?
• Can the biological characteristics of postmortembrain tissue from persons with schizophrenia be related tosymptoms of the illness? If so, is the pathology regionalor diffuse?
• Is there a definable postmortem neuropathologyand/or biology of severe cognitive dysfunction in schizo-phrenia?
Methods
The Population. Brain tissue samples used in the seriesof studies presented here were derived from a populationof long-term psychiatric inpatients who have been previ-ously described (Harvey et al. 1992; Davidson et al.1995). Subjects were patients at PPC, a large hospital thatcares primarily, though not exclusively, for persistently ill
326
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/24/3/325/1839746 by guest on 17 February 2022

Postmortem Studies Schizophrenia Bulletin, Vol. 24, No. 3, 1998
geriatric patients with schizophrenia. The series ofpatients described here represents 100 autopsies consecu-tively obtained from 1989 to 1995. Of these 100 cases, 69had antemortem diagnostic assessments and 31 were diag-nosed retrospectively by chart review. Of the 69 cases thathad antemortem diagnostic assessments, 63 had fullsymptom and cognitive assessments as well. The 31 casesassessed retrospectively did not differ in terms of age,gender distribution, or length of illness.
Subjects ranged in age from 52 to 101 years (mean =78.5, standard deviation [SD] = 10.5). All cases metDSM-III-R (American Psychiatric Association 1987) cri-teria for chronic schizophrenia. To generate a lifetimediagnosis of DSM-III-R schizophrenia, an experiencedpsychiatrist reviewed all available medical records, inter-viewed collateral informants (most often clinical staff),and used data from interviews with the patients them-selves when they were able to contribute information per-tinent to presenting symptoms and course of illness. Forthe subjects who had a postmortem diagnostic assessment,a similar procedure was followed (other than the patientinterview) within several weeks of the patient's death. Inthese cases, the main caregiver and the treating psychia-trist were interviewed, and an extensive review of medicalrecords was performed.
Psychiatric subjects without schizophrenia (n — 47)were patients at PPC who did not meet DSM-III-R crite-ria for schizophrenia or a developmental disorder but whomanifested psychiatric symptoms during life that resultedin long-term hospitalization. These subjects ranged in agefrom 53 to 106 years (mean = 76.9, SD = 11.4).
AD cases were those that met criteria for AD estab-lished by the Consortium to Establish a Registry forAlzheimer's Disease (CERAD) (Mirra et al. 1991) andwho had no other significant neuropathological findings.The age of subjects with AD (n = 135) from whom sam-ples were derived averaged 83.3 years (SD = 15.4, range56-100 years). All subjects with AD were assessed whilestill alive by trained clinical raters.
Specimens from nonpsychiatric, non-AD elderly com-parison cases (n = 50) were defined as those derived fromsubjects who had no chart history of neurological or psy-chiatric disease, who manifested no cognitive deficits orquestionable ones as defined by the Clinical DementiaRating Scale (CDR; Hughes et al. 1982), and whose tirainsat autopsy showed no neuropathological lesions other thanthose that might be expected given the subjects' age (e.g.,age-related density of senile plaques). The mean age ofthis sample was 78.5 years (SD = 13.5, range 53-96years). Tissue samples from several additional elderlycases with multi-infarct dementia (MID) were used in theneuropeptide (n = 4), neurotransmitter (n = 2), and synap-
tic protein studies (n = 3). Characteristics of subjects in allstudies are shown in table 1.
The Assessment Assessment instruments included thePositive and Negative Syndrome Scale (PANSS; Kay etal. 1987), the CERAD battery of cognitive assessments(Morris et al. 1989), and the CDR scale of Hughes et al.(1982). Interrater agreement for the PANSS was high,with intraclass correlation coefficients for its 30 itemsranging from 0.86 to 1.00 (with all p values < 0.001 basedon 54 interviews conducted by two raters). A detaileddescription of reliability in the use of these scales and theentire CERAD cognitive battery has been previously pub-lished (Harvey et al. 1992).
Specimen Retrieval and Preparation. At autopsy, thebrain was divided at the mid-sagittal plane. The right halfwas fixed in 4 percent formalin for use in neuropathologi-cal evaluations. Some fresh specimens and all brain stemsand cerebella were available for neuropathological exami-nation. The left half of the brain was coronally sectionedinto 0.5- to 0.8-mm slabs and flash-frozen in liquid nitro-gen for storage at -80 °C. These frozen sections wereused for all assays other than classical neuropadiology.
Neuropathological Methods. A detailed description ofthe neuropathological methods has been previously pub-lished (Purohit et al. 1993). Specimens were examinedusing the standardized protocol of the Mount Sinai-BronxVeterans Affairs Medical Center Alzheimer's DiseaseResearch Center, which was, in turn, adopted from proce-dures developed by CERAD (Mirra et al. 1991). Paraffintissue blocks were prepared from five neocortical areas(Brodmann areas 9, 45/47, 21/22, 39, and 17), rostral andcaudal hippocampus, the nucleus basalis of Meynert,amygdala, midbrain, pons, medulla, and cerebellum.Sections were stained with hematoxylin and eosin,thioflavine S, and modified Bielschowsky's stains.Immunohistological staining with ubiquitin was done toidentify Lewy body formation.
All neuropathological assessments were performedblind to clinical information. This assessment includedquantitative estimates (using a 4-point scale: absent,sparse, moderate, and severe) for the density of senileplaque, neurofibrillary tangles (NFTs), and other AD-related histological changes, such as amyloid angiopathy,neocortical neuronal loss, neuropil degeneration and glio-sis, hippocampal degeneration (including neuronal loss,granulovacuolar degeneration, and Hirano bodies), anddegeneration of the subcortical and brain stem nuclei. Afurther assessment of the senile plaque density in the neo-cortex was carried out using the following quantitative
327
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/24/3/325/1839746 by guest on 17 February 2022

Schizophnmia Bulletin, Vol. 24, No. 3, 1998 P. Powchik et al.
Table 1. Subject characteristics In each experiment
NeuropathologynAge, mean ± SD (range)
Gender, malerfemaleCDR
Choline acetyltransferasenAge, mean i SD (range)
Gender, male:femaleCDR
NeurotransmittersnAge, mean ± SD (range)
Gender, malerfemaleCDR
Synaptic proteinsnAge, mean ± SD (range)
Gender, malerfemaleCDR
NeuropeptidesnAge, mean ± SD (range)
Gender, male femaleCDR
Schizophrenia
10076.5±10.5(52-101)
58:422.311.2(0-5)
9578.5111.1(56-100)
52:432.2112(1-4)
Schizophrenia
1975.3110.1
(52-95)13:6
1.911.2(0-4)
1974.1 112.1
(52-95)11:8
2.011.3(0.5-4)
1971.1 112.7.
(52-92)12:7
2.211.2(0.5-4)
AD
13583.3111.5(56-100)
51:843.7211.5(3-5)
13583.3111.5(56-100)
51:84 •3.7211.5(3-5)
AD
1072.4111.1
(58-97)8:2
4.7 1 0.7 (4-5)
2473.6111.5
(58-97)16:8
4.2 1 0.9 (3-5)
1369.5 1 7.8(58-88)
9:44.4 1 0.7 (3-5)
Non-MID elderly
5076.5111.0
(52-99)22:28
0.1510.23(0-0.5)
2078.5112.1
(55-96)9:11
0.28 10.08 (0-0.5)
Non-MID elderly
782.9110.4
(70-96)5:2
0.23 10.25 (0-0.5)
1380.0110.2
(65-99)5:8
0.23 10.25 (0-0.5)
479.1 1 7.5(71-88)
4:00.1 1 0.2 (0-0.5)
Psychiatricdisorders
(not schizophrenia)
4776.9111.4
29:182.711.3 (0-5)
MID elderly
292110(85-99)
1:14.011.0(3-5)
373.2111.1
(55-80)3:0
4.011.0(3-5)
485.3 14.9
(78-92)4:0
2.611.5(2-5)Note.—AD = Alzheimer's disease;etal. 1982).
MID - multi-infarct dementia; SD - standard deviation; CDR - Clinical Dementia Rating scale (Hughes
methods: The neocortical senile plaques were counted infive areas (selected from high-senile plaque-density areasidentified at low-power scanning) in each thioflavine-S-stained slide of the neocortex, using medium-power(X250) magnification, giving a calculated visual field of0.5 mm2. The plaques that showed neuritic changesand/or amyloid cores were counted for this assessment.From these results, a mean neocortical senile plaque countper square area was calculated for each case.
Neuropathological examination also included docu-mentation of infarctions, neoplasms, cerebrovascularchanges, and other morphological abnormalities. Otherneurodegenerative disorders were also screened for (e.g.,Parkinson's disease, diffuse Lewy body disease, Jakob-Creutzfeldt disease, and Pick's disease). A neuropatholog-ical diagnosis of AD was made using the CERAD diag-nostic criteria (Mirra et al. 1991).
Biological Assays.Choline Acetyltransferase (ChAT). Inferior pari-
etal cortex from 95 persons with schizophrenia (from the100 total cases), 135 persons with neuropathologicallyconfirmed AD, and 20 normal controls was used to esti-mate ChAT. Before assay, frozen tissue slabs containingthe inferior parietal lobe were warmed to -20 °C and thendissected using a scroll saw. The dissected inferior pari-etal lobe was immersed in liquid nitrogen, crushed, andpulverized in a liquid nitrogen-cooled mortar and pestle.The powdered homogenate was aliquoted into 50-100 mgportions and kept at —80 °C until assay. The proceduresused for the ChAT activity assay were identical to thosepreviously described by Haroutunian et al. (1994).
Other Neurotransmitters. Brain tissue sampleswere stored at -80 °C until assay by high-performanceliquid chromatography with electrochemical detection
328
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/24/3/325/1839746 by guest on 17 February 2022

Postmortem Studies Schizophrenia Bulletin, Vol. 24, No. 3, 1998
based on the procedure of Maruyama et al. (1980).Cortical tissue samples (Brodmann areas 8, 32,44, 22, 36,and 7) from 19 elderly people with chronic schizophreniawithout evidence of neuropathology (12 of whom werecognitively impaired: CDR score a 1), 10 persons withneuropathologically confirmed AD, and 9 elderly normalcontrols were used. Tissue samples were extracted intoperchloric acid containing dihydroxybenzylamine(DHBA) as internal standard ethylenediamine tetraaceticacid (EDTA), sodium metabisulfite, and cysteine hydro-chloride using a Fisher Sonic Dismembranator 300 withattached microtip (at 35% power). After centrifugation(6,000 rpm X 10 min), the supernatant was filtered inmicrofilterfuge tubes (Rainin Instruments). Standard mix-tures of norepinephrine (NE), 3-methoxy-4-hydroxyphe-nolglycol (MHPG), dopamine (DA), dihydroxyphenyl-acetic acid (DOPAC), homovanillic acid (HVA), serotonin(5-HT), and 5-hydroxyindoleacetic acid (5-HIAA) werediluted in 0.1 M perchloric acid also containing DHBA asinternal standard and run in parallel with the brain tissuesamples. Samples (50-100 mL) were injected using aWaters 712 refrigerated autosampler connected to aShimadzu 6,000 pump, and detection was made with anLC-4C detector and CC-4C cell (Bioanalytical SystemsInc., West Lafayette, IN). A Phase 11 analytical column(C18 250 X 4.6 mm, 5 u,m, BAS) was protected by a C18guard column (15 X 4.6 mm, 5 u>m, Brownlee). Themobile phase consisted of 0.15 M monochloracetic acid,0.12 M sodium hydroxide, disodium EDTA (0.25 mg/L),sodium octylsulfate (300 mg/L), and methanol (8%) at pH2.7. Concentrations of amines and metabolites in the sam-ples were calculated: (Ratio sample: internal standard[IS]) X standard concentration X 2 mL/(Ratiostandard:IS) X weight of frozen tissue.
Synaptk Proteins (SP). The methods and results ofthe SP experiments are reported in detail by Gabriel et al.(1997) and summarized here. In the first series of experi-ments, presynaptic protein immunoreactivities from cere-bral cortical areas were assessed using an antibody captureimmunoassay in 19 elderly patients with schizophrenia, 24patients with AD, and 16 elderly controls. Immuno-reactivities to brain SPs were estimated by antibody-cap-ture, enzyme-linked immunoabsorbant assay (ELISA)using the previously described monoclonal antisera: EP10and SP4, which recognize synaptophysin (Honer et al.1989, 1992, 1993), and SP6 and SP14, which recognizesyntaxin and SNAP-25 immunoreactivity, respectively(Honer et al. 1993). All three proteins recognized by theseantibodies are associated with the presynaptic membraneand involved in vesicle docking and neurotransmitterrelease (Sollner et al. 1993; Bajjalieh and Scheller 1995;
Littleton and Bellen 1995). Brain tissue (cortical tissuecorresponding to Brodmann areas 24, 8, 20, and 7) forthese studies was derived from the total pool of schizo-phrenia, AD, and normal elderly brain samples andincluded tissue from 19 persons with schizophrenia, 24persons with neuropathologically confirmed AD, and 16elderly controls. The demographic details of these casesare published elsewhere (Gabriel et al. 1997) and summa-rized in table 1 here. Thirteen of the 16 elderly controlswere cognitively normal and had no discernible neu-ropathology; the other 3 were cognitively impaired and onneuropathological examination showed evidence of vascu-lar disease and multiple infarcts. These cases wereincluded in me study because the infarcts were distal to thecortical regions sampled and abnormalities had not beendetected in earlier neurochemical studies of these cases(Gabriel et al. 1993,19%).
Immunoreactivity data were combined with subjectinformation and analyzed for differences between diag-nostic groups using analysis of variance (ANOVA), forrepeated measures. Although these proteins are distinct,each is intimately associated with presynaptic elements,and therefore their immunoreactivities were treated asrepeated measures, while each cortical region was ana-lyzed separately. Differences between groups were exam-ined using Tukey's honestly significant difference (HSD)test for uneven sample sizes and a p value of less than orequal to 0.05 was considered significant
In a second experiment, brain tissued from 28 schizo-phrenia subjects who had antemortem assessments of psy-chopathology was analyzed for levels of immunoreactivityof the presynaptic proteins recognized by SP4 (synapto-physin) and SP14 (SNAP-25) using methods identical tothose described above. Part of mat antemortem assessmentwas the PANSS. Pearson correlations between SP4 andSP14 immunoreactivity and PANSS positive and PANSSnegative subscale scores were calculated.
Neuropeptides. The details of these procedureshave been previously described (Gabriel et al. 1996).Concentrations of the neuropeptides galanin, somato-statin, neuropeptide Y, corticotropin-releasing hormone(CRH), vasoactive intestinal peptide (VIP), and cholecys-tokinin (CCK) were determined in six cortical regionsfrom 19 persons with schizophrenia, 13 with AD, and 8elderly subjects (4 considered "normal elderly" and 4 withMID). Neuropeptide concentrations were quantified in sixBrodmann areas corresponding to the superior frontalgyrus, cingulate gyrus, superior temporal gyrus, andparahippocampal gyrus, as well as the superior parietalgyrus. One-way ANOVAs were performed for each pep-tide with diagnosis as the grouping variable.
329
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/24/3/325/1839746 by guest on 17 February 2022

Schizophrenia Bulletin, Vol. 24, No. 3, 1998 P. Powchik et al.
ResultsNeuropathological Findings. Table 2 gives the break-down of neuropathological findings in brain tissue derivedfrom the 100 consecutive autopsies of persons with schiz-ophrenia. Eighty-seven of the 100 cases showed no neu-ropathological evidence of a dementing illness, butnonetheless had a mean CDR score of 2.35 which isindicative of more than moderate dementia in this group.
No difference was found between the density of age-related neocortical senile plaque formation in subjects withschizophrenia and the elderly comparison group (364.9 ±427 vs. 192.6 ± 315.4, NS by Student's f test). The distrib-ution of senile plaques in the three diagnostic groupsaccording to age is shown in table 3. A two-factor ANOVA(age X diagnosis) showed a strong age effect on the den-sity of plaques (FAGE = 4.0, df = 6,176, p < 0.05), but noeffect of diagnostic group (FDIAGNOSIS = 1.8, df= 2,176,p > 0.5) and no interaction between age and diagnosis
x DIAGNOSIS = 0-9, df = 12,176, p > 0.05). Among
Table 2: Postmortem neuropathology of 100consecutive cases of schizophrenia
Finding n
Neurodegenerative diseasesAlzheimer's disease (including one case of mixed
Alzheimer's disease and diffuse Lewy bodydisease) 9
Multi-infarct dementia 1Parkinson's disease 2
Other diseasesMultiple sclerosis 1
Focal abnormalities and/or relatively acutepathology (not likely to cause chronic, slowlyprogressive cognitive decline)
Neoplastic diseases 3Atherosclerotic cerebrovascular disease 23Brain stem hemorrhage 1Capillary telangiecstasia in parietal lobe 1Frontal leukotomy 11
No significant neuropathological abnormality 48
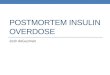
the subjects with schizophrenia, there was no correlationbetween plaque density and cognitive impairment (seefigure 1).
ChAT. Among the three groups used for these studies,one-way ANOVAs revealed significant differences in age(FA G E = 8.6, df= 2,247, p < 0.001), PMI (Fp^ = 74.1,df= 2,247, p < 0.001), and CDR score ( F ^ R = 77.8, df=2,210, p < 0.001). Co varying for these three in a one-wayanalysis of covariance (ANCOVA) with diagnostic groupas the grouping variable revealed a significant groupeffect on ChAT activity (FD I A G N 0 S I S = 18.25, df= 2,206,p < 0.0001). Post-hoc tests (Tukey's HSD for unequal /is)showed that the significant group differences were attrib-utable to differences between the AD group and the schiz-ophrenia and elderly comparison groups. There was nodifference in ChAT activity between the latter two groups(p > 0.06). When subjects with schizophrenia and longPMIs (> 8 hours) were excluded from the analysis, signifi-cant differences in parietal cortex ChAT activity remainedbetween groups (F D I A G N O S I S = 20.9, df = 2,176, p <0.001).
In this study, subjects with schizophrenia were signif-icantly cognitively impaired (mean CDR = 2.18 ± 0.12).Despite the lack of diminished cortical ChAT activity inthese subjects, there was a significant correlation of ChATactivity with their CDR scores (r = -0.29, p < 0.005),which was essentially identical to that among AD subjects(r = -0.36, p < 0.0003). These data suggest that althoughChAT activity is not diminished in subjects with schizo-phrenia compared with normal controls, its activity maynonetheless contribute to cognitive functioning.
Other Neurotransmitters. Repeated measuresANOVAs with diagnosis as the grouping variable and cor-tical region as the repeated measure were conducted foreach of the neurotransmitters and metabolites. No differ-ences between subjects with schizophrenia and normalsubjects were found in any of the neurotransmitters ortheir metabolites in any of the regions, although there wasa nonsignificant trend toward lower DA, HVA, and
Table 3. Mean senile plaques in the neocortex, grouped by age
Age range (years)
Subject group
Schizophrenia(n= 100)
Psychiatric disorders. other than
schizophrenia (n = 47)Elderly comparison
group (n = 50)
52-58
0(n=6)
0(n-1)
0(n = 3)
59-65
0(n = 6)
1.6 ±3.9(n=8)
2.1 ±3.1(n=4)
66-72
2.6 ± 3.6(n=14)2.9 ± 4.4(n = 8)
0.8 ±1.7(n=12)
73-79
1.7 ±0.3(n=14)3.1 ±4.4(n=13)
1.1 ±2.6(n=11)
80-86
4.5 ± 4.0(n = 38)1.6 ±2.8(n=9)
1.9 ±2.3(n = 8)
87-93
6.4 ± 5.3(n=15)6.1 ± 9.4(n = 4)
4.9 ± 4.7(n=10)
94-104
7.5 ± 3.4(n = 5)
3.6 ± 3.0(n = 4)
1.3 ±1.8(n = 2)
Note.—Data are mean ± standard deviation plaques per square miHimeter.
330
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/24/3/325/1839746 by guest on 17 February 2022

Postmortem Studies Schizophrenia Bulletin, Vol. 24, No. 3, 1998
Figure 1. Mean neocortical plaque counts per 100 mm2 (mean ± SEM)
0,0.5
CDR score
D medial frontal gyms; A orbital frontal gyms; O superior temporal gyrus; O inferior parietal lobe; D occipital cortex; CDR = ClinicalDementia Rating scale (Hughes et al. 1982); SEM = standard error of the mean.
DOPAC in subjects with schizophrenia compared withcontrols. Post-hoc tests showed that subjects with AD hadmarked deficits in 5-HT compared with normal subjects(p < 0.006 by Tukey's HSD test for unequal us) but notcompared with schizophrenia subjects (p = NS by Tukey'sHSD test for unequal ns), and deficits in 5-HIAA com-pared with normal subjects (p < 0.003 by Tukey's HSDtest for unequal ns) and schizophrenia subjects (p < 0.005by Tukey's HSD test for unequal ns). Subjects with schiz-ophrenia were no different from normal ones on thesemeasures.
To investigate the relationship between neurochemi-cal measures and cognition, subjects with schizophreniawere then divided according to cognitive status and com-pared with each other. Subjects with schizophrenia whohad significant cognitive impairment (i.e., those with aCDR score a 1) showed marked cortical deficits of 5-HT(FC D R = 5.6, df= 1,12, p < 0.04 by repeated measuresANOVA) and 5-HIAA (FC D R = 12.6, df = 1,11, p <0.005). Deficits of 5-HIAA were most prominent in allBrodmann areas tested, whereas deficits of 5-HT weremost prominent in Brodmann areas 32 (cingulate cortex)
331
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/24/3/325/1839746 by guest on 17 February 2022

Schizophrenia Bulletin, Vol. 24, No. 3, 1998 P. Powchik et al.
and 22 (temporal cortex). Deficits of NE, but not MHPGwere found in Brodmann areas 8, 32, 44, and 7 (all ps <0.04 by Scheffe's test). These relationships are shown infigures 2 and 3.
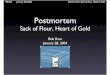
SPs. A significant diagnostic group effect was found inthe cingulate cortex (^DIAGNOSIS = 5.07, df = 2,51, p <0.005) with immunoreactivities in the anterior cingulatecortex (Brodmann area 24) of subjects with schizophreniabeing elevated compared with both control and AD cases(p < 0.02 by Tukey's HSD for unequal ns) (figure 4).Subjects with schizophrenia did not differ from elderlycontrols in the three other cortical regions, although sig-nificant group effects were found in the superior frontalgyrus (Brodmann area 8; ^DIAGNOSIS
= 10.8, df = 2,40,p < 0.0001), inferior temporal gyrus (Brodmann area 20;
^DIAGNOSIS = 9-2> 4f = 2>4 9 ' P < 0-0004), and inferiorparietal lobe (Brodmann area 7; ^DIAGNOSIS
= 3-3, df =2,30, p< 0.05).
Although there was no significant correlation be-tween PMI and presynaptic protein immunoreactivity, andadditional repeated measures ANOVA was performed ona subset of nine schizophrenia cases with the lowestPMI matched to within 100 minutes of nine controls
(PMISCHIZOPHRENIA = 4 4 1 ± 2 0 6 m i n > PMICONTROL =393 ±180 min). As in the larger sample, a significanteffect of diagnostic group was found in the cingulate cor-tex (^DIAGNOSIS
= 7-5, df= 1,11, p < 0.02). In this smallersubset of cases with similar PMIs, a significant groupeffect on presynaptic protein immunoreactivity was alsofound in the inferior temporal gyrus (^DIAGNOSIS
= U-42,df= 1,11, p < 0.006). There were no differences between
Figure 2. 5-HIAA and 5-HT in postmortem brain tissue
Cortical 5HIAA in Demented &Nondemented Schizophrenics
Cortical 5HT in Demented &Nondemented Schizophrenics
Mean; Whisker: Mean-SE, Mean+SE Mean; Whisker Mean-SE, Mean+SE
140
120
100
80
60
40
20
CDR>=1 CDR<1
• Brodmann 8A Brodmann 32O Brodmann 44O Brodmann 22D Brodmann 36A Brodmann 17
300
250
200
150
100
50
CDR>=1 CDR<1
5-HIAA = 5-hydroxyindoleacelic acid; CDR = Clinical Dementia Rating scale (Hughes et al. 1982); SE = standard error; 5-HT = serotonin.
332
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/24/3/325/1839746 by guest on 17 February 2022

Schizophrenia Bulletin, Vol. 24, No. 3, 1998 P. Powchik et al.
Figure 4. Synaptic protein activity in cinguiate cortex of subjects with schizophrenia and controls
6
SCHIZOPHRENICS CONTROLS
• SP4A SP6O EP10O SP14
Diagnostic group
Immunoactivity: Relative density per microgram of protein
nia and AD subjects compared with controls (F = 7.32,df= 2,33, p < 0.002), with prominent deficits in cinguiate,superior temporal, and parahippocampal gyri of subjectswith schizophrenia. Finally, CRH concentrations weremarkedly reduced in the AD group compared with schizo-phrenia and control groups (F = 8.46, df= 2,33, p <0.001), with the schizophrenia group showing a 24 per-cent reduction in CRH in the cinguiate gyrus comparedwith controls.
Discussion
The series of postmortem studies presented here wasdesigned and implemented with the intention of overcom-ing many, if not all, of the shortcomings of earlier studies.These neuropathological studies of schizophrenia are, toour knowledge, the largest in an antemortem-characterizedcohort and thus address the issue of small sample size.Tissue handling was uniform for all studies because sam-
ples were obtained from a single brain bank. Diagnoseswere made in most cases while the subjects were stillalive, and retrospective diagnoses were made immediatelyafter death on the basis of information in detailed clinicalrecords. Quantitative measurements of plaques, tangles,and other measures of neuropathology performed by expe-rienced research neuropathologists were the inviolate rule,not the exception, as highlighted by the use of a standard-ized assessment procedure developed by the CERADgroup (Mirra et al. 1991). Thus, the neuropathologicaldiagnostic assignments can be considered both valid andreliable. Finally, comparison groups were made up of otherwell-characterized cases whose tissues were handled iden-tically to those from the subjects with schizophrenia.
The data thus support a series of conclusions:
Schizophrenia is not characterized by classical histo-logically identifiable neuropathology. This conclusion isin line with most previous reports on smaller cohorts,
334
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/24/3/325/1839746 by guest on 17 February 2022

Postmortem Studies Schizophrenia Bulletin, Vol. 24, No. 3, 1998
most without antemortem assessments (see Shapiro1993). When leukotomized cases and the small number ofAD and Parkinson's cases were excluded, the subjectswith schizophrenia displayed remarkably little neu-ropathology. Even brain weights did not differ, in contrastto the findings of other groups (e.g., Pakkenberg 1987;Bruton et al. 1990). However, the size of the sample, thewell-characterized diagnoses of the cohort, and the unifor-mity of tissue handling and examination allow us to statewith confidence that gross neuropathology and classicalstaining methods are insufficient to differentiate the brainsof persons with schizophrenia from the brains of personswho do not have schizophrenia.
Most cases of dementia in schizophrenia are probablynot the result of neuropathologically identifiable dement-ing illnesses. The vast majority of the cohort of patientswith schizophrenia in this study had severe cognitiveimpairment. Only 13 of the 100 cases had evidence ofneuropathology that would explain that impairment In the87 cases without prominent neuropathology, the meanCDR score was 2.35, indicating moderate to severe cogni-tive and functional impairment. This is similar to the find-ings of Arnold et al. (1994) and El-Mallakh et al. (1991)in 10 demented subjects with schizophrenia, but in con-trast to those of Prohovnik et al. (1993). The Arnold studyemployed techniques quite similar to those presentedhere. The Prohovnik study, which reported a high inci-dence of AD, was heroic in its scale (more than 1,000cases) but nonetheless relied primarily on retrospectivediagnostic assessments, a dearth of cognitive information,and variable handling of tissue (which was collected overseveral decades).
AD clearly occurs in persons with definite schizo-phrenia, at a rate comparable to that seen in the generalelderly population. Other neuropathology also exists inthis cohort of subjects with schizophrenia (e.g., age-related plaque accumulation, mild vascular disease, andso on), but it is of a severity that would likely not result indementia if it occurred in an average 80-year-old. How-ever, the possibility of "normal" pathology coexisting inan already compromised brain might form the basis forsevere cognitive impairment. An analogous situationexists in AD with regard to level of education. Whenmatched for density of plaque counts, persons with higherlevels of education (which correlates with future cognitivecapacity) were less severely impaired during life (Stem etal. 1994). Stated differently, those persons with less cog-nitive capacity required less neuropathology to manifestcognitive impairment. It may be that persons with schizo-phrenia are more susceptible to pathological changes thatpersons without schizophrenia can compensate for.Arguing against this is the fact that there does not seem to
be a relationship between plaque density and cognitiveimpairment (see figure 1).
Some biological measures in schizophrenia may berelated to cognitive impairment and others to diagnosis.Cognitive impairments in patients with schizophreniashare some common biological correlates with AD. Theseinclude cortical somatostatin and serotonergic deficits.Demented subjects with schizophrenia also tend to havelower parietal lobe concentrations of SPs. They differfrom patients with AD in that cortical CRH deficits arenot present (except in the cingulate cortex), no cholinergicdeficit is present, and brain tissue does not react with Alz-50 (Powchik et al. 1993). The biological findings pre-sented here that might be specific to a diagnosis of schizo-phrenia include cortical deficits of VTP and neuropeptideY and increased SP concentrations in the cingulate andpossibly temporal cortex as well.
Reductions in 5-HT and NE may be related to cogni-tive impairment in schizophrenia. The role of 5-HT inschizophrenia has been reviewed elsewhere (Bleich et al.1988; Roth and Meltzer 1995). Among the schizophreniacases in this series of studies, the most robust associationsbetween a biological measure and cognitive impairmentwere the 5-HT and 5-HIAA deficits in the cortex of de-mented subjects with schizophrenia. Loss of raphe 5-HTneurons in AD has been previously reported (Halliday etal. 1992), but the relationship to dementia in schizophre-nia is not clear. For example, that loss of raphe neuronswas not consistently seen in patients with AD but when itoccurred, it occurred in those patients with symptoms ofdementia only and was prominent in those patients with arapid progression. The present studies did not specificallyexamine the raphe for numbers of serotonergic neurons,but there was no gross midbrain or brain stem pathology,and clinical features of dementia in schizophrenia are dif-ferent from those seen in AD (Davidson et al. 1995,1996). Specifically, the dementia in schizophrenia is gen-erally not rapidly progressive and although we do nothave reliable information about its rate of progression inthe cases studied here (because the majority were assessedonly once before death), it would be a marked coinci-dence if the demented cases were peculiar in that they dis-played rapid progression.
Earlier studies of 5-HIAA in the cerebrospinal fluid(CSF) of patients with schizophrenia may be consistentwith the current findings. For example, cerebral ventricleenlargement has been associated with decreased levels ofCSF 5-HIAA (Potkin et al. 1983). Members of that samegroup found that CSF 5-HIAA correlates with prefrontalregional cerebral blood flow (Weinberger et al. 1988).Increased ventricular size may be related to poor outcomein schizophrenia (Keefe et al. 1996) and decreased cere-
335
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/24/3/325/1839746 by guest on 17 February 2022

Schizophrenia Bulletin, Vol. 24, No. 3, 1998 P. Powchik et al.
bral blood flow with poor cognitive performance(Weinberger et al. 1988). Conversely, Csemansky et al.(1990) reported that CSF 5-HIAA correlates directly withthe severity of negative symptoms. This is just the oppo-site of what would be expected, given that cognitive per-formance is inversely correlated with the severity of nega-tive symptoms (Davidson et al. 1996).
Postmortem studies of 5-HT in schizophrenia havefocused primarily on receptor binding, and the resultshave been inconsistent (see Roth and Meltzer 1995). Weknow of only one study that looked specifically at cortical5-HT in schizophrenia (Joseph et al. 1979), and no differ-ences were found between subjects with schizophreniaand controls. Although the cases in that study were retro-spectively diagnosed, the findings were similar to thosepresented here. Moreover, the design of that experimentdid not allow for an examination of any relationshipbetween cognitive impairment and amine levels. Bridge etal. (1985) did report lower NE levels in the hippocampusof demented as compared to nondemented patients withschizophrenia but did not study 5-HT or 5-HIAA in thatseries. In addition, there have been several studies of 5-HT receptors in the cortex of patients with schizophrenia(e.g., Mita et al. 1986; Joyce et al. 1993) that may be con-sistent with the findings presented here. For example,Joyce et al. found an increased number of 5-HT2 and 5-HT1A receptors in the hippocampus and in the cingulateand temporal cortices. Similarly, Mita et al. reported adecreased number of 5-HT2 receptors in the prefrontalcortex of patients with schizophrenia and also concludedthat the findings were unrelated to neuroleptic treatment
The findings of NE in these studies are congruent withthose of Bridge et al. (1985) and are provocative, given therole of NE in cognitive processes and possibly schizophre-nia. Dysfunction of the prefrontal cortex (PFC) has longbeen implicated in schizophrenia—see the discussion byWeinberger (1993). Although most research in schizophre-nia has focused on DA, there is much evidence that thePFC is involved in cognitive functions relevant to schizo-phrenia (Goldman-Rakic 1994). The PFC displays richcatecholaminergic innervation (Lewis 1992), so dysfunc-tion of this region is likely to involve disruption of cate-cholaminergic functioning. Noradrenergic neurons project-ing to cortical regions do so through the dorsalnoradrenergic bundle (DNAB). Animal models of lesionsof the DNAB lead to a variety of reproducible cognitivedeficits. Acquisition of new information is more stronglyimpaired than previously learned information, and thisfinding is similar to the phenomenology seen in schizo-phrenia (Tamlyn et al. 1992). A variety of attentiondeficits, including deficits in sustained attention (Cole andRobbins 1992) and shifting attention (Devauges and Sara1990), can be measured in DNAB-lesioned animals.
In terms of NE's role in schizophrenia, there havebeen reports that schizophrenia symptoms are correlatedwith MHPG (e.g., Kaneko et al. 1992; Maas et al. 1993).Changes in CSF NE have been reported to help predictrelapse in people with chronic schizophrenia (vanKammen et al. 1994). In contrast, our group did not findsuch a relationship between CSF NE and either symptomsor neuropsychological measures in a small sample (Kahnet al. 1994). Others have suggested that clozapine's abilityto increase NE neurotransmission is related to its superiorclinical efficacy (Breier 1994), but peripheral NE did notdifferentiate clozapine responders from nonresponders(Davidson et al. 1993).
Synoptic organization may correlate with schizophre-nia symptoms. The immunoreactivities of the four SPsstudied here were generally elevated in the cortex ofpatients with schizophrenia compared with controls. Theonly exception was in the parietal cortex. These findingsdisagree with a previous study of synapsin in the hip-pocampus of seven persons with schizophrenia (Browninget al. 1993). However, the present studies were performedon a larger sample and did not include measurements ofSPs in the hippocampus.
A more recent study by Sower et al. (1995) may becongruous with the present findings. These authors reportincreases in growth-associated phosphoprotein (GAP)-43in the frontal and occipital cortices, but not the parietalcortex. GAP-43 is thought to be involved in synaptic reor-ganization. The elevation of SP concentrations reportedhere may represent differences in synaptic organization inpatients with schizophrenia compared with normals. It isunclear whether the differences first manifest during devel-opment or maturation (see e.g., Feinberg 1982; Keshavanet al. 1994) or over the long course of the disorder.Nonetheless, it is intriguing that the severity of some of thecore symptoms of schizophrenia would correlate with anypostmortem biological measure.
Neuropeptide abnormalities may represent a neu-rodevelopmental lesion in schizophrenia. The data pre-sented here demonstrate widespread neuropeptide deficitsin schizophrenia and may be relevant to the role ofgamma-amino butyric acid (GABAergic) neurotransmis-sion in this disorder. Somatostatin, neuropeptide Y, VIP,CCK, and CRH have all been localized to within the cor-tical GABAergic interneurons (Ong and Garey 1991;Foley et al. 1992; Rogers 1992; Dennison-Cavanagh et al.1993). The pattern of deficits seen in the present studiesdoes not fit a disorder of multiple neuropeptides contain-ing ascending afferents. For example, if a noradrenergicafferent were deficient, both neuropeptide Y and galaninshould be affected and they are not (Gabriel et al. 1994).Similarly, the lack of a galanin and consistent VIP changeagrees with the lack of cholinergic deficit found here in
336
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/24/3/325/1839746 by guest on 17 February 2022

Postmortem Studies Schizophrenia Bulletin, Vol. 24, No. 3, 1998
patients with schizophrenia. Data from these neuropeptidestudies are consistent with a deficit of GABAergicintemeurons that are neuropeptide expressing in the cor-tex of persons with schizophrenia and consistent withBenes' observations (Benes et al. 1987, 1991, 1992;Benes 1993).
Somatostatin and neuropeptide Y were both deficientin schizophrenia patients. Neuropeptide Y is co-localizedwithin a larger population of somatostatin-containing neu-rons, the majority of which also exhibit nicotinamide-ade-nine dinucleotide phosphate (NADPH) diaphorase activ-ity (Vincent et al. 1983; Unger and Lange 1992). A reportof altered distribution of NADPH-staining neurons inpostmortem cortices of subjects with schizophrenia(Akbarian et al. 1993a, 1993fc) suggests that disturbedneurodevelopment may contribute to the disorder. It maybe that the population of neurons identified by Akbarian etal. is a subpopulation of somatostatin neurons that alsocontain neuropeptide Y. The involvement of a specificclass of neurons in schizophrenia has implications forunderstanding its pathogenesis, as well as developingunique pharmacotherapeutic approaches.
Overall Implications of These Studies
Differences between patients with schizophrenia, AD, andage-matched controls were not uncommon. Thus, far frombeing a disorder in which postmortem neuropathologicalfindings are a rarity, schizophrenia appears to be charac-terized by multiple possible abnormalities. These andother results raise the question of whether all these differ-ences are real and which, if any, have a meaningful rela-tionship to the core pathology of schizophrenia.
The series reported here is a large one relative toother postmortem samples of schizophrenia. However, thesample is still too small to definitively determine whetherfactors unrelated to the schizophrenia process might reallybe accounting for some of the observed differencesbetween subjects with schizophrenia and other study pop-ulations. For example, PMI, neuroleptic status, length ofinstitutionalization, and periagonal events were variableacross this population. Whereas some patients had beenneuroleptic free for prolonged periods of time, otherswere receiving neuroleptics close to the time of theirdeath. Whereas some patients had a PMI of very fewhours, in other patients the interval was measured in days.Whereas some patients may have been virtually drug freeat the time of their agonal event, others may havereceived multiple cardioactive drugs with central nervoussystem effects just before dying. Certainly, it can be rea-sonably argued that these differences could account forsome of the postmortem findings and those of many other
studies. Even when sample sizes approach 100 patients,the many subgroupings that derive from simply creating amatrix of all possible confounding variables can yieldsample sizes that are still too small to answer specificquestions about the power of particular combinations ofconfounding variables.
Superimposed on these circumstances is the hetero-geneity of the symptoms patients present near the time ofdeath. Some patients are profoundly demented, whereasothers show a relatively normal Mini-Mental State Exam-ination (Folstein et al. 1975) or a CDR score of less than0.5. Also varying from patient to patient is the severity ofpositive and negative symptoms, as well as the balancebetween them. Thus, if one were to ask what SP abnor-malities exist in patients with a postmortem interval under3 hours, who have also been neuroleptic free for over 2years, are nondemented, and possess severe negativesymptoms, despite a sample size of over 100 patients itwould be impossible to generate a cohort of patients largeenough for a meaningful statistical analysis. Hence, thiswork points to the importance of developing multiplelarge brain banks with well-characterized patients andcomparable techniques for brain extraction and process-ing. The notion that any single brain bank can providepatient samples large enough to answer all the post-mortem questions that need to be addressed is at bestunrealistic and at worst will mislead the field for possiblydecades to come.
In part because of the complications that arise from somany potentially confounding variables, an importantaspect of this research has been to answer a seeminglystraightforward question: What is the neurochemical and/orneuropathological basis for the dementia of schizophrenia?Some clear answers to that question can be derived fromthis data base, particularly in terms of what the dementia ofschizophrenia is not. Specifically, it is not a cholinergicdeficit, characterized by neurofibrillary tangles and senileplaques, nor is it associated with the neuropeptidergicabnormalities of AD. It is less clear what the dementia ofschizophrenia is. There are hints that it may be associatedwith diminished serotonergic and noradrenergic function,but this finding needs to be replicated as well as evaluatedin greater detail. Hence, even to the straightforward ques-tion of what the dementia of schizophrenia is in a cohortcharacterized by relative homogeneity, straightforwardanswers still require significantly more investigation.
In conclusion, therefore, schizophrenia's heterogene-ity, which has dogged clinical studies for so long, isbound to be even more problematic in postmortem inves-tigations. As the field advances, it is essential that thisproblem be dealt with by an extensive antemortem evalu-ation of symptoms and by large study populations. Anational, if not international, effort will truly be necessary
337
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/24/3/325/1839746 by guest on 17 February 2022

Schizophrenia Bulletin, Vol. 24, No. 3, 1998 P. Powchik et al.
to coordinate this work and generate the resources neces-sary to apply the very promising methodologies of neuro-biology that are available to study postmortem tissue.
References
Akbarian, S.; Bunney, W.E.; Potkin, S.G.; Wigal, S.B.;Hagman, J.O.; Sandman, C.A.; and Jones, E.G. Altereddistribution of nicotinamide-adenine dinucleotide phos-phate-diaphorase cells in frontal lobe of schizophrenicsimplies disturbances of cortical development Archives ofGeneral Psychiatry, 50:169-177, 1993a.
Akbarian, S.; Vinuela, A.; Kim, J.J.; Potkin, S.G.; Bunney,W.E.; and Jones, E.G. Distorted distribution of nicoti-namide-adenine dinucleotide phosphate-diaphorase neu-rons in temporal lobe of schizophrenics implies anom-alous cortical development. Archives of GeneralPsychiatry, 50:178-187, 19936.
American Psychiatric Association. DSM-III-R:Diagnostic and Statistical Manual of Mental Disorders.3rd ed., revised. Washington, DC: The Association, 1987.
Arnold, S.E.; Franz, B.R.; Gur, R.C.; Gur, R.E.; Shapiro,R.M.; Moberg, PJ.; and Trojanowski, J.Q. Smaller neuronsize in schizophrenia in hippocampal subfields that medi-ate cortical-hippocampal interactions. American Journalof Psychiatry, 152(5):738-748, 1995a.
Arnold, S.E.; Franz, B.R.; and Trojanowski, J.Q. Elderlypatients with schizophrenia exhibit infrequent neurode-generative lesions. Neurobiology of Aging, 15(3):299-303, 1994.
Arnold, S.E.; Gur, R.E.; Shapiro, R.M.; Fisher, K.R.;Moberg, P.J.; and Gibney, M.R. Prospective clinicopatho-logic studies of schizophrenia: Accrual and assessment ofpatients. American Journal of Psychiatry, 152(5):731-737, 19956.
Bajjalieh, S.M., and Scheller, R.H. The biochemistry ofneurotransmitter secretion. Journal of BiologicalChemistry, 270:1971-1974, 1995.
Benes, F.M. Neurobiological investigations in cingulatecortex of schizophrenic brain. Schizophrenia Bulletin,19(3):537-549, 1993.
Benes, F.M.; Majocha, R.; Bird, E.D.; and Marotta, C.A.Increased vertical axon numbers in cingulate cortex ofschizophrenics. Archives of General Psychiatry,44:1017-1021, 1987.
Benes, F.M.; McSparren, J.; Bird, E.D.; SanGiovanni,J.P.; and Vincent, S.L. Deficits in small interneurons inprefrontal and cingulate cortices of schizophrenic andschizoaffective patients. Archives of General Psychiatry,48:996-1001, 1991.
Benes, F.M.; Vincent, S.L.; Alsterberg, G.; Bird, E.D.; andSanGiovanni, J.P. Increased GABAa receptor binding insuperficial layers of cingulate cortex in schizophrenics.Journal of Neuroscience, 12:924-929, 1992.
Bleich, A.; Brown, S.L.; Kahn, R.; and van Praag, H.M.The role of serotonin in schizophrenia. SchizophreniaBulletin, 14(2): 297-315, 1988.
Bogerts, B. Recent advances in the neuropathology ofschizophrenia. Schizophrenia Bulletin, 19(2):431-445,1993.
Breier, A. Clozapine and noradrenergic function: Supportfor a novel hypothesis for superior efficacy. Journal ofClinical Psychology, 55(Suppl. B): 122-225,1994.
Bridge, T.P.; Kleinman, J.E.; Karoum, E; and Wyatt, RJ.Postmortem central catecholamines and antemortem cog-nitive impairment in elderly schizophrenics and controls.Neuropsychobiology, 14(2):57-61,1985.
Browning, M.D.; Dudek, E.M.; Rapier, J.L.; Leonard, S.;and Freedman, R. Significant reductions in synapsin butnot synaptophysin specific activity in the brains of someschizophrenics. Biological Psychiatry, 34:529-535, 1993.
Bruton, C.J.; Crow, T.J.; Frith, CD. ; Johnstone, E.C.;Owens, D.G.C.; and Roberts, G.W. Schizophrenia and thebrain: A prospective cliniconeuropathological study.Psychological Medicine, 20:285-304, 1990.
Cole, B.J., and Robbins, T.W. Forebrain norepinephrine:Role in controlled information processing in the rat.Neuropsychopharmacology, 7:129-141, 1992.
Csernansky, J.G.; King, R.J.; Faustman, W.O.; Moses,J.A.; Poscher, M.E.; and Faull, K.F. 5-HJAA in cere-brospinal fluid and deficit schizophrenic characteristics.British Journal of Psychiatry, 156:501-507, 1990.
Davidson, M.; Harvey, PH.; Powchik, P.; Parrella, M.;White, L.; Knobler, H.Y.; Losonczy, M.F.; Keefe, R.S.E.;Katz, S.; and Frecska, E. Severity of cognitive impairmentin geriatric schizophrenic patients. American Journal ofPsychiatry, 152:197-207, 1995.
Davidson, M.; Harvey, P.D.; Welsh, K.A.; Powchik, P.;Putnam, K.M.; and Mohs, R.C. Cognitive functioning inlate-life schizophrenia: A comparison of elderly schizo-phrenic patients with Alzheimer's disease. AmericanJournal of Psychiatry, 153(10): 1274-1279, 1996.
Davidson, M.; Kahn, R.S.; Stern, R.G.; Hirschowitz, J.;Apter, S.; Knott, P.; and Davis, K.L. Treatment withclozapine and its effect on plasma homovanillic acid andnorepinephrine concentrations in schizophrenia.Psychiatry Research, 46(2):151-163, 1993.Dennison-Cavanagh, M.E.; Papdopoulos, G.; andPranavels, J.G. The emergence of the cortical GAB Aergicneuron: With particular reference to some peptidergic sub-populations. Journal of Neurocytology, 22:805-814, 1993.
338
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/24/3/325/1839746 by guest on 17 February 2022

Postmortem Studies Schizophrenia Bulletin, Vol. 24, No. 3, 1998
Devauges, V., and Sara, SJ. Activation of the noradrener-gic system facilitates an attentional shift in the rat.Behavioral Brain Research, 39:19-29, 1990.
El-Mallakh, R.S.; Kirch, D.G.; Shelton, R.; Fan, K.J.;Pezeshkpour, G.; Kanhouwa, S.; Wyatt, R.J.; andKleinman, J.E. The nucleus basalis of Meynert, senileplaques, and intellectual impairment in schizophrenia.Journal of Neuropsychiatry and Clinical Neurosciences,3(4):383-386, 1991.
Feinberg, I. Schizophrenia: Caused by a fault in pro-grammed synaptic elimination during adolescence?Journal of Psychiatric Research, 17:319-330, 1982.
Foley, P.; Hughes, P.D.; Bradford, H.F.; Ghatei, M.A.;Khandanian, N.; and Bloom, S.R. The presence of neu-ropeptides in GABAergic and cholinergic rat cerebrocorti-cal synaptosome sub-populations. Neuropeptides,23(2):67-72, 1992.
Folstein, M.; Folstein, S.; and McHugh, P. Mini-MentalState: A practical method for grading the cognitive stateof patients for the clinician. Journal of PsychiatricResearch 12:189-198, 1975.
Gabriel, S.M.; Bierer, L.M.; Haroutunian, V.; Purohit,D.P.; Perl, D.P.; and Davis, K.L. Widespread deficits insomatostatin but not neuropeptide Y concentrations inAlzheimer's disease cerebral cortex. NeuroscienceLetters, 155:116-120,1993.
Gabriel, S.M.; Bierer, L.M.; Purohit, D.P.; Perl, D.P.; andHaroutunian, V. Galanin-like immunoreactivity is in-creased in the postmortem cerebral cortex from patientswith Alzheimer's disease. Journal of Neurochemistry,62:1516-1523, 1994.
Gabriel, S.M.; Davidson, M.; Haroutunian, V.; Powchik,P.; Bierer, L.M.; Purohit, D.P.; Perl, D.P.; and Davis, K.L.Neuropeptide deficits in schizophrenia and Alzheimer'sdisease cerebral cortex. Biological Psychiatry, 39:82-91,1996.
Gabriel, S.M.; Haroutunian, V.; Powchik, P.; Honer, W.G.;Davidson, M.; Davies, P.; and Davis, K.L. Increased con-centrations of presynaptic proteins in the cingulate cortexof subjects with schizophrenia. Archives of GeneralPsychiatry, 54<6):559-566, 1997.
Goldman-Rakic, P.S. Working memory dysfunction inschizophrenia. Journal of Neuropsychiatry and ClinicalNeurosciences, 6(4):348-357,1994.
Halliday, G.M.; McCann, H.L.; Pamphlett, R.; Brooks,W.S.; Creasey, H.; McCusker, E.; Cotton, R.G.; Broe,G.A.; and Harper, C.G. Brain stem serotonin-synthesizingneurons in Alzheimer's disease: A clinicopathological cor-relation. Acta Neuropathologica, 84(6):638-650, 1992.
Haroutunian, V.; Davidson, M.; Kanof, P.D.; Perl, D.P.;Powchik, P.; Losonczy, M.F.; McCrystal, J.; Purohit, D.P.;Bierer, L.M.; and Davis, K.L. Cortical cholinergic mark-ers in schizophrenia. Schizophrenia Research, 12:137—144,1994.
Harvey, P.D.; Davidson, M.; Powchik, P.; Parrella, M.;White, L.; and Mohs, R.C. Assessment of dementia inelderly schizophrenics with structured rating scales.Schizophrenia Research, 7:85-90, 1992.
Honer, W.G.; Hu, L.; and Davies, P. Human synaptic pro-teins with a heterogeneous distribution in cerebellum andvisual cortex. Brain Research, 609:9-20, 1993.
Honer, W.G.; Kaufmann, C.A.; and Davies, P.Characterization of a synaptic antigen of interest in neu-ropsychiatric illness. Biological Psychiatry, 31:147-158,1992.
Honer, W.G.; Kaufmann, C.A.; Kleinman, J.E.; Casanova,M.F.; and Davies, P. Monoclonal antibodies to study thebrain in schizophrenia. Brain Research, 500:379—383,1989.
Hughes, C.P.; Berg, L.; Danziger, W.L.; Coben, L.A.; andMartin, R.L. A new clinical scale for the staging ofdementia. British Journal of Psychiatry, 14:566-572,1982.
Joseph, M.H.; Baker, H.F.; Crow, T.J.; Riley, G.J.; andRisby, D. Brain tryptophan metabolism in schizophrenia:A post mortem study of metabolites of the serotonin andkynurenine pathways in schizophrenic and control sub-jects. Psychopharmacology, 62(3):279-285, 1979.
Joyce, J.N.; Shane, A.; Lexow, N.; Winokur, A.;Casanova, M.F.; and Kleinman, J.E. Serotonin uptakesites and serotonin receptors are altered in the limbic sys-tem of schizophrenics (see comments). Neuropsycho-pharmacology, 8(4):315-336,1993.
Kahn, R.S.; Harvey, P.D.; Davidson, M.; Keefe, R.S.E.;Apter, S.; Neale, J.M.; Mohs, R .C; and Davis, K.L.Neuropsychological correlates of central monoaminefunction in chronic schizophrenia: Relationship betweenCSF metabolites and cognitive function. SchizophreniaResearch, 11(3):217-224,1994.
Kaneko, M.; Honda, K.; Kanno, T.; Horikoshi, R.;Monome, T.; Wantanabe, A.; and Kumashiro, H. Plasmafree 3-methoxy-4-hydroxyphenylglycol in acute schizo-phrenics before and after treatment. Neuropsychobiology,25(3): 126-129, 1992.
Kay, S.R.; Fiszbein, A.; and Opler, L.A. The Positive andNegative Syndrome Scale (PANSS) for schizophrenia.Schizophrenia Bulletin, 13(2):261-276, 1987.
Keefe, R.S.E.; Frecksa, E.; Apter, S.H.; Davidson, M.;Macaluso, J.; Hirshowitz, J.; and Davis, K.L. Clinical
339
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/24/3/325/1839746 by guest on 17 February 2022

Schizophrenia Bulletin, Vol. 24, No. 3, 1998 P. Powchik et al.
characteristics of Kraepelinian schizophrenia: Replicationand extension of previous findings. American Journal ofPsychiatry, 153(6):806-811, 1996.
Keshavan, M.S.; Anderson, S.; and Pettegrew, J.W. Isschizophrenia due to excessive synaptic pruning in theprefrontal cortex? The Feinberg hypothesis revisited.Journal of Psychiatric Research, 28(3):239-265, 1994.
Kleinman, J.E.; Casanova, M.F.; and Jaskiw, G.E. Theneuropathology of schizophrenia. Schizophrenia Bulletin,14(2):209-216, 1988.
Lewis, D.A. The catecholaminergic innervation of pri-mate prefrontal cortex. Journal of Neural Transmission,36{Suppl.): 179-200, 1992.
Littleton, J.T., and Bellen, H.J. Synaptotagmin controlsand modulates synaptic-vesicle fusion in a Ca2+-dependentmanner. Trends in Neurosciences, 18(4): 177-183, 1995.
Maas, J.W.; Contreras, S.A.; Miller, A.L.; Berman, N.;Bowden, C.L.; Javors, M.A.; Seleshi, E.; and Weintraub,S.E. Studies of catecholamine metabolism in schizophre-nia/psychosis: II. Neuropsychopharmacology, 8(2): 111-116, 1993.
Maruyama, Y.; Oshima, T.; and Nakajima, E. Current con-cepts: HI. Simultaneous determination of catecholaminesin rat brain by reversed-phase liquid chromatography withelectrochemical detection. Life Sciences, 26:1115-1120,1980.
Mirra, S.S.; Heyman, A.; McKeel, D.; Sumi, S.M.; Brain,B J.; Brownlee, L.M.; Vogel, F.S.; Hughes, J.P.; van Belle,G.; and Berg, L. The Consortium to Establish a Registryfor Alzheimer's Disease (CERAD): Part II. Standardi-zation of the neuropathological assessment of Alzheimer'sdisease. Neurology, 41:479-486, 1991.
Mita, T.; Hanada, S.; Nishino, N.; Kuno, T.; Nakai, H.;Yamadori, T; Mizoi, Y.; and Tanaka, C. Decreased sero-tonin S2 and increased dopamine D2 receptors in chronicschizophrenia. Biological Psychiatry, 21(14): 1407-1414,1986.
Morris, J.C.; Heyman, A.; Mohs, R.C.; Hughes, J.P.; vanBelle, G.; Fillenbaum, G.; Mellits, E.D.; and Clark, C.The Consortium to Establish a Registry for Alzheimer'sDisease (CERAD): Part I. Clinical and neuropsychologi-cal assessment of Alzheimer's disease. Neurology,39:1159-1165, 1989.
Ong, W.Y., and Garey, L.J. Distribution of GABA andneuropeptides in the human cerebral cortex: A light andelectron microscope study. Anatomical Embryology,183(4):397-413, 1991.
Pakkenberg, B. Post-mortem study of chronic schizo-phrenic brains. British Journal of Psychiatry, 151:744-752, 1987.
Pakkenberg, B. The volume of the mediodorsal thalamicnucleus and nucleus accumbens in schizophrenia.Schizophrenia Research, 7:95-100, 1992.
Potkin, S.G.; Weinberger, D.R.; Linnoila, M.; and Wyatt,R.J. Low CSF 5-hydroxyindoleacetic acid in schizo-phrenic patients with enlarged cerebral ventricles.American Journal of Psychiatry, 140:21-25, 1983.
Powchik, P.; Davidson, M.; Nemeroff, C.B.; Haroutunian,V.; Losonczy, M.; Bissette, G.; Perl, D.P.; Ghanbari, H.;Miller, B.; and Davis, K.L. Alzheimer's disease relatedprotein in geriatric schizophrenic patients with cognitiveimpairment. American Journal of Psychiatry, 150:1726-1727, 1993.
Prohovnik, I.; Dwork, A.J.; Kaufman, M.A.; and Willson,N. Alzheimer-type neuropathology in elderly schizophre-nia patients. Schizophrenia Bulletin, 19(4):805-816,1993.
Purohit, D.P.; Davidson, M.; Perl, D.P.; Powchik, P.;Haroutunian, V.; Bierer, L.; McCrystal, J.; Losonczy, M.;and Davis, K.L. Severe cognitive impairment in schizo-phrenic patients: A clinicopathological study. BiologicalPsychiatry, 33:255-260, 1993.
Rogers, J.H. Immunohistochemical markers in rat cortex:Co-localization of calretinin and calbindin-D28k withneuropeptides and GABA. Brain Research, 587(1): 147-157, 1992.
Roth, B.L., and Meltzer, H.Y. The role of serotonin inschizophrenia. In: Psychopharmacology: The FourthGeneration of Progress. Bloom, F.E., and Kupfer, D.J.,eds. New York, NY: Raven Press, 1995. pp. 1215-1227.
Shapiro, R.M. Regional neuropathology in schizophrenia:Where are we? Where are we going? SchizophreniaResearch, 10:187-239, 1993.
Sollner, T; Whiteheart, S.W.; Brunner, M.; Erdjument-Bromage, H.; Geromanos, S.; Tempst, P.; and Rothman,J.E. SNAP receptors implicated in vesicle targeting andfusion. Nature, 362:318-325,1993.
Sower, A.C.; Bird, R.D.; and Perrone-Bizzozero, N.J.Increased levels of GAP-43 protein in schizophrenic braintissues demo'nstrated by a novel immunodetectionmethod. Molecular and Chemical Neuropathology,24(1):1-11, 1995.
Stern, Y; Gurland, B.; Taternichi, T.K.; Tang, M.; Wilder,D.; and Mayeux, R. Influence of education and occupa-tion on the incidence of Alzheimer's disease. Journal ofthe American Medical Association, 271:1004-1010, 1994.
Tamlyn, D.; McKenna, P.J.; Mortimer, A.M.; Lund, C.E.;Hammond, S.; and Baddeley, A.D. Memory impairmentin schizophrenia: Its extent, affiliations and neuropsycho-logical character. Psychological Medicine, 22:101-115,1992.
340
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/24/3/325/1839746 by guest on 17 February 2022

Postmortem Studies Schizophrenia Bulletin, Vol. 24, No. 3, 1998
Unger, J.W., and Lange, W. NADPH-diaphorase-positivecell population in the human amygdala and temporal cor-tex: Neuroanatomy, peptidergic characteristics andaspects of ageing and Alzheimer's disease. Acta Neuro-pathologica, 83:636-646, 1992.
van Kammen, D.P.; Agren, H.; Yao, J.K.; O'Connor, D.T.;Gurklis, J.; and Peters, J.L. Noradrenergic activity andprediction of psychotic relapse following haloperidolwithdrawal in schizophrenia. American Journal ofPsychiatry, 151(3):379-384,1994.
Vincent, S.R.; Johansson, O.; Hokfelt, T.; Skirboll, L.;Elde, R.P.; Terenius, L.; Kimmel, J.; and Goldstein, M.NADPH-diaphorase: A selective histochemical marker forstriatal neurons containing both somatostatin- and avianpancreatic polypeptide (APP)-like immunoreactivities.Journal of Comparative Neurology, 217(3):252-263,1983.
Weinberger, D.R. A connectionist approach to the pre-frontal cortex. Journal of Neuropsychiatry and ClinicalNeurosciences, 5:241-253, 1993.
Weinberger, D.R.; Berman, K.F.; and Illowsky, B.P.Physiological dysfunction of dorsolateral prefrontal cor-tex in schizophrenia: HI. A new cohort and evidence for a
monoaminergic mechanism. Archives of GeneralPsychiatry, 89:49-59, 1988.
Acknowledgments
This research was supported by USPHS grantsMH-46436 to Michael Davidson and Peter Powchik andMH-45212 to Kenneth L. Davis from the NationalInstitute of Mental Health, and a Veterans Affairs MeritReview Grant to Vahram Haroutunian.
The Authors
Peter Powchik, M.D., is Assistant Professor of Psychiatry;Michael Davidson, M.D., is Professor of Psychiatry;Vahram Haroutunian, Ph.D., is Associate Professor ofPsychiatry; Stephen M. Gabriel, M.D., is AssistantProfessor of Psychiatry; Dushyant P. Purohit, M.D., isAssistant Professor of Psychiatry; Daniel P. Perl, M.D., isProfessor of Psychiatry and Pathology; Philip D. Harvey,Ph.D., is Associate Professor of Psychiatry; and KennethL. Davis, M.D., is Professor and Chairman, Departmentof Psychiatry, ML Sinai Medical Center, New York, NY.
341
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/24/3/325/1839746 by guest on 17 February 2022