Embed Size (px)
Citation preview

J. Neurol. Neurosurg. Psychiat., 1967, 30, 166
Pubertas praecox due to hypothalamic hamartoma:report of two cases surviving surgical removal
of the tumourD. W. C. NORTHFIELD AND D. S. RUSSELL
From The London Hospital
The association of pubertas praecox with tumoursof the third ventricle has long been recognized. Thetumour is sometimes a congenital malformation, orhamartoma, composed of redundant brain tissue.This comprises a haphazard assembly of neurones,bundles of nerve fibres, and neuroglial cells in moreor less appropriate proportions and distribution.These 'tumours' are usually about 1 to 2 cm. indiameter, but may be smaller or larger; they con-sistently lie at the base of the brain in the region ofthe tuber cinereum and mammillary bodies, to somepart of which they are usually attached by a pedicleso short that they can be described as sessile.Occasionally the mass lies free in the leptomeningeswhich provide a capsule.
Previously recorded cases will not be reviewedhere: readers are referred to the excellent survey bySchmidt, Hallervorden, and Spatz (1958), who alsoreported four new cases. Several more recentpublications are discussed by Wolman and Balm-forth (1963).The present paper is concerned with two cases in
which prolonged survival followed operative removalof the hamartoma. In particular, the modifyingeffects of operation upon the pre-existing pubertaspraecox will be noted.We are not, at the time of writing, acquainted with
any similar records. In case 2 of the communicationbyList, Dorman, Bagchi, and Bebin (1958) the patienthad lived for nine months after a limited biopsy of thetumour but, as the authors recognize, this periodwas too short for a full assessment of the effects ofoperation. But since, as we shall argue later, themechanism whereby pubertas praecox is promotedby the tumour in question is debatable, the con-sequences of complete operative removal are ofconsiderable theoretical and clinical importance.
CASE REPORTS
CASE 1 M.T., a male, was born on 18 June 1955, byforceps delivery, weight 4j lb. His mother had toxaemia
of pregnancy. At the age of 8-9 months he developedpubic hair, at first downy and later more profuse. Hisdevelopment was otherwise not remarkable, but hismother had noticed that he was always physicallystrong and she thought that he was not quite normal.At the age of 11 months he was admitted to the Hospital
for Sick Children, Great Ormond Street, where nophysical abnormalities were noted beyond precociousgenital development, facial acne, and greasiness of theskin. The extremities, on x-ray examination, showed thatbone development was only a few months in advance ofthe standard. Testicular biopsy showed considerablecellular proliferation in the tubules, simulating an adultpattern. Ventriculography revealed deformation of thethird ventricle, indicative of a hypothalamic tumour.However, in the absence of signs of raised intracranialpressure, or of cerebral impairment, the child wasdischarged with the prescription of phenobarbitone andpotassium bromide to diminish his excitability.When readmitted, at the age of 2 years, his condition
was unchanged, except that mental retardation wassuspected. This was confirmed on further admission ayear later.At the age of 31 years the boy was admitted to the
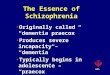
London Hospital. On examination he was abnormallytall (3 ft. 10 in. (1-168 m.)) and powerfully built (wt. 4 st.5 lb. (27-67 kg.)). His limbs and torso were disproportion-ate and the external genitalia fully developed (Fig. 1).Secondary sexual characters were obvious, his voicebeing deep and husky whilst his facial features wereheavy, with a growth of downy hair on the sides of hischeeks, and heavy eyebrows. Hair grew thickly over thescalp. Mental retardation was obvious; he talked little,but frequently laughed and giggled. He was never seen tomake sexual advances towards females. The skull circum-ference (515 cm.) was proportionate to his stature andneurological examination disclosed no abnormality.
Investigations Chemistry of blood and of urine wasnormal. The cerebrospinal fluid contained less than 20 mg.of protein per 100 ml., and less than 1 cell per c.mm.Urine contained 1-3 mg. of 17-ketosteroids in 24 hours.Skeletal radiographs for bone age corresponded to theappearances normal at 13 years; skull radiographs werenormal.
Air encephalogram The lateral and third ventricleswere dilated; air in the interpeduncular and chiasmal
166
Protected by copyright.
on 9 March 2019 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.30.2.166 on 1 April 1967. D
ownloaded from

Pubertas praecox due to hypothalamic hamartoma
FIG. 1.
FIG. 1. M. T. (case 1) aged 3 years 6 months.
FIG. 2a and b. A.E.G. in case I (see text).
cisterns outlined a rounded slightly lobulated shadowbelow the floor of the third ventricle, straddling thedorsum sellae (Figs. 2a and b).
Operation (11 November 1958) A right frontalcraniotomy disclosed a smooth greyish-white mass,
viewed between the right optic nerve, which was displacedupwards and medially, and the internal carotid artery,which was displaced ventro-laterally. On blunt dissectionthe tumour, which seemed to be about 3 cm. in diameter,appeared to be encapsulated and without any point ofattachment to the brain. At first it was removed piece-meal, but later a larger mass was recovered. Bleedingfrom the direction of the pontine cistern was easilycontrolled, and the wound was closed.The post-operative course was uneventful, apart from
some bronchitis, and the child was discharged to hishome three weeks later (12 December 1958). (Fig 3).
Macroscopic pathology (S.D. 6032-58) One large,approximately oval piece (2-2 x 1-4 x 1-0 cm., weight
FIG. 2b.
1-3 g.) of firm pink tissue with coarsely lobulated smoothglistening outer surface and a more haemorrhagic andragged opposite surface (Fig. 4) was received. Cut surfaceswere homogeneous, pale, and grey. Accompanying thiswere numerous smaller pieces (together 2 cm. diam.and up to 0-8 cm. high; weight 1-2 g.) of similar tissue.
Microscopic pathology The tissue contains maturenerve cells, varying considerably in size and shape, anddispersed fairly evenly throughout all areas (Fig. 5a).Loyez and Bielschowsky preparations demonstratenumerous myelinated nerve fibres, often in conspicuousleashes. The latter often lie beneath, and parallel with,the surface of the hamartoma. Glial cells are scatteredhaphazard throughout the tissues; numerically theycorrespond to the quota usually seen in normal cerebralgrey matter. The only cytological peculiarity is theoccurrence of occasional discrete nests of small un-differentiated cells with spherical, deeply haematoxyphilnuclei containing a central nucleolus. Their appearance
167
Protected by copyright.
on 9 March 2019 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.30.2.166 on 1 April 1967. D
ownloaded from

D. W. C. Northfield and D. S. Russell
FIG. 3. M. T. 24 days after operation; note marked loss ofmuscle substance compared with Fig. 1 (smaller child is controlofsame age).
suggests that they are primitive neuroblasts, but Biels-chowsky preparations failed to substantiate this. Nopituitary stalk tissue was found amongst the fragments.
Subsequent course This boy has been under regularobservation since the time of operation up to his presentage of 10 years and 10 months. The following table giveshis successive records of weight and height.
Age (yr.) Weight (st. lb.) Height (ft. in.)
3k 4 54 4241 4 45 4851 5 16i8910.10/12
3 1044 24 3i4 4
5 6 4 65 10 4 86 2 4 9k6 4k 4 10I
FIG. 4. Tumour from case 1.
The most obvious physical change lay in a rapid loss ofexcessive muscularity, even apparent three weeks afteroperation (Fig. 3), so that the 'infant Hercules' appearancegave place to a more normal slimness of body contours.His present appearance is shown in Figure 6. But therewas no retrogression in genital development: this hasremained static. He continued to speak with a deep,husky voice but, as time went on, this became lessnoticeable. He remained mentally backward and wasrestless, excitable, and difficult to examine. Later therewas a gradual improvement also at this level. From theage of 8 he has attended a boarding school for backwardchildren, and has made good progress. At the age of 10he was able to converse much more freely and sensibly,and his movements were more composed. Physically,
168
Protected by copyright.
on 9 March 2019 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.30.2.166 on 1 April 1967. D
ownloaded from

Pubertas praecox due to hypothalamichamartoma16
IAll k..:
.4,
1% Nl:.,,.Alb 'A'"W-m "ML--.
I
:Ikn"". .1
.04
A
Ilk,4*. qm4. 0
k.
FIG. 5a.Tumourfrom case 1.Haema-toxylin andeosin x 500.FIG. 5b.Tumourfrom case 2.Haema-toxylin andeo.sin x 175.Neurones andscatteredglial cells.
0FIG. 5a.
apart from the genitalia, his outward appearance wouldpass as normal for a boy of his age.
'Al.
Aw,
9o 44
I% $o
El
9
ElEl
414-El
41
46
44 *0.4 t.
ElP,
m9. 4
U:
V CASE 2 S.D., a male, was born on 22 November 1958and was the first child of Malay parents. Pregnancy andlabour had been normal. When 19 months old, hisparents noticed the growth of pubic hair, enlargement ofthe genitalia, and frequent erections. His Malay doctor
r prescribed prednisone which seemed to have a slightmoderating effect on these features. In this country hewas admitted, at the age of 3 years 8 months, to theQueen Elizabeth Hospital for Children, Hackney Road,London, where he was recorded as a large sturdy childwith excessive hirsuties, muscularity, and genital develop-ment. Physical features were otherwise normal. Specialinvestigations of the blood picture and chemistry ofblood and urine revealed no significant aberration;1 7-ketosteroid excretion in urine was Il-O mg. in 24 hours.9, His bone age was assessed radiographically to be that ofa 6-year-old child. Height was 31 ft. (Il-066 in.); weight3 st. 12 oz. (19.39 kg.). On 1 August 1962 he was trans-ferred to the London Hospital. On examination he wasnervous and apprehensive but appeared of normalmentality, and his voice was normal for a child. Hirsutieswas generalized but especially marked on the upper lipand pubis (Fig. 7). The external genitalia were enlarged.Neurological examination elicited no abnormal features.A skull radiograph was normal.
Air encephalography There was slight enlargement ofthe ventricles and of the aqueduct, and the fourth ventricle
* was slightly displaced posteriorly away from the clivus.4. Air in the interpeduncular cistern outlined a small roundmass situated above and behind the dorsum sellae (Fig. 8).
Operation The procedure (14 August 1962) adoptedwas the same as in case 1. But here the tumour displaced
00 4W.,
f..400,6 0
PI§f1lw
4, :k:. .Pi4
'o
4'
4,
v
169
14W
A
Protected by copyright.
on 9 March 2019 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.30.2.166 on 1 April 1967. D
ownloaded from

D. W. C. Northfield and D. S. Russell
FIG. 7. S.D. (case 2) aged 3 years 9 months.
FIG. 6. M.T., present appearance, aged 10 years 10months.
the pituitary stalk forwards to lie immediately behindthe optic chiasma. Rostrally the tumour had a fairlyfirm attachment to the tuber cinereum, a feature in whichit differed from that in case 1. It was estimated to beabout 2 cm. in diameter. Removal was piecemeal andcomplete, except perhaps for a few tags at its point ofattachment to the brain. Eventually the rostral end of thebasilar artery was seen across the resulting cavity. Inappearance and texture the tumour was similar to thatencountered in case 1.
Closure of the wound and the post-operative coursewere uneventful. The child made an excellent recoveryand was returned to his home on 27 August 1962.
Macroscopic pathology (S.D. 4833/62) About 12fragments of white tissue, each measuring up to 0 4 by0-2 cm., mixed with some blood clot were received.
Microscopic pathology The appearances so closelyresemble those described in case 1 that they need norepetition except for three points. First, the fragmentarynature of the tissue precludes the tracing of any relation-ship of the bundles of myelinated nerve fibres to thesurface of the hamartoma. Secondly, there are no fociof small, undifferentiated cells such as were noted incase 1. Thirdly, no neurosecretory substance was detected,by special staining, in any part of the tissue examined.
Subsequent course The patient returned to Malayawith his parents in October 1962. His doctor there wrote
FIG. 8. A.E.G. in case 2 (see text).
on 24 March 1966, that, in 1963, the child had someheadaches which passed off. In January 1966, he had someattacks of what appeared to be paroxysmal tachycardia.Otherwise his health has been good. He is reported asemotionally normal for his age, is intelligent and attend-ing school. The genitalia are still of adult type but,
170
;-- Y.:.:...
Protected by copyright.
on 9 March 2019 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.30.2.166 on 1 April 1967. D
ownloaded from

Pubertas praecox due to hypothalamic hamartoma
according to the mother, he has no abnormal sexualinterests. The head is 54 cm. in circumference, and height4 ft. 31 in. (1-3 cm.).
NOTE ON RADIOLOGICAL APPEARANCES XAND OPERATIVE PROCEDURE
Air encephalography is essential to the diagnosis ofthese lesions. The tumour lies below the floor of thethird ventricle in the basal cisterns, which must befilled with air in order to outline the mass. Ventriculo-graphy rarely fills the cisterns, and without theirdemonstration a filling defect in the floor of the thirdventricle (due to its indentation by the tumour) maybe erroneously ascribed to an intrinsic tumour ofthe floor. The radiological appearances of boththese cases are remarkably similar, and quite unlikethose of other tumours in this region, such ascraniopharyngioma, pituitary adenoma, and gliomaof the optic chiasma and of the hypothalamus. Inthe first case, the appearance was quite unfamiliarto one of us (D.W.C.N.) but was immediatelyrecognized by the other (D.S.R.) by reason of herprevious experience of the morbid anatomy of theserare lesions (Le Marquand and Russell, 1934-35).The situation of the tumour appeared to be
surgically inaccessible, and in the first case themother gave her permission for the right optic nerveto be divided, if this proved necessary in order toremove the tumour. In the event this was notnecessary. After the right optic nerve had beencleared of arachnoid the tumour was immediatelyperceived, in the interval between the lateral borderof the nerve and the internal carotid artery (Fig. 9).*The tumour had displaced the nerve in a rostral andmedial direction, and the artery in a ventral andlateral direction, thereby enlarging the intervalbetween these structures. After removing a smallportion of the anterior frontal operculum, to gainroom for manoeuvre, it was possible to remove thetumour through the space between the optic nerveand the carotid artery.
In the second case, the tumour was not immediatelyvisible, and the only apparent abnormality was arather long right optic nerve, separated from theinternal carotid artery by a wide interval. Inspectionmedial to the optic nerve revealed the pituitary stalklying in a more anterior plane than is usual, as thoughit were pressed forwards against the chiasma; furtherdissection and more careful scrutiny between theoptic nerve and the carotid artery brought to lightthe mass, which was removed piecemeal through thisinterval. It was not necessary to remove any frontallobe in this case.
Details of the operative procedure have beendescribed because it is commonly held that retro-
FIG. 9. Operation sketch in case 1.
chiasmal tumours cannot be approached between
the optic nerve and carotid artery. This is not the
case. The interval is usually widened by the tumour,
and provided meticulous care is taken to avoid any
trauma to the optic nerve, this route provides a
further means of reaching other posteriorly placedtumours or their extensions, such as pituitaryadenoma and craniopharyngioma.
DISCUSSION
In pubertas praecox a well-defined group of cases
is of the kind described in this paper. Therapeuticallyit is of importance to assess the benefits that may
accrue from operative removal of the offendinghamartoma. In case the patient has survived
operation for eight years, in case 2 for nearly four
years.
In neither case has the excessive development of
the external genitalia undergone regression. Possiblyit would be over-optimistic to expect this, and
testicular biopsy would be necessary to determinewhether cellular activity in the seminiferous tubuleshad subsided. Neither patient displayed undue
interest in the opposite sex at any time, so this
criterion also is lacking.The repercussions of operation upon bodily
growth, however, have been more obvious. In both
171
Protected by copyright.
on 9 March 2019 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.30.2.166 on 1 April 1967. D
ownloaded from

D. W. C. Northfield and D. S. Russell
cases there has been a gradual increase in statureaccompanied, in case 1, by a loss of excessivemuscularity and the assumption of normal bodilycontours. Moreover, in the immediate post-operativeperiod there was an obvious retardation of growth instature. In case 2 there is, unfortunately, no mentionof this latter point by the patient's Malayan doctor.The continued skeletal growth, especially in case 1,
is manifestly important. Whilst continuity ofpituitary function is thereby demonstrated, it mustbe admitted that the progress to be anticipated incases of this kind is unpredictable since survivalbeyond puberty is exceptional. In this context thereport by Wolman and Balmforth (1963) of a womanaged 62 is pertinent. She evinced precocious pubertyat the age of 7. Growth ceased at the age of 9 years.Her height was then 4 ft. 61 in. and she weighed15 st. 6 lb. The menopause occurred in the earlythirties. She married but never became pregnant. Nomental abnormality was recorded. At necropsy ahypothalamic hamartoma, measuring 1-5 x 1 x 1cm., covered the mammillary bodies and wasattached by a broad base to the tuber cinereum.The adjacent brain showed no evidence of com-pression or distortion, and both pituitary and pinealglands appeared normal.The significance of mental retardation in case 1 is
difficult to assess. It is an inconstant feature in thesepatients and its pathological background has notbeen established. The boy in case 1 has improved inthis respect, but he is still subnormal for his age.
Finally attention is called to the difficult problemof the means whereby pubertas praecox is evoked bythis type of lesion. Mounting evidence of theimportance of hypothalamic mechanisms in thecontrol and regulation of the production of pituitaryhormones (see review by Reichlin, 1963) suggeststhat excitation of gonadotrophic secretion is causedby the presence of the hamartoma. Its anatomicalrelationship to the posterior part of the tubercinereum and manumillary bodies is sufficientlyconstant to suggest that this site is of crucial import-ance in provoking the syndrome of pubertas praecox.Wolman and Balmforth have studied the nature ofthe neural connexions bridging the hamartoma andhypothalamus and found, in their case, that bands ofnerve fibres blended with the capsule of the adjacentmammillary body. Furthermore, they demonstratedneurosecretory material in some of the nerve cellsin the hamartoma. From this they concluded 'thatthe hamartoma acts as an overdrive to the posteriorhypothalamic area, using a neurosecretory mechan-ism'.
This argument holds only if there is a union ofthis kind between the hamartoma and the hypo-thalamus. It is apparently supported by the case
described by Bedwell and Lindenberg (1961) in a19-year-old negro male, without any history ofpubertas praecox, who died as a result of a motoraccident. A spherical hamartoma, approximately1 cm. in diameter, was found adjacent to the tubercinereum. It was devoid of any neural connexions.and 'caused only a mild depression of the right halfof the tuber cinereum'. On the other hand, in ourcase 1 there was seemingly no attachment of thehamartoma to the brain. This was, at operation, in.sharp distinction to the findings in case 2 and itseems unlikely that any firm union could have beenoverlooked. If this is acceptable, then it must beconceded that a peduncular attachment to the brainis not essential for the development of pubertaspraecox.
Excitation of the hypothalamic centres by pressurealone might be more in accordance with the availabledata. Thus we have on record the case of a womanaged 34 (P.M. 277.1955) who had no history ofpubertas praecox. She died from cerebral sarcoidosis.A pale grey nodule, measuring 09 cm. from side toside by 085 cm. from above down by 0 5 cm. antero-posteriorly, was attached to the tuber cinereumjust in front of the right mammillary body. Micro-scopically the cellular features were more suggestiveof a ganglioneuroma than the classical type ofhamartoma. However, Horrax, and Bailey (1928,case 3) recorded pubertas praecox in association witha ganglioneuroma of the hypothalamus, and it mustbe insisted that the cytological character of thehypothalamic mass has apparently no bearing onthe clinical picture of pubertas praecox. Thus, inaddition to ganglioneuroma, there are records of asimilar disturbance in association with hypothalamicastrocytomas, ependymal glioma, craniopharyn-gioma and, notably, pineal tumours (see Russell andRubinstein, 1963), the majority of which areteratomas.Taking all these points into consideration, there
are formidable objections to the theory advanced byWolman and Balmforth. It would seem far morelikely that the excitatory factor is purely mechanicalin its action. If so, it would seem necessary that thehamartoma, or tumour, should attain a criticalvolume before its endocrine effects became manifest,and we would argue that this may explain theobservations (noted above) in which a hypothalamichamartoma is dissociated from the condition ofpubertas praecox.
SUMMARY
Two cases of pubertas praecox are described ineach of which a hypothalamic hamartoma wasremoved. Both patients are alive eight and four yearsrespectively after the operation.
172
Protected by copyright.
on 9 March 2019 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.30.2.166 on 1 April 1967. D
ownloaded from

Pubertas praecox due to hypothalamic hamartoma
The appearance at air encephalography and theoperative approach are described.The mechanisms which may excite pubertas
praecox in these and similar cases are discussed.
REFERENCES
Bedwell, S. F., and Lindenberg, R. (1961). Hypothalamic hamartomawith dendritic proliferation and other neuronal changesassociated with 'blastomatoid' reaction of astrocytes. J.Neuropath. exp. Neurol., 20, 219-236.
Horrax, G., and Bailey, P. (1928). Pineal pathology-further studies.Arch. Neurol. Psychiat. (Chic.), 19, 394-414.
Le Marquand, H. S., and Russell, D. S. (1934-35). A case of pubertaspraecox (macrogenitosomia praecox) in a boy associated witha tumour in the floor of the third ventricle. Roy. Berks. Hosp.Rep., 3, 31-61.
List, C. F., Dorman, C. E., Bagchi, B. K., and Bebin, J. (1958). Pos-terior hypothalamic hamartomas and gangliogliomas causingprecocious puberty. Neurology (Minneap.), 8, 164-175.
Reichlin, S. (1963). Neuroendocrinology. New Engl. J. Med., 269,1182-1189; 1246-1250; 1296-1303.
Russell, D. S., and Rubinstein, L. J. (1963). Pathology of Tumours ofthe NVervous System, 2nd ed. Arnold, London.
Schmidt, E., Hallervorden, J., and Spatz, H. (1958). Die Entstehungder Hamartome am Hypothalamus, mit und ohne PubertasPraecox. Dtsch. Z. Nervenheilk., 177, 235-262.
Wolman, L., and Balmforth, G. V. (1963). Precocious puberty due toa hypothalamic hamartoma in a patient surviving to late middleage. J. Neurol. Neurosurg. Psychiat., 26, 275-280.
173
Protected by copyright.
on 9 March 2019 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.30.2.166 on 1 April 1967. D
ownloaded from