Embed Size (px)
Citation preview
Schizophrenia & Schizophrenia & Other Psychotic DisordersOther Psychotic Disorders
Cornelia Pinnell, Ph.D.Cornelia Pinnell, Ph.D.Argosy University/PhoenixArgosy University/Phoenix
Lecture Outline
• Hx of the concept of schizophrenia• Important concepts – positive & negative sxs of schizophrenia, hallucination, sxs of schizophrenia, hallucination, delusion
• Epidemiology• Schizophrenia – subtypes; other psychotic disorders
Lecture Outline
• Etiological theories• Treatment
History of the History of the concept of schizophreniaconcept of schizophreniaContributorsContributors::•• Benedict Morel (1809Benedict Morel (1809--1873)1873)•• Emil Kraepelin (1856Emil Kraepelin (1856--1926)1926)•••• Eugen BleulerEugen Bleuler (1857(1857--1939)1939)•• Kurt Schneider (1887Kurt Schneider (1887--1967)1967)
History of the History of the concept of schizophreniaconcept of schizophrenia•• Benedict Morel (1809Benedict Morel (1809--1873) used the term 1873) used the term ‘‘démense précoce’démense précoce’ to describe to describe deteriorated patients whose illnesses had deteriorated patients whose illnesses had begun in adolescencebegun in adolescencebegun in adolescencebegun in adolescence
Emil Kraepelin (1856Emil Kraepelin (1856--1926)1926)
•• Emil Kraepelin latinized Emil Kraepelin latinized Morel’s term: Morel’s term: ‘dementia ‘dementia praecoxpraecox’’ denoted a denoted a severe chronic psychotic severe chronic psychotic illness with distinct illness with distinct illness with distinct illness with distinct cognitive processes and cognitive processes and early onset, leading to early onset, leading to deterioration deterioration -- different different from manicfrom manic--depressive depressive disorder & from paranoiadisorder & from paranoia
History of the History of the concept of schizophreniaconcept of schizophrenia•• Eugen BleulerEugen Bleuler (1857(1857--1939) coined the term 1939) coined the term ‘‘schizophreniaschizophrenia’ to denote the schism between ’ to denote the schism between thought, emotion and behaviors in affected thought, emotion and behaviors in affected patients patients –– a broader concept; he did not believe a broader concept; he did not believe patients patients –– a broader concept; he did not believe a broader concept; he did not believe that a deteriorating course was necessary.that a deteriorating course was necessary.–– ‘Schizophrenic disorders’ were considered a ‘Schizophrenic disorders’ were considered a ‘series of diseases’ due to their heterogeneity‘series of diseases’ due to their heterogeneity
Eugen BleulerEugen Bleuler (1857(1857--1939)1939)
Bleuler eliminated poor Bleuler eliminated poor prognosis as criterion for prognosis as criterion for schizophrenia & specified schizophrenia & specified
–– Primary symptoms Primary symptoms (‘core’/fundamental)(‘core’/fundamental)
–– Secondary symptoms Secondary symptoms (‘accessory’)(‘accessory’)
Bleuler’s primary Bleuler’s primary symptoms of schizophreniasymptoms of schizophreniaThe four ‘A’s of schizophrenia (deficits):The four ‘A’s of schizophrenia (deficits):
––AAssociative loosening/disturbancesssociative loosening/disturbances––AAffective bluntingffective blunting––AAffective bluntingffective blunting––AAmbivalencembivalence––AAutismutism
Bleuler’s secondary Bleuler’s secondary symptoms of schizophreniasymptoms of schizophrenia
––HallucinationsHallucinations
––DelusionsDelusions
––Negativism & StuporNegativism & Stupor
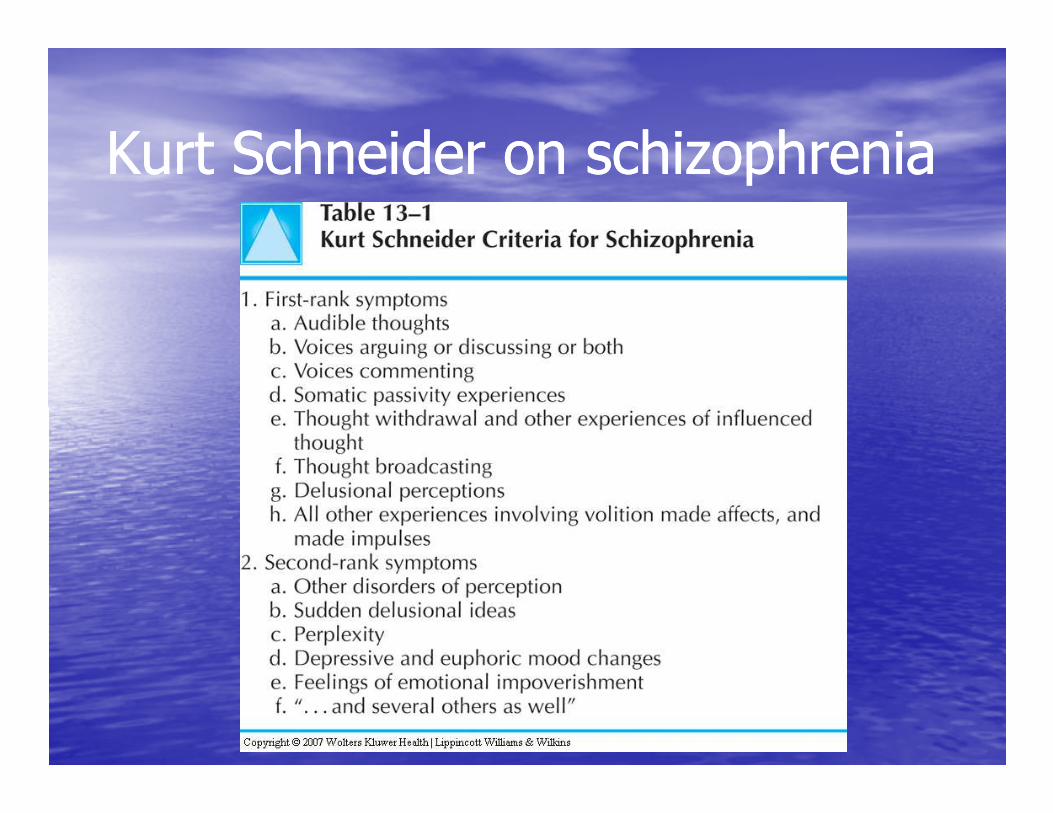
Kurt Schneider on schizophreniaKurt Schneider on schizophrenia
•• Distinguished between Distinguished between firstfirst--rankrank and and secondsecond--rank symptomsrank symptoms
Kurt Schneider on schizophreniaKurt Schneider on schizophrenia
Kurt Schneider on schizophreniaKurt Schneider on schizophrenia
•• Believed that schizophrenia could be Believed that schizophrenia could be diagnosed exclusively based on seconddiagnosed exclusively based on second--rank symptoms, in the absence of firstrank symptoms, in the absence of first--rank symptomsrank symptomsrank symptomsrank symptoms
Positive symptoms of schizophreniaPositive symptoms of schizophrenia
Florid psychosisFlorid psychosis––DelusionsDelusions––DelusionsDelusions––HallucinationsHallucinations––Positive formal thought disorderPositive formal thought disorder––Bizarre behaviorBizarre behavior
DelusionDelusion
•• A false belief based on incorrect inference about A false belief based on incorrect inference about external reality that is firmly sustained despite external reality that is firmly sustained despite what almost everyone else believes and despite what almost everyone else believes and despite what constitutes evidence to the contrary. what constitutes evidence to the contrary. what constitutes evidence to the contrary. what constitutes evidence to the contrary.
•• The belief is not accepted by other members of The belief is not accepted by other members of the person’s culture. the person’s culture.
ExamplesExamples: bizarre, d. of control, d. of : bizarre, d. of control, d. of reference, thought broadcasting, thought reference, thought broadcasting, thought insertion, etc. insertion, etc. –– organized themesorganized themes
HallucinationHallucination
•• A sensory perception that seems real but occurs A sensory perception that seems real but occurs in the absence of external stimulation of the in the absence of external stimulation of the relevant sensory organ. relevant sensory organ.
TypesTypes: Auditory (voices, sounds), gustatory : Auditory (voices, sounds), gustatory (usually unpleasant taste), olfactory, visual (usually unpleasant taste), olfactory, visual (flashes of light, images), somatic (e.g., feeling (flashes of light, images), somatic (e.g., feeling electricity), tactile (sensation of being touched electricity), tactile (sensation of being touched or something under the skin)or something under the skin)
Negative symptoms of schizophreniaNegative symptoms of schizophrenia
Deficits, diminution or loss of functioningDeficits, diminution or loss of functioning::–– Affective flatteningAffective flattening (unchanging facial (unchanging facial expression, decreased spontaneous expression, decreased spontaneous movement, poor eye contact, etc.)movement, poor eye contact, etc.)movement, poor eye contact, etc.)movement, poor eye contact, etc.)
–– AlogiaAlogia (poverty of speech content, etc.)(poverty of speech content, etc.)–– Avolition/apathyAvolition/apathy (anergia, lack of interest)(anergia, lack of interest)–– AnhedoniaAnhedonia--asociality (social withdrawal, lack asociality (social withdrawal, lack of intimacy/closeness, poor social skill)of intimacy/closeness, poor social skill)
–– AttentionAttention –– poor concentration, inattentivepoor concentration, inattentive
American bias American bias in diagnosing schizophreniain diagnosing schizophrenia•• In the 1970s studies were initiated to determine In the 1970s studies were initiated to determine why national statistics showed disproportionate why national statistics showed disproportionate frequency of affective disorders in UK and of frequency of affective disorders in UK and of schizophrenia in the USA schizophrenia in the USA schizophrenia in the USA schizophrenia in the USA
(World Health Organization)(World Health Organization)
•• FindingsFindings: the American concept of schizophrenia : the American concept of schizophrenia was broader than the UK/ European concept was broader than the UK/ European concept ––thus schizophrenia was overdiagnosed and thus schizophrenia was overdiagnosed and overtreated in the USAovertreated in the USA
Definitional changes of Definitional changes of schizophrenia in the DSMschizophrenia in the DSM
In the DSMIn the DSM--IIIIII--R, the definition of schizophrenia R, the definition of schizophrenia limits the diagnosis to limits the diagnosis to severe formssevere forms, with an , with an emphasis on Kraepelin’s notion of deterioration emphasis on Kraepelin’s notion of deterioration emphasis on Kraepelin’s notion of deterioration emphasis on Kraepelin’s notion of deterioration and on ‘positive’ symptoms (‘negative’ symptoms and on ‘positive’ symptoms (‘negative’ symptoms were ignored)were ignored)
Clinical features of schizophreniaClinical features of schizophrenia
•• No clinical sign or symptom is pathognomonic No clinical sign or symptom is pathognomonic (i.e., unique) for schizophrenia (i.e., unique) for schizophrenia -- can be found can be found in other disordersin other disorders
•• A patient’s symptoms change over timeA patient’s symptoms change over time
•• We need to take into account the patient’s level We need to take into account the patient’s level of education, intellectual ability, cultural of education, intellectual ability, cultural backgroundbackground
Diagnostic criteria for SchizophreniaDiagnostic criteria for Schizophrenia
A.A. Characteristic sxs Characteristic sxs –– positive & negative sxs positive & negative sxs (2+); only 1 if a voice keeping running (2+); only 1 if a voice keeping running commentary or 2 voices conversing commentary or 2 voices conversing ––sxs duration of at least 1 monthsxs duration of at least 1 monthsxs duration of at least 1 monthsxs duration of at least 1 month
B.B. Social/occupational dysfunctionSocial/occupational dysfunctionC.C. Continuous signs of disturbance for 6mContinuous signs of disturbance for 6mD.D. Not due to other mental disorder, substance, Not due to other mental disorder, substance,
medical condition, or pervasive developmental medical condition, or pervasive developmental disorderdisorder
Schizophrenia subtypesSchizophrenia subtypes
•• 295.30 Paranoid Type295.30 Paranoid Type•• 295.10 Disorganized Type295.10 Disorganized Type•• 295.10 Disorganized Type295.10 Disorganized Type•• 295.20 Catatonic Type295.20 Catatonic Type•• 295.90 Undifferentiated Type295.90 Undifferentiated Type•• 295.60 Residual Type295.60 Residual Type
Schizophrenia Schizophrenia 295.30 Paranoid Type295.30 Paranoid Type•• Essential feature: presence of prominent Essential feature: presence of prominent delusions or auditory hallucinations with relative delusions or auditory hallucinations with relative preservation of cognitivepreservation of cognitive functioning and functioning and affectaffectaffectaffect
•• Delusions are typically Delusions are typically persecutorypersecutory or or grandiosegrandiose, , or both; other themes may occur: jealousy, or both; other themes may occur: jealousy, religiosity, somatizationreligiosity, somatization
•• Individual may be predisposed to suicide or Individual may be predisposed to suicide or violenceviolence
SchizophreniaSchizophrenia295.10 Disorganized Type295.10 Disorganized Type•• Essential feature: disorganized speech and flat Essential feature: disorganized speech and flat or inappropriate affect (e.g., laughter not related or inappropriate affect (e.g., laughter not related to the content of speech); disorganized behavior to the content of speech); disorganized behavior (often inability to care for self)(often inability to care for self)(often inability to care for self)(often inability to care for self)
•• Associated features: grimacing, mannerism, odd Associated features: grimacing, mannerism, odd behaviorsbehaviors
SchizophreniaSchizophrenia295.20 Catatonic Type295.20 Catatonic Type•• Essential feature: marked psychomotor Essential feature: marked psychomotor disturbance that may involve motoric disturbance that may involve motoric immobility (e.g., catalepsy immobility (e.g., catalepsy –– waxy waxy flexibility, bizarre postures) or excessive flexibility, bizarre postures) or excessive flexibility, bizarre postures) or excessive flexibility, bizarre postures) or excessive motor activity motor activity –– catatonic stupor or catatonic stupor or excitement, extreme negativism, mutism, excitement, extreme negativism, mutism, peculiarities of voluntary movementpeculiarities of voluntary movement
•• Echolalia, echopraxiaEcholalia, echopraxia

SchizophreniaSchizophrenia295.90 Undifferentiated Type295.90 Undifferentiated Type
•• Essential feature:Criterion A of schizophrenia is Essential feature:Criterion A of schizophrenia is met, without meeting other criteria for other met, without meeting other criteria for other typestypestypestypes
SchizophreniaSchizophrenia295.60 Residual Type295.60 Residual Type
•• There has been at least one episode of There has been at least one episode of Schizophrenia, but current clinical picture is Schizophrenia, but current clinical picture is without prominent positive psychotic symptoms, without prominent positive psychotic symptoms, without prominent positive psychotic symptoms, without prominent positive psychotic symptoms, or with attenuated sxs or with attenuated sxs –– yet there are negative yet there are negative symptomssymptoms

Course specifiers Course specifiers (only after 1 year has lapsed)(only after 1 year has lapsed)•• Episodic With Interepisodic Residual SxsEpisodic With Interepisodic Residual Sxs•• With Prominent Negative SxsWith Prominent Negative Sxs•• Episodic With No Interepisodic Residual SxsEpisodic With No Interepisodic Residual Sxs•• ContinuousContinuous•• ContinuousContinuous
–– With Prominent Negative SxsWith Prominent Negative Sxs
•• Single Episode in Partial RemissionSingle Episode in Partial Remission–– With Prominent Negative SxsWith Prominent Negative Sxs
•• Single Episode in Full RemissionSingle Episode in Full Remission•• Other or Unspecified PatterOther or Unspecified Patter
295.40 Schizophreniform Disorder295.40 Schizophreniform Disorder
•• Criteria A, D, and E of Schizophrenia are met Criteria A, D, and E of Schizophrenia are met (impairment in social or occupational (impairment in social or occupational functioning is not required)functioning is not required)
•• An episode lasts for: An episode lasts for: •• An episode lasts for: An episode lasts for: –– at least 1m & at least 1m & –– less than 6mless than 6m
•• Specifiers:Specifiers:–– With Good Prognostic FeaturesWith Good Prognostic Features–– Without Good Prognostic FeaturesWithout Good Prognostic Features
295.70 Schizoaffective Disorder295.70 Schizoaffective Disorder
•• Disturbance in which a mood episode and Disturbance in which a mood episode and the active phase of schizophrenia occur the active phase of schizophrenia occur together and are together and are preceded or followed by preceded or followed by at least 2 weeks of delusions or at least 2 weeks of delusions or at least 2 weeks of delusions or at least 2 weeks of delusions or hallucinationshallucinations without prominent mood without prominent mood symptomssymptoms
295.70 Schizoaffective Disorder295.70 Schizoaffective Disorder
A.A. An uninterrupted period of illness during which An uninterrupted period of illness during which there is a Major Depressive Episode, a Manic there is a Major Depressive Episode, a Manic Episode, or a Mixed Episode concurrent with Episode, or a Mixed Episode concurrent with sxs that meet Criterion A for Schizophreniasxs that meet Criterion A for Schizophreniasxs that meet Criterion A for Schizophreniasxs that meet Criterion A for Schizophrenia
Specify typeSpecify type::–– Bipolar TypeBipolar Type–– Depressive TypeDepressive Type
298.8 Brief Psychotic Disorder298.8 Brief Psychotic Disorder
A.A. Presence of one or more of the following sxs: Presence of one or more of the following sxs: delusions, hallucinations, disorganized speech, delusions, hallucinations, disorganized speech, grossly disorganized or catatonic behaviorgrossly disorganized or catatonic behavior
B.B. Duration of an episode of at least 1 day, less Duration of an episode of at least 1 day, less B.B. Duration of an episode of at least 1 day, less Duration of an episode of at least 1 day, less than 1m than 1m –– with eventual full return to with eventual full return to premorbid levels of functioning premorbid levels of functioning
Specify:Specify:–– With Marked StressorsWith Marked Stressors–– Without Marked StressorsWithout Marked Stressors–– With Postpartum Onset With Postpartum Onset
297.3 Shared Psychotic Disorder297.3 Shared Psychotic Disorder
297.3 Shared Psychotic Disorder (Folie 297.3 Shared Psychotic Disorder (Folie áá Deux) Deux) A.A. A delusion develops in an individual in the A delusion develops in an individual in the
context of a close relationship with another context of a close relationship with another person(s) who has an already established person(s) who has an already established person(s) who has an already established person(s) who has an already established delusion (delusion (primary or inducer); primary or inducer); the person who the person who develops the delusion is called develops the delusion is called secondarysecondary
B.B. The delusion is similar in content to that of the The delusion is similar in content to that of the person who already has the established person who already has the established delusiondelusion
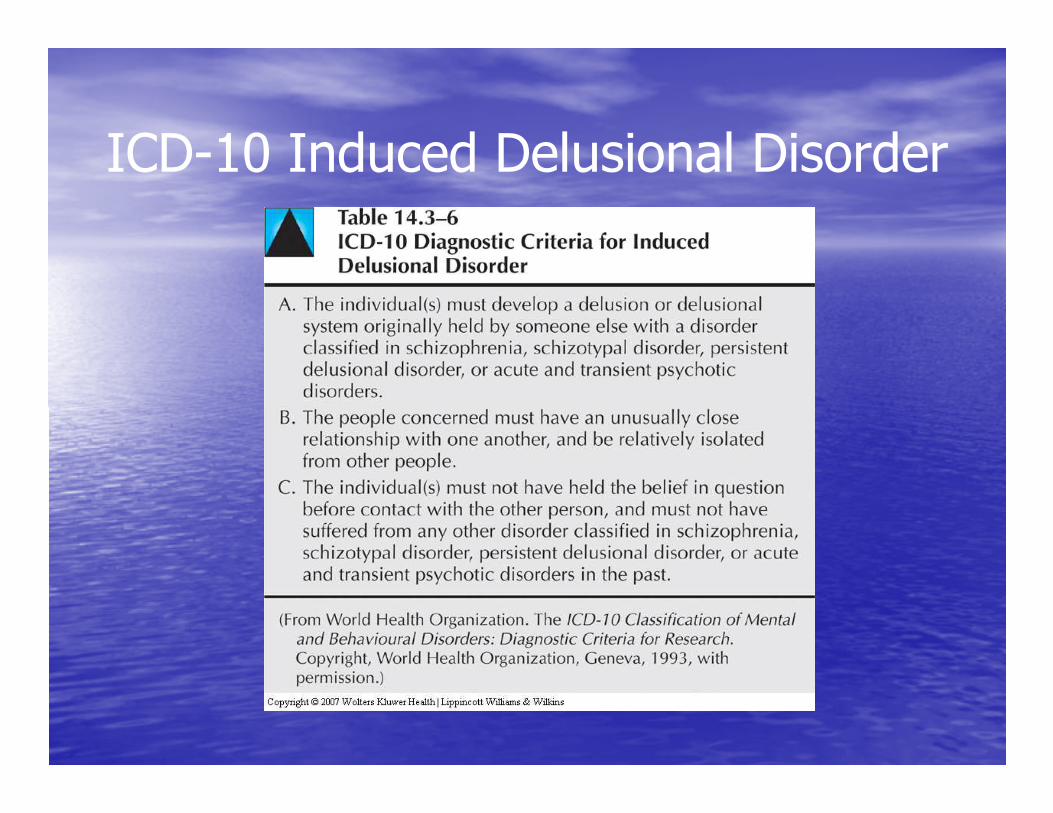
ICD-10 Induced Delusional Disorder
Examples of shared delusionsExamples of shared delusions
1.1. BizarreBizarre d. d. -- a couple is working for aliens a couple is working for aliens who will return one day and take them who will return one day and take them to their home planetto their home planet
2.2. MoodMood--congruent dcongruent d. . -- the primary is going the primary is going 2.2. MoodMood--congruent dcongruent d. . -- the primary is going the primary is going to star in a movie and make the family to star in a movie and make the family millionsmillions
3.3. NonNon--bizarre dbizarre d..-- the FBI is watching the the FBI is watching the house and tapping the phoneshouse and tapping the phones
297.1 Delusional Disorder297.1 Delusional Disorder
A.A. Nonbizarre delusions of at least 1m durationNonbizarre delusions of at least 1m durationB.B. Criterion A for Schizophrenia has never been Criterion A for Schizophrenia has never been
met (tactile and olfactory hallucinations may met (tactile and olfactory hallucinations may be present if related to the delusional theme)be present if related to the delusional theme)be present if related to the delusional theme)be present if related to the delusional theme)
C.C. Apart from the impact of the delusion(s) or its Apart from the impact of the delusion(s) or its ramifications, functioning is not markedly ramifications, functioning is not markedly impaired and behavior is not obviously odd or impaired and behavior is not obviously odd or bizarrebizarre
D.D. If mood episode occur, they are briefIf mood episode occur, they are brief
297.1 Delusional Disorder297.1 Delusional Disorder
Specify type Specify type (based on predominant delusional theme)(based on predominant delusional theme)
–– Erotomanic TypeErotomanic Type–– Grandiose TypeGrandiose Type–– Jealous TypeJealous Type–– Persecutory TypePersecutory Type–– Somatic TypeSomatic Type–– Mixed TypeMixed Type–– Unspecified TypeUnspecified Type
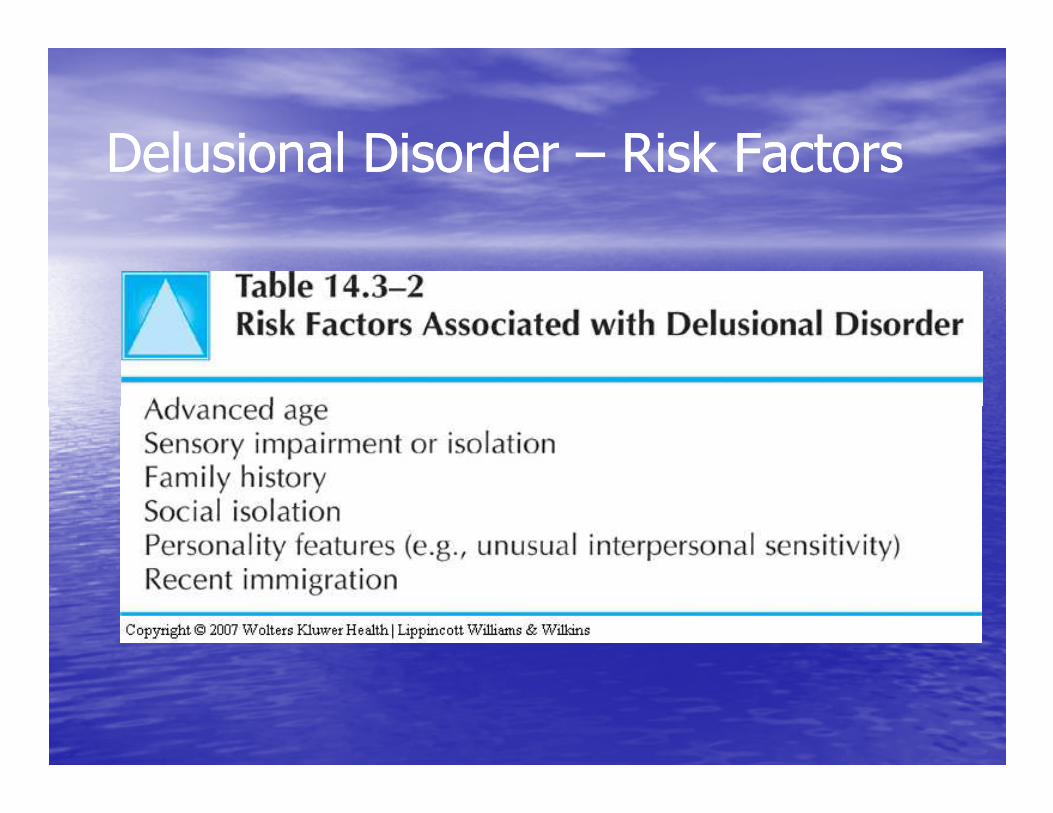
Delusional Disorder Delusional Disorder –– Risk FactorsRisk Factors
Types of delusions Types of delusions (categorized by content)(categorized by content)
•• BizarreBizarre dd.= a delusion that involves a .= a delusion that involves a phenomenon that the person’s culture phenomenon that the person’s culture would regard as totally implausiblewould regard as totally implausible
•• Delusional jealousyDelusional jealousy = the delusion that = the delusion that •• Delusional jealousyDelusional jealousy = the delusion that = the delusion that one’s partner is unfaithfulone’s partner is unfaithful
•• Erotomanic dErotomanic d. = a delusion that another . = a delusion that another person, usually of higher status, is in love person, usually of higher status, is in love with the individualwith the individual
Types of delusions Types of delusions (categorized by content)(categorized by content)
•• Grandiose dGrandiose d. = a delusion of inflated worth, . = a delusion of inflated worth, power, knowledge, identity, or special power, knowledge, identity, or special relationship to a deity or famous personrelationship to a deity or famous person
•• MoodMood--congruent dcongruent d. = content is consistent with . = content is consistent with typical themes of a typical themes of a depresseddepressed (e.g., inadequacy, (e.g., inadequacy, guilt, disease) or guilt, disease) or manic manic (power, special (power, special relationship with a deity, etc.) moodrelationship with a deity, etc.) mood
Types of delusions Types of delusions (categorized by content)(categorized by content)
•• MoodMood--incongruent dincongruent d. = content not . = content not consistent with typical themes of consistent with typical themes of depressed or manic mooddepressed or manic mood
•••• D. of being controlledD. of being controlled = a delusion in = a delusion in which feelings, impulses, thoughts, or which feelings, impulses, thoughts, or actions are experienced as being under actions are experienced as being under the control of some external force rather the control of some external force rather than being under one’s own controlthan being under one’s own control
Types of delusions Types of delusions (categorized by content)(categorized by content)
•• D. of referenceD. of reference = a delusion whose theme is = a delusion whose theme is that events, objects, or other persons in one’s that events, objects, or other persons in one’s immediate environment have a particular and immediate environment have a particular and unusual significance (usually negative)unusual significance (usually negative)unusual significance (usually negative)unusual significance (usually negative)
•• Persecutory dPersecutory d. = a delusion in which the central . = a delusion in which the central theme is that one is being attacked, harassed, theme is that one is being attacked, harassed, cheated, persecuted, or conspired againstcheated, persecuted, or conspired against
Types of delusions Types of delusions (categorized by content)(categorized by content)
•• Somatic dSomatic d. = a delusion whose main . = a delusion whose main content pertains to the appearance or content pertains to the appearance or functioning of one’s bodyfunctioning of one’s body
•••• Thought broadcastingThought broadcasting = the delusion that = the delusion that one’s thoughts are being broadcasted out one’s thoughts are being broadcasted out loud so that they can be perceived by loud so that they can be perceived by othersothers
Types of delusions Types of delusions (categorized by content)(categorized by content)
•• Thought insertionThought insertion = the delusion that = the delusion that certain of one’s thoughts are not one’s certain of one’s thoughts are not one’s own, but rather are inserted into one’s own, but rather are inserted into one’s mindmindmindmind
Other Psychotic DisordersOther Psychotic Disorders
•• 293.xx Psychotic Disorder Due to [293.xx Psychotic Disorder Due to [Indicate Indicate the General medical Condition…]the General medical Condition…]–– .81 With Delusions.81 With Delusions–– .81 With Delusions.81 With Delusions–– .82 With Hallucinations.82 With Hallucinations
•• SubstanceSubstance--Induced Psychotic DisorderInduced Psychotic Disorder•• 298.9 Psychotic Disorder NOS298.9 Psychotic Disorder NOS
Etiological theories for schizophreniaEtiological theories for schizophrenia
The cause The cause The cause The cause of schizophrenia of schizophrenia is not known!is not known!
Etiological theories for schizophreniaEtiological theories for schizophrenia
•• Biological factorsBiological factors–– Genetic Genetic –– twin & adoption studiestwin & adoption studies–– Neurochemical hypothesisNeurochemical hypothesis–– NeuropathologyNeuropathology–– NeuropathologyNeuropathology
•• PsychoPsycho--social factorssocial factors–– Psychoanalytic/psychodynamic & learningPsychoanalytic/psychodynamic & learning–– Social (industrialization, crowding) & psychoSocial (industrialization, crowding) & psycho--social/familysocial/family
•• StressStress--DiathesisDiathesis
Neurochemical hypothesisNeurochemical hypothesis
•• Dopamine hypothesisDopamine hypothesis: Schizophrenia results : Schizophrenia results from too much dopaminergic activity. from too much dopaminergic activity. –– Efficacy & potency of antipsychotics appear to Efficacy & potency of antipsychotics appear to be related to their ability to act as be related to their ability to act as be related to their ability to act as be related to their ability to act as dopaminergic antagonists. dopaminergic antagonists.
–– Drugs that increase dopaminergic activity Drugs that increase dopaminergic activity (e.g., amphetamines) act as psychotomimetic (e.g., amphetamines) act as psychotomimetic drugs (i.e., they can produce schizophreniadrugs (i.e., they can produce schizophrenia--like symptoms)like symptoms)
Neurochemical hypothesisNeurochemical hypothesis
•• Other neurotransmittersOther neurotransmitters::–– NorepinephrineNorepinephrine: it appears that abnormalities : it appears that abnormalities in the noradrenergic system predisposes to in the noradrenergic system predisposes to relapsesrelapsesrelapsesrelapses
–– GABA aminoGABA amino--acid: loss of inhibitory GABAacid: loss of inhibitory GABA--ergic neurons in the hippoocampus may lead ergic neurons in the hippoocampus may lead to hyperactivity of dopaminergic and to hyperactivity of dopaminergic and noradrenergic neuronsnoradrenergic neurons
NeuropathologyNeuropathology
•• Major brain areas implicated in schizophrenia:Major brain areas implicated in schizophrenia:–– Limbic structuresLimbic structures –– hippocampus hippocampus (disorganization of neurons)(disorganization of neurons)
–– Frontal lobesFrontal lobes –– poor blood flowpoor blood flow–– Frontal lobesFrontal lobes –– poor blood flowpoor blood flow–– Basal gangliaBasal ganglia (involved in the control of (involved in the control of movement)movement)
–– Temporal lobesTemporal lobes –– smallersmaller–– Thalamus & cerebellumThalamus & cerebellum –– loss of neuronsloss of neurons
Brain imagingBrain imaging
•• Computed tomographyComputed tomography (CT) (CT) -- lateral and third lateral and third ventricular enlargementventricular enlargement (by 40%) (by 40%) –– suggesting suggesting atrophy of brain tissue; some degree of atrophy of brain tissue; some degree of reduction in brain and cortical volume; brain reduction in brain and cortical volume; brain reduction in brain and cortical volume; brain reduction in brain and cortical volume; brain density changes (abnormalities not specific & density changes (abnormalities not specific & unique to schizophrenia!!!)unique to schizophrenia!!!)
•• Magnetic Resonance ImagingMagnetic Resonance Imaging (MRI) (MRI) -- enlarged enlarged ventriclesventricles
Brain imagingBrain imaging
•• Positron Emission TomographyPositron Emission Tomography (PET): measures (PET): measures glucose utilization or cerebral blood flow glucose utilization or cerebral blood flow --findings of findings of hypoactivity of the frontal lobeshypoactivity of the frontal lobes
•• Functional MRI & Functional MRI & Single photon emission Single photon emission •• Functional MRI & Functional MRI & Single photon emission Single photon emission tomographytomography (SPECT) (SPECT) -- blood flow, energy blood flow, energy consumption, chemical activityconsumption, chemical activity
•• Magnetic Resonance SpectroscopyMagnetic Resonance Spectroscopy (MRS): (MRS): metabolic hypoactivity in the prefrontal cortexmetabolic hypoactivity in the prefrontal cortex
Other biological hypothesesOther biological hypotheses
•• Electrophysiology Electrophysiology (EEG): high # of patients with (EEG): high # of patients with schizophrenia have abnormal records schizophrenia have abnormal records --decreased alpha activitydecreased alpha activity, more than usual , more than usual epileptiform activity, unusually epileptiform activity, unusually high sensitivity to high sensitivity to epileptiform activity, unusually epileptiform activity, unusually high sensitivity to high sensitivity to sensory stimulisensory stimuli
•• Eye movement disorderEye movement disorder (of smooth visual (of smooth visual pursuit) pursuit) –– inability to follow a moving target in inability to follow a moving target in 50% to 85% of patients with schizophrenia 50% to 85% of patients with schizophrenia
Other biological hypothesesOther biological hypotheses
•• PsychoneuroimmunologyPsychoneuroimmunology: immunologic : immunologic abnormalitiesabnormalities
•• Psychoneuroenndocrinology: Psychoneuroenndocrinology: hormonal hormonal •• Psychoneuroenndocrinology: Psychoneuroenndocrinology: hormonal hormonal abnormalities seem to be present and to abnormalities seem to be present and to correlate with poor prognosiscorrelate with poor prognosis
•• GeneticsGenetics: heterogeneous genetic basis: heterogeneous genetic basis
Psychoanalytic theoryPsychoanalytic theory
•• Schizophrenia results from Schizophrenia results from earlier fixationsearlier fixations in in development than in neurosesdevelopment than in neuroses
•• Freud postulated Freud postulated ego defectsego defects responsible for responsible for poor ego integration & a regressive response to poor ego integration & a regressive response to poor ego integration & a regressive response to poor ego integration & a regressive response to overwhelming environmental stressorsoverwhelming environmental stressors
•• Harry Stack Sullivan postulated Harry Stack Sullivan postulated early early interpersonal difficultiesinterpersonal difficulties related to overanxious related to overanxious mothering as schizophrenogenicmothering as schizophrenogenic
Psychodynamic theoryPsychodynamic theory
•• Constitutional hypersensitivity to perceptual Constitutional hypersensitivity to perceptual stimulistimuli is a deficit (i.e., a is a deficit (i.e., a defective stimuli defective stimuli barrierbarrier) that creates difficulty throughout ) that creates difficulty throughout barrierbarrier) that creates difficulty throughout ) that creates difficulty throughout development.development.
•• Psychotic symptoms have Psychotic symptoms have symbolic meaningsymbolic meaning for for the patient.the patient.
Learning theoriesLearning theories
•• Children Children imitate their parentsimitate their parents; they learn ; they learn irrational ways of thinking and acting from irrational ways of thinking and acting from parents who experience pathology themselves.parents who experience pathology themselves.parents who experience pathology themselves.parents who experience pathology themselves.
•• Poor modelsPoor models result in poor interpersonal result in poor interpersonal relationships.relationships.
Family theoristsFamily theorists
•• Communication deficitsCommunication deficits such as the such as the doubledouble--bind patterns of interaction bind patterns of interaction (Gregory Bateson)(Gregory Bateson)
•••• Schisms & skewed familiesSchisms & skewed families: one parent : one parent gets too close to a child of the opposite gets too close to a child of the opposite sex; child involved in the parental power sex; child involved in the parental power struggle (Theodore Lidz) struggle (Theodore Lidz)
Family theoristsFamily theorists
•• Pseudomutual & pseudohostile familiesPseudomutual & pseudohostile families: : maintain a façade of harmony, isolation from the maintain a façade of harmony, isolation from the outside, hostility not expressed openly (Lyman outside, hostility not expressed openly (Lyman Wynne)Wynne)Wynne)Wynne)
•• Expressed emotionsExpressed emotions (EE): high level of (EE): high level of expressed negative emotions (i.e., criticism, expressed negative emotions (i.e., criticism, hostility, overinvolvement)hostility, overinvolvement)
StressStress--diathesis modeldiathesis model
The model integrates biological, psychosocial The model integrates biological, psychosocial and environmental factors. It postulates that a and environmental factors. It postulates that a person’s vulnerability (person’s vulnerability (diathesisdiathesis) to develop ) to develop schizophrenia may be triggered by schizophrenia may be triggered by stressstress and and schizophrenia may be triggered by schizophrenia may be triggered by stressstress and and consequently the person develops the symptoms consequently the person develops the symptoms of schizophrenia. Both the diathesis and the of schizophrenia. Both the diathesis and the stress can be either biological or environmental stress can be either biological or environmental or both.or both.
Meehl, 1962Meehl, 1962
Treatment of schizophreniaTreatment of schizophrenia
From ancient times, treatments of schizophrenia From ancient times, treatments of schizophrenia have ranged from kindness have ranged from kindness have ranged from kindness have ranged from kindness and soothing medication, and soothing medication, to cruelty, to cruelty, various restraints various restraints
and death.and death.
Treatment of schizophrenia Treatment of schizophrenia in the 20in the 20thth century century -- beginningbeginning
–– It was widely believed that schizophrenia was It was widely believed that schizophrenia was incurable.incurable.
–– FreudFreud expressed a pessimistic view on the expressed a pessimistic view on the –– FreudFreud expressed a pessimistic view on the expressed a pessimistic view on the treatment of patients with schizophreniatreatment of patients with schizophrenia
–– Jung and AdlerJung and Adler reported successes in treating reported successes in treating patients with schizophreniapatients with schizophrenia
Treatment of schizophrenia Treatment of schizophrenia in the 20in the 20thth century century –– 1930s1930s
Interpersonal paradigmInterpersonal paradigm•• Harry Stack Sullivan & Frieda FrommHarry Stack Sullivan & Frieda Fromm--ReichmanReichmanreported successful outcome with modified reported successful outcome with modified versions of psychoanalytic technique versions of psychoanalytic technique –– based on based on versions of psychoanalytic technique versions of psychoanalytic technique –– based on based on building a relationship with the patient building a relationship with the patient –– at at Chestnut Lodge, Rockville, MarylandChestnut Lodge, Rockville, Maryland
•• McLean Hospital, Belmont, MassachusettsMcLean Hospital, Belmont, Massachusetts•• Austen Riggs Center, Stockbridge, MAAusten Riggs Center, Stockbridge, MA
Treatment of schizophrenia Treatment of schizophrenia in the 20in the 20thth century century –– 1940s1940s
Organic psychiatryOrganic psychiatry developed drastic treatments developed drastic treatments with reported good outcomeswith reported good outcomes–– Insulin comaInsulin coma –– Manfred Sakel, 1938Manfred Sakel, 1938–– Artificial epileptic seizuresArtificial epileptic seizures with metrazolwith metrazol–––– Artificial epileptic seizuresArtificial epileptic seizures with metrazolwith metrazol––Meduna, 1939Meduna, 1939
–– Electric shock treatmentElectric shock treatment (ECT) (ECT) –– Cerletti & Cerletti & Bini, 1950Bini, 1950
–– Prefrontal lobotomyPrefrontal lobotomy (psychosurgery) (psychosurgery) ––Antonio de Egas Monis (Nobel prize, 1949)Antonio de Egas Monis (Nobel prize, 1949)
Treatment of schizophrenia Treatment of schizophrenia in the 20in the 20thth century century –– 1950s1950s
•• Two professions of psychiatry promoted two Two professions of psychiatry promoted two directions of treatmentdirections of treatment–– PsychodynamicPsychodynamic–– Organic/biomedicalOrganic/biomedical –– controlled studies controlled studies –– Organic/biomedicalOrganic/biomedical –– controlled studies controlled studies demonstrated the effectiveness of demonstrated the effectiveness of neuroleptic drugsneuroleptic drugs in reducing sxs in acutely in reducing sxs in acutely ill patients & reducing relapse rates in ill patients & reducing relapse rates in recovered or clinically stable patientsrecovered or clinically stable patients
Treatment of schizophrenia Treatment of schizophrenia in the 20in the 20thth century century –– ‘60s ‘60s –– ’70s’70s
•• Comparative treatment studies consistently Comparative treatment studies consistently found found psychopharmacotherapy to be superior to psychopharmacotherapy to be superior to individual psychotherapyindividual psychotherapy. .
•• California study demonstrated that medication California study demonstrated that medication •• California study demonstrated that medication California study demonstrated that medication should be the treatment of choice for should be the treatment of choice for schizophrenia was the (May, 1968). schizophrenia was the (May, 1968).
•• It is now axiomatic that It is now axiomatic that schizophrenic patients schizophrenic patients must be treated with antipsychotic (neuroleptic) must be treated with antipsychotic (neuroleptic) medicationmedication
Treatment of schizophrenia Treatment of schizophrenia in the 20in the 20thth century century –– 1980s1980s
•• Psychotherapeutic interventions were viewed as Psychotherapeutic interventions were viewed as irrelevant.irrelevant.
•• The effectiveness of acute The effectiveness of acute neuroleptic drug neuroleptic drug treatmentstreatments was indisputable. was indisputable. treatmentstreatments was indisputable. was indisputable. –– Well documented adverse side effects Well documented adverse side effects (estimates vary from 5% to 90%)(estimates vary from 5% to 90%)
–– Negative symptoms were not helped by Negative symptoms were not helped by medicationmedication
Neurological side effects of neurolepticsNeurological side effects of neuroleptics
•• Extrapyramidal (EPS) Extrapyramidal (EPS) -- extrapyramidal extrapyramidal movement disordersmovement disorders–– DystoniaDystonia–– ParkinsonismParkinsonism–– ParkinsonismParkinsonism–– Akathisia Akathisia -- restlessness, insects crawling restlessness, insects crawling under the skinunder the skin
–– Tardive dyskinesia (TD) = behvioral syndrome Tardive dyskinesia (TD) = behvioral syndrome of the mouth and tongue movements of the mouth and tongue movements
Other side effects of neurolepticsOther side effects of neuroleptics
•• Pharmacokinetic or akinetic depressionPharmacokinetic or akinetic depression (drug(drug--induced dysphoric affect)induced dysphoric affect)
•• Neuroleptic malignant syndromeNeuroleptic malignant syndrome -- rare, with rare, with •• Neuroleptic malignant syndromeNeuroleptic malignant syndrome -- rare, with rare, with potentially lethal complicationspotentially lethal complications
•• Tardive dementiaTardive dementia and and tardive dysmentiatardive dysmentia•• Tardive psychosisTardive psychosis
Treatment of schizophrenia Treatment of schizophrenia in the 20in the 20thth century century –– 1990s1990s
•• Rising interest in the treatment of Rising interest in the treatment of negative negative symptomssymptoms of schizophrenia.of schizophrenia.
•• The introduction of clozapine (The introduction of clozapine (ClozarilClozaril) ) -- an an atypical antipsychotic drug with minimal atypical antipsychotic drug with minimal atypical antipsychotic drug with minimal atypical antipsychotic drug with minimal neurological side effects & more effective in neurological side effects & more effective in reducing negative symptomsreducing negative symptoms
•• Recognition of the Recognition of the role played by psychosocial role played by psychosocial factorsfactors in the onset, course and prognosis of in the onset, course and prognosis of schizophreniaschizophrenia
Treatment of schizophrenia Treatment of schizophrenia in the 20in the 20thth century century –– 1990s1990s
•• HospitalizationHospitalization -- for stabilization/restoring for stabilization/restoring functioning: medication, education about the functioning: medication, education about the disorder (symptoms, course), safe environment, disorder (symptoms, course), safe environment, reduced stress; practical orientation towards reduced stress; practical orientation towards reduced stress; practical orientation towards reduced stress; practical orientation towards living following dischargeliving following discharge
•• Behavioral therapyBehavioral therapy: social skills training; token : social skills training; token economy; milieu; pyschoeducation; vocational economy; milieu; pyschoeducation; vocational rehabilitationrehabilitation
Treatment of schizophrenia Treatment of schizophrenia in the 20in the 20thth century century –– 1990s1990s
•• Somatic treatmentsSomatic treatments: : antipsychotics antipsychotics (major (major tranquilizers) tranquilizers) -- clozapine, risperidone & clozapine, risperidone & dopamine receptor antagonists (serious adverse dopamine receptor antagonists (serious adverse sideside--effects); effects); sideside--effects); effects);
•• Therapeutic principlesTherapeutic principles: define target sxs; use a : define target sxs; use a previously effective drug; trial of minimum 4previously effective drug; trial of minimum 4--6 6 weeks; combination of medications in tx weeks; combination of medications in tx resistant patients; maintain on lowest possible resistant patients; maintain on lowest possible dosage (major reason for relapse is dosage (major reason for relapse is noncompliance with medication regimen)noncompliance with medication regimen)
Fountain House MissionFountain House Mission
“Fountain House is dedicated to the “Fountain House is dedicated to the recovery of men and women with mental recovery of men and women with mental illness by providing opportunities for our illness by providing opportunities for our illness by providing opportunities for our illness by providing opportunities for our members to live, work and learn, while members to live, work and learn, while contributing their talents through a contributing their talents through a community of mutual support.”community of mutual support.”
Fountain House OrganizationFountain House OrganizationDaily operation of the clubhouse Daily operation of the clubhouse –– unitsunits•• Clerical UnitClerical Unit•• First Floor Unit First Floor Unit –– receptionist areareceptionist area•• Horticulture Horticulture •• Horticulture Horticulture •• Dining roomDining room•• Snack BarSnack Bar•• Interpreter’s Corner Interpreter’s Corner –– deaf & hard of hearingdeaf & hard of hearing

Fountain HouseFountain House
Fountain House Fountain House –– the organizationthe organizationhttp://www.fountainhouse.orghttp://www.fountainhouse.org
Fountain House artistsFountain House artistshttp://www.fountaingallerynyc.com/Artist.cfmhttp://www.fountaingallerynyc.com/Artist.cfm
ReferencesReferences
• American Psychiatric Association (2000). Diagnostic and statistical manual of mental disorders, (4th ed., Text Revision).Washington, DC: Author.Washington, DC: Author.
• Castillo, R. J. (1997). Culture and mental illness. A client-centered approach. New York: Brooks/Cole.
ReferencesReferences
• Sadock, B. J., & Sadock, V. A. (2007). Kaplan & Sadock’s synopsis of psychiatry (10th ed.). Baltimore, Maryland: Williams and Wilkins. and Wilkins.
















![MaintenanceElectroconvulsiveTherapyin ... · paranoid schizophrenia (F20.0) according to the criteria of the International Classification of Diseases (ICD-9 [8], after admission](https://img.pdfslide.us/doc/110x75/60b452a268241249d5389fa9/maintenanceelectroconvulsivetherapyin-paranoid-schizophrenia-f200-according.jpg)