Embed Size (px)
Citation preview

Studying late-onset schizophrenia and non schizophrenia
psychosis in elderly Egyptian patientsHanan Husseina, Ahmed El Shafeia, Marwa Abd El Meguidb, Marwa El Missiryb
and Mahmoud Tamarac
Departments of aNeuropsychiatry,bNeuropsychychiatry and cGeriatric, Faculty ofMedicine, Ain Shams University, Cairo, Egypt
Correspondence to Marwa Abd El Meguid, MD,Department of Psychiatry, Institute of Psychiatry, 65 ElNozha Street, Heliopolis, Cairo, EgyptTel: + 002 0105752536; fax: + 202 22678032;e-mail: [email protected]
Received 19 May 2011Accepted 12 August 2011
Middle East Current Psychiatry
2012, 19:12–22
Background
In Egypt, the proportion of elderly people in the population is increasing markedly;
cases of late-life psychoses are increasing at a rapid pace as the population of the
world ages, and this will create a tremendous economic burden on the society
because of the increasing rates of disability.
Aim
The aim of this work was to compare the sociodemographic and clinical
characteristics, daily living functioning, and cognitive impairment between late-onset
schizophrenia and other late-onset psychotic disorders.
Patients and methods
A cross-sectional comparative study was conducted on 100 patients: 50 patients with
schizophrenia with onset after the age of 50 years (group A) and 50 patients with
nonschizophrenia late-onset psychoses (group B). All patients were interviewed using The
Structured Clinical Interview for Diagnostic and Statistical Manual of Mental Disorders
Axis-I diagnosis were assessed using the Positive and Negative Syndrome Scale, the
Functional Assessment of Activity of Daily Living scale, section B of the Cambridge Mental
Disorders of the Elderly Examination, and the Wechsler Adult Intelligence Scale.
Results
Patients in group A were significantly younger – they were mainly women (72%), the
majority were never married (54%), and 62% were living alone – compared with group
B, who were mainly married (46%) and lived more often with their families. Among
patients with late onset schizophrenia spectrum, 70% had paranoid subtype, 12% had
delusional disorder and the rest had either undifferentiated or schizoaffective subtype.
On the other hand, 70% of group B patients had psychotic symptoms due to dementia,
20% had mood disorder with psychotic symptoms; and the rest 10% had psychosis
secondary to medical illnesses. (Group B) patients had significantly lower scores on
items assessing positive symptoms and higher scores on general psychopathology
than did (Group A) patients, the scores on negative symptoms, and also the total
PANSS scores were almost similar in both groups and did not show any significant
differences. Group A patients scored significantly better in daily living functioning,
whereas a significant number of patients of group B needed partial and complete
support. Cognitive assessment revealed that group A patients scored almost within
norms, except for memory, apraxia, abstract, and perception items, compared with
group B patients who scored significantly lower in all cognitive items.
Conclusion
Patients with late-onset schizophrenia compared with patients with other late-onset
psychoses differ in a number of psychosocial and clinical variables, daily functioning,
and cognitive abilities. The results of this study contribute to the development of a
better understanding of the elderly patient population with different types of late-onset
psychoses, which have been largely ignored in research.
Keywords:
activities of daily living, cognitive functions, late-onset psychoses, late-onset
schizophrenia
Middle East Curr Psychiatry 19:12–22& 2012 Okasha Institute of Psychiatry, Ain Shams University2090-5408
Introduction
Worldwide, the number of persons aged 65 years or older
has increased from 17 million in 1900 to 342 million in
1992 and is expected to increase to 2.5 billion (compris-
ing 20% of the total population) by 2050 [1]. In other
words, the proportion of elderly people in this population
will increase by 65%. In the next 30 years, life expectancy
12 Original article
2090-5408 & 2012 Okasha Institute of Psychiatry, Ain Shams University DOI: 10.1097/01.XME.0000407866.00571.95
Copyright © Institute of Psychiatry, Ain Shams University. Unauthorized reproduction of this article is prohibited.

will increase markedly in western countries, and it is
expected to increase further [2]. In Egypt, there is
a marked increase in the proportion of elderly people in
the population; according to ‘The Statistical Year Book
2009,’ [3] people above 60 years of age constitute 6% of
the Egyptian population and this proportion is expected
to reach 11.5% by the year 2025 with the mean life
expectancy around 70.1 years [4].
Cases of late-life psychoses are increasing markedly as the
population of the world ages, and this will create a
tremendous economic burden on the society because of
the increasing rates of disability and institutionaliza-
tion [5]. It is worth mentioning that Khouzam et al. [6]
reported that up to 23% of the elderly population will
experience psychotic symptoms that may increase the
suffering of patients, family, and caregivers [5].
There is a growing awareness that late-onset psychoses
constitute a heterogenous group of serious disorders of a
complex nature, which present in different forms with
different etiologies [7,8]. These conditions include
delusional disorders, induced psychotic disorders, late-
onset schizophrenia, psychosis associated with dementia,
mood disorders with prevailing psychotic symptoms, and
others [9,10]; clinicians must remember the nonspecific
nature of psychotic symptoms to avoid errors in diagnosis
[11]. Controversy still surrounds the differential diag-
nosis of psychoses that begin late in life [12,13]. The
nosology, classification, and biological basis of psychoses
in the elderly have been much debated; primary and
secondary psychotic disorders of late life and their etiology
are commonly considered from the view point of risk
factors such as genetic predisposition triggering life events
and organic cerebral dysfunction [11]. In a recent study
by Woolley et al. [13], a total of 28.2% of patients with
a neurodegenerative disease received a prior psychiatric
diagnosis of a psychotic nature, as neurodegenerative
diseases are often misdiagnosed as psychiatric disorders.
Late-onset schizophrenia refers to schizophrenia or a
related disorder (schizoaffective, schizophreniform, or
delusional disorder) with onset of prodromal symptoms
after the age of 50 years [8]. According to Diagnostic andStatistical Manual of Mental Disorders (DSM)-III-R, the
onset of symptoms, including prodromal symptoms, must
be after the age of 45 years. DSM-IV, however, does not
specify the term ‘late onset,’ nor does it set an upper age
limit for the diagnosis of schizophrenia [9]. Although
DSM-IV and DSM-IV-TR criteria do not include codeable
diagnoses for late-onset schizophrenia, DSM-IV and
DSM-IV-TR mention differences between cases of
schizophrenia with onset after 50 years compared with
those with earlier onset. Moreover, DSM-III-R included a
late-onset category for patients with initial presentation
at the age of 50 years or later [10].
Different studies suggest that there are specific risk
factors for late-onset schizophrenia that could be identi-
fied; these include female sex, visual, auditory sensory
impairments, and premorbid schizoid personality [7].
In Egypt, with the increased longevity of life and the
change in family system toward a nuclear one, together
with the increased medical, psychiatric, and behavioral
problems in the aged population, there is a great
necessity to have carefully designed plans for mental
health promotion of the elderly [14]. There is clearly an
enormous need to clarify the clinical characteristics and
range of dysfunction in cases of late-onset psychoses to
streamline treatment recommendation for the already
complex and vulnerable elderly population, aiming to
minimize the cost of these devastating disorders through
early recognition and fast intervention.
Aim of the workThe aim of the current study was to compare the
sociodemographic and clinical characteristics, daily func-
tioning, and cognitive impairment between patients with
late-onset schizophrenia and those with other late-onset
psychotic disorders.
Patients and methodsDesign
The study design was cross-sectional and comparative in
nature, and the sample was selective. A total of 100
patients were enrolled in a 1-year period from March 2008
to February 2009; they were selected and divided into
two groups, A and B, as mentioned below.
Group A comprised 50 patients fulfilling the diagnosis of
schizophrenia and other psychotic disorders according to
DSM-IV. We also used the operational definition accord-
ing to the consensus statement by the International Late-
Onset Schizophrenia Group, which stated that the term
could be applied to those cases with onset of prodromal
symptoms after the age of 50 years and refers to
schizophrenia or a related disorder (schizoaffective,
schizophreniform, or delusional disorder) [8]. Both male
and female patients were recruited from among the
inpatients and outpatients attending the Geriatric
Hospital and Institute of Psychiatry, Ain Shams Uni-
versity Hospitals. Some cases were also recruited from
Abbasseya State Hospital because of the rarity of cases
fulfilling the following inclusion and exclusion criteria:
patients should have developed schizophrenia after the
age of 50 years; and patients should not have a life-time
history of schizophrenia, other psychoses including
schizoaffective disorder, paranoid disorder, or psychotic
symptoms secondary to other mental or general medical
disorders or dementia.
Group B comprised 50 male and female patients fulfilling
the diagnosis of late-onset nonschizophrenia psychoses
developed after the age of 50 years, including psychotic
disorders due to general medical conditions, mood
disorders with psychotic features, and dementia with
delusions and hallucinations. Patients with life-time history
of schizophrenia, schizoaffective disorder, mood disorder,
delirium, or late-stage dementia were excluded. Patients
Late-onset schizophrenia and nonschizophrenia psychosis Hussein et al. 13
Copyright © Institute of Psychiatry, Ain Shams University. Unauthorized reproduction of this article is prohibited.

were recruited mainly from inpatient and outpatient clinics
of Geriatric Ain Shams University Hospital.
Ethical issue
Ethical approval of the research protocol was obtained from
the Ain Shams University Ethical and Research Commit-
tee. The researchers described the study to the patients or
their guardians, ensured confidentiality of information, and
obtained their informed consent for participation. It was
stated that participation in the study was voluntary and
that they have the freedom to withdraw from the
assessment at any time. Informed written consent from
patients or their guardians was obtained. All 50 cases in
each study group who fulfilled the research criteria and
gave their consent were subjected to preliminary clinical
evaluation including history of illness obtained from the
patient and his or her family. Physical and neurological
examinations were conducted by a Gerontologist Specialist.
The research team also revised the medical files and
investigations of all patients.
Tools and procedures
All patients underwent the following examinations:
(a) clinical assessment, (b) assessment of daily function-
ing, (c) cognitive assessments, and (d) Fahmy and
El-Sherbini’s Social Classification Scale.
Clinical assessments included the Structured Clinical
Interview for DSM Axis-I diagnosis – clinical version [15]
and the Positive and Negative Syndrome Scale
(PANSS) [16]. The PANSS was designed to measure
the severity of psychopathology in adult patients with
schizophrenia, schizoaffective disorder, and other psycho-
tic disorders.
Assessment of daily functioning included activities of
daily living (ADL) and instrumental activities of daily
living (IADL).
The ADL scale [17] assesses certain basic abilities that a
person must possess to remain at home independently.
These abilities allow a person to perform basic self-care
tasks. Accordingly, patients were classified into the
following groups: needs no support (10), needs partial
support (six to nine), or needs full support (zero to five).
The Arabic standardized version was used [18]. The
IADL scale [17] measures two broad categories: (a) basic
self-maintenance behaviors such as feeding, dressing,
bathing, and mobility, and (b) more complex behaviors
such as managing finances, traveling, and taking medica-
tions. These abilities are higher-level abilities that allow a
person to function independently at home or in the
community. Accordingly, patients were classified into the
following groups: needs no support (10), needs partial
support (six to nine), or needs full support (zero to five).
We used the Arabic standardized version [18].
Cognitive assessments included Cambridge Mental Dis-
orders of the Elderly Examination (CAMDEX) scale [19]
and the Wechsler Adult Intelligence Scale (WAIS).
The CAMDEX scale [19] was developed to assess the
diagnosis and measurement of dementia among the
elderly. This scale assessed orientation, language (ex-
pression, comprehension), memory (both recent and
remote), and learning praxis, attention, abstract thinking,
perception, and calculation. It was translated into Arabic
and validated by Mahmoud et al. [20]. The WAIS [21] is
the most commonly administered general intelligence
test for adults, and it is also viewed as a broad assessment
of cognitive functions. The Wechsler scale provides
information about the important aspects of the patients’
intellectual functioning. We used the standardized Arabic
version of the test [22].
Fahmy and El-Sherbini’s Social Classification Scale [23] is
based on parameters such as education and work of the
father, education and work of the mother, income
crowding index, and sanitation.
Statistical analysis
Data were statistically analyzed using the Statistical
Package for Social Sciences program software version 17.0.
(SPSS Inc., Illinois, Chicago) Descriptive statistics were
obtained for numerical parametric data as means and SD and
for categorical data as number and percentage. Inferential
analyses were performed for quantitative variables using
Student’s t-test for independent data. Qualitative data were
analyzed using Pearson’s w2-test. The level of significance
was taken at P-value less than 0.05; otherwise, it was
considered nonsignificant.
ResultsTo fulfill the aim of the work, we compared the studied
groups with each other with regard to their socio-
demographic characteristics, clinical data, ADL, and
cognitive functioning.
Demographic data
Patients in group A were significantly younger (mean age
69.5 ± 3.39) – they were mainly women (72%), the
majority were never married (54%), and 62% were living
alone – compared with group B (mean age 72.5 ± 2.26),
who were mainly married (46%) and lived more often
with their families. Social class did not show any
statistical differences between the groups.
A total of 54% of group A patients graduated from
secondary schools and universities compared with only
38% of group B patients. Previous engagement in
different occupations showed striking differences, as a
higher percentage of group B patients were engaged in
jobs previously compared with group A patients
(P = 0.000). Details are illustrated in Table 1.
Age at onset, duration of illness, and family history of
psychiatric illness
Patients in group A developed their illness significantly
earlier (P = 0.001) and had longer duration of illness than
did patients in group B. Although group A patients had
higher frequency of positive family history of psychiatric
disorders compared with group B patients (8 and 4%,
14 Middle East Current Psychiatry
Copyright © Institute of Psychiatry, Ain Shams University. Unauthorized reproduction of this article is prohibited.

respectively), the difference was not statistically signifi-
cant (P40.05) (Table 1).
Medical history
Group A patients had significantly (P = 0.000) more
chest diseases (72%), auditory impairment (30%), and
musculoskeletal problems (66%) compared with group B
patients; in contrast, group B patients had significantly
(P = 0.000) more renal (56%) and neurological diseases
(50%) than group A patients. No statistically significant
difference was found between the two groups with regard
to diabetes mellitus, hypertension, cardiac diseases, and
visual impairment (Table 2).
Clinical data
Diagnostic categories
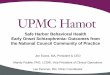
Data represented in Fig. 1a show that, among patients
with late-onset schizophrenia, 70% had paranoid subtype,
12% had delusional disorder, and the remaining had either
undifferentiated or schizoaffective subtype. In contrast,
70% of group B patients with other late-onset psychoses
had psychotic symptoms due to dementia, 20% had mood
disorder with psychotic symptoms, and the remaining 10%
had psychosis secondary to medical illnesses (Fig. 1b).
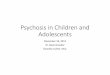
Assessment of psychotic symptoms using Positive and
Negative Syndrome Scale
Figure 2 illustrates clearly that group B patients had
significantly lower scores on items assessing positive
symptoms (including delusions, conceptual disorganiza-
tion, and hallucinatory behavior) and higher scores on
general psychopathology (including somatic concern,
anxiety, guilt feelings) than did group A patients; the
scores on negative symptoms (including blunted affect,
emotional withdrawal, poor rapport) and the total PANSS
scores were almost similar in both groups and did not
show any significant differences.
The nature and content of delusions differ from that of
group A patients who had more complex bizarre delusions
of control, passivity, and persecution in comparison with
group B patients with dementia who exhibited simple
paranoid delusion and also delusions of someone stealing or
Table 1 Sociodemographic variables
Group A Group B
Patients with late-onset schizophrenian = 50
Patients with nonschizophrenia late-onset psychosesn = 50
No % No % Test
Age, mean ± SD 69.5 ± 3.39 72.5 ± 2.26 Test used t-testP = 0.000 (VHS)
Age of onset, mean ± SD 57.24 ± 6.6 69.82Duration of illness, mean ± SD 14.06 2.68Sex
Females 36 72% 26 52% w2 = 6.0Males 14 28% 24 48% P = 0.014 (Sig)
Marital statusMarried 14 28% 23 46% w2 = 40.67Never married 27 54% 3 6% d.f. = 3Divorced 5 10% – – P = 0.000Widow 4 8% 24 48% (VHS)
Living statusSpouse 5 10% 19 38% w2 = 54.03Children 3 6% 16 32%Others 1 2% 8 16% d.f. = 4Family 10 20% 7 14% P = 0.000Alone 31 62% – – (VHS)
EducationIlliterate 7 14% 6 12% w2 = 6.52Read and write 8 16% 9 18% d.f. = 5.0Primary school 3 6% 10 20% P = 0.025Preparatory school 5 10% 6 12% (Sig)Secondary school 21 42% 12 24%University 6 12% 7 14%
Previous occupationNone 27 54% 7 14% w2 = 20.45Professional 8 16% 16 32% d.f. = 3.0Semiprofessional 4 8% 2 4% P = 0.000Skilled and others 11 22% 25 50% (VHS)
Social classHigh 9 18% 10 20% w2 = 1.124High middle 6 12% 3 6% d.f. = 3Low middle 8 16% 8 16% P = 0.771Low 27 54% 29 58% (Insig)
Family history of psychiatric illnessYes 4 8% 2 4% P40.05No 46 92% 48 96% (Insig)
d.f., degree of freedom; Insig, insignificant; Sig, significant; VHS, very highly significant.
Late-onset schizophrenia and nonschizophrenia psychosis Hussein et al. 15
Copyright © Institute of Psychiatry, Ain Shams University. Unauthorized reproduction of this article is prohibited.

hiding objects. Group B patients with depression described
somatic, hypochondriacal delusions. In addition, some
patients had delusions of guilt and nihilism, and others
had noncongruent delusions of persecution and reference.
The pattern of hallucinations in group A patients showed
multimodal hallucinations, mainly auditory, tactile, and
olfactory hallucinations. Schneiderian first-rank symptoms
such as hearing multiple voices or running commentary were
recorded in this group, whereas group B patients with
dementia had mainly visual hallucination. Group B patients
with mood disorder had auditory and olfactory hallucinations.
Functional assessment of the ADL scores revealed that
group A patients had significantly better ADL and IADL
scores, whereas a significant number of group B patients
needed partial and complete support compared with
group A patients (Table 3).
Cognitive assessment
Using section B (CAMCOG) of the CAMDEX it was
revealed that group A patients scored almost within
norms, except for memory, apraxia, abstract, and percep-
tion items, compared with group B patients who scored
lower in all cognitive items. Group A patients compared
with group B showed highly statistically significant dif-
ferences in the following parameters: language, memory,
abstract, and perception (P = 0.000). Their scores on
orientation, attention, and apraxia were significantly
lower at the following levels of significance: 0.004, 0.02,
and 0.001, respectively (Table 4).
On the WAIS, patients with late-onset schizophrenia
scored significantly better in all total and subitems of the
test. It was noticed that a very highly statistically significant
difference exists between both groups with regard to total,
performance, and verbal intelligence quotient scores, being
lower in group B than in group A. Both groups showed
discrepancy between verbal and performance intelligence
quotient, which denotes cognitive decline (Table 5).
DiscussionPsychotic manifestations constitute an important pro-
blem in the geriatric population. Some authors have
reported that psychosis was present in 26% of elderly
patients admitted to an inpatient geriatric unit and in
36% of patients admitted for the first time to a
psychiatric facility [24]. Within the psychiatric ward,
cases showing an onset after 40 years of age comprised
10.8% of the total population [25]. Early detection and
management of psychotic symptoms is associated with a
better psychosocial adjustment [24].
This study aimed to uncover some clinical aspects in a
sample of the Egyptian elderly population. The research
aimed to study a group of elderly patients with primary
psychotic disorders that appear for the first time after
the age of 50 years (group A), including schizophrenia,
delusional disorder, and schizoaffective disorders, and
compare them with a group of elderly patients
with psychotic disorders other than schizophrenia (group
B), which include psychosis associated with dementia,
Table 2 Medical history: a comparison between patients with late-onset schizophrenia and nonschizophrenia late-onset psychoses
Group A Group B
Patients with late-onset schizophrenian = 50
Patients with nonschizophrenia late onset psychosesn = 50
No % No % Test
Diabetes+ ve 19 38% 11 22% w2 = 3.04– ve 31 62% 39 78% P = 0.08 (Insig)
Cardio vascular diseases+ ve 21 42% 17 34% w2 = 0.679– ve 29 58% 33 66% P = 0.410 (Insig)
Chest diseases+ ve 36 72% 14 28% w2 = 19.36– ve 14 28% 36 72% P = 0.000 (VHS)
GIT diseases+ ve 25 50% 15 30% w2 = 4.167– ve 25 50% 35 70% P = 0.04 (Sig)
Renal diseases+ ve 6 12% 28 56% w2 = 21.569– ve 44 88% 22 44% P = 0.000 (VHS)
CNS diseases+ ve 8 16% 25 50% w2 = 13.07– ve 42 84% 25 50% P = 0.000 (VHS)
Visual impairment+ ve 18 36% 14 28% w2 = 0.735– ve 32 64% 36 72% P = 0.391 (Insig)
Auditory impairment+ ve 15 30% 5 10% w2 = 6.750– ve 35 70% 45 90% P = 0.01 (Sig)
Musculo skeletal problems+ ve 33 66% 12 24% w2 = 17.818– ve 17 34% 38 76% P = 0.000 (VHS)
Insig, insignificant; Sig, significant; – ve, negative; + ve, positive; VHS, very highly significant.
16 Middle East Current Psychiatry
Copyright © Institute of Psychiatry, Ain Shams University. Unauthorized reproduction of this article is prohibited.

mood disorders, and psychosis secondary to medical
conditions.
Demographic variables
Late-onset schizophrenia affects women two to 10 times
more than it does men [8,10]. With regard to sex, 72% of
patients with late-onset schizophrenia were significantly
predominantly women compared with only 52% of patients
with late-onset other psychoses. This result was in
accordance with a previous study by Howard et al. [8]. In
the Egyptian community, Ashour et al. [26] found that the
ratio between men and women was 1 : 3 among the elderly
with different psychiatric morbidities in Cairo hostels. The
preponderance of female patients in the group of late-onset
schizophrenia was also recorded previously by Haiba [27],
who studied paranoid symptoms in the elderly population
in Egypt. Recently in China, Yasuda and Kato [25] found
that female patients comprised 16.3%, which was signifi-
cantly higher than that of male cases (2.0%). The
robustness of this finding, coupled with the higher
incidence rates of early-onset schizophrenia in men, led
to the estrogen hypothesis, which postulates that estradiol
has antidopaminergic properties that somehow protect
women to a certain degree from puberty to menopause.
As estradiol levels decrease at midlife, this protective factor
is lost, thus predisposing vulnerable women to a second
illness-onset peak after the age of 45 years because of the
decline in estrogen with relative excess of dopamine D2
receptors [28].
Social isolation has been linked to late-onset schizophrenia;
it either plays a role in causation or may be the
consequence [29]. In our research, we found that patients
with late-onset schizophrenia were predominantly never
married or were divorced; a significant proportion of them
were living alone compared with the group of nonschizo-
phrenia late-onset psychosis patients. Our results agreed
with those of previous national and international research-
ers who found that social isolation, living alone, having no
friends, and having no regular visitors are associated with
late-onset schizophrenia [27,29,30].
Genetic factors seem to play a smaller role in the etiology
of late-onset schizophrenia [8]. Our results showed that
there were no significant differences with regard to family
history of psychiatric disorders among both studied
groups, consolidating the above-mentioned findings.
Medical history
Late-life psychotic symptoms often have a medical
etiology and may be the first symptoms of undiagnosed
medical conditions. This is because elderly people usually
take several medications with possible side effects and
drug interactions, which may contribute to the appear-
ance of psychotic symptoms [6,7].
Group B patients had significantly more frequent renal
and neurological diseases. It was also reported in Egyptian
communities that cognitive and behavioral changes were
frequently encountered in elderly patients with renal
impairment [31]. In addition, Mostafa et al. [32] had
reported a high prevalence of neurological incidents among
elderly patients presenting with psychiatric symptoms.
Group A patients with late-onset schizophrenia compared
with their group B counterparts had significantly more
frequent chest diseases, probably because of excessive
smoking, more musculoskeletal problems, and auditory
impairment, which add to their social isolation. We are in
agreement with previous studies that found that some
evidence exists of an association between sensory deficits
and psychotic symptoms [33,34]; moreover, some have
Figure 1
0%
70%
4%
0%
12%
14%
0% 10% 20% 30% 40% 50% 60% 70% 80%
Residual Schizo.
Paranoia Schizo.
Undiff. Schizo.
Disorganized Schizo.
Delusional Dis.
Schizoaffective
(a)
(b)
Residual Schizo. Paranoid Schizo. Undiff. Schizo.Disorganized Schizo. Delusional Dis. Schizoaffective
20%
70%
10%
Mood dis. With psychotic featuresPsychosis due to dementiaOthers
(a) Diagnostic categories: late-onset schizophrenia. (b) Diagnosticcategories: late-onset other psychoses.
Figure 2
35.621.5
58.1
115.2 114.6
29.621.9
63.1
0
20
40
60
80
100
120
140
Positivesymptoms
Negativesymptoms
Generalpsychopathology
Total PANSS
Group (A) Group (B)
P=0.001 P=0.634Insig.
p=0.01Sig.Sig.
p=0.06Sig.
Assessment of psychotic symptoms by PANSS: a comparison betweenpatients with late-onset schizophrenia (group A) and nonschizophrenialate-onset psychoses (group B). PANSS, Positive and NegativeSyndrome Scale.
Late-onset schizophrenia and nonschizophrenia psychosis Hussein et al. 17
Copyright © Institute of Psychiatry, Ain Shams University. Unauthorized reproduction of this article is prohibited.

suggested that late-onset schizophrenia might reflect the
impact of sensory deprivation due to uncorrected visual
and hearing deficits associated with aging [35].
Diagnostic categories
The majority of group B patients (70%) had psychosis due
to dementia, whereas 20% had mood disorder with
psychotic features, and 10% had psychosis secondary to
medical illnesses. Our results are not in agreement with
the study by Barclay and Almeida [36], who reported that
the most frequent clinical diagnoses for elderly patients
with psychotic symptoms other than schizophrenia were
dementia (40%), depression (33%), psychosis secondary
to a medical condition (7%), bipolar disorder (5%), and
the remaining due to adverse reaction to medication. Jeste
and Finkel [37] stated that the incidence of psychosis
in dementia was 30–50%, whereas Paulsen et al. [38]
reported that approximately 50% of dementia patients will
have psychotic symptoms, predominantly delusions and
hallucinations. The difference between our results and
the above-mentioned findings could be attributed to the
difference in sampling methods and techniques.
The diagnosis of paranoid disorder was by far the most
diagnostic type of schizophrenia encountered in our late-
onset schizophrenia group (70%), whereas only 12% had
delusional disorder and 14% had schizoaffective disorder.
Only 4% had undifferentiated schizophrenia. In their
study, Yasuda and Kato [25] found that the paranoid type
comprised 55.3% of the total population of late-onset
Table 3 Functional assessment of daily living: a comparison between patients with late-onset schizophrenia and nonschizophrenia
late-onset psychoses
Group A Group B
Patients with late-onset schizophrenian = 50
Patients with nonschizophrenialate-onset psychoses
n = 50
No % No % Test
(a) ADLADL (mean ± SD) 12.8 ± 9.8 7.5 ± 2.2 t = 3.7
P40.000 (VHS)Need complete support (0–5) 2 4% 5 10% w2 = 48.33Need partial support (6–0.9) 4 8% 31 62% d.f. = 2No need for support (10–12) 44 88% 14 28% P = 0.000 (VHS)
(b) IADLIADL (mean ± SD) 12.31 ± 2.81 7.6 ± 3.1 t = 4.9
P40.000 (VHS)Need complete support (0–5) 2 4% 18 36% w2 = 49.86Need partial support (6–0.9) 8 16% 20 40% d.f. = 2No need for support (10–12) 42 84% 12 24% P = 0.000 (VHS)
ADL, activities of daily living; d.f.,degree of freedom; IADL, instrumental activities of daily living; VHS, very highly significant.
Table 4 Comparison between patients with late-onset schizophrenia and nonschizophrenia late-onset psychoses
Group AMean ± SD
Group BMean ± SD
Patients with late-onset schizophrenian = 50
Patients with nonschizophrenialate-onset psychoses
n = 50 Test
Orientation 9.08 ± 1.00 5.32 ± 1.39 t = 15.47P = 0.004 (Sig)
Language 18.7 ± 2.18 15.26 ± 4.03 t = 14.61P = 0.000 (VHS)
Memory 17.20 ± 2.64 11.52 ± 5.45 t = 6.628P = 0.000 (VHS)
Attention 5.74 ± 2.38 3.1 ± 1.32 t = 12.03P = 0.02 (VHS)
Apraxia 9.45 ± 2.15 5.12 ± 2.0 t = 6.7P = 0.001 (Sig)
Abstract 4.46 ± 2.0 2.3 ± 0.7 t = 41.49P = 0.000 (VHS)
Perception 5.96 ± 1.3 4.02 ± 1.15 t = 7.76P = 0.000 (VHS)
Total 70.59 ± 13.65 46.64 ± 16.04 t = 17.0P = 0.00 (VHS)
Norms according to the Egyptian sampleOrientation Language Memory Attention Apraxia Abstract Perception9.2 ± 1.0 21.9 ± 2.6 20.7 ± 3.6 5.1 ± 1.9 10.1 ± 2.0 5.3 ± 3.2 7.8 ± 1.8
Sig, significant; VHS, very highly significant
18 Middle East Current Psychiatry
Copyright © Institute of Psychiatry, Ain Shams University. Unauthorized reproduction of this article is prohibited.

cases. The higher prevalence of paranoid schizophrenia in
our sample compared with other studies could not be
interpreted because our sample is a selective sample
rather than a random one.
Clinical picture
Symptoms of psychosis associated with late-onset schizo-
phrenia were different from that of other late-onset
psychoses. Delusions reported in dementia patients were
typically simple, nonbizarre, and of the paranoid type, for
example, morbid jealousy and delusions related to someone
stealing or hiding objects. A number of researchers have
found that delusions and hallucinations are commonly
associated with aggression, agitation, and disruptive behav-
ior in patients with dementia [39–41]. Patients with late-
onset schizophrenia tended to have complex bizarre
systematized delusions, example persecutory delusions
and suffering from a disease or spouse infidelity. Delusions
in patients with mood disorders were characterized by
somatic, hypochondriacal, guilty, or nihilistic delusions, and
also by noncongruent delusions such as persecution and
reference. These results were similar to previous findings
in the elderly Egyptian population [42–44]. From the
clinical point of view, Alexopoulos et al. [45] stated that
depressive delusions can be distinguished from delusions in
patients with dementia, in that the latter are less system-
atized and less congruent to the affective disturbance.
Controversy surrounds the differential diagnosis of
hallucinations that begin late in life [40,46]. In our study,
we reported that hallucinations in dementia were more
frequently visual than auditory; the reverse is true for
patients with schizophrenia who had multimodal hallu-
cinations. Patients with psychotic symptoms associated
with depression had mainly auditory and olfactory
hallucinations.
The severity of positive, negative, and general psycho-
pathologic symptoms was measured with the respective
subscales of PANSS. Data revealed that patients with
late-onset schizophrenia had more severe positive symp-
toms and less severe general psychopathology in contrast
to patients who had nonschizophrenia psychoses. Cohen
et al. [39] stated that negative symptoms can be difficult
to distinguish from the confounding effects of depression,
medications, and institutionalization. In our study, using
the PANSS, it was evident that scores of negative
symptoms were similar in both groups studied and were
far lower than scores on positive symptom scales; these
results are in accordance with those of the San Diego
study, which proved that lower scores on negative
symptoms tended to be associated with the higher age
group having psychotic illness [40].
Assessment of daily functioning
Assessment of daily functioning revealed that patients
with late-onset schizophrenia had significantly better
ADL and IADL scores, whereas a significant number of
patients with late-onset nonschizophrenia psychoses
needed partial and complete support. This finding may
be attributed to the medical conditions of the latter
group, who had more frequent medical, neurological, and
cognitive impairment, which negatively impacted their
ability to perform daily activities compared with those
who suffered from late-onset schizophrenia. The deterio-
rated daily functioning reflects the devastating effects of
dementia on ADL and highlights the impact of this
disability on caregivers. These findings were in accor-
Table 5 Cognitive functions using the Wechsler Adult Intelligence Scale
Group AMean ± SD
Group BMean ± SD
Patients with late-onsetschizophrenia
n = 50
Patients with nonschizophrenialate-onset psychoses
n = 50 Test
Comprehension 7.52 ± 3.54 2.52 ± 1.74 t = 8.94P = 0.000
Digit span 4.12 ± 2.55 1.12 ± 0.47 t = 10.89P = 0.000
Arithmetic 2.48 ± 1.18 1.5 ± 1.58 t = 10.63P = 0.000
Similarities 6.74 ± 1.18 3.64 ± 1.05 t = 10.00P = 0.000
Vocabulary 5.57 ± 1.30 3.5 ± 0.55 t = 10.44P = 0.00
Picture completion 6.06 ± 1.40 2.22 ± 0.99 t = 15.76P = 0.00
Block design 4.54 ± 0.99 2.84 ± 0.88 t = 14.31P = 0.00
Digit symbols 5.4 ± 12.00 1.12 ± 0.59 t = 3.10P = 0.002
Verbal IQ 80.56 ± 14.2 61.96 ± 3.86 t = 8.92P = 0.000
Performance IQ 84 ± 7.1 76.8 ± 2.6 t = 16.15P = 0.000
Total IQ 82.16 ± 13.7 63.0 ± 2.95 t = 9.65P = 0.000
IQ, intelligence quotient.
Late-onset schizophrenia and nonschizophrenia psychosis Hussein et al. 19
Copyright © Institute of Psychiatry, Ain Shams University. Unauthorized reproduction of this article is prohibited.

dance with those of previous studies, which found that
higher levels of daily functioning among elderly people
with schizophrenia were associated with better cognitive
functioning, fewer negative symptoms, better physical
health, and independent living in the community [47–49].
Cognitive assessment
Patients with a primary diagnosis of dementia suffer from a
number of psychotic symptoms, and patients with primary
functional disorders become cognitively impaired. Barclay
and Almeida [36] stated that schizophrenia does not
increase the risk of dementia. In contrast, individuals with
cognitive impairment in later life are at increased risk for
psychosis. Dementia is characterized by a progressive
decline in cognitive abilities. This was true in our research,
which illustrated that group B patients, in which 70% of
patients had a diagnosis of dementia, scored significantly
worse in all subitems of cognitive assessment according to
CAMCOG compared with group A patients. It is interest-
ing to note that several groups of investigators have
reported potentially relevant clinical, neuropsychological,
and neurobiological differences between dementia patients
with and without psychosis. Stern et al. [50] observed that,
among dementia patients, psychosis was associated with a
greater prevalence of rapid cognitive decline. Moreover, in a
study by Jeste and Finkels [37], it was noted that those
with psychosis had greater impairment on putative
neuropsychological tests of frontal lobe function compared
with dementia patients without psychosis.
The association between cognitive functions in dementia
cases with or without psychosis should be clarified in
future studies. There was much debate on this topic;
Linda et al. [51] reported that behavioral symptoms and
cognitive functions are independent dimensions, whereas
Hopkins and Libon [52] suggested a strong relationship
between severity of psychosis and poor performance on
some cognitive functions.
From the current research, the obtained results are
important in demonstrating that the cognitive deficits
associated with late-onset schizophrenia are different
from the cognitive declines associated with dementia.
The rate of decline observed among the dementia groups
in the present sample appears to be consistent with that
reported in the literature [53,54]. Thus, the onset of
schizophrenia late in life does not appear to be a mere by-
product of a dementia disorder. The same conclusion is
consistent with the findings from studies by the Mount
Sinai research group, which examined chronically insti-
tutionalized elderly schizophrenia patients. These in-
vestigators found that the pattern of cognitive deficits of
such patients was distinct from that associated with
dementia; moreover, their postmortem neuropathological
studies indicated that the prevalence of amyloid plaques
and neurofibrillary tangles was not different from that of
age-matched healthy control individuals [55]. Unfortu-
nately, in this study, we did not compare group A patients
with healthy controls; thus, we could not comment on
cognitive decline in the late-onset schizophrenia group in
comparison with the healthy elderly population.
ConclusionPatients with late-onset schizophrenia compared with
patients with other late-onset psychoses differ in a
number of psychosocial and clinical variables, daily
functioning, and cognitive abilities. The results of this
study contribute to the development of a better under-
standing of the elderly patient population with different
types of late-onset psychoses, which have been largely
ignored in research. These findings draw the attention of
policymakers and psychiatrists to the burden of psychotic
disorders in the elderly and the need for specialized
psychiatric care units providing intensified help and
rehabilitation.
Recommendations
In Egypt, research in the area of old-age psychosis is still
scarce and has been neglected. Thus, studies on this
topic on a large representative sample from different
geographical areas are highly recommended. In addition,
prospective cohort studies of elders with psychotic
disorders to determine the outcome of psychotic disorders
are mandatory. Studies addressing clarification of risk
factors to develop psychosis at later age, the impact of
psychotic symptoms on caregivers, and treatment outcome
of old-age psychosis are recommended. Future studies
should involve different disciplines. These disciplines
should cooperate together to provide evidence-based data
that can inform the public, help policymakers to make
informed decisions and plans, and stimulate further
research.
Strength and limitations of the study
One of the strengths of this study is that (according to
best of our knowledge) it is among the first studies to
compare late-onset schizophrenia with nonschizophrenia
late-onset psychoses. Although our findings shed light on
this poorly understood and investigated area of research,
the results should be considered preliminary data because
of the limitations of small size and type of sample, which
was a selective rather than a stratified random sample
representing different geographical areas in Egypt. Our
findings must be reviewed as provisional and will be
subjected to revision, as more studies are needed in the
field of elderly patients with psychotic disorders.
AcknowledgementsThe authors express their gratitude to Professor M. El Banouby, formerchair of the department of Geriatric Medicine, Ain Shams University, forhis support and guidance. The authors are grateful to Dr Hisham Sadek,Dr Ahmed El Missiry, Dr Abeer Mahmoud, Dr Hanan Hussein, Dr AhmedEl Shafie, and the other research participants from the department ofNeuropsychiatry, Ain Shams University, for their time, training on tools,guidance, advice, and efforts in completing the study assessment. Theauthors would also like to thank Dr Olfat Kahla, senior psychologist inGeriatric Hospital, Ain Shams University, for her help, and Dr MohamedHassan Taha from ‘TIT Solution’ for the statistical analysis.
Conflicts of interestsThere are no conflicts of interest.
20 Middle East Current Psychiatry
Copyright © Institute of Psychiatry, Ain Shams University. Unauthorized reproduction of this article is prohibited.

References1 Olshansky SJ, Carnes BA, Cassel CK. The aging of the human species. Sci
Am 1993; 268:46–52.
2 Spar JE, La Rue A. Anxiety disorders and late onset schizophrenia. In: SparJE, La Rue A, editors. Clinical manual of geriatric psychiatry. 1st ed.American Psychiatric Publishing; 2006. p. 302–306.
3 Central Agency for Public Mobilization and Statistics. Egypt in figures. 2009;Available at: http://www.capmas.gov.eg/pdf/indicators/pages/preface.htm.
4 El Banouby MHHealth and aging in the Eastern Mediterranean region.. In:Robinson M, Novelli W, Pearson C, Norris L, editors. Global health andglobal aging. USA: The AARP Foundation; 2007. pp. 215–226.
5 Morris SK, Jeste DVSchizophrenia and other psychotic disorders.. In: Haz-zard WR, Blass JP, Ettinger WH, Halter JB, Ouslader JG, Ouslander JG,editors. Principles of geriatric medicine and gerontology. 4th ed. New York:Mcgraw-Hill; 1998. pp. 1341–1349.
6 Khouzam HR, Battista MA, Emes R, Ahles S. Psychoses in late life: eva-luation and management of disorders seen in primary care. Geriatrics2005; 60:26–33.
7 Harris MJ, Jeste DV. Late-onset schizophrenia: an overview. Schizophr Bull1988; 14:39–55.
8 Howard R, Rabins PV, Seeman MV, Jeste DV. Late-onset schizophrenia andvery-late-onset schizophrenia-like psychosis: an international consensus. TheInternational Late-Onset Schizophrenia Group. Am J Psychiatry2000; 157:172–178.
9 McClure FS, Gladsjo JA, Jeste DV. Late-onset psychosis: clinical, researchand ethical considerations. Am J Psychiatry 1999; 156:935–940.
10 Jeste DV, Dolder CR, Nayak GV, Salzman C. Atypical antipsychotics in el-derly patients with dementia or schizophrenia: review of recent literature.Harv Rev Psychiatry 2005; 13:340–351.
11 Fuchs T. Life events in late paraphrenia and depression. Psychopathology1999; 32:60–69.
12 Rabins PV, Lavrisha M. Long-term follow-up and phenomenologic differ-ences distinguish among late-onset schizophrenia, late-life depression andprogressive dementia. Am J Geriatr Psychiatry 2003; 11:589–594.
13 Woolley JD, Khan BK, Murthy NK, Miller BL, Rankin KP. The diagnosticchallenge of psychiatric symptoms in neurodegenerative disease: rates ofand risk factors for prior psychiatric diagnosis in patients with early neuro-degenerative disease. J Clin Psychiatry 2011; 72:126–133.
14 Omar AN, Haroun A, Nagy NE. Prevalence of depressive symptoms inphysically-ill elderly inpatients. Curr Psychiatry 1998; 5:145–155.
15 First MB, Gibbon M, Spitzer RL, Williams JBW, Benjamin LS. Structuredclinical interview for DSM-IV axis II personality disorders, (SCID-II).Washington, DC: American Psychiatric Press, Inc; 1997.
16 Kay SR. Positive-negative symptom assessment in schizophrenia: psycho-metric issues and scale comparison. Psychiatr Q 1990; 61:163–178.
17 Lawton MP, Brody EM. Assessment of older people: self-maintaining andinstrumental activities of daily living. Gerontologist 1969; 9:179–186.
18 El Okl MA. Prevalence of alzheimer’s disease and other types of dementia inthe Egyptian Elderly. Faculty of Medicine, Ain Shams University; 2002.
19 Kojo K. Late-onset schizophrenic syndromes in socially isolated situations: acomparison of Janzarik’s ‘Kontaktmangelparanoid’ and late paraphrenia.Psychogeriatrics 2010; 10:83–89.
20 Mahmoud A. Clinical profile of patients attending memory clinic in Ain ShamsUniversity, Institute of Psychiatry. Ain Shams University; 2002.
21 Wechsler D. Wechsler adult intelligence scale-revised. San Antonio, TX: ThePsychological Corporation; 1981.
22 Melika LK. The Wechsler Adult Intelligence scale.Dar El Nahda El Arabia,Egypt; 1996.
23 El Sherbini FM. The Egyptian classification of social class. Egypt: Faculty ofMedicine, Tanta University; 1986.
24 Girard C, Simard M. Clinical characterization of late- and very late-onset firstpsychotic episode in psychiatric inpatients. Am J Geriatr Psychiatry2008; 16:478–487.
25 Yasuda M, Kato S. Clinical psychopathological research on late-onsetschizophrenia – mainly patients with schizophrenia from a hospitalpsychiatric ward. Seishin Shinkeigaku Zasshi 2009; 111:250–271.
26 Ashour A, Okasha A, Sadek A, Hambali M, Lotaief F, Bishry Z. Portrait of oldpeople in Cairo hostels. Egypt J Psychiatry 1982; 5:75–94.
27 Haiba AAM. A community study of paranoid symptoms in the elderly popu-lation. Faculty of Medicine, Tanta University; 2002.
28 Lehmann SW. Psychiatric disorders in older women. Int Rev Psychiatry2003; 15:269–279.
29 Riecher Rossler A, Rossler W, Forstl H, Meise U. Late-onset schizophreniaand late paraphrenia. Schizophr Bull 1995; 21:345–354, discussion355–356.
30 Cohen CI, Vahia I, Reyes P, Diwan S, Bankole AO, Palekar N, et al. Schi-zophrenia in later life: clinical symptoms and social well-being. Psychiatr Serv2008; 59:232–234.
31 El Said SMS. Study of the effect of renal impairment on cognitive function inelderly patients. Faculty of Medicine, Tanta University; 2004.
32 Mostafa MM, Akram A. Clinical deterioration in vascular dementia: role ofnew ischemic lesions, hypoalbuminemia and hyponatremia. Egypt J NeurolPsychiat Neurosurg 2004; 41:401–412.
33 Prager S, Jeste DV. Sensory impairment in late-life schizophrenia. SchizophrBull 1993; 19:755–772.
34 Howard R, Cox T, Almeida O, Mullen R, Graves P, Reveley A, et al. Whitematter signal hyperintensities in the brains of patients with late paraphreniaand the normal, community-living elderly. Biol Psychiatry 1995; 38:86–91.
35 Almeida OP, Howard RJ, Levy R, David AS. Psychotic states arising in latelife (late paraphrenia) psychopathology and nosology. Br J Psychiatry1995; 166:205–214.
36 Barclay L, Almeida O. Schizophrenia in later life. Curr Opin Psychiatry2000; 13:423–427.
37 Jeste DV, Finkel SI. Psychosis of Alzheimer’s disease and related dementias.Diagnostic criteria for a distinct syndrome. Am J Geriatr Psychiatry2000; 8:29–34.
38 Paulsen JS, Salmon DP, Thal LJ, Romero R, Weisstein Jenkins C, Galasko D,et al. Incidence of and risk factors for hallucinations and delusions in patientswith probable AD. Neurology 2000; 54:1965–1971.
39 Cohen CI. Schizophrenia into later life: Treatment, research and policy.Library of Congress: American Psychiatric Publishing Inc.; 2003.
40 Jeste DV, Twamley EW, Eyler Zorrilla LT, Golshan S, Patterson TL, PalmerBW. Aging and outcome in schizophrenia. Acta PsychiatrScand2003; 107:336–343.
41 Quin RC, Clare L, Ryan P, Jackson M. ‘Not of this world’: the subjectiveexperience of late-onset psychosis. Aging Ment Health 2009; 13:779–787.
42 Metwally AS. Prevalence of depression among Egyptian geriatric community.Faculty of Medicine, Ain Shams University; 1998.
43 El Banoty M, Ghanem M, Mortagy A, Metwally A, El Nahas A, Sayed M.Prevalence of depression among the aged Egyptian community. Curr Psy-chiatry 1999; 6:3.
44 Asaad T. Recognizing depression in patients with dementia (a comparativestudy between Alzheimer’s disease and vascular dementia in a sample ofEgyptian patients). CurrPsychiatry 2002; 9:72–73.
45 Alexopoulos GS, Meyers BS, Young RC, Kalayam B, Kakuma T, Gabrielle M,et al. Executive dysfunction and long-term outcomes of geriatric depression.Arch Gen Psychiatry 2000; 57:285–290.
46 Vahia I, Bankole AO, Reyes P, Diwan S, Palekar N, Sapra M, et al. Schizo-phrenia in later life. Aging Health 2007; 3:383–396.
47 Gupta S, Steinmeyer C, Frank B, Lockwood K, Lentz B, Schultz K. Olderpatients with schizophrenia: nature of dwelling status and symptom severity.Am J Psychiatry 2003; 160:383–384.
48 Evans JD, Heaton RK, Paulsen JS, Palmer BW, Patterson T, Jeste DV. Therelationship of neuropsychological abilities to specific domains of functionalcapacity in older schizophrenia patients. Biol Psychiatry 2003; 53:422–430.
49 Viertio S, Tuulio Henriksson A, Perala J, Saarni SI, Koskinen S, Sihvonen M,et al. Activities of daily living, social functioning and their determinants inpersons with psychotic disorder. Eur Psychiatry 2011[In Press].
50 Stern Y, Albert M, Brandt J, Jacobs DM, Tang MX, Marder K, et al. Utility ofextrapyramidal signs and psychosis as predictors of cognitive and functionaldecline, nursing home admission and death in Alzheimer’s disease: pro-spective analyses from the Predictors Study. Neurology 1994; 44:2300–2307.
51 Linda CW, Nelson LS, Sl M, Victor WC, Agnes SY, Leung PY, et al. Apo-lipoprotein epsilon-4 allele and the two-year progression of cognitive func-tion in Chinese subjects with late-onset Alzheimer’s disease. Am J AlzheimerDis Other Demen 2006; 21:92–9.
52 Hopkins MW, Libon DJ. Neuropsychological functioning of dementia patientswith psychosis. Arch Clin Neuropsychol 2005; 20:771–783.
53 Clarke R, Smith AD, Jobst KA, Refsum H, Sutton L, Ueland PM. Folate,vitamin B12 and serum total homocysteine levels in confirmed Alzheimerdisease. Arch Neurol 1998; 55:1449–1455.
54 Galasko DR, Gould RL, Abramson IS, Salmon DP. Measuring cognitivechange in a cohort of patients with Alzheimer’s disease. Stat Med2000; 19:1421–1432.
55 Palmer BW, Heaton RK, Gladsjo JA, Evans JD, Patterson TL, Golshan S,et al. Heterogeneity in functional status among older outpatients with schi-zophrenia: employment history, living situation and driving. SchizophrRes2002; 55:205–215.
Late-onset schizophrenia and nonschizophrenia psychosis Hussein et al. 21
Copyright © Institute of Psychiatry, Ain Shams University. Unauthorized reproduction of this article is prohibited.

22 Middle East Current Psychiatry
Copyright © Institute of Psychiatry, Ain Shams University. Unauthorized reproduction of this article is prohibited.