Embed Size (px)
Citation preview
Defining the CiPA Paradigm: An Update from the Ion Channel Working Group
(ICWG)
Bernard FerminiPfizer Inc.
Global Safety PharmacologyFor the ICWG
Ion Channel Working Group (ICWG)
• CiPA initiative is a consortium composed of a number of collaborators• FDA, HESI, CSRC, National Institute of Health Sciences (NIHS, Japan), Health
Canada, European Medicines Agency (EMA), Pharmaceutical and Medical Devices Agency (PMDA, Japan)
• Safety Pharmacology Society (SPS), Japan iPS Cardiac Safety Assessment (JiCSA), academics, in silico modelers
• Partners from Pharmaceutical Industry, CROs, Device companies
• ICWG (sponsored by SPS)• Builds on the considerable experience and expertise of its members in the field of
ion channels• Task with bringing together expertise and resources required to deliver best
practice recommendations for generating ion channel data • Ion Channel data needed for
• development and validation of best in silico model of human ventricular action potentials ( AP) simulations of proarrhythmic liabilities
• Co-chaired: Bernard Fermini (Pfizer); Najah Abi-Gerges (Anabios)
2
3
• Current pre-clinical guidelines (S7B) are just that: guidance and not dogma
• Allow flexibility both in measurement platform, and experimental protocol
• As a result, pre-clinical safety profiling can differ from company to company, despite adopting the same guidelines
• There is a diversity of automated patch clamp systems available offering various levels of performance, leading to some variability in the quality of data generated
• The lack of standardization in the protocols used within the industry and in the academic environment contributes to variability of data
• Current cardiac ion channel safety screening strategies focus on conductance block in an effort to define potency (IC50) however;
• kinetic of drug block can influence use- and voltage- dependency
• Evaluation of kinetic of block may lead to more complex, but more predictive in silico models
• It is therefore important to establish best practices for IC studies used to characterize drug effects (voltage protocols, temperature, reagents, etc…) so that consistent electrophysiological data may be obtained, and contribute to better prediction of proarrhythmic risk
Pre-CiPA state of Ion Channel testing
4
Objectives of ICWG
Address important questions related to best practices including:
1. Which ion channels should be selected to support in silico working group (ISWG) AP modelling efforts
2. What properties should be studied (IC50 determination, kinetics, rate/use/voltage dependence, etc…)?
3. What requirements are needed to deliver robust, reliable and reproducible ion channel data in a high throughput screening (HTS) environment

5
ICWG Deliverables (1)
Which ion channels should be selected to support in silico working group (ISWG) AP modelling efforts
• ICWG conducted and completed a survey with the purpose of collecting frequency/type data on the commonly used ion channels (ICs) in the various laboratories

6
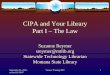
Pre-CiPA state of Ion Channel testingCardiac ion channels screened for safety (n=65)
63
24
913
85
39
2
36
11
0
10
20
30
40
50
60
70
7
ICWG Deliverables (1)
Which ion channels should be selected to support in silico working group (ISWG) AP modelling efforts
• ICWG conducted and completed a survey with the purpose of collecting frequency/type data on the commonly used ion channels (ICs) in the various laboratories
• ICWG identified 7 ICs of interest: ‒ Selected outward currents: IKr (hERG), IKs (KvLQT1/KCNE1), Ito (Kv4.3)‒ Selected inward currents: IK1 (Kir2.1), ICa-L (Cav1.2), INa (Nav1.5; peak and
late)

8
0
5
10
15
20
25
30
35
40
45
50
Room Temperature
Physiologic Temperature
Other
Pre-CiPA state of Ion Channel testingTemperature at which assays are performed (n=54)

9
ICWG Deliverables (2)
What properties should be studied? (IC50 determination, kinetics, rate/use/voltage dependence, etc…)
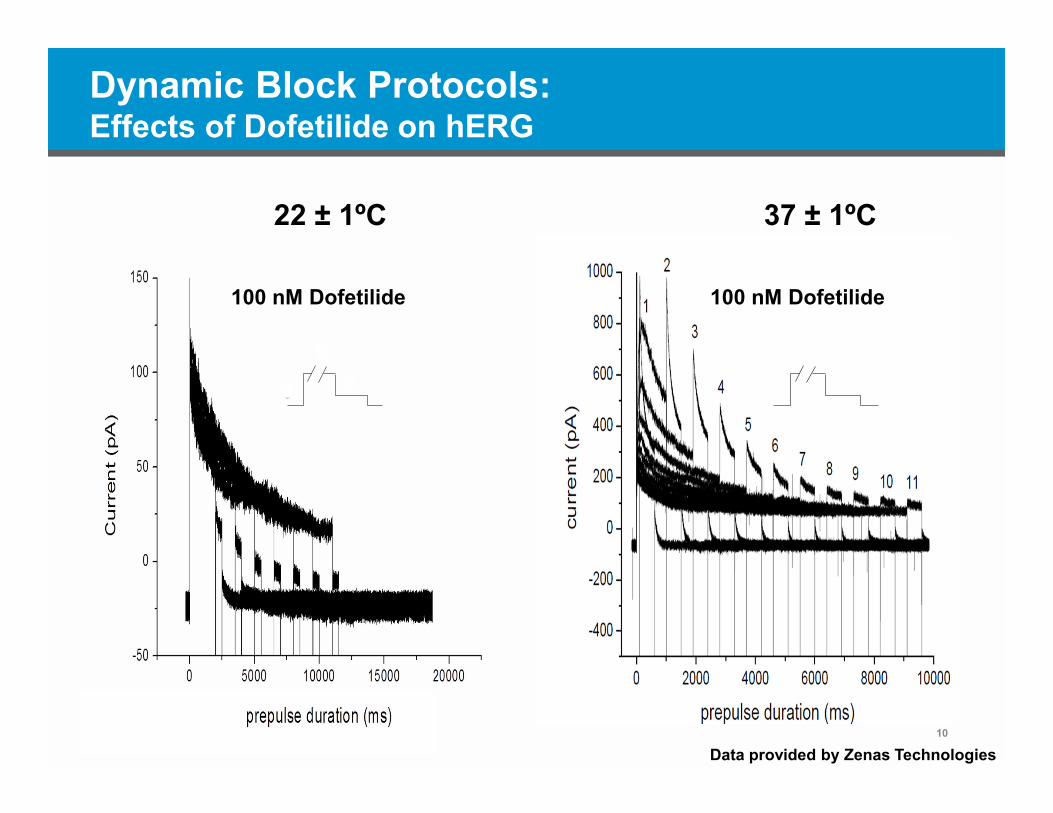
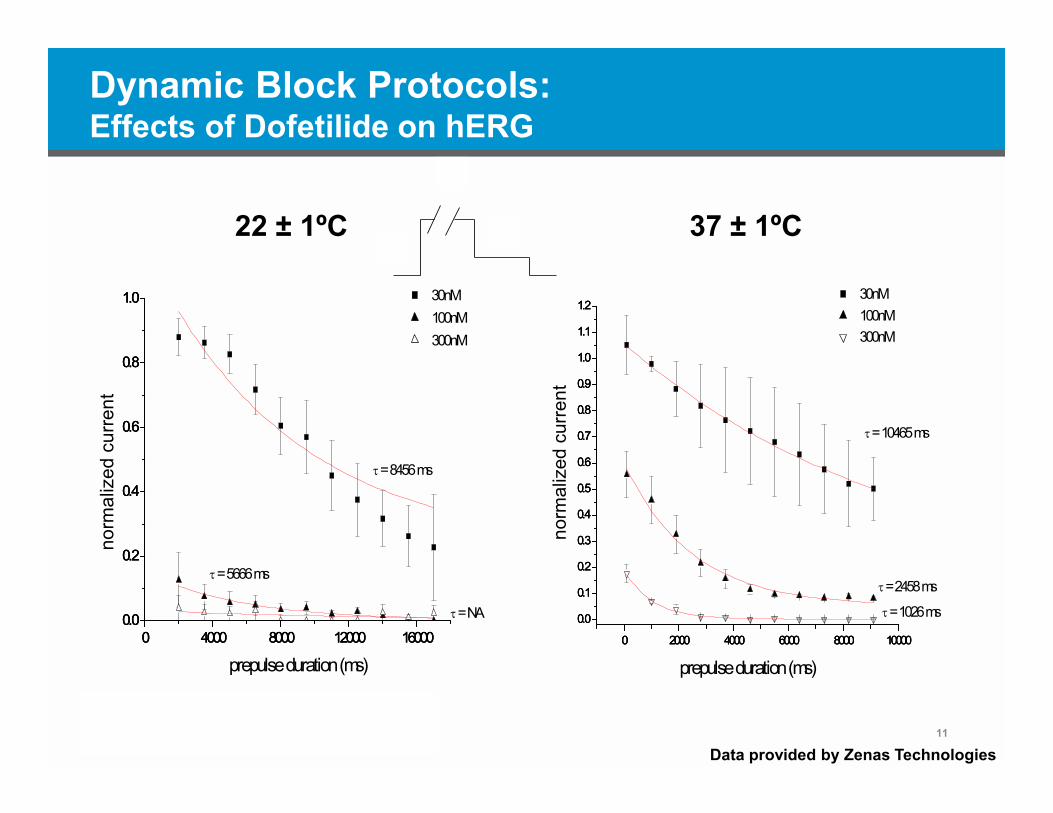
ICWG designed and delivered two sets of protocols for all 7 ICs 1. “Dynamic block” protocols that provide data on affinity, kinetics and state-
dependence of drug-channel interaction • To be used by ISWG• Keep the process simple: use protocols that are not overly complicated or challenging to
apply experimentally • Parametrize hERG as a first step • Dofetilide, cisapride and verapamil data generated • Data generated at RT and 37ºC• Work in progress
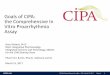
2. “Physiological” protocols that provide data on IC50, voltage/rate/use-dependence, activation/inactivation/deactivation rates• To be used in FDA sponsored study (David Strauss Lead)• Data to be generated at RT and 37°C• Pacing rates: 0.1 and 1 Hz• Some data obtained using Action Potential voltage protocol • Work in progress
22 ± 1ºC 37 ± 1ºC
10
a
b
d
Dynamic Block Protocols:Effects of Dofetilide on hERG
a
b
d
100 nM Dofetilide 100 nM Dofetilide
Data provided by Zenas Technologies
22 ± 1ºC 37 ± 1ºC
11
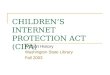
0 4000 8000 12000 160000.0
0.2
0.4
0.6
0.8
1.0
0 4000 8000 12000 160000.0
0.2
0.4
0.6
0.8
1.0
0 4000 8000 12000 160000.0
0.2
0.4
0.6
0.8
1.0 100nM
= NA
= 5666 ms
= 8456 ms
300nM
norm
aliz
ed c
urre
nt
prepulse duration (ms)
30nM
0 2000 4000 6000 8000 10000
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
1.1
1.2
0 2000 4000 6000 8000 10000
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
1.1
1.2
0 2000 4000 6000 8000 10000
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
1.1
1.2
= 10465 ms
= 1026 ms
= 2458 ms
300nM 100nM
norm
aliz
ed c
urre
nt
prepulse duration (ms)
30nM
Dynamic Block Protocols:Effects of Dofetilide on hERG
a
b
d
Data provided by Zenas Technologies

Physiological Protocols: some examplesIto (Kv4.3); IKs (KvLQT1); INa (Nav1.5)
12

Physiological Protocol ParametersAll channels
13
ICWG Protocols
Protocol HP (mV)
HP (ms)
Ramp to
(mv)
Ramp (ms)
Ramp (V/S)
Step1 (mV)
Step 1 (ms)
Step 2 (mV)
Step 2 (ms)
Ramp to (mV)
Ramp (ms)
Ramp (V/S)
Frequency (Hz)
IKr (hERG) -80 50 40 500 -80 100 1.2 TBD
IK1 (Kir2.1) -80 50 20 500 -120 115 1.2 TBD
IKs (KvLQT1/KCNE1) -80 50 60 5000 -80 115 1.2 TBD
Ito (Kv4.3) -80 50 40 10 12 40 100 -80 100 1.2 TBD
INa peak (Nav1.5) -80 50 -15 40 40 200 -80 100 1.2 TBD
INa late (Nav1.5) -80 50 -15 40 40 200 -80 100 1.2 TBD
ICa-L (Cav1.2) -80 50 0 40 30 200 -80 100 1.2 TBD

CiPA Impact on preclinical testing
• Change the manner in which cardiac safety assessment is performed in the pharmaceutical industry
• Allow standardization of all in vitro ion channel assays to characterize drug effects on cardiac repolarization
• Minimize intra- and inter-laboratory variability• Prevent early inappropriate compound attrition due to hERG liability• Provide a complete assessment of proarrhythmic risk • Likely reduce animal work• Make available a single, common, and fully validated in silico model to
quantify the risk of arrhythmia based on the ion channel data• Allow sharing of knowledge and expertise with a common goal: defining best
practice• Accomplish what the S7B guidance was unsuccessful in achieving
14
15
ICWG Next Steps
• Work closely with ISWG, and FDA.– Provide feedback and scientific input/support.– Rapid Response Team established to provide timely feedback
• Revise/modify/optimize protocols, as required‒ Only the most informative protocols will be retained as final‒ Likely that the list of 7 targeted channels will narrow once their role as
contributing to proarrhythmia are confirmed, or not
• Coordinate the generation of additional ion channel pharmacology from CiPA list using standardized protocols (IC50 + dynamic block)
• Adapt protocols to HT screening environment
• Publish the work
Conclusions
• The time has come to consider new, more comprehensive ways of preclinical testing for proarrhythmic risks
• Evolving initiative with evolving workflows addressing extremely complex issues
• Will require scientific, intellectual and practical contributions from multiple parties
• Will likely require multiple iterations before it reaches a point of applicability
• Important initiative that should be supported by all involved in cardiac safety
16
17
CiPA/SPS Ion Channel Working Group (ICWG)
Membership Affiliation Najah Abi Gerges Anabios (co-chair)Matthew Bridgland-Taylor AstraZenecaKhuram Chaudhary GSK William Crumb Zenas Technologies Bruce Damiano Janssen Gul Erdemli Novartis Bernard Fermini Pfizer Inc (co-chair)Gary Gintant AbbVie Jules C Hancox Bristol University John Imredy Merck & CoJohn Koerner FDA Jim Kramer Chantest/CRL Derek J Leishman LillyPaul Levesque BMS Anders Lindqvist Biolin Scientific Carlos Obejero-Paz Chantest/CRLDavid Rampe SanofiKohei Sawada EisaiDavid Strauss FDAJamie Vandenberg Victor Chang Cardiac Research InstituteHugo Vargas Amgen